Hyperhidrosis and Anhidrosis
PART15
Disorders of Eccrine and Apocrine Sweat Glands
AT-A-GLANCE
Primary focal (essential) hyperhidrosis:
■ Idiopathic and symmetric and can affect the palms, soles, axillae, craniofacial region, groin, other areas, or combination of body sites.
■ Treatment is based on severity of symptoms and location and follows a stepwise approach.
Secondary hyperhidrosis:
■ Can occur from underlying systemic illnesses, medications, or both (obtaining a detailed medical history is crucial).
■ The pattern of sweating is classically generalized, but sometimes can be focal or regional if caused by neurologic disease or trauma, or a primary dermatologic cause (eg, eccrine nevus).
■ Treatment should target the underlying disease process or eliminate or change medications that the patient takes, but this is often not feasible.
Anhidrosis:
■ Anhidrosis may occur because of congenital or acquired causes (secondary or idiopathic anhidrosis).
■ Can become a medical emergency leading to hyperthermia, heat stroke, or death.
INTRODUCTION
Eccrine sweating is regulated by neurohormonal mechanisms; a derangement in any part of the regulatory pathways, such as the thermal center, central or peripheral nerve transmission, or eccrine gland sweat secretion can alter sweating. Eccrine sweat glands are innervated by sympathetic nerve fibers; the main neurotransmitter, acetylcholine, binds to the muscarinic
receptors on the eccrine sweat glands to produce sweating. Disorders of eccrine sweating can be subdivided into two main categories: excessive sweating (hyperhidrosis) and reduced sweating (hypohidrosis or anhidrosis). Hyperhidrosis is a condition of excessive sweating beyond what is physiologically necessary to maintain normal body temperature. The prevalence at 4.8%, represents around 15.3 million people in the United States.1 Hyperhidrosis can be further subdivided into primary and secondary hyperhidrosis. Pathogenesis of primary or essential hyperhidrosis is poorly understood. Secondary hyperhidrosis can result from underlying systemic illnesses, including, but not limited to, central and peripheral neurologic dysfunctions, endocrine disorders, psychiatric disorders, hormonal imbalance, infections, malignancy, certain primary dermatologic disorders, and from medications or toxins.2 Hyperhidrosis can adversely impact patients’ daily activities, be occupationally restrictive, and interfere with interpersonal relationships. Anhidrosis is characterized by the inability to normally generate sweat when physiologically necessary to dissipate heat. As a result, this can become a medical emergency, leading to hyperthermia, heat stroke, or death. This chapter focuses on reviewing several disorders that can cause focal, regional, and generalized abnormalities in sweating. Please refer to Table 81-1 for an inclusive list of disorders of the eccrine glands and sweating. A review of the normal anatomy and physiology of eccrine sweat glands and sweating may be found in Chap. 6.
PRIMARY FOCAL (ESSENTIAL) HYPERHIDROSIS
Primary focal hyperhidrosis is a neurologic disorder that manifests as excessive sweating at baseline in various anatomic locations, including, but not limited to,
15
Classification of Disorders of Eccrine Sweating TABLE 81-1
Primary Focal (Essential) Hyperhidrosis Palmoplantar, axillary, craniofacial, generalized hyperhidrosis
Secondary Causes of Focal Hyperhidrosis Caused by cerebral infarction
■Frontal opercular infarct
■Brainstem stroke Associated with spinal cord injury
■Autonomic dysreflexia
■Posttraumatic syringomyelia
■Orthostatic hypotension triggered Associated with other central nervous system disorders
■Chiari type I and II malformation
■Myelopathies caused by infarction, syringomyelia, tumor
■Cold-induced sweating syndrome
■Olfactory hyperhidrosis Associated with peripheral nervous system disorders
■Peripheral motor neuropathy with autonomic dysfunction
■Dermatomal or focal hyperhidrosis caused by nerve trunk irritation
■Compensatory segmental hyperhidrosis (postsympathectomy, Ross syndrome, pure autonomic failure)
■Gustatory sweating
■Physiologic
■Idiopathic
■Postherpetic
■Post nerve injury (postsurgical, diabetic autonomic neuropathy, postinfectious, tumor invasion)
■Lacrimal sweating
■Harlequin syndrome
■Idiopathic, localized hyperhidrosis
■Idiopathic unilateral circumscribed hyperhidrosis
■Postmenopausal localized hyperhidrosis Associated with local skin disorders
■Blue rubber bleb nevi
■Eccrine angiomatous hamartoma
■Tufted angioma
■Glomus tumor
■Burning feet syndrome
■Pachydermoperiostosis
■Granulosis rubra nasi
■Pretibial myxedema
■POEMS (polyneuropathy, organomegaly, endocrinopathy, M protein, and skin changes) syndrome
Secondary Causes of Generalized Hyperhidrosis Associated with central nervous system disorders
Secondary Causes of Generalized Hyperhidrosis Associated with central nervous system disorders
■Episodic hypothermia with hyperhidrosis (Hines-Bannick or Shapiro syndrome)
■Episodic hypothermia with hyperhidrosis (Hines-Bannick or Shapiro
syndrome)
■Posttraumatic or posthemorrhagic “diencephalic epilepsy”
■Posttraumatic or posthemorrhagic “diencephalic epilepsy”
■Fatal familial insomnia and Parkinson disease Associated with fever and chronic infection
■Fatal familial insomnia and Parkinson disease Associated with fever and chronic infection
■Tuberculosis, malaria, brucellosis, endocarditis Associated with metabolic and systemic medical diseases
■Tuberculosis, malaria, brucellosis, endocarditis Associated with metabolic and systemic medical diseases
■Hyperthyroidism, diabetes mellitus, hypoglycemia, hypercortisolism, acromegaly Associated with malignancy
■Hyperthyroidism, diabetes mellitus, hypoglycemia, hypercortisolism,
acromegaly Associated with malignancy
■Leukemia, lymphoma, pheochromocytoma, Castleman disease, carcinoids, renal cell cancer Medication induced
■Leukemia, lymphoma, pheochromocytoma, Castleman disease,
carcinoids, renal cell cancer Medication induced
■See Table 81-4
■See Table 81-4
■Neuroleptic malignant syndrome
■Neuroleptic malignant syndrome
■Serotonin syndrome, other medications Toxic syndromes
■Serotonin syndrome, other medications Toxic syndromes
■Alcohol, opioid withdrawal, delirium tremens Associated with central and peripheral nervous system disorders
■Alcohol, opioid withdrawal, delirium tremens Associated with central and peripheral nervous system disorders
1460
■Familial dysautonomia (Riley-Day), Morvan fibrillary chorea
■Familial dysautonomia (Riley-Day), Morvan fibrillary chorea
Primary Autonomic Disorders with Acquired Anhidrosis Isolated sudomotor disorders
■Progressive isolated segmental anhidrosis
■Idiopathic pure sudomotor failure
■Chronic idiopathic anhidrosis Sudomotor plus other autonomic disorders
■Ross syndrome
■Pure autonomic failure
■Autoimmune autonomic neuropathy
Secondary Autonomic Disorders Associated with Anhidrosis Central nervous system lesions (eg, stroke, tumor, infection, infiltration, trauma)
■Hypothalamic lesions
■Brainstem lesions
■Spinal cord lesions Degenerative disorders
■Multiple system atrophy, dementia with Lewy body disease, Parkinson disease—autonomic failure
Peripheral Nerve Lesions Causing Anhidrosis
■Hereditary sensory and autonomic neuropathy types I, II, IV (congenital insensitivity to pain with anhidrosis)
■Guillain-Barré syndrome (acute inflammatory demyelinating polyneuropathy)
■Diabetic autonomic neuropathy
■Amyloidosis
■Lepromatous neuropathy
■Lambert-Eaton myasthenic syndrome
■Alcoholic neuropathy
■Fabry disease
■Idiopathic small-fiber neuropathy
■Erythromelalgia
■Sympathectomy and other surgical lesions
■Harlequin syndrome Anhidrosis caused by toxins, pharmacologic agents, and heat exposure
■Botulism
■Ganglionic blockers, anticholinergics, carbonic anhydrase inhibitors
■Opioids
■Heat hyperpyrexia and heat stroke
Anhidrosis Associated with Diseases of Skin and Sweat Glands A Anhidrosis caused by physical agents damaging skin A
Anhidrosis Associated with Diseases of Skin and Sweat Glands Anhidrosis caused by physical agents damaging skin
■Trauma, burns, pressure, scar formation, radiation therapy Anhidrosis caused by congenital and acquired skin diseases
■Trauma, burns, pressure, scar formation, radiation therapy Anhidrosis caused by congenital and acquired skin diseases A
■Fabry and other congenital metabolic diseases
■Fabry and other congenital metabolic diseases
■Congenital ectodermal dysplasia
■Congenital ectodermal dysplasia
■Ichthyosis
■Ichthyosis
■Neutrophilic eccrine hidradenitis
■Neutrophilic eccrine hidradenitis
■Sjögren syndrome
■Sjögren syndrome
■Systemic sclerosis (scleroderma)
■Systemic sclerosis (scleroderma)
■Incontinentia pigmenti
■Incontinentia pigmenti
■Segmental vitiligo
■Segmental vitiligo
■Bazex-Dupre-Christol syndrome Disorders affecting the sweat duct
■Bazex-Dupre-Christol syndrome Disorders affecting the sweat duct D
■Miliaria
■Miliaria
■Palmoplantar pustulosis
■Palmoplantar pustulosis
■Psoriasis
■Psoriasis
■Lichen planus
■Lichen planus
■Atopic dermatitis Disorders with abnormal sweat composition
■Atopic dermatitis Disorders with abnormal sweat composition D
■Atopic dermatitis (reduced dermcidin levels)
■Atopic dermatitis (reduced dermcidin levels)
■Cystic fibrosis (increased chloride concentration)
■Cystic fibrosis (increased chloride concentration)
the palms and soles, axillae, craniofacial region, groin, or a combination of body sites. It affects males and females equally, typically begins in childhood (palmarplantar) or during puberty (axillary), and continues to persist into adulthood, with rare reports of spontaneous improvement.
CLINICAL FEATURES
CLINICAL FEATURES
Patients may experience mild (moist or damp skin) to severe (dripping wet) excessive sweating in affected areas. Hyperhidrosis rarely presents with medical complications such as maceration or secondary infections, but it has been reported to predispose the patient to increased risk of cutaneous infection, such as pitted keratolysis, dermatophytosis, and verruca vulgaris or plantaris.3
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
The cause of primary focal hyperhidrosis is poorly understood, but is believed to be a result of sympathetic overactivity without structural defects of the eccrine glands. Evidence also suggests that hyperhidrosis has a familial component, proposing a possible genetic cause for the condition.4-6
DIAGNOSIS
DIAGNOSIS
A thorough clinical history should be obtained from the patient, including age of onset, location and symmetry of sweating, aggravating and alleviating factors, previous treatments, full past medical and surgical history, family history, and current medications that may exacerbate the condition. To establish a diagnosis of primary focal hyperhidrosis, symptoms should be present for at least 6 months without an underlying systemic cause and include at least two of the following characteristics: bilateral and symmetric sweating, impairment of daily activities because of sweating, at least one episode of sweating per week, age of onset younger than 25 years, positive family history, and cessation of sweating during sleep7 (Table 81-2). In the authors’ experience, it is key to understand if the reported sweating is physiologic or not. Sweating can be continuous (mild or severe) or phasic and can be intensified by typical triggers, such as increased temperature, anxiety, stress, and physical activity. A thorough physical examination is necessary and includes inspection for excessive moisture and any other secondary skin conditions, such as bacterial or fungal infections or skin maceration, as well as evidence of systemic findings that might indicate a secondary form of hyperhidrosis. A Minor starch-iodine test is helpful to identify the involved area of hyperhidrosis at baseline, but it does not provide any information on
15
Focal visible excessive sweating ≥6 months’ duration without apparent cause and at least two of the following:
Focal visible excessive sweating ≥6 months’ duration without apparent
cause and at least two of the following:
■Bilateral and relatively symmetric
■Bilateral and relatively symmetric
■Age of onset typically before age of 25 years
■Age of onset typically before age of 25 years
■Cessation of sweating from the focal areas during sleep
■Cessation of sweating from the focal areas during sleep
■Frequency of at least once per week
■Frequency of at least once per week
■Positive family history
■Positive family history
■Sweating impairs daily activities
■Sweating impairs daily activities
severity of the disease (Fig. 81-1). Gravimetric (weightbased) assessment is an objective measurement of the amount of sweat production, commonly performed in clinical research studies, but it is not practical for routine clinical use. The effect of hyperhidrosis on quality of life can be assessed in multiple ways and can help guide response to therapy. Two commonly used tools are the Dermatology Life Quality Index (DLQI) and The Hyperhidrosis Disease Severity Scale (HDSS), a 4-point scale that measures the severity of patients’ hyperhidrosis based on how it affects daily activities8
(Table 81-3). Both of these tools can also be used to follow the response to therapy. The diagnosis of primary focal hyperhidrosis is generally straight forward; however, based on medical history, review of systems, and physical examination, the differential diagnosis could include the possibility of underlying secondary cause(s), which are reviewed later in this chapter.
CLINICAL COURSE, PROGNOSIS, AND MANAGEMENT
CLINICAL COURSE,
PROGNOSIS, AND
MANAGEMENT
Primary focal hyperhidrosis is a chronic disorder, and it does not affect life expectancy. It does, however, have a very negative impact on the quality of life, affecting all domains of social life, sense of well-being, and
1461
15
IMPACT OF SWEATING ON DAILY ACTIVITIES
4 Intolerable; always interferes
3 Barely tolerable; frequently interferes
2 Tolerable; sometimes interferes
1 Never noticeable; never interferes
1 Never noticeable; never interferes
mental health.1 There have been advancements in treatment options. Choosing the right treatment (Table 81-4) involves consideration of body location and severity of the disorder. Properly addressing patients’ expectations is crucial in selecting the appropriate treatment and obtaining treatment compliance. First-line therapy includes over-the-counter (OTC) antiperspirants or aluminum chloride hexahydrate (10% to 35%). Aluminum chloride hexahydrate works best when applied to dry skin at bedtime and washed off after 6 to 8 hours. Patients should be counseled carefully on the proper application to reduce the risk of irritation. If moisture is present on the skin when aluminum chloride hexahydrate is applied, this can result in formation of a weak hydrochloric acid, which can cause symptoms of burning, irritation, or desquamation. If irritation occurs, it can usually be minimized by decreasing application to every other night or few times per week. However, this may also reduce efficacy. Thus, the authors recommend use of OTC clinical-strength antiperspirant on the nights when aluminum chloride hexahydrate is not being applied. There have been several studies showing beneficial results with topical glycopyrrolate ranging in concentrations from 0.5% to 2%, particularly when used for craniofacial hyperhidrosis.9,10 It is not yet commercially available in the United States at the time of writing this chapter, but it can be compounded at specialty pharmacies.
First-Line Topical Options
■Over-the-counter antiperspirants and aluminum chloride hexahydrate (10%–35%)
■Topical glycopyrrolate (0.5%–2%)
Second-Line Agents
■Intradermal botulinum toxin injections
■Electromagnetic energy thermolysis
■Tap water iontophoresis
Severe or Refractory Cases
■Endoscopic thoracic sympathectomy
Systemic Medications
Systemic Medications
■Glycopyrrolate or oxybutynin
■Glycopyrrolate or oxybutynin
■Clonidine
■Clonidine
■Propranolol
■Propranolol
1462
■Benzodiazepines
■Benzodiazepines
If the patient fails to respond to topical therapy, intradermal injection of botulinum toxin may be administered to areas of excessive sweating. Botulinum toxin acts on the cholinergic synapses, inhibiting the release of acetylcholine. Numerous studies have demonstrated the efficacy and safety of several botulinum toxin A drugs as well as botulinum toxin B to treat hyperhidrosis. However, only onabotulinum toxin A (onabotA), (BOTOX; Allergan, Irvine, CA) was approved by the U.S. Food and Drug Administration (FDA) in 2004 for the treatment of severe primary axillary hyperhidrosis in adults 18 years and older. Although its approval is for adults, the efficacy and safety of onabotA can also be extended to adolescents. A large multicenter, nonrandomized, open-label study evaluated the efficacy and safety of onabotA in adolescents ages 12 to 17 years with severe primary axillary hyperhidrosis and demonstrated that 72% of patients experienced at least a two-grade improvement in the HDSS score at 4 and 8 weeks after each of the first two treatments.11 The median duration of effect ranged from 4 to 5 months, and fewer than 6% of patients experienced treatment-related adverse effects.11
Botulinum toxin injections are also used off-label for treatment of other focal areas, such as the face or scalp, palms, soles, and inframammary and inguinal folds, with average efficacy duration of approximately 4 to 12 months.12-14 Injections are placed at the dermal subcutaneous junction where the eccrine glands reside. Electromagnetic energy thermolysis is a non-invasive procedure that can provide long-lasting reduction in axillary sweating; miraDry (Miramar Labs, Sunnyvale, CA) was cleared by the FDA in 2011 for adults with primary axillary hyperhidrosis. Microwave energy is readily absorbed by water molecules and as a result can easily target tissues with high water content, such as the eccrine glands. Eccrine glands do not regenerate, and their destruction theoretically reduces sweating in the treated area permanently. Side effects are generally minor and include edema, erythema, bruising from device vacuum suction, axillary tenderness or pain, paresthesia in the axilla or upper arm, and less commonly, blisters or burns at the treatment site, scar tissue formation, and patchy axillary alopecia (permanent).15
This technology cannot be applied to nonaxillary body sites at the time of writing this chapter. Control of palmar-plantar hyperhidrosis can be obtained via tap water iontophoresis therapy, which uses the passage of a direct electrical current onto the skin. Although the underlying mechanism of iontophoresis remains unclear, a controlled trial of 112 patients with palmar hyperhidrosis showed that after eight treatments, sweating was reduced by 81.2% from baseline with use of iontophoresis therapy.16 Treatments need to be maintained typically once to twice weekly for maximal improvement. An anticholinergic, such as glycopyrrolate, can be crushed and mixed with the water to enhance sweat reduction. Side effects are typically minor (erythema, mild pain or discomfort, and paresthesia in the treatment zone) and related to higher amperage. Severe cases of palmar hyperhidrosis that failed conservative management may be considered
for endoscopic thoracic sympathectomy (ETS). This surgical procedure carries an increased risk of creating minor to severe compensatory sweating in body segments below the treated area, as well as less common complications such as Horner syndrome, bradycardia, pneumothorax requiring chest tube drainage, pleural effusion, acute bleeding or delayed hemothorax, chylothorax, and persistent intercostal neuralgia.17
Systemic medications can be used as monotherapy or to supplement the above therapies, especially when symptoms are multifocal. The oral agents that are commonly used are anticholinergics (glycopyrrolate and oxybutynin) or clonidine, a centrally acting α2-adrenergic agonist.18 Anticholinergic agents are contraindicated in those with myasthenia gravis, paralytic ileus, and pyloric stenosis and should be used with caution in patients with closed-angle glaucoma, bladder outflow obstruction, gastroesophageal reflux disease, and cardiac insufficiency.19 They are also associated with many side effects, such as xerostomia, xerophthalmia, constipation, mydriasis, blurred vision, bradycardia (lower doses), tachycardia (higher doses), mental confusion (usually in children or older adults), and urinary hesitancy or retention. Glycopyrrolate is a quaternary amine and has limited passage across lipid membranes, such as the blood–brain barrier. Anticholinergic agents such as oxybutynin, atropine, and scopolamine are tertiary amines and can easily penetrate lipid barriers. This might explain why glycopyrrolate has fewer central nervous system side effects and may have less effect on the heart rate at lower doses.19 β-Blockers, such as propranolol and benzodiazepines, are oral agents that can be useful in stress-induced hyperhidrosis. However, long-term use of benzodiazepines is not recommended.
SECONDARY HYPERHIDROSIS
Secondary hyperhidrosis can occur because of underlying medical conditions (congenital or acquired) or as a side effect from medications or toxins. Based on a retrospective chart review study conducted over a 13-year period (1993 to 2005) of all patients (children and adults) seen at a university-based outpatient dermatology department with a diagnosis of hyperhidrosis; in patients with secondary hyperhidrosis, endocrine disease accounted for 57% of cases (including diabetes mellitus, hyperthyroidism, and hyperpituitarism); neurologic disease accounted for 32% of cases and more commonly presented as asymmetric hyperhidrosis, and the remaining causes included malignancy (pheochromocytoma), respiratory disease, and psychiatric disease.20 In this study, secondary hyperhidrosis was more often unilateral or asymmetric, generalized, and present nocturnally. Localized secondary hyperhidrosis can occur because of physiologic or pathologic gustatory sweating, central or peripheral neurologic dysfunctions, coldinduced sweating syndrome, paroxysmal localized
15
hyperhidrosis, intrathoracic neoplasms, or compensatory segmental hyperhidrosis (as in cases after ETS or as seen in Ross syndrome, which is a degenerative autonomic nervous system disorder). It can also be seen in association with certain cutaneous disorders. Generalized secondary hyperhidrosis can result from metabolic and other systemic disorders, infections and fever, malignancy (eg, lymphoma or pheochromocytoma), or derangement in the central or peripheral autonomic nervous system (eg, Riley-Day syndrome, or familial dysautonomia) and as a side effect from medications or toxins. Pathogenesis varies depending on the underlying condition. Several entities associated with secondary hyperhidrosis are highlighted below.
CLINICAL FEATURES
CLINICAL FEATURES
Patients with secondary hyperhidrosis can experience focal, regional, or generalized sweating that often persists during sleep. Although the onset of primary hyperhidrosis is often before age 25 years, secondary hyperhidrosis tends to present in adulthood, especially if it is caused by an underlying acquired disease; new symptoms of excessive sweating in adults should be carefully evaluated to ensure an underlying cause is not overlooked.20
ETIOLOGY AND PATHOGENESIS OF LOCALIZED (FOCAL OR REGIONAL) SECONDARY HYPERHIDROSIS
ETIOLOGY AND
PATHOGENESIS OF
LOCALIZED (FOCAL OR
REGIONAL) SECONDARY
HYPERHIDROSIS
GUSTATORY SWEATING
It is common to experience localized sweating on the lips, forehead, scalp, and nose while eating hot and spicy foods as a physiologic response via trigeminovascular reflex. In contrast, pathologic gustatory sweating is usually asymmetric and intense and can occur in the distribution of the auriculotemporal nerve after injury or surgery in the region of the parotid gland; this is known as Frey syndrome (Fig. 81-2). The pathophysiology is not completely understood, but is thought to be caused by aberrant regeneration of autonomic fibers after local trauma to the auriculotemporal nerve.21
Frey syndrome can also be seen in infants and children, often after birth trauma with forceps delivery, but cases of familial, bilateral Frey syndrome without birth trauma have been reported.22
Gustatory sweating may also occur after upper thoracic and cervical sympathectomy,23,24 facial herpes zoster, or chorda tympani injury25 and has been described in association with cluster headache26 and diabetes mellitus.27
1463
15
Treatment with topical glycopyrrolate,10 aluminum chloride, or botulinum toxin injection27 can be effective; rarely, intracranial section of the glossopharyngeal nerve or tympanic neurectomy is needed.
PAROXYSMAL LOCALIZED HYPERHIDROSIS
Daytime paroxysmal hyperhidrosis affecting the head, neck and upper trunk can occasionally affect older postmenopausal women and less commonly, men. Hot flashes are typically not associated with paroxysmal localized hyperhidrosis, and hormonal replacement therapy is usually ineffective. Reported history of sweating before menopause is normal, distinguishing the syndrome from craniofacial essential hyperhidrosis. Alterations in hypothalamic set point temperature range for sweating could be the contributing factor; however, the pathophysiology is not clearly understood. Symptomatic treatment with clonidine or topical or oral glycopyrrolate may be effective.28
LOCALIZED SECONDARY HYPERHIDROSIS ASSOCIATED WITH CUTANEOUS DISORDERS
Excessive sweating has also been reported in association with certain cutaneous disorders such as blue rubber bleb nevus syndrome, perilesional skin of a glomus
1464
tumor, tufted angioma, eccrine angiomatous hamartoma or eccrine nevus, Grierson-Gopalan disease, pachydermoperiostosis, and pretibial myxedema.
ECCRINE NEVUS
Eccrine nevus is a rare skin hamartoma histologically defined as focal hyperplasia or hypertrophy of eccrine glands.29 Clinically, it presents as hyperhidrotic isolated patch of skin with no epidermal changes and is frequently located on the forearm. Treatment decisions depend on the severity of the hyperhidrotic area. Isolated case reports have shown successful response to botulinum toxin injections and topical glycopyrrolate.29,30
ETIOLOGY AND PATHOGENESIS OF GENERALIZED SECONDARY HYPERHIDROSIS
ETIOLOGY AND
PATHOGENESIS OF
GENERALIZED SECONDARY
HYPERHIDROSIS
METABOLIC, INFECTIOUS, AND OTHER SYSTEMIC DISORDERS
Hyperhidrosis has been previously reported in association with diabetes mellitus, hypoglycemia, thyrotoxicosis, carcinoid syndrome, hyperpituitarism (acromegaly), congestive heart failure, dumping syndrome, menopause, malignancy, and drug withdrawal. Exogenous bacterial pyrogens that stimulate production of interleukin (IL)-1, IL-6, tumor necrosis factor, and interferons can cause fever and subsequently hyperhidrosis. These inflammatory cytokines act in the brain to induce and increase the synthesis of prostaglandins, resulting in elevation of the thermal set point.31 The simultaneous activation of antipyretic mechanisms eventually produces excessive sweating. Tuberculosis, malaria, brucellosis, and subacute bacterial endocarditis are some of the infectious etiologies that could present with generalized hyperhidrosis. With regard to malignancy, excessive production of IL-6 by Hodgkin lymphoma cells has been shown to result in fever and subsequent night sweating.32
Riley-Day Syndrome: Familial dysautonomia (FD), also known as Riley-Day syndrome, is the most intensively studied of the hereditary sensoryautonomic neuropathies (designated as hereditary sensory and autonomic neuropathy [HSAN] type III). This is an autosomal recessive disorder that affects 1 in 3600 live births in the Ashkenazi Jewish population and is caused by mutations in the IKAP gene, located on chromosome 9.33 FD is characterized by pronounced autonomic dysregulation with profuse sweating and salivation, diminished production of tears, red blotching of the skin, absence of fungiform papillae of the tongue, episodic orthostatic hypotension, arterial hypertension, reduced deep tendon reflexes, and behavioral abnormalities.33
MEDICATIONS AND TOXINS
Alteration in sweating can occur as a side effect from diverse classes of medications. Hyperhidrosis can be associated with serotonin (5-hydroxytryptamine) reuptake inhibitors, opioids, and prostaglandin inhibitors (naproxen). The mechanisms may relate to 5-hydroxytryptamine (2A) and dopamine receptor antagonism. Hyperhidrosis that commonly occurs during acute and chronic administration of opioids is mainly caused by stimulation of mast cell degranulation, resulting in the release of histamine.34 In contrast, tricyclic antidepressants occasionally cause hyperhidrosis because of their sympathomimetic effect. The presumed mechanism is inhibited reuptake of norepinephrine, leading to stimulation of peripheral adrenergic receptors and a generalized diaphoretic response. Cholinergic agonists such as pilocarpine and bethanechol and reversible cholinesterase inhibitors such as pyridostigmine can increase sweating directly or indirectly via activation of M3 cholinergic receptors on sweat glands.
DIAGNOSIS
DIAGNOSIS
Just as with primary hyperhidrosis, a thorough clinical history and physical examination are crucial, particularly focusing on constitutional symptoms (fever, unexplained weight loss, chills, night sweats, fatigue) and endocrine and neurologic systems. Inquiring about prescription and OTC medications and supplements taken daily or as needed will also aid in recognizing secondary causes. Primary hyperhidrosis may be present in patients with underlying medical conditions, but generally with an onset of symptoms at a younger age and occurs in more classic focal locations as discussed previously. A Minor starch-iodine test may be used to assess the distribution of excessive sweating. If secondary hyperhidrosis is suspected, baseline vital signs and laboratory studies are warranted, and the patient should be referred to his primary care physician for an evaluation. Neurologic consultation may also be considered if suggested by the medical history or physical exam.
CLINICAL COURSE, PROGNOSIS, AND MANAGEMENT
CLINICAL COURSE,
PROGNOSIS, AND
MANAGEMENT
Clinical course and prognosis will depend on the underlying disease that is manifesting symptoms of hyperhidrosis or discontinuing a culprit medication. Treatment should be focused on correcting or controlling the underlying disease, but symptoms may be reduced with any of the mentioned modalities listed previously.
15
ANHIDROSIS
Anhidrosis may occur because of congenital absence of sweat glands as in cases of hypohidrotic ectodermal dysplasia, hereditary metabolic disorders (Fabry disease), or acquired causes (secondary or idiopathic anhidrosis). Secondary anhidrosis or hypohidrosis can result from connective tissue diseases (Sjögren syndrome), eccrine duct obstruction (from chronic dermatoses such as psoriasis or atopic dermatitis, or acute causes such as miliaria), underlying neurologic disorders with autonomic dysfunction (congenital insensitivity to pain with anhidrosis, multiple sclerosis, Shy-Drager syndrome), peripheral neuropathies, and medications or toxins.
CLINICAL FEATURES
CLINICAL FEATURES
Patients with focal or segmental anhidrosis may become aware of their disease because of compensatory hyperhidrosis in other regions (Fig. 81-3). Generalized anhidrosis or anhidrosis with large areas of involvement usually manifests as heat exhaustion, inability to tolerate increased physical activity in a hot environment, or dizziness upon exposure to heat.
HYPOHIDROTIC ECTODERMAL DYSPLASIA
HYPOHIDROTIC
ECTODERMAL DYSPLASIA
Mutations in the ED-1 gene encoding for ectodysplasin result in X-linked hypohidrotic ectodermal dysplasia, which is the most common form of the ectodermal dysplasias. These disorders are characterized by an
1465
15
abnormal development of eccrine sweat glands, hair, and teeth.35 Autosomal-recessive and autosomal-dominant modes of inheritance have also been described.36
Affected children are at risk of experiencing life-threatening hyperpyrexia because of their inability to sweat.
CONGENITAL INSENSITIVITY TO PAIN WITH ANHIDROSIS
CONGENITAL
INSENSITIVITY TO PAIN
WITH ANHIDROSIS
Congenital insensitivity to pain with anhidrosis (CIPA), also known as HSAN type IV, is a rare autosomal recessive disorder characterized by the congenital insensitivity to noxious stimuli, anhidrosis, recurrent hyperpyrexia, mental retardation, and self-mutilating behavior.37 CIPA is reported to occur because of lossof-function variants in neurotrophic tyrosine receptor kinase 1 (NTRK1) gene. Nearly all of the associated symptoms can be attributed to the inability of NTRK1 signaling pathways to regulate the development of nociceptive, sympathetic, and central cholinergic neurons.37
FABRY DISEASE
FABRY DISEASE
Fabry disease is an inherited X-linked lysosomal storage disorder caused by deficient activity of α-galactosidase A. It presents during childhood in both male and female patients. Early manifestations include hypohidrosis, telangiectasia, angiokeratoma, acroparesthesia, and gastrointestinal symptoms.38
Later in adolescence or adulthood, manifestations can include renal, cardiac, and central nervous system dysfunction. Hypohidrosis is the second most common symptom of Fabry disease; the pathogenesis is unclear but could be the result of accumulation of glycosphingolipids in eccrine sweat glands and secondary to autonomic peripheral neuropathy.39
ACQUIRED IDIOPATHIC GENERALIZED ANHIDROSIS
ACQUIRED IDIOPATHIC
GENERALIZED ANHIDROSIS
Acquired idiopathic generalized anhidrosis (AIGA) is a rare cause of anhidrosis that can result from idiopathic pure sudomotor failure, sudomotor neuropathy, or eccrine sweat gland failure.40 The majority of AIGA cases, however, lack these pathologic abnormalities. Cases reported in literature affect primarily patients of Asian ethnicity, but it is not entirely clear if this is because of a genetic component or if AIGA is underreported in other populations. AIGA has a heterogenous clinical presentation and can include the following clinical features: acute onset, cholinergic urticaria, elevated serum immunoglobulin E levels, absence of
1466
other autonomic dysfunction, and marked response to glucocorticoids.41 Spontaneous remission has been reported in some cases of AIGA, but anhidrosis tends to persist if it has been present for a long time. Patients with generalized or partial anhidrosis involving at least 30% to 40% of their body surface area should be advised against participation in activities requiring increased endurance or working in high ambient temperatures.40
MILIARIA
MILIARIA
Miliaria results from obstruction of eccrine sweat ducts and occurs in conditions of increased heat and humidity. There are three types of clinically distinctive miliaria classified based on the level of the obstruction: miliaria crystallina, miliaria rubra, and miliaria profunda. In miliaria crystallina, ductal obstruction occurs at the stratum corneum. It presents as small, 1-mm, clear, fragile, vesicles that rupture easily (Fig. 81-4). They are commonly seen on the face and upper trunk in infants and on the trunk in adults. In miliaria rubra, obstruction occurs deeper within the epidermis and results in pruritic, 1- to 3-mm, nonfollicular, erythematous macules and papules on the upper trunk and neck. Sterile pustules may also develop and are termed miliaria pustulosa. When miliaria rubra becomes chronic or recurrent, occlusion of eccrine sweat ducts extends to a deeper level. In miliaria profunda, ductal obstruction occurs at the dermal–epidermal junction and produces asymptomatic, 1- to 3-mm white papules.
DIAGNOSIS
DIAGNOSIS
As with hyperhidrosis, a careful medical history is necessary, with special attention to medications, underlying medical conditions, and family history. Examination of the skin may not reveal the presence of anhidrosis, but could indicate compensatory hyperhidrosis. To
A B
identify possible sweat gland abnormalities, a biopsy specimen from the affected area should be obtained in patients with anhidrosis (Fig. 81-5).
CLINICAL COURSE, PROGNOSIS, AND MANAGEMENT
CLINICAL COURSE,
PROGNOSIS, AND
MANAGEMENT
Unlike treatment of hyperhidrosis, options for anhidrosis are limited. The primary cause should be identified first, and any possible contributing medications should be discontinued. Keeping the patient in cool temperatures is crucial to avoid life-threatening overheating. It can also be helpful to wear wet clothing during physical activity; however, the effectiveness of external cooling may be compromised in patients with ectodermal dysplasia, presumably because of poor capillary dilation.41,42 In cases of miliaria, treatment is usually not indicated for miliaria crystallina because of its self-limited nature. The topical application of anhydrous lanolin has resulted in dramatic improvement in patients with miliaria profunda.43
Prevention and treatment of miliaria consists of controlling exposure to heat and humidity, treating any underlying febrile illnesses, and removing occlusive clothing.
ACKNOWLEDGMENTS
The authors acknowledge the contribution of Robert D. Fealey and Adelaide A. Hebert, the former authors of this chapter.
15

Figure 81-1 Positive starch iodine test result in a patient with primary axillary hyperhidrosis.

Figure 81-2 A patient with pathologic gustatory sweating and a positive starch iodine test result.

Figure 81-3 A patient with segmental anhidrosis (yellow) with compensatory left-sided hemihyperhidrosis (purple) caused by a right greater than left-sided upper thoracic spinal cord injury (sodium alizarin sulfate indicator powder).

Figure 81-4 Miliaria crystallina with delicate, droplike vesicles and no underlying erythema.
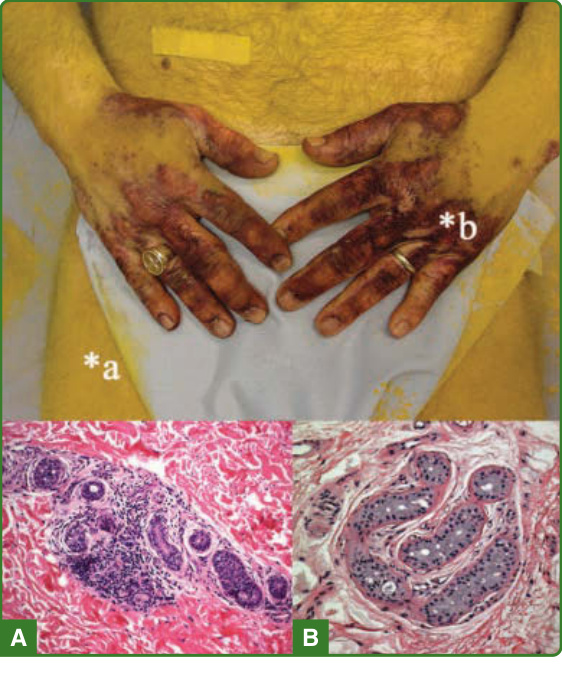
Figure 81-5 Punch skin biopsy from an anhidrotic skin site (A) shows marked perieccrine lymphocytic infiltration of sweat gland secretory coils, and sweating skin (B) shows normal sweat gland morphology.
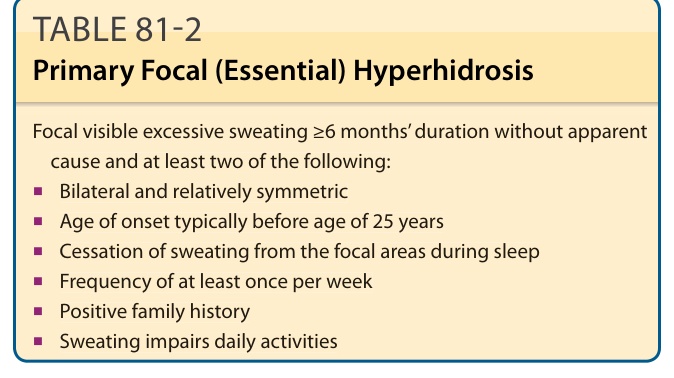
TABLE 81-2 Primary Focal (Essential) Hyperhidrosis
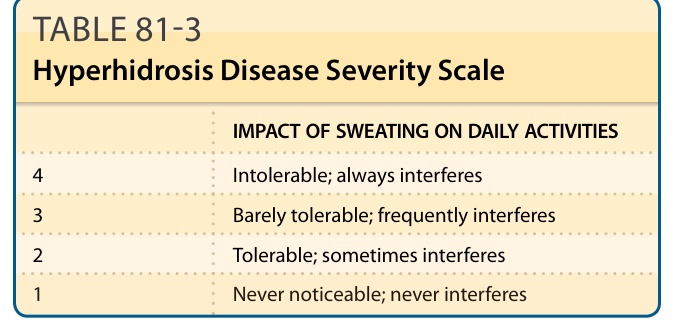
TABLE 81-3 Hyperhidrosis Disease Severity Scale
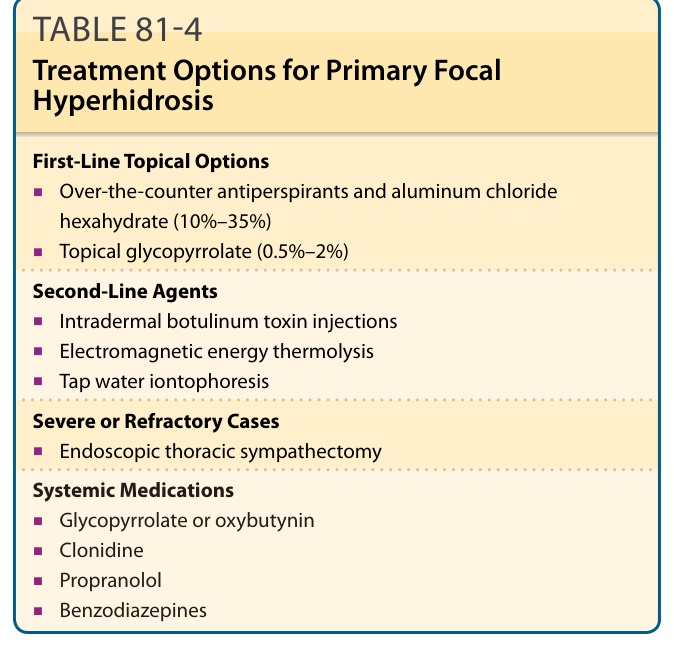
TABLE 81-4 Treatment Options for Primary Focal Hyperhidrosis