Urticaria and Angioedema
6
AT-A-GLANCE
■ Urticaria is defined as a skin disorder characterized by local transient skin or mucosal edema (wheal) and an area of redness (erythema) that typically accompany itchy sensations and diminish within 1 day.
■ Symptoms may occur either spontaneously (spontaneous or idiopathic urticaria) or in response to specific stimuli, such as physical stimuli or sweating (the increase of body core temperature).
■ Mast cells and their histamine being released either spontaneously or in response to various stimuli play a crucial role in the pathogenicity of urticaria.
■ Spontaneous or idiopathic urticaria is the subtype of urticaria that most patients experience.
■ Autoantibodies against immunoglobulin (Ig) E or the high-affinity IgE receptor (FcεRI) that activate mast cells and basophils and induce histamine release may be detected in up to half of patients with chronic spontaneous or idiopathic urticaria (type II autoimmunity).
■ A certain population of patients may develop angioedema mediated by bradykinin rather than histamine.
■ Infections, stress, fatigue, and drugs, especially nonsteroidal antiinflammatory drugs and angiotensin-converting enzyme inhibitors, may cause or aggravate urticaria or angioedema.
■ However, the mechanism of mast cell activation or the exacerbation of urticaria by various factors, except for exogenous antigens and autoantibodies, remains largely unknown.
■ Nonsedative second-generation antihistamines are the mainstay of pharmaceutical therapy.
■ Omalizumab, anti-IgE antibody, or immunosuppressive medications may be taken for the treatment of urticaria and angioedema that is refractory to antihistamines even at high doses.
INTRODUCTION
DEFINITIONS
DEFINITIONS
Urticaria is defined as a skin disorder characterized by local transient skin or mucosal edema (wheal) and an area of redness (erythema) that typically accompany itchy sensations and diminish within
a day. Angioedema is a local and transient skin or mucosal edema that develops in deep tissues mostly without itching but may accompany pain or burning sensations. Both wheals and angioedema may develop together in one patient, but either one may develop exclusively in individual patients. Whereas the term urticaria is used as an entity of disease, angioedema may mean either disease or eruption. Either wheals and angioedema or both may appear as a symptom of other disease entities, such as anaphylaxis (either wheals or angioedema), autoinflammatory syndromes (wheals), mastocytosis (wheals known as Darier sign) or hereditary angioedema (HAE; angioedema). The international guidelines advocated by the European Academy of Allergy and Clinical Immunology (EAACI)/Global Allergy and Asthma European Network (GA2LEN)/European Dermatology Forum (EDF)/World Allergy Organization (WAO) (EAACI guideline) define urticaria as a disease characterized by the development of wheals (hives), angioedema, or both and distinguishes urticaria from medical conditions in which wheals, angioedema, or both can occur as a symptom, such as a skin prick test, anaphylaxis, autoinflammatory syndromes, or HAE (bradykinin-mediated angioedema).1
HISTORICAL PERSPECTIVE
HISTORICAL PERSPECTIVE
The school of Hippocrates first described the association of urticaria with nettles and insect bites.2 Stinging nettle (Urtica dioica) contains histamine-, serotonin-, and acetylcholine-containing fluids inside the spicules and causes contact urticaria-like symptoms.3 Therefore, the name “nettles” frequently appeared in several languages until the middle of the 19th century. The word “urticaria” was first used in 1792 by Johann Peter Frank to describe the disease.2 In 1878, Paul Ehrlich first described aniline-positive cells in connective tissues and named them “Mastzellen (well-fed cells).”4
In 1910, Henry Dale clarified the physiological role of histamine on smooth muscle.5 In 1913, Hans Eppinger showed that wheals, erythema, and pain developed at sites of local injections of histamine.6 In 1937, Daniel Bovet7 developed antihistamine, which became the mainstay of treatment for urticaria. In 1953, James F. Riley showed that mast cells are the main source of histamine in the skin.8 In 1966, Kimishige Ishizaka identified immunoglobulin (Ig) E and clarified its role in type I hypersensitivity, the pathological mechanism of allergic urticaria.9
EPIDEMIOLOGY
Studies in Europe reported the lifetime prevalence (prevalence during the whole lifetime until the investigation) of urticaria as around 8% to 10%.10-12
Hellgren found a point prevalence (prevalence at the time of the investigation) of around 0.1% in the total population of Sweden,13 and more recently, Gaig and coworkers reported a point prevalence of 0.6% in the Spanish population.14 The reason for such large variations in the prevalence among reports is unclear, but possible explanations include differences in the methods employed, definition of urticaria, and geographical and cultural characteristics. Many cases of urticaria that diminish within a few weeks or develop on just a single or a few occasions may be overlooked and not included in some survey results. Chronic spontaneous urticaria (CSU) and inducible urticarias, including physical urticaria, cholinergic urticaria, and contact urticaria, that persist for more than 6 weeks can be grouped as “nonacute” or “chronic” urticaria. One study of the prevalence of CSU with the classification recommended by the EAACI guidelines found a prevalence of 0.8% in a 1-year period in Germany.12 Statistical analysis of patients with nonacute urticaria suggests that 66% to 93% have CSU, 4% to 33% a physical urticaria, and 1% to 7% have cholinergic urticaria.15-18 A limitation of many studies is that they give no information about how they evaluate combinations of multiple subtypes of urticaria. In fact, as many as half of patients with CSU may also have other types of urticaria.19 In addition, CSU can be further divided into that with concomitant angioedema, that without angioedema and that with recurrent angioedema without wheals. The available data suggest that whereas 33% to 67% of all patients with CSU exhibit wheals and angioedema, 29% to 65% exhibit only wheals and 1% to 13% only angioedema.20 Differences in prevalence by race or ethnic group are unknown, but data are scarce.20
Regarding sex, the majority of studies show that women have urticaria nearly twice as often as men do.10,12,13-15,17,18,20-27 This is true not only for CSU but also for many other types of urticaria. Among patients with CSU, the prevalence of a positive autologous serum skin test (ASST) result was reported to be higher in women than in men.28
The peak age of CSU patients is between 20 and 40 years in most studies.16,17,21,23,27,29 A survey of officebased practices for all types of urticaria in the United States reported a bimodal age distribution in patients aged birth to 9 years and 30 to 40 years.30 The first peak may represent the predominance of acute spontaneous urticaria, allergic urticaria (urticarial reactions), and cholinergic urticaria in children. Few data are available concerning the relationship between prevalence of urticaria and socioeconomic status, education, ethnic background or place of residence. A German study showed that people with a high socioeconomic status and those who live in larger cities are more likely to have urticaria.11 However, the deviations were too small to conclude whether the
6
results reflect true variations in prevalence or just differences in disease awareness. Other studies failed to show a difference in the prevalence of urticaria with regard to education, occupation, income, place of residence, and ethnic background.10,12,14,31
CLINICAL FEATURES
CUTANEOUS FINDINGS
CUTANEOUS FINDINGS
Circumscribed, raised, usually pruritic, and evanescent areas of edema that involve the superficial portion of the dermis are known as wheals. A wheal may appear mostly reddish but could also be whitish, especially when edema is significant. Edema that extends into the deep dermis or subcutaneous and submucosal layers is known as angioedema. Urticaria and angioedema may occur in any location together or individually. Angioedema commonly affects the face, especially the eyelids and lips, or a portion of the extremities (Fig. 41-1E). It may be painful but not pruritic and may last for several days. Involvement of the lips, cheeks, and periorbital areas is common, but angioedema also may affect the tongue, pharynx, or larynx. The individual lesions of urticaria arise suddenly, rarely persist for longer than 24 to 36 hours, and may continue to recur for indefinite periods. Most wheals, but not angioedema, are highly pruritic. The size, shape, and color of wheals are quite variable. Wheals on the eyelids and lips and those in the deep dermis in delayed pressure urticaria (DPU) may be difficult to be distinguished from angioedema. Certain subtypes of urticaria have characteristic morphologies. Spontaneous urticarias (acute and chronic) may involve large, small, flowerlike, or annular wheals, and they are usually heterogeneous (Fig. 41-2). The heterogeneity of wheals in size and shape is one of the characteristics of spontaneous urticaria. In severe cases of spontaneous urticaria, wheals may accompany purpura, lasting for a few days. In such cases, urticarial vasculitis should be excluded. In most cases of physical urticarias, wheals develop diffusely within the affected areas (Figs. 41-1A, 41-1B, and 41-1D), but wheals of cholinergic, adrenergic, and aquagenic urticaria are usually small (<5 mm) and disseminated in the provoked area of the skin (Fig. 41-1C). The duration of individual wheals is long in spontaneous urticarias and deep pressure urticaria and shorter in physical urticarias.32 The development of angioedema is rare in physical urticaria but may be observed in cholinergic urticaria.33-35
NONCUTANEOUS FINDINGS
NONCUTANEOUS FINDINGS
During urticarial attacks, patients often feel discomfort of the stomach and intestine. Infections of the gastrointestinal tract may induce urticaria and vice versa. Pharyngeal edema can be seen in angioedema, especially bradykinin-induced angioedema.36 Certain kinds of
685
6
A
C
E
B
D
686
A
C
6
B
D
urticarias, especially inducible ones such as allergic urticaria, and cholinergic urticaria, may develop into anaphylaxis. Anaphylaxis is defined as “a serious, lifethreatening generalized or systemic hypersensitivity reaction” and “a serious allergic reaction that is rapid in onset and might cause death.”37 It mostly, but not always, affects the skin (urticarial rash) and respiratory (dyspnea) and circulatory systems (low blood pressure, syncope). Severe cases of physical urticaria may also include systemic symptoms such as headache, dizziness, syncope, wheezing, and nausea.
COMPLICATIONS
COMPLICATIONS
AUTOIMMUNE THYROID DISEASES
The association between CSU and thyroid autoimmunity has been reported in many studies. The frequency of thyroid autoantibodies in patients with CSU is significantly higher than those in control participants.38,39
The frequency of overt and subclinical thyroid dysfunction was also significantly higher than those of a control Spanish population.39 A subgroup of patients with CSU who possess IgE antibodies against thyroid peroxidase (TPO) might evoke autoallergic degranulation of mast cells.40
OTHER AUTOIMMUNE DISEASES
Patients with CSU exhibit autoimmune diseases other than thyroid autoimmunity. Especially female patients with CSU were reported to have a significantly higher incidence of rheumatoid arthritis, Sjögren syndrome, celiac disease, type I diabetes mellitus, and systemic lupus erythematosus (SLE).41
SUBTYPES OF URTICARIA
SUBTYPES OF URTICARIA
Because there is a large variation in features in urticaria, not only in the pathogenesis but also in terms of management, urticaria has been classified by its various aspects, such as duration, trigger and mode of induction, and underlying causes. The international consensus meeting held in 2013 for making the EAACI guidelines reached a consensus for standard classification. This classification divides urticaria into acute and chronic at 6 weeks from the onset. Chronic urticaria is further classified into spontaneous urticaria and inducible urticaria. The latter is induced by physical stimuli and includes physical urticaria (cold urticaria, DPU, heat urticaria, solar urticaria, symptomatic dermographism, vibratory angioedema), cholinergic urticaria, and contact urticaria (Table 41-1). This classification
687
6
TYPES SUBTYPES ROUTINE DIAGNOSTIC TESTS (RECOMMENDED)
EXTENDED DIAGNOSTIC PROGRAMMEa (BASED ON HISTORY) FOR IDENTIFICATION OF UNDERLYING CAUSES OR ELICITING FACTORS AND FOR RULING OUT POSSIBLE DIFFERENTIAL DIAGNOSES IF INDICATED
Spontaneous urticaria Acute spontaneous urticaria None Noneb
CSU Differential blood count. ESR and/ or CRP Avoidance of suspected triggers (eg, drugs); Conduction of diagnostic tests for (in no preferred order): (i) infectious diseases (eg, Helicobacter pylori); (ii) functional auto-antibodies (eg, autologous skin serum test); (iii) thyroid gland disorders (thyroid hormones and auto-antibodies); (iv) allergy (skin tests and/or allergen avoidance test, eg, avoidance diet); (v) concomitant CIndU, see below; (vi) severe systemic diseases (eg, tryptase); (vii) other (eg, lesional skin biopsy)
Inducible urticaria Cold urticaria Cold provocation and threshold testc,d Differential blood count and ESR or CRP, rule out other diseases, especially infectionse
Delayed pressure urticaria Pressure test and threshold testc,d None
Heat urticaria Heat provocation and threshold testc,d None
Solar urticaria UV and visible light of different wavelengths and threshold testc Rule out other light-induced dermatoses
Symptomatic dermographism Elicit dermographism and threshold testc,d Differential blood count, ESR or CRP
Vibratory angioedema Test with vibration, for example, Vortex or mixerd None
Aquagenic urticaria Provocation testingd None
Cholinergic urticaria Provocation and threshold testingd None
Contact urticaria Provocation testingd None
Contact urticaria Provocation testingd None
aDepending on suspected cause.
bUnless strongly suggested by patient history, for example allergy.
cAll tests are carried out with different levels of the potential trigger to determine the threshold.
dFor details on provocation and threshold testing, refer to Magerl M, Altrichter S, Borzova E, et al. The definition, diagnostic testing, and management of chronic inducible urticarias? The EAACI/GA2LEN/EDF/UNEV consensus recommendations 2016 update and revision.
eFor further info, refer to Maurer M. Cold urticaria. In: Saini SS, Callen J, editors. UpToDate. Boston, MA: Wolters Kluwer Health; 2014. ESR, erythrocyte sedimentation rate; CRP, C-reactive protein. From Zuberbier T, Aberer W, Asero R, et al. The EAACI/GA(2) LEN/EDF/WAO Guideline for the definition, classification, diagnosis, and management of urticaria: the 2017 revision and update. Allergy. 2018;73:1393-1414, with permission. Copyright © 2018 EAACI and John Wiley and Sons.
has been maintained in the guideline updated in 2018.1
In daily practice, wheals or angioedema may also develop as a reaction to certain stimuli or as a symptom of other disease entities. This chapter describes various subtypes of urticaria that require treatment or management in clinical practice even if they are not included in the EAACI guideline. Morphological characteristics of urticaria subtypes are summarized in Table 41-2.
SPONTANEOUS URTICARIA
Spontaneous urticaria is defined as urticaria that occurs spontaneously almost every day without any apparent cause or trigger. The name “idiopathic urticaria” has also been used for the same entity for a long time, but the use of “spontaneous” urticaria has been recommended by the EAACI guidelines and endorsed by many relevant societies.1 The major skin manifestation is wheals, and they may be accompanied by angioedema in up to half of patients.20 In some cases, only angioedema may
688
appear. Compared with superficial wheals, angioedema occurs less frequently, such as every few days, weeks, or months, and the symptoms of angioedema last longer than a day, usually for a few days. The shape, size, and duration of individual wheals are highly variable and heterogeneous as described in the Cutaneous Findings in the section of “Clinical Features” and Fig. 41-2. Flowerlike or annular-shaped wheals are characteristic of this subtype of urticaria. Although symptoms may be very severe and disabling, they are mostly nonlethal. There is no qualitative difference between acute spontaneous urticaria and CSU, but acute forms tend to be more severe. Cutaneous manifestations of urticarial vasculitis and autoinflammatory syndromes may resemble long- lasting wheals observed in this type of urticaria.
SYMPTOMATIC DERMOGRAPHISM
Symptomatic dermographism, also called as urticaria factitia, dermographic urticaria, mechanical urticaria,
6
SPONTANEOUS URTICARIA TYPE (POLYMORPHIC) ANNULAR TYPE, PRUPURIC LESION
CHOLINERGIC TYPE (SMALL (<5 MM) AND DISSEMINATED) LINEAR TYPE
LOCALIZED PROVOKED AREA TYPE MUCOSAL TYPE
Spontaneous urticaria +++ ++ + none to ++a
Type I allergy mediated and many drug-induced urticarias
++ ++ none to ++a
Cold, solar, heat, and deep pressure urticarias +++ none to ±c
Symptomatic dermographism (mechanical urticaria)
+++ ++ none to ±c
Cholinergic, aquagenic, and adrenergic urticarias +++ none to ++a none to +b
Angioedema +++
Angioedema +++
aA spectrum from none to ++.
bA spectrum from none to +.
cA spectrum from non to ±.
or simply dermographism, is the most common subtype among the physical urticarias. Symptomatic dermographism is characterized by itching or burning skin sensations and the development of pruritic wheals and flare in areas exposed to shearing forces on the skin. The shape of wheals and erythema is mostly liner or consists of liner elements because of the forms of eliciting stimuli (see Fig. 41-1A). However, a widespread flare with vague margins may develop when patients extensively scratch the skin (see Fig. 41-1B). In rare and severe cases of symptomatic dermographism, erythematous lines may accompany punctate wheals characteristic of cholinergic urticaria ( cholinergic dermographism).42 Wheals and itch of this urticaria subtype develop shortly after the stimuli and disappear approximately within 30 minutes in most cases. In certain cases of DPU, wheals of symptomatic dermographism may return in the same site or newly develop 3 to 6 hours after stimulation and persist for up to 48 hours (delayed dermographism).43 In some rare cases, wheals may be markedly augmented when the skin is chilled (cold-dependent dermographism).44 There is a case report of this subtype urticaria developing in the genital region during sexual intercourse.45
COLD URTICARIA
Cold urticaria is a physical urticaria being characterized by the appearance of wheals and flare in response to cold. In most cases, local skin contact with a cold substance induces wheals and flare in the area of cold contact (cold contact urticaria). The cutaneous appearance of wheals and flare is typically flat and widely spread but may also be punctate. Itching and wheals of the skin occur within minutes and persist up to 1 hour. In severe cases, the mouth and pharynx may swell after drinking cold liquid. Patients with cold urticaria may also develop anaphylactic symptoms, including palpitations, headache, wheezing, and loss
of consciousness, and drowning may occur after cold water bathing. In rare cases, erythematous edematous and deep swelling may appear 9 to 18 hours after cold challenge (delayed cold urticaria).46
In cases of systemic cold urticaria, widespread wheals and flare develop in response to cooling of the core body temperature, not by the local exposure to cold.47
Systemic cold urticaria may be either idiopathic or secondary to underlying diseases. Patients with familial cold urticaria syndrome develop erythematous macules and infrequent wheals associated with burning and pruritus on exposure to cold; this is now classified as a subtype of cryopyrin-associated periodic syndrome (CAPS), an autosomal dominant inherited disease which is associated with a genetic mutation of NLRP3 (CIASI). It may include headaches, conjunctivitis, and arthralgias. The average delay between cold exposure and onset of symptoms is 2.5 hours, and the average duration of an episode is 12 hours.48 More recently, a new mutation in PLCG2, encoding phospholipase Cγ2, with gain of function has been identified in families with a dominantly inherited complex of cold-induced urticaria, antibody deficiency, and susceptibility to infection and autoimmunity.49 Patients with these hereditary disorders do not develop wheals and flare in response to the local ice-cube test (see the “Diagnosis” section).
HEAT URTICARIA
Heat urticaria is a rare subtype of physical urticaria characterized by wheals and flare that develop within minutes after local heat exposure to the skin and disappear within a few hours at the longest (see Fig. 41-1D). In contrast to cholinergic urticaria that involves small punctate eruptions in response to conditions that elicit sweating, patients with heat urticaria develop wheals and flare that spread in the area of skin exposed to heat, regardless of the core body temperature or sweating.
689
6
SOLAR URTICARIA
Solar urticaria is a rare subtype of physical urticaria characterized by wheals and flare that develop within minutes after local exposure of the skin to certain wavelengths of light. The urticarial lesions usually resolve within hours but may accompany headache, syncope, dizziness, wheezing, and nausea. The shape of skin eruptions in solar urticaria is consistent with the area exposed to the light of an eliciting wavelength. There may be widespread wheals, flare, or punctate redness but not the small wheals observed in cholinergic urticaria. The face and hands may develop fewer lesions than skin areas that are usually covered by clothes because of hardening due to chronic exposure to sunlight.
DELAYED PRESSURE URTICARIA
Delayed pressure urticaria is characterized by deep dermal wheals that appear in a continuously compressed region with a latency of 30 minutes or several hours after the release of the compression. The wheals last for several hours or up to 3 days and may be accompanied by a burning sensation or pain rather than the itching often seen with CSU.50 DPU may develop by itself but may often be accompanied by CSU.51
VIBRATORY URTICARIA AND ANGIOEDEMA
Vibratory urticaria and angioedema is a rare subtype of physical urticaria characterized by cutaneous swelling developing immediately at the site of contact with vibratory stimuli, such as jogging, vigorous toweling, or using lawnmowers.52 Recently, the missense mutation of ADGRE2 has been reported to be associated with familial vibratory urticaria with autosomal dominant inheritance.53
AQUAGENIC URTICARIA
Aquagenic urticaria is a rare subtype of urticaria induced by local skin exposure to water. The eruptions are induced regardless of the temperature of the water. This characteristic of aquagenic urticaria helps differentiate it from cold urticaria and heat urticaria, which may also be induced by skin exposure to water at certain temperatures. Aquagenic urticaria is characterized by small wheals, resembling eruptions of cholinergic urticaria, but wheals in this urticaria subtype are generally fewer in number as compared with eruptions of cholinergic urticaria. They are usually surrounded by wide flares. Pruritus without a wheal and flare reaction developing after exposure to water is classified as aquagenic pruritus of a different disease entity.54
CHOLINERGIC URTICARIA
Cholinergic urticaria is a distinct subtype of urticaria induced by stimuli that cause sweating and distinctive for its small urticarial eruptions. Cholinergic urticaria
690
is more common in children, adolescents, and young adults. Stimuli can be physical exercise, a hot temperature environment, or emotional or gustatory excitation. The eruptions are punctate 1- to 4-mm wheals or red spots with or without surrounding flare (see Fig. 41-1C). In severe cases, the eruptions may become confluent, generalized urticaria and even develop into anaphylaxis.35,55,56 In rare cases, such lesions may accompany angioedema (cholinergic angioedema).34,57
A case of angioedema that developed in response to exercise without punctate wheals or erythema was also reported.58 Of note, most patients who develop angioedema are female and have an associated atopic diathesis or sweat allergy.57,58 Cholinergic urticaria is usually pruritic but may be painful or sting, especially at the time when eruptions are developing. The wheal and flare reaction usually develops within 30 minutes and completely disappears within a few hours. Cholinergic urticaria must be differentiated from exercise-induced urticaria and anaphylaxis, which is induced by exercise but not by passive warming. Certain cases of cholinergic urticaria may be evoked by systemic cold stimuli (cold cholinergic urticaria). Such cases should be differentiated from familial cold urticaria. Pruritus without wheals induced by conditions that elicit sweating has also been described (cholinergic pruritus).59
A substantial proportion of patients with cholinergic urticaria may also have atopic dermatitis and show type I hypersensitivity against human sweat.60
The major antigen in sweat has been identified as MGL_1304, a protein produced and released by Malassezia globosa on human skin.61,62 Another subset of patients with cholinergic urticaria have partial impairment of sweat production.63 Most patients with this type of cholinergic urticaria complain of pain rather than itching, especially in winter.35
CONTACT URTICARIA
Contact urticaria is classified as a subtype of inducible urticaria characterized by immediate development of a wheal and flare reaction at the site of contact with specific substances. It may be either immunologic (IgE mediated) or nonimmunologic. The wheal and flare usually appears within 30 minutes and completely disappears within a few hours and may also develop into generalized urticaria and even anaphylaxis. Cold urticaria, heat urticaria, and aquagenic urticaria are also induced by contact with a substance with corresponding physical characteristics but are usually not included in this category. Cases in which oral edema and discomfort are the main symptoms, induced by contact of the oral mucosa with certain foods, are called as oral allergy syndrome (OAS).64
URTICARIAL VASCULITIS
Urticarial vasculitis is characterized by recurrent urticarial lesions that last for more than 24 hours, leaving pigmentation and demonstrating histopathologic evidence of leukocytoclastic vasculitis. Shapes of wheals
and flare observed in urticarial vasculitis are similar to those observed in spontaneous urticaria and may be indistinguishable from those of CSU with long-lasting wheals. Patients with urticarial vasculitis may also develop livedo reticularis, Raynaud phenomenon, and angioedema.65-69
URTICARIAL REACTIONS AND SYMPTOMS OF OTHER SYSTEMIC DISEASE ENTITIES Wheal Developing from Skin Test: Wheals and flare may develop in response to intracutaneous injection of histamine or antigen. However, these reactions are usually not included in urticaria as a disease entity.
Hereditary Angioedema: Hereditary angioedema is a disease entity characterized by recurrent angioedema based on a hereditary etiology. Symptoms of HAE may develop anywhere in the body, especially in the skin, gastrointestinal tract and airway, and be extremely severe. This may be clinically indistinguishable from angioedema secondary to idiopathic mechanisms (see Fig. 41-1E). Importantly, those with HAE do not develop superficial wheals. Patients with HAE may be complicated with urticaria, but it is very rare.
Anaphylaxis: Wheal and flare is the most frequent sign observed in anaphylaxis. Anaphylaxis is induced by either allergic or nonallergic mechanisms and includes systemic symptoms beyond involvement of the skin.
Darier Sign: This is a wheal and flare reaction induced by scratching a lesion of mastocytosis. Nonlesional skin does not produce such a reaction.
ETIOLOGY AND PATHOGENESIS
The common feature of urticaria is a rapid and transient vasodilation and extravasation of plasma into cutaneous or mucosal tissues accompanied by itch sensory nerve activation. These reactions are mostly explained by degranulation of cutaneous mast cells, which release histamine and other vasoactive mediators, including arachidonic acid metabolites, such as prostaglandins and leukotrienes. The crucial role of mast cells in urticaria has been proven by histologic observations of mast cell degranulation in the lesional skin of wheals, the increase of local histamine concentration in skin fluid or plasma of urticarial lesions, and the clinical efficacy of antihistamines for more than half of patients with CSU.20 Indeed, type I hypersensitivity against exogenous antigens may well explain such reactions in allergic urticaria. However, the mechanism of mast cell activation and its relationship to various underlying diseases in other types of urticaria are largely unclear.
6
TYPE I HYPERSENSITIVITY
TYPE I HYPERSENSITIVITY
Mast cells play a pivotal role in type I hypersensitivity reactions via the high-affinity IgE receptors (FcεRI) and antigen-specific IgE (Fig. 41-3). Crosslinking of FcεRI leads to the activation of numerous signaling molecules, SYK, LAT, PLCγ, and PKC, and finally results in degranulation with release of preformed mediators such as histamine and newly synthesized ones such as arachidonic acid metabolites, platelet-activating factor, and proinflammatory cytokines.63 Patients who possess antigen-specific IgE may respond to antigens that reach cutaneous mast cells via various pathways such as ingestion, inhalation, or skin exposure. If patients are exposed daily to the causative antigen, urticaria may be chronic.70 Otherwise, urticaria developing through this mechanism appears as episodic or acute urticaria. Certain dietary antigens that take time to be absorbed, such as poly-γ-glutamine contained in fermented soybeans and gel-fish, may cause symptoms after a few hours or even later.71,72 However, in most cases, urticaria symptoms develop in 15 minutes to 1 hour after the antigen exposure. Many studies suggest that the population of patients who develop urticaria because of clinically apparent, classical type I allergy against exogenous antigens, such as food and drugs, is less than 10% of the whole population of patients with urticaria.73,74
Recently, it has been proven that approximately two thirds of patients with cholinergic urticaria are sensitized by antigens in human sweat. Such patients show positive
The mechanism of mast cell and basophil activation by autoantibodies
Omalizumab
IgE
Cε3 (receptor binding site)
Omalizumab binds free IgE but not IgE bound to FcεRI.
Antigen
Anti-IgE autoantibody (IgG)
Anti-FcεRI autoantibody (IgG)
Mast cells and basophils C5b
C5a
High-affinity IgE receptor (FcεRI) Degranulation (eg, histamine)
The expression of FcεRI is gradually downregulated by the decrease of free IgE.
691
6
reactions in skin testing with autologous sweat and histamine release testing using their basophils and purified human sweat.60,61 The major antigen of human sweat for these reactions has been identified as MGL_1304, a 17-kD protein produced and released by M. globosa.62
AUTOIMMUNE MECHANISM
AUTOIMMUNE MECHANISM
An autoimmune diathesis in CSU was initially suspected because of the increased incidence of antithyroid antibodies, including antimicrosomal (peroxidase) and antithyroglobulin IgG autoantibodies, as seen in patients with Hashimoto disease.75
It is now known that one third to half of patients with CSU possess functional IgG autoantibodies against IgE76 or the high-affinity IgE receptors (FcεRI)77
that release histamine from mast cells and basophils.78
Autoantibodies against IgE crosslink IgE together with FcεRI to which the IgE bind. In cases with autoantibodies against FcεRI, they directly bind to and crosslink FcεRI without IgE. In a certain population of patients, IgE bound to FcεRI competes with the autoantibodies against FcεRI (see Fig. 41-3). The histamine-releasing (basophil-activating) activity of the autoantibodies against FcεRI is partially, if not fully, dependent on the activation the classical complement cascade.79,80
The presence of these autoantibodies may be screened using ASST and proven with the histamine release test using sera of the patients and basophils obtained from healthy individuals.81
Patients with CSU and a positive ASST result might be more intractable and reveal more severe symptoms than those with a negative ASST result.82 A recent study revealed that the time to respond to treatment with omalizumab for patients with a positive ASST result is longer than for those with a negative ASST.83
The involvement of autoantigens that bind to IgE has also been suggested both in CSU and inducible urticarias.78 Recently, the mechanism of autoimmunity involving tissue antigens recognized by IgE and that mentioned above involving IgE/FcεRI recognized by IgG have been proposed to be classified as type I and type II autoimmunities, respectively.78 The involvement of type I autoimmunity has been suggested based on passive transfer of the sensitization using sera of patients or skin tests with human skin extracts.84-93 In solar urticaria, there is evidence that an antigen on the skin may become evident on irradiation with light of crucial wavelengths followed by complement activation.94-96 Histamine release from skin tissue specimens biopsied from a patient with cold urticaria in response to cooling and rewarming suggests the presence of a pathogenic molecule in the skin that is sufficient to activate mast cells.97 However, no solid molecules have been identified to date. Autoantibodies, either IgG or IgE against thyroid antigens, such as thyroglobulin and TPO, may be detected in patients with CSU. However, they are mostly not related to abnormalities of thyroid function, and the therapeutic effect of thyroxin on urticaria
692
with normal thyroid functions is controversial.98
Furthermore, the continuous presence of autoantibodies or autoantigens cannot explain diurnal and local occurrence of wheals observed in spontaneous urticaria. Thus, no autoantigens have been identified that explain the entire clinical picture of urticaria in each patient. Nevertheless, recently observed rapid effects of omalizumab, anti-IgE antibody, on both spontaneous and physical urticarias suggest the involvement of endogenous antigens that bind to IgE in the pathogenesis of various, if not all, types of urticaria.99
Studies of some patients with physical urticaria suggested the involvement of abnormal IgE that change confirmation in response to physical stimuli and activate mast cells.100
In a subtype of urticarial vasculitis with hypocomplementemia, IgG autoantibody against C1q is identified (hypocomplementemic urticarial vasculitis syndrome).66
PSEUDOALLERGY
PSEUDOALLERGY
Nonallergic hypersensitivity to dietary pseudoallergens, including naturally occurring food ingredients such as salicylates and biogenous amines, food additives, and continuous use of oral or topical nonsteroidal antiinflammatory drugs (NSAIDs), may be relevant as a cause or a precipitating or aggravating factor for CSU. Because the mechanism of urticaria provoked by pseudoallergens remains unclear, strict exclusion and subsequent provocation testing with a suspected substance are necessary for the diagnosis.32 For a diagnosis of food pseudoallergy, a 3-week pseudoallergenfree diet may be followed by well-motivated patients. The increased sensitivity of patients with CSU to histamine in the diet (histamine intolerance) has been suggested.101 In fact, high concentrations of histamine produced in scombroid (histidine-rich fish) by bacteriaderived histidine-decarboxylase may cause anaphylactic reactions even in apparently normal individuals (scombroid poisoning).102 Moreover, symptoms of some patients with CSU may be improved by the avoidance of pseudoallergens and histamine in the diet. However, the efficacy of such diet restriction in the management of CSU is still controversial.103 Although many reports suggest that food additives aggravate chronic urticaria, they may be based on self-reporting22 or on the improvement in symptoms from stringent pseudoallergen-free diets.104 In a double-blind, placebo-controlled study, only 19% of patients responded to a provocation test with individual pseudoallergens, but the symptoms of 73% of patients ceased or were greatly reduced on the pseudoallergen-free diet. Red wines may contain vasoactive amines, including histamine, which could aggravate urticaria, but symptoms poorly correlate with histamine content.105 Notably, pseudoallergy may not be simply diagnosed based on a patient’s history.101 Thus, dietary factors, including pseudoallergens and histamine, are likely involved in the cause of CSU to some extent, but none of them by themselves may explain the mechanisms of direct mast cell activation.
COAGULATION SYSTEM
COAGULATION SYSTEM
In patients with CSU, especially those with severe symptoms, the levels of plasma coagulation markers, such as prothrombin fragment 1+2 (PF1+2), fibrin degradative products (FDPs), and D-dimer, are higher than those in healthy control participants. They correlate with disease severity and return to normal levels with remission or control of symptoms by treatments.106-110
Moreover, an increased potential for blood coagulation is also observed to correlate with disease severity in CSU.111,112 Furthermore, massive expression of tissue factors has been demonstrated in eosinophils in the lesions of CSU.108 Alternatively, small amounts of histamine and lipopolysaccharides may synergistically induce the expression of tissue factors, which is sufficient to trigger the coagulation cascade on endothelial cells.113 Activated coagulation factors, such as FVIIa, FXa, and thrombin, can activate protease-activating receptors (PARs) and may thus activate skin mast cells. In fact, medications that control coagulation and the fibrinolytic system, such as warfarin, nafamostat, and the combination of heparin and tranexamic acid, have been reported to be effective for cases of CSU.114-117
However, no direct evidence of human mast cell activation by activated coagulation factors by themselves has been reported. Moreover, no clinically apparent thrombosis is observed in patients with urticaria. Thus, it is still not clear whether abnormalities in the coagulation pathway observed in CSU are causative or epiphenomena of increased vascular permeability.
UNDERLYING DISORDERS ASSOCIATED WITH INDUCIBLE URTICARIAS
UNDERLYING DISORDERS
ASSOCIATED WITH
INDUCIBLE URTICARIAS
Symptoms of inducible urticarias are induced by specific stimuli, including specific physical conditions, sweat induction, and contact with specific substances corresponding to physical urticarias, cholinergic urticaria, and contact urticaria, respectively. As mentioned earlier, specific IgE may link such stimuli and mast cells, resulting in allergic reactions in response to the stimuli. The other mechanisms that make patients sensitive to certain stimuli remains largely unknown. However, in limited cases of cold urticaria, solar urticaria, and vibratory angioedema, definitive causes may be identified by serologic or genetic analyses.
COLD URTICARIA
Most cases of local cold urticaria are considered to be primary cold urticaria. In this type, no relation to underlying causes or abnormal findings upon clinical examination are observed. In rare cases, cryoproteins, such as cryoglobulin and cryofibrinogen, may be identified, either idiopathically or in association with
6
collagen vascular disease, chronic lymphatic leukemia, myeloma, or infectious disease, including infectious mononucleosis.86,118,119 Hereditary systemic cold urticaria may be presented as a systemic inflammatory symptom caused by genetic mutations of NLRP3 (CIASI) or PLCG2 (see the “Cold Urticaria” section of Clinical Features).
SOLAR URTICARIA
The cause of solar urticaria is usually unknown, but a rare case can be diagnosed as caused by porphyrias and classified as type VI solar urticaria.120,121
VIBRATORY ANGIOEDEMA
Recently, a missense mutation in ADGRE2 has been identified in patients with autosomal dominant vibratory urticaria and revealed to make mast cells sensitive to vibration in an IgE-independent manner.53 The role of protein coded by ADGRE2 in nonhereditary-type vibratory angioedema remains to be investigated.
NEUROLOGIC MECHANISM
NEUROLOGIC MECHANISM
It is a unique characteristic of mast cells in the skin or connective tissues that they respond to basic peptides, such as substance P, vasoactive intestinal peptide, somatostatin, neurokinin A and B, bradykinin, calcitonin gene-related peptide, and adrenocorticotropic hormone (ACTH).122-125 They also express numerous receptors for ligands, including the above-mentioned neuropeptides and acetylcholine as well as Toll-like receptors.63,78,126,127 Therefore, these neurotransmitters have been hypothesized to be triggers of mast cell activation in urticaria. However, the concentration required for a neuropeptide to induce histamine release is as high as 10-6 M,128 and the mechanism of neuropeptide release in the skin is still unclear. Recently, excessive release of acetylcholine from the cholinergic nerve terminal to compensate for impaired sweat production by sweat glands in acquired idiopathic generalized anhidrosis was suggested as a mechanism of mast cell activation and the development of cholinergic urticaria observed in this disease.63
INFECTIONS
INFECTIONS
Acute infections by viruses and bacteria are known to be often associated with spontaneous urticaria, especially with the onset of acute urticaria in children and in transient aggravation of CSU.129 Many studies have suggested chronic persistent infection by Helicobacter pylori as an important cause of CSU,130 but its significance is disputed.131,132 The relationship between many other kinds of infections and urticaria have not been substantiated.
693
6
STRESS AND FATIGUE
STRESS AND FATIGUE
Many investigators have suggested a relationship between stress or fatigue and aggravation or elicitation of urticaria.133 Patients with CSU were found to have higher levels of life event stress and perceived stress134
and experienced stressful life events before the onset of the disease.135-137 However, urticaria itself induces stress and impairs the quality of life (QOL) of patients. Moreover, the importance of psychological factors is difficult to scientifically evaluate. Depression and anxiety were found more frequently in patients with chronic urticaria in one study138 but not in another.139
Thus, it is controversial whether stress and fatigue should be included as underlying causes of urticaria. Nevertheless, with respect to QOL assessments, it is good clinical practice to ask patients with urticaria about their psychosomatic and psychiatric conditions.
OTHER ORGAN DISORDERS
OTHER ORGAN DISORDERS
In addition to infections and thyroid dysfunction, which have already been described, many other extracutaneous disorders such as collagen diseases and malignancies have been reported to underlie chronic urticaria. In some cases, the treatment of these disorders resulted in the remission of urticaria. However, reports are mostly anecdotal, and a large epidemiologic study denied the association between malignancies and chronic urticaria.140 A retrospective population-based cohort study using data from the National Health Insurance research database in Taiwan reported an increased risk of hematologic malignancies.141 With respect to physical urticaria, cryoglobulinemia was identified in several patients with cold contact urticaria (see the paragraph of “Cold Urticaria in Underlying Disorders Associated With Inducible Urticarias” in this section). However, in other cases, the relationship between these disorders and the pathogenesis of urticaria is largely unknown. Moreover, screening for malignant neoplasms as a routine test for urticaria is no longer recommended by the guidelines and consensus document.1,142
In cases of angioedema without wheals, myeloproliferative disorders and autoimmune disorders such as SLE may underlie the disease by consuming C1-hinhibitor (C1-INH) and developing autoantibodies against C1-INH, respectively, resulting in an overproduction of bradykinin143 (Fig. 41-4).
OTHER FACTORS THAT MAY INDUCE OR AGGRAVATE URTICARIAL REACTIONS
OTHER FACTORS THAT MAY
INDUCE OR AGGRAVATE
URTICARIAL REACTIONS
Various factors are known to elicit or aggravate urticaria, which are mostly preexisting. They may be a cause of episodic or acute urticaria but not fundamental causes of chronic urticarias (Table 41-3). They should be carefully evaluated and avoided, if present.
694
C1-inhibitor actions on the pathways of bradykinin generation and developing angioedema
Coagulation and fibrinolytic pathways
Contact activation pathway
FDP, D-dimer Fibrinogen Fibrin
FXI
FXIa
FIX Thrombin
Tranexamic acid, ε-Aminocaproic acid Plasminogen Plasmin
FXII FXIIa
Ecallantide, Lanadelumab, BCX7353
Prekallikrein Kallikrein Kallikrein
HMW kininogen HMW kininogen Cleaved HMW kininogen
Bradykinin
Kallikrein–kinin pathway
ACE
ACEI
Endothelial cell membrane Des-Arg9-BK
Icatibant
Bradykinin B2 receptor
ASPIRIN AND OTHER NONSTEROIDAL ANTIINFLAMMATORY DRUGS
Aspirin and other NSAIDs, which inhibit cyclooxygenase (COX)-1, may induce or aggravate wheals and angioedema. These medications may also elicit respiratory symptoms (aspirin asthma). However,
Foods: allergens such as milk and eggs (for infants), nuts, seeds, fruits, and seafood (for adults) and pseudoallergens (food additives, salicylates, histamine, and other amines) Drugs: antibiotics (β-lactams, vancomycin, polymyxin B), NSAIDs (oral, injection, topical), opioids, contrast media, opioids, ACE inhibitors (for angioedema) Vaccines Blood products: transfusions Stings: bee, wasp venoms Contactants: latex, chemicals Inhalants: latex powder, chemicals
Foods: allergens such as milk and eggs (for infants), nuts, seeds, fruits,
and seafood (for adults) and pseudoallergens (food additives, salicylates, histamine, and other amines) Drugs: antibiotics (β-lactams, vancomycin, polymyxin B), NSAIDs (oral,
injection, topical), opioids, contrast media, opioids, ACE inhibitors (for angioedema) Vaccines Blood products: transfusions Stings: bee, wasp venoms Contactants: latex, chemicals Inhalants: latex powder, chemicals
ACE, angiotensin-converting enzyme; NSAID, nonsteroidal antiinflammatory drug.
the development of skin symptoms and respiratory symptoms appears to be independent.144,145 Fooddependent exercise-induced urticaria (FDEIA) may be aggravated or induced by aspirin or NSAIDs when administered with causative dietary elements even without exercise.146,147 COX-2–selective NSAIDs tend to be safer than aspirin or other relatively potent COX-1 inhibitors. However, sensitivities of individual patients to NSAIDs are not necessarily correlated with their COX-1 inhibitory activities.145
SERUM SICKNESS
Several days to a few weeks after the administration of the offending agent, which could be not only heterologous serum, but also be certain drugs, urticaria may develop with fever, lymphadenopathy, myalgia, arthralgia, and arthritis. Symptoms are usually self-limited and last 4 to 5 days.148,149
BLOOD PRODUCTS
Urticaria may develop after the administration of blood products. It usually is the result of immune complex formation and complement activation.149 Aggregated IgG may also be responsible for urticarial reactions.149
CONTRAST MEDIA
Contrast media may cause allergic reactions after its intravenous infusion. The prevalence of allergic reactions to iodinated contrast media (ICM) is estimated to be 0.05% to 0.1% of patients undergoing radiologic studies with ICM.150 The application of nonionic dimeric ICM with higher physiological osmolality has decreased the number of immediate reactions occurring within 1 hour, but the prevalence of nonimmediate hypersensitivity reactions has increased in the past decade. Erythema and wheals with or without angioedema are the most common signs of immediate reactions, but delayed nonimmediate reactions may include a maculopapular rash.150
Most reactions are attributed to non-IgE mechanisms, but an IgE-mediated mechanism was also proven by positive skin testing or basophil activation testing in some cases.150
OTHER MAST CELL AND BASOPHIL ACTIVATORS
Opiate analgesics, polymyxin B, curare, D- tubocurarine, and vancomycin induce histamine release from mast cells or basophils, especially when given at high doses, and may cause urticaria or other cutaneous rashes upon the episode of administration.149,151 On the other hand, angiotensin-converting enzyme (ACE) inhibitors do not cause release or production of mediators by themselves but inhibit degradation of bradykinin. Unlike most other medications, these may cause or aggravate angioedema after multiple administrations over a few
6
days or longer after administration. These medications thus function as an underlying cause of angioedema rather than a direct stimulus (see Fig. 41-4).143
RISK FACTORS
RISK FACTORS
Urticaria may occur at any age, and no difference in prevalence has been reported based on race or ethnic group. Women outnumber men by two to one with CSU. CSU may be associated with infections and autoimmune disorders, such as thyroid diseases and collagen diseases (see section “Complications in the Clinical Features”). However, the prevalence of urticaria in patients with these diseases is low, and thus they are not generally thought of as risk factors. Genetic analysis of a white population indicated a strong association between HLA-DR4 and patients with CSU with functional autoantibodies against IgE or FcεRI.152 Cholinergic urticaria is often complicated by atopic dermatitis.60 Urticaria mediated by an IgE mechanism, especially those caused by latex allergy and OAS, may be associated with an atopic diathesis. Health care workers, individuals with atopic dermatitis, and patients with spina bifida have a higher risk of developing latex allergy than other people.153
DIAGNOSIS
A characteristic feature of urticaria is the transient nature of individual eruptions. Therefore, the diagnosis of urticaria itself is not difficult. However, the diagnosis of subtypes of urticaria is necessary for proper management in individual patients. Laboratory tests and provocation tests should be performed based on careful history taking and inspection. Extensive laboratory investigations add little to making a final diagnosis.154 The overall diagnostic algorithm recommended by the EAACI guidelines1 is shown in Fig. 41-5.
HISTORY TAKING
HISTORY TAKING
A thorough and comprehensive history is essential for diagnosis and the elucidation of causative or aggravating factors. Because clinical examination findings for urticaria are highly variable and depend on the subtypes of urticaria, it is most important to narrow down the clinical diagnosis based on the history and physical examination before laboratory testing. Flares in disease activity during the evening to early morning is not specific but is a common feature of spontaneous urticaria. Wheals of inducible urticaria do not usually last for more than 4 hours, except for those of DPU. In some types of physical urticaria such as delayed dermographism43 and delayed cold urticaria,46
wheals may occur several hours after the stimuli, but the wheal does not last for long. Triggers; aggravating factors, if any; and the shape, size, and duration of
695
6
Diagnostic algorithm for urticaria
Wheals
Recurrent unexplained fever? Joint or bone pain? Malaise?
Angioedema
ACE inhibitor treatment?
History
- – – +
Autoinflammatory disease? Average wheal duration >24 hr? HAE or AAE? Remission after stop?
-
-
- – –
-
-
–
–
Signs of vasculitis in biopsy? Are symptoms inducible?
- –
–
Chronic spontaneous urticaria
Acquired/ hereditary AID
Urticarial vasculitis
Provocation test
–
Chronic inducible urtricaria
ACE-Inh induced AE
HAE I-III AAE
Interleukin-1 Histamine and other mast cell mediators Bradykinin
individual wheals helps in diagnosing the subtype of urticaria (see section “Cutaneous Findings in the Clinical Features”). Urticarial vasculitis should be ruled out if individual wheals last for 24 hours or longer, especially with purpura. Mast cell–mediated angioedema (ie, non–bradykinin-mediated type) does not usually occur in the larynx. Bradykinin-mediated angioedema does not accompany superficial wheals.
LABORATORY TESTING
LABORATORY TESTING
No routine laboratory testing is necessary or recommended for acute spontaneous urticaria. If a patient’s history strongly suggests an allergic mechanism, prick tests and measurement of antigen-specific IgE
696
are recommended. For CSU, a complete blood count, erythrocyte sedimentation rate, or C-reactive protein (CRP) is recommended. For further investigation, an extended diagnostic workup such as examination for Helicobacter pylori, Type I allergy, autoantibodies, and thyroid hormone may be undertaken. It is important, however, to note that the detection of a specific disorder may not always lead to an improvement in the symptoms of urticaria. Potential blood biomarkers in CSU to distinguish patients and control participants are D-dimer, CRP, matrix metalloproteinase-9, mean platelet volume (MPV), factor VIIa, prothrombin fragment 1+2 (PF1+2), tumor necrosis factor (TNF), dehydroepiandrosterone sulphate, and vitamin D.155
Biomarkers reflecting disease severity in CSU are FDP, D-dimer, F1+2, CRP, interleukin-6 (IL-6), and MPV.110,155
Several factors, diseases, and conditions have been reported as underlying causes of urticaria. However, a systematic review of the laboratory investigations for chronic urticaria revealed that the number of diagnoses identified varied from 1% to 84% and was not related to the number of laboratory tests performed.156 Therefore, extensive workups are not recommended for routine screening of the causes of urticarias unless suggested by the medical history or physical examination.1 The recommended diagnostic tests corresponding to each urticaria subtype are summarized in Table 41-1.
DIAGNOSIS OF URTICARIA SUBTYPES
DIAGNOSIS OF URTICARIA
SUBTYPES
After thorough history taking and careful skin inspection, the following diagnostic tests should be considered based on tentative clinical diagnosis of urticaria subtype (see Table 41-1).
SPONTANEOUS URTICARIA
The diagnosis of spontaneous urticaria is made based on history and skin inspection. In addition to the spontaneous appearance of wheals of characteristic shape, diurnal variation and a long-lasting course of individual wheals may help make this diagnosis. For acute spontaneous urticaria, no routine laboratory tests are recommended, but the diseases and reactions listed in Table 41-4 should be differentiated. The presence of
Wheal-like Eruption
- Insect bites
- Erythema multiforme
- Erythema nodosum
- Drug eruptions
- Adult-onset Still disease
- Shiitake dermatitis (resembling dermographic urticaria)
- Maculopapular cutaneous mastocytosis (urticaria pigmentosa)
- Urticarial vasculitis
- Cryopyrin-associated periodic syndromes
- Schnitzler syndrome
- Polymorphic eruption of pregnancy
Angioedema-like Eruption
Angioedema-like Eruption
-
Insect bites
-
Cellulitis
-
Erysipelas
-
Episodic angioedema with eosinophilia
-
Bradykinin-mediated angioedema (eg, HAE)
-
Well’s syndrome
-
Cheilitis granulomatosa
-
Granulomatous blepharitis
-
Insect bites
-
Cellulitis
-
Erysipelas
-
Episodic angioedema with eosinophilia
-
Bradykinin-mediated angioedema (eg, HAE)
-
Well’s syndrome
-
Cheilitis granulomatosa
-
Granulomatous blepharitis
HAE, hereditary angioedema. Data from Zuberbier T, et al. Allergy 2014;69:868-87; Bernstein JA, Lang DM, Khan DA, et al. The diagnosis and management of acute and chronic urticaria: 2014 update. J Allergy Clin Immunol. 2014;133(5):1270-1277; and Hide M, et al. Nihon Hifukagakkai Zasshi 2011;121:1339-88.
6
extracutaneous signs and symptoms and long-lasting eruptions, especially with purpura or epidermal change, such as dryness and desquamation, are important signs of different or complicated diseases. For such eruptions, a skin biopsy should help solidify the diagnosis. The presence of IgG autoantibodies against IgE or FcεRI should be demonstrated by a histamine release assay using the patient’s serum and basophils from healthy donors. This test may reveal the specificity of the autoantibodies against IgE, FcεRI, and degrees of their dependence on or competition with IgE for histamine release. However, this assay is somewhat cumbersome and requires special equipment, which has therefore limited its application. A solid phase assay, such as enzyme-linked immunosorbent assay, is relatively easy and quantitative but not specific.79 Alternatively, skin reactions evoked by ASST81 have been widely used as a screening test because of their relative simplicity and high sensitivity. In ASST, 0.05 mL of autologous serum is intradermally injected on the volar forearm skin along with normal saline and 10 µg/mL of histamine as the negative and positive controls, respectively.
SYMPTOMATIC DERMOGRAPHISM (MECHANICAL URTICARIA)
For the diagnosis of symptomatic dermographism, several instruments have been developed and used to determine the threshold of individual patients. The forearm is more suitable for this test than the abdomen, back, or pretibial areas. The result is considered positive if the patient shows a wheal and reports itching at the site of provocation at 36 g/mm2 or less. A wheal response without itching on provocation at 60 g/mm2
or higher indicates the less clinically significant simple dermographism.32 Reactions of this subtype of urticaria and other inducible urticarias, except for DPU, should be evaluated 5 to 10 minutes after testing.
COLD CONTACT URTICARIA
Cold provocation is performed by applying a wrapped ice cube or cold water for 5 minutes. In this way, the threshold duration of cold application can be determined. The use of a thermoelectric element (TempTest)157 can be used to determine the threshold by temperature.32 These tests induce wheal formation in cold contact urticaria but not for systemic cold urticaria, in which patients develop widespread wheals in response to cooling of the core body temperature or to cold wind.47,49
Systemic cold urticaria should be differentiated from cold contact urticaria because it may be a manifestation of autoinflammatory disease (familial cold urticaria; see Cold Urticaria in section “Clinical Features”).
HEAT URTICARIA
Provocation of heat contact urticaria is performed by applying hot metal, water, or a glass cylinder filled with hot water at 45°C to the skin of the volar forearm.
697
6
The TempTest157 used for cold contact urticaria may also be used for this type of urticaria. Cholinergic urticaria, solar urticaria, and aquagenic urticaria, which may also be associated with high temperatures or hot water, should be differentiated.
SOLAR URTICARIA
Solar urticaria should be differentiated from polymorphic light eruption. A provocation test for solar urticaria should be done on the buttock skin, but parts of the trunk that are usually covered by clothes can also be tested. The light source may be sunlight or a slide projector from a distance of 10 cm with or without filters or a monochromator (ultraviolet [UV] A or B, or visible light).32
DELAYED PRESSURE URTICARIA
Provocation may be performed by suspending a 7-kg weight on a 3-cm shoulder strap for 15 minutes or applying rods supported in a frame to the back, thighs, or forearm. Unlike the other inducible urticarias, the skin reaction should occur after a latent period, typically 2 to 4 hours after the pressure has been applied. Skin biopsies reveal an inflammatory infiltrate with prominent eosinophils but no vasculitis.32
VIBRATORY URTICARIA AND ANGIOEDEMA
The forearms are held on a flat plate placed on a vortex mixer that runs at between 780 and 1380 rpm for 10 minutes. The site of application should be assessed for swelling 10 minutes after testing.32
AQUAGENIC URTICARIA
Provocation is performed by attaching wet clothes at body temperature for 20 minutes. Wiping the test area with an organic solvent and challenging with saline instead of tap water may increase the reactivity.1,32,158
CHOLINERGIC URTICARIA
The diagnosis is established by an appropriate provocation test for the patient’s age and general condition (eg, on a treadmill or stationary bicycle). To differentiate from exercise-induced anaphylaxis, a passive warming test should be done, recording core body temperature to achieve an increase of 1.0°C or more. Skin testing with intradermal injection of 0.1 mL of acetylcholine at 100 µg/mL may reinforce the diagnosis of cholinergic urticaria. The test result should be considered positive if the test site shows satellite wheals around the injection site. The specificity of this test seems to be high, but the sensitivity is approximately 30% to 50%.32
698
CONTACT URTICARIA
For the diagnosis of contact urticaria, the suspected substance is applied in its original form or as an extract on a normal looking area of the volar forearm or the upper back for 15 to 20 minutes. If this test result is negative, occlusive application is applied followed by a prick test. For patients with a history of severe symptoms, tests should be started with sufficiently diluted suspected substances. In vitro tests may also be used for contact urticaria from Type I allergy, such as latex allergy.32
URTICARIAL VASCULITIS
Urticaria-like eruptions that last for longer than 24 hours should be differentiated from urticarial vasculitis. Clinical features such as fevers, malaise, arthralgia, uveitis, diffuse glomerulonephritis, and obstructive and restrictive pulmonary disease may be diagnostically helpful, but histologic examination of a skin biopsy is essential for confirmation of the diagnosis.67,159
ANGIOEDEMA
Angioedema is diagnosed mostly by its clinical features, including localized mucosal or deep skin edema that is nonpitting and lasts for hours to a few days. If angioedema is induced by specific stimuli that are also known to induce superficial wheals or occurs together with wheals, it is likely mast cell mediated and is classified as a subtype of urticaria (see Table 41-1). If angioedema occurs spontaneously without wheals, a bradykinin-mediated mechanism should be carefully differentiated. Whereas mast cell–mediated spontaneous angioedema can be severe but is mostly nonlethal, bradykinin-mediated angioedema can be lethal.143 The mechanisms of bradykinin production and degradation with related molecules are shown in Fig. 41-4.
Hereditary Angioedema: HAE is classified into three subtypes based on the condition of C1-INH.143,160 Patients with type I lack C1-INH protein, but those with type II lack activity of C1-INH because of genetic point mutations. Type III, also called as HAE with normal C1-INH, is a rare subtype of HAE. Type III develops mostly in females, and a gain-offunction mutation of factor XII may be identified in some patients. Recently, new genetic mutations, one in an angiopoietin-1 gene and another in a plasminogen gene, were identified in families with type III HAE.161,162 Whereas the levels of C1-INH activity and C4 are decreased in both type I and type II HAE, C1-INH protein concentration is low only in type I HAE. During attacks of HAE, coagulation markers, such as D-dimer, FDP and PF1+2 may increase.163,164 Prodromal symptoms, such as erythema marginatum, may precede HAE attacks in up to 50% of patients.
Acquired Angioedema: Bradykinin-mediated angioedema may develop either by overconsumption of C1-INH caused by myeloproliferative diseases
or because of the presence of autoantibodies against C1-INH. In the case of overconsumption of C1-INH, the level of C1q is decreased, as well as those of C1-INH and C4.
Angiotensin-Converting Enzyme Inhibitor– Induced Angioedema: ACE is a dipeptidylcarboxypeptidase that converts angiotensin I to angiotensin II and cleaves bradykinin. Therefore, its inhibitor, ACE inhibitor, used for the treatment of hypertension, inhibits degradation of bradykinin.
AUTOINFLAMMATORY SYNDROME
Autoinflammatory diseases are a diverse group of inherited conditions characterized by systemic inflammation in the absence of infection and are accompanied by a range of organ-specific manifestations.165
Two of them, Schnitzler syndrome and cryopyrinassociated periodical syndrome (CAPS), are known to include urticaria-like symptoms.
Schnitzler Syndrome: Schnitzler syndrome is characterized by urticaria-like eruptions and monoclonal IgM or possibly IgG gammopathy accompanied by systemic symptoms such as fever and bone and muscle pain.166,167 Its histology resembles an urticarial vasculitis or neutrophilic urticaria.
Cryopyrin Associated Periodical Syndrome: Familial cold-autoinflammatory syndrome, Muckle-Wells syndrome, and chronic infantile neurologic cutaneous articular syndrome may include an urticaria-like eruption. The eruption may be induced by exposure to cold but may also develop spontaneously and does not usually cause pruritus. Patients may develop periodic fever, arthralgia, amyloidosis, and nerve deafness. The common and crucial cause of these syndromes has been identified as gainof-function mutations in NLRP3 (CIASI), resulting in overproduction of IL-1β.168 Skin biopsy demonstrates neutrophil-dominant cell infiltration, but gene analysis is most definitive for making the diagnosis.
URTICARIA AND ANAPHYLAXIS INDUCED BY EXERCISE
Exercise may induce urticaria in patients with cholinergic urticaria and in patients with exercise-induced anaphylaxis. Some patients may develop urticaria and anaphylaxis regardless of food intake (exercise-induced anaphylaxis [EIA]), but others develop symptoms only when they exercise after eating certain foods (FDEIA). The demonstration of specific food allergen-reactive IgE in the serum may help but may not be sufficient for making the diagnosis of FDIEA.146,147 The presence of anti–ω5-gliadine IgE in adults has been reported to be an exceptionally good marker for FDEIA caused by wheat in terms of both sensitivity and specificity.169 An exercise challenge test is typically performed according to the protocol of Bruce and colleagues.170 The sensitivity of provocation testing for FDEIA was reported to be up to 70%.169
6
EVALUATION OF DISEASE CONDITIONS
EVALUATION OF DISEASE
CONDITIONS
Urticaria and underlying conditions in patients with urticaria should be evaluated in both specific and comprehensive ways.
DISEASE SEVERITY
Disease severity of inducible urticarias may be evaluated according to the threshold for eliciting factors (see Table 41-1). For spontaneous urticaria and angioedema, questionnaire-based scores may be used. The urticaria activity score over 7 consecutive days (UAS7) is a unified and simple scoring system that records daily wheals and itching and has been validated in comparison with the Dermatology Life Quality Index (DLQI).171 Disease activity of angioedema may be evaluated by a 4-week-long record of edema in terms of frequency, duration, subjective sensations, and disability of patients (Angioedema Activity Score [AAS]).172
For CSU, coagulation and fibrinolysis markers, such as D-dimer, FDP, PF1+2, and CRP, have been reported to reflect disease severity or activity (see Coagulation System in the section “Etiology and Pathogenesis”), but their sensitivities are low.173 Serum levels of proinflammatory cytokines, such as IL-6, TNF, and IL-23, may also reflect disease activity in certain patients but are of doubtful usefulness.32,174 Peripheral blood basopenia and low release of histamine from basophils may also be associated with disease activity,175,176 but the value of these markers is at present confined to the research laboratory.177
QUALITY OF LIFE
CSU has a high overall impact on QOL as compared with other common dermatologic conditions,178-180 The QOL of patients with superficial urticaria and that of patients with angioedema may be evaluated using the Chronic Urticaria Quality of Life Questionnaire (CU-Q2oL)181 and Angioedema Quality of Life Questionnaire (AE-QoL),182 respectively.1
CONTROL STATUS
The tools mentioned earlier—UAS-7, AAS, CU-Q2oL, and AE-QoL—may not adequately cover conditions of inducible urticarias and angioedema. More recently, an easy and comprehensive method of evaluation for all kinds of urticaria and angioedema has been developed. It is called the Urticaria Control Test (UCT), and it may be applied to all kinds of urticaria and angioedema.183
The short version of the UCT asks only four retrospective questions about the patient’s condition over the previous 4 weeks. These instruments have been translated and validated in many languages. The AAS, AE-QoL, and UCT are now available in various languages from Moxie GmbH, Berlin, Germany.184
699
6
PATHOLOGY
PATHOLOGY
Pathological findings in urticaria consist of edema in the dermis and perivascular and interstitial infiltration of inflammatory cells. Inflammatory cells usually consist of lymphocytes, eosinophils, and neutrophils. Commonly, lymphocytes are dominant in the perivascular area, but eosinophils and neutrophils tend to have an interstitial distribution. A few reports revealed an increase in mast cells in perivascular areas and the interstitium of lesions,185-187 but others did not.188 The presence of basophils has been demonstrated with specific antibodies.189 The degree of infiltration of these inflammatory cells varies according to subtypes of urticaria, individual variability, and the time from the onset of wheals (Figs. 41-6A to 41-6C). Detailed studies
A
700
B
of infiltrated lymphocytes revealed that they are both Th1 and Th2, or Th0 because they express IL-4, IL-5, and interferon (IFN)-γ.190 Neutrophils and eosinophils exist in dermal capillaries, and this is considered as an early change in numerous inflammatory skin diseases, including urticarias. Infiltration of neutrophils is prominent especially in acute urticaria and physical urticarias. Urticaria or urticaria-like eruptions that persist for longer than a day and involve predominantly neutrophilic infiltration without apparent vasculitis may also be called neutrophilic urticaria, neutrophilic urticarial dermatosis, or urticaria-like neutrophilic dermatosis.191-193 Similar changes may be observed in the skin lesions of CAPS and Schnitzler syndrome. Eosinophils may play a more important role than suggested by hematoxylin and eosin staining because extracellular eosinophil major basic protein is frequently
C
D
deposited in spontaneous wheals.194 Moderately dense infiltrates of eosinophils were observed in DPU.51 These cellular changes correlated with moderate upregulation of the vascular endothelial adhesion molecules E- selectin, intercellular adhesion molecules 1, and vascular cell adhesion molecule 1 on perivascular cells.195
Urticaria with histologic evidence of vasculitis ( venulitis) is defined as urticarial vasculitis (Fig. 41-6D). However, in clinical practice, it may sometimes be difficult to differentiate lesions of urticarial vasculitis from those of spontaneous urticaria when all histopathological features of vasculitis, including endothelial cell damage, fibrin deposition, leukocytoclasis, and erythrocyte extravasation, are not present in the skin specimen.68 Moreover, a continuum of histologic changes between urticaria and urticarial vasculitis has been recognized in a series of patients with intermediate histologic features.196,197 Some authors suggest that leukocytoclasis or fibrin deposition with or without erythrocyte extravasation may be sufficient for a diagnosis in difficult cases.68
IMAGING
IMAGING
Imaging examinations such as ultrasound, computed tomography (CT), or magnetic resonance imaging (MRI) are not required for ordinary urticarias. In cases of edema developing in pharyngeal and laryngeal areas or in the gastrointestinal tract, especially caused by bradykinin-mediated angioedemas, imaging tests might be useful or even essential. Patients with HAE may present with episodic swelling in various body parts, such as the face, neck, bowel, genitals, and extremities. Airway obstruction caused by edema of the larynx, oropharynx, and prevertebral soft tissue may cause suffocation, and this can be detected by endoscopy, radiographs, CT scans, and MRI examinations.36,198 Patients may also have acute abdominal pain caused by swelling of the gastrointestinal tract. Imaging in such situations may be helpful to avoid unnecessary surgical interventions.198
DIAGNOSTIC ALGORITHM
DIAGNOSTIC ALGORITHM
A diagnosis of urticaria or angioedema (or both) should be made based on careful observation of the skin and history taking followed by clinical examination to confirm the diagnosis and evaluate disease severity. It is recommended not to perform extensive screening or workup without a known clinical diagnosis of an urticaria subtype.1 The algorithm recommended by EAACI guidelines is shown in Fig. 41-5.
DIFFERENTIAL DIAGNOSIS
The diagnosis of urticaria is not difficult in most cases if suddenly appearing and transiently disappearing eruptions are confirmed by patient’s history and
6
clinical observations. Diseases that may manifest similar symptoms to urticaria and angioedema are listed in Table 41-4. Diseases that include wheals or angioedema should be differentiated by the presence of nonurticarial, mostly extracutaneous symptoms, such as fever and arthralgia.
CLINICAL COURSE AND PROGNOSIS
A study showed that most patients (85%) who had an acute spontaneous urticaria and began treatment within 1 week of disease onset improved shortly afterward. However, approximately 7% of this cohort continued to have symptoms for more than 1 year. Prolongation of disease activity tends to be seen among patients who required other medications in addition to a standard dose of antihistamine.199 Other studies, albeit from specialized centers, indicate that most patients have CSU for more than 1 year.14-18,22,200,201
Moreover, a considerable number of patients even seem to be affected for longer than 5 years. In some rare cases, urticaria may even last for up to 50 years.200
A retrospective study using Kaplan-Meier methods of patients with CSU who visited a tertiary medical center revealed the estimated improved rates at 12 months, 24 months, and 60 months as 36.6%, 51.2%, and 66.1%, respectively.201
However, the reported time course is highly variable among studies. Reported remission rates at 1 year ranged from 20% to 80%. Among these studies, four factors appear to be associated with prolonged prognosis, namely, (1) initial disease severity, (2) presence of angioedema, (3) combination of CSU and physical urticaria(s), and (4) autoreactivity (positive ASST result).20 A recent retrospective study showed that patients with CSU and positive ASST results responded more slowly to omalizumab than those with negative ASST results.83
MANAGEMENT
INTERVENTIONS
INTERVENTIONS
The treatment of urticaria and angioedema consists of two basic approaches. One is the identification and removal of the cause or factors that aggravate the condition. Another is the continuous use of antisymptomatic treatment with medications. For inducible urticaria, the avoidance of stimuli that induce symptoms is important, but in certain subtypes (solar urticaria, heat contact urticaria, cold contact urticaria, cholinergic urticaria, and urticaria induced by type I food allergy), repetitive exposure to slight stimuli may rather reduce the sensitivity of the patients (hardening or tolerance). Aggravating factors, if applicable for individual cases, should be removed to the extent possible (see section “Etiology and Pathogenesis” and Table 41-3). The algorithm of pharmaceutical treatment recommended by current guidelines1 is essentially the same for all subtypes
701
6
of chronic urticaria, except for bradykinin-mediated angioedema. In many cases of mast cell–mediated urticaria, especially in spontaneous urticaria, symptoms can be controlled to acceptable levels without identification of the cause. On the other hand, antihistamines, corticosteroids, and adrenaline are all ineffective for bradykinin-mediated angioedema.
MEDICATIONS
MEDICATIONS
Medication should be taken continuously rather than an on-demand basis for both spontaneous urticaria and inducible urticaria patients who develop symptoms daily or almost daily.1 However, if symptoms develop only occasionally, a schedule of medication use may be determined on a case-by-case basis. For HAE, three aims of medications should be considered based on the severity and frequency of the symptoms: on-demand therapy for emerging symptoms, short-term prophylaxis, and long-term prophylaxis.143,160
FIRST-LINE THERAPY
The second-generation nonsedating antihistamines are the mainstay of treatment for all kinds of mast cell–mediated urticaria. Generally, first-generation sedating antihistamines are no longer recommended. Although they appear to help with sleep at night, there may be carry-over effects of sedation in the morning and may cause paradoxical excitation or possibly epilepsy in children.
SECOND-LINE THERAPY
For intractable cases resistant to standard doses of antihistamines, increased dosing of antihistamines up to fourfold is recommended in EAACI guideline202
and practice parameters by the American Academy of Allergy, Asthma and Immunology (AAAAI) and the American College of Allergy, Asthma and Immunology (ACAAI)142 (American consensus document). Numerous reports have demonstrated the efficacy of high-dose antihistamines. Recently, a meta-analysis of using high dose antihistamines showed that this significantly improved control of pruritus but not wheal number.203
THIRD- AND FOURTH-LINE THERAPY
For cases in which high-dose antihistamines fail to achieve enough improvement, several additional therapies are recommended. The guideline published by the British Society for Allergy and Clinical Immunology (BSACI)202 and the American consensus document142 recommend adding antileukotrienes before the use of omalizumab and cyclosporine. However, EAACI guideline published in 2018 recommend adding omalizumab first as the third line therapy.1 Systemic
702
corticosteroids are recommended only to be used in limited circumstances, especially for severe symptoms in acute urticaria and acute aggravation of CSU. It should be noted that continuous use of corticosteroids (longer than 10 days) is not recommended because of the risk of side effects.1,142,203 The treatment algorithms published in EAACI guidelines1 and the American consensus document142 are shown in Fig. 41-7. The efficacy and safety of omalizumab, anti-IgE antibody, for the treatment of urticaria has been well studied, and it is now approved for the treatment of CSU in many countries.204-206 The proposed mechanism of action of omalizumab is shown in Fig. 41-3. A recent meta-analysis of randomized controlled studies showed that a dosage of 300 mg/month is recommended for intractable CSU regardless of the levels of serum total IgE.204 In theory, omalizumab inhibits circulating IgE and consequently decreases the number of FcεRI on mast cells and basophils. Although it takes 2 months or longer for omalizumab to decrease the number of cell surface FcεRI, the clinical effect of omalizumab on CSU may become apparent within 1 week.100 Moreover, omalizumab is effective for virtually all subtypes of urticaria mediated by mast cells, including DPU and urticarial vasculitis,99,207 although such usage is off label. A number of possible mechanisms have been hypothesized, but none of them so far can fully explain its effect on urticaria.100
EXCEPTIONAL CASES AND OTHER MEDICATIONS IN THE TREATMENT OF URTICARIA
In most cases of DPU and urticarial vasculitis, antihistamines are not effective. Systemic steroids or other immunosuppressive or modulatory agents may be necessary to suppress symptoms.208 As supplementary or alternative treatments, the following may also be used in combination with antihistamines for refractory cases: histamine H2-blockers, dapsone (diaphenylsulfone, DDS), antifibrinolytics (tranexamic acid or ε-aminocaproic acid) especially for patients with angioedema, methotrexate, tacrolimus, hydroxychloroquine, intravenous immunoglobulin therapy, plasmapheresis, and narrow-band UVB.1,209 However, evidence supporting the use of these medications is still weak, and reports are anecdotal. Moreover, most drugs have the potential for causing serious side effects. Most important, none of the pharmaceutical treatments mentioned has been proven to modify the natural course of urticaria in terms of achieving a cure. Therefore, it is important to consider a balance between the burden of symptoms and that of treatment. Treatment of bradykinin-mediated HAE, as recommended in various guidelines and consensus documents,143,160 is illustrated in Fig. 41-4. Icatibant, ecallantide, and purified or recombinant C1-INH are used for acute attacks. Purified or recombinant C1-INH, lanadelumab, and BCX7653 are used or are under development for use as prophylaxis. A few studies have reported the efficacy of icatibant for acute
6
Treatment algorithm for chronic urticaria
Second-generation H1
-Antihistamines (sgAH)
If inadequate control: After 2-4 wks or earlier, if symptoms are intolerable
Increase sgAH dose (up to 4x)
If inadequate control: After 2-4 wks or earlier, if symptoms are intolerable
Add-on to sgAH: Omalizumab
If inadequate control: Within 6 mo or earlier, if symptoms are intolerable
Add-on to sgAH: Ciclosporin
A B
Step 4
Add an alternative agent
• Omalizumab or cyclosporine
• Other antiinflammatory
agents, immunosuppressants, or biologics
Step 3
Dose advancement of potent antihistamine (eg, hydroxyzine or doxepin) as tolerated
Step 2
One or more of the following:
• Dose advancement of second-generation antihistamine
used in step 1
• Add another second-generation antihistamine
• Add H2 antagonist
• Add leukotriene receptor antagonist
• Add first-generation antihistamine to be taken at bedtime
Step 1
• Monotherapy with second-generation antihistamine
• Avoidance of triggers (eg, NSAIDs) and relevant physical factors if physical urticaria or angioedema syndrome is present
• Begin treatment at step appropriate for patient’s level of severity and previous treatment history
• At each level of the step approach, medication(s) should be assessed for patient tolerance and efficacy
• Step down in treatment is appropriate at any step after consistent control of urticaria or angioedema is achieved
attacks of angioedema caused by ACE inhibitors,210,211
although one study contradicted these findings.212
TREATMENT IN PEDIATRIC PATIENTS
The principle of treatment for children with urticaria is the same as for adults.1 Dosing should follow the relevant manufacturer’s recommendations.
TREATMENT IN PREGNANT AND LACTATING WOMEN
Use of any systemic treatment should generally be avoided in pregnant women, especially in the first trimester. Moreover, antihistamines cross the placenta. On the other hand, there is no reliable evidence that the medications listed in the algorithm of EAACI guideline are teratogenic. Thus, the same treatment principles and algorithm are suggested for both pregnant and lactating women with urticaria.1 Among antihistamines, chlorphenamine is often chosen based on its long availability and safety record.213 Current guidelines on urticaria support the use of cetirizine and loratadine desirably after the first trimester of pregnancy if the benefits of an antihistamine are considered to outweigh any risks of administration for an individual patient.1,202
COUNSELING
COUNSELING
No particular methods have been established for urticaria, but patients with CSU may have substantial impairment of their QOL, as much as with ischemic heart disease.214 Patients with hereditary diseases, such as HAE and autoinflammatory syndromes, should be offered qualified counseling as necessary.
TREATMENT ALGORITHM
TREATMENT ALGORITHM
The treatment algorithm recommended in EAACI guideline and the American consensus document are shown in Fig. 41-7.
PREVENTION AND SCREENING
PREVENTION AND
SCREENING
There are no measures for preventing or screening for the development of urticaria. On the other hand, all family members of patients with HAE type I and type II who are older than 1 year old are
703
6
recommended to undergo screening for the diagnosis of HAE. A case of a 9-year-old boy who died from the first attack of HAE has been reported.215 Early diagnosis and preparation for attacks should reduce the risk.
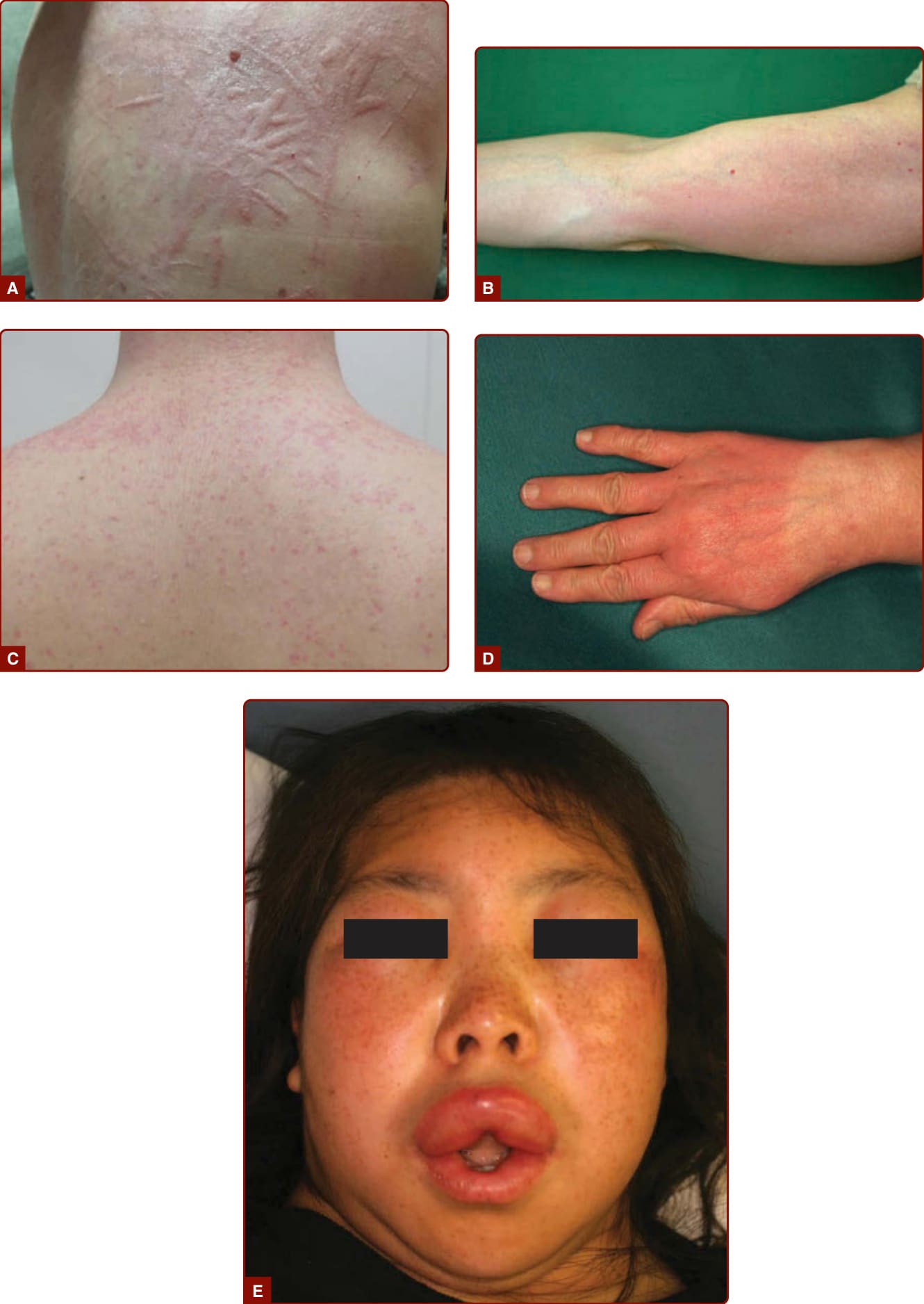
Figure 41-1 Clinical presentation of symptomatic dermographism (A and B), cholinergic urticaria evoked by exercise (C), local contact urticaria evoked by immersion in hot water (D), and hereditary angioedema (E).
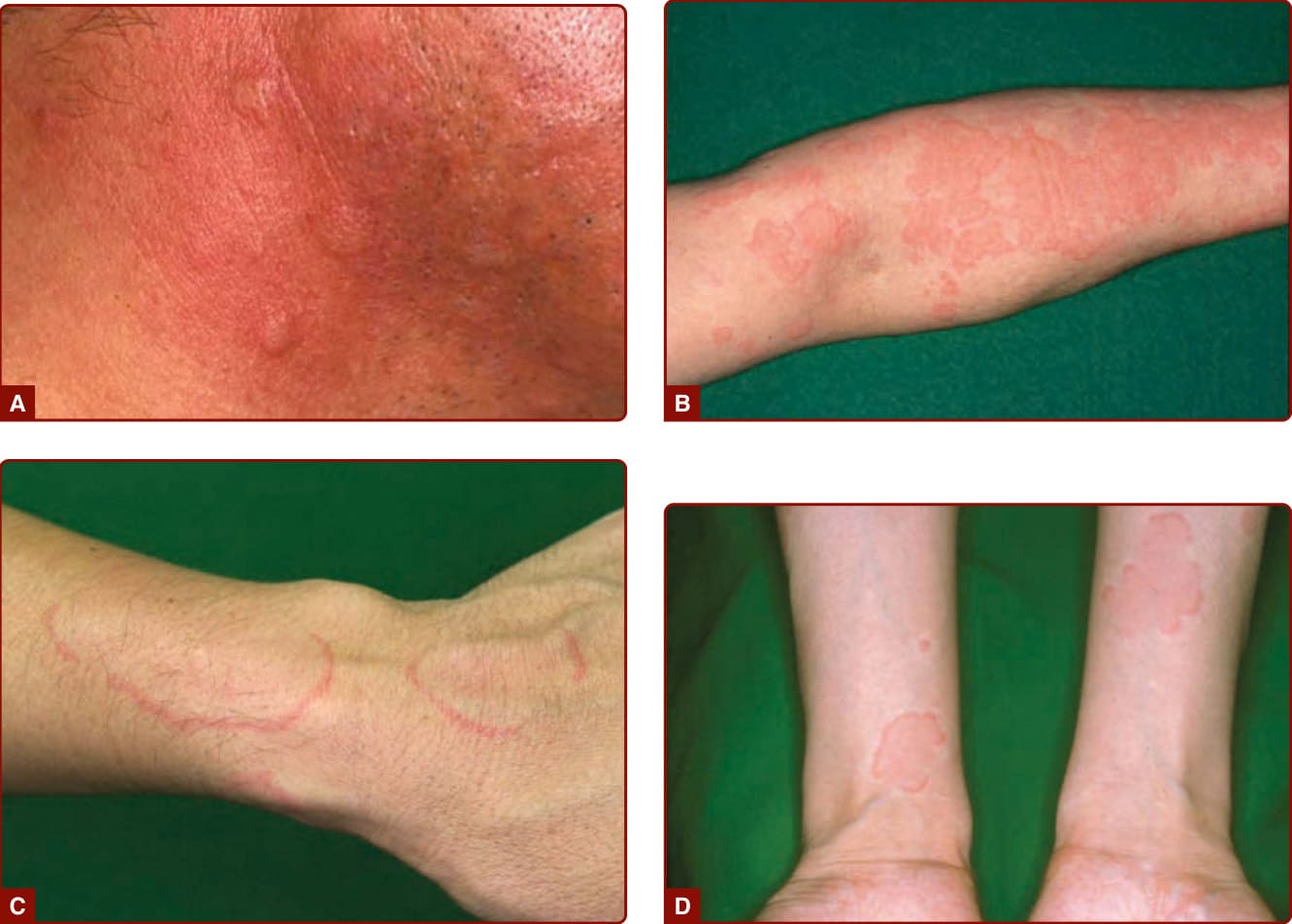
Figure 41-2 Clinical presentation of acute urticaria (A), chronic spontaneous urticaria (CSU) (B), CSU with an annular shape (C), and CSU with a flower shape (D). (Images A, B, and D, reproduced from JDA. 2012;122(11):2627-2634, with permission.)
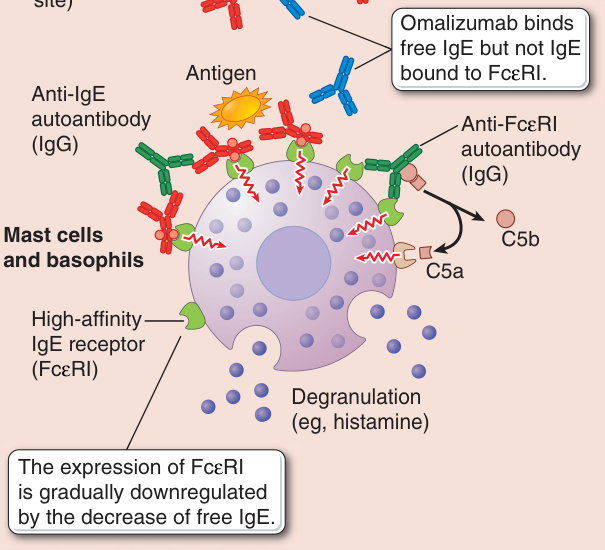
Figure 41-3 The pathogenesis of autoimmune urticaria and the proposed mechanism of action of omalizumab for autoimmune urticaria. FcεRI, the high-affinity immunoglobulin E receptor; Ig, immunoglobulin.
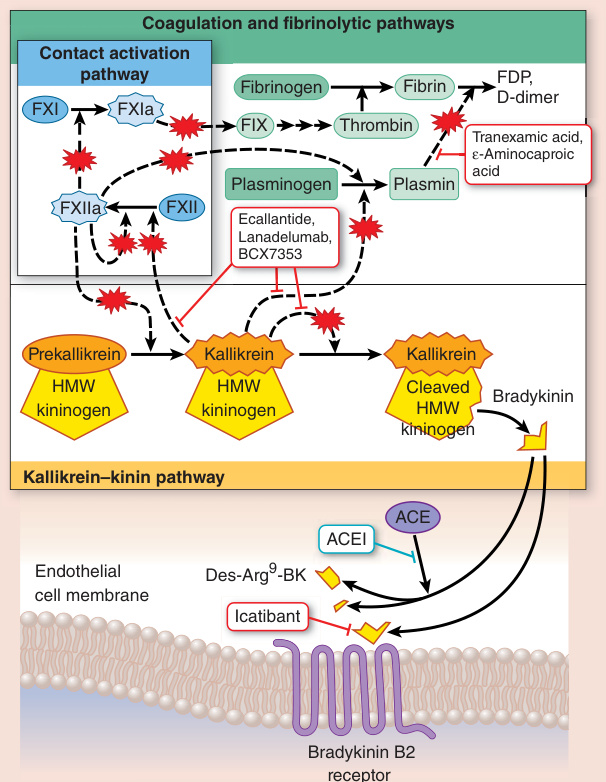
Figure 41-4 C1 inhibitor actions on pathways involved in bradykinin production. Points of inhibition by C1 inhibitor are shown by red blasts; other known mechanisms of pathway inhibition are also detailed. ACE, angiotensinconverting enzyme; ACEI, angiotensin-converting enzyme inhibitor; F, factor; FDP, fibrin degradative product; HMW, high molecular weight. (Information in this illustration was derived from Zuraw BL. Clinical practice. Hereditary angioedema. N Engl J Med. 2008;359:1027-1036.)
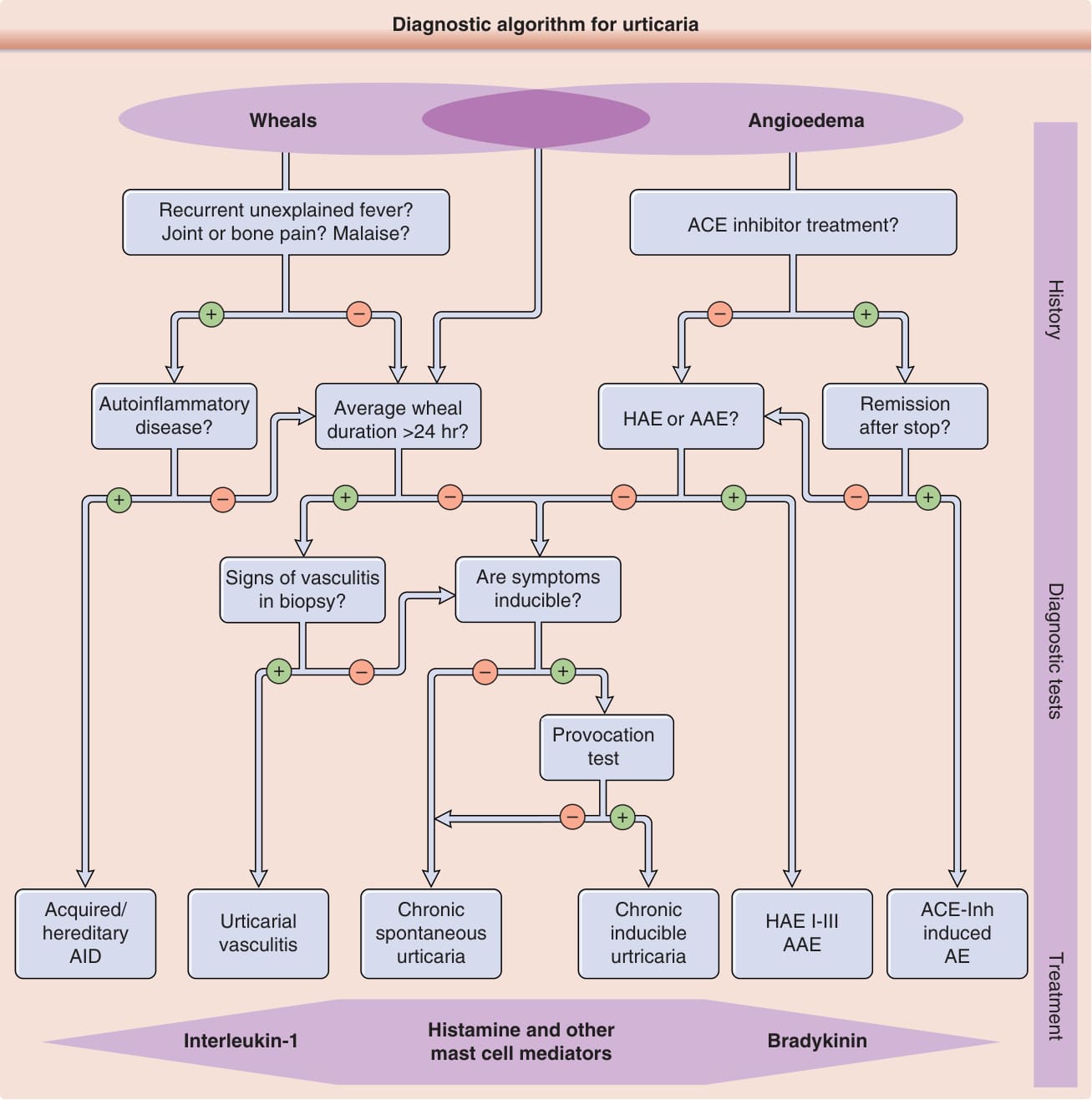
Figure 41-5 Diagnostic algorithm for urticaria. AAE, acquired angioedema due to C1-inhibitor deficiency; ACE-Inh, angiotensin-converting enzyme inhibitor; AE, angioedema; AID, auto-inflammatory disease; HAE, hereditary angioedema. (From Zuberbier T, Aberer W, Asero R, et al. The EAACI/GA(2) LEN/EDF/WAO Guideline for the definition, classification, diagnosis, and management of urticaria: the 2013 revision and update. Allergy. 2014;69:868-887, with permission. Copyright © 2014 John Wiley & Sons.)
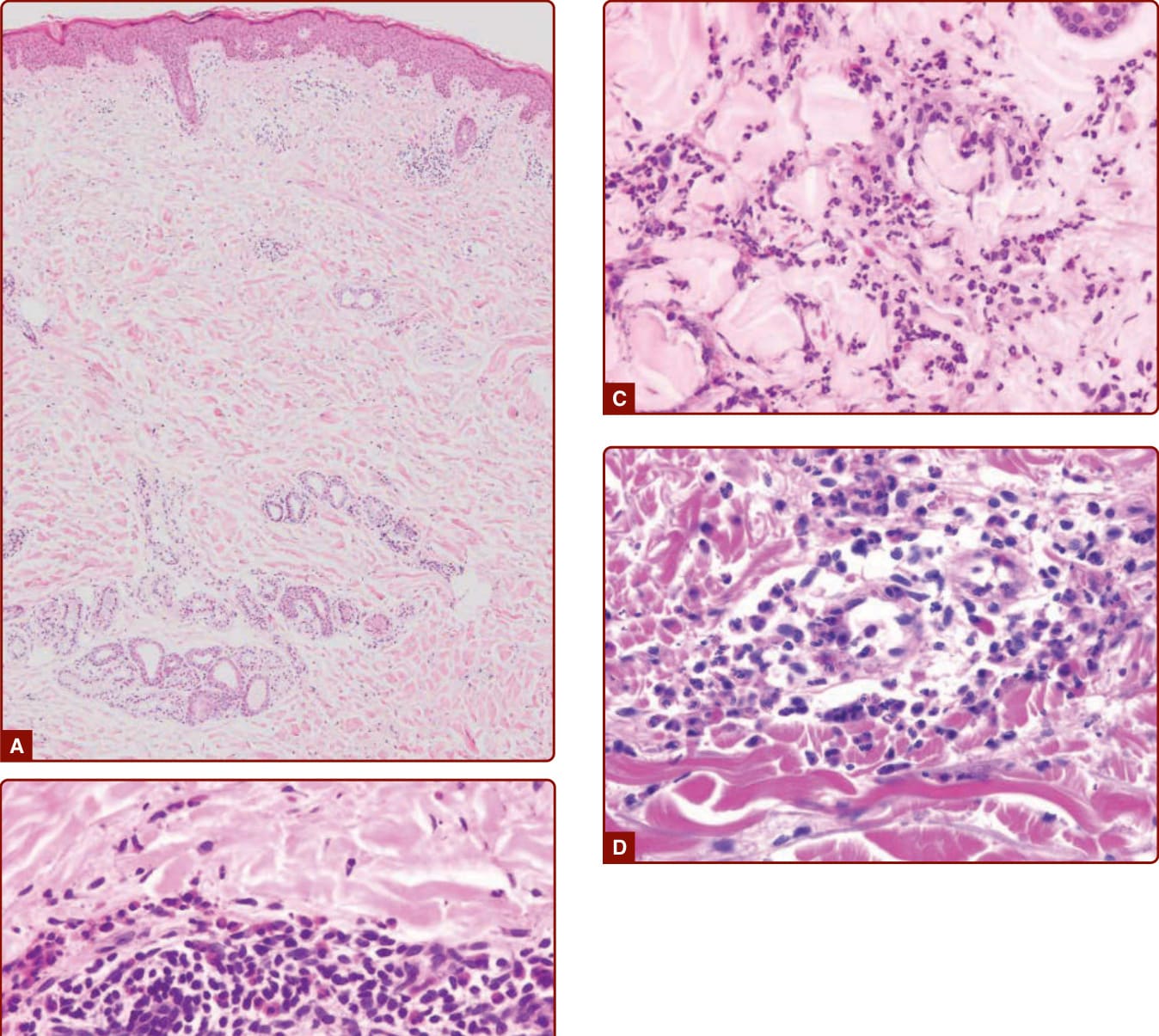
Figure 41-6 Histopathological presentation of urticaria. A, Edema of the dermis. B, Perivascular infiltration of lymphocytes and eosinophils. C, Neutrophilic urticaria. D, Urticarial vasculitis. (Reproduced from Shindo H. Histopathology of urticaria (Jinmashin No Byouri-Soshiki-Zou), In: Furue M, Hide M eds. Hifuka Asset 16. Tokyo, Japan: Nakayama-Shoten; 2013:62-70.)
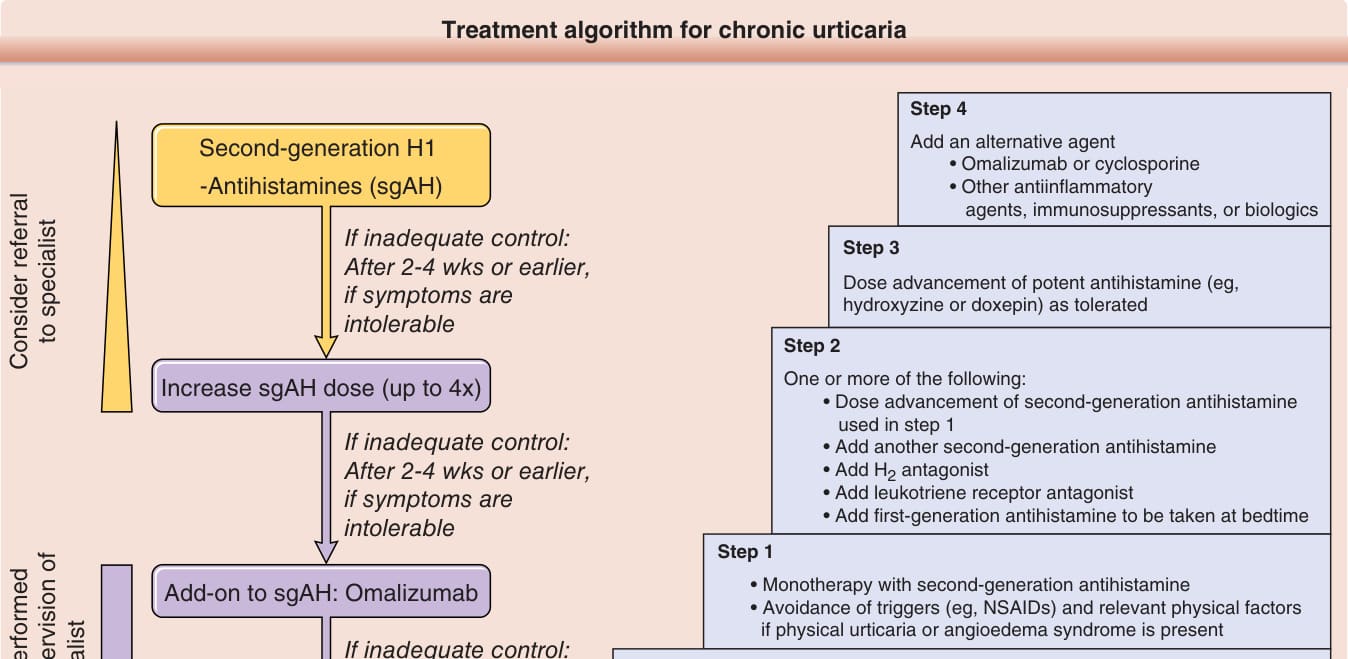
Figure 41-7 Treatment algorithm for chronic urticaria recommended by the European Academy of Allergy and Clinical Immunology/Global Allergy and Asthma European Network/European Dermatology Forum/World Allergy Organization (A) and that for chronic urticaria by the American Academy of Allergy, Asthma and Immunology and the American College of Allergy, Asthma and Immunology (B). NSAID, nonsteroidal antiinflammatory drug. (Image A, from Zuberbier T, Aberer W, Asero R, et al. The EAACI/GA(2) LEN/EDF/WAO Guideline for the definition, classification, diagnosis, and management of urticaria: the 2017 revision and update. Allergy. 2018;73:1393-1414, with permission. Copyright © 2018 EAACI and John Wiley and Sons. Image B, From Bernstein JA, Lang DM, Khan DA, et al. The diagnosis and management of acute and chronic urticaria: 2014 update. J Allergy Clin Immunol. 2014;133:1270-1277, with permission. Copyright © American Academy of Allergy, Asthma & Immunology.)
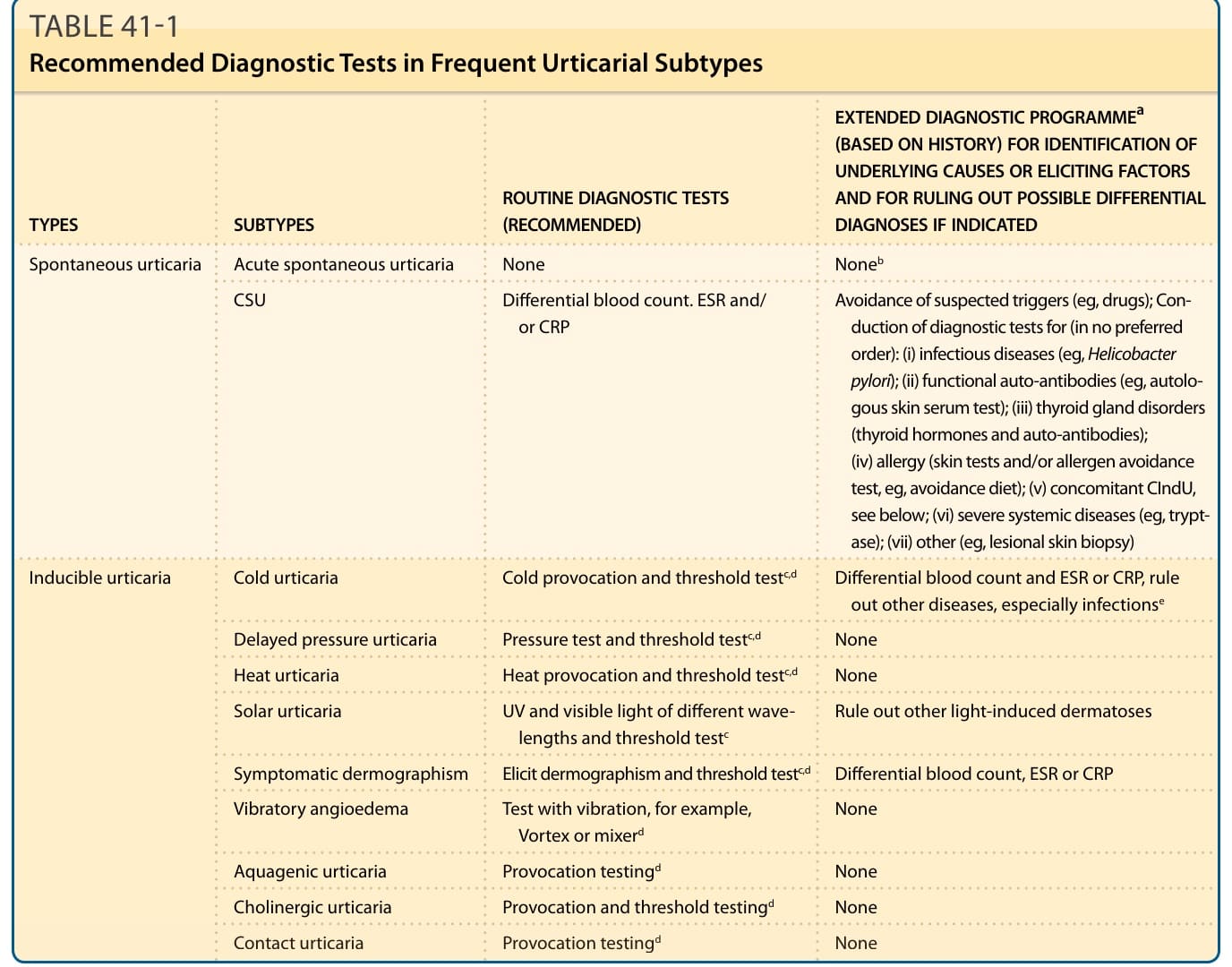
TABLE 41-1 Recommended Diagnostic Tests in Frequent Urticarial Subtypes
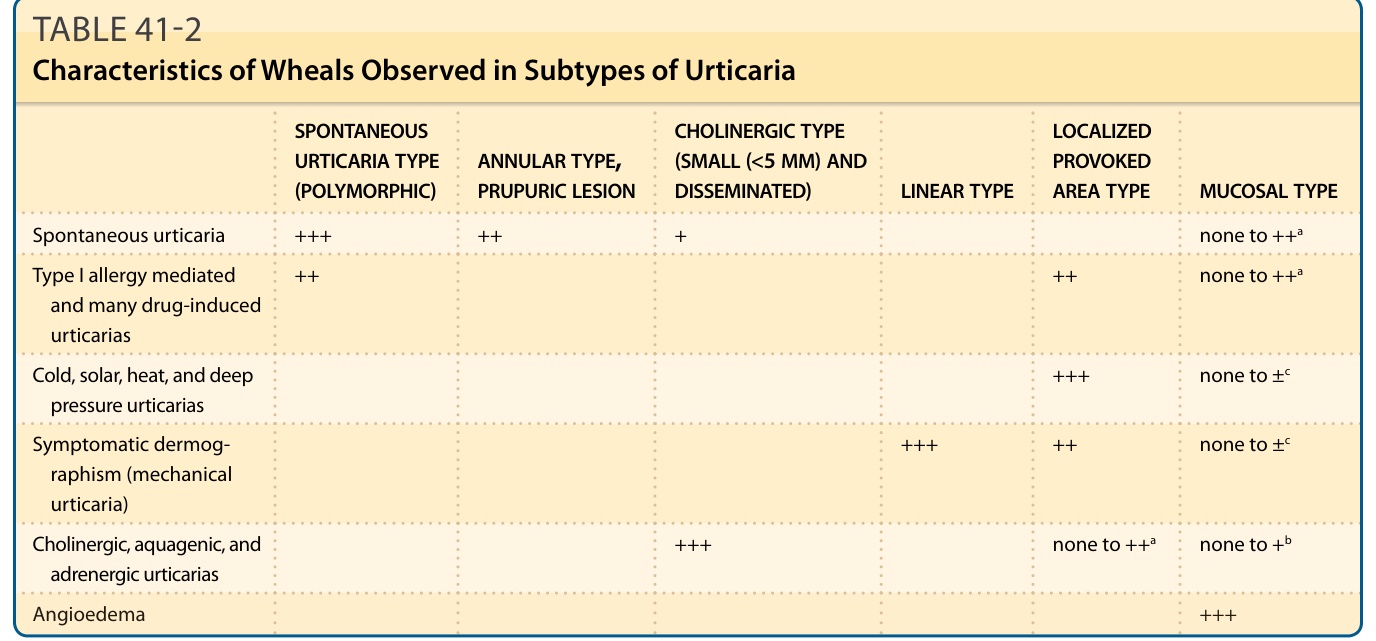
TABLE 41-2 Characteristics of Wheals Observed in Subtypes of Urticaria
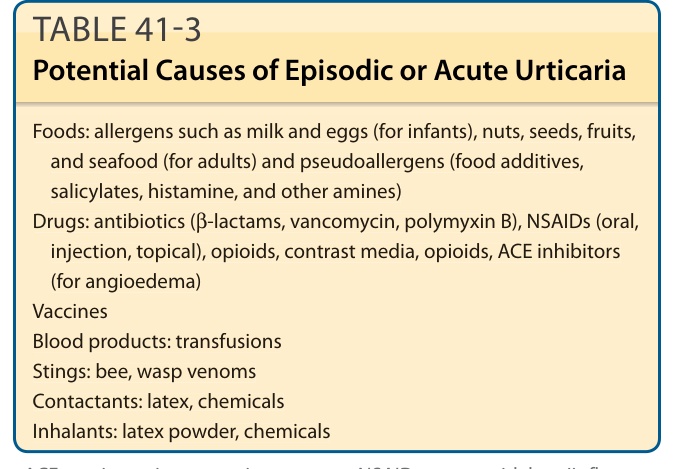
TABLE 41-3 Potential Causes of Episodic or Acute Urticaria
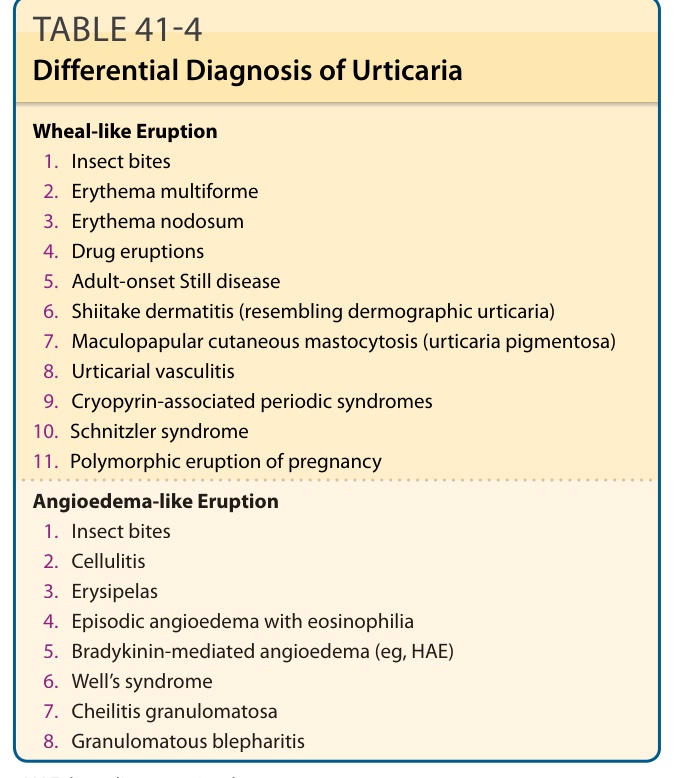
TABLE 41-4 Differential Diagnosis of Urticaria