Hirsutism and Hypertrichosis
16
HIRSUTISM
AT-A-GLANCE
■ Hirsutism is defined as terminal body hair growth in women in a male distribution.
■ Women with a Ferriman-Gallwey score of 8 or higher are considered hirsute.
■ Women with mild to moderate hirsutism and regular menstrual cycles are most likely diagnosed with idiopathic hirsutism; hormone testing is not necessary.
■ Hormone testing is necessary in women with moderate to severe hirsutism and all women with hirsutism and irregular menstrual cycles or signs of virilisation.
INTRODUCTION
INTRODUCTION
Hirsutism is a condition in which excessive hair in women grows in a male pattern distribution. It has a significant psychosocial impact on the affected individual as well as a number of medical consequences for the skin. The main driving factors are the higherthan-normal androgen levels, either in circulation or locally, and an increased sensitivity of the hair follicle to androgens. This condition differs from hypertrichosis in which the excess hair has a more generalized distribution and independent of androgens. Hirsutism may result from various causes, with polycystic ovarian syndrome (PCOS), nonclassical congenital adrenal hyperplasia (CAH), and adrenal or ovarian tumors being among the major causes, or hirsutism may be idiopathic. Hirsutism can cause the affected individual embarrassment, leading to social withdrawal and even depression.1,2 A recent study has identified that patients view their condition as more severe than do their clinicians, which is associated with a negative effect on their quality of life.3 The authors suggest that treatment be guided by the level of patient’s distress with the hair growth.
EPIDEMIOLOGY
EPIDEMIOLOGY
The prevalence of hirsutism is unknown. Approximately 5% to 15% of the female population of reproductive age is thought to be affected by hirsutism,
and it is one of the most common complaints of patients presenting to dermatology offices.4,5 The variability in concentration of hair follicles is influenced by ethnicity and strong family inheritance. Asians, with lower hair concentration, are much less likely to present with hirsutism resulting from an androgen excess state compared with their Mediterranean counterparts.6 As a result, the cut-off value for diagnosis of hirsutism varies among different ethnic populations. The prevalences of hirsutism were estimated to be 38% in Greece, 21.2% in Australia, 10.8% in Iran, 10.5% in India, 8.3% in Turkey, 7.1% in Spain, and 2% in Thailandand.7,8 A study of North American women with hirsutism identified that 25% to 33% of white women have terminal hairs on the upper lip and periareolar area, as well as the linear alba, with normal androgen levels. The degree of facial and body terminal hair was similar in black and white women in North America with a prevalence of 4.3% and 5.4%, respectively.9 Hirsutism may also be influenced by age. Most of the patients are women of reproductive age, and the growth pattern is heaviest at a younger age compared with older age.10
PATHOGENESIS
PATHOGENESIS
The hair growth cycle is made up of three phases: anagen (growth phase), catagen (involution), and telogen (rest phase). The cycle is under hormonal influence in a site-specific pattern. The maturation of vellus (small, straight, and nonpigmented) hair to terminal (long, curlier, and pigmented) hair is the result of the activation of androgen receptors in the hair follicle.11 During puberty, an increase in androgen levels drives vellus hair to differentiate into terminal hair, as well as sebaceous gland development (see Chap. 6 for more detail). In women, the androgens are produced in the ovaries and adrenal glands and are subject to peripheral conversion. Enzymatic conversion of cholesterol to pregnenolone is the rate-limiting step of all steroid hormone production. This step is under the influence of luteinizing hormone (LH) in the ovary and adrenocorticotropic hormone (ACTH) in the adrenal cortex.11 Although both testosterone and dihydrotestosterone (DHT) are capable of converting vellus hair to terminal hair, DHT is the most potent androgen. DHT is produced from the peripheral enzymatic conversion of testosterone by 5α-reductase within the hair follicle.11 Binding of DHT to its nuclear receptor activates genes responsible for conversion of vellus hair to terminal hair in androgen sensitive areas of the body. However, excess circulating androgens
16
alone do not explain the pathogenesis of hirsutism because some women have hirsutism without evidence of androgen excess (idiopathic hirsutism; see below).12 In these individuals, local factors and variability in end-organ sensitivity are thought to be the underlying cause.
CLINICAL FINDINGS AND DIAGNOSIS
CLINICAL FINDINGS
AND DIAGNOSIS
Hirsutism can be categorized as primary or idiopathic in 5% to 15% of affected patients with regular menstrual cycles and normal levels of circulating androgens12 versus secondary hirsutism associated with underlying causes (Table 90-1). In evaluating patients, it is important to obtain a thorough history of their symptoms and signs. Apart from hirsutism, other cutaneous signs of hyperandrogenism include acne, acanthosis nigricans, androgenetic alopecia, seborrheic dermatitis, and signs of virilization. Signs of virilization include clitoromegaly, male pattern balding, deepening voice, or decreased breast size.13 It is also important to review the patient’s list of medications
and supplements to be assured that these are not contributing to androgen excess. The abrupt and rapid onset of hirsutism should raise suspicion of malignancy. The most commonly involved areas are the upper lip > thighs > lower abdomen > upper back.14
The modified Ferriman and Gallwey (mFG) scoring scale is a systematic assessment tool for the degree of hirsutism of nine body locations, which when combined, allow for an overall diagnosis of hirsutism. It was developed by Ferriman in 1961 and later modified by Hatch in 1981.15,16 It assigns a score of 1 to 4 in nine body areas, with an increasing numeric score corresponding to greater hair density (Fig. 90-1). Excess hair distribution in the nine anatomical areas evaluated by the mFG scale (upper lip, chin and cheeks, chest, abdomen, pubic area and lower abdomen, arms, legs, upper back and lower back, and buttocks) characterize patients with hirsutism.15,17 The score varies from 0 (no hair) to 4 (extensive hair growth) in each area. Normal hair growth is defined by a score of 8 or less, mild hirsutism is defined by a score of 8 to 14, and a score of greater than 15 indicates moderate to severe hirsutism.18 The anatomical distribution and the extent of body involvement may vary among individual patients. An alternative simplified scoring system with three body parts (upper abdomen, lower abdomen, and chin) with
ETIOLOGY FINDINGS COMMENT
Idiopathic hirsutism (IH) Regular ovulation and normal to slightly elevated androgen levels Often presents with mild to moderate hirsutism
Mean age, BMI, and hip and waist circumference higher in IH vs patients with metabolic disturbance13
Polycystic ovarian syndrome (PCOS) Hyperandrogenism; menstrual irregularities, including oligomenorrhea, amenorrhea, and infertility; and impaired glucose tolerance, hyperlipidemia, and obesity
Nonclassic congenital adrenal hyperplasia Autosomal recessive inheritance of 21-hydroxylase deficiency Rarely secondary to 11β-hydroxylase deficiency Hirsutism, acne, alopecia, anovulation, and menstrual dysfunction
HAIR-AN Hyperandrogenism (HA), insulin resistance (IR), and acanthosis nigricans (AN) Considered a subtype of PCOS
Cutaneous findings of acanthosis nigricans may also be observed in 5% of obese women with insulin resistance Warrants endocrinology evaluation for impaired glucose tolerance as increased risk for type 2 diabetes mellitus16,18
Patients often present accelerated bone age maturation and increased basal or stimulated 17-OHP
Insulin elevated; elevated or high-normal levels of testosterone and androstenedione but normal levels of LH and prolactin30
SAHA Seborrhea (S), acne (A), hirsutism (H), and alopecia (A)
Hyperprolactinemia Presents with amenorrhoea, galactorrhea, and infertility Associated with stress, pituitary adenoma, pregnancy, drug intake, and primary hypothyroidism with elevated TSH
Cushing syndrome Centripetal fat distribution, thinning of the skin with striae, glucose intolerance, osteoporosis, and proximal muscle weakness; signs and symptoms of hyperandrogenism and menstrual irregularities
■Multiple causes:
■Adrenal neoplasm
■Ectopic ACTH-secreting tumor
■Pituitary tumor (Cushing disease)
Pregnancy Most common areas involved are the upper abdomen, lower abdomen, lower back, upper lip, and thighs52 Serum total testosterone levels and mFG score increase with the progression of pregnancy Associated with physiological changes of pregnancy
Acromegaly Elevated random serum GH and IGF-1 Patients can present with abnormal growth of the hands and
Acromegaly Elevated random serum GH and IGF-1 Patients can present with abnormal growth of the hands and feet, arthritis, sleep apnea, headache, and impaired vision
1556
feet, arthritis, sleep apnea, headache, and impaired vision
ACTH, adrenocorticotropic hormone; BMI, body mass index; GH, growth hormone; HCG, human chorionic gonadotropin; IGF, insulin-like growth factor; LH, luteinizing hormone; mFG, modified Ferriman and Gallwey;17-OHP; 17-hydroxyprogesterone; TSH, thyroid-stimulating hormone.
16
The Ferriman-Gallwey scale
Upper lip
1 2 3 4
Chin
1 2 3 4
Chest
1 2 3 4
Abdomen
1 2 3 4
Pelvis
1 2 3 4
Upper arms
1 2 3 4
Thighs
1 2 3 4
Upper back
1 2 3 4
Lower back
1 2 3 4
1557
16
a cut-off score of 3 was able to distinguish hirsute from nonhirsute women with an accuracy of 87.5%.19
The diagnosis of hirsutism can be challenging because many physicians are not familiar with the Ferriman and Gallwey scoring scale and, among those who are, discrepancies exist in their interpretation of the scoring value. Furthermore, the diagnostic score varies among different ethnic populations: for example, 2 or 3 or greater for Asians and 9 to 10 or greater for Mediterraneans.7,20 Also, there is no consensus on how many body regions are to be included in the scoring system. Another challenge is that most patients presenting for evaluation will have used various cosmetic measures to remove excess hair, thus leading to an inaccurate assessment.
ASSOCIATED CAUSES
ASSOCIATED CAUSES
IDIOPATHIC HIRSUTISM
Idiopathic hirsutism occurs in a subgroup of hirsute patients who present with hirsutism, regular ovulation, and normal to slightly elevated androgen levels in the absence of features that suggest other causes of hirsutism. Its prevalence is 4% to 7%, and it is a diagnosis of exclusion21 (Figs. 90-2 and 90-3). The pathogenesis remains unclear. The intrinsic hyperresponsiveness of androgen receptors to normal circulating levels of androgens and increased activity of the 5α-reductase enzyme at the hair follicle are postulated thoeries.12 The increased local circulation of androgens is caused by increased gene expression of the steroid-converting enzymes 17β-hydroxysteroid dehydrogenase and steroid sulfatase, resulting in decreased levels of estradiol/testosterone.22
POLYCYSTIC OVARIAN SYNDROME
Polycystic ovarian syndrome, also known as Stein- Leventhal syndrome after the clinicians who first described the condition, is the most common associated
1558
cause of hyperandrogenism in women of reproductive age and is a common secondary cause of hirsutism23 (Fig. 90-4). The other clinical characteristics of PCOS can include chronic anovulation, insulin resistance, and infertility.24 Apart from hirsutism, the hyperandrogenic state causes PCOS patients to also present with other cutaneous manifestations, including acne, acanthosis nigricans, alopecia, and seborrheic dermatitis.25 More than 50% of women with PCOS present with hirsutism that tends to have a more truncal distribution.26 Alternatively, individuals of certain ethnicities may lack the feature of hirsutism, as in the Asian patient with PCOS.20,27 PCOS increases the risk of type 2 diabetes mellitus and cardiovascular dysfunction. Both the reproductive and the metabolic manifestations of PCOS are exacerbated by being overweight or obese.28
HAIR-AN
A subset of PCOS patients are classified as HAIR-AN because of the presence of hyperandrogenism (HA),
insulin resistance (IR), and acanthosis nigricans (AN). This syndrome is found in 1% to 5% in women presenting with hyperandrogenism. The underlying cause is associated with insulin resistance with compensatory hyperinsulinemia.29 The clinical presentation can include various combinations of oily skin, hirsutism, acne, menstrual irregularities, androgenic alopecia, signs of virilization (deepening of voice, clitoromegaly and changes in muscle mass), insulin resistance with diabetic symptoms, as well as acanthosis nigricans.30
If ovarian biopsy is performed, the most consistent histopathologic finding is islands of hyperplastic theca cells in ovarian stroma known as hyperthecosis, with normal adrenal function. There are reports of association with other autoimmune or endocrine diseases such as Hashimoto thyroiditis, Graves disease, vitiligo, Cushing syndrome, Cohen syndrome, acromegaly, CAH, and insulinoma.30,31
SAHA SYNDROME
The constellation of cutaneous manifestations such as seborrhea, acne, hirsutism, and androgenetic alopecia is identified as SAHA syndrome. Apart from seborrhea, which is present in 100% of the cases, the other conditions can be variable in presentation. The condition is further divided into idiopathic, ovarian, adrenal, and hyperprolactinemic types,32 and it can be associated with PCOS, cystic mastitis, obesity, and infertility. SAHA syndrome is prevalent in 17.7 % of PCOS patients, and this variety of PCOS is associated with greater insulin resistance.33
ADRENAL AND OVARIAN HIRSUTISM
Adrenal hyperplasia is associated with a defect in the enzyme responsible for the synthesis of cortisol, which leads to the accumulation of precursors that are diverted into androgen synthesis. Late onset or nonclassic CAH is an autosomal recessive disorder caused by mutations in the CYP21A2 gene, which causes deficiency in 21 hydroxylases. This results in the defective conversion of 17-hydroxyprogesterone (17-OHP) to 11-deoxycortisol. Rarely, it also can be caused by a deficiency in 11–hydroxylase. It is often diagnosed after the age of 10 years and can present with peripubertal hirsutism, oligomenorrhea, acne, infertility, alopecia, primary amenorrhea, and premature pubarche.34 An elevated 17-OHP, substrate of 21-hydroxylase, level is the biochemical hallmark of the disease. Increased circulation of ACTH as in Cushing syndrome (pituitary origin) or ectopic origin can also be associated with overstimulation of adrenal androgens production. Adrenal tumors are a rare cause of hirsutism. Whereas adrenal adenomas secrete testosterone, adrenal carcinomas secrete testosterone, dehydroepiandrosterone sulfate (DHEAS), and cortisol. Symptoms may be acute and quite severe.
16
Hirsutism with galactorrhea must raise suspicions of hyperprolactinemia. Hyperprolactinemia may be associated with various conditions, either physiological or nonphysiological. Whereas some drugs (phenothiazines, benzodiazepines, and others) as well as prolactinoma, hypothyroidism, or idiopathic hyperprolactinemia are nonphysiological, lactation and stress represent physiological causes. Apart from PCOS, in women of reproductive age, pregnancy as a possible cause of hirsutism should also be ruled out. The excess androgens produced during pregnancy can be caused by luteoma of pregnancy, hyperreactio luteinalis, or aromatase deficiency in the fetus. Sertoli-Leydig cell tumors, granulosa-theca cell tumors, and hilus cell tumors are the ovarian tumors known to secrete excess androgens. They have low metastatic potential, and the treatment is surgical. Hirsutism can also be associated with other endocrinopathies, including acromegaly, hyperprolactinemia, and thyroid dysfunction.
EVALUATION
EVALUATION
To determine the cause of hirsutism, a detailed clinical, medication, and family history with physical examination is needed. After diagnosing hirsutism by an increased mFG score, diagnostic studies should focus on identification of the most likely cause (see Table 90-1). Functional causes almost always have a peripubertal onset with slow progression. Signs of virilization such as clitoromegaly or balding or of defeminization such as breast tissue atrophy are extremely rare.35 Often, the severity of the hirsutism does not correlate well with the magnitude of androgen excess. Signs of infertility with oligo- or amenorrhea, insulin resistance, abdominal obesity, or acanthosis nigricans favor PCOS. The chronicity of the symptoms may direct the investigation. If the hirsutism is long standing and mild to moderate, testosterone or androstenedione measurements are recommended. Free testosterone is a more sensitive biochemical marker of hyperandrogenism than total testosterone, but as stated earlier, the levels can be normal in women with hirsutism. With sudden onset of hirsutism, with or without virilization or high testosterone levels, other measurement of adrenal marker levels (cortisol and DHEAS) and ovarian and adrenal imaging are highly recommended (Fig. 90-5). After androgen excess is confirmed, further tests should be considered such as a pregnancy test (if the patient has amenorrhea), pelvic ultrasonography (if an ovarian neoplasm or PCOS is suspected), measurement of DHEAS and early morning 17-OHP (if CAH or adrenal neoplasm is suspected), and a prolactin level. Further testing may also include measurement of thyroid function, adrenocortical function, and insulin-like growth factor 1. Further workup typically begins with dexamethasone suppression testing to determine the source of androgen excess production. If androgen
1559
16
HAIR-AN
Exclude secondary causes
No Yes
Sudden onset +/– virilization
No Yes
Consider malignancy (imaging study to R/O adrenal and pelvic mass) T >200 ng/dL
Regular menstrual cycle (ovulatory)
Hirsutism
Idiopathic hirsutism (N T) vs idiopathic hyper androgenism (elevated T)
Medications or exogenous testosterone
Impaired result on GTT
Elevated prolactin Positive β-hCG
Positive GTT result and hyperprolactinemia
Elevated cortisol on 24-hr urine cortisol, late-night salivary cortisol, or DST
(see Table 90-3) Positive GTT result and elvated fasting cholesterol and triglycerides, LH-to-FSH ratio >3 Normal to elevated T
Elevated 17-OH progesterone and ACTH
Elevated GH and IGF-1
Elevated TSH
excess is not suppressible by dexamethasone, the presence of Cushing syndrome, neoplasm, and PCOS must be considered. If androgen excess is dexamethasone suppressible, an ACTH test for CAH is indicated. A serum testosterone level greater than 200 ng/dL is highly suggestive of adrenal or ovarian tumor, and further imaging studies may be warranted, such as abdominal computed tomography for adrenal or ovarian neoplasm.
TREATMENTS
TREATMENTS
The cultural norm of absence of hair as being more desirable in females has driven hirsute women to seek various methods of removing excess body and facial hair. Patients affected by hirsutism have lower quality of life and symptoms of both anxiety and depression.39 Along with treatment options directed at excess unwanted hair, patients should be evaluated for their social support, and psychological treatment should be offered when necessary.39,40 Before the onset of therapy, it is important to advise patients that treatment will never be curative, and the effects of any drug or treatment will not likely become evident for several months; thus, chronic treatment will be necessary.7
The major treatment options can be categorized as physical modalities that are patient administered, such as shaving and depilation, versus physician- or aesthetician-directed therapy such as oral medications, electrolysis, and laser therapy (Table 90-2). The pharmacologic strategies aim to control the dermatologic symptoms by both lowering androgen levels and controlling the effect of androgens at the tissue level. Lifestyle modification with weight loss and diet changes in patients with PCOS may improve insulin resistance,44
menstrual regularity, and hirsutism score.45
Direct hair removal can be achieved with nonpermanent techniques such as shaving, depilatories (last 12 hours to a few days), waxing, threading and sugaring (last up to 4 weeks), and photoepilation (intense pulsed light), or permanent hair reduction techniques such as electrolysis and laser (photodestruction). Bleaching hair in the affected areas to a similar color as the skin is a form of camouflage used to make hair less obvious. In patients with moderate to severe hirsutism and women with androgen excess, additional medical therapy may be necessary. There is only one prescription medication that is approved for the treatment of unwanted facial hair in women. This drug, topical eflornithine, has been shown to slow down the hair growth cycle and can be used in combination with other hair removal techniques. Eflornithine works through inhibiting ornithine decarboxylase, which results in a shortening of the anagen phase of the hair growth cycle. The major adverse effects of topical eflornithine are burning or tingling of the treated area. First-line medical therapy of hirsutism is oral contraceptives (OCPs), usually in combination with antiandrogens, such as spironolactone and flutamide.
16
Studies with oral ethinyl-estradiol plus cyproterone acetate showed this combination to be superior at control of hyperandrogenism and for the restoration of menstrual regularity in patients with PCOS compared with metformin alone in PCOS patients.46 In studies in which various forms of oral antiandrogens were compared, the effectiveness of finasteride, cyproterone acetate, and flutamide were shown to be equally effective in decreasing hirsutism.47 Glucocorticoids can be considered for women with hirsutism caused by nonclassic CAH who have a suboptimal response to or cannot tolerate oral contraceptives or antiandrogens or who are seeking ovulation induction. In women with severe forms of hyperandrogenemia, such as ovarian hyperthecosis, who have a suboptimal response to oral contraceptives and antiandrogens, gonadotropinreleasing hormone (GnRH) agonists can also be considered. Although the benefit of such therapy can be maintained long term, the initial response may not be evident until 6 to 12 months after the start of therapy. Therefore, to manage patient expectations and to emphasize the importance of maintaining chronic long-term treatment, patients must be made aware of slow clinical response of oral therapies and be followed closely by trained physicians.35
ANDROGEN SUPPRESSION
The androgenic symptoms that may be attenuated by OCPs treatment include hirsutism and acne, primarily through the ability of OCPs to raise sex hormone– binding globulin and lower free testosterone levels. When treating mild to moderate alopecia or hirsutism, combination with an androgen antagonist should be considered as OCPs as monotherapy are not very effective. OCPs containing the second-generation progestin levonorgestrel have been associated with lower venous thromboembolic risk than those containing other progestins.48 When combined with estrogen, Leuprolide, a long-acting GnRH analog, has been shown to decrease hirsutism significantly over OCPs alone,49 and this benefit was greater in PCOS than in idiopathic hirsutism.36
The biological activity of androgens can also be inhibited by androgen receptor blockers. Antiandrogens (cyproterone acetate, chlormadinone acetate, drospirenone, spironolactone, flutamide, and bicalutamide) prevent androgen cellular action by blocking intracellular androgen receptors.50,51 Cyproterone acetate and chlormadinone acetate block androgen receptors in target organs (ovaries and adrenal gland) but also reduce 5α-reductase, which converts testosterone to 5α-dihydrotestosterone, a more potent androgen. Cyproterone acetate has steroidal side effects and can cause abnormalities in liver function and menstrual irregularity. Because of its progestin activity, it needs to be combined with estrogens in women who have a uterus. Spironolactone, a potassium-sparing diuretic that acts as an aldosterone antagonist, is the most studied of the androgen receptor blockers for hirsutism. Because of its androgen-antagonizing activity, it is also
1561
16
MECHANISM OF ACTION DOSAGE ADVERSE EFFECTS COMMENTS
Oral contraceptive pills (OCPs) Suppress ovarian androgen synthesis Increase SHBG
Single pill a day Headaches Migraines Risk of VTE Melasma Alopecia (upon discontinuation)
Spironolactone Competitive inhibitor of AR and 5α-reductase Increases SHBG Decreases androgen synthesis
First-line therapy (in women not seeking to conceive) Contradictions:
■Uncontrolled HTN
■Thromboembolic disorder
■Breast cancer
■Active smoker (absolutely if older than 35 yr)
■Cardiovascular disease
Starting dosage is 50 mg twice daily and may be increased to a total daily dose of 200 mg
Cyproterone acetate Competes with DHT for binding to the androgen receptor
Low dose (2 mg) in OCPs 12.5–100 mg as monotherapy or with estrogen
Flutamide and bicalutamide Nonsteroidal competitive inhibitor of androgen receptor binding
Polyuria Hypotension Headaches Fatigue Syncope Hyperkalemia Irregular menses Teratogen Decreased libido
Avoid combination with other potassium-sparing diuretics and thiazides Contraindicated in patients with renal failure Recommend combination with OCPs Pregnancy Category C
Fluid retention Depression Menstrual irregularities Teratogen Increased risk of liver dysfunction
Not available in the United States Contraindicated during pregnancy and breastfeeding and with liver diseases
Flutamide: 62.5–250mg, twice daily Bicalutamide: 25 mg/day
Teratogen Hepatotoxicity Diarrhea Nausea Vomiting
Recommend combination with OCPs Pregnancy Category D
Glucocorticoids Suppress adrenal function Prednisone: 5-7.5 mg by mouth at bedtime Dexamethasone: 0.5 mg at bedtime
GnRH agonist (Leuprolide acetate, depot suspension)
Suppresses gonadotropin and ovarian androgen secretion
7.5 mg monthly intramuscularly, with 25–50 ug of transdermal estradiol
Ketoconazole Cytochrome P450 enzyme inhibitor and decreases adrenal steroid production
Hyperglycemia Hypertension Cushingoid changes Esophageal reflux and peptic ulcer disease Psychosis and agitation Increased risk of infections Adrenal suppression
Indicated for hirsutism secondary to CAH Not recommended in patients with uncontrolled diabetes and hypertension When used as monotherapy, does not significantly improve hirsutism Pregnancy Category C
Osteoporosis if not combined with estrogen–progestin
Pregnancy Category X
400–600 mg by mouth daily Headache Nausea Hair loss
Pregnancy Category C
Finasteride Inhibits 5α-reductase 1–5 mg by mouth Headaches Decreased libido Pregnancy Category X
Metformin Insulin-sensitizing agent 850 mg twice a day or
Metformin Insulin-sensitizing agent 850 mg twice a day or 500 mg three times a day
500 mg three times a day
Rare lactic acidosis GI distress
Must ensure normal
Rare lactic acidosis GI distress Must ensure normal renal function before starting Pregnancy Category B
renal function before starting Pregnancy Category B
AR, androgen receptor; CAH, congenital adrenal hyperplasia; GI, gastrointestinal; GnRH, gonadotropin-releasing hormone; HTN, hypertension; SHBG, sex hormone–binding globulin; VTE, venous thromboembolic event. Data from Refs. 38 and 41 to 43.
1562
used as a therapeutic modality in androgenetic alopecia in postmenopausal women. It is usually administered in conjunction with OCPs to help to minimize the dysfunctional uterine bleeding that is one of the major side effects of this medication. The beneficial effect may take up to 6 months to observe. Flutamide is used in dosages of 62.5 to 500 mg/day. Because liver toxicity is a potential side effect, serum transaminases should be measured frequently. Other side effects that have been reported include dry skin, diarrhea, nausea, and vomiting. Bicalutamide (a dosage of 25 mg/day) is a new and potent, well-tolerated nonsteroidal pure antiandrogen. It was developed for treating prostate cancer. It has been shown effective in the treatment of patients with PCOS-induced and idiopathic hirsutism.52
However, hepatotoxic effects in the treatment of prostate cancer have been reported starting at doses of 50 mg/day.53
The oral medications finasteride and dutasteride, both 5α-reductase inhibitors, may improve hirsutism by antagonizing the production or biological activity of DHT.
ELECTROLYSIS AND LASERS
Electrolysis and laser hair reduction are the only hair removal methods that may provide permanent hair reduction or long-lasting results. Electrolysis uses a fine needle insertion into individual follicles to destroy the hair follicle via current (galvanic electrolysis), a high-frequency alternating current (thermolysis), or a blend of the two.54 Major disadvantages of this technique include potential scarring, follicular hyperpigmentation, and pain. Because this technique is time consuming, especially with extensive hair growth, and requires a well-trained operator, it can become costly. The regrowth rate of hair with this technique is approximately 40%.50
There have recently been major advances in the field of laser hair removal. Laser treatments remove dark hair quickly through photothermolysis by selectively damaging the pigmented part of the hair follicle. It may take 3 to 6 months before regrowth is evident. Several treatment cycles are required with the spacing between treatments depending on the body area being treated. The most commonly used devices are 755-nm alexandrite laser, 800-nm diode laser, and 1064-nm Nd:YAG (neodymium-doped yttrium aluminum garnet) laser and intense pulsed light sources.55 Laser treatments are less painful and much quicker than electrolysis. Electrolysis is the favored method of treatment for lightly pigmented hair because only anagen hair follicles with dark bulb areas can be destroyed by the light source of laser. The major adverse effects of laser and intense pulsed light include postinflammatory pigmentary change, folliculitis, reactivation of herpes simplex, and paradoxical hypertrichosis, although these are all rare complications when laser is performed by properly trained providers.
16
HYPERTRICHOSIS
AT-A-GLANCE
■ Hypertrichosis is defined as hair growth that is excessive in a localized or diffuse pattern not considered to be in a male pattern distribution.
■ The hair growth in hypertrichosis can be lanugo, vellus, or terminal.
■ Many genetic syndromes have hypertrichosis as a common finding.
■ Metabolic disorders and medications can contribute to the development of hypertrichosis.
■ Therapy should always consist of direct hair removal with or without medical therapy.
INTRODUCTION
INTRODUCTION
Hypertrichosis is defined as hair growth that is considered excessive for age, sex, or ethnicity in areas of the body not considered to be in a pattern of male secondary characteristic. However, it can be seen in both sexual and nonsexual areas.56 Hypertrichosis can be congenital or acquired, and causes include familial factors, medications, and metabolic disorders.57 The hair types seen in hypertrichosis can be lanugo, vellus, or terminal.
CONGENITAL FORMS OF HYPERTRICHOSIS
CONGENITAL FORMS OF
HYPERTRICHOSIS
Congenital forms of hypertrichosis can be localized or diffuse (Table 90-3). The generalized (diffuse) forms tend to occur as a secondary characteristic in a number of well-described syndromes except in the four cases in which the syndrome is defined by the condition of hypertrichosis. The hypertrichosis-defined conditions are congenital hypertrichosis lanuginosa (CHL) and congenital generalized hypertrichosis, osteochondrodysplasia with hypertrichosis (also known as Cantú syndrome), and gingival fibromatosis with hypertrichosis. Congenital hypertrichosis lanuginosa, at times controversially referred to as Ambras syndrome, is a rare, inherited disorder in which an excess of lanugo hair remains over the entire body after birth or may develop in the first few months of life.58 Only the palms, soles, mucous membranes, and glans penis are spared. Some of these patients lose the hair during childhood, but others retain the excess body hair. The disease is very rare with the first reports appearing in the German literature in the 1870s, approximately 50 cases reported in the current world literature, and an estimated incidence of 1 in 10,000,000.59,60 CHL is associated with genetic abnormalities in chromosome 8q
1563
16
ETIOLOGY SPECIFIC DISORDERS
Congenital Disorders Diffuse
Congenital hypertrichosis lanuginosa Congenital generalized hypertrichosis Cantú syndrome Gingival fibromatosis with hypertrichosis Congenital syndromes with secondary hypertrichosis
■Cornelia de Lange syndrome
■Mucopolysaccharidosis disorders
■Hurler Syndrome
■Hunter Syndrome
■Sanfilippo Syndrome
■Stiff skin syndrome
■Winchester syndrome
Localized
■Rubinstein-Taybi syndrome
■Schinzel-Giedion syndrome
■Barber-Say syndrome
■Coffin-Siris syndrome
■Lawrence-Seip syndrome
■Hemimaxillofacial dysplasia
■Craniofacial dysostosis
■Hypomelanosis of Ito Spinal dysraphism Faun tail deformity Congenital nevocellular nevus Congenital Becker nevus Smooth muscle hamartoma Nevoid hypertrichosis Underlying neurofibroma Hypertrichosis cubiti Hemihypertrophy Hairy congenital malformation of palms and soles Hairy pinnae Anterior cervical hypertrichosis
Metabolic Disorders Thyroid disorders Anorexia nervosa Porphyria Malignancy Fetal alcohol syndrome Malnutrition
Medications Dilantin Cyclosporine Glucocorticoids Minoxidil Diazoxide Phenytoin Anabolic steroids Danazol Penicillamine Psoralens Streptomycin Isotretinoin Cetuximab Testosterone Valproic acid. Topical prostaglandin inhibitors
Other
Other Acquired Post-laser hair removal Local pressure or inflammation: casts, lichen simplex, biting, insect bites Human immunodeficiency virus: trichomegaly Acrodynia Infection Dermatomyositis
Post-laser hair removal Local pressure or inflammation: casts, lichen simplex,
Acquired
biting, insect bites Human immunodeficiency virus: trichomegaly Acrodynia Infection Dermatomyositis
1564
(insertion 8q23-24 and deletion 8q23), although other chromosomal abnormalities have been reported.61
Congenital generalized hypertrichosis is similar to CHL in presentation but with terminal hair growth on the body instead of lanugo hair. Only one family has been reported in the literature with this disorder, which is thought to be X-linked with gene mapping to X24-q27.1.62,63
Osteochondrodysplasia with hypertrichosis (Cantú syndrome) is an autosomal dominant disorder characterized by newborns with thick scalp hair and excessive hair growth on the forehead, face, back, and extremities. Some have thick or curly eyelashes. The hypertrichosis usually persists over time. Associated findings include skeletal abnormalities and a variety of cardiac abnormalities.64 The diagnosis is established based on clinical findings and confirmed by detection of a heterozygous pathogenic variant in ABCC9 or KCNJ8.65,66
Gingival fibromatosis with hypertrichosis is a rare genetic syndrome characterized by severe overgrowth of the hair and gums.67,68 Seizures have been reported as part of the syndrome.69 Overlap of the characteristics of this condition with other syndromes have been reported, making the diagnosis of this form of hypertrichosis complicated.70
Of the syndromes in which hypertrichosis is a secondary characteristic, the most commonly reported is Cornelia de Lange syndrome, also known as Brachmann-de Lange syndrome. It is characterized by severe mental retardation, cutis marmorata, frequent limb abnormalities, and characteristic facial features (micrognathia, high palate, low frontal hair line) with the hypertrichosis most prominent as thickened convergent (synophrys) eyebrows with hypertrichotic eyelashes.71,72
The most commonly reported genetic cause of Cornelia De Lange syndrome is a mutation in NIPBL, which accounts for up to 80% of cases, although other gene mutations have been reported to account for the rest of the cases. All the causative genes for this disorder are thought to encode proteins related to cohesion complex function.73,74
The mucopolysaccharidoses (MPS) are a constellation of disorders that result from a deficiency of lysosomal enzymes responsible for glycosaminoglycan metabolism. Several of the MPS are considered to have associated hypertrichosis: Hurler syndrome, Hunter syndrome, and Sanfilippo syndrome.75
Other less common syndromes with the secondary characteristic of diffuse hypertrichosis are listed in Table 90-3.
LOCALIZED CONGENITAL HYPERTRICHOSIS
LOCALIZED CONGENITAL
HYPERTRICHOSIS
Congenital hypertrichoses localized to a single body part include hypertrichosis cubiti (hairy elbows), hairy pinna, anterior cervical hypertrichosis, hairy polythelia (hair tufts along the mammary line), overlying plexiform neurofibromas with spinal dysraphism (when
presenting over the sacral midline, it is called “faun tail deformity”) in association with congenital nevi, and occasionally in association with Becker nevi.76 They can be present at birth or soon thereafter, but many of these disorders present later in childhood.77 When any of these disorders are found in the midline, it is imperative to look for underlying neurologic deficits and spinal deformities.78
OTHER ACQUIRED FORMS OF HYPERTRICHOSIS
OTHER ACQUIRED FORMS
OF HYPERTRICHOSIS
There is a long list of medications that can cause hypertrichosis (see Table 90-3), so a full medical history can easily identify the culprit (Fig. 90-6). Porphyria and other metabolic disorders are important forms of acquired hypertrichosis. The most common porphyrias to cause hypertrichosis are porphyria cutanea tarda and erythropoietic porphyria (Gunther disease), but hereditary coproporphyria and variegate porphyria may produce excessive hair growth as well.79
TREATMENT
TREATMENT
The treatment of hypertrichosis mirrors that of hirsutism. The general approach to treatment will differ based on the patient age, ethnicity, and extent of hair.80
For situations when there is an underlying metabolic process or a medication is involved, the underlying cause should be addressed. For other conditions in which the hair is persistent, treatments can be divided into depilatory methods (removal of hair along the hair shaft) and epilatory methods (removal of the entire hair shaft including the hair bulb).75 Depilatory methods include mechanical and chemical methods of removal, such as shaving, waxing, sugaring, threading,
16
tweezing, and chemical depilation. These methods are all temporizing and can produce mild to moderate pain or irritation of the treated skin. For more permanent hair removal, electrolysis and laser can be used. Although permanent hair reduction has improved in efficacy over the past 2 decades, the achievement of complete permanent hair removal remains elusive. Electrolysis for extensive cases can be time consuming, and appropriately trained operators can be difficult to find.81
Laser hair reduction has been used successfully in treating various forms of hypertrichosis but can also be time consuming and expensive.82,83
Laser hair epilation can rarely lead to paradoxical hypertrichosis, so this must be considered as well.84
When considering recommendations for hair removal, it is important to underscore the possibility of injury with both in-the-home and professionally performed treatments. Between the years 1994 and 2014, there were nearly 300,000 hair removal–related injuries seen in U.S. emergency departments. There were nearly equal numbers of men and women presenting for injuries, with 60% of the injuries occurring at home. Because this study only examined the injuries severe enough to present for treatment and tabulated only injuries caused by scissors, clippers, and razors, it is likely that hair-removal injury rates are actually much higher than reported.85
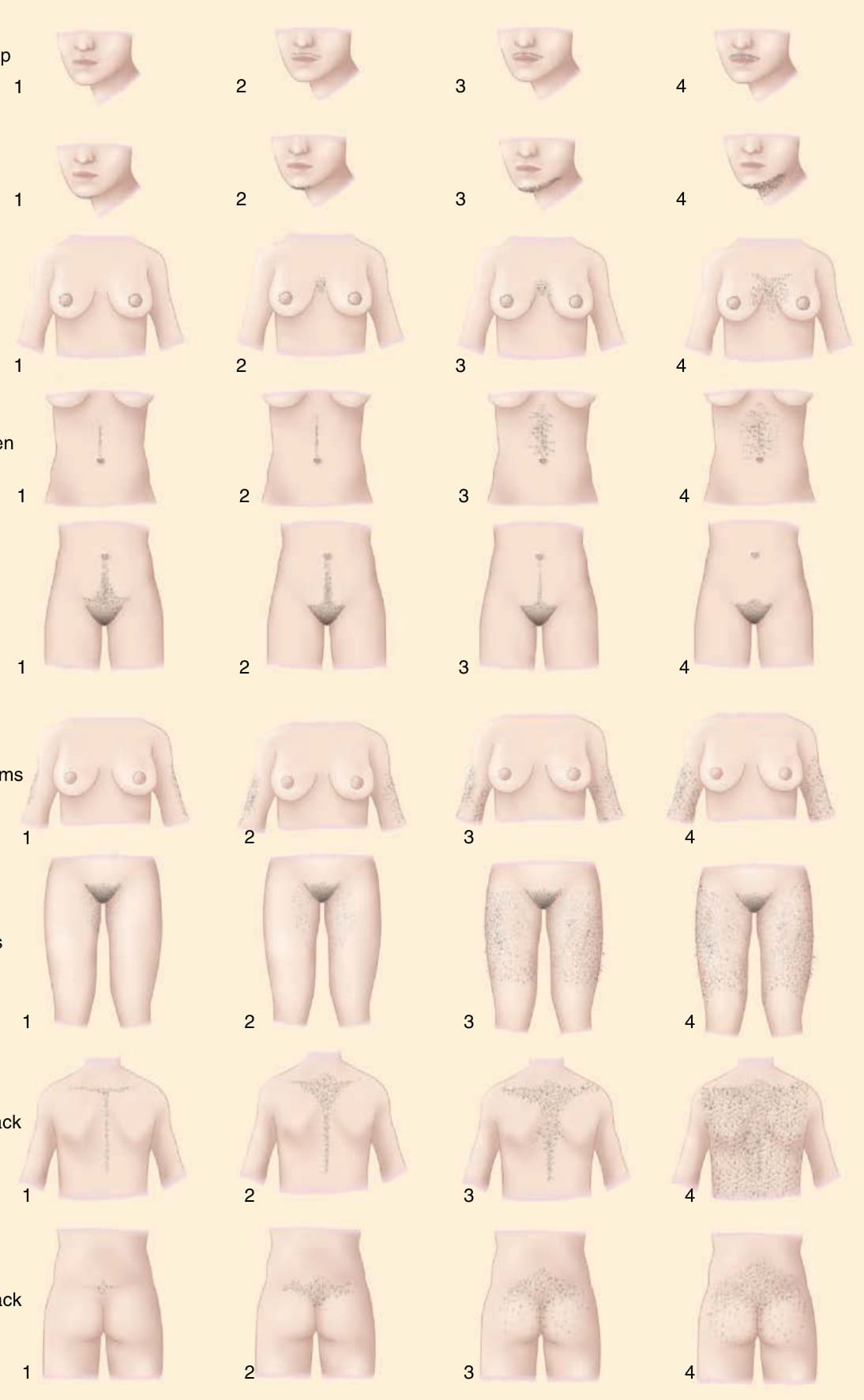
Figure 90-1 The Ferriman-Gallwey scale.

Figure 90-2 Dark terminal hair of the upper lip and chin in a middle-age woman.

Figure 90-3 Hirsutism of the lateral face and jawline in the young woman.

Figure 90-4 Hirsutism of the chin with associated pseudofolliculitis barbae.
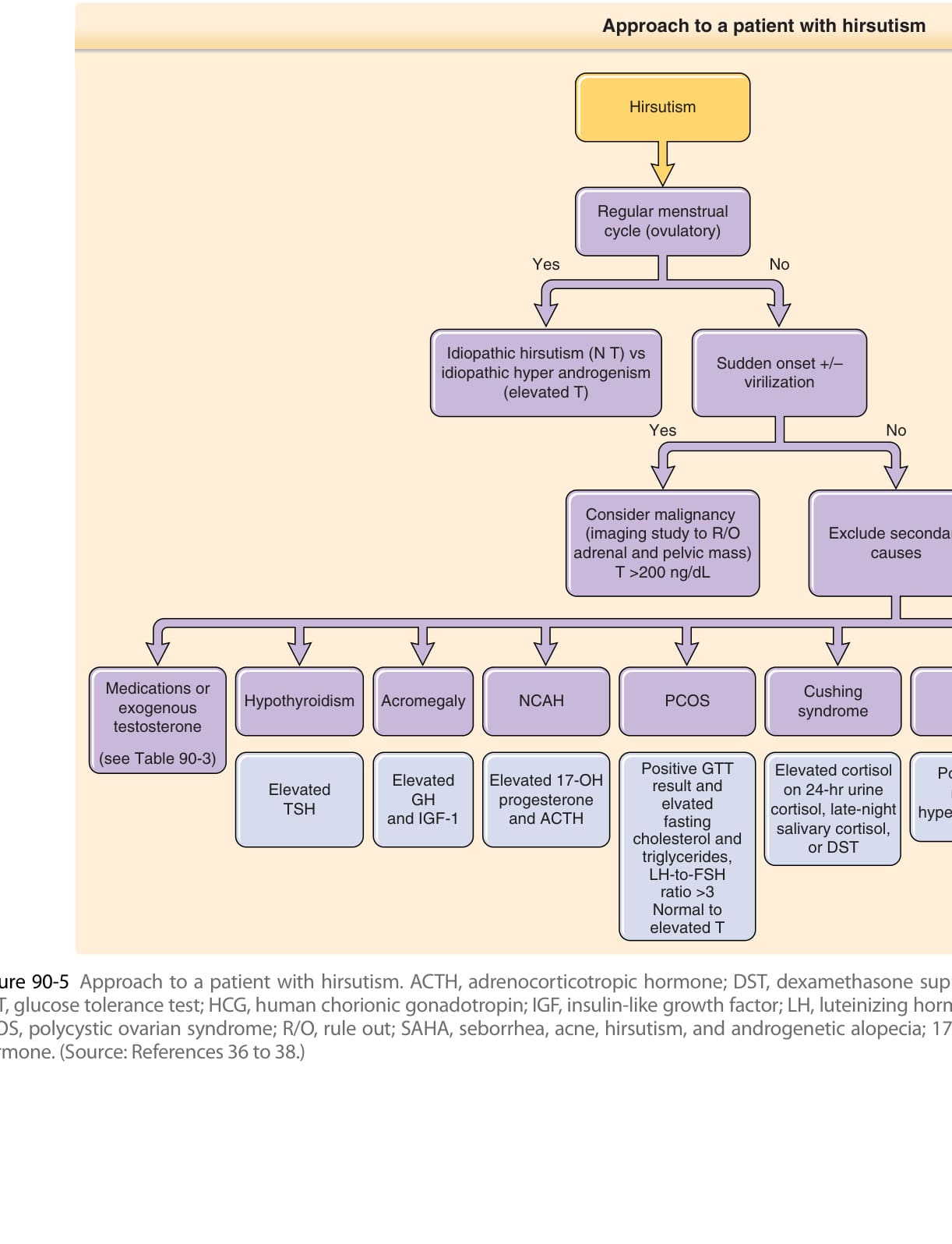
Figure 90-5 Approach to a patient with hirsutism. ACTH, adrenocorticotropic hormone; DST, dexamethasone suppression test; FSH, follicle-stimulating hormone; GH, growth hormone; GTT, glucose tolerance test; HCG, human chorionic gonadotropin; IGF, insulin-like growth factor; LH, luteinizing hormone; NCAH, non-classical adrenal hyperplasia; NT, normal testosterone; PCOS, polycystic ovarian syndrome; R/O, rule out; SAHA, seborrhea, acne, hirsutism, and androgenetic alopecia; 17-OH, 17-hydroxyprogesterone; T, testosterone; TSH, thyroid-stimulating hormone. (Source: References 36 to 38.)

Figure 90-6 Hypertrichosis of the forehead in a patient applying topical minoxidil to the scalp.
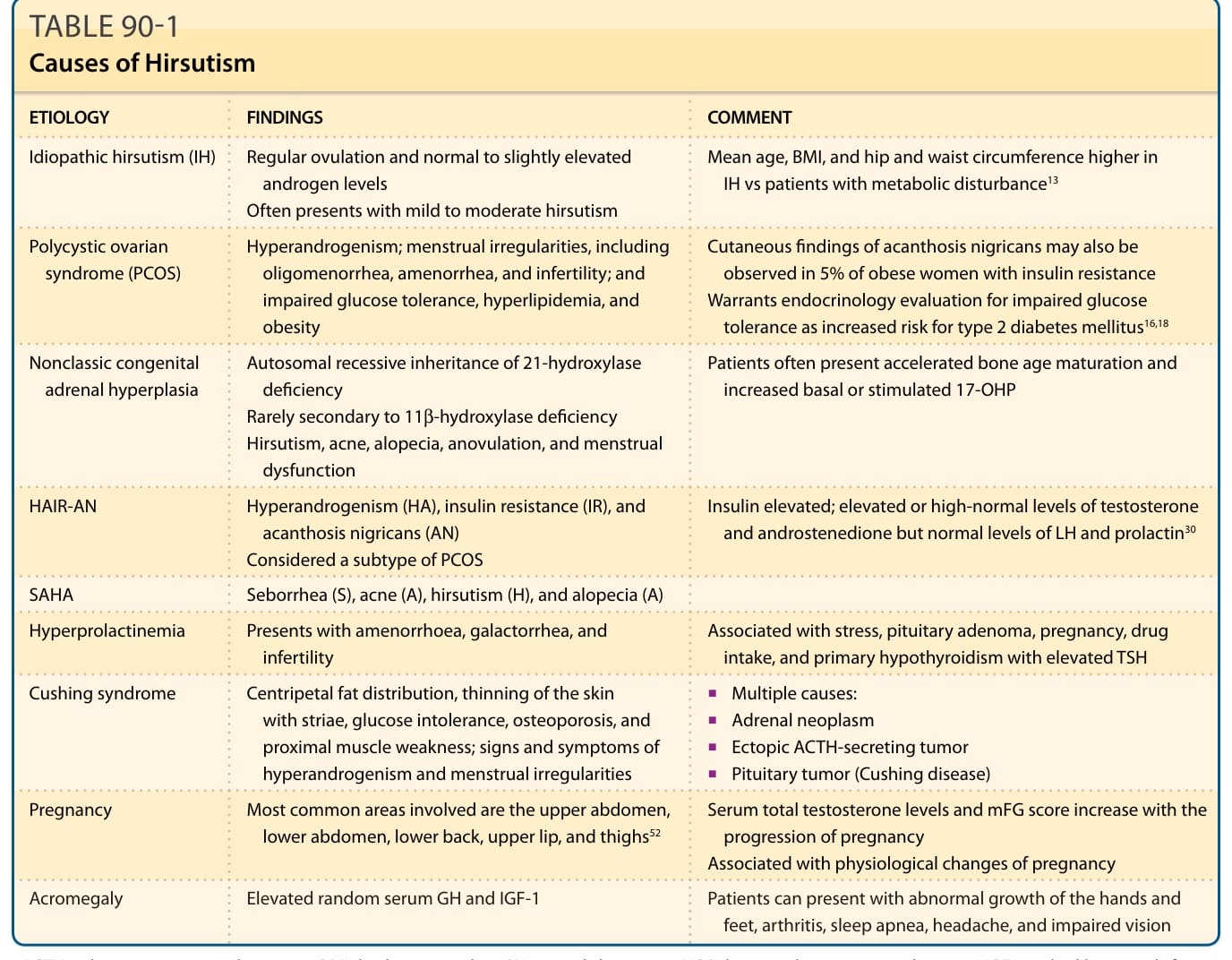
TABLE 90-1 Causes of Hirsutism
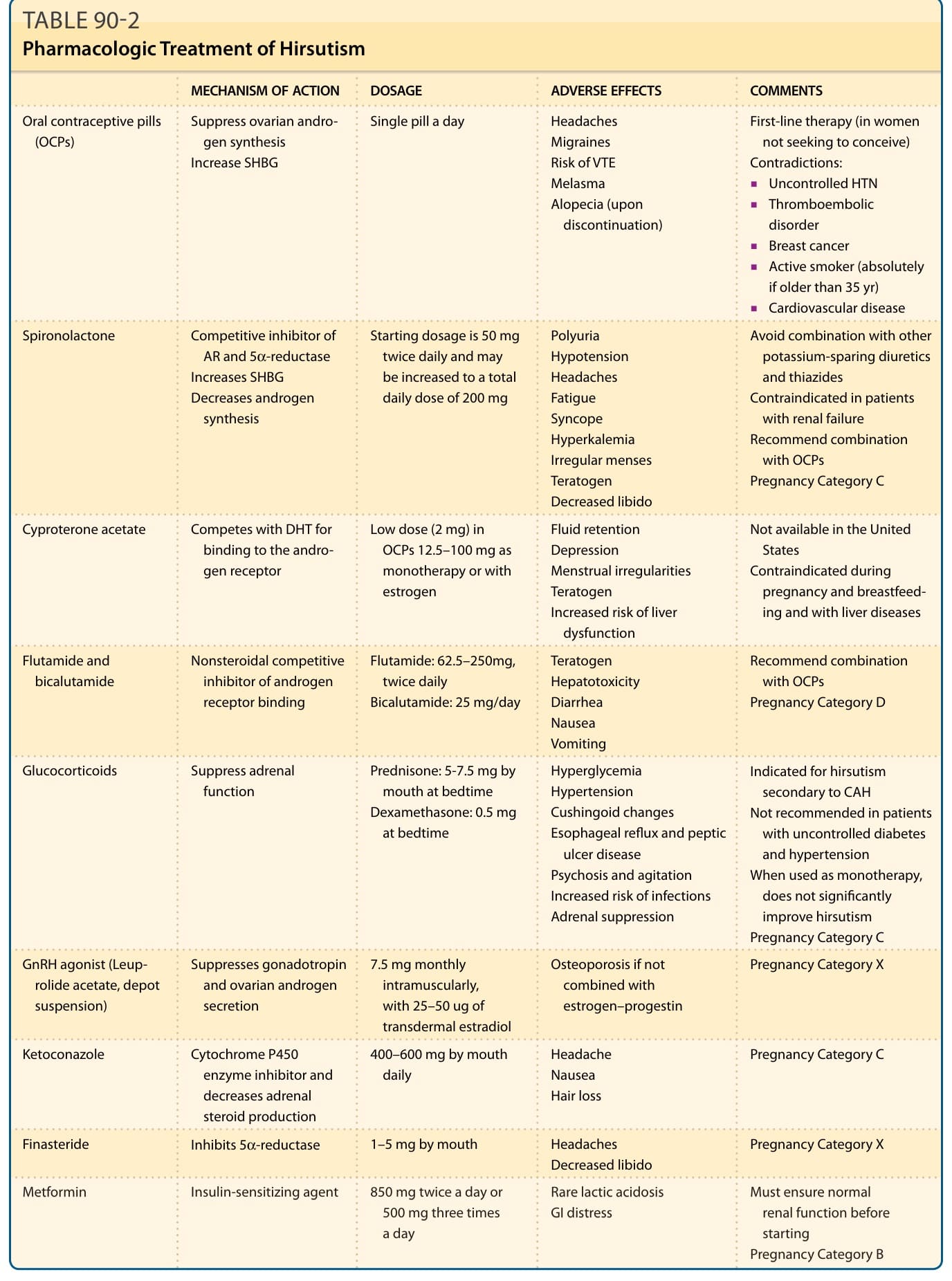
TABLE 90-2 Pharmacologic Treatment of Hirsutism
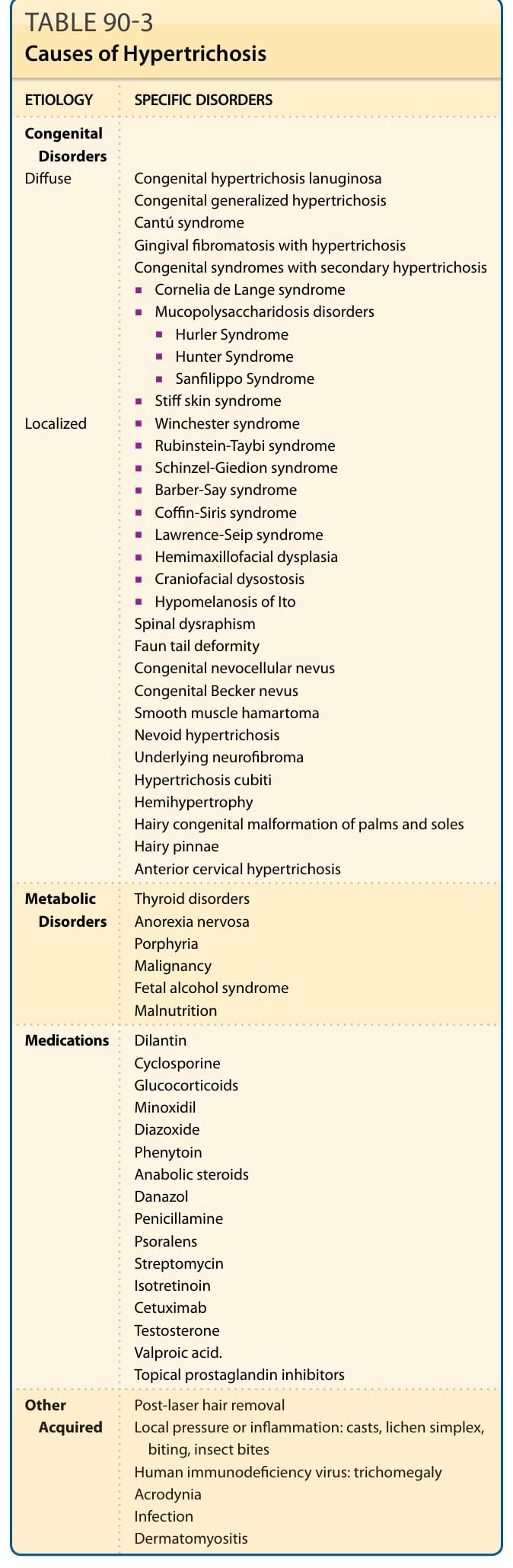
TABLE 90-3 Causes of Hypertrichosis