Solar Urticaria
17
AT-A-GLANCE
■ An uncommon form of chronic inducible urticaria
■ Erythema and itchy wheals occur within minutes of sunlight exposure and resolve within hours.
■ May be disabling and, rarely, life threatening.
■ Phototesting confirms the diagnosis, determines the trigger threshold, and identifies the eliciting wave lengths.
■ Sensitivity may be to ultraviolet B, ultraviolet A, visible light, and/or any combination, but most commonly to ultraviolet A and visible light.
■ Sunlight avoidance, high–protection factor broad-spectrum sunscreens, and antihistamines may help.
■ Omalizumab may be a helpful second-line treatment
■ Phototherapy may also help but is usually not feasible as long-term treatment
INTRODUCTION
DEFINITIONS
DEFINITIONS
Solar urticaria (SolU) is defined by the appearance of a whealing response within minutes of exposure to sunlight.1 SolU is a rare type of physical urticaria. Physical urticarias, together with cholinergic urticaria, contact urticaria, and aquagenic urticaria, are subforms of chronic inducible urticaria, one of the 2 forms of chronic urticaria, the other one being chronic spontaneous urticaria. SolU usually is primary, where the cause is unknown. Very rarely, SolU is linked to cutaneous porphyria or systemic lupus erythematosus (SLE) and is then termed secondary SolU.
HISTORICAL PERSPECTIVE
HISTORICAL PERSPECTIVE
Chronic inducible urticaria and their characteristic features, that is, wheal responses at skin sites exposed to urticariogenic triggers, were first described by Hippocrates.2 The first reports of SolU are from the 18th century, and in 1887, SolU was identified as being sunlight-dependent.3,4
EPIDEMIOLOGY
The prevalence of SolU is low, but conclusive prevalence data are missing. It has been estimated that 3 in 100,000 are affected.5 SolU reportedly accounts for 7% of all photodermatoses6 and for less than 0.5% of all chronic urticaria cases.7 SolU predominantly affects women in the third decade of life. Most patients show symptoms perennially, some only during spring to autumn.5
CLINICAL FEATURES
CUTANEOUS FINDINGS
CUTANEOUS FINDINGS
SolU is characterized by erythema and itchy wheals that develop rapidly at skin sites exposed to sun or artificial light (Fig. 96-1). Light-exposed skin first shows diffuse erythema, followed by whealing associated with itch and/or, less frequently, burning and stinging. Wheals in SolU generally develop within a few minutes up to 1 hour of exposure and disappear usually within 1 hour and after a maximum of 24 hours of cessation of exposure, without leaving visible changes of the skin. SolU typically affects skin areas that are normally shielded by clothing and it spares skin sites that are frequently exposed to light such as the hands and the face, presumably because chronically sun-exposed areas show “hardening” or tolerance. SolU patients typically experience their first signs and symptoms after prolonged sun exposure on the first sunny days in spring. Rare variants include fixed SolU, which is characterized by the reoccurrence of light-induced whealing in the same location8 and delayed SolU, where the onset of signs and symptoms after UV exposure is delayed by up to several hours. In some SolU patients, bruised skin is more sensitive to light.9 Light-induced angioedema may occur.
NONCUTANEOUS FINDINGS AND COMPLICATIONS
NONCUTANEOUS FINDINGS
AND COMPLICATIONS
Systemic involvement is rare and only occurs when large areas of skin are affected. Generalized signs and symptoms include malaise, nausea, dizziness, headaches, wheezing, dyspnea, loss of consciousness, and even anaphylactic shock, which is rarely fatal.
A
B
17
ETIOLOGY AND PATHOGENESIS
The signs and symptoms of SolU are due to the degranulation of skin mast cells and their subsequent release of histamine and other proinflammatory mediators. These mediators cause vasodilation (erythema) and increased extravasation (wheals, angioedema) and activate sensory nerves of the skin (itch). Widespread light-induced whealing in SolU patients can result in transiently increased blood levels of histamine.10
Skin mast cell degranulation in SolU is due to exposure of the skin to UVA (320 to 400 nm), visible (400 to 600 nm), less commonly UVB (280 to 320 nm), and, rarely, infrared (>600 nm) radiation. The underlying mechanism of mast cell degranulation has not been characterized in detail but is held to involve IgE that is specific for photo-induced neoantigens that act as autoallergens. This IgE is bound to the high-affinity IgE-receptor, FceRI, on cutaneous mast cells, which get activated by neoantigen-mediated crosslinking of IgE and FceRI. The wide range of relevant wavelengths is explained by the contribution of several different neoantigens/photoautoallergens with unique action spectra.11,12 The range of eliciting wavelengths can narrow or broaden during the course of the disease, suggesting that the relevant neoantigens may vary over time. In some patients, skin exposure to distinct wavelength radiation, the so-called inhibition spectrum,
can inhibit whealing in response to the eliciting wavelength spectrum.
RISK FACTORS
RISK FACTORS
Specific risk factors for SolU or predictors for the severity or course of the disease have not yet been identified. SolU affects both genders and shows a female preponderance. The peak age of onset of symptoms is 20 to 40 years. There appears to be no influence of the skin type on the occurrence or severity of SolU.13,14
DIAGNOSIS
SUPPORTIVE STUDIES
SUPPORTIVE STUDIES
The diagnosis of SolU is based on a thorough history. All patients who present with a history of rapid development of itching and whealing after exposure to light, should be investigated for SolU. Patients who report the occurrence of recurring itchy wheals should be asked if whealing can be induced, for example, by sun exposure. Patients who report the development of sunlight-induced skin lesions should be asked if these lesions resemble wheals, for example, if they are itchy, accompanied by erythema, short-lived, and transient.
1651
17
Photodocumentation including self-documentation with smartphone cameras of skin lesions at the time of occurrence is helpful.
LABORATORY TESTING
In SolU, routine laboratory tests are all within normal limits and not helpful for diagnosing the disease. Porphyria and SLE should be excluded by tests for antinuclear antibody (ANA) / extractable antinuclear antibody (ENA) and blood, urine and stool testing for porphyrins, respectively.
PATHOLOGY
SolU skin lesions, within the first hours after elicitation by irradiation, show vasodilation, edema, and perivascular neutrophils and eosinophils in the upper dermis. After 24 hours, mononuclear cells are the dominating infiltrating cells.15 The histopathologic features of SolU do not allow for its distinction from other forms of urticaria.
PHOTOTESTING
Phototesting is essential for confirming the diagnosis of SolU. It also assesses disease activity by determining trigger thresholds and defines individual eliciting and inhibition spectra. Phototesting is performed by exposing patients to ultraviolet radiation and visible light at skin sites that have been protected from light for several days, most commonly the buttocks. No sunscreens, photoactive medications, or urticaria treatments should be used before phototesting, and the washout phase for antihistaminic and immunosuppressive medication prior to test needs to be adequate. Phototesting is done with the help of solar simulators with filters (UVA and UVB) or monochromators (UVA and UVB, visible light) separately for UVA at 6 J/cm,2 UVB at 60 mJ/cm,2 and visible light. The test is considered positive if the test site exhibits a palpable and clearly visible itchy wheal and flare reaction at 10 minutes after phototesting. In patients with a positive phototest reaction, threshold testing is done with a range of doses of the eliciting wavelengths, for example, with UVA at 2.4, 3.3, 4.2, 5.1, and 6.0 J/cm2 and with UVB at 24, 33, 42, 51, and 60 mJ/cm2 (Fig. 96-2). Threshold testing determines the minimal urticarial dose, a marker of disease activity and response to therapy. In patients with a negative phototest and convincing history of lightinduced whealing, SolU should not be excluded, and sunlight phototesting is recommended. Reasons for a negative phototest in patients with SolU include mild disease activity, with variable occurrence of signs and symptoms limited to erythema in some patients, prior intake of antihistamines or other medications that inhibit the development of wheals,
1652
A
B
and/or refractoriness of the skin due to previous light exposure of the test site.
DIAGNOSTIC ALGORITHM
DIAGNOSTIC ALGORITHM
See Fig. 96-3.
DIFFERENTIAL DIAGNOSIS
See Table 96-1.
CLINICAL COURSE AND PROGNOSIS
The mean duration of SolU is 5 to 7 years, but cases with disease duration of up to 50 years have been reported.16 In a recent study, the median duration from disease onset to disease resolution was 63 months, and 50% of patients experienced complete spontaneous remission within 5 years of disease onset.17 In contrast, older studies found rates of resolution of 12%, 26%, and 46% after 5, 10, and 15 years, respectively.5,18
MANAGEMENT
AVOIDANCE OF THE TRIGGER
AVOIDANCE OF THE TRIGGER
All SolU patients should avoid the sun, wear protective clothing, and use high-protection broad-spectrum sunscreens, especially when the threshold is in the ultraviolet spectrum.
17
Diagnostic algorithm and diagnostic work up for solar urticaria
History: Occurrence of signs and symptoms within minutes after sun/light exposure Rule out differential diagnoses (by history and laboratory test [eg, ANA, ENAs, anti-ds-DNA, porphyrine levels in blood, urine, stool] and phototesting with reading after 10 minutes, 48 and 72 hours)
NO
YES
History: First symptoms in early childhood. Painful and burning skin after UV/light exposure rather than itchy wheals
YES
NO
Phototesting: Wheals within minutes after testing
NO
YES
Determine trigger threshold by graded phototesting to determine disease activity of SolU / Determine disease control with Urticaria Control Test (UCT)
Rule out erythropoietic protoporphyria (determine protoporphyrine levels in erythrocytes)
Double check for possible reasons of negative test, eg, intake of antihistamines/ Consider differential diagnoses and read test sites also after 48 and 72 hours
MEDICATIONS
MEDICATIONS
Treatment with nonsedating H1 antihistamines at standard dose is the recommended first-line treatment. Evidence for the efficacy and safety of antihistamine treatment in SolU comes from controlled and uncontrolled studies,19,20 case series and reports, as well as clinical experience. In case of insufficient response to treatment with a standard-dosed nonsedating secondgeneration antihistamine, doses should be increased up to 4-fold. This recommendation is largely based on the results of studies of other forms of inducible urticaria. Antihistamines work, but not in all patients. Updosing is needed in many. Treatment with omalizumab, a monoclonal antibody directed against IgE, is recommended in patients who do not achieve sufficient control with the combined use of sunscreens and antihistamine treatment. For omalizumab, a complete or partial response in doses of up to 450 mg every 4 to 8 weeks
has been reported in several case studies.21-30 The best evidence comes from a recent open-label French multicentric Phase II study with 10 patients31 that shows that omalizumab, at 300 mg every 4 weeks, is of benefit in half of the treated patients. Two reports showed no improvement.32,33
Other therapies that have been reported to be effective in some but not all patients include ciclosporin34
and intravenous high-dose immunoglobins.35,36
Afamelanotide, an alpha-MSH analog and melanocortin receptor agonist recently licensed for the treatment of erythropoietic protoporphyria, was shown to protect SolU patients from the development of signs and symptoms in a small open-label study.37
PROCEDURES
PROCEDURES
Tolerance to UV light can be achieved by desensitization achieved by phototherapy. This treatment is
1653
17
DISORDER DISTINGUISHING FEATURES COMMON FEATURES
Polymorphic light eruption Skin lesions: Papules, papulovesicles, eczematous appearance; occur within hours to days after UV exposure (not within minutes); resolve within several days (not minutes to hours).
May spare face and hands (hardening).
Lupus erythematosus Skin lesions: Occur within days to weeks after UV exposure (not within minutes); resolve within weeks (not minutes to hours). ANAs are positive. Skin lesions with wheallike appearance.
Photoexacerbated eczema (atopic, seborrheic) Skin lesions: No wheals; occur within hours to days after UV exposure (not within minutes); resolve within several days (not minutes to hours).
Photoallergic/phototoxic contact dermatitis Skin lesions: No wheals; occur within hours to days after UV exposure (not within minutes); resolve within several days (not minutes to hours). Photoallergic contact dermatitis: Photopatchtest is positive.
Erythropoietic protoporphyria First symptoms in early childhood and lifelong persistence. Skin (lesions) is/are painful/ burning but not itchy. The pain/burning often persists for hours to days. Elevated levels of protoporphyrin in erythrocytes.
Onset within minutes after UV exposure. Skin lesions may be wheallike.
Porphyria cutanea tarda Increased skin vulnerability in UV-exposed areas. Skin lesions comprise blisters, erosions, scars, milia, hyper- and hypopigmentation, hypertrichosis, elastosis (but not wheals). Elevated porphyrin levels in urine. Liver enzymes frequently elevated.
Drug or chemical photosensitivity Patient uses medication. Skin lesions: Occur within hours to days after UV exposure (not within minutes); resolve within several days (not minutes to hours).
Heat urticaria Phototesting is negative; heat testing is positive. Signs/symptoms identical
Heat urticaria Phototesting is negative; heat testing is positive. Signs/symptoms identical to SolU.
cumbersome and requires high patient compliance.38
Phototherapy needs to be continued to maintain its effect. Discontinuation of phototherapy, in virtually all patients, results in the loss of protection from lightinduced whealing.39
to SolU.
Phototherapy carries the usual risks of long-term phototherapy and should be done with caution because of the risk of anaphylaxis, particularly in severely affected individuals. So-called rush hardening protocols have been described (multiple UVA
Treatment algorithm for solar urticaria
Second-generation H1-Antihistamine (sgAH)
If inadequate control: After 2 to 4 weeks or earlier, if symptoms are intolerable
Increased sgAH dose (up to 4×)
If inadequate control: After 2 to 4 weeks or earlier, if symptoms are intolerable
Add on to sgAH: Omalizumab
If inadequate control: After 2 to 4 weeks or earlier, if symptoms are intolerable
Add on to sgAH: Ciclosporin
Additional treatment options include: phototherapy (UV-hardening), intravenous immunoglobulins, antimalarials, plasmapheresis
1654
exposures with increasing doses during the same day) and may help some patients.40,41
COUNSELING
COUNSELING
Avoidance of sun exposure and the use of high– protection factor broad-spectrum sunscreens and appropriate clothing can help to prevent the development of SolU signs and symptoms.
MONITORING OF TREATMENT RESPONSES AND DISEASE ACTIVITY
MONITORING OF
TREATMENT RESPONSES
AND DISEASE ACTIVITY
Disease activity and control as well as response to treatment should be assessed at every patient visits. Suitable ways to do so include the urticaria control test (UCT) and trigger threshold phototesting.42,43
TREATMENT ALGORITHM
TREATMENT ALGORITHM
See Fig. 96-4.
ACKNOWLEDGMENTS
The authors acknowledge that this contribution is based, in part, on some of the content of the chapter by Travis W. Vandergriff and Paul R. Bergstresser on “Abnormal Responses to Ultraviolet Radiation: Idiopathic, Presumed Immunologic, and Photoexacerbated” in the 8th edition of Fitzpatrick’s Dermatology in General Medicine.
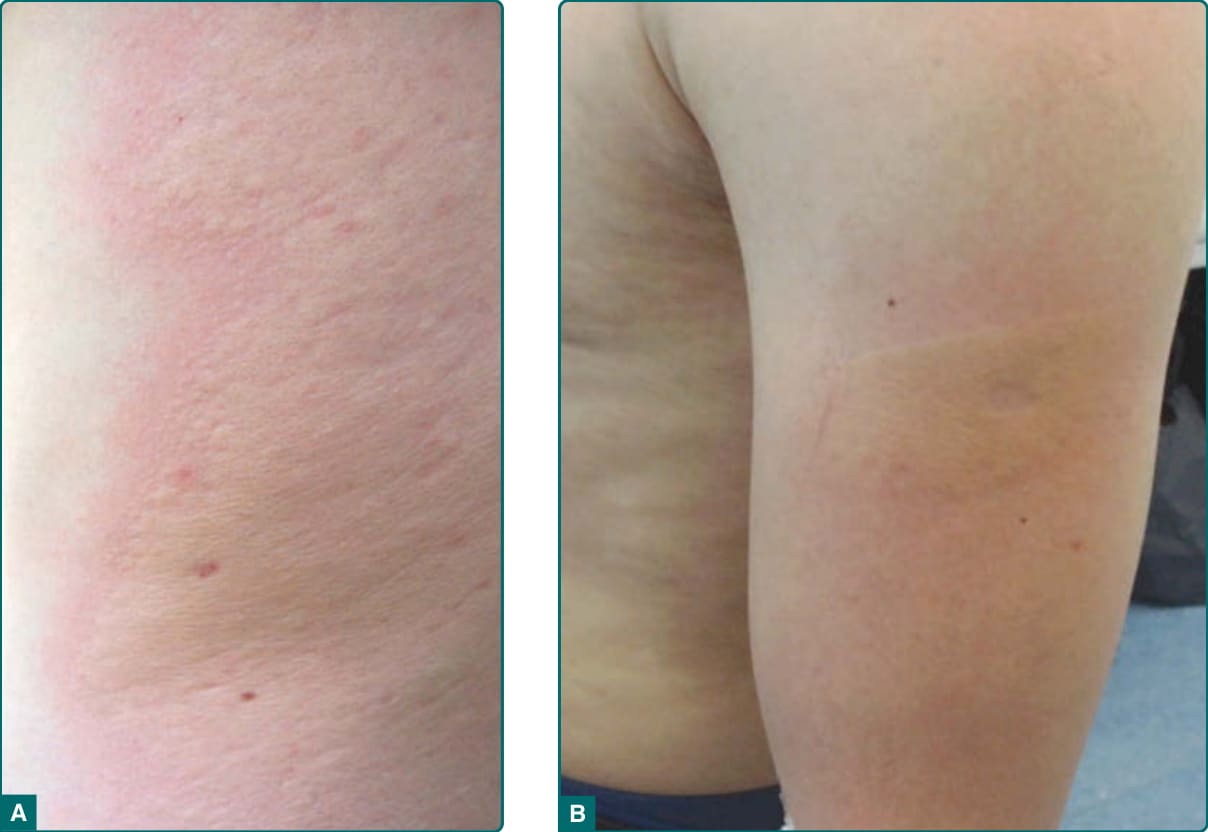
Figure 96-1 Solar urticaria. Pruritic wheals with a surrounding flare occurring 20 minutes after outdoor sun exposure at the arm. A, Close-up of the wheal. B, Lateral arm overview.
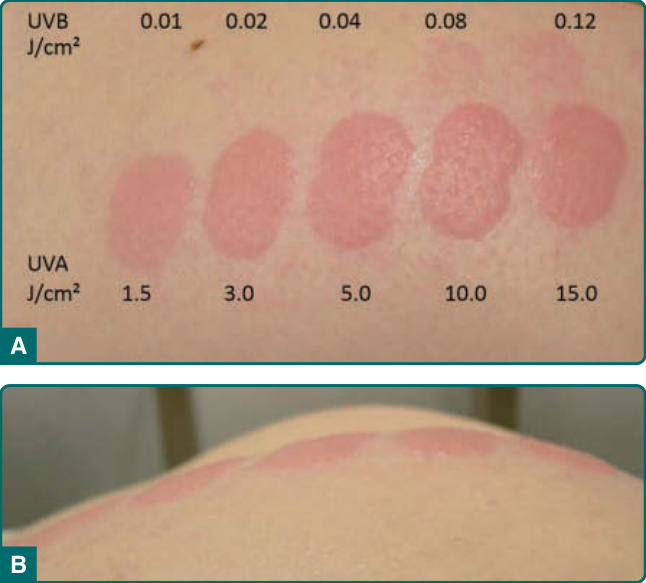
Figure 96-2 UVA and UVB testing with a solar simulator. A, Overview. B, lateral photography to demonstrate the elevation of the wheals.
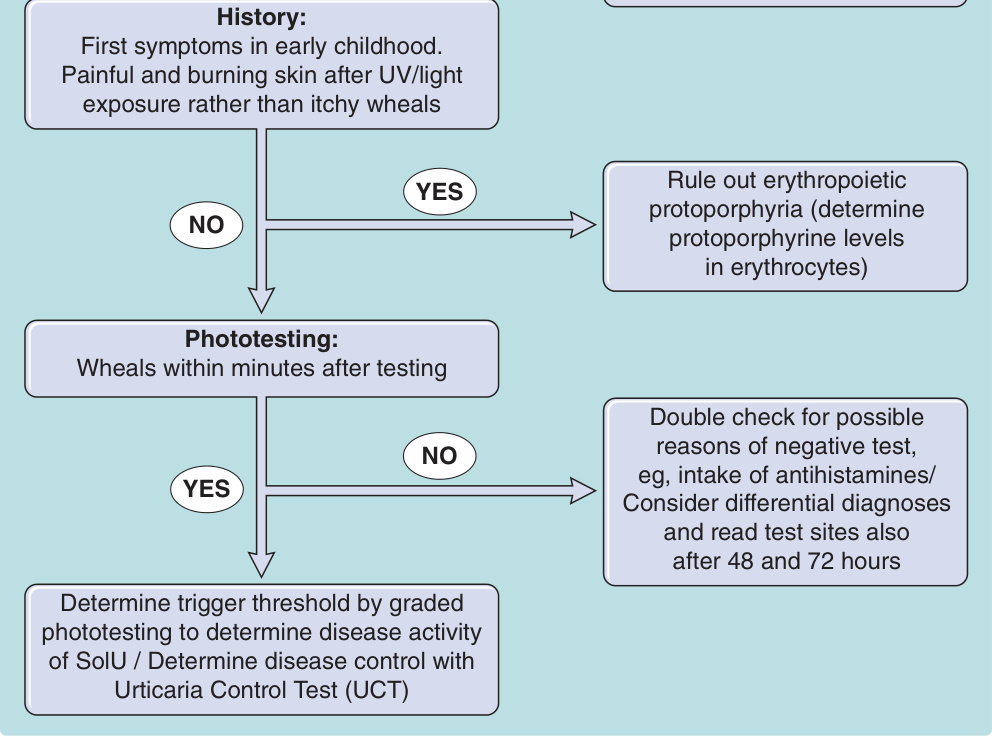
Figure 96-3 Diagnostic algorithm and diagnostic workup for solar urticaria.
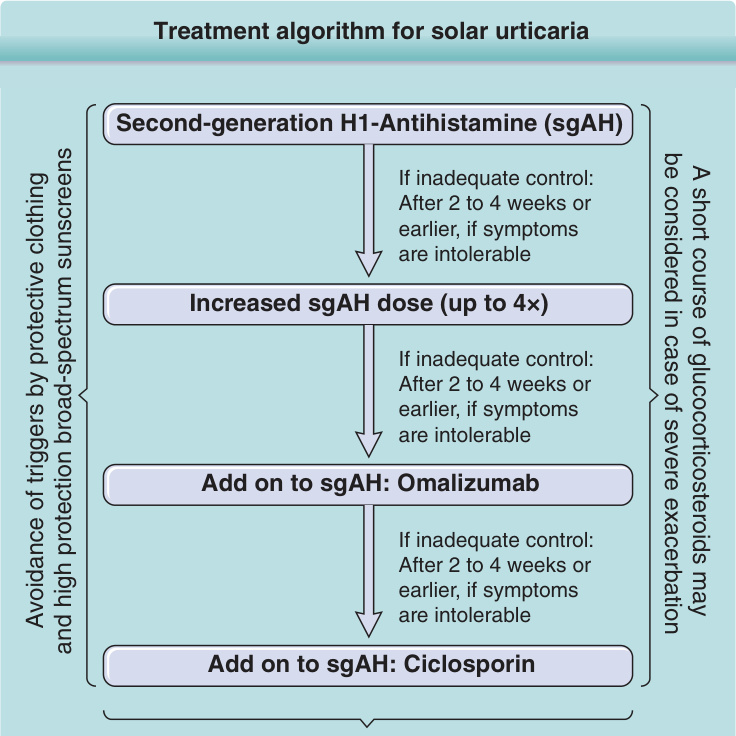
Figure 96-4 Treatment algorithm for solar urticarial.
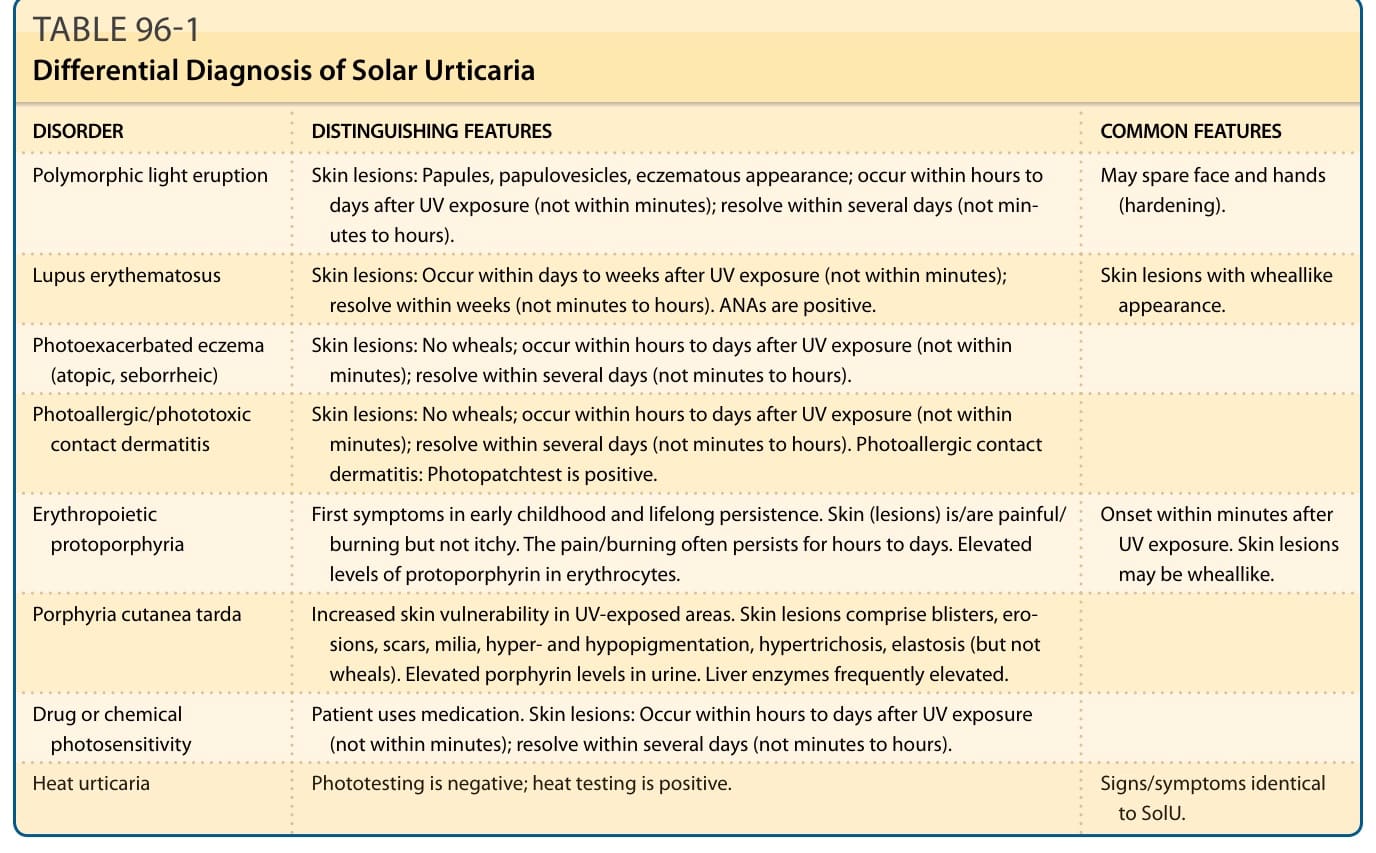
TABLE 96-1 Differential Diagnosis of Solar Urticaria