Rosacea
14
AT-A-GLANCE
■ Rosacea is a common facial skin disease in many countries.
■ Signs and symptoms for rosacea include flushing, transient erythema, persistent erythema, telangiectasia, papules, pustules, phymata, edema, pain, stinging or burning, and (very rarely) pruritus.
■ The pathophysiology of rosacea is poorly understood; however, a genetic predisposition along with trigger factors activate a dysregulated neurovascular, innate immune, and adaptive immune system.
■ Taking a thorough family and patient history and performing a clinical examination are crucial to diagnose rosacea.
■ All clinical features have to be considered with severity scores for a proper treatment, combined with assessing patient’s quality of life.
■ Approved topical or systemic drugs exist for various, but not all, features of rosacea and should be used on the basis of pathophysiology and while considering efficacy and side effect profiles.
■ Knowledge about the beneficial use of physical therapies and their limitations is important for best medical practice in patients with rosacea.
■ Education about disease progress, general skin care, cosmetic usage and medication effects and potential adverse events is mandatory; teaching of proper topical use guarantees better treatment results.
■ Education to prevent exacerbating “trigger factors” is critical for successful management of patients with rosacea.
INTRODUCTION
Rosacea is a common chronic inflammatory skin disease that almost exclusively affects the central facial skin and rarely affects the extrafacial (neck, forehead) skin. Rosacea derives from the Greek word meaning “rose-like,” which describes the main symptomatology of repeated flushing alone or in combination with transient or persistent erythema. Clinically, the condition is characterized by prolonged flushing (transient erythema), persistent erythema, telangiectasia, papules, pustules, and phymatous changes, often accompanied by burning, stinging, or even migraine-like pain (cutaneous rosacea). Eyes can be also involved (ocular rosacea). Because of their different pathophysiologies,
the terms acne rosacea and adult acne are no longer used to describe this disorder.1,2
Worldwide, more than 20 million patients are estimated to have rosacea, although reliable statistics are lacking.3 Because of its obvious facial location, rosacea is associated with a significant disease burden and impaired quality of life.4 The etiology and pathophysiology of rosacea are poorly understood, so the therapy of rosacea is still unsatisfactory; currently used treatment modalities mainly aim to control the clinical signs and symptoms rather than target causes or prevent disease.5-9
EPIDEMIOLOGY AND DISEASE BURDEN
In many countries, rosacea is more prevalent than asthma or diabetes. Depending on the country, rosacea affects at least 2% to 18% of individuals, with the highest level reported in Celtic populations. A Swedish study described a prevalence of 10% for rosacea,10 and a German study found 12.3% of the population to be affected.11 In 2010, an epidemiologic study from Ireland reported a prevalence of 13.9% for rosacea.12 The prevalence of rosacea probably depends on the genetic make-up of the population being studied. The condition affects women more often than men (3:1) and typically starts a decade earlier in women than in men; the normal age of onset is generally considered to be 35 to 45 years in women and 45 to 55 years in men, although recent studies suggest an earlier clinical onset with flushing, which is often not recognized as an early sign of rosacea.1,13,14 Research indicates that the first, often unrecognized, signs can occur in the second decade of a patient’s life, more often in women than in men. Rosacea is often misinterpreted as a disease of alcohol overconsumption or “lying,” which can stigmatize patients. The facial distribution of the disease is generally recognized to have a significant negative psychological impact on patients, although the statistical evidence for this effect is poor. Patients report significantly impaired self-esteem and may become unemployed, stop socializing, get divorced, or develop depression.15 However, not all of the disease burden is psychological because patients may also have potentially severe stinging or burning associated with the flushing or erythema.3,16
CLINICAL FINDINGS
Rosacea is, in most cases, a symmetric skin disease affecting the central face, nose, chin, central cheeks, and glabella; the forehead (more common in bald
4
14
men), neck, and chest are only rarely affected. The perioral or periorbital regions, or areas behind the ears, are rarely affected. The clinical findings can vary substantially among rosacea-affected patients. In general, all possible signs or symptoms are flushing, transient erythema, persistent erythema, telangiectasia, papules, pustules, phymata, edema, pain, stinging or burning, and (very rarely) pruritus.16-18 Although flushing is the hallmark of rosacea, some patients develop rosacea without much flushing. Classically, most patients describe the disease development as a “crescendo” manifestation with increased numbers of “flushes” after exposure to trigger factors. Sooner or later, most patients develop persistent erythema with or without telangiectasia. Notably, comedones are absent, which differentiates papulopustular rosacea from acne or Favre-Racouchot disease. The clinical findings are gender and age dependent: in younger female and male patients, flushing and erythema are often the first symptoms; in older adult patients, telangiectasia can be a first sign. Rhinophyma is a characteristic of male patients. The clinical picture is also dependent on the special susceptibility of the patient toward trigger factors; for example, a patient who has high susceptibility to ultraviolet (UV) radiation as a trigger factor may have an asymmetric facial erythema caused by window exposure (eg, driver vs. co-driver). The progression of rosacea is relatively slow, evident only after thorough history taking.
PERSISTENT ERYTHEMA
PERSISTENT ERYTHEMA
Persistent erythema (from Greek erythros, red) is defined as erythema that lasts for at least 3 months. It constitutes an abnormal redness of the skin or mucous membranes caused by vasodilation of arterioles or capillaries, resulting in increased perfusion and thus redness. Persistent (perilesional) erythema can be found around papules and pustules. Clinically, patients with persistent erythema present with a striking clinical appearance: there is profound central facial erythema predominant on the projecting facial anatomical features (Fig. 79-1). The erythema depth ranges from pink-red to deep burgundy red.
PHYMATA
PHYMATA
Phymata (phyma, Greek meaning swelling, mass) represents a macroscopic lesion that is uniquely associated with rosacea. Phymatous rosacea is a persistent, firm, nonpainful, nonpitting swelling of the tissue of the nose (rhinophyma), chin (gnathophyma), forehead (metophyma), or eyelids (blepharophyma) that seldom begins before the age of 40 years. Phymatous changes, fortunately, are a rare malady in patients with rosacea, but affected patients are often involuntarily subjected to speculations about insalubrious alcohol consumption. Correspondingly, “brandy nose” has been used as
1420
A
B
a misleading label to describe rhinophyma. Typically, phymata do not resolve spontaneously. Rhinophyma, which occurs almost 20 times more often in male patients than in female patients, is often apparent initially in the skin of the alae nasi and at the distal end of the nose as dilated patulous follicles (Fig. 79-2A). Humps and grooves are prominent, resembling a “peau d’orange” appearance of the nose. Compression produces a white pasty matter that is composed of sebum, corneocytes, bacteria, and sometimes Demodex folliculorum mites. When rhinophyma becomes marked (Fig. 79-2B), it leads to the greatest deformity in this region and sometimes affects more proximal areas of the nose, as far as adjacent portions of the cheeks. Rhinophyma of the fibrous form
A
B
C
14
D
E
F
1421
4
14
(Fig. 79-2C) manifests with asymmetry of the nasal swelling caused by diffuse hyperplasia of connective tissue and sebaceous hyperplasia. Large actinic comedones can be prominent (sometimes called “potato nose”). In the fibroangiomatous form, the nose then appears copper to dark red, is grossly enlarged, and presents a network of ectatic veins and sometimes pustules. Although gross nasal distortion rarely occurs, the cosmetic impact is very significant in disease management. The incidence of both basal and squamous cell carcinomas has been reported to be higher in rhinophyma-affected skin than in nonlesional skin. However, this observation has not been unambiguously confirmed. There is no consistent relationship between the duration, severity, or any other feature of rosacea and the occurrence of rhinophyma; therefore, rhinophyma should be designated a condition of the skin that is closely associated with rosacea rather than a disorder that occurs as a consequence of the disease. Gnathophyma (Fig. 79-2D) is a rare occurrence, with the central chin typically being involved, while the lower half of the helices of the ears and the lobes are mainly affected in otophyma. Edema in this region may be present in severe inflammatory papulopustular rosacea. Other locations of phymata can involve the forehead (metrophyma; Fig. 79-2E) and eyelids (blepharophyma; Fig. 79-2F). The clinical picture of persistent edema and phymatous changes may overlap in some patients. Swelling is often associated with erythema and sometimes with other manifestations of rosacea (papules, pustules, telangiectasias) and occasionally ocular inflammation. Rhinophymata are particularly frequent when associated with seborrhea. Contrarily, seborrhea is not particularly associated with rhinophymata and often occurs in rosacea devoid of phyma.
FLUSHING AND TRANSIENT ERYTHEMA
FLUSHING AND TRANSIENT
ERYTHEMA
Flushing involves reactive vascular changes in the face that can be observed in normal individuals for a few seconds or few minutes. Physiologically, it can occur in response to various stimuli, especially heat, certain foods, alcohol, exercising, or stressful emotional stimuli. By contrast, moderate cooling alleviates the redness and has a transient therapeutic effect. Prolonged or more frequent than normal nonphysiological flushing manifests itself over hours to days and can develop into persistent erythema. Flushing in rosacea is a pathophysiological neurovascular process in the central face experienced for more than 5 to 10 minutes because of neuropeptide release. Because of its sudden noncontrollable appearance, it is embarrassing and very unpleasant for patients and is often associated with sensory symptoms such as stinging, burning pain. Flushing can be associated with persistent erythema, papules, pustules, or phymata or can occur as a single symptom. Both genders are
1422
equally susceptible to flushing without age preference, although in women, it is more frequent during menopause. Prolonged and frequent flushing is, with erythema, the most common complaint in patients with rosacea. Rosacea flushing can often be linked to typical trigger factors, mostly heat, hot steam (kitchen, beverages), red wine and certain other alcoholic beverages, medications such as niacin or topical glucocorticosteroids, noxious cold, and hormonal changes (menopause), rarely systematic disease. It may be accompanied with systemic symptoms such as wheezing, diarrhea, or headache and may be associated with sweating, indicating a role of nerves and mast cells in flushing pathophysiology. In particular, the release of gastrin hormonal mediators from the gastrointestinal (GI) tract have a systematic effect leading to frequent facial flushing and then persistent vasodilatation and telangiectasias on the face. Transient erythema is a prolonged unphysiological flushing that persists for more than 5 minutes and possibly as long as weeks or a few months but for no more than 3 months.
BLUSHING
BLUSHING
Blushing is not a characteristic feature of rosacea. We are briefly mentioning it in this chapter because although different in many aspects, the terms “flushing,” “transient erythema,” “persistent erythema,” and “blushing” are often inappropriately used to describe redness of the facial skin, which leads to confusion. Blushing, in contrast to flushing, is almost exclusively induced by emotionally stressful situations and not by spicy food or other rosacea trigger factors. Blushing has a more pinkish appearance than persistent erythema or flushing and is located on rosacea-atypical sites. It is characterized by sudden transient (mostly <5 minutes), pinkish involuntary redness of the peripheral cheeks, ears, retroauricular areas, neck, and chest, which can occur over years and often starts in early adulthood. “Pale islands” in between the salmon-like redness are also characteristic of blushing and cannot be found in flushing or transient or persistent erythema, indicating that a more autonomic neural process, often associated with enhanced sweating, also a sign of autonomic neural involvement. As with flushing, blushing can be also associated with skin sensations such as stinging or burning, as well as increased sweating but often milder than in flushing.
TELANGIECTASIA
TELANGIECTASIA
Telangiectasia can be defined as a permanent visible dilated blood vessel on the skin or mucosal surface. Multiple telangiectatic blood vessels build the clinical picture of telangiectasia (Fig. 79-3), which can develop
in the absence of any disease (genetically acquired, socalled primary or “essential” telangiectasia) or coexist or even precede skin (eg, rosacea) or systemic (eg, scleroderma) diseases, defined as secondary telangiectasia. In the new classification,16,19 telangiectasia are classified as a primary feature of rosacea, which can coexist with or without any other rosacea features. They can occur very sparsely or densely and be widely distributed in patients with rosacea.
PAPULES AND PUSTULES
PAPULES AND PUSTULES
Papules (Fig. 79-4A and B) can occur with or without pustules and can develop into cysts and nodules (rosacea conglobate), depending on the cytokines and chemokines released.20 Papules and pustules caused by rosacea can be easily recognized in most cases because of their mostly centrofacial distribution and the lack of comedones and scales, although multiple differential diagnoses of course need to be considered (see Differential Diagnosis). The papules in rosacea are mostly small, low pain, dome shaped, and red in color and usually present as multiples. They can also develop into edematous plaques, resembling lupus erythematosus. The lesions tend to occur symmetrically on the centrofacial skin but can extend to the neck, chest (Fig. 79-4B), and forehead, even in children. Forehead rosacea almost exclusively develops in patients with male pattern baldness, supporting the concept that UV radiation is a trigger factor for rosacea.
14
A
B
1423
4
14
Papules and pustules can, rarely, resolve spontaneously after 4 to 8 weeks, notably without scarring. The condition waxes and wanes because of trigger factors, emphasizing the value of maintenance therapy and tapering strategy. Papules and pustules are often associated with erythema or flushing, which mostly remains after antibiotic therapy (see combination therapy). Telangiectasias, phymatous changes, and ocular rosacea can also accompany papules and pustules.
OCULAR ROSACEA
OCULAR ROSACEA
Ocular rosacea is a frequent, bothersome, and often underestimated feature of rosacea. It involves the eyelids, eyelashes, or eyes of patients with rosacea and, if left untreated, bears risk of blindness. Ocular rosacea occurs in 25% of all patients with rosacea and in as many as 50% of patients with papules and pustules.21
Rosacea may affect many compartments of the eyes (Fig. 79-5), such as margins of the eyelids, glands of Zeiss, meibomian glands, lacrimal glands, conjunctiva, cornea, sclera, and iris.9,16,22,23 Typically, patients report a “foreign body” sensation of itching, burning, and stinging in the eyes and grittiness around the eyes. Inspection of the eyes is important; they often have red, swollen, crusty, or scaly margins. Telangiectasia of the conjunctiva may also occur.
RARE SUBFORMS OF ROSACEA
RARE SUBFORMS OF
ROSACEA
LUPOID OR GRANULOMATOUS ROSACEA
Lupoid rosacea is a distinct subform of rosacea defined by chronic, therapy-resistant, 0.2- to 0.3-cm-sized, often
1424
follicular brown-red or red papules that can develop to epithelioid (lupoid), granulomatous plaques and nodules on the cheek, forehead, or chin. The skin appears thickened and erythematous. Typically, the centrofacial and perioral regions of the face are affected. The upper and lower eyelids are involved in some cases. Diascopy reveals a follicle-associated lupoid infiltrate. Rare cases of lupoid rosacea have been observed after treatment with infliximab or etanercept. Whether lupoid rosacea and lupus miliaris disseminates faciei depict distinct disease entities is not yet clarified.
ROSACEA CONGLOBATE
Rosacea conglobate (Fig. 79-6) is a rare, chronic, and severe form of rosacea that resembles acne conglobate with hemorrhagic nodular abscesses and indurated plaques on erythematous background.
ROSACEA FULMINANS (PYODERMA FACIALE-O’LEARY)
Rosacea fulminans is a rare, acute or subacute, developing, maximal variant of rosacea with acne conglobate– like progression and predilection for postadolescent (20–30 years) women, particularly pregnant women; men are affected only rarely. Associations with seborrhoic dermatitis, a common inflammatory skin condition, and Crohn disease, a chronic inflammatory bowel disease, have been described without disclosing a
mechanistic connection to rosacea fulminans. The clinical findings develop within days to weeks and can affect the complete face—particularly the chin, cheeks, forehead, and nose—or remain localized, especially when present on the neck or trunk. The lesions present papulopustules and coalescent purplish nodules as well as associated abscesses, which often form confluent fistulae that drain a serous, seropurulent, or mucoid discharge. Reddish to violaceous firm swelling of the face is commonly noted. Patients often report an oiliness of the skin before the outbreak of rosacea fulminans. Despite the horrendous clinical picture, systemic symptoms such as fatigue, fever, arthralgia, and anaemia are usually absent. When the disease is controlled, it does not recur.
HALOGEN ROSACEA
Ingestion of iodides or bromides might cause a rosacealike reaction or deteriorate a persisting rosacea. The clinical findings resemble acne-like rashes or those described for rosacea conglobate. Patients can develop erythematous pustules, vegetative nodules, in extreme cases fungating nodules, small to large blisters, exudative plaques, ulcer (sometimes necrotic), a circumscribed panniculitis, or combinations of these presentations. Potential sources of halogen exposure are citrus-flavored soft drinks (cola drinks), (sea)food, diagnostic radiocontrast media, pool disinfectants, certain topical antiseptics, permanent hair wave formulations, and various products often not considered as potential sources, such as vitamin preparations and medications (eg, thyroid medication, chemotherapeutics). The amount of halogen required to cause a halogen rosacea is variable. The condition typically improves in 4 to 6 weeks after elimination of the exposure. Scarring and postinflammatory pigmentation might occur as residuals.
STEROID ROSACEA
When a patient with rosacea is treated with topical corticosteroids for a prolonged time, the atrophic side effects of the medication sometimes lead to an aggravation of the condition. The complexion changes to a deep flaming red or copper-red covered by a network of telangiectases (Fig. 79-7). The atrophic skin develops patches of scales, follicular papulopustules, nodules, and secondary comedones. The presentation is typically restricted to the area of corticosteroid application. Patients report a severe discomfort and nagging pain sensation.
GRAM-NEGATIVE ROSACEA
Prolonged treatment of a rosacea patient with a topical or systemic antibiotic that covers gram-positive bacteria will select gram-negative pathogens and thereby complicate the rosacea complexion. The characteristic clinical finding is the development of miniscule yellow pustules on a preexisting or newly formed erythema background. The clinical picture is not distinguishable from papulopustular rosacea. However, because of the
14
A
B
difference in therapy, the discriminating it from (grampositive) papulopustular rosacea is essential.
PERSISTENT EDEMA OF ROSACEA
Edema in rosacea should be distinguished from the diffuse idiopathic solid upper-facial edema (sometimes called Morbihan disease or edematous rosacea). Morbihan disease (Fig. 79-8; named after a region of northern France where patients with this problem were
1425
4
14
first identified) typically is not preceded by significant cutaneous inflammation. The cause of this type of facial swelling is unknown, and any relationship of chronic Morbihan disease to the typical pathophysiology of rosacea described later is doubtful. However, in rosacea, edema is present as hard, nonpitting swellings of mainly the caudal half of the face (ie, forehead, eyelids, cheeks, and nose) but also the glabella. Although the initial edema might not be constantly experienced, the later swelling is persistent and accompanied by erythema. In particular, swelling of the upper and lower eyelids causing visual difficulties is perceived as aggravating by the patient. Patients also report skin tightness and, infrequently, pruritus. Systemic reactions are profoundly absent. Edema in rosacea tends to become chronic, with flare-ups and periods of partial regression.
ETIOLOGY AND PATHOPHYSIOLOGY
Epidemiologic, clinical, and genetic studies indicate a genetic as well as environmental origin of rosacea; however, the pathophysiological mechanisms that initiate and perpetuate this chronic relapsing inflammatory skin disease are still poorly understood.
GENETICS AND ASSOCIATED CLUES REGARDING MECHANISMS OF DISEASE
GENETICS AND
ASSOCIATED CLUES
REGARDING MECHANISMS
OF DISEASE
A positive family history markedly increases the chances of developing rosacea. Moreover, monozygous twins with rosacea have a higher correlation of National Rosacea Society clinical score criteria than heterozygous twins.24
1426
Null mutation polymorphisms in the glutathione S-transferase (GST) gene have been found in patients with rosacea, which indicates that increased oxidative stress may be associated with rosacea pathogenesis.25,26 Two single-nucleotide polymorphisms (SNPs) found in patients with rosacea of European descent encode for butyrophilin-like 2 (BTNL2) and human leukocyte antigen (HLA)-DRA loci.26,27 Whereas HLA-DRA showed strong staining at sites of perifollicular inflammatory infiltrates, epidermal Langerhans cells, and endothelial cells, staining using an anti-BTNL2 antibody revealed diffuse expression in keratinocytes, perifollicular inflammatory infiltrates, and endothelial cells of papulopustular patients with rosacea. A polymorphism in NOD2/CARD15 was observed in a patient with granulomatous rosacea;28 the gene encodes a caspase recruitment protein involved in Toll-like receptor (TLR) function, including the function of TLR-2. Finally, a polymorphic variant of TACR3 was also observed in patients with rosacea;29 this gene encodes a tachykinin receptor subtype that responds to substance P family members, a neuropeptide critically involved in neurogenic inflammation, flare, and edema.
COMORBIDITIES AND ASSOCIATED CLUES REGARDING MECHANISMS OF DISEASE
COMORBIDITIES AND
ASSOCIATED CLUES
REGARDING MECHANISMS
OF DISEASE
Recent studies indicate that an increased risk of rosacea may be associated with inflammatory diseases of the GI tract, such as Crohn’s disease, ulcerative colitis, celiac disease or small intestinal bacterial overgrowth (SIBO) syndrome,26,30-33 probably caused by shared disease susceptibility to the HLA-DRA locus. Other associations to metabolic diseases such as diabetes,34 hypertension, dyslipidemia, and coronary artery disease35-37 have been found, possibly owing to low levels of highdensity lipoprotein–associated proteins or enzymes (eg, paraoxonase-1),38,39 increased cathelicidin levels,40 or endoplasmic reticulum stress.40-42
Patients with rosacea notably have various associations to neurologic disorders and neurodegenerative diseases, such as Alzheimer disease,43 Parkinson disease,44 migraine,45 depression,46 anxiety disorders,47
complex regional pain syndrome, and glioma.48
ENVIRONMENTAL TRIGGER FACTORS AND ASSOCIATED CLUES REGARDING MECHANISMS OF DISEASE
ENVIRONMENTAL TRIGGER
FACTORS AND ASSOCIATED
CLUES REGARDING
MECHANISMS OF DISEASE
Characteristic trigger factors for the initiation or aggravation of rosacea include heat (and, rarely, noxious
TRIGGERa REPORTED INCIDENCE (%) PUTATIVE RECEPTOR OR PATHWAY
Sun exposure 81 NALP3, TLR-2, TRPV4
Emotional stress 79 NALP3, TLR-2, TRPV1
Hot weather 75 TRPV1,2
Wind 57 NALP3, TLR2-, TRPV(?)
Heavy exercise 56 NALP3, TLR-2, TRPV1
Alcohol consumption 52 NALP3, TLR-2, TRPV1
Hot baths 51 TRPV1
Cold weather 46 TRPA1
Spicy foods 45 TRPV1
Humidity or osmotic changes 44 TRPV4
Indoor heat 41 TRPV1
Certain skin-care products 41 NALP3, TLR-2, TRPA1
Heated beverages (steam) 36 TRPV1
Certain cosmetics (eg, formaldehyde) 27 NALP3, TLR-2, TRPA1
Medications 15 NALP3, TLR-2, TRPV(?)
Microorganismsb NR NALP3, TLR-2
Garlic, mustard oil NR TRPA1
Noxious heat (52°C) NR TRPA1
Noxious heat (52°C) NR TRPA1
aMost common patient-reported triggers adapted from the National Rosacea Society (NRS; http://www.rosacea.org/patients/materials/triggersgraph .php) and modified from Holmes and Steinhoff.6
bMicroorganisms not reported as a known trigger in NRS survey. NALP3, NACHT-, LRR-, and PYD, domains-containing protein 3; NR, not reported; TLR-2, Toll-like receptor 2; TRPA1, transient receptor potential ankyrin 1; TRPV, transient receptor potential vanilloid. Modified from Holmes AD, Steinhoff M. Integrative concepts of rosacea pathophysiology, clinical presentation and new therapeutics. Exp Dermatol. 2017;26(8):659-67; with permission. Copyright © 2017, John Wiley & Sons.
cold), UV radiation, spicy food, certain alcoholic beverages (red wine more than white wine), stress, and microbial infestation on the face or in the gut (eg, demodex, bacterial overgrowth) (Table 79-1).16,49
Demodex mites are particularly found in association with papulopustular lesions.50
Which and how trigger factors induce papules and pustules is still unclarified and may include demodex mites, cutaneous or GI bacteria, a dysbalanced microbiota system in the gut (eg, SIBO syndrome), or stomach infection (eg, Helicobacter pylori). Whether the classical rosacea triggers, such as heat, UV radiation, some alcoholic beverages, hormonal dysregulation, or stress, are capable of triggering these eruptions is unknown.
HEAT, NOXIOUS COLD
Recent transcriptome and quantitative immunohistochemistry data indicate a role of transient receptor
14
potential (TRP) ion channels (eg, TRP vanilloid type 1 [TRPV1] and TRP ankyrin type 1 [TRPA1]), which can be activated by temperature changes (Fig. 79-9).1,51
Whether any noxious cold receptor(s) may trigger rosacea is unknown.
ULTRAVIOLET RADIATION
Sun exposure is a well-accepted trigger factor for rosacea. Indeed, sun exposure may be the trigger factor for rosacea on the bald scalp. However, to what extent UVA, UVB, or temperature increases account for rosacea symptom induction is not clear. The fact that patients behind glass shields develop asymmetric rosacea erythema and flushing indicates a role for at least UVA in rosacea. UV radiation induces neuroinflammation, endoplasmic reticulum stress, and innate immune responses and promotes skin fibrosis or solar elastosis, characteristics of rosacea. UVB triggers TRP vanilloid type 4 (TRPV4) activation on keratinocytes and is increased in tissue of patients with chronic photodermatitis and rosacea, suggesting a molecular pathway of UVB-induced rosacea through TRPV channels (see Fig. 79-9).52
MICROORGANISMS
Whether a dysbalance of the skin or GI microbiota contributes to the pathophysiology of rosacea, and if so which microorganisms are involved, is still poorly understood. Demodex folliculorum is a commensal of human and animal skin, predominantly in oily skin close to the pilosebaceous glands,53,54 and is increased in some patients with rosacea, predominantly in those with phymata as well as papules and pustules.55
Whether demodex mites are significantly enhanced in erythematous skin is unknown,56-58 but treatment that reduces demodex mite density positively correlates with clinical improvement.59,60 Which molecules or substrates produced by, or associated with, demodex mites account for rosacea is unknown. Candidates include Bacillus oleronius, proteases or chitins, which can activate protease-activated receptors (eg, PAR-2)61
or TLRs (eg, TLR-2),62 thereby releasing cytokines, chemokines, and matrix metalloproteinases (MMPs) and prostanoids, and attracting immune cells (see Fig. 79-9).
MECHANISMS OF DISEASE
MECHANISMS OF DISEASE
The already mentioned trigger factors probably initiate release of proinflammatory mediators from keratinocytes (eg, cathelicidin, vascular endothelial growth factor [VEGF], endothelin-1), endothelial cells (nitric oxide [NO], pituitary adenylate cyclase activating peptide [PACAP]), mast cells (cathelicidin, MMPs, tumor necrosis factor [TNF]-α), macrophages (interferon [IFN]-γ, TNF, MMPs, interleukin [IL]-26), helper-1 T (TH1) cells (IFN-γ), and helper-17 T (TH17) cells.
1427
4
14
Innate and adaptive immunity in rosacea
Bacteria Ultraviolet irradiation Demodex mite Skin barrier Heat > 37°C Irritants (FA, SDS, etc)
VitD Myd88
TLR-2
?
LL37(i)
(+MMPs)
LL37(a)
KLK5 IL-6, CXCL8, IL-12
PAR-2
ERDR1
Inflammation Angiogenesis CXCL5
aKLK5
IL-18
TSLP CCL5 CXCL8
TNF, IL-1
CXCL-20,19
TH 1
ROS, IFNγ, IL-6
IL-6
Neutrophil
TH 17
IL-8
KLK5/7 Trypsins MMP-2, -9
IL-1
Macrophage
TNF
IL-17
ROS
CCL2
VEGF, TNF-α
Mast cell
Angiogene sis
TGF-β, TNF-α
MMP-1, -2, -9
Fibrosis
CXCL8/9/10, CCL5/10
? Proteases
ER stress
TRPV1
TRPA1
TRPV4
IL-22 IL-17 CCL20 CCL5
ROS IL-1β, IL-6 TNF-α CXCL8
ET-1
Vasodilation IL-6, MMP1
?
Autoimmune damages?
TRPV1
TRPA1
B cell prolif
ETAR
Plasma cell
Substance P CGRP/ADM PACAP ATP, MMP-1
TGF-β
Nerve
Vasodilation, pain, Immunomodulation
1428
Triggers such as heat, noxious cold, exercising, spicy food, ethanol (or other ingredients or certain alcoholic beverages), and pH changes can directly activate sensory nerves to release vasoactive and proinflammatory neuromediators. Likewise, exercising and ethanol can activate release of neurotransmitters such as acetylcholine or neuropeptides such as PACAP from autonomic nerves. Some receptors that are responsive to rosacea trigger factors have indeed been discovered.41,51,63 Most of the trigger factors activate TRP ion channels on sensory nerves to induce neurogenic inflammation through release of neuropeptides such as substance P or PACAP. Neuropeptides are potent inducers of edema and vasodilation, the basis of flushing and erythema.56,64,65 The individual reactivity to otherwise innocuous triggers, however, is still not understood, but a genetic predisposition appears to influence this phenomenon. The genes involved have yet to be confirmed, but two SNPs have recently been identified and involve a major histocompatibility complex predisposition.26 It may well transpire that several of these factors are relevant and that each of the rosacea subtypes has different factors that are important to their initiation and progression.
IMMUNE RESPONSES
Similar to psoriasis and atopic dermatitis, innate immunity is known to have an essential role in the initiation and maintenance of rosacea. However, recent results point also to an important role of cytotoxic T-cell response in the pathophysiology of rosacea.6,66 How the adaptive and innate immune systems are connected in rosacea is still unclear (see Fig. 79-9).
Skin Barrier Dysfunction: Patients with rosacea suffer from increased transepidermal water loss (TEWL), as well as pH increase of the facial skin, both markers for skin barrier dysfunction.67,68 Increased TEWL leads to enhanced epidermal “leakage” and thus access for microbes, and an alkali pH enhances enzyme activity, for example, of kallikreins (KLK), such as KLK-5,-6,-7 or -12, which are enhanced in rosacea skin.1,5 KLK-5 activates LL-37 activity, which stimulates erythema, cytokine release, and angiogenesis.40,69 In addition, KLKs-5-,7 (and probably others) activate PAR-2, which is involved in several inflammatory
14
responses (see Fig. 79-9). Notably, both LL-37 and PAR-2 are upregulated in rosacea skin tissue, and PAR-2 upregulates LL-37 expression levels.70 The precise role and therapeutic impact of skin barrier dysfunction and restoration awaits further clarification. Toll-Like Receptors, Proteases, and Cathelicidin: TLR-2 is upregulated in patients with rosacea41,71 and induces release of proinflammatory cytokines, chemokines, proangiogenic factors, and proteases.56,63,72 TLR-2 induces upregulation and activation of the innate immune peptide cathelicidin via KLK-5 (see Fig. 79-9),41 leading to erythema, immune response, and angiogenesis through release of serine proteases, MMPs, cytokines, chemokines, and proliferation of endothelial cells.41,73,74 A role of cathelicidins in rosacea inflammation is now widely accepted,40 although direct functional in vivo data in humans is still missing. TLR-2 is also able to facilitate the activation of the NLRP3 inflammasome, which mediates IL-1β release and further inflammatory reactions.75 IL-1β expression is elevated in rosacea and mediates inflammatory responses therein. The upstream stimulator of TLR-2 in rosacea is still unknown. Microbes can activate TLRs on keratinocytes, although a direct link between demodex mites or certain bacteria, such as Bacillus oleronius, and TLRs in rosacea skin has not yet been demonstrated. Likewise, the connection between the intestinal microbiota flora dysbalance and the inflammatory responses in the skin are also unknown. Notably, vitamin D is enhanced in patients with rosacea and has been demonstrated to increase TLR-2 and KLK-5 mRNA expression levels, thereby regulating TLR-2, KLK-5, and LL-37 levels in rosacea.76
Inflammasome: The inflammasome consists of the rosacea trigger–responsive NALP3, caspase-1, and the adaptor protein apoptosis-associated speck-like protein (ASC), and orchestrates cleavage and activation of an rosacea-upregulated IL-1.56,75,77 Nucleotidebinding oligomerization domain (NOD)-like receptor (NALP3) is an integral member of the IL-1β inflammasome complex in keratinocytes that is required for inflammasome activation in rosacea.56 Inflammasome activation results in neutrophil chemotaxis, IL-1- and TNF-mediated inflammation amplification,
and release of neuropeptides such as substance P, calcitonin gene-related peptide (CGRP), adrenomedullin (ADM), and pituitary adenylate cyclase-activating polypeptide (PACAP), as well as adenosine triphosphate (ATP) from cutaneous sensory nerves, or endothelin-1 (ET-1) and IL-6 from keratinocytes. These products mediate an increase in vasodilation (flushing), vascular permeability (edema), or blood flow and enhance inflammatory circuits of adaptive and innate immune system, such as by leukocyte recruitment, T-cell or macrophage activation, and degranulation of mast cells. The released products of mast cell granules are especially involved in angiogenesis (vascular endothelial growth factor [VEGF], transforming growth factor [TGF]-β) and fibrosis (TGF-β, MMPs-1, -2, and -9). Substance P can induce release of chemokines from mast cells which can modulate function of TH1 cells (through CCL5, CXCL10), macrophages, or dendritic cells (via CCL2), thereby regulating adaptive immunity. It is furthermore known that activation of neuronal TRPA1, TRPV1, and TRPV4 lead to painful burning sensations, which may be similar to that observed in patients with rosacea. Of note, patients with rosacea rarely have pruritus as neural sensation. Through neural mediators, the sensory and autonomic nervous systems contribute to pain, vasodilation (flushing, erythema), plasma extravasation (edema), and immunomodulation (innate and adaptive immune cells). ETAR, endothelin receptor type A; FA, fatty acid; SDS, sodium dodecyl sulfate.
1429
4
14
and prostaglandin E2 synthesis, which supports pustule formation, heat pain sensation, and vascular responses, respectively. The inflammasome-activated cellular network of keratinocytes, macrophages, mast cells, and neutrophils (in papulopustular rosacea) creates a highly inflammatory milieu in rosacea. The concomitant production of reactive oxygen species (ROS) and MMPs further contribute to tissue damage, vasorelaxation, vasopermeability, and late-onset fibrosis in rosacea.
Imbalanced Adaptive Immunity: Both, T and B lymphocytes play a role in rosacea. Histological analysis and transcriptome studies reveal the presence of predominantly CD4+ and to a lower extent CD8+
T cells and cytokines in rosacea skin,20,78,79 with the dominance of CD4+ TH1 and TH17 cells and their corresponding cytokines. Cytokine expression profiles of all skin rosacea phenotypes demonstrate elevated TH1 cytokines IFN-γ, TNF, and TH17 cytokines IL-17A and IL-22.20 TH17 cells induce VEGF, which contributes to angiogenesis in rosacea (see Fig. 79-9). Because IFN-γ is a potent activator of macrophages, a close communication of adaptive and innate immune networks is likely to be present in rosacea. Rosacea eruptions, however, are also associated with T-cell immunosuppression after infection80 or therapeutic intervention (eg, corticosteroids, calcineurin inhibitors, phototherapy).81-83 Patients with eruptions of rosacea commonly present with Demodex mite infestation, supporting a parallel between Demodex proliferation and T-cell activity, and antibodies against Demodex have been found in patients with rosacea.80,81
In rosacea, immunologic tolerance is well preserved through relative high numbers of tolerogenic (regulatory) T cells compared with other skin.79 Other important molecules involved in rosacea pathophysiology through regulating adaptive immune responses are Erdr184 and IL-18,85 supporting the concept that TH1 immune responses, induction of ROS molecules,86 and angiogenesis are all important contributors of rosacea.87
NEUROVASCULAR DYSREGULATION AND NEUROINFLAMMATION
Skin hypersensitivity and flushing are direct consequences of neural stimulation in any condition or disease, including rosacea.88 The human face is to a certain extent physiologically unique because it is one of the few regions in the human skin where the blood vessels are under control of the sympathetic, parasympathetic, and sensory nerves. This fact implies that (nor)epinephrine, acetylcholine, and neuropeptides can modulate the state of the blood vessel diameter. Because autonomic nerves also release neuropeptides under certain circumstances and all mediators are involved in inflammatory processes and immune defense control, neuroinflammatory processes are involved in the perpetuation and maintenance of unphysiological
1430
(“diseased”) flushing and transient erythema. To which extent early immune responses may also induce neurovascular dysregulation is currently unknown. Flushing in patients with rosacea is pathophysiologically neurogenic inflammation, as described by Jancso and Szolcsanyi 50 years ago.89 Histopathologically, upper dermal edema and leukocytes can be found, which corresponds with neurogenic inflammation in animal ex vivo and in vivo studies. Thus, also not clearly shown in dermatopathological studies, transient erythema can be seen as an inflammatory process and cannot be explained by merely prolonged vasodilation. The molecular basis of the “neurovascular” genes, mediators, and receptors activated in rosacea are partially clarified (Fig. 79-10). However, it is still unknown whether the neurovascular system is mechanistically up- or downstream of the inflammatory cascade. It is certain that flushing and erythema are part of the inflammatory process and not merely a dilated vessel and cosmetic problem. Prolonged flushing lasting longer than 5 minutes is always part of the neurogenic inflammation cascade56,90 characterized by erythema (vasodilation), edema (postcapillary plasma extravasation), and recruitment of leukocytes to site of inflammation. Sensory neuron density is moderately increased in the erythematotelangiectatic rosacea.51,90
The various TRPs appear to render the thermal, chemical, and mechanical rosacea stimuli into clinical manifestations of rosacea.91 Because TRP channels can cross-talk with neuropeptide receptors, the interaction between these two types of receptors may be involved in sustaining neurovascular responses and inflammation in rosacea, particularly TRPA1 and TRPV1.1,51
TRPV1, TRPV2, TRPV3, TRPV4, and TRPA1 ion channels are broadly expressed on neuronal and non-neuronal cells in rosacea skin.51 Thus, TRPs might thereby establish the neuroimmune and neurovascular communication observed in rosacea. The variety of neuronal and vascular pathways that seem to be involved in rosacea neuroinflammation and pain, as well as skin hypersensitivity, explains the unique trigger profiles of individual patients with rosacea (see Table 79-1 and Fig. 79-10). Furthermore, pathophysiological outcomes may differ depending on individual receptor activation profiles and downstream cellular activation targets, providing a hypothesis for the phenotypic variability seen in rosacea. The autonomic nervous system, via stress-induced increase of the skin sympathetic nerve activity (SSNA), may also contribute to the pathophysiology of rosacea through increased blood flow (erythema), neuroinflammatory responses (cytokine release), and pain induction,92,93 for example, through release of cortisolreleasing hormone (CRH),94 PACAP,65 or NO.95 Clearly, autonomic dysregulation is involved in facial flushing (Fig. 79-11).66,92,96 This may be due to release of neuropeptides such as PACAP. In contrast, the skin shows normal vascular responses to application of epinephrine, norepinephrine, and acetylcholine in patients with rosacea.
14
Neurovascular communication in rosacea
Bacteria
Bacteria proteases
Protease
s t n a tirrI r e g g ir T UVB
Microbes Vitamin D
Alc. pH PAR-2 Excercise TRPV4
Protease PAR-2
SP: edema CGRP: vasodilation PACAP: vasodilation ATP: pain ET-1: pain
Cytokines ? Chemokines ? MMPs
ATP
TH 17 TH 1 Macrophage Neutrophil Mast cell
TLR2
pH- ∆
ET 1
TRPA1 TRPV1
TLR2
ETAR (?)
Pain Inflammation Vasodilation Edema Pain
SP CGRP PACAP ET-1 ATP
CGPR SP
Pain Vasodilation Edema
Proteases such as kallikreins (KLKs)-5, -6, and -7 activate protease-activated receptor-2 (PAR-2) on keratinocytes, endothelial cells, macrophages, mast cells, and sensory nerves, thereby contributing to innate and adaptive immune activation, vasoregulation and pain. PAR-2 induces release of various neuropeptides (SP, CGRP, PACAP) from nerves, as well as cytokines, chemokines, reactive oxygen species (ROS), and matrix metalloproteinases (MMPs) from cutaneous and immune cells. Although SP primarily promotes plasma extravasation (edema) and CGRP and PACAP vascular dilation, all can initiate pain sensations. PAR-2 is also regulated by various exogenous rosacea trigger factors as well as microbial agents and interacts with Toll-like receptors (TLRs).119-124 TLRs are pattern recognition receptors (PRR) that sense pathogen-associated molecular patterns (PAMPs). Notably, TLR-2 is also upregulated in patients with rosacea41,71 and induces release of neuropeptides, proinflammatory cytokines, chemokines, proangiogenic factors, and proteases such as KLK-5.56,63,72 However, the stimulator of TLR-2 in rosacea is still unknown. Via KLK-5-release, TLR-2 can activate PAR-2 and activate the innate immune peptide cathelicidin,41 leading to neuropeptide release and subsequent angiogenesis, erythema, plasma extravasation, and immune modulation. Thus, TLR and PAR-2 can be seen as a “forefront” of innate immunity in rosacea. ETAR, endothelin receptor type A; UV, ultraviolet.
1431
4
14
Regulation of facial blood vessels in rosacea
UVB
Irritative Inflammation Irritative Heat
Stress
LL37 TRPA1 TRPV4 pH
Stress
IL-6
ACh
Parasympathetic nerves Sympathetic nerves
Parasympathetic vasodilation
Excercise- ∆
MRGPRX2
TRPV4
TRPV1
?
TRPV1
Degranulation
TRPV1
Sensory nerves
TRPA1
IL-6R
Sympathetic vasodilation Sensory vasodilation
CGRP PACAP NO VIP ACh ACh
Vasodilation Pain? Vasodilation Edema Pain?
PHYMATOUS CHANGES, FIBROSIS, AND GLANDULAR HYPERPLASIA
Although a significant percentage of male patients with rosacea develop phymata, mostly on the nose, a pathophysiological link of chronic inflammation and skin fibrosis or sebaceous hyperplasia is unknown. A role of seborrhea has not been demonstrated
1432
convincingly for patients with rosacea, and some even have “dry skin.” Mast cells and B cells are critical contributor to skin fibrosis through release of MMPs, which is one plausible pathway for the development of phymata through chronic inflammation.20,97 The pathophysiological link between chronic inflammation and glandular hyperplasia is still enigmatic (Fig. 79-12).
14
Exogenous and endogenous trigger factors for fibrosis and glandular hyperplasia in rosacea
Irritants
Hair
Stress
Keratinocyes Epidermis
PAR-2
Proteases Dermis
Sebaceous glands
?
CRH Endocannabinoids EGF FOXo? PPAR?
CRHR
Neuropeptides
Hair follicle
CRH
Demodex mite
Bacteria
TLR2 agonist
Demodex proteases Bacteria proteases
Inflammation
Keratinocytes Keratinocytes
Proteases
Alc. pH
Barrier disruption
Proteases (MMPs)
? ?
TLR2
TGF-β, IL-6
B cell
PAR-1 PAR-2
PAR-2
IL-6R
Mast cell Fibroblasts
TLR2
IL-6
TGF-BR
TGF-β
Fibrosis (?) Glandular hyperplasia
Proteases MMPs
Immune cells
1433
4
14
TELANGIECTASIA
The pathophysiology of telangiectasia is unknown but differs from sun damage (chronic photodermatitis, heliodermatitis).98 One possible explanation is that proteases, MMPs, and growth factors from the transforming growth factor or fibroblast growth factor family destroy the architecture of the extracellular matrix, thereby reducing the tissue resistance for blood vessels, which subsequently leads to irreversible vasodilation.99 This, however, awaits further clarification through research.
GASTROINTESTINAL TRACT
The role of H. pylori in rosacea is controversial.100,101
More convincing evidence derives from studies in which patients with SIBO syndrome (eg, after surgeries, metabolic diseases) develop a microbiota flora in favor of proinflammatory, instead of protective, bacteria in the GI tract.102 Rifaximin, a drug that through T-cell modulation reinstalls the physiological flora in the GI tract, alleviates rosacea symptoms in the majority of cases (but not of patients with H. pylori through H+
pump blockers), which supports this hypothesis.32,103,104
DIAGNOSIS OF ROSACEA
The diagnosis of rosacea is led by the clinical features (see Clinical Findings) along with taking a thorough patient history (age, gender, trigger factors, hormonal changes, profession, hobbies, gut surgeries, Demodex infestation, exercising, heat exposure, noxious cold exposure, drinking and eating habits) and family history (positive family history). No diagnostic markers or laboratory workup exists to diagnose rosacea. To differentiate from other skin or systemic diseases, however, laboratory workup and diagnostic tools may be used. Histopathology, especially in the early erythematous stage, is often nonspecific; however, a biopsy may be helpful to exclude other differential diagnoses (see Differential Diagnosis).
HISTOPATHOLOGY OF ROSACEA
HISTOPATHOLOGY OF
ROSACEA
Histologically, rosacea is characterized by numerous features, depending on the presenting symptoms or subtype. In erythematous skin and telangiectasia, a perivascular inflammatory infiltrate consisting mainly of TH1 and TH17 cells, as well as macrophages and mast cells, can be observed;5,20 depending on severity, these cells can be sparse to numerous. In addition, blood and lymphatic vessels are markedly dilated, and a microscopically visible dermal edema can be found in all stages but is rarely found clinically. Papules consist of CD4+ TH1 and TH17 cells, macrophages, mast cells, and plasma cells. In pustules, additional neutrophils can be found.
1434
In phymatous rosacea lesions, the infiltrate still consists of TH1 and TH17 cells, macrophages, mast cells, and more plasma cells than in nonphymatous rosacea. Glandular hyperplasia and follicular plugging without comedones can be found as well as fibrosis and increase in fibroblasts.5 In phymatous rosacea and often follicular or perifollicular inflammation, Demodex folliculorum is present up to 50% of tissue specimen; these mites are most abundant in phymatous skin, which may account for the folliculitis and perifolliculitis. Whether Langerhans cells or dendritic cells are enumerated in all lesions is still unclear. Some authors found increased Langerhans cell density but others not.5
In ocular rosacea, dilation of blood and lymphatic vessels as well as obstruction of the meibomian gland can be observed. Granulomatous rosacea is characterized by dermal edema and vasodilation as well as dermal granulomas of the tuberculoid type with T cells and macrophages as well as multinucleated giant cells and plasma cells. The marked upper dermal vasodilation of blood and lymphatic vessels differentiates it from other granulomatous disorders such as lupus vulgaris. In rosacea fulminans, besides the infiltrate mentioned earlier, numerous epithelioid cells as well as occasionally granulomas with multinucleated giant cells can be observed. The histopathologic findings in patients with combined erythema and telangiectasia are relatively mild and not diagnostic. Upper dermal blood vessels usually appear prominent, and there may be a mild perivascular infiltrate composed mainly of lymphocytes with an admixture of histiocytes. The most consistent abnormality is a change in the collagen of the upper dermis, so-called “solar elastosis.” This represents the result of chronic actinic damage. The histopathological changes in some patients are characterized by marked fibrosis in the superficial and reticular dermis, accentuated around follicles and increased number of fibroblasts, but others (especially the obstructive form) show deposition of mucin in the dermis. The collagen in the upper dermis often shows changes of solar elastosis, which is marked in patients with rhinophyma secondary to actinic damage.
CLASSIFICATION
CLASSIFICATION
Currently, two classification systems exist: The first, described in 2002, regards rosacea as a syndrome or typology with four distinct clinical subtypes: (1) erythematotelangiectatic, (2) papulopustular, (3) phymatous, and (4) ocular rosacea Table 79-2).17,105 The severity can be graded as mild, moderate, or severe.106 These subtypes may be discrete variants or may progress from one subtype to another, with overlaps observed. The improvement brought by this classification was to determine a more structured phenomenology into this enigmatic skin disease and helped physicians on a daily basis to monitor the therapeutic success of each
SUBTYPE (NUMBER AND NAME)a CLINICAL CHARACTERISTICS
Subtype 1: erythematotelangiectatic Persistent central facial erythema, frequent flushing; may be telangiectatic vessels
Subtype 2: papulopustular Erythematous dome-shaped papules, some with surmounting postulation in a centrofacial distribution on a background of persistent erythema
Subtype 3: phymatous Persistent facial swelling with hypertrophy of tissue (rhinophyma); different variants described
Subtype 4: OR Ocular inflammation (eg, blepharitis,
Subtype 4: OR Ocular inflammation (eg, blepharitis, conjunctivitis, or meibomian gland dysfunction; chalazion)
conjunctivitis, or meibomian gland dysfunction; chalazion)
aEach subtype can be graded as mild, moderate, and severe.
subtype. The disadvantage is that the clinically accumulated symptoms (eg, erythema and telangiectasia) may be based on different pathophysiologies and are thus preventing a more pathophysiology-based understanding of the disease. Moreover, many patients present with an overlap of all subtypes (eg, papulopustular and ocular or phymatous with or without erythema), which complicates a clear-cut classification. Finally, a frequent, if not dominant symptom—flushing—is neglected or subclassified as erythema, which is pathophysiologically incorrect. Consequently, a modified classification or grading system was introduced in 2016 to 2017,16,19 emphasizing each possible symptom in rosacea and subclassifying them as diagnostic, major, or secondary features based on how important or selective the symptom is to make the diagnosis (eg, there are almost no differential diagnoses for a phymata or persistent central facial erythema) Table 79-3). Although also not perfect, the new classification considers more thoroughly the many overlap patients existing in the “real-world situation,” outlying the subtype classification and leaving more room for a pathophysiology-based classification and therapy.13,18,107 Thus, the new classification likely reflects more precisely the clinical reality of the disease presentation, although validating data are missing.16,13
A recent expert group assessed phymatous changes as an individually diagnostic sign of rosacea and persistent centrofacial erythema associated with periodic intensification by potential trigger factors as a minimum diagnostic sign of rosacea. Flushing, telangiectasia, and inflammatory papules or pustules are considered major features but are not diagnostic of rosacea. The centrofacial location of diagnostic and major features is essential for rosacea diagnosis. The bilateral facial location of a presentation is considered typical but not essential. Stinging sensation, edema, dry sensation, and
14
DIAGNOSTIC FEATURESa MAJOR FEATURES SECONDARY FEATURES
Persistent centrofacial erythema associated with periodic intensification by potential trigger factors
Flushing or transient erythema Burning sensation of the skin
Phymatous changes Inflammatory papules and pustules Stinging sensation of the skin
Telangiectasia Edema
Ocular manifestations
Dry sensation of
Dry sensation of the skin
Ocular manifestations
■Eyelid margin telangiectasis
■Eyelid margin
the skin
telangiectasis
■Blepharitis
■Blepharitis
■Keratitis, conjunctivitis, or sclerokeratitis
■Keratitis, con-
junctivitis, or sclerokeratitis
aAll features can present as mild, moderate, or severe. Modified from Tan J, Almeida LMC, Bewley A, et al. Updating the diagnosis, classification and assessment of rosacea: recommendations from the global ROSacea COnsensus (ROSCO) panel. Br J Dermatol. 2017;176(2): 431-438 and Gallo RL, Granstein RD, Kang S, et al. Standard classification and pathophysiology of rosacea: The 2017 update by the National Rosacea Society Expert Committee. J Am Acad Dermatol. 2018;78(1):148-155.
burning sensation are considered secondary features (symptoms) of rosacea.
DIAGNOSTIC TOOLS
DIAGNOSTIC TOOLS
Diagnostic tools are available for some of the major features of rosacea Table 79-4).
CLINICAL MANIFESTATION DIAGNOSTIC TOOL
Flushing Flushing Assessment Tool (FAST) Global Flushing Severity Score (GFSS)
Persistent erythema Investigator’s Global Assessment (IGA) Clinician’s Erythema Assessment (CEA)/ Patient’s Self-Assessment (PSA)
Telangiectasia None
Papules or pustules Lesion counts Investigator’s Global Assessment
Phymatous changes None
Ocular manifestations Pending
Ocular manifestations Pending
Modified from Tan J, Almeida LMC, Bewley A, et al. Updating the diagnosis, classification and assessment of rosacea: recommendations from the global ROSacea COnsensus (ROSCO) panel. Br J Dermatol. 2017; 176(2):431-38.
1435
4
14
GROUP PRESENTATION
1 Distal end, apex of nose
2 Distal half nose, apex, alae,
3 Distal half of nose, apex, alar nodules
4 Complete nose, including bridge and nasofacial sulci
4 Complete nose, including bridge and nasofacial sulci
Modified from Clark DP, Hanke CW. Electrosurgical treatment of rhinophyma. J Am Acad Dermatol. 1990;22(5 Pt 1):831-37.
THE GRADING OF SEVERITY OF ROSACEA
THE GRADING OF SEVERITY
OF ROSACEA
The grading of rosacea is divided into mild, moderate, and severe. The grading provides the physician with a practical tool to evaluate the patient’s need for a certain therapy and helps to monitor the response to therapeutic intervention.16
A clinical scale based on the morphological involvement has been introduced for assessment of the severity of rhinophymata Table 79-5). No widely accepted classification exists for telangiectasia.17,106 The severity of papules and pustules in rosacea may be graded according to the numbers of papules and pustules (few, several, or many) and whether plaques (confluent inflammatory lesions on a raised area of erythema) are present. Ocular rosacea should be graded Table 79-6), and ophthalmologic consultation should be initiated promptly in moderate to severe cases.
DIFFERENTIAL DIAGNOSIS
Clinically, the classical (vulgaris) rosacea has to be differentiated from various diseases and rarer rosacea forms Table 79-7), such as granulomatous, lupoid, fulminans, conglobata. Most prominent disorders that may be confused with rosacea are seborrheic dermatitis, acne vulgaris, chronic discoid lupus erythematosus, sarcoidosis, polymorphous light eruption, and erysipelas (see Table 79-7). Thorough examination may be necessary to exclude multisystem involvement if other diagnoses are suspected. The list of diseases mimicking the rosacea phenotype is vast and includes
Mild: mild itch, dryness or grittiness of the eyes; fine scaling of eyelid margins; telangiectasia and erythema of eyelid margins; mild conjunctival injection. Moderate: burning of eyes; crusting or irregularity of eyelid margins with erythema and edema; formation of chalazion or hordeolum) Severe: pain, photosensitivity, blurred vision, loss of eyelashes, severe conjunctival inflammation, corneal changes, scleritis or episcleritis, uveitis, iritis
Mild: mild itch, dryness or grittiness of the eyes; fine scaling of eyelid
margins; telangiectasia and erythema of eyelid margins; mild conjunctival injection. Moderate: burning of eyes; crusting or irregularity of eyelid margins
with erythema and edema; formation of chalazion or hordeolum) Severe: pain, photosensitivity, blurred vision, loss of eyelashes, severe
conjunctival inflammation, corneal changes, scleritis or episcleritis, uveitis, iritis
1436
disorders of various etiopathologies. Consideration of the differential diagnoses on the basis of the main feature of skin presentation is therefore useful (Tables 79-8 to 79-16). Helpful observations to differentiate various forms of flushing are shown in Table 79-11.
MANAGEMENT OF ROSACEA
Before therapy, the features and severity of the disease should be rated to define the right therapy, although it should be remembered that some of the features may not be visible or present at consultation. Evaluation of the medical history (including steroids, topical calcineurin inhibitors, brome) should be undertaken, and drug triggers should be ceased. Trigger avoidance is important to improve the condition and protect from relapses and is thus as important as therapy (Fig. 79-13 and Table 79-17).
GENERAL SKIN CARE
GENERAL SKIN CARE
Thorough education and instructions for proper general skin care is a critical component of adequate rosacea management because consequent application of adequate nonirritating skin care can significantly prevent or attenuate relapses or tone down dry skin or pain sensations (see Table 79-17). Moreover, educating patients about behavioral strategies and approaches to reduce the facial skin symptoms will reduce the psychological disease burden and significantly improve patient’s quality of life and patient outcome. Essential skin care advice elements are (1) avoidance of trigger factors, (2) usage of foundations and facial coverage without aggravating symptoms of rosacea, (3) use of sunscreen SPF (sun protection factor) of at least 30+, (4) frequent use of moisturizers if dry skin is an issue, (5) usage of drying cleansing for an oily nose, (6) regular use of gentle cleansers for the whole face, (7) use of matte green–toned foundations to mask skin redness, and (9) avoidance of rubbing the face.
FIRST-LINE, SECOND LINE, AND OFF-LABEL TREATMENTS
FIRST-LINE, SECOND
LINE, AND OFF-LABEL
TREATMENTS
Based on new knowledge, a phenotype-driven treatment algorithm has recently been developed (see Fig. 79-13) relating to the major cutaneous features of flushing, transient erythema, persistent erythema, papules or pustules, telangiectasia, phymata, and pain sensations. For each feature, first-line therapies vary on the basis of their pathophysiology (Fig. 79-14) and clinical severity. Given that the different symptoms derive from different pathophysiologies, the combination of various topical with systemic treatments or
14
Most Prominent Differential Diagnosis to Rosacea and Investigations TABLE 79-7
DIFFERENTIAL DIAGNOSIS INVESTIGATION
Acne vulgaris
■Comedones, no flushing, different age peak, no phymatous changes
Acne vulgaris ■Comedones, no flushing, different
age peak, no phymatous changes
■Patients with SLE often have other areas of cutaneous involvement such as the sides and V of the neck
■Patients with SLE often have other
Systemic lupus
Systemic lupus erythematosus (SLE)
erythematosus (SLE)
areas of cutaneous involvement such as the sides and V of the neck
■Systemic reactions
■Systemic reactions
■ANA and anti-DNA (anti-Ro, anti-La)
■ANA and anti-DNA (anti-Ro, anti-La)
■Skin biopsy, histopathologic examination; direct and indirect immunofluorescence
■Skin biopsy, histopathologic
examination; direct and indirect immunofluorescence
■Skin biopsy, histopathologic examination
■Skin biopsy, histopathologic
Chronic discoid lupus
Chronic discoid lupus erythematosus (CDLE)
erythematosus (CDLE)
examination
■Direct immunofluorescence (IgG, IgM, IgA, C1, C3)
■Direct immunofluorescence (IgG,
IgM, IgA, C1, C3)
■Photosensitivity
■Photosensitivity
■UV-induced pruritus
■UV-induced pruritus
■History, photosensitive eruptions, distribution more peripheral
■History, photosensitive eruptions,
Photodamage (heliodermatitis)
Photodamage
(heliodermatitis)
distribution more peripheral
Allergic photoreaction
■Heliotropic macropattern
Allergic photoreaction ■Heliotropic macropattern
■Diffusely bordered eczema
■Diffusely bordered eczema
■Eczematous “satellite” lesions
■Eczematous “satellite” lesions
■History, photopatch test
■History, photopatch test
Toxic photoreaction
■Heliotropic macropattern
Toxic photoreaction ■Heliotropic macropattern
■Sharply bordered eczema
■Sharply bordered eczema
■History
■History
Polymorphic light eruption
■More monomorphic
Polymorphic light eruption ■More monomorphic
■Photo provocation, early and late assessment
■Photo provocation, early and late
assessment
■Skin biopsy, histopathologic examination
■Skin biopsy, histopathologic
examination
Dermatomyositis
■Muscle weakness
Dermatomyositis ■Muscle weakness
■Anti-Jo antibody
■Anti-Jo antibody
Seborrheic dermatitis
■Slight yellow to orange tinge or scales on erythematous ground
Seborrheic dermatitis ■Slight yellow to orange tinge or
scales on erythematous ground
■More itch, less stinging or burning
■More itch, less stinging or burning
■Distribution and more eczematous
■Distribution and more eczematous
Contact dermatitis
■Morphology of eczema
Contact dermatitis ■Morphology of eczema
■Patient history
■Patient history
■Exposition
■Exposition
DIFFERENTIAL DIAGNOSIS INVESTIGATION
Facial atopic dermatitis
■Blood work (IL-16, ECP, IgE)
■Skin biopsy and histopathologic examination
■Anamnesis, patient history, eczema morphology, pruritus
Erysipelas
■Serology (leucocytosis, CRP)
■ASO, ADB titer
■Fever
■Medication
Steroid-induced acneiform folliculitis, steroid rosacea
■History
■No pustules, distribution, history, histology
Jessner lymphocytic infiltrate
Sarcoidosis
■Serology (ACE, sIL-2R, Neopterin, Ca2+)
■Serum electrophoresis (IgG)
■Cell count
■Histology
Perioral dermatitis
■Unaffected perioral zone
■History of “intensive” local therapy
■No flushing; rarely, erythematous plaques
■Facial swelling in the morning
Obstruction of superior vena cava
■Breathing difficulty
■Upper limb edema
■Neck edema
■Pemberton’s sign
■Radiography, CT scan, bronchoscopy
Syphilis
■Serology,
■TPHA, VDRL, FTA(Abs) test
■Liquor serology
Tuberculosis
■Skin biopsy, Ziehl-Neelsen stain
■QuantiFERON-TB GIT test
■Radiography
Haber syndrome
■Family history
■Hereditary transmission (autosomal dominant
■Burning sensation
■Brownish pigmentation, induration
ADB, anti-DNase B; ACE, angiotensin converting enzyme; ANA, antinuclear antibody; ASO, anti-streptolysin O; CRP, C-reactive protein; CT, computed tomography; C1, complement component 1; C3, complement component 3; FTA(Abs), fluorescent treponemal antibody absorption; Ig, immunoglobulin; IL, interleukin; sIL-2R, soluble interleukin-2 receptor; TPHA, treponema pallidum hemagglutination assay; UV, ultraviolet; VDRL, Venereal Disease Research Laboratory.
CONDITION FEATURES
Lupus pernio (sarcoid of the nose) Shiny brown, red, or violaceous, firm swelling of nose; can be monomorph and singular; may be asymmetrical; may extend to medial cheeks; diascopy reveals “apple jelly nodules” in lupus pernio; dermoscopy and biopsy help establish diagnosis; workup for systemic involvement required
Basal or squamous cell carcinoma Age; histology; both mimic or occur in association with rhinophyma; rapid growth and surface erosion or ulceration requires biopsy
Lymphoma or angiosarcoma Rare; intranasal biopsy may be necessary to diagnose lymphoma; nasal lymphomas may be mistaken for rhinophyma but do not show glandular hyperplasia but a shiny surface
Lupus vulgaris (TB) Geographical differences of prevalence; can mimic rhinophyma, but scarring often present; also extrafacial; histology
Acrocyanosis Bluish discoloration of nose, especially in cold weather; usually no deformity; no glandular hyperplasia
1437
Lupus erythematosus Erythema but no flushing history; scales (CDLE); tendency to scarring is a features of CDLE; more rarely, papules and pustules
Lupus erythematosus Erythema but no flushing history; scales (CDLE); tendency to scarring is a features of CDLE; more rarely, papules and pustules
CDLE, chronic discoid lupus erythematosus; TB, tuberculosis.
4
14
Rosacea Demodicosis Drug induced (eg, cortisone) Contact dermatitis Seborrheic dermatitis Tinea Dermatomyositis Lupus erythematosus Polymorphous light eruption Disorders of flushing Facial erysipelas, Jessner lymphocytic infiltrate, polymorphic light eruption Granuloma faciale, lymphocytoma cutis, facial sarcoid Heliodermatitis, atopic dermatitis, contact and photo contact dermatitis Photodermatitis
Rosacea Demodicosis Drug induced (eg, cortisone) Contact dermatitis Seborrheic dermatitis Tinea Dermatomyositis Lupus erythematosus Polymorphous light eruption Disorders of flushing Facial erysipelas, Jessner lymphocytic infiltrate, polymorphic light
eruption Granuloma faciale, lymphocytoma cutis, facial sarcoid Heliodermatitis, atopic dermatitis, contact and photo contact
dermatitis Photodermatitis
even topical with systemic treatments and physical therapy has to be considered (see Fig. 79-13).7,108
If one of the first-line therapies fails, alternative first-line options should be considered or secondline therapies chosen. These therapies should always be combined with an adequate general skin care and prevention therapy.
PERSISTENT ERYTHEMA
For persistent erythema, approved therapeutic regimens are topical brimonidine gel (1%) and oxymetazoline crème (1%). Beta-blockers such as carvedilol can be used off label and should be tapered down.109 Intense pulse light as well as lasers can be used but should be avoided in patients with rosacea with somatosensations such as pain without pretreatment to avoid aggravation of pain symptoms through neuroinflammation Table 79-18).8
Rosacea Benign causes: emotion (blushing), anxiety, stress, climacteric flushing, hyperthermia, temperature (both hot and cold), sun exposure, fever, exercise, fluorescent lights, foods, beverages, drugs, alcohol, sodium nitrate Drug-induced (eg, bromindione), peptic ulcer episodes of diarrhea Systemic diseases: carcinoid syndrome, mastocytosis, polycythemia vera, anaphylaxis, allergy, Zollinger-Ellison syndrome, Rovsing syndrome, Frey syndrome Neurologic: see later Tumors: medullary carcinoma of thyroid, renal carcinoma, pancreatic cell tumor (VIP, PACAP, and so on), pheochromocytoma, bronchogenic carcinoma Postsurgical (gastric, prostate, orchiectomy) Idiopathic
Rosacea Benign causes: emotion (blushing), anxiety, stress, climacteric flush-
ing, hyperthermia, temperature (both hot and cold), sun exposure, fever, exercise, fluorescent lights, foods, beverages, drugs, alcohol, sodium nitrate Drug-induced (eg, bromindione), peptic ulcer episodes of diarrhea Systemic diseases: carcinoid syndrome, mastocytosis, polycythemia
vera, anaphylaxis, allergy, Zollinger-Ellison syndrome, Rovsing syndrome, Frey syndrome Neurologic: see later Tumors: medullary carcinoma of thyroid, renal carcinoma, pancreatic
cell tumor (VIP, PACAP, and so on), pheochromocytoma, bronchogenic carcinoma Postsurgical (gastric, prostate, orchiectomy) Idiopathic
1438
PACAP, pituitary adenylate cyclase activating peptide; VIP, vasoactive intestinal peptide.
■Menopausal flushing is usually diffuse on the face and the skin often appears shiny because this type of flushing is typically associated with sweating (so-called “hot flushes”). The average hot flush lasts about 4 minutes. Women with hot flushes have an increased body core temperature and a reduced thermo-neutral zone (the body core temperature range above which sweating occurs and below which shivering occurs).130
■Menopausal flushing is usually diffuse on the face and the skin
often appears shiny because this type of flushing is typically associated with sweating (so-called “hot flushes”). The average hot flush lasts about 4 minutes. Women with hot flushes have an increased body core temperature and a reduced thermo-neutral zone (the body core temperature range above which sweating occurs and below which shivering occurs).130
■Hormonal therapy (eg, estrogen) is the standard treatment and can decrease the frequency and severity of hot flushes by up to 90%.
■Hormonal therapy (eg, estrogen) is the standard treatment and can
decrease the frequency and severity of hot flushes by up to 90%.
■The flushing that occurs with the carcinoid syndrome, mastocytosis, and pheochromocytoma is not usually accompanied by sweating and so fall into the category of “dry flushing.”
■The flushing that occurs with the carcinoid syndrome, mastocyto-
sis, and pheochromocytoma is not usually accompanied by sweating and so fall into the category of “dry flushing.”
■Flush associated with the carcinoid syndrome has been classified into four different patterns. One pattern involves the face and chest and is relatively brief, lasting less than 5 minutes. In other patients, the flush can be prolonged for more than 5 minutes. Persistent edema and “leonine facies” have been reported in a patient with longstanding carcinoid syndrome.131
■Flush associated with the carcinoid syndrome has been classified
into four different patterns. One pattern involves the face and chest and is relatively brief, lasting less than 5 minutes. In other patients, the flush can be prolonged for more than 5 minutes. Persistent edema and “leonine facies” have been reported in a patient with longstanding carcinoid syndrome.131
■Flushing may occur in patients with mastocytosis after exercise, ingestion of alcohol or codeine, or injection of polymyxin B. Palpitations, diarrhea, and pruritus may accompany it. Dermatographia is often present.
■Flushing may occur in patients with mastocytosis after exercise,
ingestion of alcohol or codeine, or injection of polymyxin B. Palpitations, diarrhea, and pruritus may accompany it. Dermatographia is often present.
■Hyperhidrosis, piloerection, and episodic hypertension in association with flushing can occur in patients with phaeochromocytoma. It affects the face, neck, chest, and trunk for 15 minutes to several hours.
■Hyperhidrosis, piloerection, and episodic hypertension in associa-
tion with flushing can occur in patients with phaeochromocytoma. It affects the face, neck, chest, and trunk for 15 minutes to several hours.
■Flushing and severe pruritus or a burning sensation after a hot bath has been reported to patients who have polycythemia. This group appears plethoric and can associate with facial telangiectasias, which affect the face but also distal extremities. The veins of the sclera, retina, and oral mucosa may also be distended.
■Flushing and severe pruritus or a burning sensation after a hot bath
has been reported to patients who have polycythemia. This group appears plethoric and can associate with facial telangiectasias, which affect the face but also distal extremities. The veins of the sclera, retina, and oral mucosa may also be distended.
If erythema is associated with mild, moderate, or severe pain, topical or systemic analgesic therapy such as lidocaine gel (up to 4%), polidocanol cream (in mild cases), or even systemics such as nonsteroidal antiinflammatory drugs (eg, ibuprofen) should be applied; antidepressants or neuroleptics (eg, amitriptyline, gabapentin, pregabalin) may also need to be prescribed.110
If suspicious of the cause of pain, consultation of a neurologists is advised to rule out other pain syndromes, such as trigeminal neuralgia, small-fiber neuropathy, or early multiple sclerosis.
Chronic discoid lupus erythematosus Drug induced (eg, cortisone) Senile atrophy Basal cell carcinoma Dermatomyositis Haber syndrome Carcinoid syndrome Systemic lupus erythematosus Heliodermatosis, polymorphous light eruption Naevus flammeus Poikiloderma Sarcoidosis
Chronic discoid lupus erythematosus Drug induced (eg, cortisone) Senile atrophy Basal cell carcinoma Dermatomyositis Haber syndrome Carcinoid syndrome Systemic lupus erythematosus Heliodermatosis, polymorphous light eruption Naevus flammeus Poikiloderma Sarcoidosis
Rosaceiform dermatitis (check drug history, eg, steroid, calcineurin inhibitor intake) Acne vulgaris (comedones, cysts, and scarring on the chest and back in males) Perioral dermatitis (check topical steroid usage) Seborrheic dermatitis (pityriasis capitis is often marked) Pityriasis folliculorum or demodicosis (skin scraping is helpful) Tinea faciei, Candida spp. (scraping or swabs for culture), contact dermatitis (patch testing is helpful) Ulerythema ophryogenes, Jessner lymphocytic infiltrate, lymphocytoma cutis, sarcoid (skin biopsy is helpful) Morbihan disease, polycythemia, polymorphic light eruption, photosensitive eruption (blood tests and phototesting are helpful) T. faciei
Rosaceiform dermatitis (check drug history, eg, steroid, calcineurin
inhibitor intake) Acne vulgaris (comedones, cysts, and scarring on the chest and back
in males) Perioral dermatitis (check topical steroid usage) Seborrheic dermatitis (pityriasis capitis is often marked) Pityriasis folliculorum or demodicosis (skin scraping is helpful) Tinea faciei, Candida spp. (scraping or swabs for culture), contact
dermatitis (patch testing is helpful) Ulerythema ophryogenes, Jessner lymphocytic infiltrate, lymphocy-
toma cutis, sarcoid (skin biopsy is helpful) Morbihan disease, polycythemia, polymorphic light eruption, photo-
sensitive eruption (blood tests and phototesting are helpful) T. faciei
FLUSHING AND TRANSIENT ERYTHEMA
Early rosacea is often associated with flushing or transient erythema. Laser therapy (see discussion of physical therapies) is the common treatment used (see Table 79-18). Off-label use of topical adrenergic receptor modulators (eg, brimonidine, oxymetazoline) may alleviate flushing intensity and frequency. Avoidance of triggers (see Table 79-1) is likely to prevent or alleviate flushing, and thus patients should be advised to keep a diary of events. If unsure with any topical agents, patients should test the medication or cosmetic on one spot on one side of the face first. If pain symptoms are associated, the same applies as for persistent erythema. In addition, topical lidocaine (4%) may be helpful.
TELANGIECTASIA
Telangiectasia can only be treated with either laser therapy (see discussion of physical therapies) or 0.5% to 1.0% aethoxysclerol injections, similar to leg sclerotherapy. However, contraindications have to be considered, and the potential induction of vasoocclusion advocates for a cautious application by specialists. Steroid use and sun exposure should be avoided, and sunscreens are helpful to prevent sun damage followed by destruction of the extracellular matrix.
PAPULES AND PUSTULES
Papules and pustules are primary clinical signs and features of rosacea. The basic therapy (avoiding triggers or irritating substances on the affected skin,
Perioral dermatitis Steroid rosacea Small nodular sarcoidosis
Perioral dermatitis Steroid rosacea Small nodular sarcoidosis
14
Acne conglobate Acne fulminans Halogen rosacea Gram-negative folliculitis
Acne conglobate Acne fulminans Halogen rosacea Gram-negative folliculitis
application of photoprotective agents, appropriate cosmetic coverage, stress management, and optimized skin cleansing and moisturizing routines) as outlined for patients with erythema also applies to patients who develop rosacea with papules and pustules. In general, mild to moderate papules and pustules respond well to topical therapy such as ivermectin (1%), metronidazole (0.75%–1%), azelaic acid (15%), sodium sulfacetamide, and sulphur. Successful nonapproved (off-label) therapy has been described with topical erythromycin (2%), tretinoin or isotretinoin, clindamycin, and permethrin. However, good evidence indicates that papules and pustules resolve faster and longer using a combination therapy, for example. using the slow-release doxycycline and topical ivermectin. Off-label use with oxytetracycline 500 mg twice a day, doxycycline 100 mg twice a day, minocycline 50 mg/day, erythromycin 500 mg twice a day has been reported with good success and tolerability. In severe or resistant cases, systemic metronidazole, clarithromycin, and azithromycin have relatively rapid onsets of efficacy and fewer tendencies for GI adverse effects than erythromycin and less hyperpigmentation tendency than minocycline. If Demodex mite numbers are increased, a short course of permethrin cream should be applied in addition to approved ivermectin cream therapy. After 3 or 4 months, depending on improvement, systemic therapy can be tapered down while topical therapy is continued. If erythema remains an issue, topical adrenergic receptor blockers (brimonidine, oxymetazoline) may be continued. Topical maintenance therapy may be beneficial to avoid reoccurrence. Successful treatment of papules and pustules have been reported using laser, light, or photodynamic therapy but remains to be clarified.8
PHYMATA
There is substantial evidence that low-dose isotretinoin has a beneficial effect in early as well as
Acne vulgaris Acneiform exanthema Acneiform syphilid Rosacea conglobate or fulminans Follicular pyoderma Tinea barbae
Acne vulgaris Acneiform exanthema Acneiform syphilid Rosacea conglobate or fulminans Follicular pyoderma Tinea barbae
1439
4
14
Symptom manifestation-dependent therapy regimen in rosacea
Connective tissue/ sebaceous hyperplasia
Ocular rosacea Persistant erythema Teleangiectasia
Flushing/ transient erythema
Papules and Pustules
General measures: patient education, avoidance of triggers, sun protection, skin care, doctor-patient relationship, and so on
Patient management
Topical therapy:
– Brimonidine 3 mg/g (++++)
Oxymetazoline creme 1%
Oxymetazoline creme 1%
Medicinal
Systemic therapy:
Beta blockers, eg, carvedilol
Beta blockers, (eg, carvedilol)
Low-dose antibiotics (eg, minocycline 50 mg every other day)
Physical interventions
Maintenance
IPL (++)
IPL (++)
Laser (++)
Laser (++)
Low-dose antibiotics (eg, minocycline 50 mg twice weekly)
Eyelid hygiene
Artificial, lipidcontaining tears
Severity
Topical therapy:
Topical therapy:
– Ivermectin 10 mg/g (++++) – Azelaic acid 150 mg/g (++++) – Metronidazole 7,5 mg/g (+++)
– Ivermectin 10 mg/g (++++)
Systemic therapy:
– Low-dose, modified- release doxycycline 40 mg (++++)
In severe and/or treatment-resistant rosacea:
Combination of topical and/or systemic antiinflammatory therapy
Systemic therapy:
Systemic therapy:
Systemic therapy:
Topical therapy:
– Low-dose isotretinoin (++++) – Doxycycline (++++) – Tetracycline (+++) – Azithromycin (+) – Clarithromycin
– Permethrin – Benzyl benzoate – Retinoids – Calcineurin- inhibitors
– Low-dose isotretinoin
– Doxycycline: low-dose (40 mg) or conventional dose – Low-dose isotretinoin
Topical therapy:
In severe and/or treatment-resistant rosacea:
– Cyclosporin A (++) – Azithromycin – Tetracycline – Steroids
Combination of topical and/or systemic antiinflammatory therapy
Ablative laser
Surgical intervention (eg, dermabrasion or tangential excision)
Topical therapy:
– Ivermectin 10 mg/g – Azelaic acid 150 mg/g – Metronidazole 7,5 mg/g
established rosacea because of its inhibitory effect on sebaceous glands as well as some antiinflammatory capacity.111 This can be also used before laser and dermatosurgery procedures to reduce size and inflammation. It is often recommended to stop isotretinoin before surgery because isotretinoin inhibits keratinocyte-mediated wound healing. However,
1440
no controlled studies exist to inform whether this is also true for low-dose isotretinoin. Rarely, dapsone is used in these cases. For laser treatment options or surgical therapy, including surgery, cryosurgery, radiofrequency ablation, electrosurgery, and thermosurgery, see the later discussion of physical and surgical procedures.
14
ALLOWED NOT ALLOWED
Use powder cosmetics with a matte finish; the best is green (complementary color of red). Use cream or liquid cosmetics.
Try cosmetics before buying them if possible. Use old cosmetics.
Wear light earth tones (tan, peach, matte green) for eye shadow. Wear deep eye shadows (blue, purple, red, or pink).
Apply a separate sunblock after topical medication and before cosmetics. Use moisturizer on dry skin with at least SPF20+. Use cosmetics containing perfume.
Avoid cosmetics using formaldehyde, propylene glycol, alcohol, toners, and palmitic, oleic acid, and other irritants. Purchase cosmetics with more than 10 ingredients.
Use a flat or soft brush applicator without rubbing. Apply with a sponge or fingers. Massage creams into the skin. Use peeling “rejuvenating” agents.
Use facial foundation of power or cream variety with matte finish. Use light-reflective powders containing mica.
Wear only black mascara. Use nail polish.
Use pencil forms of eyeliner. Start applying new medications or cosmetics on weekends or vacations on
Use pencil forms of eyeliner. Start applying new medications or cosmetics on weekends or vacations on one site and take photos to compare sites to reveal potential irritations.
one site and take photos to compare sites to reveal potential irritations.
SPF, sun protection factor.
Waterproof eye cosmetics are best avoided.
Waterproof eye cosmetics are best avoided.
Current pathomechanism-based therapeutic strategies in rosacea
Mast cell mediators (MMPs, cytokines, proteases, amines, cathelicidin)
TLR-2 Serine proteases/ PARs Cathelicidin (AMP)
AZA
Isotretinoin
Doxycycline
IVM
εACA(X1)
Cytokines, chemokines, growth factors, ICAMs, VCAMs, fibrosis, vasodilation, innate immune cells, AMPs (X1)
Cytokines, chemokines, MMPs, neuropeptides, glandular hyperplasia, fibrosis
Various immune cells
Th cell (TIMP)
MNZ, Doxycycline
TCI
Na sulfa
IVM
IVM
AA
Cytokines, chemokines, MMPs, proteases, growth factors
Cytokines, chemokines, growth factors, MMPs, oxidative burst
Cromolyn sodium
εACA
Doxycycline
(Protease inhibitors)
Laser Tx
IVM
IVM (topical)
Cytokines, chemokines, neuropeptides, prostanoids, cell adhesion, growth factors
Cytokines, chemokines, growth factors, fibrosis, oxidative burst
Vascular SMCs/ECs
Variable
α2 AR
Brimonidine
Laser
Oxymetazoline
α1/α2 AR
Betablocker (systemic)
Fibrosis, vasodilation
Vasodilation (NO, PACAP, CGRP, SP)
1441
4
14
METHOD SYMPTOM TO TREAT EVALUATION OR SIDE EFFECTS
Laser therapy
PDL laser Erythema, telangiectatsia Advantage over IPL: more selective treatment of blood vessels More effective than Nd:YAG Purpura induction with short pulse duration Prevention of purpura with longer pulse duration of 40–50 ms Side effects: hyper- or hypopigmentation
PTP laser Telangiectasia (erythema) Short healing process, well tolerated Low risk of scaring Better for treatment of telangiectasia than erythema Good safety and tolerability profile
Nd:YAG laser Erythema, telangiectasia Minor pain sensation Less painful than PDL Combination with PDL possible in therapy-resistant cases Risk for atrophic scars
Light therapy IPL Erythema, teleangiectatsia, papules or pustules Good safety and tolerability profile Time-saving procedure
Surgical intervention Dermabrasion Phymata Risk of bleading
Electrocautery Phymata Rapid procedure Potential side effect: cartilage damage Protracted wound healing disorder Atrophic scaring
Laser (CO2- or Er:YAG laser) Phymata Co2: low risk for bleeding Er:YAG: low scaring risk CO2–Er:YAG combination
Scalpel excision Phymata Risk of intraoperative bleeding Deep tissue excisions or resections Risk: resection of excessive tissue
Scalpel excision Phymata Risk of intraoperative bleeding Deep tissue excisions or resections Risk: resection of excessive tissue
Er:YAG, erbium-doped yttrium aluminium garnet; IPL, intense pulsed light; Nd:YAG, neodymium-doped yttrium aluminum garnet; PDL laser, pulsed-dye laser; PTP, potassium–titanyl–phosphate. Modified from Hofmann MA, Lehmann P. Physical modalities for the treatment of rosacea. J Dtsch Dermatol Ges. 2016;14(Suppl 6):38-43; with permission. Copyright © 2016, John Wiley & Sons.
FACIAL LYMPH EDEMA (MORBIHAN DISEASE)
For facial edema based on lymphatic vessel dilation, no approved or standard therapy exists. Oral isotretinoin, Dapsone, hydroxychloroquine, minocycline, and combined doxycycline–prednisolone have each been tried with mixed results.112-114
OCULAR ROSACEA
Every patient with cutaneous rosacea should be questioned about eye symptoms, such as itchy, dry eyes with a foreign body sensation, and avoidance of light. Bloodshot eyes in combination with a thorough family and skin history is often indicative of the disorder. The management of ocular rosacea has to be defined as a multidisciplinary effort with ophthalmologists and dermatologists involved with or without general practitioners. The severity can range from mild to severe and may lead to chronic defects, even blindness.9,16,22,23
General basic includes is eyelid hygiene (warm compresses, meibomian gland expression, dilute baby
1442
shampoo scrubs, and lubricating drops) and artificial tear substitutes for mild ocular burning or stinging followed by topical and systemic therapy in more severe cases Table 79-19). UV-blocking sunglasses can also be helpful. A proper education about general eye care improves success of treatment (see Table 79-19). In patients with ocular rosacea, screening for cutaneous features is obligatory.
PAIN
See the section on “Erythema and Flushing.”
MAINTENANCE THERAPY
MAINTENANCE THERAPY
Compared with other inflammatory skin diseases, such as atopic dermatitis or psoriasis, the rosacea maintenance therapy regimen is poorly validated and depends on available modalities and the patient’s expectance. In the authors’ experience, maintenance therapy is superior to sudden discontinuation. General skin care should always be continued, as recommended earlier.
THERAPY COMMENT
Artificial tears Frequently needed for “dry eyes” of ocular rosacea; use several times daily
Eyelid and eyelash hygiene Using warm soaks or compresses; can use saline or dilute baby shampoo lavage; overnight creams soften scale and remove plugs from meibomian gland orifices
Expression of meibomian glands
Following hygiene gentle manual massage extrudes thickened, wormlike secretions from glands
Topical antibiotics Effective treatment for infected blepharitis applied twice daily after eyelid hygiene
Topical steroids Fucidic acid; metronidazole, erythromycin, and azelaic acid are main options; topical steroids should be used with caution; 1% hydrocortisone cream for blepharitis; may be used in antibiotic–steroid combination
Tacrolimus– cyclosporine Insufficient evidence to know indications or role in therapy as yet
Systematic antibiotics As used for PPR; minocycline, doxycycline, oxytetracycline, erythromycin commonly used; 6–12 wk of therapy; response begins after 2 wk; metronidazole used rarely; relapse common after course of therapy completed
Surgery Incision and curettage for chalazion after eyelid everted; required for keratitis if impending perforation
Other therapies Topical sulfur, zinc, and ichthammol prepara-
Other therapies Topical sulfur, zinc, and ichthammol preparations; hexachlorocyclohexane; vitamin B2 orally or parentally; omega-3 fatty acid dietary supplementation; topically applied cold tea or tea tree oil
tions; hexachlorocyclohexane; vitamin B2 orally or parentally; omega-3 fatty acid dietary supplementation; topically applied cold tea or tea tree oil
PHYSICAL AND SURGICAL THERAPIES IN ROSACEA
PHYSICAL AND SURGICAL
THERAPIES IN ROSACEA
PHYSICAL METHODS
Physical methods such as light and laser therapies, as well as surgical interventions, are important and adequate additions to the often symptom-oriented topical or oral therapies used for rosacea. In an efficient and mostly long-lasting fashion, they supplement the conservative treatment and general skin care. Because several features coexist in many patients, multimodal therapy is often demanded. In patients with erythema and telangiectasia, for example, a combination of topical vasoconstrictors with light or laser therapy is incremental because telangiectasias do not respond to topical or systemic treatment. An initial medical therapy of erythema can also unmask telangiectasias, which are then easier to approach with physical methods.7,115
14
In general, long-term efficacy and safety data from controlled, blinded trials for many procedures are very sparse. However, repetitions of laser procedures are regarded as safe. In ablative procedures of phymata, the risk for scarring is enhanced compared with nonablative techniques; however, no scientific data exist that would validate this generally accepted observation. For the treatment of erythema and telangiectasia, various light and laser systems exist (see Table 79-18). Laser systems are, for example, the frequency-doubled potassium-titanyl-phosphate laser (PTP; 532 nm), neodymium-doped yttrium aluminum garnet laser (Nd:YAG; 1.064 nm), and pulsed-dye laser (585–595 nm). They act in wavelengths, which are absorbed by hemoglobin and subsequently lead to blood vessel destruction. Light lamps such as intense pulsed lights (spectrum range of 500-1.200 nm) operate using specific filters in the wavelength of hemoglobin absorption. Older laser generations, such as the argon laser, are out of date because the newer generation lasers exert lower adverse event profiles related to dyspigmentation, scaring, pain, and economic downtime.8,116,117
A recent Cochrane review performed a metaanalysis on various laser therapies and concluded for all studies a low to moderate evidence level.118 However, pulsed-dye laser was superior to Nd:YAG laser and comparable to intense pulsed-light laser. Other studies were not comparable.
SURGICAL INTERVENTIONS
Surgical intervention therapies to treat phymata are scalpel excisions, dermabrasion, electrosurgery and CO2- or erbium:YAG laser (see Table 79-18). The classical surgical excision and resection is a rapid option for large phymata, with a relatively high bleeding rate. This risk is lower with electrosurgery, which in contrast has a higher risk of deeper tissue destruction. Dermabrasion can be used in mild as well as severe phymata. A good option is also the CO2 laser, which has a relatively lower risk of bleeding.8
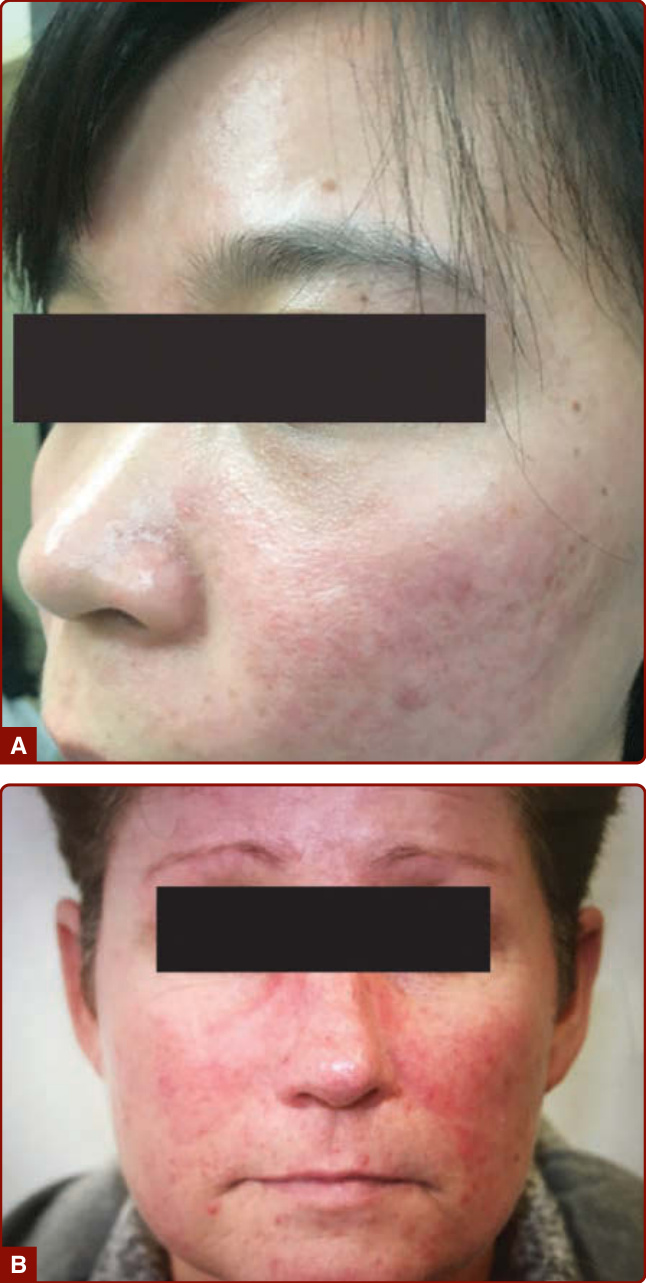
Figure 79-1 A, Persistent erythema in patients with rosacea. B, Although mostly symmetrical, persistent erythema can present with asymmetrical distribution and intensity based on underlying trigger factor. (Image A, used with permission from Professors H. Xie and J. Li, University Hospital Changsha, China.)

Figure 79-2 Phymata in patients with rosacea. A, In the initial stages, rhinophyma is often apparent only at the distal end of the nose as dilated patulous follicles or plaque. B, Marked rhinophyma. C, Asymmetric fibrous form of rhinophyma with asymmetrical clinical appearance. D, Mild gnathophyma. E, Metrophyma in combination with granulomatous plaques on the cheeks. F, Blepharophyma. (Image A, used with permission from Professors H. Xie and J. Li, University Hospital Changsha, China. Image F, used with permission from James E. Fitzpatrick.)
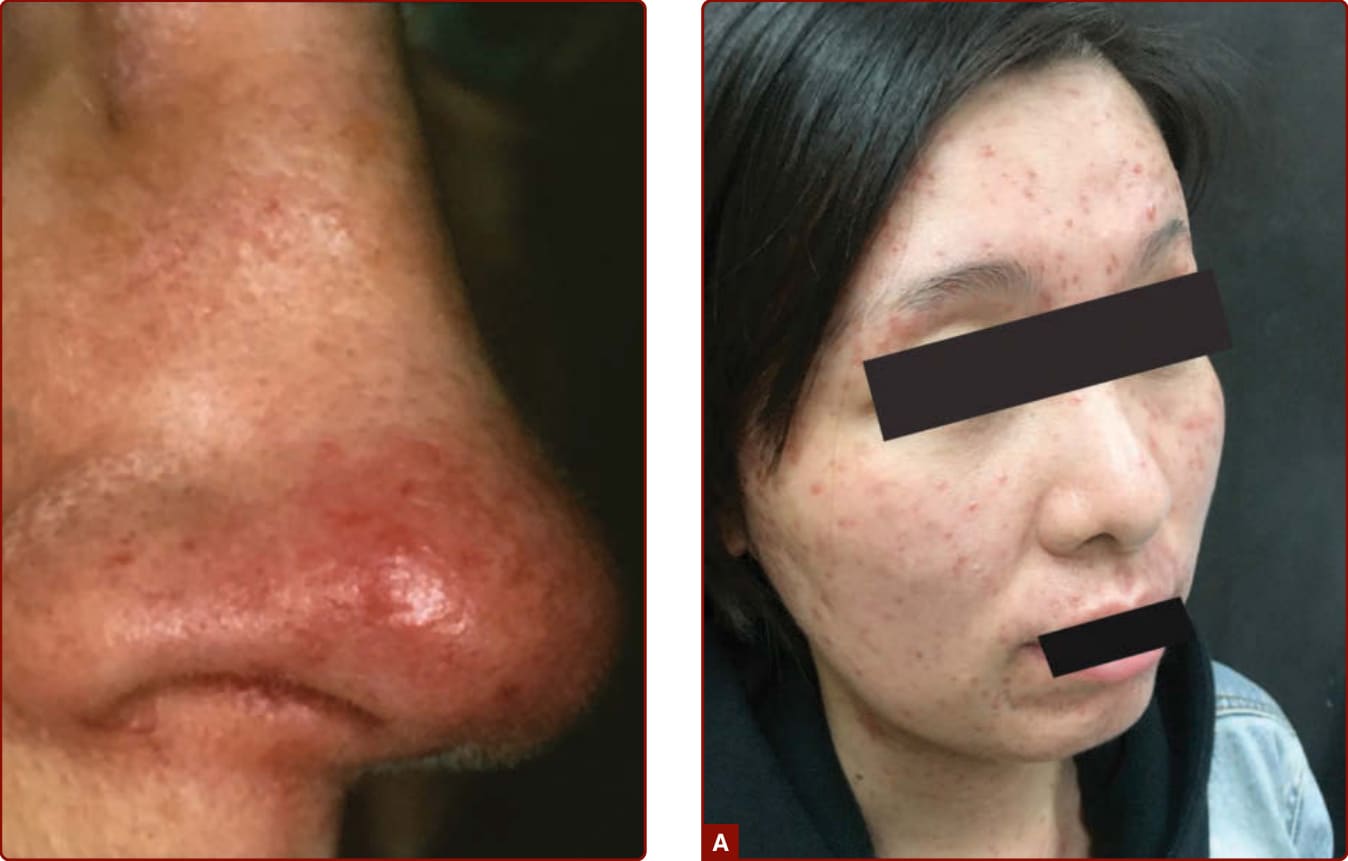
Figure 79-3 Telangiectasia in a patient with rosacea.

Figure 79-4 Individual with rosacea with mild chronic facial erythema and disseminated facial papules and pustules (A). Papules and pustules can develop extrafacially, mostly on the neck, trunk, or bald scalp, indicating ultraviolet light as a trigger factor on bald scalp rosacea (B). (Image A, used with permission from Professors H. Xie and J. Li, University Hospital Changsha, China.)

Figure 79-5 Ocular rosacea may affect many compartments of the eyes. Ophthalmology referral is advised, and systemic therapy is recommended in most cases.

Figure 79-6 Conglobate form of rosacea, which can clinically resemble conglobate form of acne but occurs predominantly in older age groups more often than acne.

Figure 79-7 Steroid rosacea. A, An adult patient with primarily telangiectatic rosacea with rare acneiform papules that was the result of prolonged use of topical glucocorticosteroid (Valisone), which may increase colonization of Demodex mites because of immunosuppression. (From the Fitzsimons Army Medical Center Teaching Files.) B, A pediatric patient with steroid rosacea. (Used with permission from the William Weston Collection.)

Figure 79-8 Morbihan disease. An adult patient with non to mild erythematous cushionlike edema of the lower eyelids. It may include the forehead, nose, glabella, and central cheeks. It can occur in men and women.
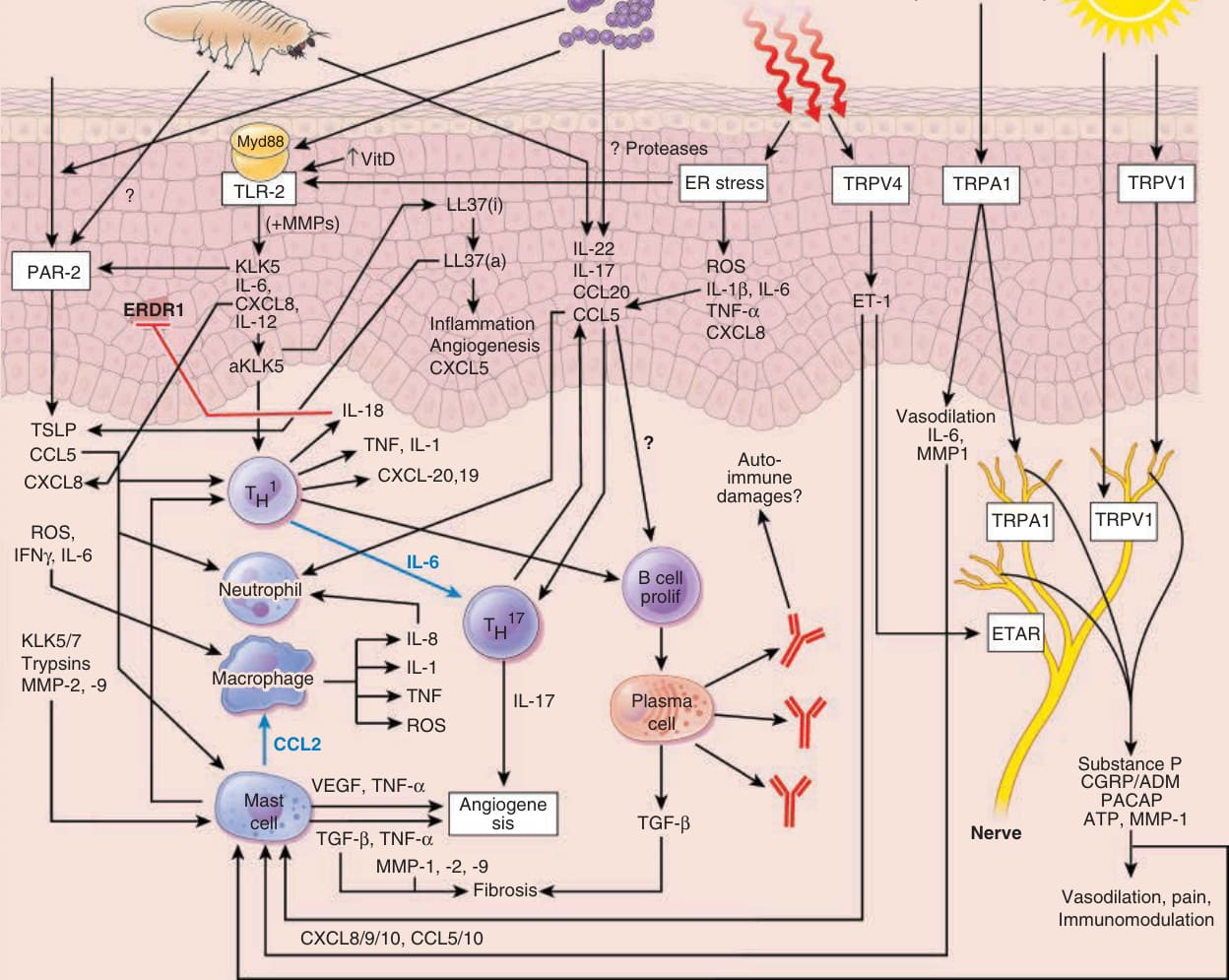
Figure 79-9 Dysregulation of innate and adaptive immune system in rosacea. Environmental triggers are shown at the top of the figure, with their known or assumed downstream signaling effects shown below. Protease-activated receptor-2 (PAR-2) not only induces neuroinflammation or pain but also stimulates release of cytokines such as interleukin (IL)-1, tumor necrosis factor (TNF), IL-6, IL-8, thymic stromal lymphopoietin (TSLP), chemokines, matrix metalloproteinases (MMPs), and prostaglandins; recruits neutrophils and T cells or macrophages to the site of inflammation; and induces mast cell release. Because PAR-2 is expressed by keratinocytes, endothelial cells, mast cells, macrophages, and neutrophils; is regulated by microbial products; and interacts with TLRs, a role of serine proteases and PARs in rosacea innate immune responses can be assumed.119-124 Cytokine expression profiles of all skin rosacea phenotypes demonstrate elevation of the cytokine interferon (IFN)-γ,20 which can be produced by type 1 helper T cells and natural killer cells, and because IFN-γ is a potent activator of macrophages, this is likely a close communication of the adaptive and innate immune networks in rosacea. TLR-2 is known to increase the expression of the serine protease KLK-5.125 Notably, the lesional skin of patients with rosacea was shown to express more KLK-5 than the skin of healthy control participants.40 In addition, Yamasaki and coworkers41 revealed that the increased capacity for releasing KLK-5 is calcium dependent; the ligand for TLR-2 triggers an influx of calcium, which in turn induces the increased release of KLK-5. In this process, calcium functions as the stimulus for transcription of KLK-5, with TLR-2 regulating the functional release of KLK-5.41 Via KLK-5, TLR-2 induces upregulation and activation of the innate immune peptide human cathelicidin (the active form of which is LL-37),41 leading to erythema, immune response, and angiogenesis through release of serine proteases, MMPs, cytokines, chemokines, and proliferation of endothelial cells.40,41,73,74,126 KLK-5 protein activity can also be regulated by serine protease inhibitors of Kazal-type (SPINKs).72 Among these, SPINK6 was identified in human skin as a specific inhibitor of KLKs.72 However, its putative role in rosacea should be further explored. KLK-5 is also mediated by MMPs. Specifically, the activation of KLK-5 occurs after the cleavage of its proenzyme form by MMP-9.72 Notably, enhanced expression of MMP-2 and MMP-9 was observed in the skin of patients with rosacea.127 Such increased expression of MMPs has potential implications for the solarmediated degeneration that is observed in rosacea.128 In addition, MMP-mediated initiation of KLK-5 activation leads to further activation of LL-37, the processed form of cathelicidin. Increased expression of transient receptor potential (TRP) channels of the vanilloid subfamily (TRPV1–4) was found in lesional skin of rosacea patients.51 TRP channels are widely acknowledged as polymodal sensors of environmental and endogenous irritative signals and can be activated by typical rosacea triggers (eg, heat, ultraviolet B, temperature changes, pungent compounds from vegetable and spices, alcohol, mechanical stimuli, irritants). Activation of TRPs increases intracellular calcium concentrations
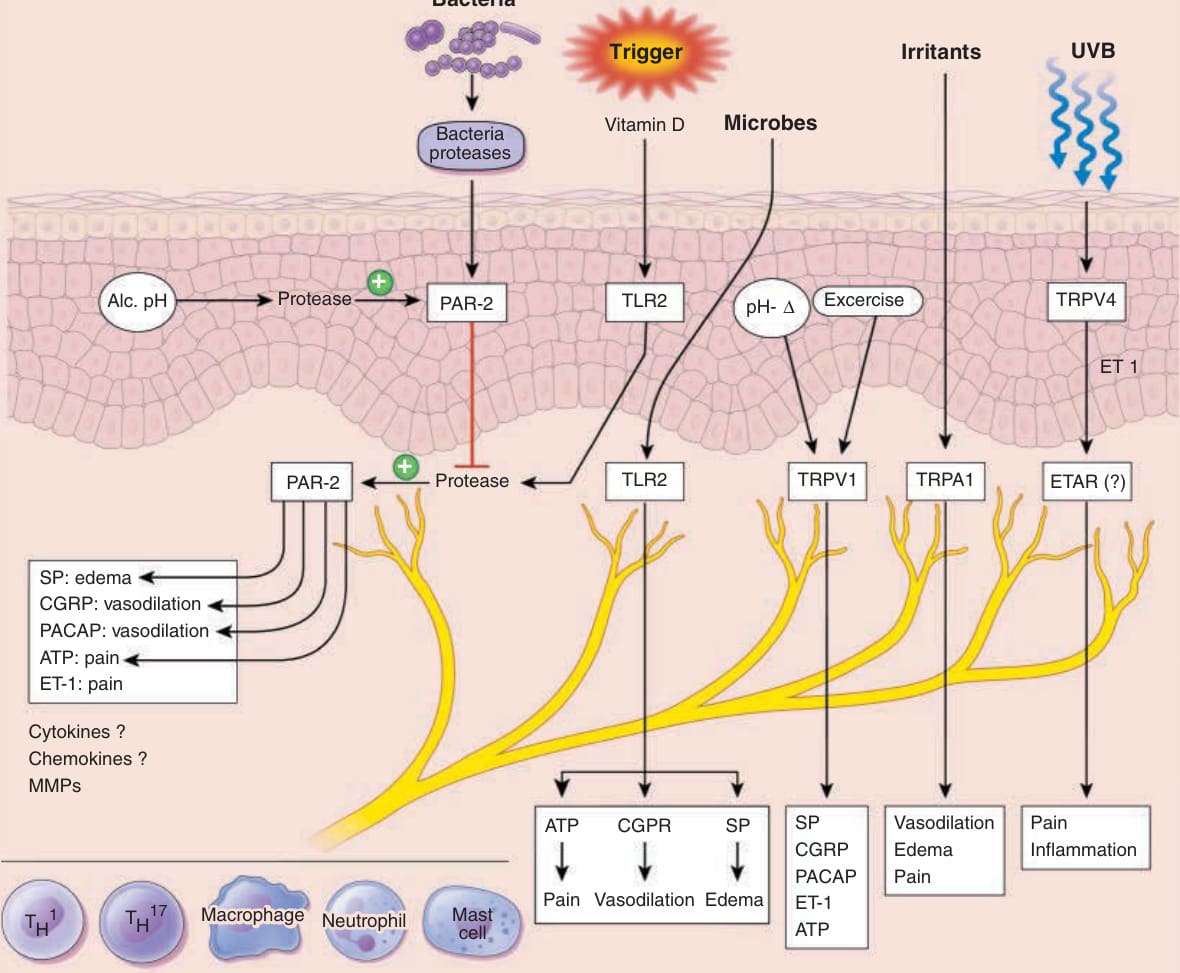
Figure 79-10 Neurovascular communication in rosacea. Notably, a polymorphism in the TAC3 gene has been identified in rosacea, which encodes for neurokinin receptor-3 and induces neuroinflammation, pain, and immune responses in various tissues. Thus, overstimulation of neurokinin receptor-3 may contribute to neurovascular and neuroimmune changes in rosacea through substance P and other tachykinins.129 Activation of neuronal transient receptor potential (TRP) ion channels through rosacea trigger factors can lead to release of vasoactive neuropeptides (eg, pituitary adenylate cyclase activating peptide [PACAP], substance P [SP], and calcitonin gene-related peptide [CGRP]),91 which are involved in rosacea-associated vasodilation,90 plasma extravasation, and leukocyte recruitment, also via induction of mast cell degranulation.5 SP-positive nerve fibers are enhanced in patients with rosacea. Also, PACAP-positive nerves are anatomically closely associated with mast cells that release a number of vasoactive mediators.65 Finally, agonist and one of the receptors for CGRP are increased at mRNA levels in patients with rosacea.98 Because TRP channels can cross-talk with neuropeptide receptors, the interaction of both receptors may be involved in sustaining neurovascular responses and inflammation in rosacea, particularly TRP ankyrin type 1 (TRPA1) and TRP vanilloid type 1 (TRPV1).1,51
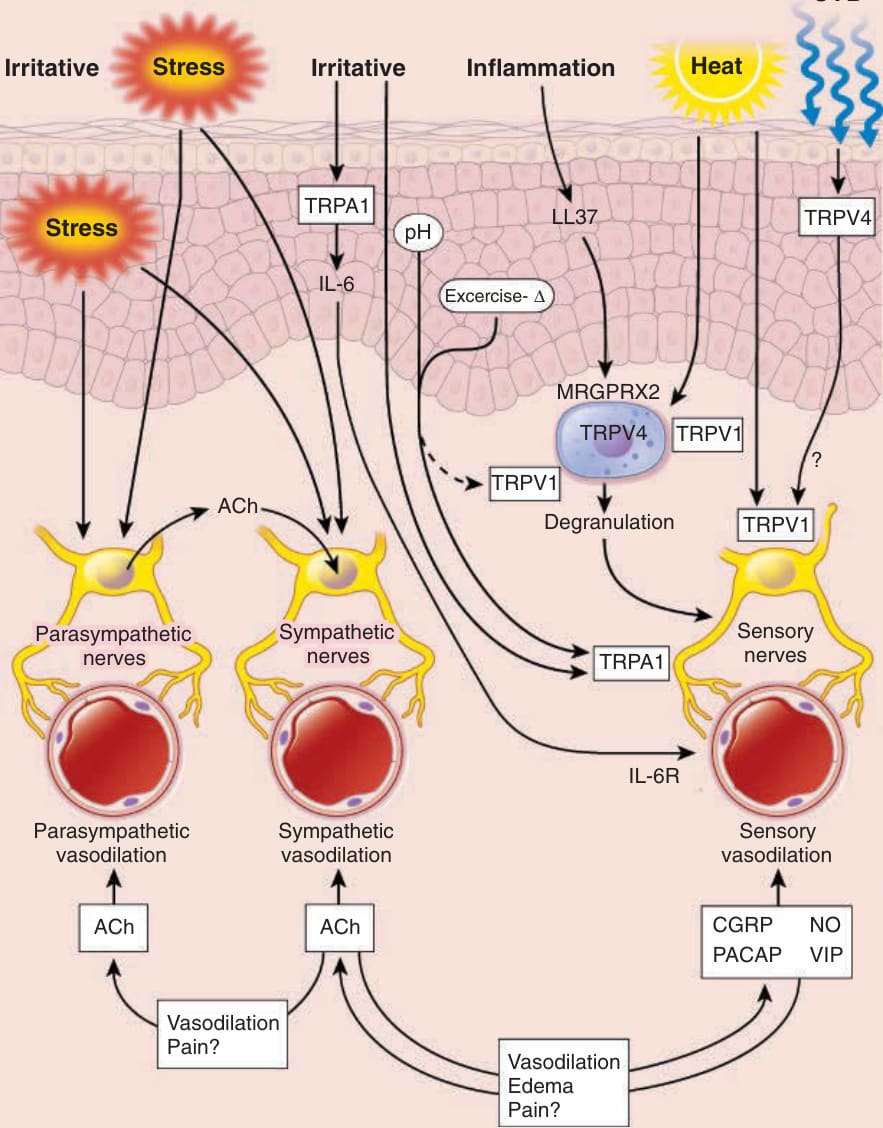
Figure 79-11 Potential pathomechanism of facial flushing in rosacea. Flushing involves an immediate (in contrast to persistent erythema) reactive vascular response to various “irritative” stimuli (within seconds to minutes), induced by trigger factors (eg, spicy food, certain alcohols [Alc], ultraviolet [UV] B, heat, noxious cold, exercising, or stressful emotional stimuli; top of the figure). Most of the trigger factors capably activate transient receptor potential (TRP) ion channels (eg, TRP vanilloid type 1 [TRPV1], TRP ankyrin type 1 [TRPA1], TRP vanilloid type 4 [TRPV4]) on keratinocytes, immune cells, or sensory nerves to induce neurogenic inflammation through release of neuropeptides such as substance P, calcitonin generelated peptide (CGRP), adrenomedullin (ADM), pituitary adenylate cyclase activating peptide (PACAP), or vasointestinal peptide (VIP) from sensory nerves. Neuropeptide release from sensory nerves is either directly facilitated by the irritant stimulus or established via intermediate signals derived from keratinocytes (eg, interleukin [IL]-6), endothelial cells (eg, tumor necrosis factor [TNF]-α, IL-1), or immune cells (eg, mast cells). Neuropeptides are potent inducers of vasodilation, the basis of flushing and erythema, plasma extravasation (leading to edema), and pain. In addition, stressful stimuli also hyperstimulate the autonomic nervous system, especially sympathetic and parasympathetic vasodilator fibers, thereby regulating release of acetylcholine (ACh), for example, a potent vasoregulator and immunomodulator. NO, nitric oxide.
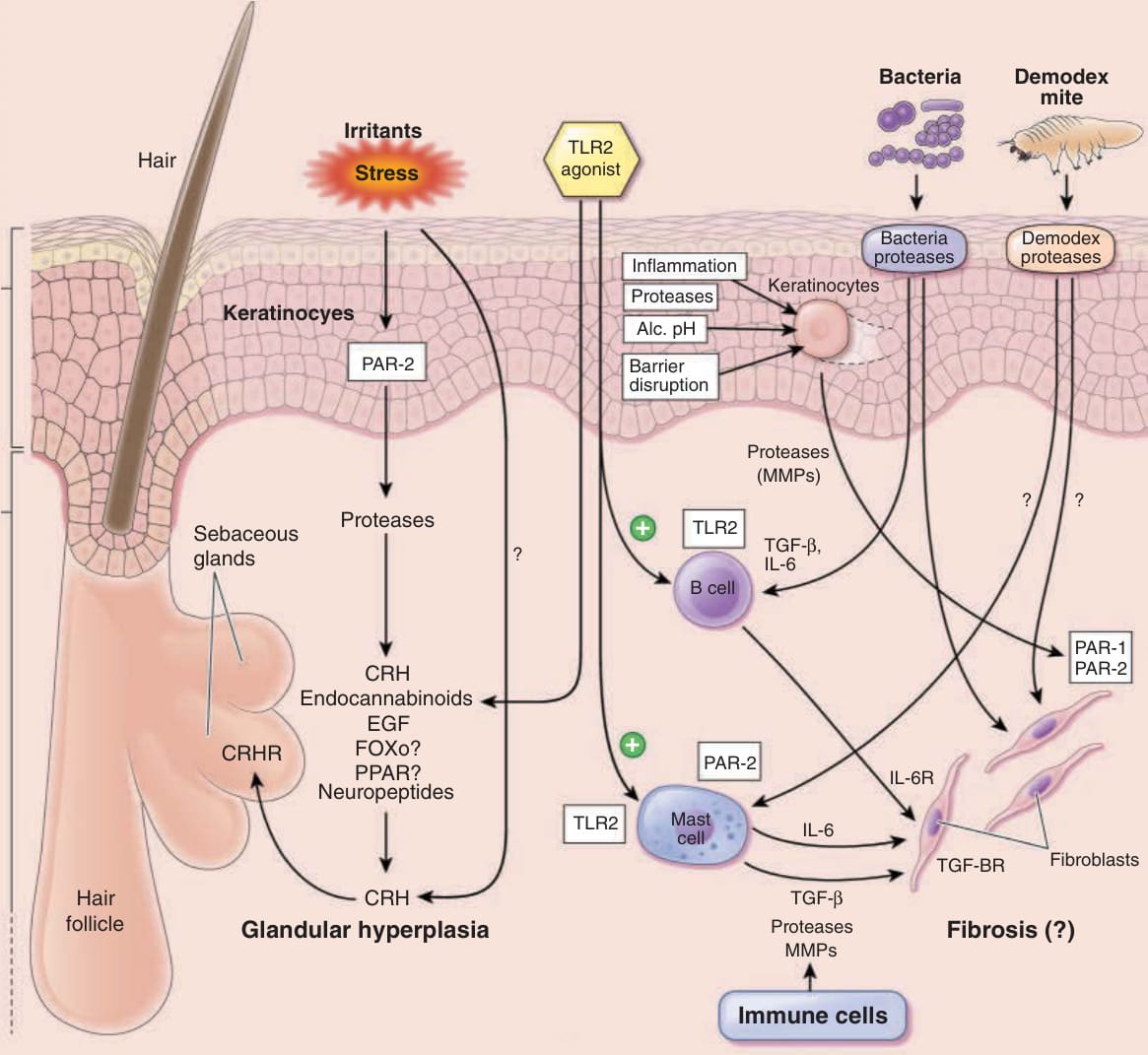
Figure 79-12 Pathomechanism and current therapy strategies for fibrosis and glandular hyperplasia in rosacea. Phymata are verrucous nodules and plaques based on glandular hyperplasia of sebaceous glands and fibroblast activation. They develop through either clinically visible chronic inflammation (chronic erythema, papules or pustules) or sometimes clinically unremarkable skin (subclinical phyma). In any case, they develop because of persistent inflammatory processes accompanied by edema. Histopathologically, phymata are characterized by a perivascular lymphocytic infiltrate, enlarged sebaceous glands and follicles, dilated vessels, remodeled myofibroblasts, and fibrosis. The dysregulated inflammatory process can be triggered by multiple exogenous and endogenous factors. Cell wall components are recognized by Toll-like receptor 2 (TLR2, CD282) leading to the activation of the innate immune system in form of macrophages and mast cell activation or adaptive immune cells (eg, B cells), which readily release a cocktail of profibrotic mediators (eg, interleukin [IL]-6, IL-4, transforming growth factor [TGF]-β, platelet-derived growth factor [PDGF]) that remodel and activate dermal fibroblasts to deposit excessive amounts of extracellular matrix, a hallmark of fibrosis. Demodex or bacterial-derived proteases or endogenous proteases (eg, kallikreins, matrix metalloproteinases) can engage in this fibrotic process by activating resident skin cell- (eg, keratinocytes, fibroblasts) and immune cells (eg, mast cells, macrophages) through cytokine receptors (IL-4, IL-6) growth factor receptors (eg, TGF-β, PDGF), protease-activated receptor-2 (PAR-2) or TLRs. Low pH and barrier disruption additionally activate keratinocytes to release profibrotic proteases that can target fibroblastderived PAR-2. The precise pathomechanism of sebaceous glandular hyperplasia is far from being understood. An important signaling network appears to be triggered by stress that probably activates keratinocytic PAR-2, causing protease release, and might interfere with the corticotropin-releasing hormone and cannabinoid system, the modulation of epidermal growth factor (EGF) and neuropeptide abundance and peroxisome proliferator-activated receptor gamma (PPARγ) activation. Each target is involved in the regulation of lipid and glucose metabolism, cell proliferation and differentiation, or inflammation that fundamentally regulate sebogenesis, sebaceous gland proliferation, and consequently glandular hyperplasia. Alc, alcohol; CRH, cortisol-releasing hormone; MMP, matrix metalloproteinase.
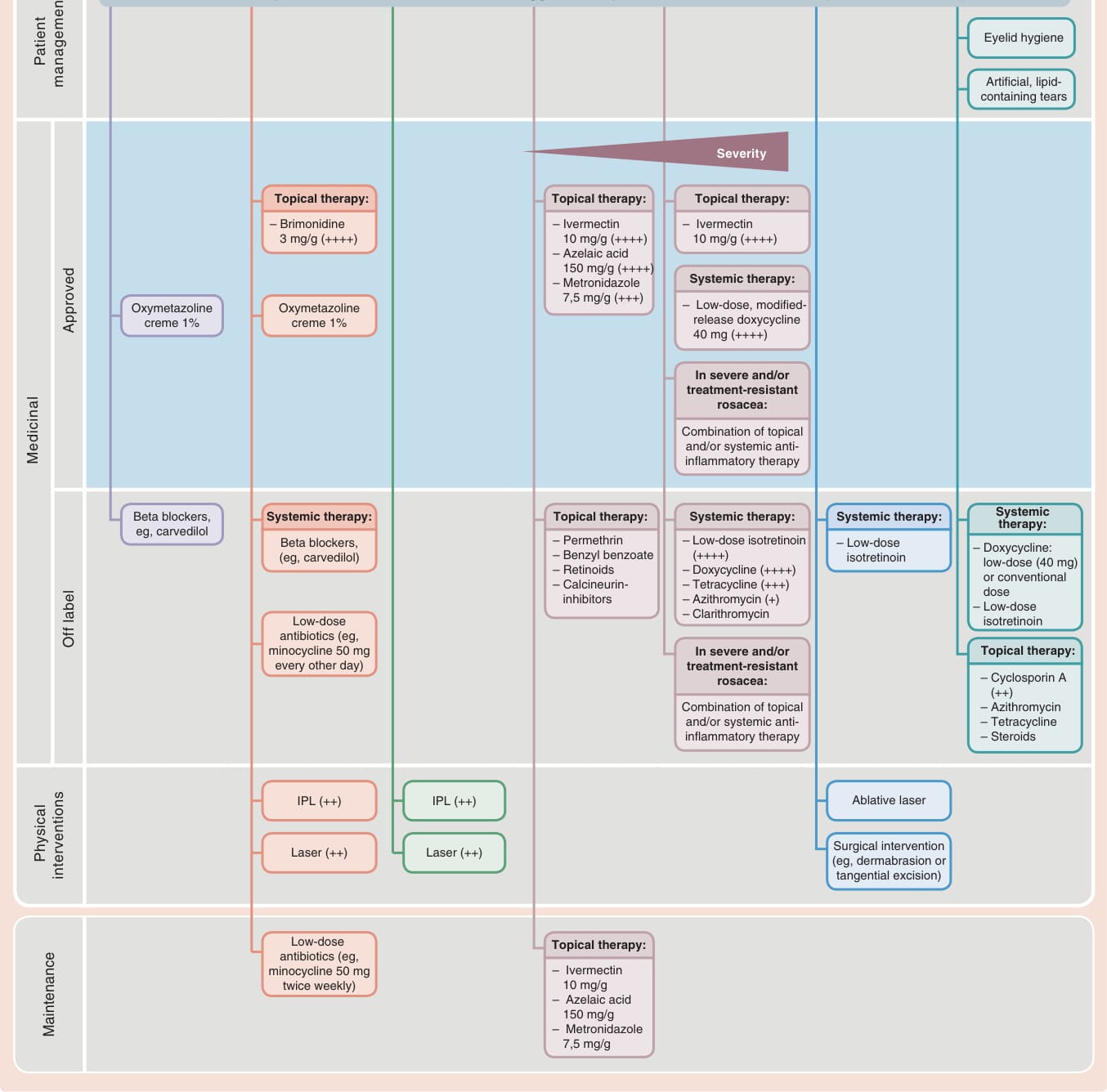
Figure 79-13 Symptom manifestation-dependent therapy regimen in rosacea. IPL, intense pulsed light. (Modified from Schaller M, Schöfer H, Homey B, et al. Rosacea management: update on general measures and topical treatment options. J Dtsch Dermatol Ges. 2016;14(Suppl 6):17-27; with permission. Copyright © 2016, John Wiley & Sons.)
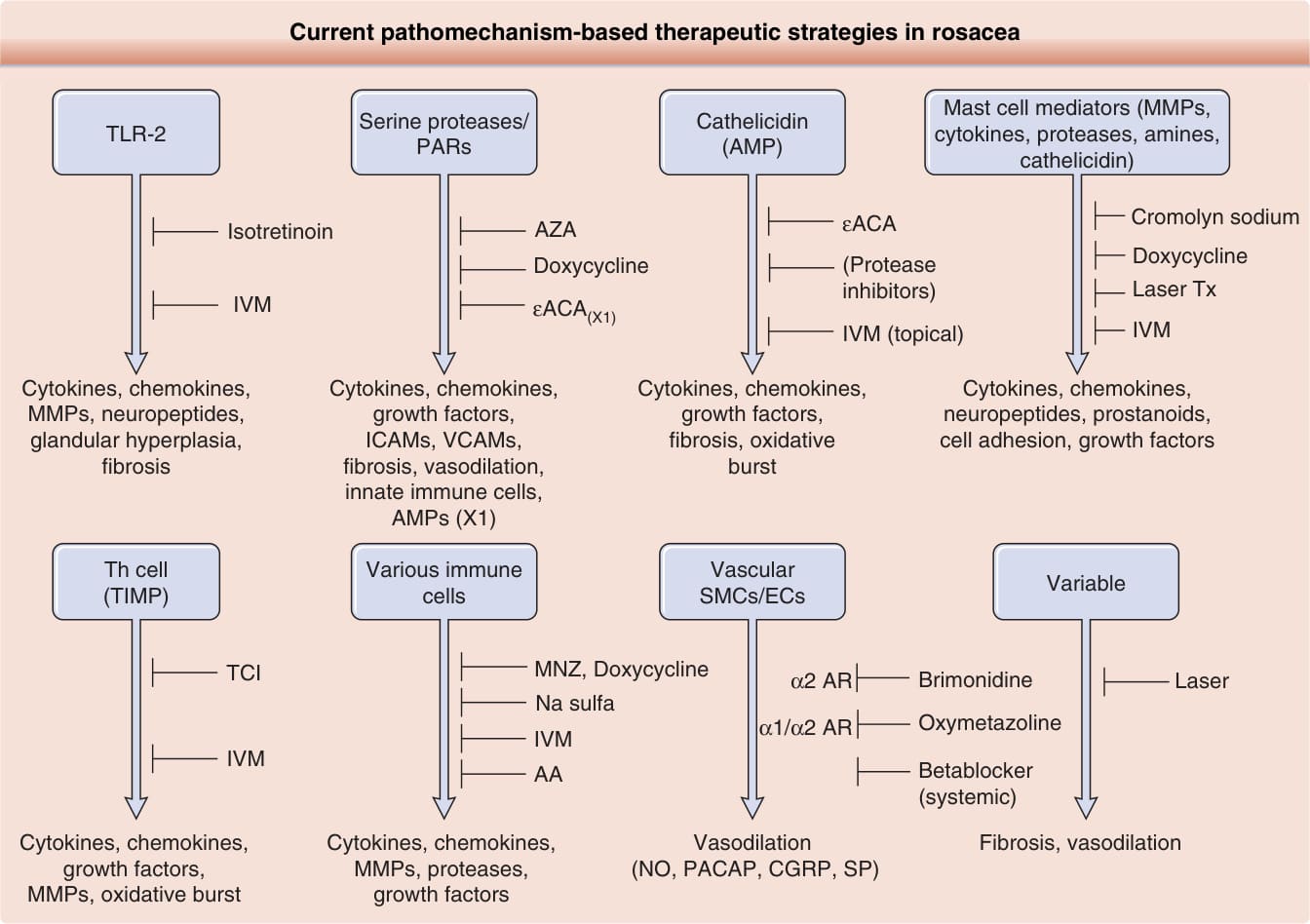
Figure 79-14 Current pathomechanism-based therapeutic strategies in rosacea. AA, azelaic acid; AMP, antimicrobial peptide; AZA, azathioprine; εACA, ε-aminocaproic acid; AR, adrenergic receptor; CGRP, calcitonin gene-related peptide; ECs, endothelial cells; ICAM, intercellular adhesion molecule; IVM, ivermectin; MMP, matrix metalloproteinase; MNZ, minocycline; NO, nitric oxide; PACAP, pituitary adenylate cyclase-activating peptide; PAR, protease-activated receptor; SMC, smooth muscle cell; SP, substance P; TCI, T cell inhibitor; TIMP, tissue inhibitor of metalloproteinases; Th, T helper; TLR, Toll-like receptor; Tx, treatment; VCAM, vascular cell adhesion protein.
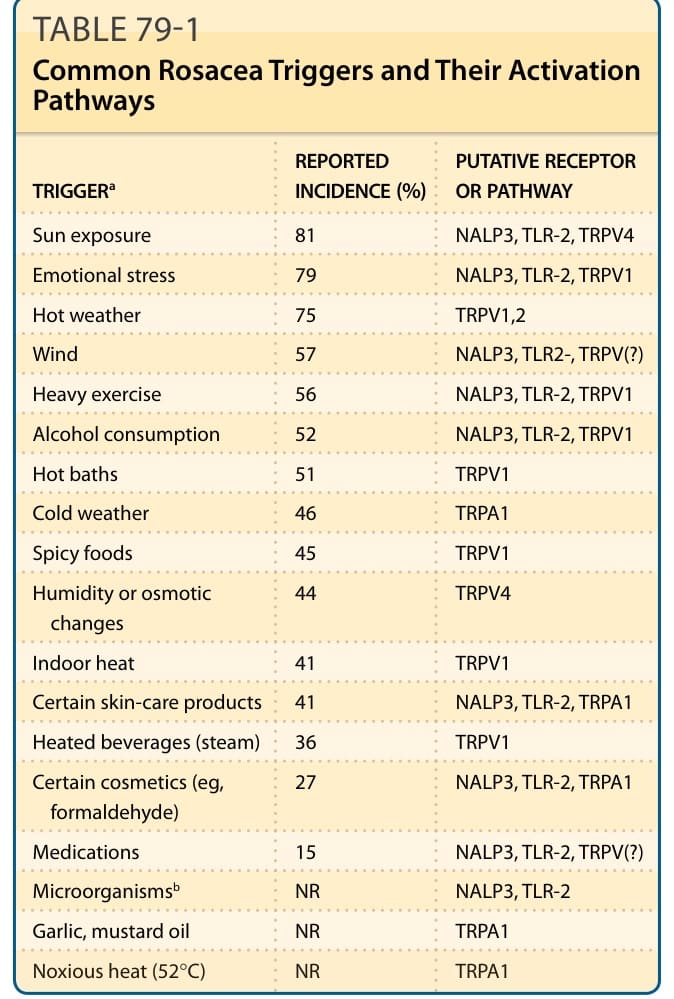
TABLE 79-1 Common Rosacea Triggers and Their Activation Pathways
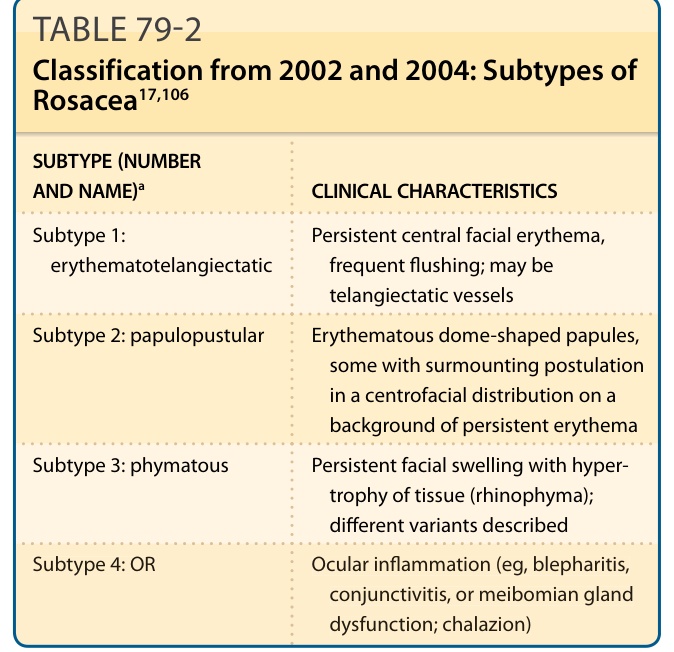
TABLE 79-2 Classification from 2002 and 2004: Subtypes of Rosacea17,106
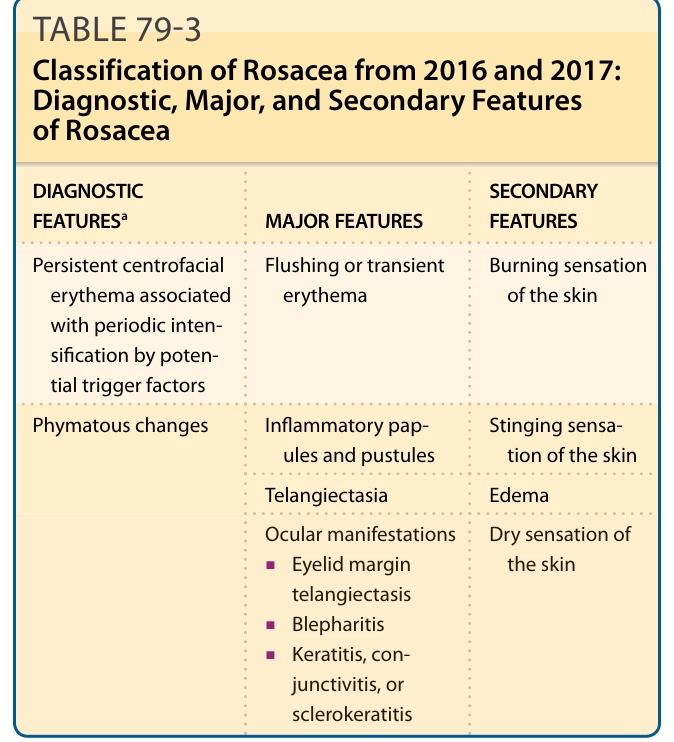
TABLE 79-3 Classification of Rosacea from 2016 and 2017: Diagnostic, Major, and Secondary Features of Rosacea
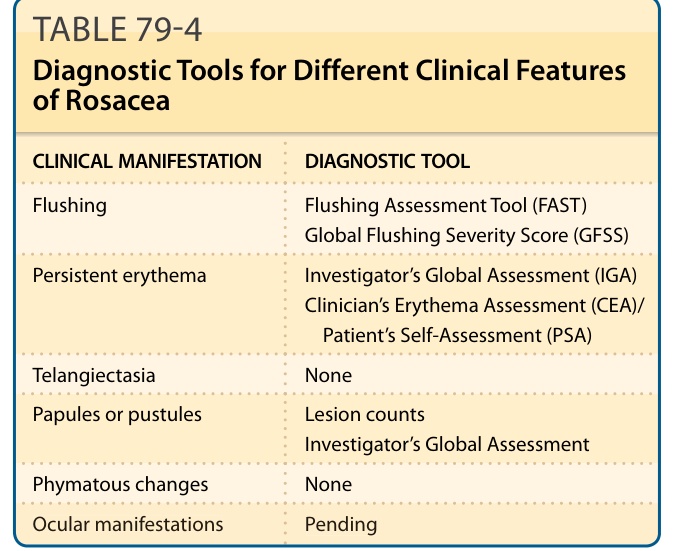
TABLE 79-4 Diagnostic Tools for Different Clinical Features of Rosacea
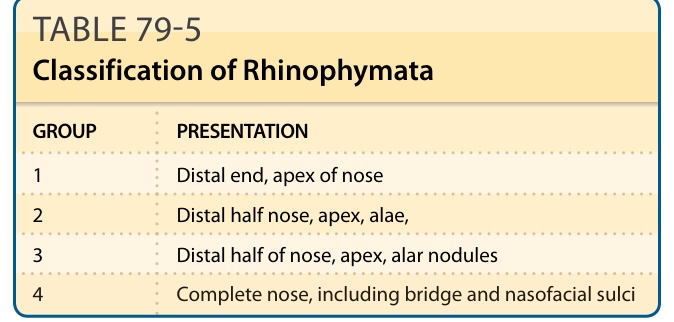
TABLE 79-5 Classification of Rhinophymata
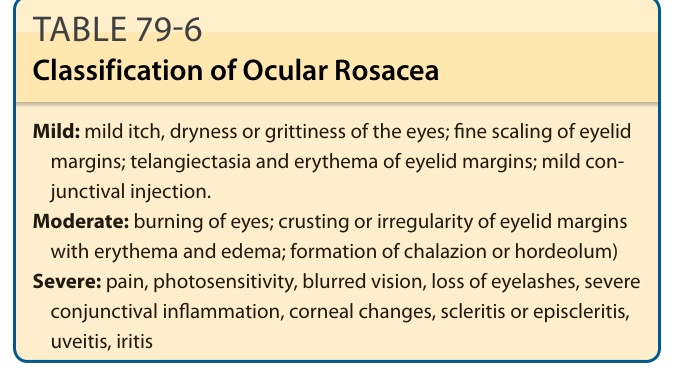
TABLE 79-6 Classification of Ocular Rosacea
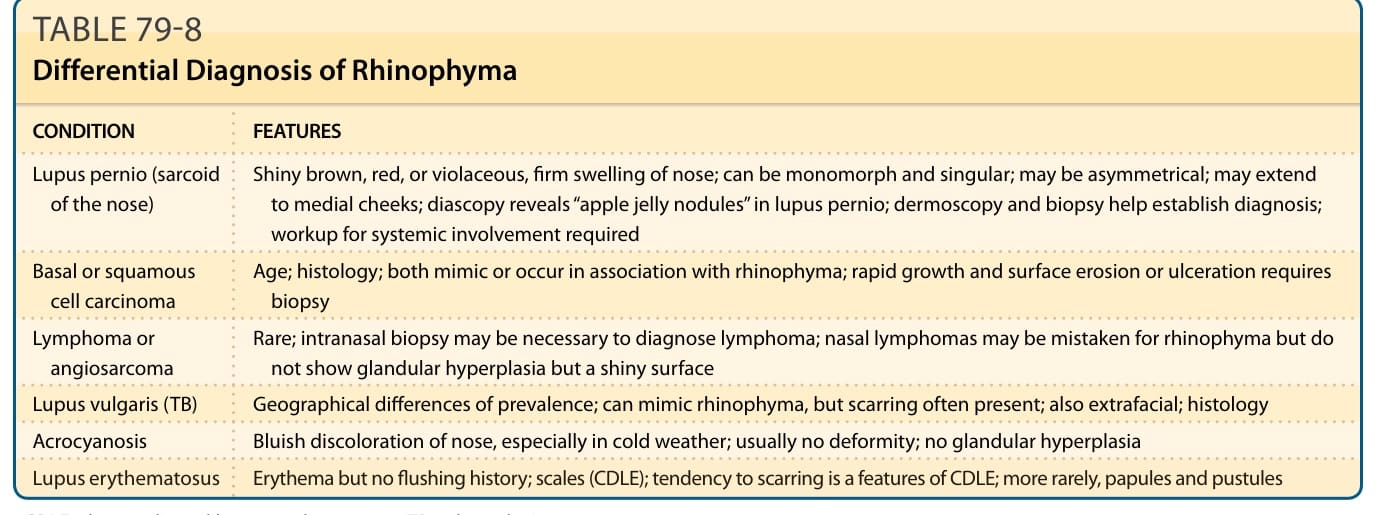
TABLE 79-8 Differential Diagnosis of Rhinophyma
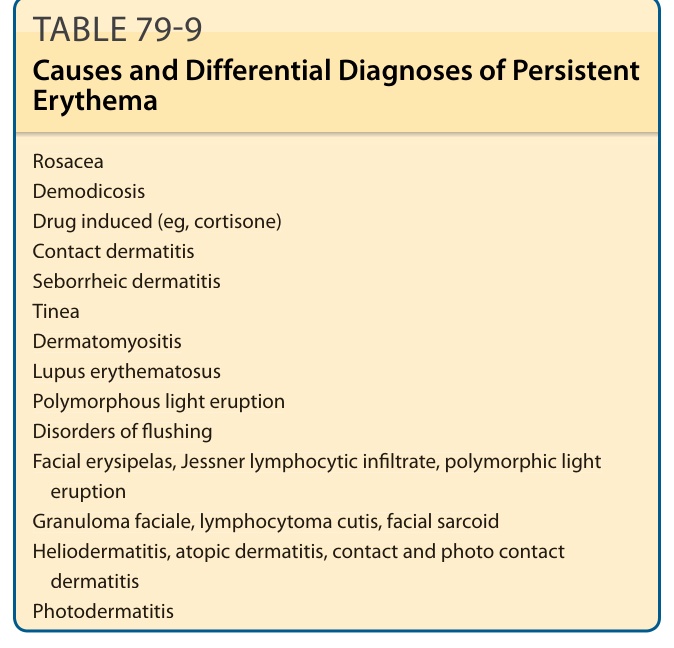
TABLE 79-9 Causes and Differential Diagnoses of Persistent Erythema
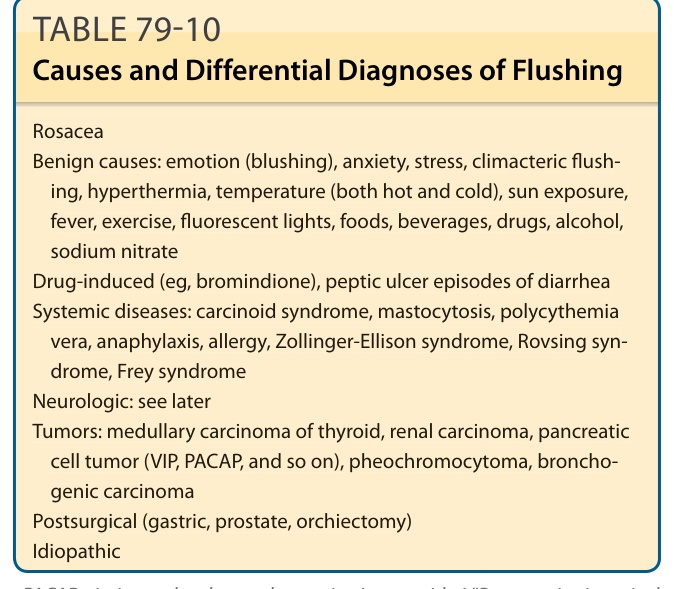
TABLE 79-10 Causes and Differential Diagnoses of Flushing
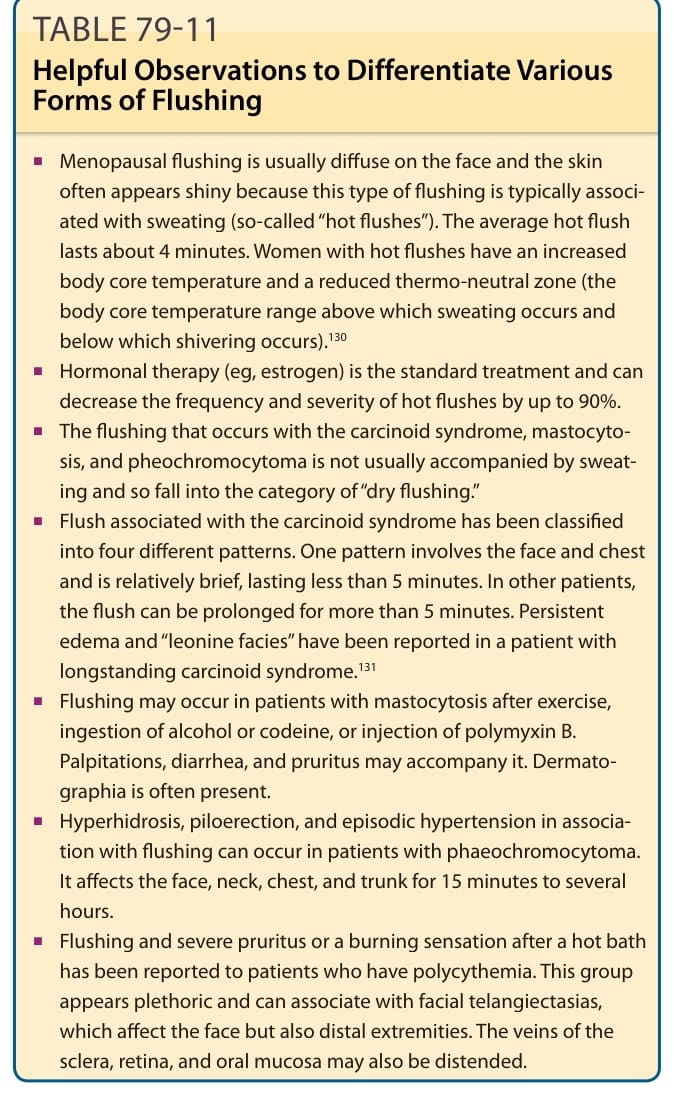
TABLE 79-11 Helpful Observations to Differentiate Various Forms of Flushing
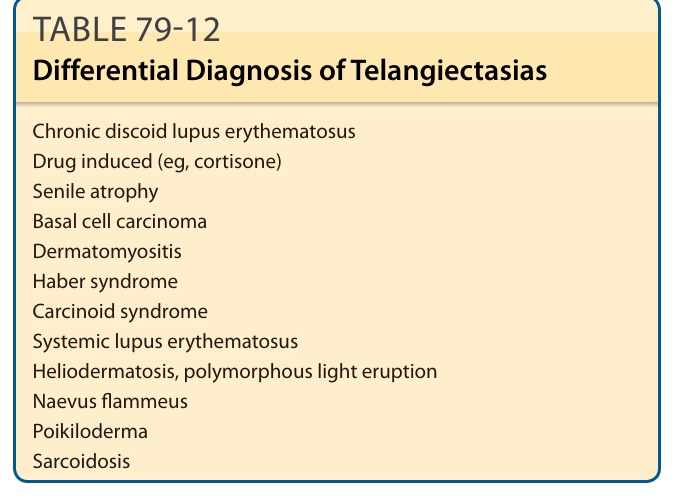
TABLE 79-12 Differential Diagnosis of Telangiectasias
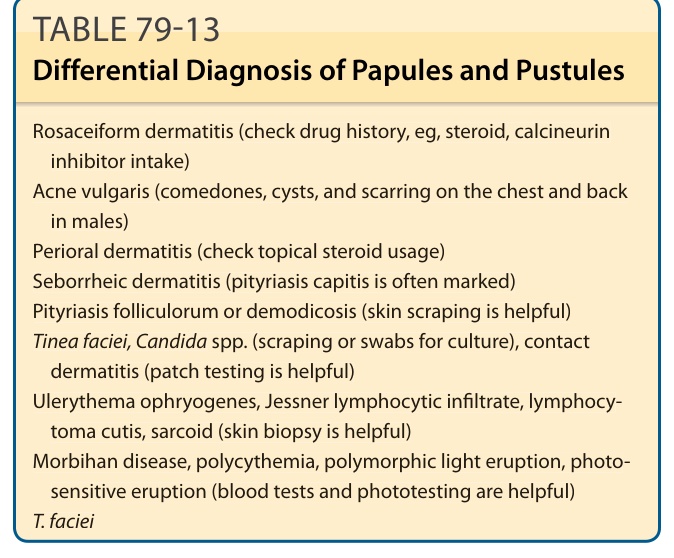
TABLE 79-13 Differential Diagnosis of Papules and Pustules
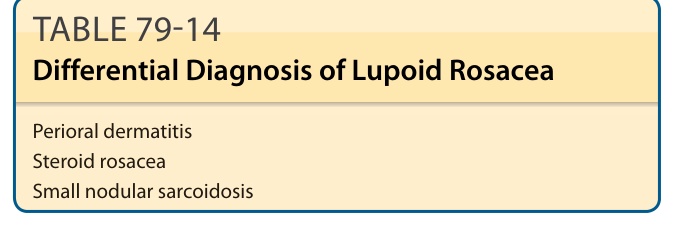
TABLE 79-14 Differential Diagnosis of Lupoid Rosacea
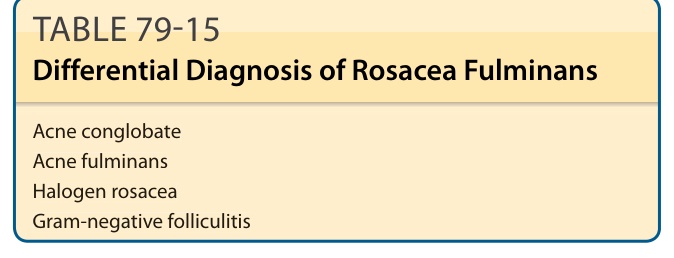
TABLE 79-15 Differential Diagnosis of Rosacea Fulminans
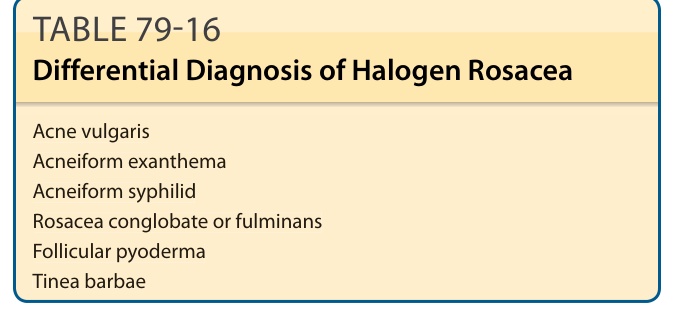
TABLE 79-16 Differential Diagnosis of Halogen Rosacea
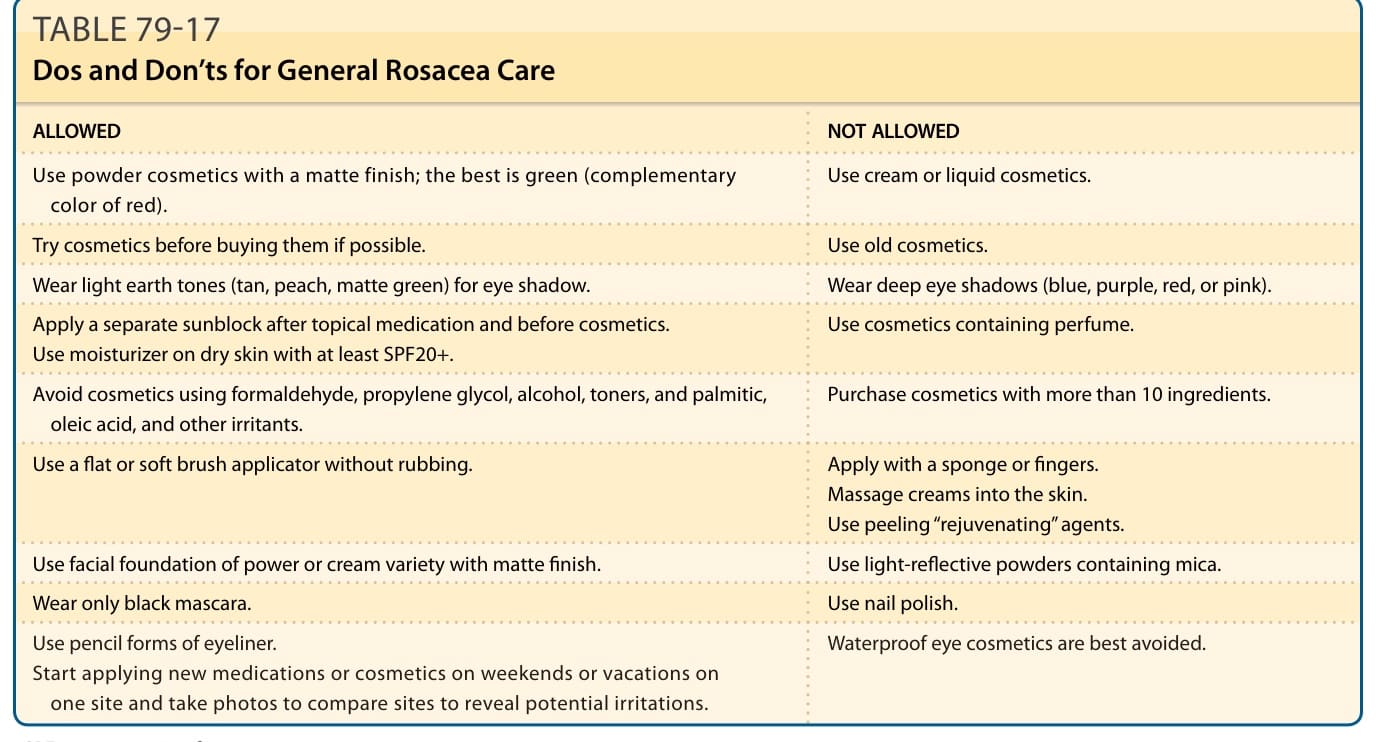
TABLE 79-17 Dos and Don’ts for General Rosacea Care
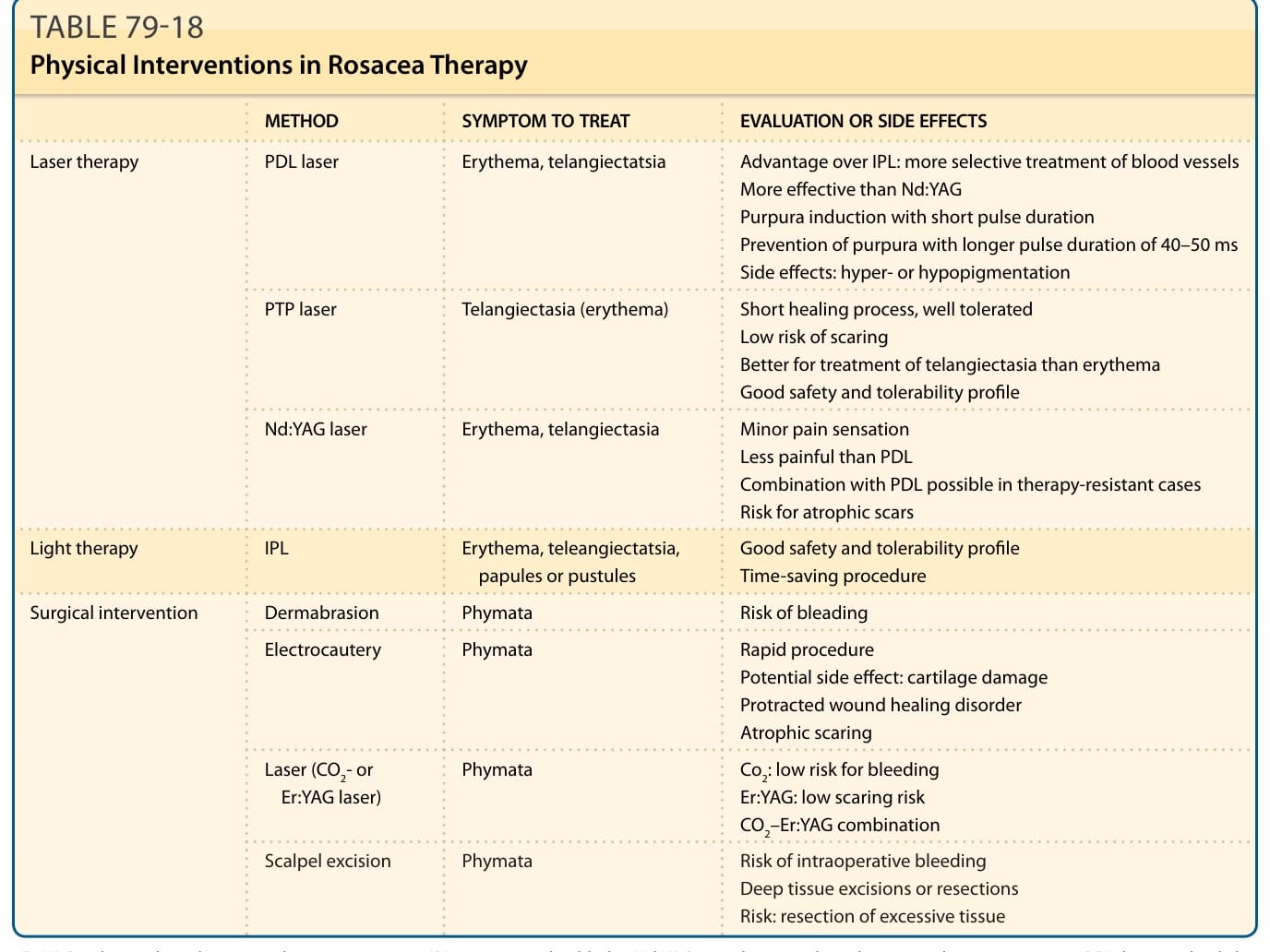
TABLE 79-18 Physical Interventions in Rosacea Therapy
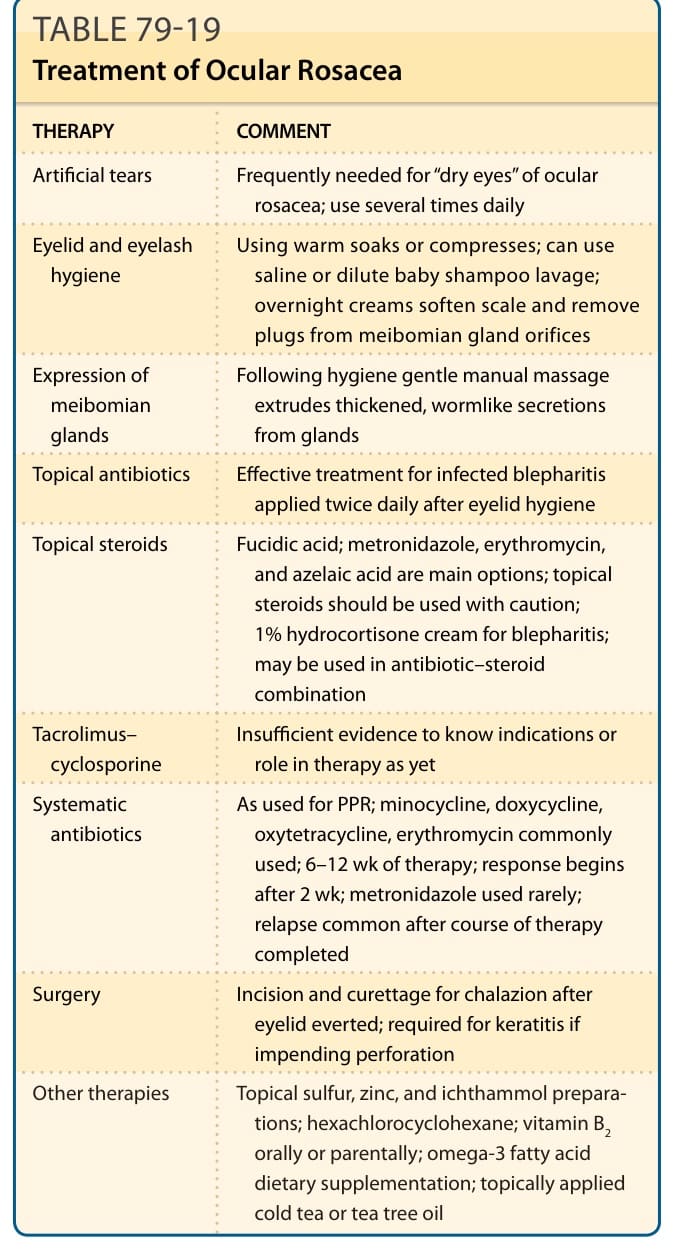
TABLE 79-19 Treatment of Ocular Rosacea