Telogen Effluvium
16
AT-A-GLANCE
■ Telogen effluvium is characterized by increased telogen club hair shedding.
■ Telogen effluvium is the most common cause of diffuse hair loss.
■ Telogen effluvium is subdivided into acute telogen effluvium, chronic diffuse telogen hair loss, and chronic telogen effluvium.
■ Differential diagnoses include alopecia areata incognita and psychogenic pseudoeffluvium.
■ Spontaneous recovery can be expected once a cause is identified and eliminated.
INTRODUCTION
Telogen effluvium (TE) was originally described by Kligman in 1961.1 TE is best characterized by a premature termination of the anagen (growing) phase of hair follicles, with a resultant increase in telogen (resting) phase hairs leading to excessive and diffuse loss of club hairs.1 Classically, TE refers to an acute hair loss subsequent to a variety of stresses including those caused by febrile diseases, childbirth, emotional disturbance, chronic systemic diseases, or the administration of heparin.1 TE can be a physiologic event in the newborn.1 Later studies revealed that the trigger and manifestation of TE were variable.2,3 TE represents the most common cause of diffuse hair loss.3 In clinics, truly diffuse hair loss is not often encountered.4
The most common reason bringing TE patients to the clinic is the increase in hair shedding after shampooing or brushing alone.4 Typically, TE is self-limiting, and full recovery can be expected once the specific causes are identified and corrected.3,4 However, especially in nonclassical chronic TE in women, distinction between female pattern hair loss is often challenging.5 In this chapter, the clinical features, pathophysiology, and differential diagnoses of TE are discussed.
EPIDEMIOLOGY
Approximately, the loss of more than 25% of scalp hairs has been reported to be necessary to clinically detect diffuse hair loss.1 Therefore, most TE cases are likely to be subclinical, making estimation of its real incidence or prevalence quite difficult.2,4 Female predominance has been noted in TE, probably because of stronger awareness of daily hair conditions and more dynamic hormonal changes including menstruation and gestation.4,6 In theory, incidence of classic acute
TE following known triggering events would not be distinct between the sexes.4 TE can occur in children but the incidence has been reported to be low.7 Elderly women are more likely to suffer from classic acute TE.4 Chronic TE (CTE) represents a unique form of unknown etiology that affects the whole scalp and is mostly seen in middle-aged women.8,9
CLINICAL FEATURES
Depending on the clinical course and symptoms, TE can be subdivided into 3 subgroups: classic acute TE,1 chronic diffuse telogen hair loss,2,4,10 and chronic telogen effluvium8,9 (Table 86-1). Irrespective of clinical subtypes, the most representative manifestation of TE is diffuse excessive shedding of club hairs.1,2,4,8,9 It should be noted that in severe TE cases, apparent diffuse or bitemporal hair thinning can be observed; however, hair loss is often subclinical and increased hair shedding can be the only objective sign in TE.1,4 In some cases, hair shedding has already peaked out and shed hairs carried by a patient alone is indicative of TE history.4 The clinical features of each subset are listed below.
ACUTE TE
ACUTE TE
This is the most classic type of TE originally described by Kligman in 1961.1 Typically, acute and diffuse hair shedding is noted 2 to 4 months from causative events.1-3 The presence of this latency period, probably reflecting the duration of catagen and telogen periods, has been considered to be characteristic for this type of TE.1 No sign of inflammation or scarring is observed on the scalp.3 Usually, shed hairs demonstrate the morphology of club hairs in the late stage of telogen without an enclosing sac (root sheath cells) and pigmentation.1 The amount of shedding hairs is significantly influenced by age, gender, race, or sampling methods, yet, in the original study by Kligman, the average number of hairs shed daily during classic TE ranged from 109 (postpartum case) to 646 (heparin-induced case).1 Usually gradual decrease and termination of hair shedding and the regrowth of new anagen hairs can be expected by 3 to 6 months.1,2
CHRONIC DIFFUSE TELOGEN HAIR LOSS
CHRONIC DIFFUSE
TELOGEN HAIR LOSS
A temporal insult usually triggers sudden-onset diffuse hair shedding as seen in acute TE, which recovers after the elimination of triggering stress.2 However,
16
CLINICAL SUBTYPE ETIOLOGYa
Acute telogen effluvium (acute TE) Effluvium of the newborn Febrile illness Surgery Pregnancy Weight loss (crash diet) Drugs (may cause CDTHL)
Chronic diffuse telogen hair loss (CDTHL)
Thyroid disease Aging Malnutrition Iron deficiency (controversial) Zinc deficiency (severe cases) Systemic illness Psychological stress (controversial) STD (HIV infection and syphilis) Miscellaneous
Chronic telogen
Idiopathic (shortening of anagen)
Chronic telogen effluvium (CTE) Idiopathic (shortening of anagen)
effluvium (CTE)
aEach etiology may explain both acute TE and CDTHL.
telogen hair shedding may last longer than 6 months.2,4
Chronic diffuse telogen hair loss (CDTHL) is one such condition that is secondary to various causes, including thyroid disorders, acrodermatitis enteropathica, malnutrition, and drugs (Fig. 86-1).2,4,10 The relation between CDTHL and the causative factors needs to be reversible and reproducible.
CHRONIC TELOGEN EFFLUVIUM
CHRONIC TELOGEN
EFFLUVIUM
CTE is an idiopathic form of diffuse club hair loss seen in middle-aged women in their fourth to sixth decade
1508
(Fig. 86-2).8,9 Telogen hair shedding extends more than 6 months to several years with fluctuation. The patient tends to have denser hair than average before the onset and could have been able to grow very long hair, especially in their childhood,8,11,12 implying that anagen duration is intrinsically prolonged.2 Typically, the onset of CTE is abrupt, and the amount of shed hairs is quite large. The patient may claim that the shed hairs block the drain after shower or bring a sack of shed hair to convince excessive hair loss.8 Telogen club hairs can be pulled out easily from the vertex and occipital areas.2 Marked bitemporal recession of hair is frequently observed.8,9 Female pattern hair loss needs to be excluded. A rare male case of CTE also has been reported.13
ETIOLOGY AND PATHOGENESIS
ETIOLOGY
ETIOLOGY
In the normal human scalp, the number of total hair follicles and the ratio between anagen and telogen hair are maintained as constant.14 On average, telogen hair accounts for around 10% of scalp hairs.15 Any factors that affect the duration of each phase of hair cycles with resultant abnormal increase of club hair loss can be potential TE triggers. As described above, TE consists of heterogeneous subsets with distinct pathophysiology, and therefore it is technically difficult to fully delineate the etiology. However, past observations listed definitive/probable causative factors (Table 86-1).
EFFLUVIUM OF THE NEWBORN
Physiologic type of TE can be seen in infants.1 The shedding starts within 4 months after birth. This type of effluvium may be regarded as “total replacement
of the first pelage completed before the first 6 month of life.”1 Telogen counts in this form of effluvium are around 60% to 80% and higher than other pathogenic TEs. The hair loss pattern may resemble that of androgenetic alopecia in some cases.1
FEBRILE ILLNESS
Hair loss in the influenza epidemic of 1971 has been described.16 Kligman reported 4 pediatric cases of acute TE that developed after pertussis, pneumonia, and influenza.1 Hair shedding appeared 3 to 4 months after the illness and continued for 3 to 4 weeks. Complete hair regrowth was achieved in these cases. Febrile illness was probably a common cause of TE in the preantibiotic era, and it still needs to be counted as a trigger in critically ill patients, including those with acute sepsis.16 High fever can cause physiologic stress to hair-producing matrix cells and lead to early anagen release,14 or alternatively, high levels of interferons may contribute to the development of acute TE.17,18
SURGERY
Major surgery can trigger postoperative TE.15,19 It is a matter of debate whether surgery alone or other factors accompanying surgery, for example, fever; general anesthesia; and changes in hormone, cytokine, or nutrition levels triggered acute TE. Rhytidectomy has been reported to cause “local” TE.20
PREGNANCY
Postpartum alopecia or telogen gravidarum is probably the most widely recognized form of classic TE observed 2 to 3 months after childbirth.14,21 Using a trichogram (forced plucking of hairs), progressive increase in anagen hairs during pregnancy has been reported.21,22 Lynfiend reported a high anagen hair rate (94.4% on average) during the second and third trimesters, whereas telogen hairs accounted for 25.5% at 6 weeks postpartum.21 A recent analysis of 116 pregnant women with digital image analysis software (Trichoscan) has confirmed the increase in anagen rate during pregnancy.23 However, the increase in telogen rate after delivery was only 3% and the authors suggested that postpartum TE may not be as frequent as generally thought.23 This observation is supported by other investigators.24,25 Accumulated clinical observations suggest that postpartum TE exists1; however, as most descriptions are based on studies conducted in the 1960s, further revisit and dissection of the pathophysiology using modern technology is needed to draw definitive conclusions.
THYROID DISEASE
Association between hypothyroidism and TE has been well established.26 The manifestation is more likely
16
to be CDTHL rather than acute TE (Fig. 86-1).4 Hair regrowth can be observed around 8 weeks after the initiation of thyroid hormone replacement in patients with hypothyroidism, with telogen hair loss clearly indicating their link.27 No correlation between the severity of thyroid dysfunction and the degree of effluvium has been demonstrated.26
Compared with hypothyroidism, the role of hyperthyroidism in TE, especially in CDTHL, is less clear and requires further investigation.26,28
AGING
Diffuse hair loss in the scalp and body can be seen in elderly subjects with histopathologic increase in telogen ratio.29 Incidence of TE tends to be higher in elder individuals.30 Senility may be a risk factor for TE or CDTHL.
WEIGHT LOSS (CRASH DIET)
A vigorous weight loss (11.7 to 24.75 kg within 3 weeks to 3 months) can result in remarkable increase in telogen counts (25% to 50%) and lead to acute TE (Fig. 86-3).31 Calorie restriction of 0 to 1200 kcal per day has been reported to be associated with hair loss.26
MALNUTRITION
An increase in telogen hair ratio has been noted in protein-deficient elderly subjects and children with protein-calorie malnutrition, though only in severely affected cases.32,33 The effect of malnutrition on the hair cycle may be variable, and CDTHL may be observed in those seriously malnourished.26
1509
16
IRON DEFICIENCY
Iron deficiency has been implicated in the pathogenesis of TE.26 Previous studies demonstrated that iron supplementation to CTE patients resulted in a reduction of hair shed or a decrease in telogen rate.34 Recent studies revealed that serum ferritin levels were reduced in women but not significantly in CTE patients compared with control subjects.35,36 Thus, the role of iron deficiency in TE is still controversial, and the efficacy of iron supplementation in CDTHL or CTE needs to be assessed in further clinical trials. A serum ferritin level less than 40 ng/ml may be considered as iron deficient in the general population.35
ZINC DEFICIENCY
Acrodermatitis enteropathica is an autosomal recessive disorder characterized by zinc malabsorption with resultant hair loss, acral and periorificial dermatitis, diarrhea, immunodeficiency, mental and neurologic disturbances, and growth retardation.26 CDTHL is a typical pathophysiology for hair loss.4 Supplemental zinc should improve all symptoms, including hair loss.26
Acquired zinc deficiency resembling acrodermatitis enteropathica may develop in parenteral alimentation, GI tract surgery, pancreatitis, inflammatory bowel disease, or AIDS nephropathy as well as in premature infants26 and cause acute TE or CDTHL. In contrast, the contribution of moderately low serum zinc levels to the development of CTE remains elusive.36
SYSTEMIC DISEASE
In addition to one-time-only febrile illness or endocrine/metabolic disorders, a variety of systemic diseases have been reported to be associated with diffuse hair loss.26 CDTHL in connection with lymphoproliferative disease, advanced malignancy, collagen disease (systemic lupus erythematosus and dermatomyositis), hepatic disease, chronic renal failure, systemic amyloidosis, eosinophilia-myalgia syndrome, and inflammatory bowel disease have been reported.4,26 Extensive acute TE has been reported to be characteristic for Cronkhite-Canada syndrome but full recovery can be expected once the underlying condition is healed.37
PSYCHOLOGICAL STRESS
The general perception is that psychological stress can play a role in the increase in hair shedding. In fact, Kligman in his original report of TE mentioned about psychological events as a potential cause of effluvium.1 The contribution of psychological stress to the development of TE has been suggested; however, it is not fully supported by a high level of scientific evidence.26
1510
SEXUALLY TRANSMITTED DISEASES
HIV infection and secondary syphilis have been reported to be associated with CDTHL.4 The mechanism is not fully elucidated but the observations suggest that HIV and syphilis tests need to be included when screening for TE causes.
DRUGS
Many drugs have been reported to cause TE (Table 86-2).4,26,38-42 However, exact incidence rates have not been documented in most agents.26 To conclude an etiologic role of some drug in TE, other potential causes of TE need to be excluded and the hair loss should resolve after the discontinuation of the medication.26,41
The cause-effect relationship can further be supported with the reappearance of TE when a drug is readministered. Early entry of anagen hair follicles into telogen (immediate anagen release) represents a main mechanism of drug-induced TE.41 In many cases, the shedding starts 2 to 3 months after the initiation of the
Androgen hormone (testosterone, anabolic steroids, proandrogenic supplements [DHEA], contraceptives containing progesterone) Anticoagulants (heparins, warfarin, [possible; dabigatran, rivaroxaban]) Antihistamines (cimetidine, ranitidine) Anti-infective agents Antifungals (clotrimazole, fluconazole, itraconazole, terbinafine) Antivirals (acyclovir, imiquimod, indinavir) Antituberculosis (ethambutol, isoniazid) Antiparasitic drug (albendazole, mebendazole) Antimitotic agents (colchicine, methotrexate) Antithyroid agents (propylthiouracil, methimazole) Cardiovascular drugs ACE inhibitors (captopril, enalapril, moexipril, ramipril) Beta-adrenoceptor antagonists (metoprolol, propranolol) Disease-modifying antirheumatic drug (leflunomide) HPV vaccine Dopamine precursor and agonists (levodopa, bromocriptine, pergolide pramipexole,) Interferons (interferon a-2b, γ) Intravenous immunoglobulin Metabolic disease therapeutics (allopurinol, cholestyramine, clofibrate, fenofibrate, triparanol, nicotinic acid) Minoxidil (at initiation or withdrawal) Nonsteroidal antiinflammatories (ibuprofen, naproxen, salicylates) Oral contraceptives (cyproterone, drospirenone) Psychotropics Amphetamines Anticonvulsants (lamotrigine, phenytoin, valproic acid) Antidepressants (fluoxetine, sertraline, tricyclic antidepressants) Mood stabilizers (lithium, sodium valproate) Pyridostigmine bromide Retinoid, vitamin A and its derivatives (acitretin, etretinate, isotretinoin) Spironolactone Sulfasalazine
Androgen hormone (testosterone, anabolic steroids, proandrogenic
supplements [DHEA], contraceptives containing progesterone) Anticoagulants (heparins, warfarin, [possible; dabigatran,
rivaroxaban]) Antihistamines (cimetidine, ranitidine) Anti-infective agents
Antifungals (clotrimazole, fluconazole, itraconazole, terbinafine) Antivirals (acyclovir, imiquimod, indinavir) Antituberculosis (ethambutol, isoniazid) Antiparasitic drug (albendazole, mebendazole) Antimitotic agents (colchicine, methotrexate) Antithyroid agents (propylthiouracil, methimazole) Cardiovascular drugs
ACE inhibitors (captopril, enalapril, moexipril, ramipril) Beta-adrenoceptor antagonists (metoprolol, propranolol) Disease-modifying antirheumatic drug (leflunomide) HPV vaccine Dopamine precursor and agonists (levodopa, bromocriptine,
pergolide pramipexole,) Interferons (interferon a-2b, γ) Intravenous immunoglobulin Metabolic disease therapeutics (allopurinol, cholestyramine, clofibrate,
fenofibrate, triparanol, nicotinic acid) Minoxidil (at initiation or withdrawal) Nonsteroidal antiinflammatories (ibuprofen, naproxen, salicylates) Oral contraceptives (cyproterone, drospirenone) Psychotropics
Amphetamines Anticonvulsants (lamotrigine, phenytoin, valproic acid) Antidepressants (fluoxetine, sertraline, tricyclic antidepressants) Mood stabilizers (lithium, sodium valproate) Pyridostigmine bromide Retinoid, vitamin A and its derivatives (acitretin, etretinate,
isotretinoin) Spironolactone Sulfasalazine
ACE; angiotensin-converting enzyme.
medication.1,41 Usually, the recovery from TE can be expected around 3 months after the termination of a causative drug.41
Anticoagulants, such as heparin and warfarin, have been recognized as a trigger of TE (Fig. 86-4).1,42 Other important TE inducers include antiinfective agents, cardiovascular drugs, psychotropics, oral contraceptives, and retinoids (Table 86-2).4,26,41,42
MISCELLANEOUS
Biotin or fatty acid deficiency; exposure to heavy metals including arsenic, thallium, and selenium; sunlight and UV ray exposure; and contact dermatitis are reported to be possible triggers for TE.4
PATHOGENESIS
PATHOGENESIS
Exact mechanisms modulating hair cycle to increase telogen hairs have not been fully delineated. Headington proposed 5 distinct pathogeneses accounting for TE.14 Recently, the concept that exogen, a hairshedding process, is an actively controlled biochemical event independent from each phase of hair cycle has been widely accepted,43,44 which sheds new light on the pathophysiology of TE.
IMMEDIATE ANAGEN RELEASE
Premature termination of anagen and entry into telogen can be a common mechanism for acute TE.14 Many drug- or stress-induced TE respectively represented by those induced by heparin and drugs in the heparin family or febrile illness1 can be explained by this phenomenon.14 Recovery can be expected once external insults are withdrawn and the normal hair cycle restarts.14
16
DELAYED ANAGEN RELEASE
The anagen period is prolonged in most hair follicles but eventually terminated, resulting in an abrupt increase in telogen hairs. This may cause synchronous telogen hair shedding.14 Delayed anagen release has been observed in the postpartum period21,23; however, whether or not this prolongation truly leads to TE remains an open question.23-25
SHORT ANAGEN
Headington suggested that idiopathic anagen shortening could be observed in some individuals (a short anagen syndrome).14 Theoretically, shorter anagen results in a higher telogen rate, with resultant effluvium. An example of this phenomenon is a decrease in anagen period in etretinate-treated patients.45
IMMEDIATE TELOGEN RELEASE
The hair follicle is programmed to release club hair to approximately 100 days after the end of previous anagen and enters into new anagen.46 TE may result from earlier entry into anagen as the frequency of hair shedding should increase.14 The shedding phase observed at the initiation of topical minoxidil can be explained by this mechanism.46
DELAYED TELOGEN RELEASE
The telogen phase is sustained in this case but immediately after, the anagen is initiated, resulting in an increase in shedding club hairs.14 This situation is observed in seasonal molting in mammals and, probably, in humans traveling from low-daylight to highdaylight conditions.14
MODULATED EXOGEN (PROVISIONAL)
Exogen refers to a term during which club hairs are shed from the telogen root sheath sac.44 Recent studies have suggested that exogen is not a passive process cued by the new anagen hair shaft but a step characterized by proteolytic activity.47 In rodents, the club hair is retained in the hair follicle even after the initiation of new anagen and contributes to protection from external insults.44 In the human scalp, exogen is believed to take place sometime around the transition between telogen and anagen.44 The presence of “kenogen” follicles, the telogen hair follicle without the hair shaft, suggests that shedding of club hair and the anagentelogen transition do not always keep their orders.44
To what extent does exogen play a role in the pathogenesis of TE remains elusive. Technically, immediate or delayed telogen release also can be explained by accelerated or delayed exogen. Consideration of the role of exogen may enable further dissection of TE pathophysiology
1511
16
DIAGNOSIS
TE should be suspected when a patient claims diffuse hair shedding exclusively consisting of club hairs. In typical acute TE cases with large amounts of telogen hair loss, detailed history attempting to identify possible triggers as described above in the preceding 3 to 4 months is helpful for the diagnosis of TE.3 It should be noted that triggering events are not identifiable in up to 33% of acute TE cases.14,48 The diagnosis of TE needs to be made based on the medical history and the findings implying increased telogen hair shedding obtained by the examinations listed below.
HAIR EXAMINATION
HAIR EXAMINATION
HAIR APPEARANCE
The assessment of global hair thickness and part width may be useful; however, as described above, TE can be subclinical in many cases and needs to be evaluated by quantitative approaches.
HAIR LOSS COUNT
Patients often bring shed hairs collected after shampooing or brushing during a certain period. Counting shed hair in such way can be quantitative with patient cooperation and skilled hands49 but usually not. At the same time, hair loss count alone can allow making the diagnosis in severe TE cases. In addition, it gives an idea for the patient condition and further evaluation. Thus, hair loss count still provides valuable information for clinicians. Despite hard efforts by investigators, the definitive “normal hair loss count” has not been fixed.4 In his landmark study, Kligman reported that daily telogen hair loss by regular combing and brushing was 11 to 113, varying considerably among individuals, with an average number of 47.1 A later study reports the daily shed count to be 40 to 180.50 A daily telogen hair loss more than 100 has been widely used as the “gold standard” for distinguishing abnormal hair loss.1,50 This number can be a useful yardstick. Yet, it should be noted that the score is not fully supported by scientific evidence.50
HAIR PULL TEST
To be strict, the hair pull test is performed in a patient who has not shampooed for more than 24 hours prior to examination.51 About 40 to 60 hairs are grasped between the thumb and fingers and pulled firmly alongside with hair shafts.51 The process needs to be repeated in at least 3 scalp areas, including the frontal, occipital, and temporal regions.52 Active hair shedding is indicated when more than 10% of tested hairs were collected.51 Careful attention needs to be paid to the morphology of hair roots as positive findings can
1512
be observed in other hair loss disorders (Fig. 86-5).4 Of note, the presence of tapered “pencil point” hairs suggests alopecia areata.4
In clinics, the hair pull test can be more casually adopted to patients at any time to check if effluvium is present. Perhaps, the increase in hair loss is suggested when more than 5 to 6 hairs were consistently pulled from 2 or more areas. The examiner should be aware that negative hair pull does not exclude TE.4
TRICHOGRAM
Trichogram is a semiinvasive technique and represents the most commonly used technique to evaluate hair cycles in the past.4,52 The patient undergoing this procedure should not wash her or his hair 3 to 5 days before examination.4,52 Fifty to 100 hairs were clumped by rubber-armed forceps or needle holder and forcibly plucked and investigated for the root morphology under a light microscope.1,4,52 Usually, sites 2 cm from the front line and midline are sampled.52
The procedure may yield artifacts if an examiner is unskilled and if it is uncomfortable for the patient, but it provides the telogen-anagen ratio, which is crucial for TE diagnosis.4,52 Normal values vary among the reports: telogen 13% ranging from 4 to 20% may set a standard.1 Acute TE can be suggested if the telogen rate exceeds 25%.1
PHOTOTRICHOGRAM AND TRICHOSCAN
The phototrichogram is basically a comparison of sequential photographs of a shaved scalp area to detect growing hairs.52 The procedure is noninvasive but, as it requires shaving, can be refused by a patient. The method provides little quantitative information with regard to the hair cycle phase and may be useful when a remarkable increase in telogen (nongrowing) hairs
is observed.52 Trichoscan is an automated version of phototrichogram using digital software for analyzing dermoscopy images.52 These techniques are more frequently adopted for the evaluation of hair growth (in clinical trials) rather than effluvium.
TRICHOSCOPY (DERMOSCOPY)
Recently, trichoscopy (dermoscopy without immersion gel; dry-dermoscopy) attracts great interest as a method for the diagnosis of hair disorders.53 The technique enables the distinction of clinically resembling disorders including TE, androgenetic alopecia (AGA) and diffuse alopecia areata (AA).53 The decrease in hair density and empty hair openings (active phase) or short-vellus hairs (recovery phase) may be seen in TE (Fig. 86-6). Other signs suggestive of AGA or AA, such as hair diameter diversity, broken hairs, black dots, and tapering hairs, should be absent. In this sense, the diagnosis of TE by this technique is rather based on the exclusion.54 Trichoscopy is useful for early detection of regrowth of short vellus hairs in the recovery phase of TE.
HISTOLOGY
Histopathologic examination is an invasive but most reliable and informative method for the evaluation of hair loss disorders.15 For the diagnosis of TE, a quantitative assessment by means of hair counts (eg, total hair numbers, terminal vs vellus hair ratio [indicating miniaturization], telogen-anagen ratio) is indispensable, which can be achieved by horizontal sectioning of a 4-mm punch biopsy specimen at the level between reticular dermis and subcutaneous tissue.9,55
The histopathologic findings of TE are a normal total hair count, an increase in telogen hair ratio, normal hair size, and absence of significant inflammation or fibrotic changes.55 The telogen count greater than
16
20% support the diagnosis of TE; however, the number can vary depending on the baseline of each patient.55
In CTE, histologically-detectable increase in telogen hairs can be moderate, around 11% on average.9 Again, the number can be variable, and multiple biopsies can enhance the accuracy of the diagnosis.56
GENERAL EXAMINATION
GENERAL EXAMINATION
MEDICAL HISTORY AND PHYSICAL EXAMINATION
Interview of medical history and daily medication potentially associated with telogen hair loss can be beneficial, especially in CDTHL cases. Varying degrees of trichodynia has been reported to be seen in TE and may help the diagnosis.57 Physical examination for thyroid swelling, skin, and nail condition can be performed to detect subclinical thyroid or collagen disease.
LABORATORY EXAMINATION
A battery of laboratory tests should be performed when the cause is not identified or needs to be evaluated for its status. Recommended items include urine analysis, complete blood count, erythrocyte sedimentation rate, total protein and albumin, aspartate transaminase and alanine transaminase, blood urea nitrogen/creatinine, lactate dehydrogenase, serum ferritin and zinc, T3, T4, thyroid-stimulating hormone, antinuclear antibody, sex hormones (testosterone, luteinizing hormone, and follicle-stimulating hormone in females), prolactin, C-reactive protein, syphilis, and HIV tests.3,4
DIFFERENTIAL DIAGNOSIS
A condition that possibly manifests diffuse hair loss needs to be included in the differential diagnoses. Of note, female pattern hair loss, alopecia areata incognita, and psychogenic pseudoeffluvium can present quite similar clinical features and thus should be excluded.4,46 Their distinction can be very challenging, especially in women.46,56
FEMALE PATTERN HAIR LOSS
FEMALE PATTERN
HAIR LOSS
Female pattern hair loss (FPHL) preferentially affects the top of the scalp, and the frontal hairline is usually preserved.46 Some patients can demonstrate a triangular reduction in hair density in the frontal scalp behind a preserved fringe resembling a Christmas tree.46 FPHL can be distinguished from TE in cases at an advanced stage with typical “patterned” hair loss. However, an early-stage FPHL without apparent hair loss may
1513
16
report an increase in hair shedding with diffuse distribution similar to that in CTE.46,56 The history and common approaches, such as hair pull test, trichogram, as well as laboratory investigation are usually not valuable in distinction.2,4,46,52 Dermoscopic investigation of an affected area may enable the differentiation when characteristic FPHL signs, including hair diameter diversity, peripilar signs (a brown halo around the follicular ostium), and empty follicles, are present.46
A quantitative histopathologic examination using horizontal sections adopting the terminal to vellus-like hair ratio (FPHL<CTE) can help confirm the diagnosis; however, multiple biopsies are necessary for diagnostic accuracy.56
ALOPECIA AREATA INCOGNITA
ALOPECIA AREATA
INCOGNITA
Alopecia areata incognita is a rare variant of alopecia areata characterized by acute and diffuse loss of hairs without apparent alopecic patches.58 Hair pull test is strongly positive and collects telogen hairs.59 Exclamation mark hairs with dystrophic roots are hardly found.4 The diagnosis can be challenging.4,46 Detection of numerous yellow dots of various size and uniform in color by dermoscopy or peribulbar lymphocytic infiltration by histopathologic examination can help establish the diagnosis.4,46,59
PSYCHOGENIC PSEUDOEFFLUVIUM
PSYCHOGENIC
PSEUDOEFFLUVIUM
Psychogenic pseudoeffluvium is typically seen in women aged between 35 and 50 years or in men under 35 years.4 The affected individuals claim hair shedding; however, clinicopathologic examinations fail to detect any evidence of active hair loss.4,46 The condition is included in body dysmorphic disorder and, in some cases, underlying depressive or anxiety disorders may be present which require appropriate psychiatric management.4,46
CLINICAL COURSE, PROGNOSIS, AND MANAGEMENT
Clinical course and prognosis of TE can be variable. However, normal hair regrowth can be expected within several months once a triggering cause is successfully identified and eliminated.1,4,46 In some cases, the hair texture may be altered.46 CTE represents an idiopathic form of TE, and its chronology remains elusive.4 A long-term follow-up of CTE cases reported no visible reduction in hair density even after continuous and
1514
fluctuating hair loss for more than 7 to 8 years, suggesting a favorable prognosis.60
In principle, the management of TE consists of observation until spontaneous resolution, reassurance that hair loss should terminate and not lead to total baldness and psychological support represented by counseling.1,2,4,46 The explanation of hair cycle and the pathophysiology of TE may help reducing frustration and anxiety of the patients. For those not convinced, periodical sampling of shed hairs under a constant condition (eg, after shampooing everyday [Fig. 86-7]) or demonstration of an image of regrowing hairs can enable a patient to realize the recovery. Distinction between CDTHL and CTE requires exclusion of etiologic factors.2 Well-organized clinical and laboratory examinations assessing possible causes listed above should be performed. Medications tend to be less regarded as a cause and needs to be fully evaluated.2
Currently, treatment options for CTE are limited.4,46
Topical minoxidil may be beneficial; however, increase in telogen hair loss may be experienced 2 to 6 weeks after treatment initiation.26
Further dissection of the pathophysiology of TE, especially that of CTE, and the elucidation of the mechanism of exogen are indispensable to better manage this common hair loss.
ACKNOWLEDGMENTS
The author would like to thank the Department of Dermatology, Keio University School of Medicine, for permitting the use of images.

Figure 86-1 Chronic diffuse telogen hair loss due to Hashimoto disease.

Figure 86-2 Chronic telogen effluvium in a middle-aged woman.

Figure 86-3 Acute telogen effluvium started 3 months after crash diet (weight loss of more than 10 kg within 2 to 3 months).

Figure 86-4 Acute telogen effluvium triggered by the administration of warfarin.

Figure 86-5 Telogen club hairs with intact hair roots collected by hair pull test.

Figure 86-6 The most characteristic dermoscopic finding of telogen effluvium is an increase in short-vellus hairs.
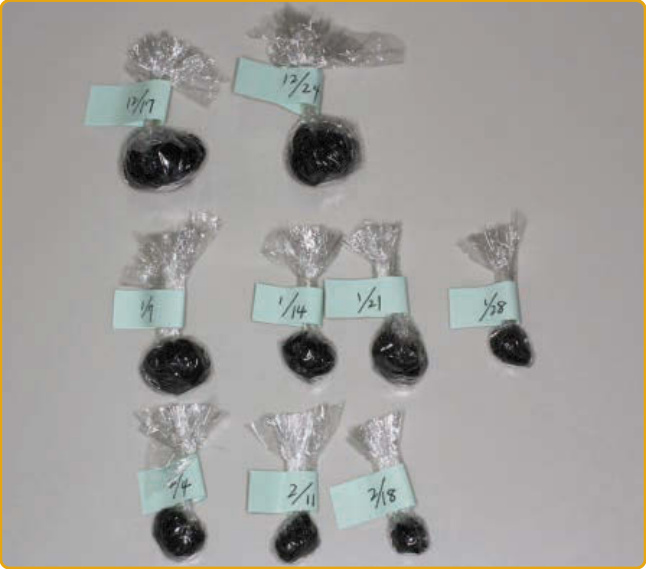
Figure 86-7 Packs of shed hairs collected by periodical sampling confirm spontaneous resolution.
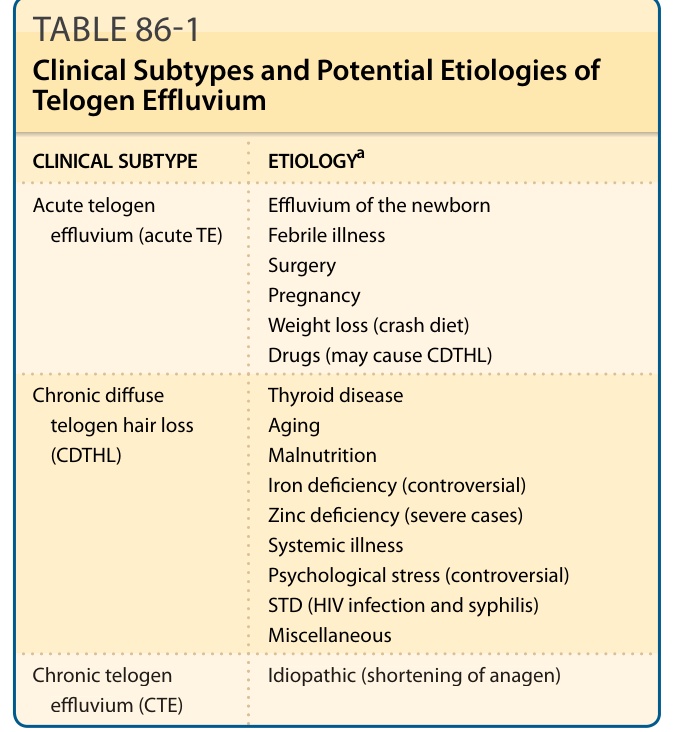
TABLE 86-1 Clinical Subtypes and Potential Etiologies of Telogen Effluvium
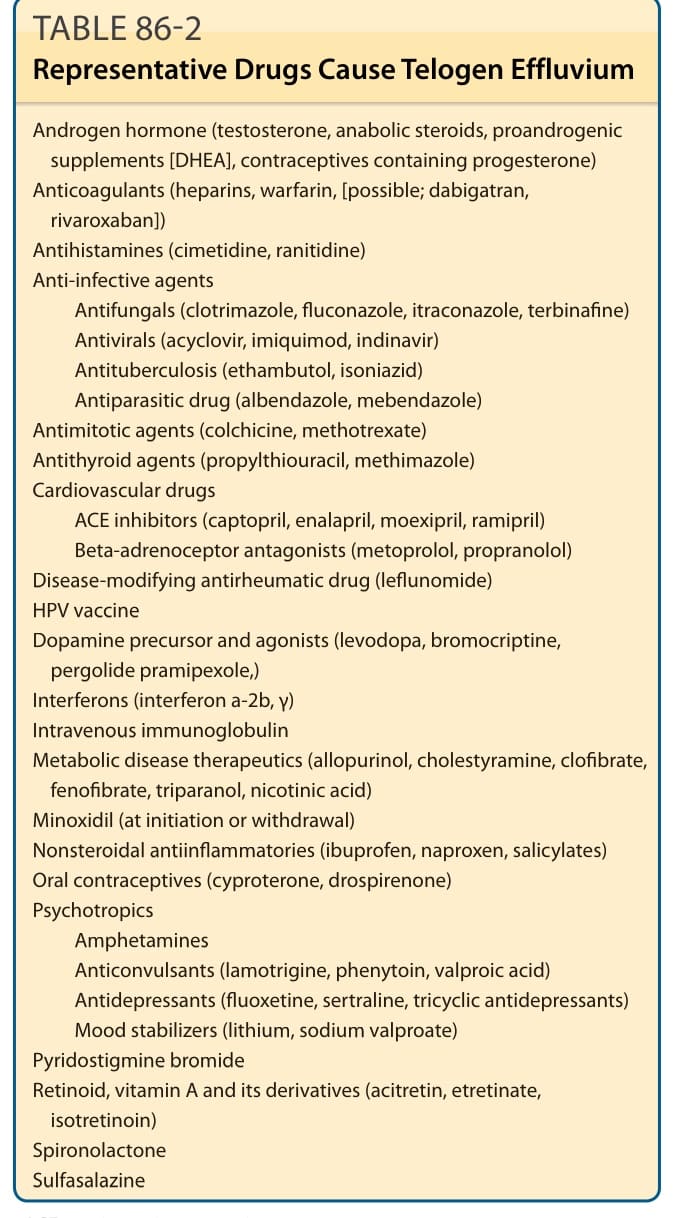
TABLE 86-2 Representative Drugs Cause Telogen Effluvium