Actinic Dermatitis
17
Many diseases are caused by abnormal responses to ultraviolet radiation (UVR) and visible light exposure. This textbook includes separate chapters on other idiopathic (usually presumed immune-mediated) photodermatoses, including polymorphic light eruption/ polymorphous light eruption (PLE/PMLE), actinic prurigo, hydroa vacciniforme (HV), and solar urticaria, and photodermatoses as a manifestation of metabolic diseases such as the cutaneous porphyrias. This chapter discusses conditions with a dermatitis on exposed sites, whether or not covered sites are also affected. These conditions include chronic actinic dermatitis, photoallergic contact dermatitis, drug-induced photosensitivity, and manifest as a dermatitis (eg, caused by thiazides) and photoaggravation of other dermatitides (atopic eczema, seborrheic dermatitis, and, often when caused by an airborne allergen, allergic contact dermatitis). Frequently, clinical assessment alone is insufficient to distinguish between true abnormal cutaneous photosensitivity (as in chronic actinic dermatitis) and photoaggravation, not true photosensitivity, of another dermatitis, and investigation with some form of phototesting can be necessary for definitive diagnosis, with important implications for management.
CHRONIC ACTINIC DERMATITIS
AT-A-GLANCE
■ Chronic actinic dermatitis is a rare, acquired, persistent eczematous eruption of exposed skin, sometimes having pseudolymphomatous (reticuloid) features.
■ It commonly affects older men, but is increasingly recognized in women and in younger people, including children.
■ Histologic features are eczematous, but pseudolymphomatous forms may be virtually indistinguishable from cutaneous T-cell lymphoma.
■ It usually involves severe ultraviolet B sensitivity but often also involves ultraviolet A sensitivity and sometimes sensitivity to visible light.
■ Persistent light reaction, actinic reticuloid, photosensitive eczema, and photosensitivity dermatitis are all considered either clinical variants or old diagnostic terms.
■ It is likely the result of a delayed-type hypersensitivity reaction against an endogenous photoinduced epidermal antigen(s).
■ Therapy consists of strict avoidance of the relevant ultraviolet and visible rays, along with topical and intermittent oral steroids, and topical calcineurin inhibitors. Occasionally, phototherapy (ultraviolet B, broadband ultraviolet A, ultraviolet A1, or psoralen-ultraviolet A photochemotherapy) can be used, guided by the findings of investigation, particularly phototesting. If these measures are insufficient, or cause too much disruption to quality of life, then systemic immunosuppression (such as azathioprine or methotrexate) is required.
EPIDEMIOLOGY
EPIDEMIOLOGY
Chronic actinic dermatitis (CAD),1 formerly called the photosensitivity dermatitis/actinic reticuloid syndrome,2 occurs across the world.3-5 As it is frequently impossible to definitively diagnose CAD without some form of phototesting, it is likely that some persons with this condition are being labeled as having photoaggravated atopic eczema. CAD is possibly more common in people of darker-skin phototypes, but can be found in all peoples.4,6 Perhaps, melanin plays a part in causing this condition. CAD has not been reported in people with albinism.
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
Studies of the clinical, histologic, and immunohistochemical features of CAD all show it to resemble the delayed-type hypersensitivity reaction of allergic contact dermatitis,7,8 even in its severe pseudolymphomatous form (formerly called actinic reticuloid), in which the clinical and histologic features duplicate those seen in longstanding allergic contact dermatitis. It is highly probable that CAD is an allergic reaction. In addition to hypersensitivity to cutaneous photoantigens, patients with CAD often have concomitant allergic contact dermatitis to airborne and other ubiquitous allergens, including plant compounds, fragrances, and medicaments.8-18 Commonly implicated allergens include sesquiterpene lactones from plants of the Compositae family and sunscreens.16 The percentages with contact allergy as part of CAD vary according to the report; it seems likely that the relevant allergens will differ in different parts of the world and that the more locally relevant patch test agents are tested the higher will be the percentages with identified contact allergy.
17
Although photopatch testing is impossible in some persons with CAD (because the ultraviolet A photosensitivity can be too severe to allow irradiation of a photopatch test series), it can sometimes be done using an ultraviolet A minimal erythema dose assessment to determine a safe dose of ultraviolet A for this testing. This can be performed in those in whom it is helpful to determine whether or not there is photoallergy.4
When CAD occurs in the absence of an obvious contact allergen, the relevant novel antigen must be either directly radiation-induced or formed indirectly as a result of secondary oxidative metabolism. Important support for the latter possibility comes from the fact that albumin can become antigenic in vitro through photooxidation of its histidine moieties. There is no evidence for a genetic susceptibility to CAD; however, one stimulus for the acquisition of skin reactivity may be concurrent allergic contact dermatitis to recognized exogenous sensitizers or photosensitizers. These sensitizers are often airborne and may predispose by altering cutaneous immunity, and thus permit immunologic recognition of an endogenous photoantigen. Longstanding endogenous eczema, drug-induced photosensitivity, HIV infection,19 and possibly PLE/PMLE also may play similar roles. On the other hand, in addition or instead, chronic photodamage in frequently sun-exposed elderly outdoor enthusiasts may impair normal UVR-induced skin immunosuppression sufficiently for endogenous UVR-induced photoantigens to be recognized, as apparently also occurs for genetic reasons in PLE/ PMLE.20 There is much work left to be done to identify the immunologic mechanisms that account for CAD. Determining the action spectrum for CAD should theoretically help identify the postulated antigens, and the action spectra for CAD have been shown to resemble that of sunburn in many patients.21 However, the eruption in CAD is eczematous, and much lower doses of UVR are required to evoke CAD than to produce erythema. In any event, the ultraviolet chromophore for some patients may be the same as that of sunburn, namely DNA,21 with UVR-damaged DNA serving directly as an antigen in CAD. In other patients with CAD, however, the photoallergen must be different, because a few patients react only to ultraviolet A (UVA) radiation,22 and some patients react only to visible light.23
In summary, CAD appears to be an allergic contact dermatitis-like reaction against UVR-altered DNA or similar or associated molecules, perhaps as a result of enhanced immune reactivity resulting from concomitant airborne contact dermatitis, or other longstanding preexisting dermatitis, or a reduced immunosuppressive capacity in ultraviolet-exposed skin.
CLINICAL FEATURES
CLINICAL FEATURES
HISTORY
CAD may arise de novo in apparently normal skin or in the skin of patients with previous endogenous eczema (often atopic or seborrheic eczema),
1640
photoallergic or allergic contact dermatitis, or, rarely, PLE/PMLE. Concurrent allergic contact sensitivity to plant allergens, fragrances, or sunscreens is common. The condition classically affects middle-aged and elderly men; however, CAD is increasingly recognized in younger people, particularly in those with atopic eczema,24-27 although it is rarely present in children. The disorder is usually worse in summer in countries with marked seasonal variations, developing within minutes to hours after sunlight exposure and producing an itchy confluent erythematous eruption that occasionally remits over several days with scaling as long as exposure ceases and the reaction is mild. However, severely affected patients sometimes do not recognize that exacerbations are related to sunlight exposure, especially when affected all year round and when the wavelengths of sensitivity extend to longer UVA or visible wavelengths not associated with normal sunburn.
CUTANEOUS LESIONS
The lesions of CAD are eczematous, patchy or confluent, and acute, subacute, or chronic (Figs. 95-1 and 95-2). In severe cases, lichenification is common. Less commonly, scattered or widespread erythematous, shiny, infiltrated pseudolymphomatous papules or plaques are present on a background of erythematous, eczematous, or normal skin. Habitually exposed areas are most often affected, commonly with sharp cutoff at clothing lines. There is sparing of deep skin creases, upper eyelids, finger webs, and skin behind the earlobes. In severe disease, eczema of the palms and soles also may be found. Eyebrows, eyelashes, and scalp hair may be stubbly or altogether lost from constant rubbing and scratching. Erythroderma, usually accentuated on exposed sites, rarely supervenes. Variable,
A
B
sometimes geographic, sparing of exposed areas of the face or elsewhere, as well as irregular hyperpigmentation and hypopigmentation, sometimes vitiligo-like, may also occasionally be found.
LABORATORY TESTS
LABORATORY TESTS
HISTOLOGY
Histologic features include epidermal spongiosis and acanthosis, sometimes with hyperplasia. There is usually a predominantly perivascular lymphocytic cellular infiltrate confined to the upper dermis that in milder cases may resemble chronic eczema.28 CAD cannot be diagnosed on histopathology but a biopsy of the eruption, whether naturally occurring or provoked on phototesting, can be helpful in confirming an eczema and not another pattern of inflammation. Severe CAD, however, may mimic cutaneous T-cell lymphoma
17
C
D
(CTCL), on occasion being virtually indistinguishable. Features mimicking CTCL include epidermal Pautrierlike microabscesses and deep, dense epidermotropic mononuclear cell infiltration, sometimes with atypia. Typically, there is no marked increase in mitoses. T-cell receptor gene rearrangement studies are normally done if there is suspicion of CTCL. However, T-cell receptor clonality also may be observed in benign dermatoses, so even identification of a clone does not completely rule out CAD, rather than lymphoma, as the diagnosis.
BLOOD TESTS
Assessment of lupus autoantibodies is usually done to exclude the unlikely possibility of cutaneous lupus erythematosus. In severe or erythrodermic CAD, there may be large numbers of circulating CD8+ Sézary cells without other suggestions of malignancy.29 HIV status should be assessed if there is suspicion that this may be a predisposing or associated factor. Serum
1641
17
immunoglobulin E may be elevated (even among those whose CAD has not supervened upon atopic eczema), with higher levels of immunoglobulin E correlating with more-severe disease.
PHOTOTESTING
Phototesting is essential to make the diagnosis of CAD. Almost invariably one finds low erythemal thresholds and eczematous or pseudolymphomatous responses after irradiation with ultraviolet B (UVB), usually with UVA, and frequently also with visible wavelengths (accounting for presentations such as described after a tungsten light was used when ear cleaning).30 A small number of patients genuinely seem to react only to UVA (although the possibility of another diagnosis such as drug reaction must be revisited if only UVA sensitivity is found), and fewer still only to visible light, in which case, drug photosensitivity must also be considered. Testing should be done on uninvolved skin of the back with no topical or systemic steroid therapy for at least the preceding few days to avoid false-negative results.31,32 Various sources can be used for phototesting, including the irradiation monochromator, which allows the delivery of different doses of different ultraviolet and visible wavebands (which can be fairly narrow but which are not truly monochromatic).33-36 If an irradiation monochromator is not available, then a series of different sources with filters can be used to sample through at least UVB and UVA (for which phototherapy treatment sources can be used) and visible light (such as using a slide projector). When such fairly elaborate equipment is not available, sunlight can be used (at least in warmer parts of the world) with a template devised to allow small areas of skin to have different durations of exposure and using a piece of window glass to filter out UVB, which enables testing with whole-spectrum sunlight and sunlight minus UVB. The output from the sun can be very variable, but the severity of abnormal photosensitivity in CAD is usually severe, so as long as a control population has been tested to establish what is normal, then such relatively crude testing is useful. Monochromatic and broad-spectrum sources both induce abnormal responses, with monochromatic sources determining the action spectrum for disease induction and broad-spectrum sources tending to demonstrate acute eczema.
PATCH AND PHOTOPATCH TESTING
Patch testing and photopatch testing (when possible; sometimes the sensitivity to UVA on its own precludes irradiating with even a tiny dose of UVA for photopatch testing) are also important in suspected CAD, because contact sensitivity, including to airborne allergens such as Compositae oleoresins (including, where it occurs, parthenium),16,37-39 colophony,40,41 and methylisothiazolinone (the airborne dermatitis of which can be photoaggravated),42,43 alone may resemble CAD or even coexist with CAD. In addition, occasional
1642
■Photoexacerbated atopic or seborrheic eczema
■Photoexacerbated atopic or seborrheic eczema
■Drug or chemical photosensitivity
■Drug or chemical photosensitivity
■Cutaneous T-cell lymphoma
■Cutaneous T-cell lymphoma
■Eczematized actinic prurigo
■Eczematized actinic prurigo
■Photoallergic contact dermatitis
■Photoallergic contact dermatitis
■Photoaggravated airborne contact allergic dermatitis
■Photoaggravated airborne contact allergic dermatitis
Note: The other conditions described in the text as capable of causing an exposed-site dermatosis do not cause a dermatitis unless the dermatitis is superimposed, such as someone who has PLE/PMLE but develops superimposed dermatitis changes perhaps because of having atopic eczema.
secondary contact or photocontact sensitivity to sunscreens or other topical therapies may complicate the clinical picture.44
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
COMPLICATIONS
COMPLICATIONS
A relationship to CTCL was considered a possibility.45
However, when this was studied at a population level (and misclassifications in diagnostic databases were corrected) it was found that CTCL and CAD did not coexist more than would be expected by chance.46
Results of T-cell receptor, immunoglobulin gene rearrangement, and other studies are usually negative in CAD.47 In addition, CAD gradually resolves in many patients, there is no higher incidence of malignancies, and life expectancies are thought to be normal.48
However, CTCL itself may present very rarely with severe CAD-like photosensitivity, and careful investigation to exclude CTCL is necessary when the disease suspected.49-51
PROGNOSIS AND CLINICAL COURSE
PROGNOSIS AND
CLINICAL COURSE
Once established, CAD usually persists for years before resolving gradually (Dawe et al).48 Particularly severe phototest sensitivity and a number of completely separate contact allergens seem to be predictors of a poorer prognosis for resolution. In that study, young age and female sex were also associated with a poorer prognosis for resolution but when that study was done, CAD was considered to be a disease of old men so was likely more often not diagnosed in younger people and in women (and only diagnosed in the more severely affected young people and women).48
TREATMENT
TREATMENT
Treatment of CAD is often difficult and not fully effective. Rigorous avoidance of UVR and exacerbating contact allergens is essential, along with regular application of high-protection-factor broad-spectrum topical sunscreens of low irritancy and allergenic potential. Ideally, sunscreen photoprotection should be guided by knowledge of the wavelengths (UVB, UVB and UVA, or UVB, UVA, and visible) implicated in each individual. Strong topical corticosteroids, such as clobetasol propionate 0.05%, are also often needed and frequently produce marked symptomatic relief without adverse effects, even after long-term use, if confined to affected skin. Occasional oral steroid use is often helpful for disease flares. In more-resistant disease, the topical calcineurin inhibitors—tacrolimus and pimecrolimus—sometimes produce good results if tolerated.52-58 For refractory CAD, however, oral immunosuppressive therapy is often necessary and generally helpful if tolerated. Azathioprine 1.5 to 2.5 mg/kg/day can produce remission in months,59-65
after which it may be reduced in dosage, or perhaps discontinued in the winter. While less studied for this indication, methotrexate is also used, especially when CAD has arisen on a background of atopic eczema. Cyclosporine 3.5 to 5 mg/kg/day can be rapidly effective,66,67 but is more likely to produce adverse effects, and so is generally not a good long-term treatment. Mycophenolate mofetil is less often used.68,69
More localized skin immunosuppression by psoralen activated by UVA treatment also can be effective,70,71
and is often initially accompanied by oral and topical corticosteroid therapy to reduce disease flares.71
PREVENTION
PREVENTION
The risk of CAD can possibly be reduced by moderating outdoor pursuits, especially those associated with plant allergen exposure, such as gardening, even more so for individuals who already have a tendency to develop eczematous eruptions in exposed areas. In those persons who are already developing CAD, avoidance of UVR is critical, and patients should be aware that indoor lighting with fluorescent lamps, including compact fluorescent energy-saving lamps, is also a source of UVA and UVB. 72,73
PHOTOEXACERBATED DERMATITIS
Several dermatoses that are not caused by UVR may be worsened by it (Table 95-2). Mechanisms of this phenomenon, termed photoexacerbation, have rarely been studied. The initial condition may be severely worsened even if it was originally only mild or subclinical. These disorders are relatively common. Such conditions, especially the eczemas, psoriasis, and acne,
17
■Acne
■Acne
■Atopic eczema
■Atopic eczema
■Carcinoid syndrome
■Carcinoid syndrome
■Cutaneous T-cell lymphoma
■Cutaneous T-cell lymphoma
■Dermatomyositis
■Dermatomyositis
■Disseminated superficial actinic porokeratosis
■Disseminated superficial actinic porokeratosis
■Erythema multiforme
■Erythema multiforme
■Familial benign chronic pemphigus (Hailey-Hailey disease)
■Familial benign chronic pemphigus (Hailey-Hailey disease)
■Keratosis follicularis (Darier disease)
■Keratosis follicularis (Darier disease)
■Lichen planus
■Lichen planus
■Lupus erythematosus
■Lupus erythematosus
■Pellagra
■Pellagra
■Pemphigus foliaceus (erythematosus)
■Pemphigus foliaceus (erythematosus)
■Pityriasis rubra pilaris
■Pityriasis rubra pilaris
■Psoriasis
■Psoriasis
■Reticulate erythematous mucinosis syndrome
■Reticulate erythematous mucinosis syndrome
■Rosacea
■Rosacea
■Seborrheic eczema
■Seborrheic eczema
■Transient acantholytic dermatosis (Grover disease)
■Transient acantholytic dermatosis (Grover disease)
■Viral infections
■Viral infections
improve with sunlight exposure in most patients, perhaps because cutaneous reactivity is reduced, but in a small proportion of individuals, it is instead aggravated. If photoexacerbation does occur, the new eruption generally develops or worsens initially at sites typical of the basic disorder (Fig. 95-3), followed at times by extension to other areas. In photoexacerbated seborrheic eczema, however, an unpleasant sensation at the exposed sites may be the first or only feature.
1643
17
Treatment consists of minimizing sunlight exposure, protection with suitable clothing, application of highprotection-factor broad-spectrum sunscreens, and careful treatment of the underlying disorder. Taking these steps alone often improves the problem. If these actions are inadequate, phototherapy often helps, for example, in seborrheic or atopic eczema and psoriasis. Often a particular value in distinguishing between photoaggravation and true photosensitivity in these conditions is to decide whether or not phototherapy can be used. Phototherapy is contraindicated in cutaneous lupus erythematosus or dermatomyositis becauseaggravation of the systemic disease is a risk. Photoexacerbated acne commonly requires treatment with oral isotretinoin.
APPROACH TO THE PATIENT WITH A DERMATOSIS ON PHOTOEXPOSED SITES
CLINICAL FEATURES
CLINICAL FEATURES
Patients with abnormal photosensitivity present in 3 ways: (a) sporadic or (b) persistent eruptions in sunlight-exposed areas (Fig. 95-4), or, infrequently, (c) erythroderma. When sporadic, the patient usually considers sunlight exposure to be responsible; when persistent, the physician often must identify the association. Careful history taking is essential, first to confirm that sunlight exposure is responsible and then to make a diagnosis. Information of considerable importance are age at disease onset, gender, family history, previous sunlight sensitivity, occupation, leisure pursuits, and systemic and topical drug (or chemical) use. Additional relevant details include distribution of lesions; effects of season; exposure times required for induction; time between exposure and the appearance of lesions; duration of the eruption after exposure ceases; effects of sunlight received through window glass (implicating UVA and visible light); presence of systemic symptoms; and patientassessed morphologies (progression of the disease before the clinic visit). In terms of age and sex, young women are more likely to develop PLE/PMLE; women or girls more commonly develop actinic prurigo; children of either gender may have HV, xeroderma pigmentosum, or erythropoietic protoporphyria; elderly men or younger individuals with a history of eczema most often develop CAD. A family history of sunlight sensitivity may be present in patients with PMLE/PLE, actinic prurigo, xeroderma pigmentosum, and the porphyrias. CAD is common in outdoor enthusiasts exposed to both sunlight and airborne allergens (it is important to also consider it in patients from other demographics), although exacerbations of disease, despite sunscreen
1644
use, invoke the possibility of sunscreen allergy. An eruption appearing in minutes and remitting within 2 hours suggests solar urticaria or, occasionally, photosensitivity to drugs, such as amiodarone. Onset within 20 minutes to several hours, with resolution over days suggests PLE/PMLE, HV, erythropoietic protoporphyria, cutaneous lupus erythematosus, or other photoexacerbated dermatoses, or other drug photosensitivities, such as to thiazides. Systemic malaise is uncommon, but well recognized, in PMLE/ PLE, HV, and solar urticaria. Development of lesions after exposure through window glass suggests an inducing spectrum that includes UVA and/or visible light. The eruption described by patients with PMLE/ PLE is generally that of small or large, elevated, pruritic, red or skin-colored, and often clumped spots of papules, sometimes confluent, that usually involve several, but not all exposed sites. In HV, blistering with scar formation occurs, and in solar urticaria, elevated pruritic wheals are often confluent. In erythropoietic protoporphyria and amiodarone drug photosensitivity, a marked burning sensation, without visible change, has been reported. In erythropoietic protoporphyria, relatively lengthy exposure may lead to firm, colorless or pink, diffuse swelling. In most drug photosensitivity reactions and in xeroderma pigmentosum, an exaggerated sunburn-like reaction is possible, which in many forms of xeroderma pigmentosum is maximal at 2 to 3 days. Finally, in photoexacerbated dermatoses, the eruption resembles that of the primary disorder. Photosensitivity eruptions are usually present on some, and occasionally all, of the forehead; nose; upper cheeks; tip of the chin; rims of the pinnae; back and sides of the neck; upper chest; backs of the hands and feet; and extensor aspects of the limbs. Covered areas also may be involved, but to a lesser extent. On the other hand, portions of the face protected by hair or customarily in shadow, such as upper eyelids, finger webs, skin creases, and skin under the nose, lower lip, chin, and backs of earlobes, are frequently unaffected, except when there is associated airborne contact dermatitis. Excoriated papules suggest actinic prurigo, whereas eczematous lesions or, very rarely, light-associated erythrodermas suggest CAD, photoexacerbated atopic, or seborrheic eczema. Finally, skin fragility, bulla formation, and atrophic superficial scarring suggest hepatic porphyria or pseudoporphyria, especially if there has been drug or excessive alcohol intake. Clinical appraisal along with the history usually results in a diagnosis, although for complete certainty, several of the studies listed below may be appropriate.
LABORATORY STUDIES
LABORATORY STUDIES
If the diagnosis is not certain, appropriate additional studies include an assessment of the antinuclear antibody and extractable nuclear antibody panel. If
17
Distribution of exposure in photodermatitis
Spared area: Triangle behind ear
Spared area: Neck creases Spared area: Upper eyelid
Spared area: Under chin
Spared area: Above upper lip
Male
Spared area: Triangle behind ear
Spared area: Upper eyelid
Spared area: Under chin
Spared area: Above upper lip
Female
Spared area: Under watch strap and palms
Spared area: Neck creases
Spared area: Under watch strap and palms
KEY
Rarely or never exposed
Often exposed Habitually exposed
present at significant titers, cutaneous lupus erythematosus should be considered. In addition, examination of blood, urine, and stools for porphyrins should be considered.
Biopsies may be helpful. Lesional histologic features are characteristic in several photodermatoses, especially PMLE, HV, and CAD. However, with the exception of HV, histopathologic changes in
1645
17
DISEASE
ACTION SPECTRUM FREQUENCY OF ABNORMAL FINDINGS
Polymorphic light eruption UVA more often than UVB Only sometimes
Actinic prurigo UVA more often than UVB Only sometimes
Hydroa vacciniforme More often UVA Only sometimes
Chronic actinic dermatitis UVB ± UVA ± visible light Virtually always
Solar urticaria UVB, UVA, or visible, or combination Usual
Xeroderma pigmentosum UVB Usual
Photoexacerbated dermatoses UVB, UVA, or combination Rare
Photoexacerbated
UVB, UVA, or
Rare
dermatoses
combination
UVA, ultraviolet A radiation; UVB, ultraviolet B radiation.
photodermatoses are rarely entirely diagnostic. These are reviewed in the preceding disease descriptions. Phototesting of normal back skin with a monochromator in CAD and solar urticaria often produces the papules or wheals of the condition itself, frequently at low irradiation doses, and this also may identify the action spectrum. Phototesting also helps to confirm xeroderma pigmentosum through the delayed development of erythema over 2 to 3 days, with an abnormally low-dose threshold, often eventuating in blister formation (Table 95-3). In eczematous photosensitivity, patch and photopatch testing are also essential to identify relevant allergens. Finally, special techniques, such as the assessment of DNA excision repair or of RNA synthesis recovery rate in cultured fibroblasts after UVR exposure, are essential for the diagnoses of certain genophotodermatoses.
PHOTOTESTING
Techniques of phototesting vary greatly from country to country and from center to center. Although it is the investigational technique of choice for photodermatoses when the diagnosis is uncertain or when details of the inducting action spectrum are required, phototesting remains unavailable in many clinical centers. The cost of the equipment and its infrequent use in most clinical practices means that patients should be referred for consultation to such centers whenever indicated. Phototesting falls into 2 categories: (a) monochromator phototesting (testing to wavebands, it is not strictly monochromatic, produced by an irradiation monochromator),35 usually of the upper back with selected wavebands and selected doses to identify the action spectrum for the disorder and to provoke
1646
the eruption (frequently responses at 24 hours and later after irradiating small circles of back skin with a monochromator look eczematous in CAD), and (b) photoprovocation with a broad-spectrum source to induce the eruption for its clinical appearance and subsequent biopsy if indicated. Table 95-3 lists the disorders for which monochromatic testing may be helpful. For precise characterization of the wavelength dependency of a disorder, monochromator testing, preferably with a xenon arc irradiation monochromator, should be employed. For photoprovocation, the favored device is often a solar simulator, usually a xenon arc-filtered source that produces a spectrum that resembles the terrestrial sunlight spectrum at noon at sea level on a cloudless midsummer’s day in temperate regions of the world. Keep in mind that the terrestrial spectrum at noon in June varies considerably between Iceland and Kenya, as it also does between high elevations and sea level. So, a solar simulator is only ever a simulator of a certain “type” of sunlight. Several suitable protocols also have been described for using simple broad-spectrum metal halide or fluorescent light sources with filters if necessary. In some parts of the world, sunlight with filters also has been used, although this method is generally too unpredictable for clinical use. The mainstay of phototesting is a monochromator. It is composed of a high-pressure xenon arc source that emits radiation along a pathway incorporating a diffraction grating angled to produce the required waveband at the exit slit. Such equipment needs regular calibration of output and wavelength. Because even large centers cannot always afford such equipment, lesser alternatives have been created, such as metal halide or fluorescent light sources of sufficient output intensity. With such sources, the UVB, UVA, and visible light components of patient photosensitivity can be studied, based on deviation from normal erythemal reactions throughout the UVR spectrum. Monochromator phototesting is preferably performed on unaffected skin of the upper back, lateral to the paravertebral groove whereas lesion induction, except when done relatively easily with the monochromator, as in solar urticaria and CAD, is best undertaken using broadband sources with output directed over larger areas of skin known to be susceptible to the eruption. PLE/PMLE, actinic prurigo, and HV are conditions in which repeated irradiation with UVAemitting or UVB-emitting or combined sources is often required to reproduce the disease. It is important that the use of potent topical and systemic steroids be avoided when possible for at least several days before phototesting to prevent falsenegative results.31,32 It is not certain how much the other oral immunosuppressive agents affect testing (and in CAD severe abnormal sensitivity can still be seen in those on azathioprine, methotrexate, or ciclosporin), but they should be stopped whenever possible as well. False-positive results may also occur in patients with widespread disease (with the possibility of photoaggravation of an underlying process being
mistaken for true photosensitivity), and the eruption should first be well-controlled whenever possible, if necessary by keeping the patient in a reduced-light environment. However, it is often difficult to fulfill these requirements if the eruption is active, and in such circumstances, testing may need to be undertaken with knowledge of its limitations. All phototesting should be undertaken at carefully standardized sequential doses (often a geometric series) and wavelengths, and the results read at consistent times after exposure in carefully controlled conditions of light and temperature. Furthermore, because testing involves UVR exposure, potentially harmful to both skin and eyes, the patient and the investigator should be protected with appropriate clothing, shielding and goggles.
PHOTOPATCH TESTING
Chapter 97 discusses photopatch testing in greater detail. Photopatch testing is an established investigational tool designed to identify photoallergic contact dermatitis, although it also can be employed to help identify phototoxic agents. It is essentially a more complex version of patch testing, and it is used in patients with exposed-site eczema, whether or not they also have another photodermatosis, to determine whether photoallergy is also present. The methodology of photopatch testing has received less attention than allergen testing or phototesting, as it resides between the 2 specialty areas of photodermatology and contact dermatology. However, consensus methodology is now available.74-78
Using this approach, test materials (usually sunscreens, topical nonsteroidal, and antiinflammatory agents in Europe and North America—it is important to consider what might be locally relevant, eg, some antiseptics still used in soap in parts of the world— and other possible causative agents) are applied in duplicate for 24 to 48 hours to normal skin. One set of test sites is then uncovered and irradiated with a broad-spectrum UVA source, usually at 5 J/cm2 from fluorescent UVA lamps (as used for psoralen activated by UVA), and the results read 24 and 48 hours later. Ideally, at the time of application of the patch tests (if 24 hours before planned irradiation), irradiations to determine the minimal erythemal dose with the planned UVA source should be conducted, especially if severe photosensitivity such as in CAD is possible. Sometimes if the minimal erythemal dose is extremely low the results preclude irradiation with any UVA, but sometimes they allow photopatch testing to proceed using a dose lower than the standard 5 J/cm2. Strongly positive reactions at sites exposed to both chemical agent and UVA, with no reactions at the covered control sites, confirms a diagnosis of photoallergy. Occasionally, however, contact irritation or contact allergy occurs in both sites, making a diagnosis of photoallergy uncertain. One should also be alert to the possibility that all irradiated sites may become positive (especially if the patient is photosensitive and a UVA minimal erythemal dose was not done), suggesting
17
that underlying widespread UVA photosensitivity is responsible. Furthermore, the identification of potential photoallergens is still primitive, often with separation of phototoxicity from photoallergy uncertain. Once again, testing for photoallergy is best conducted in regional centers or by physicians with appropriate experience.
ACKNOWLEDGMENTS
The author is grateful to the previous authors for the earlier versions of this chapter, Travis W. Vandergriff, Paul R. Bergstresser, John L. M. Hawk, and James Ferguson. I have not made changes for “changes sake,” but I have added to or changed the text where new knowledge is available, where extra information might be useful, and to make this chapter as useful as possible in all parts of the world.

Figure 95-1 Chronic actinic dermatitis: infiltrated eczematous eruption on the face.
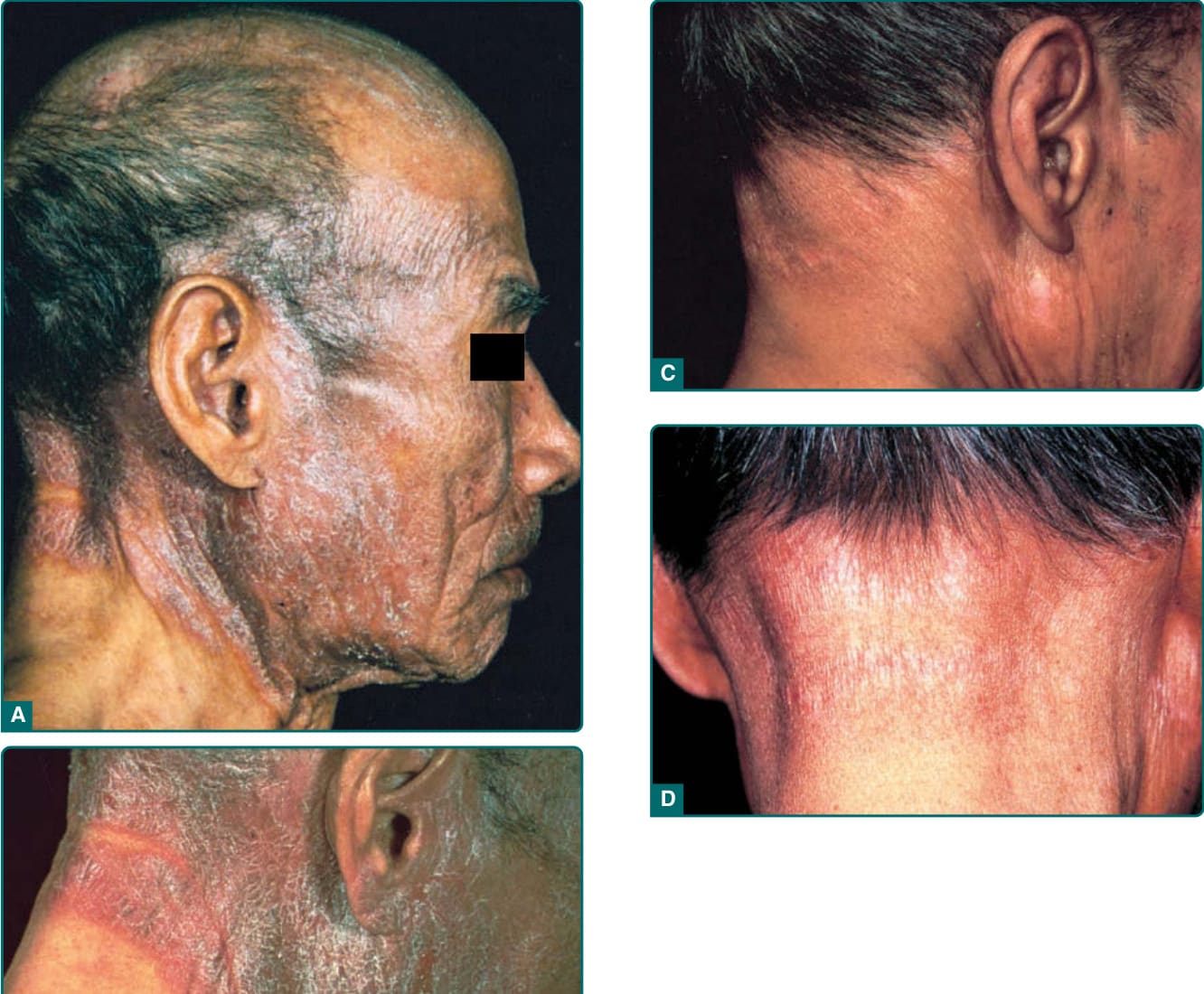
Figure 95-2 Chronic actinic dermatitis: A and B, Severe ultraviolet and light-induced eczema of the face and neck. C and D, Patient in full remission after low-dose psoralen plus ultraviolet A irradiation over weeks, with initial highdose oral steroid cover to prevent initial exacerbation.

Figure 95-3 Photoexacerbated seborrheic dermatitis, affecting the face only at sites of predilection for the seborrheic eruption.
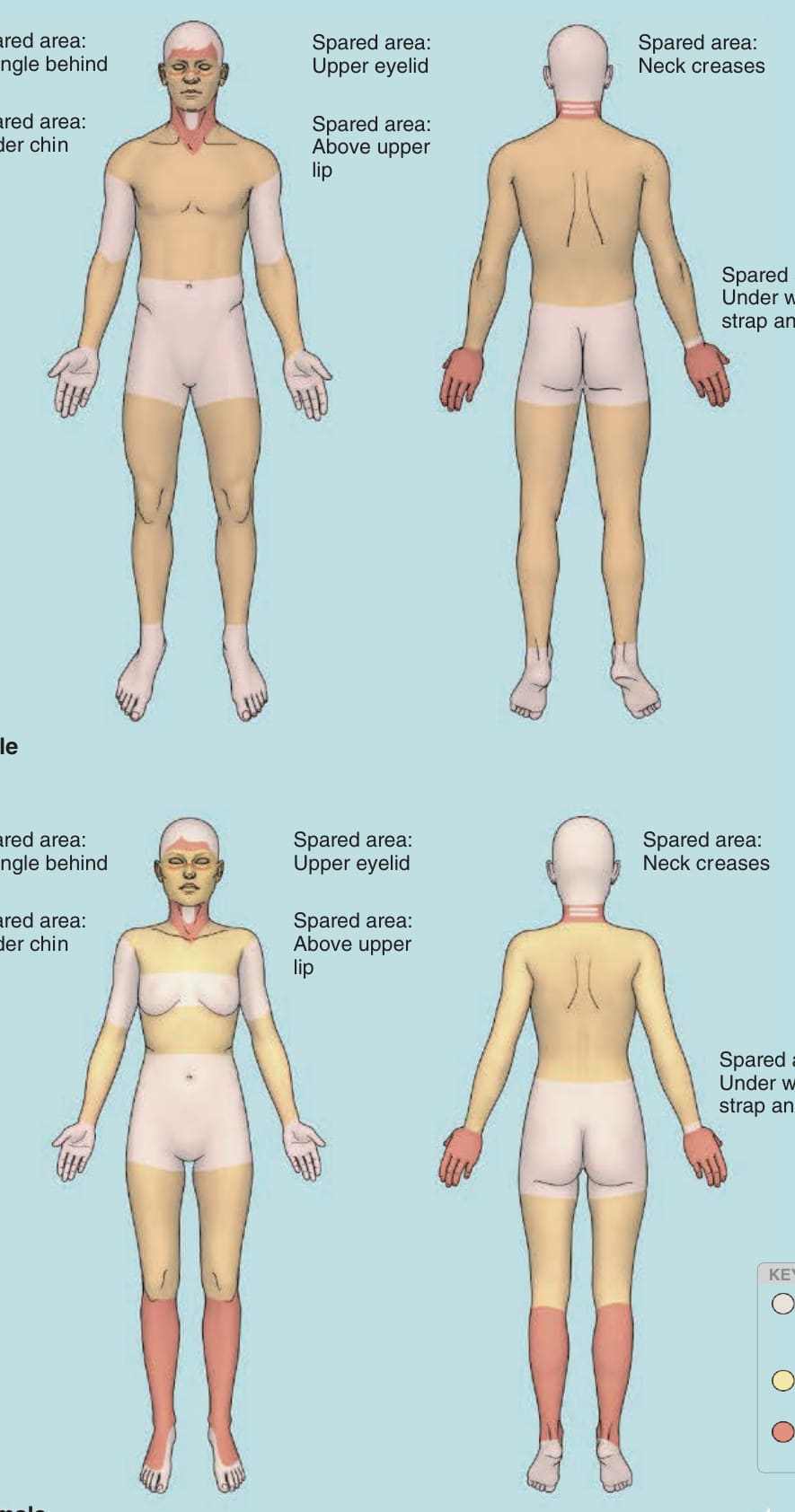
Figure 95-4 Distribution of exposure in photodermatitis. (From Wolff K, Johnson RA, Saavedra AP, et al. Fitzpatrick’s Color Atlas and Synopsis of Clinical Dermatology, 8th ed. New York, NY: McGraw-Hill; 2017, with permission.)
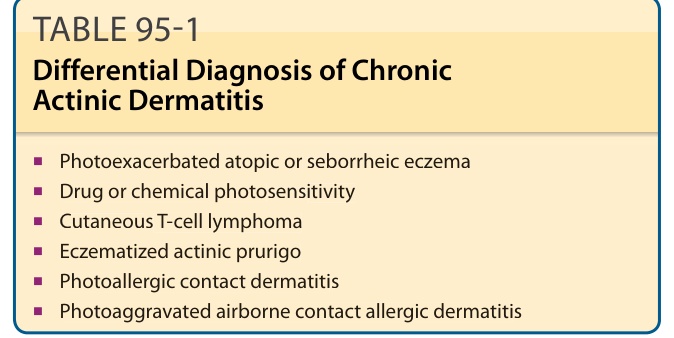
TABLE 95-1 Differential Diagnosis of Chronic Actinic Dermatitis
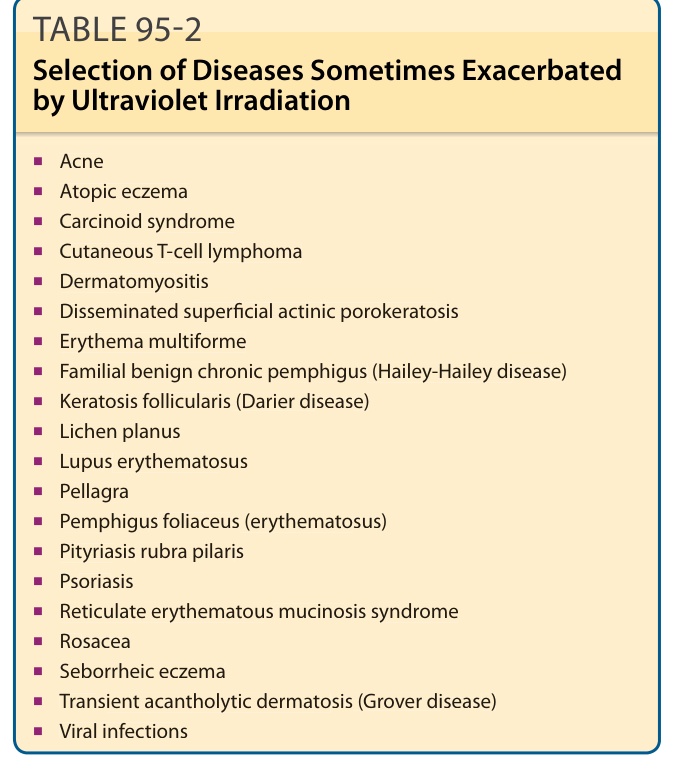
TABLE 95-2 Selection of Diseases Sometimes Exacerbated by Ultraviolet Irradiation
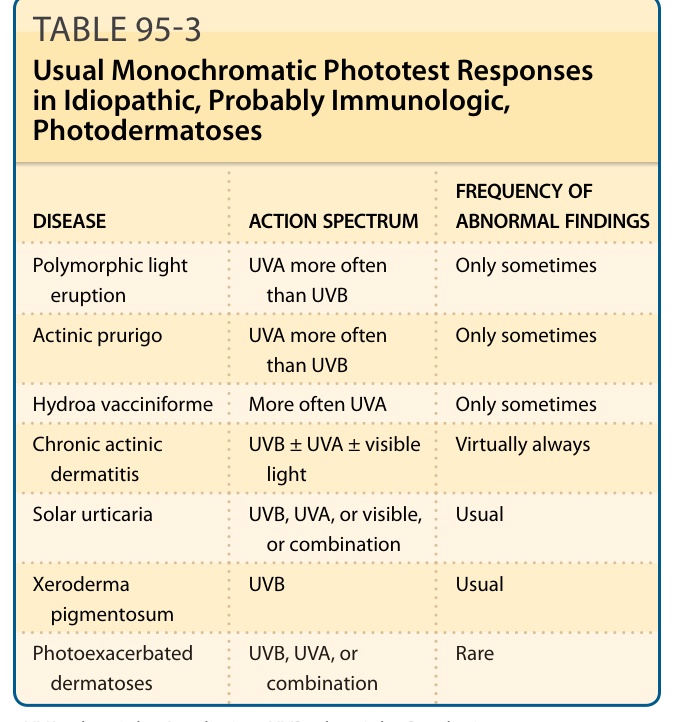
TABLE 95-3 Usual Monochromatic Phototest Responses in Idiopathic, Probably Immunologic, Photodermatoses