Fox-Fordyce Disease
15
AT-A-GLANCE
■ A rare, itchy, chronic papular eruption localized to apocrine gland–bearing areas of the body with unclear etiology.
■ Females are disproportionately affected compared to males (9:1), with age of onset most commonly between 13-35 years of age.
■ Hyperkeratotic plugging of the follicular infundibulum at the apocrine gland duct insertion site is thought to be the primary pathophysiologic event, leading to duct dilation, rupture, inflammation, and pruritus.
■ No definitive cure; oral antihistamines and topical clindamycin may help alleviate symptoms and induce remission.
Fox-Fordyce disease is a chronic, itchy, papular eruption involving apocrine gland–rich areas of the body. Lesions are characterized by numerous firm, flesh-colored, follicular-based papules arranged in a grouped configuration.1 Fox-Fordyce disease was first described in 1902 by George Henry Fox and John Addison Fordyce in 2 patients with axillary disease.2
The pubic, perineal, areolar, umbilicus, and sternal areas also can be involved.3,4 Fox-Fordyce disease is otherwise known as apocrine miliaria; however, the centrality of apocrine gland dysfunction to the disease pathophysiology remains controversial.1,5
EPIDEMIOLOGY
The incidence of Fox-Fordyce disease is unknown; however, it is considered a rare disease. Epidemiologic studies suggest Fox-Fordyce disease disproportionately affects females.3,6 Females between the ages of 13 and 35 years comprise more than 90% of cases. Fox- Fordyce disease is rarely reported before puberty or after menopause.7 There is no known racial predilection for the disease.
CLINICAL FEATURES
HISTORY
HISTORY
Fox-Fordyce disease typically manifests after the onset of puberty, most commonly in the axillae. Patients may notice lesions for the first time with shaving.8
Diagnosis is often delayed for years,9-11 as the eruptions may only itch initially with onset12 or not at all.11
The number of lesions accumulate slowly over time.13
Pruritus is intermittent and intense. Itchiness is made worse by sympathetic stimulation, including sweating, emotional stress or excitement, and warm weather.13
Family history is usually unremarkable.
CUTANEOUS FINDINGS
CUTANEOUS FINDINGS
Fox-Fordyce lesions manifest as grouped, symmetrically distributed, monomorphic, dome-shaped papules (1 to 3 mm) that are typically follicular based, flesh-colored to mildly erythematous, and intermittently pruritic (Figs. 83-1 and 83-2). Excoriations and lichenification are often present secondary to scratching. The axillae are most commonly affected. The pubic, perineal, areolar, umbilicus, and sternal areas also can be involved. Diminished sweat production is frequently observed in affected areas.11
COMPLICATIONS
COMPLICATIONS
Localized superinfections secondary to repeated scratching can be managed with antihistamines and standard antibiotic therapy. Although hidradenitis suppurativa has been observed in conjunction with Fox- Fordyce disease, there is no evidence that Fox-Fordyce disease progresses to hidradenitis suppurativa.6,14
ETIOLOGY AND PATHOGENESIS
The etiology of Fox-Fordyce disease is unclear. The tendency of Fox-Fordyce disease to present at puberty and remit after menopause suggests a hormonal component to the disease.15,16 Improvements also have been reported during pregnancy16,17 and with use of oral contraceptives.18,19 Alterations in follicle-stimulating hormone,20 estrogen,21 and premenstrual urinary gonadotropins21 have been noted in case reports. Rarely, Fox-Fordyce disease has been observed in men,13,20
preadolescent girls,7,9,22 and postmenopausal women,21
suggesting hormonal factors may not be responsible in all cases. In fact, hormonal analyses in 2 patients with Fox-Fordyce disease found no aberrations.11,23
Genetics likely play a role in Fox-Fordyce disease; however, no clear genetic defect or polymorphism has been reported. The disease has been observed among siblings17 and monozygotic twins,8,24 as well as sisters17
and father and daughter.25 Two patients with Turner syndrome26 and 1 patient with a small deletion on
15
chromosome 21 were also reported to have had Fox- Fordyce disease.20
Several case reports have described Fox-Fordyce– like eruptions developing after laser hair removal.12,27,28
It is thought that laser-induced thermal damage to the follicular infundibulum causes altered keratinocyte maturation and subsequent plugging of the apocrine gland duct insertion site.12 Eruptions tend to occur several months after initiating laser hair removal27 and do not appear to be associated with particular laser wavelengths.27
PATHOPHYSIOLOGY
Hyperkeratotic obstruction of the follicular infundibulum at the apocrine gland duct insertion site is believed to be the primary pathophysiologic event.4 The intraluminal obstruction leads to glandular distension and eventual ductal rupture. The subsequent expulsion of glandular contents into the surrounding dermis then causes an inflammatory response that manifests clinically as the intensely pruritic, dome-shaped, perifollicular papules. However, attempts to recreate the disease process by blocking the apocrine ducts in the experimental setting have failed to elicit the clinical
1476
manifestations.29 Notably, Fox-Fordyce disease has been described in cases with histologic evidence of intraepidermal sweat duct obstruction, suggesting that apocrine and/or eccrine duct obstruction may be another trigger for the disease.4,9
DIAGNOSIS
Fox-Fordyce disease is a clinical diagnosis based on careful history and cutaneous findings. Histopathologic analysis can facilitate with diagnosis, but findings are variable and nonspecific. Imaging and laboratory testing are not useful.
HISTOPATHOLOGY
HISTOPATHOLOGY
Histopathologic features of Fox-Fordyce lesions (Figs. 83-3 and 83-4) are variable and should not be relied upon for making or excluding the diagnosis.1
The most consistent finding is hyperkeratosis of the infundibular epithelium and dilation of the follicular infundibulum (Fig. 83-3).1 Perifollicular and periductal xanthomatosis cells are frequently seen.30
Focal spongiosis of the upper infundibulum along with perifollicular adventitial fibrosis and lymphohistiocytic infiltrate also were consistently observed.3,30
Other findings include vacuolar alterations at the dermato–epithelial junction of the infundibula; smatterings of dyskeratotic cells throughout the infundibula; and tiny columns of cornoid lamella-like parakeratosis in close proximity to the acrosyringium of the apocrine duct, with eosinophilic keratinocytes found underneath.1 The existence of pathognomonic “sweat retention” vesicles described by Shelly and Levy6 is controversial, as these vesicles are rarely demonstrated in histologic specimens. There is evidence that transverse sectioning, rather than conventional vertical sectioning, produces a higher yield of hair follicle units and more readily demonstrates the histopathologic features of Fox-Fordyce disease.31
DIFFERENTIAL DIAGNOSIS
Fox-Fordyce eruptions can be mistaken for irritant contact dermatitis, lichen amyloidosis, granular hyperkeratosis, lichen nitidus, eruptive syringoma, or infectious folliculitis (Table 83-1). Fox-Fordyce disease should also be distinguished from early stages of hidradenitis suppurativa,6,14 a chronic pustular dermatosis that also localizes to apocrine gland–rich regions of the body; however, the purulence, discharge, and sinus tracking of hidradenitis suppurativa are not observed in Fox- Fordyce disease.
CLINICAL COURSE AND PROGNOSIS
Fox-Fordyce disease is chronic, difficult to treat, and has no definitive cure. On occasion, remission has occurred after menopause.15,16
MANAGEMENT
Therapeutic knowledge is derived primarily from case reports. Table 83-2 summarizes select therapeutic strategies for Fox-Fordyce disease.
■Irritant contact dermatitis
■Irritant contact dermatitis
■Chronic dermatitis
■Chronic dermatitis
■Lichen amyloidosis
■Lichen amyloidosis
■Granular hyperkeratosis
■Granular hyperkeratosis
■Lichen nitidus
■Lichen nitidus
■Syringoma
■Syringoma
■Axillary papillary mucinosis
■Axillary papillary mucinosis
■Infectious folliculitis
■Infectious folliculitis
■Early-stage hidradenitis suppurativa
■Early-stage hidradenitis suppurativa
■Scabies
■Scabies
15
Symptomatic therapies
■Oral antihistamines
■Low-dose doxepin
Topical therapies
■Short-term steroids
■Calcineurin inhibitors
■Tretinoin
■Adapalene
■Clindamycin in propylene glycol solution
Oral therapies
■Isotretinoin
■Oral contraceptives
Procedural therapies
Procedural therapies
■Intralesional steroid injection
■Intralesional steroid injection
■Intralesional botulinum toxin injection
■Intralesional botulinum toxin injection
■Surgical excision
■Surgical excision
■Microwave thermal ablation
■Microwave thermal ablation
CONSERVATIVE AND SYMPTOMATIC MEASURES
CONSERVATIVE AND
SYMPTOMATIC MEASURES
Stress reduction and heat avoidance may help minimize pruritus. First-generation oral antihistamines can be useful for alleviating itch, especially during the night. Low doses of doxepin (<10 mg), up to 3 times a day, can be used as an alternative to oral antihistamines.32 There is no evidence to suggest that shaving or deodorant use worsen symptoms; however, thick creams and lotions, which can exacerbate follicular obstruction, should be avoided.
TOPICAL AND MEDICAL THERAPIES
TOPICAL AND MEDICAL
THERAPIES
Topical steroid creams are first-line therapies and can temporarily relieve itching; however, continuous application for more than 10 to 14 days is discouraged because of the risk of skin thinning and formation of striae.33 Intradermal triamcinolone34 may help alleviate itching during acute flares, but can also cause cutaneous atrophy with repeated administrations. Topical calcineurin inhibitors (1% pimecrolimus cream, 0.1% tacrolimus) can be used as alternatives to steroids and will not thin the skin. Pimecrolimus 1% cream applied twice daily over 8 weeks induced complete remission in 1 patient and partial remissions in 2 patients.35 Topical tretinoin can be effective36 but is often abandoned because of excessive irritation of the skin. Topical 0.1% adapalene gel, which is better tolerated than tretinoin, produced mild-to-moderate improvements in itch and number of papules in 1 case when applied every other day for 2 months.37 Side effects of adapalene included erythema and burning sensation.37 In 2 cases, topical
1477
15
clindamycin in propylene glycol solution led to rapid resolution of papules after 1 month of treatment without recurrence at 6 to 9 months.17,38
Other medical therapies include diethylstilbestrol,6
oral contraceptives,19 testosterone,39 corticotropin,6
ultraviolet light therapy,40 and X-ray therapy.23 Oral isotretinoin dosed at 15 to 30 mg daily for 16 weeks induced near-complete remission of lesions and pruritus in 1 case20; however, lesions recurred 3 months after discontinuing therapy, accompanied by a more intense pruritus than before.20 A one-time injection of botulinum toxin type A (2 units diluted into 2.5 mL of 0.9% saline at multiple points 2-cm apart in axillae) produced complete remission 15 days after injections without recurrence at 8 months of followup.41
PROCEDURAL THERAPIES
PROCEDURAL THERAPIES
Case reports suggest different procedural therapies, including electrocautery, excision-liposuction with curettage, microwave thermal ablation,42 and laserbased excisions,43,44 can be curative, but are generally late-line options because of concern about infection, hypertrophic scarring, and/or disfiguration.44

Figure 83-1 Fox-Fordyce disease with skin-colored papules involving the axilla. (Image used with permission from the Graham Library of Wake Forest Department of Dermatology.)
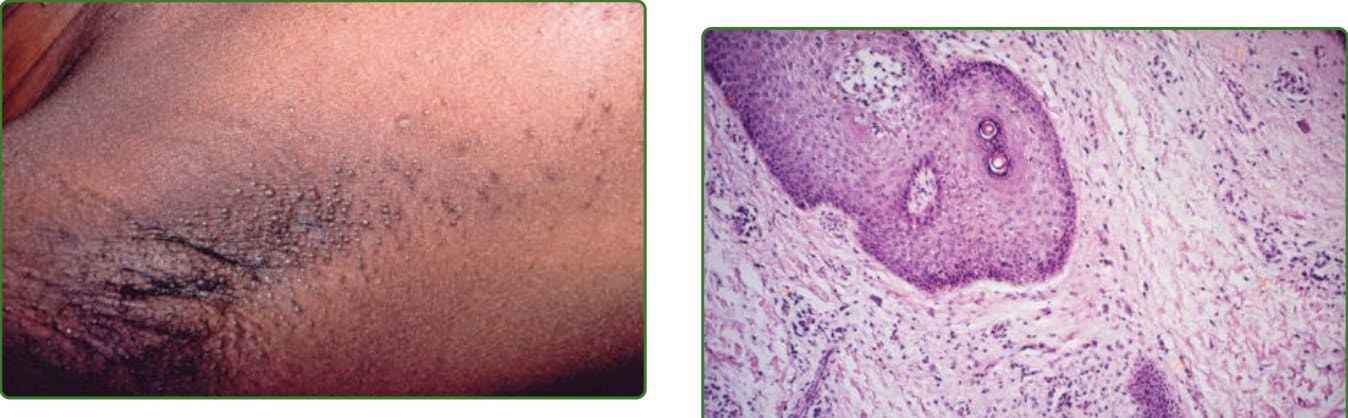
Figure 83-2 Fox-Fordyce in a dark-skin patient with welldemarcated papules on the axilla. (Image used with permission from the Graham Library of Wake Forest Department of Dermatology.)
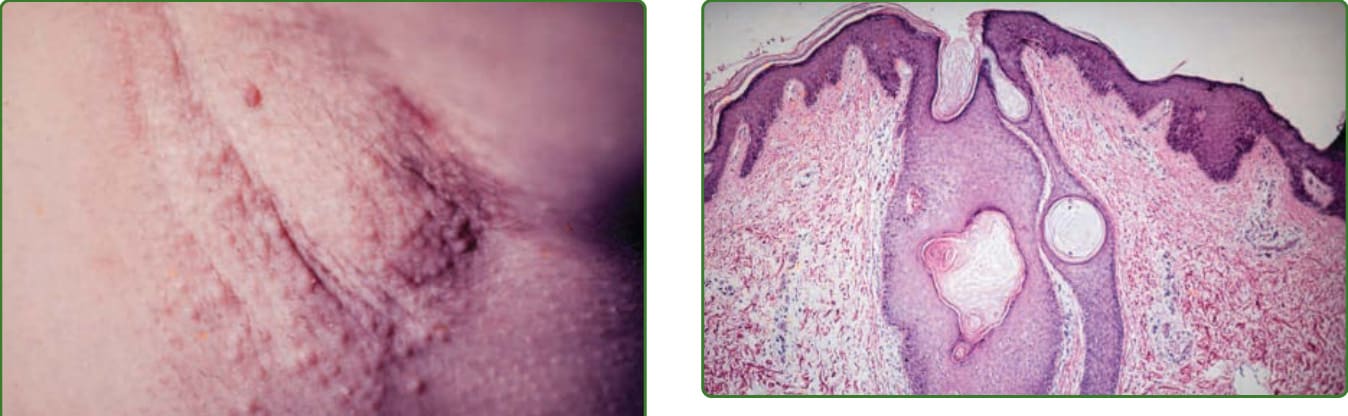
Figure 83-3 Follicular infundibular and excretory duct of apocrine gland with dilation, hyperkeratosis, and plugging. (Image used with permission from the Graham Library of Wake Forest Department of Dermatology.)
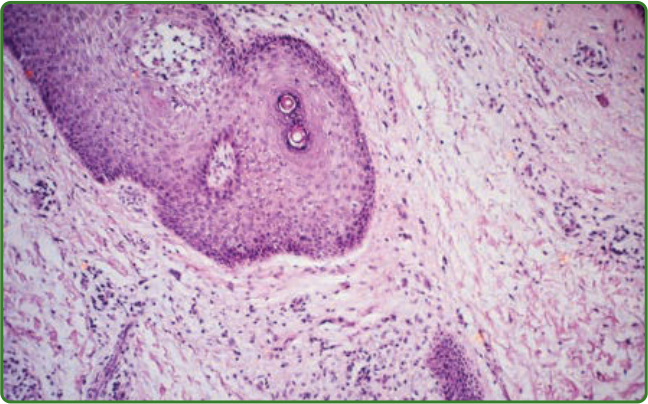
Figure 83-4 Fox-Fordyce disease in the nipple region. (Image used with permission from the Graham Library of Wake Forest Department of Dermatology.)
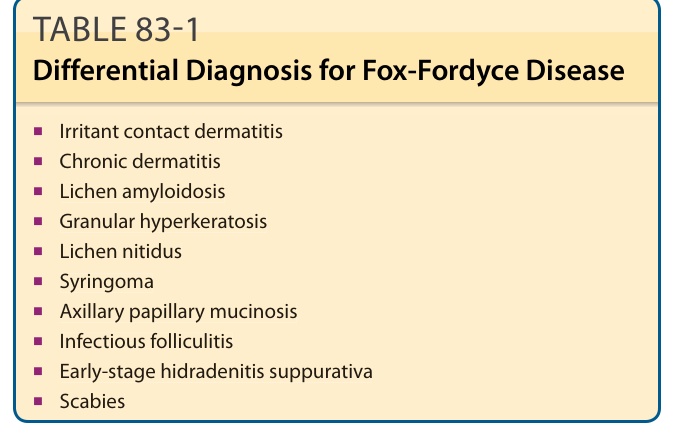
TABLE 83-1 Differential Diagnosis for Fox-Fordyce Disease
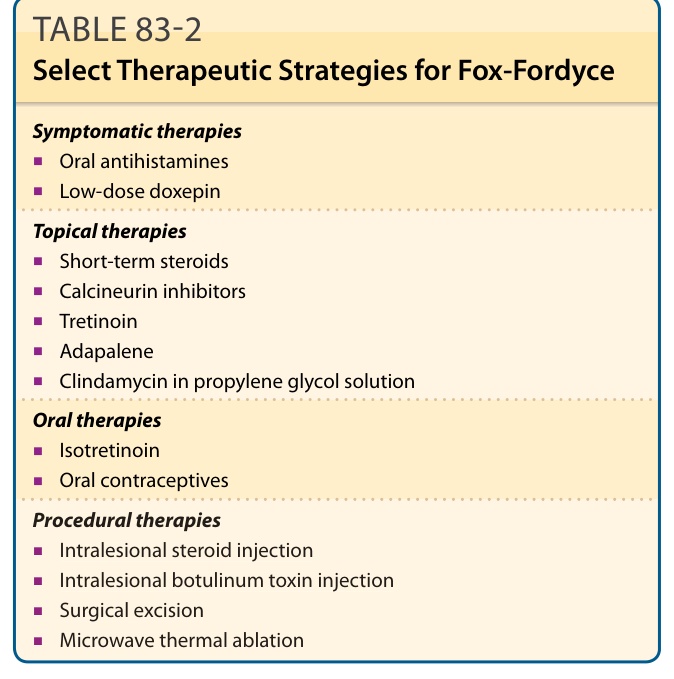
TABLE 83-2 Select Therapeutic Strategies for Fox-Fordyce