Phototoxicity and Photoallergy
17
AT-A-GLANCE
■ Photosensitivity to exogenous agents is broadly divided into phototoxicity and photoallergy; it is caused by topical or systemic agents that absorb ultraviolet A (UVA) radiation.
■ Phototoxicity occurs in anyone exposed to sufficient doses of phototoxic agent and UV radiation; it usually manifests as an exaggerated sunburn reaction.
■ Photoallergy is an immune reaction to a UVA-modified chemical, commonly topical sunscreen agents and antimicrobials in the United States and the United Kingdom, and topical nonsteroidal antiinflammatory agents in Europe. It presents as eczematous eruption on sun-exposed areas.
■ Phototoxicity and photoallergy do occur in patients with skin of color, frequently resulting in postinflammatory hyperpigmentation.
■ History taking is an important part of the evaluation; phototesting and photopatch testing are sometimes helpful.
■ Differential diagnosis includes contact allergic or contact irritant dermatitis, airborne contact dermatitis, and other photodermatoses.
■ Management consists of identification and avoidance of the precipitating agent, photoprotection, and symptomatic therapy.
Photosensitivity may be caused by exogenous or endogenous agents. It occurs when a compound, classically one with unsaturated double bonds in a 6-carbon ring, absorbs radiation energy in its action spectrum, usually ultraviolet A (UVA) wavelengths. Exogenous photosensitizers can be agents administered systemically or applied topically. Well-characterized examples of photosensitivity induced by endogenous photosensitizers are the cutaneous porphyrias, which are associated with enzymatic defects in heme biosynthetic pathways that result in elevated levels of porphyrins, known phototoxic agents. This is covered in Chap. 124. This chapter focuses on photosensitivity induced by exogenous agents, which can be divided into phototoxicity and photoallergy. Phototoxicity is the result of direct tissue injury caused by the phototoxic agent and radiation. It can occur in all individuals exposed to adequate doses of the agent and the activating wavelengths of radiation (Table 97-1). In contrast, photoallergy is a type IV delayed hypersensitivity response to a molecule that has been modified by absorption of photons. It has a sensitization phase,
occurs only in sensitized individuals, and requires only a minimal concentration of the photoallergen (Table 97-1).
PREVALENCE
Even though hundreds of medications in the United States are reported to cause photosensitivity, only a small number of them induce reactions frequently or have been well studied (Tables 97-2 to 97-5).1 In evaluations performed at photodermatology centers in New York City, Melbourne, Singapore, and Detroit, photosensitivity induced by systemic drugs was documented in 5% to 16% of the referred patients.2-5 These data from different parts of the world indicate that photoallergy and phototoxicity do occur in patients with skin of color, frequently resulting in postinflammatory hyperpigmentation. Studies on photopatch testing published between 2011 and 2016 from different parts of the world showed from 1.5% to 74% of patients who had photopatch testing performed had positive response.6-12
Most of the photosensitivity induced by systemic medications are phototoxicity, whereas those induced by topical agents are photoallergy. However, it should be noted that clinically, it is not always possible to clearly differentiate between phototoxicity and photoallergy. Because many drug-induced photosensitivity has not been well-studied, it is possible that it is underestimated.1,13
PHOTOTOXICITY
CLINICAL FEATURES
CLINICAL FEATURES
ACUTE PHOTOTOXICITY
This occurs within hours of exposure to the phototoxic agent and UV radiation. Symptoms are drugdose and UV-dose dependent; at sufficient doses, the patient complains of a burning and stinging sensation on exposed areas, such as forehead, nose, V area of the neck, and dorsa of the hands (Fig. 97-1). Erythema and edema may appear within hours of exposure; in severe cases, vesicles and bullae may develop accompanied by pruritus. Protected areas, such as nasolabial folds, postauricular and submental areas, and areas covered by clothing, are spared. A notable exception to these kinetics is psoralen-induced phototoxicity, in which the acute response first appears after 24 hours, and peaks at 48 to 72 hours; this is the rationale for administering psoralen plus UVA (PUVA) photochemotherapy treatments 48 to 72 hours
17
PHOTOTOXICITY PHOTOALLERGY
Clinical presentation Exaggerated sunburn reaction: erythema, edema, vesicles, and bullae; burning, stinging; frequently resolves with hyperpigmentation Eczematous lesions; usually pruritic
Histologic features Eosinophilic keratinocytes, epidermal necrosis, dermal edema, sparse dermal infiltrate of lymphocytes, macrophages, and neutrophils Spongiotic dermatitis, dermal lymphohistiocytic infiltrate
Pathophysiology Direct tissue injury Type IV delayed hypersensitivity response
Occurrence after first exposure Yes No
Onset after exposure Minutes to hours 24-48 hours
Dose of agent needed for reaction Large Small
Cross-reactivity with other agents None Common
Diagnosis
Topical agent Clinical Photopatch tests
Systemic agent Clinical + phototests Clinical + phototests; possibly
Systemic agent Clinical + phototests Clinical + phototests; possibly photopatch tests
apart. The phototoxic response resolves with a varying degree of hyperpigmentation, which may last for months. At lower drug/UV doses, gradual tanning only, without preceding sunburn-like reaction, can be seen.
PHOTOONYCHOLYSIS
Separation of the distal nail from the nail bed, which could be asymptomatic, is a manifestation of acute phototoxicity, with the nail plate serving as a lens to focus UV energy on the nail bed. It has been reported with doxycycline and other tetracyclines,13 fluoroquinolones, psoralens, benoxaprofen, clorazepate dipotassium, olanzapine, aripiprazole, indapamide, and quinine (Fig. 97-2).
AGENT EXPOSURE
Phototoxic Agents
Fluorescein Used topically to visualize the anterior surface of the eye
Furocoumarins Occur naturally in plants (especially Compositae species), including fruits and vegetables (lime, lemon, celery, fig, parsley, and parsnip); used in topical photochemotherapy
Rose bengal Used in ophthalmologic examinations
Tar Used as topical therapeutic agent; found in roofing materials
Photosensitizing Agenta
Fluorouracila Topical treatment of actinic keratoses
Retinoidsa For treatment of acne and photoaging
Retinoidsa For treatment of acne and photoaging
1658
aInduces exaggerated ultraviolet response because of skin irritancy.
photopatch tests
SLATE-GRAY PIGMENTATION
Asymptomatic blue-gray pigmentation on sunexposed areas is associated with exposure to several agents.14-16 These agents include amiodarone, chlorpromazine, clozapine, imipramine and, less commonly, desipramine. A drug metabolite–melanin complex is postulated to be the cause of this alteration. Minocycline can induce blue-gray pigmentation on sun-exposed areas such as face (Fig. 97-3), frequently on sites of acne scars, forearms, and shins; however, it also has been reported in non–sun-exposed sites such as mucosal surface, trachea, tympanic membrane, teeth, and cartilage. Chronic exposure to diltiazem, a benzothiazepine calcium channel blocker, has resulted in photodistributed, reticulated, slate-gray pigmentation. Slate-gray pigmentation seen in argyria involves the nail lunulae, mucous membranes, and sclerae. A photochemical reaction, in which silver granules are deposited in the dermis, results in these pigmentary alterations.
PSEUDOPORPHYRIA
The development of porphyria cutanea tarda–like cutaneous changes of skin fragility, vesicles, and subepidermal blisters is associated with several phototoxic agents (Fig. 97-4). In contrast to porphyria cutanea tarda, the porphyrin profile is normal or in the upper range of normal in these patients. Naproxen is the most commonly reported causative agent. Other drugs and treatment modality incriminated include amiodarone, β-lactam antibiotics, celecoxib, ciprofloxacin, cyclosporine, diflunisal, etretinate, furosemide, imatinib, nabumetone, nalidixic acid, narrowband UVB, oral contraceptives, oxaprozin, ketoprofen, mefenamic acid, the tetracyclines, tiaprofenic acid, torsemide, and voriconazole.17,18
Systemic Phototoxic Agents TABLE 97-3
CLASS GENERIC NAME (COMMON U.S. TRADE NAMES)a
Antiandrogen
Bicalutamide (Casodex) Flutamide (Eulexin)
Antifibrotic agent Pirfenidone (Esbriet)
Antifungal agents
Griseofulvin (Fulvicin, Grifulvin V, Gris-PEG)b
Voriconazole (Vfend)c
Antimalarials
Chloroquine (Aralen) Quinineb
Antimicrobials
Sulfonamides Tetracyclines Demeclocycline (Declomycin)c
Doxycycline (Adoxa, Doryx, Monodox, Periostat, Vibra-Tabs, Vibramycin)c
Minocycline (Arestin, Dynacin, Minocin) Tetracycline (Helidac, Sumycin) Trimethoprim (Bactrim, Polytrim, Primsol, Septra)c
Quinolones Ciprofloxacin (Cipro) Enoxacin (Penetrex)b
Gemifloxacin (Factive) Lomefloxacin (Maxaquin, Okacyn, Uniquin)b,c
Moxifloxacin (Avelox, Moxeza, Vigamox) Nalidixic acid (NegGram)b,c
Norfloxacin (Noroxin, Chibroxin–ophthalmic solution) Ofloxacin (Floxin, Ocuflox–ophthalmic solution) Sparfloxacin (Zagam)c,d
Cardiac drugs
Amiodarone (Cordarone, Nexterone, Pacerone)c
Quinidine (Quinaglute, Quinidex)b
Diuretics
Furosemide (Lasix)c
Thiazides Bendroflumethiazide (Aprinox, Naturetin) Bendroflumethiazide/Nadolol (Corzide) Chlorothiazide (Diuril)c
Hydrochlorothiazide (Apo-Hydro, Aquazide, BPZide, Dichlotride, Esidrex, Hydrochlorot, HydroDIURIL, HydroSaluric, Hypothiazid, Microzide, Oretic, and others; frequently used as a fixed dose combination with other classes of hypertensive drugs)c
Dyes
Fluorescein (Ful-Glo, Fluorescite, AK-Fluor) Methylene blue
Furocoumarins
Psoralens 5-Methoxypsoralenc
8-Methoxypsoralen (Oxsoralen-Ultra)c
Hypoglycemics
Hypoglycemics Sulfonylureas
Sulfonylureas Chlorpropamide (Diabinese) Glipizide (Glucotrol) Glipizide/Metformin (Metaglip) Glyburide (DiaBeta, Glynase, Micronase) Glyburide/Metformin (Glucovance) Tolazamide (Tolinase) Tolbutamide (Orinase)c
Chlorpropamide (Diabinese) Glipizide (Glucotrol) Glipizide/Metformin (Metaglip)
Glyburide (DiaBeta, Glynase, Micronase) Glyburide/Metformin (Glucovance)
Tolazamide (Tolinase) Tolbutamide (Orinase)c
Azathioprine (Azasan, Imuran)
Azathioprine (Azasan, Imuran)
17
CLASS GENERIC NAME (COMMON U.S. TRADE NAMES)a
Immunosuppressant Acetic acid derivative
Nonsteroidal antiinflammatory drugs
Diclofenac (Cambia, Cataflam, Flector, Pennsaid, Solaraze, Voltaren, Zipsor) Alkanone derivative Nabumetone (Relafen)c,d
Anthranilic acid derivative Mefenamic acid (Ponstel) Cyclooxygenase-2 inhibitor Celecoxib (Celebrex) Enolic acid derivative Piroxicam (Feldene)b,c
Propionic acid derivatives Ibuprofen (Advil, Medipren, Motrin, Nuprin) Ketoprofenb
Naproxen (Aleve, Anaprox, Naprelan, Midol, Naprosyn, Rugby, Select)c
Oxaprozin (Daypro) Tiaprofenic acid (Surgam, Surgamyl, Tiaprofen) Salicylic acid derivative Diflunisal (Dolobid) Capecitabine (Xeloda)
Oncologic drugs
Crizotinib (Xalkori) Dacarbazine (DTIC, DTIC-Dome) Dabrafenib (Tafinlar) Docetaxel (Docefrez, Taxotere) Fluorouracil (Adrucil) Methotrexate (Rheumatrex)e
Paclitaxel (Abraxane, Onxol, Taxol) Vemurafenib (Zelboraf)c
Vinblastine (Velban)
Photodynamic therapy agents Porfimer (Photofrin)c
Verteporfin (Visudyne)c
Psychotropic drugs
Alprazolam (Niravam, Xanax) Chlordiazepoxide (Librium) Clozapine (Clozaril, FazaClo) Phenothiazines Chlorpromazine (Largactil, Thorazine)c
Perphenazine (Trilafon) Prochlorperazine (Compazine, Compro)c
Thioridazine (Mellaril) Trifluoperazine (Stelazine) Tricyclics Amitriptyline (Elavil) Amitriptyline/Perphenazine (Duo-Vil, Etrafon, Triavil, Triptafen) Desipramine (Norpramin) Imipramine (Tofranil) Dapsone
Other Hypericin (St John’s wort) Pyridoxine (vitamin B6) Ranitidine (Zantac)
Other
Hypericin (St John’s wort) Pyridoxine (vitamin B6) Ranitidine (Zantac)
aAlthough it is the policy not to use trade names in this book, exceptions are made in cases in which we consider this information to be highly useful.
bAlso reported as a systemic photoallergen.
cCommonly reported.
dWithdrawn from the United States market.
eInduces erythema on previously ultraviolet-exposed sites.
1659
17
GROUP CHEMICAL NAME (TRADE NAME)a
Sunscreens (see Chap. 197)
Benzophenones Benzophenone-3 (oxybenzone)b
Benzophenone-4 (sulisobenzone) Para-aminobenzoic acid (PABA) derivatives Ethylhexyl dimethyl PABA (padimate O)b
PABAb
Cinnamates Ethylhexyl methoxycinnamate (octinoxate)b
Ethoxyethyl methoxycinnamate (cinoxate) Others Butyl methoxydibenzoylmethane (avobenzone, Parsol 1789)b
Octocrylene (octocrylene)b
Octyl triazone Phenylbenzimidazole sulfonic acid (ensulizole)
Fragrances
6-Methylcoumarinb
Musk ambretteb
Sandalwood oil
Antiinfective agents
Surface disinfectants: halogenated salicylanilides Dibromosalicylanilide (dibromsalan, DBS)b
Tetrochlorosalicylanilide (Irgasan BS200)b
Tribromosalicylanilide (tribromsalan, TBS)b
Skin cleansers Chlorhexidine (Hibiclens) Hexachlorophene (pHisoHex) Pesticides Bithionol (thiobis-dichlorophenol)b
Dichlorophene (G4, Korium, Teniatol) Dimethylol dimethyl hydantoin Fenticlor (bis-hydroxy-chlorophenyl sulfide)b
Personal care products Triclosan (Irgasan DP300, Microban, Lexol 300) Topical antifungals Buclosamide (Jadit, butylchlorosalicylamide) Multifungin (bromochlorosalicylanilide, BCSA)
Others Antibiotic for cattle
Antibiotic for cattle Olaquindoxb
Olaquindoxb
Nonsteroidal antiinflammatory agents (topical) Etofenamate Fepradinol Flufenamic acid Ketoprofen (Oruvail gel, Powergel, Tiloket gel)b
Nonsteroidal antiinflammatory agents (topical)
Etofenamate Fepradinol Flufenamic acid Ketoprofen (Oruvail gel, Powergel, Tiloket gel)b
Phenothiazines Chlorpromazine (Thorazine)b
Phenothiazines
Chlorpromazine (Thorazine)b
Promethazine (Phenergan)b
Promethazine (Phenergan)b
Miscellaneous Acyclovir cream (Zovirax) Clioquinol (Vioform, iodochlorhydroxyquin) Cadmium sulfide Cinchocaine (Dibucaine) Thiourea (thiocarbamide, sulfourea)
Miscellaneous
Acyclovir cream (Zovirax) Clioquinol (Vioform, iodochlorhydroxyquin) Cadmium sulfide Cinchocaine (Dibucaine) Thiourea (thiocarbamide, sulfourea)
aAlthough it is the policy not to use trade names in this book, exceptions are made in cases in which we consider this information to be highly useful.
bCommonly reported to be photoallergens.
1660
PROPERTY GENERIC NAME (U.S. TRADE NAMEa)
Antifungal Griseofulvin (Fulvicin, Grifulvin V, Gris-PEG)
Antimalarial Quinine
Antimicrobials
Quinolone Enoxacin (Penetrex)
Cardiac medication Quinidine (Quinaglute, Quinidex)
Nonsteroidal antiin- flammatory drugs Ketoprofen Piroxicam (Feldene)
Vitamin Pyridoxine hydrochloride (vitamin B6)
Vitamin Pyridoxine hydrochloride (vitamin B6)
aAlthough it is the policy not to use trade names in this book, exceptions are made in cases in which we consider this information to be highly useful.
ACCELERATED PHOTO-INDUCED CHANGES
This has been uniquely described with voriconazole, a broad-spectrum antifungal agent.18 Immunosuppressed patients receiving voriconazole for longer than 12 weeks can develop photosensitivity, pseudoporphyria, photoaging, lentigines, or premature dermatoheliosis; in addition, squamous cell carcinoma and melanoma have been described in patients who were on voriconazole for longer than 12 months.
PHOTODISTRIBUTED TELANGIECTASIA
This has been reported with calcium channel blockers, including nifedipine, amlodipine, felodipine, and diltiazem, with the antibiotic cefotaxime, and with the antidepressants venlafaxine and escitalopram.19
17
LICHENOID PHOTOSENSITIVE ERUPTION
This has been reported with doxycycline, capecitabine,20
and other agents.
PERSISTENCE OF PHOTOSENSITIVITY AND EVOLUTION TO CHRONIC ACTINIC DERMATITIS
Phototoxicity usually resolves after discontinuation of the causative agent; however, persistence of photosensitivity for many years after the cessation of exposure, resulting in the development of chronic actinic dermatitis has been reported (Fig. 97-5). This has been reported with thiazides, quinidine, quinine, and amiodarone.
CHRONIC EFFECTS
These are best exemplified by the manifestations in patients who have received long-term PUVA photochemotherapy. These effects include premature aging of the skin, lentigines, squamous cell and basal cell carcinomas, and melanoma.
PHOTOTOXIC AGENTS
PHOTOTOXIC AGENTS
TOPICAL AGENTS
1661
17
and retinoids induce exaggerated UV response as a result of their irritant effect on the skin, although systemically administered fluorouracil can induce phototoxicity. Topical exposures to furocoumarins, which are present in limes, celery, figs, and parsnips, may occur in individuals coming into regular contact with them (bartenders, salad chefs, gardeners) and in patients receiving topical photochemotherapy with psoralens. Crude coal tar, although no longer commonly used in dermatologic therapy, is well documented to produce a burning and stinging sensation on exposure to UVA (known as “tar smarts”).
SYSTEMIC AGENTS
PATHOPHYSIOLOGY
PATHOPHYSIOLOGY
Several pathways eventuate in the development of phototoxic tissue damage, and for many phototoxic agents more than one pathway is responsible.21
PHOTODYNAMIC PROCESSES
This involves absorption of radiation energy by the photosensitizer and formation of an excited molecule. Subsequent generation of reactive oxygen species result in tissue injury. Phototoxicities induced by porphyrins, quinolones, nonsteroidal antiinflammatory agents, tetracyclines, amitriptyline, imipramine, sulfonylureas, hydrochlorothiazide, furosemide, and chlorpromazine are examples of photodynamic phototoxic reactions.
GENERATION OF PHOTOPRODUCTS
Stable photoproducts induced by exposure to radiation can be responsible for tissue injury. Phototoxic products have been demonstrated on irradiation of phenothiazines, chlorpromazine, tetracyclines, quinolones, and nonsteroidal antiinflammatory agents.
BINDING TO SUBSTRATE
An example of this mechanism is the covalent binding of 8-methoxypsoralen to pyrimidine bases of the DNA molecules upon exposure to UVA, which results in the formation of a crosslink between the DNA strands.
1662
INFLAMMATORY MEDIATORS
Mediators of inflammation and inflammatory cells participate in phototoxic tissue injury. Biologically active products of complement activation, mast cell-derived mediators, eicosanoids, proteases, and polymorphonuclear leukocytes contribute to the development of phototoxicity induced by porphyrins, demeclocycline, and chlorpromazine.
APOPTOSIS
In addition to generating reactive oxygen species, photodynamic therapy also is a potent inducer of apoptosis.22 This is discussed in detail in Chap. 199.
HISTOPATHOLOGY
HISTOPATHOLOGY
Acute phototoxicity is characterized by individual necrotic keratinocytes and, in severe cases, epidermal necrosis (see Table 97-1). There may be epidermal spongiosis, dermal edema, and a mild infiltrate consisting of neutrophils, lymphocytes, and macrophages. Slate-gray pigmentation is associated with increased dermal melanin and dermal deposits of the drug or its metabolite.23 Histologic features of lichenoid eruptions are similar to those of idiopathic lichen planus; however, there may be a greater degree of spongiosis and dermal eosinophilic and plasma cell infiltrates, and a larger number of necrotic keratinocytes and cytoid bodies. In pseudoporphyria, as in porphyria cutanea tarda, there is dermal–epidermal separation at the lamina lucida and deposits of immunoglobulins at the dermal–epidermal junction and surrounding blood vessel walls.
MANAGEMENT
MANAGEMENT
Identification and avoidance of the causative phototoxic agent, along with rigorous photoprotection, are the most important steps in management. Photoprotection includes seeking shade when outdoors, wearing photoprotective clothing, a widebrimmed hat, sunglasses, and applying sunscreen to exposed areas.24 Because the action spectrum for most agents is in the UVA range, high sun protection factor, broad-spectrum sunscreens should be used (see Chap. 197). Acute phototoxicity can be managed with topical corticosteroids and compresses; systemic corticosteroids can be used for the most severely affected patients. Management of patients with slate-gray pigmentation, lichenoid eruption, pseudoporphyria, and photodistributed telangiectasia is symptomatic only, and patients should be advised that it will take months after the discontinuation of the offending agent for the condition to resolve. For patients with slate-gray pigmentation, hydroquinone or hydroquinone-containing
combination products can be used; however, because the location of pigments is in the dermis, these products are not completely effective. Patients with nonsteroidal antiinflammatory drug-induced pseudoporphyria who require nonsteroidal antiinflammatory drugs should be switched to a different class of agents or to those that are less photosensitizing, such as indomethacin or sulindac.17
PHOTOALLERGY
CLINICAL MANIFESTATIONS
CLINICAL MANIFESTATIONS
In sensitized individuals, exposure to the photoallergen and sunlight results in the development of a pruritic, eczematous eruption within 24 to 48 hours after exposure (see Table 97-1). Although the morphology is clinically indistinguishable from that of allergic contact dermatitis, the distribution of the eruption in photoallergy is predominantly confined to sun-exposed areas; however, in severe cases, it may spread to the covered areas, albeit at a lower intensity. Unlike the lesions in phototoxicity in fair-skinned individuals, those in photoallergy usually resolve without significant postinflammatory hyperpigmentation. Lichenoid eruption also has been reported. As with phototoxicity, persistence of photosensitivity and evolution to chronic actinic dermatitis (see Chap. 95) have been reported after exposure to photoallergens, including chlorpromazine, dioxopromethazine, halogenated salicylanilides, ketoprofen, musk ambrette, olaquindox, and quinidine.25 A proposed mechanism is that UV radiation alters the carrier protein that originally binds the photoallergen; this results in the formation of a neoantigen that stimulates the immune system over the long term. This hypothesis is supported by the observation that the histidine moiety in albumin can undergo oxidation in the presence of salicylanilide, which binds to albumin.
PHOTOALLERGENS
PHOTOALLERGENS
TOPICAL AGENTS
In the United States, Canada, Europe, and the United Kingdom, common photoallergens include UV filters (benzophenone-3, octocrylene, avobenzone, octinoxate), and topical nonsteroidal antiinflammatory drugs (ketoprofen, etofenamate).7-11,26 In China, chlorpromazine and para-aminobenzoic acid were the most common photoallergens in a 10-year study.12 Table 97-4 lists the common photoallergens.
SYSTEMIC AGENTS
These are listed in Table 97-5. Photoallergy caused by systemic agents is not as well documented nor studied. All but one of the photoallergens (pyridoxine) are also phototoxic and were discussed earlier in this
17
chapter (see “Phototoxic Agents: Systemic Agents” and Table 97-3).
HISTOPATHOLOGY
HISTOPATHOLOGY
The histologic features are similar to those of allergic contact dermatitis. There is epidermal spongiosis associated with infiltrate of mononuclear cells in the dermis (see Table 97-1).
PATHOPHYSIOLOGY
PATHOPHYSIOLOGY
Photoallergy is a type IV delayed hypersensitivity response requiring the presence of both photoallergen and the activating wavelengths of radiation (UVA)27; this is the reason that photopatch testing is done using UVA as a light source. After the absorption of UV energy, a photoallergen may be converted to an excited state molecule, which subsequently reverts to ground state by releasing the energy. In this process, the molecule may conjugate with a carrier protein to form a complete antigen. This is thought to be the mechanism of photoallergy induced by halogenated salicylanilides, chlorpromazine, and para-aminobenzoic acid. Alternatively, a photoallergen may form a stable photoproduct on exposure to radiation, which in turn may conjugate with a carrier protein to form a complete antigen. Sulfanilamide and chlorpromazine have both been shown to participate in this reaction. Once the complete antigen is formed, the mechanism of photoallergy is identical to that of contact allergy. The antigen is taken up and processed by epidermal Langerhans cells, which then migrate to regional lymph nodes to present the antigen to T lymphocytes. Cutaneous lesions develop when the activated T lymphocytes circulate to the exposed site to initiate an inflammatory response.
MANAGEMENT
MANAGEMENT
Management is identical to that of phototoxicity: identification and avoidance of the photoallergen, sunprotective measures, and symptomatic therapy.
EVALUATION OF PATIENTS WITH PHOTOTOXICITY AND PHOTOALLERGY
The evaluation of patients with phototoxicity and photoallergy is similar to the evaluation of patients with other photosensitivity disorders. A history of exposure to known photosensitizers is most important. It is also helpful to ascertain whether window glass-filtered sunlight can induce the cutaneous eruption, because UVB is filtered out by window glass. Distribution of
1663
17
the cutaneous eruption is a helpful clue to the type of photosensitizer responsible. Widespread eruption suggests systemic photosensitizers, whereas topical photosensitizers produce lesions only in areas that have been exposed to both sensitizers and radiation. Vesicular and bullous eruptions are most commonly associated with phototoxicity, whereas eczematous eruptions strongly suggest photoallergy; usually, phototoxicity is associated with a burning sensation, and photoallergy with pruritus. Skin biopsy findings also may be helpful in differentiating these 2 conditions: necrotic keratinocytes are commonly seen in phototoxicity, whereas spongiotic dermatitis is associated with photoallergy (see Table 97-1). Phototests and photopatch tests are an integral part of the evaluation of photosensitivity when history and physical examination alone are insufficient to determine the responsible agent. Approximately 10% to 20% of patients who undergo photopatch testing have clinically relevant positive results, which leads to the diagnosis of photoallergic contact dermatitis.2,9
The procedures for phototesting and photopatch testing are generally as follows, although there are variations in testing methods. On day 1, exposure to UVB and UVA to determine minimal erythema doses is carried out, and duplicate sets of photoallergens are applied symmetrically to different sites on the back and covered by an opaque tape. On day 2, the minimal erythema doses are determined. One of the duplicate set of photoallergens is exposed to 10 J/cm2 of UVA or 50% of the minimal erythema dose to UVA, whichever is lower. After irradiation, the exposed site is covered again with an opaque tape. On day 3, both irradiated and nonirradiated test sites are uncovered, and the reactions are graded. On day 5 or day 8, the irradiated and nonirradiated sites are evaluated for delayed reactions. Reaction only at an irradiated site indicates photoallergy. Reaction of equal intensity at both irradiated and covered sites indicates allergic contact dermatitis. Reaction at both sites, but with higher intensity at the irradiated site, signifies both photoallergy and allergic contact dermatitis. Well-defined erythema that resolves promptly indicates an irritant dermatitis.
DIFFERENTIAL DIAGNOSIS OF PHOTOTOXICITY AND PHOTOALLERGY
Airborne allergic contact dermatitis is characterized by involvement of skinfolds on exposed areas, such as the nasolabial folds and the eyelids that receive minimal direct sunlight. It also involves exposed areas that are relatively sun protected, such as the postauricular areas and area under the chin. Allergic contact dermatitis and irritant contact dermatitis occur at sites of contact, in both sun-exposed and sun-protected areas. Other photodermatoses can be differentiated from phototoxicity and photoallergy by their characteristic time course and morphology and lack of exposure to
1664
photosensitizers. Polymorphous light eruption manifests itself within a few hours of sun exposure as pruritic papules, plaques, and, uncommonly, vesicles on sun-exposed sites and resolves in a few days. Chronic actinic dermatitis presents as chronically lichenified plaques on sun-exposed areas. Lesions of solar urticaria appear within minutes of sun exposure as mildly pruritic urticaria and resolve within a few hours.

Figure 97-1 Sulfamethoxazole-trimethoprim–induced phototoxicity. Note the resolving erythema and fine scales on dorsum hand and forearm, and sparing of area covered by watch on the wrist.

Figure 97-2 Distal onycholysis in a patient receiving psoralen plus ultraviolet A therapy.
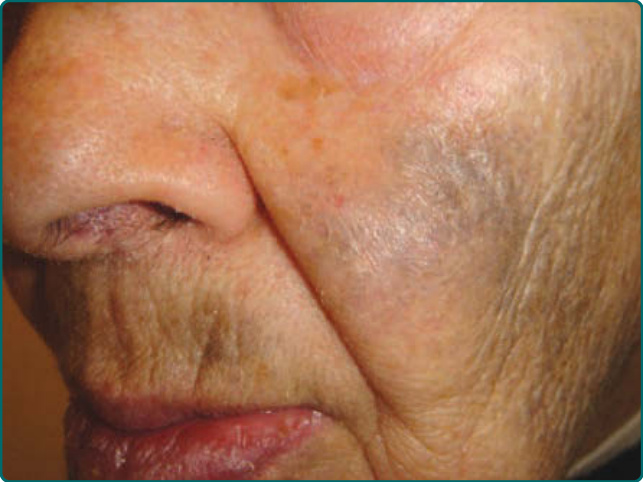
Figure 97-3 Minocycline-induced blue-gray pigmentation on cheeks and upper lip.

Figure 97-4 Pseudoporphyria. Crusted erosion and healed hypopigmented scar on dorsum of hand.
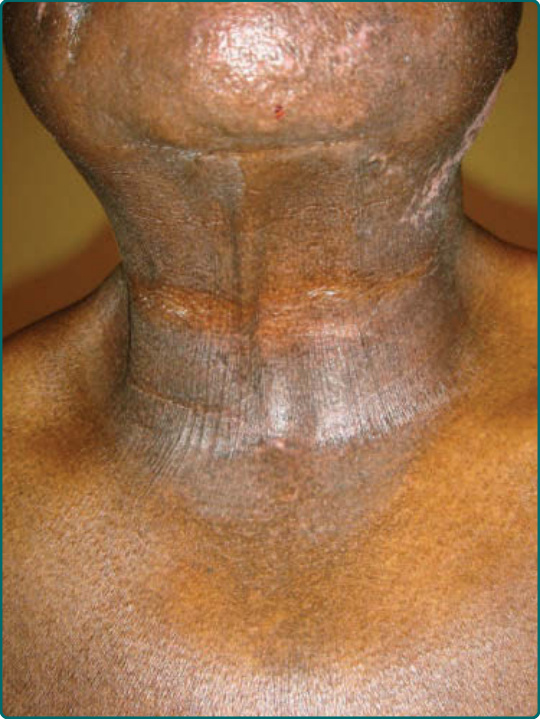
Figure 97-5 Chronic actinic dermatitis. Note the lichenification and hyperpigmentation on sun-exposed areas, and sparing of skin folds.
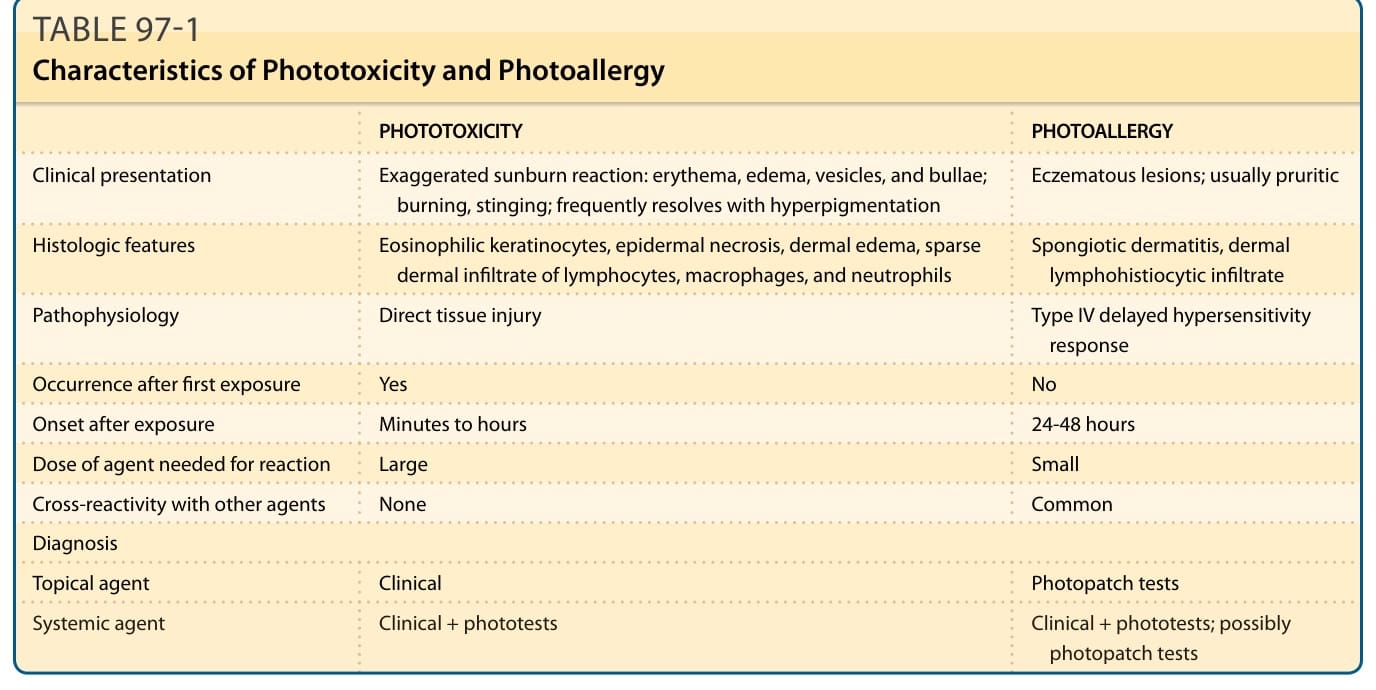
TABLE 97-1 Characteristics of Phototoxicity and Photoallergy
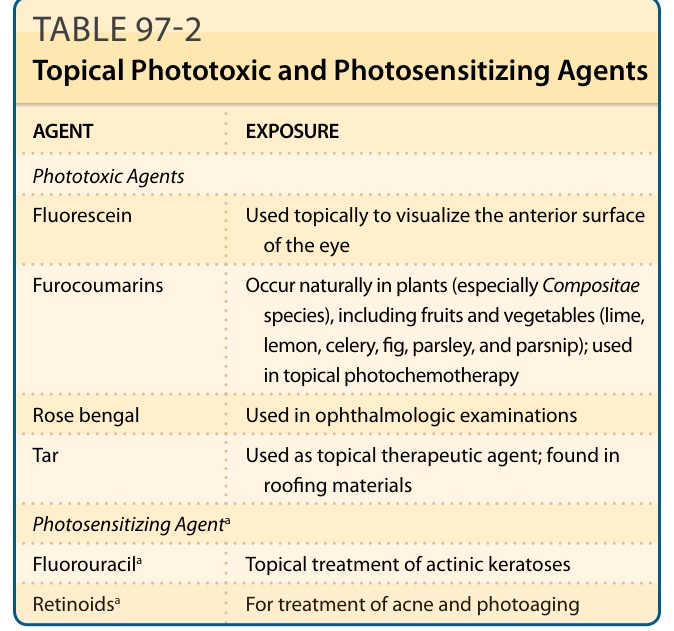
TABLE 97-2 Topical Phototoxic and Photosensitizing Agents
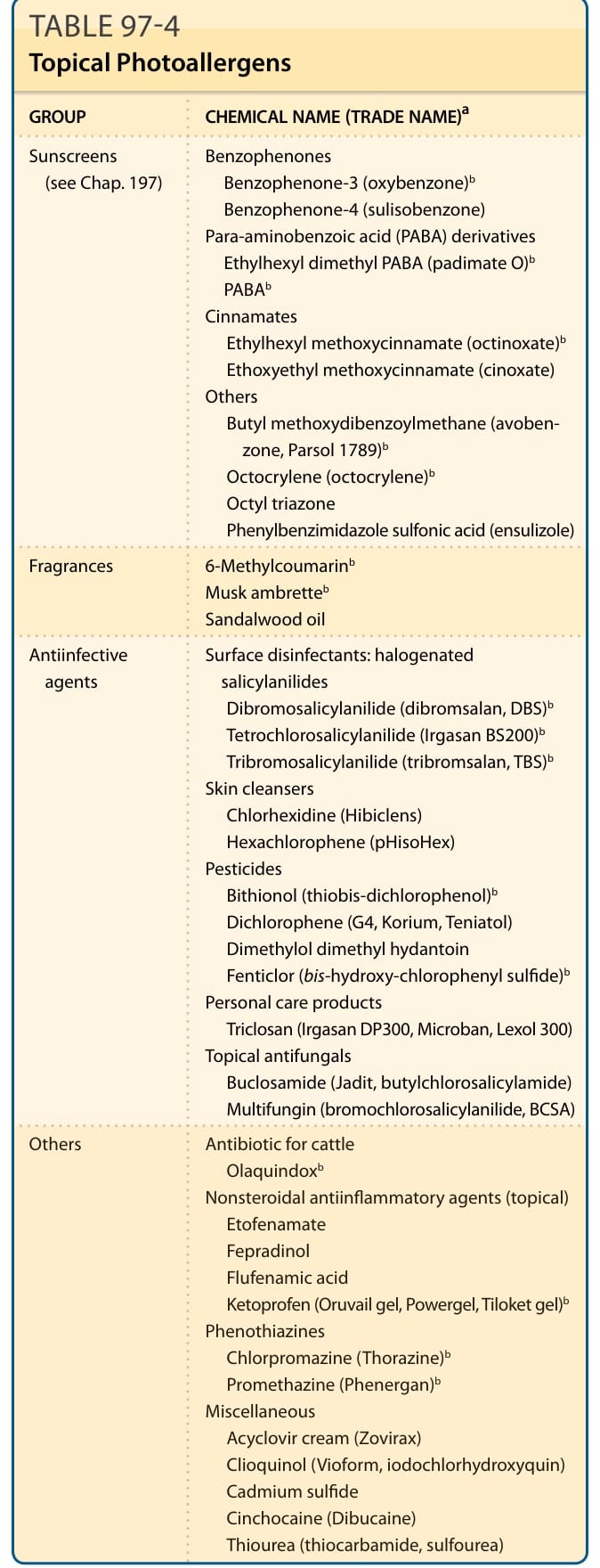
TABLE 97-4 Topical Photoallergens
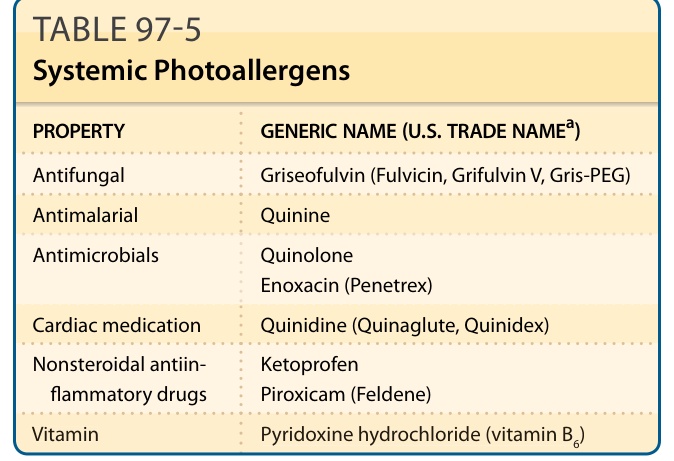
TABLE 97-5 Systemic Photoallergens