Bromhidrosis and Chromhidrosis
15
BROMHIDROSIS
AT-A-GLANCE
■ Bromhidrosis refers to an offensive or unpleasant body odor arising from apocrine or eccrine gland secretions.
■ Chronic disorder that most often develops in the axillae, but may also involve the genitals or plantar aspect of the feet.
■ The best-characterized short-chain fatty acid causing odor is ε-3-methyl-2-hexenoic acid.
■ Surgical removal of affected glands may be effective.
Body odor, osmidrosis, is a common phenomenon in a postpubertal population. Bromhidrosis refers to offensive body odor that is excessive or particularly unpleasant, which prominently arises from apocrine and eccrine glands. Bromhidrosis is most often reported in the axillae (apocrine bromhidrosis). This condition may contribute to impairment of an individual’s psychosocial functioning. The terminology in the literature is sometimes confusing, using osmidrosis to imply offensive odor, and bromhidrosis to imply osmidrosis in the setting of concomitant hyperhidrosis (excessive eccrine sweat gland secretion).1
EPIDEMIOLOGY
EPIDEMIOLOGY
Apocrine bromhidrosis usually occurs after puberty. It exhibits a male predominance, which may be a reflection of greater apocrine gland activity in men than in women. There is no seasonal or geographic predilection, although summer months or warm climates may aggravate the disease. Poor personal hygiene also may be a contributing factor. Bromhidrosis is usually an individual condition, whereas apocrine bromhidrosis has been reported in asian families.2
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
Apocrine secretion is predominantly responsible for odor production, primarily through bacterial action
on its components.3 It is accepted that the odorous steroids, the so-called pheromones, among them 16-androstenes, 5α-androstenol, and 5α-androstenone, contribute to osmidrosis.4,5 5α-Reductase type I is expressed in apocrine glands. Individuals with osmidrosis have increased levels of 5α-reductase in their apocrine glands. Because this enzyme catalyzes the conversion of testosterone to 5α-dihydrotestosterone, levels of 5α-dihydrotestosterone may be greater than testosterone in the skin of affected individuals.6
The biotransformation of these steroids is complex and further research is required to delineate these pathways. Moreover, the axilla hosts many different bacteria, most of which are Gram-positive. Bromhidrosis has been particularly associated with the action of aerobic Corynebacterium species.3 Axillary bacterial florae produce the distinctive axillary odor by transforming nonodoriferous precursors in sweat to ammonia and short-chain, malodorous, volatile fatty acids. The most common of these are ε-3-methyl-2-hexenoic acid and (RS)-3-hydroxy-3-methlyhexanoic acid, which are released through the action of a specific zincdependent N-alpha-acyl-glutamine aminoacylase from Corynebacterium species.6,7 ε-3-Methyl-2-hexenoic acid is delivered to the surface of the skin on 2 binding proteins, apocrine-secretion binding proteins 1 (ASOB1) and 2 (ASOB2). ASOB2 has been identified as apolipoprotein D.8
One study proposed an autosomal dominant inheritance pattern for apocrine bromhidrosis. Newer studies have found a strong relationship between bromhidrosis and wet ear wax associated with the single nucleotide polymorphism rs 17822931 of the ABCC11 gene.9,10
Eccrine secretions are distributed in a generalized fashion, are usually odorless, and serve a thermoregulatory function. The effect of hyperhidrosis on eccrine osmidrosis and bromhidrosis is unclear. Some advocate that excessive eccrine sweat improves apocrine bromhidrosis by flushing away excessive apocrine secretions. Others postulate that eccrine sweat augments apocrine bromhidrosis by encouraging local spread of apocrine sweat components and enhancing the moist environment in which bacteria flourish; that is, eccrine bromhidrosis may develop from the action of bacteria on keratin that has been softened by eccrine secretions. A plantar location is characteristic for eccrine bromhidrosis. Certain foods (garlic, curry, alcohol), drugs (bromides), toxins, or metabolic causes (disorders of amino acid metabolism) may result in eccrine bromhidrosis; the latter being fish odor syndrome (trimethylaminuria), phenylketonuria, cat syndrome, isovaleric acidemia, hypermethioninemia, and food, drug, toxin ingestion.2
15
CLINICAL FINDINGS
CLINICAL FINDINGS
HISTORY
Patients complain of an unpleasant body odor. The axillae are the most commonly affected site, although the genitals or plantar feet also may be affected.3 The diagnosis is usually clinical. What constitutes a “normal” amount of body odor varies considerably among individuals and ethnic groups. In Asian populations, only slight odor is often considered diagnostic.11,12
CUTANEOUS LESIONS
Physical examination of the affected individual is usually unremarkable.
LABORATORY TESTS
There are no associated laboratory abnormalities.
PATHOLOGY
Although some reports do not reveal any abnormalities in the apocrine glands of affected individuals, an increase in the numbers and size of apocrine glands has been reported.11
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
Apocrine bromhidrosis can be distinguished from eccrine bromhidrosis, which is far less common. Moreover, further conditions should be distinguished from bromhidrosis; Table 82-1 outlines the differential diagnosis of bromhidrosis.
TREATMENT
TREATMENT
GENERAL MEASURES
Frequent washing of the axillae, use of a deodorant or antiperspirant (aluminum chloride hexahydrate), perfumes, and changing of soiled clothing can help. Removal of axillary hair may minimize odor by preventing bacteria and sweat accumulation on the hair shafts. Antibacterial soaps or topical antibacterial agents also may be beneficial.
NONSURGICAL THERAPY
The injection of botulinum toxin A has been reported to successfully treat genital13 and axillary bromhidrosis.14 The frequency-doubled, qualityswitched neodymium:yttrium-aluminum-garnet laser
1470
■Apocrine bromhidrosis
■Apocrine bromhidrosis
■Eccrine bromhidrosis
■Eccrine bromhidrosis
■Fish odor syndrome (trimethylaminuria)
■Fish odor syndrome (trimethylaminuria)
■Phenylketonuria
■Phenylketonuria
■Sweaty feet syndrome
■Sweaty feet syndrome
■Odor of cat syndrome
■Odor of cat syndrome
■Isovaleric acidemia
■Isovaleric acidemia
■Hypermethioninemia
■Hypermethioninemia
■Food, drug, toxin ingestion
■Food, drug, toxin ingestion
■Liver failure (fetor hepaticus)
■Liver failure (fetor hepaticus)
■Renal failure
■Renal failure
■Nasal foreign body in children
■Nasal foreign body in children
■Poor hygiene
■Poor hygiene
■Olfactory hallucinations/Schisophenia
■Olfactory hallucinations/Schisophenia
■Body dysmorphic disorder
■Body dysmorphic disorder
■Erythrasma
■Erythrasma
■Trichomycosis axillaris
■Trichomycosis axillaris
also has been reported to be an effective noninvasive therapy for axillary bromhidrosis.15
SURGERY
Several surgical measures have been investigated in the treatment of apocrine bromhidrosis. Patient selection is important because surgery is potentially associated with postoperative scar formation, prolonged healing times, infection, and other complications. Upper thoracic sympathectomy has been successful in treating apocrine bromhidrosis either in isolation or in association with palmar hyperhidrosis.1 Surgical removal of the culprit apocrine glands can be achieved either by the removal of subcutaneous tissue in isolation or in combination with axillary skin.16-20 Surgical subcutaneous tissue removal also has been used in association with CO2 laser ablation.21,22 Although surgical excision may be highly efficacious, depending on the depth of tissue removed and surgical technique used, regeneration and return of apocrine function/osmidrosis and bromhidrosis may develop. Superficial liposuction,21 tumescent superficial liposuction with curettage,23 and ultrasound-assisted liposuction,24 as well as their combinations,25 have efficacy in the management of apocrine bromhidrosis. Liposuction curettage can be considered the primary choice among surgical procedures used to treat patients with bromhidrosis because of its fewer complications.24 In a series of 375 patients, more than 90% reported a satisfactory reduction in odor after ultrasound-assisted liposuction.26 This technique uses ultrasound to liquefy fat and sweat glands. In contrast, laser hair removal may be associated with intensification of bromhidrosis.27 The newly reported treatment using a microwave-based device may be an effective alternative treatment for axillary hyperhidrosis/bromhidrosis.28
PROGNOSIS AND CLINICAL COURSE
PROGNOSIS AND
CLINICAL COURSE
Apocrine bromhidrosis is a chronic and nonremitting condition.29 Patients with apocrine bromhidrosis often feel self-conscious and embarrassed by their condition and may develop a psychosocial functioning impairment. Patients with body dysmorphic disorders may present claiming bromhidrosis.
CHROMHIDROSIS
AT-A-GLANCE
■ Rare, chronic condition characterized by the secretion of colored sweat.
■ Axillary and facial involvement is most common. Areola involvement has been reported.
■ Caused by an increased number of lipofuscin granules in the luminal secretory cells of the apocrine glands.
■ Secretions may be yellow, blue, green, brown, or black.
■ Wood light examination may demonstrate fluorescence of secretions and stained clothes.
■ Adequate therapy is lacking. Reports of treatment efficacy with manual expression, capsaicin, and botulinum toxin.
Chromhidrosis is a rare condition characterized by the secretion of colored apocrine sweat. Two variants of apocrine chromhidrosis are recognized: axillary and facial.29 Involvement of the mammary areola also has been described.30,31 Yonge first recognized facial chromhidrosis in 1709. Shelley and Hurley described this entity in 1954 and associated it with an increased number of lipofuscin granules in apocrine glands.32
EPIDEMIOLOGY
EPIDEMIOLOGY
Chromhidrosis is a rare disease. The worldwide prevalence is unknown. Onset of chromhidrosis is usually at puberty, at the time of increased apocrine gland activity. However, rare cases of onset in infancy have been reported.33 The disease persists throughout life, improving in the aged. It is reported most commonly in African Americans.29 Geographic predilections have never been described. Most of the cases reported in the literature involve women; however, there is a lack of sound scientific evidence supporting a female preponderance.
15
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
The pigment responsible for causing apocrine chromhidrosis is lipofuscins that are produced in the apocrine secretory cells and excreted to the skin surface. Lipofuscin is a golden-colored pigment that is not specific to apocrine glands. In chromhidrosis, the lipofuscin granules are in a higher state of oxidation, thereby imparting various colors of pigment, such as yellow, green, blue, or black. Higher states of oxidation produce darker colors.29,34 It is uncertain why this only develops in some individuals. One case of facial chromhidrosis was successfully treated with capsaicin.35 Nerve endings with receptors for substance P have been found around eccrine sweat glands, suggesting that substance P, a potent vasodilator, may play a role in sweat production and chromhidrosis.29
True eccrine chromhidrosis is very rare and occurs when water-soluble pigments are excreted from eccrine glands after the ingestion of certain dyes or drugs, such as quinine or cranberry juice.34,36 Eccrine chromhidrosis also has been reported in association with alkaptonuria (ochronosis), hyperbilirubinemia37,38
and hematohidrosis (bleeding diathesis).
CLINICAL FINDINGS
CLINICAL FINDINGS
HISTORY
Individuals with chromhidrosis often describe a sensation of warmth, a prickling sensation, or tingling feeling before apocrine gland secretion. Triggers for colored sweating are usually emotional or physical stimuli.29 The morbidity associated with chromhidrosis stems from the emotional distress experienced by affected individuals.39 Staining of undershirts and handkerchiefs are common complaints.
CUTANEOUS LESIONS
Individuals with chromhidrosis develop colored sweat in the axillae, face, or mammary areolae area (Fig. 82-1).29-31 The pigment produced ranges in color from yellow to blue, green, brown, or black. The quantity of pigmented sweat produced is usually quite small (approximately 0.001 mL at each follicular orifice).41 The droplets are odorless and dry quickly. Dried secretions appear as dark flecks within affected areas. Axillary involvement causes staining of shirts and undergarments. Facial chromhidrosis commonly develops close to the lower eyelid, including the malar cheeks, and occasionally the forehead.39,40 Colored sweat also can be manually expressed by squeezing in the affected area. Such a maneuver also may be therapeutic.29
1471
15
A
B
SPECIAL TESTS
An examination of yellow, blue, or green secretions using a Wood light (360 nm) produces a characteristic yellow fluorescence. Black or brown pigment rarely autofluoresces.29 Secretions can be manually expressed if not present at the time of examination. Stained clothing may also fluoresce with Wood lamp examination.41 Apocrine glands can be stimulated to produce colored secretions by the injection of epinephrine or oxytocin.
1472
LABORATORY TESTS
It is reasonable to check a complete blood cell count to exclude a bleeding diathesis, homogentisic levels in urine to exclude alkaptonuria, and bacterial and fungal cultures of affected areas to exclude pseudoeccrine chromhidrosis.34
PATHOLOGY
PATHOLOGY
The luminal cells of the apocrine sweat glands have an eosinophilic cytoplasm, a large nucleus, and may contain lipofuscin, iron, lipid, or periodic acid–Schiff– positive and diastase-resistant granules.42 Under light microscopy using hematoxylin-and-eosin staining, an increased number of (yellow to brown) lipofuscin granules may be present in the apical portion of luminal secretory cells of the apocrine glands. The number of granules varies. Additionally, autofluorescence of paraffin-embedded nonstained sections can be demonstrated using a 360-nm wavelength.41 The granules are positive on periodic acid–Schiff stains. Schmorl stain also may be weakly positive.43
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
Chromhidrosis must be distinguished from pseudochromhidrosis (Table 82-2).34,44 Pseudoeccrine chromhidrosis refers to the development of colored sweat when surface compounds or molecules mix with sweat to produce pigment. A classic example of this type is the formation of blue sweat in copper workers.39 Extrinsic dyes, paints, fungi, and chromogenic bacteria (eg, Corynebacterium species) are other causes of pseudochromhidrosis.29,34
TREATMENT
TREATMENT
Adequate therapy for chromhidrosis is lacking. Manual expression of colored secretions may result in a temporary improvement in symptoms for the following 48 to 72 hours.35 Botulinum toxin type A has been reported as being successful in one patient with facial chromhidrosis. This patient experienced a substantial reduction in pigmented sweat and the results were sustained for 4 months.45 Capsaicin is a topical cream that depletes and prevents reaccumulation of substance P levels in unmyelinated, slow-conducting type C sensory fibers.
■Pseudoeccrine chromhidrosis42
■Pseudoeccrine chromhidrosis42
■Blue sweat with copper exposure
■Blue sweat with copper exposure
■Extrinsic dyes, paints
■Extrinsic dyes, paints
■Chromogenic bacteria (eg, Corynebacterium species), Pseudomonas
■Chromogenic bacteria (eg, Corynebacterium species), Pseudomonas
Case reports demonstrate the efficacy of capsaicin in the treatment of facial chromhidrosis.35 For pseudochromhidrosis, topical and oral erythromycin seems to be the most effective treatment, both in unidentified and identified chromogenic bacteria cases.44
PROGNOSIS AND CLINICAL COURSE
PROGNOSIS AND
CLINICAL COURSE
Apocrine chromhidrosis is a chronic disease that improves in old age as apocrine gland activity diminishes. Disease-associated morbidity is a result of psychosocial dysfunction experienced by affected individuals.

Figure 82-1 A, Blue-black sweat produced in a patient with facial apocrine chromhidrosis after gentle squeezing of the cheeks. (Reproduced with permission from Chang YC, Anderson N, Soeprono F. Bilateral facial pigmentation. Dermatol Online J. 2007;13[3]:16.) B, Blue-black apocrine pigmentation of the axilla and the inflammatory boils of a male patient with hidradenitis suppurativa.
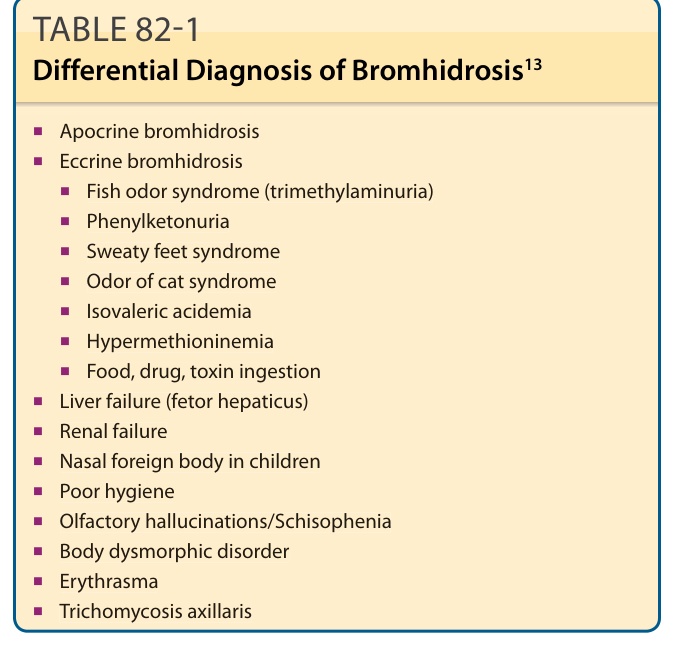
TABLE 82-1 Differential Diagnosis of Bromhidrosis13

TABLE 82-2 Differential Diagnosis of Chromhidrosis34