Sweet Syndrome
PART6
Neutrophilic, Eosinophilic, and Mast Cell Disorders
AT-A-GLANCE
■ Sweet syndrome, also referred to as acute febrile neutrophilic dermatosis, is characterized by a constellation of symptoms and findings: the acute onset of fever, neutrophilia, tender erythematous skin lesions that typically show mature neutrophils in the upper dermis, and—after initiation of systemic corticosteroids—a prompt improvement of both symptoms and lesions.
■ Extracutaneous manifestations of Sweet syndrome can include cardiovascular, central nervous system, gastrointestinal, hepatic, musculoskeletal, ocular, oral, otic, pulmonary, renal, and splenic organs.
■ Infection of the upper respiratory tract and/or gastrointestinal tract, inflammatory bowel disease, and pregnancy may be associated with classical Sweet syndrome.
■ In individuals with previously undiagnosed or relapsing hematologic malignancies and solid tumors, malignancy-associated Sweet syndrome may occur as a cutaneous paraneoplastic syndrome.
■ The onset of the dermatosis in patients following the initiation of certain medications—drug-induced Sweet syndrome—is most commonly associated with granulocyte colony-stimulating factor.
■ The pathogenesis of Sweet syndrome remains to be established; cytokines—directly or indirectly—may have an important etiologic role.
■ Corticosteroids, potassium iodide, and colchicine are the first-line oral systemic agents for treating Sweet syndrome.
■ Indomethacin, clofazimine, cyclosporine, and dapsone are the second-line oral systemic agents for treating Sweet syndrome.
■ Localized Sweet syndrome lesions may be effectively treated with the topical application of high-potency corticosteroids or intralesional corticosteroids.
DEFINITION
Sweet syndrome (also known as acute febrile neutrophilic dermatosis) is typically characterized by the acute onset of pyrexia and painful cutaneous lesions that are composed of a dense dermal inflammatory infiltrate of mature neutrophils. Neutrophilia is also frequently present. Both the condition-associated symptoms and the dermatosis-related lesions promptly resolve after initiation of treatment with systemic corticosteroids.1
HISTORICAL PERSPECTIVE
Dr. Robert Douglas Sweet, originally described acute febrile neutrophilic dermatosis in the August- September 1964 issue of the British Journal of Dermatology. He summarized the cardinal features of “a distinctive and fairly severe illness” that had been encountered in 8 women during the 15-year period from 1949 to
1964. In Dr. Sweet’s department, the condition was originally referred to as the Gomm-Button disease “in eponymous honor of the first two patients” with the disease. Subsequently, this acute febrile neutrophilic dermatosis has become best known by the eponym “Sweet syndrome.”1-3
EPIDEMIOLOGY
Numerous individuals with Sweet syndrome have been reported. There is no racial predilection and the distribution of Sweet syndrome cases is worldwide.1
The dermatosis may present in various clinical settings: classical, malignancy-associated, and druginduced (Tables 36-1 and 36-2).4-7
6
CLASSICALa DRUG-INDUCEDb
(1) Abrupt onset of painful erythematous plaques or nodules (2) Histopathologic evidence of a dense neutrophilic infiltrate without evidence of leukocytoclastic vasculitis (3) Pyrexia >38oC (100.4°F) (4) Association with an underlying hematologic (most commonly acute myelogenous leukemia) or visceral malignancy (most commonly carcinomas of the genitourinary organs, breast, and gastrointestinal tract), inflammatory disease (Crohn disease and ulcerative colitis), or pregnancy, or preceded by an upper respiratory (streptococcosis) or gastrointestinal (salmonellosis and yersiniosis) infection or vaccination (5) Excellent response to treatment with systemic corticosteroids or potassium iodide
(A) Abrupt onset of painful erythematous plaques or nodules (B) Histopathologic evidence of a dense neutrophilic infiltrate without evidence of leukocytoclastic vasculitis (C) Pyrexia >38oC (100.4°F) (D) Temporal relationship between drug ingestion and clinical presentation, or temporally related recurrence after oral challenge (E) Temporally related resolution of lesions after drug withdrawal or treatment with systemic corticosteroids
( ) y p y p (6) Abnormal laboratory values at presentation (3 of 4): erythrocyte sedimentation rate
(6) Abnormal laboratory values at presentation (3 of 4): erythrocyte sedimentation rate >20 mm/h; positive C-reactive protein; >8000/µL leukocytes; >70% neutrophils
20 mm/h; positive C-reactive protein; >8000/µL leukocytes; >70% neutrophils
aThe presence of both major criteria (1 and 2), and 2 of the 4 minor criteria (3, 4, 5, and 6) is required to establish the diagnosis of classical Sweet syndrome; the patients with malignancy-associated Sweet syndrome are included with the patients with classical Sweet syndrome in this list of diagnostic criteria.
bAll 5 criteria (A, B, C, D, and E) are required for the diagnosis of drug-induced Sweet syndrome. Adapted with permission from Walker DC, Cohen PR: Trimethoprim-sulfamethoxazole-associated acute febrile neutrophilic dermatosis: case report and review of drug induced Sweet’s syndrome. J Am Acad Dermatol. 1996;34:918-923. Copyright 1996, American Academy of Dermatology, Inc., Mosby-Year Book, Inc., St. Louis, MO.
Medications Associated with Drug-Induced Sweet Syndrome
Abacavir Abatacept Aceclofenac Acyclovir Adalimumab All-trans-retinoic acid Amoxicillin Amoxapine Azacitidine Azathioprine Benzylthiouracil Bortezomib Carbamazepine Celecoxib Chloroquine Ciprofloxacin 13-Cis retinoic acid Citalopram Clindamycin Clozapine Contraceptives Cyclooxygenase-2 inhibitor Diazepam Diclofenac Doxycycline Efavirenz Erythropoietin Esomeprazole Etanercept Furosemide Granulocyte colony-stimulating factor Granulocyte-macrophage colony-stimulating factor Hydralazine Imatinib mesylate Infliximab Interferon alpha (pegylated) Interferon beta-1b
Abacavir Abatacept Aceclofenac Acyclovir Adalimumab All-trans-retinoic acid Amoxicillin Amoxapine Azacitidine Azathioprine Benzylthiouracil Bortezomib Carbamazepine Celecoxib Chloroquine Ciprofloxacin 13-Cis retinoic acid Citalopram Clindamycin Clozapine Contraceptives Cyclooxygenase-2 inhibitor Diazepam Diclofenac Doxycycline Efavirenz Erythropoietin Esomeprazole Etanercept Furosemide Granulocyte colony-stimulating factor Granulocyte-macrophage colony-stimulating factor Hydralazine Imatinib mesylate Infliximab Interferon alpha (pegylated) Interferon beta-1b
588
Interleukin-2 Ipilimumab Isotretinoin Ketoconazole Lamivudine Lenalidomide Levonorgestrel/ethinyl estradiol (Triphasil) Levonorgestrel-releasing intrauterine system (Mirena) Lithium Lopinavir Minocycline Mitoxantrone Nitrofurantoin Norfloxacin Ofloxacin Omeprazole Orphenadrine citrate Pegfilgrastim Perphenazine Phenylbutazone Piperacillin/tazobactam Propylthiouracil Quinupristin/dalfopristin Radiocontrast agent Riboflavin Ritonavir Ruxolitinib Stavudine Sulfa Sulfasalazine Ticagrelor Topotecan Trimethoprim-sulfamethoxazole Triphasil Vemurafenib Vorinostat
Interleukin-2 Ipilimumab Isotretinoin Ketoconazole Lamivudine Lenalidomide Levonorgestrel/ethinyl estradiol (Triphasil) Levonorgestrel-releasing intrauterine system (Mirena) Lithium Lopinavir Minocycline Mitoxantrone Nitrofurantoin Norfloxacin Ofloxacin Omeprazole Orphenadrine citrate Pegfilgrastim Perphenazine Phenylbutazone Piperacillin/tazobactam Propylthiouracil Quinupristin/dalfopristin Radiocontrast agent Riboflavin Ritonavir Ruxolitinib Stavudine Sulfa Sulfasalazine Ticagrelor Topotecan Trimethoprim-sulfamethoxazole Triphasil Vemurafenib Vorinostat
CLINICAL FEATURES
HISTORY
HISTORY
Patients with Sweet syndrome may appear dramatically ill. Fever and leukocytosis often accompany the skin eruption. However, the skin disease can be concurrently present with the fever for the entire episode of the dermatosis or follow the fever by several days to weeks. Other Sweet syndrome associated symptoms include arthralgia, general malaise, headache, and myalgia (Table 36-3).1
6
CUTANEOUS FINDINGS
CUTANEOUS FINDINGS
LESION MORPHOLOGY
Sweet syndrome cutaneous lesions typically appear as tender, red or purple-red, papules or nodules. The skin eruption can present as either a single lesion or multiple—often asymmetrically distributed—lesions (Fig. 36-1). The transparent, vesicle-like appearance of the lesions, described as an “illusion of vesiculation,” results from the pronounced edema in the upper dermis (Fig. 36-2). Central clearing may result in annular
CLINICAL FORM
CLASSICAL (%)a HEMATOLOGIC MALIGNANCY (%)a SOLID TUMOR (%)a DRUG-INDUCED (%)b
CHARACTERISTIC
Epidemiology
Women 80 50 59 71
Prior upper respiratory tract infection 75-90 16 20 21
Recurrencec 30 69 41 67
Clinical Symptoms
Feverd 80-90 88 79 100
Musculoskeletal involvement 12-56 26 34 21
Ocular involvement 17-72 7 15 21
Lesion Location
Upper extremities 80 89 97 71
Head and neck 50 63 52 43
Trunk and back 30 42 33 50
Lower extremities Infrequent 49 48 36
Oral mucous membranes 2 12 3 7
Laboratory Findings
Neutrophiliae 80 47 60 38
Elevated erythrocyte sedimentation ratef 90 100 95 100
Anemiag Infrequent 82 83 100
Abnormal platelet counth Infrequent 68 50 50
Abnormal renal functionI 11-50 15 7 0
Abnormal renal functionI 11-50 15 7 0
aPercentages for classical, hematologic malignancy, and solid-tumor-associated Sweet syndrome adapted with permission from Cohen PR, Kurzrock R: Sweet’s syndrome and cancer. Clin Dermatol. 1993;11:149-157. Copyright 1993, Elsevier Science Publishing Co., Inc., New York, NY.
bPercentages for drug-induced Sweet syndrome adapted with permission from Walker DC, Cohen PR: Trimethoprim-sulfamethoxazole-associated acute febrile neutrophilic dermatosis: case report and review of drug induced Sweet’s syndrome. J Am Acad Dermatol. 1996;34:918-923. Copyright 1996, American Academy of Dermatology, Inc., Mosby-Year Book, Inc., St. Louis, MO.
cRecurrence following oral rechallenge testing in the patients with drug-induced Sweet syndrome.
dTemperature greater than 38oC (100.4°F).
eNeutrophil count greater than 6000 cells/µL.
fErythrocyte sedimentation rate greater than 20 mm/h.
gHemoglobin less than 13 g/dL in men and less than 12 g/dL in women.
hPlatelet count less than 150,000/µL or greater than 500,000/µL.
iThis includes hematuria, proteinuria, and renal insufficiency.
589
6
or arcuate patterns in the later stages; indeed, these lesions can appear targetoid. In patients with malignancy-associated Sweet syndrome, the lesions may appear bullous, become ulcerated, and/or mimic the morphologic features of pyoderma gangrenosum. Over a period of days to weeks, the lesions enlarge; subsequently, they may coalesce and form irregular sharply bordered plaques (Fig. 36-3). The lesions usually resolve without scarring—either spontaneously or after treatment. In one-third to two-thirds of patients, the lesions are associated with recurrent episodes of Sweet syndrome.1
590
A
B
CUTANEOUS PATHERGY AND ISOTOPIC RESPONSE
A dermatosis-associated feature of Sweet syndrome is cutaneous pathergy. This form of skin hypersensitivity occurs when Sweet syndrome skin lesions appear at sites of cutaneous trauma such as prior biopsies, injections, intravenous catheter placement, scalding, and venipuncture. They also include sites of insect bites and cat scratches, areas that have received radiation therapy, and places that have been contacted by sensitizing antigens or henna tattoo.1,7,8
The dermatologic eponym “Wolf’s isotopic response” describes the occurrence of a new skin disorder at the site of another unrelated and already healed skin disease. Sweet syndrome has presented in this manner: lesions affecting a lymphedematous leg or postmastectomy arm and a bullous variant of Sweet syndrome on the side of the cheek and neck where a herpes zoster infection previously occurred in a 75-year-old man.9-11
In addition, lesions have been photodistributed or localized to the site of a prior phototoxic reaction (sunburn) in some Sweet syndrome patients.12
PUSTULAR DERMATOSIS
Sweet syndrome can present as a pustular dermatosis. The lesions appear as tiny pustules on the tops of the red papules or erythematous-based pustules. Some of the patients previously described as having the “pustular eruption of ulcerative colitis” are perhaps more appropriately included in this clinical variant of Sweet syndrome.13,14
NEUTROPHILIC DERMATOSIS OF THE DORSAL HANDS
A localized, pustular variant of Sweet syndrome, when the clinical lesions are predominantly restricted to the dorsal hands, is described as “neutrophilic dermatosis of the dorsal hands” or “pustular vasculitis of the dorsal hands.” In these individuals, the lesions are similar to those of Sweet syndrome in morphology and rapid resolution after systemic corticosteroids and/or dapsone therapy was initiated. Many of patients with this form of the disease also had concurrent oral mucosa, arm, leg, back, and/or face lesions.2,15
SUBCUTANEOUS PANNICULITIS
Subcutaneous Sweet syndrome lesions usually present as erythematous, tender dermal nodules on the extremities. The lesions mimic erythema nodosum when they are located on the legs. One study reported findings of panniculitis in 80% of patients in which the hypodermis was affected. Therefore, even in a patient with biopsy-confirmed Sweet syndrome, tissue evaluation of one or more new dermal nodules may be necessary to establish the correct diagnosis as Sweet syndrome can present concurrently or sequentially with erythema nodosum.3,8,15-17
HISTIOCYTOID VARIANT
Histiocytoid Sweet syndrome was initially described by Requena et al. in 2005. The skin lesion morphology is similar to that of idiopathic Sweet syndrome. However, the dermal infiltrate is composed of mononuclear cells with a histiocytic appearance—representing immature myeloid cells.18
This variant of Sweet syndrome is often associated with malignancy. Drug-induced histiocytoid Sweet syndrome has also been observed in patients receiving bortezomib.18,19
GIANT CELLULITIS-LIKE VARIANT
A morphologically distinctive clinical variant of Sweet syndrome, characterized by relapsing widespread giant lesions, is giant cellulitis-like Sweet syndrome.
6
In 2013, it was originally reported in 3 morbidly obese individuals. In 2014, 2 additional patients were described, and in 2015, a sixth patient with concurrent histiocytoid Sweet syndrome was reported.18,20-22
Giant cellulitis-like Sweet syndrome has been observed in 5 women and 1 man, ranging in age from 48 years to 72 years (median = 61 years). The upper leg and buttocks were the most common locations of their skin lesions (Fig. 36-4). Most of the patients (66%) were obese and half of the patients had cancer.18,20-22
NECROTIZING VARIANT
Necrotizing Sweet syndrome is a new variant of neutrophilic dermatosis that mimics necrotizing fasciitis. It clinically presents as the rapid onset of edematous, erythematous, warm cutaneous lesions. An infectious etiology for the lesions is absent. Biopsy shows a deep-tissue neutrophilic infiltration and soft-tissue necrosis.23
NONCUTANEOUS FINDINGS
NONCUTANEOUS FINDINGS
POTENTIAL ORGANS
The bones, central nervous system, ears, eyes, kidneys, intestines, liver, heart, lung, mouth, muscles, and spleen can be sites of extracutaneous manifestations of Sweet syndrome (Table 36-4).1,7
BONE INVOLVEMENT
In children, dermatosis-related sterile osteomyelitis has been reported.1
591
6
Bone Acute sterile arthritis; arthralgias; focal aseptic osteitis; pigmented villonodular synovitis; sterile osteomyelitis (chronic recurrent multifocal osteomyelitis)
Central nervous system Acute benign encephalitis; aseptic meningitis; brain single-photon emission computed tomography (SPECT) abnormalities; brainstem lesions; cerebrospinal fluid abnormalities; computerized axial tomography abnormalities; electroencephalogram abnormalities; encephalitis; Guillain-Barré syndrome; idiopathic hypertrophic cranial pachymeningitis; idiopathic progressive bilateral sensorineural hearing loss; leukoencephalopathy; magnetic resonance imaging abnormalities; neurologic symptoms; “neuro-Sweet disease”; pareses of central origin; polyneuropathy; psychiatric symptoms
Ears Tender red nodules and pustules that coalesced to form plaques in the external auditory canal and the tympanic membrane
Eyes Blepharitis; chemosis; conjunctival erythematous lesions with tissue biopsy showing neutrophilic inflammation; conjunctival hemorrhage; conjunctivitis; dacryoadenitis; episcleritis; glaucoma; iridocyclitis; iritis; limbal nodules; ocular congestion; periocular swelling; peripheral ulcerative keratitis; retinal vasculitis; scleritis; uveitis
Kidneys Mesangiocapillary glomerulonephritis; urinalysis abnormalities (hematuria and proteinuria)
Intestines Intestine with extensive and diffuse neutrophilic inflammation; neutrophilic ileal infiltrate; pancolitis (culture-negative)
Liver Hepatic portal triad with neutrophilic inflammation; hepatic serum enzyme abnormalities; hepatomegaly
Heart Aortic stenosis (segmental); aortitis (neutrophilic and segmental); cardiomegaly; coronary artery occlusion; heart failure; myocardial infiltration by neutrophils; vascular (aorta, brachiocephalic trunk and coronary arteries) dilatation
Lung Bronchi (main stem) with red-bordered pustules; bronchi with neutrophilic inflammation; pleural effusion showing abundant neutrophils without microorganisms; chest roentgenogram abnormalities; corticosteroid-responsive culture-negative infiltratives; pulmonary tissue with neutrophilic inflammation
Mouth Aphthous-like superficial lesions (buccal mucosa, tongue); bullae and vesicles (hemorrhagic: labial and gingival mucosa); gingival hyperplasia; necrotizing ulcerative periodontitis; nodules (necrotic: labial mucosa); papules (macerated: palate and tongue); pustules (individual and grouped: palate and pharynx); swelling (tongue); ulcers (buccal mucosa and palate)
Muscles Magnetic resonance imaging (T1-weighted and T2-weighted) abnormalities: high signal intensities caused by myositis and fasciitis; myalgias (in up to half of the patients with idiopathic Sweet syndrome); myositis (neutrophilic); tendinitis; tenosynovitis
Spleen Aseptic abscess; splenomegaly.
Spleen Aseptic abscess; splenomegaly.
From Cohen PR, Kurzrock R. Sweet’s syndrome revisited: a review of disease concepts. Int J Dermatol. 2003;42:761-778, with permission.
CARDIAC INVOLVEMENT
Sweet syndrome-associated cardiovascular involvement may occur in children. A 22-month-old white boy with Sweet syndrome developed postinflammatory elastolysis and Takayasu arteritis. Cardiovascular involvement resulting from elastolysis of the heart and aorta occurred in 3 children who were ages 17 months, 16 months, and 7 months; 2 of the patients died.24,25
Cardiovascular involvement, including coronary artery occlusion, occurred in a 43-year-old man with Sweet syndrome.26
CENTRAL NERVOUS SYSTEM INVOLVEMENT
A wide variety of neurologic symptoms have been observed in neuro-Sweet disease. This rare variant of the dermatosis, which can affect regions of the central nervous system, was originally proposed by Hisanaga et al. in 1999. Neuro-Sweet disease, in a 72-yearold man, presented with self-remitting and reversible parkinsonism. In a 49-year-old man, optic nerve involvement with panuveitis was reported. Bilateral endogenous endophthalmitis with chorioretinitis arising from nontuberculous mycobacterial infection occurred in a 47-year-old Thai woman with underlying
592
Sweet syndrome. Radiation therapy-induced neuro- Sweet disease was described in a 67-year-old woman with oral squamous cell carcinoma.27-30
OCULAR INVOLVEMENT
Ocular manifestations of Sweet syndrome may be the presenting feature of the condition. In classical Sweet syndrome, the incidence of ocular involvement (such as conjunctivitis) is variable. However, in the malignancy-associated and drug-induced forms of the dermatosis it is uncommon.1
ORAL INVOLVEMENT
Mucosal ulcers of the mouth are uncommon in patients with classical Sweet syndrome. However, they occur more frequently in Sweet syndrome patients with hematologic disorders. The oral lesions—similar to extracutaneous manifestations of Sweet syndrome occurring at other sites—typically resolve after initiation of treatment with systemic corticosteroids.1
OTIC INVOLVEMENT
In a 65-year-old woman with a 10-year history of Sweet syndrome, a rapid, profound loss of hearing was reported; bilateral, progressive sensorineural hearing
loss after a severe exacerbation of Sweet syndrome had been diagnosed 7 years prior.31
SPLEEN INVOLVEMENT
Spleen and lymph node involvement was preceded by parvovirus B19 infection in a 45-year-old white woman with Sweet syndrome.32
COMPLICATIONS
COMPLICATIONS
Complications may occur in Sweet syndrome patients. They can either be directly related to the mucocutaneous lesions or indirectly related to the Sweet syndrome-associated conditions. Antimicrobial therapy may be necessary if the skin lesions become secondarily infected. Reappearance of the dermatosis may herald the unsuspected discovery that the cancer has recurred in patients with malignancy-associated Sweet syndrome. Disease-specific treatment may be warranted for systemic manifestations of Sweet syndrome-related conditions such as inflammatory bowel disease, sarcoidosis, and thyroid disease.1,7
ETIOLOGY AND PATHOGENESIS
ASSOCIATED CONDITIONS
ASSOCIATED CONDITIONS
ASSOCIATED DISEASES
Several conditions have been observed to occur either before, concurrent with, or following the diagnosis of Sweet syndrome (Table 36-5). Behçet disease, cancer, erythema nodosum, infections, inflammatory bowel disease, pregnancy, relapsing polychondritis, rheumatoid arthritis, sarcoidosis, and thyroid disease may be etiologically related to the development of Sweet syndrome. The association between Sweet syndrome and other conditions remains to be established.1
Sweet syndrome associated with differentiation syndrome (an inflammatory reaction with increased capillary permeability that occurs in up to 25% of patients with acute promyelocytic leukemia treated with all-trans-retinoic acid) was suspected in a 50-yearold man with acute promyelocytic leukemia who underwent chemotherapy with idarubicin and alltrans-retinoic acid.33 The histiocytoid variant of Sweet syndrome is associated not only with medications, but also with several other conditions, including autoimmune diseases, infections and inflammation, inflammatory bowel disease, and malignancy (Table 36-6).18
Giant cellulitis-like Sweet syndrome was associated with obesity (4 of 6 patients) and malignancy (3 of 6 patients): hematologic dyscrasia (multiple myeloma or myelodysplastic syndrome/myeloproliferative disorder) and breast cancer (Table 36-7).18,20-22
6
ASSOCIATED NEUTROPHILIC DERMATOSES
The unifying characteristic of neutrophilic dermatoses of the skin and mucosa is an inflammatory infiltrate of mature polymorphonuclear leukocytes. Concurrent or sequential occurrence either of erythema elevatum diutinum, neutrophilic eccrine hidradenitis, pyoderma gangrenosum, subcorneal pustular dermatosis, and/or vasculitis with Sweet syndrome has been observed. These conditions can display similar clinical and pathologic features; however, the location of the neutrophilic infiltrate helps differentiate them.2,3,34,35
CONCURRENT LEUKEMIA CUTIS
Sweet syndrome may present as either a paraneoplastic syndrome (signaling the initial discovery of an unsuspected malignancy), a drug-induced dermatosis (following treatment with either all-trans-retinoic acid, bortezomib, granulocyte colony-stimulating factor (G-CSF), or imatinib mesylate), or a condition whose skin lesions concurrently demonstrate leukemia cutis in patients with hematologic disorders. The most frequent hematologic dyscrasias associated with leukemia cutis (characterized by abnormal neutrophils) and Sweet syndrome (consisting of mature polymorphonuclear leukocytes) being present in the same skin lesion are acute myelocytic leukemia and acute promyelocytic leukemia. Other associated hematologic disorders that have been associated with concurrent Sweet syndrome and leukemia cutis include myelodysplastic syndrome and either chronic myelogenous leukemia or myelogenous leukemia not otherwise specified.1,7
One of the hypotheses to explain concurrent Sweet syndrome and leukemia cutis in the same lesion is “secondary” leukemia cutis; in patients with “secondary” leukemia cutis, the circulating immature myeloid precursor cells are innocent bystanders that have been recruited to the skin as the result of an inflammatory oncotactic phenomenon stimulated by the Sweet syndrome lesions. Another possibility is the occurrence of “primary” leukemia cutis. In patients with “primary” leukemia cutis, the leukemic cells within the skin constitute the bonified incipient presence of a specific leukemic infiltrate. Finally, in patients with “primary” leukemia cutis who were being treated with G-CSF, it is possible that the atypical cells of leukemia cutis developed into mature neutrophils of Sweet syndrome as a result of G-CSF therapy-induced differentiation of the sequestered leukemia cells.1
SYSTEMIC INFLAMMATORY RESPONSE SYNDROME
Sweet syndrome can occur with systemic inflammatory response syndrome. A 76-year-old man with
593
6
Sweet Syndrome and Associated Conditions TABLE 36-5
Probably bona fide associated conditions
Probably bona fide associated conditions
■Cancer: hematologic malignancies (most commonly acute myelogenous leukemia) and solid tumors (most commonly carcinomas of the genitourinary organs, breast, and gastrointestinal tract)
■Cancer: hematologic malignancies (most commonly acute myelog-
enous leukemia) and solid tumors (most commonly carcinomas of the genitourinary organs, breast, and gastrointestinal tract)
■Infections: most commonly of the upper respiratory tract (streptococcosis) and the gastrointestinal tract (salmonellosis and yersiniosis)
■Infections: most commonly of the upper respiratory tract (strep-
tococcosis) and the gastrointestinal tract (salmonellosis and yersiniosis)
■Inflammatory bowel disease: Crohn disease and ulcerative colitis
■Inflammatory bowel disease: Crohn disease and ulcerative colitis
■Medications: most commonly granulocyte colony-stimulating factor
■Medications: most commonly granulocyte colony-stimulating
factor
■Pregnancy
■Pregnancy
■Vaccinations (bacille Calmette-Guérin [BCG] and influenza) Possibly bona fide associated conditions
■Vaccinations (bacille Calmette-Guérin [BCG] and influenza) Possibly bona fide associated conditions
■Behçet disease
■Behçet disease
■Erythema nodosum
■Erythema nodosum
■Relapsing polychondritis
■Relapsing polychondritis
■Rheumatoid arthritis
■Rheumatoid arthritis
■Sarcoidosis
■Sarcoidosis
■Thyroid disease: Grave disease and Hashimoto thyroiditis Validity of associated conditions remains to be established
■Thyroid disease: Grave disease and Hashimoto thyroiditis Validity of associated conditions remains to be established
■α1-Antitrypsin deficiency
■α1-Antitrypsin deficiency
■Antineutrophilic cytoplasmic antibody–associated vasculitis
■Antineutrophilic cytoplasmic antibody–associated vasculitis
■Ankylosing spondylitis
■Ankylosing spondylitis
■Anti–factor VIII inhibitor
■Anti–factor VIII inhibitor
■Antiphospholipid syndrome
■Antiphospholipid syndrome
■Aortitis (Takayasu arteritis)
■Aortitis (Takayasu arteritis)
■Aplastic anemia
■Aplastic anemia
■Autoimmune disorders: cholangitis, dermatomyositis, lupus erythematosus (subacute and systemic), pemphigus vulgaris, and Sjögren syndrome
■Autoimmune disorders: cholangitis, dermatomyositis, lupus erythe-
matosus (subacute and systemic), pemphigus vulgaris, and Sjögren syndrome
■Autologous stem cell transplant
■Autologous stem cell transplant
■Bronchiolitis obliterans and organizing pneumonia
■Bronchiolitis obliterans and organizing pneumonia
■Chemical fertilizer
■Chemical fertilizer
■Chronic fatigue syndrome
■Chronic fatigue syndrome
■Chronic recurrent multifocal osteomyelitis
■Chronic recurrent multifocal osteomyelitis
■Celiac disease
■Celiac disease
■Cirrhosis (cryptogenic)
■Cirrhosis (cryptogenic)
■Common bile duct and intrahepatic duct stones
■Common bile duct and intrahepatic duct stones
■Congenital dyserythropoietic anemia
■Congenital dyserythropoietic anemia
■Congenital neutropenia (Kostmann syndrome)
■Congenital neutropenia (Kostmann syndrome)
■Cutis laxa (acquired, Marshall syndrome)
■Cutis laxa (acquired, Marshall syndrome)
■Differentiation syndrome
■Differentiation syndrome
■Dressler syndrome (postmyocardial infarction syndrome)
■Dressler syndrome (postmyocardial infarction syndrome)
■End-stage renal disease
■End-stage renal disease
■Eosinophilic granuloma
■Eosinophilic granuloma
■Familial Mediterranean fever
■Familial Mediterranean fever
Sweet syndrome-associated pulmonary involvement also experienced systemic inflammatory response syndrome. Sepsis refers to systemic inflammatory response syndrome caused by infection. Yet, this man’s systemic inflammatory response syndrome was attributed to Sweet syndrome because his cultures were persistently negative.36,37
PATHOGENESIS
PATHOGENESIS
The pathogenesis of Sweet syndrome remains to be definitively established and may be multifactorial.
594
■Fanconi anemia
■Fanconi anemia
■Glycogen storage disease (type Ib)
■Glycogen storage disease (type Ib)
■Granuloma annulare
■Granuloma annulare
■Hemophagocytic syndrome
■Hemophagocytic syndrome
■Immunoglobulin A nephropathy (Berger disease)
■Immunoglobulin A nephropathy (Berger disease)
■Immunizing agent (BCG vaccination and flu)
■Immunizing agent (BCG vaccination and flu)
■Immunodeficiency diseases: chronic granulomatous disease, common variable immunodeficiency, complement deficiency, HIV infection, and primary T-cell immunodeficiency disease
■Immunodeficiency diseases: chronic granulomatous disease,
common variable immunodeficiency, complement deficiency, HIV infection, and primary T-cell immunodeficiency disease
■Infections: Anaplasma phagocytophilum, bartholinitis, bronchitis, Campylobacter spp., Capnocytophaga canimorsus, Chlamydia, Chlamydophila pneumoniae, cholangitis, cholecystitis, coccidioidomycosis, cytomegalovirus, dermatophyte, Entamoeba histolytica, Epstein-Barr virus, Francisella tularensis, Helicobacter pylori, hepatitis (acute or chronic hepatitis B, autoimmune, cholestatic, chronic active, hepatitis C, and prior hepatitis A), herpes simplex, herpes zoster, histoplasmosis, HIV, leprosy, leptospirosis, lymphadenitis (not otherwise specified and subacute necrotizing), mycobacteria avium, chelonae, nontuberculous, and tuberculous, otitis media, pancreatitis, parvovirus B19, Pasteurella multocida bronchitis, Penicillium spp., Pneumocystis carinii pneumonia, pyelonephritis, sporotrichosis, Staphylococcus aureus, Staphylococcus epidermidis (methicillin-resistant), subacute bacterial endocarditis, tonsillitis, toxoplasmosis, tuberculosis, tularemias (glandular), ureaplasmosis, urinary tract, and vulvovaginitis
■Infections: Anaplasma phagocytophilum, bartholinitis, bron-
chitis, Campylobacter spp., r Capnocytophaga canimorsus, Chlamydia, Chlamydophila pneumoniae, cholangitis, cholecystitis, coccidioidomycosis, cytomegalovirus, dermatophyte, Entamoeba histolytica, Epstein-Barr virus, Francisella tularensis, Helicobacter pylori, hepatitis (acute or chronic hepatitis B, autoimmune, cholestatic, chronic active, hepatitis C, and prior hepatitis A), herpes simplex, herpes zoster, histoplasmosis, HIV, leprosy, leptospirosis, lymphadenitis (not otherwise specified and subacute necrotizing), mycobacteria avium, chelonae, nontuberculous, and tuberculous, otitis media, pancreatitis, parvovirus B19, Pasteurella multocida bronchitis, Penicillium spp., Pneumocystis carinii pneumonia, pyelonephritis, sporotrichosis, Staphylococcus aureus, Staphylococcus epidermidis (methicillin-resistant), subacute bacterial endocarditis, tonsillitis, toxoplasmosis, tuberculosis, tularemias (glandular), ureaplasmosis, urinary tract, and vulvovaginitis
■Kidney transplantation
■Kidney transplantation
■Kikuchi disease
■Kikuchi disease
■Malabsorption
■Malabsorption
■Microscopic polyangiitis
■Microscopic polyangiitis
■Mid-dermal elastolysis
■Mid-dermal elastolysis
■POEMS syndrome (polyneuropathy, organomegaly, endocrinopathy, M protein, and skin changes)
■POEMS syndrome (polyneuropathy, organomegaly, endocrinopa-
thy, M protein, and skin changes)
■Postoperative (pneumonectomy)
■Postoperative (pneumonectomy)
■Psoriasis vulgaris
■Psoriasis vulgaris
■Rhinosinusitis
■Rhinosinusitis
■Sialadenitis
■Sialadenitis
■Still disease
■Still disease
■Takayasu arteritis
■Takayasu arteritis
■Thermal injury
■Thermal injury
■Transient acantholytic dermatosis (Grover disease)
■Transient acantholytic dermatosis (Grover disease)
■Ureter obstruction
■Ureter obstruction
■Urticaria (chronic)
■Urticaria (chronic)
■Urticaria pigmentosa
■Urticaria pigmentosa
■Wegner granulomatosis
■Wegner granulomatosis
■Welding burns
■Welding burns
ANIMAL MODELS
Animal models of Sweet syndrome have been described. An alteration in the gene encoding protein tyrosine phosphatase nonreceptor type 6— originally found in a mouse with clinical and histopathologic characteristics resembling Sweet syndrome—appears to be involved in the pathogenesis of certain subsets of neutrophilic dermatoses, including Sweet syndrome. In a female standard poodle dog (after treatment with the nonsteroidal antiinflammatory drug firocoxib) and in multiple dogs (temporally associated with the administration of carprofen) a condition presenting
Autoimmune diseases
■Positive lupus erythematosus serologies
■Relapsing polychondritis
■Rheumatoid arthritis
■Systemic lupus erythematosus
Infections/inflammation
■Conjunctivitis
■Methicillin-resistant Staphylococcus aureus (pneumonia)
■Parotitis
■Sinusitis
Inflammatory bowel disease
■Crohn disease
■Ulcerative colitis
Malignancies
■Acute myelogenous leukemia
■Breast carcinoma
■Chronic lymphocytic leukemia
■Chronic monocytic leukemia
■Chronic myelogenous leukemia
■Hodgkin lymphoma
■Leukemia cutis (from acute myelomonocytic leukemia)
■Lymphoma
■Monoclonal gammopathy of undetermined significance
■Multiple myeloma
■Myelodysplastic syndrome
■Myelodysplastic syndrome/myeloproliferative disorder
■Renal carcinoma
Medications
■Azacitidine
■Azathioprine
■Bortezomib
■Cox-2 inhibitor
■Decitabine
■Trimethoprim-sulfamethoxazole
Other conditions
Other conditions
■Diabetes mellitus
■Diabetes mellitus
■Erythema nodosum
■Erythema nodosum
■Eyelid edema
■Eyelid edema
■Familial Mediterranean fever
■Familial Mediterranean fever
■Glomerulonephritis
■Glomerulonephritis
■Hypertension
■Hypertension
■Immunosuppression
■Immunosuppression
■None
■None
■Polyarteritis nodosa
■Polyarteritis nodosa
■Pregnancy
■Pregnancy
From So JK, Carlos CA, Frucht CS, et al. Histiocytoid giant cellulitis-like Sweet’s syndrome: case report and review of the literature. Dermatol Online J. 2015;21(3):4 with permission.
as a sterile neutrophilic dermatosis, and similar to Sweet syndrome, has been observed; subsequent examination also revealed extracutaneous involvement of the esophagus, heart, lungs, and tarsus (joint space and synovium). In addition, a sterile neutrophilic dermatosis of the skin—similar to Sweet syndrome—has been described in a female Dachshund; the condition responded rapidly to corticosteroid therapy.38-40
6
BACTERIAL, VIRAL, OR TUMOR ANTIGENS
A hypersensitivity reaction to an eliciting bacterial, viral, or tumor antigen may elicit Sweet syndrome. The accompanying fever and peripheral leukocytosis suggests the possibility of a septic process. Indeed, in patients with classic Sweet syndrome, a febrile upper respiratory tract bacterial infection or tonsillitis may precede skin lesions by 1 to 3 weeks. Also, Sweet syndrome patients with Yersinia enterocolitica intestinal infection have improved with systemic antibiotics.1
FAMILIAL MEDITERRANEAN FEVER
The systemic manifestations of familial Mediterranean fever resemble those of Sweet syndrome. Indeed, the simultaneous occurrence of both conditions has been observed. In addition, the causative gene mutation for familial Mediterranean fever was detected in a patient with chronic myelogenous leukemia-associated Sweet syndrome. Hence, these conditions may have a similar pathogenesis.7
HUMAN LEUKOCYTE ANTIGEN SEROTYPES
A 5-week-old Japanese girl with Sweet syndrome and non-B54 types of human leukocyte antigen was reported. She is one of the youngest patients reported with the dermatosis. The potential importance of genetic background in association with Sweet syndrome is suggested by this observation.41
CYTOKINES
Circulating autoantibodies, dermal dendrocytes, immune complexes and leukotactic mechanisms have all been postulated to contribute to the pathogenesis of Sweet syndrome. The immunoreactivity of several cytokines (interleukin [IL]-1, IL-8, IL-17, and tumor necrosis factor-α), inflammatory cell markers (CD3, CD163, and myeloperoxidase), metalloproteinases (metalloproteinase-2 and metalloproteinase-9), and vascular endothelial growth factor have displayed significantly higher values in the lesional skin of patients with Sweet syndrome from non-Sweet syndrome individuals or patients with other neutrophilic dermatoses. The observation of a 48-year-old white woman with coexisting Sweet syndrome, Hashimoto thyroiditis, and psoriasis suggests the possibility of a CD4+ T-cell dysfunction in the pathogenesis of the dermatosis. Complement does not appear to be essential to the disease process. Antibodies to neutrophilic cytoplasmic antigens have been demonstrated in some patients; however, these are thought to represent an epiphenomenon.1,42,43
The development of Sweet syndrome symptoms and lesions may—directly and/or indirectly—be caused by
595
6
AS SYMPTOMS WBC (cells/uL) OTHER LABS ASSOC DIS TX RESPONSE REF
62M Fever Malaise 10.6+ ANA– CRP+ Ob MM Amox Pred No effect from antibiotics; good response from oral prednisone 20 C1
48F Fever Malaise 24+ CRP+ Ob Pred Good control 20 C2
54F Fever 4.1 Creat+ TC– Ob PBC Si
Pred Excellent 21
60F^ Fever 10.3 TC– – Col Pred Dap
Response, but recurrence on colchicine and prednisone; excellent response to dapsone and prednisone
22
68F Fever Malaise 11.3+ CRP+ TC– Br Ob Surg Top Transient improvement then recurrence with topical corticosteroid; remission after surgical treatment of breast carcinoma
72F Fever Foot pain
73.5+ LDH+ TC–
20 C3
MDS/MPD Top Excellent 18
72F Fever Foot pain 73.5+ LDH+ TC– MDS/MPD Top Excellent 18
The site of skin lesions and (number of patients) were: lower extremity (6 patients) [18,20 (cases 1,2, and 3), 21,22]; trunk (5 patients) [18,20 (cases 1 and 2), 21,22]; buttock (3 patients) [20 (cases 1 and 2), 21]; upper extremity (2 patients) [20 (case 2), 21]; and head and neck (1 patients).21
Negative; ^, patient was in her “60’s”; +, elevated; Amox, amoxicillin/clavulanic acid; ANA, antinuclear antibody; AS, age (in years) and sex; Assoc dis, associated disease; Br, breast carcinoma; Col, colchicine; CR, current report; Creat, serum creatinine; CRP, C-reative protein; Dap, dapsone; F, female; LDH, lactate dehydrogenase; M, male; MDS/MPD, myelodysplastic/myeloproliferative disorder; MM, multiple myeloma; Ob, obesity; PBC, primary biliary cirrhosis; Pred, prednisone; Ref, reference; Si, sicca syndrome; Surg, surgical treatment of breast carcinoma; TC, tissue culture; Top, topical corticosteroid; Tx, treatment; WBC, white blood cell. From So JK, Carlos CA, Frucht CS, et al. Histiocytoid giant cellulitis-like Sweet’s syndrome: case report and review of the literature. Dermatol Online J. 2015;21(3):4 with permission.
cytokines. A patient with myelodysplastic syndromeassociated Sweet syndrome demonstrated elevated serum levels of G-CSF and IL-6; the individual was not receiving the drugs. An infant with classical Sweet syndrome had detectable levels of intraarticular synovial fluid granulocyte-macrophage colony-stimulating factor (GM-CSF). Compared to dermatosis patients with inactive Sweet syndrome, a study demonstrated that the serum G-CSF level was significantly higher in individuals with active Sweet syndrome. And, in a patient with acute myelogenous leukemia-associated Sweet syndrome and neutrophilic panniculitis, the level of endogenous G-CSF was closely associated with Sweet syndrome disease activity.1,7,17
IMMUNOHISTOCHEMICAL STUDIES
Significantly elevated levels of helper T-cell type 1 cytokines (IL-2 and interferon-gamma [IFN-γ]) and normal levels of a helper T-cell type 2 cytokine (IL-4) in the sera of Sweet syndrome patients have been observed in immunohistochemical studies. Serial measurements of cerebral spinal fluid IL-6, IFN-γ, IL-8, and interferon-inducible protein-10 were elevated as compared to levels in control subjects with neurologic disorders and also correlated with total cerebral spinal fluid cell counts in a patient with neuro-Sweet disease presenting with recurrent encephalomeningitis. This data suggests an important role of the helper T-cell type 1 cell (whose cytokines include
596
IFN-γ and interferon-inducible protein-10) and IL-8 (a specific neutrophil chemoattractant) in the pathogenesis of neuro-Sweet disease. Other studies postulated that cytokine release into the dermis accounted for decreased epidermal staining for IL-1 and IL-6. In summary, G-CSF, GM-CSF, IFN-γ, IL-1, IL-3, IL-6, and IL-8 are potential cytokine candidates in the pathogenesis of Sweet syndrome.1,7,12,17
PHOTOSENSITIVITY
Photosensitivity may play a role in the pathogenesis of Sweet syndrome. Experimental induction of Sweet syndrome has been elicited by phototesting. Also, in a woman who was receiving trimethoprim-sulfamethoxazole, photodrug-associated Sweet syndrome developed in sun-exposed areas. Although the mechanism of pathogenesis is unknown, one hypothesis suggests an isomorphic Koebner reaction. Another postulated theory associates ultraviolet-B radiation with neutrophil activation and epidermal production of tumor necrosis factor-α and IL-8.12,44-46
DIAGNOSIS
DIAGNOSTIC CRITERIA
DIAGNOSTIC CRITERIA
In 1986, diagnostic criteria for classical or idiopathic Sweet syndrome were proposed by Su and Liu.
They were modified in 1994 by von den Driesch (see Table 36-1). Infection (upper respiratory tract or gastrointestinal tract), inflammatory bowel disease, or pregnancy may be associated with Sweet syndrome. A seasonal preference for the onset of Sweet syndrome for either autumn or spring has been observed.7,12,47
Classical Sweet syndrome most commonly occurs in women; onset appears between the ages of 30 years and 60 years. Yet, classical Sweet syndrome has also been observed in younger adults and children. Brothers who developed the dermatosis at 10 and 15 days of age are the youngest Sweet syndrome patients. In the neonatal period, the appearance of Sweet syndrome in the first 6 weeks of life often heralds a serious underlying disorder, thus requiring a thorough investigation for the associated condition.48,49
It is appropriate to distinguish the classical form of Sweet syndrome from the malignancy-associated variant of this condition as there is a temporal association with the discovery or relapse of cancer and the onset or recurrence of many Sweet syndrome cases. A comprehensive review of 66 pediatric Sweet syndrome patients observed an associated hematologic
A
C
6
malignancy in 44% of 30 children between 3 years and 18 years of age. In adults, malignancy-associated Sweet syndrome is most often associated with acute myelogenous leukemia and does not have a female predominance. Carcinomas of the genitourinary organs, breast, and gastrointestinal tract are the most frequently occurring cancers in Sweet syndrome patients with dermatosis-related solid tumors.1,7,47,50
In 1996, Walker and Cohen established the criteria for drug-induced Sweet syndrome (see Table 36-1). G-CSF is the most frequently observed agent associated with this variant of the dermatosis. However, other medications are also implicated in eliciting drug-induced Sweet syndrome (Fig. 36-5; see Table 36-2).7,10,18,33,51-55
SUPPORTIVE STUDIES
SUPPORTIVE STUDIES
LABORATORY TESTING
A complete blood cell count with leukocyte differential and platelet count, evaluation of acute-phase
B
597
6
reactants (such as the erythrocyte sedimentation rate or C-reactive protein), serum chemistries (evaluating hepatic function and renal function), and an urinalysis should be performed. As there appears to be a bona fide association between thyroid disease and Sweet syndrome, it is also reasonable to perform a serologic evaluation of thyroid function.1
Peripheral leukocytosis with neutrophilia and an elevated erythrocyte sedimentation rate and are the most consistent laboratory findings in Sweet syndrome. However, in patients with biopsy-confirmed Sweet syndrome, leukocytosis is not always present. For example, in some of the patients with malignancyassociated Sweet syndrome, anemia, neutropenia, and/or abnormal platelet counts may be observed.1
Urinalysis abnormalities (hematuria and proteinuria) and hepatic serum enzyme elevation may be observed in patients with kidney and liver involvement. Abnormalities in cerebrospinal fluid analysis may be observed in patients with central nervous system involvement.1,7
PATHOLOGY
When the diagnosis of Sweet syndrome is suspected, evaluation of a lesional skin biopsy is helpful. As the pathologic findings of Sweet syndrome are similar to those observed in cutaneous lesions caused by infectious agents, lesional tissue should also be submitted for bacterial, fungal, mycobacterial, and, possibly, viral cultures.1
Characteristically, a diffuse infiltrate of mature neutrophils is present in the papillary and upper reticular dermis (Fig. 36-6). However, the inflammatory infiltrate can also involve the epidermis or adipose tissue. In contrast to the infiltrate of mature neutrophils typically seen in Sweet syndrome, histiocytoid Sweet syndrome is characterized by a dermal infiltrate composed of immature granulocytes that are histiocytic mononuclear cells (Fig. 36-7). Morphologically, the small cells of
598
histiocytoid Sweet syndrome appear similar to neutrophils; however, they stain for CD15, CD43, CD45 (LCA), CD68, HAM56, lysozyme, and MAC 387—thereby identifying a monocytic-histiocytic profile (Fig. 36-8).7,18
The inflammation in the dermis is typically dense and diffuse. However, it can also be perivascular. In addition, the dermal inflammation can demonstrate “secondary” changes of leukocytoclastic vasculitis; these changes are considered to be an epiphenomenon and not representative of a “primary” vasculitis.2
Exocytosis of neutrophils into the epidermis can result in neutrophilic spongiotic vesicles or subcorneal pustules. The condition is referred to as “subcutaneous Sweet syndrome” when the neutrophils are located either entirely or partially in the subcutaneous fat.1,3
The spectrum of pathologic changes described in cutaneous lesions of Sweet syndrome has expanded; it now includes concurrent leukemia cutis, vasculitis,
A B
6
and variability of the composition or the location of the inflammatory infiltrate. Edema in the dermis, swollen endothelial cells, dilated small blood vessels, and fragmented neutrophil nuclei (referred to as karyorrhexis or leukocytoclasia) may also be present (Fig. 36-9). However, the overlying epidermis is normal and fibrin deposition or neutrophils within the vessel walls (changes of “primary” leukocytoclastic vasculitis) are usually absent.1,2
The inflammatory infiltrate of Sweet syndrome lesions may also contain lymphocytes or histiocytes. In some patients with either idiopathic or drug-induced or malignancy-associated Sweet syndrome, the cutaneous lesions contain eosinophils. In some of the Sweet syndrome patients with hematologic disorders, abnormal neutrophils (leukemia cutis)—in addition to mature neutrophils—comprise the dermal infiltrate.56-58
Extracutaneous sites can also show pathologic findings of Sweet syndrome. They often, appear as sterile neutrophilic inflammation in the involved organ. These changes have been observed in the aorta, bones, intestines, liver, lungs, and muscles of patients with Sweet syndrome.1,7
IMAGING
Abnormalities on brain single-photon emission computed tomography, computerized axial tomography,
electroencephalograms, and magnetic resonance imaging may be observed in patients with central nervous system involvement. In a 62-year-old man with Sweet syndrome, magnetic resonance imaging findings of dermatosis-associated neutrophilic fasciitis and musculoskeletal involvement were reported. Pleural effusions and corticosteroid-responsive culture-negative infiltrates on their chest roentgenograms may be noted in patients with pulmonary involvement.1,59
DIFFERENTIAL DIAGNOSIS
CLINICAL DIFFERENTIAL DIAGNOSIS
CLINICAL DIFFERENTIAL
DIAGNOSIS
The skin and mucosal lesions of Sweet syndrome mimic those of other conditions (Table 36-8). The clinical differential diagnosis of Sweet syndrome includes infectious and inflammatory disorders, neoplastic conditions, reactive erythemas, vasculitis, other cutaneous conditions, and other systemic diseases.1,7,47
Patients with Behçet disease, similar to those with Sweet syndrome, may develop lesions at sites of trauma. An important differentiator between Sweet syndrome and Behçet disease is human leukocyte
599
6
■Acral erythema
■Acral erythema
■Azathioprine hypersensitivity reaction
■Azathioprine hypersensitivity reaction
■Bacterial sepsis
■Bacterial sepsis
■Behçet disease
■Behçet disease
■Bowel bypass syndrome
■Bowel bypass syndrome
■Cellulitis
■Cellulitis
■Chloroma
■Chloroma
■Chronic atypical neutrophilic dermatosis with lipodystrophy and elevated temperature (CANDLE) syndrome
■Chronic atypical neutrophilic dermatosis with lipodystrophy and
elevated temperature (CANDLE) syndrome
■Dermatomyositis
■Dermatomyositis
■Drug eruptions
■Drug eruptions
■Erysipelas
■Erysipelas
■Erythema elevatum diutinum
■Erythema elevatum diutinum
■Erythema multiforme
■Erythema multiforme
■Erythema nodosum
■Erythema nodosum
■Familial Mediterranean fever
■Familial Mediterranean fever
■Gemcitabine-associated Sweet syndrome-like eruptions
■Gemcitabine-associated Sweet syndrome-like eruptions
■Granuloma faciale
■Granuloma faciale
■Halogenoderma
■Halogenoderma
■Leprosy
■Leprosy
■Leukemia cutis
■Leukemia cutis
■Leukocytoclastic vasculitis
■Leukocytoclastic vasculitis
■Lupus erythematosus
■Lupus erythematosus
■Lymphangitis
■Lymphangitis
■Lymphoma
■Lymphoma
■Metastatic tumor
■Metastatic tumor
■Neutrophilic eccrine hidradenitis
■Neutrophilic eccrine hidradenitis
■Panniculitis
■Panniculitis
■Periarteritis nodosa
■Periarteritis nodosa
■Pyoderma gangrenosum
■Pyoderma gangrenosum
■Rheumatoid neutrophilic dermatitis
■Rheumatoid neutrophilic dermatitis
■Rosacea fulminans
■Rosacea fulminans
■Schnitzler syndrome
■Schnitzler syndrome
■Syphilis
■Syphilis
■Systemic mycosis
■Systemic mycosis
■Thrombophlebitis
■Thrombophlebitis
■Tuberculosis
■Tuberculosis
■Urticaria
■Urticaria
■Viral exanthem
■Viral exanthem
Adapted from Cohen PR, Kurzrock R: Sweet’s syndrome and cancer. Clin Dermatol. 1993;11:149-157. Copyright © Elsevier.
antigen analysis. In Japan, the B51 marker is significantly higher in Behçet disease, whereas the B54 marker is more frequently associated with Sweet syndrome.60
Other conditions in the clinical differential diagnosis of Sweet syndrome include azathioprine hypersensitivity reaction, chronic atypical neutrophilic dermatosis with lipodystrophy and elevated temperature (CANDLE) syndrome, and gemcitabine-associated Sweet syndrome-like eruptions. In addition, not only cellulitis and other infections, but also periodic syndromes (such as familial Mediterranean fever) can be included in the differential diagnosis of giant cellulitis-like Sweet syndrome. Therefore, biopsy of the skin lesion for histology, as well as tissue cultures, should be considered in individuals for whom this variant of Sweet syndrome is suspected.18,61-63
600
HISTOLOGIC DIFFERENTIAL DIAGNOSIS
HISTOLOGIC DIFFERENTIAL
DIAGNOSIS
The histologic differential diagnosis of Sweet syndrome includes conditions microscopically characterized by either neutrophilic dermatosis or neutrophilic panniculitis (Table 36-9). Because the pathologic changes associated with Sweet syndrome are similar to those observed in an abscess or cellulitis, culture of lesional tissue for bacteria, fungi, and mycobacteria should be considered to rule out infection. Leukemia cutis not only mimics the dermal changes of Sweet syndrome, but can potentially occur within the same skin lesion as Sweet syndrome; however, in contrast to the mature
■Abscess/cellulitis: Positive culture for infectious agent
■Abscess/cellulitis: Positive culture for infectious agent
■Arthropod bite reaction: History of exposure to arthropods
■Arthropod bite reaction: History of exposure to arthropods
■Bowel (intestinal) bypass syndrome: History of jejunal-ileal bypass surgery for morbid obesity
■Bowel (intestinal) bypass syndrome: History of jejunal-ileal bypass
surgery for morbid obesity
■Erythema elevatum diutinum: Erythematous asymptomatic plaques often located on the dorsal hands and elbows; younger lesions have microscopic features of leukocytoclastic vasculitis, whereas older lesions have dermal fibrosis and mucin
■Erythema elevatum diutinum: Erythematous asymptomatic
plaques often located on the dorsal hands and elbows; younger lesions have microscopic features of leukocytoclastic vasculitis, whereas older lesions have dermal fibrosis and mucin
■Granuloma faciale: Yellow-to-red-to-brown indurated asymptomatic facial plaques; there is a grenz zone of normal papillary dermis beneath which there is a dense diffuse inflammatory infiltrate of predominantly neutrophils (with microscopic features of leukocytoclastic vasculitis) and numerous eosinophils
■Granuloma faciale: Yellow-to-red-to-brown indurated asymptom-
atic facial plaques; there is a grenz zone of normal papillary dermis beneath which there is a dense diffuse inflammatory infiltrate of predominantly neutrophils (with microscopic features of leukocytoclastic vasculitis) and numerous eosinophils
■Halogenoderma: Neutrophilic dermal infiltrate with necrosis and pseudoepitheliomatous hyperplasia with intraepidermal abscesses; history of ingestion of bromides (leg lesions), iodides (facial lesions), or topical fluoride gel to teeth during tumor radiation therapy to face
■Halogenoderma: Neutrophilic dermal infiltrate with necrosis and
pseudoepitheliomatous hyperplasia with intraepidermal abscesses; history of ingestion of bromides (leg lesions), iodides (facial lesions), or topical fluoride gel to teeth during tumor radiation therapy to face
■Leukemia cutis: Dermal infiltrate consists of immature neutrophils
■Leukemia cutis: Dermal infiltrate consists of immature neutrophils
■Leukocytoclastic vasculitis: Vessel wall destruction—extravasated erythrocytes, fibrinoid necrosis of vessel walls, karyorrhexis, and neutrophils in the vessel wall
■Leukocytoclastic vasculitis: Vessel wall destruction—extravasated
erythrocytes, fibrinoid necrosis of vessel walls, karyorrhexis, and neutrophils in the vessel wall
■Lobular neutrophilic panniculitides: In addition to subcutaneous Sweet syndrome, these include α1-antitrypsin deficiency syndrome, factitial panniculitis (secondary to the presence of iatrogenic or self-induced foreign bodies), infectious panniculitis (secondary to either a bacterial, fungal, mycobacterial, or protozoan organism), pancreatic panniculitis, rheumatoid arthritis–associated panniculitis
■Lobular neutrophilic panniculitides: In addition to subcutaneous
Sweet syndrome, these include α1-antitrypsin deficiency syndrome, factitial panniculitis (secondary to the presence of iatrogenic or self-induced foreign bodies), infectious panniculitis (secondary to either a bacterial, fungal, mycobacterial, or protozoan organism), pancreatic panniculitis, rheumatoid arthritis–associated panniculitis
■Neutrophilic eccrine hidradenitis: Neutrophils around eccrine glands, often in patients with acute myelogenous leukemia receiving induction chemotherapy
■Neutrophilic eccrine hidradenitis: Neutrophils around eccrine
glands, often in patients with acute myelogenous leukemia receiving induction chemotherapy
■Neutrophilic urticarial dermatosis: An urticarial eruption demonstrating perivascular and interstitial neutrophilic infiltrate with intense leukocytoclasia, but without vasculitis and without dermal edema, that is often associated with a systemic disease such as Schnitzler syndrome, adult-onset Still disease, lupus erythematosus, and the hereditary autoinflammatory fever syndromes
■Neutrophilic urticarial dermatosis: An urticarial eruption demonstrat-
ing perivascular and interstitial neutrophilic infiltrate with intense leukocytoclasia, but without vasculitis and without dermal edema, that is often associated with a systemic disease such as Schnitzler syndrome, adult-onset Still disease, lupus erythematosus, and the hereditary autoinflammatory fever syndromes
■Pyoderma gangrenosum: Ulcer with overhanging, undermined violaceous edges
■Pyoderma gangrenosum: Ulcer with overhanging, undermined
violaceous edges
■Rheumatoid neutrophilic dermatitis: History of rheumatoid arthritis, nodules, and plaques
■Rheumatoid neutrophilic dermatitis: History of rheumatoid
arthritis, nodules, and plaques
Adapted from Cohen PR: Paraneoplastic dermatopathology: cutaneous paraneoplastic syndromes. Adv Dermatol. 1995;11:215-252.
polymorphonuclear neutrophils found in Sweet syndrome, the dermal infiltrate in leukemia cutis consists of malignant immature leukocytes.1,3,7
The pathologic changes in the adipose tissue of subcutaneous Sweet syndrome lesions can be found either in the lobules, the septae, or both. Therefore, conditions characterized by a neutrophilic lobular panniculitis also need to always be considered and ruled out.1,3
The pathologic differential diagnosis of histiocytoid Sweet syndrome includes leukemia cutis and other inflammatory dermatoses histopathologically characterized by histiocytes interstitially arranged between dermal collagen bundles such as interstitial type of granuloma annulare, interstitial granulomatous dermatitis with arthritis, and methotrexate-induced rheumatoid papules.18
Arthropod bite reaction has also mimicked the pathologic changes observed in Sweet syndrome. Unrelated to the use of medication, the presence of eosinophils in Sweet syndrome may range from rare to abundant. Although a dense inflammatory infiltrate of neutrophils is characteristic of Sweet syndrome, sites of arthropod bites with abundant eosinophils and some neutrophils may be misinterpreted as the dermatosis.16,64
CLINICAL COURSE AND PROGNOSIS
In some patients with classical Sweet syndrome, the symptoms and lesions of the dermatosis eventually resolved without any therapeutic intervention. However, the lesions may persist for weeks to months. Successful management of the cancer occasionally results
LINE MEDICATION DOSE
First
6
in clearing of the related dermatosis in patients with malignancy-associated Sweet syndrome. Similarly, spontaneous improvement and subsequent resolution of the syndrome typically follows discontinuation of the associated medication in patients with druginduced Sweet syndrome. In some of the patients who had associated tonsillitis, solid tumors, or renal failure, surgical intervention resulted in the resolution of Sweet syndrome.1,7,12,47
Following either spontaneous remission or therapyinduced clinical resolution, Sweet syndrome may recur. The duration of remission between recurrent episodes of the dermatosis is variable. In cancer patients, the reappearance of dermatosis-associated symptoms and lesions may represent a paraneoplastic syndrome that is signaling the return of the previously treated malignancy. Sweet syndrome recurrences are more common in this patient population.1,7,47
MANAGEMENT
MEDICATIONS
MEDICATIONS
FIRST-LINE TREATMENTS
The therapeutic mainstay for Sweet syndrome is systemic corticosteroids (Table 36-10). Improvement of the symptoms and resolution of the mucocutaneous lesions promptly results after initiation of therapy. In patients with refractory disease, daily pulse methylprednisolone administered intravenously may be necessary. For treating localized Sweet syndrome lesions, topical (such as 0.05% clobetasol propionate) or intralesional (such as triamcinolone acetonide at a dose
Prednisone 1 mg/kg/day (usually ranging from 30 mg-60 mg) as a single, oral, morning dose. Within 4-6 weeks, taper dose to 10 mg/day; however some patients may require 2-3 months of treatment or intravenous therapy.
Methylprednisolone sodium succinate Intravenously administered (up to 1000 mg/day) over 1 or more hours, daily for 3-5 days. This is followed by a tapering oral dose of corticosteroid or another immunosuppressant agent.
Potassium iodide Administered orally as 300 mg enteric-coated tablets, TID (for a daily dose of 900 mg) or as a saturated solution (1 g/mL of water) of potassium iodide (SSKI; also referred to as Lugol’s solution), beginning at a dose of 3 drops TID (9 drops/day = 450 mg/day) and increasing by 1 drop TID, typically to a final dose of 21 drops/day (1050 mg) to 30 drops/day (1500 mg).a
Colchicine Administered orally at a dose of 0.5 mg TID (for a daily dose of 1.5 mg).
Second
Indomethacin Administered at an oral daily dose of 150 mg for 7 days, and then 100 mg/day for 14 days.
Clofazimine Administered orally at a daily dose of 200 mg for 4 weeks, and then 100 mg/day for 4 weeks.
Cyclosporine Administered as monotherapy or as a second-line agent (after failure of first-line therapy or as a corticosteroidsparing agent). Initial oral daily dose ranges from 2 mg/kg/day to 4 mg/kg/day to 10 mg/kg/day.
Dapsone Administered as either monotherapy or in combination therapy. Initial oral dose ranges from 100 mg/day to
Dapsone Administered as either monotherapy or in combination therapy. Initial oral dose ranges from 100 mg/day to 200 mg/day; the latter dose is either administered as a single dose or divided into 2 equal doses.
200 mg/day; the latter dose is either administered as a single dose or divided into 2 equal doses.
aWhen a “standard” medicine dropper (which dispenses 20 drops per mL) is used, 1 drop = 0.05 mL (or 50 mg when the concentration of potassium iodide is 1000 mg/mL). From Cohen PR, Kurzrock R: Sweet’s syndrome revisited: a review of disease concepts. Int J Dermatol. 2003;42:761-778, with permission.
601
6
between 3.0 mg/cc and 10.0 mg/cc) corticosteroids may be effective.1,7,12,17,34
Other first-line systemic treatments for Sweet syndrome are potassium iodide and colchicine (see Table 36-10). Potential drug-induced side effects of potassium iodide include vasculitis and hypothyroidism. Gastrointestinal symptoms such as diarrhea, abdominal pain, nausea and vomiting are potential adverse effects from colchicine that may improve after lowering the daily dose of the drug.1,7,34
SECOND-LINE TREATMENTS
Indomethacin, clofazimine, cyclosporine, and dapsone are second-line systemic agents for Sweet syndrome (see Table 36-10). They have all been used as monotherapy after first-line therapies have failed or in the initial management of the patient. In addition, either as a corticosteroid-sparing agent or with other drugs, cyclosporine and dapsone have been used in combination therapy.1,7,34
ANTIBIOTICS
In some patients, Sweet syndrome lesions have improved after receiving systemic antibiotics. These patients not only include individuals with Staphylococcus aureus secondarily impetiginized lesions treated with an antimicrobial agent to which their bacterial strain is susceptible and patients with inflammatory bowel disease treated with metronidazole, but also persons with dermatosis-related Yersinia or Chlamydia infection treated with either doxycycline, minocycline, or tetracycline.1,7,34
OTHER AGENTS
In addition, predominantly in case reports, effective treatment of Sweet syndrome also has been described with other drugs, such as antineoplastic therapies (azacitidine, chlorambucil, cyclophosphamide, and rituximab), danazol, etretinate, hepatitis therapy, immunoglobulin, IFN-α, and tumor necrosis factors antagonists (adalimumab, etanercept, infliximab, and thalidomide).7,34,51,65,66 Anakinra (an IL-1 receptor antagonist) in combination with oral prednisone was promptly effective in resolving the symptoms, and subsequently the clinical lesions, of Sweet syndrome in a patient with longstanding disease that was refractory to other therapies; it also resulted in dramatic clinical and biologic improvement in a 66-year-old man who had a 5-year history of Sweet syndrome that was refractory to various conventional treatments.67,68
Pentoxifylline was hypothesized to be beneficial for treating Sweet syndrome; however, when used as monotherapy, it was not found to be efficacious.2 Some of the drugs used for the treatment of Sweet syndrome, such as azacitidine, minocycline, and the tumor necrosis factor-inhibitors adalimumab, etanercept, infliximab, and lenalidomide, also have been observed to elicit the condition.1,7,34,55
602
MALIGNANCY WORKUP
MALIGNANCY WORKUP
In 1993, Cohen and Kurzrock proposed recommendations for the initial malignancy workup in newly diagnosed Sweet syndrome patients without a prior cancer. Their recommendations were based on the neoplasms that had concurrently been present or subsequently developed in previously cancer-free Sweet syndrome patients and the age-related recommendations of the American Cancer Society for early detection of cancer in asymptomatic persons. The recommendations included: (a) a detailed medical history; (b) a complete physical examination, including: (i) examination of the thyroid, lymph nodes, oral cavity, and skin; (ii) digital rectal examination; (iii) breast, ovary, and pelvic examination in women; and (iv) prostate and testicle examination in men; (c) laboratory evaluation: (i) carcinoembryonic antigen level; (ii) complete blood cell count with leukocyte differential and platelet count; (iii) pap test in women; (iv) serum chemistries; (v) stool guaiac slide test; (vi) urinalysis; and (vii) urine culture; and (d) other screening tests: (i) chest roentgenograms; (ii) endometrial tissue sampling in either menopausal women or women with a history of abnormal uterine bleeding, estrogen therapy, failure to ovulate, infertility, or obesity; and (iii) sigmoidoscopy in patients older than 50 years of age. Cohen and Kurzrock also suggested that it was reasonable to check a complete blood cell count with leukocyte differential and platelet count every 6 to 12 months as the initial appearance of dermatosis-related skin lesions had been reported to precede the diagnosis of a Sweet syndrome–associated hematologic malignancy by as long as 11 years.1,47

Figure 36-1 Unilateral lesions of Sweet syndrome around the eye and upper lip consisting of plaques and pseudovesicular papules suggesting herpes simplex.

Figure 36-2 Multiple confluent papules and plaques of Sweet syndrome that at first sight give the illusion of vesiculation but are solid on palpation. (From Hönigsmann H, Kempter R, Wolff K. Acute febrile neurophilic dermatosis [Sweet’s syndrome]—report of two cases [author’s transl] [in German]. Wien Klin Wochenschr. 1979;91(24):842-847, with permission.)
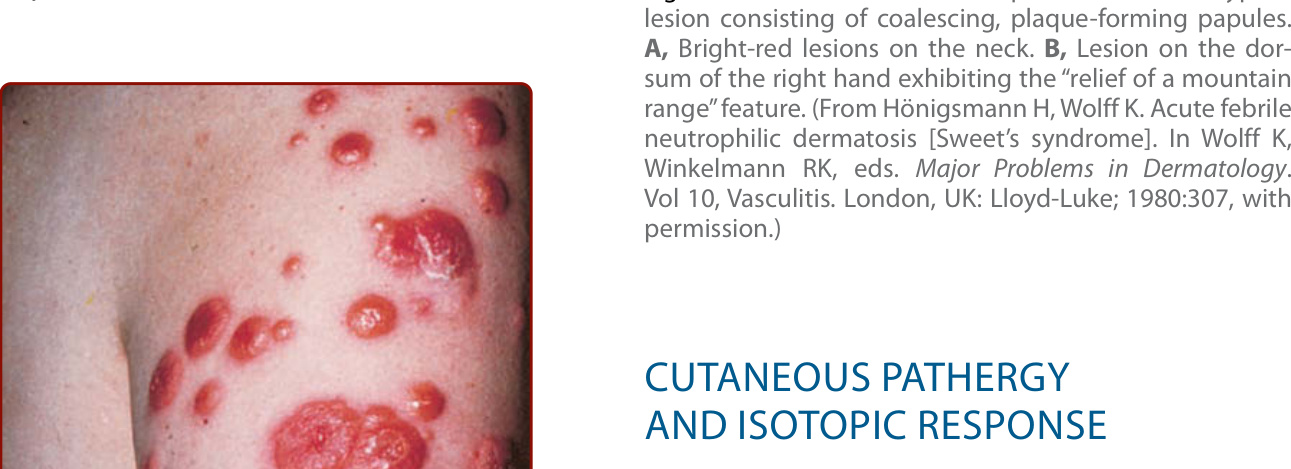
Figure 36-3 Acute febrile neutrophilic dermatosis. Typical lesion consisting of coalescing, plaque-forming papules. A, Bright-red lesions on the neck. B, Lesion on the dorsum of the right hand exhibiting the “relief of a mountain range” feature. (From Hönigsmann H, Wolff K. Acute febrile neutrophilic dermatosis [Sweet’s syndrome]. In Wolff K, Winkelmann RK, eds. Major Problems in Dermatology. Vol 10, Vasculitis. London, UK: Lloyd-Luke; 1980:307, with permission.)

Figure 36-4 Histiocytoid giant cellulitis Sweet syndrome presenting as an erythematous plaque on the left lateral thigh of a 72-year-old woman who had an unclassified myelodysplastic syndrome/myeloproliferative disorder. (From So JK, Carlos CA, Frucht CS, et al. Histiocytoid giant cellulitis-like Sweet’s syndrome: case report and review of the literature. Dermatol Online J. 2015;21(3):4, with permission.)

Figure 36-5 Distant (A) and closer (B and C) views of the left (B) and right (C) palms of an 86-year-old woman with proton pump inhibitor–induced Sweet syndrome. The painful erythematous-based pustules and pseudovesicular violaceous plaques on her hands appeared within 6 hours after she took an initial dose of esomeprazole. Previously, she had developed similar hand lesions on day 8 of omeprazole, which resolved after a short course of oral prednisone. (From Cohen PR. Proton pump inhibitor-induced Sweet’s syndrome: report of acute febrile neutrophilic dermatosis in a woman with recurrent breast cancer. Dermatol Pract Concept. 2015;5:113-119, published under a Creative Commons Attribution License [http://creativecommons.org/licenses/by-nc/3.0/], with permission.)
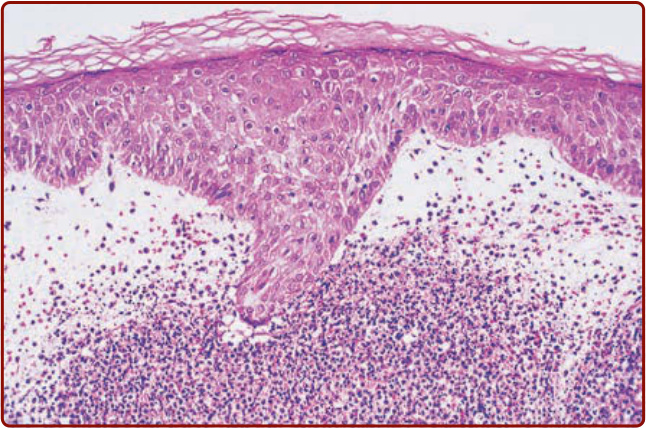
Figure 36-6 Histopathologic presentation of acute febrile neutrophilic dermatosis (Sweet syndrome) demonstrates massive edema of the papillary dermis and a dense diffuse infiltrate of mature neutrophils throughout the upper dermis (hematoxylin and eosin stain). (From Cohen PR, Holder WR, Tucker SB, et al. Sweet’s syndrome in patients with solid tumors. Cancer. 1993;72:2723-2731, with permission. Copyright © 2006 John Wiley & Sons.)
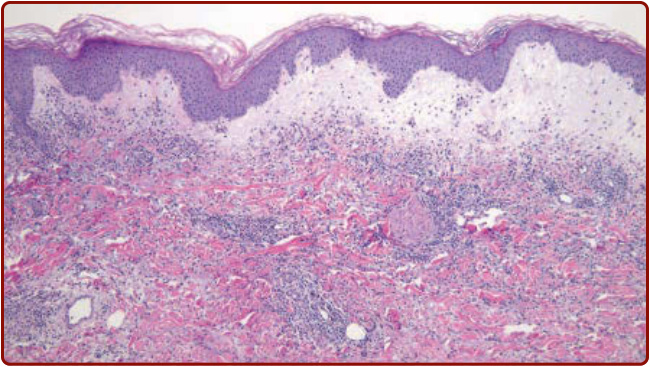
Figure 36-7 An intermediate magnification view of the histopathologic presentation of histiocytoid giant cellulitis Sweet syndrome shows prominent superficial dermal edema with a perivascular and interstitial inflammatory dermal infiltrate consisting of histiocytoid and immature granulocytic cells admixed with lymphocytes, eosinophils, and occasional neutrophils. (From So JK, Carlos CA, Frucht CS, et al. Histiocytoid giant cellulitis-like Sweet’s syndrome: case report and review of the literature. Dermatol Online J. 2015;21(3):4, with permission.)
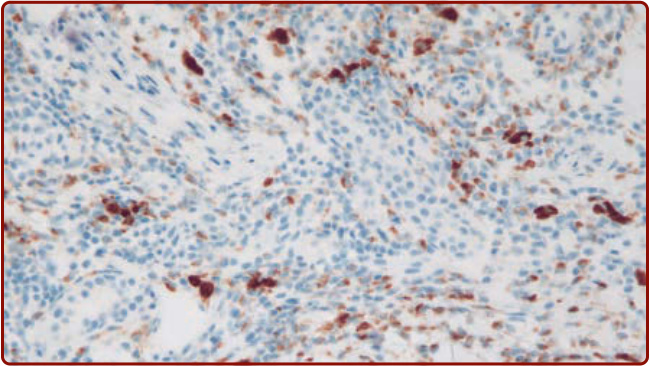
Figure 36-8 A high magnification view of the immunoperoxidase staining of the skin biopsy from the histiocytoid giant cellulitis Sweet syndrome shows positive staining of the CD68 (a histiocyte marker) cells comprising the dermal infiltrate. (From So JK, Carlos CA, Frucht CS, et al. Histiocytoid giant cellulitis-like Sweet’s syndrome: case report and review of the literature. Dermatol Online J. 2015;21(3):4, with permission.)
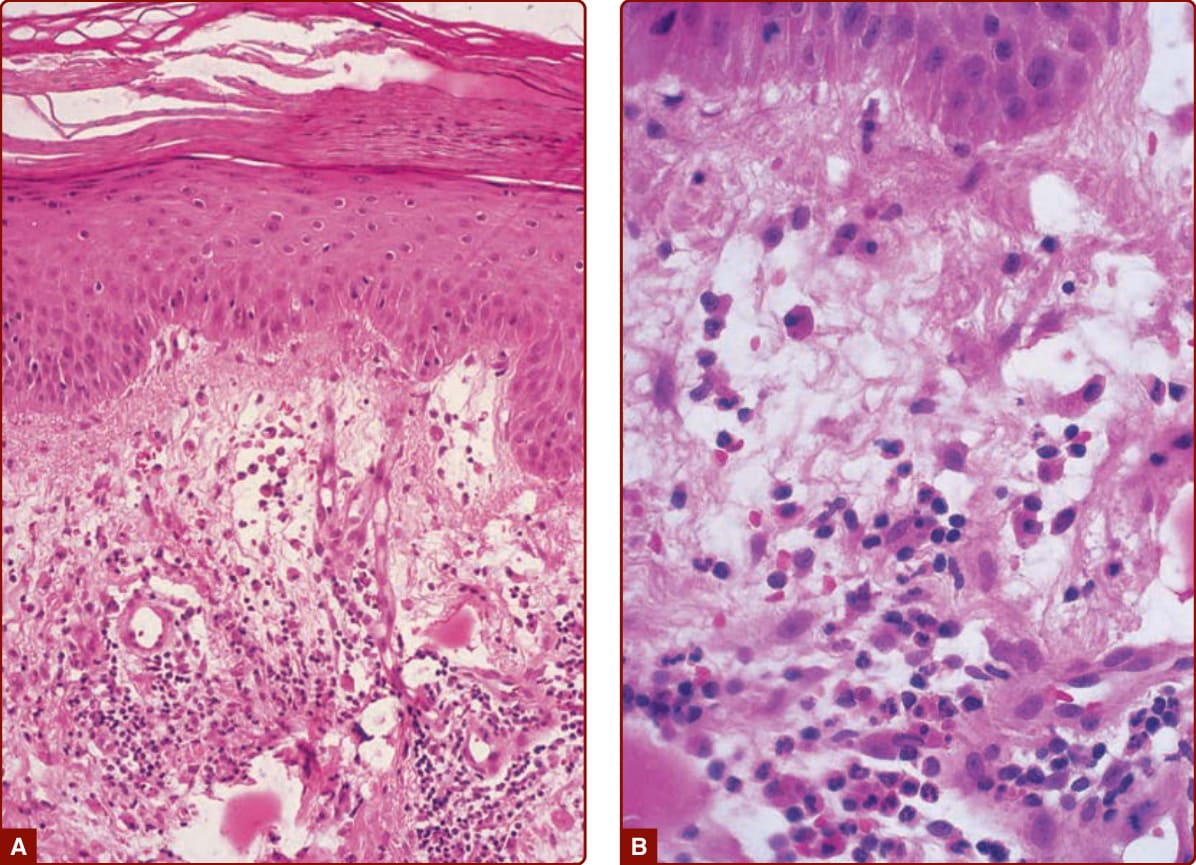
Figure 36-9 Characteristic histopathologic features of Sweet syndrome are observed at low (A) and high (B) magnification: papillary dermal edema, swollen endothelial cells, and a diffuse infiltrate of predominantly neutrophils with leukocytoclasia, yet no evidence of vasculitis (hematoxylin and eosin stain). (From Cohen PR, Holder WR, Rapini RP. Concurrent Sweet’s syndrome and erythema nodosum: a report, world literature review and mechanism of pathogenesis. J Rheumatol. 1992;19:814-820, with permission.)
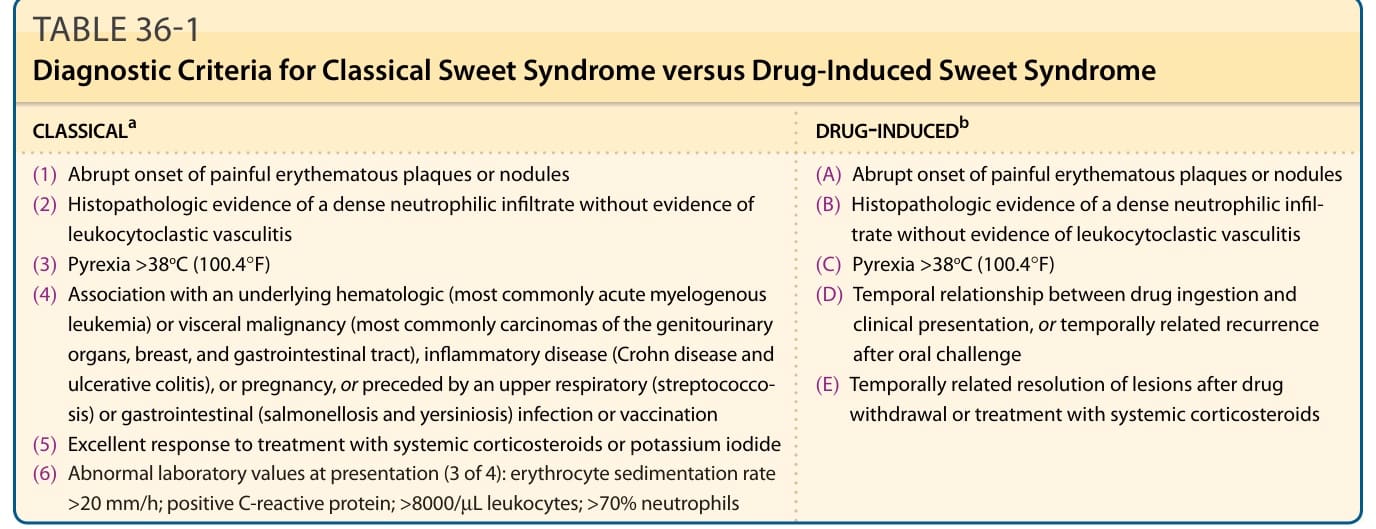
TABLE 36-1 Diagnostic Criteria for Classical Sweet Syndrome versus Drug-Induced Sweet Syndrome
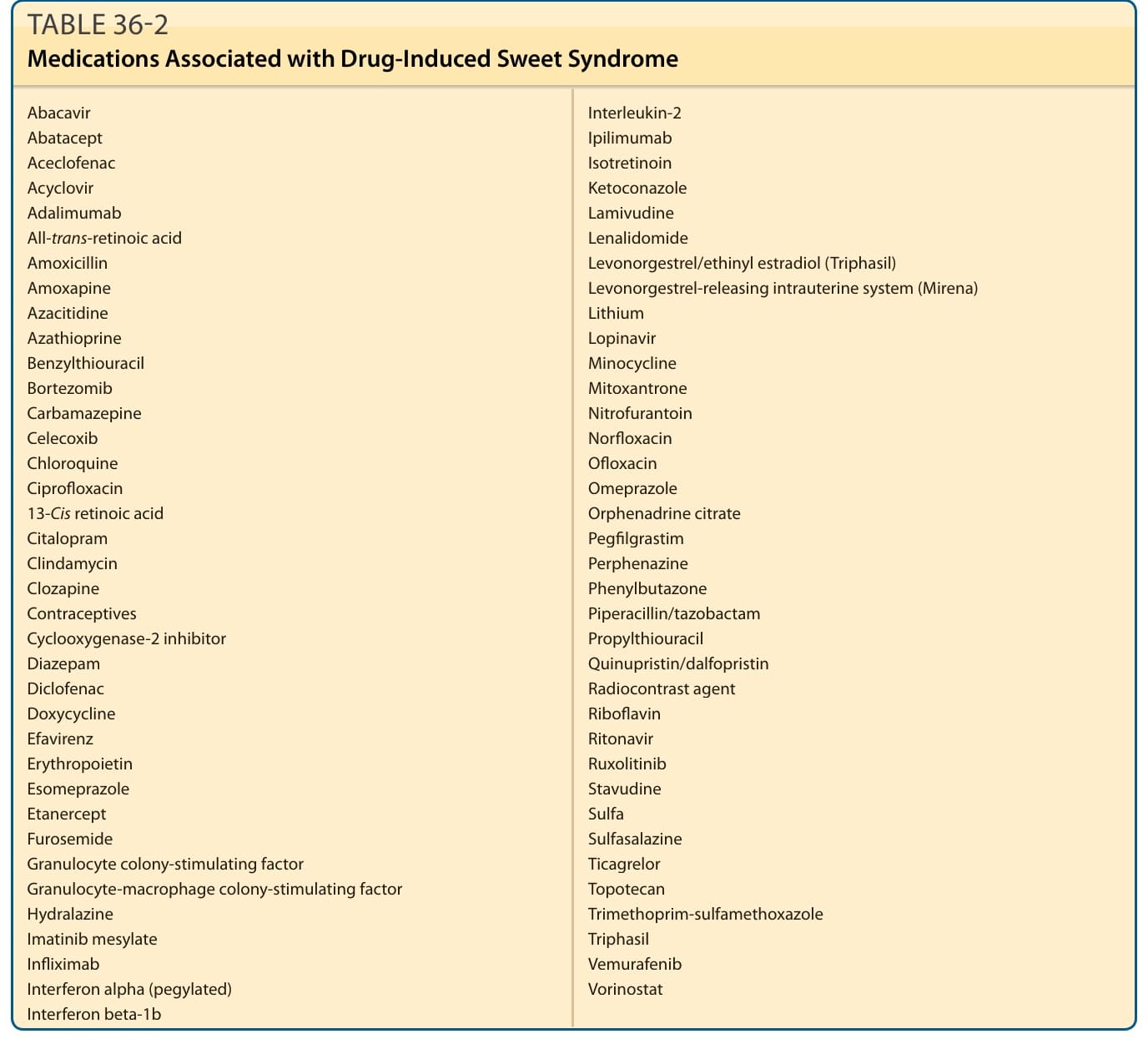
TABLE 36-2
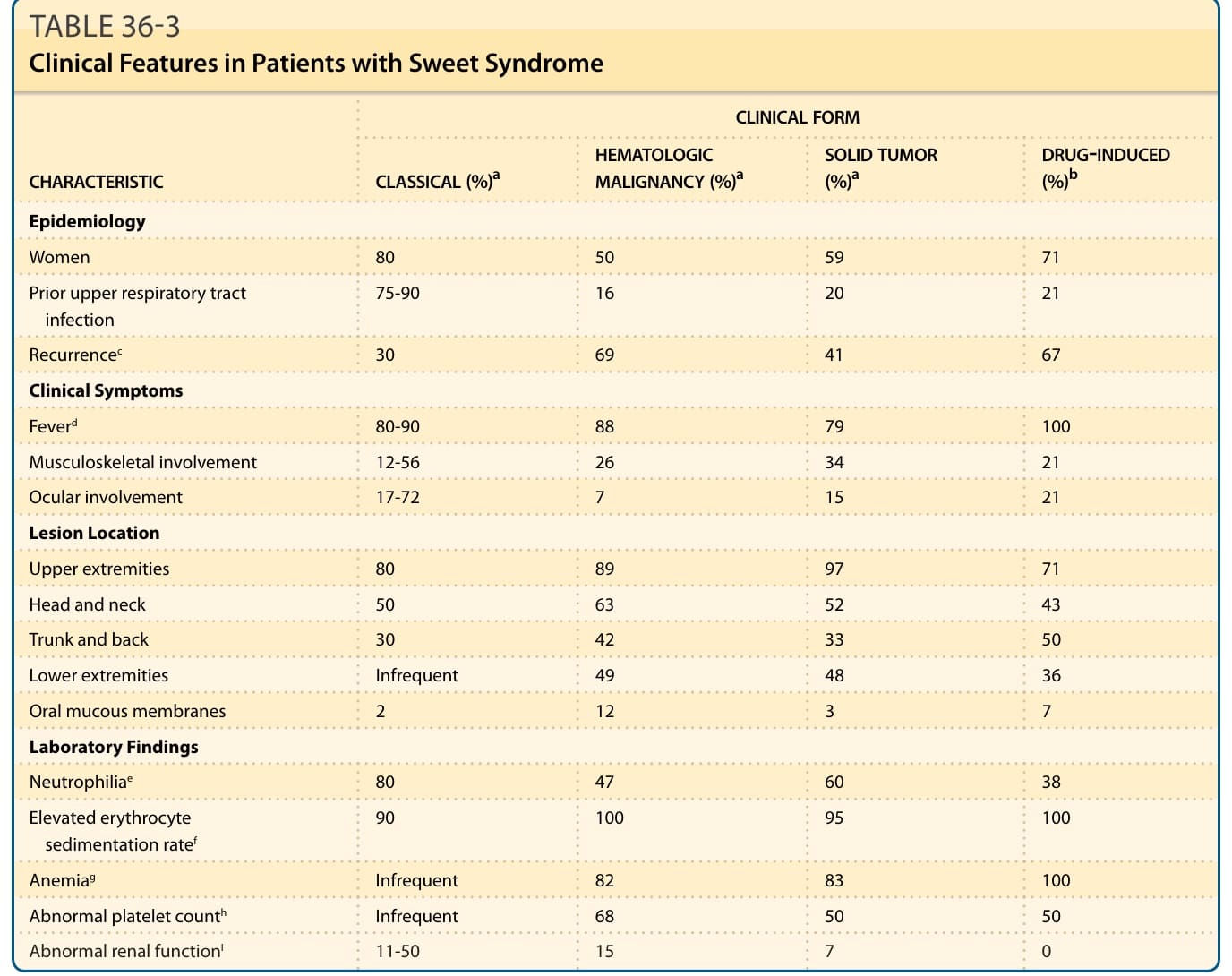
TABLE 36-3 Clinical Features in Patients with Sweet Syndrome
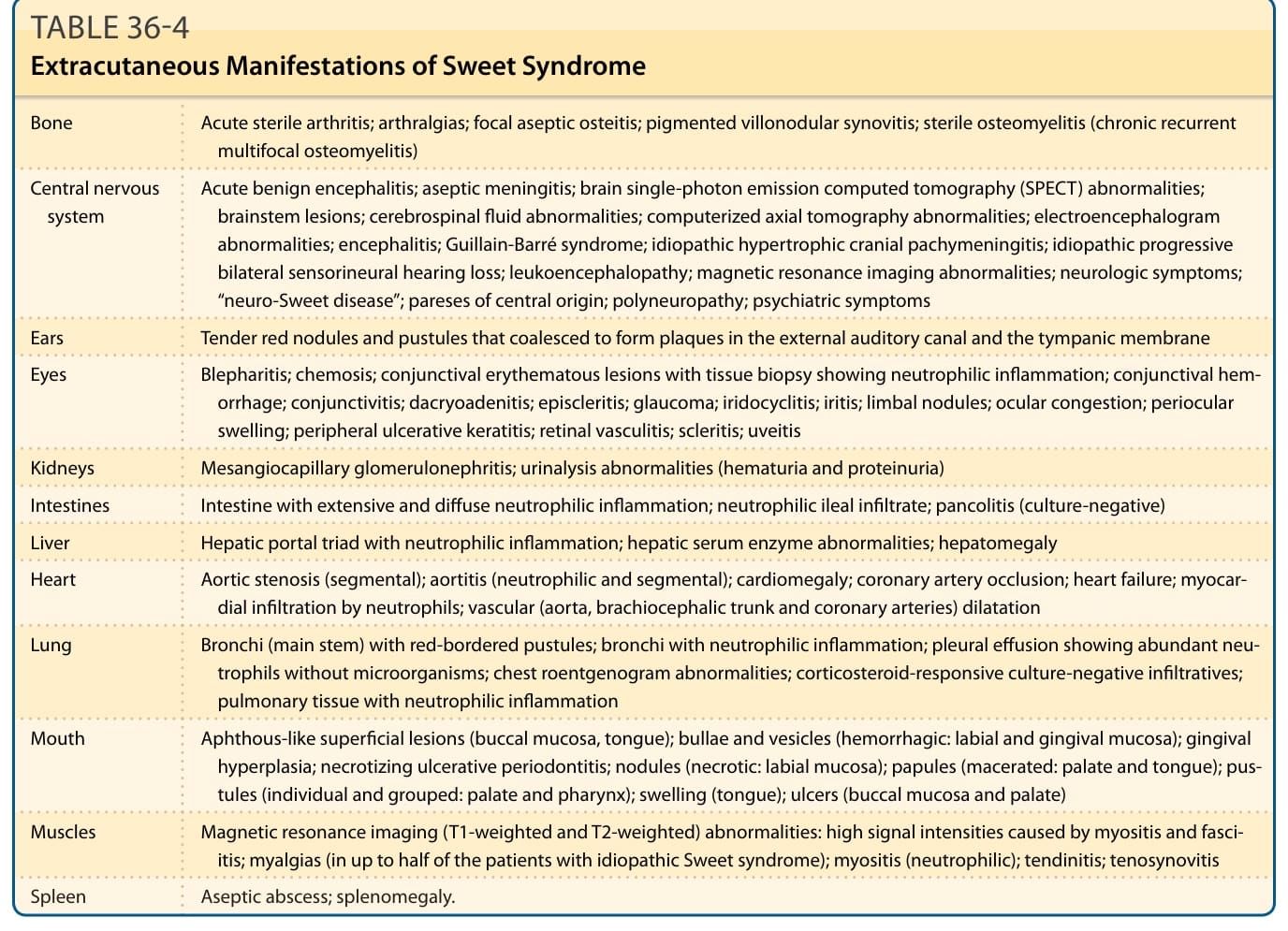
TABLE 36-4 Extracutaneous Manifestations of Sweet Syndrome
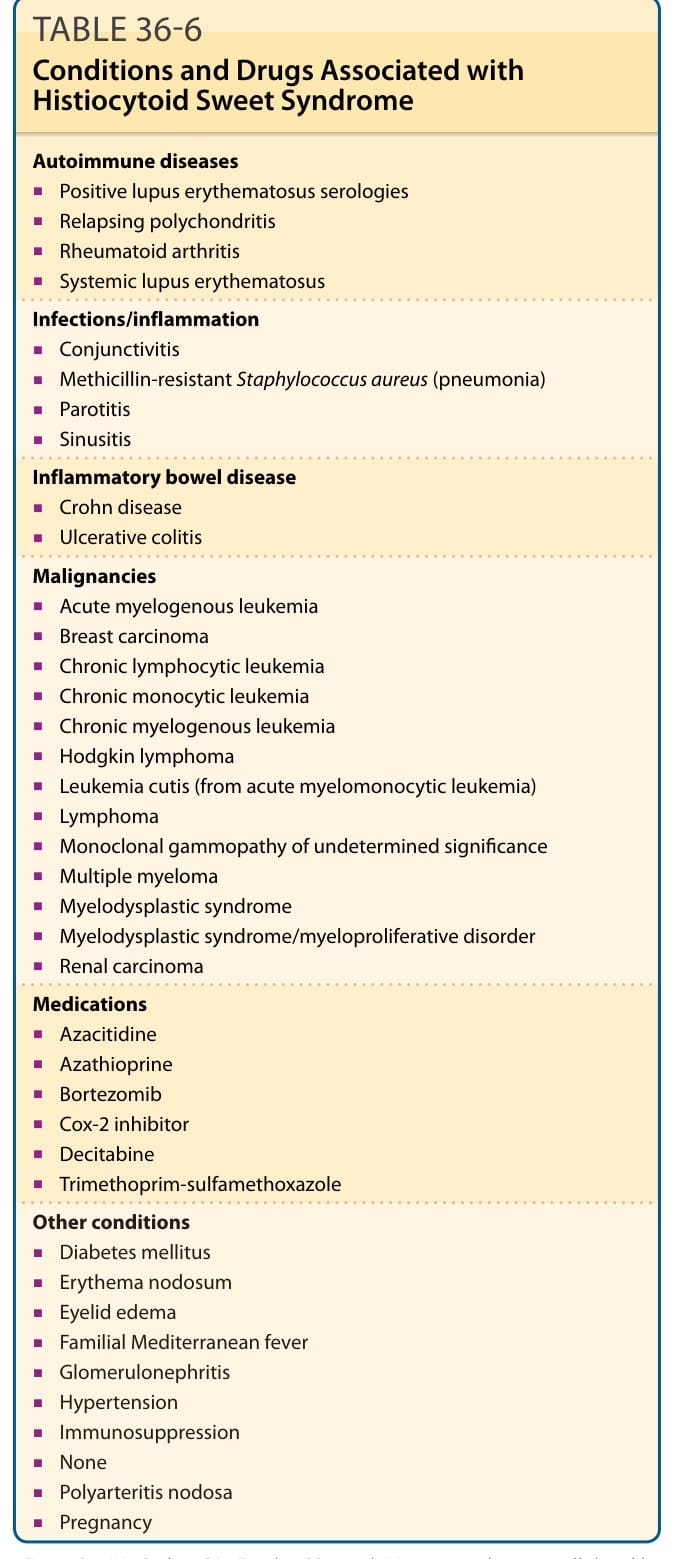
TABLE 36-6 Conditions and Drugs Associated with Histiocytoid Sweet Syndrome
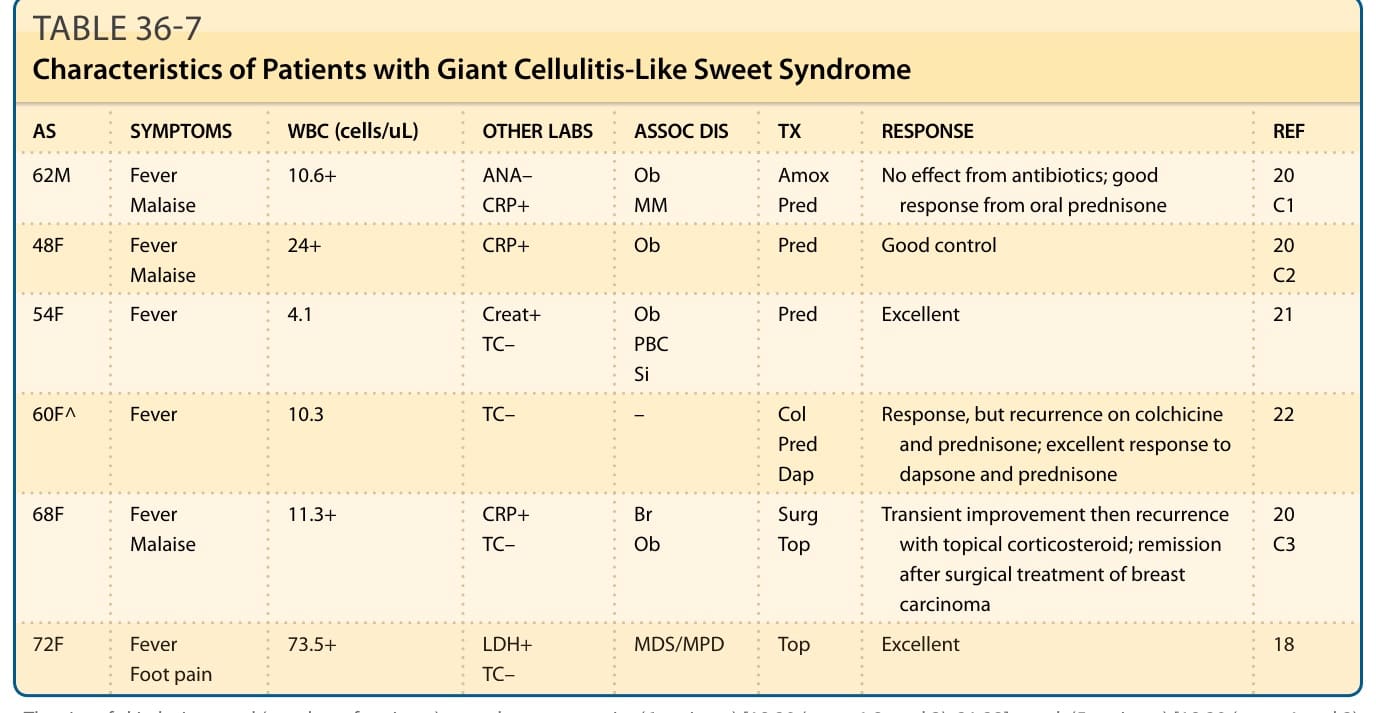
TABLE 36-7 Characteristics of Patients with Giant Cellulitis-Like Sweet Syndrome
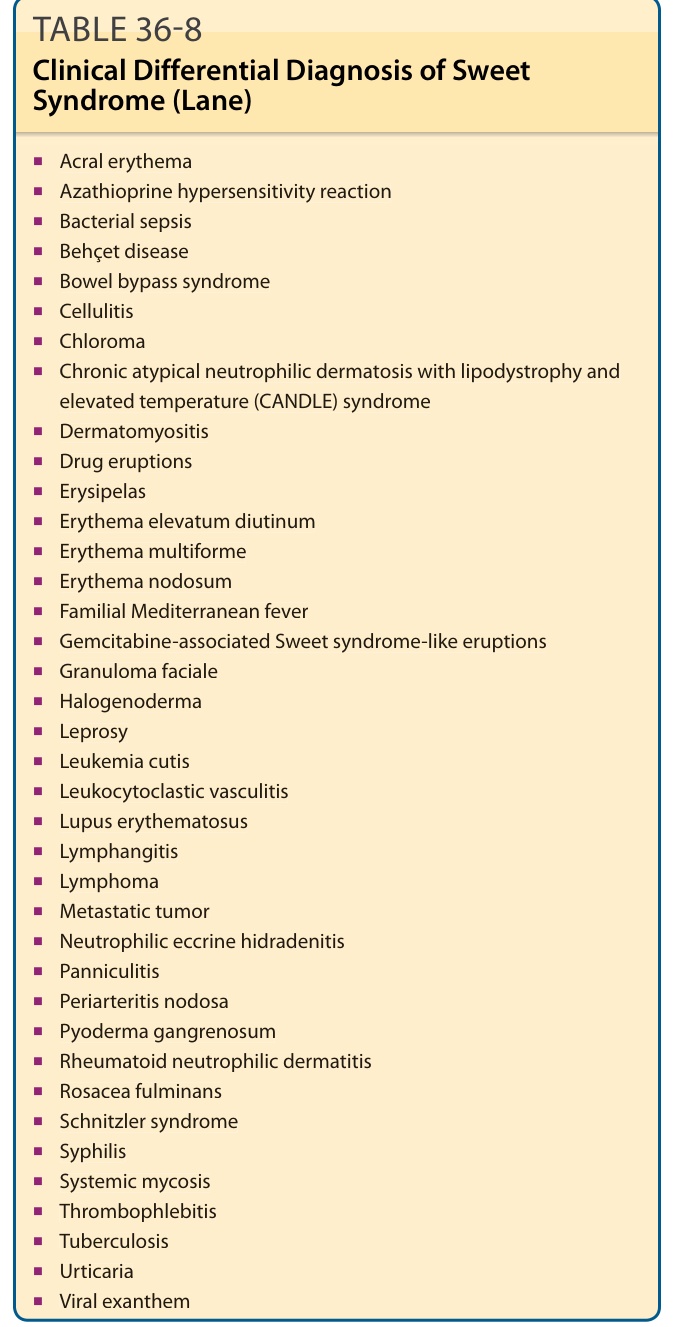
TABLE 36-8 Clinical Differential Diagnosis of Sweet Syndrome (Lane)
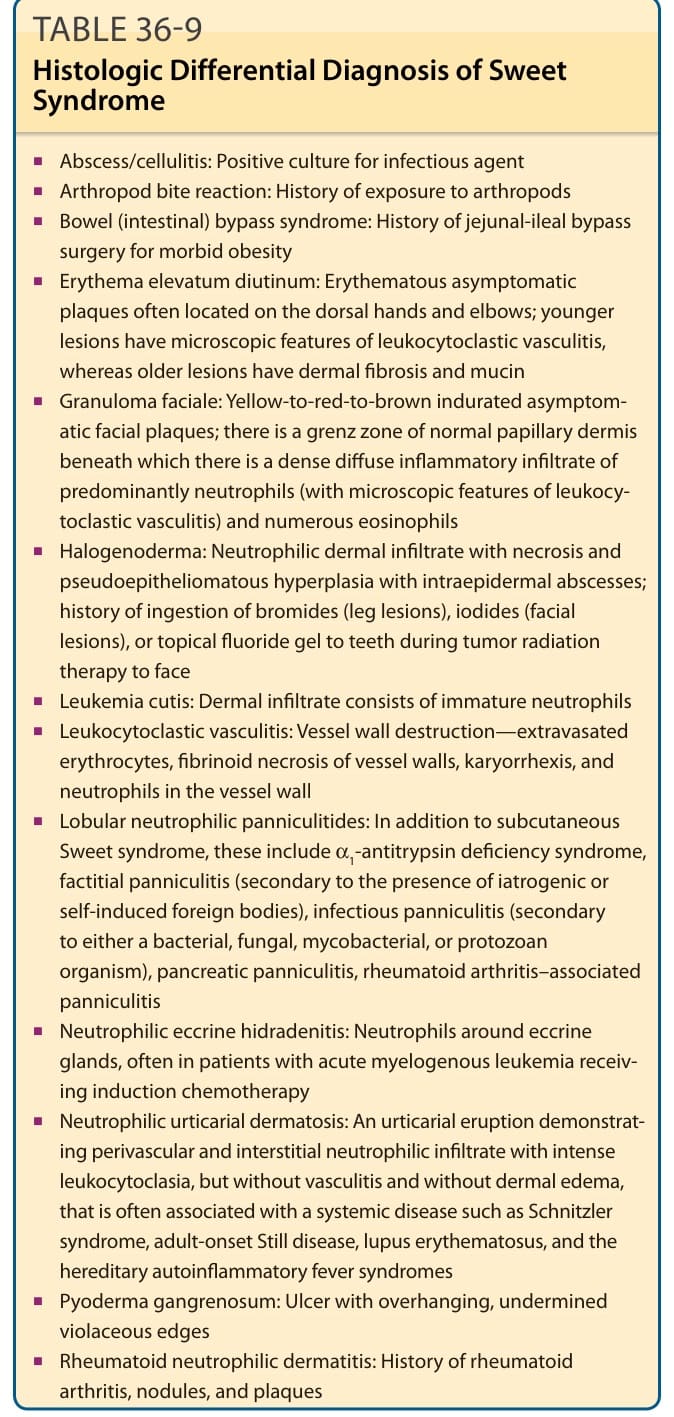
TABLE 36-9 Histologic Differential Diagnosis of Sweet Syndrome
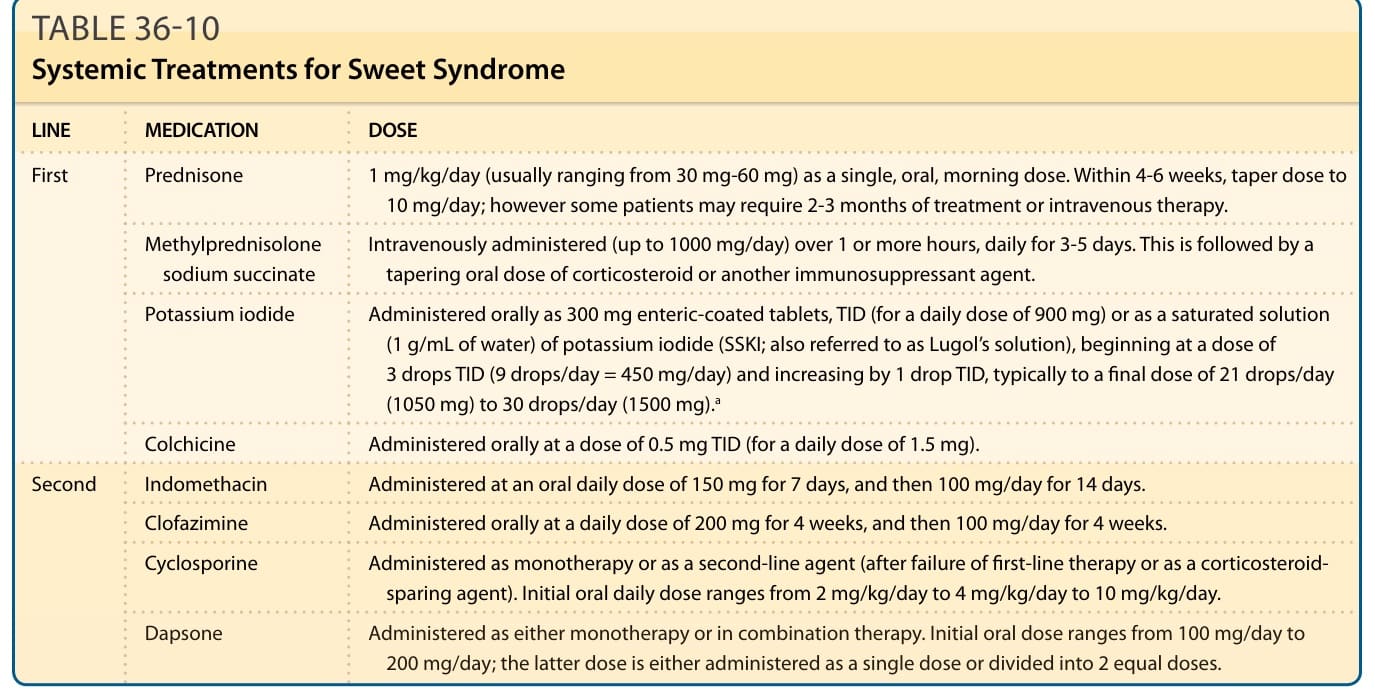
TABLE 36-10 Systemic Treatments for Sweet Syndrome