Hidradenitis Suppurativa
15
AT-A-GLANCE
■ Hidradenitis suppurativa is a chronic and debilitating inflammatory disorder of the hair follicles that localizes to intertriginous and anogenital regions of the body.
■ Lesions are characterized by inflammatory nodules, subcutaneous abscesses, and sinus tracts.
■ Reproductive-age women are disproportionately affected.
■ Hyperkeratotic plugging of the terminal hair follicle is a consistent histologic finding of early disease and is thought to be the primary pathophysiologic event.
Hidradenitis suppurativa (HS), otherwise known as acne inversa, is a multifactorial, chronic inflammatory disorder of the hair follicles in intertriginous and anogenital regions of the body. HS is characterized by recurrent, deep-seated, painful, subcutaneous nodules, sinus tracts, and hypertrophic scarring. The long-term sequelae, including chronic pain, skin contractures, and disfigurement, can detrimentally impact activities of daily living, social functioning, and psychosocial well-being.1,2
EPIDEMIOLOGY
Robust epidemiologic data on HS is lacking. The reported point prevalence of HS worldwide is between 0.00033% and 4.1%.3 As of this writing, only 1 population-based incidence study has been published.4 Among residents of Olmsted County, Minnesota (population 144,000 in 2010), the overall annual age- and sex-adjusted incidence rate of HS was 6 per 100,000 person-years over a 40-year period.4
Between 1970 and 2008, the age- and sex-adjusted incidence rate rose steadily from 4.3 per 100,000 personyears to 9.6 per 100,000 person-years.4 The etiology of this trend is unclear but may be related to concomitant rises in risk factors among the general population, including obesity and metabolic syndrome, as well as improved physician recognition of HS.5
For unknown reasons, women are disproportionately affected (female-to-male ratio is 3.3:1) and more likely to develop axillary and genitofemoral lesions.4
Men, on the other hand, tend to develop perineal and perianal disease.4 Among women, the impact of menstruation, menopause, and pregnancy on the natural history of HS is inconsistent and warrants further study. Although unconfirmed by population-based
studies, data suggests that black patients may be disproportionately affected by HS.6-9
CLINICAL FEATURES
HS is a chronic relapsing and remitting disease with an unpredictable clinical course, leading to detrimental impacts on quality of life. Lesions may begin as tenderness or pruritus that progresses to a tender papule or deep-rooted nodule (Fig. 84-1). Nodules can become quite large and painful. They may resolve slowly without drainage or progress to an abscess-like lesion that eventually ruptures and drains purulent material before involuting (Fig. 84-2). Involution may take 7 to 10 days,10 but in some patients, healing may be delayed, resulting in persistent open wounds with variable amounts of granulation tissue (Fig. 84-3). The process then reoccurs in adjacent and/or other intertriginous sites. With repeated episodes, epithelial strands may develop from ruptured follicular epithelium,11 leading to sinus tract formation and intermittent drainage of foul-smelling serosanguinous and/or purulent material (Fig. 84-4). Over time, the healing process leads to exuberant scar formation, depositing densely fibrotic dermal plaques and ropelike bands (Fig. 84-5). The long-term disease sequelae, including dermal contractures and disfigurement, can detrimentally impact activities of daily living, social functioning, and psychosocial well-being (Figs. 84-6 to 84-8).1,2
COMPLICATIONS
QUALITY OF LIFE
QUALITY OF LIFE
HS is a burdensome and distressing disease that has a detrimental impact on quality of life. The degree of quality-of-life impairment, as measured by the Dermatology Life Quality Index, is more severe for HS than for other dermatologic conditions, including alopecia, psoriatic arthritis, and chronic urticaria.1,12
The highest single Dermatology Life Quality Index score is for disease-associated pain and discomfort.12
Anogenital involvement is associated with a significantly worse Dermatology Life Quality Index score compared to other sites.13 HS-associated debility may cause professional setbacks. In one report, HS resulted in work absences in 58.1% of patients.13
Work absences occurred 1 to 10 times per year, totaling 33.6 days lost on average per patient per year (SD: 26.1 days).13 Twenty-three percent of patients reported hindrance of professional advancement secondary to disease-related morbidity.13
SYSTEMIC COMPLICATIONS
SYSTEMIC COMPLICATIONS
A small number of patients (4% to 6%) may develop a normocytic and/or microcytic anemia of little clinical significance secondary to chronic inflammation.14
Rare cases of renal amyloidosis associated with severe HS have been reported.15 Sepsis arising from infected lesions is a rare but fatal complication.16
15
LOCAL COMPLICATIONS
LOCAL COMPLICATIONS
Fibrosis and dermal contractures can limit joint mobility. Vaginal, urethral, and/or anal strictures can develop from chronic anogenital and perineal inflammation, leading to incontinence.17 Urethral fistulization secondary to genital involvement has been reported.8
Inflammation, scarring, and destruction of lymphatic drainage routes can lead to disfiguring elephantiasis (see Fig. 84-7)18 and verrucous lymphangiomas,19
requiring surgical reconstruction.
1481
15
SQUAMOUS CELL CARCINOMA
SQUAMOUS CELL
CARCINOMA
Squamous cell carcinoma (SCC) is an infrequent complication of longstanding chronically inflamed lesions, occurring in 4.6% of HS cases (see Fig. 84-8).20 As of this writing, a total of 86 cases of SCC arising from HS
1482
lesions had been recorded in the literature.21 Males with anogenital disease are preferentially affected.20,21
HS-associated anogenital SCC is often associated with high-risk human papillomavirus strains, most commonly human papillomavirus-16.22 HS-associated SCC also tends to be more locally aggressive and metastasizes to lymph nodes with greater frequency (50% of cases) than SCC from any cause (5% to 10% of cases).20
Thus, practitioners should have a low threshold to biopsy any nonhealing wound in an area of chronic HS. Patients with HS are deemed to be at 50% greater risk of developing malignancies of any kind compared to the healthy individuals,23 although smoking status is not accounted for in the calculation of this statistic.
ETIOLOGY AND PATHOGENESIS
The etiology of HS is multifactorial and remains to be fully elucidated. It is likely that a combination of factors, including genetic predisposition, aberrant immunity, hormonal dysregulation, and environmental modifiers, are involved in the pathophysiology of this complex disease.
FOLLICULAR OCCLUSION
FOLLICULAR OCCLUSION
Keratinous occlusion of the terminal hair follicle is a consistent histologic finding of early HS24 and is thought to be the primary pathophysiologic event.25 An aberrant immune response to commensal flora25 and/ or shear forces causing microtrauma to the deep part of the hair follicles in intertriginous skin26 are believed to contribute to the initial lymphocytic perifolliculitis, hyperkeratosis, and hyperplasia of the infundibular epithelium.24 This accumulation of keratinous debris leads to plugging and dilation of hair follicles. With subsequent rupture, follicles expel their contents (keratin, hair, sebum, bacteria) into the surrounding dermis. This incites a florid lymphohistiocytic foreign-body– type inflammatory response that engulfs the pilosebaceous units and adnexal structures, giving rise to the clinical findings.
ADNEXAL STRUCTURES
ADNEXAL STRUCTURES
HS was once thought to originate in the apocrine glands. It is now clear, however, that the apocrine glands are only secondarily involved.27 On the other hand, sebaceous gland atrophy appears to be an early event in disease pathogenesis, preceding the onset of lymphocytic follicular inflammation and hyperkeratosis of the infundibulum.28 Whether sebaceous gland atrophy represents a primary event or is a reflection of upstream processes remains to be determined.
GENETICS
GENETICS
HS can develop sporadically or be inherited in familial forms. One-third of patients with HS report a positive family history of the disease.29 Familial forms are thought to arise from autosomal dominant inheritance of highly penetrant single gene mutations, whereas sporadic cases are thought to result from defects in several genes.29,30 Loss-of-function mutations in the genes encoding subunit proteins of the γ-secretase complex—presenilin (PSEN1/ PSEN2), presenilin enhancer-2 (PSENEN), nicastrin (NCSTN)—also have been identified in families with HS.31,32 In animal models, γ-secretase deficiency leads to sebaceous gland atrophy, a histologic finding in HS, as well as epidermal cyst formation.33 Defective γ-secretase also impairs the Notch signaling pathway, which mediates normal hair follicle development, promotes antiinflammatory regulatory T-cell activity, and suppresses toll-like-receptor–induced proinflammatory responses.34,35 Together, these data suggest that defective γ-secretase and/or Notch signaling may serve a pathophysiologic role in HS. No associations between human leukocyte antigen antigens and HS have been reported.36,37
15
SMOKING
SMOKING
According to a multivariate analysis, the odds of having HS are substantially higher among current smokers than nonsmokers (odds ratio [OR] 12.55; 95% confidence interval [CI] 8.58 to 18.38).38 Smoking also is associated with the development of more-severe disease.39 Whether smoking is merely a risk factor or plays a direct role in disease pathogenesis is still controversial. Nicotine is thought to promote follicular occlusion by increasing sweat gland secretion and inducing hyperplasia of the follicular infundibulum.39 Nicotine is also thought to induce neutrophil chemotaxis and stimulate release of proinflammatory cytokines.40
Smoking cessation may improve symptoms41 as well as reduce the rates of de novo lesion formation following excisional surgery.42
ANDROGENS
ANDROGENS
The propensity for HS to develop after puberty suggests an androgenic basis for the disease. However, the role of androgen remains unclear. Androgen modulation therapy has demonstrated therapeutic benefit equivalent to that of oral antibiotic therapy.43 Yet, after adjusting for body mass index, there was no significant difference in the level of circulating androgens between women with HS and healthy controls.44,45
Additionally, the expression of androgen receptors46
and the 5-α-reductase enzyme47 on the apocrine glands is similar in HS lesions and healthy skin.
OBESITY
OBESITY
A higher body mass index is associated with greater odds of having HS (OR 1.12; 95% CI 1.08 to 1.15).38 Obesity is likely not causative but rather exacerbates HS via augmenting tissue mechanics, that is, promoting sweat retention and occlusion, and increasing friction and maceration in skinfolds.39 Greater adiposity may also alter the androgenic milieu by reducing global levels of sex hormone-binding globulin44 and/or augmenting peripheral conversion of sex hormones.47,48
Weight loss is recommended in overweight patients with HS. A study found that weight loss of more than 15% after bariatric surgery was associated with a 20% reduction in active disease.41
IMMUNE DYSREGULATION
IMMUNE DYSREGULATION
A growing body of literature implicates immune dysregulation as an integral part of disease pathogenesis.49
The proinflammatory cytokine, tumor necrosis factor (TNF)-α, is markedly elevated in HS lesions and in the serum of patients with HS compared to healthy
1483
15
controls.50 Interleukin (IL)-1β, another potent proinflammatory cytokine, is also strikingly elevated in lesional and perilesional skin (34- to 115-fold higher in lesional compared to healthy skin).49 IL-1β can promote inflammation by driving differentiation of IL-17– secreting CD4+ helper T cells (Th17) cells. The IL-23/ Th17 pathway is implicated in numerous autoimmune diseases, including rheumatoid arthritis, lupus, multiple sclerosis, and psoriasis.51 Levels of IL-12 and IL-23 are significantly elevated (2.6- to 5.2-fold) in lesional HS skin compared to that of healthy controls,52 with an increased number of Th17 cells infiltrating the dermis in the lesional HS skin compared to healthy skin.52
BACTERIA
BACTERIA
Whether bacterial involvement of HS lesions is a primary or secondary pathophysiologic event remains controversial. Traditional bacterial cultures taken from involved sites are often negative or grow commensal skin flora.53 Coagulase-negative staphylococcus and anaerobic bacteria are the most frequently isolated organisms.53 Deeptissue samples from the dermis grow a preponderance of coagulase-negative staphylococcus.53 It has been postulated that an overzealous immune response to commensal flora within hair follicles triggers the initial follicular inflammation.25,54 Topical and oral antibiotics tend to improve symptoms in most patients; however, long courses of therapy are often needed, and relapse is common. Bacterial biofilm formation may help explain the intractability of skin lesions despite long-term antibiotic therapies.55
COMORBIDITIES AND ASSOCIATED DISEASES
HS is frequently associated with other diseases of follicular occlusion. The tetrad of HS, acne conglobata, dissecting cellulitis of the scalp, and pilonidal cysts is well documented.56 HS also has been described as a component of several autoinflammatory syndromes, including PASH (pyoderma gangrenosum, acne, and HS),57 PAPASH (pyogenic arthritis, pyoderma gangrenosum, acne, and HS),58 and PsAPASH (psoriatic arthritis and PASH).59 Mutations in the NCSTN60
and PSTPIP1 (proline-serine-threonine phosphatase interacting protein 1)61 genes have been observed in PASH. Improvement of PASH and PAPASH with IL-1 receptor antagonist therapy suggests IL-1β may also play a pathogenic role.57,58 HS is also associated with inflammatory bowel disease.62,63 Twenty-six percent of patients with Crohn disease and 18% of patients with ulcerative colitis reported having HS.62 Coexistence of Crohn disease and HS is associated with a more fulminant disease course, especially in patients with perianal involvement.64 However, patients with HS do not appear to harbor CARD15/NOD2 polymorphisms associated with the inflammatory pathways of
1484
Crohn disease.65,66 Clinical improvement of concurrent Crohn disease and HS with anti–TNF-α therapy has been reported.67 Seronegative spondyloarthropathies, amyloidosis, genetic keratin disorders, and SCCs are also commonly cited in patients with HS.56 Several large studies have demonstrated that disease of hormonal and/or metabolic disequilibrium are frequently comorbid with HS.68-70 Patients with HS had significantly higher odds of also having metabolic syndrome (OR 1.61; 95% CI 1.36 to 1.89), diabetes mellitus (OR 1.41; 95% CI 1.19 to 1.66), obesity (OR 1.71; 95% CI 1.53 to 1.91), and hypertension (OR 1.14; 95% CI 1.02 to 1.28).70
DIAGNOSIS
HS is a clinical diagnosis based on 3 criteria (Table 84-1), all of which must be present for the definitive diagnosis. First, typical lesions must be present. These include deep-seated painful nodules, abscesses, draining sinuses, double-open comedones (Fig. 84-9), and bridged scars. It is important to distinguish HS lesions from common mimickers, including simple folliculitis and bacterial furunculosis (Table 84-2 outlines the differential diagnosis for HS). Second, lesions must exhibit a typical distribution, with 1 or more typical lesions in the axillae, groin, buttocks, perineal, or inframammary region. Nonclassical or ectopic sites may be present (eg, thighs, abdominal skinfolds) but must be accompanied by lesions in typical areas. Sites of involvement, in decreasing frequency, are: axillary, inguinal, perineal and perianal, mammary and inframammary, buttock, pubic region, chest, scalp, retroauricular, and eyelid.71 Third, there must be a clear history of symptom chronicity and recurrence.38,72 No formal guidelines for the clear history criteria exist. Delays in diagnosis are not uncommon, with 7 years being the average time from symptom onset to diagnosis.10 Having 2 recurrences over a 6-month period has been suggested as one measure of chronicity.3 Figure 84-10 provides an example of a proposed diagnostic algorithm.73
SEVERITY
SEVERITY
The Hurley staging system (Table 84-3) is the most widely used approach to assessing disease severity.
-
Typical lesion (1 or more): painful nodules, abscesses, draining sinuses, double-open comedones, bridged scars
-
Typical distributiona: axillae, groin, buttocks, perineal, and inframammary regions
-
Chronicity and recurrence of symptoms
-
Typical lesion (1 or more): painful nodules, abscesses, draining
sinuses, double-open comedones, bridged scars
2. Typical distributiona: axillae, groin, buttocks, perineal, and infra-
mammary regions
3. Chronicity and recurrence of symptoms
aAtypical or ectopic sites may be affected but at least 1 typical area must be involved.
Stage I is defined by recurrent abscesses without scarring or sinus tracts; stage II is defined by recurrent abscesses with scarring and sinus tract(s), separated by normal skin; and stage III is defined by recurrent abscesses with diffuse scarring and interconnected sinus tracts with minimal to no normal skin between lesions.74 The vast majority of HS patients (68%) have stage I disease; stage II and stage III disease develop in 28% and 4% of HS patients, respectively.74,75
Although useful for rapid classification of disease severity, the Hurley system does not account for the dynamic changes of lesion progression and regression, which are important for assessing therapeutic response. Other scoring systems have been developed to more accurately capture disease nuance. These systems include the Sartorius score,76 an HS-specific Physician Global Assessment,77 the HS Severity Index,78 and the HS Clinical Response Score.79 These systems, however, are generally considered too cumbersome for clinical practice but remain useful in research settings.
EARLY LESIONS LATE LESIONS
Acne vulgaris Carbuncle Cellulitis Cutaneous blastomycosis Dermoid cyst Erysipelas Folliculitis Furuncle Inflamed epidermoid cysts Lymphadenopathy Perirectal abscess Pilonidal cyst
Actinomycosis Anal fistula Cat scratch disease Crohn disease Granuloma inguinale Ischiorectal abscess Lymphogranuloma venereum Nocardia infection Noduloulcerative syphilis Pilonidal disease Tuberculosis abscess Tularemia
Acne vulgaris Carbuncle Cellulitis Cutaneous blastomycosis Dermoid cyst Erysipelas Folliculitis Furuncle Inflamed epidermoid cysts Lymphadenopathy Perirectal abscess Pilonidal cyst
Actinomycosis Anal fistula Cat scratch disease Crohn disease Granuloma inguinale Ischiorectal abscess Lymphogranuloma venereum Nocardia infection Noduloulcerative syphilis Pilonidal disease Tuberculosis abscess Tularemia
Adapted from Alikhan A, Lynch PJ, Eisen DB. Hidradenitis suppurativa: a comprehensive review. J Am Acad Dermatol. 2009;60(4):539-61.
15
CLINICAL PHENOTYPES
CLINICAL PHENOTYPES
Several clinical phenotypes of HS have been proposed.72,80 Using latent class analysis (a multivariate regression model) without any a priori hypotheses, Canoui-Poitrine and colleagues identified 3 distinct phenotypes from a large, prospective crosssectional study of 618 patients.80 The classic “axillary– mammary” subtype, characterized by breast and axillary involvement with hypertrophic scarring, accounted for 48% of the patients. The “follicular” subtype, characterized by a predilection for follicular lesions (eg, epidermal cysts, pilonidal sinus, comedones, severe acne) and atypical topography involving the ears, chest, back, or legs, comprised 26% of the patients. Compared to those of the classic axillary– mammary subtype, patients of the follicular subtype were also more likely to be male smokers with a family history of HS and greater disease severity.80 The “gluteal” subtype, characterized by follicular papules, folliculitis, and gluteal involvement, comprised 26% of patients. Patients with the gluteal subtype tended to be smokers with lower body mass indexes and more indolent disease compared to the axillary– mammary subtype.80
LABORATORY TESTING
LABORATORY TESTING
Patients with acute lesions may exhibit leukocytosis, elevated erythrocyte sedimentation rate, low serum iron levels, and serum protein abnormalities on serum electrophoresis.81 Chemistries, complete blood counts, and blood cultures should be sent for patients who are febrile or appear toxic.81 Purulent drainage should be sent for bacterial cultures and sensitivities.81 If there is a concern for infection, a deep-tissue culture should be sent for bacterial and fungal organisms.
IMAGING
IMAGING
Ultrasonography and MRI may be used to visualize lesions for staging and surgical planning, although these strategies are rarely used.82 Ultrasonography features may reveal subclinical fluid collections in 76.4% of the patients, fistulous tracts in 29.4%, dermal pseudocysts in 70.6%, and widening of the hair follicles in 100%.83 MRI findings are nonspecific. Skin thickening and induration of subcutaneous tissue that are low signal on T1-weighted images and high-signal on T2-weighted and short tau inversion recovery (STIR) images are typical.84 With IV contrast, abscesses appear as subcutaneous rim-enhancing collections that are low signal on T1-weighted images and high-signal on T2-weighted and STIR images.84
1485
15
Proposed algorithm for evaluating a patient diagnosed with hidradenitis suppurativa
- Is there more than a single inflamed lesion?
- Is the course chronic with new and recurrent lesions?
- Are the lesions bilateral?
- Are the lesions located primarily in the milk line?
If the answer is “no” to 1 or more of these 4 questions
I&D; get culture for bacteria, fungi, and mycobacterial microbes
Culture is sterile or more than a single species is recovered
The answer is “yes” to all 4 questions
Culture is positive for a single species only
Is there a history of GI symptoms and signs?
No
Diagnosis is: INFECTION
Yes
Treat with appropriate antibiotic
Biopsy: get GI evaluation
Biopsy and GI evaluation are compatible with a diagnosis of CROHN DISEASE
A clinical diagnosis of HIDRADENITIS SUPPURATIVA is established
No
Proceed to treatment
Yes
Treat or refer for treatment
HURLEY STAGE CHARACTERISTICS
I Recurrent abscesses without scarring or sinus tract formation
II Recurrent abscesses with scarring and sinus tract formation separated by normal skin
III Recurrent abscesses, diffuse scarring, and inter-
III Recurrent abscesses, diffuse scarring, and interconnecting sinus tracts with minimal to no normal skin between lesions
connecting sinus tracts with minimal to no normal skin between lesions
1486
HISTOPATHOLOGY
HISTOPATHOLOGY
Follicular occlusion is a nonspecific but universal histopathologic finding in HS irrespective of disease duration.85 Early lesions are characterized by follicular hyperkeratosis of the terminal hair follicles, hyperplasia of the follicular infundibulum, and perifolliculitis.24,86 These processes lead to keratinous plugging of the terminal hair follicles, a consistent histologic finding that precedes follicular dilation and rupture.24 Epidermal psoriasiform hyperplasia
(lacking parakeratosis) and subepidermal perifollicular collections of lymphocytes also have been observed in early disease.24 More mature lesions may exhibit noncaseating granulomas, abscesses, epidermal cysts, sinus tracts, granulation tissue, and dermal fibrosis.27,87
Subcutaneous inflammation, fibrosis, and fat necrosis also can be observed. Apocrinitis may occur by extension; however, apocrine gland involvement is seen in 12% to 30% of cases.27,85,87 However, secondary inflammation of the eccrine glands is more often present (19% to 32% of cases).27,85,87 Primary inflammation of the apocrine glands is rare, occurring in 5% of lesions.27,85,87
Acutely, the inflammatory infiltrate is largely comprised of T-lymphocytes and neutrophils at the follicular epithelium with variable extension into the adnexal structures.24 A histopathologic analysis of surgical specimens found a marked CD8+ T-lymphocyte epitheliotropism in the follicular and subepidermal inflammatory infiltrates of early HS lesions.24 The ratio of CD8+ cytotoxic T-lymphocytes to CD4+ helper T-lymphocytes also appears to increase over the lifetime of active lesions.86 In chronic lesions, lymphocytes, histiocytes, and multinucleated giant cells predominate, generating foreign-body granulomas around ruptured hair follicles and skin adnexa.88 Eosinophils and plasma cells are also seen on occasion.87 Notably, recent immunohistochemistry studies report elevated IL-17 and IL-23 expression along with distinct dermal infiltrates of Th17 helper T cells within lesional and perilesional skin.49,52
CLINICAL COURSE AND PROGNOSIS
Disease onset is typically after puberty, with a reported age range from 16 to 81 years.4 Because HS can resemble other pustular dermatoses, delays in diagnosis of 7 to 12 years are not uncommon.89 In one cross-sectional survey, patients reported having 4.6 painful boils per month, with each boil lasting an average of 6.9 days.90
Mean duration of disease was 18.8 years, with the most-severe symptoms occurring early in the disease course (after a mean of 6.4 years from disease onset).90
Disease activity generally declines after 50 years of age.38 Remissions are significantly more likely in nonsmokers, those who have quit smoking, and in nonobese individuals.41
MANAGEMENT
HS is a complex, heterogeneous disease with unpredictable responses to therapy. Therefore, formal treatment guidelines for HS do not exist, and therapeutic decisions are generally guided by disease severity. Hurley stage I disease (mild) is typically amenable to medical therapy alone; Hurley stage II disease (moderate) may require both medical therapy and localized surgical excisions; Hurley stage III disease (severe) often requires extensive, wide excisional surgical procedures with advanced grafting and flap procedures. There is no cure for HS. The overall goals of therapy are to prevent formation
15
of primary lesions and to reduce the impact of disease sequelae (eg, fibrosis, contractures, sinus tracts) on quality of life. Tables 84-4 and 84-5 and Fig. 84-11 offer a proposed management algorithm.
LIFESTYLE MODIFICATIONS AND HOME REMEDIES
LIFESTYLE MODIFICATIONS
AND HOME REMEDIES
Smoking cessation and weight management are important components of symptom mitigation at all stages of disease. Nonsmokers achieved a higher rate of remission (40%) than active smokers (29%) over a mean followup period of 22 years.41 Rates of new lesion formation following excisional surgery were lower among those who ceased smoking versus those who continued smoking.42 Weight loss of 15% or more from baseline after bariatric surgery was also associated with a 20% reduction in number of active, eruptive sites.41
Conservative measures, such as stress reduction, warm baths, warm compresses, and hydrotherapy, may help alleviate symptoms.91 Taking “bleach baths” (ie, one-quarter cup of regular bleach diluted in a full tub or 40 gallons of water) and/or washing the affected areas with topical cleansing agents (eg, chlorhexidine gluconate or benzoyl peroxide solution) 2 to 3 times per week can reduce bacterial load and decrease malodor.9
Resorcinol 10% to 15% cream, a topical peeling agent traditionally used for acne, can improve pain and reduce the duration of painful abscesses.92 Dressings are useful for managing drainage, decreasing malodor, and protecting apparel from stains. Wound dressings are sometimes covered by insurance; abdominal (eg, ABD) gauze pads and sanitary pads can be used as alternatives. Short courses of nonsteroidal antiinflammatory drugs can help alleviate pain and reduce inflammation. Patients should be counseled to avoid tight clothing, prolonged exposure to heat and humidity, and shaving, if these are noted as triggers.90 Consumption of insulinotropic milk and dairy products, as well as hyperglycemic foods, upregulate the PI3K/ Akt-signaling pathway, leading to nuclear deficiency of FoxO1 transcription factor.93,94 Deficiency in FoxO1 is thought to play a role in acne vulgaris and acne-like eruptions.94 Further research is needed in this area, but decreasing exposure to dairy and high-glycemic-index foods may be an adjunct to medical therapy, either directly or indirectly, by promoting weight loss. Applying minced turmeric root as a poultice to active sites or ingesting diluted turmeric (1 teaspoon of turmeric powder diluted in one-quarter cup liquid) 3 times daily has had anecdotal success in ameliorating symptoms. Curcumin, the active ingredient in turmeric, may help reduce inflammation via suppression of TNF-α.95
A 6-month course of high-dose zinc gluconate supplementation (90 mg daily, tapered by 15 mg every 2 months) improved clinical status in a cohort
1487
15
THERAPY CATEGORY OF EVIDENCE STRENGTH OF RECOMMENDATION
First-line
■Clindamycin (topical)a
■Clindamycin/rifampicin (oral)b
■Adalimumab (subcutaneous)c
■Tetracycline (oral)
Second-line
■Zinc gluconate
■Resorcinol (cream)
■Intralesional corticosteroid
■Systemic corticosteroid
■Infliximab
■Acitretin/etretinate
Third-line
■Colchicine
■Botulinum toxin (subcutaneous)
■Isotretinoin
■Dapsone
■Cyclosporine
■Hormones
Surgery
■Excision or curettage of individual lesions
■Total excision of lesions and surrounding hair-bearing skin
■Secondary intension healing
■Primary closure
■Reconstruction with skin grafting and negative pressure wound therapy
■Reconstruction with flap plasty
■Deroofing
■CO2 laser therapy
■Neodymium:yttrium-aluminum-garnet (Nd:YAG) laser
■Intense pulsed light
Pain Control
■Nonsteroidal antiinflammatory drugs
■Opiates
Dressings
Dressings
■No studies have been published as of this writing on the use of specific dressings or wound care methodology in hidradenitis suppurativa; choice of dressing is based on clinical experience
■No studies have been published as of this writing on the use of specific
dressings or wound care methodology in hidradenitis suppurativa; choice of dressing is based on clinical experience
aSingle double-blind, placebo-controlled, randomized trial. Hurley stages I to II.
bEvaluated in case series.
Possible B C A B
IIb III I IIb
C C D D B C
III III IV IV Ib/IIa III
D D D D D D
IV IV IV IV IV IV
C B B C C A/B D A A D
III IIb IIb III III Ia/IIa IV Ib Ib IV
D D
IV IV
IV
D
IV D
cMultiple prospective, randomized, double-blind, placebo-controlled trials (Pioneer 1 and 2). Adapted from Gulliver W, Zouboulis CC, Prens E, et al. Evidence-based approach to the treatment of hidradenitis suppurativa/acne inversa, based on the European guidelines for hidradenitis suppurativa. Rev Endocr Metab Disord. 2016;17(3):343-351, with permission.
CATEGORY OF EVIDENCE STRENGTH OF RECOMMENDATION
Ia: Metaanalysis of randomized controlled trials Ib: Randomized controlled trial A: Category I evidence
IIa: Controlled study without randomization IIb: Quasiexperimental study B: Category II evidence or extrapolated from category I evidence
III: Nonexperimental descriptive studies such as comparative, correlation, and case-control studies C: Category III evidence or extrapolated from category I or II evidence
IV: Expert committee reports or opinion or clinical experience of
D: Category IV evidence or extrapolated from category II or III evidence
IV: Expert committee reports or opinion or clinical experience of respected authorities, or both D: Category IV evidence or extrapolated from category II or III evidence
respected authorities, or both
Data from Guyatt G, Oxman AD, Vist GE, et al. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008; 336:924; and from Gulliver W, Zouboulis CC, Prens E, et al. Evidence-based approach to the treatment of hidradenitis suppurativa/acne inversa, based on the European guidelines for hidradenitis suppurativa. Rev Endocr Metab Disord. 2016;17(3):343-351, with permission.
1488
15
Proposed algorithm for management of hidradenitis suppurativa based on disease severity
Establish Diagnosis of HS made by dermatologists or other health care professional with expert knowledge in HS
Adjuvant therapy (pain management, weight loss, and tobacco abstinence/treatment of super infections/appropriate dressings)
Hurley stage I – III/disease activity HiSCR, PGA, sartorius score/patient-reported outcomes DLQI/pain assessment
Deroofing Laser/ Local Excision Local Excision
Hurley I
PGA Clear (Minimal)
Hurley II Hurley III
Wide Excision
PGA Mild PGA Moderate PGA Severe – Very Severe
Topical Clindamycin 1% lotion BID × 12 weeks Tetracycline 500 mg PO BID × 4 months
Oral Clindamycin 300 mg PO BID Rifampicin 600 mg PO daily × 10 weeks
Improved Failed Improved Failed
Retreat - Flared Retreat - Flared
Adalimumab
Improved Failed
Improved: maintain therapy
Consider second-line therapy
Consider third-line therapy
of 22 patients with therapy-resistant mild-to-moderate HS.96 Eight patients achieved complete remission while 14 patients achieved partial remission.96 Mild side effects (nausea, vomiting, abdominal distension, esophagitis) were reported in 14% of patients.96 Therapeutic benefit is thought to derive from the antioxidant and antiinflammatory properties of zinc gluconate.
MEDICAL THERAPY
MEDICAL THERAPY
ANTIBIOTIC THERAPY
Topical and oral antibiotic therapy are the mainstays of management of mild-to-moderate HS. A randomized,
1489
15
double-blind, placebo-controlled trial demonstrated that clindamycin 1% lotion applied twice daily to affected areas reduced the number of pustules, inflammatory nodules, and abscesses in patients with Hurley stage I and mild stage II disease.97,98 Topical metronidazole 0.75% or erythromycin 2% can be trialed as alternatives to clindamycin. A 4-month trial of oral tetracyclines can be used for their antiinflammatory effect in any disease stage. For more-severe disease (Hurley stage II) that is refractory to topical clindamycin and/or oral tetracyclines, a regimen of 300 mg of clindamycin and 300 mg of rifampin taken 2 to 3 times daily may be effective.99
Triple therapy with rifampin (10 mg/kg/day), moxifloxacin (400 mg/day), and metronidazole (500 mg 3 times daily) can be used as an alternative antibiotic regimen for resistant or severe disease.100 There is weak-to-moderate evidence supporting a course of dapsone (50 to 200 mg daily for 4 to 12 weeks) in refractory HS.101
BIOLOGIC THERAPY
Patients with moderate-to-severe HS who are unresponsive to, or intolerant of, antibiotic therapy may benefit from 40 mg weekly subcutaneous adalimumab, a monoclonal antibody specific to TNF-α.77 Nonresponders to adalimumab therapy may benefit from infliximab, a chimeric monoclonal antibody inhibitor of TNF-α, dosed at 5 mg/kg at weeks 0, 2, and 6, followed by every 8 weeks thereafter.78 Ustekinumab (an IL-12 and IL-23 inhibitor) and anakinra (an IL-1α and IL-1β inhibitor) have been used in small numbers of patients for HS with anecdotal success.102,103
IMMUNOSUPPRESSANT THERAPY
Overall, there is weak evidence supporting use of oral glucocorticoids, colchicine, cyclosporine, azathioprine,104 and methotrexate in HS.105 Intralesional steroid injections of triamcinolone acetonide suspension, 5 to 10 mg/mL, can decrease inflammation in acutely flaring lesions, but is not an effective long-term strategy.105,106
HORMONAL THERAPY
Androgen modulation therapy can be trialed as secondline therapy for patients with mild-to-moderate HS. Small case series have shown improvement with spironolactone 100 to 150 mg daily,107 as well as finasteride 5 mg daily.108
METFORMIN
Metformin, an insulin-sensitizing biguanide agent used in Type 2 diabetes mellitus, is an appealing second-line option for women with HS and comorbid polycystic ovarian syndrome and/or metabolic syndrome. By improving insulin sensitivity, metformin is
1490
thought to counter insulin resistance–induced ovarian androgen production. In a small prospective study of 25 patients with HS who had failed standard-line therapies, metformin dosed at 500 mg to 1500 mg daily reduced clinical severity and improved quality of life in 72% of patients over a course for 24 weeks.109
RETINOIDS
Topical tretinoin and oral isotretinoin are largely ineffective for HS110 but are still commonly prescribed.111 In a retrospective study of 88 patients with HS who had been treated with oral isotretinoin (dosing range 20 to 140 mg/kg/day) over a mean duration of 7.8 months, only 14 (16%) demonstrated clinical response.112 Case reports suggest that acitretin, a second-generation retinoid, may have better efficacy in HS compared to isotretinoin.110 In 1 retrospective study, 12 of 12 patients treated with 0.25 to 0.88 mg/kg acitretin for 9 to 12 months showed clinical improvement.113 More recently, alitretinoin, a first-generation retinoid with similar properties to acitretin, produced 50% reduction in Sartorius score in 6 of 14 patients when dosed at 10 mg daily for 24 weeks.114
SURGICAL THERAPY
SURGICAL THERAPY
EXCISIONAL SURGERY
Excisional surgical interventions are a cornerstone for managing chronic HS. The vast majority of patients (>90%) are satisfied with results after surgery.115 For milder disease, simple incision and drainage procedures, local excisions, and/or deroofing of sinus tracts typically suffice.116 More-severe disease will likely require wide local excisions with primary closure, split-thickness grafting, flap advancements, and/or healing by secondary intention.117 Optimal surgical closure is controversial and depends on characteristics of the surgical site, a topic that has been well reviewed elsewhere.117
Unfortunately, disease recurrence is common after surgery and many patients will require reexcisions throughout the lifetime of the disease.118 A recent systematic review of surgical interventions for HS reported a 13% recurrence rate for wide local excisions; 22% recurrence rate for local incision; and 27% recurrence rate after deroofing.119 Interestingly, the recurrence rate after wide local excision was lower for graft (6%) and flap (8%) closure than for primary closure (15%).119 Some authors maintain, however, that disease recurrence after surgery is likely related to the adequacy of original excision and/or severity of disease rather than type of surgical closure.120
LASER THERAPY
Lasers are growing in use as adjunctive therapies for HS. Laser therapies mitigate flares by debulking tissue
as well as reducing the number of hair follicles, sebaceous glands, and bacteria in affected areas.121 Longpulse 1065-nm neodymium-doped yttrium aluminum garnet (Nd:YAG) laser surgery, and both ablative and fractional CO2 laser surgery have been used successfully in the management of HS122 and are amenable to outpatient settings.
OTHER THERAPY OPTIONS
Cryotherapy improved symptoms in 8 of 10 patients with limited, painful nodules123; however, most patients reported significant pain with the procedure, postprocedure ulceration and/or infection, and long healing times (average of 25 days).123
Radiotherapy for HS was popular in the past but fell out of favor in the 1970s following the advent of cheaper, more easily administered topical and oral therapies.124 Recent case series have reported moderate success among patients with chronic HS who have failed medical and traditional surgical therapies.124,125
Prospective studies are needed to better evaluate its efficacy in chronic HS. Intralesional botulinum toxin A injections may have efficacy for HS.126 Botulinum toxin A is thought to alleviate HS by diminishing or even abolishing eccrine, apocrine, and pilosebaceous gland function,126 which prevents excretions and follicular rupture. Substantive trials are lacking.
PAIN MANAGEMENT
PAIN MANAGEMENT
Current approaches to managing pain in HS derive from expert opinions as well as general pain management guidelines.127 Topical analgesics, oral acetaminophen, and oral nonsteroidal antiinflammatory drugs are considered first-line therapy for pain in HS.127 Persistent and breakthrough pain may require stepup therapy with oral opioid analgesics. Pharmacotherapy targeting neuropathic pain pathways may be beneficial, especially given that they may concomitantly ameliorate comorbid depression and itch.127 More studies are needed to determine optimal pain regimens for patients with HS as well as to educate dermatologists, pain management specialists, and general practitioners about the pain associated with HS.
MENTAL HEALTH
MENTAL HEALTH
Literature concerning the management of mental health morbidity in HS is scant. Qualitative studies indicate that a majority of patients feel symptoms of depression.128 Whether incidence of clinical depression is higher among patients with HS compared to patients without HS is unclear.129 A cross-sectional study in Israel reported that the incidence of depression (5.9% vs 3.5%) and anxiety (3.9% vs 2.4%) were significantly
15
higher among patients with HS when compared to age- and gender-matched controls without HS.130 No formal management guidelines exist for the psychosocial comorbidities of HS. Nevertheless, routine screening and referral of patients with signs of depression to mental health specialists are important. Patient support groups and forums also may be beneficial.
ACKNOWLEDGMENTS
The author would like to acknowledge Powell Perng, BS, for his invaluable contribution to this chapter.

Figure 84-1 Inflammatory subcutaneous nodule of hidradenitis suppurativa with adjacent scars from previous lesions.

Figure 84-2 Multiple inflammatory nodules of hidradenitis suppurativa in the axilla.

Figure 84-3 Inflammatory nodules of hidradenitis suppurativa rupture and drain, leaving behind persistent ulcerations in the axilla. (Copyright © Katherine Püttgen, MD. Used with permission.)

Figure 84-4 Sinus tracts and purulent drainage associated with chronic hidradenitis suppurativa in the axilla.

Figure 84-5 Dense fibrotic plaques and rope-like scars associated with chronic hidradenitis suppurativa in the axilla. (Copyright © Katherine Püttgen, MD. Used with permission.)
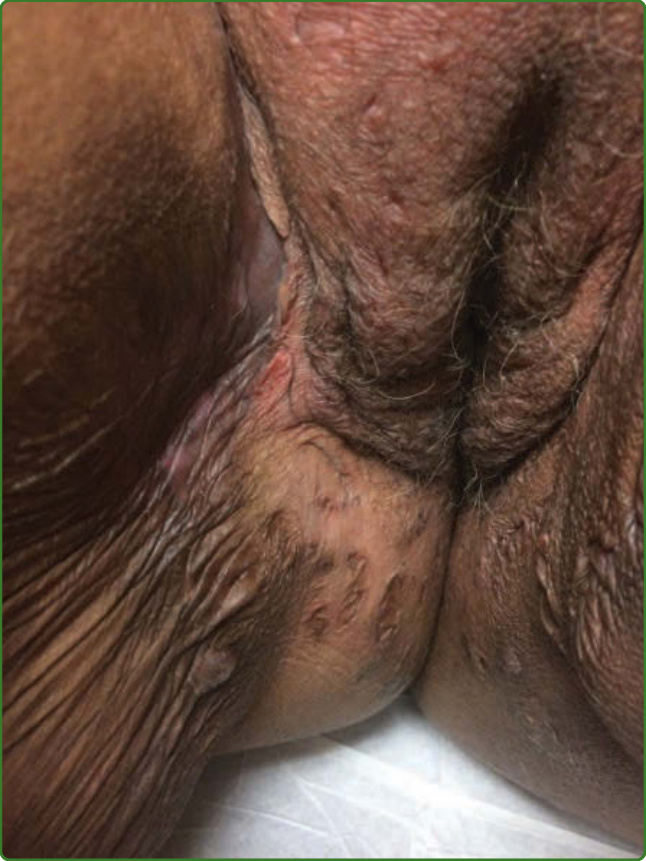
Figure 84-6 Disfiguring atrophic scars in the groin from recurrent lesions of hidradenitis suppurativa.

Figure 84-7 Scrotal lymphedema associated with longterm hidradenitis suppurativa in the inguinal folds.

Figure 84-8 Squamous cell carcinoma arising in longstanding hidradenitis suppurativa on the buttocks.

Figure 84-9 Atrophic scars and double-open comedones associated with hidradenitis suppurativa in the axilla.
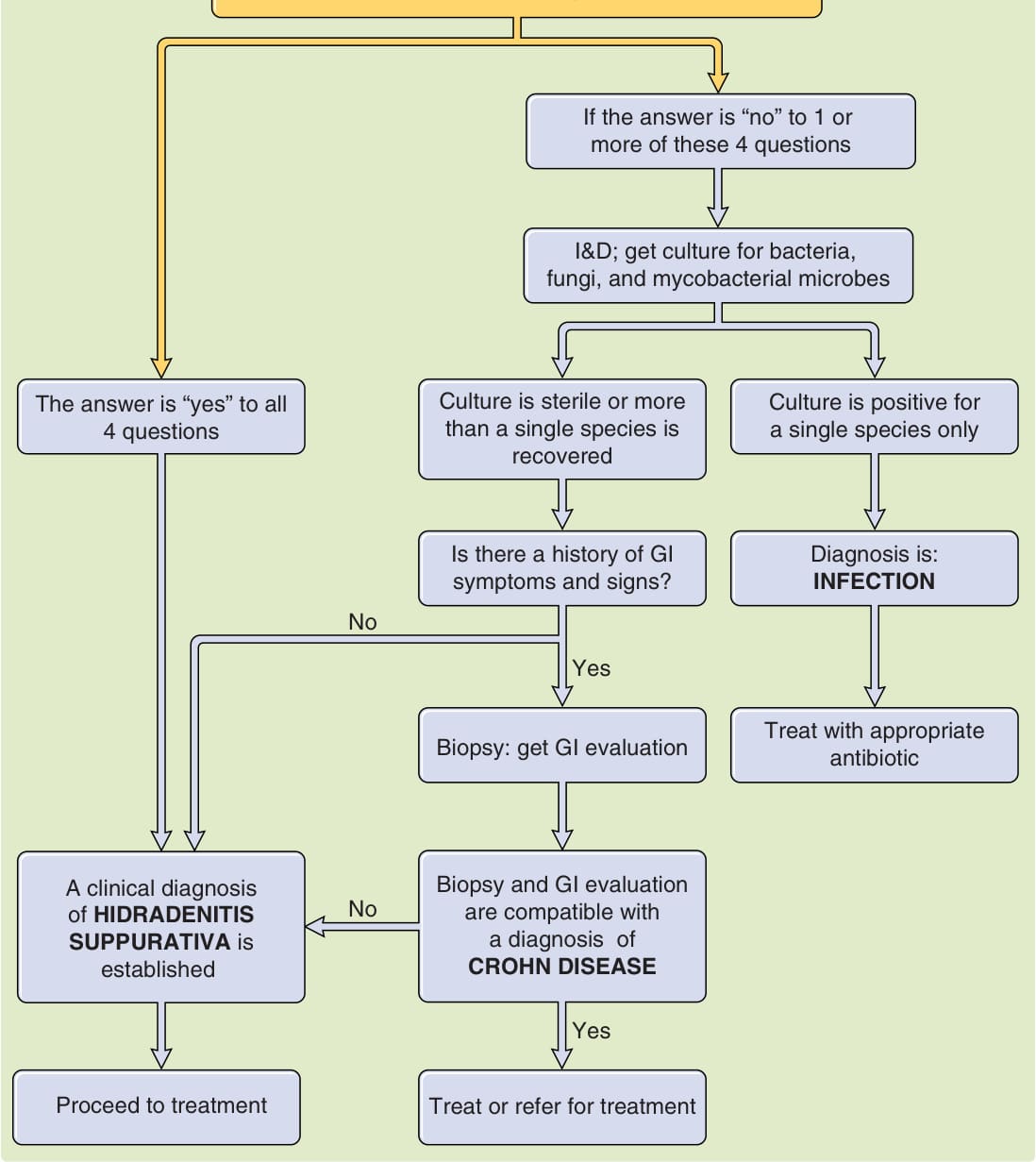
Figure 84-10 Proposed algorithm for evaluating a patient in whom a diagnosis of hidradenitis suppurativa is being considered. I&D, incision and drainage. (From Alikhan A, Lynch PJ, Eisen DB. Hidradenitis suppurativa: a comprehensive review. J Am Acad Dermatol. 2009;60[4]:539-561, with permission. Copyright © American Academy of Dermatology.)
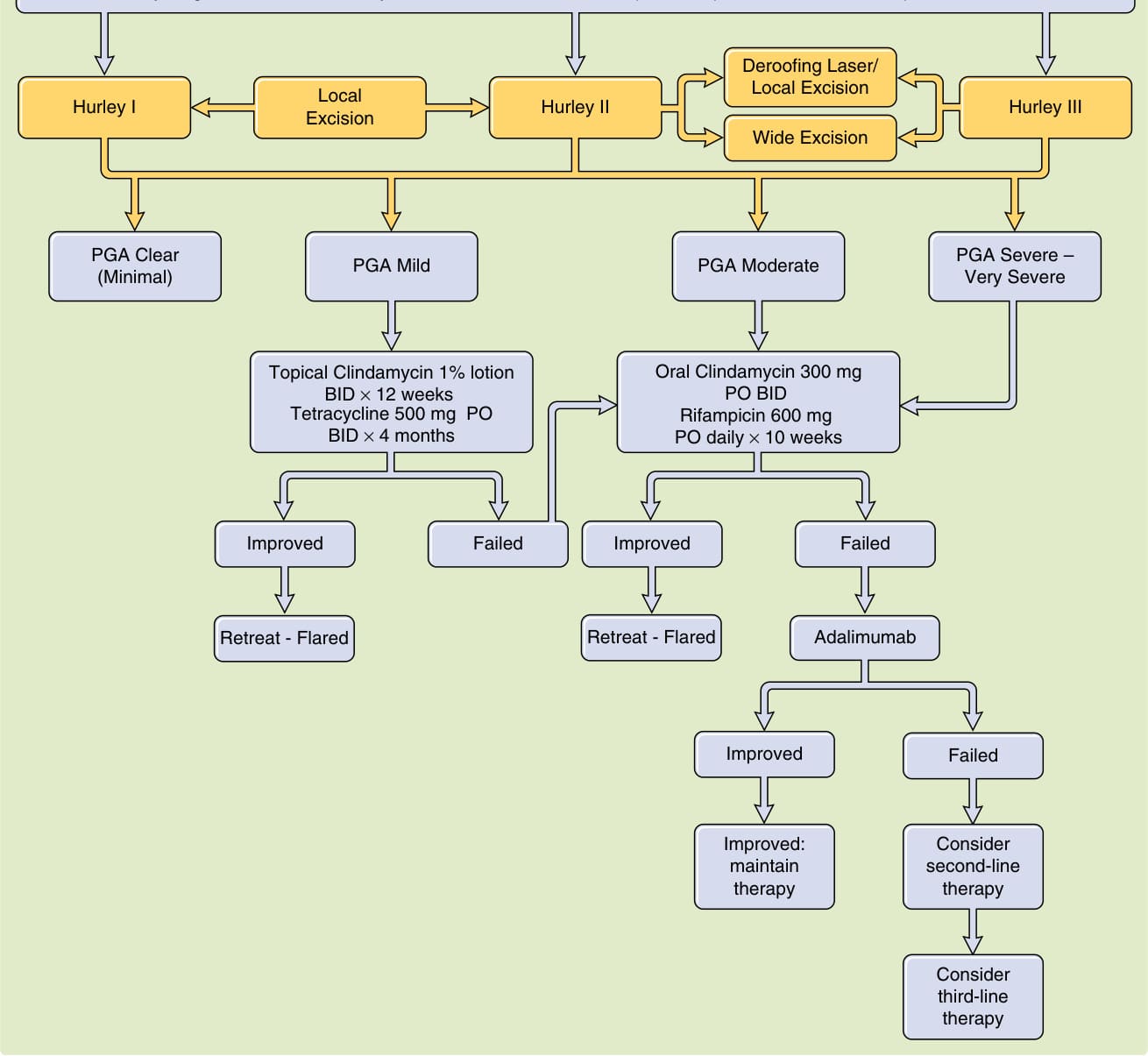
Figure 84-11 Proposed algorithm for management of hidradenitis suppurativa (HS) based on disease severity. BID, twice daily; DLQI, Dermatology Life Quality Index; HiSCR, Hidradenitis Suppurativa Clinical Response; OD, once daily; PGA, Physician Global Assessment; PO, by mouth. (From Gulliver W, Zouboulis CC, Prens E, et al. Evidence-based approach to the treatment of hidradenitis suppurativa/acne inversa, based on the European guidelines for hidradenitis suppurativa. Rev Endocr Metab Disord. 2016;17[3]:343-351, with permission.)
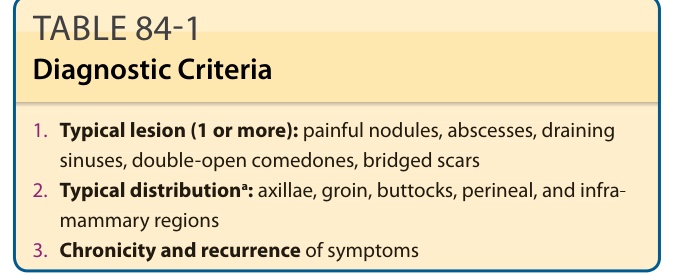
TABLE 84-1 Diagnostic Criteria
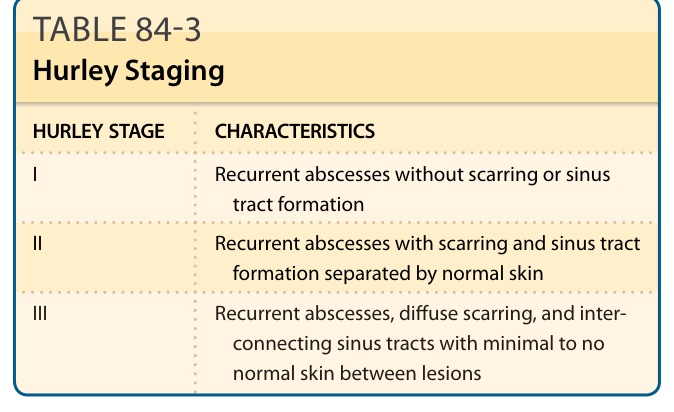
TABLE 84-3 Hurley Staging
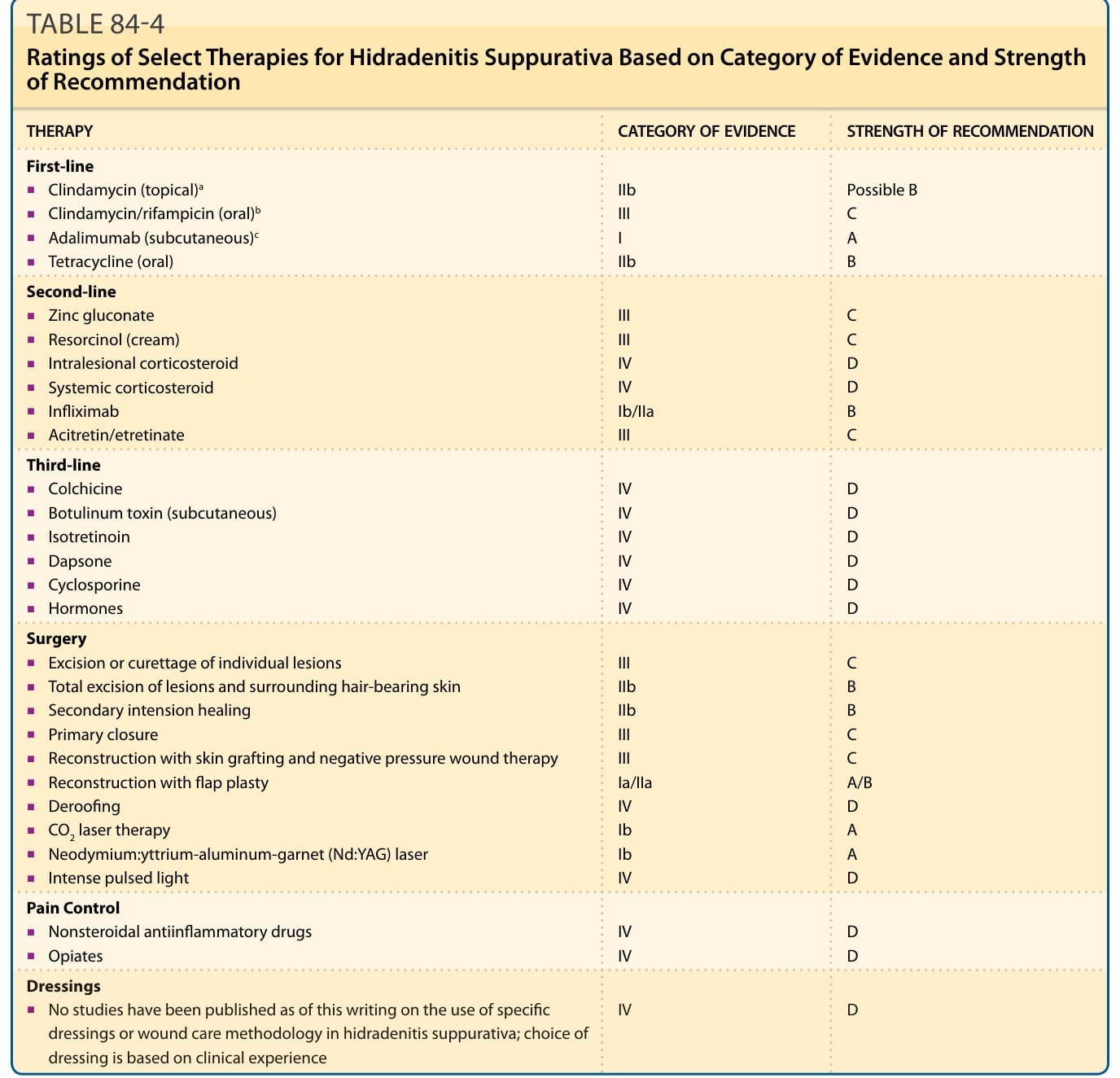
TABLE 84-4 Ratings of Select Therapies for Hidradenitis Suppurativa Based on Category of Evidence and Strength of Recommendation
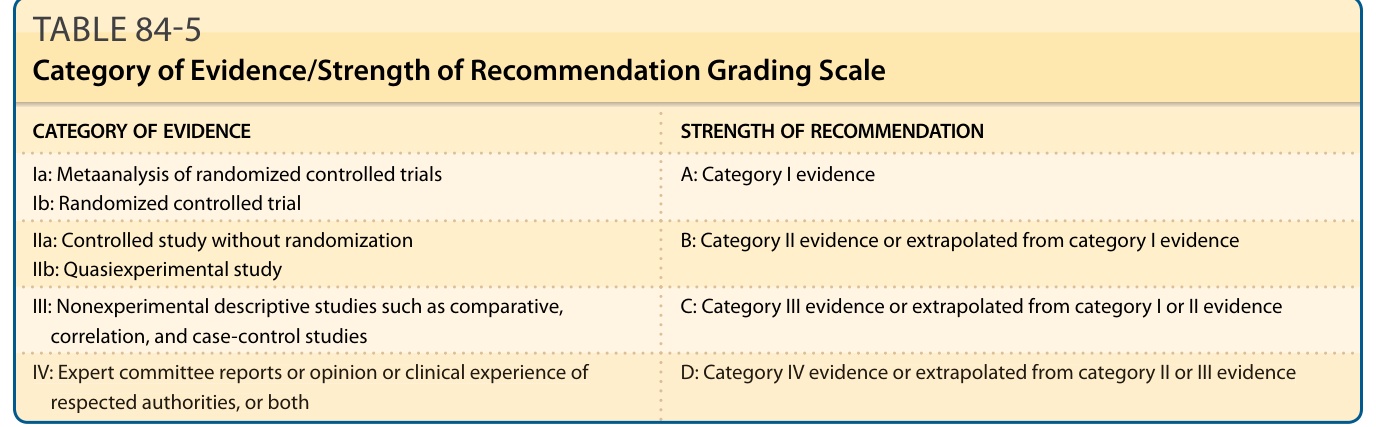
TABLE 84-5 Category of Evidence/Strength of Recommendation Grading Scale