Dermatitis Herpetiformis
9
AT-A-GLANCE
■ Intensely itchy, chronic papulovesicular eruption distributed symmetrically on extensor surfaces.
■ Characterized histologically by dermal papillary collections of neutrophils.
■ Granular immunoglobulin A deposits in normalappearing skin are diagnostic.
■ Epidermal transglutaminases appear to be the dominant autoantigens.
■ Most, if not all, dermatitis herpetiformis patients have an associated gluten-sensitive enteropathy.
■ The rash responds rapidly to dapsone therapy and, in many patients, to strict adherence to a glutenfree diet.
HISTORICAL PERSPECTIVE
In 1884, Louis Duhring first described the clinical features and natural history of a polymorphous pruritic disorder that he called dermatitis herpetiformis (DH); however, the critical elements in the pathogenesis of DH remained unknown until the 1960s.1 In 1888, Brocq described patients with a very similar disorder and called it dermatite polymorphe prurigineuse.2 In addition, he analyzed Duhring’s report and excluded several types of patients from the diagnosis. Since 1888, several important discoveries have been made. In 1940, Costello3 demonstrated the efficacy of sulfapyridine in the treatment of DH. In early 1960s, Pierard and Whimster4 and MacVicar et al5 found that early lesions of DH are characterized by neutrophilic microabscesses in the dermal papillae. In 1967, Cormane6
found that the skin of DH patients contained granular immunoglobulin deposits in dermal papillary tips, and in 1969, van der Meer7 extended these studies and found that the most regularly detected immunoglobulin (Ig) deposited in DH is IgA. The association between DH and intestinal abnormalities was first observed by Marks et al8 in 1966. Fry et al9 and Shuster et al10 identified the intestinal findings as a glutensensitive enteropathy. In 1973, Fry et al11 demonstrated that strict adherence to a gluten-free diet would improve the skin disease as well as reverse the intestinal abnormality, as occurs in celiac disease. Katz et al12
identified a strong association between DH and certain histocompatibility antigens in 1972. In 1979, Jablonska and Chorzelski13 distinguished those patients with linear IgA deposits from those with granular IgA deposits and defined a distinct entity. In 1999, Dieterich et al14
identified antibodies to tissue transglutaminases in the sera from DH patients. Distinguishing between various types of transglutaminases enabled Sárdy et al,15
in 2002, to demonstrate that epidermal transglutaminase (eTG) is the dominant autoantigen in DH. In 2016, Görög et al16 demonstrated circulating transglutaminase 3–IgA immune complexes in DH patients.
EPIDEMIOLOGY
The prevalence of DH in various white populations varies between 10 in 100,000 persons and 75 in 100,000 persons.17-19 The male-to-female ratio ranges from 1.1 to 1 to 1.5 to 1. It may start at any age, including in childhood; however, the second, third, and fourth decades of life are the most common ages. After presentation, DH persists indefinitely in most patients, although with varying severity. Patients with DH have an associated glutensensitive enteropathy (celiac disease) that is usually asymptomatic.
CLINICAL FEATURES
CUTANEOUS FINDINGS
CUTANEOUS FINDINGS
The primary lesion of DH is an erythematous papule, an urticaria-like plaque, or, most commonly, a vesicle (Figs. 59-1, 59-2, and 59-3). Large bullae occur infrequently. Vesicles, especially if they occur on the palms, may be hemorrhagic. The continual appearance and disappearance of lesions may result in hyperpigmentation and/or hypopigmentation. Patients may present with only crusted lesions, and a thorough search may not reveal a primary lesion. The herpetiform (herpes-like) grouping of lesions is often present in some areas (Figs. 59-1 and 59-3), but patients also may have many individual nongrouped lesions. Symptoms vary considerably from the usually severe burning and itching in most patients to the almost complete lack of symptoms in a rare patient. Most patients usually can predict the eruption of a lesion as much as 8 to 12 hours before its appearance because of localized stinging, burning, or itching. The usual symmetric distribution of lesions on elbows, knees, buttocks, shoulders, and sacral areas is seen in most patients at one time or another (Figs. 59-1 to 59-4). Although these regions are affected most commonly, most patients have scalp lesions and/or lesions in the posterior nuchal area. Another commonly affected area is the face, especially along the mandible, on the upper eyelid, and facial hairline. Mucous membrane lesions are rare.
NONCUTANEOUS FINDINGS
NONCUTANEOUS FINDINGS
GASTROINTESTINAL FINDINGS
Most, if not all, DH patients have an associated GI abnormality that is caused by gluten sensitivity.8-10,20
9
The pathology of the gluten-sensitive enteropathy (gluten-sensitive enteropathy) is described below.
MALIGNANCY
Most large studies have reported a significant increase in non-Hodgkin lymphomas in patients with DH and an occasional GI lymphoma, but no other increased risk of malignancy.21-23 Retrospective studies suggest a protective role for a gluten-free diet against GI lymphomas.24 Hervonen and coworkers reported that 11 (1%) of 1104 patients with DH developed a
Dermatitis herpetiformis
1003
9
lymphoma from 2 to 31 years after the diagnosis of DH.25 Of interest, only 2 lymphomas were of the enteropathy-associated type, whereas 8 were B-cell type lymphomas and 1 was unclassified. The patients with DH who developed lymphoma had adhered to a gluten-free diet less strictly than did patients without lymphoma.25 Of interest, the mortality rate for patients with DH was equal to or lower than in the general population.23,26 Lewis et al used the General Practice Research Database in the United Kingdom to study a cohort of 846 DH patients and 4225 matched controls. They report no increased risk of malignancy in the DH patients. They suggest a population bias of hospitalized patients in smaller studies resulted in either differences in the degree of intestinal inflammation or unrelated illnesses increasing frequencies of malignancy in the DH patients.26 These studies suggest that patients with DH may not have an increased risk of malignancy.
OTHER DISEASES
In addition to celiac disease, atrophic gastritis, and pernicious anemia, DH patients have a higher incidence of other autoimmune diseases, such as thyroid disease, insulin-dependent diabetes, lupus erythematosus, Sjögren syndrome, and vitiligo.27-29 This predilection for associated autoimmune diseases may be a result of the high frequency of the 8.1 ancestral haplotype in these DH patients.30 Neurologic disease has been reported in patients with isolated celiac disease, including epilepsy, ataxia, opsoclonus-myoclonus, and dementia; however, confirmation of these findings awaits confirmation with large epidemiologic studies.31,32 Some authors have proposed that patients with DH may be at higher risk for these neurologic complications as a consequence of longstanding ingestion of gluten; however, Wills and coworkers found no evidence of immune-mediated neurologic disease in their evaluation of patients with DH.33
Patients with untreated celiac disease also have been found to have an increased frequency of bone loss.34 Patients with DH frequently continue on glutencontaining diets with a longstanding, albeit low grade, malabsorption. Di Stefano et al demonstrated a significantly reduced bone mineral density in patients with DH on gluten-containing diets.35 Other studies have refuted this and still others have found no increase in fracture rate in patients with DH.27,36
ETIOLOGY AND PATHOGENESIS
Gluten, a protein found in wheat, barley, and rye, plays a critical role in the pathogenesis of DH. Oats, long thought to contain gluten and play a role in inducing DH lesions, are devoid of toxicity in patients with DH.37,38 As in celiac disease, there is an increased density of small bowel intraepithelial T cells with a γ/δ T-cell receptor in the jejunum of patients with DH.39 The finding that T-cell lines from patients with DH
1004
produce significantly more interleukin (IL) 4 than those from patients with celiac disease and that gut biopsies from symptomatic patients with isolated celiac disease show increased expression of interferon-γ suggests that different cytokine patterns may play a role in the varied clinical manifestations of these 2 diseases.40,41 Systemic evidence of the gut mucosal immune response has also been found in the serum and the skin of patients with DH. Patients with DH on regular gluten-containing diets have increased serum IL-2 receptor levels and serum IL-8 levels, increased endothelial cell E-selectin expression in skin, and an increased expression of CD11b on circulating neutrophils.42-44 These systemic manifestations of the gut mucosal immune response may play a role in creating the proinflammatory environment in the skin necessary for the development of skin lesions. The enteropathy seen in DH patients probably relates to the IgA deposits that are found in the skin of these patients, although a direct relationship has not been demonstrated. Patients with a clinical picture consistent with DH and partial IgA deficiency have been reported.45
eTGs appear to be the dominant autoantigens in DH.14,15 Dermal deposits of eTG have been shown to colocalize with cutaneous deposits of IgA, in the papillary tips and because eTGs are strongly expressed in the upper epidermis, it has been suggested that in regions of trauma they may diffuse through the basement membrane after release from epidermal keratinocytes.46 eTGs were also found in uninvolved skin at least 5 cm away from the lesion suggesting additional factors involved in the production of DH lesions.46 It is also known that patients with both gluten-sensitive enteropathy and DH have circulating IgA antibodies directed against eTGs.14,47 There appears to be a predilection for these circulating IgA autoantibodies to bind to eTG in DH, whereas the predilection is for autoantibodies to bind tissue transglutaminases in patients with celiac disease.15 The precise role of the circulating IgA anti-eTG in the development of skin lesions in patients with DH is not known but circulating IgA anti-eTG does decrease after the institution of a gluten-free diet.48 However, children with celiac disease have lower levels of circulating IgA anti-eTG when compared to adults with celiac disease, whereas levels of circulating IgA antibodies against tissue transglutaminase are not significantly different between children and adults with celiac disease.49 This observation has led to the hypothesis that epitope spread over time results in the development of IgA anti-eTG and that this late onset of IgA anti-eTG antibodies may play a role in the typical development of DH in the second to third decade of life.49 The mechanism whereby the IgA anti-eTG binds to skin in patients with DH is not fully understood. One longstanding hypothesis is that IgAcontaining circulating immune complexes are responsible for the IgA deposits in DH skin. The discovery of IgA anti-eTG antibodies has led to the suggestion that IgA–eTG immune complexes may be depositing in the skin of DH patients. This concept has recently received considerable traction in that circulating IgA–TG immune complexes have been identified in DH patients
at higher levels before instituting a gluten-free diet.16
It is possible that the IgA anti-eTG binds initially via antigen–antibody circulating immune complexes and that ability of transglutaminase to crosslink proteins results in the IgA crosslinking to dermal proteins, perhaps fibrin or fibrinogen, resulting in the stable, longlasting IgA deposits seen in the skin of patients with DH.50 This hypothesis awaits confirmation. Whether the IgA skin deposits play a role in the pathophysiology of blister formation is not known. The finding of IgA and complement in almost all skin sites, not only in lesional skin, makes one postulate that if IgA (either alone or as a part of an immune complex) does play a role, additional factors are still needed to explain the initiation of lesions. Takeuchi et al demonstrated that minor trauma to skin results in increased expression of IL-8 and E-selectin, both of which may predispose to a neutrophilic inflammatory infiltrate.51 These findings, coupled with the typical appearance of DH lesions on extensor surfaces at sites of trauma, suggest that local cytokine/chemokine production after trauma may be one of the inciting factors of DH skin lesions. It may be that after the initial neutrophilic infiltrate binds to the cutaneous IgA, factors such as cytokines, chemokines, and proteases are released that both directly result in blister formation and induce basal keratinocytes to produce collagenases or stromelysin-1 that further contributes to the formation of blisters.52,53 Other studies suggest that T cells may play a role in the pathogenesis of the skin lesions; however, no specific T-cell responses to gluten have been detected.54,55
It has been known for some time that iodides, administered orally, can exacerbate or elicit eruptions of DH, and this has, in former times, been used for diagnostic purposes. The availability of immunopathologic techniques for the detection of IgA deposits in skin has made such provocation tests obsolete. There is a marked increase in the incidence of certain major histocompatibility complex antigens in patients with DH. Worldwide studies have found that 77% to 87% of DH patients have human leukocyte antigen (HLA)-B8 (compared with 20% to 30% of unaffected individuals).12,55,56,57 In addition, the class II major histocompatibility complex antigens HLA-DR and HLA- DQ are associated with DH even more frequently than is HLA-B8.58,59 Park et al60 reported that more than 90% of patients expressed Te24, which was later shown to be similar to HLA-DQw2; this finding has been confirmed by others. Molecular studies indicate that susceptibility to DH is not associated with a unique HLA-DQw2 molecule.61,62 Virtually all patients with DH have genes that encode the HLA-DQ (α1∗0501, β1∗02) or the HLA- DQ (α1∗03, β1∗0302) heterodimers, a pattern identical to that seen in celiac disease.61,63 This strong association between susceptibility genes and DH and celiac disease is important clinically and pathophysiologically in that there is a strong concordance of these 2 diseases in monozygotic twins.62 Furthermore, first-degree relatives of both DH and celiac disease patients are often (4% to 5%) affected with one or the other of these diseases.64 Non–major histocompatibility complex susceptibility genes are also associated with DH.
9
DNase-hypersensitivity regions 1 and 2, which function as enhancers for the Ig heavy-chain regulatory region, are found with higher frequencies in DH patients.65
Marietta et al have reported an HLA-DQ8 transgenic nonobese diabetic mouse that when immunized with gluten developed neutrophilic skin lesions along with cutaneous deposits of IgA; withdrawal of dietary gluten resulted in resolution of the skin lesions.66
Although differences between the animal model and DH in patients exist, further investigation of this mouse model may provide important information regarding the pathogenesis of DH.
DIAGNOSIS
LABORATORY TESTING
LABORATORY TESTING
DIRECT IMMUNOFLUORESCENCE
After Cormane demonstrated that both perilesional and uninvolved skin of patients with DH contained granular Ig deposits located in dermal papillary tips, van der Meer found that the most regularly detected Ig class in DH skin was IgA (Fig. 59-5).6,7 Although most patients have granular IgA deposits in their skin, some deposits have a more distinct fibrillary pattern of IgA deposits.67 For the most part, IgA deposits have not been seen in the skin of patients with celiac disease except for the study of Cannistraci et al.68,69
1005
9
The significance of the latter findings in the pathogenesis of DH is not known.69
Finding granular IgA deposits in normal-appearing skin is the most reliable criterion for the diagnosis of DH.70,71 These IgA deposits are unaffected by treatment with drugs, but may decrease in intensity or disappear after long-term adherence to a gluten-free diet.72,73 The IgA deposits are not uniformly intense throughout the skin and may be detected more easily in normalappearing skin near active lesions.74 In DH, other immunoglobulins are sometimes bound to the skin in the same areas as the IgA.71 IgA deposits also may be seen in the skin of patients with bullous pemphigoid, scarring pemphigoid, Henoch-Schönlein purpura, and alcoholic liver disease, although in different patterns of distribution than those seen in DH. Because of the IgA skin deposits and the association between DH and celiac disease, several groups have studied the IgA subclasses in DH. IgA1 is the predominant (or exclusive) subclass that has been identified in the skin of DH patients.75,76 Most IgA1 is produced in the bone marrow, whereas most IgA2 is produced at mucosal sites. This does not negate the possibility that the IgA1 in skin may still be of mucosal origin because IgA1 is the predominant IgA subclass of IgA antibodies directed against dietary proteins produced in gut secretions in patients with DH.77,78
Kantele et al reported a DH association with an increase in circulating IgA1-plasmoblasts with skinhoming receptors (CLA) as compared to those with IgA2.78 The third component of complement (C3) is frequently found in the same location as IgA. The presence of C3 in both perilesional and normal-appearing skin is not affected by treatment with dapsone (diaminodiphenyl sulfone), but C3 may not be detectable after treatment with a gluten-free diet.73,80 C5 and components of the alternative complement pathway also may be seen in areas corresponding to the IgA deposits. The C5–C9 membrane attack complex, which is formed as the terminal event in complement activation, is also seen in normal-appearing and perilesional skin of patients.81 The exact site of the IgA deposits in DH skin has been studied by immunoelectron microscopy. Early studies indicated that IgA is preferentially associated with bundles of microfibrils and with anchoring
A
fibrils of the papillary dermis immediately below the basal lamina.82,83 Other studies, however, indicate that some or almost all of the IgA deposits are related to nonfibrillar components of skin and other connective tissues.83-85 There is also no agreement as to whether the IgA deposits in DH colocalize to fibrillin, a major component of the elastic microfibrillar bundles.85,86
SERUM STUDIES
Chorzelski et al described an IgA antibody that binds to an intermyofibril substance (endomysium) of smooth muscle.87 Sárdy et al showed that these IgA autoantibodies have specificity for transglutaminase, particularly for eTG.15 Although a majority of DH patients on gluten-containing diets have circulating anti eTG antibodies, and this serum assay is thought to be quite sensitive, a significant number of patients do not have circulating anti-eTG antibodies.49,88,89
PATHOLOGY
The histology of an early skin lesion (clinically nonvesicular) is characterized by dermal papillary collections of neutrophils (microabscesses), neutrophilic fragments, varying numbers of eosinophils, fibrin, and, at times, separation of the papillary tips from the overlying epidermis (Fig. 59-6). In addition, in such early lesions, the upper and middle dermal blood vessels are surrounded by a lymphohistiocytic infiltrate, as well as some neutrophils and an occasional eosinophil.4,5 At times, early lesions may be difficult or impossible to differentiate from those of linear IgA disease (see Chap. 58), the bullous eruption of lupus erythematosus (see Chap. 61), bullous pemphigoid (see Chap. 54), or the neutrophil-rich form of epidermolysis bullosa acquisita (see Chap. 56). The histology of older lesions shows subepidermal vesicles that may be impossible to differentiate from other subepidermal bullous eruptions, such as bullous pemphigoid, erythema multiforme, bullous drug eruption, and pemphigoid gestationis. Immunofluorescent localization and ultrastructural studies of the site of blister formation in DH demonstrate that the blister forms above the
B
1006
lamina densa, within the lamina lucida. This is thought to occur because the lamina lucida is the most vulnerable component of the dermal–epidermal junction.90
The pathology of the DH-associated enteropathy is essentially the same as seen in celiac disease that is unassociated with DH, although the lesion in the latter is usually much more severe; this applies to the epithelial cell derangement as well as to the character of the lymphoplasmacytic infiltrate. Over the past 45 years the prevalence of severe villous atrophy in DH patients has decreased in Finland.91 The distribution of the GI lesion in the small intestine is, as a general rule, more widespread in celiac disease. The functional changes in the bowel and clinical sequelae encountered in the enteropathy associated with DH and those seen in celiac disease are similar but again differ in degree, those in the latter being more severe. Thus, in DH one observes steatorrhea (20% to 30% of patients), abnormal D-xylose absorption (10% to 33% of patients), and occasional anemia secondary to iron or folate deficiency. In patients not taking dapsone or related drugs, the anemia is usually caused by malabsorption. In addition to the small intestinal lesion, patients with DH have an increased incidence of achlorhydria and atrophic gastritis.92,93 Reports of pernicious anemia and antibodies to gastric parietal cells are thus likely to be more than the result of chance.
DIFFERENTIAL DIAGNOSIS
DH may be confused with numerous other conditions because of its pleomorphic manifestations and the occasional lack of diagnostic lesions (Table 59-1). Neurotic excoriations, eczema, papular urticaria, transient acantholytic dermatosis, pemphigoid, pemphigoid gestationis, erythema multiforme, and various other dermatoses can be differentiated easily on the basis of histologic and immunologic criteria. Linear IgA disease may be more difficult to differentiate clinically and histologically, but it is distinctive immunologically. A high index of suspicion is very helpful in that even in the absence of primary lesions, DH can be diagnosed based on the typical in vivo–bound granular IgA deposits in normal-appearing skin.
Consider
■Eczema
■Atopic dermatitis
■Papular urticaria
■Neurotic excoriations
■Bullous pemphigoid
■Pemphigoid gestationis
■Linear immunoglobulin A dermatosis
■Atopic dermatitis
Rule Out
Rule Out
■Scabies
■Scabies
9
CLINICAL COURSE AND PROGNOSIS
After presentation, DH persists indefinitely in most patients, although with varying severity. A rare patient will have extreme waxing and waning of disease whereby they may be free of disease for up to a year at a time even without treatment. Two long-term studies of immunologically verified patients have suggested that the disease in approximately 10% to 12% of DH patients eventually remits.94,95 Nonsteroidal antiinflammatory drugs may cause an exacerbation of the DH even in those who disease is well controlled with either dapsone or gluten-free diet.96
MANAGEMENT
SULFONES
SULFONES
Diaminodiphenyl sulfone (dapsone), sulfoxone (diazone—not available in the United States), and sulfapyridine (not generally available in the United States) provide prompt improvement in symptoms and signs of the disease. Symptoms may abate in as few as 3 hours or as long as a few days after the first pill is taken, and new lesions no longer erupt after 1 to 2 days of treatment. Exacerbations occur from hours to days after cessation of treatment. This response to therapy was, for a long time, the most important element in making a diagnosis. The preferred treatment for an adult is dapsone at an initial dosage of 100 to 150 mg/day (this usually can be taken once a day). A rare patient may require 300 to 400 mg of dapsone for initial improvement. Patients should be instructed to take the minimal dose required to suppress signs and symptoms. Not all patients require daily treatment; in rare cases, 25 mg weekly is sufficient. Sulfapyridine, in a dosage of 1.0 to 1.5 g daily, is particularly useful in patients intolerant of dapsone, in elderly patients, and in those with cardiopulmonary problems. The pharmacology, mechanism(s) of action, adverse effects, and monitoring of dapsone are discussed in Chap. 187.
GLUTEN-FREE DIET
GLUTEN-FREE DIET
EFFECT ON THE SMALL INTESTINE
The intestinal lesion in DH responds to dietary gluten withdrawal. The time course of the response in adults with DH is the same as that in adults with celiac disease.
EFFECT ON THE SKIN DISEASE
Strict adherence to a gluten-free diet will, after variable periods of time (from 4 months to 1 year), reduce or completely eliminate the requirement for medication
1007
9
in most, but not all, patients. The most extensive early study by Fry et al has been confirmed by several groups.97 However, it is only the very highly motivated patient who can adhere to the diet, which requires counseling by a dietitian who is very familiar with its use. The general availability of gluten-free foods (and standardized labelling in the United States) in most food markets has made adherence to this diet much easier than in previous times. Despite this, there are still patients who remain refractory to gluten-free diet treatment.97
ELEMENTAL AND OTHER DIET THERAPY
ELEMENTAL AND OTHER
DIET THERAPY
Studies in small numbers of DH patients have indicated that elemental diets (composed of free amino acids, short-chain polysaccharides, and small amounts of triglycerides) can be very beneficial in alleviating the skin disease within a few weeks.98,99 The beneficial effect on the skin disease may be achieved even if the patient ingests large amounts of gluten.100 Unfortunately, elemental diets are difficult to tolerate for long periods. Interestingly, complete resolution of the skin lesions of DH has also been reported by adherence to the high-protein, unlimited fat, low-carbohydrate diet popularized as the “Atkins Diet.”100 Further studies are needed to confirm this report.

Figure 59-1 Extensive eruption with grouped papules, vesicles, and crusts on the back.

Figure 59-2 Papules, vesicles, and crusts on knees.

Figure 59-3 This patient has many firm-topped vesicles and bullae, some erosions, and residual hyperpigmentation. Some of the vesicles are arranged in an annular pattern.
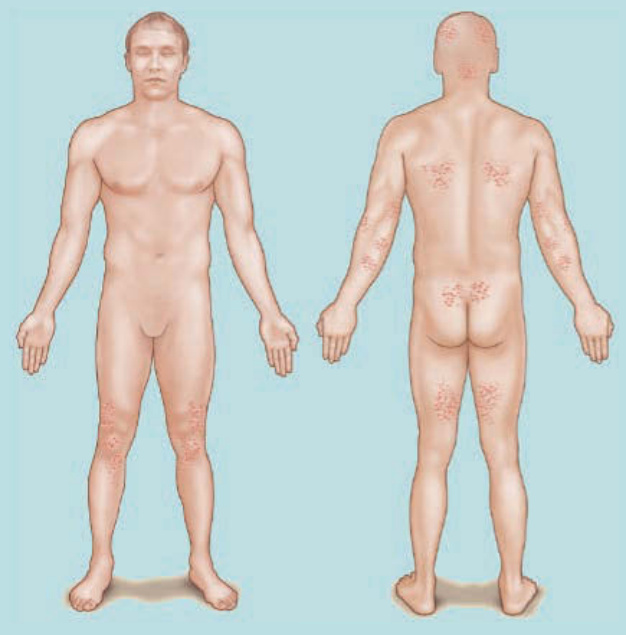
Figure 59-4 Pattern of distribution.
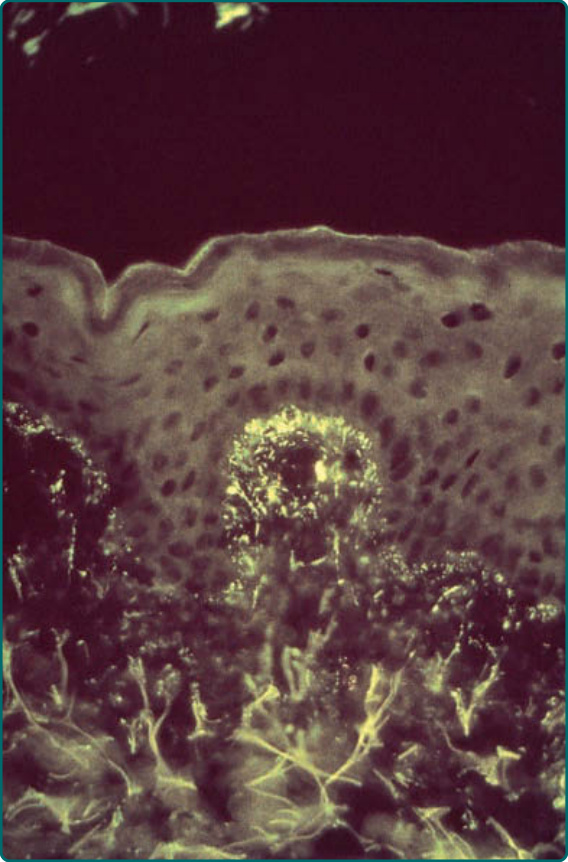
Figure 59-5 Direct immunofluorescence showing granular dermal papillary deposits of immunoglobulin A.
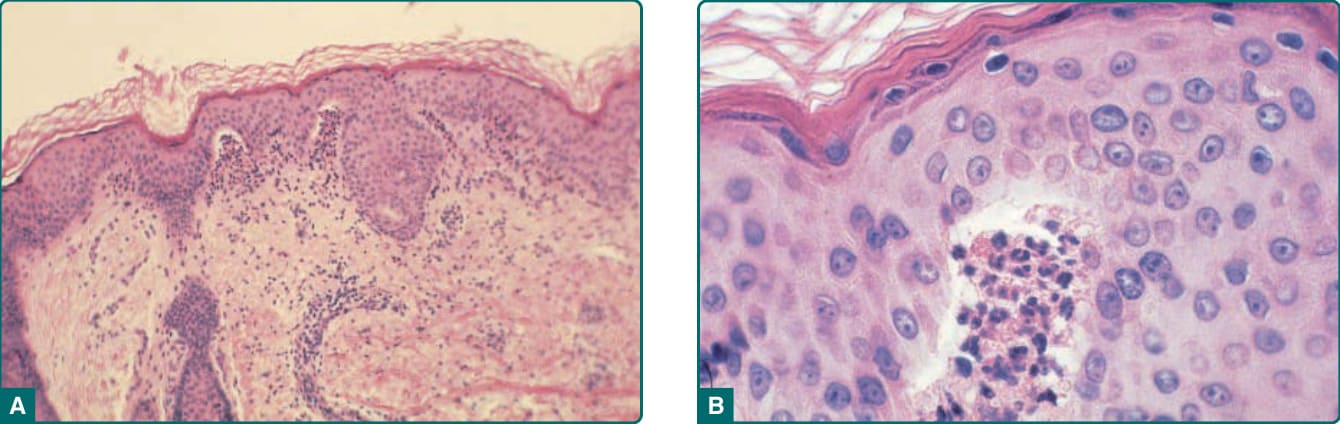
Figure 59-6 Biopsy of an early lesion showing dermal papillary collections of neutrophils and eosinophils and subepidermal vesiculation at low (A) and high (B) magnification.