Eosinophilic Diseases
6
REGULATION OF THE PRODUCTION AND ACTIVATION OF EOSINOPHILS
AT-A-GLANCE
■ Eosinophils are bone marrow–derived cells that circulate transiently and normally account for up to 6% (up to 600/mm3) of circulating blood leukocytes.
■ Eosinophils primarily are tissue-dwelling cells, but only in certain tissues in humans, with an average tissue life span of 2 to 5 days that may be increased with eosinophil survival factors for up to 14 days.
■ As proinflammatory cells, the presence of eosinophils within most tissues is associated with pathologic states that include infections, allergic reactions and atopic diseases, fibrotic disorders, reactive eosinophilias, and hypereosinophilic syndromes.
■ Eosinophils play a role in innate and adaptive immune responses, which may explain why they are present in normal, noninflamed tissues such as the gastrointestinal tract and lymphoid tissues.
■ This section reviews the biologic actions of eosinophils with particular focus on what controls eosinophil production, activation, and tissue trafficking.
■ Pharmacologic manipulation of eosinophil inflammation is possible as new, more specific strategies are emerging.
ONTOGENY AND DEVELOPMENT
ONTOGENY AND
DEVELOPMENT
Eosinophils develop in the bone marrow from multipotential, stem cell–derived CD34+ myeloid progenitor cells in response to eosinophilopoietic cytokines and growth factors (Fig. 40-1). They are released into the circulation as mature cells.1-3 Important stimulatory cytokines and growth factors for eosinophils include interleukin (IL)-3, granulocyte-macrophage colonystimulating factor (GM-CSF), and IL-5. Activated T cells likely are the principal sources of IL-3, GM-CSF, and IL-5 that induce eosinophil differentiation in bone
marrow. However, depending on pathogenic stimuli, eosinophilopoietic cytokines may be released by other cell types, including mast cells, macrophages, natural killer cells, endothelial cells, epithelial cells, fibroblasts, and even eosinophils, themselves.4 IL-3 and GM-CSF are pluripotent cytokines that have effects on other hematopoietic lineages. IL-5 is the most selective eosinophil-active cytokine, but it is relatively late acting. Although it is both necessary and sufficient for eosinophil differentiation, IL-5 demonstrates maximum activity on the IL-5 receptor (IL-5R)–positive eosinophil progenitor pool that first is expanded by earlier acting pluripotent cytokines such as IL-3 and GM-CSF4; expression of the high-affinity IL-5R is a prerequisite for eosinophil development. Exodus from the bone marrow also is regulated by IL-5. IL-3 and GM- CSF, along with IL-5, promote survival, activation, and chemotaxis of eosinophils through binding to receptors that have a common β chain (CD131) with IL-5R, and unique α chains.
INTERACTIONS OF EOSINOPHILIC FACTORS AND CYTOKINES AND INTRACELLULAR SIGNALING
INTERACTIONS OF
EOSINOPHILIC FACTORS
AND CYTOKINES AND
INTRACELLULAR SIGNALING
The interactions of eosinophilopoietic factors with their receptors stimulate a cascade of complex biochemical events through signal transduction. Signaling events progress in 4 steps: (a) juxtamembranous signaling in which membrane-anchored tyrosine kinases and lipid kinases are activated; (b) signal interfacing which serves to transduce juxtamembranous signals to cytosolic signals; (c) mobile signaling in which cytosolic signaling molecules translocate from the receptor site to other cellular compartments including the nucleus, mitochondria, and cytoskeleton; and (d) transcription activation resulting from nuclear translocation and initiation of gene transcription. Studies show the pivotal role of IL-5 in immune responses involving eosinophils through receptordriven signaling.5 IL-5 binds to the α chain of the IL-5R and induces recruitment of the common β (βc) chain to IL-5R. Janus kinase (JAK) 2 tyrosine kinase is constitutively associated with IL-5Rα, and JAK1 tyrosine kinase with IL-5Rβc; both are activated with IL-5 binding as part of the juxtamembranous step. Adaptor proteins, src homologs and collagen (Shc), SH2-containing phosphatase-2 (SHP-2), growth factor receptor-bound protein 2 (Grb2), Vav, and lipid
6
Eosinophils from undifferentiated hematopoietic cells to their fate in tissue
Transcription factors
GATA-1 FOG-1 C/EBPα Pu.1
Differentiation in bone marrow
CD34+
IL-5
CCL11
Release into circulation
L-selectin is shed
IL-5Rα+ CCR3
Rolling
P-selectin
Cytokines
IL-3 GM-CSF IL-5
CD34
IL-5Rα
CD34+ IL-5Rα+
CCR3 L-selectin
CD34+ IL-5Rα+ CCR3 L-selectin
VLA4
Tethering Flattening Diapedesis
VCAM-1 E-selectin ICAM-1
CCL24
CCL11
CCL26 LTB4
Transmigration through blood vessels into skin
Fate in tissue
FAS (CD95) TGFβ Siglec-8 Bcl-2
CD30 CD45 CD52 CD69
Degranulation: Apoptosis
Dermal eosinophil
Cytolytic Piecemeal Regulated secretion/ exocytosis
TNFα IFNγ CD40 Leptin
GM-CSF IL-3 IL-5
Priming, activation, and survival
650
kinases, phosphatidylinositol 3-kinase, function in the interfacing step. The activation of JAK2 and signal transducer and activator of transcription (STAT) 5 is essential for IL-5–dependent signal transduction. The Ras guanosine triphosphatase–extracellular signalregulated kinase and also known as Ras–mitogenactivated protein kinase pathway, in addition to the JAK2-STAT5 pathway, is important in IL-5 signaling in the mobile step. The JAK-STAT and Ras–mitogenactivated protein kinase pathways converge at various levels in IL-5 signaling of eosinophils. Multiple other interactive signal transduction pathways induce
6
and regulate gene expression for eosinophil growth, development, activation, and survival.6
EOSINOPHIL ULTRASTRUCTURE AND GRANULE CONTENT
EOSINOPHIL
ULTRASTRUCTURE AND
GRANULE CONTENT
Products of eosinophils and localization of distinctive granule proteins
Reactive oxygen intermediates
Miscellaneous
Lipid mediators
Leukotriene C4/D4/E4 Eoxin C4/D4/E4 Prostaglandin E1/E2/F1α 5-HETE 5,15- and 8,15-diHETE Platelet-activating factor (PAF) Thromboxane B2
Galectin-10 (Charcot-Leyden crystal protein) Mitochondrial DNA (DNA traps)
O2 H2O2 Hydroxyl radicals Singlet oxygen
Enzymes
β-Glucuronidase Arylsulfatase B Acid phophatase Catalase Histaminase Collagenase Matrix metalloproteinase 9 α-Mannosidase Phospholipase A2 Cyclooxygenases 5-Lipoxygenase 15-Lipoxygenase Leukotriene C4 synthase Lysozyme NADPH oxidase
A
CCL5
MBP-1
MBP-2
EPO EDN ECP
B
Granule-derived proteins
Major basic protein (MBP)-1 Eosinophili peroxidase (EPO) Eosinophil derived neurotoxin (EDN or RNase2) Eosinophil cationic protein (ECP or RNase3) MBP-2
Cytokines
GM-CSF, IFNγ, IL-1, IL-2, IL-3, IL-4, IL-5, IL-6, CXCL8 (IL-8), IL-10, IL-12, IL13, IL-16, TGF-α, TGF-β1, fibroblast growth factor-2, vascular endothelial growth factor, nerve growth factor, TNF-α, MIP-1α, PDGF, CCL3, CCL5, CCL11, CXCL13
Surface receptors
CCR3, CD4, LTB4, PAF, C3a, C5a, CR1, CR3, IgA (CD89), IgG (CD16, CD32); immunoglobulin-like, CD50 and CD54, CD62L, VCAM-1 (CD106); cytokine receptors - IL-1, IL-2 (CD25), IL-3 (CD123), IL-4 (CD124), IL-5 (CD125), IL-8, IL-9 (CD129), IL-13, IL-31, GM-CSF (CD116), IFN-γ (CD119), TNF-α (CD120), TGF-β; adhesion molecules - integrins, β1, β2, β7; selectins, carbohydrates, enzymes, histamine, stem cell factor, HLA-DR, β adrenergic, PAR-2, TLR-7, TLR-8, CD48; and apoptosis and signaling factors, CD30, CD45, CD52, CD69, CD95
651
6
Mature eosinophils are 12 to 17 µm in diameter and, therefore, slightly larger than neutrophils. They typically have a bilobed nucleus with highly condensed peripheral chromatin. Eosinophils have distinctive cytoplasmic granules, demonstrated by their staining properties with acidic dyes such as eosin, and by their unique electron microscopy appearance. These specific or secondary granules are composed of an electrondense core and a less-electron-dense matrix, the core being a crystalline lattice by electron microscopy. In cross section, the eosinophil contains approximately 30 of these membrane-bound, core-containing, secondary granules.1 Five highly basic proteins are found within the granules: (a) major basic protein (MBP)-1, (b) MBP-2, (c) eosinophil-derived neurotoxin (EDN) also known as ribonuclease (RNase)2, (d) eosinophil cationic protein (ECP) also known as RNase3, and (e) eosinophil peroxidase (EPO). Several other types of proteins are found in secondary granules and include enzymes, cytokines, growth factors, and chemokines. Eosinophils contain 3 other types of cytoplasmic granules, referred to as (a) primary granules, (b) small granules, and (c) secretory vesicles. Primary granules are of variable size, round, uniformly dense, present in 1 to 3 per electron microscopy cross section, and more common in immature eosinophilic promyelocytes. These granules may contain Charcot-Leyden crystal protein (also known as galectin-10), which also can be found in neutrophils7; Charcot–Leyden crystals are characteristically found in asthmatic sputum and in feces from patients with helminth infections or eosinophilic gastroenteritis. Small granules contain acid phosphatase and arylsulfatase and are present at 2 to 8 per electron microscopy cross section. Secretory vesicles, also referred to as tubulovesicular structures or microgranules, are characterized by their small, dumbbell-shaped appearance and their albumin content. They are the most abundant granules in number, with approximately 160 per electron microscopy cross section. Normal eosinophils contain varying numbers of non–membrane-bound lipid bodies, which are the principal stores of arachidonic acid. Lipid bodies also contain the enzymes, cyclooxygenase, 5- and 15-lipoxygenase, which are required to synthesize prostaglandins, leukotrienes (LTs), and eoxins, and are increased in activated eosinophils.1
BIOLOGIC FUNCTIONS
BIOLOGIC FUNCTIONS
In mammals, such as the mouse and humans, the eosinophil is released as a mature cell into the circulation from the bone marrow, but is present in the blood only transiently, ranging from 8 to 18 hours. Eosinophils comprise a small portion, normally 6% or less, of circulating leukocytes. They are primarily tissuedwelling cells, but only in certain tissues in humans, with an average tissue life span of 2 to 5 days. This may be prolonged by cytokines that increase eosinophil survival for up to 14 days. Under normal circumstances, a
652
balance exists between bone marrow production and release of eosinophils, their time in circulation, and their entrance into tissues. Changes in any one of the compartments causes an increase or decrease in circulating and tissue eosinophils. Eosinophilia in blood or tissue or both is associated with helminthiasis, allergic hypersensitivity, and other pathologic conditions. In humans, bone marrow, spleen, lymph node, thymus, and gastrointestinal tract from the stomach through the colon, sparing the esophagus, are the only tissues in which eosinophils normally reside.8 Furthermore, the gastrointestinal tract is the only organ other than bone marrow in which extracellular eosinophil granule protein deposition is observed even under homeostatic conditions. Eosinophils and their granule proteins are found in the lamina propria in normal gastrointestinal tract and are not found in Peyer patches or epithelium. Eosinophils in the lamina propria are reported to be able to induce the differentiation of regulatory T cells by producing transforming growth factor (TGF)-β1 and all-trans retinoic acid.9 The recruitment of eosinophils to the gastrointestinal, thymic, uterine, and mammary tissues is under the control of the CC chemokine, CCL11.10,11 Eosinophils can also respond to tissue-damage signals and promote tissue remodeling. One study showed that eosinophils can migrate to areas of tissue injury or necrosis though the high-mobility group box-1 protein (HMGB1) released from necrotic cells and the receptor for advanced glycation end products expressed on eosinophils.12 Moreover, it is proposed that eosinophils may play a role in the repair of gastric mucosal tissue during Helicobacter pylori infection.13
Once eosinophils enter tissues, most do not recirculate. Several possible mechanisms exist for removal of tissue eosinophils, including shedding of the cells across mucosal surfaces into the lumen of the intestinal or respiratory tract, engulfment of apoptotic eosinophils by macrophages, and lysis or degranulation with cellular degeneration. In various inflammatory conditions, including those affecting the skin, striking numbers of free granules and/or eosinophil granule protein deposition are present in the absence of intact eosinophils.1 Isolated eosinophil granules express extracellular domains for interferon (IFN)-γ receptor and CCR3 and, upon stimulation, respond independently as organelles by releasing ECP.14
ROLE OF EOSINOPHILS IN IMMUNE FUNCTION
ROLE OF EOSINOPHILS IN
IMMUNE FUNCTION
Shortly after their discovery by Paul Ehrlich in 1879, eosinophils were observed in association with helminth infections. Theories have been promulgated that eosinophils are important for host defense against parasites spawning numerous studies.15 For example, in vitro studies demonstrated that eosinophils are cytotoxic to large nonphagocytosable organisms, such as multicellular helminthic parasites. Eosinophils bind
to host-derived immunoglobulins and complement components on the surface of their targets (so-called antibody- or complement-) dependent cytotoxicity. They also bind to carbohydrate ligands expressed on parasites, such as the LewisX-related molecules, and cell adhesion molecules similar to selectins. Eosinophils are activated to release their granule products with deposition of these biologically active proteins in and around the parasites causing disruption of the parasite’s integument and, ultimately, death of the organism. The granule proteins have different effects. ECP produces fragmentation and disruption whereas MBP-1 produces a distinctive ballooning detachment of the tegumental membrane, and EDN is active only at high concentrations, causing crinkling of the tegumental membrane.16 However, in murine models in which blood, marrow, and tissue eosinophilia is largely abolished by neutralizing IL-5 activity, the intensities of primary or secondary parasitic infection are unchanged, indicating that eosinophils have little or no role in parasitic host defense in these models.1 The results must be interpreted cautiously because mouse and human eosinophils have functional differences, and mice are not natural hosts of many of the parasites tested experimentally. Eosinophils also release cytotoxic granule proteins onto the surface of fungal organisms and into the extracellular milieu in fungal infections. Eosinophils kill fungi in a contact-dependent manner. Eosinophils adhere to the fungal cell wall component, β-glucan, via a β2-integrin surface molecule, CD11b.17 Eosinophils do not express other common fungal receptors, such as dectin-1 and lactosylceramide, and, specifically, do not react with chitin. However, chitin, which is a polymer that confers structural rigidity to fungi, helminths, crustaceans, and insects, induces accumulation of eosinophils in tissues through production of LTB4 in mice.18 Eosinophils also are activated by fungal organisms that release proteases, such as Alternaria, through protease-activated receptors (PARs). For example, fungal aspartate protease activates eosinophils through PAR-2, thereby mediating the innate responses of eosinophils to certain fungi.19
As a granulocyte, the eosinophil is capable of phagocytosing and killing bacteria and other small microbes in vitro, but eosinophils cannot effectively defend against bacterial infections when neutrophil function is deficient. Nevertheless, investigations reveal that eosinophils may have a role in innate immunity against bacteria using a unique mechanism, DNA trap.20 Eosinophils rapidly release mitochondrial DNA when exposed to bacteria, a complement component, C5a, or CCR3 ligands. The traps contain eosinophil granule proteins, ECP and MBP, and have antimicrobial effects. In the extracellular space, the granule proteins and mitochondrial DNA form structures that bind and kill bacteria both in vitro and in vitro. Eosinophils, unlike neutrophils, do not undergo cell death as part of this process. This may be an important innate immune response, particularly in mucosal epithelium.20
Eosinophils may have other roles in immune responses as well. Through major histocompatibility
6
complex class II expression and IL-1α production, they can function as antigen-presenting cells for a variety of viral, parasitic, and microbial antigens, including staphylococcal superantigens, and allergens.21,22
Eosinophils are recruited to secondary lymphoid structures to promote the proliferation of effector T cells, even though they are unable to affect naïve T cells.23
Eosinophils, as sources of cytokines, influence T-cell– dependent responses.1 In keeping with the prominence of eosinophils in allergic disorders, eosinophils are involved in T-cell polarization favoring T-helper (Th)2 by promoting Th1 apoptosis in addition to their influence via cytokine expression.21,24-27
Interestingly, it is also reported that eosinophils play a role in helminth parasite-elicited protection against autoimmunity, as observed in a mouse model of multiple sclerosis.28
In allograft rejection, a number of studies have demonstrated the diagnostic and prognostic value of eosinophils, especially in the acute rejection of allografts.29,30
On the other hand, a recent study indicated that a lower eosinophil count in peripheral blood predicts adverse prognosis of allograft rejection in heart transplant patients.31 Further investigation into these possible roles of eosinophils and their mechanisms in acute allograft rejection is warranted.
ROLE OF EOSINOPHILS IN DISEASE
ROLE OF EOSINOPHILS
IN DISEASE
The activities of eosinophil-derived products include direct cytotoxic effects on structural cells and microbes, increased vascular permeability, procoagulant effects, innate immune responses to some parasites, viruses, fungi, and tumor cells, enhancement of leukocyte migration, amplification of effector T-cell responses, and, possibly, mammary gland development. Collectively, these varied biologic actions provide the pathophysiologic basis for the signs and symptoms observed in eosinophil-associated diseases. Eosinophils in lymph nodes and spleen are especially increased after allergen exposures or microbial insults.32,33 In allergic inflammation, the involvement of eosinophils is promoted by the stimulation of thymic stromal lymphopoietin, a cytokine that is mainly secreted by epithelial cells in response to allergens or other environmental stimuli.34-36 Eosinophils have been found in several cancers, particularly in lymphomas, leukemias, and colon cancer. Clinical studies indicate that certain tumors associated with tissue and/or peripheral eosinophilia have a more favorable prognosis,37 whereas in other tumors, such as nodular sclerosing Hodgkin disease, Sézary syndrome, and gastric carcinomas, they are thought to confer a poor prognosis. In Sézary syndrome, the tumor cells produce IL-5 and, therefore, are responsible for the eosinophilia, which is a reflection of tumor burden.38 Where eosinophilia is a good prognostic factor, eosinophils are considered to be part of an effective host response to the tumor.39,40
653
6
EOSINOPHIL CONSTITUENTS AND THEIR ACTIVITIES
EOSINOPHIL CONSTITUENTS
AND THEIR ACTIVITIES
The eosinophil contains and produces myriad factors that implicate its role in inflammation and tissue destruction and remodeling (see Fig. 40-2).41
Products released by eosinophils include chemoattractants, colony-stimulating factors, and endothelial-activating cytokines. In addition to toxic cationic proteins from specific granules and oxidative products released into tissues following activation, these factors include arachidonic acid–derived lipids, hydrolytic enzymes, neuropeptides, colonystimulating factors, and cytokines/chemokines that facilitate further leukocyte recruitment to sites of inflammation (see Fig. 40-2). Surface molecule expression is important in all aspects of eosinophil biology, from promoting growth and differentiation to eosinophil trafficking into tissue to activation and/or priming of the cells to senescence. Numerous membrane factors are expressed on eosinophils that further direct eosinophil biologic effects.
EOSINOPHIL GRANULE PROTEINS
Among the products of eosinophils that are most damaging to the host are the specific granule’s cationic proteins. Knowledge of their biologic actions provides insight into their functions in human disease. Once deposited, the granule proteins persist in tissues for extended times—EPO for 1 week, ECP for 2 weeks, EDN for 2.5 weeks, and MBP-1 for 6 weeks.42 Each of these proteins induces direct tissue damage to both host cells, including myocytes, endothelium, neurons, epithelium, and smooth muscle, and microbes. All 4 of the cationic granule proteins (EPO, ECP, EDN, and MBP-1) likely contribute to the edema observed in skin diseases because of their vasodilatory effects, with contribution from mast cells and basophil histamine release by MBP-1.43 Eosinophil granule proteins stimulate various cells in addition to mast cells and basophils, including neutrophils and platelets. Nodules, eosinophilia, rheumatism, dermatitis, and swelling (NERDS), episodic angioedema with eosinophilia (Gleich syndrome), urticaria, eosinophilic cellulitis (Wells syndrome), and insect bite reactions demonstrate variable degrees of edema that are probably explained, at least in part, by this mechanism. Eosinophil granule proteins injected into skin produce lesions, including dose-dependent wheal-andflare reactions by MBP and ulcerations by ECP and EDN.44,45
MAJOR BASIC PROTEIN
MBP comprises the crystalloid core of the specific eosinophil granule. It was so named because it accounts
654
for a major portion (approximately 55% in guinea pig) of the eosinophil granule protein and has a high isoelectric point (calculated at greater than pH 11) that is so strongly basic it cannot be measured accurately. It is now known that MBP is expressed as 2 homologs, MBP-1 and MBP-2, coded by different genes on chromosome 11. MBP-1 directly damages helminths and also lethally damages mammalian cells and tissues, examples of which are its ability to cause exfoliation of bronchial epithelial cells and to kill tumor cells. MBP-1 exerts its effects by increasing cell membrane permeability through surface charge interactions leading to disruption of the cell-surface lipid bilayer. MBP-1 and MBP-2, but none of the other eosinophil granule proteins, stimulate histamine and LTC4 release from human basophils. Furthermore, MBP-1 and MBP-2 stimulate neutrophils, inducing release of superoxide, lysozyme, and IL-8. MBP-1 and EPO are potent platelet agonists causing release of 5-hydroxytryptamine and promoting clotting.
EOSINOPHIL PEROXIDASE
EPO is highly basic, pI 10.8, localized in the matrix of the specific eosinophil granule and is a key participant in generating reactive oxidants and free radical species in activated eosinophils. EPO consists of a heavy chain and a light chain encoded with a prosequence. Although MBP is present in the highest molar concentration in eosinophil granules, EPO, by weight, is the most abundant protein constituting approximately 25% of the specific eosinophil granule’s total protein mass. EPO kills numerous microorganisms in the presence of hydrogen peroxide, generated by eosinophils and other phagocytes, and halide. This combination of products also initiates mast cell secretion. EPO binding to microbes, including Staphylococcus aureus, greatly potentiates their killing by phagocytes. EPO-coated tumor cells are spontaneously lysed by activated macrophages.
EOSINOPHIL CATIONIC PROTEIN AND EOSINOPHIL-DERIVED NEUROTOXIN
ECP (or RNase3) and EDN (or RNase2) are homologous proteins with sequence identity in 37 of 55 amino acid residues. ECP also has neurotoxic activity. ECP and EDN play a role in viral host defense to RNA viruses.46-48 EDN induces the migration and maturation of dendritic cells.49 It also is an endogenous ligand of Toll-like receptor 2 (TLR2) and can activate myeloid dendritic cells by triggering the Toll-like receptor 2–myeloid differentiation factor 88 signaling pathway.27 Based on its ability to serve as a chemoattractant and activator of dendritic cells along with enhancing antigen-specific Th2-biased immune responses, EDN functions as an alarmin, alerting the adaptive immune system to preferentially enhance antigen-specific Th2 responses.27
LIPID MEDIATORS
Lipid bodies in eosinophils are storage sites for arachidonic acids. Eosinophils produce several arachidonic acid metabolites, including cysteinyl LTs from the 5-lipoxygenase pathway (LTC4, LTD4, and LTE4) and thromboxanes and prostaglandins (PGs) from the cyclooxygenase pathway (thromboxane B2, PGE2, and PGF1α).50,51
CYTOKINES
Eosinophils are a considerable source of growth factors and regulatory and proinflammatory cytokines and chemokines.1,52 The various growth factors produced by eosinophils include TGF-α, TGF-β, fibroblast growth factor (FGF)-2, vascular endothelial growth factor, nerve growth factor, and plateletderived growth factor (PDGF)-β. There is evidence that these growth factors induce stromal fibrosis and basement membrane thickening at sites of chronic eosinophilic inflammation including nasal polyps, asthmatic airways and, likely, in certain skin disorders, such as atopic dermatitis.1 Another group of cytokines produced by eosinophils modulates other immune cells and includes tumor necrosis factor (TNF)-α, macrophage inflammatory protein-1α (CCL3), IL-1α, IL-2, IL-3, IL-4, IL-5, IL-6, CXCL8 (IL-8), IL-10, IL-12, IL-13, IL-16, GM-CSF, and IFN-γ.52 Additional chemokines produced by eosinophils are CXCL13 (B-lymphocyte chemoattractant factor), CCL5 (regulated on activation, normal T cells expressed and secreted [RANTES]), and CCL11, in addition to CCL3 and CXCL8. All these cytokines are constitutively produced in low levels in resting eosinophils and induced in inflammatory conditions with activation of eosinophils by engagement of receptors with immunoglobulins, complement and cytokines, including those produced by eosinophils, themselves, in an autocrine manner. Notably, eosinophils produce the 3 principal cytokines involved in their own growth and differentiation—IL-3, IL-5, and GM- CSF—as well as CCL5 and CCL11, the chemokines important in their own chemotaxis. In summary, the eosinophil-derived cytokines may function in both an autocrine and paracrine fashion and likely have pathophysiologic relevance.
SURFACE EXPRESSION
SURFACE EXPRESSION
Eosinophils express numerous receptors and other factors on their surface membranes through which they communicate with the extracellular environment, but no single surface protein is uniquely expressed on eosinophils. These receptors have been identified either by flow cytometry or by functional assays, and can be grouped as follows: chemotactic factor and complement receptors, including chemokine, LT, and platelet-activating factor (PAF);
6
immunoglobulin supergene family member receptors, including immunoglobulins; cytokine receptors; adhesion molecule receptors; receptors involved in apoptosis; and miscellaneous receptors and surface factors. Eosinophil membrane proteins are promising targets for therapeutic modulation of eosinophil effects (see “Pharmacologic Manipulation” below).
CHEMOTACTIC FACTOR AND COMPLEMENT RECEPTORS
Chemotactic factors are important in orchestrating cellular trafficking to sites of inflammation as well as physiologic homing (eg, eosinophils to gastrointestinal tract). The eosinophil has receptors for many chemotactic agents, including LTB4, PAF, bacterial products (N-formyl-methionyl-leucyl-phenylalanine), and the complement anaphylatoxins C3a and C5a. Eosinophils express complement receptor (CR)1 (CD35), a receptor for C1q that also binds C4b, C3b, and iC3b, and CR3 (Mac-1, CD11b/CD18) in addition to receptors for C3a and C5a. These are important receptors in eosinophil effector functions. The binding of chemokines to their respective receptors mediates many biologic effects, which, in addition to cell shape change and migration, includes cell activation, receptor internalization, induction of the respiratory burst with generation of toxic oxygen metabolites, and transient activation of integrin adhesiveness. The chemotaxins listed above have potent effects on eosinophils but are nonselective in that they are active on other leukocytes. Because many eosinophil-associated diseases are characterized by tissue eosinophil infiltration with little or no neutrophil infiltration, the identification of the CCR3 receptor and its ligands was an important breakthrough in discovering eosinophil-selective chemotaxins.53 Specific members of the chemokine family are critical for the cellular trafficking of eosinophils. The major ligands of CCR3, CCL5, CCL11, CCL13 (monocyte chemotactic protein-4), CCL24 (eotaxin-2), and CCL26 (eotaxin-3) play a critical role in both the homeostatic and inflammation-induced recruitment of eosinophils to tissue sites.54,55
IMMUNOGLOBULIN GENE SUPERFAMILY MEMBER RECEPTORS
Many of the studies of eosinophil functions, including phagocytosis, antigen-dependent cytotoxicity, oxygen metabolism, LTC4 production, and eosinophil survival, have been performed using immunoglobulin (Ig) G-coated targets. Among eosinophil surface receptors for the Ig family members, the most highly expressed receptor is FcγRII (CD32), which binds aggregated IgG, particularly of the subclasses IgG1 and IgG3. The binding of IgG to this receptor may be important in eosinophil degranulation in parasitic and allergic diseases, along with other eosinophil functions.1 Freshly isolated eosinophils express only FcγRII (CD32) of the IgG receptors, but eosinophils can be stimulated by
655
6
cytokines, particularly IFN-γ, to express FcγRI (CD64) and FcγRIII (CD16), as well as to augment FcγRII (CD32) expression. Intercellular adhesion molecule (ICAM)-1 (CD54) and ICAM-3 (CD50) are members of Ig superfamily expressed on eosinophils and are likely important in leukocyte–leukocyte and leukocyte–tissue cell adhesion through leukocyte function-associated antigen-1 (αLβ2; CD11a/CD18) as its counterligand (see Fig. 40-1).
CYTOKINE RECEPTORS
Cytokine receptors are present at low levels on the surfaces of eosinophils. Receptors for IL-3 (CD123), IL-5 (CD125), and GM-CSF (CD116) are readily detected and, all share a common β chain (CD132). Eosinophil activation has been observed by a variety of other cytokines through presumed and/or detected receptors. These include stem cell factor (c-kit receptor; CD117), IFN-γ (CD119), TNF-α (CD120), IL-4 (CD124), IL-9 (CD129 and CD132), IL-13 (gp65), IL-2 (CD25), IL-31, and TGF-β receptors. Many of these receptors are for cytokines that eosinophils produce, providing further evidence that they have autocrine functions.
ADHESION MOLECULE RECEPTORS
Adhesion molecule receptors are expressed on the eosinophil cell surface to mediate trafficking to and within tissues, and for general cell–cell interactions.56 These receptors fall into three groups: (a) Ig superfamily, (b) selectins and their glycoprotein counterligands, and (3) integrins. L-selectin (CD62L) and P-selectin glycoprotein ligand-1 (PSGL-1, CD162) are expressed at high levels on eosinophils, whereas E-selectin ligands, as an example, sialyl–Lewis-X (CD15s), are expressed at very low levels. P-selectin together with PSGL-1 is the most important selectin pair in eosinophil migration into tissues. Eosinophils express a variety of integrins (β1, β2, and β7) on their surface, which facilitate their adhesion to extracellular matrix proteins, vascular cellular adhesion molecule (VCAM)-1 (CD106) on activated endothelium, or ICAM-1 present on resting or activated epithelium and activated endothelium. Integrins are composed of 2 subunits that exist as noncovalently associated heterodimers, with α and β subunits. The β1 integrins expressed on eosinophils include α4β1 (very late antigen [VLA]-4), which binds to VCAM-1 found on activated endothelium and the extracellular matrix protein, fibronectin. Eosinophil adhesion to fibronectin induces the autocrine production of eosinophilactivating survival cytokines, IL-3, IL-5, and GM-CSF.
RECEPTORS INVOLVED IN APOPTOSIS
Eosinophils express several “death receptors,” which are involved in apoptotic pathways, such as Fas
656
receptor (CD95), Siglec-8, CD30, CD45, Campath (CD52), and CD69, along with important intracellular regulators of eosinophil apoptosis, such as the members of the B-cell leukemia/lymphoma (Bcl)-2 and inhibitor of apoptosis families.57 Diseases characterized by eosinophilia likely result, in part, from delayed or defective apoptotic pathways allowing accumulation and persistence of eosinophils in blood and/or tissues.
FACTORS WORKING TOGETHER
FACTORS WORKING
TOGETHER
The various products elaborated by eosinophils in response to receptor activation do not necessarily function independently but often act in concert to mediate their biologic effects. For example, the release of TGF-α, TGF-β, FGF-2, vascular endothelial growth factor, matrix metalloproteinase-9, and inhibitors of matrix metalloproteinases from activated eosinophils collectively induce fibroblast proliferation and extracellular matrix protein production. Eosinophils contribute factors of their own and influence factor production from other cells; for example, eosinophil mediators induce platelet release of TGF-β. After intradermal eosinophil infiltration, there is production of extracellular proteins, including tenascin and procollagen 1, as well as myofibroblast formation.58 Eosinophil-induced fibrosis is observed in the lungs and heart of patients with hypereosinophilic syndrome, in and around organs in other fibrosing/sclerosing disorders, and in the skin of patients with eosinophilic fasciitis (Shulman syndrome), eosinophilia–myalgia syndrome, and toxic oil syndrome.59 Eosinophil granule proteins, MBP-1 and EDN, along with other neuroactive mediators produced by eosinophils, such as nerve growth factor, vasoactive intestinal peptide, and substance P, likely affect nerve physiology. In fact, eosinophils and eosinophil granule proteins are often observed in close proximity to nerve endings.60,61 Eosinophil-induced nerve dysfunction is likely an important part of the gastric dysmotility observed in subjects with food allergies, the dysfunction of vagal muscarinic M2 receptors observed in patients with asthma, and may also contribute to itch along with other physiologic aberrations in atopic dermatitis and other cutaneous diseases.61,62
Collectively, the eosinophil’s response to surface factors determines its role in health and disease.
TISSUE TRAFFICKING
TISSUE TRAFFICKING
The selective recruitment of eosinophils into sites of inflammation results from interactions among eosinophil-activating cytokines, chemokine-inducing cytokines, and endothelial-activating cytokines (see Fig. 40-1). Similar to other leukocytes, selectin, integrin, and Ig gene superfamily members contribute
to the signaling involved in eosinophil trafficking. In particular, eosinophils constitutively express the integrin, VLA-4, which interacts with its ligand, VCAM-1, induced on endothelial cells by cytokines, especially Th2 cytokines (IL-4 and IL-13).63 After movement through vessels, eosinophils adhere to extracellular matrix proteins. Here, surface factors, such as CD11b/ CD18 (Mac-1), bind to fibrous proteins such as fibronectin, laminin, and collagen, and, not only determine where eosinophils will reside, but likely prolong their survival.64 In this regard, the CD11b/CD18 (Mac-1) integrin is also critical for eosinophil effector functions, including degranulation.65
EOSINOPHIL-ACTIVATING CYTOKINES
Eosinophil-activating cytokines can be produced by many cell types in addition to T cells and mast cells, including keratinocytes, endothelial cells, and monocytes, along with eosinophils, themselves. The eosinophil-activating cytokines, IL-3, IL-5, GM- CSF, and others, enhance chemotactic responses, in addition to multiple other effects on eosinophils, such as promoting maturation, cell survival, and LT production.66
ENDOTHELIAL-ACTIVATING CYTOKINES
During eosinophil migration, at least 3 types of endothelial activations occur. The first is the expression of P-selectin, which occurs when Weibel-Palade bodies in endothelial cells are transported to the cell surface rapidly after exposure to histamine, LTs, and a host of other inflammatory mediators. Expression of P-selectin on the endothelial cell surface initiates leukocyte rolling, via CD162 (PSGL-1), which is the important initial step before firm adhesion and transendothelial migration. A second type of endothelial activation is that induced by nonspecific activators such as IL-1 and TNF-α. These cytokines stimulate endothelial expression of E-selectin, ICAM-1, and VCAM-1, to which eosinophils firmly adhere, or “tether.” They also induce production of chemokines by endothelial cells. The third type of endothelial activation is that induced by IL-4 and IL-13. These cytokines selectively induce VCAM-1, which is centrally involved in the recruitment of VLA-4–positive cells, including eosinophils, basophils, and lymphocytes, into sites of allergic inflammation.
CHEMOKINES
The transition from rolling to firm adherence is substantially increased by CCR3 ligands, the CC chemokines. Induction of the expression of chemokines by activated endothelial cells results in higher levels of chemokines on or near the endothelial surface, which transiently affect β1-integrin and β2-integrin avidity, resulting in firm adhesion of the eosinophil
6
to the endothelial cell. However, chemokines produced by structural cells such as fibroblasts, smooth muscle cells, and epithelium probably are more important in directing migration and activation of eosinophils within tissues than those expressed on endothelial cells.67
Tissue chemokine expression forms a gradient signal that guides eosinophils into tissue. CCL11 guides eosinophils into tissue locations in which eosinophils are normally present, thymus, uterus, mammary gland, and gastrointestinal tract.68 In Th2 disorders, Th2 cytokines induce chemokine expression. In skin, IL-4, IL-13, and TNF-α stimulate CCL11, CCL24, and CCL26 production from mast cell and lymphocyte sources, as well as from fibroblasts (CCL11 and CCL26) and keratinocytes (CCL26).69 As in eosinophilic esophagitis, CCL26 may be important in atopic dermatitis in which serum CCL26 levels correlate with disease activity.70
Arachidonic acid metabolites, particularly, the cysteinyl LTs, LTC4, LTD4, and LTE4, and PGD2, are involved in eosinophil trafficking as evidenced by the observations that LT receptor antagonists reduce blood and lung eosinophilia and that mice, depleted of LTB4 receptors, have markedly reduced lung eosinophilia after allergen exposure. Eosinophil, basophil, and Th2 cell recruitment occurs, to some extent, through CRTH2 (CD294), the high-affinity PGD2 type 2 receptor.
ACTIVATION OF EOSINOPHILS
ACTIVATION OF
EOSINOPHILS
Various inflammatory mediators activate eosinophils. In addition to cytokines, TNF-α, GM-CSF, IL-3, and IL-5, the inflammatory mediators include complement components, C3a and C5a, lipid mediators, LTC4 and PAF, and chemokines, as well as engagement of IgA and IgG Fc receptors. IL-33 regulates eosinophils in the mechanisms of allergic inflammatory response. Nuclear factor κB and mitogen-activated protein kinase pathways are activated upon IL-33 ligation to receptors on eosinophils, promoting the cell surface expression of CD11b and ICAM-1 and the production of proinflammatory cytokines such as IL-6, IL-8, and IL-13.30,71 Eosinophil differentiation from CD117+ hematopoietic progenitor cells is directly induced by IL-33 in an IL-5-dependent manner.72
CD11b/CD18 (Mac-1)-dependent cellular adhesion is a critical component for degranulation and superoxide production induced by GM-CSF and PAF eosinophil activation and likely is an in vitro mechanism that results from eosinophil contact with stromal cells and/or proteins.73 Members of the CC chemokine subfamily (CCL5, CCL7 [MCP-3], CCL11, CCL13 [MCP-4], and CCL24) that bind to the chemokine receptor, CCR3, also potently activate eosinophils. Activated eosinophils develop a number of phenotypic changes, including a reduction in granules, vacuolization, and
657
6
an expansion of their cytoplasm, leading to a reduction in cell density and are referred to as hypodense. The number of hypodense cells predicts allergic disease severity. A cell-surface marker that distinguishes hypodense from normodense eosinophils has not been identified, but there are several surface markers with enhanced expression on in vitro or in vitro–activated or hypodense cells: αM integrin (CD11b), αX integrin (CD11c), FcγRIII (CD16), hyaluronic acid receptor (CD44), ICAM-1 (CD54), CD69, and HLA-DR (human leukocyte antigen-D related).74
Upon recruitment and activation in tissues, eosinophils have various effects as detailed in previous sections. In tissues, eosinophils release granule contents into their extracellular space via 3 mechanisms: piecemeal degranulation, regulated secretion (also referred to as regulated exocytosis), and cytolytic degranulation.
PHARMACOLOGIC MANIPULATION
PHARMACOLOGIC
MANIPULATION
Eosinophil-associated disease is a term that, strictly speaking, refers to diseases in which eosinophil numbers or eosinophil granule protein levels (or other eosinophil products) are associated with disease activity. This term encompasses multiple heterogeneous disorders, including skin diseases, in which targeting eosinophils and/or their products is a therapeutic goal. Many available treatments reduce eosinophil numbers, thereby inhibiting eosinophilic inflammation, including glucocorticoids, calcineurin inhibitors, IFN-α, IFN-γ, LT antagonists, myelosuppressive/cytotoxic drugs, and, possibly, antihistamines. However, none is specific for eosinophils. It is only in recent years that selective and direct reduction of eosinophils has been achieved, and these therapies have provided new insight into disease pathogenesis.75
Among the nonselective drugs for eosinophil reduction, glucocorticoids generally are very effective. The immediate (within 3 hours) reduction in circulating eosinophils observed after systemic administration of glucocorticoids likely occurs as a consequence of sequestration into extramedullary organs (liver, spleen, and lymph node), as has been shown in rodents. Glucocorticoids affect eosinophil infiltration into tissues by 4 mechanisms: sequestration into lymphoid tissues, induction of eosinophil apoptosis, reduction of eosinophil production by bone marrow, and alterations in the production of the cytokines/chemokines important in eosinophil trafficking.76-78 Glucocorticoids suppress the production of several cytokines important for the induction of adhesion molecules on endothelial cells, including IL-1, TNF-α, IL-4, and IL-13, and the release of eosinophil-active chemokines, including CCL5, CCL7, and CCL11. Unfortunately, “steroid resistance” develops in some patients, and long-term administration of glucocorticoids is associated with limiting side effects.
658
Calcineurin antagonists, such as cyclosporine, tacrolimus, and pimecrolimus, broadly inhibit T-cell cytokine release, including those that specifically induce eosinophilic inflammation (IL-4, IL-5, and GM-CSF). They also decrease the expression of CCL5, CCL11, and IL-5 with associated decreased tissue eosinophilia as has been shown in atopic dermatitis.79 Mammalian target of rapamycin (mTOR) inhibitors, including rapamycin, have direct effects on eosinophils, decreasing eosinophil granule protein release after IL-5 activation.80 The use of these therapeutic agents are limited by their side effects, including immunosuppression, as well as other metabolic effects that may be in part genetically determined.81
Several myelosuppressive drugs, including hydroxyurea, vincristine sulfate, cyclophosphamide, methotrexate, 6-thioguanine, 2-chlorodeoxyadenosine and cytarabine combination therapy, pulsed chlorambucil, and etoposide, may be beneficial in eosinophil-associated disease alone or as steroid-sparing agents. Hydroxyurea has been particularly effective in decreasing circulating eosinophil numbers. In myeloproliferative hypereosinophilic syndrome (chronic eosinophilic leukemia) with the FIP1L1-PDG- FRA mutation that codes for a tyrosine kinase, imatinib mesylate, a tyrosine kinase inhibitor, is approved for the treatment of chronic myelogenous leukemia and the hypereosinophilic syndrome, and has produced rapid, complete or near-complete remissions.82 Patients who have features of myeloproliferative hypereosinophilic syndrome (HES) but who lack FIP1L1-PDGFRA still may respond to imatinib.83
Alemtuzumab is a monoclonal antibody to CD52 that is used to deplete CD52+ lymphocytes in the treatment of chronic (B-cell) lymphocytic leukemia and T-cell lymphoma. Eosinophils, but not neutrophils, also express CD52, and alemtuzumab has been useful in treating patients with refractory HES, including those with abnormal T cells,84-86 but has serious limiting side effects from cytopenias, infusion reactions and infections. Mepolizumab is the first humanized monoclonal antibody against IL-5. It has proved effective in inhibiting eosinophilia and in reducing asthma exacerbation rates.87
Benralizumab is an anti–IL-5 receptor α (IL-5Rα) humanized monoclonal antibody. This therapy produced reduced eosinophilia in a dose-dependent manner in a Phase I trial on persons with asthma.88 As other eosinophilopoietic factors may circumvent the requirement for IL-5 in some cases, targeting IL-5Rα is considered to be more effective in reducing eosinophils than therapies directed at IL-5 itself.89
Both IFN-α and IFN-γ may be therapeutically beneficial in eosinophil-associated disease by inhibiting eosinophil degranulation and inflammatory mediator release. IFN-α may be better tolerated than IFN-γ and is used as a steroid-sparing agent predominantly in patients with lymphocytic variant HES, but also may be useful in myeloproliferative variant HES.90,91
EOSINOPHILS IN CUTANEOUS DISEASES
AT-A-GLANCE
■ Eosinophils may be seen in skin biopsy specimens from a broad range of cutaneous diseases but are not pathognomonic for any dermatosis.
■ Eosinophils are an important component of the characteristic histologic pattern in a limited number of diseases, including the following:
■ Angiolymphoid hyperplasia with eosinophilia.
■ Eosinophilic, polymorphic, and pruritic eruption associated with radiotherapy.
■ Eosinophilic pustular folliculitis.
■ Erythema toxicum neonatorum.
■ Eosinophilic ulcer of the oral mucosa.
■ Eosinophilic vasculitis.
■ Granuloma faciale.
■ Hypereosinophilic syndromes.
■ Incontinentia pigmenti.
■ Kimura disease.
■ Pachydermatous eosinophilic dermatitis.
■ Wells syndrome (eosinophilic cellulitis).
■ Clinical reaction patterns with eosinophil involvement include diseases in which eosinophils probably play a pathogenic role and are a component of the histologic pattern, but are not essential for diagnosis.
■ Evidence for involvement of eosinophils in cutaneous diseases is provided by observation of intact eosinophils in lesional tissue sections and/or by immunostains for their toxic granule proteins, which are deposited in tissues.
Eosinophils have myriad inflammatory activities that implicate them in disease.41,54,92 Peripheral blood eosinophilia and/or tissue infiltration by eosinophils occur in a variety of common and unusual diseases, including those of infectious, immunologic, and neoplastic etiologies. Organ-specific eosinophil disorders occur in the skin, lung, and gastrointestinal tract.93-95
Eosinophils are conspicuous in tissue sections stained with hematoxylin and eosin because of their intense avidity for eosin dye. Common dermatoses associated with eosinophils in lesional tissues include arthropod bites and drug eruptions. Parasitic infections, especially those caused by ectoparasites and helminthes, typically have a marked host response with eosinophilia.33,96 Autoimmune blistering diseases, such as bullous pemphigoid and the various forms of pemphigus, often have prominent eosinophil infiltration, including histologic presentation as eosinophilic spongiosis.97,98 Infiltration of eosinophils in the subcutaneous tissues, so-called eosinophilic panniculitis, is not a specific diagnosis but rather is seen to a variable degree in diverse entities.99,100 Eosinophils may
6
be found in Langerhans cell histiocytosis,101 cutaneous epithelial neoplasms,102 and lymphoproliferative disorders.103 Although eosinophils constitute one of the histologic features in numerous cutaneous diseases, eosinophil infiltration represents a criterion for histologic diagnosis in relatively few entities (Table 40-1).
■Diseases characterized by tissue eosinophils
■Diseases characterized by tissue eosinophils
■Angiolymphoid hyperplasia with eosinophilia
■Angiolymphoid hyperplasia with eosinophilia
■Eosinophilic, polymorphic, and pruritic eruption associated with radiotherapy
■Eosinophilic, polymorphic, and pruritic eruption associated with
radiotherapy
■Eosinophilic pustular folliculitis
■Eosinophilic pustular folliculitis
■Classical (Ofuji disease)
■Classical (Ofuji disease)
■Infantile/neonatal
■Infantile/neonatal
■HIV-associated
■HIV-associated
■Erythema toxicum neonatorum
■Erythema toxicum neonatorum
■Eosinophilic ulcer of oral mucosa
■Eosinophilic ulcer of oral mucosa
■Granuloma faciale
■Granuloma faciale
■Hypereosinophilic syndromes
■Hypereosinophilic syndromes
■Kimura disease
■Kimura disease
■Pachydermatous eosinophilic dermatitis
■Pachydermatous eosinophilic dermatitis
■Wells syndrome (eosinophilic cellulitis)
■Wells syndrome (eosinophilic cellulitis)
■Diseases typically associated with tissue eosinophils
■Diseases typically associated with tissue eosinophils
■Arthropod bites and sting reactions
■Arthropod bites and sting reactions
■Bullous dermatoses
■Bullous dermatoses
■Pemphigoid
■Pemphigoid
■Pemphigus
■Pemphigus
■Incontinentia pigmenti
■Incontinentia pigmenti
■Dermatoses of pregnancy
■Dermatoses of pregnancy
■Drug reactions
■Drug reactions
■DRESS (drug rash with eosinophilia and systemic symptoms)/ drug hypersensitivity syndrome
■DRESS (drug rash with eosinophilia and systemic symptoms)/
drug hypersensitivity syndrome
■Interstitial granulomatous drug reaction
■Interstitial granulomatous drug reaction
■Histiocytic diseases
■Histiocytic diseases
■Langerhans cell histiocytosis
■Langerhans cell histiocytosis
■Juvenile xanthogranuloma
■Juvenile xanthogranuloma
■Parasitic diseases/infestations
■Parasitic diseases/infestations
■Urticaria and angioedema
■Urticaria and angioedema
■Eosinophilic granulomatosis with polyangiitis
■Eosinophilic granulomatosis with polyangiitis
■Histologic patterns defined by eosinophils
■Histologic patterns defined by eosinophils
■Eosinophilic spongiosis
■Eosinophilic spongiosis
■Acute dermatitis
■Acute dermatitis
■Allergic contact dermatitis
■Allergic contact dermatitis
■Arthropod bite
■Arthropod bite
■Immunobullous diseases
■Immunobullous diseases
■Pemphigoid
■Pemphigoid
■Pemphigus
■Pemphigus
■Incontinentia pigmenti
■Incontinentia pigmenti
■Eosinophilic panniculitis
■Eosinophilic panniculitis
■Arthropod bite
■Arthropod bite
■Erythema nodosum
■Erythema nodosum
■Gnathostomiasis
■Gnathostomiasis
■Injection granuloma
■Injection granuloma
■Vasculitis
■Vasculitis
■Wells syndrome
■Wells syndrome
■Eosinophils of doubtful, limited, or no value in histologic diagnosis
■Eosinophils of doubtful, limited, or no value in histologic diagnosis
■Drug reaction versus graft-versus-host disease
■Drug reaction versus graft-versus-host disease
■Granuloma annulare
■Granuloma annulare
■Interstitial granulomatous dermatitis
■Interstitial granulomatous dermatitis
■Neoplasms
■Neoplasms
■Lymphoproliferative disorders (except hypereosinophilic syndrome types)
■Lymphoproliferative disorders (except hypereosinophilic
syndrome types)
659
■Keratoacanthoma
■Keratoacanthoma
6
The absence, presence, or number of eosinophils in skin biopsy specimens is often of limited value in reliably choosing among differential diagnoses with different and potentially important implications for clinical management, such as drug reaction versus acute graft-versus-host disease.104,105 Eosinophils play a role in certain categories of clinical reactions, particularly those characterized by edema.43 The degree of tissue eosinophil granule protein deposition in such diseases, that exhibit relatively few or no intact eosinophils, suggests that the pathogenic influence of eosinophils may be unrelated to their numbers in tissues. The degree of cutaneous eosinophil infiltration should be taken in the context of other clinical features, other histologic features, and knowledge that its diagnostic power has limitations.106 However, eosinophils do have potent biologic activities, particularly imparted by their distinctive granules, and eosinophils may play a pathogenic role in the absence of identifiable cells in tissues.
HYPEREOSINOPHILIC SYNDROMES
HYPEREOSINOPHILIC
SYNDROMES
AT-A-GLANCE
■ Spectrum of entities defined by criteria (Table 40-2).
■ Cutaneous lesions are common and may be the presenting sign.
■ Two major HES subtypes and several variants.
■ Lymphocytic HES characterized by T-cell clones that produce IL-5.
■ Variant HES subtypes may evolve into lymphocytic HES.
■ Organ-restricted.
■ Associated with specific disorders such as eosinophilic granulomatosis with polyangiitis (formerly known as Churg-Strauss syndrome).
■ Undefined with benign, complex, and episodic presentations.
■ Myeloproliferative HES associated with a deletion on chromosome 4 that produces a tyrosine kinase fusion gene Fip1-like 1/PDGFRα or other mutation associated with eosinophil clonality.
■ Responsive to imatinib.
■ Severely debilitating mucosal ulcers portend a grim prognosis unless HES is treated.
■ Overlap with mastocytosis.
■ Familial HES variant, family history of documented persistent eosinophilia of unknown cause.
■ Associated embolic events constitute a medical emergency.
■ Eosinophilic endomyocardial disease occurs in HES and in patients with prolonged peripheral blood eosinophilia from any cause.
660
HES consists of a spectrum of disorders that occur worldwide and span all age groups. More than 90% of patients with myeloproliferative HES and the mutant gene are males, but lymphocytic HES shows equal gender distribution. The relative frequencies of these subtypes are unknown, although up to 25% of HES patients may have lymphocytic HES. Rare familial cases have been reported. A miniepidemic of eosinophilic esophagitis, a subtype of overlap HES with organ-restricted disease, emerged over the last decade with prevalence estimates as high as 1:2500 among children and 1:4000 among adults.107,108
CLINICAL FEATURES
Patients satisfying HES diagnostic criteria (see Table 40-2) present with signs and symptoms related to the organ systems infiltrated by eosinophils.109-111
HES often presents with skin lesions that may be the only manifestations of HES.112-114 Pruritic erythematous macules, papules, plaques, wheals, or nodules are present in more than 50% of patients.115 CD3– CD4+ lymphocytic HES patients exhibit a particularly high prevalence of skin manifestation, as high as 94%.116
Lesions may involve the head, trunk, and extremities. Urticaria and angioedema occur in all HES subtypes and are characteristic of certain variant subtypes. Erythema annulare centrifugum,117 bullous pemphigoid,118
lymphomatoid papulosis,119 livedo reticularis, purpura and/or other signs of vasculitis,120-123 Wells syndrome (eosinophilic cellulitis),124,125 and multiple other mucocutaneous manifestations126 may be found in patients with HES (Table 40-3). The complications are mostly hematologic, cardiovascular, pulmonary, and neurologic.127
In myeloproliferative HES, the usual presenting complex includes fever, weight loss, fatigue, malaise, skin lesions, and hepatosplenomegaly.111,128-130
Mucosal ulcers of the oropharynx or anogenital region
- Blood eosinophilia >1500 eosinophils/mm3 on at least 2 separate determinations or evidence of prominent tissue eosinophilia associated with symptoms and marked blood eosinophilia.
- Exclusion of secondary causes of eosinophilia, such as parasitic or viral infections, allergic diseases, drug-induced or chemicalinduced eosinophilia, hypoadrenalism, and neoplasms.
Original Criteria289
Original Criteria289
■Peripheral blood eosinophilia of at least 1500 eosinophils/mm3.
■Peripheral blood eosinophilia of at least 1500 eosinophils/mm3.
■Longer than 6 months; or
■Longer than 6 months; or
■Less than 6 months with evidence of organ damage.
■Less than 6 months with evidence of organ damage.
■Signs and symptoms of multiorgan involvement.
■Signs and symptoms of multiorgan involvement.
■No evidence of parasitic or allergic disease or other known causes of peripheral blood eosinophilia.
■No evidence of parasitic or allergic disease or other known causes
of peripheral blood eosinophilia.
■Angioedema
■Angioedema
■Bullae (bullous pemphigoid)
■Bullae (bullous pemphigoid)
■Dermographism
■Dermographism
■Digital gangrene
■Digital gangrene
■Eczema
■Eczema
■Eosinophilic cellulitis (Wells syndrome)
■Eosinophilic cellulitis (Wells syndrome)
■Erosions
■Erosions
■Erythema
■Erythema
■Erythema annulare centrifuge
■Erythema annulare centrifuge
■Erythroderma
■Erythroderma
■Excoriations
■Excoriations
■Livedo reticularis
■Livedo reticularis
■Lymphomatoid papulosis
■Lymphomatoid papulosis
■Macules
■Macules
■Mucosal ulcers (oral and genital)
■Mucosal ulcers (oral and genital)
■Nail-fold infarctions
■Nail-fold infarctions
■Necrosis
■Necrosis
■Nodules
■Nodules
■Papules
■Papules
■Patches
■Patches
■Pruritus
■Pruritus
■Purpura
■Purpura
■Raynaud phenomenon
■Raynaud phenomenon
■Splinter hemorrhages
■Splinter hemorrhages
■Ulcers
■Ulcers
■Urticaria
■Urticaria
■Vasculitis
■Vasculitis
Modified from Leiferman KM, Gleich GJ, Peters MS. Dermatologic manifestations of the hypereosinophilic syndromes. Immunol Allergy Clin North Am. 2007;27(3):415-441, and Stetson CL, Leiferman, KM. Eosinophilic dermatoses. In: Bolognia JL, Jorizzo JL, Rapini RP, et al, eds. Dermatology. 2nd ed. St. Louis, MO: Mosby; 2008:369-378.
(Fig. 40-3) are also seen. Cardiac disease occurs frequently.131 Eosinophils adhere to endocardium and release granule proteins onto endothelial cells, thrombus formation follows, and, finally, subendocardial fibrosis with restrictive cardiomyopathy occurs. Mitral or tricuspid valvular insufficiency results from tethering of chordae tendineae.131 Cardiac abnormalities
6
that are essentially identical to those of HES but are confined to the intramural regions can occur without appreciable peripheral blood eosinophilia.132,133 Splinter hemorrhages and/or nail-fold infarcts may herald the onset of thromboembolic disease. The central and peripheral nervous system, lungs, and, rarely, kidneys may be affected.111 Patients with myeloproliferative HES frequently present with clinical features resembling those of chronic myelogenous leukemia and, depending on the classification, are regarded as having chronic eosinophilic leukemia. Although chromosomal abnormalities characterize this subtype and the disease may evolve into definite leukemia, the relatively mature nature of the eosinophils and lack of evidence for clonal expansion may preclude such classification. Lymphocytic HES commonly is associated with severe pruritus, eczema, erythroderma, urticaria, and angioedema, as well as lymphadenopathy and, rarely, endomyocardial fibrosis.134
Eosinophilic granulomatosis with polyangiitis is a variant HES subtype. Other variant HES subtypes include Gleich syndrome,44 in which eosinophil counts fluctuate with extreme angioedema.
ETIOLOGY AND PATHOGENESIS
Eosinophils are implicated as the cause of most end-organ damage in all HES subtypes.41,75 Clinical improvement usually parallels a decrease in eosinophil count. Patients with lymphocytic HES have abnormal T-cell clones with unusual surface phenotypes, including CD3+ CD4– CD8– and CD3– CD4+. These T cells display activation markers, such as CD25, and secrete Th2 cytokines, including high levels of IL-5.134,135 An 800-kilobase deletion on chromosome band 4q12 that codes for a tyrosine kinase has been found in myeloproliferative HES.136 Patients with this FIP1L1-PDGFRA gene mutation form a distinct subset of HES, with cardiomyopathy and endomyocardial fibrosis, that responds to imatinib. Patients in this HES subset have elevated serum tryptase levels and increased atypical spindle-shaped mast cells in
A B C
661
6
bone marrow.137-139 Although they do not have clinical manifestations of systemic mastocytosis or exhibit all its immunologic markers, these patients satisfy criteria for mastocytosis.140 The FIP1L1-PDGFRA gene is detected in mast cells,141 eosinophils, neutrophils, and mononuclear cells. Many HES patients also have marked neutrophilia, likely caused by the aberrant gene in the neutrophil lineage. Thus, alteration of several cell lines probably contributes to the pathogenesis of myeloproliferative HES.142,143 Myeloproliferative HES with abnormalities of PDGFRB and FGFR1, other well-characterized variants of myeloproliferative HES, has the potential to progress to aggressive myeloid malignancies.144 Therefore, it is recommended to assess other translocations in patients with negative PDGFRA screening. Multiple other chromosomal abnormalities have been identified in myeloproliferative HES, including translocations, partial and complete chromosomal deletions, and trisomies 8, 15, and 21. Myeloproliferative HES with documented mutations also is known as chronic eosinophilic leukemia. The World Health Organization has an updated 2008 classification scheme for myeloid disorders and eosinophilia.145,146 The etiology of the other HES variants is not well understood, although patients in several HES subtypes, including with episodic angioedema and eosinophilia (Gleich syndrome)44 and the NERDS syndrome,147 have developed T-cell clones.148
DIAGNOSIS
A key criterion for diagnosis is marked peripheral blood eosinophilia (see Table 40-2).109,149-151 Other causes of eosinophilia, including allergic and parasitic diseases, should be excluded. Tests to detect organ involvement, particularly measurement of liver enzyme levels, are important. Because eosinophilic endomyocardial disease can develop in any patient with prolonged peripheral blood eosinophilia, patients should undergo periodic echocardiography along with close observation for signs of thromboembolism. Increased serum levels of IgE are often present in lymphocytic HES, and levels of vitamin B12 and tryptase may be increased in myeloproliferative HES. The Chic2 fluorescent in situ hybridization assay detects the deletion that produces the FIP1L1-PDGFRA gene product and should be performed, because patients with this mutation respond to treatment with imatinib.139,141 Alternatively, the mutant gene can be detected by a polymerase chain reaction assay. Both tests are available commercially. In patients who lack the fusion gene, testing for other clonal cytogenetic abnormalities or abnormal clonal T-cell populations is warranted.137 Cytoflow of peripheral blood lymphocytes and immunophenotyping of tissue lymphocytes should be performed for the diagnosis of lymphocytic HES and repeated periodically to detect transformation from a variant HES type to lymphocytic HES or to T-cell lymphoma.134 Table 40-4 an HES evaluation assessment scheme for patients with eosinophilia. The cutaneous histopathologic features of HES vary with the type of lesion. Skin biopsy specimens from
662
■History
■History
■Attention to travel (parasite exposure)
■Attention to travel (parasite exposure)
■Ingestants (drugs, health foods, food supplements, and food allergy)
■Ingestants (drugs, health foods, food supplements,
and food allergy)
■Close contacts with itch (ectoparasites)
■Close contacts with itch (ectoparasites)
■Physical examination
■Physical examination
■Cutaneous features (see Table 40-3)
■Cutaneous features (see Table 40-3)
■Cardiovascular signs
■Cardiovascular signs
■Murmur of mitral insufficiency
■Murmur of mitral insufficiency
■Nails for splinter hemorrhage (medical emergency)
■Nails for splinter hemorrhage (medical emergency)
■Hepatosplenomegaly
■Hepatosplenomegaly
■Lymphadenopathy
■Lymphadenopathy
■Laboratory studies
■Laboratory studies
■Repeated complete blood counts with differentials
■Repeated complete blood counts with differentials
■Cytogenetics for chromosomal abnormalities to include
■Cytogenetics for chromosomal abnormalities to include
■FIP1L1-PDGFRA (CHIC2 gene) deletional mutation
■FIP1L1-PDGFRA (CHIC2 gene) deletional mutation
■T-cell subsets for clonality by cytoflow/T-cell receptor gene rearrangement
■T-cell subsets for clonality by cytoflow/T-cell receptor gene
rearrangement
■B-cell clonality analyses
■B-cell clonality analyses
■Inflammatory and immunologic markers
■Inflammatory and immunologic markers
■Erythrocyte sedimentation rate
■Erythrocyte sedimentation rate
■C-reactive protein
■C-reactive protein
■Rheumatoid factor
■Rheumatoid factor
■Antiproteinase 3 and antimyeloperoxidase (cytoplasmic antineutrophil cytoplasmic antibody and perinuclear antineutrophil cytoplasmic antibody)
■Antiproteinase 3 and antimyeloperoxidase (cytoplasmic
antineutrophil cytoplasmic antibody and perinuclear antineutrophil cytoplasmic antibody)
■IgE level
■IgE level
■Strongyloides IgG antibody
■Strongyloides IgG antibody
■IL-5 serum level
■IL-5 serum level
■Metabolic parameters
■Metabolic parameters
■Liver function tests to include aspartate aminotransferase and alanine aminotransferase
■Liver function tests to include aspartate aminotransferase
and alanine aminotransferase
■Renal function tests to include creatinine, blood urea nitrogen and urinalysis for protein and sediment
■Renal function tests to include creatinine, blood urea
nitrogen and urinalysis for protein and sediment
■Muscle enzymes to include creatine phosphokinase and aldolase
■Muscle enzymes to include creatine phosphokinase and
aldolase
■B12 serum level
■B12 serum level
■Mast cell/basophil tryptase (protryptase) level
■Mast cell/basophil tryptase (protryptase) level
■Coagulation factors
■Coagulation factors
■Troponin (before initiation of imatinib treatment)
■Troponin (before initiation of imatinib treatment)
■Serum protein analyses
■Serum protein analyses
■Serum protein electrophoresis
■Serum protein electrophoresis
■Quantitative immunoglobulins
■Quantitative immunoglobulins
■Immunofixation electrophoresis for monoclonal proteins
■Immunofixation electrophoresis for monoclonal proteins
■Imaging tests
■Imaging tests
■Echocardiography
■Echocardiography
■Computerized tomography of chest, abdomen, and pelvis
■Computerized tomography of chest, abdomen, and pelvis
■Gastrointestinal endoscopy, as indicated
■Gastrointestinal endoscopy, as indicated
■Pulmonary function tests, as indicated
■Pulmonary function tests, as indicated
■Bone marrow aspirate and biopsy with staining for tryptase and reticulum (myelofibrosis)
■Bone marrow aspirate and biopsy with staining for tryptase and
reticulum (myelofibrosis)
■Tissue biopsy of skin and/or other accessible affected organs
■Tissue biopsy of skin and/or other accessible affected organs
■Histologic examination
■Histologic examination
■Direct immunofluorescence for immunobullous disease
■Direct immunofluorescence for immunobullous disease
■Immunostaining for eosinophil granule proteins
■Immunostaining for eosinophil granule proteins
Modified from Gleich GJ, Leiferman KM. The hypereosinophilic syndromes: current concepts and treatments. Br J Haematol. 2009;145(3):271-85, with permission. Copyright © 2009 Blackwell Publishing Ltd.
urticarial lesions resemble idiopathic urticaria, with generally mild, nonspecific perivascular and interstitial infiltration of lymphocytes, eosinophils, and, occasionally, neutrophils. Immunostaining reveals
extensive deposition of eosinophil granule proteins, in the absence of intact eosinophils, in episodic angioedema with eosinophilia,44 HES with mucosal ulcers,45
and in synovial tissues in NERDS.147 Other than in eosinophilic granulomatosis with polyangiitis, vasculitis only rarely is associated with HES.120-122
DIFFERENTIAL DIAGNOSIS
including those associated with thrombosis, such as Behçet syndrome, Crohn disease, ulcerative colitis, and Reiter syndrome. Others considerations are recurrent aphthous stomatitis, immunobullous diseases,
■Parasitic infection
■Parasitic infection
■Ectoparasitic infestation
■Ectoparasitic infestation
■Urticaria
■Urticaria
■Hereditary angioedema
■Hereditary angioedema
■Atopic dermatitis
■Atopic dermatitis
■Contact dermatitis
■Contact dermatitis
■Drug reaction
■Drug reaction
■Fungal infection
■Fungal infection
■Mycosis fungoides
■Mycosis fungoides
■Sézary syndrome
■Sézary syndrome
■Behçet syndrome
■Behçet syndrome
■Crohn disease
■Crohn disease
■Ulcerative colitis
■Ulcerative colitis
■Reiter syndrome
■Reiter syndrome
■Recurrent aphthous stomatitis
■Recurrent aphthous stomatitis
■Erythema multiforme
■Erythema multiforme
■Lichen planus
■Lichen planus
■Immunobullous disease
■Immunobullous disease
■Herpes simplex infection
■Herpes simplex infection
■Syphilis
■Syphilis
6
erythema multiforme, lichen planus, herpes simplex infection, and syphilis.
CLINICAL COURSE, PROGNOSIS, AND MANAGEMENT
Myeloproliferative HES with mucosal lesions portend an aggressive clinical course; death is likely within 2 years of presentation if the disorder is untreated.129,155
In contrast to myeloproliferative HES, lymphocytic HES generally follows a benign course, and T-cell clones can remain stable for years. Patients should be observed closely and regarded as having premalignant or malignant T-cell proliferation, because the disease may evolve into lymphoma, especially in CD3– CD4+ T-cell populations.156
During the decade or more after diagnosis, HES may evolve into acute leukemia and, less commonly, is associated with B-cell lymphomas. The overall 5-year survival rate for HES patients is 80%; congestive heart failure from the restrictive cardiomyopathy of eosinophilic endomyocardial disease is a major cause of death, followed by sepsis. The goal of treatment is to relieve symptoms and improve organ function while keeping peripheral blood eosinophils at 1000 to 2000/mm3 and minimizing treatment side effects (Fig. 40-4). Recent reviews have delineated evaluation and management of HES.29,70-72,77,82,128,149-151 Corticosteroids are one of the most commonly used and most effective therapeutic agents in the treatment of HES.116 They are considered the first-line therapy in patients without the gene mutation, once Strongyloides infection has been excluded.157
Approximately 70% of patients will respond, with peripheral eosinophil counts returning to normal. Patients with elevated thymus and activation-regulated chemokine (TARC) and with lymphocytic HES have particularly favorable responses to steroid therapy.89,110,158 Patients for whom glucocorticoid monotherapy fails have a worse prognosis generally; in such cases, or when long-term side effects become problematic, other treatments should be used. Myeloproliferative HES is responsive to imatinib.159 In patients with the mutant gene FIP1L1-PDGFRA, administration of imatinib mesylate is indicated and usually induces hematologic remission, but endomyocardial disease may worsen during the first several days of treatment. Troponin levels should be monitored before and during imatinib therapy.160,161 To improve cardiac function, glucocorticoids should be given before and with initiation of imatinib therapy. Imatinib resistance can develop.162-164 Effective treatment of HES in imatinibresponsive patients results in improvement of associated conditions, including cardiac involvement with endocarditis165 and myelofibrosis,166 and skin disease with bullous pemphigoid.118 Patients who have features of myeloproliferative HES but who lack FIP1L1- PDGFRA still may respond to imatinib.83 IFN-α has been beneficial in treating myeloid and lymphocytic HES.90,91 In one patient, loss of the FIP1L1-PDGFRA mutation after several years of IFN-α therapy was
663
6
Hypereosinophilic syndrome (HES): classification and treatment
FIP1L1-PDGFRA gene mutation
Familial Family members with persistent eosinophilia of unknown cause
Negative
Myeloproliferative forms Lymphocytic forms
Positive
Chronic eosinophilic leukemia Clonal eosinophils or Cytogenic abnormalities and/or blasts
Myeloproliferative HES Etiology undetected 4 or more of: Dyplastic eosinophils High serum B12 High serum tryptase Anemia Thrombocytopenia Hepatosplenomegaly Marrow hypercellularity Spindle-shaped mast cells and/or myelofibrosis
Imatinib alone (dose sufficient to eradicate FIP1L1-PDGFRA, 100-400 mg/day) or with glucocorticoids if cardiac involvement
Associated with Churg-Strauss, inflammatory bowel disease, sarcoidosis, HIV, and other diseases
Undefined Overlap Associated with other organ-restricted eosinophilic disorders
Treat specific disease
Benign, no organ involvement
Complex, organ dysfunction but not myeloproliferative or lymphocytic variant
Episodic, cyclical angioedema, and eosinophilia
Monitor for development of T-cell clone (or FIP1L1-PDGFRA)
Monitor for cardiac disease Systemic glucocorticoids 0.5-1 mg/kg/day
Other tyrosine kinase inhibitors, new agents in development
Interferon-α Consider trial of imatinib therapy (up to 50% of responsive patients do not have FIP1L1-PDGFRA mutation)
One or combinations of the following agents: Hydroxyurea Extracorporeal photopheresis PUVA Dapsone Methotrexate Vincristine sulfate Cyclophosphamide 6-Thioguanine 2-Chlorodeoxydenosine and cytarabine Pulsed chlorambucil Etoposide Cyclosporine Intravenous immunoglobulin Alemtuzumab IL-5 monoclonal antibody (currently only in clinical trials) Bone marrow transplantation (only after failure of above)
664
associated with complete remission.167 Extracorporeal photopheresis alone or in combination with IFN-α or other therapies represent additional therapeutic options. Other treatments for HES with reported benefit include hydroxyurea, dapsone, vincristine sulfate, cyclophosphamide, methotrexate, 6-thioguanine, 2-chlorodeoxyadenosine and cytarabine combination therapy, pulsed chlorambucil, etoposide, cyclosporine, intravenous Ig, and psoralen plus ultraviolet A phototherapy.168 Refractory disease may respond to infliximab (anti–TNF-α)169 or alemtuzumab (anti- CD52),84-86 as well as to bone marrow and peripheral blood stem cell allogeneic transplantation.170,171 Two monoclonal antibodies against human IL-5 (mepolizumab and reslizumab) are associated with clinical improvement and reductions in peripheral blood and dermal eosinophils, particularly in patients with lymphocytic HES.172-176 Treatments targeting IL-5 have provided new insights into understanding eosinophilassociated disease.75
WELLS SYNDROME
WELLS SYNDROME
AT-A-GLANCE
■ Single or multiple lesions commonly located on the extremities or trunk.
■ Lesions may be painful or pruritic.
■ Associated with general malaise but uncommonly with fever.
■ Edematous and erythematous lesions evolve into plaques with violaceous borders.
■ Blisters may be a prominent feature.
■ Multiple recurrences.
■ Peripheral blood eosinophilia common.
■ Histologic pattern characterized by dermal infiltration with eosinophils, and flame figures surrounded by histiocytes.
■ Systemic glucocorticoids usually therapeutic.
CLINICAL FEATURES
Cutaneous edema was the common clinical thread in the first 4 cases reported by Wells.177 After prodromal burning or itching, lesions begin with erythema and edema (Fig. 40-5A), sometimes in the form of annular or arcuate plaques or nodules (Fig. 40-5B). Over a period of days, they evolve into large edematous plaques with violaceous borders. Bullae may develop.178-181 Individual lesions gradually change from bright red to brown-red and then to blue-gray or greenish-gray, resembling morphea (Fig. 40-5C). Lesscommon clinical presentations include papules, vesicles (Fig. 40-6), and hemorrhagic bullae. The cutaneous lesions may be single or multiple and may be located
6
A
B
C
at any site, but typically involve the extremities and, less often, the trunk.182 The most frequent systemic complaint in patients with Wells syndrome is malaise; fever occurs in a minority of cases. Some patients have
665
6
an associated underlying disorder such as hematologic or nonhematologic malignancies.
ETIOLOGY AND PATHOGENESIS
The etiology and pathogenesis of Wells syndrome is unclear. A nonspecific hypersensitivity reaction in response to exogenous and/or endogenous stimuli is regarded as the important pathomechanism.183 Some cases appear to be idiopathic, while many others suggest a triggering event, such as insect bites, viral or bacterial infections, and drugs and vaccines. The association with an underlying disorder, such as a malignancy, also has been reported.
DIAGNOSIS
Peripheral blood eosinophilia is observed in approximately 50% of patients. Skin lesions histologically are characterized by diffuse dermal infiltration with eosinophils, histiocytes, and foci of amorphous and/or granular material associated with connective tissue fibers, which Wells termed flame figures.177 In the early stages, there also is dermal edema. Later, histiocytes palisade around flame figures. Vasculitis is usually absent.184 In addition to 8 patients with the syndrome, the 1979 report of Wells and Smith includes 9 patients with the typical histologic features of eosinophilic cellulitis but in association with a variety of clinical diagnoses, including pemphigoid, eczema, and tinea.185 This and subsequent reports of flame figures in lesions from patients with a wide spectrum of diseases (Table 40-6) indicate that the flame figure is characteristic for, but not diagnostic of, Wells syndrome.186 When examined for eosinophil granule MBP by immunofluorescence, flame figures show bright extracellular staining (Fig. 40-7), indicating that extensive eosinophil degranulation has occurred.187
DIFFERENTIAL DIAGNOSIS
666
■Arthropod bite
■Arthropod bite
■Ascariasis
■Ascariasis
■Bronchogenic carcinoma
■Bronchogenic carcinoma
■Eosinophilic granulomatosis with polyangiitis
■Eosinophilic granulomatosis with polyangiitis
■Colonic adenocarcinoma
■Colonic adenocarcinoma
■Dental abscess
■Dental abscess
■Dermographism
■Dermographism
■Drug reaction
■Drug reaction
■Eczema
■Eczema
■Eosinophilic fasciitis
■Eosinophilic fasciitis
■Eosinophilic pustular folliculitis
■Eosinophilic pustular folliculitis
■Herpes gestationis
■Herpes gestationis
■Herpes simplex infection
■Herpes simplex infection
■HIV
■HIV
■Hymenoptera sting
■Hymenoptera sting
■Hypereosinophilic syndrome
■Hypereosinophilic syndrome
■Immunobullous diseases
■Immunobullous diseases
■Mastocytoma
■Mastocytoma
■Molluscum contagiosum
■Molluscum contagiosum
■Myeloproliferative diseases
■Myeloproliferative diseases
■Onchocerciasis
■Onchocerciasis
■Vaccinations
■Vaccinations
■Tinea
■Tinea
■Toxocariasis
■Toxocariasis
■Urticaria
■Urticaria
■Ulcerative colitis
■Ulcerative colitis
■Varicella
■Varicella
A
B
■Urticaria
■Urticaria
■Erysipelas
■Erysipelas
■Acute cellulitis
■Acute cellulitis
■Pemphigoid
■Pemphigoid
■Morphea
■Morphea
Urticaria, erysipelas, and acute cellulitis should be considered in the differential diagnosis of the early stages of Wells syndrome (see Fig. 40-5A). Later, plaques may resemble morphea (see Fig. 40-5C). The presence of blisters may suggest pemphigoid (see Fig. 40-6). Flame figures are the hallmark of Wells syndrome, but, because they have been identified in biopsy specimens from other dermatoses (see Table 40-6), they are not alone sufficient for the diagnosis. However, a diagnosis of Wells syndrome in the absence of flame figures should be met with skepticism, even in the presence of dermal infiltration with eosinophils and histiocytes.186
CLINICAL COURSE, PROGNOSIS, AND MANAGEMENT
Wells syndrome resolves without scarring, usually within weeks to months, but multiple recurrences are common. Lesions usually improve dramatically after administration of systemic glucocorticoids, and tapering of steroid dose over 1 month is well tolerated in most patients. Recurrences or persistent cases can be effectively maintained with low-dose (5 mg) alternateday prednisone.188 For patients who fail to respond, or who experience relapse often enough to raise concerns about the long-term side effects of systemic glucocorticoid therapy, other options, such as minocycline, dapsone, griseofulvin, and antihistamines, may be beneficial. Cyclosporine and IFN-α also have been used with success. For treatment of mild disease, topical glucocorticoids may be sufficient. It also can be beneficial to treat the underlying condition or triggering factor.189-191
ANGIOLYMPHOID HYPERPLASIA WITH EOSINOPHILIA (EPITHELIOID HEMANGIOMA)
ANGIOLYMPHOID
HYPERPLASIA WITH
EOSINOPHILIA (EPITHELIOID
HEMANGIOMA)
AT-A-GLANCE
AT A GLANCE
■ Kimura disease (KD) occurs mainly in Asian males; angiolymphoid hyperplasia with eosinophilia (ALHE) occurs in all races, with a female predominance.
■ KD is found in a younger age group than ALHE.
6
■ Both ALHE and KD are characterized by recurrent dermal and/or subcutaneous lesions, primarily of the head and neck area.
■ ALHE lesions tend to be smaller, more superficial, and more numerous than those of KD.
■ KD tends to involve subcutaneous tissues, regional lymph nodes, and salivary glands.
■ ALHE may be painful, pruritic, or pulsatile, whereas KD is generally asymptomatic.
■ Peripheral blood eosinophilia present in both diseases.
■ Increased IgE levels are found only in KD.
■ Renal disease is associated only with KD (reported incidence of 10% to 20%).
■ Histopathologic features:
■ Dominant feature of KD is lymphoid proliferation, often with germinal centers, whereas ALHE is characterized by vascular proliferation with numerous large epithelioid or histiocytoid endothelial cells.
■ Fibrosis is characteristic of KD and is limited or absent in ALHE.
■ Inconspicuous to numerous eosinophils in ALHE.
■ Eosinophil abscesses may occur in KD.
Angiolymphoid hyperplasia with eosinophilia (ALHE) occurs in both males and females, but there is a slight female predominance. Patients are generally in the third to fifth decade of life. In contrast to Kimura disease (KD), which develops mainly in Asian males at puberty, ALHE has no racial predilection.
CLINICAL FEATURES
ALHE shows a predilection for the head and neck area, including the ears,192 and is characterized by solitary, few, or multiple, sometimes grouped, erythematous, violaceous, or brown papules, plaques, or nodules of the dermis and/or subcutaneous tissues (Fig. 40-8). Lesions may be associated with pruritus or pain, or may pulsate. Although they are confined to the skin in most patients, mucosal involvement may occur.193
ETIOLOGY AND PATHOGENESIS
The pathogenesis of ALHE is unknown, but it has been considered a vascular proliferation arising in response to or in association with underlying vascular malformation. There is a history of trauma in some cases. ALHE has been reported to occur in pregnancy, which implies that sex hormones may be a factor in its development.194 ALHE also has developed in patients with T-cell clonality, which suggests that it may be an early or low-grade T-cell lymphoma and further highlights a relationship between T cells and eosinophils, particularly T cells with the Th2 phenotype.195,196
667
6
A
B
DIAGNOSIS
Approximately 20% of patients have peripheral blood eosinophilia; IgE levels are unremarkable. There is no association with renal disease. The dominant histologic feature is a well-defined area, in the dermis and/or subcutis, of prominent vascular proliferation with large epithelioid or histiocytoid endothelial cells that contain abundant eosinophilic cytoplasm, often with cytoplasmic vacuoles. There are variable numbers of eosinophils and lymphocytes,197 with an occasional finding of lymphoid nodules. In their report of 116 patients with ALHE, Olsen and Helwig found 53 cases in which “an arterial structure” appeared to be associated with venules or “was the area of endothelial
668
■Kimura disease
■Kimura disease
■Pyogenic granuloma
■Pyogenic granuloma
■Epithelioid hemangioendothelioma
■Epithelioid hemangioendothelioma
■Epithelioid angiosarcoma
■Epithelioid angiosarcoma
■Kaposi sarcoma
■Kaposi sarcoma
proliferation,” which provided evidence that these lesions may represent a form of arteriovenous shunt.198
The stroma typically is myxoid, and fibrosis is minimal or absent. Mast cells may be a component of the histologic picture.
DIFFERENTIAL DIAGNOSIS
ALHE KD
Gender Typically middle-aged females Predominantly youngadult Asian males
Symptoms Pruritus, pain, pulsation Asymptomatic
Lesion type and location Small and superficial, with overlying erythema; head and neck region
Large, mainly subcutaneous; overlying skin normal; head and neck region; may involve regional lymph nodes and salivary glands
Lymphoid follicles Uncommon Prominent lymphoid follicles with germinal centers
Vascular proliferation Prominent vascular proliferation with large epithelioid/ histiocytoid endothelial cells; evidence of underlying vascular malformation may be evident
Some stromal vascularity with unremarkable endothelial cells
Fibrosis Absent or limited Prominent
Serum immunoglobulin E level
Normal Increased
Nephropathy Absent Present in up to 20%
Nephropathy Absent Present in up to 20% of patients
of patients
Kaposi sarcoma—all of which lack a noticeable eosinophil infiltrate. Although it is nonspecific, the dermoscopic finding of ALHE with polymorphous vascular pattern may be helpful in differential diagnosis from other vascular tumors.199
CLINICAL COURSE, PROGNOSIS AND MANAGEMENT
ALHE tends to be chronic and nonremitting over months to years. Intervention is dictated in part by the number, location, size of lesions, and the patient’s general health.200 Patients with solitary or a few small lesions may benefit from excision or Mohs surgery,201 but there may be recurrence at the surgical site (Fig. 40-10). A variety of other treatment modalities have been used with success, including systemic and intralesional glucocorticoid administration, IFN-α therapy,202 cryotherapy,203 laser therapy,204 and topical application of tacrolimus.205
KIMURA DISEASE
KIMURA DISEASE
6
A
B
MANAGEMENT
Surgical excision is the treatment of choice when feasible in patients with a single or a limited number of nodules, but lesions may recur.206,207 Other therapeutic options include systemic glucocorticoids, cyclosporine, and radiation therapy.208,209 The presence of renal disease may influence or dictate the therapeutic regimen.
■Angiolymphoid hyperplasia with eosinophilia
■Angiolymphoid hyperplasia with eosinophilia
669
■Lymphoma
■Lymphoma
6
The finding of PDGF-α and c-kit in tissues from KD patients suggests that imatinib or another tyrosine kinase inhibitor may be effective in the disease.210
EOSINOPHILIC PUSTULAR FOLLICULITIS
EOSINOPHILIC PUSTULAR
FOLLICULITIS
AT-A-GLANCE
■ Three clinical types that are characterized by follicular papules and pustules, and may involve the head, trunk, and extremities.
■ Classic eosinophilic pustular folliculitis (Ofuji disease).
■ Typically occurs in Japanese patients, who have chronic, recurrent follicular pustules, with a tendency to form circinate plaques, in a seborrheic distribution.
■ Eosinophilic pustular folliculitis associated with immunosuppression.
■ Most often occurs in patients with human immunodeficiency virus infection, who have severely pruritic papules of the face and upper trunk.
■ Eosinophilic pustular folliculitis of infancy/ neonatal period.
■ Follicular pustules of the scalp.
■ Tendency for recurrences and chronicity (except eosinophilic pustular folliculitis of infancy).
■ Characterized by follicular and perifollicular eosinophil infiltration.
■ Associated with peripheral blood eosinophilia.
CLINICAL FEATURES
At present, eosinophilic pustular folliculitis (EPF) is divided into 3 variants: classical EPF, immunosuppression-associated EPF, and infantile EPF.211 Immunosuppression-associated EPF may be subdivided into an HIV-associated type and a malignancy-associated type.212-214 Classical EPF presents as recurrent crops or clusters of follicular papules and pustules, which may form an annular pattern and usually resolve in 7 to 10 days (Fig. 40-11A). Lesions predominantly involve the face and trunk but also may affect the extremities, with involvement of the palms and soles in approximately 20% of patients.215 In infantile type of EPF, lesions typically are located on the scalp, but also may be found on the face and extremities. In some neonates who have pustular eruptions that clinically resemble EPF and typically have peripheral blood eosinophilia, the disorder may be classified more appropriately under the term eosinophilic pustulosis because the cutaneous infiltrates are not folliculocentric.216 In contrast,
670
A
43x05a
B
HIV-associated EPF tends to manifest as extremely pruritic discrete follicular papules, typically involving the head and neck and often the proximal extremities (Fig. 40-11B). Rosenthal et al emphasized the urticarial quality of such lesions.217
ETIOLOGY AND PATHOGENESIS
The etiology of EPF remains unknown. The occasional association with HIV infection suggests the possible contribution of immunocompromised status to the development of EPF. Interestingly, some cases of HIVassociated EPF develop lesions after starting highly active anti-retroviral therapy (HAART), indicating that
EPF may occur as a result of immune reconstruction rather than immunodeficiency in these HAART-treated cases.218-220 Drugs,221,222 parasitic or viral infections,223,224
and pregnancy225,226 are also reported as possible factors related to EPF. The higher expression of ICAM-1 and leukocyte function-associated antigen-1 on the follicular epithelium, and VCAM-1 around hair follicles in EPF lesions, suggest that these molecules are relevant to the selective migration of eosinophils and lymphocytes to the hair follicles in EPF.227 One study demonstrated that an interaction between PGD2 and a chemoattractant receptor-homologous molecule expressed on T-helper type 2 (CRTH2) cells may be involved in the pathogenesis of classical EPF and that indomethacin may exert its therapeutic effect by reducing CRTH2 expression, as well as by inhibiting PGD2 synthesis.228
DIAGNOSIS
Patients suspected of having EPF should be evaluated for underlying immune deficiency, particularly HIV infection. Peripheral blood eosinophilia is a component of all 3 types of EPF. TARC is reported to be elevated in serum and to correlate with peripheral blood eosinophilia.229 Although patients with classical EPF usually have eosinophilia with leukocytosis, HIV-positive patients often exhibit eosinophilia with lymphopenia. Low CD4+ T-cell counts and high IgE levels are typical of HIV-associated EPF.217 Elevated serum IgE is uncommon in infantile EPF.230 Histologically, the most striking feature is the infiltration of eosinophils into hair follicles and perifollicular areas, sometimes with follicular damage. The infiltrates also may contain lymphocytes and neutrophils, and may be perivascular as well as follicular.231 Flame figures can also be observed in infantile EPF.230 Follicular mucinosis has been noted in association with EPF232; however, T-cell clonality is not observed in EPF-associated follicular mucinosis.233
DIFFERENTIAL DIAGNOSIS
■Folliculitis, bacterial or fungal
■Folliculitis, bacterial or fungal
■Seborrheic dermatitis
■Seborrheic dermatitis
■Palmar–plantar pustular psoriasis
■Palmar–plantar pustular psoriasis
■Acne, including acne neonatorum
■Acne, including acne neonatorum
■Erythema toxicum neonatorum
■Erythema toxicum neonatorum
■Acropustulosis
■Acropustulosis
■Follicular mucinosis
■Follicular mucinosis
6
there is head and neck involvement, and palmar– plantar pustular psoriasis may also be included in the differential diagnosis when there is hand and foot involvement. Acneiform eruption, rosacea, and lupus miliaris disseminatus faciei may resemble EPF. Erythema toxicum neonatorum, acropustulosis, and acne neonatorum also should be considered in infants. Follicular mucinosis usually is clinically and histologically distinguishable from EPF. One of the most important differential diagnoses is cutaneous T-cell lymphoma, which can resemble EPF both clinically and histopathologically.212
CLINICAL COURSE, PROGNOSIS, AND MANAGEMENT
The infantile type of EPF has a good prognosis, whereas classical and HIV-associated EPF are characterized by recurrences. Postinflammatory pigmentation may be seen as lesions resolve, but scarring does not occur. Topical glucocorticoids and topical calcineurin inhibitors generally are the first approach to the treatment of all types of EPF. Topical tacrolimus is helpful for facial lesions.234 Nonsteroidal antiinflammatory drugs, particularly indomethacin, also are recommended as first-line therapy; clinical improvement may be observed within 2 weeks and is associated with a decrease in peripheral blood eosinophil counts.235-237 Ultraviolet light therapy (ultraviolet B or psoralen and ultraviolet A) may be beneficial. Topical permethrin, systemic retinoids, systemic glucocorticoids, cyclosporine, itraconazole, metronidazole, cetirizine, minocycline, dapsone, and IFNs have been tried with success.235,236 Antiretroviral treatment that results in increased CD4 cell counts often is associated with improvement in HIV-associated EPF. The first-line treatment of infantile EPF is observation or topical steroid therapy. Infantile EPF tends to resolve spontaneously within several years and usually shows good response to topical steroids.230
PAPULOERYTHRODERMA OF OFUJI
PAPULOERYTHRODERMA
OF OFUJI
AT-A-GLANCE
AT A GLANCE
■ Papuloerythroderma tends to occur in elderly males.
■ The lesions are usually pruritic.
■ Erythroderma-like eruptions formed by confluent flat-topped, red-to-brown papules are characteristic.
■ The unique sparing of the abdominal skin folds is termed deck-chair sign.
671
(Continued)
6
AT-A-GLANCE (Continued)
■ Approximately 20% of cases are associated with hematologic or visceral malignancies.
■ Papuloerythroderma may progress to cutaneous T-cell lymphoma.
■ The majority of cases are associated with peripheral blood eosinophilia.
■ Ultraviolet treatment and corticosteroids are usually effective; however, the disorder is sometimes refractory to treatment.
CLINICAL FEATURES
Papuloerythroderma of Ofuji was described as a distinctive pattern of erythroderma by Ofuji in 1984.238
Many cases occur in elderly males, especially in the eighth or ninth decades. Itchy erythroderma-like eruptions formed by the coalescence of flat-topped, red-to-brown papules with a cobblestone appearance is characteristic (Fig. 40-12).239 It affects the limbs and trunk; the face and flexures are usually spared. The characteristic sparing of the abdominal skin folds is called deck-chair sign. Mucous membranes, hair, and nails are always spared. Palmoplantar keratoderma and dermatopathic lymphadenopathy are reported in approximately 20% of patients.239
Approximately 20% of cases with papuloerythroderma are associated with hematologic neoplasms such as non-Hodgkin lymphoma and leukemia or visceral malignancies including gastric, colon, and prostate carcinomas.240-243
ETIOLOGY AND PATHOGENESIS
The pathogenesis of papuloerythroderma is unknown. It remains controversial whether it is an independent clinical entity or a unique manifestation of an underlying disorder. Malignancy, atopic diathesis, infections and drug intake are reported to
672
be possible causes of papuloerythroderma. Several findings (eosinophil infiltration of the lesional skin and occasional association of atopic diathesis) suggest a role for T lymphocytes polarized toward the Th2 phenotype in the pathogenesis of papuloerythroderma, although the target antigens of those T lymphocytes are unclear. It is reported that the percentages of circulating CCR4+ CD4+ Th2 cells are higher than those of CXCR3+ CD4+ Th1 cells in patients with drug-induced papuloerythroderma.244
A recent study demonstrated that the percentages of IL-4–producing, IL-13–producin, and IL-22– producing CD4+ and CD8+ T cells were significantly higher in the circulations of patients with papuloerythroderma than in the circulations of healthy controls. In addition, the expression of both cutaneous lymphocyte antigen and CCR4 was markedly upregulated in those cells. These findings suggest that skin-homing Th2/Th22 cells may contribute to the pathogenesis of papuloerythroderma.245
DIAGNOSIS
Characteristic flat-topped, red-to-brown confluent papules and the deck-chair sign are highly diagnostic, although the deck-chair sign is observed in other erythrodermas, such as psoriasis and atopic dermatitis.243,246 Peripheral eosinophilia is detected in more than 80% of patients.239 Lymphocytopenia and increased serum IgE are sometimes observed. Histopathology shows nonspecific spongiotic dermatitis-like patterns, that is, acanthosis, spongiosis, and infiltration of lymphocytes, histiocytes, and variable amounts of eosinophils distributed in the mid-upper dermis and around microvessels, which resemble chronic dermatitis.239
DIFFERENTIAL DIAGNOSIS
Typical papuloerythroderma can be distinguished from other erythrodermas by its characteristic clinical appearance. Some cases show histologic findings of cutaneous T-cell lymphoma such as mycosis fungoides.247,248 It was also reported that papuloerythroderma progressed to cutaneous T-cell lymphoma.246
As it can be associated with atopic diathesis, malignancies, infections, and drugs,239 underlying complications must be examined.
CLINICAL COURSE, PROGNOSIS, AND MANAGEMENT
Papuloerythroderma tends to be chronic over years and non–self-limiting. Oral prednisolone is effective in the majority of cases. Ultraviolet treatment alone or in combination with oral and topical corticosteroids is reported to be very efficient.242 Etretinate,249 cyclosporine,250 and IFN251 are also reported as effective for papuloerythroderma. However, papuloerythroderma is frequently refractory to treatment.
GRANULOMA FACIALE
GRANULOMA FACIALE
AT-A-GLANCE
■ Granuloma faciale is an uncommon inflammatory dermatosis characterized clinically by reddish brown papules and plaques primarily involving the face.
■ The pathology shows changes of a chronic leukocytoclastic vasculitis with a mixed infiltrate containing eosinophils, extensive perivascular fibrin deposition, and dermal fibrosis.
■ Etiology is unknown.
Granuloma faciale occurs predominantly in adult men and women. There is a slight male predominance, and mean age at presentation is 52 years.252,253 Granuloma faciale can occur in individuals of any race; however, it is more common in whites.
CLINICAL FEATURES
Granuloma faciale is characterized by solitary papules, plaques, or nodules. The lesions are typically asymptomatic red, brown, or violaceous plaques that are soft, smooth, and well circumscribed, often showing follicular accentuation and telangiectasia (Figs. 40-13 and 40-14). The prominent follicular openings sometimes show a “peau d’orange” appearance. Ulceration is rare. Lesions are most common on the face. Sites of predilection include the nose, preauricular area, cheeks, forehead, eyelids, and ears.252,254 Rarely, patients may present with multiple lesions or lesions on the trunk or extremities. Extrafacial lesions have been reported both as isolated findings and in conjunction with facial lesions. Lesions are typically asymptomatic;
6
however, patients may complain of tenderness, burning, or pruritus.252 Photoexacerbation of lesions has been reported.255 It is rarely associated with systemic disease.256
ETIOLOGY AND PATHOGENESIS
The etiology of granuloma faciale is unknown. The disease can be considered a localized chronic fibrosing vasculitis.257 Immunofluorescence studies have revealed deposition of immunoglobulins and complement factors in the vessel walls consistent with a type III immunologic response, marked by deposition of circulating immune complexes surrounding superficial and deep blood vessels.258,259 However, other authors have described negative results with immunofluorescence.254
DIAGNOSIS
An extensive laboratory evaluation is not required. Peripheral blood eosinophilia is occasionally detected. The diagnosis may be established by a combination of clinical findings and confirmatory tissue biopsy results. A punch biopsy that includes the full thickness of the dermis is recommended. Histologic examination shows a normal-appearing epidermis, which may be separated from the underlying inflammatory infiltrate by a narrow grenz zone (Fig. 40-15). Within the dermis is a dense and diffuse infiltrate of lymphocytes, plasma cells, eosinophils, and neutrophils with evidence of leukocytoclasis (Fig. 40-16). The inflammatory infiltrate surrounds the blood vessels, which show evidence of fibrin deposition. In later stages, the perivascular fibrin deposition becomes extensive and dominates the histologic picture. Deposition of hemosiderin may contribute to the brown color seen clinically. Electron microscopy studies confirm the presence of an extensive eosinophilic infiltrate with Charcot–Leyden crystals and numerous histiocytes filled with lysosomal vesicles; however, cases with few
673
6
eosinophils in the infiltrate have also been described.260
Immunoglobulins, fibrin, and complement can be found deposited along the dermal–epidermal junction in a granular pattern and around blood vessels by direct immunofluorescence.258 Recently, dermoscopy has come to be used for assisting the diagnosis. It reveals a translucent white-gray or pink background intermingled with whitish streaks and elongated telangiectasias. The finding of dilated follicular openings,
674
which are more evident under dermoscopy, is of value in the differential diagnosis.261
DIFFERENTIAL DIAGNOSIS
The clinical differential diagnosis for granuloma faciale includes discoid lupus erythematosus, polymorphous light eruption, fixed drug eruption, benign lymphocytic infiltrate of Jessner, lymphoma cutis, pseudolymphoma, sarcoidosis, granuloma annulare, tinea faciei, insect bite reaction, xanthogranuloma, mastocytoma, actinic keratosis, basal cell carcinoma, Langerhans cell histiocytosis, and rosacea (Table 40-12). The diagnosis can be reliably made by histologic examination. Absence of serologic evidence of lupus erythematosus helps differentiate these lesions from the lesions of discoid lupus erythematosus. The primary histologic differential diagnosis is erythema elevatum diutinum (EED). Both diseases represent chronic forms of fibrosing small vessel vasculitis and may be related. However, there are several clinical and histologic differences. EED is characterized by multiple lesions, primarily located on extensor surfaces of the extremities in a symmetric acral distribution. The trunk and face are typically spared in EED. Histologically, both show a chronic fibrosing vasculitis.262 However, a grenz zone of normal collagen beneath the epidermis is not typical of EED. Eosinophils and plasma cells are more prominent in granuloma faciale, whereas
Most Likely
■Face
■Sarcoidosis
■Benign lymphocytic infiltrate of Jessner
■Rosacea
■Extrafacial
■Erythema elevatum diutinum
Consider
■Face
■Discoid lupus erythematosus
■Lymphoma cutis
■Angiolymphoid hyperplasia with eosinophilia
■Tinea faciei
■Actinic keratosis
■Basal cell carcinoma
■Xanthogranuloma
■Mastocytoma
■Extrafacial
■Granuloma annulare
■Benign lymphocytic infiltrate of Jessner
■Fixed drug eruption
Always Rule Out
Always Rule Out
■Face
■Face
■Discoid lupus erythematosus
■Discoid lupus erythematosus
■Trunk
■Trunk
■Erythema elevatum diutinum
■Erythema elevatum diutinum
neutrophils are more frequently found in EED. EED may be associated with systemic conditions, primarily monoclonal gammopathies, and shows an excellent response to dapsone.263,264 The histologic and clinical differential may also include ALHE. However, the lesions of ALHE contain blood vessels with prominent “hobnail” endothelial cells that protrude into the vascular lumina rather than perivascular fibrin deposition. One case of tinea faciei caused by Trichophyton rubrum has been described with clinical and histologic changes consistent with granuloma faciale.265
CLINICAL COURSE, PROGNOSIS, AND MANAGEMENT
Granuloma faciale tends to be chronic and rarely resolves spontaneously. Lesions may be present for weeks or months. It is usually resistant to treatment and tends to relapse after treatment. A variety of medical and surgical therapies have been used in the treatment of granuloma faciale (Table 40-13). Because of the small number of patients involved, randomized trials to evaluate these treatments are lacking. Resistance to therapy and cosmetic complications should be discussed with the patient before initiation of therapy. Topical and intralesional steroids have been administered with modest improvement.252,266 Cryosurgery has been applied with effective results.267,268 Because the disease is known to be a variant of chronic leukocytoclastic vasculitis, dapsone 25 to 100 mg/day has been used with benefit in a number of patients.269,270 Topical tacrolimus ointment 0.1% also has been used with success.271
Surgical excision may be an option for small lesions. Lesions of granuloma faciale have been treated with a variety of medical lasers. In multiple studies using pulsed-dye lasers at 585 to 595 nm, clinical improvement has been demonstrated.272-275 A carbon dioxide laser also has been applied with varying success.276
The use of an argon laser resulted in total resolution of the granuloma faciale with subsequent scarring. The lesions in 2 patients were reported to respond to the potassium-titanyl-phosphate 532-nm laser in combination with tacrolimus ointment 0.1%.277 Case studies
TOPICAL PHYSICAL SYSTEMIC
First-line therapy Topical corticosteroids Cryotherapy Dapsone, 50-100 mg/day
Intralesional steroids
Pulsed-dye laser
Second-line therapy Topical tacrolimus ointment Surgical excision
Second-line
Topical tacroli-
Surgical
therapy
mus ointment
excision
6
suggest a beneficial effect of tacrolimus ointment,278,279
as well as pimecrolimus cream 1%.279
CLINICAL REACTION PATTERNS WITH EOSINOPHIL INVOLVEMENT
There are a variety of diseases in which eosinophils may be present in cutaneous lesions, with or without associated peripheral blood eosinophilia, but either the histologic pattern is unremarkable or eosinophils are not critical for the histologic diagnosis of the given entity (see Table 40-1). In many of these dermatoses, the eosinophil loses its morphologic integrity after disruption through cytolysis and is not identifiable histologically.280 However, toxic granule proteins and other inflammatory eosinophil products are deposited in skin, persist for extended periods of time, and cause tissue effects.42,45 Clinical reaction patterns associated with eosinophil involvement include edema, chronic dermatitis/pruritus (eg, atopic dermatitis and prurigo nodularis), drug reactions, blisters (eg, pemphigoid), fibrosis, and vasculitis. Eosinophils may be observed in a variety of cutaneous and extracutaneous neoplasms.
EOSINOPHILIC FASCIITIS
EOSINOPHILIC FASCIITIS
Eosinophilic fasciitis usually presents with pain, erythema, edema, and induration of the extremities, as well as peripheral blood eosinophilia and hypergammaglobulinemia.281 Contractures and rippling of the skin may develop. Groove sign is a characteristic finding of eosinophilic fasciitis, consisting of a depression along the course of the superficial veins that is more marked upon elevation of the affected limb.282 There is infiltration of lymphocytes, plasma cells, mast cells, and eosinophils, as well as increased thickness of the fascia.
EOSINOPHILIA-MYALGIA SYNDROME
EOSINOPHILIA-MYALGIA
SYNDROME
Eosinophilia-myalgia syndrome, historically related to ingestion of certain lots of L-tryptophan,283 is characterized by marked peripheral eosinophilia, disabling generalized myalgias, pneumonitis, myocarditis, neuropathy, encephalopathy, and fibrosis,284 a constellation of features that are similar to but distinguishable from eosinophilic fasciitis.285,286 Cutaneous abnormalities of eosinophilia-myalgia syndrome include edema, pruritus, a faint erythematous rash, hair loss, and peau d’orange or morphea-like skin lesions.287 Lungs, heart, and nervous system may be affected.288 There is a prominent inflammatory infiltrate in the perimysium and fascia, and striking evidence of eosinophil granule protein deposition in skin and around muscle bundles.283
675
6
ACKNOWLEDGMENTS
The author gratefully acknowledges the following researchers for their valuable contributions: Kristin M. Leiferman, Lisa A. Beck, and Gerald J. Gleich for the section “Regulation of the Production and Activation of Eosinophils”; Kristin M. Leiferman and Margot S. Peters for the section “Eosinophils in Cutaneous Diseases” (excluding the section “Granuloma Faciale”); and David A. Mehregan and Darius R. Mehregan for parts of “Granuloma Faciale.”
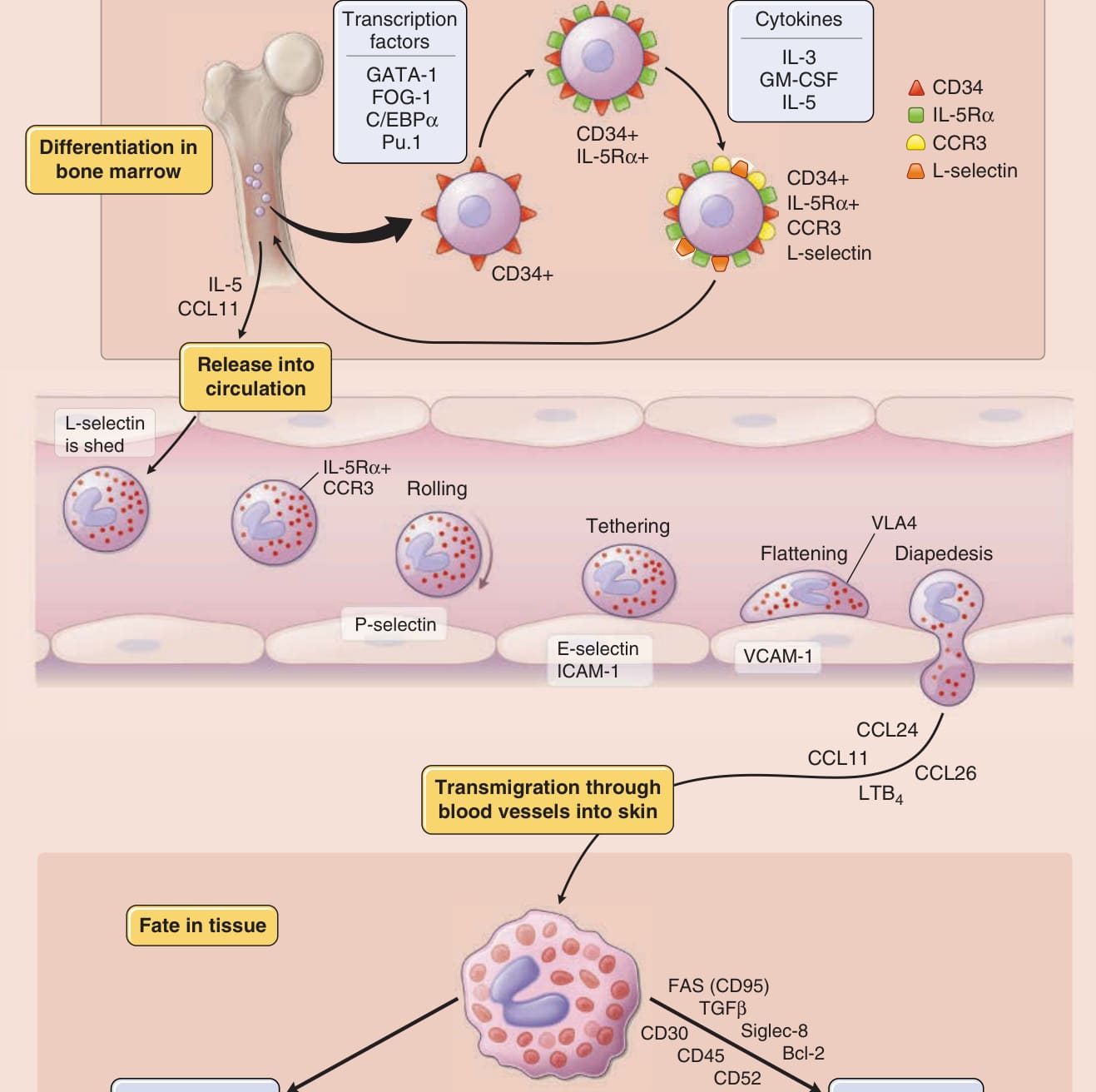
Figure 40-1 The progression of eosinophils from undifferentiated hematopoietic cells to their fate in tissue. The image depicts the eosinophil’s life from differentiation in the bone marrow to vascular transmigration to its fate in tissue with key factors noted. GM-CSF, granulocyte-macrophage colony-stimulating factor; ICAM, intercellular adhesion molecule; IFN, interferon; IL, interleukin; LTB4, leukotriene B4; TGF, transforming growth factor; TNF, tumor necrosis factor; VCAM, vascular cell adhesion molecule.
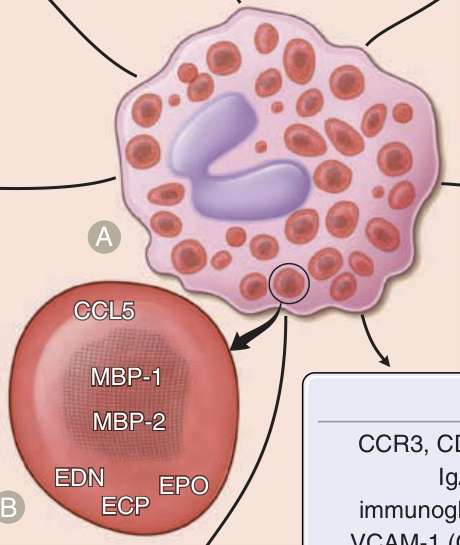
Figure 40-2 shows the products of eosinophils and localization of granule proteins.
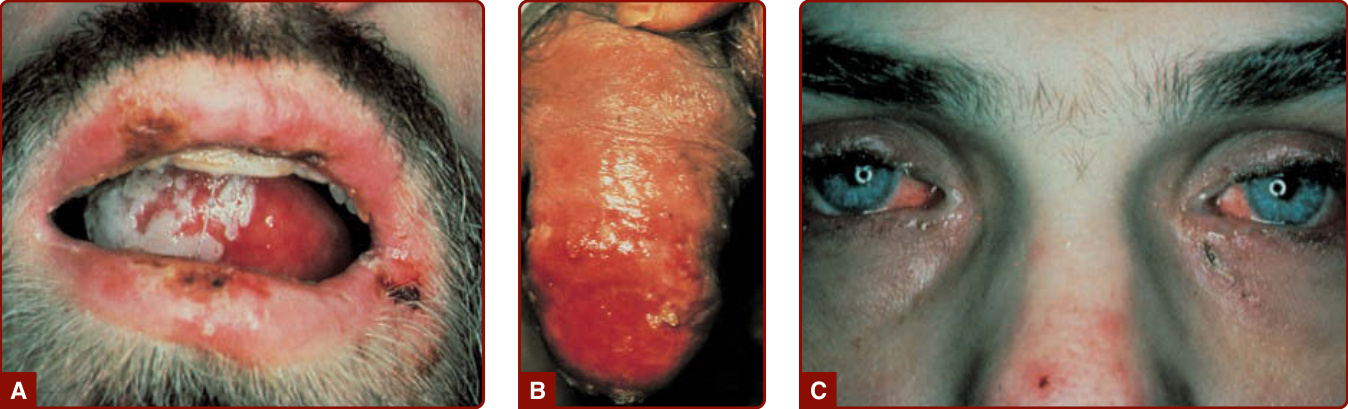
Figure 40-3 Hypereosinophilic syndrome. Mucosal erosions and ulcers of the mouth (A) and glans penis (B); conjunctival irritation (C).
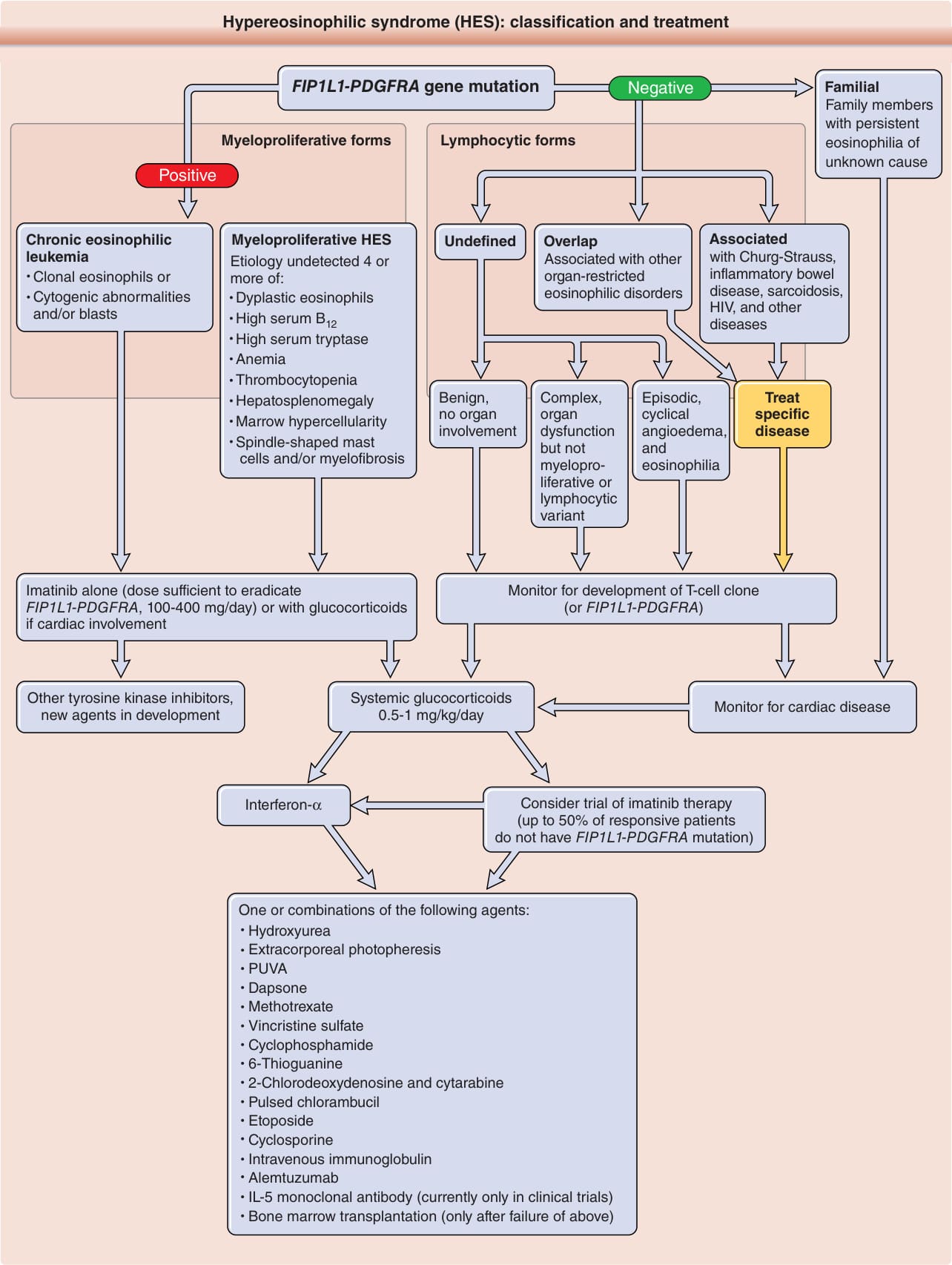
Figure 40-4 Hypereosinophilic syndrome (HES): classification and treatment. Provisional classification consists of myeloproliferative, lymphocytic and familial forms of HES. Chronic eosinophilic leukemia with clonal eosinophilia and myeloproliferative HES with features of the disease but without proof of clonality are included in the myeloproliferative forms of HES; HES with eosinophil hematopoietin-producing T cells with or without a documented T-cell clone constitute the lymphocytic forms of HES. Further HES classification refinement is expected in the near future from a multidisciplinary consensus compendium that is in preparation. FIP1L1-PDGFRA, Fip1-like 1 gene/platelet-derived growth factor receptor-α gene; IL-5, interleukin 5; PUVA, psoralen plus ultraviolet A phototherapy. (Information from Roufosse F, Weller PF. Practical approach to the patient with hypereosinophilia. J Allergy Clin Immunol. 2010;126(1):39-44; Klion AD. Approach to the therapy of hypereosinophilic syndromes. Immunol Allergy Clin North Am. 2007;27(3):551-556; and Stetson CL, Leiferman KM. Eosinophilic dermatoses. In: Bolognia JL, Jorizzo JL, Rapini RP, et al. Dermatology. 2nd ed. St. Louis, MO: Mosby; 2008:369-378.)
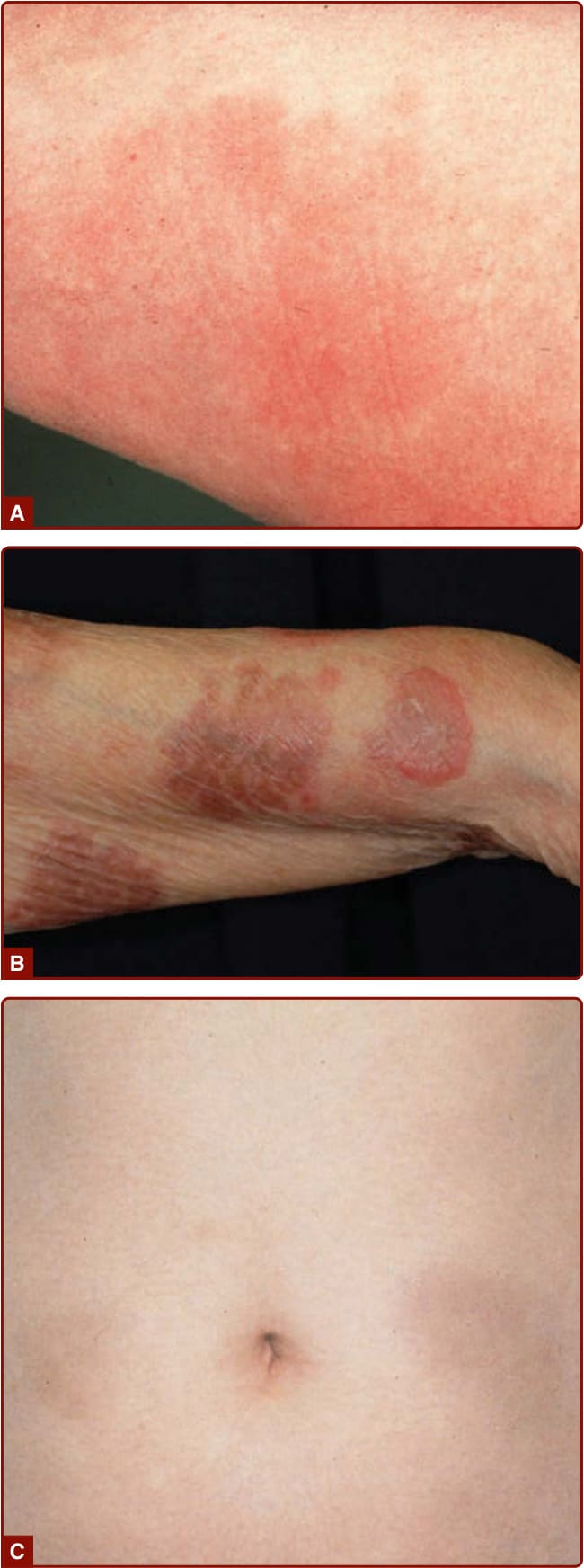
Figure 40-5 Wells syndrome. A, Early lesion with erythema and edema. B, An arcuate plaques and pigmentation. C, Late lesion resembling morphea.

Figure 40-6 Familial Wells syndrome. Plaques with erythema, edema, vesicles, and bullae resembling acute dermatitis or pemphigoid. (From Davis MD, Brown AC, Blackston RD, et al. Familial eosinophilic cellulitis, dysmorphic habitus, and mental retardation. J Am Acad Dermatol. 1998;38(6, pt 1):919-928, with permission. Copyright © American Academy of Dermatology.)
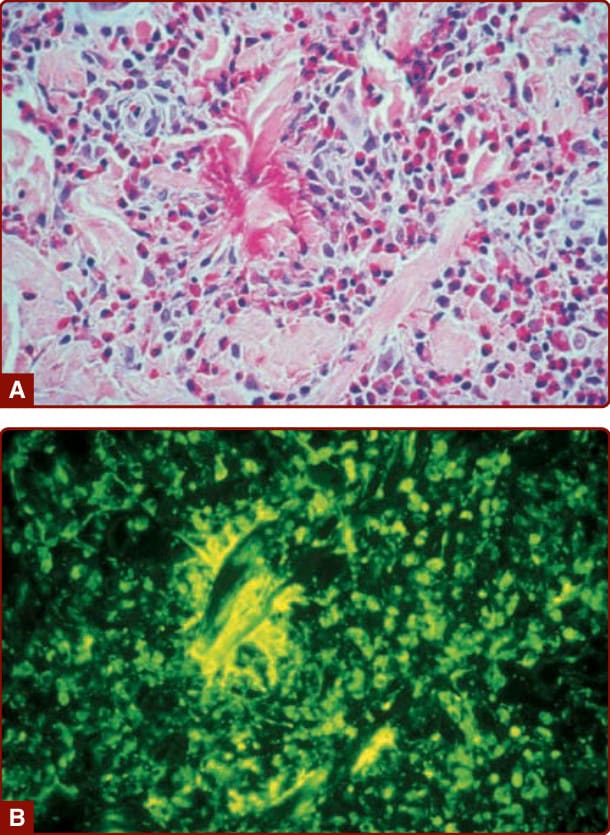
Figure 40-7 Flame figure in familial Wells syndrome. A, Hematoxylin and eosin–stained section. B, Eosinophil granule major basic protein immunostain (of serial section to A) shows extensive granule protein deposition localized to the flame figure. (Original magnification ×400.)
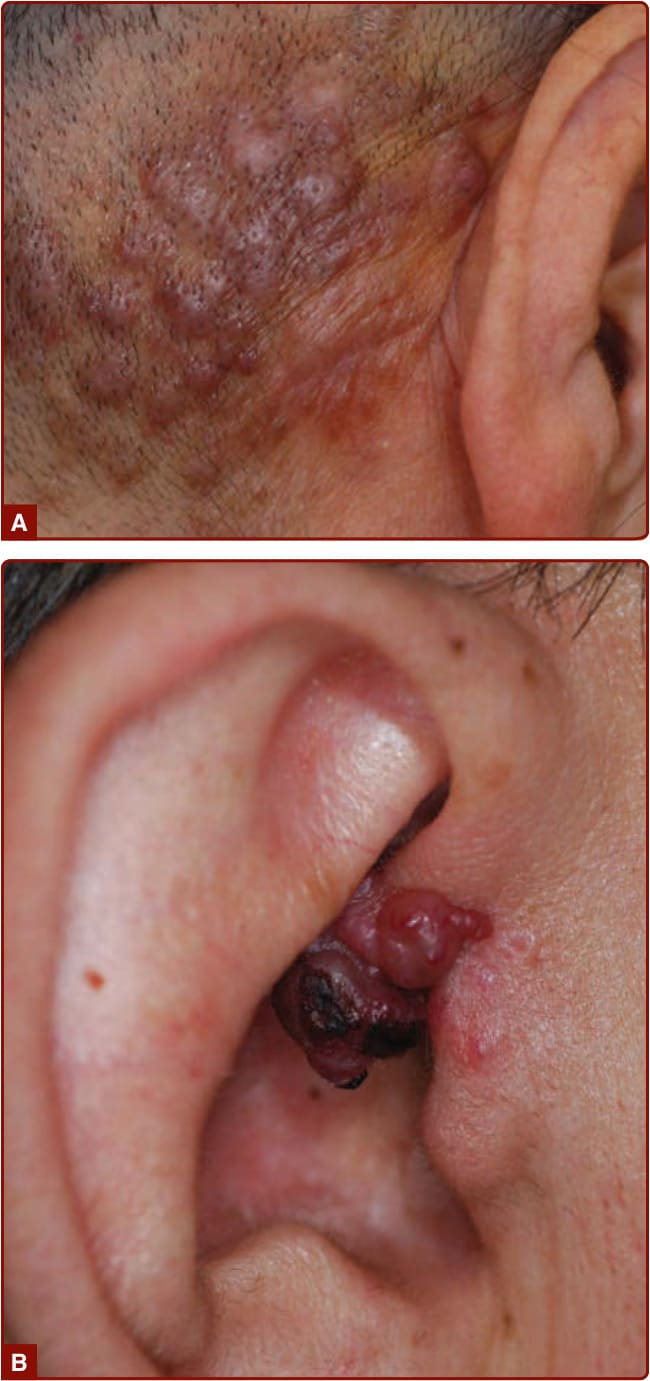
Figure 40-8 Angiolymphoid hyperplasia with eosinophilia. A, Multiple grouped brown nodules. B, Reddish papules.

Figure 40-9 Kimura disease. Solitary brownish nodules and multiple papules.
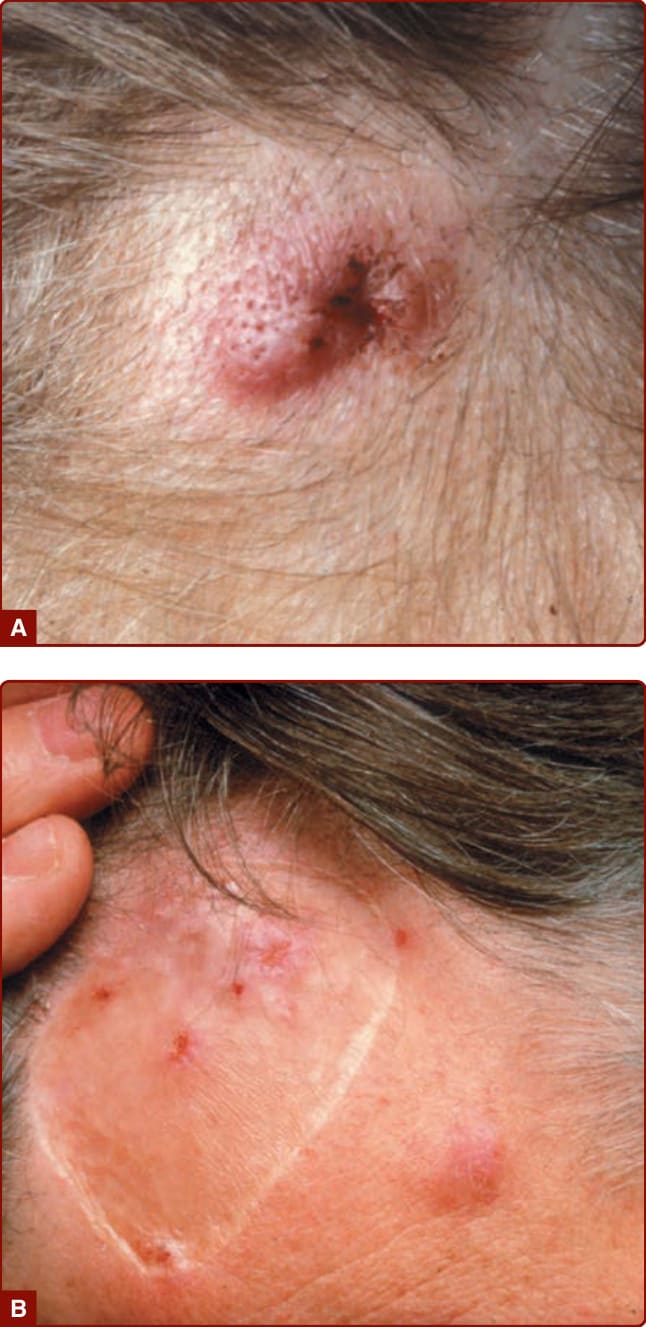
Figure 40-10 Angiolymphoid hyperplasia with eosinophilia. A, Forehead nodule. B, Recurrence of lesions in skin graft and adjacent sites 6 years after surgical removal of lesion in A.
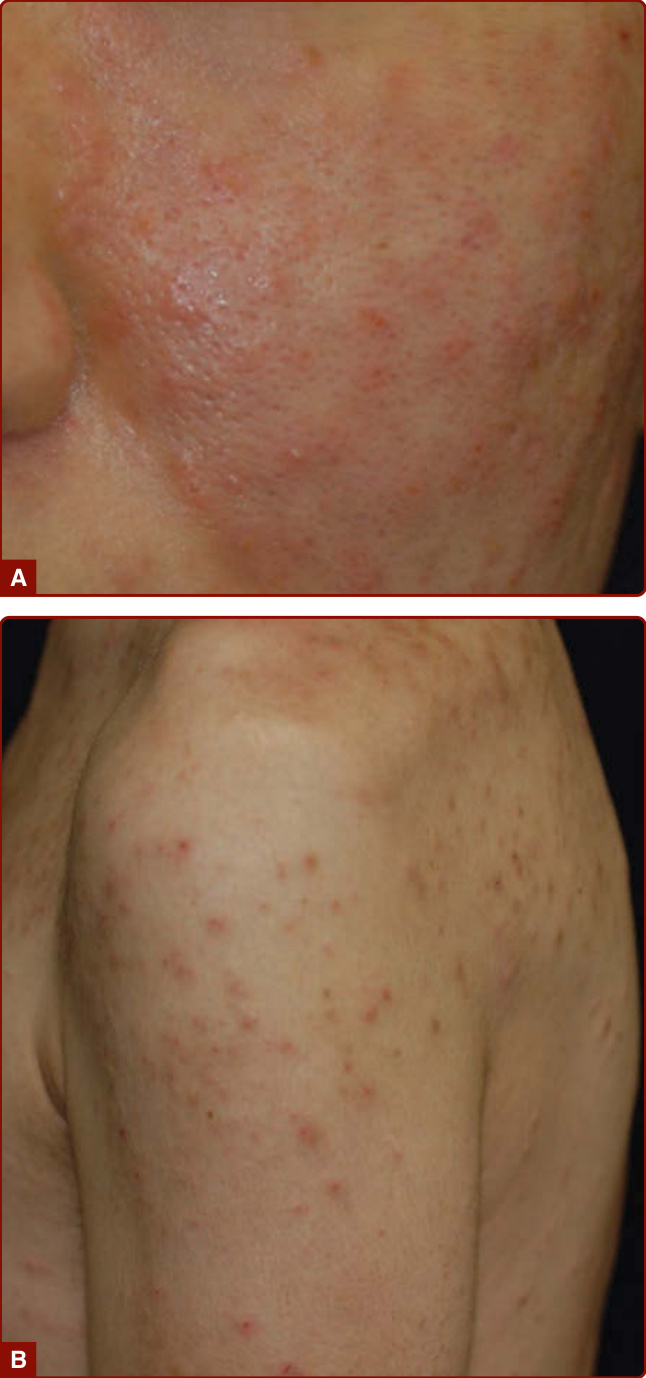
Figure 40-11 Eosinophilic pustular folliculitis. A, Itchy reddish papules and pustules on the cheek. B, An HIVassociated case with itchy red papules on the upper arm, shoulder, and back.

Figure 40-12 Papuloerythroderma of Ofuji. Flat-topped red-to-brown papules with a cobblestone appearance on the abdomen. The sparing of the skin folds, called deckchair sign, is seen.

Figure 40-13 Granuloma faciale. Raised edematous plaques on cheek showing prominent follicular ostia.
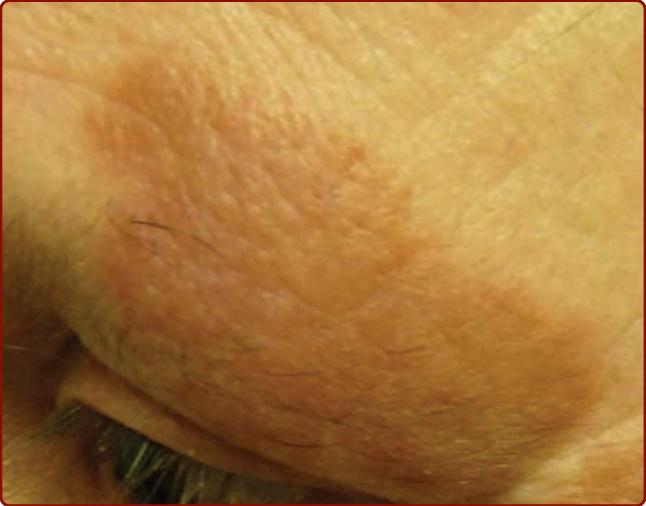
Figure 40-14 Granuloma faciale. Single plaque on the temple showing prominent follicular ostia and central dell.
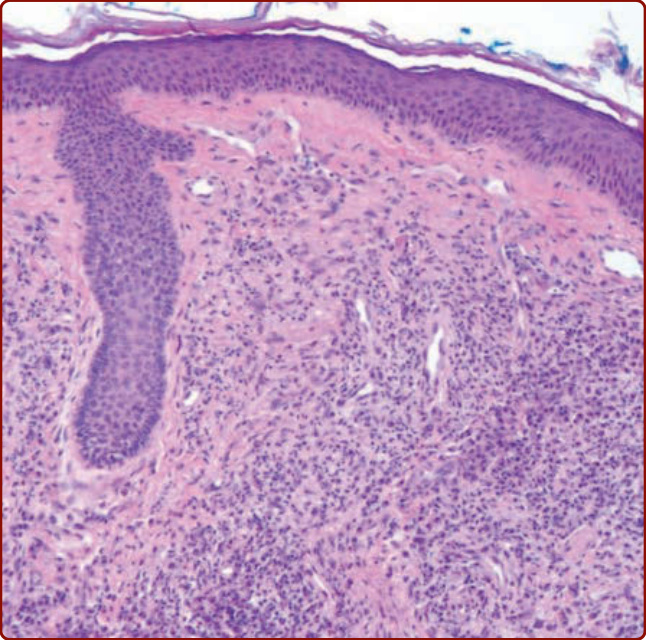
Figure 40-15 Granuloma faciale. This low-power histologic section shows a mixed infiltrate of lymphocytes, histiocytes, neutrophils, plasma cells, and eosinophils. There is sparing of a narrow grenz zone between the inflammatory infiltrate and the overlying epidermis.
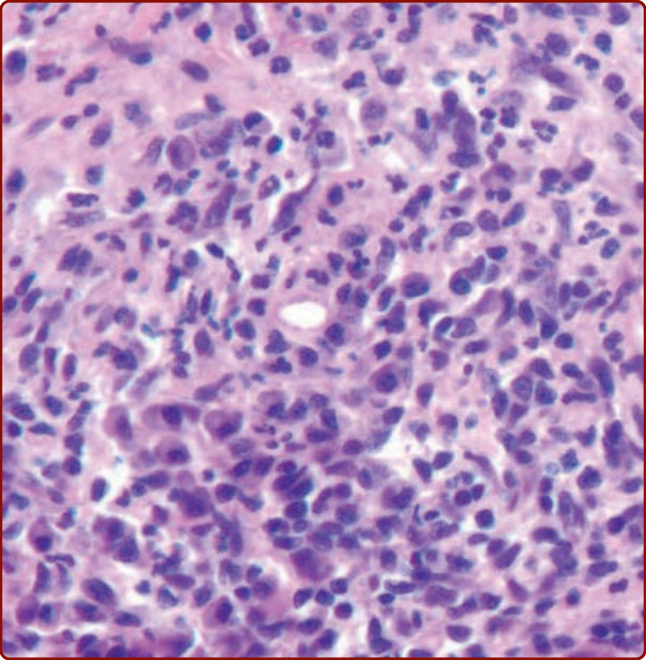
Figure 40-16 Granuloma faciale. This histologic section shows perivascular deposition of fibrin and a mixed infiltrate of lymphocytes, neutrophils, and eosinophils.
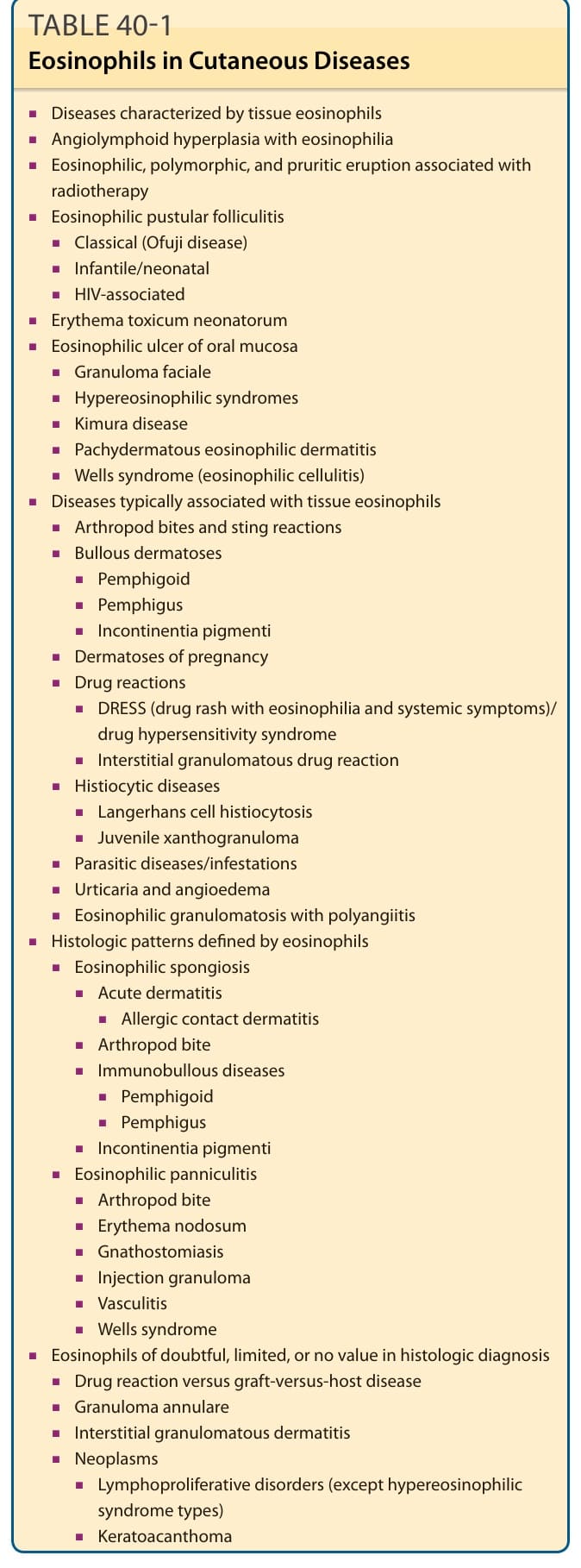
TABLE 40-1 Eosinophils in Cutaneous Diseases
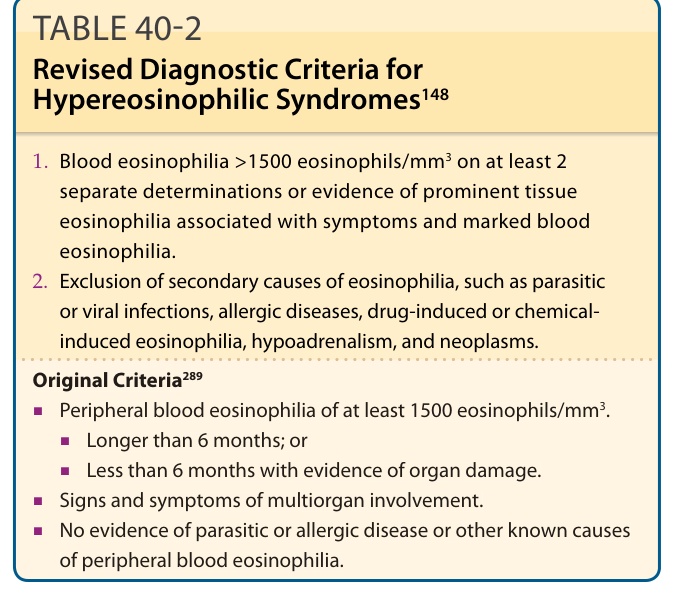
TABLE 40-2 Revised Diagnostic Criteria for Hypereosinophilic Syndromes148
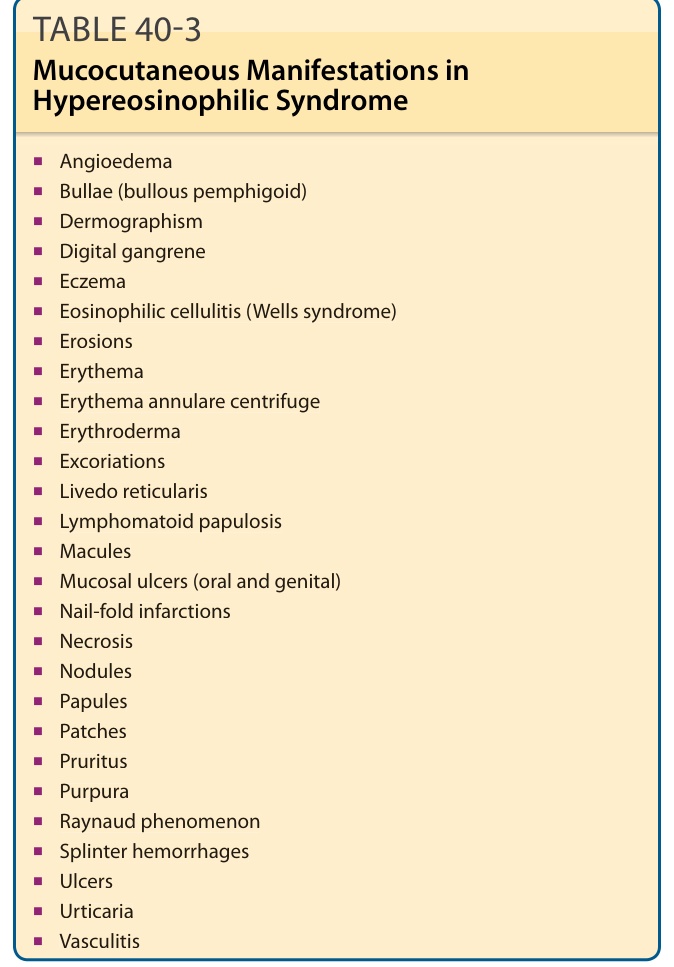
TABLE 40-3 Mucocutaneous Manifestations in Hypereosinophilic Syndrome
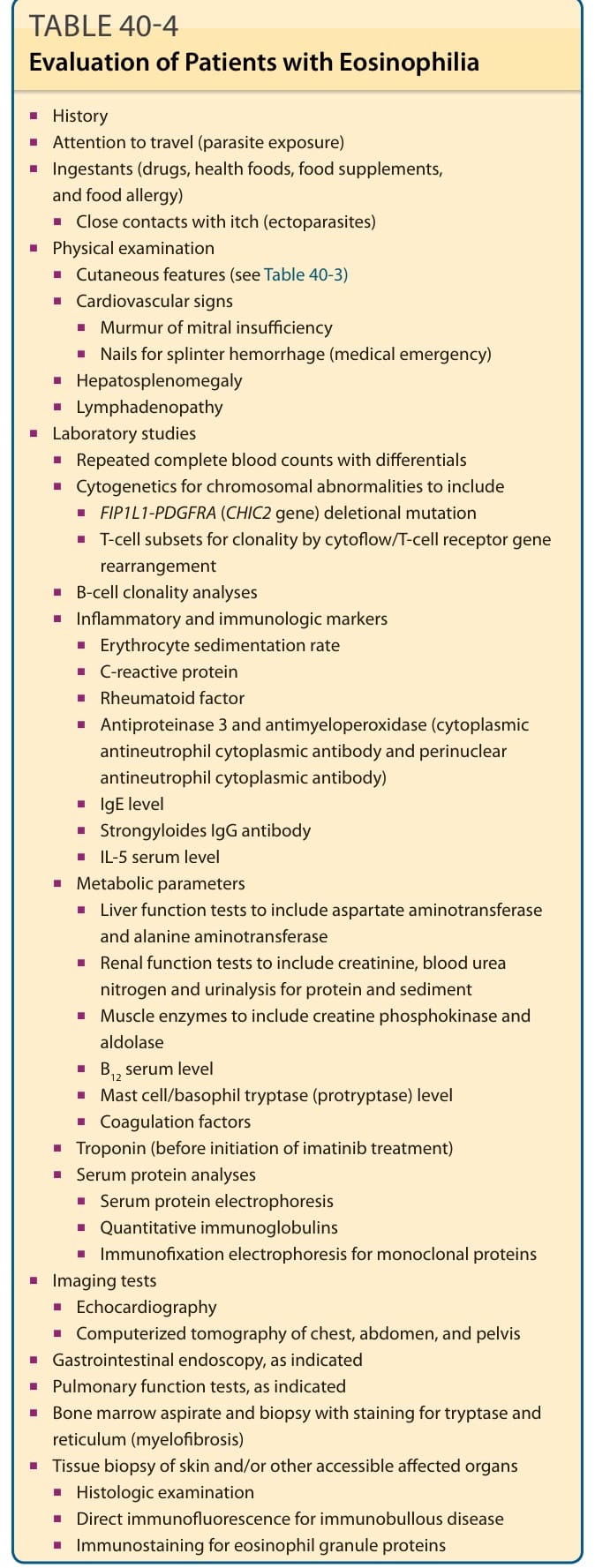
TABLE 40-4 Evaluation of Patients with Eosinophilia
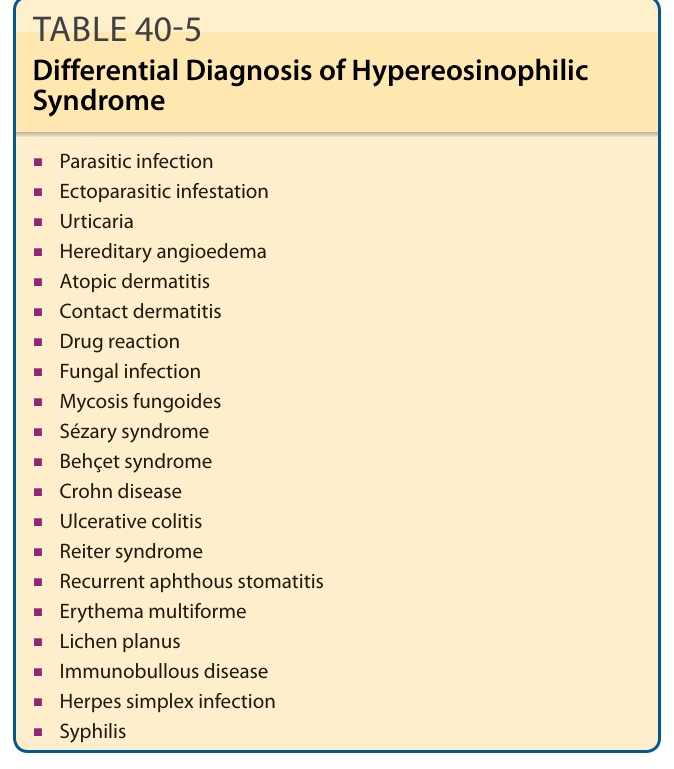
Table 40-5 outlines the differential diagnosis of HES. Clinically, parasitic infections and infestations may closely resemble HES.152 A history of travel to endemic areas or certain dietary exposure implicates helminthiasis. Along with eosinophilia, total serum IgE levels higher than 500 IU/mL commonly are found in helminthic infections. Examination of stool samples for ova and parasites and serologic testing for Strongyloides antibodies should be performed. In patients with isolated urticarial plaques with or without angioedema, the differential diagnosis includes common and persistent urticaria,153,154 but demonstration of multiorgan involvement supports HES. HES with episodic angioedema may resemble hereditary angioedema clinically, although patients with hereditary angioedema often have a family history of the disease rarely have the markedly elevated eosinophil counts that characterize HES, and may be distinguished by complement abnormalities. Pruritic eczematous lesions of lymphocytic HES may resemble those of atopic dermatitis, contact dermatitis, drug reaction, fungal infection, and T-cell lymphoma. There are multiple diseases in the differential diagnosis of patients with orogenital ulcers,129
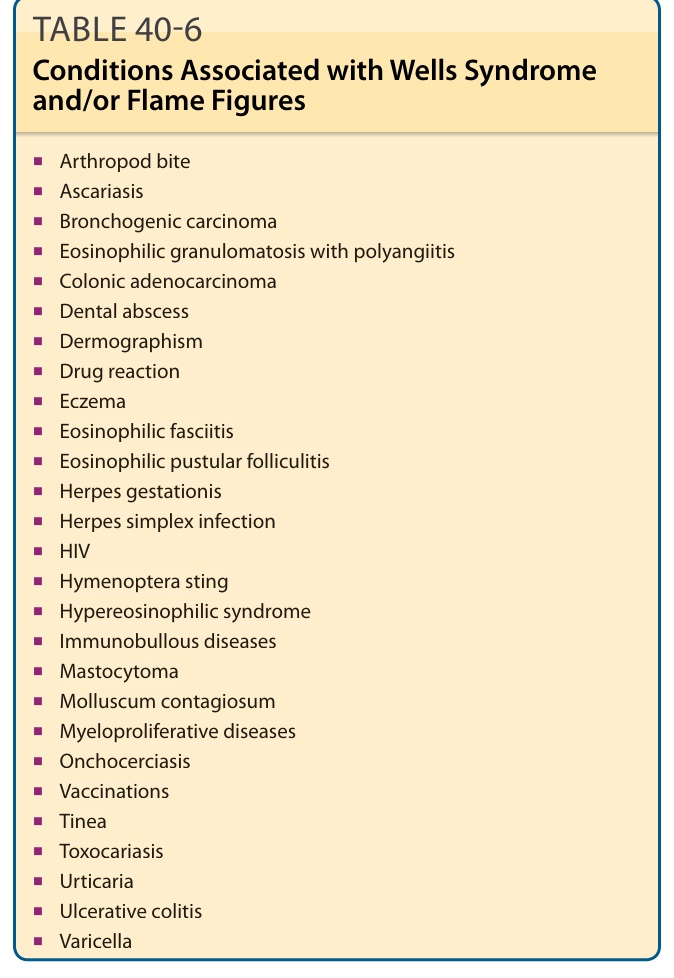
TABLE 40-6 Conditions Associated with Wells Syndrome and/or Flame Figures
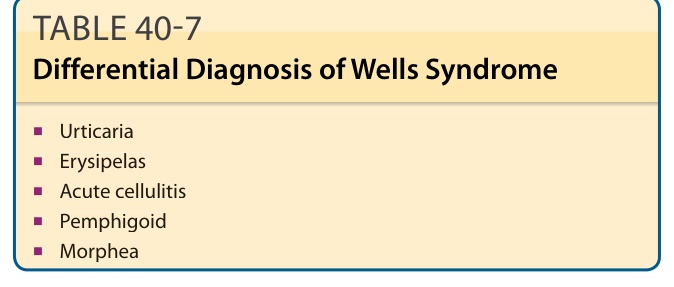
Table 40-7 outlines the differential diagnosis of Wells syndrome.
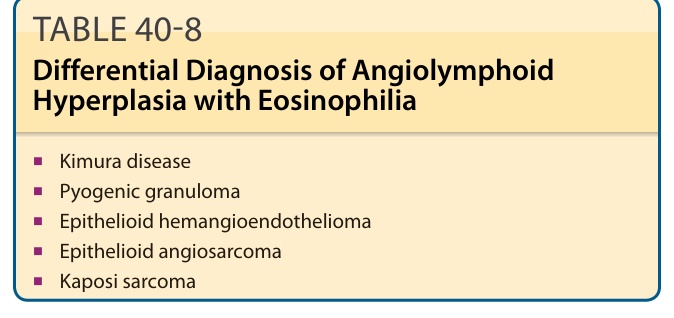
TABLE 40-8 Differential Diagnosis of Angiolymphoid Hyperplasia with Eosinophilia
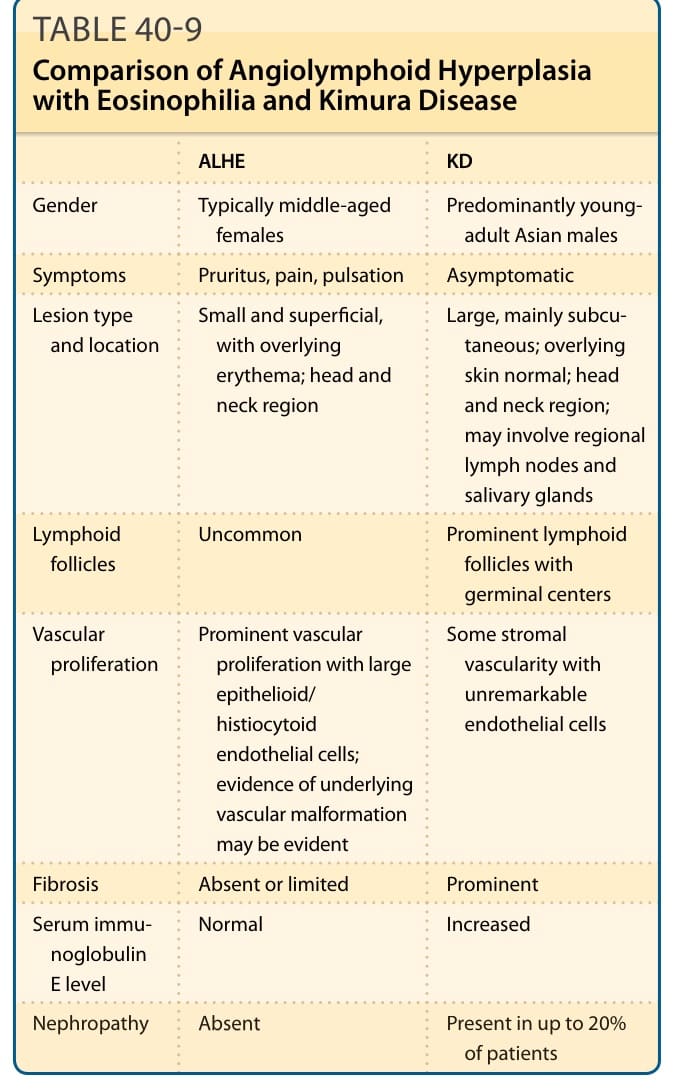
TABLE 40-9 Comparison of Angiolymphoid Hyperplasia with Eosinophilia and Kimura Disease
Table 40-10 outlines the differential diagnosis of KD.
Table 40-11 outlines the differential diagnosis of EPF. Folliculitis secondary to bacterial or fungal infection must be kept in mind, particularly in immunosuppressed patients. Based on the distribution of lesions, seborrheic dermatitis should be considered, when
TABLE 40-12 Differential Diagnosis of Granuloma Faciale
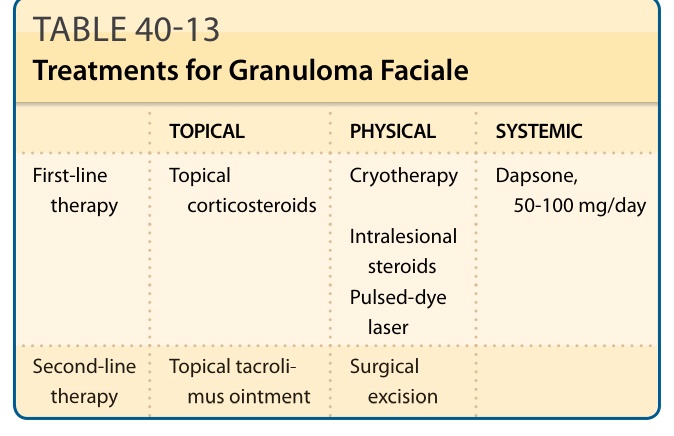
TABLE 40-13 Treatments for Granuloma Faciale