Burns
17
AT-A-GLANCE
■ Burns are common in adults and kids; most are small and managed in the outpatient setting with dressing changes.
■ Serious burns require inpatient care, ideally in a verified burn center.
■ Large burns are managed in 4 general phases:
■ Initial evaluation and resuscitation.
■ Wound debridement and biologic closure.
■ Rehabilitation and reconstruction.
■ Long-term outcome quality tends to be very good in patients surviving large burns.
EPIDEMIOLOGY
In the year 2016, 486,000 patients in the United States received medical care for burns. In other words, 3 of every 3000 persons in the United States sustained a burn injury requiring medical attention.1 Although the incidence of burn injury appears large, it has actually decreased by 60% since the early 1990s as the result of safety implementations, reduction in tobacco use and alcohol abuse, prevention education programs, change in home cooking practices, and decreased industrial employment.2 Although some professions carry an increased risk of burn injury, the majority of burns occur at home. Males sustain the majority of burn injuries, and are twice as likely as females to require admission to a specialized burn center. Sadly, almost every 2.5 hours someone dies as a result of a fire, making the likelihood of fire-related death in the United States 1.5:1000.1
Of all United States patients receiving medical care for burns, only 5% to 10% are hospitalized for burn care, illustrating the tremendous role of outpatient care in the management of disease burden.1,3 While not all of the other 90% to 95% patients receiving medical care for burns will require outpatient followup, of those who do, 30% will ultimately be admitted to the hospital for pain management or surgery (thus the importance of educating outpatient providers). Outpatient providers are most familiar with scald burns, as this is the most common mechanism of injury in the outpatient setting, whereas flame burns are the majority of inpatient burns.4 Only 60% of hospitalized burn patients receive care at one of the 128 burn centers in the United States, which average about 200 patients per burn center each year. The organization of specialized, accredited burn centers has been arguably the most effective intervention in improving mortality of burn patients in the last half-century, with burn center survival rates now higher than 96%.1,5
Worldwide, burn injury poses a far more dramatic societal burden with much less optimistic outcomes. Yearly, 11 million people require treatment for burn injuries—more than the combined incidence of tuberculosis and HIV, and slightly less than the incidence of all combined malignant neoplasms—with 300,000 deaths annually. Socioeconomic disparities in treatment are vast, with 90% of all burn deaths sustained in low- to middle-income countries. Worldwide, injury is the cause of death in 1 in 10 persons, with burns as the fourth leading cause of injury-related death. For children who survive burn injury, 15% sustain long-term temporary disability, and 8% permanent disability— rates only superseded by near-drowning. In low- to middle-income countries, the prevalence of permanent disability attributable to burn injury is 12.5 times higher than in high-income countries. The aforementioned disparities likely arise from a mixture of inadequate safety measures, limited prevention outreach, lack of specialized burn centers, and deficiencies in training and resources necessary to provide impactful burn care.
CLINICAL FEATURES
Clinical manifestations of burn injury are determined by depth and breadth of tissue destruction (Table 99-1). Two independent systems of describing the depth of burn injury exist: that of “degrees” and of “thickness.” Patients tend to be more familiar with the degrees system, whereas most medical and surgical providers will communicate using the thickness system. Both are interchangeable and should be used with awareness of one’s audience.
SUPERFICIAL BURN (FIRST- DEGREE BURN)
SUPERFICIAL BURN (FIRST-
DEGREE BURN)
Superficial burns involve only the epidermis. Like a sunburn, the skin is warm, erythematous, painful, blanching, and dry without blisters or eschar (Fig. 99-1). The epithelium remains intact, but will begin to slough within 7 to 14 days. They are self-limited and have no potential for scar.
PARTIAL-THICKNESS BURN (SECOND-DEGREE BURN)
PARTIAL-THICKNESS BURN
(SECOND-DEGREE BURN)
Partial thickness burns involve the epidermis and penetrate to the dermis, but do not completely penetrate
17
SECOND-DEGREE BURN (SUPERFICIAL PARTIAL THICKNESS) SECOND-DEGREE BURN (DEEP PARTIAL THICKNESS) THIRD-DEGREE BURN (FULL THICKNESS)
FIRST-DEGREE BURN (SUPERFICIAL)
Clinical appearance Painful, dry burn with no blisters or eschar formation, blanching
Exquisitely painful, wet, weeping burn, blanching
Less painful, pale, nonblanching Insensate, dry, waxy, nonblanching with eschar formation
Epidermis + + + +
Dermis Papillary – + + +
Reticular – – + +
Subcutaneous tissue – – – +
Prognosis Self-limited with sloughing
Heals in 2 weeks with
Prognosis Self-limited with sloughing within 7-14 days; no risk of scarring
Heals in 2 weeks with proper wound care; low risk of scarring
within 7-14 days; no risk of scarring
proper wound care; low risk of scarring
through the dermis or down to the subcutaneous tissue. These burns appear wet, weeping, and erythematous, and are exquisitely painful, with blisters or sloughing epidermal remnant (Fig. 99-2). They are further divided into 2 categories:
■ Superficial partial thickness burn: blanching, more painful, hyperemic and erythematous, typically heal in approximately 2 weeks with appropriate wound care, low risk of scar and pigment change. Involves epidermis and papillary dermis. These
1680
3 weeks to heal; debridement
Surgical excision with skin
3 weeks to heal; debridement and grafting may be necessary; high risk for scarring and pigmentary changes
Surgical excision with skin grafting necessary for healing; contractures, hypertrophic scars are common
and grafting may be necessary; high risk for scarring and pigmentary changes
grafting necessary for healing; contractures, hypertrophic scars are common
can be managed conservatively with dressing changes or xenograft.
■ Deep partial-thickness burn: nonblanching, less painful, pink or pale, require more than 3 weeks to heal, high risk of hypertrophic scar and pigment change, outcomes may be improved by excision and grafting. Involves epidermis, papillary dermis, and reticular dermis. These typically require debridement and grafting.
FULL-THICKNESS BURN (THIRD-DEGREE BURN)
FULL-THICKNESS BURN
(THIRD-DEGREE BURN)
Full-thickness burns penetrate to the subcutaneous tissue and beyond, affecting all dermal layers. These burns are dry, leathery, waxy, nonblanching, insensate, and eschar is frequently shades of brown, white, gray, or black. The transition from adjacent partial-thickness
burn is clear by the lack of tissue edema. They will not heal without surgical excision with skin grafting or tissue transposition. Sequela, such as contractures and hypertrophic scars, are common.6,7 Of note, “fourthdegree burn” has been used to refer to burn injuries that penetrate to and/or expose deep structures (eg, bone, muscle, tendon) (Fig. 99-3). Skin grafting alone is not adequate treatment for burns of this severity, and limb loss may occur.8
Breadth of injury is described as a percentage of total body surface area (TBSA) that is affected; its measurement is addressed in section “Fluid Resuscitation”. Damaged tissues in burn wounds are almost always heterogeneous. Characterization of different regions of burns also can be described as the zone of coagulation (cell death), zone of stasis (cell injury that can either recover or transform into zone of coagulation), or zone of hyperemia (cells that will recover from injury) (Fig. 99-4). Despite multiple classifications for burn depth, no objective measure of burn depth exists,
17
leaving clinicians to rely on subjective assessments. Third-degree burns should be debrided within the first 3 to 5 days to avoid cellulitis and wound infections.
COMPLICATIONS
While it may appear that the sequelae of burn injury are limited to the integumentary system, there are many other systemic and local sequelae that must be considered when evaluating burn patients. Burns sustained in structural fires have a high incidence of smoke inhalation injury, wherein the pulmonary epithelium sustains direct thermal injury with ensuing edema and airway obstruction. Perioral burns and the presence of ashes and soot around or within the mouth and oropharynx are highly suspicious for inhalation injury and require emergent intervention to protect the airway. Carbon monoxide and cyanide toxicity are also associated with smoke inhalation injury, and the presence of inhalation injury alone doubles the mortality rate of burn injury.9 Circumferential burns of the extremities are at risk for the development of compartment syndrome as the underlying tissues becomes increasingly swollen and edematous and constricted by the eschar. If untreated, pressures can cause nerve impingement and vascular compromise. In electrical injuries, the muscle tissues swell and become restricted by the overlying fascia at which point the fascia muscle be surgically released. Similarly, full-thickness burns of the trunk restrict and compromise respiratory function, particularly in children, necessitating escharotomy of the chest to improve ventilation. Finally, excess resuscitation can cause abdominal compartment syndrome, which is defined as bladder pressure over 30 mm Hg. Patients often present with oliguria and abdominal distension. In these patients, first steps include escharotomy of the abdominal full-thickness burns, as well as paralysis and laying the patient flat. Fluids should be immediately decreased and diuresis or continuous renal replacement therapy should be considered to avoid a decompressive laparotomy. If these noninvasive measures fail to relieve the abdominal compartment syndrome, then a laparotomy might be required. Acute stress gastritis (Curling ulcer) with accompanying bleeding may develop in the gastric or duodenal mucosa as a result of intravascular volume depletion. Acute renal failure may occur following inadequate resuscitation or thermal injury to muscle as a consequence of massive myoglobinuria, particularly in electrical burns. Ectopic bone formation known as heterotopic ossification may develop in patients with large TBSA burns causing severe pain, contractures, and restricting range of motion.10 This most commonly occurs in the elbow and is more frequent if the burn injury includes the upper extremity.11-13 Burns induce a hypermetabolic state which is proportional to the size of burn injury, leading to muscle catabolism, hyperglycemia, and increased lipid liberalization with consequent steatosis. Finally, infection and sepsis are the most common cause of death in burn patients.14
1681
17
ETIOLOGY AND PATHOGENESIS
BURN PATHOPHYSIOLOGY
BURN PATHOPHYSIOLOGY
The pathophysiology of burn injury can be appreciated by considering 2 paradigms: loss of skin organ function and production of an inflammatory response. First, skin as an organ serves many functional purposes, not the least of which includes barrier protection against microbes, absorption and mitigation of mutagenic electromagnetic radiation, water and vapor impermeability, body thermoregulation, sensory perception, and motion-enabling elasticity balanced with sheer-resistant tensile strength. When skin is burned, these functions are lost. Microbe translocation into tissue or blood is unimpeded, leading to cellulitis, bacteremia, and sepsis. Unprotected from ultraviolet radiation, melanin-deficient burn scars are prone to squamous cell carcinoma development (eg, Marjolin ulcer). Loss of both the lamellar bodies of the stratum granulosum and the keratin-rich epidermal stratum lucidum and stratum corneum permits unregulated insensible vapor losses from transudates and interstitial fluid, causing intravascular volume depletion. Destruction of the dermal papillary plexus and eccrine sweat glands hinders autonomic hypothalamic regulation of body temperature and increased sensitivity to temperature fluctuations, especially in patients with high TBSA burns. Mechanoreceptor damage leads to long-term sensory loss, even in mild partial-thickness burns.15 Destruction of native tissue elastin and migration and proliferation of fibroblasts in the wound site, with subsequent myofibroblast differentiation and deposition of irregular collagen bundles, produce function-limiting contractures and inelastic scar with only 80% tensile strength of native tissue. Second, the inflammatory response to burn injury is profound and biphasic; an initial insult of inflammatory mediator release from necrotic tissue is followed by bacterial eschar invasion and establishment of a nidus. Local inflammatory response causes vasodilation and increased capillary permeability, promoting transudate production and insensible fluid losses. In burns greater than 20% TBSA, the initial insult from inflammatory mediator release triggers a systemic inflammatory response, manifesting as fever, hyperdynamic circulation, increased basal metabolic rate, and muscle catabolism.7 Depending on the severity of insult, in some patients this state will persist for 1 or 2 years postburn.16 Initially, burn wounds are sterile, but during the first week after injury, eschar becomes colonized and toxin exposure increases. In burns greater than 40% TBSA, bacterial load becomes so large that without intervention, sepsis and death are imminent. Beyond the colonization of the eschar, the excess dead tissue stimulates a massive inflammatory response which can lead to cardiovascular collapse.
1682
FLAME BURN
FLAME BURN
Thermal injuries, caused by fire or flames, are the most common burn etiology reported over the past decade.1
Thermal injuries are associated with the highest risk of death and complications compared to all other burn etiologies. Flame burns most commonly occur at home (64%), while work fires and recreational fire burns account for 12% and 6% of flame burns, respectively. When considering thermal injuries, it is important to consider smoke inhalation as it significantly impacts the morbidity and mortality of patients recovering from flame burns. The majority of inhalation injuries occur while the patient was indoors or in an enclosed space, and very few occur in patients who were burned while outside. Inhalation injury is present in 17% of patients with flame burns. The presence of smoke inhalation in burn patients is associated with an overall mortality rate of 24%, compared to the mortality rate of 4% in those patients without smoke inhalation damage.
SCALD BURN
SCALD BURN
Scalds are the second leading cause of burn injuries and are the most common mechanism of burns in the pediatric population. More than 50% of scalds are associated with food preparation or consumption, with a smaller proportion associated with bathing.17,18
Common mechanisms, including pulling a tablecloth, reaching up and tipping a container near the edge of a counter, pulling electric cords attached to kitchen appliances, and carrying containers with hot liquids.19,20 Contact burns from touching a hot object are extremely common in the pediatric population as well. Overall, contact burns make up 9% of burns reported, but they are the third leading cause of burns in children. Scald burns tend to cause a greater inflammatory response than flame burns.
ELECTRICAL BURN
ELECTRICAL BURN
Although only 4% of burns admitted to burn centers are caused by electricity, they pose the greatest diagnostic, therapeutic, and prognostic challenge among burn mechanisms. Notably, TBSA is an unreliable surrogate for burn severity, as it does not reflect the degree of internal tissue and organ damage caused after skin penetration by electrical current. To pass through dry human skin, a current must either surmount a huge amount of resistance, gain access to internal tissues through skin deficits such as cuts or burns, or induce skin breakdown (common above 500 volts [V]). Electrocution injuries are traditionally classified as low voltage (<1000 V) or high voltage (>1000 V), but ultimately it is the current (amperage) of the electricity and its direction of travel that ultimately determine ensuing tissue damage and lethality. For example,
only 20 milliamperes (mA) are required to paralyze respiratory muscles, and only 100 mA to induce ventricular fibrillation. Typical North American alternating current outlets have an average amperage of 15 to 20 amperes.21 Although TBSA does not represent burn severity, duration of contact with electrical source is proportional to tissue destruction. During electric shock by alternating current, both flexor and extensor muscles are stimulated, but the strength of flexors is greater than that of extensors, causing the “no let-go” phenomenon, and increasing contact time and tissue destruction. Primary electrical tissue injury is greatest in areas with the least cross-sectional area, such as digits, wrist, and toes. Burn injuries will often be present at the entrance and exit sites of the current, indicating a general path through the internal structures. For example, electrical shocks that cross the thorax are more likely to induce ventricular fibrillation, and limbs with entrance and exit sites are those at risk for compartment syndrome. Current will pass through highly conducting soft tissues, contact bone, and then continue along bone until exit. Bone has the greatest resistance of all body tissues, and therefore generates the most heat as current flows through it. Bone heating leads to severe thermal injury of deep invested muscles and tendon insertions which can cause swelling and compartment syndrome. All compartments between the entrance and exit wound should be monitored closely by examination and direct measurement of compartment pressures if concern for compartment syndrome exists. If compartment pressures are greater than 30 mm Hg, then fasciotomies should be performed. Massive myoglobinuria may result, necessitating renal protective fluid resuscitation. Damaged endothelium in major vessels leads to thrombosis. Cataracts may also develop. Apart from current flow, electrical burns are also caused by electrical arcs (temperatures upwards of 4000°C [7232°F]) and flame injury from ignited clothing. Secondary electrical injury can result from explosive shock waves generated by electric arcs, causing blunt trauma and tympanic membrane rupture. Longterm complications of high-voltage electrical injury also includes cataracts, and these patients should followup with ophthalmology as an outpatient. Lightning strike is exceedingly rare but can be catastrophic. Typically, patients who survive a lightning strike are at high risk for arrhythmias and compartment syndrome between the entry and exit points.22
CHEMICAL BURN
CHEMICAL BURN
Slightly more than 3% of burn center admissions are chemical burns, and with equal proportions occurring at work and at home. According to the Centers for Disease Control and Prevention, carbon monoxide, ammonia, chlorine, hydrochloric acid, and sulfuric acid are the chemicals with the highest frequency of associated injury, although carbon monoxide is likely not directly burn related.23 Important clinical categories of
17
chemical burns include alkali, acid, hydrofluoric acid, phenol, and white phosphorous. Acids induce burn damage through binding of hydrogen ions to proteins, inducing coagulation. Alkali burns are typically deeper and more serious than acid burns, as hydroxide ion saponification of fats induces liquefactive necrosis and permits further depth of chemical penetration. Mortality from chemical injury is low, and treatment cost is small relative to other injury mechanisms. Chemical burns are unique in that they will continue to progress after the initial insult until the offending agent is eliminated. Initiating immediate treatment in the field is associated with reduced injury severity and shorter hospital stay. Great care must be taken to protect health care personnel from exposure upon intake of patients, wherein clothing and accessories should be removed. It is advisable for solids or powders to be removed by brushes or dusting, as wetting with irrigation may provoke injuries in some cases (eg, calcium oxide, alkali metals). Otherwise, irrigation of the wound with copious amounts of water or saline should be initiated immediately. Attempts at neutralizing pH with a complementary chemical should not be undertaken, as heat from the consequent exothermic reaction can worsen the severity of the burn.24
Management of certain chemical exposures, such as hydrofluoric acid, white phosphorous, and phenol, require specialized therapy, and toxicology should be consulted. Although chemicals should not be neutralized, certain chemicals require specific treatments. Hydrofluoric acid is toxic because of the fluoride ion that binds calcium, but can be neutralized with topical calcium gel (1 ampule of calcium gluconate in 100 g of lubricating jelly). If symptoms persist, you can consider intraarterial calcium infusion (10 mL calcium gluconate diluted in 80 mL of saline, infused over 4 hours) and/or subeschar injection of dilute (10%) calcium gluconate solution. Phenol is commonly used in disinfectants and chemical solvents with poor water solubility. Phenol causes protein disruption and denaturation that result in coagulation necrosis. Treatment of phenol exposure includes copious water irrigation and cleansing with 30% polyethylene glycol or ethyl alcohol.22
STEVENS-JOHNSON SYNDROME AND TOXIC EPIDERMAL NECROLYSIS
STEVENS-JOHNSON
SYNDROME AND TOXIC
EPIDERMAL NECROLYSIS
Given the expertise of burn teams taking care of large body surface area burns, patients with desquamating skin processes, such as Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN), are often transferred to the burn unit. These are acquired blistering disorders of cutaneous and mucosal surfaces that are differentiated only by the affected TBSA: SJS less than 20% often with mucosal involvement, and TEN greater than 40%. Through an unknown mechanism of presumed immunologic origin, the epidermal–dermal
1683
17
junction begins to separate after starting new medications (particularly antiepileptic drugs or nonsteroidal antiinflammatory agents). The combined incidence of SJS and TEN in the United States is approximately 3800 per year, or 12 cases per million persons per year.25
Diagnosis should be made by biopsy as analyzed by dermatology or a dermatopathologist. Steroids and IV immunoglobulin are controversial for SJS and TEN, and much of the burn literature does not support its use. Treatment is supportive and patients should have a robust airway assessment and should be flagged as “difficult airway” patients. Severe intraoral swelling may require intubation. If there is ocular involvement, ophthalmology should examine these patients and any vaginal mucosal involvement warrants evaluation by an obstetrician-gynecologist. For wound care, a nonadherent antimicrobial gauze such as Acticoat is preferred and mineral oil should be used on the skin to keep it from shearing off.
DIAGNOSIS
ASSESSING THE BURN
ASSESSING THE BURN
The initial care of a burn patient can be likened to that of any trauma patient. Over time, guidelines such as Advanced Trauma Life Support and Advanced Burn Life Support have standardized the care of trauma patients and have improved overall patient outcomes. Thus, given the extent of injuries that a burn patient may present with, it is important to follow a standard algorithm. A complete history and physical should be performed with specific focus placed on the cause and timing of the injury, concomitant injuries, and treatments received prior to arrival. The ultimate goal is to stabilize the patient and ensure a proper assessment of the burn so that further care can be transitioned to a burn center, if necessary.
AIRWAY ASSESSMENT
AIRWAY ASSESSMENT
Assessment should begin with evaluation of the airway, breathing, and circulation. Inhalation injuries can occur in approximately 10% of all burn patients, but are notably present in 70% of those who eventually die of their burn.26 Thus, it is important to specifically note such findings as soon as the patient presents with nasal passage or posterior pharynx blockage, facial burns, changes in voice quality, shortness of breath, and carbonaceous sputum in the nasal or oral passages. If there is any concern that the airway is compromised, a nasopharyngeal scope or bronchoscope can be used to directly visualize the airway. Some clinicians consider the use of these tools to be mandatory in any patient who presents with facial burns no matter the extent of the burn itself. Although patients may not present with obvious airway compromise by manifesting the symptoms as stated above, airway edema can progress
1684
very quickly making an intubation that would have been easily performed on initial presentation very difficult because of progressive swelling and obliteration of anatomic landmarks. Endotracheal intubation may be required for several days until edema subsides as the mucosal slough and secretions accumulate, obstructing the airway and atelectasis progresses. In these patients, frequent bronchoscopic suctioning should be performed until soot no longer exists. Although the data are inconclusive, most centers also recommend inhaled heparin-albuterol-Mucomyst to treat airway swelling and clots. Systemic steroids can be considered if there are no other burns outside of the inhalation injury. If inhalation injury progresses to acute respiratory distress syndrome, typical acute respiratory distress syndrome protocols should be followed, including lung-protective ventilation (keeping keep pressures less than 30 mm Hg) with permissive hypercapnia. In some instances, identifying both the causative agent and the extent of the injury may aid in the recovery process. In particular, the possibility of carbon monoxide (CO) poisoning must also be assessed. Given the increased affinity of CO for hemoglobin molecules, oxygen (O2) becomes displaced which creates a hypoxic environment in the body. Formal diagnosis of CO poisoning is based on CO levels in the blood. Symptoms of CO poisoning typically begin with headaches at levels of approximately 10%, whereas CO in the blood becomes toxic at levels of approximately 50% to 70%. While the half-life of CO is normally 4 hours at room air, its half-life is shortened with treatment. It is recommended to treat CO poisoning empirically, especially in those patients presenting with agitation, reddish appearance of mucous membranes, and altered consciousness, given that delivery of 100% O2 (fraction of inspired O2 [FiO2] 100%) reduces the half-life of CO to 30 to 90 minutes. In patients with toxic levels of CO in the blood, more extreme measures are necessary, including the use of hyperbaric O2 at 2.5 atmospheres with 100% O2. Hyperbaric O2 will reduce the half-life of CO to 15 to 23 minutes. Consequently, prompt and aggressive evaluation and maintenance of the airway is the most important initial step in management of a burn patient. Finally, cyanide poisoning can cause severe complications and Cyanokit can be given in the field by paramedics as prophylaxis.
FLUID RESUSCITATION
FLUID RESUSCITATION
After initial stabilization of the patient has been performed, the next step is to determine the extent of the burn injury. For superficial burns, treatment of the burn wound oftentimes requires both topical antimicrobial agents and corticosteroids to minimize inflammation.27
Microorganisms proliferate rapidly in burn wounds, particularly in patients with impaired immune function caused by the burn. Topical antimicrobial agents delay the interval between injury and colonization and maintain low levels of wound flora. The specific
antibiotics and antiseptics for topical therapy in minor burns were discussed earlier in section “Wound Care”. Antibiotics, however, should not be given unless signs of infection exist. For full-thickness burns and some deep partialthickness burns, identifying the extent of the burn injury is crucial. TBSA is used to design fluid administration regimens and defines overall prognosis of patients. Criteria for transfer to a burn center are also based on this concept.28 Only partial-thickness and fullthickness burns are totaled to calculate TBSA. If small areas in various distributions are affected, it may be easier to use the patient as a ruler with one palm size representing 1% TBSA. Most emergency departments and burn units also have body surface charts available for use (the Lund & Browder Chart), but also follow the “rule of nines,” wherein the body is partitioned into areas and each region constitutes 9% of the TBSA (Fig. 99-5). Regions on the adult that constitutes 9% of the TBSA include the head and arms, while the legs, anterior trunk, and posterior trunk account for 18% of TBSA each. In children, the arms each account for 9% of the TBSA, while the legs account for 14%. The head and neck region, the anterior trunk, and the posterior trunk each account for 18% in children. Careful estimation of TBSA is essential for proper early management of burn patients, as patients who have burns of more than 20% TBSA commonly require IV fluid resuscitation. The Parkland Formula (Table 99-2; 4 mL × % TBSA × weight [kg]) is most commonly used to calculate fluid
17
(4 mL × % TBSA × weight [kg])/2 = first half to be administered in the first 8 hours = second half to be administered over the following 16 hours
(4 mL × % TBSA × weight [kg])/2
= first half to be administered in the first 8 hours = second half to be administered over the following 16 hours
TBSA, total body surface area.
requirements within the first 24 hours.29 It is extremely important to note that the original timing of the injury is what is used in the calculation, not the time of initial presentation. Half of this volume is administered in the first 8 hours after the injury and the second half is administered over the next 16 hours. For example, if a 70-kg (154-lb) patient with 10% TBSA burns sustained at 10 am presents at 12 pm, the fluid to be administered in the first 8 hours is calculated using the following formula: [(4 mL × 10% × 70 kg)/2]/6 hours. Lactated Ringer solution is recommended to avoid complications associated with metabolic acidosis with normal saline or abnormal fluid shifts with colloid fluids.29
Then, dextrose 5% in lactated Ringer solution is commonly used as maintenance fluids. Although such formulas exist, it is important to note that proper resuscitation is based on overall fluid status as represented by urine output, with the goal of 0.5 mL/kg/h in adults and 1 mL/kg/h in children, and fluids should
Lund & Browder Chart (adult)
Rule of Nines:
9%
Head:
3.5
18%
Chest/Abdomen:
1
18%
Back:
9%
Each Arm:
2 2
18%
Each Leg:
13
1%
Genitals:
1.5 1.5
1
3.5
1
2 2
13
1.5 1.5
2.5 2.5
1.5 1.5
4.75
4.75
3.5 3.5
1.75
1.5 1.5
4.75
4.75
3.5 3.5
1.75
1.75
1.75
1685
17
be adjusted accordingly. Given the immobility associated with severe burn injuries and the abnormal fluid shifts that occur, aggressive hydration also accounts for potential rhabdomyolysis, leading to acute kidney injury that can occur in this setting. Pulmonary status is also an indicator of fluid status but in more of a delayed fashion. Complications such as pulmonary edema result from fluid overload and necessitate daily evaluation of O2 requirements and ventilator settings. Once the Parkland Formula (see Table 99-2) is begun, the patient’s vital signs and urine output should be closely monitored and laboratory studies should be drawn frequently. Fluids should be increased or decreased based on the response of the patient. Although the urine output is considered a “gold standard,” early urine output can be slow while the patient is in shock and if tailoring fluids only to urine output, overresuscitation may occur. In addition, close monitoring of the patient’s laboratories are necessary to determine the trend in organ perfusion. Laboratory values that might help assess organ perfusion include lactate, base deficit, central venous O2, and/or pH. Although any one of these values alone does not provide a sensitive marker of the patient status, trending these values during resuscitation can help direct if the current fluid rate is causing a positive trend. If the organs are perfused, decreases in lactate and base deficit as well as increases in central venous O2 and normalization of pH should be observed. Finally, a monitor of cardiac output during large resuscitations can help guide fluid and assess for early cardiac failure. Such cardiac output monitors include esophageal Doppler monitors, pulse pressure variation monitors (FloTrac) and thermodilution monitors (PiCCO). In large burns that involve the face, an ophthalmologic consultation should be obtained. As the patient becomes edematous from the resuscitation, it is imperative that the globe is kept moisturized with a lubricant. Ophthalmologic consultants can help assess
globe pressure, injury to the cornea and glaucoma, which often occur in electrical injury. Thus, even though burn injuries may initially appear to be a focal area of trauma, the assessment of all systematic manifestations is paramount and must be stabilized before the burn itself is addressed.
WOUND CARE ASSESSMENT AND TREATMENT
As previously discussed, the depth, location, size, and duration of the burn injury are the most important factors to consider in the assessment of a burn. Burns can present for reconstruction in the acute or chronic phase, and reconstructive options are very different depending upon when a patient presents. Acute burn injuries require prompt intervention and serial examinations. On initial evaluation, it is important to rule out and prevent the development of circumferential burns that can lead to tissue ischemia and subsequent necrosis by limiting perfusion to the distal tissues.26 The overarching concept, however, in acute burn reconstruction is early debridement and grafting. All blisters and nonviable tissue must be debrided upon presentation. After the initial debridement, dressing changes are initiated while the patient is stabilized from a systemic standpoint. There are a variety of options for dressing materials (Table 99-3), and the appearance of the burn is mainly what dictates this choice. Although the indications for systemic antibiotic therapy have not been clearly defined within the literature, use of antimicrobial dressings is recommended. Silvadene is a silvercontaining cream that has broad-spectrum coverage against both Gram-negative and Gram-positive bacteria that needs to be changed on a daily basis. Although
INDICATIONS MECHANISM OF ACTION PRECAUTIONS
Silvadene Partial- and full-thickness injuries Broad-spectrum coverage vs Grampositive and Gram-negative bacteria Contraindicated in sulfa-allergic patients; avoid use near eyes Leukopenia known side effect
Sulfamylon Burns over cartilaginous areas; for open burn wound therapy Broad-spectrum coverage vs Grampositive and Gram-negative bacteria Associated with increased pain; risk for hyperchloremic metabolic acidosis; chronic use at risk for fungal infection
Silver nitrate Soaking dressings, 2-4 times a day Antifungal coverage Hyponatremia Stains skin, adjacent surfaces
Bacitracin Facial burns Dressings changed daily or every other day Antibacterial Daily dressing change required
Xeroform Partial-thickness skin graft donor sites Dressings changed daily or every other day Antibacterial Daily dressing change required
Acticoat Partial-thickness injuries with low risk for infection Dressings changed every 5 days
Antimicrobial silver impregnated
Acticoat Partial-thickness injuries with low risk for infection Dressings changed every 5 days Antimicrobial silver impregnated dressings
1686
dressings
its use is contraindicated in patients with sulfa allergies and over wounds near the eyes, Silvadene is commonly used over both partial-thickness and full-thickness injuries.30 Laboratory values, including complete blood counts, must be followed while patients are using this medication in the acute phase because of possible leukopenia, which is a known side effect of this medication. If leukopenia develops, Silvadene should be stopped; however, patients rarely develop any serious complications. Additionally, Gram-negative infections can cause leukopenia and should be ruled out if this arises. Sulfamylon is an analogous agent that is used over cartilaginous areas such as the nose or ear because of increased penetration of this dressing over these areas as compared to other dressing types. As topical Sulfamylon cream can be used without dressings, it can be used for open burn wound therapy and regular examination of the burn wound surface. However, both the cream and a 5% solution of Sulfamylon are equally effective.31 Sulfamylon has better penetration than Silvadene but may also cause increased pain. Patients should be monitored for complications such as hyperchloremic metabolic acidosis that can occur with use of this dressing as a result of its mechanism of action. Finally, chronic Sulfamylon can lead to fungal infection given that it does not cover any fungal species. This can be avoided by mixing with amphotericin. Silver nitrate also can be used by soaking dressings in 0.5% to 1% concentration and applied 3 to 4 times a day. Unlike Sulfamylon, silver nitrate does cover fungal species and thus may be preferable postoperatively if concern for infection exists. Typically, silver nitrate is applied as a soak to a dressing 2 to 3 times per day. It can cause leaching of cations causing hyponatremia. Additionally, it stains the skin as well as the floor and any equipment it comes in contact with. Bacitracin and Xeroform are additional examples of antimicrobial-type dressing regimens and should be changed every day or every other day. Even though both can be used anywhere on the body, bacitracin is commonly used for facial burns, whereas Xeroform is often used for partial-thickness skin graft donor sites. Regardless of the type of dressing used, wounds should be examined daily, given the predisposition of this wound niche to become infected. For patients who are at lower risk of infection based on the appearance of wounds, dressings may be changed with less frequency to achieve a balance between pain control and the need for wound coverage. Acticoat is one such option that is mainly used in partial-thickness injuries. This dressing consists of silver-impregnated sheets that have antimicrobial properties and can be changed less frequently, reducing pain and cutting cost and only needs to be changed every 5 days.32 The nanocrystalline particles in Acticoat are able to reduce wound infection and promote wound healing compared to older silver products, including silver nitrate.33 When using Acticoat, it is important to remember to activate it with water and not normal saline as the sodium can leech out the silver. While dressing changes are sometimes used to nourish and optimize a wound before and after operative
17
interventions, dressings also have the potential to completely heal a wound without the need for surgical intervention depending on the overall appearance of the burn and patient as a whole. Thus, a proper wound care team must not only include a critical care physician and surgeon, but it must also include a specialized wound care nurse to appropriately address this central modality of care for any burn patient.
MANAGEMENT
TRIAGE
TRIAGE
Upon presentation for care, a primary and secondary trauma survey should be performed, with special attention paid to signs of airway involvement and injury. Examination should be performed looking for intraoral swelling, hoarse voice, soot or singed nasal hairs. Nasopharyngeal scope examination can be performed in the emergency department for confirmation of airway involvement. Early intubation is recommended for patients with severe airway involvement or patients with large TBSA burns (>20% deep partial or full thickness) that will require Parkland large fluid resuscitation. Large-bore IV access should also be obtained in nonburned regions and arterial access, central line access and Foley catheter should be established to help guide resuscitation. Access to a burn center is crucial to optimize outcomes given the intricacies of airway management and complex resuscitative strategies.
OUTPATIENT CARE
OUTPATIENT CARE
In outpatient setting or prior to transfer, the clinician must ensure the burn process has stopped by
■Burn location, size, extent, depth, and circumferential components influence decisions regarding outpatient care, hospitalization, or transfer.
■Burn location, size, extent, depth, and circumferential components
influence decisions regarding outpatient care, hospitalization, or transfer.
■Burn percentage is best estimated using the Lund & Browder diagram that compensates for the changes in body proportions with age. An alternative is a “rule-of-nines” for adults and children.
■Burn percentage is best estimated using the Lund & Browder
diagram that compensates for the changes in body proportions with age. An alternative is a “rule-of-nines” for adults and children.
■In the adult rule-of-nines, the head and neck is given 9%, each lower extremity is given 18%, each upper extremity is given 9%, and the anterior and posterior torso are each given 18%.
■In the adult rule-of-nines, the head and neck is given 9%, each
lower extremity is given 18%, each upper extremity is given 9%, and the anterior and posterior torso are each given 18%.
■In the pediatric rule-of-nines, the head and neck is given 18%, each lower extremity is given 15%, each upper extremity is given 10%, and the anterior and posterior torso are each given 16%.
■In the pediatric rule-of-nines, the head and neck is given 18%, each
lower extremity is given 15%, each upper extremity is given 10%, and the anterior and posterior torso are each given 16%.
■For scattered or irregular burns, the entire palmar surface of the patient’s hand represents approximately 1% of the body surface over all ages.
■For scattered or irregular burns, the entire palmar surface of the
patient’s’s’ hand represents approximately 1% of the body surface over all ages.
1687
17
removing all potentially hot or constricting items such as clothes, rings, or belts. Patient should also undergo decontamination and steps to ensure all chemicals are sufficiently diluted. Once at a burn center, the burns should be scrubbed with antimicrobial soap and subsequently wrapped in an antimicrobial dressing for transport. Practice patterns vary between centers but certain characteristics are universal. The wound should be kept clean and inspected for infection. Desiccated exudates and topical medications should be cleansed at least once daily. Burns selected for outpatient management are small and superficial with a corresponding low risk of infection, so clean rather than sterile technique is reasonable. If topical agents rather than membrane dressings are used, wounds may be cleansed with lukewarm tap water and a bland antimicrobial soap. Soaking adherent dressings prior to change will decrease the pain associated with daily wound care. It is important to instruct each patient to return promptly if erythema, swelling, increased tenderness, lymphangitis, odor, or drainage develops so that infectious complications can be addressed early. Pain and anxiety can be an issue for many. Some will benefit from pain medicine given 30 to 60 minutes prior to a planned dressing change. Increasing pain and anxiety associated with dressing changes; inability to keep scheduled followup appointments; delayed healing; signs of infection or a wound that appears deeper than appreciated at the time of the initial examination should prompt early return and specialty evaluation. Finally, wounds of the face, ears, hands, genitals, and feet have functional and cosmetic importance. Early specialty evaluation may be warranted, as initial care can have an impact on long-term outcome.
VACCINATION
VACCINATION
A tetanus toxoid vaccine should be given to all burn patients with partial-thickness or full-thickness burns.34 In very young children and persons with highrisk tetanus wounds (ie, burn older than 6 hours at presentation, immunodeficiency, or soil contamination in wound), tetanus immunoglobulin should also be administered (tetanus toxoid is not given in children younger than age 4 years).35
PAIN
PAIN
Burn pain is multifactorial and frequently severe, particularly in patients with partial-thickness burns. As burn wounds heal, they initially become increasingly painful. Scheduled narcotics are first-line medications for the management of outpatient burn pain, and acetaminophen and nonsteroidal antiinflammatory drugs should play a secondary role in management. Scheduled dosing of narcotics provides superior pain control in burn patients as compared to as needed dosing,
1688
and allows for tapering down as the healing process progresses. Despite this, some patients may have inadequate control on short-acting narcotics. In this case, the patient should be interrogated about the nature of their pain. Frequently, pain intolerance is associated with wound dressing changes, which often occur daily. Anticipatory administration of narcotics before dressing changes can improve pain. Silver-coated dressings require less-frequent dressing changes, and if available, may aid in pain management. Furthermore, anxiety or acute stress disorders associated with dressing changes exacerbates pain, and scheduled administration of low-dose anxiolytics may manage pain without increased narcotic dosages. Pulsing or throbbing pain accompanied by warmth at the wound site may be associated with inflammatory progression, and in this case nonsteroidal antiinflammatory drugs may be appropriate. Otherwise, therapy may be escalated to long-acting scheduled narcotics. If pain cannot be controlled at home, the patient should be admitted for pain management.36,37
INFECTION
INFECTION
The infection rate of burns managed in the outpatient setting is 5%, which increases to 11% to 15% in diabetic patients. Usually these infections develop in the first 7 to 10 days, and normal flora organisms, such as Staphylococcus, are usually the culprits. Wound culture or quantitative culture is not necessary, as these infections present as cellulitis and may be reliably diagnosed clinically, with good response to first-generation cephalosporins. Infections occurring after the first 10 days, however, are more likely caused by Gram-negative rods, and patients benefit from wound culture and empiric coverage with ciprofloxacin. If symptoms progress to a combination of fever, chills, weakness, nausea, and/or vomiting, inpatient admission should be considered. Although burn wound infection looms as a feared complication, antibiotic prophylaxis is not appropriate and evidence does not support its use.36
Patients should be instructed to measure temperatures once or twice daily, with a measurement above 38°C (100.4°F) warranting urgent clinical evaluation. The wound should be well dressed with limited exposure to the environment. An antimicrobial barrier at the burn site should be maintained through application of silver-impregnated dressings or antimicrobial creams and ointments. Patients should avoid swimming in rivers, lakes, oceans, and even hot-tubs in order to avoid possible exposure to more virulent bacteria such as Pseudomonas. Tissue edema creates a nidus for infection, a risk factor easily managed by extremity elevation or a compression wrap (eg, ACE bandage). Patients should be educated about signs of infection, and if black or gray spots develop on the healing wound they should present immediately for evaluation. If undergoing treatment
for infection, followup must be frequent (multiple visits weekly), and if hindered by provider availability, patient availability or travel, or suspected patient adherence, then admission for inpatient care may be appropriate.
PRURITUS
PRURITUS
The majority of burn patients with both deep and superficial burns will experience clinically significant pruritus during their recovery. Regardless of severity, 90% of patients will experience pruritus during the first month after being burned. In 40% of patients, it will persist for at least 2 years, and roughly half of these chronic pruritus patients will experience consequent sleep disturbance. Risk factors for developing chronic pruritus include female gender, young age, skin grafting, raised or thick scars, and dry skin.38
The differentiation between transient and chronic postinjury pruritus can be understood by their distinguishable pathophysiologies. Mast cells produce and release histamine in response to the acute inflammatory burn reaction immediately following injury. As healing ensues, mast cell degranulation frequency decreases, and the majority of patients experience resolution. In full-thickness or grafted burns, however, afferent pathways have been destroyed, leading to general hypoesthesia. Despite this, such injuries predispose patients to the highest risk for chronic pruritus. Experts suggest that a neuropathic state of effective nociceptive hyperinnervation may develop in the setting of deafferentation because of release of selective neuropeptides from healing burn scar and degeneration of central inhibitory pathways regulating nociception.39 Exact pathophysiologic mechanisms of chronic pruritus, however, remain unknown. Evidence for treatment of burn pruritus is limited to 3 categories: topicals, antihistamines, and neuropathic agents. Selection of therapy generally follows aforementioned pathophysiologic reasoning. Nonetheless, the contribution of dry skin to pruritus should not be underestimated, and care should be taken for topical, bland, nonfragranced moisturizers to be applied to healed wound sites. Frequency of application is more important to achieve therapeutic effect than the product type, and patients should be advised to apply the moisturizer multiple times daily. When combined with antihistamines such as diphenhydramine, cetirizine, and hydroxyzine, early pruritus can be effectively managed. Cetirizine, a selective H1-blocker, is more effective than general antihistamines such as diphenhydramine.40 In patients with chronic pruritus, therapy with gabapentin and pregabalin is indicated—therapy that aligns with presumed neuropathic mechanisms. Similar to pain management, both antihistamines and neuropathic agents exhibit superior clinical benefits when doses are scheduled.6
17
SCAR
SCAR
Thermal burn injures can cause tremendous morbidity, leaving the patient with not only cosmetic but also functional impairments. Hypertrophic scarring is a major complication after burn injury with a prevalence of 32% to 72%. Several risk factors have been identified that contribute to its development, including the localization of the burn injury, burn depth, time to heal, and skin color.41,42 Although the precise mechanism by which hypertrophic scarring occurs remains unclear, strong and persistent expression of transforming growth factor-β and its receptors is associated with postburn hypertrophic scarring. Furthermore, a critical step in the healing process that is altered is the transition from granulation tissue into normal scarring. During this remodeling process, wound epithelization and scar collagen is formed, but accompany a gradual decrease in cellularity as a result of apoptosis. However, early immature hypertrophic scars caused by burns are hypercellular and during the process of remodeling and maturing, fibroblast density does not resemble that of normal healing.43
More specifically, apoptosis of myofibroblasts occurs 12 days after injury in normal wound healing, but in hypertrophic scar tissue, the maximum apoptosis occurs much later—at 19 to 30 months.44 These events result in a significantly higher percentage of myofibroblasts and the hypertrophy of the scar tissue following severe burn injuries. Although hypertrophic scarring often cannot be avoided, there are several steps that can optimize a burn scar:
- Wound closure of a burn that is likely not to heal on its own in 3 weeks;
- Avoidance of sun contact of the scar during the first 6 months;
- Compression garments for those who can tolerate treatment for up to 1 year; and
- Keeping the scar moist.
One of the key pathologic factors that needs to be addressed in any hypertrophic scar is tension. A new concept of “scar rejuvenation” has emerged with the key idea being to improve the environment of the scar without actual excision of the scar. The most important step in rejuvenating the scar is release of the tension. Rather than excising, the scar, this involves just releasing the area of greatest tension. Despite not removing any tissue, a large defect is often created once the tension is released. This defect can then be treated by adding new tissue such as a full-thickness skin graft or a thick split-thickness skin graft. Additional ways to relieve tension involve the use of tissue rearrangements such as a Z-plasty. A Z-plasty lengthens the scar at the expense of width, thereby alleviating tension along the central access of the hypertrophic scar. In general, Z-plasty rearrangements are made with 60-degree angles to maximize tissue gain without causing excess tension on the donor-site closure. The corner can be made at 90 degrees and then the rest of
1689
17
the limb at 60 degrees to improve blood flow to the tip of the flap and to avoid flap necrosis. Additionally, flaps should be kept thick to avoid flap ischemia. Alternative V-Y advancements are useful if there is healthy surrounding tissue and a combination of Z-plasty and V-Y advancement flaps, as in a 5-flap jumping man, are helpful for web spaces.45
Current treatment strategies for hypertrophic scars include surgical manipulation, intralesional corticosteroid injections, cryotherapy, and laser therapy. Surgical manipulation to remove the excess skin remains the traditional treatment for hypertrophic scar. Newer studies investigating the role of fat grafting into scars have shown promise to further improve function and appearance.46 Patients who have undergone fat transfer report satisfactory results 6 months after the procedure, indicating considerable improvement in the features of the skin, skin texture, and thickness. Histologic examination demonstrated new collagen deposition, neovascularization, and dermal hyperplasia in regions treated with fat grafting, which mimicked surrounding undamaged skin. Additionally, intralesional corticosteroids suppress the inflammatory process in wounds, diminish collagen synthesis, and enhance collagen degradation.47
Conversely, cryotherapy induces vascular damage that leads to anoxia and, ultimately, tissue necrosis, and has yielded marked improvement of hypertrophic scars.48 However, its efficacy is limited to the management of small scars. Lastly, since the introduction of laser treatment in the mid-1980s, the therapeutic use of additional lasers with different wavelengths have been employed. The most encouraging results have been obtained with the 585-nm wavelength pulseddye laser, which has been recognized as an excellent therapeutic option for the treatment of younger hypertrophic scars.49 Pulsed-dye laser induces the dissociation of disulfide bonds in collagen fibers and leads to collagen fiber realignment, decreased fibroblast proliferation, and neocollagenesis. However, it is necessary for repeated treatments, generally between 2 and 6 treatments, for optimal resolution. Newer, exciting research has demonstrated the benefit of fractional photothermolysis in the treatment of hypertrophic scarring. Although the exact mechanism is unknown, this concept uses a CO2 laser, which is an ablative laser that targets water in the underlying tissues (10,600 nm). The laser creates columns of tissue destruction, which stimulates collagen production in adjacent uninjured columns of tissue. The adjacent uninjured tissue allows for more rapid tissue regeneration from their follicles and sweat glands. Overall, this creates a smoother appearance and enables meshed grafts to appear less obvious.10 Patients have described less tightness as well as decreased pruritus.50 The key to this treatment modality is the fractionated nature of the laser, which allows for remodeling of the disorganized collagen without undue thermal injury to the surface. Different strategies are used for fractional CO2 lasers with some clinicians preferring high density and low energy and others preferring low density and high energy.
1690
ACKNOWLEDGMENTS
We would like to thank Dr. Joshua Peterson, MD for his assistance and guidance in figure and textual development of this chapter.

Figure 99-1 Superficial burn to the right aspect of the neck, in this case superficial area largely on the perimeter of the burn. Blistering represents partial-thickness burn of central area.

Figure 99-2 Partial-thickness burn of the left arm with blistering. Blisters are flaccid and contain serous fluid; burns of this degree are the most painful.
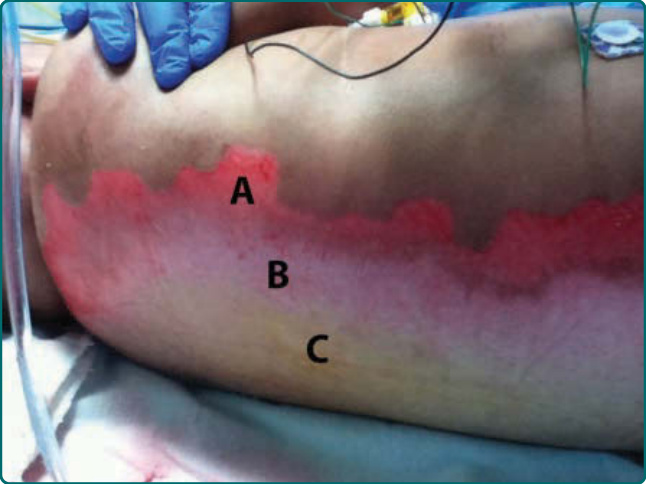
Figure 99-3 Full-thickness burn of the back demonstrating zones of injury according to Jackson’s thermal wound theory. A, Zone of hyperemia (cells that will recover from injury); B, zone of stasis (cell injury that can either recover or transform into zone of coagulation); C, zone of coagulation (cell death).

Figure 99-4 Fourth-degree burn of ankle with exposed tendon and muscle.
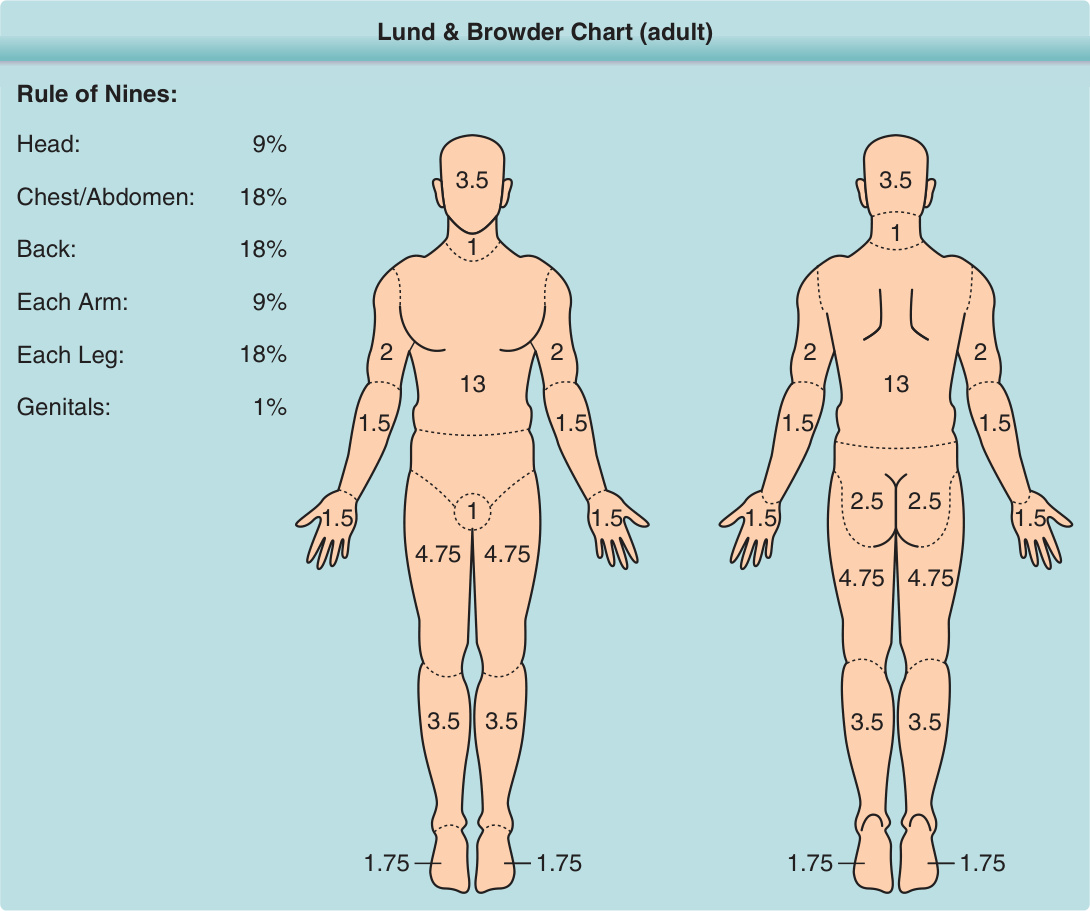
Figure 99-5 Rule of nines and the Lund & Browder Chart are methods commonly employed to estimate the total body surface area (TBSA) of a burn. Numbers in Lund & Browder Chart indicate percent TBSA of body region.
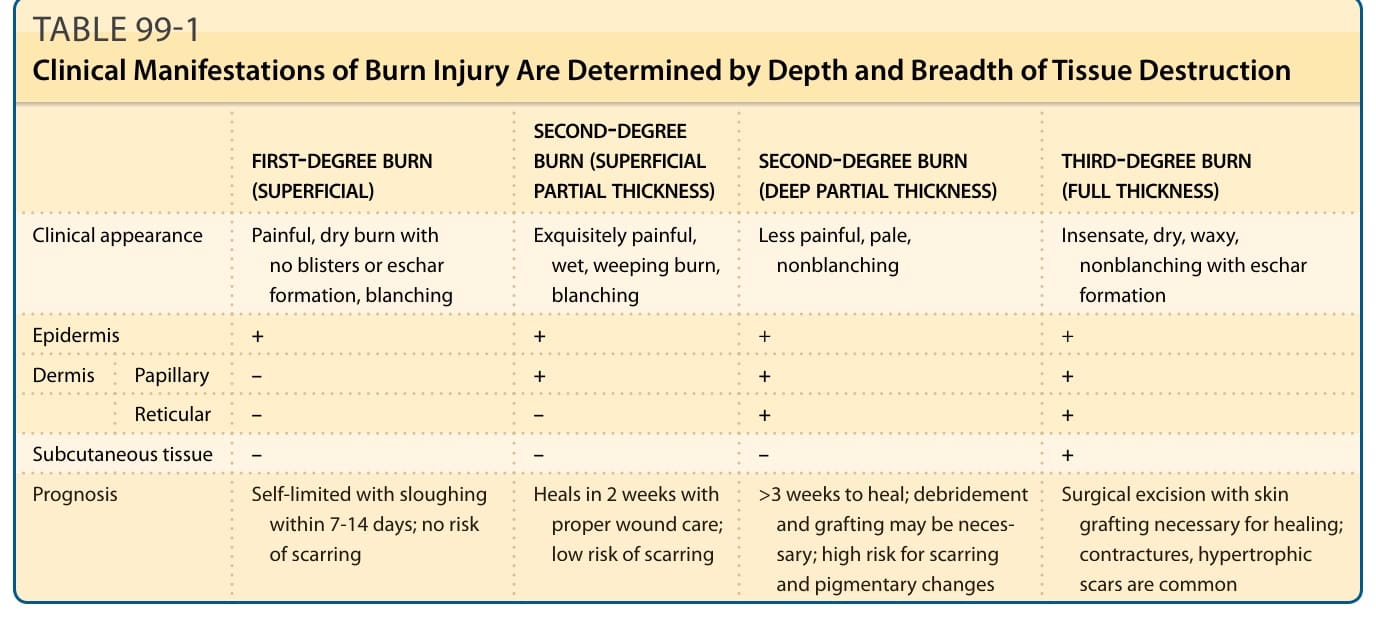
TABLE 99-1 Clinical Manifestations of Burn Injury Are Determined by Depth and Breadth of Tissue Destruction
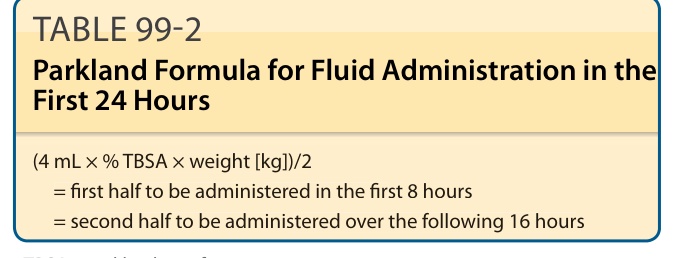
TABLE 99-2 Parkland Formula for Fluid Administration in the First 24 Hours
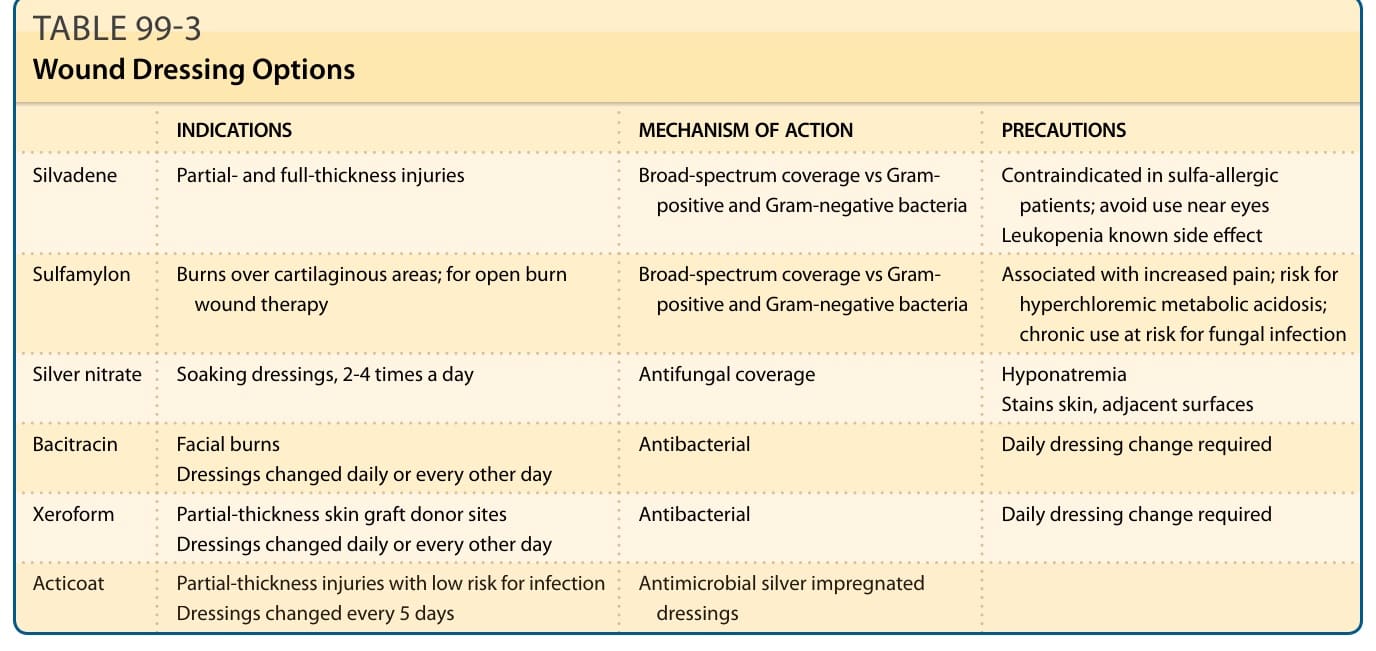
TABLE 99-3 Wound Dressing Options
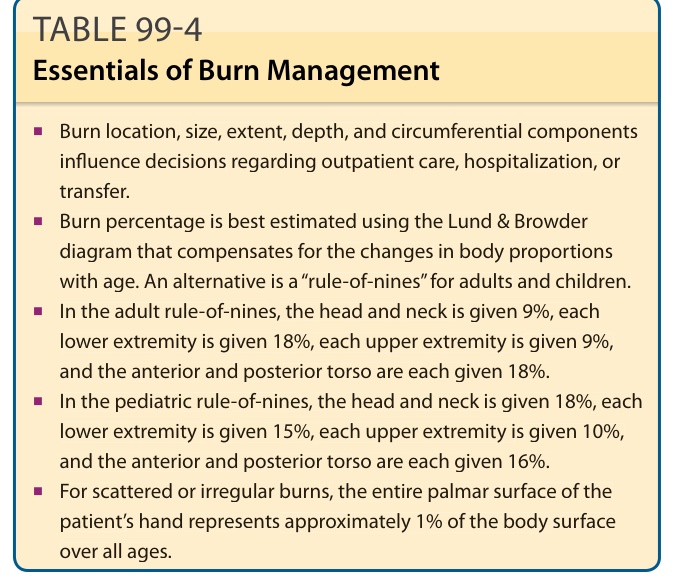
Table 99-4 outlines the essentials of burn management.