Cicatricial Alopecias
16
AT-A-GLANCE
■ Scarring alopecia occurs in a heterogeneous etiologic group of various disorders.
■ The inflammatory process leads to permanent destruction of hair follicular stem cell structure and subsequent replacement with fibrous tissue.
■ The destructive process can occur as a primary or secondary cicatricial alopecia.
■ Loss of hair-producing attribute finalizes this process and results clinically in permanent alopecia.
■ No evidence-based treatment is available.
Cicatricial or scarring alopecias comprise a diverse group of scalp disorders that result in permanent hair loss (Fig. 88-1). The destructive process can occur as a primary or secondary cicatricial alopecia. Primary cicatricial alopecia refers to a group of idiopathic inflammatory diseases, characterized by a folliculocentric inflammatory process that ultimately destroys the hair follicle. Secondary cicatricial alopecias can be caused by almost any cutaneous inflammatory process of the scalp skin or by physical trauma, which injures the skin and skin appendages. Regardless of whether a cicatricial alopecia is primary or secondary in nature, all scarring alopecias are characterized clinically by a loss of follicular ostia and pathologically by a replacement of hair follicles with fibrous tissue. Cicatricial alopecias are psychosocially distressing for the affected patient and medico-surgically challenging for the treating physician.
PRIMARY CICATRICIAL ALOPECIAS
EPIDEMIOLOGY
EPIDEMIOLOGY
Inflammatory cicatricial alopecias are rare skin diseases. The epidemiology is basically unknown.
CLASSIFICATION1
CLASSIFICATION
1
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
Little is known about most of the etiologies. Hence the exact mechanisms that cause follicle stem cell destruction are not completely understood, and there is no cure as of this writing. Primary cicatricial alopecias are characterized by an inflammatory infiltrate affecting the upper, permanent portion of the follicle referred to as the infundibulum, and below it, the isthmus of the follicle. The isthmus is the home of pluripotent hair stem cells, which are found in the bulge region where the arrector pili muscle attaches to the outer root sheath. Pluripotent hair follicle stem cells are responsible for the renewal of the upper part of the hair follicle and sebaceous glands, and for the restoration of the lower cyclical component of the follicles at the onset of a new anagen period.1,2 Damage to the bulge area and the sebaceous gland with the isthmus may result in an incomplete hair cycle and can be associated with chronic follicular inflammation and foreign-body reaction.3 It has been assumed that scarring hair loss is a consequence of damage to the isthmus, affecting either stem cells or sebaceous glands.4-7
CLINICAL FEATURES
CLINICAL FEATURES
Primary cicatricial alopecia usually affects the central and parietal scalp before progressing to other sites of the scalp. Isolated alopecic patches showing atrophy and a lack of follicular ostia with inflammatory changes, such as diffuse or perifollicular erythema, follicular hyperkeratosis, pigment changes, tufting, and pustules, provide hints to the diagnosis.8,9 However, clinically visible inflammatory change might be absent in the affected lesions and may present histologically as inflammatory infiltrates in the deep dermis and subcutaneous tissue.
DIAGNOSIS
DIAGNOSIS
Diagnostic tools such as a 10-fold magnifying dermatoscope with and without polarized light can help to identify the presence or absence of follicular ostia, perifollicular erythema, and follicular hyperkeratosis in the affected areas. A thorough examination of the entire scalp, a detailed clinical history, as well as skin biopsies of an
16
Alopecia subtypes
Alopecia
Diffuse
Failure of follicle production
Nonscarring
Hair shaft abnormality
Production decline
Abnormality of cycling
-
Triangular alopecia
-
Male/female pattern hair loss
-
Telogen effluvium
-
Anagen effluvium
-
Loose anagen syndrome
-
Alopecia areata (diffuse)
Hair breakage
- Trichotillomania
- Traction alopecia
- Infection
- Shaft abnormality
Unruly hair
Abnormality of cycling
- Alopecia areata
- Syphilis
active lesion are crucial in the correct diagnosis of most cicatricial alopecias. Patient-reported symptoms, such as itching or pain, might be used as approximate indicators of disease activity but also can be completely absent. Presence of other indirectly related symptoms, such as sun sensitivity, can also help support a particular diagnosis (eg, discoid lupus erythematosus [DLE]). A scalp biopsy is necessary to confirm a scarring alopecia diagnosis. The following recommendations were developed at the consensus meeting on cicatricial alopecia1 in February 2001: One 4-mm punch biopsy including subcutaneous tissue should be taken from a clinically active area, processed for horizontal sections and stained with hematoxylin and eosin. Elastin (acid alcoholic orcein), mucin, and periodic acid–Schiff stains
Focal
Scarring
Primary Cicatricial
Secondary Cicatricial
Lymphocytic
Infection
Traumatic hair loss
-
Discoid lupus erythematosus
-
Lichen planopilaris/ Frontal fibrosing alopecai
-
Classic pseudopelade of Brocq
-
Central centrifugal cicatricial alopecia
-
Alopecia mucinosa
-
Keratosis follicularis spinulosa decalvans
-
Traumatic injuries
-
Traction alopecia
-
Trichotillomania
-
Pressure alopecia
Neutrophilic
- Folliculitis decalvans
- Dissecting folliculitis
Mixed
- Acne keloidalis nuchae
- Acne necrotica
- Erosive pustular dermatosis
may provide additional diagnosis-defining information. A second 4-mm punch biopsy from a clinically active disease-affected area should be cut vertically into 2 equal pieces. One half provides tissue for transverse cut routine histologic sections, and the other half can be used for direct immunofluorescence studies.10-12
PROGNOSIS/CLINICAL COURSE
PROGNOSIS/CLINICAL
COURSE
Once the hair follicle is destroyed and replaced by fibrous tissue, there is no hope for hair regrowth.
1525
16
Lymphocytic Primary Cicatricial Alopecia
■Chronic cutaneous lupus erythematosus (discoid lupus erythematosus)
■Lichen planopilaris
■Classic lichen planopilaris
■Frontal fibrosing alopecia
■Graham-Little syndrome
■Classic pseudopelade of Brocq
■Central centrifugal cicatricial alopecia
■Alopecia mucinosa
■Keratosis follicularis spinulosa decalvans
Neutrophilic Primary Cicatricial Alopecia
■Folliculitis decalvans
■Dissecting cellulites/folliculitis (perifolliculitis abscedens et suffodiens)
Mixed Cicatricial Alopecia
Mixed Cicatricial Alopecia
■Folliculitis (acne) keloidalis
■Folliculitis (acne) keloidalis
■Folliculitis (acne) necrotica
■Folliculitis (acne) necrotica
■Erosive pustular dermatosis
■Erosive pustular dermatosis
Various medical treatment options may fail and the inflammatory process may continue and leave the patient with a disfiguring permanent alopecia.
TREATMENT
TREATMENT
The main goal in treating primary cicatricial alopecia is to stop the inflammation and further progression of the disease. If hair loss is already extensive and/ or medical treatment fails, patients should be advised about camouflage techniques, such as hairpieces and wigs. Women with extensive scarring lesion on the crown and vertex benefit highly from a well-designed hairpiece, which can look very natural, particularly if the frontal hair line is preserved and is usually more comfortable to wear than a full wig. Hair restoration surgery, including hair transplantation and scalp reduction, can be an option for burned out cicatricial alopecia. No disease activity should occur on the scalp for at least 1 year after therapy after which hair restoration surgery can begin. The patient has to be warned about a possible limited graft survival and disease recurrence, which seems to be higher in neutrophilic primary scarring alopecia.
LYMPHOCYTIC PRIMARY CICATRICIAL ALOPECIAS
LYMPHOCYTIC PRIMARY
CICATRICIAL ALOPECIAS
CHRONIC CUTANEOUS LUPUS ERYTHEMATOSUS (DISCOID LUPUS ERYTHEMATOSUS)
DLE, together with lichen planopilaris (LPP), is the most common cause of inflammatory cicatricial
1526
alopecia.8 Females are more often affected than males and the disease is more common in adults (with first onset typically at 20 to 40 years of age) than in children.13-15 Of patients with DLE, approximately 26% to 31% of children and 5% to 10% of adults will develop systemic lupus erythematosus.15,16 Patients with DLE also have a higher incidence of concurrent alopecia areata. Moreover, DLE also is associated with verruciform xanthoma and papulonodular dermal mucinosis.17
Clinical Presentation: DLE usually presents with 1 or more erythematous, atrophic, and alopecic patches on the scalp. Follicular hyperkeratosis, hyperpigmentation, hypopigmentation, and telangiectasia can be present.3,18 Hyperpigmentation is frequently found in the center of the lesion. Active lesions can be sensitive or pruritic, and the patient might report a worsening after ultraviolet light exposure (Fig. 88-2).
Pathology: Characteristic features of early, active DLE lesions are lymphocyte-mediated interface dermatitis with vacuolar degeneration of the basal cell layer and necrotic keratinocytes, a thickening of the basement membrane and destruction of sebaceous glands. Elastic fibers are frequently destroyed throughout the reticular dermis.5,10 The lymphocytic infiltrate is predominantly found in the upper part of the follicle but also can be found in deeper parts of the follicle, in the interfollicular epidermis, and around the periadnexal vessels.19-22 Direct immunofluorescence typically shows a linear granular deposition of immunoglobulin (Ig) G and C3 at the dermoepidermal junction. IgM, C1q, and, rarely, IgA also can be found.
Management and Treatment: Hydroxychloroquine at a dose of 200 to 400 mg daily in adults or 4 to 6 mg/kg in children is highly effective at managing. A baseline ophthalmologic examination and complete blood count is required before the therapy is started.13,15 Bridge therapy with oral prednisone (1 mg/kg) tapered over the first 8 weeks of treatment might be helpful in adult patients with rapidly progressive disease.8,9 In limited or slowly progressive DLE, intralesional triamcinolone acetonide should be used at a concentration of 10 mg/mL every 4 to 6 weeks, alone or in addition to oral therapy.8 Intralesional triamcinolone acetonide can
be used with or without topical class I or class II corticosteroids. Topical corticosteroids alone also are effective at managing in milder forms of DLE.9,10,15,20 Oral acitretin and isotretinoin have also shown some effectiveness at managing.23,24 Immunosuppressive therapies, such as mycophenolate mofetil, methotrexate, and azathioprine, should only be considered if the above therapies fail. Multimodal aggressive therapy in rapidly progressive DLE might reverse early alopecic patches and save hair follicles from the destructive process.25
LICHEN PLANOPILARIS AND FRONTAL FIBROSING ALOPECIA
LPP is a follicular variant of lichen planus. Together with DLE, this is the most common cause of primary cicatricial alopecia. LPP can be divided into classic LPP, Graham-Little syndrome, and frontal fibrosing alopecia (FFA). The typical age of onset of classic LPP is around the fifth decade, and women are more often affected than men. Extracranial lichen planus may occur in up to 28% of patients.6,26,27 Graham-Little syndrome is a very rare condition that predominantly affects female adults. It is characterized by LPP of the scalp, noncicatricial of the eyebrows, axilla, and groin, and keratosis pilaris. FFA was first described by Kossard in 1992.28 FFA predominantly affects postmenopausal women. However, some cases of affected men or premenopausal women are reported.29-31 Although as of this writing there are no epidemiologic data on the incidence or prevalence of FFA, FFA seems to be fast on the rise. In many hair clinics, FFA has become the most frequently seen form of cicatricial alopecia.32 Causes and trigger factors and whether FFA is a variant of LPP or its own entity is as of this writing unknown. Lichenoid drug eruptions can be triggered by many drugs. Some of the most common drugs that cause lichenoid drug eruption are gold, antimalarials, and captopril. Actinic lichenoid drug eruption is confined to sun-exposed sites. The most likely drugs to cause lichenoid drug eruption are quinine and thiazide diuretics.33-35 Whether drugs play a role as trigger factors in LPP and FFA is not clear.
Clinical Presentations of Lichen Plano- pilaris and Frontal Fibrosing Alopecia: Classic LPP typically starts at the crown and vertex area. In classic LPP, the affected areas usually show perifollicular erythema and follicular hyperkeratosis. The alopecic areas of LPP are often smaller, irregularly shaped and interconnected, which can lead to a reticulated clinical pattern as compared to DLE. However, overlapping clinical features with those of DLE are frequently seen. Patients complain about itching, burning sensations and sensitivity of the scalp (Fig. 88-3). FFA is characterized by a frontal, band-like or circumferential scarring alopecia.5 In some cases, a few hairs are spared in the original frontal hairline. Follicular hyperkeratosis and perifollicular erythema may
16
be found in a band-like pattern in the frontal hairline. Alopecia of the eyebrows is also frequently seen in FFA (Fig. 88-4). Graham-Little syndrome presents with lesions of classic LPP on the scalp, nonscarring alopecia of axillae, pubic area, and eyebrows, as well as keratosis pilaris of the trunk and extremities.
Pathology: LPP and FFA show similar histopathologic features. A lymphocytic infiltrate and interface dermatitis are predominantly found in and around the upper permanent part of the hair follicle. Unlike DLE, the vascular plexus is not affected by inflammation and mucin deposits are absent.5 Direct immunofluorescence typically shows globular cytoid depositions of IgM, and, rarely, IgA, IgG, or C3, in the dermis around the infundibulum.36
Management and Treatment: First-line treatment for moderately active classic LPP lesions is intralesional triamcinolone acetonide at a concentration of 10 mg/mL every 4 to 6 weeks or in combination with topical class I or class II corticosteroids.8,24 For FFA
1527
16
near the face, triamcinolone acetonide at 2.5 mg/mL injected 1 cm behind the hair line should be used. Topical minoxidil may be given in patients with concomitant androgenetic alopecia to improve thickness of the remaining hair. Newer studies suggest preliminarily that injections of platelet-rich plasma might be useful as additional treatment.37 More studies are required. Studies on the efficacy of oral medication are limited. Oral cyclosporine, retinoids, antimalarials, and griseofulvin3,18,38-41 have a positive effect in patients with rapidly progressive LPP. Oral corticosteroids as bridge therapy in the first weeks of treatment might be considered in very active cases. The treatment of Graham-Little syndrome is typically similar to the management of classic LPP. In FFA a lower dose of intralesional triamcinolone acetonide (2.5 to 5 mg/mL) and topical application of minoxidil or topical tacrolimus can be considered, although no effective treatment has yet been reported.
CLASSIC PSEUDOPELADE OF BROCQ
Pseudopelade of Brocq (PPB) is classified as an idiopathic lymphocytic primary cicatricial alopecia that predominantly affects the scalp. Women between 30 and 50 years of age are most frequently affected.6
Clinical Presentation: PPB usually affects the vertex and occipital area of the scalp. It presents with small flesh-toned alopecic patches with irregular margins. This pattern has been described as “foot prints in the snow.”42 PPB can also present as a noninflammatory, centrifugally spreading, patch of alopecia, which might be seen as a variant of central centrifugal cicatricial alopecia (CCCA) in whites. Follicular hyperkeratosis and perifollicular or diffuse erythema are mostly absent.18 Clinically, the features may overlap with LPP. Pathology: Early PPB lesions typically show a sparse to moderate lymphocytic infiltrate around the follicular infundibulum with a complete destruction of the sebaceous glands.43 In later disease stages, hair follicles are completely replaced by fibrous tracts. Unlike DLE and LPP, interface dermatitis is usually absent and the elastic fibers are preserved and thickened in PPB.44
Management and Treatment: Intralesional triamcinolone acetonide at a concentration of 10 mg/mL every 4 to 6 weeks in combination with topical corticosteroids is the treatment of first choice. Hydroxychloroquine, oral prednisone, and isotretinoin have shown some effectiveness in treating PPB.6,18,45,46
CENTRAL CENTRIFUGAL CICATRICIAL ALOPECIA
CCCA is the most common form of primary cicatricial alopecia in women of African descent. The etiology of CCCA is not fully understood. An autosomal mode of inheritance, chemical hair grooming practices, and traction-inducing hair styles seem to be the
1528
major pathogenic factors.20,47-50 CCCA is rarely seen in whites (sometimes called “central elliptical pseudopelade”) and African American men. Because of clinical and histopathologic similarities, there is a debate as to whether or not CCCA is a variant of PPB.
Clinical Presentation: CCCA presents with a skin-colored patch of scarring alopecia on the crown, gradually progressing centrifugally to the parietal areas. In 2008, Olsen and associates developed a photographic scale to identify the pattern and severity of CCCA in the general community.51 Perifollicular hyperpigmentation and polytrichia might be present.8
Patients may complain about pain, itching, tenderness, and “pins-and-needle” sensations (Fig. 88-5).52
Pathology: Pathologic features of CCCA include dermal hyalinization, hair fiber granulomas, loss of follicular epithelium, follicular lymphocytic inflammation of the lower infundibulum and up to the isthmus, premature desquamation of the inner root sheath, and fibrous connective tissue. Similarities to PPB have been discussed.3,20
Management and Treatment: Early diagnosis is crucial in the management of CCCA. Early screening is suggested because CCCA has been described in children.53 More natural, less traumatizing hair care practices are recommended.10,18,54,55
Screening of family members also may be useful because of the genetic pathogenicity.48 Topical and intralesional corticosteroids, and tetracycline are effective in active progressive cases.20 Systemic treatment with tetracyclines, hydroxychloroquine, immunosuppressive medication (eg, mycophenolate mofetil and cyclosporine), and antiandrogens also have been described to be successful.55 Wigs and hairpieces can help camouflage the alopecia and are frequently used by women with CCCA.
ALOPECIA MUCINOSA
Alopecia mucinosa can present as indurated, welldemarcated erythematosus or skin-colored patches of scarring or nonscarring alopecia that can be accompanied by diffuse hair loss56 and alopecia of the eyebrows.57 Grouped follicular papules, follicular cysts, and follicular hyperkeratosis may be present in some cases. Early lesions of alopecia mucinosa show mucin deposition in the outer root sheath and replacement of the entire pilosebaceous unit by pools of mucin in more advanced lesions.5,57 Strictly speaking, alopecia mucinosa is not a primary cicatricial alopecia because the hair follicle is not replaced by a true scar.5
Alopecia mucinosa can occur idiopathically or in the setting of cutaneous T-cell lymphoma or mycosis fungoides.58 Cell atypia and monoclonal populations of T-lymphocytes can be present in the idiopathic form of alopecia mucinosa as well as in mycosis fungoides.58
Management and Treatment: A complete workup is necessary to rule out an underlying malignancy such as mycosis fungoides and Sézary syndrome, its advanced end point. Oral corticosteroids, minocycline, and isotretinoin are effective. Topical and intralesional corticosteroids, dapsone, indomethacin, and light therapy also have been used with variable outcomes.59
KERATOSIS FOLLICULARIS SPINULOSA DECALVANS
Keratosis follicularis spinulosa decalvans together with keratosis atrophicans faciei (also called ulerythema ophryogenes or keratosis pilaris rubra atrophicans faciei) and atrophoderma vermiculata belongs to a heterogeneous group of congenital follicular keratinizing disorders. Keratosis follicularis spinulosa decalvans is X-linked, usually develops during adolescence, and mostly presents with scarring alopecic patches, follicular hyperkeratosis, and, rarely, pustules.5 Eyebrow and eyelash involvement also can be present. Keratosis follicularis spinulosa decalvans shows an inflammatory infiltrate consisting of lymphocytes and neutrophils in the infundibular area in early lesions. Later, the infiltrate is predominantly lymphocytic and the follicle is eventually replaced by fibrous tissue. The condition may improve with age. Careful calculation of risks and benefits in the treatment of children, teenagers, and young adults is important. Topical and intralesional corticosteroids as well as oral retinoids have shown some effectiveness.60
NEUTROPHILIC PRIMARY CICATRICIAL ALOPECIA
NEUTROPHILIC PRIMARY
CICATRICIAL ALOPECIA
FOLLICULITIS DECALVANS
Approximately, 11% of all primary cicatricial alopecia cases are diagnosed with folliculitis decalvans (FD).3,6
16
FD predominantly occurs in young and middle-aged adults with a slight preference for the male gender. A bacterial infection involving Staphylococcus aureus, in combination with hypersensitivity reaction to “superantigens” and defect in host cell–mediated immunity have all been suspected as possible pathogenetic factors.3,61,62
Clinical Presentation: FD frequently starts at the vertex area of the scalp with erythematous alopecic patches, follicular pustules and follicular hyperkeratosis. Tufted folliculitis is typically found in FD but can also occur in other cicatricial inflammatory alopecias. Tufted folliculitis is characterized by multiple hairs (5 to 15) emerging from a single, dilated, follicular orifice. In older lesions, pustules might be absent but progressive scarring may still continue (Fig. 88-6). An overlap with acne keloidalis is possible as some patients with acne keloidalis not only develop cicatricial lesion on the nape of the neck but also develop progressive cicatricial alopecia that resembles FD in other areas of the scalp. Patients frequently complain about pain, itching, and/or burning sensations.
Pathology: Early lesions are characterized by keratin aggregation in the infundibulum with numerous intraluminal neutrophils, as well as an intrafollicular and perifollicular neutrophilic infiltrate.3,5,18 Sebaceous glands are destroyed early. In advanced lesions, the infiltrate may consist of neutrophils, lymphocytes, and plasma cells, and extend into the dermis.8,18 Hairshaft granulomas with foreign-body giant cells are frequently found.3,18 In end-stage lesions, follicular and interstitial dermal fibrosis, as well as hypertrophic scarring, can be observed.18
Management and Treatment: Treatment of FD in general is difficult and disease activity can be noted over many years. Bacterial cultures with the testing of antibiotic sensitivities are recommended. Eradication of S. aureus with minocycline, erythromycin, cephalosporins, and sulfamethoxazole-trimethoprim has shown some effectiveness. Relapse can often be observed after the antibiotics are discontinued.9,61,63 If so, the patient might have to stay on low-dose antibiotics for many years. Although rifampin in combination
1529
16
with clindamycin has shown good response, this combination also has shown a higher incidence of side effects.61,64 Oral fucidic acid alone or in combination with other agents has also shown to be effective in some patients.65 Oral therapy should be combined with topical antibiotics such as mupirocin, 1.5% fusidic acid, and 2% erythromycin,64,65 and antibacterial cleansers. Intralesional triamcinolone acetonide at a concentration of 10 mg/mL every 4 to 6 weeks might help to reduce the inflammation and symptoms such as itching, burning, and pain.6,9 Intranasal eradication of S. aureus with topical antibacterial agents are described as useful.18
DISSECTING FOLLICULITIS
Dissecting folliculitis (or dissecting cellulites or perifolliculitis capitis abscedens et suffodiens of Hoffman) is related to acne conglobata and hidradenitis suppurativa. These 3 diseases have been described as the follicular occlusion triad. Dissecting folliculitis predominantly occurs in young men between 18 and 40 years of age.8 African American men seem to be more commonly affected than white men. The pathogenesis of dissecting folliculitis may include follicular occlusion, seborrhea, androgens, and secondary bacterial overpopulation, as well as an abnormal host response to bacterial antigens.66-73
Clinical Presentation: Dissecting folliculitis typically presents with fluctuating nodules, abscesses, and sinuses, which frequently show spontaneous discharge of pus, as well as with erythematous, follicular papules and pustules. Initial lesions are mostly found on the vertex and occipital scalp. Multifocal lesions can form an intercommunicating ridge and seropurulent exudates can be discharged when pressure is applied to 1 region of the scalp (Fig. 88-7). The lesions can be pruritic and tender. Chronic and relapsing courses results in cicatricial alopecia that can occur as hypertrophic or keloidal scars.73
Pathology: The main histologic feature is an intrafollicular and perifollicular neutrophilic infiltrate with follicular occlusion in early lesions.5 In more advanced
1530
stages, interconnecting sinus tracts lined by squamous epithelium, follicular perforation, and perifollicular and deep dermal abscesses are typical findings.5,18,22
Management and Treatment: Multimodal treatment has been reported with successful results, such as systemic antibiotics (minocycline, tetracycline, cloxacillin, erythromycin, cephalosporin, or clindamycin with or without rifampin), intralesional corticosteroids, and oral prednisolone.74,75 The benefits of systemic antibiotics are most likely a result of their antiinflammatory effects rather than their antibacterial action. Isotretinoin at a dose of 0.5 to 1 mg/kg/day prolongs remission.76,77 Incision and drainage of therapy-resistant, painful nodules, marsupialization with curettage of the cyst wall, and complete scalp extirpation with skin grafting have been reported, but should be an exception for extreme and therapy refractory cases.77-80
MIXED PRIMARY CICATRICIAL ALOPECIAS
MIXED PRIMARY
CICATRICIAL ALOPECIAS
ACNE KELOIDALIS NUCHAE
Acne keloidalis nuchae predominantly occurs in African American men 14 to 25 years of age. This idiopathic primary cicatricial alopecia might be triggered by trauma (shirt collars) or infection (Demodex or bacteria). Clinically, acne keloidalis nuchae presents with skin-colored follicular papules, pustules, and plaques, as well as keloid-like scarred lesions in the occipital scalp (Fig. 88-8). Histologically, acne keloidalis is characterized by an acute inflammation with neutrophilic or lymphocytic infiltration and chronic granulomatous inflammation around the isthmus and the lower infundibulum. Monthly intralesional triamcinolone acetonide (10 to 40 mg/mL) alone or combined with topical 2% clindamycin or oral (tetracyclines) antibiotics is the treatment of first choice.3,10,20,81,82 Class I or class II topical steroids alone or in combination with topical antibiotics for mild cases of acne keloidalis nuchae, as well as topical retinoids, cryotherapy, and laser therapy,
have shown some success. Surgical excision of extensive keloidal lesions may be considered but should be reserved for therapy refractory, extensive, and symptomatic cases.
ACNE NECROTICA (VARIOLIFORMIS)
Acne necrotica varioliformis is a very rare, chronic condition, which predominantly occurs in adults. Frontal and parietal scalp, as well as seborrheic areas of the face are most commonly affected. Acne necrotica presents with umbilicated, pruritic, or painful papules that undergo central necrosis. The condition leaves varioliform, or smallpox-like scars.83,84 Histology shows a suppurative, necrotic, infundibular folliculitis with lymphocytic or mixed inflammatory infiltrate.84
Oral antibiotics, isotretinoin, and intralesional or topical corticosteroids have shown success.85 Excision of larger scarred areas can be considered.
EROSIVE PUSTULAR DERMATOSIS
Erosive pustular dermatosis is an uncommon disorder predominantly occurring in elderly women.86,87 The characteristic lesion is a suppurative, necrotic, erosive papule or plaque.86,88 Histology of early lesions is nonspecific, but older lesions show an extensive, chronic, mixed inflammatory infiltrate in the dermis, and later dermal fibrosis. Treatment includes class I or class II topical steroids with or without topical antibiotics, systemic antibiotics, and oral isotretinoin.86,88
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
SECONDARY CICATRICIAL ALOPECIA
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
In secondary cicatricial alopecias, permanent hair loss is caused by various other scalp conditions not
■Alopecia areata
■Alopecia areata
■Secondary cicatricial alopecia
■Secondary cicatricial alopecia
■Temporal triangular alopecia
■Temporal triangular alopecia
■Trichotillomania
■Trichotillomania
■Secondary syphilis (alopecia areolaris)
■Secondary syphilis (alopecia areolaris)
16
related to the hair follicle. In these conditions, the primary event develops outside the follicular unit, and leads to incidental destruction of the follicle. Possible causes are congenital defects, trauma, inflammatory conditions, infections, neoplasms, and, rarely, drugs (Table 88-3). Permanent, chronic traction alopecia and scars from surgery can be considered secondary scarring alopecias as well.89
CLINICAL FEATURES
CLINICAL FEATURES
A thorough clinical history is crucial in the diagnosis of secondary cicatricial alopecia. Diagnosis in early stages can sometimes be made based on specific clinical and histologic features of the underlying disorder. Follicular orifices are lost clinically, and histology shows extensive scarring with fibrosis, loss of elastic fibers and adnexal structures.89
PROGNOSIS AND CLINICAL COURSE
PROGNOSIS AND
CLINICAL COURSE
Prognosis and clinical course of secondary cicatricial alopecia depend on the underlying disease. Once scar tissue has formed and the adnexal structures are destroyed no hair regrowth can be expected.
TREATMENT
TREATMENT
Treatment is specific in active conditions, whereas in localized end-stage lesions, specific medical treatment is no longer efficient and hair restoration surgery techniques become the mainstay of therapy.
TINEA CAPITIS
TINEA CAPITIS
Tinea capitis is a common cause of hair loss in children secondary to an infection with dermatophytes species. The etiologic agent varies in different parts of the world. Presently, Trichophyton tonsurans accounts for approximately 90% of cases of tinea capitis in the United States and United Kingdom.90
Ectothrix infection, most commonly caused by Microsporum spp. (especially Microsporum canis) and Epidermophyton spp. destroy the hair cuticle and masses of spores are located outside of the hair shaft. The alopecic patches usually show signs of inflammation and scaling with brittle grayish hair stumps. The areas may show a yellow-green fluorescence under Wood light examination. Endothrix infections are most commonly caused by Trichophyton spp. (especially T. tonsurans subspecies sulfureum).91,92 The fungus is capable of invading the hair and masses of spores can be found
1531
16
Secondary Cicatricial (Permanent) Alopecias: A Classification Based on Etiology TABLE 88-3
■Ectodermal dysplasias
Genodermatoses and developmental defects with permanent alopecia (excluding congenital hypotrichoses and atrichias)
■Aplasia cutis congenita
■Incontinentia pigmenti
■Porokeratosis of Mibelli
■Ichthyosis
■Hereditary epidermolysis bullosa
■Meningocele
■Hamartoma
■Organoid nevi (sebaceous, epidermal) vascular malformations
■Darier disease
■Fibrodysplasia
■Mechanical trauma and pressure
Physical and chemical injury
■Scratching
■Burns
■Freezing
■Chemical injury
■Insect bites
■Radiation
Infections Bacterial
Infections Bacterial
■Carbuncle
■Carbuncle
■Leprosy
■Leprosy
■Tertiary syphilis
■Tertiary syphilis
■Tuberculosis–lupus vulgaris Viral
■Tuberculosis–lupus vulgaris Viral
■Zoster
■Zoster
■Varicella Tinea capitis
■Varicella Tinea capitis
■Kerion
■Kerion
■Favus Protozoal
■Favus Protozoal
■Leishmania
■Leishmania
■Psoriasis (rarely)
Inflammatory dermatoses
■Pityriasis amiantacea
■Arteritis temporalis
■Pyoderma gangrenosum
■Graft-versus-host disease Sclerosing
■Morphea
■Scleroderma en coup de sabre and Parry-Romberg syndrome
■Lichen sclerosus et atrophicus Bullous
■Cicatricial pemphigoid
■Porphyria cutanea tarda
■Acquired epidermolysis bullosa Granulomatous
■Sarcoidosis
■Granuloma anulare
■Necrobiosis lipoidica (including Miescher granulomatosis)
Neoplastic Infiltration
Neoplastic Infiltration
■Lymphoproliferative disorders
■Lymphoproliferative disorders
■Mastocytosis Benign solid neoplasms
■Mastocytosis Benign solid neoplasms
■Cysts
■Cysts
■Vascular tumors
■Vascular tumors
■Adnexal tumors
■Adnexal tumors
■Plasmacytoma Malignant solid tumors
■Plasmacytoma Malignant solid tumors
■Angiosarcoma
■Angiosarcoma
■Dermatofibrosarcoma protuberans
■Dermatofibrosarcoma protuberans
■Malignant fibrous histiocytoma
■Malignant fibrous histiocytoma
■Melanoma
■Melanoma
■Squamous cell carcinoma
■Squamous cell carcinoma
■Basal cell carcinoma
■Basal cell carcinoma
■Metastasis (alopecia neoplastica)
■Metastasis (alopecia neoplastica)
■Lymphoma
■Lymphoma
Adapted by permission from Springer: Finner AM, Shapiro J. Secondary cicatricial and other permanent alopecias. In: Blume-Peytavi U, Tosti A, Whiting DA, et al, eds. Hair Growth and Disorders. Berlin, Germany: Springer-Verlag; 2008:229, Table 12.1. Copyright © 2008.
within the hair shaft on microscopic examination. The hair breaks off directly at the skin surface, which clinically presents as “black dots.” Hair loss, inflammation, and scaling may be minimal; consequently, this type of tinea capitis is often dismissed as seborrheic or atopic dermatitis. Favus is a specific type of tinea capitis characterized by patelliform scales (scutula), which are sulfuric-yellow concretions of hyphae and skin debris in the follicular orifices and exhibit a distinct malodorous smell. A kerion is a deep, highly inflammatory fungal infection of the scalp. It presents as a highly suppurative, boggy, nodular, deep folliculitis with fistulas and pus secretion. To establish a diagnosis, hair shafts should be plugged out and cultured, as well as examined after potassium hydroxide preparation. Favus and kerion may lead to scarring hair loss and should be treated aggressively. 93-96
Systemic antifungal treatment such as terbinafine, itraconazole, ketoconazole, griseofulvin, and fluconazole is indispensable to treat tinea capitis. The choice of the systemic antifungal agent depends on the type
1532
of fungus.95,97,98 Especially in children, social contacts must be sought and treated to prevent reinfection. Topical sporicidal agents, such as selenium or ketoconazole help to limit the spread of the infectious spores.99
TRAUMATIC HAIR LOSS
TRAUMATIC HAIR LOSS
An acute or chronic mechanical insult to the scalp hair may lead to reversible or irreversible alopecia of the scalp. Traumatic alopecias are usually of 3 types: acute trauma, prolonged traction, and pressure.
TRAUMATIC INJURIES
Minimal or severe injuries to the scalp can result in alopecia. It usually presents with fine streaks of hair loss in the injured scalp area, but if the wound borders undergo contusion or destruction, this may result
in irregular and large patches of hair loss. Traumatic hair loss can occur after scalp surgery, especially after extensive scalp reduction or large donor strip harvesting in hair restoration surgery, if too much tension is applied with wound closure. This type of hair loss is usually reversible but also can be permanent. Traumatic birth induced alopecia is infrequent; causes include mechanical extractor marks, tears or contusions or resulting infections. Aplasia cutis congenita should be considered in the differential diagnosis of cicatricial alopecia at birth.100
TRACTION ALOPECIA
Prolonged traction of the hair may lead to transient or if continued over a period of time, may lead to follicular atrophy, resulting in cicatricial alopecia. Chronic traction can be caused by tight pony tails, braids, heavy dead locks or extensive use of rollers. As a consequence of ethnic differences in hair fragility and cultural differences in hair-styling practices, marginal traction alopecia is more commonly seen in African American women from hair braiding and weaving procedures (Fig. 88-9).101 Patchy traction alopecia in the frontal hairline or temples is commonly seen in Sikh boys, whose hair is usually tight up in a “topknot.”102
Cicatricial alopecia caused by prolonged traction can be treated with hair transplantation, if the patient discontinues the injuring hairstyles and sufficient donor hair supply is available.
TRICHOTILLOMANIA (HAIR PULLING DISORDER)
Trichotillomania (greek: tricho = hair, tillo = pull, mania = excessive excitement) is a form of traumatic alopecia caused by an irresistible compulsion to pull out or twist or break of one’s own hair. Two forms of trichotillomania can be distinguished: infantile or early-onset trichotillomania, which starts in early childhood, is typically of short duration and may resolve
16
spontaneously or with simple interventions.103,104 The clinical presentation is usually quite distinctive with a single or multiple asymmetrical, occasionally geometrically shaped, areas of hair loss on the scalp or other areas of the body (Fig. 88-10). The areas are not smoothly devoid of hairs, as seen in alopecia areata, but display short or bristly anagen hair. Most important in the therapy of trichotillomania is the education of patient and/or parents, and in lateonset trichotillomania, the treatment of the underlying psychopathology. Especially if patients deny the self-inflicting nature of their hair loss, a referral to a psychiatrist or psychologist is usually refused and treatment becomes difficult.
PRESSURE ALOPECIA
Pressure alopecia can occur after a patient was unconscious and completely immobile for a certain length of time. Hair loss is presumably a result of ischemia caused by the pressure of the body weight to a certain scalp area. The ischemic injury may lead to permanent hair loss.
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
■Primary cicatricial alopecia
■Primary cicatricial alopecia
■Alopecia areata
■Alopecia areata
■Temporal triangular alopecia
■Temporal triangular alopecia
■Trichotillomania
■Trichotillomania
1533
■Secondary syphilis (alopecia areolaris)
■Secondary syphilis (alopecia areolaris)
16
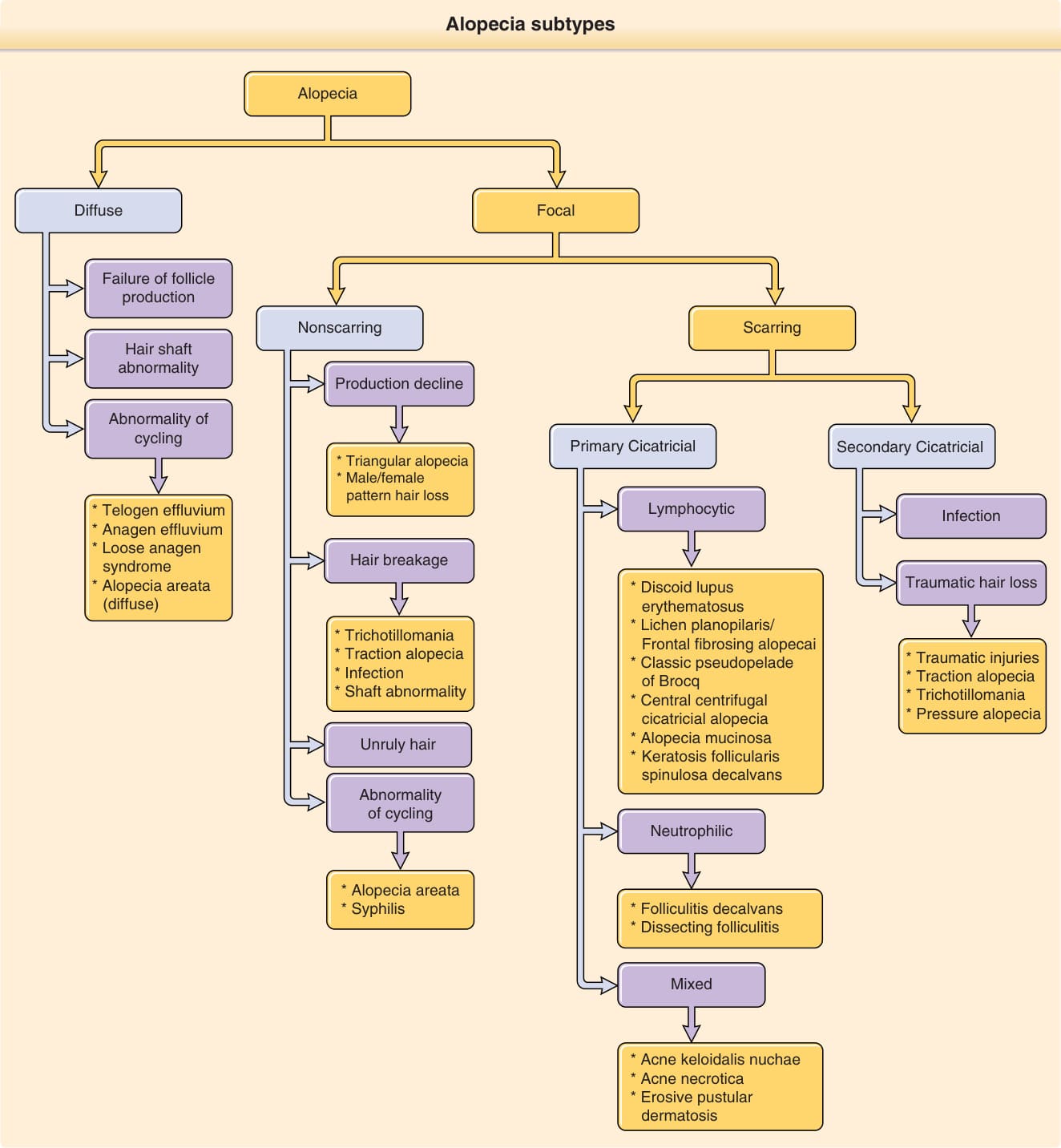
Figure 88-1 Alopecia subtypes.

Figure 88-2 Discoid lupus erythematosus.

Figure 88-3 Extensive lichen planopilaris.

Figure 88-4 Frontal fibrosing alopecia.
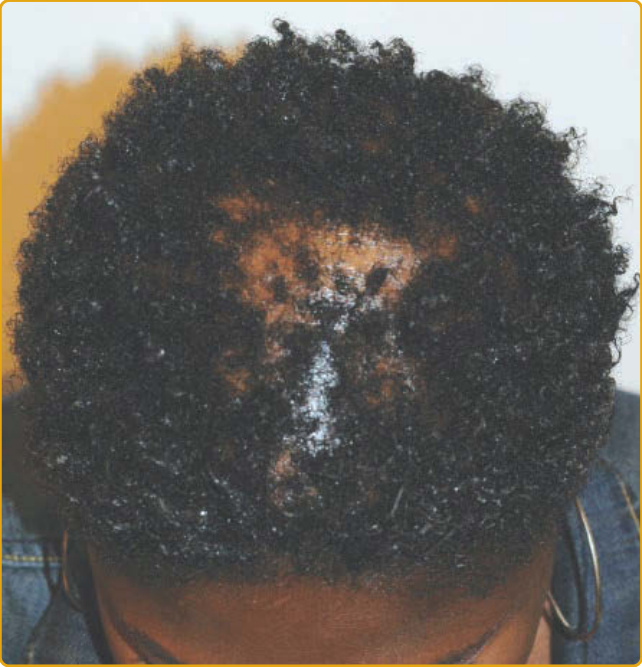
Figure 88-5 Central centrifugal cicatricial alopecia.

Figure 88-6 Folliculitis decalvans.
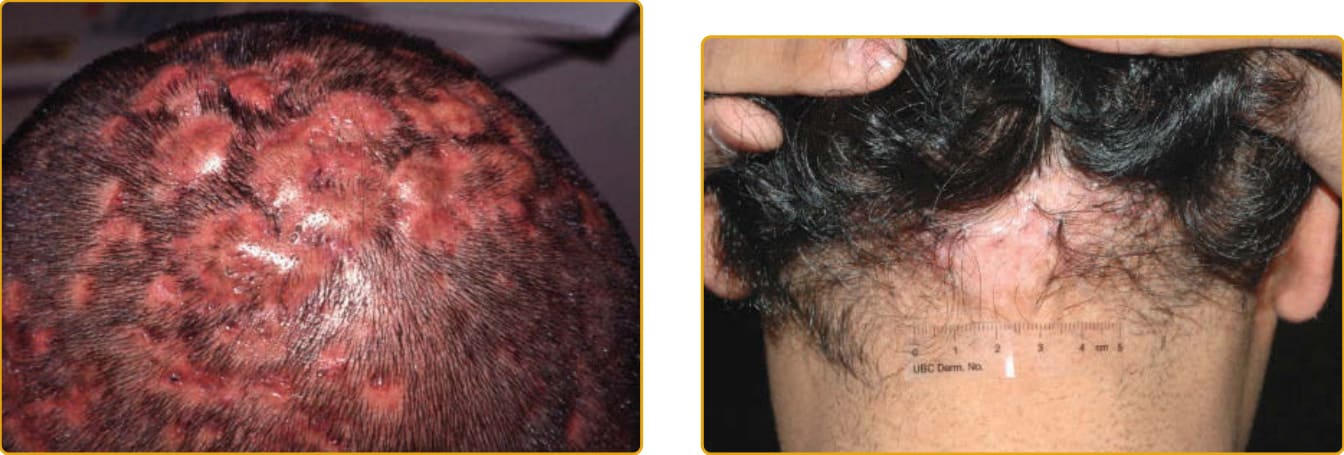
Figure 88-7 Dissecting cellulitis.

Figure 88-9 Traction alopecia.

Figure 88-10 Trichotillomania.
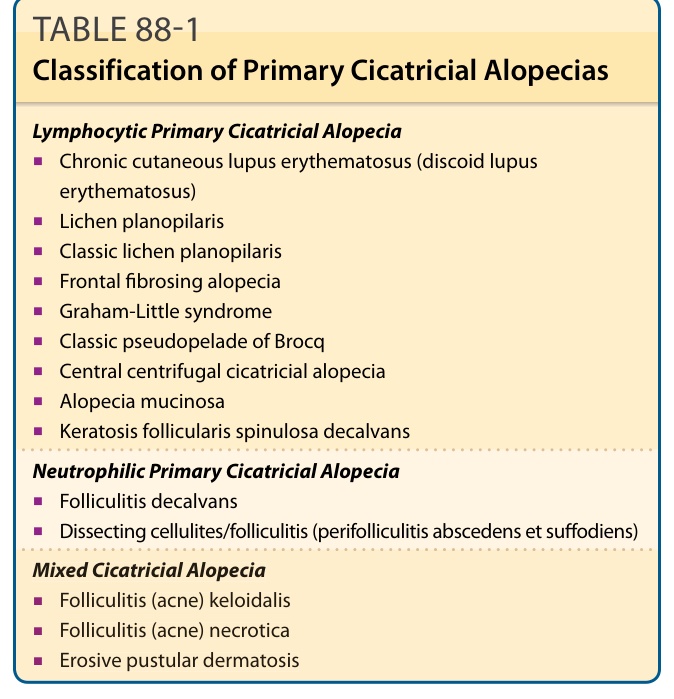
Table 88-1 outlines the classification of primary cicatricial alopecias.
Table 88-2 outlines the differential diagnosis of primary cicatricial alopecias.
Table 88-4 outlines the differential diagnosis of secondary cicatricial alopecias.