Nail Disorders
16
The diagnosis and treatment of nail diseases require an in-depth knowledge of the anatomy, physiology, and pathology of the nail unit (see Chap. 8). It is an integral part of the tip of the digit, and its anatomy, growth characteristics, and functions vary between the different fingers and toes, which have to be considered when faced with a diseased nail. There are different ways to classify nail disorders and a compromise between a scientifically based etiologic classification and a more clinico-morphologically based one appears to be a practical approach to nail disorders. This chapter discusses specific nail changes either resulting from particular nail disorders or from dermatologic or systemic diseases, the peculiarities, including etiopathogenetic aspects, of which are not repeated here if they are not specific for the nail lesions.
NAIL SIGNS AND NAIL- SPECIFIC CONDITIONS
ANONYCHIA, HYPONYCHIA, AND DOUBLE NAIL
ANONYCHIA, HYPONYCHIA,
AND DOUBLE NAIL
Complete or almost complete lack of the nail is called anonychia, severe hypoplasia, or hyponychia. The condition is usually inborn, may be a genetic trait or the result of drug or toxin-induced lack of nail formation during embryogenesis. Several different types are known, ranging from a round tip of the digit without any visible change of the skin to an area that may correspond to the nail field, or a hyperkeratosis. When there is no terminal phalanx and no nail growth this is called Cooks syndrome or atelephalangia with anonychia. Hyponychia may be on all or several digits and is more common. A particular form with half-side index fingernail hypoplasia and a Y-shaped radiologic alteration of the distal phalanx is characteristic for Iso-Kikuchi syndrome. Micronychia may be a sign of phenytoin and alcohol fetopathy and is a constant feature of congenital onychodysplasia of Iso-Kikuchi (COIF [congenital onychodysplasia of index finger] syndrome). Racket nail is a short wide nail, mostly of the thumb, which develops from the age of 12 years on and is the result of a premature ossification of the epiphysis of the distal phalanx. The bone cannot grow longitudinally but continues to get broader because of apposition on the sides. This condition is autosomal dominant with variable expression and penetrance. Very short nails (brachyonychia) may develop in patients under chronic hemodialysis who develop a tertiary hyperparathyroidism with resorption of the bone of the terminal phalanx.
A rudimentary double nail of the fifth toe is a relatively frequent finding in subjects of all races. The nail may be slightly wider and have a slight longitudinal indentation or be discernable as a complete accessory nail (Fig. 91-1).1
CHROMONYCHIA
CHROMONYCHIA
The nail may show a variety of color changes that may be caused by true coloration of the nail plate or alterations of the matrix and nail bed shining through the nail plate (Table 91-1). Leukonychia is the most common color change. It is caused by alterations in the keratinization of the nail plate with the nail cells being parakeratotic and/or having an eosinophilic cytoplasm in histologic sections. Often, these changes slowly disappear so that the free margin of the nail plate appears normal. Morphologically, there may be small patches or transverse bands, mainly seen in children and youngsters, probably the result of an overzealous manicure (Fig. 91-2). Total diffuse leukonychia (Fig. 91-3) is inborn in most cases. Subtotal diffuse leukonychia is sometimes seen in chronic liver disease. Many longitudinal white bands are characteristic for Hailey-Hailey disease. Apparent leukonychia is a result of nail bed pallor. It may disappear with temperature change or pressure. Muehrcke lines are a pair of 2 whitish transverse lines and are said to be a sign of hypalbuminemia (Fig. 91-4). Pseudoleukonychia is the white surface of the nail, which is infected by fungi. It was also termed (pseudo) leukonychia trichophytica although nondermatophyte molds also may be causative (Fig. 91-5). Erythronychia is the term for red nails. It may appear as red spots in the matrix (Fig. 91-6),2 one or more longitudinal streaks in the distal matrix and nail bed (Figs. 91-7 and 91-8). Multiple red bands are commonly caused by inflammatory conditions such as lichen planus, whereas a single red band may represent specific tumors such as onychopapilloma (Fig. 91-7) or Bowen disease; hence a biopsy is indicated. Alternating narrow white and red bands are seen in Darier disease. Chloronychia is the term for green nails. In almost all cases, it is caused by a colonization of the nail by Pseudomonas aeruginosa. Often, 1 margin of the nail is involved with circumscribed swelling and detachment of the proximal nailfold, lack of the cuticle, and lateral onycholysis (Fig. 91-9). However, it is also seen in distal onycholysis and onycholysis over subungual tumors. Although Pseudomonas colonization is harmless for the patient, it may pose a risk for immunosuppressed individuals and these patients should not work in kitchens, bakeries, other food industry jobs, or
in surgery, premature, and newborn wards and intensive care units. The treatment of choice of P. aeruginosa colonization is soaking in diluted white vinegar, 2 or 3 times daily for 10 minutes, then brushing the fingers dry. Household bleach for fingertip baths can be used
White–Leukonychia
■True leukonychia: hereditary, acquired; punctate, striate, diffuse (total, subtotal), multiple narrow white longitudinal lines: Hailey- Hailey disease, Darier disease
■Causes: idiopathic, microtrauma, manicure induced, liver disease, renal insufficiency
■Apparent leukonychia: pale nail bed in anemia, Raynaud syndrome, scleroderma
■Pseudoleukonychia: superficial white onychomycosis
Brown to Black–Melanonychia
■Melanin: activation of matrix melanocytes (functional melanonychia), matrix lentigo, nevus, melanoma
■Microbial pigments: Proteus spp, Klebsiella spp, melaninproducing fungi
■Exogenous: silver nitrate, potassium permanganate, heavy smoking, dirt
■Blood: acute or chronic trauma, friction
Green–Chloronychia
■Pseudomonas aeruginosa (pyocyanin)
Red–Erythronychia
■Red lunula: spotted or diffuse: acute nail involvement in several dermatoses such as erythema multiforme, alopecia areata, psoriasis, lupus erythematosus
■Longitudinal erythronychia: onychopapilloma, Bowen disease; multiple narrow red lines: dyskeratosis follicularis of Darier (often with some white lines in between).
Yellow–Xanthonychia
■All very thick nails appear yellow, often also onycholytic nails are yellow
■Yellow nail syndrome (triad of chronic bronchopulmonary infection, edema of the distal extremities, and extremely slow-growing yellow nails)
Blue–Azure Nail (Glauconychia)
Blue–Azure Nail (Glauconychia)
■Copper sulfate; gray-blue lunulae: ingestion of silver nitrate
■Copper sulfate; gray-blue lunulae: ingestion of silver nitrate
16
undiluted or 1:1 diluted in water. Other disinfective agents may be used in addition. Topical antibiotics such as gentamycin are sometimes used, but are no more efficacious. Systemic antibiotics do not reach the site of infection because Pseudomonas mainly colonizes an onycholytic nail. In rare cases, systemic treatment with ciprofloxacin may be indicated. Blue nails were seen developing in persons swimming in water with copper sulfate as a disinfective agent. Slate-gray to bluish nail matrix is a sign of argyria.3
Melanonychia denotes brown-to-black nail pigmentation. Although this term is generally used for melanin pigmentation of the nail, many other agents may stain the nail brown, such as potassium permanganate or tobacco smoke. Silver nitrate makes the nail jet-black (Fig. 91-10). Some bacteria cause dirty grayish discoloration (Fig. 91-11). Melanonychia may be diffuse and total, transverse or longitudinal. Usually, a brownto-black band develops in the nail running from the proximal nailfold into the free margin of the nail plate. It is caused by melanocyte activation, a lentigo, nevus,
1569
16
or melanoma of the matrix. Multiple melanonychias in several or all digits are common in dark-skinned individuals and Asians and are a physiologic phenomenon seen in almost all African Americans (Fig. 91-12). Pregnancy, a variety of drugs, vitamin B12 deficiency, Addison disease, HIV infection, some dermatoses such as ungual lichen planus, and Bowen disease of the nail (particularly when associated with human papillomavirus [HPV] Type 56) may exhibit melanonychias. The
1570
association of lenticular labial, oral, and genital mucosal brown spots with melanonychias is characteristic for Laugier-Hunziker-Baran syndrome. Friction from rubbing shoes may cause longitudinal melanonychia of the little or big toenail, and onychophagia may cause melanocyte activation with subsequent melanonychia. Longitudinal nail pigmentation is the most frequent sign of nail melanoma and requires a meticulous evaluation. Single-digit melanonychia in an adult requires a biopsy.
SUBUNGUAL HEMATOMA
SUBUNGUAL HEMATOMA
A single, heavy trauma that is usually well-remembered because of its intense pain, or repeated microtraumas, most commonly from ill-fitting shoes or
particular sports activities, lead to bleeding under the nail (Fig. 91-13). The blood is located between the overlying nail and the underlying matrix and nail bed
A
16
epithelium and is therefore not degraded to hemosiderin by macrophages; consequently, it remains Prussian blue–negative or Perls stain–negative. With time it is included into the newly formed nail. It takes some months to slowly grow out but, in contrast to melanonychia, it never reaches into the free margin of the nail plate; this is one of the most reliable criteria for differential diagnosis. It also does not form a regular longitudinal band and when growing out a normal nail reappears. Dermatoscopy shows round red to dark-brown globules. Acute subungual hematoma can be drained by drilling a small hole into the nail plate to release the blood. Hematomas occupying more than 50% of the nail field are commonly associated with a fracture of the distal phalanx.
SPLINTER HEMORRHAGES
SPLINTER HEMORRHAGES
Splinter hemorrhages are narrow red to almost black longitudinal lines in the distal nail bed and are caused by blood that is enclosed in the subungual keratin (Fig. 91-14). They develop either from thrombosed or ruptured capillaries that run longitudinally in the nail
B
1571
16
bed. They are characteristic for trauma, psoriasis, and some other inflammatory nail and systemic diseases, such as scleroderma, systemic lupus erythematosus, rheumatoid arthritis, antiphospholipid syndrome, and hematologic malignancies. Splinter hemorrhages also are characteristic for bacterial endocarditis with subsepsis lenta (39%) where they may occur together with Osler nodes (6.7%), Janeway lesions (2.2%), and retinal hemorrhages called Roth spots (3%). Oblique splinter hemorrhages may be a sign of trichinosis.
ONYCHOLYSIS
ONYCHOLYSIS
Detachment of the nail from the distal nail bed is called onycholysis. All conditions with abnormal subungual hyperkeratosis will eventually cause onycholysis. These may be inflammatory nail diseases such as psoriasis (Fig. 91-15), lichen planus (Fig. 91-16), atopic dermatitis, and pityriasis rubra pilaris, or infections such as onychomycoses, or tumors of the nail bed. Direct trauma resulting from overzealous nail cleaning is the
1572
cause of onycholysis semilunaris (Fig. 91-17). This is characterized by sharply delimited proximal margins that may look like a half moon. Repeated frictional trauma is another cause, particularly in the asymmetric gait nail unit syndrome (see below). Onycholysis is usually colonized by a variety of microorganisms, both bacteria and fungi. Treatment is the avoiding of moisture, cutting the nail back to the adherent part, brushing the nail bed twice daily with a disinfective solution, and applying an antimicrobial cream. Approximately one-half of the regrowing nail will remain attached to the nail bed; however, once having been onycholytic, a nail remains susceptible to reoccurrence of onycholysis.
SUBUNGUAL HYPERKERATOSIS AND ONYCHOGRYPOSIS
SUBUNGUAL
HYPERKERATOSIS AND
ONYCHOGRYPOSIS
Hyperkeratosis of the nail bed is a frequent event (Fig. 91-18). It is characteristic for onychomycoses
where it contains most of the fungi, and for psoriasis. Other frequent causes are trauma, allergic and toxic contact, and atopic dermatitis. It is virtually always associated with onycholysis, except in pachyonychia congenita, where the nail covers an excessive nail bed hyperkeratosis in a horseshoelike fashion. Onychogryposis (the common spelling, onychogryphosis, is etymologically incorrect as gryphos means a mythical animal that is half bird–half lion, whereas grypos means horn, hence it should be written onychogryposis) is an exaggeration of nail bed and matrix hyperkeratosis. It consists of innumerable stacks of keratin layers piled up one over the other, grows upward, is opaque and often has the shape of a ram’s horn. There is usually no contact with the nail bed anymore and the nail pocket is extremely short. It is mainly seen in elderly, neglected, and debilitated individuals (Fig. 91-19). Treatment is by nail avulsion, often completed by nail matrix cauterization to prevent regrowth of a grypotic nail.
16
PTERYGIUM
PTERYGIUM
Pterygium (from Greek for wing formation) is the bridging of the nail pocket by connective tissue, in most cases scars. It is very common in lichen planus (Fig. 91-20), but is occasionally seen in other conditions, such as bullous pemphigoid, but particularly also after trauma. It first divides the nail into 2 parts, but may lead to complete nail destruction when it occupies almost the entire nail pocket.
PTERYGIUM INVERSUM
PTERYGIUM INVERSUM
When the nail plate does not separate correctly from the nail plate at the hyponychium and remains attached, a painful hyperkeratosis obliterates the distal groove. This is quite common in acral scleroderma and Raynaud syndrome, but also may be idiopathic (Fig. 91-21). Nail trimming can be very difficult and painful.
1573
16
BEAU LINES AND ONYCHOMADESIS
BEAU LINES AND
ONYCHOMADESIS
A temporary slowdown or even arrest of nail formation results in a transverse groove that runs parallel to the lunula border (Fig. 91-22). It may be shallow at the lateral portions and deeper centrally. Onychomadesis is the result of a longer-lasting arrest of nail matrix proliferation that eventually results in a proximal gap in the nail and proximal onycholysis (Fig. 91-23). It may end up in loss of the nail. The faster a nail grows the more pronounced the lesion; hence Beau lines and onychomadesis are much more common in fingernails than in toenails. Repeated Beau lines indicate repeated trauma, such as chemotherapy cycles. Equally distributed Beau lines hint at a general cause, whereas onesided lines are seen after surgery of the extremity or a single-digit line at previous finger or toe surgery. A great many different causes are known, ranging from high fever to other serious diseases. Localized Beau lines and onychomadesis were also seen several weeks after hand-foot-and-mouth disease (coxcackie- virus infection). Trauma, cosmetic manipulations,
1574
onychophagia, and onychotillomania are other causes and explain why the fingernails are predominantly affected (Table 91-2).
PITTING AND TRACHYONYCHIA
PITTING AND
TRACHYONYCHIA
Pits are small depressions in the nail surface resulting from minute foci of abnormal keratinization in the apical matrix. This produces small mounds of parakeratosis that tend to break away from the nail when this emerges from under the proximal nailfold. Sometimes, the parakeratosis is not shed and small ivory-colored spots are seen. Pits are the most frequent sign of nail psoriasis (Fig. 91-24) where they are deep and of regular size, whereas those developing in alopecia areata and atopic dermatitis are more shallow and less-well delimited. Large surface defects are typical for pustular psoriasis and are called elkonyxis (Table 91-3). Trachyonychia is the term for rough nails (Fig. 91-25). In addition to multiple pits, longitudinal striations and ridges such as seen in ungual lichen planus may cause
this condition. When many nails are affected the diagnosis of 20-nail syndrome can be made. Longitudinal grooves are the result of pressure on the nail matrix, which is usually the result of a small tumor in the proximal nailfold (Fig. 91-26).
BRITTLE NAILS
BRITTLE NAILS
Brittle nails are a very common complaint in daily practice, particularly by women. Multiple longitudinal fissures, often associated with nail thinning and ridges, are the hallmark of onychorrhexis (Fig. 91-27). Defective keratinization is thought to be one of the causes. Onychoschizia is the lamellar splitting of the nail at its free end (Fig. 91-28). It is usually confined to fingernails and occurs much more often in women than in men, pointing to the importance of environmental factors, such as frequent water contact that results in hydration and dehydration of the nail, which leaks cementing lipoproteins out. In babies with koilonychia of the big toenail, onychoschizia is common. Other causes are some dermatoses, onychomycosis, peripheral
16
■Generalized: Acute severe diseases, high fever, some drugs (retinoids), zinc deficiency, autoimmune bullous diseases, menstruation (often repeated)
■Generalized: Acute severe diseases, high fever, some drugs
(retinoids), zinc deficiency, autoimmune bullous diseases, menstruation (often repeated)
■One extremity: carpal tunnel syndrome (hand), surgery with extremity tourniquet, reflex sympathetic dystrophy (regional pain syndrome)
■One extremity: carpal tunnel syndrome (hand), surgery with
extremity tourniquet, reflex sympathetic dystrophy (regional pain syndrome)
■One or several digits: nail surgery, hand-foot-and-mouth disease, trauma
■One or several digits: nail surgery, hand-foot-and-mouth disease,
trauma
■Psoriasis
■Psoriasis
■Eczema
■Eczema
■Alopecia areata
■Alopecia areata
■Lichen planus
■Lichen planus
■Graft-versus-host disease
■Graft-versus-host disease
■Rheumatoid arthritis
■Rheumatoid arthritis
1575
16
neuropathies and vascular disease, occupational traumas, and a variety of drugs, particularly those interfering with nail growth (Table 91-4). The role of nutrition is frequently overestimated.4
INGROWN NAILS
INGROWN NAILS
Ingrown nails also affect adults and the elderly, but to a much lesser degree in terms of frequency. The most common type is distal–lateral ingrowing of the edge of the big toenail (Fig. 91-29), rarely of neighboring toes, and even less frequently of fingers (Fig. 91-30). There are many theories as to why and how ingrown nails develop and several are not exclusive of another one. Commonly, there is a discrepancy between too wide a nail plate and too narrow a nail bed. Usually, this is true for the distal portion where most pressure from shoes acts on the toes. The tip is compressed, it hurts, and the patient tries to cut the edge away, thereby leaving a kind of a spicule behind that pierces into the soft tissue of the distal portion of the nail sulcus causing pain, suppuration, granulation tissue, swelling, and,
1576
with time, fibrosis of the nailfold.5 Further etiologic factors are tight socks, hyperhidrosis, and overcurvature of the nails. Treatment is either conservative with insertion of a wisp of cotton between the offending nail and the nail sulcus, taping to pull the soft tissue away from the nail, or protection of the soft tissue from the nail margin by a gutter, which requires a local anesthesia. There are many more conservative approaches; however, all require consistent compliance from both the physician and the patient. Surgery is either to narrow the nail or to remove the swollen soft tissue (see Chap. 205).
RETRONYCHIA
RETRONYCHIA
Proximal ingrowing of the nail is called retronychia. It is caused by a single strong or repeated minor trauma to the nail that eventually results in a backward movement of the nail plate. Most patients are children, adolescents, and young adults with 1 or 2 swollen, bluish, proximal nailfolds of their big toes (Fig. 91-31). The lunula is no longer present. On pressure, granulation tissue may emerge from under the nailfold. Careful clinical examination reveals that there is a major onycholysis of the nail that allows the plate to be pushed backward. This leads to a horizontal split in the matrix. As the nail bed is mainly responsible for the forward growth
Note: General disorders tend to affect all nails; fingernail-only involvement points at an etiology linked to wet work. Single-digit nail splitting is most likely a circumscribed disease or tumor.
Note: General disorders tend to affect all nails; fingernail-only involve-
ment points at an etiology linked to wet work. Single-digit nail splitting is most likely a circumscribed disease or tumor.
■Chronic anemia; iron deficiency; zinc deficiency; vitamins A, B6, and C deficiencies; hypervitaminosis A; genetic diseases with disturbance of keratin formation
■Chronic anemia; iron deficiency; zinc deficiency; vitamins A, B6, and
C deficiencies; hypervitaminosis A; genetic diseases with disturbance of keratin formation
■Local damage from trauma, alkalis, detergents, overzealous manicure
■Local damage from trauma, alkalis, detergents, overzealous
manicure
of the nail, this mechanism may no longer function and 1 or more new nails will be formed under the old proximal nail portion lifting this up. Its margin is very hard and sharp so that it cuts into the undersurface of the proximal nailfold with each step. The Y-shaped, W-shaped, or serrated proximal nail margin is well seen when the nail is avulsed, which is the treatment of choice.6
16
A
B
PINCER NAILS (NAIL OVERCURVATURE)
PINCER NAILS (NAIL
OVERCURVATURE)
Overcurvature of the nails is commonly called pincer nails, tubed nails, trumpet nails, and the like. The most common variant shows a distally increasing curvature (Fig. 91-32), but it may also remain at the same degree (tile nail) or exhibit sharp lateral bends. Half-side overcurvature is quite common. There are 2 types: acquired as a result of foot deformation, degenerative distal interphalangeal osteoarthritis (mainly in fingers), and some dermatoses, and hereditary with symmetrical involvement of the big toenails and often some, but very rarely all, lesser toenails. The big toenails show lateral deviation, the affected lesser nails are medially deviated. The base of the distal phalanx is widened, which can be felt by sliding palpation of the toe. Systematic radiographic examinations of the toes show that the distal phalanx is asymmetrical and often shows distally pointing exophytes that may correspond to the insertion of the interosseous ligament; they are much more pronounced medially than laterally, which explains in part the increasing lateral deviation of the nail plate. Furthermore, a distal dorsal traction osteophyte is commonly seen, which has to be removed when surgically flattening and spreading out the nail bed. In the distal portion,
1577
16
A
B
the overcurved nail pinches the nail bed and heaps it up, resulting in a reactive subungual hyperkeratosis.7 Treatment is by long-term application of nail braces to decrease the curvature, or a surgical procedure.
EFFECTS OF NAIL TREATMENT
EFFECTS OF NAIL
TREATMENT
The nails are not only subject to many environmental and traumatic influences, but also the target of cosmetic and medical treatments that often have a profound effect on the integrity of the nail. Nail hardeners are frequently prescribed for brittle nails. They contain formaldehyde that renders the nails harder and decreases their elasticity. Nail varnish is usually well tolerated but the tosyl formaldehyde resin may be the cause of allergic contact dermatitis. Artificial nails made from acrylics or cyanoacrylates may also cause contact dermatitis, often in the face and neck, less frequently of the nails; here, the reaction may persist for a long time, even after removal of the artificial nails, and be associated with long-lasting or even persisting pain. Gel nails are presently very popular. They are very hard and their removal requires harsh treatment with a coarse file that thins the nail plate and thus damages
1578
it. Chemical peels of the nail with 70% glycolic acid to improve their surface have been described8; their rationale remains to be clarified. Overzealous manicure is the cause of many untoward effects such as onycholysis semilunaris, wavy nail surface, loss of the cuticle with penetration of foreign substances under the proximal nailfold and subsequent paronychia, and bacterial colonization and infection. Urea in high concentrations is used to soften mycotic nails; urea 40% paste under occlusion for 3 to 5 days makes the infected nail portions soft enough to allow them to be scraped off.
INFLAMMATORY NAIL DISORDERS
PSORIASIS
PSORIASIS
AT-A-GLANCE
■ Psoriasis is the dermatosis with the most frequent nail involvement.
■ Approximately 50% of all psoriatics have nail changes at a given time, but 90% will have nail alterations at least once in their life.
■ Nail involvement is even more frequent in psoriatic arthritis.
■ The most frequent nail changes are pits, subungual hyperkeratosis, onycholysis, salmon spots, red lunulae, splinter hemorrhages, leukoplakia, and psoriatic paronychia.
■ Infection with pathogenic fungi is frequent and should be treated first.
Psoriasis is the skin disease with the most frequent nail involvement. At the time of consultation, approximately 50% of the patients present with nail changes. Over their lifetime, up to 90% of all psoriatics will develop nail alterations. The prevalence is even higher in psoriatic arthritis.
ETIOLOGY AND PATHOGENESIS
There appears to be neither a gender nor race predilection. In contrast to skin, there is no association of human leukocyte antigen (HLA)-C0602 with nail and joint involvement, and nail psoriasis is often associated with inflammation at the insertion points of tendons and ligaments, giving rise to enthesitis. The nail lesions were thought to represent an aberrant response to tissue stressing of the integrated nail–joint apparatus, rather than being the result of an autoimmunity. The nail-and-joint disease may be linked to tissue-specific factors, including tissue biomechanical stressing and microtrauma that lead to activation of aberrant innate immune responses.9
CLINICAL FEATURES
Psoriasis causes both very specific and ambiguous nail lesions (Figs. 91-33 to 91-35). The most characteristic and most frequent signs are pits representing small, sharply delimited depressions in the nail surface of remarkably even size and depth. They may be haphazardly arranged or sometimes show parallel transverse or short longitudinal lines (Fig. 91-33). They are thought to arise from tiny psoriatic lesions in the apical matrix leading to parakeratosis that breaks off leaving these hole-like lesions. When the parakeratosis remains it is seen as an ivory-colored spot in the proximal third of the nail plate (Fig. 91-34). Pits may be single, which is not yet psoriasis specific, or multiple. Ten pits per nail or more than 50 pits on all nails are seen as proof of nail psoriasis. Rarely, red spots are seen in the lunula usually representing a very active psoriasis lesion with dilation of the capillaries and thinning of the suprapapillary plate.10 Complete nail destruction following crumbling of the plate is a sign of total matrix affection (Fig. 91-35). Leukonychia is seen when the psoriatic lesion is in the mid to distal matrix and parakeratotic cells are incorporated into the nail plate, making it optically appear white. It is commonly an ill-defined white transverse band, but other morphologies are possible. Splinter hemorrhages are some millimeters long, reddish–dark-brown to black
16
streaks of barely 1 mm in diameter. They are analogous to the Auspitz phenomenon on the skin and result from damage to the dilated capillaries in the nail bed causing the blood to clot in these longitudinally arranged small vessels. Salmon spots are frequent. They represent psoriatic plaques in the distal matrix
1579
16
and the nail bed. The nail looks like paper on which a drop of oil has fallen: A yellowish-brownish spot with a red margin shines through the plate. The reason for this is that the squames of the psoriasis lesion are imbibed with serum and compressed under the nail. When such a salmon spot reaches the hyponychium, part of the parakeratosis breaks out and psoriatic onycholysis develops, which typically has a reddish proximal margin differentiating it from most other causes of onycholysis. In addition, there is often subungual hyperparakeratosis without oil-drop phenomenon causing onycholysis. Psoriatic hyperkeratosis may be marked and sometimes so extreme that it resembles pachyonychia congenita. Psoriasis involving both the dorsal and ventral surface of the proximal nailfold causes thickening and rounding of its free edge, which, in turn, are associated with loss of the cuticle, thus giving the pattern of chronic paronychia. In psoriatic arthritis, nail involvement is often severe with psoriatic paronychia, complete nail destruction, and swelling of the distal interphalangeal joint. Psoriatic pachydermoperiostosis is a condition closely related to psoriatic arthritis but usually without obvious nail changes. Mainly the big toe is considerably thickened and often painful. Pustular psoriasis occurs in 3 different forms, all of which also involve the nail. In the palmar plantar pustular psoriasis of Barber-Königsbeck, all nail changes described above as well as larger surface defects called elkonyxis, plus subungual yellow spots representing large Munro abscesses may be seen (Fig. 91-36). Generalized pustular psoriasis of von Zumbusch occasionally causes red areas with a rim of small pustules that may affect the nail. Subungual abscesses are frequent. The most notorious form of pustular psoriasis is acrodermatitis continua suppurativa of Hallopeau. Often beginning with a single digit, the skin of the distal phalanx becomes red, develops some pustules that migrate under the nail and cause nail dystrophy, which, with time, may lead to complete disappearance of the nail unit so that only a red smooth digit tip is left until the disease slowly wanes off. However, acrodermatitis continua suppurativa may also initially involve several fingers and toes and run a very severe course
1580
(Fig. 91-37). A mutation in the gene for the interleukin-36 receptor antagonist leading to a defect in interleukin-36 receptor antagonist was found in generalized pustular psoriasis and acrodermatitis continua suppurativa, supporting the assumption that these conditions belong to the group of autoinflammatory diseases.11,12
Reiter disease, also known as reactive arthritis, is a systemic condition with characteristic joint, mucosal, eye, genitourinary, skin, and nail changes. The latter are very similar to pustular psoriasis although they usually have a more brownish tint because of the content of erythrocytes in the pustules (Fig. 91-38). Histopathology also shows spongiform pustules.
16
PSORIASIS ONYCHOMYCOSIS
Frequency High, most common dermatosis with nail involvement Very high: up to 30% to 40% of all nail diseases
Course Chronic, often recurrent Chronic, often progressive
Symptoms Usually embarrassing cosmetically and functionally Embarrassing, sometimes pain
Signs
Variable, depending on nail structure involved
■Pits
■Very common, regular
■Onycholysis
■Common
■Discoloration
■None to yellow
■Spores and hyphae
■Rarely spores
■Transverse furrows
■Rare
■Skin lesions elsewhere
■Very common
Variable, depending on severity and type of onychomycosis
■Rare, irregular
■Common
■Yellow to brown
■Very frequent
■Rare
■Often tinea
Trauma May induce Köbner phenomenon Important predisposing factor
Heredity Strong hereditary component, particularly in juvenile
Autosomal dominant susceptibility to develop
Heredity Strong hereditary component, particularly in juvenile onset psoriasis Autosomal dominant susceptibility to develop onychomycosis
onset psoriasis
DIAGNOSIS
In most cases, nail psoriasis is diagnosed on clinical grounds. Skin lesions elsewhere plus 1 or several psoriatic nail features suggest the correct diagnosis. Histopathology is usually pathognomonic and helps to delineate nail psoriasis from other conditions, particularly onychomycosis. Reiter disease requires additional laboratory examinations.
DIFFERENTIAL DIAGNOSIS
ASSOCIATIONS
Psoriasis is a frequent skin disease. Hence co-occurrence with other dermatoses that may also involve the nail is not exceptional. The most important association is that with onychomycosis as both conditions may look very similar, but a psoriatic nail may be colonized with pathogenic fungi and a true infection of the psoriatic nail is not infrequent (see Table 91-1).
COURSE
Why nail psoriasis often improves and worsens is unknown, although trauma may play an important role in the exacerbation of nail psoriasis. There may be periods without any nail alterations.
TREATMENT
Nail psoriasis is very resistant to almost all topical treatments whereas systemic therapies clearing the skin are usually also effective in nail psoriasis. The problem of all topical treatments is the penetration of the drug to the diseased tissue: through the nail plate in nail bed
onychomycosis
psoriasis, through all layers of the proximal nailfold plus the underlying nail in matrix lesions. Hence, pits, even though often being rather inconspicuous, are the most resistant to treatment. Nevertheless, a 3-month trial of a combination of a vitamin D3 derivative with a potent corticosteroid is warranted. The less of the nail is present, the easier is penetration of the drug to the very psoriatic lesion. The list of other drugs tried is long and mostly comprises anecdotal reports and small case series. Injections of triamcinolone acetonide crystal suspension, 10 mg/mL every 6 weeks, into the proximal nailfold often improves nail psoriasis, but is painful and cumbersome for the patient. Methotrexate injections were also given with some success; however, this cytostatic drug may slow down nail growth and make an improvement visible only very late. The best treatment results are those with systemic antipsoriatic therapies, including biologics (see Chap. 28 for details).13
ECZEMA
ECZEMA
AT-A-GLANCE
■ Eczema is a traditional dermatologic term denoting a frequent reaction of the epidermis to a large variety of different stimuli; it is often used synonymously with “dermatitis.”
■ Virtually all nail components may show eczematous changes: matrix, nail bed, periungual skin.
■ Allergic contact dermatitis may be the result of nail cosmetics, particularly acrylic nails; this type of contact dermatitis may last longer than the actual duration of exposition.
1581
(Continued)
16
AT-A-GLANCE (Continued)
Continued
AT A GLANCE (
)
■ Toxic contact dermatitis may be indistinguishable from allergic dermatitis and psoriasis.
■ Atopic dermatitis may cause rough nails when the matrix is involved, or very shiny nails when they are used to rub the itchy skin.
■ Nummular eczema is occasionally seen on the proximal nailfold.
In this context, the term eczema is used as a collective one comprising allergic contact dermatitis, toxic/ irritant contact dermatitis, atopic dermatitis, and nummular eczema; seborrheic eczema does not occur in the nail unit. They have a common denominator, the socalled spongiotic dermatitis.
CLINICAL FEATURES
Although differing in typical cases the clinical features may be similar between the different forms of eczema (Fig. 91-39), particularly in chronic eczema. Acute allergic contact dermatitis exhibits redness of the periungual skin with tiny vesicles that tend to break and ooze. Serous crusts follow. Secondary infection with pyogenic micrococci leads to impetiginization. With time, oozing disappears, the redness decreases, and desquamation develops followed by cracking, particularly of the volar aspects and transition to the hyponychium and lateral nailfolds. The nails may become grossly deformed with deep asymmetric transverse furrows and ridges. Matrix and nail bed involvement is rather rare, but when present, for example, in patients with an allergy to artificial nails, may be painful. The nail itself loses its transparency as the spongiotic dermatitis of the matrix leads to inclusion of serum in the plate. The nail bed appears to be hyperkeratotic, even though this is a mixture of subungual keratin with serum inclusions. Chronic allergic contact dermatitis of the proximal nailfold leads to swelling, loss of the acute angle of its free margin with disappearance of the cuticle and separation of the underlying nail plate.
1582
Toxic contact dermatitis rarely begins acute with erythema, vesicle formation, and oozing, such as from certain plants like garlic. Chronic irritant contact dermatitis is characterized by redness, scaling, fissures, and paronychia. It is often indistinguishable from chronic allergic dermatitis. Nummular eczema of the nail region mainly involves the proximal nailfold with round red infiltrated plaques exhibiting tiny papules that are covered with a small serosanguinolent crust. Atopic dermatitis may affect the nail in different ways. Shiny nails are characteristic in chronic itchy atopic dermatitis of children and young and middleaged adults. These individuals “learned” not to harm their skin by scratching with the free margin of the nails and to relieve the itch by rubbing with the back of the distal phalanx. The use of emollients may enhance the polishing action of this habit. Atopic pulpitis sicca demonstrates desquamation and cracking of the finger and toe tips and is often also a feature of atopic winter feet. Painful cracks starting in the lateral nail groove of the thumbs and extending to pulp are often seen in elderly atopics. Frank “eczematous” changes are exceptional. Trachyonychia is the term for rough nails and a hallmark of the so-called 20-nail dystrophy. In author’s experience, most cases are caused by atopic dermatitis, although psoriasis, alopecia areata, and nail lichen planus were also found as the underlying disorder.14
Many nails, rarely all 20 nails, are affected, but often 1 or more nails remain normal despite progression of the alterations. The nails become very rough, lose their shine and transparence, often turn partly koilocytotic, and the cuticles become thickened and ragged. Most cases are children between 6 and 10 years of age, sometimes younger. The condition usually runs a protracted course until, in many cases, the nails become normal from age of 14 to 16 years on.
ETIOLOGY AND PATHOGENESIS
The rare occurrence of allergic and irritant contact dermatitis on toenails as compared to fingernails points at the importance of nail cosmetics as well as a number of household allergens. The household allergens are complicated by the fact that (immediatetype) contact allergy to food may be chronic and superimposed by chronic irritation as well as colonization with yeasts.15 Painful matrix and nail bed dermatitis is characteristic for acrylate allergy. The exact etiopathogenesis of nummular eczema is not yet fully elucidated.
DIAGNOSIS
Acute allergic contact dermatitis is usually diagnostic, although rare cases of acute irritant contact dermatitis may look identical. Skin tests are commonly applied both to make the diagnosis as well as find out the responsible allergen. In acrylate allergy, ectopic skin
lesions may characteristically be found on the neck, décolleté, and around the eyes, a result of vapors of the acrylic monomer. Atopic dermatitis almost invariably demonstrates lesions on other body sites that may vary according to the age of the patient. In nummular eczema, lesions are commonly seen on the forearms and lower legs. Twenty-nail dystrophy is diagnosed in children when more than 10 nails are involved. Histopathology shows a spongiotic dermatitis in acute cases, but a more psoriasiform epidermal hyperplasia in chronic eczema. Persistent allergic contact dermatitis caused by acrylates exhibits a dense, often band-like lymphocytic infiltrate, exocytosis, and spongiosis with massive acanthosis of the matrix and nail bed epithelium as well as lymphocytes and serum in the nail plate. Nummular lesions show spongiotic vesicles in the upper half of the epidermis with clotted serum on top. In trachyonychia, there is a very severe spongiotic inflammation with strong exocytosis of T lymphocytes that migrate upward and become part of the nail plate.
DIFFERENTIAL DIAGNOSIS
Chronic allergic and irritative contact dermatitis are difficult to distinguish from each other, as well as from psoriasis, ungual lichen planus, and alopecia areata. Careful examination of the entire skin is a must for each dermatologist. Chronic paronychia occurs in all contact dermatitides. Parakeratosis pustulosa is a rare condition that mainly occurs in young girls and exhibits vesiculopustular lesions of the hyponychium extending into the distal nail bed. After some weeks the condition resembles an eczema or psoriasis. Twenty-nail dystrophy usually represents an eczematous reaction.
CLINICAL COURSE, PROGNOSIS, AND MANAGEMENT
Except for acute allergic contact dermatitis, all other eczemas usually run a protracted course. However, even grossly distorted nails may become completely normal when the cause is found and eliminated and the condition adequately treated, which may be difficult in persons who have to handle food and/or expose their hands to a harsh environment. In addition, smoking and nail cosmetics, as well as particular habits, often complicate treatment. Twenty-nail dystrophy is a disease of children and said to disappear spontaneously at the age of approximately 16 years. Periungual eczematous lesions respond to topical steroids, but chronic paronychia may require intralesional steroid injections. Very severe and painful lesions may have to be treated systemically as transungual penetration is insufficient for matrix and nail bed involvement. Very recalcitrant paronychia can be treated surgically by a beveled excision of the thickened part of the proximal nailfold.
16
ALOPECIA AREATA
ALOPECIA AREATA
AT-A-GLANCE
■ Nail involvement in alopecia areata is frequent: the more severe the alopecia areata, the more frequent the nail involvement.
■ The nails are rough, as if sandpapered, with innumerable small pits.
■ The surface may keep its shine or have lost it.
■ The nails often lose their transparence due to inclusion of serum globules, this makes them also brittle.
CLINICAL FEATURES
Alopecia areata (AA) affects between 6 and 7 million individuals in the United States. The prevalence of nail abnormalities varies between 10% and 65%. They may precede, occur concurrently with, or follow hair loss activity. There is no known age, race, or ethnic preponderance. In contrast to other autoimmune diseases, the hair follicle does not usually sustain permanent injury and maintains its potential to regrow hair. AA often affects the nails; the more severe the AA, the more likely is nail involvement. Thus nail changes are rare in the most frequent mild type of AA with only a few bald patches and a high rate of spontaneous resolution, whereas nail changes are rather the rule in AA universalis. However, it is generally accepted that there may be nail AA without hair loss. Two types of nail alterations are seen: rough nails that have lost their shine and pitted nails with surface shine (Fig. 91-40). The nails may lose their transparence, get thicker, become brittle and split distally. The cuticles may become ragged. Koilonychia is a sign of very severe nail involvement.
ETIOLOGY AND PATHOGENESIS
AA is an autoimmune disease mediated by naturalkiller group 2 member D expressing CD8+ lymphocytes and it can be assumed that the etiology of nail AA is not different from that of hairy skin. However, the pathogenesis appears to be variable as nails do not fall off in contrast to hair, and the histopathologic pattern of inflammation in hair follicles and nails are different; exact data are not yet known. AA preferentially affects pigmented hairs, and the hair of AA patients frequently shows a change in color when it regrows following an acute episode of AA. Although this might indicate a relationship between AA, pigmentation, and melanin-concentrating hormone signaling nails are usually not pigmented in light-skinned individuals. Whether or not duplications in MCHR216 are important for the involvement in nail AA pathogenesis remains to be elucidated.
1583
16
DIAGNOSIS
In the typical case, the diagnosis is self-evident. However, AA is a relatively frequent disorder and associations with other conditions potentially affecting the nail are possible. Thus, ruling out atopic dermatitis, psoriasis, lichen planus, or onychomycosis may be warranted. The real problem is to make the diagnosis of isolated nail AA. Nail biopsy shows a spongiotic dermatitis with lymphocyte exocytosis involving the matrix; thus the histopathologic pattern is different from that of the scalp. The nail surface is wavy and often serum inclusions are seen in the nail plate.17 There are no laboratory examinations that help make the diagnosis of nail AA.
DIFFERENTIAL DIAGNOSIS
In the presence of round bald spots on the scalp, the diagnosis of a pitted nail is obvious. However, pits were also observed in different eczemas, lichen planus, ichthyosis vulgaris, and, above all, psoriasis. In psoriasis, the pits are deeper and a bit larger.18
DISEASE ASSOCIATIONS
Asthma, allergic rhinitis, atopic dermatitis, thyroid disease, and autoimmune diseases, such as thyroiditis and vitiligo are common associated diseases.
1584
CLINICAL COURSE, PROGNOSIS, AND MANAGEMENT
Occurring more commonly in severe AA, the nail changes usually run a protracted course over years. Successful systemic treatments will greatly improve the nails. Tofacitinib is a Janus kinase inhibitor with a good effect on hair loss and nail changes in nail AA. It is assumed that other Janus kinase inhibitors also might be beneficial for the treatment of nail changes in AA.19 Apremilast did not induce hair regrowth in severe AA. Topical treatments with steroids or steroid– calcipotriol combinations are often tried, but mostly in vain. Injections of triamcinolone acetonide crystal suspension, 0.5 to 1 mg per proximal nailfold, have to be repeated every 4 to 6 weeks, but are cumbersome and painful. The prognosis of nail AA is linked to that of AA in general. The nail lesions may persist longer than the hair loss. Permanent nail dystrophy after resolution of the AA is not observed. The patient has to be counseled concerning the nature of the disorder and the chronicity of nail lesions in AA. This is particularly important in children where the parents require detailed information as to the natural course of AA and its nail alterations.
LICHEN PLANUS OF THE NAILS
LICHEN PLANUS
OF THE NAILS
AT-A-GLANCE
■ Lichen planus rarely affects the periungual skin, most commonly the proximal matrix and less frequently the nail bed.
■ Matrix involvement leads to longitudinal ridging and splitting until the distal nail plate breaks away and a pterygium develops.
■ Nail bed affection causes subungual hyperkeratosis with onycholysis.
■ Postlichen atrophy is the end stage of ungual lichen planus.
■ Variants of ungual lichen planus include pigmented lichen planus, ulcerated lichen planus, and bullous lichen planus.
CLINICAL FEATURES
Nail lichen planus is a chronic disease that usually occurs in association with typical skin lesions (Figs. 91-41 and 91-42). Depending on the particular structure of the nail apparatus affected, variable clinical alterations develop. Most commonly, the apical matrix is involved leading to ridging, rough nails, loss of nail shine, longitudinal
surface defects, and splits. Nail bed lichen planus is rare; it may cause subungual orthokeratosis with subsequent onycholysis. Even bullous lichen planus of the nails is possible.20 Involvement of the proximal nailfold results in a bluish-red discoloration, sometimes associated with swelling. Longstanding nail lichen planus may lead to nail thinning and obliteration of the nail pocket with pterygium formation. The nail edge may look frayed. As the apical matrix is the site of the nail stem cells,21 scarring with permanent nail dystrophy may occur. Ulcerating nail lichen planus is very rare. Finally, a progressive nail atrophy may develop characterized by nail thinning and extreme fragility thus very similar to nails in amyloidosis.
ETIOLOGY AND PATHOGENESIS
The similarity of clinical and histopathologic nail alterations in graft-versus-host disease with those of lichen planus has supported the view that it is an autoimmune disorder. Nonwhites appear to have nail lichen planus more frequently. There is a high frequency of HLA-A3, HLA-A5, HLA-B7, HLA-DR1, and HLA-DR10. The histopathology of nail lichen planus is characteristic. There is a dense epitheliotropic lymphocytic infiltrate around the apical matrix leading to vacuolar basal cell degeneration with thinning of the epithelium and impaired nail substance formation. As this is not evenly distributed over the width of the matrix
16
longitudinal furrows and splits develop. Severe infiltration causes epithelial consumption and, finally, deficient nail formation, obliteration of the nail cul-de-sac, and pterygium.
DIAGNOSIS
Nail lichen planus is usually diagnosed clinically. There are no blood tests. Lichen planus lesions on the skin, oral, and genital mucosa should be looked for. Ultimately, a nail biopsy can confirm the diagnosis. Bullous nail lichen planus may mimic yellow nail syndrome.
DIFFERENTIAL DIAGNOSIS
All nail conditions causing rough nails with longitudinal ridging and surface defects have to be considered. The diagnosis is more obvious with fingernail than toenail lesions. Amyloidosis involving the nails looks very similar.
DISEASE ASSOCIATIONS
These are the same as with cutaneous lichen planus: AA, vitiligo, localized scleroderma, Castleman tumor with pemphigus vulgaris, and chronic liver disease.
1585
16
CLINICAL COURSE, PROGNOSIS, AND MANAGEMENT
Nail lichen planus is particularly chronic and stubbornly resistant to almost all topical treatments. Slight variations in the disease intensity may be observed. Some patients have mild disease with almost no progression whereas others may experience rapid exacerbation with cicatricial nail dystrophy. Once a pterygium has developed, nail lichen planus is no longer amenable to treatment. Furthermore, there may be a Koebner phenomenon when using harsh treatment methods. Despite the lack of controlled studies for topical treatment modalities, the combination of a steroid with calcipotriol is recommended, which may induce some improvement or stop disease progression. Perimatricial injections of triamcinolone acetonide every 4 to 8 weeks, either with or without a needle, are often successful and may be continued by IM injections, 0.5 to 1 mg/kg bodyweight. However, up to 50% of the responders may experience a recurrence.22 Biologics are highly effective in recalcitrant cases.23
AUTOIMMUNE BULLOUS DISEASES
AUTOIMMUNE BULLOUS
DISEASES
AT-A-GLANCE
■ Even though all autoimmune bullous disease can affect the nail unit, the clinical changes are nonspecific and do not permit a conclusive diagnosis.
■ Chronic paronychia, hyperkeratosis, and oozing with crusting are common to all autoimmune bullous diseases.
Among the autoimmune bullous diseases, pemphigus vulgaris, pemphigus vegetans, bullous pemphigoid, cicatricial pemphigoid, and epidermolysis bullosa acquisita may affect the nails. However, nail lesions are rarely specific enough as to allow the exact diagnosis to be made. Associated skin lesions may suggest a blistering disease.
CLINICAL FEATURES
Chronic paronychia with oozing and crust formation are the most common initial signs (Fig. 91-43), followed by onychomadesis (see Fig. 91-23) and sometimes by loss of the nail, of nail involvement. Pterygium formation and permanent nail loss were observed in bullous pemphigoid, cicatricial pemphigoid, and acquired epidermolysis bullosa. Large clear periungual blisters are occasionally seen in bullous pemphigoid. They may be followed by erosions with crusting and sometimes superficial impetiginization. Pemphigus vegetans of
1586
the distal phalanx may resemble a very severe form of acrodermatitis continua suppurativa of Hallopeau with extensive pustulation and often a markedly pronounced pustular margin.
ETIOLOGY AND PATHOGENESIS
They are dealt with in the chapters on autoimmune bullous disorders. It was once thought that nail involvement in pemphigus vulgaris might be a sign of a particularly aggressive course or even a special subtype; however, this has not been substantiated.
DIAGNOSIS
The diagnosis may be suspected in case of a longstanding oozing and crusting paronychia with development of onychomadesis and even nail loss. However, serologic investigations including enzyme-linked immunosorbent assay tests and indirect immunofluorescence, and in case of skin lesions, a biopsy, are usually necessary to make the diagnosis.
DIFFERENTIAL DIAGNOSIS
The various autoimmune bullous diseases require immunoserologic and histopathologic examinations for their differentiation.
DISEASE ASSOCIATIONS
Other autoimmune phenomena and diseases may be associated.
CLINICAL COURSE, PROGNOSIS, AND MANAGEMENT
The course of the nail lesions is linked to that of the cutaneous and mucous membrane lesions. Their efficacious therapy will also control the nail alterations albeit with some delay. Nail lesions take between 6 and 18 months to grow out. Pterygium is permanent.
SO-CALLED CONNECTIVE TISSUE DISEASES
SO-CALLED CONNECTIVE
TISSUE DISEASES
Lupus erythematosus and its particular form of chilblain lupus, dermatomyositis, and scleroderma may affect the nail unit.
CLINICAL FEATURES
All these disorders may cause alterations of the nailfold capillaries. They may be reduced in number, dilated, tortuous, shorter, and show aneurysms and bleeding. This is easily seen when using a fluorescent dye that gives evidence of vessel leakage. However, even though often stressed in the rheumatologic literature, most of these changes do not allow a safe distinction to be made between them. Some changes are more typical for dermatomyositis, which is also characterized by Gottron papules of the dorsal aspect of phalanx, less frequently on the distal phalanx (Fig. 91-44). Periungual erythema and red lunula may be seen in acute lupus erythematosus whereas in chilblain lupus
A
B
16
the changes reach from pernio-like nonspecific violaceous-blue hue with some telangiectasias to ulceration of the tip of the toe and the nail unit. Chronic discoid lupus erythematosus may cause red streaks in the nail bed, ridging of the nail, and dystrophy. White bands were seen in the diffusely brown nail of a black patient who had leukoderma of the head as a result of chronic discoid lupus erythematosus. Onycholysis, pterygium, and clubbing are nonspecific signs.24
Scleroderma with its acral variant often shows ulceration of the pulp and narrowing of the tip of the finger. The nail insidiously bends volarly giving the aspect of a parrot beak. The nail surface is dull and may show pronounced ridging. The plate is often nontransparent.
ETIOLOGY AND PATHOGENESIS
The etiology is that of the cutaneous involvement. Infarctions of the nailfold capillaries may lead to necrosis and scars. The degree of matrix affection determines that of the nail changes. Most sclerodermatous nail alterations are said to be secondary to the associated vascular damage.
DIAGNOSIS
As isolated nail changes in these connective tissue diseases are exceptional, the diagnosis is usually made by their skin lesions and immunoserologically (Fig. 91-45). Capillary alterations are easily seen by dermatoscopy and laser scanning confocal microscopy; the latter also permits the blood flow to be observed.
DIFFERENTIAL DIAGNOSIS
Capillary microscopy of the nailfold may give a hint at the diagnosis of an autoimmune disease; however, despite many claims, it is very difficult to differentiate them purely on capillary microscopy. Nail plate changes may have to be distinguished from lichen planus. Red lunulae are seen in acute AA of the nail and some other diseases, as well as in drug reactions. Periungual erythema may be caused by HIV infection or treatment with cytotoxic agents.
1587
16
DISEASE ASSOCIATIONS
Mixed connective tissue disease exhibits features of lupus erythematosus plus dermatomyositis and sometimes even scleroderma. Other immune disorders may be associated. The association with erythema multiforme is called Rowell syndrome. Vasculitis accompanies systemic lupus erythematosus in 10% to 20% of patients.
CLINICAL COURSE, PROGNOSIS, AND MANAGEMENT
The clinical course, prognosis and management are those of the skin lesions, however, the nail alterations usually take longer to respond.
VASCULITIS AND VASCULOPATHIES
VASCULITIS AND
VASCULOPATHIES
Nail changes of the “true” vasculitides, as well as of occlusive and infectious vasculopathies, are mentioned.
CLINICAL FEATURES
Leukocytoclastic vasculitis may affect the distal phalanx with the nail unit, particularly of the toes. Dark red small palpable spots develop both on the proximal nailfold and the pulp, which have a tendency to leave small necroses and tiny scars. Under the nail, they are seen as dark red spots and may be painful. In “benign” gonococcal sepsis, small hemorrhagic papules may develop on the distal phalanx, involving also the proximal nailfold. Similar lesions were also observed in pneumococcal and meningococcal sepsis; however, these are very serious diseases that are not diagnosed by their nail involvement. Livedoid vasculopathy, also called livedo reticularis, is a typical disorder of the legs that causes painful torpid ulcers. It is often called atrophie blanche when located in the ankle region.25 It may affect the free margin of the proximal nailfold of toes, exhibiting lichenoid papules with reddening and white lines (Fig. 91-46).
ETIOLOGY AND PATHOGENESIS
The etiology and pathogenesis of the vasculitides and vasculopathies are not different from those of the skin lesions. Hypercoagulability in association with stasis are assumed to underlie livedoid vasculopathy. In infectious vasculitides, microbial thrombi are said to be responsible, but a general toxic response has also to be discussed.
DIAGNOSIS
The diagnosis of the nail lesions depends on that of the skin disease.
1588
DIFFERENTIAL DIAGNOSIS
Osler nodules are small painful nodules and bleedings in the fingertips in bacterial endocarditis.
DISEASE ASSOCIATIONS
Vasculitis is often seen in conjunction with systemic lupus erythematosus, but may also occur in a variety of infections and as a drug reaction.
CLINICAL COURSE, PROGNOSIS, AND MANAGEMENT
The clinical course depends on whether or not the cause of the vasculitis is found and removed. Large necrotic lesions heal with scars that may distort the nail.
INFECTIOUS NAIL DISEASES
AT-A-GLANCE
■ Otherwise banal infections are often disproportionately painful, for instance digital herpes simplex.
■ Subungual warts may be very painful because of pressure on the bone; those under the proximal nailfold mimic chronic paronychia.
■ In hand-foot-and-mouth disease, small oval blisters may occur around the nail, and possibly also in the matrix region, causing late onychomadesis.
■ Bullous impetigo presents as a blister with a stable roof that may extend around the nail.
(Continued)
AT-A-GLANCE (Continued)
Continued
AT A GLANCE (
)
■ Deep bacterial infections may reach down to the bone; these whitlows (felons) cause pain and require surgical exploration.
■ Syphilis may occur as a primary chancre, which also may be atypically painful, or as a subungual papular exanthem causing onycholysis.
■ Both tuberculosis, leprosy and atypical mycobacterioses occur in the nail unit and cannot be diagnosed on clinical grounds alone.
■ Fungal nail infections are extremely common. Independent of the pathogen, the clinical types look similar; hence cultural identification is warranted.
■ Leishmaniasis can present as ulcerating paronychia.
■ Nail infestation by Sarcoptes scabiei is very often overlooked as it may mimic psoriasis or acrokeratosis paraneoplastica of Bazex; it is refractory if not treated correctly and often the source of reinfection and small institutional epidemics.
VIRAL INFECTIONS
VIRAL INFECTIONS
A variety of viruses may infect the nail and periungual skin and cause skin lesions that are sometimes different from what is seen on normal skin.
HERPES VIRUS INFECTIONS
The most important Herpesviridae affecting the nail are herpes simplex virus Type 1 (HHV1), Type 2 (HHV2), varicella-zoster virus (HHV3), and HHV8 found in Kaposi sarcoma.
Herpes Simplex of the Nail Apparatus— Clinical Features: The primary herpes simplex infection rarely causes nail lesions although virus inoculation may take place during the disease in fingersucking babies. Recurrent digital herpes simplex is occasionally seen in children, adolescents, and in certain professions, such as dentists (before they started routinely wearing gloves). Small vesicles are seen to develop that first have a clear content, which, after some days, becomes yellowish while the blisters tend to merge (Fig. 91-47). From the beginning, a visible red streak is commonly seen extending from the finger to the arm; this lymphangitis is usually associated with pain. After 7 to 10 days, the tenderness decreases, and the blister content may turn hemorrhagic and finally dry. After 2 to 3 weeks, the blister roof sheds.
Herpes Simplex of the Nail Apparatus— Etiology and Pathogenesis: In children, recurrent digital herpes simplex is usually caused by HHV1 whereas in adults, HHV1 and HHV2 are the
16
A
B
C
causative agents, with each being the cause in approximately 50% of patients.
Herpes Simplex of the Nail Apparatus— Diagnosis: The diagnosis is made clinically by an experienced dermatologist. A classical Tzanck smear is helpful in the early stage. Immunofluorescence
1589
16
with specific HHV antibodies not only confirms the diagnosis but may also distinguish infections caused by HHV1 from those caused by HHV2. Immunohistochemistry with HHV1 and HHV2 antibodies on histologic sections is also positive. Polymerase chain reaction is another option. However, when the lesion is too old, all tests may fail.
Herpes Simplex of the Nail Apparatus— Differential Diagnosis: Acute paronychia, bullous impetigo (runaround), whitlow (felon), and other bacterial infections have to be considered as part of the differential diagnosis. However, the repetitive nature of digital herpes simplex and its painful course are typical.
Herpes Simplex of the Nail Apparatus— Disease Associations: Severe and even ulcerative herpes simplex is seen in immunocompromised individuals.
Herpes Simplex of the Nail Apparatus— Clinical Course, Prognosis, and Management: Recurrent digital herpes simplex is frequently misdiagnosed as an acute paronychia. The patients consult their family physician or a surgeon who treat it as an acute whitlow by opening the blisters, disinfection, antiseptic baths, systemic antibiotics and splinting of the digit. Only after repeated recurrences may the patient be referred to a dermatologist who can make the diagnosis from the clinical course. Recurrences may come in waves: several waves in relatively short intervals that then become longer and finally turn into a herpes-free period for several months or even some years until the recurrences restart. There are no controlled studies proving the value of long-term antiviral prophylaxis.
Varicella and Herpes Zoster: Varicella may involve the nail region with a few characteristic vesicles, and herpes zoster may, although rarely, extend to the distal digits. The diagnosis is made from the skin lesions (Fig. 91-48). However, onychomadesis was observed in children several weeks after chickenpox; it may be assumed that unnoticed viral blisters of the
1590
matrix were the cause. Treatment follows the general rules of HHV3 therapy.
HUMAN PAPILLOMAVIRUS INFECTIONS Clinical Features: Common warts belong to the most frequent infections of humans. On the proximal nailfold, they are round papules with a rough keratotic surface; on the lateral folds they are often oval (Fig. 91-49). Subungual warts have an unspecific appearance often lifting the nail up and they are commonly painful. Under the proximal nailfold they raise it from the underlying nail and cause a marked swelling. At the hyponychium there may just be a rim-like thickening of the keratin that swells after 5 minutes in water.
Etiology and Pathogenesis: Infection with HPV types 1, 2, 3, 4, and 7 is the most common cause for viral warts of the nail unit. It is believed that infectious virus particles get into the epidermis via microwounds; however, how this exactly happens is still not fully understood.
Diagnosis: The diagnosis of viral warts is clinical. Histopathology is characteristic in young warts, but may be very inconspicuous in old ones. Immunohistochemistry with an antibody against a common papillomavirus antigen can be helpful. Serologic studies do not help. Polymerase chain reaction and in situ hybridization help to identify the HPV type.
Differential Diagnosis: The differential diagnosis of ungual warts is extensive and depends also on the localization within the nail unit. Subungual warts, particularly when painful, may be mistaken for a subungual exostosis. Other subungual tumors and inflammatory processes may have to be considered.
Disease Associations: Periungual warts are common in children and adolescents. However, severe immunodeficiency states and iatrogenic immunosuppression may be associated with innumerable warts in many locations.
Clinical Course, Prognosis, and Management: It is said that the average life span of a banal wart is approximately 2 years. However, clinical experience shows that periungual warts—like palmar and plantar ones—often exist much longer and may give rise to new ones during this period. They often grow very fast to a certain size and then remain stable for many months or years. The prognosis is good as the no-risk HPV types do not progress to carcinoma. Management of periungual and subungual warts is difficult. There are surprisingly few randomized controlled studies, but they all show that aggressive keratolysis with salicylic acid is superior to wait-andsee. Salicylic acid plus cryotherapy is more efficacious than cryosurgery alone. Second-line treatments are laser, either ablative with CO2 laser or with nonablative lasers. One regimen using the pulsed-dye laser to coagulate the vessels to the wart has been shown to be efficacious in more than two-thirds of cases. A variety of immune therapies, such as contact allergens and different vaccines, have been used with variable effect. Imiquimod may be tried off-label after aggressive keratolysis; however, the 3-times weekly regimen recommended for condylomata acuminata is not enough for ungual warts. Here, a daily treatment under occlusion is necessary, eliciting a marked inflammatory reaction. Third-line treatments comprise compounded cidofovir as a topical therapy; however, cidofovir is very expensive and therefore rarely used except in cases of an excessively large number of ungual warts.
ENTEROVIRUS INFECTIONS
A variety of different enteroviruses may cause periungual erythema; however, this is not specific enough to allow a particular diagnosis to be made. The most characteristic infection is hand-foot-and-mouth disease.
Clinical Features: Hand-foot-and-mouth disease is a vesicular disease characterized by intraoral aphthoid lesions that cause less discomfort than common aphthous ulcers, with small vesicles on the palms, soles, and around the nails (Fig. 91-50). They are usually oval in shape, the covering epidermis is gray from necrosis, and surrounded by a narrow erythematous rim. In ridged skin, the long axis of the vesicles is along the dermatoglyphics. Mild fever may be present in the beginning. Small outbreaks of this infection typically occur in spring and autumn. Many infections remain virtually asymptomatic and escape notice. After approximately 6 weeks, some patients develop onychomadesis of single nails, probably as a sign of direct matrix involvement.26
Etiology and Pathogenesis: In most cases, the cause of hand-foot-and-mouth disease is an
16
infection with enterovirus Type 71 and Coxsackieviruses, mainly Types A5 and A16, and rarely B or other enteroviruses. The infected cells swell, necrose, form a reticular, and, finally, a multilocular vesicle. After some days, this dries out and leaves a dry scab of necrotic epidermis and serum.
Diagnosis: The characteristic slightly oval vesicles with a gray blister roof and a narrow red margin, together with oral lesions reminiscent of aphthous ulcers, permit the diagnosis to be made. Serology may confirm the serotype.
Differential Diagnosis: As skin vesicles may be scarce the oral mucosal lesions may be mistaken for viral lesions of other enteroviruses, for example, herpangina.
Disease Associations: There are no characteristic disease associations.
Clinical Course, Prognosis, and Management: The clinical course is self-limited. The vesicles usually disappear within 7 to 10 days. The prognosis is good. There is no specific antiviral therapy.
BACTERIAL INFECTIONS
BACTERIAL INFECTIONS
Most bacterial infections are caused by streptococci or staphylococci. Enterobacteria are mainly seen in toes. Clinical variants of impetigo are the most common bacterial infections. Paronychias and whitlows are also seen.
COCCAL INFECTIONS Clinical Features: The most characteristic bacterial infection is a bullous impetigo (Fig. 91-51) that runs around the proximal part of the nail, hence the common term runaround. It starts with a clear blister of the proximal and lateral nailfold that soon becomes putrid and often also hemorrhagic. Pain is usually mild. Extension under the nail is exceptional in adults, but may occur in children and is seen as a yellowish lake of pus under the nail. It is commonly painful.
1591
16
When the infection occurs primarily under the nail it is called a subungual whitlow. It exhibits the features of an abscess. Deep soft-tissue infections cause considerable pain and are usually treated by surgeons with incisions and pus evacuation.
Etiology and Pathogenesis: Most of these infections are caused by staphylococci, rarely by streptococci. Subungual P. aeruginosa infections are rare. Small lacerations often from hangnails and other minor wounds are the portal of entry.
Diagnosis: The course of the infections is sufficiently characteristic to make the correct diagnosis. Bacterial swabs may confirm the infection.
Differential Diagnosis: The main differential diagnosis is recurrent digital herpes simplex, which is more painful, develops a lymphangitis, and starts with a group of small clear blisters that coalesce and later becomes putrid.
Disease Associations: There are no specific disease associations.
Clinical Course, Prognosis, and Management: When treated early the lesions disappear within 1 to 2 weeks. The prognosis of most cases is excellent. Uncomplicated bullous impetigo of the nail is treated with opening of the blister, disinfective baths twice a day, and antimicrobial creams. However, extension under the nail, particularly in children, should immediately prompt institution of systemic Staphylococcus-fast antibiotics that may be changed according to the sensitivity profile of the bacteria cultured from a swab. This is essential as the matrix in
1592
children may be permanently damaged within 24 to 48 hours in a subungual whitlow.
PSEUDOMONAS INFECTION Clinical Features: P. aeruginosa is a ubiquitous pathogen quite frequently seen in the nail apparatus. Most cases are colonizations causing a green to brownish-black nail and often a localized marginal paronychia as evidenced by circumscribed swelling and loss of the cuticle (Fig. 91-52). Deep infections are rare in immunocompetent subjects.
Etiology and Pathogenesis: The dorsal and ventral surfaces of the nails may be severely colonized by P. aeruginosa, which can form a bacterial biofilm.
Diagnosis: The greenish color of the nail is very characteristic so that bacterial cultures are usually not needed to make the diagnosis. The color can be scraped off in most cases, but soon returns if the bacteria are not addressed.
Differential Diagnosis: Both exogenous and other enterobacteria causing a grayish discoloration, particularly Klebsiella spp. and Proteus spp., may have to be considered.
Disease Associations: It appears that coinfection with yeasts and/or dermatophytes makes the nails more susceptible to Pseudomonas colonization.
Clinical Course, Prognosis, and Management: The clinical course is chronic with insidious aggravation. The prognosis for the immunocompetent is very good. However, these individuals should not work as doctors or nurses in newborn, cancer, or gnotobiotic units, or as scrub nurses in the surgical theater as they can spread their infection. It is also advisable that they do not work in the food industry, in bakeries, butcheries, or other professions with direct contact with foods, such as chefs. The management is usually not complicated. Baths with diluted white vinegar 2 or 3 times a day for 5 to 10 minutes, then brushing the digits dry, are often sufficient. This may be completed with a topical antimicrobial drug or
disinfective. Topical antibiotics like gentamycin may be used in addition. Systemic antibiotics are not the first choice for 2 reasons: (a) the bacterial biofilm is approximately 1000 times less sensitive to antibiotics than isolated bacteria of the same species, and (b) the green nail is almost always onycholytic, thus not in contact with the nail bed so that the antibiotic cannot reach the biofilm. Ciprofloxacin, levofloxacin, and polymyxin B show the highest activity against Pseudomonas, followed by gentamicin and ofloxacin, whereas the bactericidal antibiotic cefuroxime and the bacteriostatic antibiotic chloramphenicol are less active.
FUNGAL INFECTIONS
FUNGAL INFECTIONS
The nail apparatus is an extremely frequent site of infection for a great variety of different fungi. They may cause various acute, subacute and chronic infections. Fungal infections may be classified according to their pathogens into dermatophyte, yeast, and nondermatophyte mold infections, according to their time course (acute, subacute, subchronic, chronic), and, above all, according to their mechanism of infection (Table 91-6). Onychomycoses affect toenails 7 to 10 times more frequently than they affect fingernails, which is thought to be attributable to the 3 times faster growth of fingernails as compared to toenails.
CLINICAL FEATURES
Onychomycoses are often seen as the most frequent nail disorders making up approximately 40% to 50% of all nail diseases. The vast majority are distal or distal–lateral subungual onychomycoses (Fig. 91-53). In the beginning, there is a distal subungual keratosis with an irregular border toward the nail bed. This slowly and insidiously progresses proximally while the nail may become discolored, nontransparent, and break distally. After some months or years, there is often no more progression but
Onychomycoses According to Pathogens
■Dermatophytes
■Yeasts
■Nondermatophyte molds
Onychomycosis According to the Entry of the Fungi
■Distal and distal–lateral subungual onychomycosis
■Proximal white subungual onychomycosis: with/without paronychia
■Superficial white/black onychomycosis: superficial form, deep form
■Endonyx onychomycosis
■Total dystrophic onychomycosis: secondary to any of the above forms, primary in chronic mucocutaneous candidiasis
Most Important Differential Diagnoses
Most Important Differential Diagnoses
■Nail psoriasis, asymmetric gait nail unit syndrome, chronic nail dystrophy in the elderly, in chronic venous insufficiency, in impaired arterial circulation, ungual lichen planus, eczema
■Nail psoriasis, asymmetric gait nail unit syndrome, chronic nail dys-
trophy in the elderly, in chronic venous insufficiency, in impaired arterial circulation, ungual lichen planus, eczema
16
the subungual hyperkeratosis may continue to thicken. Often, there is a mild and inconspicuous desquamation around the nail or even an obvious tinea pedis is observed. Sometimes, a yellow streak develops that is formed like a narrow wedge in proximal direction. The lateral edge of the nail is frequently onycholytic. Superficial white onychomycosis is a condition mostly seen on the toenails as chalky-white patches with no shine of the nail surface (Fig. 91-54). When
1593
16
occurring on fingernails, the white discoloration is inhomogeneous and more cloudy, but the nail surface remains shiny; this is the typical form of HIV infections (Fig. 91-55). Proximal subungual onychomycosis is also rare. Clinically, it is seen as a white to yellowish discoloration of the nail that grows out from under the proximal nailfold (Fig. 91-56). The plate may be onycholytic under the whitish area. Repeated arched white lines are seen as recurrences from an internal focus. Endonyx onychomycosis is a rare form in which the fungus only grows in the nail plate without affecting the subungual tissue. The nail is nontransparent, discolored, and dermatoscopy may show air-filled channels in the nail plate. All these different onychomycoses may lead to total dystrophic onychomycosis where the nail is substituted by irregular keratotic debris full of fungi. Primary total dystrophic onychomycosis is characteristic for chronic mucocutaneous candidiasis (Fig. 91-57), which represents a group of immune defects with impaired defense against Candida albicans. Chronic oral lesions, involvement of the scalp and other regions, and granulomatous lesions coexist.
1594
ETIOLOGY AND PATHOGENESIS
The most common causes of onychomycoses are dermatophytes, particularly Trichophyton rubrum, Trichophyton mentagrophytes var interdigitale, much more rarely Epidermophyton floccosum, Trichophyton violaceum, and Trichophyton soudanense. In warm climates, C. albicans can cause a clinically identical nail infection as it has enzymes that also degrade keratin. Other yeasts may be found, but their pathogenic role is often not clear. Nondermatophyte molds were mainly seen in tropical climates but are now emerging pathogens in Central Europe. The pathogenesis is characteristic for each of the onychomycosis forms described. The pathogenic fungus grows from the tip of the digit through the hyponychium toward the nail bed in distal–lateral subungual onychomycosis. The nail bed reacts with a hyperkeratosis that harbors the vast majority of the fungi, whereas the overlying nail plate is a barrier for the fungi rather than their site of infection. When the fungus advances proximally, an inflammatory infiltrate develops in the nail bed and epithelium with accumulations of neutrophils very similar to Munro microabscesses; however, there is much less parakeratosis in onychomycosis. Often, a yellow streak or narrow wedge is seen under the nail extending from the distal nail bed proximally. Here, huge amounts of compressed, mostly very thickwalled fungi are seen; this phenomenon is called dermatophytoma. In proximal subungual (white) onychomycosis, the fungus infects first the undersurface of the proximal nailfold via the cuticle and grows toward the matrix. When this is reached, the fungi are included into the newly formed nail substance and can be found in all layers of the nail plate. Superficial white onychomycosis is a rare form of infection of the dorsal surface of the nail plate. In temperate climates, it is mainly caused by T. mentagrophytes. Histologically, chains of small spores and, rarely, short slender hyphae are seen on the nail. When this infection extends under the proximal nailfold it may invade deeper layers of the nail plate. In HIV patients, fungi are seen directly under
the surface, showing both spores and short hyphae; they are commonly T. rubrum. Endonyx onychomycosis is a rare infection, mainly caused by T. soudanense or T. violaceum that are exclusively found within the nail plate. All these forms may progress to total dystrophic onychomycosis, although in a variable frequency. The nail is completely destroyed and substituted by irregular keratotic debris. The nail bed and matrix often show papillomatosis and acanthosis. Rarely, this is found as an acute infection.
DIAGNOSIS
Although most onychomycoses can be diagnosed clinically they should be confirmed by direct microscopy, after clearing of the subungual keratotic debris with 10% to 20% potassium hydroxide, culture, and histopathology. The rate of false-negative results, particularly for cultures, is very high, commonly between 30% and 60%, but histopathology has proved to be doubly sensitive. Furthermore, it can distinguish between colonization and true infection; however, species identification is not possible. Modern methods to confirm a fungal infection comprise polymerase chain reaction and matrix-assisted laser desorption/ionization–timeof-flight spectroscopy. These methods are expensive and require reference DNA and proteins, respectively.
DIFFERENTIAL DIAGNOSIS
Onychomycosis make up approximately 40% to 60% of all nail diseases. Consequently, it is frequently diagnosed without laboratory proof, risking that roughly 50% of the diagnoses are not correct. The most important differential diagnosis is nail psoriasis. Both are frequent, may involve the nails only, cause discoloration, loss of nail transparency, brittle nails, and subungual hyperkeratosis; however, the most frequent sign of nail psoriasis, the pits, are rare in onychomycoses. Onycholysis in psoriasis often has a brownish-reddish proximal margin corresponding to the salmon spot, which is not seen in onychomycosis. Dermatoscopy of this margin exhibits a proximal border that is irregularly serrated and was called the “aurora borealis” sign. Histologically, subungual hyperkeratosis and neutrophil accumulations in the subungual hyperkeratosis are seen in both conditions and called Munro microabscesses; in psoriasis, there is more parakeratosis around them, which is mostly arranged as obliquely ascending columns. The “asymmetric gait nail unit syndrome” is a condition of toenails,27 in which onycholysis usually affects 1 corner of the big toenail. It is a result of orthopedic abnormalities leading to rubbing and pressure against shoes. It is very often confounded with onychomycosis, but regularly negative for fungi in all laboratory tests. Additional important differential diagnoses are nail lichen planus, nail eczema, trachyonychia, pityriasis rubra pilaris, nail changes in cutaneous lymphomas, and, above all, nonspecific nail dystrophy in the elderly, persons with chronic venous and lymphatic
16
stasis, peripheral neuropathy, impaired arterial blood supply, and repeated trauma in sportsmen like soccer players, particularly when the big toenails are involved.
DISEASE ASSOCIATIONS
Onychomycoses are usually associated with tinea of the hand and/or feet. They are more frequent in patients with nail psoriasis. Particularly severe and fast progressing onychomycoses are observed in immunosuppression. Peripheral neuropathy, arterial and venous insufficiency, and traumatically damaged nails are risk factors for onychomycoses and hence often associated. Onychomycoses are more frequently seen in diabetic patients. In the two-feet-one-hand syndrome, the tinea of both soles and 1 palm is very often accompanied by onychomycosis, most frequently T. rubrum. It is thought that scratching habits are the cause of the unilateral hand involvement.28
CLINICAL COURSE, PROGNOSIS, AND MANAGEMENT
Most onychomycoses run a chronic protracted course. For unknown reasons, they may stop progressing after years and remain virtually unchanged for decades if not treated. The prognosis as to the nail destruction is good in more than 90% of patients, and complete recovery, even after severe total dystrophic onychomycosis, is possible. In contrast to this, the management of most onychomycoses is still challenging. Any associated fungal skin infection has to be treated. Hygienic measures, such as regular disinfection of shoes and socks, wearing open shoes whenever possible, changing the footwear daily, and washing socks at 60°C (140°F) are of paramount importance. Infected nail material and subungual keratosis should be removed as much as possible. This can be accomplished with a nail clipper and later with the application of 40% urea paste under occlusion for 3 to 5 days. This softens the infected keratin and allows it to be scraped off atraumatically. Usually, this procedure has to be repeated 2 or 3 times. Surgical nail avulsion should be abandoned as it represents a severe iatrogenic trauma to the nail apparatus, rendering it more susceptible to fungal infection. In cases of less than 50% involvement of the nail or when the matrix is not affected, topical treatment with 8% ciclopirox lacquer (Penlac), 10% efinaconazole (Jublia) and 5% tavaborole (Kerydin) solution or 5% amorolfine (Loceryl, not marketed in the United States) follows for many months, including some months beyond clinically visible clearing. However, even the new antifungal drugs have complete cure rates lower than 20%. When more than 50% of the nail is affected or the infection reaches the matrix at any point, systemic treatment is indicated. Dermatophytes respond best to terbinafine (Lamisil) 250 mg daily, whereas yeasts and some nondermatophyte molds are better treated with itraconazole 400 mg/day for 1 week
1595
16
TREATMENT MODALITY INDICATION MYCOLOGIC CURE COMPLETE CURE
Ciclopirox 8% lacquer Trichophyton rubrum onychomycosis 29%, 36% 6%, 9%
Efinaconazole 5% solution Dermatophyte onychomycosis 55%, 53% 18%, 15%
Tavaborole 8% solution Dermatophyte onychomycosis 31%, 36% 7%, 9%
Itraconazole Dermatophyte onychomycosis 63%, 66% 22%, 22%
Terbinafine Dermatophyte onychomycosis 60% 46%, 44%
Neodymium:yttrium-aluminum-garnet (Nd:YAG) laser Temporary increase in clear nail 11% –
Neodymium:yttrium-aluminum-garnet (Nd:YAG) laser Temporary increase in clear nail 11% –
Compiled from Gupta AK, Versteeg SG, Shear NH. Onychomycosis in the 21st century: an update on diagnosis, epidemiology, and treatment. J Cutan Med Surg. 2017;21:525-39.
every 4 weeks. This pulse therapy has been shown to be at least as efficacious as continuous itraconazole 200 mg/day. Fluconazole was given once at 150 mg per week, but this dose appears to be too low for individuals weighing more than 70 kg (154 lbs). Controlled trials have shown that the combination of topical plus systemic treatment can reduce the failure rate of systemic therapy alone by 50%.29 Nevertheless, even combined treatments have cure rates not better than 70% to 75%. Results of combined treatment with systemic and the new antifungals are not yet available. Lasers were approved by the U.S. Food and Drug Administration for the temporary increase in clear nail. Their mycologic cure rate was 11% with no complete cure rates given. Photodynamic treatment of onychomycoses is still in an experimental phase (Table 91-7). Recurrences are very frequent. The reasons may be the persisting risk factors including the hereditary susceptibility to fungal nail infection and the potential to reinfect in the own household and public sports facilities.
NAILS IN GENERAL DISEASE
Nail alterations in systemic diseases usually affect all digits but they may vary in intensity according to the growth characteristics of the individual nails.
CARDIOVASCULAR AND PULMONARY DISEASES
CARDIOVASCULAR AND
PULMONARY DISEASES
Clubbing is a characteristic sign of chronic hypoxemia and thus frequently indicates a cor pulmonale. The finger tips and often also the toe tips are enlarged, giving the look of a drumstick. The nail size is increased and both the longitudinal and transverse curvatures are more pronounced so that the nail is round like a watch glass (Fig. 91-58). Quite often, the lunula is very big. Nail bed and lunula are cyanotic. The angle between
1596
the proximal nailfold and the nail plate (angle of Lovibond) is greater than 180 degrees. When the 2 opposite fingers are held together, there is a narrow lozenge space between the proximal nail areas in normal persons whereas this diamond-shaped window is absent in clubbed nails, and the angle between the free nail margins is greater than 30 degrees (Schamroth sign). In addition, many other conditions are associated with clubbing (Table 91-8). Unilateral clubbing may hint at arterial insufficiency of this extremity. The cause of clubbing is still not known, but the prevailing hypothesis is that megakaryocytes are incompletely degraded to normal-size platelets in the lungs and may strand in the capillary network of the digits where they disintegrate and release their various growth factors. Splinter hemorrhages were once seen as an indicator of bacterial endocarditis. However, there is a plethora of other associations. Yellow nail syndrome (YNS) is a characteristic triad of signs: yellow, thick, extremely slow-growing nails with onycholysis, often also spontaneous nail loss and complete disappearance of the cuticle (Fig. 91-59), chronic sinus-bronchopulmonary infection and edema of the distal extremities. Chronic GI diseases and a variety of internal cancers also have been observed in association with the yellow nail syndrome.
Cardiovascular
■Cor pulmonale
■Cardiac insufficiency
■Open foramen ovale, Eisenmenger complex
■Aortic aneurysm
Bronchopulmonary
■Chronic obstructive and suppurative pulmonary diseases
■Intrathoracic tumors
■Hypertrophic pulmonary osteoarthropathy
Gastrointestinal
■Hepatic disorders
■Inflammatory bowel diseases
■Polyposis intestini
■GI neoplasms
■Bacillary and amebic dysentery
Blood Dyscrasias
Blood Dyscrasias
■Chronic methemoglobinemia (eg, in heavy smokers)
■Chronic methemoglobinemia (eg, in heavy smokers)
INTESTINAL AND HEPATIC DISEASES
INTESTINAL AND HEPATIC
DISEASES
Most nail changes seen in malnutrition, anorexia nervosa, bulimia, or kwashiorkor are nonspecific: the nails may be thin, brittle, and have lost their shine. In acrodermatitis enteropathica and acquired zinc deficiency there are often periungual erosions with crusting, the nail edges may break through the epidermis of the nail grooves and cause granulation tissue (Fig. 91-60). Very similar lesions are seen in glucagonoma dermatitis. In severe liver disease, the nails may turn white and opaque. In Terry nails, a distal normal-colored band remains. Muehrcke lines are 2 parallel white bands in the middle of the nail bed that do not move out and are seen in severe hypoalbuminemia. The nails may turn bluish in Wilson disease.
16
UROGENITAL DISEASES
UROGENITAL DISEASES
So-called half-and-half nails are seen in chronic renal insufficiency and under long-term hemodialysis. The proximal half of the nail is whitish, the distal half tends to be brownish (Fig. 91-61).
AMYLOIDOSIS
AMYLOIDOSIS
Systemic amyloidosis may have profound effects on the cutaneous appendages including the nails. They insidiously become thinner, fragile, ridged, and lose their shine, resembling late ungual lichen planus (Fig. 91-62). Subungual hemorrhage may occur.
1597
16
PSYCHOLOGICAL DISORDERS
PSYCHOLOGICAL
DISORDERS
A number of autoaggressive nail conditions are known that are commonly described as psychological disorders. Some are extremely frequent, such as chewing of the nails (onychophagia), picking of the periungual skin (perionychotillomania) and habitual pushing back of the cuticle and pressing on the lunula with another fingernail. Onychophagia is frequent in children, but it often lasts into adulthood (Fig. 91-63). Perionychotillomania is more a condition of adults who continuously pull off hangnails and other tiny skin tags. This habit tic results in a central depression of the nail with a washboard aspect, an unusually long lunula and loss of the cuticle (Fig. 91-64). This must not be confused with the Heller’s median canaliform dystrophy of the thumb nails, which is characterized by a median split in the nail plate that starts in the proximal portion, extends distally, and typically shows oblique furrows running proximally on both sides, thus giving the aspect of a Christmas tree (Fig. 91-65). Trauma is also the main cause. More-severe autoaggressive behaviors are onychoteiromania where the nails are virtually rubbed away, onychotillomania where the nail is pulled out in pieces (Fig. 91-66), and onychotemnomania where a cutting device is used to remove all the nail. Onychodaknomania is a frankly psychotic behavior; the patients bite on their nails in the lunula or proximal nail bed region to produce pain. Many of these patients have a deprivation syndrome.30 All these behavioral abnormalities are difficult to treat. Psychological support may be necessary. N-acetyl cysteine in a dose of 1800 to 2400 mg/day has been successfully used in a number of obsessive-compulsive disorders, including autoaggressive nail conditions. Nail chewing may spread periungual warts and lead to melanocyte activation with the development of brown streaks in the nails.
1598
INTOXICATIONS
INTOXICATIONS
High doses of arsenic cause transverse white nail discoloration. The high arsenic content is important for medicolegal reasons. Cadmium and other heavy metals, as well as many drugs, can be recovered from nails many months after their intake. Toxic doses of vitamin A are destructive of the nail.
DRUG REACTIONS
Some drugs cause characteristic, although rarely specific, nail alterations (Table 91-9). They are most often observed under the treatment with cytostatic drugs. They may cause white lines, Beau lines, or onychomadesis, with the white lines being the least-severe and onychomadesis being the most-severe form of a similar reaction pattern, namely, growth retardation. Brown nail pigmentation may occur and represents an activation of matrix melanocytes. Taxanes cause painful subungual hemorrhagic abscesses that may require withdrawal of the drug. The use of frozen gloves and socks may partially prevent these adverse effects. Targeted anticancer therapies, particularly with epidermal growth factor receptor inhibitors and multiple kinase inhibitors, render the skin very fragile, leading the nail edge to break through and cause granulation tissue that looks similar to pyogenic granulomas.
This phenomenon is also seen under therapy with indinavir, a reverse transcriptase inhibitor, and retinoids. Retinoids are also associated with fragile nails and paronychia. Beta-blockers induce acral ischemia. Bleomycin may also lead to digital ischemia, and permanent nail loss was repeatedly seen after bleomycin treatment of periungual warts. Photochemotherapy with psoralens and ultraviolet A can induce multiple longitudinal brown streaks in several nails. Photoonycholysis is rarely seen during administration of some tetracyclines and fluoroquinolones, as it is painful,
16
may be hemorrhagic, and occurs in the central nail bed of 1 or more nails. Its pathomechanism remains dubious as the nail plate absorbs almost all ultraviolet B and more than 95% of ultraviolet A light, and the skin is often not affected. Acyclovir does induce longitudinal melanonychias.
GENODERMATOSES AFFECTING THE NAIL
Nail involvement in hereditary and congenital disorders is very frequent. Some are highly specific and characterize the genodermatosis, others are frequently seen, many may accompany other severe diseases.
PACHYONYCHIA CONGENITA
PACHYONYCHIA
CONGENITA
Pachyonychia congenita is a group of 5 molecular biologically well-defined diseases of cytokeratins KRT6a, KRT6b, KRT6c, KRT16, and KRT17. Its traditional
1599
16
Cytostatic and Targeted Therapies
■White lines
■Beau lines
■Onychomadesis
■Muehrcke lines
■Hemorrhagic onycholysis and subungual abscesses
■Melanonychia
■Granulation tissue
Bleomycin
■Permanent nail loss
Reverse Transcriptase Inhibitors
■Granulation tissue
Acyclovir
■Melanonychia
a-Blockers
■Digital ischemia
■Lichenoid-psoriasiform changes
Retinoids and High-Dose Vitamin A
■Brittle nails
■Paronychia
■Granulation tissue
Photochemotherapy with Psoralens and Ultraviolet A
Photochemotherapy with Psoralens and Ultraviolet A
■Melanonychia
■Melanonychia
■Photoonycholysis
■Photoonycholysis
classification into Type 1 Jadassohn-Lewandowsky syndrome and Type 2 Jackson-Lawler syndrome has now been abandoned as there were too many overlaps. Clinically, pachyonychia congenita shows painful callus-like palmar and plantar hyperkeratoses, monstrous thickening of the subungual hyperkeratosis that is covered by a horseshoe-like nail usually of normal thickness (Fig. 91-67), oral leukokeratosis with no potential for malignant degeneration, natal teeth, and vellus hair cysts. These cysts are mainly seen in KRT17 and KRT6a mutations. Nail changes occur in more than 80% of the patients and develop during infancy. Whether a late-onset pachyonychia congenita exists is not yet clear. Virtually all nails are affected. They are dark, appear thick (although this is the subungual keratosis), and the nail itself is overcurved and difficult to trim.
1600
ECTODERMAL DYSPLASIAS
ECTODERMAL DYSPLASIAS
By definition, any hereditary disorder involving at least 2 of the cutaneous adnexa—hair, nails, sweat glands, and teeth—are ectodermal dysplasias. Roughly 30 of the more than 200 ectodermal dysplasias are now molecular biologically defined. For clinical convenience, the ectodermal dysplasias are subdivided into hidrotic and hypohidrotic ectodermal dysplasias. The most frequent ectodermal dysplasias are characterized by hair and nail involvement with normal sweat gland function and normal teeth, particularly the Clouston type, with dysplastic nails that often exhibit distally increasing plications, and are short, thickened, or brittle (Fig. 91-68). Three types of hypohidrotic ectodermal dysplasias are known, autosomal recessive, X-linked recessive, and autosomal dominant. Clinically, they
present with hypoplastic nails, hypodontia, hypotrichosis, and inability to sweat adequately, which renders the babies at risk for hyperthermia when they are kept too warm. Frontal bossing and the characteristic midface hypoplasia give the affected individuals a very similar appearance, even when they belong to different races.
BULLOUS EPIDERMOLYSIS GROUP
BULLOUS EPIDERMOLYSIS
GROUP
There are 3 distinct, large groups of hereditary bullous epidermolyses: simplex, junctional, and dystrophic. Nail lesions in the simplex types are rare, but are quite common in the course of the junctional and dystrophic bullous epidermolyses. Anonychia is the consequence of repeated blistering of the nail organ and leaves smooth digit tips covered with a shiny epidermis. One dystrophic epidermolysis bullosa is characterized by predominant nail lesions and hence called the nail type (Fig. 91-69). It may be identical with epidermolysis bullosa pruriginosa and pretibial epidermolysis bullosa. The big toenails are dystrophic and thickened; later the other toenails may follow. A pretibial reticular
16
hyperkeratosis with tendency to develop blisters, and often itch, may be seen.
NAIL-PATELLA SYNDROME
NAIL-PATELLA SYNDROME
Nail-patella syndrome is caused by a mutation in the homeobox gene LMXB1, which is necessary for the anterior–posterior orientation during organogenesis. In nail-patella syndrome, nail involvement is characterized by hypoplasia, which is more marked on the thumbs, decreasing toward the fifth digit, and on the medial side of the nail. The lunula exhibits a triangular shape. The patella is hypoplastic or may be absent. Radiographs often show iliac horns. There may be eye involvement and a severe membranous glomerulopathy with protein loss.
DYSKERATOSIS CONGENITA
DYSKERATOSIS CONGENITA
Dyskeratosis congenita is characterized by pigmentary abnormalities of the skin, nail dystrophy, oral leukoplakias with a tendency to malignant degeneration and severe immune deficiency that is similar, but not identical, to Fanconi anemia.
DISEASES OF CORNIFICATION
DISEASES OF
CORNIFICATION
The group of ichthyoses is now called mendelian disorders of cornification. Nail changes are rare and not specific, such as rough nails and loss of surface shine. Severe subungual hyperkeratoses similar to those of pachyonychia congenita were observed in a case of epidermolytic palmar plantar keratosis; however, the affected nail also exhibited a fungal infection, which might have triggered the hyperkeratosis (Fig. 91-70).
1601
16
CONGENITAL MALALIGNMENT OF THE BIG TOENAIL
CONGENITAL
MALALIGNMENT OF
THE BIG TOENAIL
Congenital malalignment of the hallux nail, first described as congenital nail dystrophy, is a fairly common condition. The child may be born with normal nails and develop the condition later, or the nails may be abnormal at birth. Apparently, the disorder can also appear later in life, precipitated by a trauma in an individual with lateral deviation of the distal phalanx of the hallux. Sometimes only one side is affected. Identical twins may have identical unilateral involvement. In classical cases, the affected nail is triangular, thickened, oyster shell–like, discolored, and onycholytic. There is a false distal nailfold and a considerably shortened nail bed (Fig. 91-71). The degree of onycholysis and nail bed shrinkage determine the chances of spontaneous resolution and also of any type of treatment. If resolution has not started by the age of 2 years, it will likely not
1602
occur. Symptoms are rare and the children are often only presented to the dermatologist around puberty when the ugly nails are seen as an esthetic problem. Systematic radiographic examinations in more than 40 of our patients have shown that there is virtually always a lateral deviation of the distal phalanx called hallux valgus interphalangeus, a lateral deviation of the proximal great toe phalanx leading to classical hallux valgus, and a medial deviation of the first metatarsal bone because of an oblique distal surface of the first cuneiform bone. This forms an arch of the first ray, which self-perpetuates as a result of the action of the flexor and extensor hallux tendons. Early treatment by taping of this orthopedic abnormality is beneficial in those cases where the nail bed shrinkage, onycholysis, and distal nailfold are not too pronounced.
NAIL TUMORS
Tumors of the nail apparatus may originate from all tissue components present in the distal phalanx. Hence, more than 130 different tumors and tumor-like lesions under and around the nail unit have been described. Most of them are rare and their clinical appearance is often not pathognomonic. Analogous to the hair follicle, a few tumors are nail-specific, but these neoplasms have only been described since 30 years. Tumors of the nail unit exhibit certain growth patterns that allow some of their components to be diagnosed. Tumors in the proximal nailfold exert pressure on the matrix, resulting in a furrow in the nail plate. Lesions under the matrix may cause bulging with increased curvature of one half of the nail. Nail bed neoplasms may cause onycholysis and elevation of the nail plate from the bed. Slow-growing benign tumors usually alter the nail shape, whereas fast-growing tumors may destroy the nail.
BENIGN NAIL TUMORS
BENIGN NAIL TUMORS
Only the most important nail tumors are dealt with here.
EPITHELIAL AND FIBROEPITHELIAL TUMORS Onychocytic Matricoma: First described under the name subungual seborrheic keratosis, this name has now been abandoned in favor of onychocytic matricoma.31 Clinically, there is a longitudinal brownish to dirty-yellow lesion under the nail that shines through the plate. Looking under the free margin of the nail reveals a thickening of keratotic material (Fig. 91-72). Surgical removal demonstrates an acanthoma histologically made up of mainly basaloid cells. Round keratin inclusions are similar to squamous eddies but their keratinization mode is via a keratogenous zone like normal nail formation.
Onychomatricoma: More than 200 cases of onychomatricoma have been reported since its first description in 1992.32 It is a fibroepithelial neoplasm originating from the matrix. The nail is thickened, funnel-shaped, yellow, striated, and may show splinter hemorrhages (Fig. 91-73). At the free end of the plate, small holes can be recognized. Dermatoscopy shows that the tunnels contain capillaries that may run a long distance distally in the nail; in rare cases they remain patent, and may cause bleeding upon nail trimming. This clinical appearance is caused by a densely cellular fibrous stroma with long filiform projections that are all covered with normal matrix epithelium extending into the nail. Thus the surface of nail-producing matrix is massively enlarged causing the nail thickening. Variants of this tumor are myxoid onychomatricoma and pigmented onychomatricoma, with pigmented onychomatricoma being an important differential diagnosis of subungual melanoma.
16
Onychopapilloma: This is another recently described nail-specific tumor that arises from the distal matrix and produces a thread of abnormal keratin. Clinically, it is seen as a whitish, ivory-colored, yellowish, reddish, or light-brown band of 4 to 8 mm in width in the nail, similar to onychocytic matricoma (Fig. 91-74). End-on dermatoscopy of the nail shows, however, a circumscribed thinning of the nail plate over the keratotic distal end of the onychopapilloma. Often, the nail tends to break here and a V-shaped onycholysis develops in the distal nail bed. Treatment is by tangential excision of the entire lesion from the hyponychium to the mid-matrix.33
Subungual Filamentous Tumor: Subungual filamentous tumor is clinically seen as a whitish to yellowish line of 1 to 2 mm that does not widen with time. The nail may show a short longitudinal fissure at its free margin. A tiny round keratotic tip is seen under the nail. Its relation to onychopapilloma is not clear.
Ungual Fibrokeratoma: Fibrokeratomas of the nail unit are quite common. They are sausage-like lesions with a keratotic tip. Most arise from under the proximal nailfold and remain lying on it causing a longitudinal groove (Fig. 91-75). When a fibrokeratoma originates from the mid-matrix, it grows within the nail
1603
16
plate until the overlying nail lamella breaks away and a sharply delimited groove remains. Subungual fibrokeratomas arise from the most distal matrix or nail bed and cause a ridge. Multiple ungual fibrokeratomas, so-called Koenen tumors, are a sign of the tuberous sclerosis complex and occur in approximately 50% of these patients after the age of 12 years. Treatment is by incision around the tumor down to the bone and extirpation.
Myxoid Pseudocysts: These lesions are very common pseudotumors of middle-aged and elderly individuals and were known as “dorsal finger cysts.” Most occur in the proximal nailfold of the fingers, rarely on toes, where they exert pressure on the underlying matrix, resulting in a regular longitudinal groove (Fig. 91-76). When the lesion drains into the nail pocket the groove is very irregular, mirroring the periods of increased and released pressure. Subungual localization is rare and often seen as a violaceous lesion on one side of the matrix associated with hemi-overcurvature. Women are more frequently affected. Degenerative distal interphalangeal osteoarthritis with Heberden nodes is usually seen. Treatments vary from repeated punctures and expression of the viscous gelatinous mucin, to injection of steroids or sclerosants, infrared or laser coagulation, cryotherapy, and surgery. The recurrence rate is high except for the technique with intraarticular injection of methylene blue to visualize a potential connecting stalk to the joint, ligation of it, and meticulous extirpation of the myxoid material.
1604
Glomus Tumor: Although rare, this is the bestknown nail tumor because of its highly characteristic symptoms. Patients usually present with the complaint of an extremely painful digit tip. Clinical examination reveals a violaceous red spot under the nail of a finger, from which a reddish line may sometimes extend distally (Fig. 91-77). The slightest shock and cold precipitate the pain that radiates into the arm. Probing allows to exactly locate the tumor, but variable high-frequency ultrasound and magnetic resonance tomography may sometimes be needed. Treatment is by meticulous enucleation of the tumor and repair of the matrix and nail bed.
Subungual Exostosis and Subungual Osteochondroma: Both lesions are often seen as being the same condition and are confounded, although there are important differences. Osteochondromas arise from the epiphysis region of the distal phalanx and have a hyaline cartilage cap, whereas subungual exostoses originate from the corona unguicularis, are thus more distal, and have a fibrous cap. The nail plate is lifted up by a stone-hard nodule that, in case of exostosis, has a characteristic collarette-like margin representing the former border of the hyponychium (Fig. 91-78). Most subungual exostoses occur in children and young adults, commonly the big toe. Trauma was thought to be the cause. The recent finding of a chromosome translocation suggests a true tumor nature; however, it is not clear whether the examined lesions were exostoses or osteochondromas. A radiograph confirms the diagnosis and helps to preoperatively estimate the extent of surgery.
MALIGNANT NAIL TUMORS
MALIGNANT NAIL TUMORS
SQUAMOUS CELL CARCINOMA
Squamous cell carcinoma is the most frequent malignant neoplasm of the nail. Its in situ form is Bowen disease. Most commonly seen around fingernails, Bowen disease may clinically resemble a flat agglomeration of warts (Fig. 91-79). Paronychia may be associated. Melanonychia is a feature in dark-skinned persons and association with HPV56. Other high-risk HPV are HPV16, HPV18, and HPV35, but many more were found, hinting at a possible genitodigital transmission. Bowen disease is slowly and insidiously growing and may result in large irregular periungual areas of velvety, red and scaling skin. Extension under the nail to the nail bed and matrix are common, and leukonychia is characteristic for matrix involvement. Ulceration and crust formation indicate invasive growth (Fig. 91-80), which is, however, a late event. Bone invasion and metastases are rare in the Bowen type of squamous cell carcinoma, but occur in the common squamous cell carcinoma type.
16
Treatment of choice is Mohs surgery, but amputation is required in case of bone invasion.
OTHER MALIGNANT NAIL TUMORS
Basal cell carcinoma is exceedingly rare in the nail unit. Onycholemmal carcinoma is a very slow-growing subungual tumor that clinically presents as a longstanding oozing mass. The diagnosis is made by histopathology.
THE MELANONYCHIA PROBLEM
THE MELANONYCHIA
PROBLEM
The challenging problem of brown nail pigmentation is dealt with here. This is important as nail melanoma is the most serious nail condition and the rate of misdiagnoses and diagnostic delays is very high.
BENIGN MELANONYCHIAS
A brown streaky pigmentation of the nail is called longitudinal melanonychia (LM). LM does not primarily
1605
16
Age at Onset
■Babies—benign
■Children—mostly benign
■Adolescents—probably benign
■Adults until age 30 to 35 years—suspicious
■Adults older than age 40 years—highly suspicious
■Adults older than age 50 years—probably melanoma
Color and Internal Structure of the Brown Band
Color and Internal Structure of the Brown Band
■Regular light-brown band on a gray background—functional LM
■Regular light-brown band on a gray background—functional LM
■Regular brown band on a brown background—lentigo
■Regular brown band on a brown background—lentigo
■Regular brown band with dark brown spots on brown background—nevus
■Regular brown band with dark brown spots on brown
background—nevus
■Irregular brown band with asymmetric, unevenly spaced lines of variable length, proximal widening of the band—melanoma
■Irregular brown band with asymmetric, unevenly spaced lines of
variable length, proximal widening of the band—melanoma
include the type of pigment responsible for it. Bacterial, fungal, blood, and various exogenous pigments can cause band-like or diffuse brown to black nail pigmentations. It is the color itself, not its intensity, that is important; the internal architecture of a pigmented streak, its extension in the nail, whether it is associated with nail dystrophy or onycholysis, its time course and development, the patient’s age, gender, skin type, and profession are all important for the evaluation of LM (Table 91-10). Four lesion types can induce a true LM: melanocyte activation in the matrix results in functional melanonychia. This is the rule for LM in pigmented persons, including many children (Fig. 91-81), because of repeated trauma, such as friction or onychophagia, during pregnancy, under chemotherapy, and a variety of other drugs. A matrix lentigo is a numerical increase in melanin-producing cells (Fig. 91-82). A matrix nevus is characterized by the nest-like agglomeration of melanocytes in the matrix; most are seen in children and are junctional (Fig. 91-83). Pigmented melanoma of the matrix also causes LM (Fig. 91-84). None of the underlying pathologic processes can be safely distinguished on clinical grounds alone although dermatoscopy may help in certain respects. An LM with regular color and banding, symmetrical diameter, and no nail dystrophy is most likely benign. Periungual pigmentation in children may be a sign of a congenital nevus. LM in children and adolescents is commonly regarded as being benign. Particularly in children, an LM may fade with age, but rarely may become darker, particularly in children with skin types IV to VI. Although childhood nail melanoma is extremely rare, a single rapidly increasing LM in a light-skinned child is best excised. The tangential excision technique can prevent postsurgical nail dystrophy. It is recommended to tangentially excise all acquired matrix melanocyte proliferations in adults, and if parents insist, also in children. This approach and the growing awareness of nail melanomas among dermatologists have now led to fewer advanced nail melanomas among the author’s patients.
1606
A
B
C
UNGUAL MELANOMA
Nail melanoma is a subtype of acral melanoma. It makes up 1.5% to 2.5% of all melanomas in lightskinned individuals, 10% to 20% in Asians, and up to 25% in Africans, although the absolute numbers are very similar. With nails representing less than 1% of the body surface area the nail is overrepresented as a site for melanomas.34 In fact, as subungual melanomas with melanonychia derive from the matrix, which represents only one-quarter to one-third of the nail field,
this is a particular area of concentration of melanoma development. The peak incidence of nail melanoma is from the fifth to seventh decades of life, but nail melanomas may occur in children and in the very old. There is no clearcut gender predominance. Thumbs, big toes, index fingers, and middle fingers are the most common sites.
16
Periungual pigmentation is called the Hutchinson sign and represents periungual spread of the in situ component (Fig. 91-85). Most subungual melanomas are pigmented and start with an LM, which is irregular in contrast to benign LMs (see Table 91-10). Proximal widening indicates rapid growth of the lesion. Nail dystrophy is a sign of an advanced melanoma. Dermatoscopy helps to determine the internal structure of the LM and allows a micro-Hutchinson sign to be seen. Approximately 25% to 33% of nail melanomas are amelanotic and pose great diagnostic challenges (Fig. 91-86). They usually arise from the nail bed, cause onycholysis that may ooze, and are frequently misdiagnosed as a pyogenic granuloma, ingrown nail, or wart, or even onychomycosis. Unfortunately, even pigmented nail melanomas are usually diagnosed very late with a diagnostic delay of years to decades. This is why the prognosis of nail melanomas is so poor, with 5-year survival rates of 15% to 20% for invasive nail melanomas.
Diagnosis: A diagnostic algorithm considering several factors was proposed to facilitate the diagnosis of pigmented melanoma (Table 91-11); it is not useful for amelanotic melanomas and LM in children.35
1607
16
Treatment: Treatment of nail melanoma is by surgery. In situ and early invasive melanomas can be removed by wide local excision with preservation of the digit,36,37 whereas distal amputation is recommended for advanced melanomas. Hutchinson sign responds to topical immunotherapy with imiquimod.38
Disease Associations: Ungual melanomas occur more frequently in those subjects with a personal or family history of melanoma. Ultraviolet exposure is not associated with nail melanoma. Histopathologically, there is a frequent association with multiple subungual onycholemmal cysts, which must not be mistaken for subungual squamous cell carcinoma.39,40
Clinical Course, Prognosis, and Management: As the diagnostic delay is often years or even decades many melanoma patients come late with advanced tumors, although this is exceptional in the author’s practice. The list of misdiagnoses is long and often incomprehensible for an experienced dermatologist. In situ and early invasive melanomas have a very good prognosis; however, advanced and metastatic melanomas have a 5-year survival rate of 15% to 24%.
A— Age: most ungual melanomas occur between 40 and 70 years of age; African Americans, native Americans, Asians: a higher percentage of nail melanomas B— Brown to black band in the nail, breadth over 3 mm, irregular or blurred border C— Change: Rapid increase in width and growth rate, nail dystrophy does not improve despite adequate therapy; color D— Digit: thumb > big toe > index finger; single-digit involvement; very rarely more affected E—Extension of pigmentation: Hutchinson sign F— Family or personal history of melanoma or so-called dysplastic nevi
A—Age: most ungual melanomas occur between 40 and 70 years of
age; African Americans, native Americans, Asians: a higher percentage of nail melanomas B—Brown to black band in the nail, breadth over 3 mm, irregular or
blurred border C—Change: Rapid increase in width and growth rate, nail dystrophy
does not improve despite adequate therapy; color D—Digit: thumb > big toe > index finger; single-digit involvement;
very rarely more affected E—Extension of pigmentation: Hutchinson sign F—Family or personal history of melanoma or so-called dysplastic
1608
nevi
There are no controlled studies concerning the efficacy of new targeted and immune checkpoint inhibitor therapies on nail melanoma, although there is no reason not to assume that they will have a similar activity. Postoperatively, patients are seen for followup examinations at regular intervals, depending on tumor thickness and stage. It has to be stressed that ungual melanomas are not particularly aggressive and that it is the delay in diagnosis and treatment that makes their prognosis so poor.

Figure 91-1 Rudimentary double nail of the little toe.

Figure 91-2 Leukonychia punctata.

Figure 91-4 Muehrcke lines in hypoalbuminemia after more than 7 weeks of high fever.

Figure 91-5 Pseudoleukonychia in superficial white onychomycosis; the white spots are on the surface of the nail plate.

Figure 91-6 Red spot in the lunula of a patient with acute nail psoriasis.

Figure 91-7 Longitudinal erythronychia caused by an onychopapilloma.

Figure 91-8 Multiple red lines in dyskeratosis follicularis Darier (A) and white lines in Hailey-Hailey disease (B).

Figure 91-9 Green nail caused by Pseudomonas abscess under the nail.

Figure 91-10 Jet-black nail surface stain from 5% silver nitrate solution used to etch what was thought to be granulation tissue protruding from under the proximal nailfold.

Figure 91-11 Dirty grayish nail discoloration caused by Proteus spp.

Figure 91-12 Melanonychia caused by melanin production in the matrix of a dark-skinned person.

Figure 91-13 Subungual hematoma in a little boy with congenital malalignment of the big toenail. This condition is often associated with large subungual hematomas from minor trauma. The figure shows that the hematoma grows out with its proximal border being parallel to the presumed lunula border and free nail end.

Figure 91-14 Splinter hemorrhages in a patient with chronic diarrhea.

Figure 91-16 Lichen planus of the nail bed causing onycholysis.

Figure 91-17 Onycholysis semilunaris induced by overzealous manicure.

Figure 91-18 Hyperkeratosis of the nail bed.

Figure 91-19 Onychogryphosis in a 63-year-old woman.

Figure 91-20 Pterygium in nail lichen planus.

Figure 91-21 Pterygium inversum in a 54-year-old patient with Guillain-Barré syndrome.
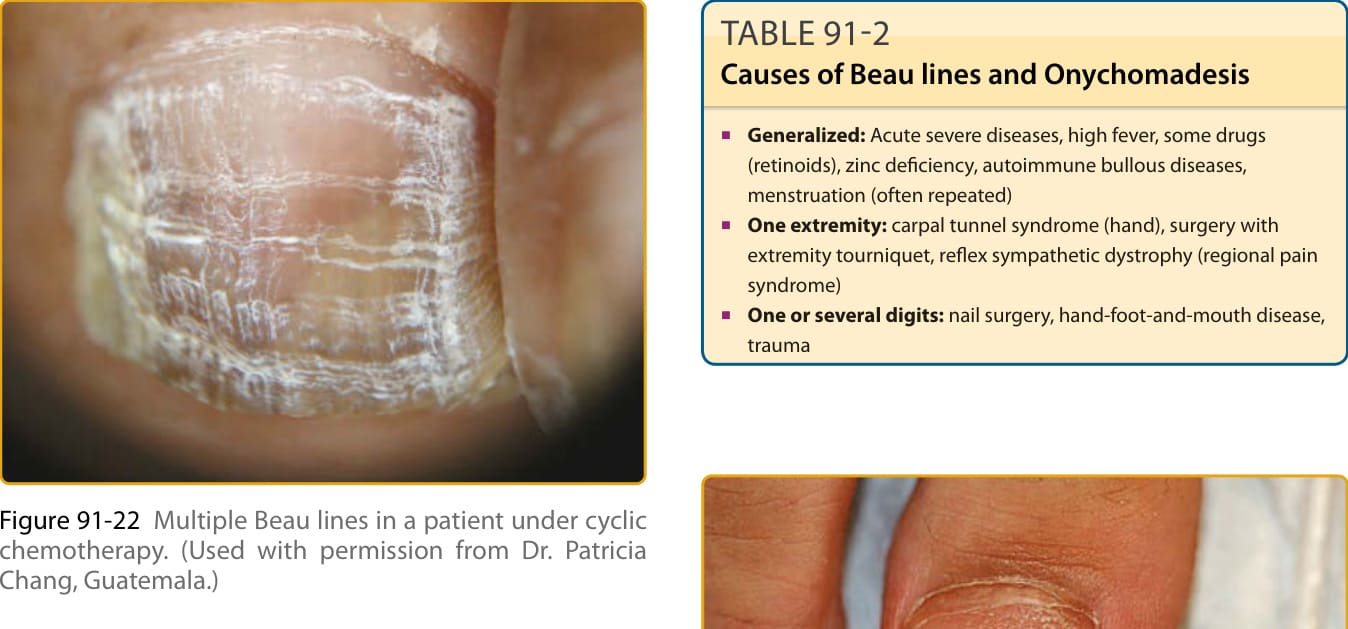
Figure 91-22 Multiple Beau lines in a patient under cyclic chemotherapy. (Used with permission from Dr. Patricia Chang, Guatemala.)

Figure 91-23 Onychomadesis after hand-foot-and-mouth disease.

Figure 91-24 Psoriatic pitting.

Figure 91-25 Trachyonychia in an 11-year-old boy with atopic dermatitis.

Figure 91-26 Longitudinal groove in a patient with a myxoid pseudocyst.

Figure 91-27 Onychorrhexis.

Figure 91-28 Onychoschizia.

Figure 91-29 Ingrown nail of the big toe.

Figure 91-30 Ingrown nail of the finger in a patient under targeted anticancer treatment with cetuximab.
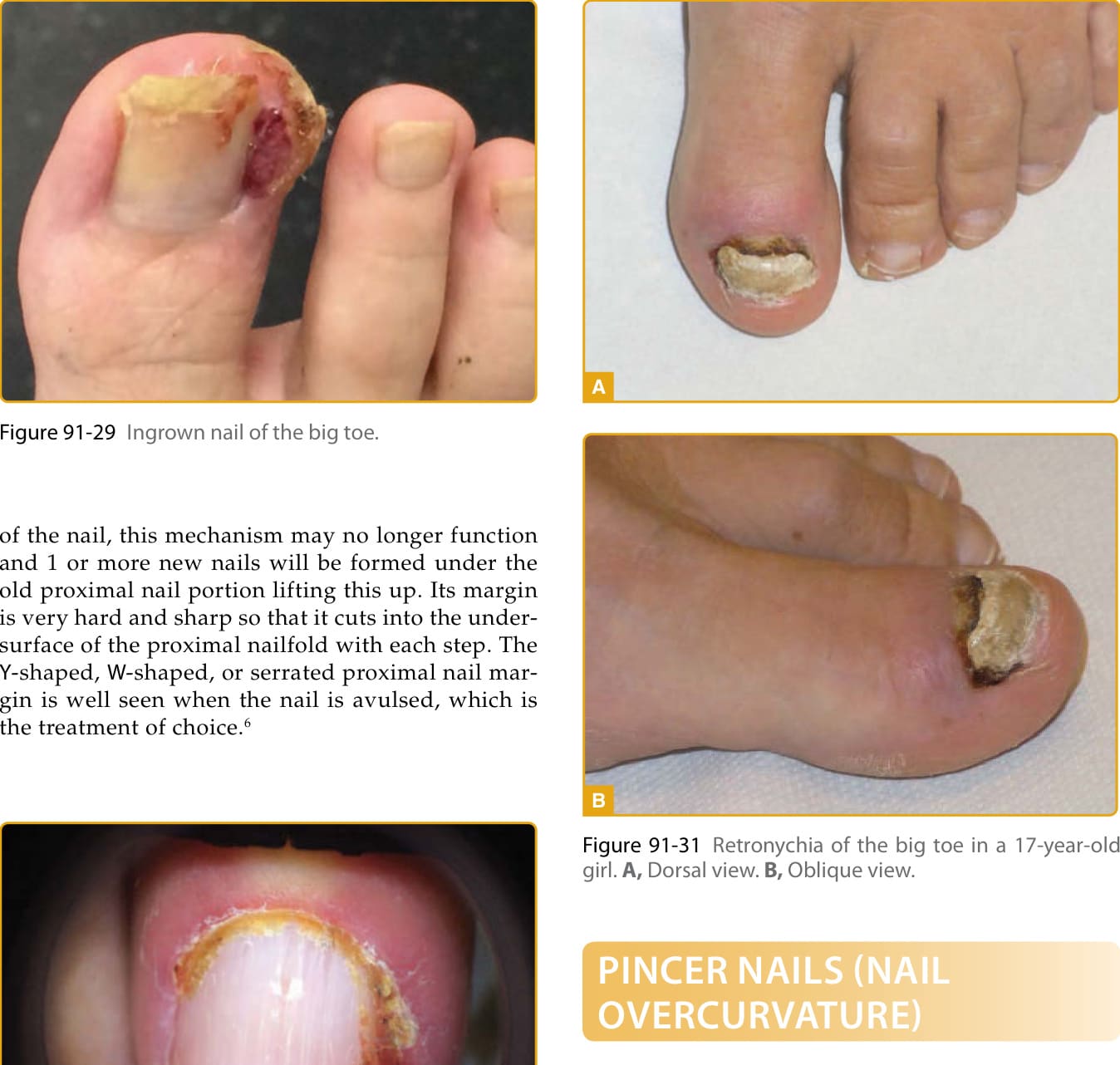
Figure 91-31 Retronychia of the big toe in a 17-year-old girl. A, Dorsal view. B, Oblique view.

Figure 91-32 A, Pincer nails of the thumbs in a 53-year-old woman. B, Pincer nails of the toes in a 38-year-old woman.

Figure 91-33 Nail psoriasis with pits arranged in a line.
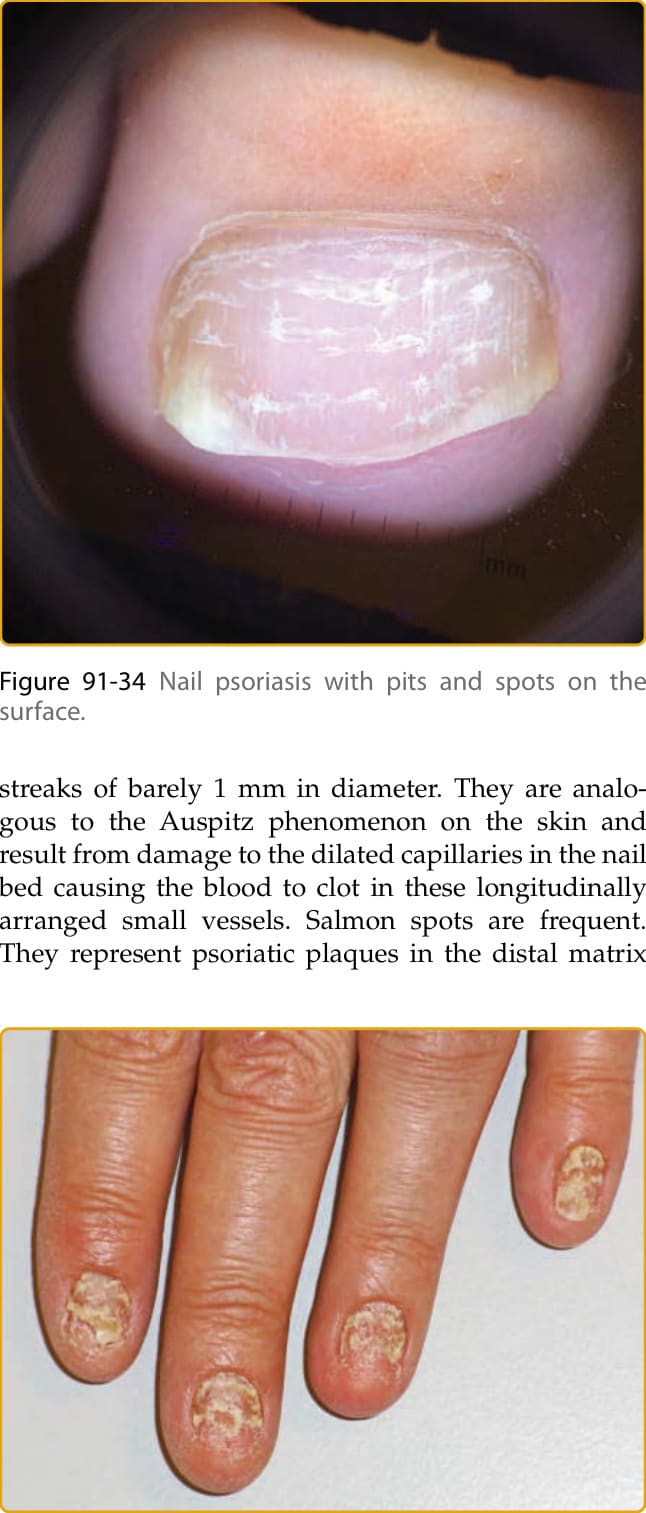
Figure 91-34 Nail psoriasis with pits and spots on the surface.

Figure 91-35 Nail psoriasis destroying the entire nail.

Figure 91-36 Nail involvement in pustular psoriasis of Barber-Königsbeck.

Figure 91-37 Acrodermatitis continua suppurativa of Hallopeau.

Figure 91-38 Nail changes in Reiter disease. (Used with permission from Dr. Robert Baran, France.)

Figure 91-39 Nail eczema in a gardener handling tulips.

Figure 91-40 Alopecia areata of the nail.

Figure 91-41 Lichen planus of the nails.

Figure 91-42 Lichen planus of the nails.

Figure 91-43 Bullous pemphigoid of the nail.

Figure 91-44 Dermatomyositis. A, Capillary microscopy shows avascular areas and aneurysms. B, Gottron papules on the distal phalanges.
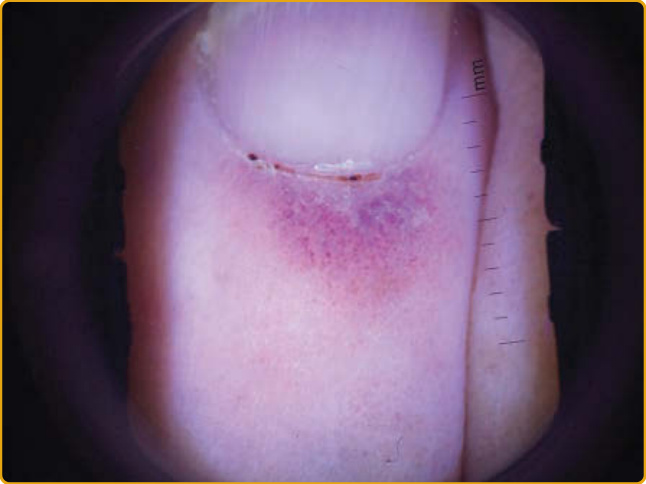
Figure 91-46 Livedoid vasculopathy involving the proximal nailfold.
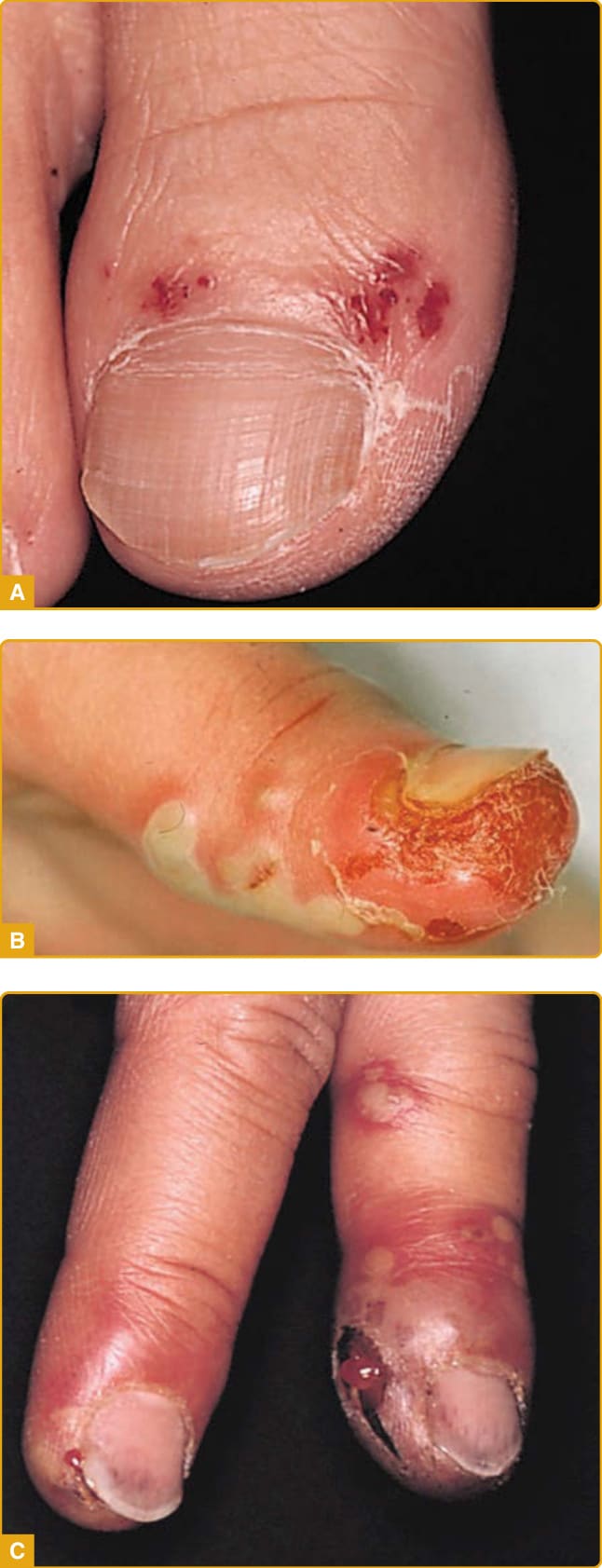
Figure 91-47 Recurrent herpes simplex of the toe (A), thumb (B), and fingers (C).

Figure 91-48 Generalized verrucous herpes zoster in a patient with advanced Hodgkin disease.

Figure 91-50 Hand-foot-and-mouth disease.

Figure 91-51 Bullous impetigo of the nailfold, so-called runaround.

Figure 91-52 Pseudomonas aeruginosa colonization of the nail in a patient with an onychomatricoma.

Figure 91-53 Distal–lateral subungual onychomycosis.

Figure 91-54 White superficial onychomycosis, caused by Fusarium spp, of the toe in an immunocompetent person.

Figure 91-55 Superficial white onychomycosis caused by Trichophyton rubrum in an AIDS patient.

Figure 91-56 Proximal white subungual onychomycosis.

Figure 91-57 Total dystrophic onychomycosis in a 10-yearold boy with chronic mucocutaneous candidiasis.

Figure 91-58 Clubbing in a patient with trisomy 21 and Eisenmenger complex.

Figure 91-59 Yellow nail syndrome.

Figure 91-60 Acrodermatitis enteropathica with blisters and erosions on the periungual skin.

Figure 91-61 Half-and-half nail in a patient with renal insufficiency.
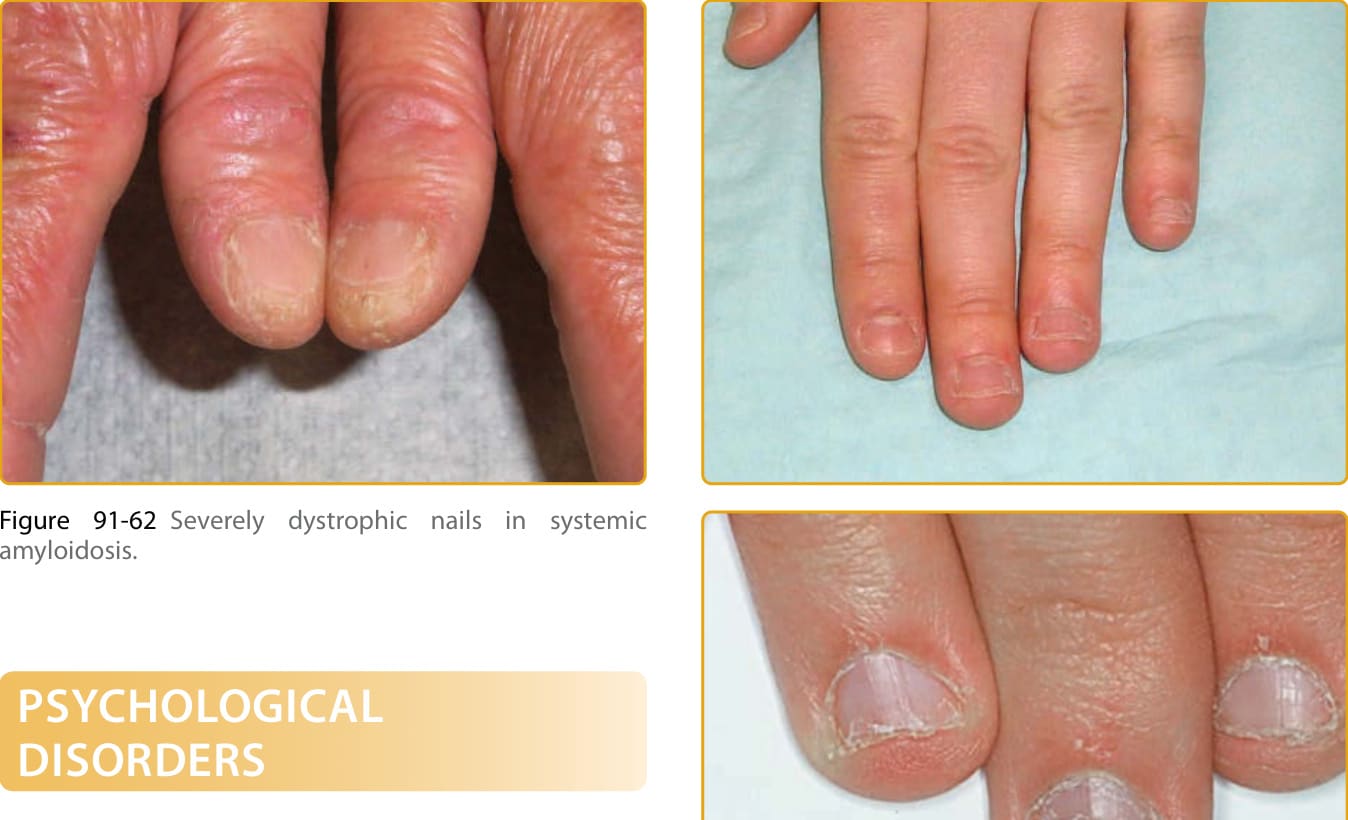
Figure 91-62 Severely dystrophic nails in systemic amyloidosis.

Figure 91-63 Onychophagia.

Figure 91-64 Perionychotillomania (habit tic): habitual pushing back of the proximal nailfold.

Figure 91-65 The Heller’s median canaliform dystrophy of the thumbnail.

Figure 91-66 Onychotillomania.

Figure 91-67 Pachyonychia congenita.
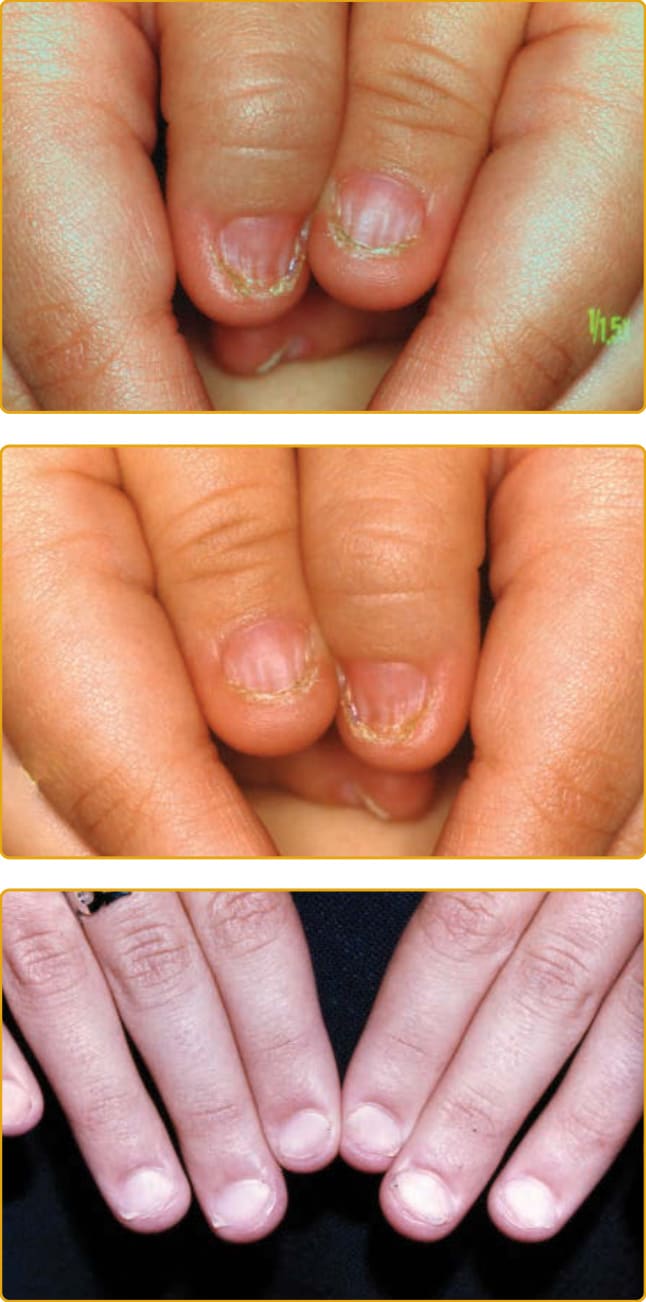
Figure 91-68 Hidrotic ectodermal dysplasia with folded nails.

Figure 91-70 Epidermolytic keratosis palmaris et plantaris with nail involvement.

Figure 91-71 Congenital malalignment of the big toenail.

Figure 91-72 Onychocytic matricoma.
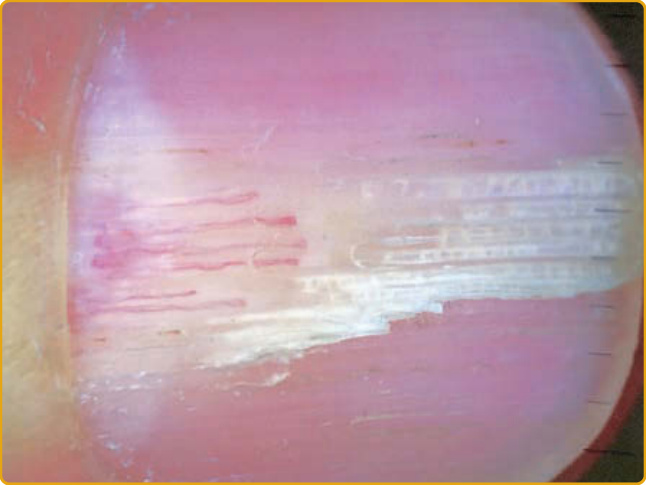
Figure 91-73 Onychomatricoma.

Figure 91-74 Onychopapilloma.

Figure 91-75 Fibrokeratoma of the nail.
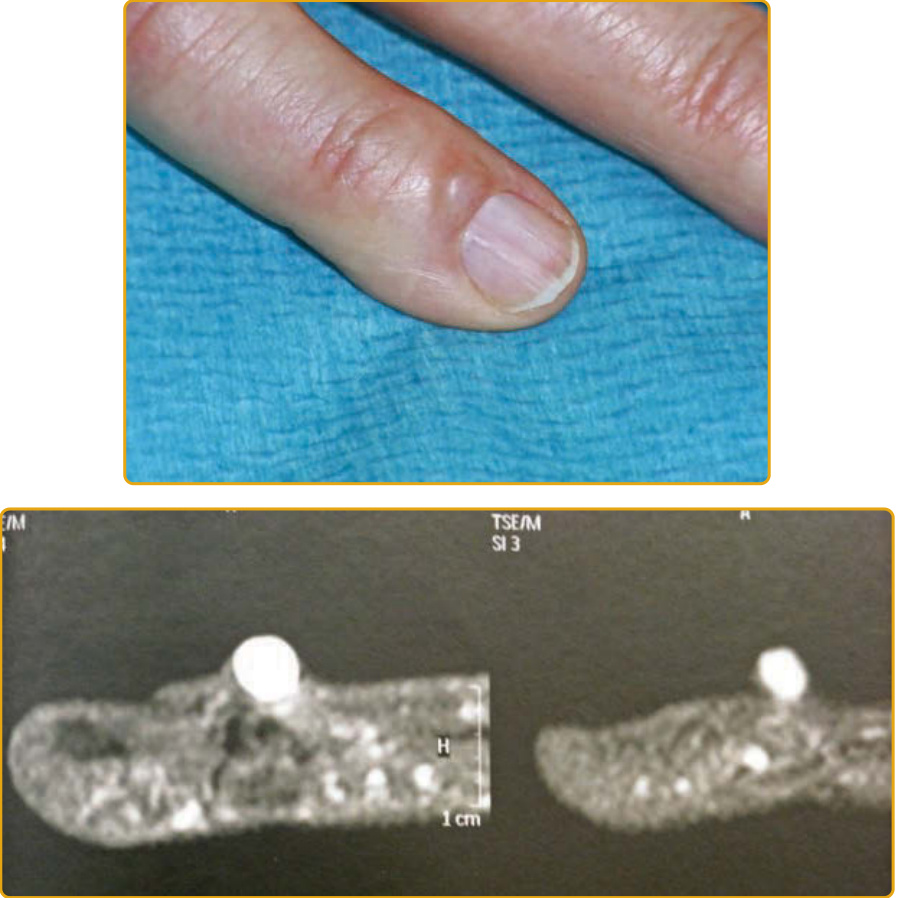
Figure 91-76 Myxoid pseudocyst in the proximal nailfold causing a longitudinal groove in the nail. In the magnetic resonance tomography, the content of the myxoid pseudocyst stands out due to its high water content. A connecting stalk is seen as a sinuous narrow band extending from the lesion to the joint.

Figure 91-77 Glomus tumor.

Figure 91-78 Subungual exostosis of the big toe.

Figure 91-80 Bowen disease’ of the nail with an invasive component.
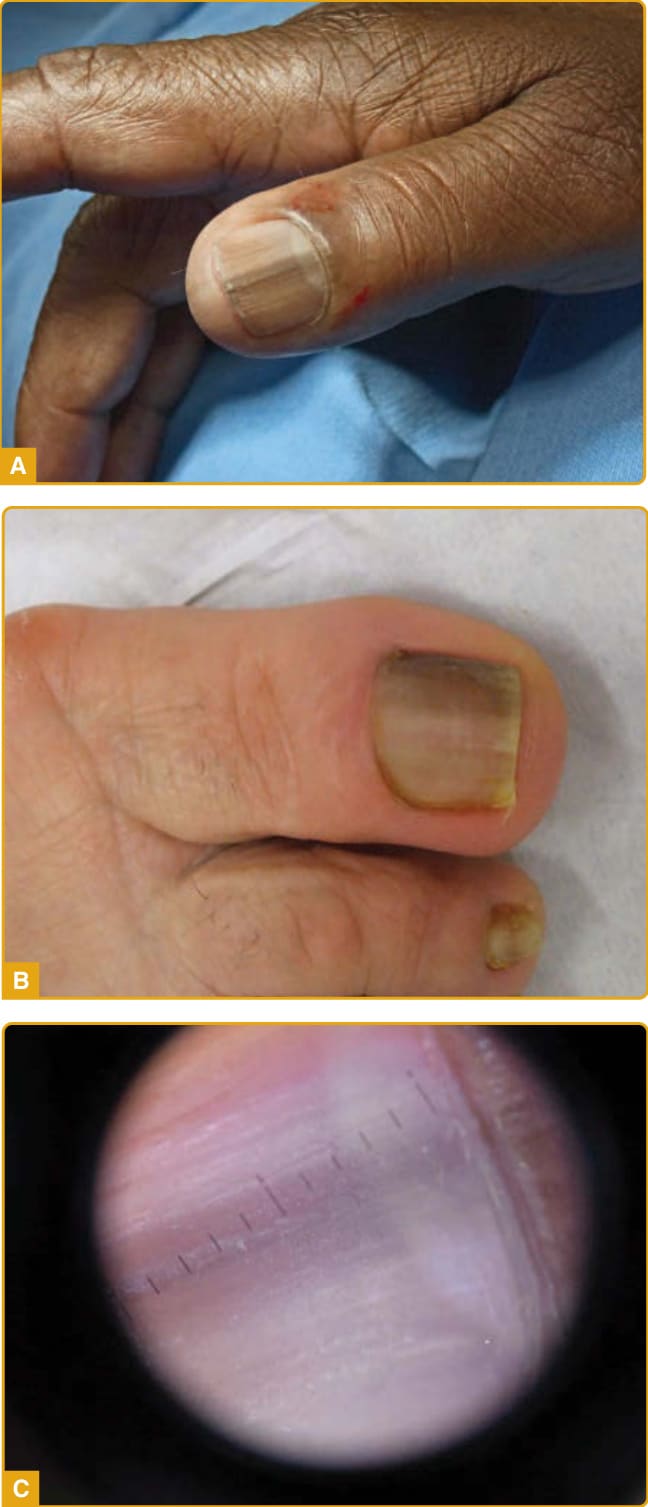
Figure 91-81 A, Functional melanonychia in a dark skinned person. B, due to friction. C, drug-induced functional melanonychia.

Figure 91-82 Melanonychia caused by a matrix lentigo.

Figure 91-83 Melanonychia caused by a matrix nevus.

Figure 91-84 Matrix melanoma causing longitudinal melanonychia with irregular outline.

Figure 91-85 Subungual melanoma with Hutchinson sign.

Figure 91-86 Amelanotic melanoma of the nail bed.
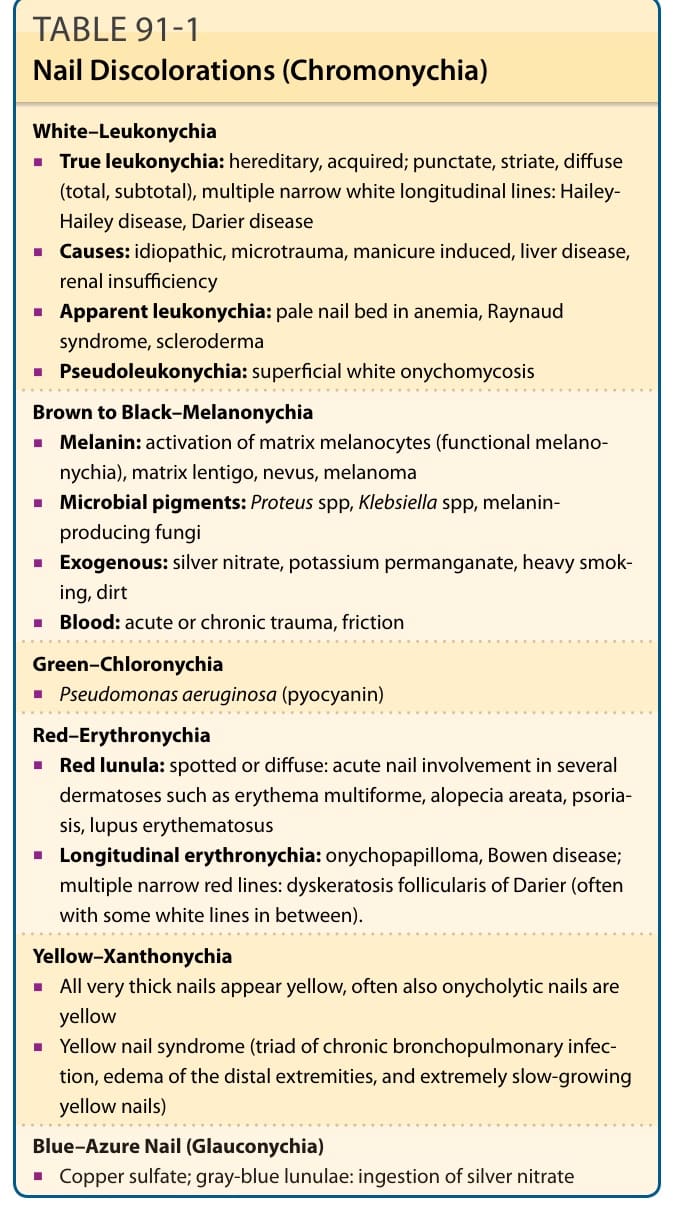
TABLE 91-1 Nail Discolorations (Chromonychia)
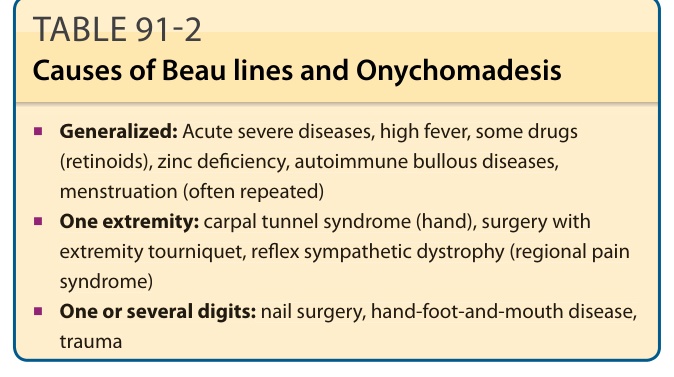
TABLE 91-2 Causes of Beau lines and Onychomadesis
TABLE 91-3 Causes of Pitting and Trachyonychia
TABLE 91-4 Causes of Brittle Nails
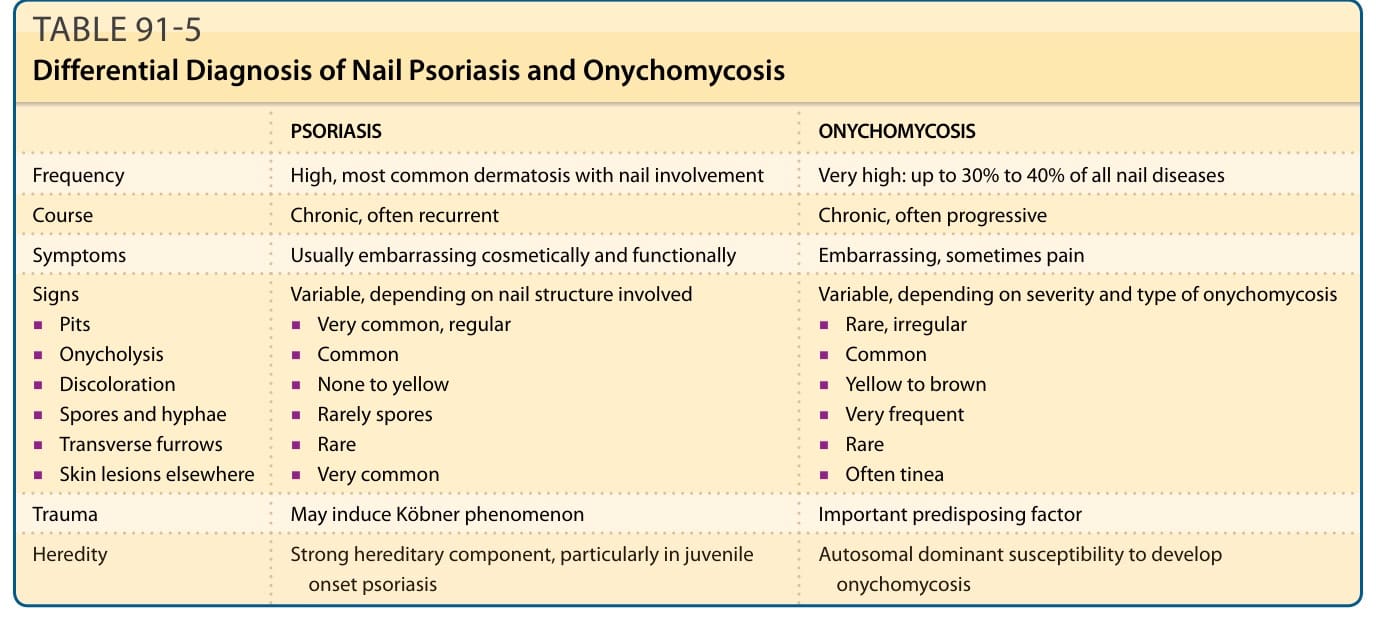
TABLE 91-5 Differential Diagnosis of Nail Psoriasis and Onychomycosis
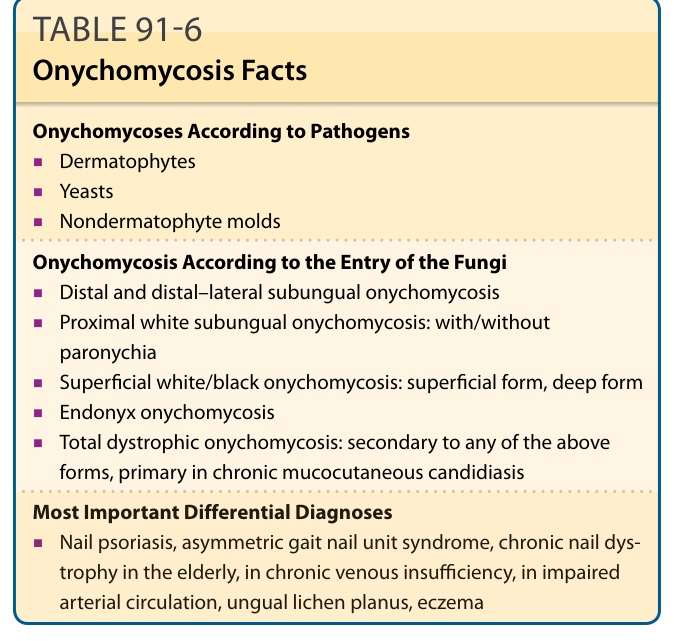
TABLE 91-6 Onychomycosis Facts
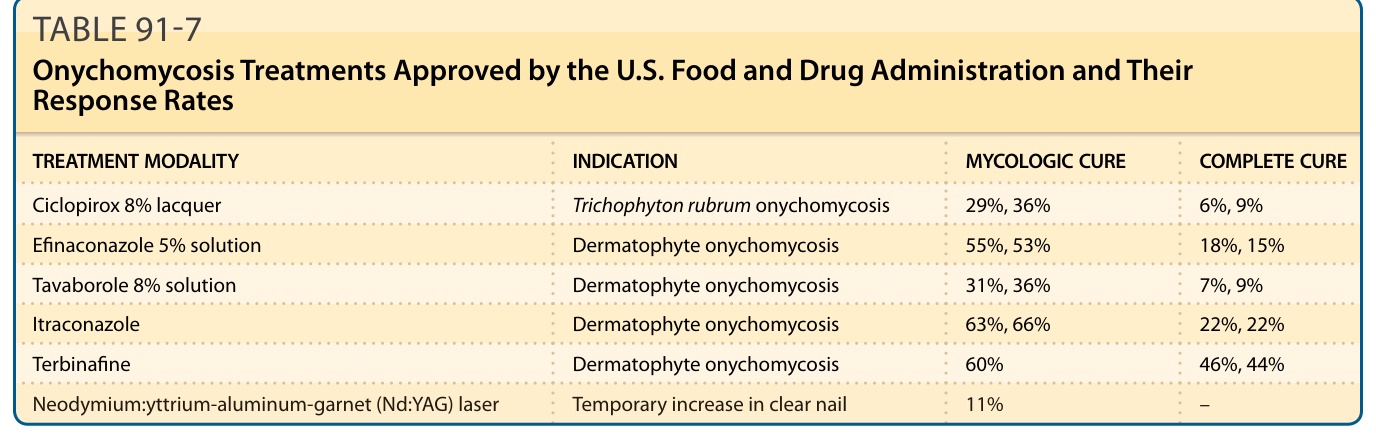
TABLE 91-7 Onychomycosis Treatments Approved by the U.S. Food and Drug Administration and Their Response Rates
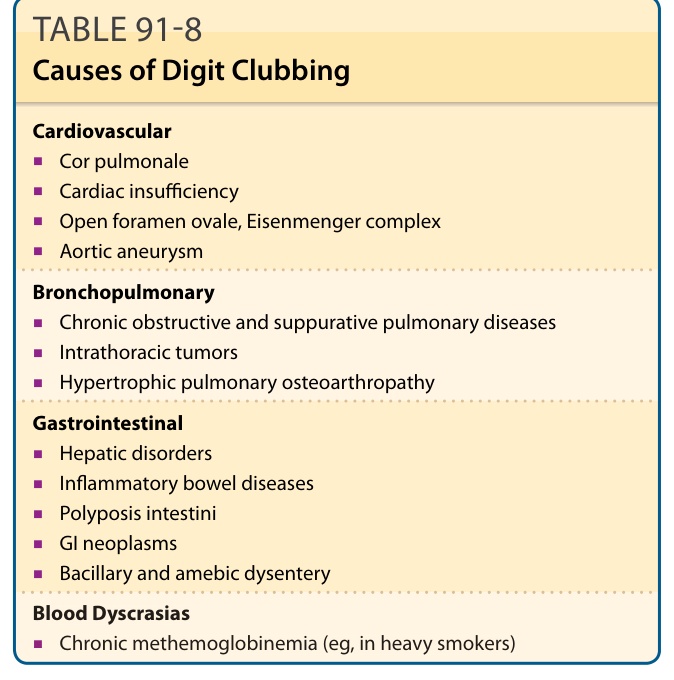
TABLE 91-8 Causes of Digit Clubbing
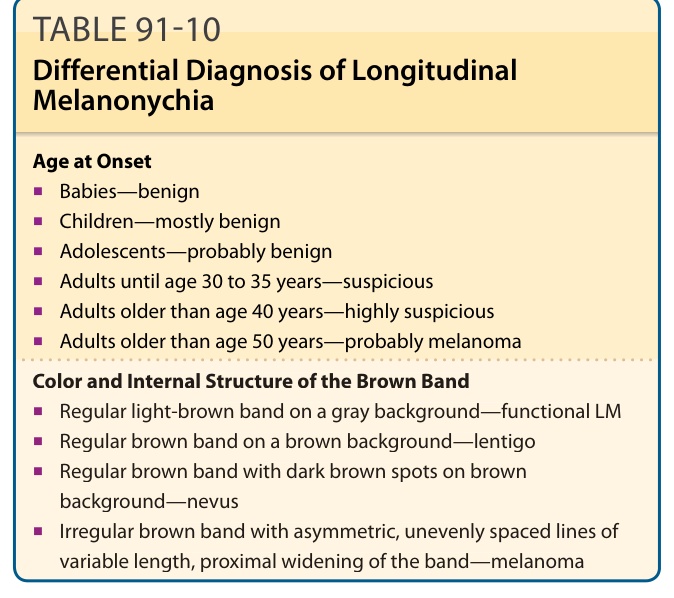
TABLE 91-10 Differential Diagnosis of Longitudinal Melanonychia
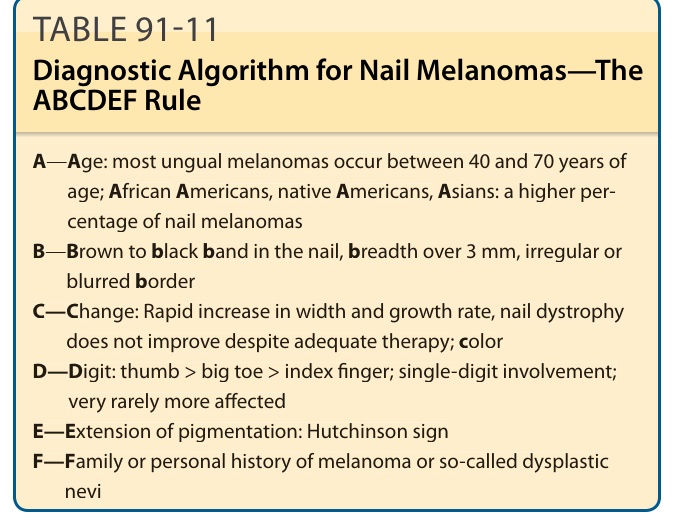
TABLE 91-11 Diagnostic Algorithm for Nail Melanomas—The ABCDEF Rule