Vitiligo
13
AT-A-GLANCE
■ Vitiligo is a common autoimmune disease of the skin that causes depigmentation through T-cell– mediated destruction of melanocytes.
■ Pathogenesis is multifactorial, including genetic predisposition, autoimmunity, and environmental factors.
■ Vitiligo can cause significant social stigma, with serious implications for mental health.
■ Correlates with increased risk of other autoimmune diseases, but decreased risk of skin cancer.
■ Clinical signs of lesional activity include confetti, trichrome, and inflammatory lesions, as well as koebnerization.
■ Reversible with treatment, but only in areas with normally pigmented hair.
■ Effective treatments include topical and oral immunosuppressants, phototherapy, and chemical depigmenting agents.
■ Emerging treatments include targeted immunotherapy and melanocyte-stimulating hormones.
DEFINITION AND HISTORY
Vitiligo, an acquired skin disease of progressive melanocyte loss, is clinically characterized by well-defined milky-white macules that may also include white hairs, or poliosis. The term vitiligo initially appears in the first century, although clinical features consistent with vitiligo were described in ancient medical texts during the second millennium before Christ.1-3 Historically, vitiligo has been confused with leprosy, an infectious disease of the skin that results in ill-defined hypopigmentation. Some texts sought to differentiate the 2 diseases, while others conflated them. As early as 1500 bc, the Ebers Papyrus listed 2 diseases that affected skin color—one associated with “swellings,” which may have been leprosy, and another that exclusively affected the color, which was likely vitiligo. In the book of “Leviticus” in the Bible, also dated between 1500 and 1400 bc, a number of skin diseases could make one “unclean” and required examination by the priest to determine whether isolation was warranted. Skin swelling, lightening, poliosis, and evolution of lesions over time were assessed to make this determination. This protocol may have been designed to distinguish vitiligo from leprosy or other skin diseases. In India, vitiligo was described in the Atharva Veda (1400 bc) and the Buddhist Vinay Pitak (224 to 544 bc) under the term
“Kilas,” a Sanskrit word “derived from kil,” meaning white.3-5 Hippocrates (460 to 355 bc) did not discriminate between vitiligo and leprosy. In fact, he included lichenoid eruptions, leprosy, psoriasis, and vitiligo under the same category. Still, today, in geographic areas with high incidence of leprosy, the 2 diseases are often confused.
EPIDEMIOLOGY
PREVALENCE
PREVALENCE
There have been very few studies conducted in the general population that aim to determine the prevalence of vitiligo. This is a difficult task, because unlike other diseases that cause significant morbidity and mortality, affected patients may not present to a medical facility to be counted. Thus, most estimates of prevalence are based on prospective surveys, retrospective observational studies, and prospective studies in selected populations, which may underestimate or overestimate the prevalence, depending on the approach. The largest epidemiologic study was performed in 1977 in Denmark, on the island of Bornholm, with a calculated prevalence of 0.38%.6 A study in black people from the French West Indies found it to be similar to established data for white people.7 However, peaks of prevalence have been reported in subpopulations in India (8.8%) in relationship to chemically induced depigmentation.8,9 Similarly, higher incidences of vitiligo in Mexico and Japan have been reported.9 Although the different prevalence rates of vitiligo in various populations could certainly be the result of genetic or environmental differences, one potential reason could be the different social and/or cultural stigmas that influence reporting.9 In light of these challenges, the prevalence of disease is typically stated to be similar all over the world, estimated at 0.5% to 1%.10,11
PATIENT DEMOGRAPHICS
PATIENT DEMOGRAPHICS
Vitiligo can begin at any age, although it usually starts before the third decade of life with almost half of patients presenting before the age of 20 years, and a third before the age of 12 years.9,10,12-14 The segmental variant of vitiligo, affecting only 1 side of the body, tends to occur earlier in life.14 A study in Jordan reported that the prevalence of vitiligo gradually increases with age (0.45% younger than age 1 year; 1% aged 1 to 5 years old, 2.1% aged 5 to 12 years old).15 Males and females appear to be affected equally, although females may seek treatment more frequently.10,11
QUALITY OF LIFE
QUALITY OF LIFE
Vitiligo is frequently dismissed as “cosmetic,” however it is often psychologically devastating for patients.16 Numerous studies show that patients with vitiligo feel stigmatized, have low self-esteem with poor body image, and suffer a considerable psychosocial burden.17,18 Thus, vitiligo may have a significant impact on quality of life, and patients reportedly have mental impairment similar to psoriasis and atopic dermatitis.19 Differences in Dermatology Life Quality Index (DLQI) scores have been noted in various cultural groups, which may reflect different social stigmas of having the disease. For example, the mean of Dermatology Life Quality Index scores was 4.95 in a Belgian population, whereas Indian patients experienced a mean of 7.06 in patients with a successful treatment outcome, and 13.12 in those who failed treatment.20
CLINICAL FEATURES
PRESENTATION PATTERNS
PRESENTATION PATTERNS
Typically, vitiligo lesions are asymptomatic, white, nonscaly macules and patches with distinct margins that fluoresce when illuminated by Wood lamp examination. Although a number of patterns have been described, most can be grouped together, except for the segmental variant of vitiligo, which follows a different disease course and experiences a different treatment response. Thus, we will describe these forms separately and highlight differences important to recognize when developing a management plan. Vitiligo lesions may involve any part of the body, usually with a symmetrical distribution (Figs. 76-1 and 76-2). The disease can start at any site of the body, although the face, as well as acral and genital locations, are often the initial sites. A number of specific clinical patterns have been defined, which include acrofacial, mucosal, generalized, universal, mixed, and rare forms. However, this distinction is not often easy to make, as there is often overlap among these forms, or evolution from one to another. Because many clinicians are familiar with these forms and describe vitiligo accordingly, we briefly describe each one. Acrofacial vitiligo is reportedly more common in adults and typically involves the hands, feet, and face, particularly the orifices. This form may evolve to typical generalized vitiligo. Vitiligo universalis is a rare form of widespread disease. It is usually seen in adults, although cases in children have been reported.14 The form is named “universalis” because it affects a large proportion of the body, frequently defined as greater than 80% of the body surface area. Despite this widespread involvement, hairs may be spared. Classically, vitiligo universalis results from longstanding disease that steadily progresses to nearly complete whitening of the skin.
13
Distribution of vitiligo
Hypomelanosis of hair
r
In Mucosal vitiligo, the oral and/or genital mucosae are primarily involved (Fig. 76-3). When strictly limited to the mucosa, the differential diagnosis of lichen sclerosus et atrophicus should be carefully considered (see also section “Differential Diagnosis”). Furthermore, both conditions in the same patients are reported to coexist.21
Focal vitiligo consists of small, isolated lesions. In a recent report, long-term followup of 53 cases of focal vitiligo have shown that almost 50% of these cases progress to involve larger areas without any clinical sign that might predict this progression.22
The segmental variant of vitiligo is seen in 10% to 15% of vitiligo patients who present to the clinic. It is characterized by a unilateral and segmental, or block-shaped,
1331
13
distribution of the lesions (Fig. 76-4). Typically, a single contiguous segment is involved, although 2 or more segments with ipsilateral or contralateral distribution have been described.23 Mixed vitiligo is a rare form of vitiligo that refers to the occurrence of a clear example of segmental vitiligo plus additional macules or patches that do not fit the segment (Fig. 76-5). These additional patches may be remote from the segmental involvement and are bilateral and symmetrical, affecting the contralateral side.24 In segmental vitiligo, there is frequently early involvement of the follicular melanocyte reservoir, resulting in poliosis. The disease usually spreads over the segment within 6 to 12 months, and then stabilizes.25 Although this may initially be difficult to distinguish from focal vitiligo, the rapid progression of segmental disease usually makes it clear within a few weeks to months. CLINICAL MARKERS OF DISEASE ACTIVITY
1332
CLINICAL MARKERS OF
DISEASE ACTIVITY
In addition to recognized anatomical patterns of vitiligo, there are lesional patterns that indicate disease activity, which are important to recognize when determining the best treatment approach for patients. These patterns include the Koebner phenomenon, trichrome lesions, confetti-like depigmentation, and inflammatory lesions. For example, one study reported that the Koebner phenomenon in vitiligo patients was associated with higher body surface area involvement in vitiligo and poorer response to treatment.26 Disease activity also has been partially quantified through scoring systems such as the vitiligo disease activity score (VIDA), which relies on patient recall, and the Koebner phenomenon in vitiligo score (K-VSCOR), which is focused on clinical signs. The Koebner phenomenon, also called the isomorphic response, describes the observation that depigmentation occurs readily at the site of skin trauma in patients with active vitiligo. This can be recognized as linear marks of depigmentation where the skin has been scratched, lacerated, or burned, or nonlinear macules and patches at the site of known skin injury, such as erosions and abrasions (Fig. 76-6). Trichrome vitiligo is characterized by blurring of lesional borders because of the presence of a hypopigmented
zone between the depigmented and normally pigmented border. This results in the appearance of 3 distinct colors: the depigmented skin, normally pigmented skin, and hypopigmented skin (Fig. 76-7). This pattern is associated with active, rapidly spreading vitiligo.27
Confetti-like depigmentation consists of multiple small macules of depigmentation clustered together, often at the edge of existing vitiligo lesions (Fig. 76-8). One study used serial photography to demonstrate that these small macules grew and coalesced into larger depigmented areas after just a few weeks,
13
identifying this sign as an important marker of disease activity.28
Inflammatory vitiligo is a very rare form of vitiligo characterized by the presence of erythema, scale, and itch at the border of hypopigmented or depigmented lesions (Fig. 76-9). This inflammatory phase is typically transient, lasting just a few weeks to months but rapidly progressing to involve large areas of the body. Early histologic studies in vitiligo were done on inflammatory lesions, where the immune infiltrate could be readily observed.29
1333
13
The VIDA score is a 6-point scale that was developed with the aim of assessing and monitoring vitiligo activity.30 Because this scoring is based on the patient’s recollection of disease activity, it may be subject to recall bias. Active vitiligo is defined as the spread of existing lesions or onset of new lesions. The VIDA scores range from +4 (activity lasting 6 weeks or less) to −1 (vitiligo stable for 1 year or more with spontaneous repigmentation). One of the limitations of the VIDA score is that different lesions can have different scores, making it difficult to use in daily practice. Finally, the K-VSCOR uses the Koebner phenomenon and anatomical location of lesions to determine disease activity in vitiligo patients.31 It is based on the presence or absence of vitiligo lesions at 6 different areas of the body (forehead + scalp areas, eyelids, wrists, genital + belt areas, knees and tibial crests) as well as disease duration. The K-VSCOR ranges from 0 to 56, with 56 corresponding to the highest likelihood of having the Koebner phenomenon, which serves as an indicator of disease activity in the clinic. Further validation is needed to predict the extension of lesions over a longer period of time.
DISEASE ASSOCIATIONS
DISEASE ASSOCIATIONS
Vitiligo is an autoimmune disease of the skin that is associated with a number of other autoimmune diseases in other organs through increased incidence of type 1 diabetes, autoimmune thyroiditis, pernicious anemia, Addison disease, lupus, and alopecia areata, in both vitiligo patients and their family members.32,33
This strongly implicates inherited factors that predispose patients and their family members to a group of autoimmune diseases, and the breadth of diseases found in this overlap suggests that the predisposition is toward autoimmunity in general, rather than specific diseases themselves. Up to 20% of vitiligo patients have at least 1 additional autoimmune disease, and most of these patients (13% to 19%) have autoimmune thyroid disease. This increased risk has prompted some to advocate testing thyroidstimulating hormone (TSH) in all patients with vitiligo, because the pretest probability of finding a positive result is higher in this patient population. Others suggest, however, that this is unnecessary, because many patients will develop thyroid disease much earlier or later than the onset of vitiligo, and recommend that the presence of symptoms should drive TSH screening.34
There has always been some concern that vitiligo patients have a higher risk of skin cancers than the general population because of their loss of pigment in the skin. Although this makes some intuitive sense, the data do not support this hypothesis. Two large studies, one of 1307 participants35 and another of 10,040 participants,36 reported that vitiligo patients have close to 3-fold lower risk of developing melanoma, basal cell carcinoma, and squamous cell carcinoma compared to
1334
controls. This protection was maintained even when factors like reduced sun exposure and/or increased exposure to phototherapy were factored in. Controls included partners of patients in one study and vascular surgery patients in another. The remarkable agreement between these 2 studies strongly suggests that the data are representative, despite the individual weaknesses of each study. Protection from melanoma is least surprising, as immune surveillance against neoplastic melanocytes should be heightened in vitiligo patients, and because genetic risk alleles for vitiligo are simultaneously protective against melanoma.37 However, why the incidence of basal cell carcinoma and squamous cell carcinoma are also lower in vitiligo patients is not clear.
DISEASE COMPLICATIONS
DISEASE COMPLICATIONS
Melanocytes are found not only in the epidermis of the skin, but also in the mucous membranes, hair follicles, uveal tract, retinal pigment epithelium, membranous labyrinth of the inner ear, heart, and meninges of the brain. Typically, these sites are spared in vitiligo patients, with the exception of hair follicles, which can be involved when present within lesions. However, some studies report hearing changes in vitiligo patients, with sensorineural hearing loss present with a wide range of prevalence (20% to 60%), depending on the study.38-40 However, sensorineural hearing loss frequently goes undetected by the patient, and is only observed with formal testing. Ocular abnormalities have been reported in vitiligo patients as well, including pigment changes, scarring, and even uveitis in up to 5% of patients.41,42 Vogt-Koyanagi-Harada syndrome (VKHS) and Alezzandrini syndrome represent severe, rare forms of vitiligo that affect organs other than the skin. VKHS results in skin depigmentation with prominent poliosis, as well as hearing loss, visual changes, meningitis, and flu-like symptoms. The skin manifestations occur after the systemic ones, so those with classic vitiligo are not known to progress to VKHS.43 Alezzandrini syndrome has been described in 7 patients, and is characterized by segmental vitiligo (unilateral depigmentation) on the face with poliosis, plus ipsilateral hearing loss and visual changes.44-46
ETIOLOGY AND PATHOGENESIS
COMPETING HYPOTHESES AND THE CONVERGENCE THEORY
COMPETING HYPOTHESES
AND THE CONVERGENCE
THEORY
Vitiligo is an autoimmune disease of the skin in which CD8+ T cells target melanocytes and destroy them, leaving areas without pigment production, which is
clinically manifest as white macules and patches. The pathogenesis has been debated for many years, with multiple hypotheses offered as alternative explanations as to what lies at the root of the disease. These alternative hypotheses include cellular stress causing degeneration of melanocytes, chemical toxicity causing melanocyte death, and neural changes that influence melanocytes or their ability to produce melanin. The reason for these alternative explanations were research observations over the years suggesting that much more than simply autoimmune targeting of perfectly normal melanocytes was occurring in vitiligo. Early clinical observations that other autoimmune diseases occurred frequently in vitiligo patients and their family members hinted, through guilt by association, that vitiligo was itself an autoimmune disease. Additionally, antimelanocyte antibodies appeared to be elevated in vitiligo patients compared to healthy controls, also implicating immune responses in disease pathogenesis. However, others found that melanocytes cultured from vitiligo patients, and thus separated from immune influences, were abnormal—they did not grow well, were susceptible to exogenous oxidative stress, and appeared to have elevated cellular stress. This was manifest by the presence of reactive oxygen species and a dilated endoplasmic reticulum, a marker of activation of the unfolded protein response which is involved in stress responses.47-52 But histologic studies revealed that CD8+ T cells infiltrated lesional epidermis and were found next to dying melanocytes, strongly supporting T-cell–mediated cytotoxicity as the key event in vitiligo.29,53 Finally, one group reported that CD8+ T cells isolated from lesional skin of a patient and then coincubated with nonlesional skin from that same patient resulted in melanocyte targeting and death, demonstrating that CD8+ T cells were both necessary and sufficient to cause melanocyte destruction in vitiligo patient skin.54
These seemingly unrelated and conflicting observations were later tied together by the convergence theory, which suggested that all of these pathways may synergize to cause vitiligo in patients.55 Now it appears that melanocytes in vitiligo patients are indeed abnormal and are more sensitive to cellular processes like melanogenesis and energy consumption. This results in the production of reactive oxygen species and activation of the unfolded protein response, which initiate the secretion of signaling intermediates from melanocytes that act as danger signals to alert the innate immune system. Next, innate immune cells activate and recruit adaptive immune CD8+ T cells to the skin, where they find the abnormal melanocytes and kill them. Thus, cellular stress within the melanocyte and autoimmunity work together to cause what we see clinically as vitiligo.56,57
Additional studies have now revealed that certain chemicals, typically phenols, induce the cellular stress response in melanocytes by acting as analogs of tyrosine, also a phenol.56 Thus, these chemicals act as exogenous environmental agents that induce and exacerbate vitiligo by initiating the cellular stress
13
response in otherwise well-compensating melanocytes. Consequently, the “chemical theory” can be incorporated into the inclusive convergence theory as well. Finally, the neural hypothesis was based on the clinical appearance of segmental vitiligo, misinterpreting the unilateral nature of disease for being associated with dermatomes, which is not the case.58-60
Others reported that catecholamines were increased in the urine of vitiligo patients; however, catecholamines are also secreted by melanocytes, which is a more likely source in vitiligo. Case reports of vitiligo clearing after unilateral nerve injuries suggested nerves as important players in disease pathogenesis, but further observations noted the opposite result as well, eliminating this as strong evidence. The role of emotional stress in worsening vitiligo has been offered as evidence, yet this is common in many diseases that do not appear to be influenced by nerves. Finally, some animals control their pigmentation through innervation (primarily fish), but this has never been observed in mammals. Thus, the “neural hypothesis” remains unsupported by evidence and should be discarded for now.58
T CELLS AND CYTOKINES IN AUTOIMMUNITY
T CELLS AND CYTOKINES IN
AUTOIMMUNITY
As mentioned above, CD8+ T cells play a critical role during the progression of vitiligo, serving as the primary immune effectors that destroy melanocytes. Studies using human tissues and a mouse model of vitiligo have revealed that interferon (IFN)-γ is a key cytokine that drives the disease.61-64 IFN-γ is secreted by melanocyte-reactive autoimmune CD8+ T cells, and induces the production of CXCL10 and other chemokines from keratinocytes, which promote the further recruitment of additional T cells that progressively destroy more melanocytes as the disease spreads.64,65
Multiple groups have found that IFN-γ–induced chemokines are elevated in the serum and skin of vitiligo patients, and these may serve as useful biomarkers of disease activity in the future.64,66-68 In addition, targeting the IFN-γ–chemokine axis during disease may be an effective novel treatment strategy (see section “Emerging Therapies”).69
THE SEGMENTAL VARIANT OF VITILIGO, A SPECIAL CASE
THE SEGMENTAL
VARIANT OF VITILIGO,
A SPECIAL CASE
As mentioned above, segmental vitiligo was initially thought to mirror the distribution of nerves via dermatomes, which led to the “neural hypothesis.” Close inspection, however, reveals that segmental vitiligo lesions rarely, if ever, follow dermatomes, and frequently cross these zones in a perpendicular direction.
1335
13
Depigmented blocks of segmental vitiligo also do not appear to follow blaschkoid lines, especially on the trunk, which are narrow and S-shaped.59,60 So, the question arises, what defines a segment of vitiligo, and what is the pathogenesis of this variant, considering that immune-mediated disorders do not typically respect the midline? One hypothesis that is gaining acceptance is that segmental vitiligo results from a general autoimmune predisposition combined with melanocytes that have acquired a postzygotic mutation that alters their susceptibility to autoimmune attack, like activation of the cellular stress pathways discussed above. This has the potential to explain (a) why it is unilateral (melanocytes migrate from the neural crest and do not cross the midline), (b) its rapid evolution and stabilization (normal melanocytes create the stable border of the lesion), (c) its resistance to treatments (abnormal melanocytes are unstable and have an impaired ability to repigment the skin), and (d) the successful response to surgical therapies (normal melanocytes transplanted from another region are stable and resistant to autoimmune attack).70
RISK FACTORS IN VITILIGO
RISK FACTORS IN VITILIGO
Similar to other autoimmune diseases, a number of factors influence the risk of developing vitiligo. These include both genetic factors and environmental factors. Vitiligo is more common in family members of affected patients, as 15% to 20% of patients have a family member with the disease, strongly suggesting that genetics influences the risk of getting disease. While the prevalence of vitiligo in the general population is close to 1%, the prevalence in first-degree relatives is 7%, and the prevalence in identical twins of affected individuals is 23%, clearly demonstrating a role for genes in disease. However, the fact that concordance between identical twins is not 100% also clearly demonstrates nongenetic influences in disease, which may represent environmental factors, stochastic influences (those that occur by chance), or both. Modern genome-wide association studies have identified approximately 50 genetic loci that contribute to the risk of developing vitiligo, clearly demonstrating that it is inherited in a polygenic fashion with a complex interplay among multiple genes that contribute to the total risk. Of these loci, the majority are involved in regulating the immune system, representing key molecules in both innate and adaptive immunity, and thus strongly support the conclusion that disease is immune-mediated. Others appear to influence cellular apoptosis pathways and still others direct melanocyte function, including melanogenesis, supporting a role for the melanocyte in conferring risk for disease. Importantly, those genes involved in melanogenesis also influence the risk of developing melanoma, but in the opposite direction, suggesting that immune responses in vitiligo may be protective against melanoma, and thus may have evolved to protect against the development of this devastating cancer.37
1336
In addition to genetic influences, environmental influences are important in vitiligo. The first chemical exposure to be definitively linked to the onset of vitiligo occurred in a group of leather factory workers in
1939. A large proportion of these workers developed depigmentation on their hands and lower arms, and monobenzyl ether of hydroquinone, or monobenzone, was implicated as the cause. Because some of the workers also developed depigmentation at sites remote from the exposure, depigmentation was not simply the result of direct toxicity to the melanocyte, but an exacerbation of the autoimmune destruction.71
Other chemicals have been similarly implicated since then, including 4-tert-butyl phenol and 4-tertbutylcatechol.72 An outbreak of vitiligo occurred in Japan in 2013, when a cosmetic company created a new skin lightening cream that resulted in more than 18,000 users getting vitiligo at the site of application and in remote areas.72 Another study revealed that the use of permanent hair dyes may increase the risk of getting vitiligo by as much as 50%.73 The common characteristic of implicated chemicals is that they are phenols with a chemical structure that resembles the amino acid tyrosine, also a phenol. Mechanistic studies reveal that these chemicals act as tyrosine analogs, which are taken up by melanocytes instead of tyrosine, interact with tyrosinase, and induce cellular stress pathways that then activate immune inflammation to initiate or exacerbate vitiligo.56,74-76
DIAGNOSIS
CLINICAL EXAMINATION
CLINICAL EXAMINATION
The diagnosis of vitiligo is usually a clinical one, as there is usually no need for additional laboratory or histologic testing to confirm the diagnosis. On physical examination it is important to differentiate vitiligo from its segmental variant, as these 2 forms have different clinical course, prognosis, and treatment responses. Vitiligo is usually characterized by well-defined, symmetrical depigmented lesions that can be distributed on any part of the body, but with a preference for the face (particularly periorificial areas), genitals, and acral areas. Wood lamp examination in a dark room is helpful in differentiating the depigmentation of vitiligo from hypopigmentation seen in other diseases. The disease is also characterized by cycles of flares and stabilization that are unpredictable, which can be distressing for patients. Additional clinical signs that may help with the diagnosis of vitiligo are the presence of multiple halo nevi and poliosis. The presence of repigmentation can be recognized as perifollicular pigmented macules from pigmented hairs at hair-bearing sites (Fig. 76-10) or convex patterns of pigment at lesional borders in glabrous skin (Fig. 76-11). Hair-bearing sites without poliosis repigment easily, whereas glabrous skin and lesions containing mostly white hairs respond poorly.
In the segmental variant of vitiligo, the lesions are unilateral, typically do not cross the midline, and are organized into block-like patterns, in contrast to the dermatomes of zoster or blaschkoid lines of keratinocyte disorders like segmental Darier disease. These blocks of depigmentation may represent zones of skin that have been affected by postzygotic mutations that create a mosaic distribution of abnormal melanocytes (discussed under section “Segmental Variant Special Case” above).59,60 The evolution of segmental vitiligo is distinct in that the onset is usually acute with rapid progression over 6 to 12 months before it becomes stable and unchanging for the remaining life of the individual.
13
LABORATORY TESTING
LABORATORY TESTING
Because vitiligo is associated with other autoimmune diseases such as thyroid diseases, clinicians should consider laboratory testing for these other diseases when patients’ symptoms warrant them. TSH is commonly tested to rule out concomitant Hashimoto thyroiditis, although in the absence of symptoms this testing may not be necessary.34 Complete blood count and antinuclear antibody testing can be considered in the context of light sensitivity, as phototherapy is a standard in vitiligo treatment. During followup, clinicians should consider testing for other autoimmune markers whenever patients have suggestive signs and symptoms.
HISTOLOGY
HISTOLOGY
When the history and physical examination are consistent with vitiligo, there is usually no need for skin biopsy to confirm the diagnosis. However, when the presentation is unusual, biopsy may help to rule out other disorders of pigment abnormalities that fall within the differential diagnosis (discussed below). When performed, histologic examination and immunohistochemical studies reveal a complete loss of melanocytes within the epidermis,55 and biopsy near the lesional border during progression may demonstrate an inflammatory infiltrate of CD4+ and CD8+ T cells in an interface pattern, with primarily CD8+ T cells infiltrating the epidermis.77
DIFFERENTIAL DIAGNOSIS
The differential diagnosis of vitiligo is broad and is presented concisely in Tables 76-1 and 76-2. In general, inherited hypomelanoses are present at or within a few months after birth, whereas vitiligo is rarely, if ever, present that early. Wood lamp examination helps to differentiate the depigmentation of vitiligo from hypopigmentation of most other diseases. Specifically, vitiligo and its segmental variant have different considerations when thinking about differential diagnoses, because the former is symmetric, often more widespread, and progressive, whereas the latter is focal, unilateral, and stable. The differential diagnosis of vitiligo includes inflammatory, postinflammatory, neoplastic, and genetic (mostly congenital) disorders of depigmentation. The first helpful step is to determine whether the lesion or lesions are congenital, remembering that in fair skin, lesions may not become apparent until after the first few months of life, often after the first sun exposure. A number of genodermatoses may be initially misdiagnosed as vitiligo, but the most frequent are piebaldism and tuberous sclerosis. In piebaldism, the combination of white forelock, anterior body midline depigmentation,
1337
13
CONDITION DISTINGUISHABLE FEATURES
Inherited Hypomelanoses
Piebaldism (KIT mutation) (Fig. 76-12) White forelock, anterior body midline depigmentation and bilateral shin depigmentation present at birth (with absence of melanocytes); autosomal dominant
Waardenburg syndrome (PAX3 mutation) White forelock, white skin macules, hypertelorism, heterochromic or hypoplastic blue irides, deafness, early graying, ± Hirschsprung disease
Tuberous sclerosis (TSC1 and TSC2 mutations) (Fig. 76-13) Hypomelanotic macules (ash leaf) present within the first years of life; angiofibromas at age 3-4 years; ungual fibromas; cephalic and lumbar (shagreen patch) fibrous plaques; and hypopigmented “confetti” macules appearing in childhood to early adolescence; seizures; autosomal dominant
Ito hypomelanosis Hypopigmented skin macules and patches along Blaschko lines in a linear pattern, unilateral or bilateral pattern; usually develops within the first 2 years of life; sporadic; chromosomal or genetic mosaicism
Infectious Disorders
Tinea versicolor (Fig. 76-14) Well-demarcated finely scaling patches in highly sebaceous areas; yellow-green fluorescence on Wood light
Treponematoses (syphilis and pinta) Postinflammatory hypopigmented/depigmentated patches) on the neck on trunk, limbs. Positive testing for serologic treponemal infection
Leprosy (tuberculoid/ borderline forms) (Fig. 76-15) Mainly hypopigmented patches; localized anesthesia
Postinflammatory Hypopigmentation
Discoid lupus erythematosus, scleroderma, lichen sclerosis et atrophicus, psoriasis
History of preexisting condition
Paramalignant Hypomelanoses
Mycosis fungoides (Fig. 76-16) Scattered irregular hypopigmented patches on non–sun-exposed areas. Atrophic epidermal surface. Plaque and tumor lesions of mycosis fungoides may be present concurrently. Histology: epidermotropism of atypical lymphocytes
Cutaneous melanoma Dyschromic lesion combining pigmented areas with depigmentation around or within the tumor
Idiopathic Disorders
Idiopathic guttate hypomelanosis Hypopigmented well-circumscribed macules, sharply defined and small in size. Usually localized on photoexposed areas, especially the legs. Very slowly progressive and nonconfluent
Progressive macular hypomelanosis Nummular, nonscaly hypopigmented spots lesions of the trunk, often confluent. Punctiform red fluorescence on Wood lamp
Postinflammatory pigment loss History of preceding eruption/injury
Melasma Hyperpigmented macules and patches, often limited to the face. The contrast between lighter and darker skin may
Melasma Hyperpigmented macules and patches, often limited to the face. The contrast between lighter and darker skin may appear hypopigmented; dermoscopy may show capillary network
appear hypopigmented; dermoscopy may show capillary network
bilateral shin depigmentation, and large islands of sparing are hallmarks of the disease. Family history will often make the diagnosis of piebaldism straightforward, as it is most often dominantly inherited.
CONDITION DISTINGUISHABLE FEATURES
Nevus anemicus Poorly demarcated white macule surrounded by erythema, which disappears with diascopy.
Nevus depigmentosus Well-delimited hypopigmented macule usually present at birth with irregular, saw-toothed border. Hairs within the lesion generally remain pigmented. The lesion is stable in size but will expand in proportion to growth with age. In fair skin types, parents may note the lesion after first photoexposure of the child
Nevus
Well-delimited hypopigmented macule usually
depigmentosus
present at birth with irregular, saw-toothed border. Hairs within the lesion generally remain pigmented. The lesion is stable in size but will expand in proportion to growth with age. In fair skin types, parents may note the lesion after first photoexposure of the child
1338
Distinguishing vitiligo from tuberous sclerosis relies on the hypopigmented nature of ash-leaf spots, as well as their stability over time. Of course, the presence of seizures or other cutaneous symptoms that may appear later, such as shagreen patches or angiofibromas, should prompt further investigation for tuberous sclerosis. If the lesions in question are acquired, the most common differential diagnoses are pityriasis versicolor and postinflammatory hypopigmentation, such as pityriasis alba. Here, a Wood lamp examination is quite helpful, as lesions of vitiligo are depigmented and enhance, while others are hypopigmented and do not. In addition, neoplastic hypomelanoses, in particular hypopigmented mycosis fungoides, should be ruled out. Hypopigmented mycosis fungoides is distributed in sun-protected areas and is hypopigmented, rather than depigmented. Isolated genital involvement should be carefully differentiated from the diagnosis
of lichen sclerosus et atrophicus as this diagnosis can be quite destructive and often is irreversible. Lichen sclerosus is often symptomatic, following a figure-ofeight pattern around the anus and introitus in women, frequently with signs of atrophy and fissuring of the skin. In longstanding cases, it may be accompanied by resorption of normal structures like the labia minora as well as narrowing of the introitus. A complicating factor in the differential diagnosis includes reports of concomitant genital lichen sclerosus and vitiligo. Biopsy can be helpful in difficult cases. For segmental vitiligo, nevus depigmentosus is the most common consideration in the differential
13
diagnosis. However nevus depigmentosus is usually congenital or recognized within a few months of life and is stable in size, growing only in proportion to the child. In contrast to its name, it is typically hypopigmented rather than depigmented, and the border is frequently jagged rather than smooth, both notable differences from vitiligo. When biopsy is performed, histology displays normal or a slightly decreased number of melanocytes with reduced melanin content, rather than absence of melanocytes. Nevus anemicus is another to condition to rule out and is usually present at birth. Clinically, nevus anemicus corresponds to a poorly demarcated white macule surrounded by erythema, which, contrary to segmental vitiligo, does not
1339
13
show accentuation when examined with Wood lamp. It also disappears with diascopy, or other gentle pressure on the skin.
CLINICAL COURSE AND PROGNOSIS
Vitiligo has an unpredictable course with a disposition toward cycles of flares and phases of stability. Early whitening of the hairs is unusual, although this may appear later in the course of the disease. Repigmentation in hair-bearing locations is likely, and may either occur spontaneously, after specific therapeutic intervention, or following sun exposure. However, lesions in glabrous skin are much slower to respond, as they improve from slower marginal repigmentation that is limited to only a few millimeters total, despite longterm treatment. There is some evidence that episodes of stress may trigger disease onset and/or relapse. In contrast, the course of segmental vitiligo is rapid but selflimited, with rapid stabilization and rare progression after this has occurred. The early involvement of hairs makes segmental vitiligo less responsive to treatment, although if caught early good results may be obtained.
MANAGEMENT
When developing a management plan for vitiligo patients, multiple factors should be considered. A thorough examination of patients under natural and Wood
1340
lamp light is important to assess the extent of disease. In addition, social and demographic details, family history of the patient, as well as the patient’s relevant medical history, should be elicited at the initial consultation. The skin phototype, presence of halo nevi, disease duration and extent, and activity are key items in guiding therapeutic management. Scoring of disease activity by evaluating the probability of Koebner phenomenon also can be considered.31
As of this writing most therapies that are effective for vitiligo were developed for other inflammatory skin diseases and are thus used off-label. The management plan for patients with vitiligo will vary according to disease activity and extent. For example, if a patient presents during active progression, combination therapy that includes oral antiinflammatories may be important to halt the progression of disease, as other therapies, such as phototherapy, may take weeks to months to become effective. If the disease is stable, monotherapy is an option as the likelihood of progression while the responses slowly develop is minimal.
TOPICAL THERAPIES
TOPICAL THERAPIES
Topical therapies may be used as monotherapy when there is limited surface involvement (less than 5% body surface area); however, they are often used in combination with phototherapy. Two main classes of topical drugs are used in vitiligo: topical steroids and topical calcineurin inhibitors. The advantages of topical corticosteroids are good efficacy, ease of application, high compliance rate, and low cost. The drawbacks of topical corticosteroids are their side effects, which include skin atrophy, telangiectasia, hypertrichosis, acneiform eruptions, and striae, as well as increased intraocular pressure (exacerbation of glaucoma) when used around the eyes. Typically, ultrapotent formulations are required for reliable efficacy, and most published studies have evaluated the class I steroid clobetasol. They should be applied twice daily and can be used in a discontinuous scheme, such as cycles of 1 week on treatment followed by 1 week off treatment for up to 6 months, to avoid side effects. For childhood vitiligo, a class II potency steroid with a good safety profile, like mometasone, is a good choice. Lower-potency steroids do not have strong evidence to support their use. Advantages of topical calcineurin inhibitors include their good efficacy and excellent safety profile.78 They can be used on areas that are not ideal for steroids, such as on the face, neck, intertriginous areas, and on children. Of note, warnings have been placed on the long-term use of topical calcineurin inhibitors in relation to an increased risk of cancer; however, these concerns are based on risks associated with oral dosing of these drugs and have not been observed with topical use. A recent systematic review and metaanalysis concluded that the use of topical steroids and calcineurin inhibitors was unlikely to increase the risk of lymphoma in patients with atopic dermatitis.79
Although some concerns about the combining of phototherapy with these drugs promotes skin cancer have been raised, the combination of light therapy with topical calcineurin inhibitors increases their efficacy80
and there is no clinical data that supports these concerns for increased cancer risk. Thus, clinicians should proceed with these treatments but with caution, and patients should be counseled of these facts when prescribed these therapies, at least until these warnings are removed from the packaging. A recent report tested topical tacrolimus as maintenance therapy in patients who achieved repigmentation through other methods.81 In this randomized controlled study of 35 patients, more than 90% of those treated with tacrolimus 0.1% only twice weekly maintained their pigmentation without a relapse of their vitiligo, whereas only 60% did so in the placebo group. A small number of studies have compared topical calcineurin inhibitors and topical steroids without significant difference in efficacy between the 2 groups.82
PHOTOTHERAPY AND COMBINATION THERAPIES
PHOTOTHERAPY AND
COMBINATION THERAPIES
Because of its efficacy, ease of use, and relatively good safety profile, full-body phototherapy should be considered the first treatment option in patients with more than 5% of the body surface area affected, especially if the disease is rapidly spreading (Fig. 76-17). For those with more limited, focal disease, targeted phototherapy can be considered because of its very high efficacy. However, phototherapy is time-consuming and devices may not be readily accessible to all patients. When this is the case, home phototherapy can be considered, where units are prescribed and purchased for use in the patient’s home. Although the strength of home units does not match those in the physician’s office, the convenience of getting phototherapy at home often results in excellent responses.83 Most units require a prescription from a dermatologist, who must provide ongoing codes to enable continued use of the unit after regular in-office assessments. Because some patients with vitiligo have circulating antinuclear antibodies that could sensitize them to light, screening for antinuclear antibodies prior to phototherapy can be considered, particularly if there is a history of sun sensitivity. Overall, the risk-to-benefit profile of all treatments should be considered when developing a management strategy for each patient. Historically, phototherapy has been administered using different sources, including oral or topical psoralen plus ultraviolet A (PUVA), broadband ultraviolet B, narrowband ultraviolet B (nbUVB), and targeted phototherapy with excimer laser. These are outlined below:
PSORALEN AND ULTRAVIOLET A
PUVA was the first phototherapy treatment reported to be effective for vitiligo; it has since, however, become
13
A
B
associated with adverse effects that include nausea, ocular damage, and phototoxic reactions, as well as an increased risk of skin cancer.84 A 2015 Cochrane review reported that the efficacy of PUVA was inferior to nbUVB in achieving greater than 75% repigmentation in vitiligo patients.85 In another study, color matching of treated areas with normal skin was inferior in PUVA compared to nbUVB.86 In addition, nbUVB treatment has fewer short-term (painful erythema) and long-term (epidermal thickening, atrophy, and photocarcinogenesis) adverse reactions than PUVA.56 Thus, PUVA is no longer first-line therapy for vitiligo, and has been largely replaced by nbUVB. However, PUVA may be considered in patients who fail to repigment with other modalities.86-88 Like other methods of phototherapy, PUVA is typically administered 2 or 3 times weekly.
NARROWBAND ULTRAVIOLET B
nbUVB has largely replaced other modalities because of its efficacy and better safety profile. It provides 2 particular benefits: (a) repigmentation and (b) stabilization, which is important in those who have active disease. Njoo and colleagues achieved greater than 75% repigmentation in 53% and stabilization in 80%
1341
13
of children with twice-weekly nbUVB.89 Increased benefit has been reported with the addition of topical corticosteroids and calcineurin inhibitors. The 2015 Cochrane update for interventions in vitiligo reported that 35 of 96 randomized controlled trials used nbUVB as either monotherapy or in combination with other treatments.90 nbUVB has potent immunosuppressive effects locally and is able to induce melanocyte differentiation and melanin production.91
Treatment with nbUVB should be 2 to 3 times weekly, starting with a dose of 200 millijoules (mJ) with an increase of 10% to 20% increments until reaching the minimal erythema dose, which corresponds to the lowest dose resulting in asymptomatic, visible erythema on depigmented skin that lasts less than 24 hours. A total of 9 to 12 months or more of treatment is required to achieve full repigmentation, with at least 6 months of therapy before determining that the disease is nonresponsive.86 When used on its own, nbUVB has been reported to induce repigmentation rates ranging from 40% to 100%, depending on the location of the lesion.89,92-95
TARGETED ULTRAVIOLET B PHOTOTHERAPY
Targeted UVB phototherapy is achieved using excimer lasers and lamps. They reportedly are equally effective, although excimer lamp induces more erythema.96 Because of their small treatment size, targeted phototherapy is indicated in patients with limited, focal vitiligo (less than 5% of the body surface area affected with stable disease).97 Targeted phototherapy is also reportedly the treatment that achieves highest efficacy for segmental vitiligo in its early phase (ie, disease onset of less than 6 months to 1 year). It is also reportedly safe and effective for long-term treatment of pediatric vitiligo patients.98
COMBINATION THERAPIES
In the most recent update of the Cochrane review, combination therapies using any type of light were considered the most effective treatment for vitiligo. Even though not necessarily synergistic or even additive, the additional benefit of adding topical therapies when undergoing phototherapy appears to be worthwhile. If large areas are involved, sites that are important to the patient, such as the face and hands, may be selected for adjuvant topical therapy. The combination of oral steroid pulse therapy, such as dexamethasone on weekends or prednisone on alternate days, with light therapy is reportedly helpful in controlling rapidly spreading vitiligo until phototherapy achieves a therapeutic dose.99
PSYCHOLOGICAL INTERVENTIONS
PSYCHOLOGICAL
INTERVENTIONS
The psychological impact of vitiligo includes poor self-perception, low quality of life, poor interpersonal
1342
relationships, depression, and anxiety.100-104 Thus, psychological interventions such as cognitive-behavioral therapy and hypnosis have been shown to improve quality of life, reduce anxiety, improve coping with disease, and even enhance repigmentation in vitiligo.101,105-107 Importantly, adolescents with vitiligo are uniquely susceptible to social pressure and stigma, and thus should be screened for psychological impairment and referred for management.
COSMETICS
COSMETICS
Cosmetic camouflage, especially on visible areas such as the face and the hands, can improve quality of life in patients with vitiligo.108,109 There are now several water-resistant camouflage dyes and creams that are available with a wide range of color and shades covering all skin types.
DEPIGMENTATION THERAPY
DEPIGMENTATION
THERAPY
Ever since the observation that monobenzone potently induced and exacerbated vitiligo in exposed individuals, it has been used as a treatment for vitiligo to depigment the skin, removing the remaining pigment and evening out the tone.110 In fact, it is the only Food and Drug Administration–approved medical therapy for vitiligo. For patients with widespread disease that would be difficult to reverse with the conventional treatments discussed above (many suggest greater than 80% body surface area or significant poliosis), monobenzone can be prescribed as a 20% topical cream to be applied 1 to 2 times daily. It can take 1 to 2 years for complete depigmentation, and it even affects areas remote from the site of application, so it cannot be used for just local depigmentation. Up to 20% of patients develop a contact dermatitis to the cream, which is located only in pigmented skin and may limit treatment. If this occurs, the strength can be decreased to 10%, and concurrent use of topical steroids may limit the reaction. Hair, eyes, and other locations where melanocytes are found are typically spared during depigmentation therapy with monobenzone. Even though this is a drastic and permanent approach to therapy, patients are typically happy with the result. They must be counseled that their skin will be sun-sensitive for the rest of their lives, and sun protection must be strictly followed.
NONTRADITIONAL TREATMENTS
NONTRADITIONAL
TREATMENTS
There are numerous nontraditional treatments that have been suggested for vitiligo. Of these, khellin, ginkgo biloba, vitamins and nutritional supplements,
Polypodium leukotomos, topical and systemic phenylalanine, topical calcipotriene, and pseudocatalase cream have been used. Current evidence for their efficacy is weak at best and adding them to a therapeutic strategy should be carefully considered in light of this lack of evidence.
SURGICAL THERAPIES
SURGICAL THERAPIES
Surgical therapies for vitiligo can be very successful; however, a key part of surgical therapy is patient selection. Surgery in vitiligo should be reserved for patients with highly stable disease, which has been defined as the absence of new or growing lesions for 1 to 2 years.111 Segmental vitiligo patients are well suited for this approach because their disease stabilizes quickly, but those who do not have this variant have much-less-successful outcomes. Several techniques for surgical treatment exist for vitiligo, which can broadly be divided into tissue grafting and cellular grafting. Tissue grafts include thin and ultrathin split-thickness skin grafts, suction blister epidermal grafts, mini punch grafts, and hair follicle grafts. These approaches all use solid-tissue grafts whose size is matched to the donor site in a 1:1 ratio. Alternatively, cellular grafts include noncultured epidermal cell suspension, cultured “pure” melanocytes, cultured epithelial grafts, and autologous noncultured extracted hair follicle suspension. These approaches
A
13
transplant suspensions of keratinocytes and melanocytes and can cover larger surface areas with up to a 1:10 ratio of donor-to-recipient area. Each technique has advantages and disadvantages. In general, tissue grafts are easier to perform than cellular grafts, but are limited by the need to harvest tissue in a 1:1 ratio to the donor site. Split-thickness grafting is easy and inexpensive, but frequently results in color mismatch and occasional failure of the graft to take. Punch grafting is easy to perform and inexpensive but should be used in limited areas because of frequent side effects, such as cobblestoning, which describes healing at the recipient site with raised grafts that are visible and palpable, like cobblestones on a path.112 Blister grafting gives better cosmetic results without cobblestoning, but it is time-consuming and may be more difficult to perform because of handling and placement of the very thin blister roof graft.113-117
Because of their improved donor-to-recipient-site ratio, excellent outcomes in percent repigmentation and color match, as well as improved healing, cellular grafts are becoming the first-line in surgical management of stable vitiligo (Fig. 76-18). The most commonly used technique, the melanocyte keratinocyte transplant procedure, creates a suspension of keratinocytes and melanocytes from donor epidermis that is enzymatically digested and mechanically disrupted into a single cell suspension. This technique has been optimized and simplified over the past few years and now requires minimal laboratory support. It is usually conducted in 2 steps. The first consists of shaving an ultrathin skin
B
1343
13
donor graft (Fig. 76-19A), which is rinsed and incubated in 0.25% trypsin for 30 minutes at 37°C (98.6°F) before manually removing the epidermis from the dermis, disrupting the epidermis mechanically, and centrifuging
A
C
the epidermal fragments to create a cellular pellet (Fig. 76-19B, C). This pellet is resuspended in lactated ringers or normal saline in a 1mL syringe. The second step consists of applying this cellular suspension over
B
D
1344
the recipient site that was previously dermabraded or laser treated to remove the epidermis (Fig. 76-19D). The recipient site is then covered with an appropriate dressing for 4 to 7 days, depending on the treated area.118,119
TREATMENT ALGORITHM
TREATMENT ALGORITHM
We propose 2 treatment algorithms, one for vitiligo (Fig. 76-20) and another for the segmental variant of disease (Fig. 76-21).
EMERGING THERAPIES
EMERGING THERAPIES
As discussed above, vitiligo is driven primarily by the destruction of melanocytes by CD8+ T cells that secrete IFN-γ, which induces chemokines that recruit additional T cells in an ongoing, positive feedback loop. Future targeted therapies are likely to target this and other synergistic cytokine pathways, similar to recent advancements in the treatment of psoriasis. However, psoriasis treatments are ineffective for vitiligo because the interleukin-23–interleukin-17– tumor necrosis factor-α cytokine axis that drives psoriasis is not active in vitiligo.69
13
Examples of future targeted therapies include inhibition of Janus kinases (JAKs), which are required for the signaling of many cytokines, including IFN-γ. In small case studies and series, JAK inhibitors have been reported to promote repigmentation of vitiligo patients, including oral tofacitinib, oral ruxolitinib, and topical ruxolitinib.120-126 Ongoing clinical trials are currently testing JAK inhibitors as new treatments for patients with vitiligo. In addition, biologics that target other members of the IFN-γ–chemokine signaling axis may be effective, such as antibodies against CXCR3 or its ligands, which have been reported effective in a mouse model of vitiligo.64,127 Additional cytokine-targeted biologics have been developed for other diseases and may be repurposed for vitiligo.69 Side effects should be considered for any immunotherapy, which may include increased incidence of infections or decreased tumor surveillance. Finally, in addition to targeted immunotherapy, treatments that promote melanocyte regeneration, proliferation, and/or migration could also be effective treatments, particularly when combined with immunosuppressive treatments. One example that has been tested in vitiligo patients is afamelanotide, an α-melanocyte–stimulating hormone analog, which, in conjunction with nbUVB, increased the rate and extent of repigmentation in vitiligo patients.128,129 Side effects of this treatment included nausea, abdominal pain, and darkening of the normal skin of patients, which led to
Treatment algorithm for vitiligo
Vitiligo/Nonsegmental Vitiligo
• Avoid triggering factors (trauma inducing Koebner phenomenon, chemicals)
• Consider screening for other forms of autoimmunity, including autoimmune thyroiditis
• Offer psychological support if needed
• Offer camouflage counseling
Stable disease
Unstable/active disease
Oral minipulse steroids (3 to 6 months) + nbUVB + topical treatment
Extensive and widespread involvement (>5% BSA) Limited involvement (<5% BSA)
Topical treatment (TIM for face/intertriginous areas and corticosteroids for body)
Excimer laser/lamp
Combination therapies
Combination therapies
• Topical treatment (TIM for face/intertriginous areas and sequential potent steroids for body)
• nbUVB
1345
13
Treatment algorithm for segmental vitiligo
Segmental Vitiligo
Unstable disease/disease onset of less than 6 months to 1 year
Oral minipulse steroids (3 to 6 months) + excimer lamp + topical treatment
Stable disease/disease onset of more than 1 year
Combination therapies
• Topical treatment (TIM for face and alternating potent topical steroids/TIM for body)
• Excimer laser/lamp
If failure, surgical treatment
dissatisfaction and withdrawal of some participants from the study owing to the increased prominence of lesions against the darker background of normal skin. In summary, recent advances in our understanding of vitiligo have led to the development of new treatment strategies that may have improved efficacy in our treatment of patients with vitiligo. As with any new therapy, safety will have to be monitored and carefully considered when making recommendations for patients suffering with this psychologically, but not physically, debilitating disease. This marks an exciting time for both patients with vitiligo and their caregivers, who are gaining deeper insight into their disease, and may have improved options for management in the near future.
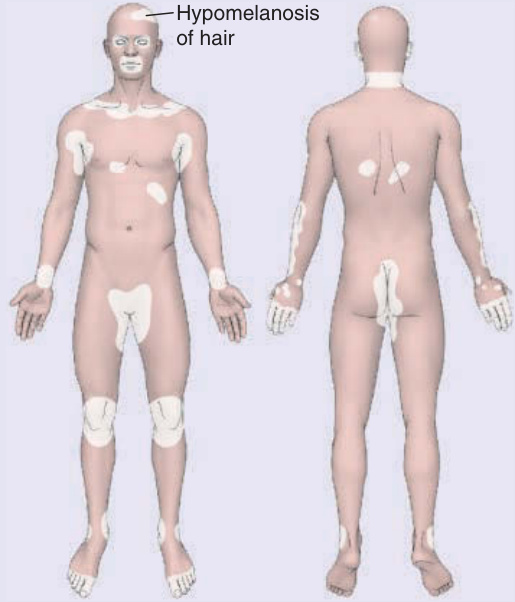
Figure 76-1 Distribution of vitiligo. (From Wolff K, Johnson R, Saavedra AP, et al. Fitzpatrick’s Color Atlas and Synopsis of Clinical Dermatology. 8th ed. New York, NY: McGraw-Hill; 2017, with permission.)

Figure 76-2 Symmetrical patchy depigmentation of vitiligo.
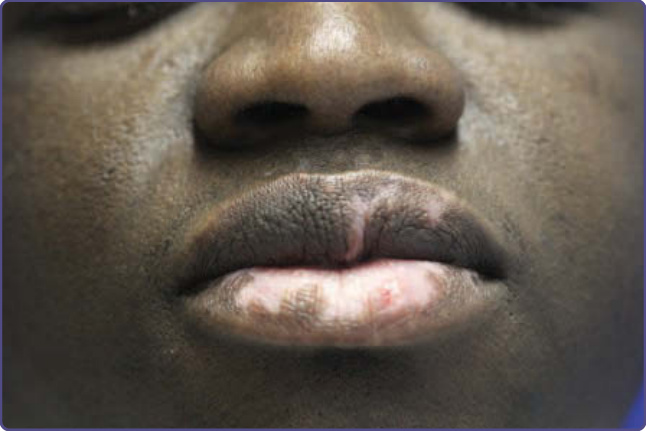
Figure 76-3 Mucosal vitiligo, limited to the lips.

Figure 76-4 Unilateral, block-like depigmentation of the segmental variant of vitiligo.

Figure 76-5 Mixed vitiligo, made up of a segmental lesion on the back plus additional bilateral lesions in remote areas.

Figure 76-6 Linear depigmentation in locations of skin trauma.
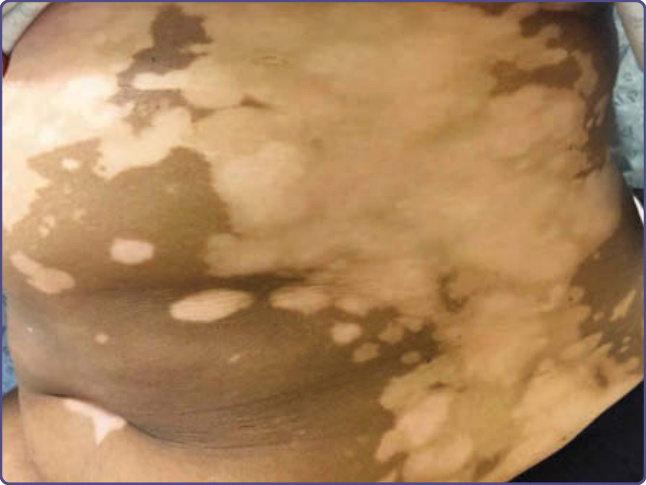
Figure 76-7 Trichrome vitiligo comprised of normal pigmentation, depigmentation, and a zone of hypopigmentation between them.

Figure 76-8 Multiple scattered macules of confetti depigmentation in vitiligo.

Figure 76-9 Inflammatory vitiligo characterized by erythema and scaling at the margin of the depigmented lesion. (Used with permission from Dr. Shyam Verma.)
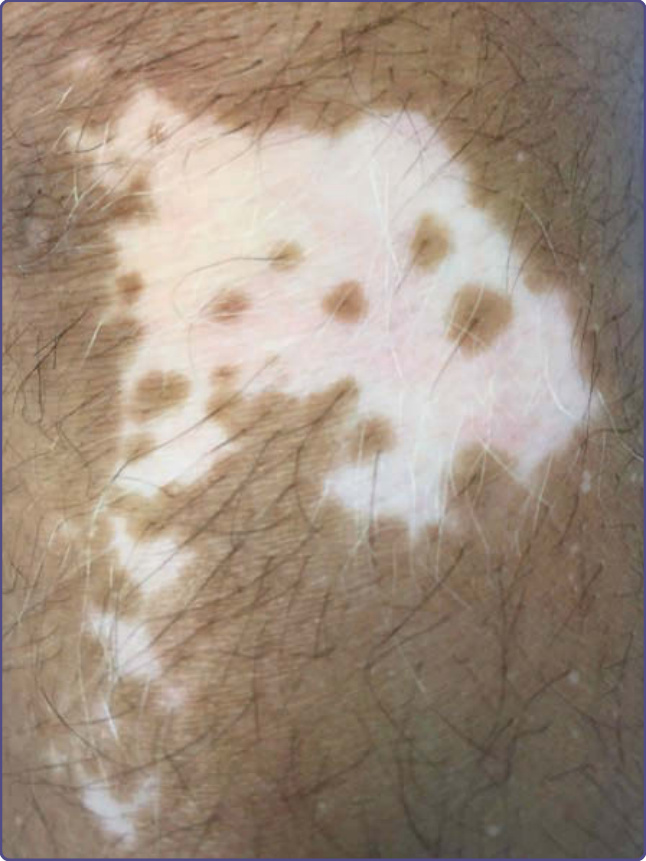
Figure 76-10 Perifollicular repigmentation. Note the lack of repigmentation from white hairs.

Figure 76-11 Marginal repigmentation in glabrous skin.

Figure 76-12 Piebaldism. Note large central midline patch of depigmentation with islands of sparing.

Figure 76-13 Ash-leaf macules in tuberous sclerosis.
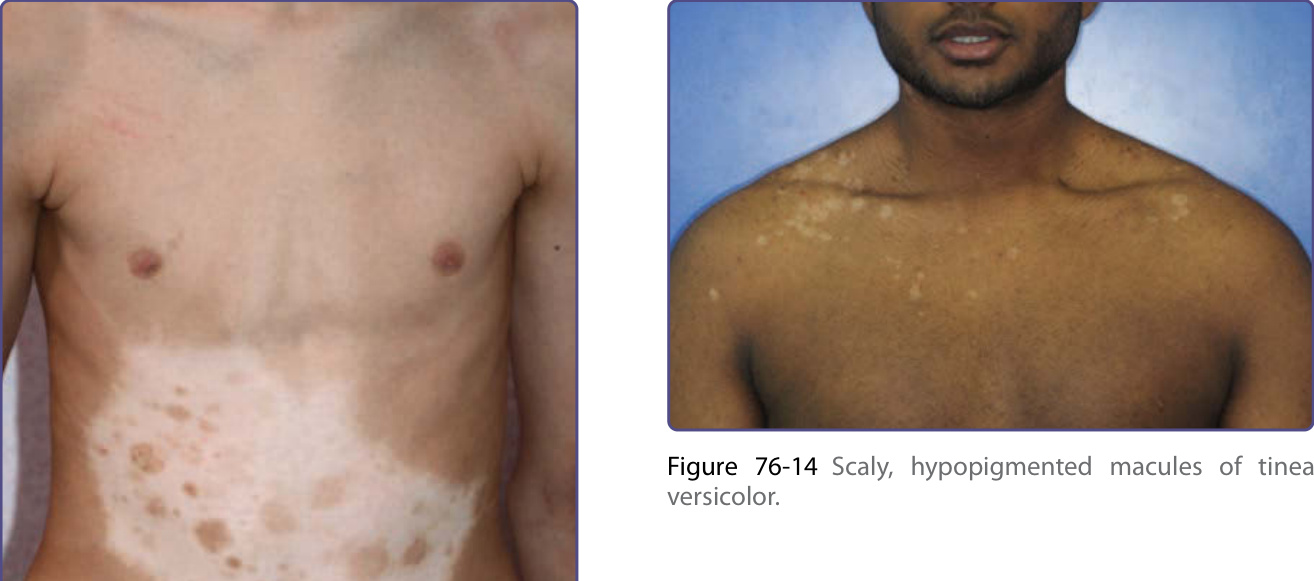
Figure 76-14 Scaly, hypopigmented macules of tinea versicolor.

Figure 76-15 Hypopigmented patches of leprosy.

Figure 76-16 Hypopigmented patches of mycosis fungoides.
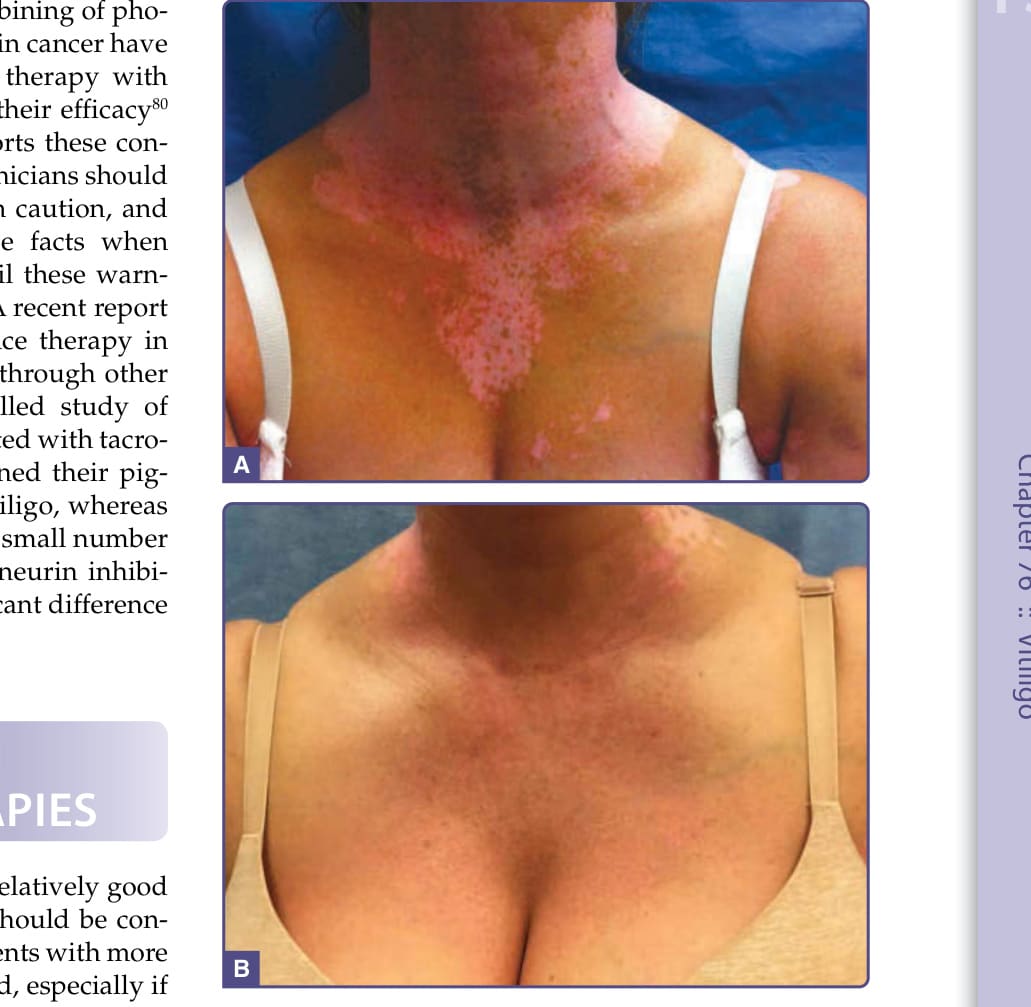
Figure 76-17 Excellent response after about 1 year of narrowband ultraviolet B phototherapy; (A) before and (B) after therapy.
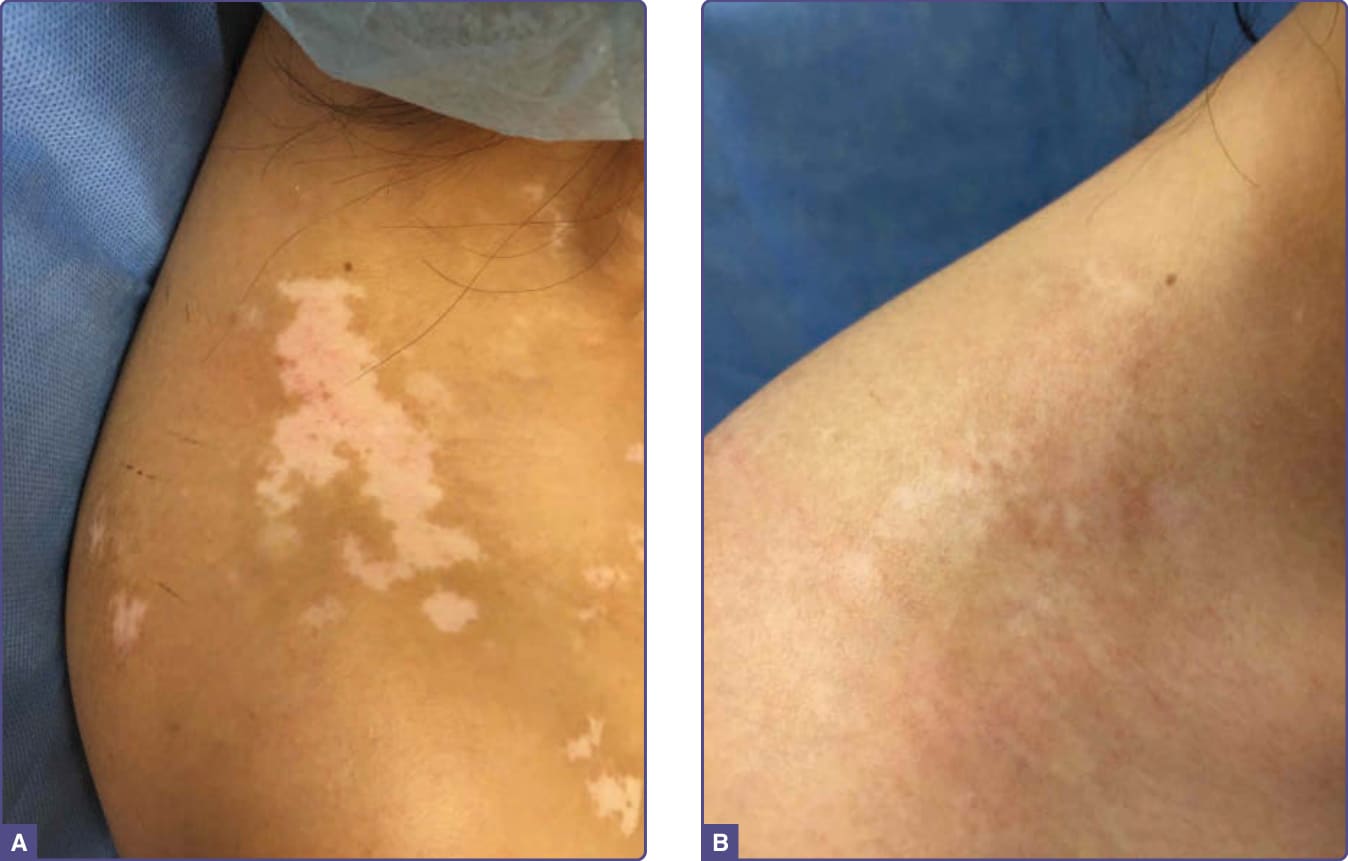
Figure 76-18 Surgical therapy of segmental vitiligo using the melanocyte keratinocyte transplant procedure; (A) before and (B) after therapy.

Figure 76-19 Melanocyte keratinocyte transplant procedure. A, Harvesting of thin skin graft. B, Processing of the skin graft to remove the epidermis and mechanically disrupt it into small pieces. C, Pellet of melanocytes and keratinocytes after centrifugation. D, Dermabraded skin lesions ready for application of cell suspension.
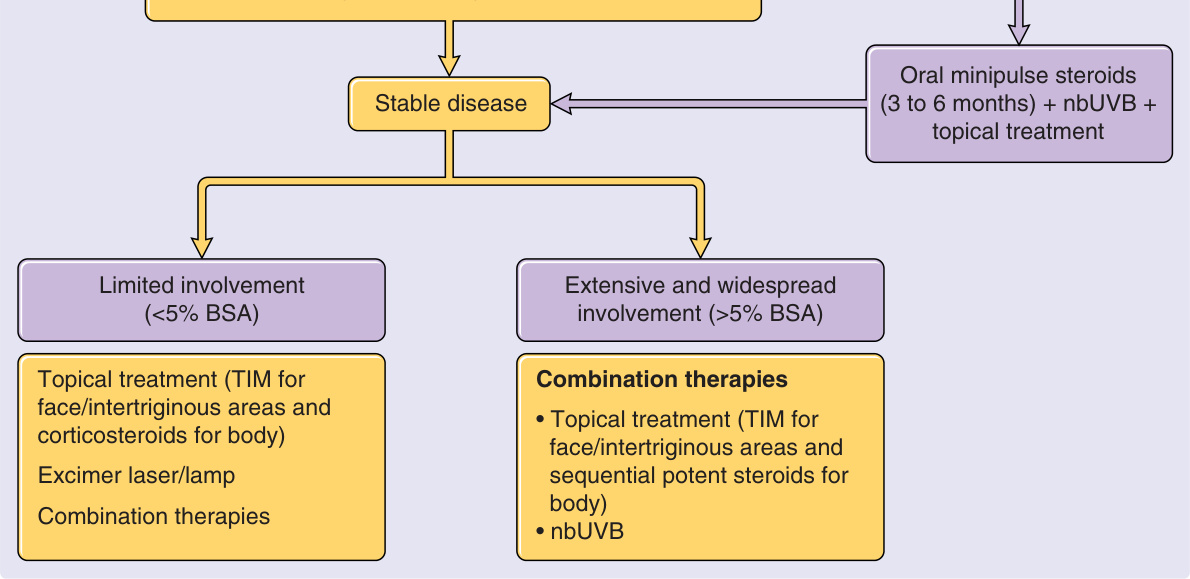
Figure 76-20 Treatment algorithm for vitiligo. BSA, body surface area; nbUVB, narrowband ultraviolet B; TIM, topical immunomodulators.
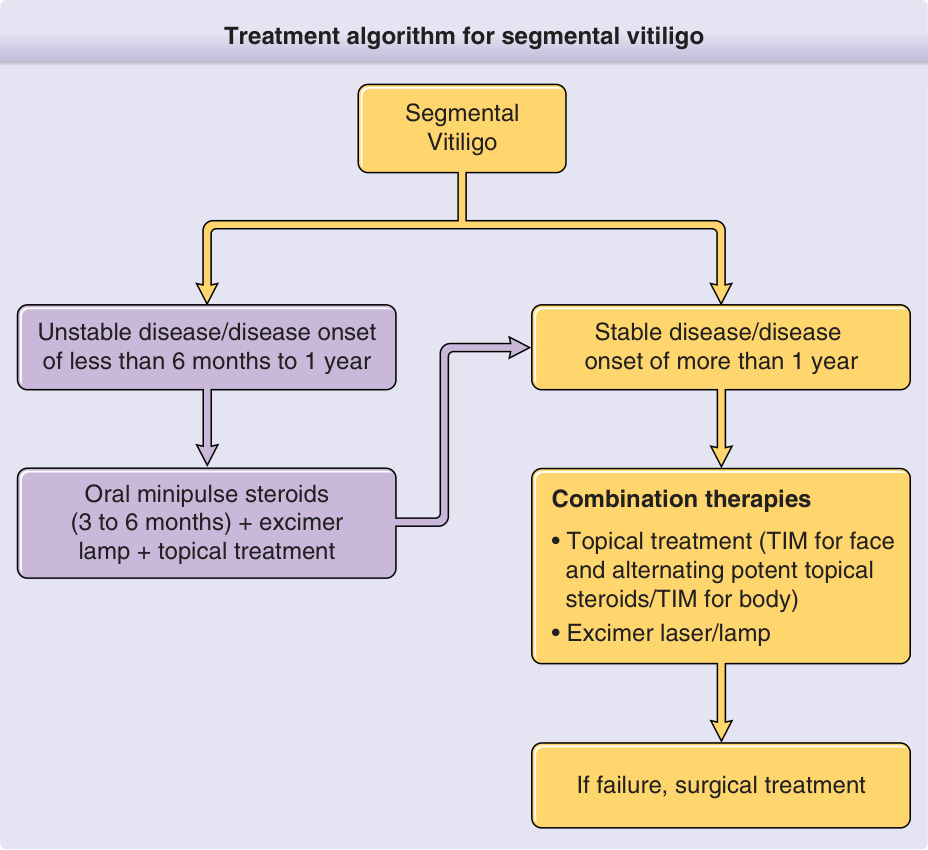
Figure 76-21 Treatment algorithm for segmental vitiligo. TIM, topical immunomodulators.
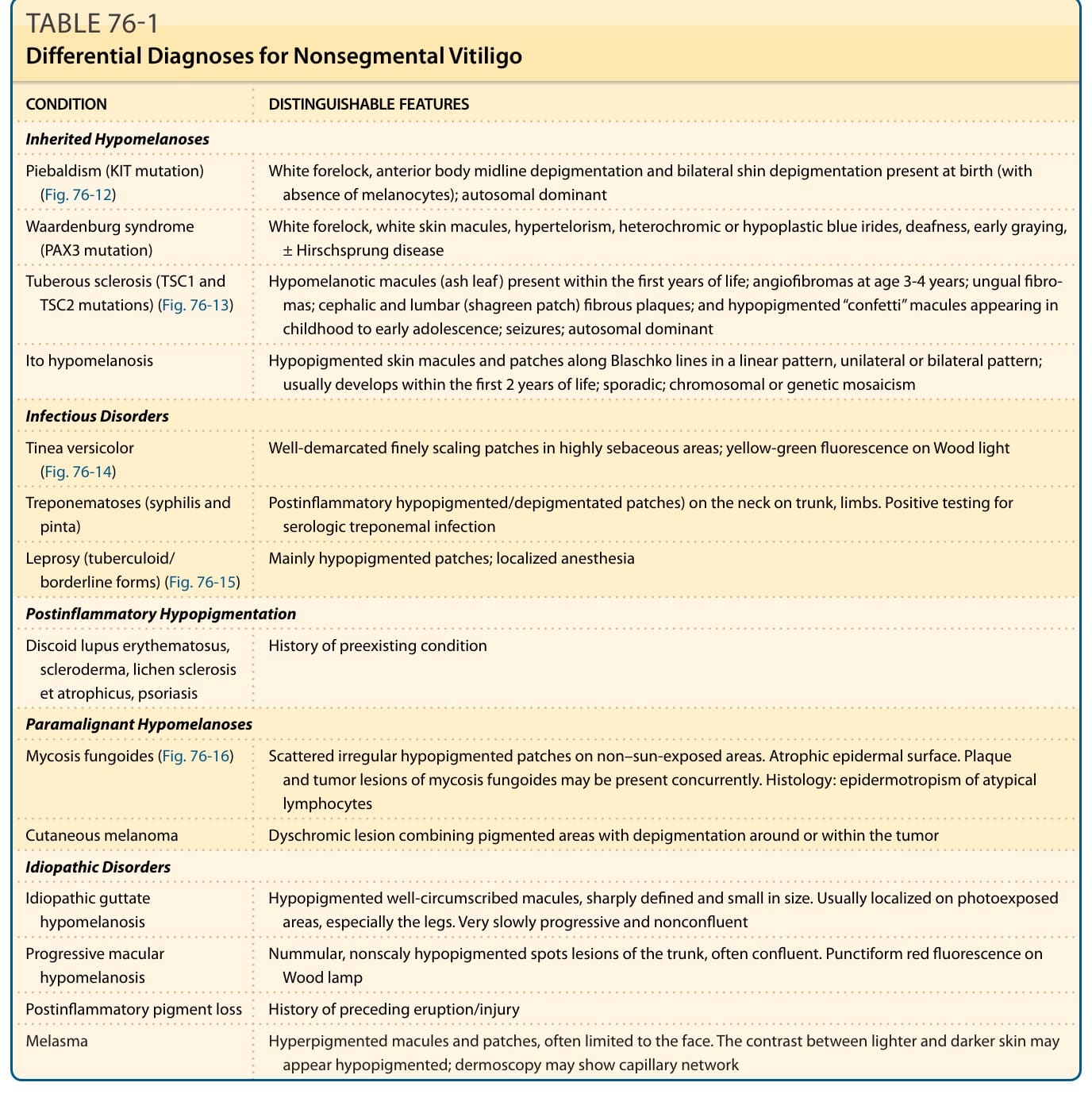
TABLE 76-1 Differential Diagnoses for Nonsegmental Vitiligo
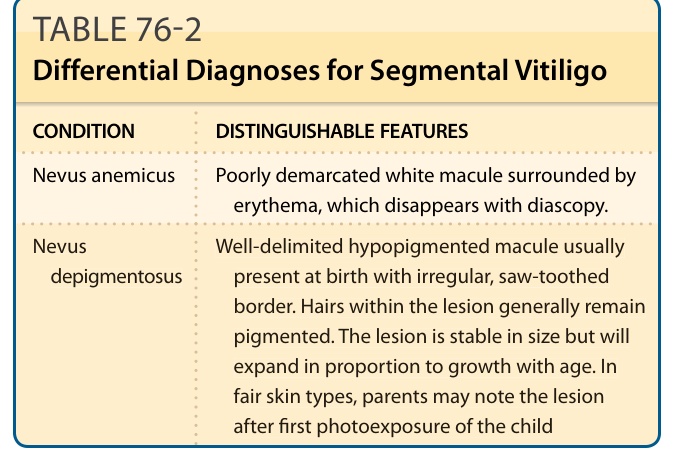
TABLE 76-2 Differential Diagnoses for Segmental Vitiligo