Hydroa Vacciniforme
17
AT-A-GLANCE
■ A rare, chronic, scarring photodermatosis sometimes associated with Epstein-Barr virus infection.
■ Characterized by recurrent sunlight-induced crops of papulovesicles and vesicles, most commonly on the face and dorsa of the hands.
■ Onset commonly in childhood, remitting most often at puberty.
■ May be a scarring variant of polymorphic light eruption.
■ Focal intraepidermal vesiculation, reticular degeneration of the epidermis, epidermal and upper dermal necrosis, and sometimes ulceration are typical histologic changes.
■ Avoidance of ultraviolet radiation including the use of broad-spectrum sunscreens is the only established therapy, but there may be a role for antivirals.
■ A severe, often fatal lymphoma resembling hydroa vacciniforme is distinguished by fever, facial edema, and systemic symptoms.
DEFINITION
Hydroa vacciniforme (HV) is a rare, chronic photodermatosis with onset typically occurring in childhood and a tendency to remission in adolescence. HV is characterized by photoinduced papules and vesicles that invariably scar after healing.
HISTORICAL PERSPECTIVE
HV was first described in 1862 by Bazin.
EPIDEMIOLOGY
HV is reported most often in North America, Europe, and Japan but is known to occur globally. The disease has its onset in childhood, most often presenting before age 8 years; presentation in adulthood is unusual. Patients with light pigmentation are affected preferentially. The disease is rare, with one estimate of the prevalence of HV being 0.34 cases per 100,000 individuals with an approximately equal sex ratio.1 There is male predominance for severe forms, whereas milder disease is more common in females.1,2 Cases of HV are normally sporadic, and familial incidence is exceptional.
CLINICAL FEATURES
HISTORY
HISTORY
HV commonly develops in early childhood and resolves spontaneously by puberty, although, in some patients, it is lifelong. HV eruptions typically occur in summer,3 often with an intense burning or stinging sensation followed by the appearance of individual or confluent papules and then vesicles, all within hours of sunlight exposure (Fig. 94-1). This is followed by umbilication, crusting, and progression to permanent pock scarring within weeks.
CUTANEOUS FINDINGS
CUTANEOUS FINDINGS
HV is characterized initially by erythema, sometimes with swelling, followed by the eruption of tender papules and vesicles within 24 hours of sun exposure. The eruption affects the cheeks and to a lesser extent other areas of the face, as well as the backs of the hands and dorsal aspects of the arms. The distribution tends to be symmetrical. Vesicles may occasionally become confluent and hemorrhagic. Later, papules and vesicles umbilicate and develop ulceration. Within weeks to months, lesions heal leaving permanent, depressed, hypopigmented scars. These scars are invariably present and resemble those seen in vaccinia (“pock marks”), hence the “vacciniforme” nomenclature.
NONCUTANEOUS FINDINGS
NONCUTANEOUS FINDINGS
Oral ulcers and eye involvement also occur in HV.4-6
Ophthalmologic complications include conjunctival hyperemia, corneal erosions or ulcerations, iritis, keratitis, and uveitis.6-8 Oral involvement presents as ulceration resembling aphthae or as gingivitis.6,9
COMPLICATIONS
COMPLICATIONS
Scars invariably ensue eruptions of HV. A quality-oflife study indicates that HV causes embarrassment and self-consciousness among children with the disease.10
The negative impact of HV on quality of life exceeds previously reported indices for atopic dermatitis and psoriasis.10
Patients with severe presentations of HV-like eruptions along with systemic symptoms may develop a lymphoproliferative disorder with sometimes fatal systemic lymphoma. This entity (HV-like lymphoma) is later addressed in the section “Differential Diagnosis”.
ETIOLOGY AND PATHOGENESIS
The exact pathogenesis of HV is not known. No chromophores have been identified, and although ultraviolet B minimal erythema dose responses are normal in most patients, some have increased ultraviolet A sensitivity.2 Nevertheless, its clear relationship to sunlight exposure, its distribution, and its early clinical appearances are all similar to that of polymorphous light eruption (PMLE), which suggests a relationship with that disease. On the other hand, fully developed HV eruptions are more severe than those found in PMLE, are associated with permanent scarring, and are unresponsive to treatments ordinarily effective in PMLE, apart perhaps from sunscreens and, occasionally, prophylactic phototherapy. It is now widely recognized that chronic infection by Epstein-Barr virus (EBV) plays a role in the pathogenesis of HV in many cases,11-13 although a relationship between EBV and HV in all populations has not been established. EBV nucleic acids are found in the cutaneous lesions of HV in 85% to 95% of patients, but not in lesional skin of control patients.12,14 By electron microscopy, virions can be detected within lymphocytes as well as keratinocytes.13 EBV DNA is found consistently in the peripheral blood of patients with HV, and higher levels correlate with disease activity and severity.13,15 Patients with HV are also found to have higher percentages of circulating γδ T-cells, with demonstrable EBV infection of those cells.15
17
DIAGNOSIS
SUPPORTIVE STUDIES
SUPPORTIVE STUDIES
LABORATORY TESTING
Blood, urine, and stool porphyrin concentrations should be assessed to exclude cutaneous porphyria, and an antinuclear antibody and extractable nuclear antibody to exclude the small possibility of cutaneous lupus erythematosus. Evidence of EBV viremia may support the diagnosis or indicate disease activity.
PHOTOTESTING
Phototesting may show increased sensitivity to shortwavelength ultraviolet A in some patients.2,16,17 However, phototesting usually does not discriminate HV from other photodermatoses. Simulated solar irradiation may also induce erythema at reduced doses or occasionally provoke the typical vesiculation of HV (Fig. 94-2).
PATHOLOGY
Early histologic changes include intraepidermal vesicle formation with spongiosis and subsequent focal epidermal keratinocyte necrosis. There is a dermal perivascular neutrophil and lymphocyte infiltrate. The lymphocytes are predominantly T cells, and approximately 5% to 20% of infiltrating lymphocytes may show evidence of EBV integration on in situ hybridization.15
Older lesions show necrosis, ulceration, and scarring. Vasculitic features have been reported.2 In some cases, there also may be a septal or lobular panniculitis. Healed pock-like lesions show dermal fibrosis in the pattern of a scar.
1635
17
OTHER TESTS
Viral studies for herpes infection or other viral disorders should be undertaken if photoexacerbation or photoinduction of these other disorders seems at all possible.
DIAGNOSTIC ALGORITHM
DIAGNOSTIC ALGORITHM
DIFFERENTIAL DIAGNOSIS
■Photoexacerbated viral dermatoses such as herpes simplex
■Photoexacerbated viral dermatoses such as herpes simplex
■Erythropoietic protoporphyria
■Erythropoietic protoporphyria
■Polymorphic light eruption
■Polymorphic light eruption
■Actinic prurigo
■Actinic prurigo
■Subacute cutaneous lupus
■Subacute cutaneous lupus
■Xeroderma pigmentosum
■Xeroderma pigmentosum
■Hydroa vacciniforme-like lymphoma
■Hydroa vacciniforme-like lymphoma
as hydroa vacciniforme–like lymphoma (HVLL).18
The nomenclature of this entity is somewhat controversial, as some reports in the literature describe a “severe HV-like eruption” occurring in patients with chronic EBV infection and other associated disorders, such as hypersensitivity to mosquito bites and the
Differentiating abnormal responses to ultraviolet radiation
Are lesions present despite rigorous avoidance of sunlight? OR Are lesions present in photoprotected sites?
NO
Consider patient’s age
Young adult
Consider photoexacerbated primary dermatosis
YES
Child Elderly
Are pock scars present?
NO
YES
Do excoriations, swallow scars, or dyspigmentation predominate?
Hydroa vacciniforme
Does the patient have a history of atopic or contact dermatitis? OR Does the patient pursue outdoor hobbies?
NO YES NO YES
Actinic prurigo
Phototoxic or photoallergic drug eruption
Does the patient take a photosensitizing medication?
Chronic actinic dermatitis
NO YES
Consider onset and duration of lesions
Onset within hours to days, resolution within days to weeks
1636
Onset within minutes, resolution within hours
Polymorphic light eruption
Solar urticaria
hemophagocytic syndrome. HVLL has been identified mostly in children and young adults from Latin America and Asia.19 HVLL eruptions are distinguished from true HV by the development of lesions in both exposed and sun-protected skin and by the presence of systemic symptoms such as fever, hepatosplenomegaly, and lymphadenopathy.12,18,20 Facial edema with swelling of the lips and nose is common in HVLL, as is an eruption of papulovesicles on the legs.19,21 Histologically, HVLL is distinguished by an angiocentric/angiodestructive infiltrate of atypical cytotoxic lymphocytes.18,19,21
Clonal rearrangement of the T-cell receptor gene typifies HVLL but not HV.18 The distinction between an HVLL and true HV is important because patients with a HVLL have a grave prognosis, with the possibility of fulminant and rapidly fatal disease.19,21,22
CLINICAL COURSE AND PROGNOSIS
HV often resolves in adolescence but may occasionally persist into adult life. Males have a later onset and longer duration of the disorder than females.1 Age of onset appears to have prognostic value. Isolated cutaneous HV tends to present in early childhood, with a median age of onset around age 5 years.23 Conversely, “severe” variants of HV and HVLL have their onset later in the first or second decade of life,19,21,23 with one study identifying onset at age 9 years or later as significantly associated with mortality.23
MANAGEMENT
INTERVENTIONS
INTERVENTIONS
MEDICATIONS
HV often proves to be a refractory disease. Controlled clinical trials evaluating medical management of HV have not been performed. Occasionally, antimalarials appear to have helped, but their true value has not been established. Topical steroids, topical calcineurin inhibitors, and oral immunosuppressive medication tend to prove ineffective. In patients with chronic EBV infection, antiviral therapy with acyclovir and valacyclovir was reported in a small series of patients to reduce the frequency and severity of eruptions.24
Improvement also has been reported in isolated cases with administration of dietary fish oil.25,26
PROCEDURES
As with PMLE, prophylactic phototherapy with narrowband ultraviolet B or psoralen and ultraviolet A, particularly psoralen and ultraviolet A, may be helpful but must be administered with care to avoid disease exacerbation.2,13,27
17
COUNSELING
The mainstay of treatment of patients with HV relates to counseling regarding strict sun protection and avoidance strategies, including the use of broadspectrum sunscreens.
PREVENTION
PREVENTION
In mild cases of HV, sun avoidance and sunscreen use prevent HV eruptions.

Figure 94-1 Hydroa vacciniforme. Vesicular, bullous, and crusted facial lesions, which heal with vacciniform scars.

Figure 94-2 Hydroa vacciniforme. Induction of papulovesicles by ultraviolet A exposure.
Figure 94-3 shows an algorithm for abnormal responses to ultraviolet radiation.
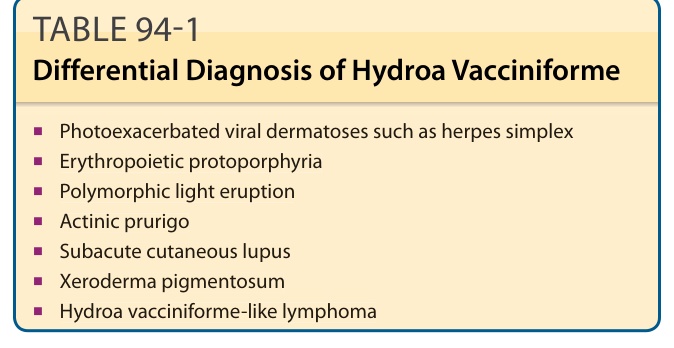
Table 94-1 outlines the differential diagnosis of HV. Importantly, HV must be distinguished from a similar entity designated by the World Health Organization