Androgenetic Alopecia
PART16
Disorders of the Hair and Nails
AT-A-GLANCE
■ Androgenetic alopecia (AGA) is a nonscarring progressive miniaturization of the hair follicle in genetically predisposed men and women, usually in a specific pattern distribution.
■ AGA onset may be at any age following puberty, showing an increasing frequency with age.
■ The etiology of AGA is multifactorial and polygenic with, as of this writing, 12 genetic regions recognized to associate with AGA in men. In men, AGA is an androgen-dependent trait. Even though the role of androgens in female AGA is less certain than in men, there is a subset of women with AGA and associated hormonal dysregulation.
■ Generally, diagnosis of AGA is based on history and clinical examination. Depending on patient history and clinical evaluation, however, additional diagnostics may become necessary to exclude differential diagnoses; for example, ferritin level or thyroid-stimulating hormone in diffuse effluvium or endocrinologic workup in women with signs of hyperandrogenism.
■ Biopsy is very rarely indicated in AGA. Biopsy is indicated only if, for example, the differential diagnoses cicatricial alopecia or diffuse alopecia areata are suspected.
■ AGA has a naturally progressive course, meaning that the main therapeutic aim is the prevention of disease progression or enhancement of hair growth during the early, mild to moderate stages of the disease.
■ The best clinical evidence according to current study data exists for topical application of minoxidil in both genders and for the oral intake of finasteride in men. Alternatively, cosmetically satisfactory results can be achieved using hair transplantation in nonprogressive stable AGA with sufficient available donor area.
DEFINITION
Androgenetic alopecia (AGA) is the most common type of hair loss, a nonscarring progressive miniaturization of the hair follicle with shortening of the anagen phase in genetically predisposed men and women, usually in a specific pattern distribution.1
Life quality may be significantly impaired in affected individuals, independent of severity, age, or gender.
EPIDEMIOLOGY
Although AGA onset may be at any age following puberty, there is an increasing frequency with age. Reportedly, approximately 50% to 60% of men are affected by the age of 50 years increasing to approximately 80% by the age of 70 years and beyond.2,3 The prevalence of AGA is reportedly lower and its severity less among Asians, Native Americans, and African Americans compared to the European population.4,5 Approximately 10% to 20% of Chinese men are affected by the age of 40 to 49 years, rising to 40% to 60% by the age of 70 years and beyond.6,7
The frequency and severity of AGA is lower in women than in men, but it still affects a sizeable proportion of the population. Reported prevalence rates in white women in the United Kingdom and United States range between 3% and 6% in women younger than 30 years of age, increasing to 29% to 42% in women 70 years of age and older.8,9 AGA is less common and appears to start later in life in Asian women with a reported prevalence of 25% in Korean10 and of 12% to 15% in Chinese women 70 years of age and older.6,7
16
CLINICAL FEATURES
MALE PATTERN HAIR LOSS
MALE PATTERN HAIR LOSS
MALE PATTERN, HAMILTON- NORWOOD TYPE
This is the most frequent clinical pattern in men with AGA, and only occasionally observed in women. Recession of the frontal hairline, mainly in a triangular pattern is the characteristic finding, later followed by a vertex thinning with progression until the top of the scalp is completely bald (Figs. 85-1 and 85-2). Occipital area and sides of the scalp are spared even in longstanding male pattern hair loss.
FEMALE PATTERN HAIR LOSS
FEMALE PATTERN
HAIR LOSS
FEMALE PATTERN, LUDWIG TYPE
The so-called female pattern hair loss is characterized by a diffuse thinning of the centroparietal region with maintenance of the frontal hair line (Fig. 85-3). It is the most common type of AGA in women; it is occasionally observed in men. There are 2 scales describing this pattern, the 3-point Ludwig scale (Fig. 85-4) and the 5-point Sinclair scale (Fig. 85-5).
Hamilton-Norwood classification of male pattern hair loss
I II
IIa
III vertex III
IV
IIIa
V IVa
VI VII Va
1496
16
CHRISTMAS TREE PATTERN
Frequently observed in women, the Christmas tree pattern shows diffuse centroparietal thinning similar to the Ludwig pattern with an additional breaching of the frontal hair line (Fig. 85-6).
ETIOLOGY AND PATHOGENESIS
RISK FACTORS
RISK FACTORS
The etiology of AGA is multifactorial and polygenic.1
MEN
MEN
Male AGA is largely determined by genetic factors.11,12
There is a strong paternal influence on the risk of balding.3 Although once thought to be an autosomal dominant trait, it is now clear that AGA has a complex polygenic basis. As of this writing, molecular studies
Ludwig classification of female pattern hair loss
I II III
1497
16
Sinclair scale for grading female pattern hair loss
have recognized 12 genetic regions associated with AGA. Candidate genes include genes for the androgen receptor (AR), histone-deacetylases (HDAC) 4 and 9, and the WNT molecule WNT10A.13
In men, AGA is an androgen-dependent trait.14 Dihydrotestosterone is the androgen chiefly responsible for the follicular pathology. Dihydrotestosterone probably acts primarily on dermal papilla, the predominant site of androgen receptor and type II 5α-reductase expression within the hair follicle. A number of signaling molecules have been implicated in the inhibition of hair growth in AGA including transforming growth factor (TGF)-β1 and transforming growth factor-β2,14 dickkopf 1 (a member of the WNT signaling family),15 and interleukin-6.16 There is also evidence for involvement of prostaglandins in AGA. The enzyme prostaglandin D2 synthase and its product prostaglandin D2 are elevated in balding scalp skin; prostaglandin D2 has an inhibitory effect on hair growth in animal and in in vitro experiments.17
WOMEN
WOMEN
Less is known about the etiology of AGA in women. There is an increased frequency of balding in
Olsen scale
Male pattern (Hamilton) Diffuse (Ludwig) Frontal accentuation (Olsen)
1498
first-degree male relatives of women with AGA, which suggests there is at least some genetic commonality between female and male AGA.18 Case-control geneassociation studies have found a weak association between the AR/EDA2 locus and early-onset female AGA, but no association with the 11 autosomal loci that associate with male AGA.19-21 There is a weak association with the gene for estrogen receptor 2 (ESR2), which suggests the involvement of estrogenic pathways in female AGA.22,23 As of this writing there have been no genome-wide studies in women. The role of androgens in female AGA is also less certain than in men. Nevertheless, there is a subset of women with AGA and associated hormonal dysregulation.
DIAGNOSIS
Generally, AGA is a clinical diagnosis. Depending on patient history and clinical evaluation, further diagnostics may be necessary.
PATIENT HISTORY
PATIENT HISTORY
Patient and family history of the first manifestation of hair loss and of the course of hair loss (chronic or intermittent) should be documented. Patients with AGA usually complain about a longstanding, slowly progressing reduction of hair density, sometimes even without noticing significant hair loss. Patients typically describe hair thinning with an accentuation of the frontal, parietal, or vertex region, but diffuse thinning is possible as well. Pruritus and trichodynia may present as initial signs of AGA. The family history for AGA is often positive. A positive family history for other hair disorders may facilitate differential diagnostic conclusions and lead to further diagnostic procedures. In women, especially in those with peripheral signs of hyperandrogenism (Fig. 85-7), a gynecologic history is recommended, including among other possibilities, menstrual cycle disturbances and intake of hormonal contraception. Furthermore, a detailed patient history should be performed to rule out other causes for the hair loss or
16
aggravating factors. Patient interview should include systemic and newly diagnosed diseases (eg, infections, thyroid function disorders, and surgical procedures) that occurred 6 months to 1 year prior to the first signs of hair loss, and nutritional behavior (especially chronic deficient diet or rapid significant weight loss) possibly leading to diffuse effluvium (see section “Differential Diagnosis”). Lifestyle procedures, such as special hairstyles causing traction, and environmental factors like smoking and ultraviolet radiation exposure should be considered.1 A drug history should be taken to identify a possibly drug-related hair loss, such as after treatment with chemotherapeutic agents, hormones with proandrogenic or antithyroid action, intake of anabolic steroids, or supplemental androgens. Allergies and intolerances should be recorded as they might be important for the choice of the appropriate therapy (eg, contact dermatitis caused by propylene glycol in topical solutions)1 as well as cosmetic habits (eg, hair care and color, hair style).
CLINICAL EXAMINATION
CLINICAL EXAMINATION
Clinical examination should involve the scalp skin and hair, facial and body hair, and skin, as well as the nails.
SCALP EXAMINATION
The scalp skin usually appears normal in AGA, but frequently associated findings include seborrhea and/or seborrheic dermatitis.1 Inflammatory or infectious diseases, as well as alopecia areata and scarring alopecia
like lichen planopilaris or frontal fibrosing alopecia, which can mimic AGA, should be considered (see section “Differential Diagnosis”). Balding scalp examination should include checking for photodamage and field cancerization. Thus, clinical examination of the scalp should focus on possible signs of inflammation, like erythema, scaling, or hyperkeratosis, and signs of scarring, such as skin atrophy and loss of hair follicle ostia. However, atrophy of scalp skin also may be present in longstanding AGA.1
HAIR EXAMINATION Scalp Hair: Hair should be parted to assess scalp hair density. Part width should be compared between the frontal, occipital, and temporal regions to examine the distribution of alopecia (see Figs. 85-1 through 85-6, Hamilton-Norwood, Ludwig, and Olsen scales). Dermoscopy/trichoscopy can be helpful in assessing hair follicle openings to exclude scarring alopecia and in identifying short and fine miniaturized hairs. Hair caliber variations might also be present. The hair pull test (Sabouraud maneuver) can be implemented to provide information on hair shedding. For this test, approximately 50 to 60 hairs are grasped between the thumb, index, and middle fingers from the base of the hairs near the scalp and firmly, but not forcefully, tugged away from the scalp. If more than 10% of the grasped hairs are pulled away from the scalp, this constitutes a positive pull test and confirms active hair shedding.1 In AGA, the hair pull test may be positive in the frontal region, while it is typically negative in the occipital region.
1499
16
Facial and Body Hair Examination: Facial and body hair density and/or distribution changes can be found as a result of ethnic hypertrichosis, hypertrichosis caused by medications, or hirsutism. Signs of acne, seborrhea, oily skin, and obesity might present peripheral signs of hyperandrogenism. Even though some women with AGA complain of reduction of eyebrows or eyelashes, this finding points to other types of alopecia, like alopecia areata or frontal fibrosing alopecia (see section “Differential Diagnosis”)24 rather than to AGA.
NAIL EXAMINATION
Nail abnormalities are not characteristic for AGA, but may contribute to differential work up of alopecia areata, certain deficiencies, and lichen planus.1
DIAGNOSTIC TOOLS
DIAGNOSTIC TOOLS
DERMOSCOPY
Dermoscopy, a noninvasive technique, improves examination of scalp skin and hair shafts by magnification (eg, assessment of hair follicle openings, hair shaft caliber variations). The findings can be saved for future comparison using videodermoscopy. In AGA, hair diameter variations, loss of trio groups with single terminal hairs, and an increased number of vellus hairs can be seen.
GLOBAL PHOTOGRAPHY
Global photographs are helpful tools for the objective evaluation of the course of hair growth, hair volume, and hair density in clinical studies, and for long-term followup in daily practice. For followup assessment, a standardized technique should be implemented, for example, by using a stereotactic device assuring a constant view, magnification, and lighting.
AUTOMATIC DIGITALIZED SYSTEM FOR HAIR DENSITY AND ANAGEN/TELOGEN HAIRS (PHOTOTRICHOGRAM)
These systems allow measurement of hair density and the anagen-to-telogen ratio for diagnostic and followup purposes, but they are mainly used for standardized and reproducible tools in clinical studies. Typical findings in AGA are reduced hair density in a pattern distribution compared to the occipital area. The anagen-to-telogen ratio is normal or decreased when comparing frontal or vertex to the occiput. These techniques are helpful for long-term followup and quantification of hair density.
TRICHOGRAM
The trichogram is not indicated as a routine diagnostic tool in AGA. It should only be considered in individual
1500
cases to rule out other differential diagnoses or comorbidities.1 The trichogram should only be performed by dermatologists who are familiar with this technique and perform it routinely.
BIOPSY
A biopsy, mostly performed as a deep, 4-mm, cylindrical punch, is indicated in AGA only in cases where the diagnosis is uncertain, such as where scalp changes are suggestive of cicatricial alopecia or diffuse alopecia areata. Scalp biopsies should be evaluated by dermatopathologists who are experienced in hair pathology using both vertical and horizontal sectioning. The preferred area for biopsy is the central scalp in an area representative of the hair loss process. Biopsies should not be taken from the bitemporal area as miniaturized hairs may be present in this region independent of AGA.1 Histologically AGA presents an increased number and proportion of miniaturized (vellus-like) hair follicles with a typically less than 3:1 ratio of terminal to vellus-like hair follicles, compared with a greater than 7:1 ratio in the normal scalp. Other features include an increased telogen-to-anagen ratio and an increase in the number of follicular stelae (tracts beneath miniaturized follicles). A mild perifollicular lymphohistiocytic infiltration, primarily around the upper hair follicle, also may be present, as well as perifollicular fibrosis, in longstanding AGA.
LABORATORY TESTING
LABORATORY TESTING
In men, laboratory testing for the diagnosis of AGA is not necessary, except if the history or clinical examination indicate another underlying disorder or associated disease. Literature data indicate a possible positive association between AGA and insulin resistance, metabolic syndrome, hypertension, and benign prostate hyperplasia in men.25 Furthermore, laboratory testing might be indicated before introducing specific therapies (eg, measurement of the prostate-specific antigen value before introducing finasteride therapy; see section “Medications”). In women, an extensive endocrinologic workup is not necessary, except if the history and clinical examination indicate androgen excess. In this case, an interdisciplinary approach involving gynecologists, endocrinologists, and dermatologists is recommended to rule out/ distinguish between the different causes associated with hyperandrogenism, such as polycystic ovary syndrome, congenital adrenal hyperplasia, androgen-secreting tumors, or Cushing syndrome. For this purpose the free androgen index, sex hormone-binding globulin, and prolactin should be determined and further laboratory testing (eg, 17-OH-progesterone, follicle-stimulating hormone, estradiol, or cortisol) should be considered. The measurements should be optimally taken between 8:00 and 9:00 am, ideally between the second and fifth day of the menstrual cycle, in order to standardize and
facilitate interpretation. Furthermore, it is advisable to perform blood hormone testing at least 2 months after stopping any hormonal intake, including oral contraception, as estrogens lead to elevated sex hormonebinding globulin levels and consequently falsify the outcome of the free androgen index.1
Measurement of ferritin level or thyroidstimulating hormone may be considered depending on patient history, especially when diffuse effluvium is suspected. Literature data indicate a possible supportive role of adequate serum ferritin levels during treatment of diffuse androgen-dependent alopecia in women, even though contradictory data also have been published.1
Interdisciplinary evaluation must be decided individually, based on age, clinical findings, and associated findings. Especially in children and adolescents
16
with premature onset of AGA, an interdisciplinary approach involving the dermatologist and pediatric endocrinologist should be taken. If significant psychological distress is observed, especially in women and young patients with early onset of AGA, psychological referral should be considered for the development of coping strategies.
DIAGNOSTIC ALGORITHM
DIAGNOSTIC ALGORITHM
A diagnostic evaluation form for AGA has been proposed by the European Consensus Group that includes history, clinical examination, laboratory and hair examination tests, diagnostic techniques and clinical documentation (Fig. 85-8).1
Clinical algorithm for the diagnosis of androgenetic alopecia
Classify pattern
Perform test
Negative
Hair loss
YES
NO
No primary suspicion of AGA check DD
Pattern distribution?
Positive
Check DD in addition
No active hair loss Active hair loss
Examine scalp skin
Normal
Men Men Women
Seborrheic dermatitis
Women
YES
Further suspicion of AGA?
Pathologic
Other scalp disorders
Check DD
Women
Check for signs of hormonal dysregulation (menstrual cycle, body hair examination, acne, seborrhea)
Normal
Pathologic
Women
Women
AGA
Perform hormonal laboratory tests
Suspicion of hyperandrogenism refer to endocrinologist
Pathologic
Normal
1501
16
DIFFERENTIAL DIAGNOSIS
TELOGEN EFFLUVIUM
TELOGEN EFFLUVIUM
Telogen effluvium is an acute or chronic diffuse hair loss caused by an increased number of hair follicles in telogen, possibly leading in the time course to a reduced hair density over the entire scalp. Telogen effluvium is usually associated with a precipitating event, like a severe illness or psychological trauma, crash diet or certain medications, and the results of the hair pull test are diffusely positive (Fig. 85-9B).
DIFFUSE ALOPECIA AREATA
DIFFUSE ALOPECIA AREATA
Diffuse alopecia areata typically does not follow a patterned distribution. Although not always present, a personal or family history of alopecia areata, the detection of patchy or total hair loss, hair loss in other body sites, and nail abnormalities offer support to this
Telogen Effluvium
■Associated with precipitating event
■Hair pull test diffusely positive
Diffuse Alopecia Areata
■No pattern of distribution
■Personal or family history of alopecia areata
■Hair loss in other body sites
■Nail changes
Central Centrifugal Cicatricial Alopecia
■Scarring alopecia of the vertex region
■Most commonly in women of African descent
■Dermoscopy and histologic evaluation shows scarring alopecia
Frontal Fibrosing Alopecia
■Frontotemporal, band-like scarring
■Associated with loss of eyebrows
■Perifollicular erythema and hyperkeratosis
■Histology shows lymphocytic scarring alopecia
Early Traction Alopecia
■History of chronic tension in the hair shaft (tight braiding)
Hypotrichosis Simplex
■Diffuse, progressive loss of scalp and body hair from early childhood
■No anomalies of skin, nails, or teeth
Ectodermal Dysplasia
Ectodermal Dysplasia
■Skin, appendages, nails, and teeth associated
■Skin, appendages, nails, and teeth associated
■Delayed physical/psychological development and sweating disorders
■Delayed physical/psychological development and sweating
1502
disorders
diagnosis. A biopsy is useful for confirming the diagnosis if clinically not distinct (see Fig. 85-9A).
CENTRAL CENTRIFUGAL CICATRICIAL ALOPECIA
CENTRAL CENTRIFUGAL
CICATRICIAL ALOPECIA
Central centrifugal cicatricial alopecia is a scarring alopecia of the vertex region that most commonly occurs in women of African descent (Fig. 85-10A). The dermoscopic detection of loss of follicular ostia confirms the scarring type. Biopsies can be useful to confirm the diagnosis.
FRONTAL FIBROSING ALOPECIA
Frontal fibrosing alopecia is a frontotemporal bandlike scarring alopecia, characterized by frontotemporal band like recession, loss of eyebrows, perifollicular erythema and hyperkeratosis (see Fig. 85-10C, D). The detection of clinical and histologic signs consistent with a lymphocytic scarring alopecia aid in diagnosis.
TRACTION ALOPECIA
TRACTION ALOPECIA
Traction alopecia occurs as a result of chronic tension on the hair shaft (see Fig. 85-10B). Although the hair loss is reversible initially, hair loss may become permanent if tension on the hair follicles continues. History of tight braiding of the hair is useful for diagnosis.
HYPOTRICHOSIS SIMPLEX OR ECTODERMAL DYSPLASIA
HYPOTRICHOSIS SIMPLEX
OR ECTODERMAL
DYSPLASIA
It is important to differentiate between congenital or acquired hair loss in adolescents. Hereditary hypotrichosis simplex is characterized by diffuse and progressive hair loss of the scalp and the body, beginning during early childhood. There are no anomalies of the skin, nails, or teeth. The group of ectodermal dysplasias comprise a large, heterogenous group of inherited disorders involving the skin, its appendages, nails, and teeth. Delayed physical/psychological development and sweating disorders may be present.
CLINICAL COURSE AND PROGNOSIS
The course of AGA is naturally progressive, meaning that the main therapeutic aim is the improvement or even merely prevention of disease progression. This can mainly be achieved during the early, mild to
A
B
16
A B C D
1503
16
moderate stages of the disease. Irrespective of its clinical progression, AGA provokes significant distress and has an often underestimated psychosocial impact on the affected patients.26
MANAGEMENT
MEDICATIONS
MEDICATIONS
The best clinical evidence according to current study data concerns the topical application of minoxidil. Minoxidil prevents further progression of the disease and leads to an increase in hair density and hair thickness both in male patients older than 18 years of age with mild to moderate AGA (2% to 5% solution; 1 mL or half a cap of 5% foam twice daily) and female patients older than 18 years of age (2% solution; 1 mL twice daily or half a cap of 5% foam once daily). The response to treatment should be assessed at 6 months. If successful, treatment needs to be continued to maintain efficacy.27
The patients should be informed about transitory increased telogen hair shedding, usually appearing within the first 8 weeks of therapy initiation. Furthermore, after end of therapy with topical minoxidil, increased hair loss follows. The main side effect of topical minoxidil is hypertrichosis, mostly from local spreading or excessive continuous topical application. To avoid contamination of the pillow with subsequent facial contact patients should be advised to apply the drug at least 2 hours before going to bed. Irritant and allergic contact dermatitis may also occur. Irritation is more common with the 5% solution because of its higher content in propylene glycol. Contact dermatitis resulting from propylene glycol or from minoxidil itself should be confirmed by patch testing. It is recommended to pause topical minoxidil use during pregnancy and lactation, owing to the lack of data during this period.27
In male patients older than 18 years of age with mild to moderate AGA, a systemic therapy with the 5α-reductase type 2 inhibitor finasteride (1 mg/day) improves or to prevents progression of AGA. For greater efficacy, the combination of oral finasteride (1 mg once daily) and topical minoxidil can be considered. Patients under treatment with finasteride should be aware of reduction of prostate-specific antigen, which is important in prostate cancer screening in men. Further reported side effects of finasteride are impaired sexual function, including erectile dysfunction, ejaculation dysfunction, reduced ejaculate volume, and loss of libido. A possible negative impact of finasteride on those who have a constitutive predisposition to psychological disorders, leading to alteration of mood/depression has been reported; gynecomastia; testicular pain; hypersensitivity reactions; and possible negative impact on spermatogenesis in those men with preexisting conditions relating to infertility should be mentioned. Postfinasteride syndrome, defined as various symptoms persisting for months or years after discontinuation of finasteride treatment, including sexual dysfunction, loss
1504
of libido, depression, suicidal ideation, impaired cognition, fatigue, and decreased penile sensitivity, probably occurring in men with a history of sexual dysfunction or a personal or family history of psychiatric illness, are also discussed in the literature. Consequently, finasteride is contraindicated in patients with active depression or current sexual dysfunction. The response to treatment should be assessed at 6 months, although in some men it may not become evident before 12 months. If successful, treatment needs to be continued to maintain efficacy. In case of ineffective treatment with 1 mg finasteride over 12 months, the off-label use of the 5α-reductase inhibitor dutasteride, which inhibits the isoenzymes type 1 and type 2, at a dose of 0.5 mg a day can be considered. Finasteride is not indicated in women and is contraindicated in pregnant women and women of childbearing potential, because of the risk of feminization of a male fetus. Finasteride-treated men must avoid donating their blood.27
In female postmenopausal patients, finasteride 1 mg failed to show efficacy; however, finasteride 5 mg may be effective in female normoandrogenic premenopausal and postmenopausal patients. However, no placebo-controlled trials are available in this population. In women of childbearing age, the use of a safe contraceptive method is indispensable.27
Clinical studies on the efficacy of topical finasteride preparations are currently underway. Antiandrogens and estrogenic drugs are being used in the treatment of AGA, although evidence of efficacy for any of these treatments is insufficient. In male patients, the use of systemic estrogens or androgenreceptor antagonists is not recommended. In women with AGA and clinical or biochemical evidence of hyperandrogenism, the use of oral antiandrogens (chlormadinone acetate, cyproterone acetate, drospirenone, spironolactone, flutamide) in combination with an estrogen as an oral contraceptive pill can be considered. Side effects of cyproterone acetate include depressive mood changes and liver toxicity. There is an increased risk of venous thromboembolism in patients taking estrogen-containing oral contraceptives, which may be greater in those taking cyproterone acetate than other oral contraceptives. Spironolactone 100 to 200 mg per day taken continuously is an alternative option because of its antiandrogenic effect, but should also be combined with a safe contraceptive in women of childbearing age. Side effects include menstrual disturbances and hyperkalaemia.27
As of this writing, there is insufficient literature evidence on the effect of topical alfatradiol, topical natural estrogens or progesterones, or topical fluridil.27
PROCEDURES
PROCEDURES
SURGERY
In AGA, hairless or thinning areas can be cosmetically covered, albeit with a decreased density, using
hair restoration surgery. Hair restoration surgery involves hair transplantation, scalp reduction surgery, or a combination of both. Hair transplantation is less invasive than scalp reduction surgery. Over the last decades, hair transplantation has evolved into a microsurgical procedure. Follicular units of 1 to 4 hairs are transplanted in large numbers and high densities. Hair surgery, especially follicular unit transplantation, can be considered to improve AGA in suitable patients with sufficient donor hair supply and medically controlled or spontaneously stabilized AGA, especially in the frontoparietal area. The result greatly depends on the skills of the surgical team and the adjustment of the surgical plan to individual patient characteristics. As hair surgery does not influence progression of AGA, long-term results in early stages depend on spontaneous or medical stabilization of AGA. In men, a combination of finasteride 1 mg and/or topical minoxidil with follicular unit transplantation may reduce postoperative progression of AGA.27
NONPERMANENT HAIR REPLACEMENT MEASURES
Nonsurgical hair replacement methods include, in addition to full and partial hair replacement measures (wigs), various hair-binding techniques and hair extension and supplementation techniques, either performed by the patients themselves (eg, sprinkle hair) or by specialized personnel (eg, camouflage techniques, bonding).28
INTERVENTIONS Low-Level Laser Therapy: Low-level laser therapy, including the exposure of tissues to low levels of visible or near infrared light, can be used as an ancillary treatment for AGA. Low-level laser therapy can be performed at home, using a LaserComb or wearing for a certain amount of time a helmet whose power cord is plugged into a standard outlet. Duration of therapy and frequency varies for the different devices. Current studies evaluating laser devices show inconsistent results thus providing low quality evidence.27 However, an improvement in total hair count has been partly reported after using such devices.29,30
MISCELLANEOUS
MISCELLANEOUS
Besides the above-mentioned evidence-based therapeutic approaches, there is a wide range of molecules, products, and interventions claiming to promote hair growth in AGA. These include platelet-rich plasma, mesotherapy, botulinum toxin injections, pulsed electromagnetic/static field devices, topically applied caffeine, melatonin, retinoids, biochanin A,
16
adenosine, prostaglandin analogs, herbal preparations, and nutritional supplements (eg, biotin, zinc, copper, amino acids, micronutrients and combination preparations). For most of these products controlled clinical studies are scarce and largely of low evidence level. Detailed information on these products and the available literature can be found in the current S3 guidelines for the treatment of AGA in women and in men.27 Based on currently available literature data no evidence-based recommendation can be given for these miscellaneous products. Their use as a supportive strategy within an individually tailored management approach is at the discretion of the treating dermatologist and the decision of the patient. Further controlled studies to prove the relevance of these and other new approaches in the treatment of AGA are needed.
COUNSELING
COUNSELING
AGA is the most common hair loss disorder, affecting both men and women. Taking into account the high prevalence and the psychosocial burden and the often significant impairment of life of affected patients, the need for competent counseling and development of a trusting patient–physician relationship becomes apparent. To enhance therapy compliance, the patient must be informed in detail about the therapeutic goal, the possible treatment options, and their potential side effects. The naturally progressive nature of the disease should be pointed out, as well as the often limited response to therapy, particularly in advanced AGA. Practical counseling with tips on handling the disease in daily life should be offered. In individual cases with high emotional overlay, particularly in women, professional psychological help might be helpful. Overall, counseling dermatologists should develop a therapeutic personalized plan for each patient based on clinical status, demands, needs, and complaints. The individualized concept should comprise pharmacologic evidence-based recommendations, hair care and cosmetic tips, and psychological counseling. The physician and patient must decide together on the best suited individualized therapy, considering the expected results, practicality, and compliance.
SCREENING
SCREENING
Early diagnosis and treatment to prevent progression of AGA is important in genetically predisposed families. In patients with longstanding advanced AGA, especially in male pattern baldness, scalp examination should include screening for benign and malignant skin lesions, such as actinic keratoses, squamous cell carcinoma or basal cell carcinoma as a result of increased ultraviolet exposure of the balding scalp and the lack of protecting full hair.
1505
16
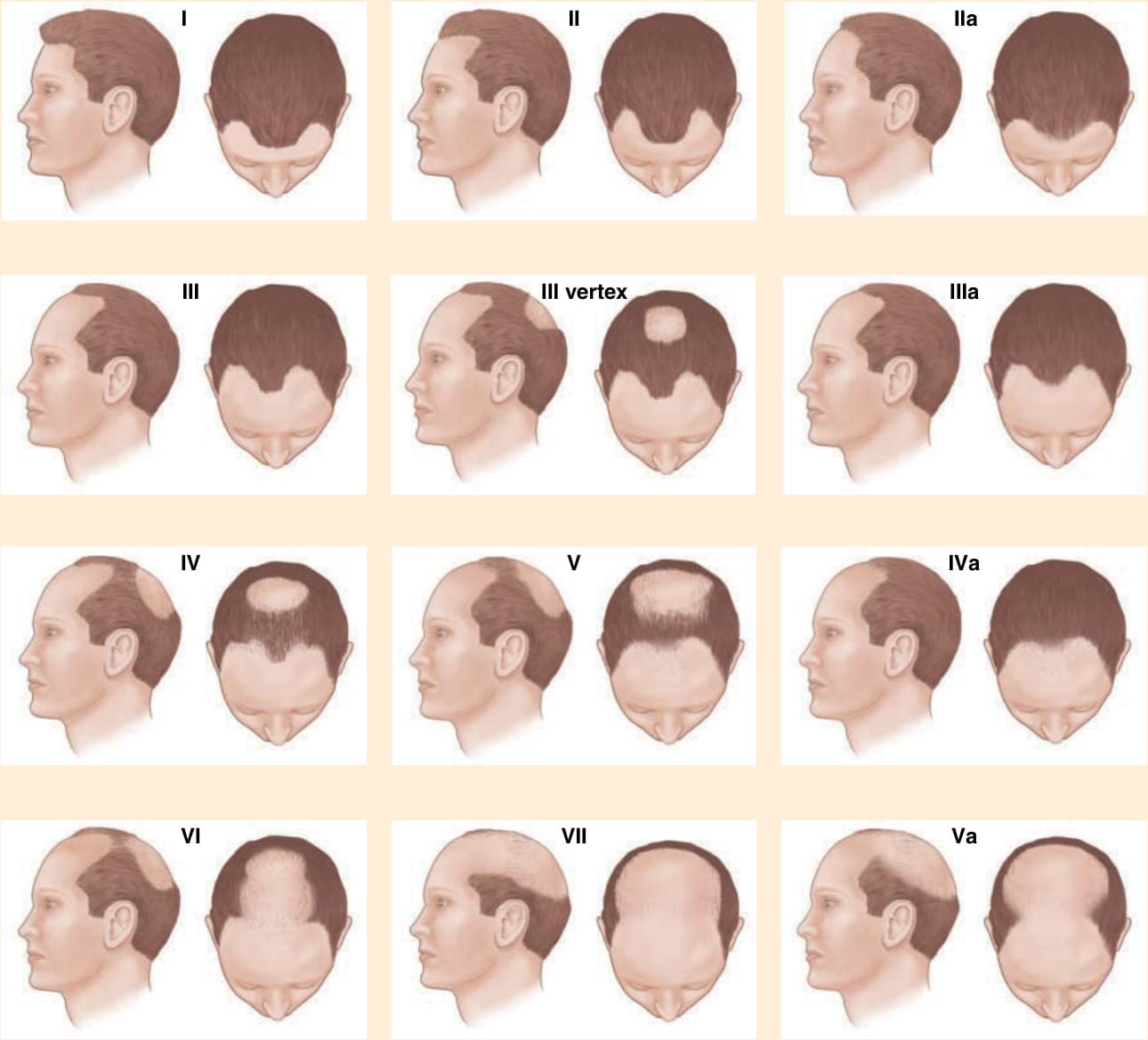
Figure 85-1 Hamilton-Norwood classification. (Redrawn from Blume-Peytavi U, Blumeyer A, Tosti A, et al. S1 guideline for diagnostic evaluation in androgenetic alopecia in men, women and adolescents. Br J Dermatol. 2011;164[1]:5-15.)

Figure 85-2 Male-pattern androgenetic alopecia, grade III vertex according to the Hamilton-Norwood classification. Standardized global photography overview (Canfield system).

Figure 85-3 Female pattern androgenetic alopecia, grade III according to the Ludwig classification.
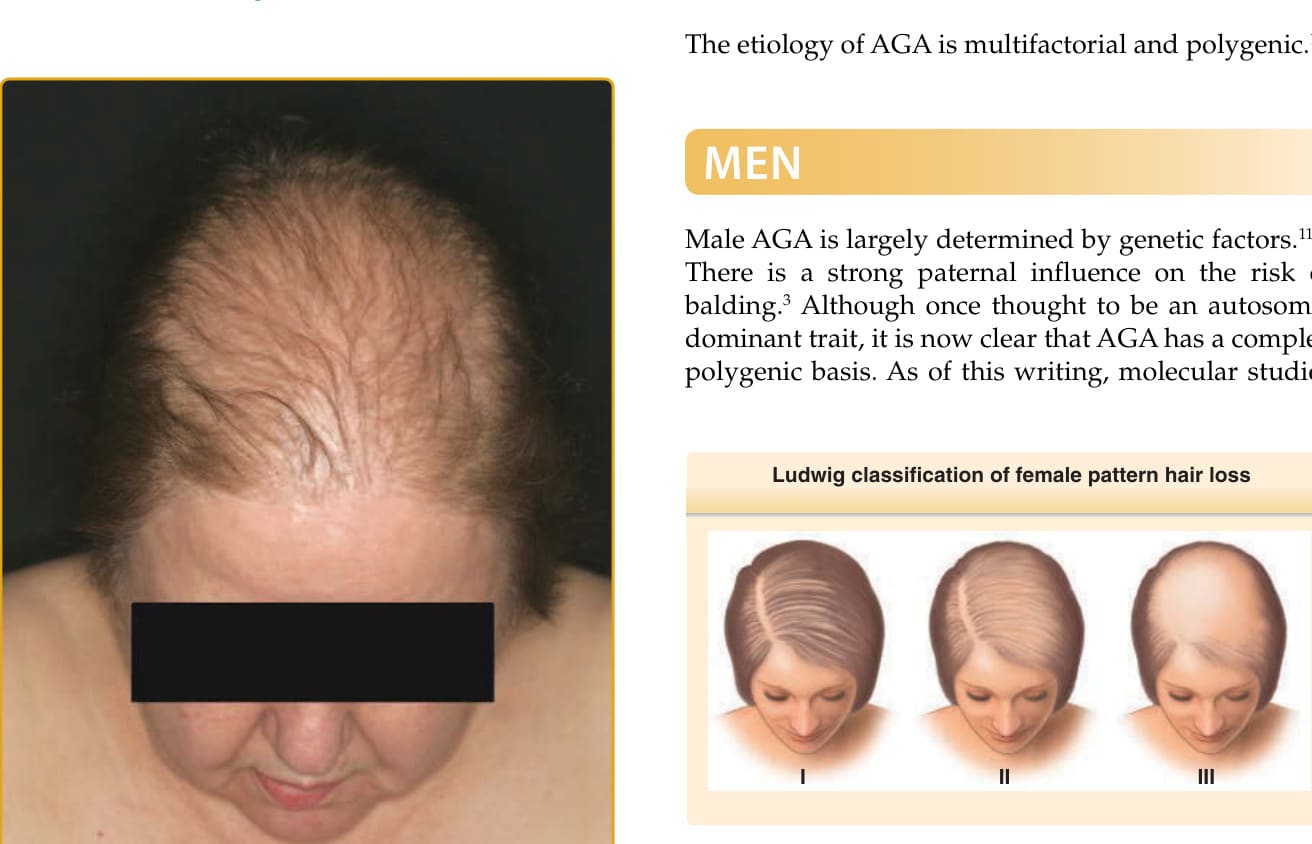
Figure 85-4 Ludwig pattern of hair loss (3-point scale). (Redrawn from Blume-Peytavi U, Blumeyer A, Tosti A, et al. S1 guideline for diagnostic evaluation in androgenetic alopecia in men, women and adolescents. Br J Dermatol. 2011;164[1]:5-15.)

Figure 85-5 Sinclair scale for grading female pattern hair loss (5-point scale). (Redrawn from Blume-Peytavi U, Blumeyer A, Tosti A, et al. S1 guideline for diagnostic evaluation in androgenetic alopecia in men, women and adolescents. Br J Dermatol. 2011;164[1]:5-15.)
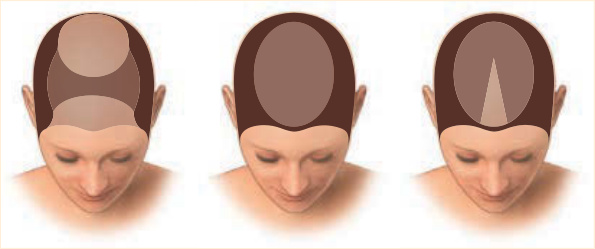
Figure 85-6 Olsen scale: Christmas tree pattern in female pattern hair loss. (Redrawn from Blume-Peytavi U, Blumeyer A, Tosti A, et al. S1 guideline for diagnostic evaluation in androgenetic alopecia in men, women and adolescents. Br J Dermatol. 2011;164[1]:5-15.)

Figure 85-7 Female pattern androgenetic alopecia, facial hypertrichosis, and seborrhea oleosa in an adolescent 15-year old girl.
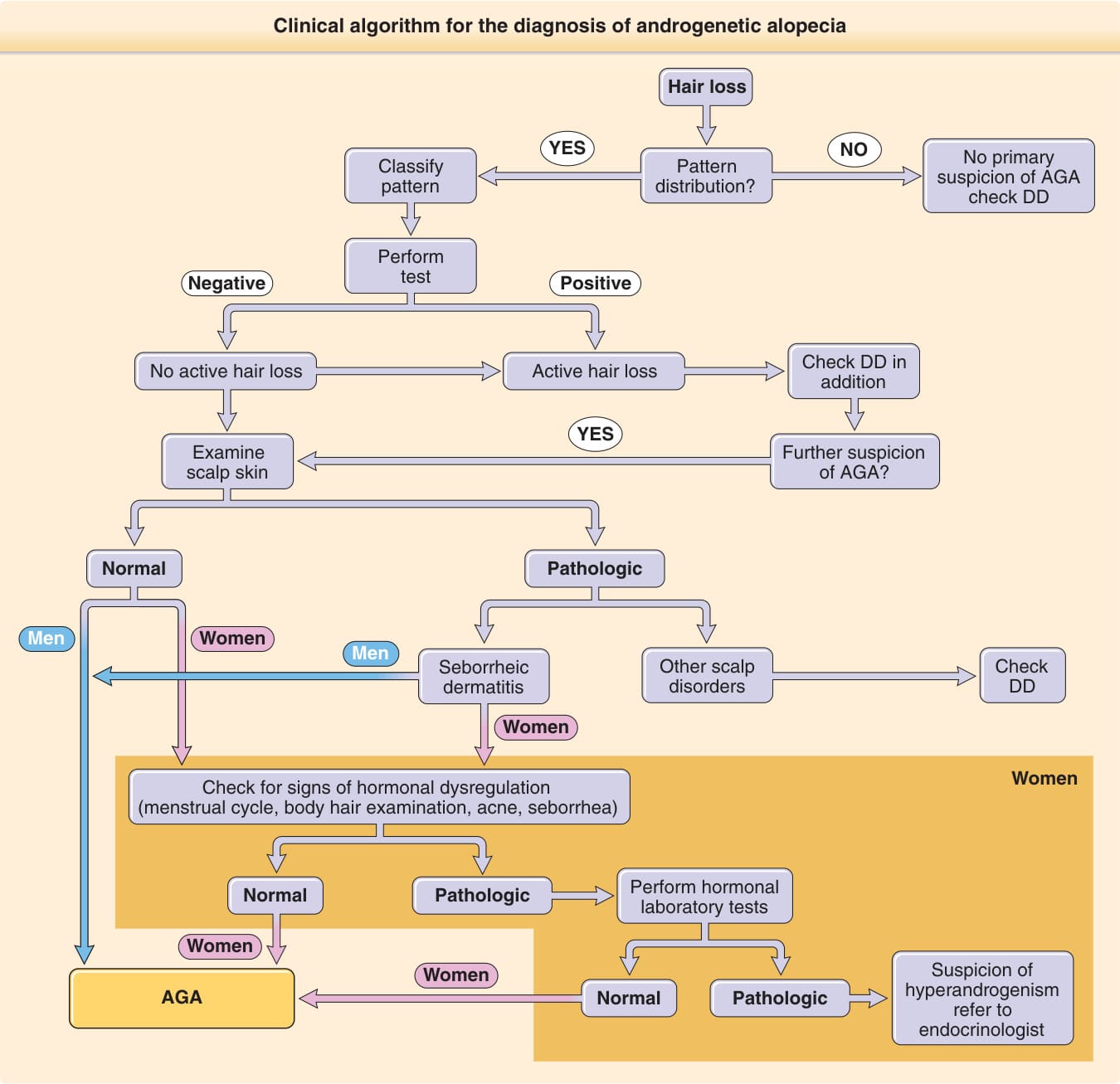
Figure 85-8 Clinical algorithm for the diagnosis of androgenetic alopecia (AGA). DD, differential diagnosis. (Adapted from Blume-Peytavi U, Blumeyer A, Tosti A, et al. S1 guideline for diagnostic evaluation in androgenetic alopecia in men, women and adolescents. Br J Dermatol. 2011;164[1]:5-15, with permission. Copyright © 2011 John Wiley & Sons.)

Figure 85-9 Differential diagnosis between female pattern androgenetic alopecia and (A) diffuse alopecia areata or (B) diffuse effluvium may present a challenge; a detailed patient and family history, laboratory testing and/or biopsy might be necessary.

Figure 85-10 Hair disorders mimicking androgenetic alopecia. A, Central centrifugal cicatricial alopecia; B, traction alopecia; C, frontal fibrosing alopecia; and D, coexisting frontal fibrosing alopecia and androgenetic alopecia Ludwig grade III in a postmenopausal woman.
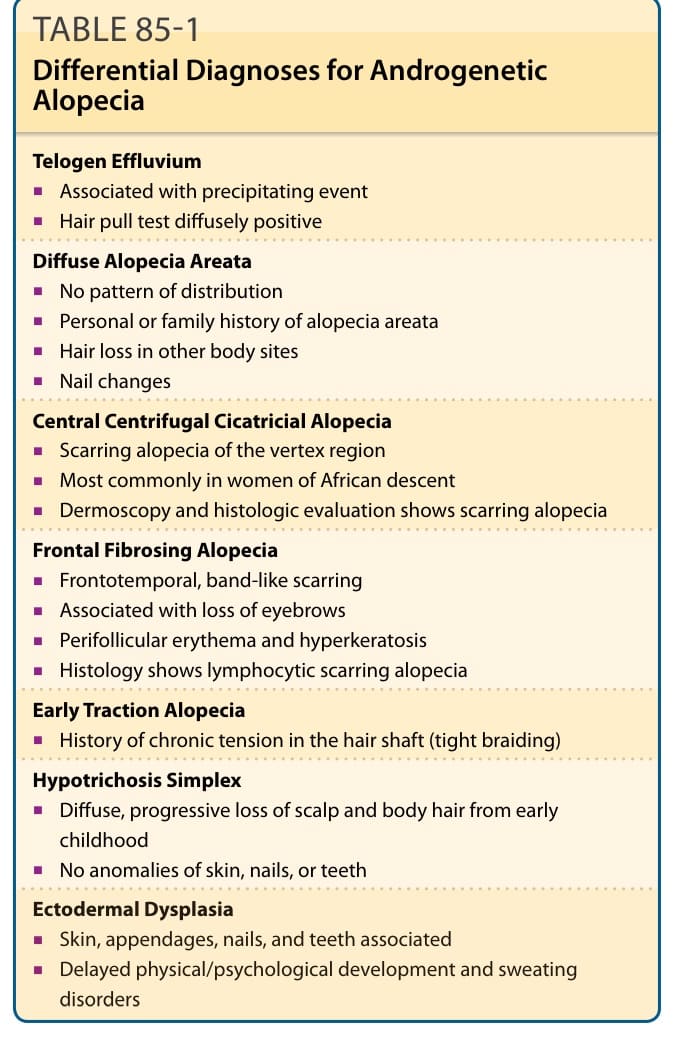
Table 85-1 outlines the differential diagnosis of AGA. Multiple hair and scalp disorders may present with clinical features that resemble or coexist with AGA.