Alopecia Areata
16
AT-A-GLANCE
■ Alopecia areata is a nonscarring hair disorder.
■ It occurs in both genders equally and can affect every age group, although incidence at in younger age groups is higher.
■ It is the most common form of hair loss in children. Clinically, it presents with well-demarcated round or oval bald spots on the scalp or other parts of the body.
■ Of patients with alopecia areata, 5% develop hair loss of their entire scalp hair (alopecia areata totalis) and 1% develop alopecia areata universalis (loss of total body hair).
■ Nail changes include pitting or sandpaper nails.
■ Alopecia areata is thought to be an autoimmune disease with a possible hereditary component.
■ In general, alopecia areata is a medically friendly condition, but it can coexist with other autoimmune disorders such as Hashimoto thyroiditis and vitiligo.
Alopecia areata is a common autoimmune hair disorder. This nonscarring, usually patchy hair loss condition can affect any hair-bearing area. At any given time, approximately 0.2% of the world population is suffering from alopecia areata. It has an estimated lifetime risk of 1.7%1,2; it is a common cause of abruptonset hair loss, but occurs less often than androgenetic alopecia or telogen effluvium. Both sexes are equally affected. Although it may occur at any age, incidence at younger ages is higher. Alopecia areata is the most common form of alopecia seen in children. The familial occurrence is approximately 15%, but expression of the disorder is variable between different family members. Of patients suffering from alopecia areata, 5% develop hair loss of their entire scalp hair (alopecia areata totalis) and 1% develop alopecia areata universalis (loss of total body hair).
CLINICAL FEATURES
Alopecia areata is characterized by an acute onset. It typically presents with oval- or round-shaped, wellcircumscribed, bald, patches with a smooth surface in a diffuse distribution (Figs. 87-1 and 87-2). Alopecia totalis results in the loss of the entire scalp hair and may occur suddenly or follow partial alopecia (Fig. 87-3). Partial alopecia may be observed in other areas of the
body as well. Loss of total body hair is called alopecia areata universalis and may occur suddenly or follow longstanding partial alopecia. Characteristic hallmarks of alopecia areata are socalled black dots (cadaver hairs, point noir), resulting from hair that breaks off by the time it reaches the skin surface. Exclamation point hairs, which have a blunt distal end and taper proximally, appear when the broken hairs (black dots) are pushed out of the follicle. Localization of the initial patch occurs most often on the scalp, but may occur on any hair-bearing part of the body. Patches are usually without further symptoms, but may cause mild itching and erythema. In addition to this well-demarcated localized form, alopecia areata can also present in a diffuse generalized pattern that resembles androgenic alopecia or telogen effluvium. Involvement of nails can occur with nail pitting and a sandpaper-like appearance. Alopecia areata has been described in association with a variety of other disorders, including cataracts, thyroid disease, vitiligo, atopic dermatitis, psoriasis, Cronkhite-Canada, and Down syndrome.3,4
ETIOLOGY AND PATHOGENESIS
Alopecia areata is a chronic, organ-specific autoimmune disease. Autoactive cytotoxic CD8 T cells, which affect hair follicles and sometimes nails,5-11 and an interferon-γ–driven immune response, which includes interferon-γ and interferon-γ–induced chemokines, have been identified as the main drivers of disease pathogenesis.12 The importance of a cytotoxic subset of CD8+ NKG2D+ (natural-killer group 2 member D-positive) T cells within the inflammatory infiltrate in alopecia areata and an upregulation in the hair follicle itself of 2 NKG2D ligands have been discovered in several studies.10,11 Furthermore, other cell types, including natural killer cells, may play a regulatory role in alopecia areata.5,8,13,14
Patients with alopecia areata seem to have a genetic predisposition to the disease. There is a high frequency of a positive family history of alopecia areata in affected individuals, ranging from 10% to 42% of cases,15 and a much higher incidence of a positive family history in early-onset alopecia areata.16 A genome-wide association study10 and a large genome-wide association study metaanalysis17 have identified numerous loci that imply a strong role for variants in genes that direct and influence immune responses.13
Many patients report the experience of major emotional stress prior to the onset of alopecia. Stress
16
1518
perception seems to be a risk factor that may influence the onset and exacerbation of alopecia areata.18 Moreover, an antioxidant–oxidant imbalance can be found in many autoimmune disorders as well as in patients suffering from emotional and environmental stress. Several studies support an association between oxidative stress and alopecia areata.19-24
DIAGNOSIS
Clinical features, such as shape and look of the patches, presence of exclamation point hairs, and nail changes (pitting or sandpaper nails), lead to the diagnosis of alopecia areata (Fig. 87-4). In most patients the physical findings are so characteristic that the diagnosis is obvious. Patchy or complete loss of eyebrows and eyelashes can also lead to the diagnosis of alopecia areata (Fig. 87-5). Sudden and rapid loss of the entire scalp hair (alopecia areata totalis) or the entire body hair (alopecia areata universalis) are diagnostic for alopecia areata. A dermatoscopic evaluation will help to support the diagnosis by showing the presence of follicular ostia. The presence of either follicular ostia, exclamation point hair, cadaver hair (residual hair shafts visible as black dots in the follicular ostia), or yellow dots that will confirm the diagnosis. These features are even
more visible with a trichoscopic evaluation at higher magnification.25,26 In the acute stages gentle pulling from the periphery of bald areas will yield more than 10 hairs. White hairs are sometimes spared by the disease. This can lead to canities subita, a sudden whiting of the hair. In this case, all pigmented hairs fall out and the patient is left with only white hair. Moreover, positive family history and/or the presence of associated diseases may give further evidence. Diffuse alopecia areata can be very difficult to diagnose. In cases of doubt, a scalp biopsy (a 4-mm punch processed for horizontal sections) should be taken to confirm the diagnosis of alopecia areata. Additionally, laboratory tests should be performed to rule out thyroid dysfunction27 and iron or vitamin deficiencies.
PATHOLOGY
Scalp biopsy reveals a generalized miniaturization and a marked increase in catagen and telogen hair follicles. In the acute phase, alopecia areata is characterized by a peribulbar immune infiltrate centered around the hair bulb which has been described as a “swarm of bees.” This infiltrate is made up of predominantly CD4 and CD8 T cells and natural killer cells.28 Sometimes mast cell, plasma cells and eosinophils also can be seen.13,14,29
The histopathologic features of alopecia areata, however, are stage-dependent. The classic inflammatory infiltrate may be missing or markedly less in subacute or chronic forms.30 Sometimes an immune infiltrate is visible around the bulb of miniaturized hairs in the upper dermis.30 Alopecia areata should be in the differential diagnosis whenever high percentages of telogen hairs or miniaturized hairs are present, even in the absence of peribulbar inflammation.
DIFFERENTIAL DIAGNOSIS
COMPLICATIONS
Relapsing course and progress of hair loss to severe forms of alopecia totalis or universalis are dreaded
■Temporal triangular alopecia
■Temporal triangular alopecia
■Tinea capitis
■Tinea capitis
■Early scarring alopecia
■Early scarring alopecia
■Trichotillomania
■Trichotillomania
■Secondary syphilis (alopecia areolaris)
■Secondary syphilis (alopecia areolaris)
■Androgenetic alopecia
■Androgenetic alopecia
■Telogen effluvium
■Telogen effluvium
■Anagen effluvium
■Anagen effluvium
16
complications. Missing hair on the scalp and face, including nasal hair and eyelashes and eyebrows can increase incidence of sunburns and skin cancers, as well as of nasopharyngeal and ophthalmologic inflammation. Although the condition is not life threatening, changes in appearance frequently cause a diminished sense of personal well-being and self-esteem, leading to severe depressive mood and withdrawal from social situations.
PROGNOSIS AND CLINICAL COURSE
The course of the disease is very variable and characterized by an irregular relapsing course, with approximately 25% of affected individuals having a solitary episode. Spontaneous regrowth of hair is common. Different body areas appear to regrow independently. Approximately 60% of patients have at least a partial regrowth by 1 year, but this is often followed by repeated episodes of hair loss. Approximately 40% of the relapses occur within the first year, but a large percentage of patients may relapse after 5 years. Hair can regrow white but may change to the patient’s natural color over time. Poor prognosis is linked to involvement of the occiput and/or hairline, chronic relapsing course, presence of nail changes, and when onset is in childhood.31-33
Patients with alopecia areata have a 5% risk of losing their entire scalp hair (alopecia areata totalis) and an estimated 1% risk for progressing to alopecia areata universalis, characterized by total body and scalp hair loss. The number of patients progressing to alopecia areata totalis is higher in the younger age groups, and in patients with hair loss from the trunk and extremities.
TREATMENT
Very little evidence-based data is available for the treatment of alopecia areata; recommendations are mainly based on case series and clinical experience (Fig. 87-6). At this time there is no single therapy that can alter the natural course of the disease. All available treatments for alopecia areata are palliative, only controlling the ongoing episode of hair loss and not curing the condition itself. However, helpful treatment guidelines have been published.31-33
CONSERVATIVE MANAGEMENT
CONSERVATIVE
MANAGEMENT
Alopecia areata shows a high rate of spontaneous remission, especially in those patients with a short history and limited scalp involvement. On the other hand, in alopecia areata totalis and universalis, treatments have a high failure rate. After the discussion of possible risks and benefits of all options, no treatment may be a legitimate option for some patients.
1519
16
Treatment algorithm for alopecia areata
Alopecia areata
Age
Over age 10 Under age 10
Topical corticosteroids (mometasone) +/– Topical 5% minoxidil
Less than 50% scalp involvement
Topical corticosteroids +/– intralesional corticosteroids +/– Topical 5% minoxidil
Extent of disease
Greater than 50% scalp involvement
Scalp prosthesis
JAK inhibitors +/– intralesional corticosteroids
Topical immunotherapy (DPCP)
Successful response Successful response
Successful response
Yes Yes Yes No No
No
Continue DPCP as needed
Continue as needed
Topical immunotherapy Topical immunotherapy SADBE Continue JAK inhibitor therapy +/– intralesional corticosteroids
TOPICAL CORTICOSTEROIDS
TOPICAL CORTICOSTEROIDS
Superpotent (class I) and potent (class II) topical corticosteroids are widely used to treat alopecia areata. Evidence of efficacy has been proven for class I corticosteroids when applied under occlusion34 and for class II corticosteroids when used in combination with minoxidil.35
INTRALESIONAL CORTICOSTEROIDS
INTRALESIONAL
CORTICOSTEROIDS
Intralesional corticosteroid (triamcinolone acetonide or triamcinolone hexacetonide) injection is first-line therapy for adult patients with less than 50% scalp involvement. Triamcinolone acetonide is used at concentrations from 2.5 to 10 mg/mL. Treatment is repeated every 4 to 6 weeks; the total amount injected per session varies from 15 to 40 mg.31-33,36-38
1520
An initial response is often seen after 4 to 8 weeks.
Some patients experience indentation of the scalp skin in the injection sites as the result of a nonpermanent atrophy of the subcutaneous fat. Permanent skin atrophy can occur if the same skin area is injected repeatedly over months and years. If no regrowth can be seen after 4 months of treatment, other treatment options should be considered. Intralesional corticosteroids injections are usually used on the scalp, eyebrows and beard area and can be combined with topical treatment.
PLATELET-RICH PLASMA
PLATELET-RICH PLASMA
Reports state that the use of platelet-rich plasma injections as monotherapy or in combination with other therapies are beneficial in the treatment of alopecia areata.39-41 In a double-blind trial, platelet-rich plasma was superior to low-dose triamcinolone acetonide and placebo injection.42,43 Further studies are necessary to determine the effectiveness of platelet-rich plasma in the therapy of alopecia areata.41
SYSTEMIC CORTICOSTEROIDS
SYSTEMIC
CORTICOSTEROIDS
Systemic corticosteroids are effective in the treatment of alopecia areata. However, the regrown hair frequently falls out again when the treatment is discontinued. The use of systemic corticosteroids is controversial. They should not be used as routine treatments because they do not alter the long-term prognosis and can cause side effects, such as striae, acne, obesity, cataracts, and hypertension. Dosages vary from an initial 20 to 40 mg dose of prednisone daily, with tapering down to 5 mg daily in a few weeks or different pulse therapies regimens with short-term high doses of oral prednisolone (100 to 300 mg) or IV methylprednisolone (250 mg).31,32,34,36
TOPICAL MINOXIDIL
TOPICAL MINOXIDIL
There is some evidence of clinically acceptable hair regrowth using topical minoxidil 5% solution.44,45 Better results can be achieved when minoxidil is used in combination with class I or class II topical corticosteroids or anthralin.35 Minoxidil shows little efficacy in alopecia areata totalis and universalis.
PROSTAGLANDIN ANALOGS
PROSTAGLANDIN ANALOGS
Prostaglandin analogs like latanoprost and bimatoprost have been studied for their use in the treatment of alopecia areata of eyelashes and eyebrows. Some studies showed hair regrowth of eyelashes and eyebrows after the treatment with prostaglandin analogs.46 However, several reports showed a negative outcome after the use of latanoprost and bimatoprost.47-49 Prostaglandin analogs may have some use as an adjuvant therapy.
ANTHRALIN
ANTHRALIN
Anthralin is an irritant that may have a nonspecific immunomodulating effect (anti–Langerhans cell) and is usually used in the treatment of psoriasis.50 Several studies have shown efficacy in the treatment of alopecia areata with cosmetically acceptable varying from 20% to 25% for patchy alopecia areata.51,52 Anthralin is used as a 0.2% to 1% cream or ointment. It is usually applied daily to the affected scalp areas and left on for 20 to 30 minutes for the first 2 weeks, and then for 45 minutes daily for 2 weeks, up to a maximum of 1 hour daily. Some patient may tolerate overnight therapy.36,51 When therapy is effective, new hair growth can usually be seen after 2 to 3 months of treatment. Because of its good safety profile, anthralin is a good treatment choice for children. Side effects of anthralin are irritation, scaling, folliculitis, and regional
16
lymphadenopathy. Anthralin is not suitable for the treatment of eyebrows and the beard area. Patients should be cautious not to get anthralin in the eyes and to protect the treated skin areas from ultraviolet radiation. Brown discoloration of the treated skin and brown staining of clothes and linen may occur. The patient should be advised to rinse off the anthralin with cool or lukewarm water, as hot water increases the likelihood of brown stains of tiles and bathtub.
TOPICAL IMMUNOTHERAPY
TOPICAL IMMUNOTHERAPY
Although not approved by the U.S. Food and Drug Administration (FDA), topical immunotherapy seems to be a very effective therapeutic option with a good safety profile in the treatment of chronic severe alopecia areata. The exact mechanism of action is not fully understood. A decrease in the peribulbar CD4+/ CD8+ lymphocyte ratio and a shift in the position of T-lymphocytes away from the perifollicular area to the interfollicular area and dermis are thought to be responsible for the immunomodulating effect.53-55
The desired effect of the treatment is the creation of a contact dermatitis. Diphenylcyclopropenone is the most commonly used contact sensitizer. Diphenylcyclopropenone is compounded in an acetone base and stored in opaque bottles to protect the solution from photodegradation. Applying a small amount of a 2% solution to a small scalp area 1 week prior to treatment start, sensitizes the patient. The diphenylcyclopropenone solution is then applied weekly to the scalp, starting at a concentration of 0.0001%. The scalp should not be washed for 48 hours after treatment and should be protected from ultraviolet radiation. Carefully increase the concentration every week until the patient develops a mild erythema and mild itching. The treatment is continued with this concentration; the usual highest concentration used is 2%. Success rates vary from 17% to 75%, with the lowest success rates being in patients with alopecia areata totalis and universalis.56 Side effects include lymphadenopathy in 100% of patients, severe contact eczema, discoloration of the skin including vitiliginous patches and hyperpigmentation on the scalp and other parts of the body. Extreme caution is indicated in patients with atopic dermatitis and dark skin types.
PHOTO(CHEMO)THERAPY
PHOTO(CHEMO)THERAPY
Ultraviolet B light has been reported to be useful in some patients with alopecia areata.57 Further therapeutic options include both oral and topical administration of psoralen followed by ultraviolet A irradiation. Psoralen and ultraviolet A therapy may affect T-cell function and antigen presentation, and possibly inhibit the local immunologic attack against the hair follicle by depleting Langerhans cells.58 Photo(chemo)therapy shows a very high relapse rate, especially after tapering
1521
16
the treatment. Today’s major concern about long-term ultraviolet irradiation of any kind is its promotion of all types of skin cancer, including melanoma. Consequently, phototherapy should only be considered in exceptional cases.56
CYCLOSPORINE
CYCLOSPORINE
Systemic cyclosporine at doses of 4 to 6 mg/kg/day has been shown to have a beneficial effect in some patients with alopecia areata.56,59 Side effects of oral cyclosporine include elevated serum transaminases and cholesterol levels, as well as headaches, dysesthesia, fatigue, diarrhea, gingival hyperplasia, flushing, and myalgia. Cyclosporine can be combined with low-dose oral prednisone and may be considered in patients with severe atopic dermatitis and alopecia areata. However, because of its side-effect profile and the high recurrence rate observed after discontinuation, cyclosporine seems to be a relatively impractical treatment for alopecia areata.
JANUS KINASE INHIBITORS
JANUS KINASE INHIBITORS
Recent mechanistic data support a role for Janus kinase (JAK)-mediated pathways in alopecia areata11,60
Interferon-γ, interleukin-2, and interleukin-15 play a significant role in maintaining the autoreactive CD8+ T-cell infiltrate in alopecia areata. Their receptors signal through JAK1, JAK2, and JAK3. The inhibition of these cytokine receptors with JAK inhibitors can lead to a reversal of alopecia areata. Several case reports show that JAK inhibitors are a promising class of drugs for alopecia areata even in cases of severe or widespread disease. Oral baricitinib and tofacitinib citrate (approved by the FDA for mild rheumatoid arthritis) and oral ruxolitinib (approved by the FDA for myelofibrosis) have shown a good treatment outcome with full regrowth of scalp hair in widespread alopecia areata.61-65
CAMOUFLAGE, WIGS, AND HAIRPIECES
CAMOUFLAGE, WIGS, AND
HAIRPIECES
When despite treatment alopecia is progressive and there is no hope for hair regrowth, permanent adaptation to the disease is necessary. Extensive alopecia areata of the scalp can be camouflaged with wigs and hair pieces. In women with alopecia areata of the eyebrows, permanent makeup may be considered. The treating physician should provide psychological support. Local alopecia areata support groups and annual meetings of the National Alopecia Areata Foundation (www.naaf.org) can be very helpful for patients and their relatives.
1522

Figure 87-1 Patch of alopecia areata with mild peachy erythema and some fine residual hairs.

Figure 87-2 Patient with patchy alopecia areata.
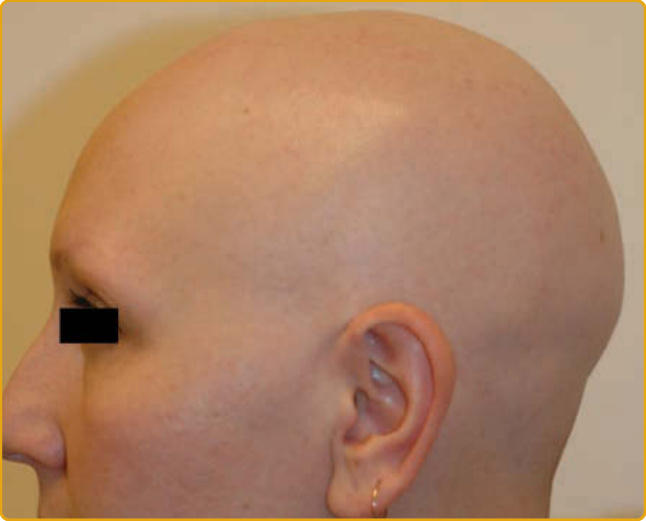
Figure 87-3 Patient with alopecia areata totalis.

Figure 87-4 Patch of alopecia area with exclamation point hair.

Figure 87-5 Patient with alopecia areata of the eyebrows.
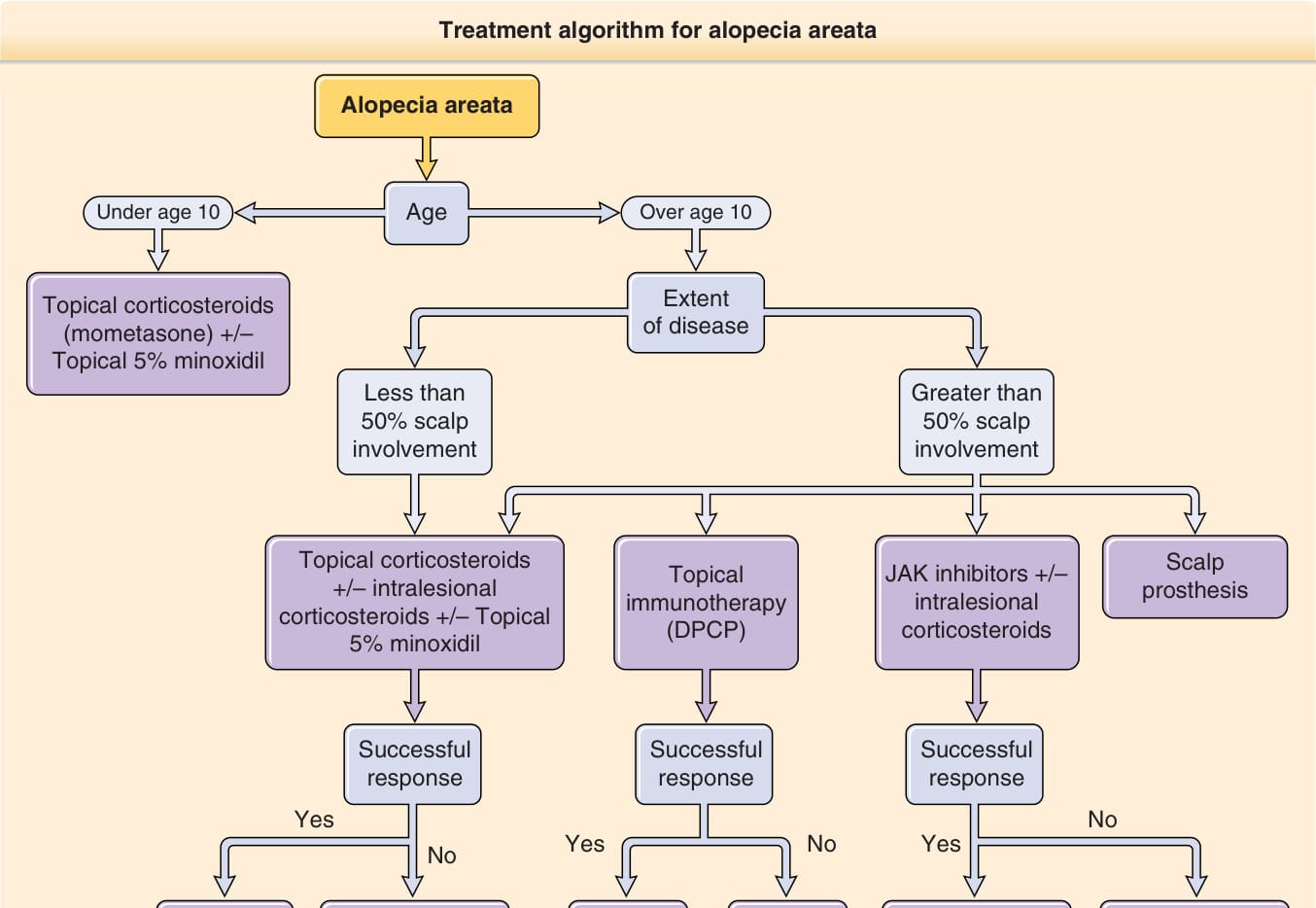
Figure 87-6 Treatment algorithm for alopecia areata. DNCB, dinitrochlorobenzene; DPCP, diphenylcyclopropenone; PUVA, psoralen and ultraviolet A; SADBE, squaric acid dibutylester. (From Strazzulla LC, Wang EHC, Avila L et al. Alopecia areata: An appraisal of new treatment approaches and overview of current therapies. J Am Acad Dermatol. 2018;78:15-24. Copyright © Lauren Strazzulla, Lorena Avila, and Jerry Shapiro, with permission.)