Cold Injuries
17
AT-A-GLANCE
■ Skin is important for maintaining core body temperature within a narrow physiologic range.
■ Cold weather, wind, humidity, dampness, and altitude combine to inflict skin damage.
■ Freezing and nonfreezing conditions can both produce cold injuries.
■ Frostbite occurs after exposure to intensely cold air, liquids, or metals. Several degrees of frostbite are recognized.
■ Self-inflicted freeze injuries from inhalant abuse and peer challenges are emerging.
■ Winter xerosis and acrocyanosis are common consequences of prolonged exposure to cold.
■ Pernio is an acral eruption of edematous violaceous papules occurring in cool rather than freezing exposures, and seen more frequently in lean persons.
■ Cold urticaria is rare and occurs at the sites of localized cooling.
■ Cold panniculitis typically occurs on legs and cheeks.
Many physiologic, behavioral, and environmental factors predispose to cold injuries. Marked increases in convective, conductive, or radiant heat loss are responsible for the immediate effects of cold exposure. A cold environment can be a threat to the skin, and can lead to subsequent fall in core body temperature. Cold injuries are becoming more prevalent among the general population.1 Outdoor work, winter sports, windy conditions, humidity, altitude, and skin contact with cold objects are environmental factors that may predispose an individual to cold damage.2 Insulation from clothing is insufficient when garments are too light, wet, tight, permeable to wind, or inadequate to cover the cold sensitive body parts. Frostbite prevails among winter sport enthusiasts, such as cross-country skiers and backpackers, who get lost or trapped in a snowstorm.3-8 Accidental exposure to liquefied gas is an emerging cause of severe cold injuries.9
The human capacity for physiologic adaptation to cold is minimal. This deficiency may cause problems because seasonal changes in the outdoor environment can be quite dramatic, even in the temperate zones of the world. Skin is important in thermoregulation. Cutaneous blood flow and the resulting skin temperature may vary widely to preserve the core body
temperature.10,11 In fact, the body can maintain a constant core temperature of approximately 37°C (98.6°F) over a range of external temperatures between 15°C and 54°C (59°F and 129.2°F). In addition to external temperature, physiologic, behavioral, and environmental factors modulate skin responses to cold exposure.
THERMOREGULATION AND PHYSIOLOGIC RESPONSE TO COLD
Cutaneous thermoregulation is complex. As external temperature decreases, central thermoregulation centers in the hypothalamus signal other hypothalamic control centers to generate or conserve heat. Core body temperature is prioritized and maintained largely by controlling cutaneous blood flow. Arteriovenous anastomoses are abundant in acral areas, and they regulate the volume of blood passing through the skin. When the skin is cooled, there is usually an immediate vasoconstrictive response to reduce the amount of blood flowing at the skin surface. Without this vasoconstriction there would be significant heat transfer from the blood flowing in the skin to the environment, leading eventually to core temperature drop. The parallel arrangement of large arteries and veins in the limbs allows countercurrent exchange of heat. Vasoconstriction caused by cold results in shunting of blood from the superficial to the deep venous system, and heat is transferred from arteries to veins. Thus, the venous blood returning to the heart has already received heat transferred from the arteries before the heat can be lost to the environment. In prolonged cold exposures, the skin experiences a paradoxical cyclic vasodilation known as the hunting reaction of Lewis, to protect against skin necrosis from prolonged vasoconstriction.12,13 If cold exposure continues, there is an eventual reflex constriction of the arteries and veins in the extremities resulting in increased venous pressure, decreased capillary perfusion, sludging, hypoxia, microvascular thrombus formation, and surrounding tissue damage.14 Segmental vascular necrosis ensues in areas of erythrostasis. The rate of tissue freezing impacts the nature of cold injury.15 Slow freezing results in extracellular formation of ice whereas fast freezing tends to produce intracellular ice. Extracellular ice crystals alter the osmotic properties of tissues and disturb the flow of water and electrolytes across the cell membranes. Thawing may
be as damaging as the freezing itself, and repeated freeze and thaw cycles, as may occur in accidental injury, compound the damage. The rewarming rate is also important. In slow rewarming, ice crystals become larger and more destructive. Other biologic factors influence vasoconstriction and tissue damage besides temperature. Painful stimuli, mental stress, arousal stimuli, deep breaths, and other stimuli of the autonomic nervous system can produce cutaneous vasoconstriction in warm subjects.16,17 Increased blood viscosity (vascular sludging) also influences the negative effects of cold on the skin. Blood viscosity is strongly influenced by blood flow rates, hematocrit, platelet adhesiveness, concentrations of proteins, and the presence of abnormal proteins, such as fibrinogen. Individual factors predisposing to cold injuries include skin conditions with transepidermal water loss (eg, atopic dermatitis), physical injuries, leanness, low physical fitness level, fatigue, dehydration, previous cold injuries, sickness, trauma, poor peripheral circulation, poor clothing insulation, and old age.2
Newborns, the elderly, and individuals with acute or chronic impaired mental faculties remain the most vulnerable (Fig. 98-1). Many cases are associated with alcohol consumption, homelessness in urban centers, and car breakdown. Smoking and psychotropic drug use can also increase injury. Given the presence of many cold-adapted enzymes, the skin may function more effectively when slightly cooled. In the case of adipose tissue, mild long-term exposure to cooling may lead to progressively better insulation. Consequently, overweight persons are more likely to survive prolonged accidental cold exposure.18
Habitually cold-exposed skin also develops a more efficient system for shunting blood away from the surface. These adaptive mechanisms are most flexible during the first years of life. Tissues in the aged are less able to develop new shunts. In contrast, individuals who have experienced previous severe cold injury may have a profoundly delayed or absent hunting
17
reaction in the affected limbs, making them more susceptible to recurrent cold injury with pain, hyperesthesia, or paresthesia.19,20 Some of these individuals also have chronically cool skin.
CLASSIFICATION OF SKIN COLD INJURIES
Skin cold injuries can be divided into freezing and nonfreezing cold injuries. Although freezing injuries typically have clear associations with cold exposure by patient history, exposures that cause nonfreezing skin conditions are less likely to be associated or recounted by patients. Some of these conditions involve many variables other than temperature. Clinical recognition is generally easy, but awareness of potential uncommon associated disorders is important.
FROSTBITE
Frostbite occurs when tissue freezes after exposure to extremely cold air, liquids, or metals. The clinical effects of accidental injury that lead to the death of tissues are similar to those caused by cryosurgery.21
Tissue injury results from initial vasoconstriction followed by intracellular and extracellular ice crystal formation.10 This causes metabolic derangements in cells, electrolyte imbalances, membrane lysis, and cell death. Thawing can further exacerbate tissue damage through ischemia–reperfusion and increasing inflammation. Vascular stasis then occurs, followed lastly by a late ischemic phase that results in the eventual infarction of tissues, largely from damage to microcirculation.
■Vasoconstriction
■Vasoconstriction
■Hunting reaction
■Hunting reaction
■Immersion foot
■Immersion foot
■Pulling-boat hands
■Pulling-boat hands
■Acrocyanosis
■Acrocyanosis
■Chilblains
■Chilblains
■Cold urticaria
■Cold urticaria
■Cold panniculitis
■Cold panniculitis
■Erythromelalgia
■Erythromelalgia
■Raynaud phenomenon
■Raynaud phenomenon
■Sclerema neonatorum
■Sclerema neonatorum
■Subcutaneous fat necrosis of the newborn
■Subcutaneous fat necrosis of the newborn
■Livedo reticularis
■Livedo reticularis
■Cryoglobulinemia
■Cryoglobulinemia
■Cold agglutinins
■Cold agglutinins
1667
■Cryofibrinogenemia
■Cryofibrinogenemia
17
Frostbite commonly affects fingers, toes, ears, nose, and cheeks.22,23 Extreme and often conductive heat loss at a given body site freezes the tissues and results in localized blistering and necrosis (Fig. 98-2). The clinical presentation of frostbite falls into 3 categories that correspond to frostnip (mild frostbite), superficial frostbite, and deep frostbite with tissue loss. Frostnip involves only the skin and damage is reversible (Fig. 98-3). There is a sensation of severe cold progressing to numbness followed by pain. Erythema is usually present on the cheeks, ears, nose, fingers, and toes. There is no edema or bleb formation. Frostnip is the only form of frostbite that can be treated safely in the field with first aid measures. Superficial frostbite involves the skin and immediately subcutaneous tissues. It includes the previously described signs but with the pain subsiding to feelings of warmth. This is a sign of severe involvement. The skin has a waxy appearance, but deeper tissues remain soft and resilient. Clear blebs form, accompanied by edema and erythema within 24 to 36 hours after thawing. Lesions may become eroded (Fig. 98-4). Deep frostbite extends to the deep subcutaneous tissue. The injured skin becomes white or bluish
1668
white with a variable degree of anesthesia. Most often the affected skin becomes deceptively pain free, and the discomfort of feeling cold vanishes. The tissue is totally numb, indurated with immobility of joints and extremities. Muscles may be paralyzed. Nerves, large blood vessels, and even bone may be damaged. Large blisters form 1 to 2 days after rewarming, and they can be classified according to depth, as in heat-induced burns (Fig. 98-5). Frostbite blister fluid contains high amounts of prostaglandins, including prostaglandin F2α and thromboxane A2. These mediators may contribute to increased vasoconstriction, platelet aggregation, leukocyte adhesiveness, and, ultimately, progressive tissue injury. The blister fluid begins to be resorbed within 5 to 10 days, which leads to the formation of
hard, black gangrene. Weeks later, a line of demarcation occurs, and the tissues distal to the line undergo autoamputation (Fig. 98-6). Prevention is key to protecting individuals from the effects of cold weather; frostbite, frostnip, and hypothermia always should be taken seriously. Table 98-2 lists prognostic factors.7,8,24-26 Wearing protective clothing, a warm hat, earflaps, and scarf, together with preventive behavior, such as turning bare areas away from the wind, are the most important procedures for preventing frostbite. Nonmedicated waterless ointments are traditionally used for protection against facial frostbite, but their benefit is undocumented. The thermal insulation they provide is indeed minimal.22,23 The
Good prognostic signs
Large, clear blebs extending to the tips of the digits Rapid return of sensation Rapid return of normal (warm) temperature to the injured area Rapid capillary filling time after pressure blanching Pink skin after rewarming
Poor prognostic
Hard, white, cold, insensitive skin Cold and cyanotic skin without blebs after
Poor prognostic signs
Hard, white, cold, insensitive skin Cold and cyanotic skin without blebs after rewarming Dark hemorrhagic blebs Early evidence of mummification Constitutional signs of tissue necrosis, such as fever and tachycardia Cyanotic or dark red skin persisting after pressure Freeze–thaw–refreeze injury
signs
rewarming Dark hemorrhagic blebs Early evidence of mummification Constitutional signs of tissue necrosis, such as
fever and tachycardia Cyanotic or dark red skin persisting after pressure Freeze–thaw–refreeze injury
17
use of protective emollients may lead to a false sense of safety and increased risk of frostbite, probably through neglect of other, more efficient protective measures.27-29
In less-extreme conditions, however, some specific topical formulations bring beneficial effects.30 The most effective products are those reducing transepidermal water loss and perspiration because these biologic functions cause emission of body thermal energy and further cool the skin. The first consideration in frostbite treatment is to be aware that the victim may be suffering from hypothermia.7,14,31,32 Prompt recognition and treatment are of paramount importance, because many hypothermia victims can recover from very low body temperatures. Treatment in an adequate medical facility can make the difference between full recovery and lifelong problems. Even if the victim appears to be dead from exposure to cold, resuscitative efforts should be started and continued until the proper core body temperature is reached.14
Because of the difficulty in assessing the depth of frostbite injury, conservative waiting after the frostbite episode is often encouraged in an attempt to delineate the extent of tissue loss. Care providers should avoid trauma, friction, pressure, massaging with snow, and refreezing. Slow rewarming increases tissue damage, making rapid rewarming the keystone of treatment.33
Rewarming should be performed in a water bath between 37°C and 39°C (98.6°F and 102.2°F) until the most distal parts of the body are flushed.29,34,35 Large amounts of analgesics may be required. The damaged part should be elevated, and blisters should be left intact. Surgical debridement is often best delayed until 1 to 3 months after demarcation. However, triple-phase bone scans, MRI, and magnetic resonance angiography can be used to predict ultimate tissue loss and to assess the possibility of earlier surgical intervention.36-38
There is no uniformly accepted protocol for other measures allegedly beneficial in the treatment of frostbite injury.32 Intraarterial reserpine and sympathectomy have been used to reverse vasospasm, which may contribute to tissue loss. Their role is controversial, although some patients have benefited from this therapy. To counteract vasoconstriction caused by local release of inflammatory mediators, the use of topical aloe vera, which inhibits thromboxane synthetase, and oral ibuprofen, which inhibits cyclooxygenase, has been advocated. Oxpentifylline has been presented as an advanced therapy.39 In addition, several adjunctive therapies, including vasodilators, thrombolysis, and hyperbaric oxygen, are sometimes useful.40 Tetanus toxoid should be given in the case of open wounds. Surgery and amputation remain the ultimate strategies to help the victims.41
Sequelae of frostbite include permanent hypersensitivity to cold and, less often, hyperhidrosis.42 Squamous cell carcinoma is a rare outcome, usually occurring on the heel 20 to 30 years later.43 Epiphyseal plate damage or premature fusion may occur in children. Premature fusion can result in shortened digits, joint deviation, and dystrophic nails. In addition, frostbite arthritis,
1669
17
resembling osteoarthritis, may occur weeks to years later. Frostbite may also lead to ossification of one or both ears.44
IATROGENIC COLD INJURY
The most common in-office procedure performed in dermatology in the United States is cryodestruction using liquid nitrogen.45 This destructive therapy causes localized cutaneous tissue freezing in a series of freeze–thaw cycles, leading to cell death in the targeted lesions, similar to a localized frostbite reaction. Vigorous tissue responses and overly aggressive treatments may lead to significant reactions, pain, and patient concern in the days following treatment. Vesicles and even large bullae, including hemorrhagic bullae, can occur acutely (Fig. 98-7). This can be followed by hemorrhagic crusting, hypopigmentation, and even scarring.
A
B
1670
SELF-INFLICTED COLD INJURY
While accidental or incidental exposure to cool, cold, or freezing temperatures is the cause of many cold injuries and dermatoses, such injuries also may be self-inflicted by patients. Intentional and unintentional contact with cold substances, often through the misuse of household and industrial chemicals, can induce damage to the skin. Chemicals that are capable of coldinduced skin injury include the fluorinated hydrocarbons in propellants, refrigerants, and liquefied petroleum gases (eg, propane, butane), which are used as solvents and fuels.46,47 Although these compounds can cause injury through accidental spray or drip exposures from pressurized canisters, such as occupational exposure to liquid nitrogen or pressurized ammonia,48
they also may be intentionally abused for the purpose of achieving an altered mental state. Inhalant abuse, which involves deliberately breathing volatile substances through the nose or mouth to achieve “a high” has been an emerging problem since the 1960s.49 Slang terms for inhalant abuse include huffing, sniffing, snorting, dusting, glading, and bagging, depending on the substance involved and mode of inhalation.50 The peak ages of inhalant abuse has been reported to be 14 to 15 years.50 Individuals at increased risk include persons of low socioeconomic status and those with a history of criminal behavior, incarceration, depression, suicidal ideation, antisocial personality traits, unstable home life, or other drug use. The problem has been particularly widespread among Native American and Alaskan Native youth. Inhalation of amyl nitrite or butyl nitrite to augment sexual pleasure, referred to as “popping” or “snapping,” also has been a practice among certain cultural groups, including men who have sex with men.51
Because of the low temperatures of inhalants, frostbite has been observed on the face, fingers, forearms, oral, laryngeal, and tracheal surfaces (Fig. 98-8A).46-49
This may present as well-demarcated edema, erythema, cyanosis, and vesiculation concentrated around the nose, mouth, or even periorbital area (Fig. 98-8B).49
Other skin findings may include a perioral or perinasal dermatitis with pyoderma (“huffer’s rash”), contact dermatitis, yellow-stained facial dermatitis caused by nitrites,52 and ichthyosis-like dermatitis from paradichlorobenzene in mothballs.53 Extracutaneous manifestations of inhalant abuse can include conjunctival injection, headache, drowsiness, slurred speech, ataxia, disorientation, arrhythmia, vomiting, increased secretions, respiratory difficulty, and syncope.50
Pressurized gasses are not the only source of selfinflicted cold injury. Around 2012, a social media fad emerged in which teens applied table salt and ice cubes to the skin, challenging each other to see who could withstand the painful contact the longest.54 Similar to salting an icy winter road, the salt rapidly decreases the freezing point of water to below 0°C (32°F), enhancing the ability to induce local frostbite.55,56 A series of
A
B
case reports have emerged in the literature in which teenage patients have presented to clinicians with factitial skin damage from the “salt-and-ice challenge.” Lesions consist of painful, sharply demarcated, geometric or drip pattern, dusky erythematous patches, which may become bullous (Fig. 98-9).54,56 Common locations include the palmar hands, forearms, and back.54-56 Pathology on hematoxylin-and-eosin stain
17
A
B
shows an interface dermatitis with extensive epidermal necrosis.56 When confronted about possible self-infliction, patients frequently deny such behaviors, especially in the presence of parents or family members.
1671
17
NONFREEZING COLD INJURY AND DAMPNESS
Nonfreezing cold injury occurs when tissues are cooled to temperatures between 0°C and 15°C (32°F and 59°F) for hours to days.35 This type of injury, historically known as “trench foot,” is exacerbated by dampness and has claimed numerous casualties in warfare. Cold, wet conditions at temperatures above freezing and limb dependency resulting from immobility and constrictive footwear are important pathogenic factors. Although classically thought to affect feet, nonfreezing cold injury can occur in other areas of the body.35 Persistent erythema of the face and the hands is not a rare finding (Fig. 98-10).
WINTER XEROSIS
Minor but long-term cold exposure combined with environmental desiccation may have profound effects on the biology of the epidermis, leading, for example, to winter xerosis.57,58 Many individuals present with dryness of the skin, particularly on the lower extremities, during wintertime (Fig. 98-11). The hands, forearms, cheeks, lips, and trunk also may be affected. Itching, a dry appearance, chapping, and cracking of the stratum corneum can be prominent. The condition is markedly influenced by cold environments, especially in combination with low humidity.42,59 Predisposing factors include atopic dermatitis, ichthyosis, and increasing age. Excessive washing exacerbates winter xerosis. Indeed, irritant dermatitis of the hands worsens in a cold and dry environment.60 Emollients and improvement in the environmental temperature and humidity are helpful in controlling this condition.
1672
ACROCYANOSIS
Vasoconstriction can alter both skin temperature and skin color, resulting in a blue to violaceous acrocyanosis, a bilateral dusky mottled or confluent red to blue discoloration of the hands, feet, nailbeds, and sometimes the face (Fig. 98-12). It is persistent and accentuated by cold exposure. When the temperature is very low, the skin may be bright red. Trophic changes and pain do not occur, and pulses are present. This condition must be distinguished from obstructive arterial disease (see Chap. 148) and Raynaud phenomenon (see Chap. 145), which is clearly episodic, often segmental, and painful. Acrocyanosis is genetically determined and usually starts in adolescence. Chronic vasospasm of small cutaneous arterioles or venules with a secondary dilation of the capillaries and subpapillary venous plexus has been postulated. Stasis in the papillary loops with aneurysmal dilation at the tips redistributes blood flow to the subpapillary venous plexus. The blood flow may be compromised by altered erythrocyte flexibility, increased platelet adhesiveness, and other plasma viscosity factors. Cold agglutinins may exacerbate the acrocyanosis manifestations.61,62 The “puffy hand syndrome” is defined by the presence of hand edema superposed on acrocyanosis.63
Tissues are less sclerotic in acrocyanosis than in Raynaud phenomenon. In cases developing for the first time late in life, an underlying myeloproliferative disorder should be excluded. Remittent necrotizing acrocyanosis is associated with enhanced susceptibility to cooling and pain, as well as ulceration and gangrene of the fingers. Arteriolar occlusion by thrombi or intimal proliferation may occur. Cold pain should be distinguished from cold allodynia and cold hyperalgesia. There is no effective treatment for acrocyanosis. Supportive measures to keep the skin warm are helpful.
PERNIO (CHILBLAINS)
Pernio, also called perniosis or chilblains, is a condition of localized inflammatory lesions caused by continued exposure to cool temperatures (above freezing).64,65
Dampness and wind contribute to disease flares by increasing thermal conductivity and convection. Absolute temperature is less important than the cooling of nonadapted tissue. Abnormal vascular response to cold and minor trauma are believed to play a role.66
The condition shows a genetic predisposition. It has been described most often in temperate regions, where winters are commonly cold and damp. Pernio is seen less often in very cold climates, where well-heated houses and warm clothing are available. When occurring in these colder regions, it is more common to occur during the cool early spring season rather than winter. Pernio is more common in children, women, and persons with low body mass index. Spontaneous remission is common when spring arrives, and relapse is frequent during the following winters. Pernio develops acutely as single or multiple, burning, erythematous to violaceous macules, edematous papules, plaques, and nodules (Fig. 98-13). Patients may complain of itching, burning, or pain. In severe cases, blisters, pustules, and ulceration may occur. Characteristic locations include the dorsal and plantar surfaces of the toes, but the fingers, heels, nose, ears, and other sites, like the calves and thighs, can be affected.67,68 Lesions usually resolve in 1 to 3 weeks but may become chronic in elderly people with venous stasis. A papular form of pernio resembling erythema multiforme can occur at all times of the year, usually in crops on the sides of the fingers,69 often superimposed on a background of acrocyanosis. Idiopathic perniosis is characterized histologically by edema of the papillary dermis and by the presence of superficial and deep perivascular lymphocytic infiltrates. Necrotic keratinocytes and lymphocytic vasculitis also have been reported. Thickening of blood vessel walls with intimal proliferation may lead to obliteration of the vascular lumen.70-72
A peculiar clinical presentation may occur in young women riding horses for several hours daily during winter.73,74 Indurated red-to-violet tender plaques develop on the lateral calves and thighs (see Fig. 98-13D). The condition is quite similar to the nodular perniotic lesions described in adolescent girls with erythrocyanosis. For prophylaxis, experienced
17
riders usually wear baggy riding pants that provide insulation and are not tight enough to compromise the circulation. Perniotic lesions have been described in association with myeloproliferative disorders,75 probably as a consequence of blood flow changes, presence of cold agglutinins, and altered inflammatory response on cooling. Chilblains lupus is a distinct disease in which lesions occur as a variant of chronic cutaneous lupus or in the setting of systemic lupus erythematosus.72 Additional associations reported in cases of secondary pernio include connective tissue diseases other than lupus, monoclonal gammopathies, hyperviscosity syndromes, cryoglobulinemia, antiphospholipid positivity, and viral infections.72,76 Of note, lupus pernio is a variant of sarcoidosis (see Chap. 35) and is unrelated to cold injuries. The unfamiliarity of physicians with pernio sometimes gives rise to unnecessary hospital admissions with expensive laboratory and radiologic evaluations and, at times, hazardous therapy. All patients with pernio should undergo a detailed history, review of systems, and physical examination with or without a skin biopsy based on the degree of clinical certainty.76 Laboratory workup (eg, complete blood count with peripheral smear, serum protein electrophoresis, antinuclear and extractable nuclear antigen antibodies, rheumatoid factor, cold agglutinins, and antiphospholipid antibodies) should be conducted only if the history and physical suggest a possible underlying systemic disease. Pernio demonstrating a chronic course (continuous for at least 4 weeks and, in some cases, 8 weeks or longer, or episodic in nature), persistence into warm weather months, and onset in the elderly may be suggestive of an associated connective tissue disease, hematologic malignancy, or other systemic condition.66,72,76,77
The most important point in management of pernio is prevention through the use of adequate, loose, insulating clothing and appropriate warm housing and workplace. Tight garments, such as gloves, stockings, and shoes, are especially to be avoided in cases in which there is concomitant peripheral vascular disease. Instead, mittens can be useful for the hands. Minimizing moisture and maintaining blood circulation by avoiding immobility are also helpful. Once pernio occurs, treatment is symptomatic with rest and warmth. Other conservative measures include smoking cessation and application of a midpotency topical steroid up to twice daily until lesions resolve. Associated systemic diseases, if present, should be treated. Second-line therapy for pernio consists of the addition of a calcium channel blocker, such as nifedipine 20 to 60 mg/day. Third-line and alternative management options include aspirin, pentoxifylline, nicotinamide, topical minoxidil, topical nitroglycerin, and tacrolimus ointment. A related condition known as pulling-boat hands has been described, characterized by the presence of erythematous macules and plaques on the dorsum of the hands and fingers of sailors aboard rowboats.78
Small vesicles developed later, accompanied by itching, burning, and tenderness. These individuals were exposed to long periods of high humidity, cool air, and
1673
17
A
B
wind, an ideal setting for the development of nonfreezing cold injury. In addition, hours of vigorous rowing daily produced repetitive hand trauma.
COLD URTICARIA AND POLYMORPHOUS COLD ERUPTION
Acquired cold urticaria is a form of physical urticaria. Lesions occur at sites of localized cooling, usually when the area is rewarmed. The disease is recognized
1674
C
D
by wheal and flare-type reactions and/or angioedema. Its morphology is indistinguishable from other forms of urticaria. The condition may be idiopathic or associated with some serologic abnormality.79-83 It accounts for approximately 2% of cases of urticaria (see Chap. 41). Immunoglobulin E and, more rarely, immunoglobulin M have been implicated in the pathogenesis. Histamine from mast cell degranulation is one of the most important mediators, but leukotrienes, platelet-activating factor, and others also have been implicated. Familial cold urticaria is a rare autosomal dominant condition with onset at an early age and persistence throughout life.84-86 Urticaria develops when the patient is exposed to generalized cooling, particularly chilling
wind, rather than local cold application. In addition to urticaria, headache, fever, arthralgia, leukocytosis, and swelling of the oral mucosa and esophagus can occur. The delayed type of familial cold urticaria is characterized by localized angioedema developing 24 to 72 hours after cold exposure. Coexistence with dermatographism or cholinergic urticaria is common. Alarming signs resembling histamine shock may lead to loss of consciousness. Death while swimming in cold water has been reported. A mutation in the CIAS1 gene, which is responsible for cold-induced autoinflammatory syndrome, has been identified.85
Cold urticaria may occur in 3% to 4% of patients with cryoglobulinemia, and it also may be associated with cold agglutinins, cryofibrinogens, and cold hemolysins. It has been reported in cases of infectious mononucleosis in association with either cryoglobulins or cold agglutinins, but such occurrences are rare. Cold urticaria also may be a sign of the Muckle-Wells syndrome that associates urticaria, deafness, and amyloidosis.87 In this rare genetic disorder, recurrent bouts of urticaria, fever, chills, and malaise may occur from birth and persist throughout life. Helicobacter pylori has been suggested as a causative agent in some cases of acquired cold urticaria.88
Diagnosis of cold urticaria is confirmed by a cold challenge induced by an ice cube wrapped in a plastic bag placed on the skin of the forearm for periods varying from 30 seconds to 10 minutes (Fig. 98-14). Wheals form on rewarming. Sometimes water at 7°C (44.6°F) is more effective, presumably because it causes lesssevere vasoconstriction. Peltier effect-based temperature challenge appears to be an improved method for diagnosis.89 The Peltier effect relies on using 2 different sufficiently cold, microprocessor-controlled heattransferring metals to generate a precise skin surface temperature to induce lesions.
17
Avoiding cold wind exposure and swimming in cold water are important preventive measures in cold urticaria. In the acquired form, 50% of cases improve or resolve within 5 to 6 years.86 Second-generation H1 antihistamines, up to 4 times the standard dose, are first-line for treatment.86 Adjunctive agents and therapies for refractory cases include sedating antihistamines, H2 blockers, montelukast, omalizumab, cyclosporine, and other immunosuppressives. Patients should also be considered for epinephrine pen prescription because of the anaphylaxis risk. Desensitization to cold is possible by immersing 1 arm into water at 15°C (59°F) for 5 minutes daily. Cold erythema seems to be a related disorder with erythema and pain but without urticaria. Familial polymorphous cold eruption is a rare autosomal dominant disease characterized by childhood onset of nonpruritic, erythematous patches often accompanied by influenza-like symptoms and leukocytosis after generalized exposure to cold. Results of the ice cube test are negative. The pathogenesis remains unknown. The disease frequently has been referred to as familial cold urticaria, although the skin lesions are not urticarial.90
COLD PANNICULITIS AND RELATED ENTITIES
Nonfreezing injuries also can lead to inflammatory reactions in the subcutaneous fat layers, a condition called cold panniculitis. This condition is more common in children than in adults. It most commonly affects the cheeks and legs. Eating popsicles is a common trigger in children who develop the condition on the cheeks, so this entity is sometimes referred to as “popsicle panniculitis.” Tender erythematous subcutaneous nodules appear 1 to 3 days after exposure. Delayed presentation in an adult has been reported 10 days after initiation of post–surgical procedure cold therapy.91 Because of the adipocyte apoptosis that can result from the cold temperature, mild subcutaneous atrophy in the form of dimpling can occasionally follow cold panniculitis. Cosmetic device manufacturers have capitalized on this fat loss effect to manufacture and market fat-cooling devices to reduce fat layers for improved cosmetic contouring.92 When suspecting cold panniculitis, an ice cube challenge to the patient’s skin for 10 minutes should result in the development of an erythematous subcutaneous plaque 12 to 18 hours later. A perivascular mixed infiltrate with neutrophils, lymphocytes, and histiocytes is present at the dermal–subcutaneous junction after 24 hours, followed by a well-developed, primarily lobular panniculitis at 48 to 72 hours. An overlying superficial and deep perivascular dermal lymphocytic infiltrate also may be seen. Some adipocytes are necrotic and rupture to form cystic spaces. Infants have a higher content of saturated fatty acids in adipose tissue than do adults, and this may result in
1675
17
solidification at less-cold temperatures.93,94 Cold panniculitis should be distinguished from other related disorders, including erythrocyanosis with nodules, sclerema neonatorum, and subcutaneous fat necrosis of the newborn. When the diagnosis is clear from history, biopsy to confirm cold panniculitis is not usually necessary, and care usually consists of reassurance and supportive analgesia as necessary. Lesions typically subside spontaneously within 2 to 3 weeks.
SCLEREMA NEONATORUM AND SUBCUTANEOUS FAT NECROSIS OF THE NEWBORN
See Chaps. 64 and 103.
RAYNAUD PHENOMENON
See Chap. 145.
CRYOGLOBULINEMIA
See Chap. 144.
LIVEDO RETICULARIS
See Chap. 148.
ERYTHROMELALGIA
See Chap. 148.
ACKNOWLEDGMENTS
We would like to thank Gérald E. Piérard, Pascale Quatresooz, and Claudine Piérard-Franchimont, the authors of the previous version of this chapter.

Figure 98-1 Reticulate appearance of cooled skin in a newborn resulting from the anatomic pattern of the blood supply and factors influencing flow, such as arteriolar vasoconstriction and the increased viscosity of cooled blood.
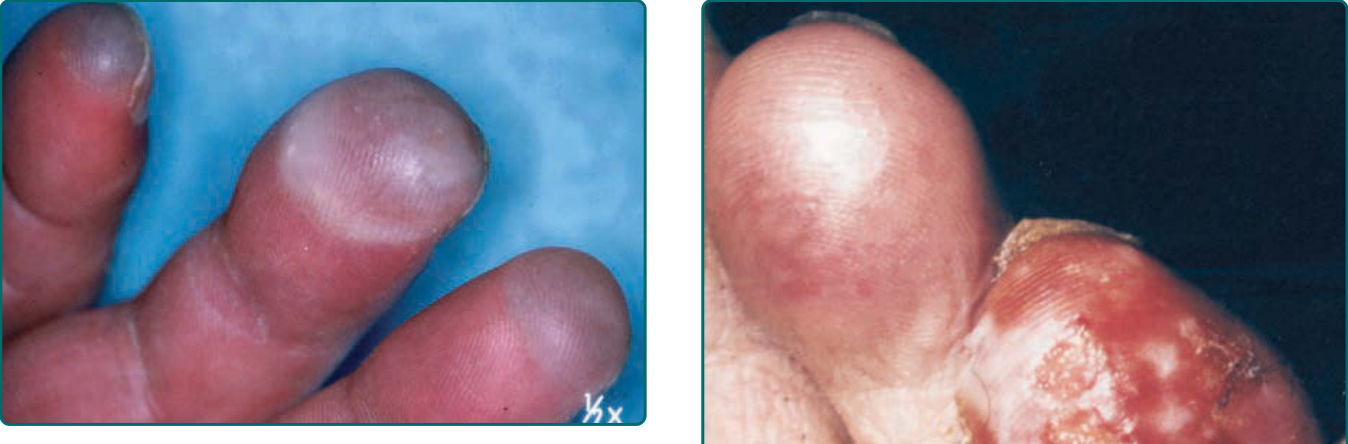
Figure 98-2 Bullous frostbite following contact with a cold steel sheet.

Figure 98-3 Frostnip.

Figure 98-4 Superficial frostbite.

Figure 98-5 Deep frostbite after rewarming. Large blisters have formed. Note cyanosis of the toes as a sign of impending necrosis. This cold injury occurred in a homeless person who was found on the street after heavy alcohol consumption and overnight snowfall.

Figure 98-6 Dry gangrene of all fingers in a mountain climber 5 weeks after being caught in a snowstorm.

Figure 98-7 Iatrogenic bullae from liquid nitrogen treatment. Blister fluid may range from clear (A) to hemorrhagic (B) in appearance.

Figure 98-8 A, Dorsal hand frostbite and (B) “huffer rash” from inhalant abuse.

Figure 98-9 A and B, Acute, subacute, and chronic lesions inflicted by the “salt-and-ice challenge.”
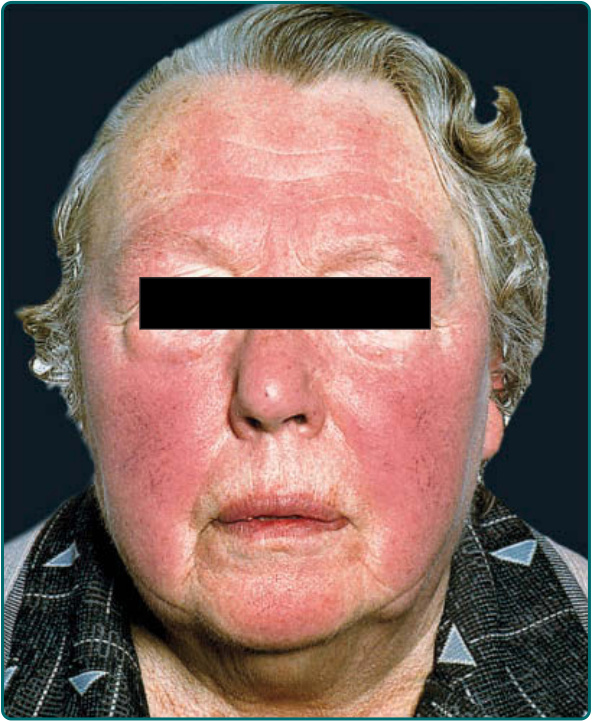
Figure 98-10 Facial redness in a person exposed to cold winters in a temperate climate.

Figure 98-11 Xerosis of the legs of an elderly man in winter.

Figure 98-12 Acrocyanosis of the toes of an elderly woman with peripheral vascular disease. Note the contrast with the examiner’s palmar skin in the background.

Figure 98-13 Pernio is common at sites such as the hands and feet when they are exposed to cooling, moisture, and tight garments. A, Pernio of the dorsal toes. B, Pernio of the plantar feet. C, Pernio of the fingertip. D, Equestrian chilblains from horse riding on a cold morning with inadequate clothing.
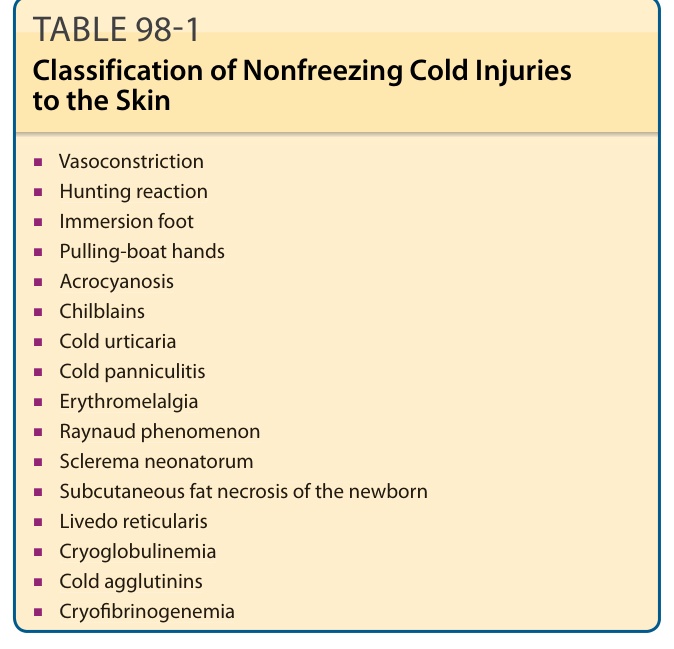
Table 98-1 outlines the classification of nonfreezing cold injuries. Treatment, both physical and pharmacologic, is aimed at keeping the body warm and maintaining vasodilation.
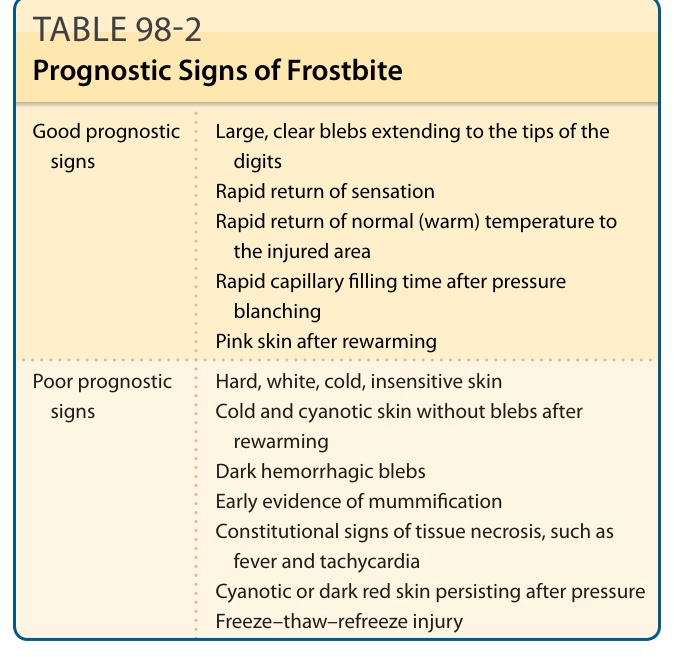
TABLE 98-2 Prognostic Signs of Frostbite