Sarcoidosis
5
AT-A-GLANCE
■ Sarcoidosis is a multisystem disease characterized by granulomatous inflammation of unknown etiology commonly occurring in the lung and the skin, but any organ system can be affected.
■ The type of cutaneous lesion may suggest prognosis. Lupus pernio lesions are associated with chronic disease course and scarring. Erythema nodosum lesions portend an acute self-resolving course.
■ Specific lesions of sarcoidosis have a varied clinical morphology, including macules, papules, plaques, nodules, and ulcerations.
■ Topical, systemic, and intralesional corticosteroids are the mainstay of therapy.
■ Patients initially diagnosed with cutaneous sarcoidosis should get baseline testing to look for deleterious systemic disease, including a physical examination; neurologic review of systems; a chest radiograph; an electrocardiogram; pulmonary function tests; urine analysis; complete blood count; comprehensive metabolic panel; serum calcium level; tuberculosis screening; and an ophthalmologic examination.
Sarcoidosis is a multisystem disease characterized by granulomatous inflammation. It is theorized to be a disease of hyperactivation of the immune system, but its etiology is unknown.
HISTORICAL PERSPECTIVE
Although the lungs are the organs most commonly afflicted, sarcoidosis was actually first described in the late 1800s because of its skin manifestations. Boeck reported a case of “multiple benign sarkoid of the skin” as he believed the skin lesions resembled sarcomas but were benign.1
EPIDEMIOLOGY
Sarcoidosis occurs worldwide and may affect all ages and races. Disease onset is most common in the third decade of life and is slightly higher in women.2 Sarcoidosis has a higher incidence with greater distance from the equator. The highest prevalence of sarcoidosis is found in whites in Denmark and Sweden, and in persons of African descent in the United States.3 In the United States, the lifetime risk of sarcoidosis is 2.4%
in African Americans and 0.85% in whites.3 The incidence rate of sarcoidosis in the United States is 17.8 per 100,000 for African Americans and 8.1 per 100,000 for whites; the prevalence rate is 141.8 per 100,000 for African Americans and 49.8 per 100,000 for white individuals.4 The highest prevalence is in African American women (178.5 per 100,000).4 African Americans tend to have more severe symptomatic disease. African Americans are more likely to have extrapulmonary disease,5 require treatment,6 and have a lower rate of clinical recovery7,8 than whites.
CLINICAL FEATURES
CUTANEOUS FINDINGS
CUTANEOUS FINDINGS
With the advent of penicillin, sarcoidosis has replaced syphilis as the great mimicker for dermatologists. The diverse variety of cutaneous sarcoidosis is bewildering. Almost all primary morphologies have been reported, including macules, papules, patches, plaques, and nodules. Alopecia occurs with scalp involvement and nail changes also occur. Epidermal changes of scaling, telangiectasia, and atrophy exist. Cutaneous lesions of sarcoidosis may occur before, coincident with, or after systemic involvement. Classically, lesions are divided into two categories: specific and nonspecific. Specific lesions have granulomatous inflammation histologically similar to the pattern seen in sarcoid lesions in other organs. Nonspecific skin findings are reactive and do not exhibit sarcoidal granulomas.
SPECIFIC CUTANEOUS LESIONS
Despite the diversity in appearance, there are several clinical presentations of specific lesions that are typical of cutaneous sarcoidosis.
Papules and Plaques: The most common presentation is the papular form (Figs. 35-1 and 35-2). These firm 1- to 5-mm papules often have a translucent red-brown or yellow-brown color. The yellowbrown coloration as reminiscent of “apple jelly” and is accentuated with the pressing of a glass slide to the skin (diascopy) (Fig. 35-3). In addition to the color change, the granulomatous lesions have a nodular quality that is appreciated with diascopy. The apple jelly appearance and nodules is not pathognomonic for sarcoidosis, as other granulomatous skin conditions,
CLINICAL MANIFESTATIONS
Lupus pernio Symmetric, violaceous, indurated plaques and nodules on nose, earlobes, cheeks, and digits
Mikulicz syndrome Sarcoidal granulomas on mucosal surface and tongue, with bilateral enlargement of the lacrimal, parotid, sublingual, and submandibular glands
Darier-Roussy sarcoid Presents as persistent subcutaneous nodules that may be tender or painless; occurs on extremities
Lofgren syndrome Erythema nodosum with bilateral hilar adenopathy, arthralgia, and fever; often the presenting manifestation of sarcoidosis
Heerfordt
Fever, parotid gland enlargement, facial palsy, and
Heerfordt syndrome Fever, parotid gland enlargement, facial palsy, and anterior uveitis
syndrome
anterior uveitis
including lupus vulgaris and granuloma annulare, may exhibit similar diascopic properties. However, dermoscopy may prove useful in distinguishing the cutaneous granulomas of sarcoidosis from necrobiotic granulomas. Even after therapy, dermoscopic findings of pink homogenous background, translucent orange areas, fine white scaling, and scar-like depigmentation are significantly associated with cutaneous sarcoidosis compared to necrobiosis lipoidica, granuloma annulare, and rheumatoid nodules.9
Epidermal changes may or may not be present (Figs. 35-4 and 35-5), but the lesions often have a waxy appearance, which reflects mild epidermal atrophy. Papular lesions occur most commonly on the face and neck, with a predilection for periorbital skin. Typically the papular lesions are asymptomatic without pain or pruritus; the most common complaint is cosmetic disfigurement. Plaques, both annular and nonannular, and nodules may develop from papular lesions and may retain the translucent yellow-brown coloration (Fig. 35-6).
Lupus Pernio: Lupus pernio describes the relatively symmetric, violaceous, indurated plaques and nodules occurring on the nose, earlobes, cheeks, and digits (Figs. 35-7 and 35-8). The name lupus pernio is a
5
misnomer preserved from the erroneous notion that these lesions might be related to lupus vulgaris and cold injury when lupus pernio was first described by Besnier in the 19th century. This distinctive clinical variant is associated with a higher incidence of systemic involvement and upper respiratory tract disease.10 Lupus pernio lesions may directly extend into the nasal sinus, leading to epistaxis, nasal crusting, and sine bone involvement. Angiolupoid lesions are pink and violaceous papules and plaques with prominent telangiectasias that usually occur on the face; they are often considered a variant of lupus pernio.
Scar Sarcoid: Cutaneous sarcoidosis occurs preferentially within scar tissue, at traumatized skin sites, and around embedded foreign material such as silica and tattoo ink (Fig. 35-9). Scars become inflamed and infiltrated with sarcoidal granulomas. Inflammation of old scars may precede or parallel systemic disease activity. Infiltrated scars may be tender or pruritic and the only finding of a patient with significant systemic involvement. The presence of sarcoidal granulomas surrounding foreign material does not establish the diagnosis of sarcoidosis, nor does foreign material in the presence of granulomas exclude the diagnosis.
573
5
Subcutaneous Nodules (Darier-Roussy Sarcoid): Rarely, sarcoidosis can present as persistent subcutaneous nodules (Darier-Roussy sarcoid).11
The nodules may be tender or painless, and preferentially occur on the extremities.
Hypopigmented Areas: Lesions appearing to be hypopigmented macules occur primarily in darkly pigmented persons (Fig. 35-10). However, upon careful palpation, induration can usually be appreciated in the areas that have granulomatous inflammation histologically. Some hypopigmented truly macular areas likely reflect postinflammatory pigment alteration as well.
Alopecia: Alopecia, both scarring and nonscarring, may occur with cutaneous lesions on hair-bearing skin such as the face and scalp. Annular plaques may have alopecia centrally. The reversibility is dependent on the degree of fibrosis and destruction of the hair follicle.
Nail Findings: Nail plate deformation and discoloration occur rarely including clubbing, subungual hyperkeratosis, and nail plate destruction. Granulomas in the nail matrix or adjacent bone lead to nail changes.
574
Mucous Membranes: Sarcoidal granulomas may cause papules and plaques of the mucosal surface and tongue. Infiltration of the gingiva causing “strawberry gums” mimicking Wegner granulomatosis may occur. Sarcoidosis is one cause of Mikulicz syndrome, the bilateral enlargement of the lacrimal, parotid, sublingual, and submandibular glands.
Additional Cutaneous Findings: A myriad of additional clinical presentations have also been reported. These include ichthyosis,12 erythroderma,13
ulcerations14 (Fig. 35-11), morphea-form plaques,15
lichen nitidus-like papules,16 folliculitis-like lesions,17
psoriasiform plaques,18 gyrate erythema,19 verrucous lesions,17 faint erythema, genital lesions,20,21
palmar erythema,22 discoid lupus-like plaques,23 lowerextremity edema,24 lesions mimicking tuberculoid leprosy, areas mimicking polymorphous light eruptions,17
and pustular lesions.17
NONSPECIFIC CUTANEOUS LESIONS
Erythema nodosum is the main nonspecific cutaneous manifestation of sarcoidosis. Erythema nodosum with bilateral hilar adenopathy, arthralgia, and
5
fever is frequently the initial manifestation of sarcoidosis (Lofgren syndrome). These patients tend to have an acute form of sarcoidosis with eventual resolution. Other nonspecific cutaneous manifestations of sarcoidosis are much less common. The neutrophilic dermatoses, Sweet disease and pyoderma gangrenosum, have been reported. Most patients with pyoderma gangrenosum have concomitant erythema nodosum.25 Nonspecific erythematous eruptions resembling viral exanthems or drug reaction without histologic evidence of granulomas occur very rarely with acute sarcoidosis. Additionally, patients with sarcoidosis may have pruritus without granulomatous inflammation leading to prurigo nodules.26 Erythema multiforme had been regularly cited as a nonspecific cutaneous manifestation of sarcoidosis,17 but reports of histologically proven erythema multiforme with interface dermatitis are virtually nonexistent in the literature,27,28 and any association is more likely coincidental. Erythroderma and nonspecific lower-extremity edema have been described as both specific and nonspecific lesions of sarcoidosis.24,26,29,30
NONCUTANEOUS FINDINGS
NONCUTANEOUS FINDINGS
Sarcoidosis is a multisystemic disease by definition and essentially all organ systems can be involved. However, symptoms are often lacking and diagnosis of systemic involvement is commonly found incidentally on routine testing, such as a chest radiograph.
PULMONARY SARCOIDOSIS
The lung is the most common organ involved with sarcoidosis. Findings on pulmonary examination are usually absent, and patients are usually asymptomatic. Dyspnea, cough, chest pain, hypoxemia, and wheezing may occur. Sarcoid lesions directly infiltrate the parenchyma of the lungs, which can lead to
575
5
pulmonary fibrosis. Fibrotic disease can lead to pulmonary hypertension and chronic Aspergillus infection. Additionally, lesions distort the airways and cause an obstructive lung disease. Pulmonary function tests are more likely to be abnormal when chest radiographs reveal abnormal lung parenchyma, but also may be abnormal without parenchymal findings.
OCULAR SARCOIDOSIS
The eyes are involved in at least 25% of sarcoidosis patients and involvement can be vision threatening.31
Patients may initially be asymptomatic warranting routine ophthalmologic examination.32 Redness, burning, itching, and dryness are the most common symptoms when present. Any portion of the eye may be involved with uveitis being most common. Lacrimal gland enlargement may occur (Fig. 35-12). Uveitis can lead to glaucoma and cataracts. Other manifestations include conjunctivitis, lacrimal gland involvement leading to keratoconjunctivitis sicca (dry eyes), and optic neuritis. Optic neuritis may rapidly lead to vision loss. Heerfordt syndrome, which includes fever, parotid gland enlargement, facial palsy, and anterior uveitis, is a classic presentation of sarcoidosis.2
576
CARDIAC SARCOIDOSIS
Clinical evidence of cardiac involvement is found in only 5% of sarcoidosis patients, but myocardial granulomas have been found in approximately 25% of patients at time of autopsy.33 Most clinical problems are related to cardiac arrhythmias or left ventricular dysfunction.34 Sudden death may occur. Congestive heart failure may result when the myocardium is massively infiltrated with granulomas. An electrocardiogram is recommended for every patient diagnosed with sarcoidosis.
NEUROSARCOIDOSIS
Any portion of the central or peripheral nervous system may be affected. Neurosarcoidosis has a predilection for the base of the brain, and cranial neuropathies are the most common manifestation.35 The facial nerve is the most frequently involved. Mass lesions may develop in the brain or spinal cord. Aseptic meningitis and peripheral neuropathy can occur.
RENAL SARCOIDOSIS
The kidneys may be affected by direct granulomatous inflammation or by nephrolithiasis resulting from hypercalcemia. Activated sarcoidal macrophages have increased 1α-hydroxylase activity. This converts 25-hydroxyvitamin D to 1,25-dihydroxyvitamin D, the active form of the vitamin, resulting in hypercalcemia, hypercalciuria, and nephrolithiasis.36
HEPATIC SARCOIDOSIS
Liver involvement is common but rarely causes any clinically relevant signs or symptoms. Histologic evidence of sarcoidal granulomas is common and the liver can be a good site to biopsy to confirm the diagnosis. An increase in serum alkaline phosphatase occurs in approximately 33% of patients,37 but does not mandate treatment. Treatment is reserved for patients with significant symptoms (hepatosplenomegaly, abdominal pain, pruritus), evidence of synthetic dysfunction, or hyperbilirubinemia. Rarely, primary biliary cirrhosis-type disease and portal hypertension may develop.38
OTHER ORGANS
The sinuses and upper airway are commonly involved with sarcoidosis, a condition known as sarcoidosis of the upper respiratory tract. Nasal sarcoidosis of the upper respiratory tract is often associated with lupus pernio and may cause severe epistaxis and nasal crusting. Sarcoidosis may involve the spleen, and may be associated with reduction in any blood cell line. Splenic sequestration and
bone marrow involvement may lead to leukopenia. Thrombocytopenia may result from bone marrow involvement, splenic sequestration, or from an idiopathic thrombocytopenic purpura-like syndrome related to hypergammaglobulinemia often seen in patients with sarcoidosis.39
ETIOLOGY AND PATHOGENESIS
Sarcoidosis is triggered by exposure to an antigen(s) with hyperactivity of the cell-mediated immune system leading to granulomatous inflammation. Presumably antigen-presenting cells, such as macrophages, recognize, process, and present the processed sarcoid-inducing antigen to CD4+ T cells of the T-helper (Th)1 subtype. The processed antigen is presented to these lymphocytes via human leukocyte antigen (HLA) class II molecules on the antigen-presenting cells that have undergone enhanced expression from exposure to the sarcoidosis antigen and possibly interferon gamma (IFN-γ).40,41 These activated macrophages produce interleukin (IL)-12 which induces lymphocytes to shift toward a Th1 profile and causes T lymphocytes to secrete IFN-γ. These activated T cells release IL-2 and chemotactic factors that recruit monocytes and macrophages to the site of disease activity. IL-2 and other cytokines also expand various T-cell clones. IFN-γ further activates macrophages and transforms them into giant cells.40 Tumor necrosis factor (TNF)-α, IL-2, and other cytokines may also be important in stimulating macrophages (Fig. 35-13). There is also evidence that CD4+ T cells of the Th17 subtype and Th17 cytokines also may play a role in the development of the lesions.42 The identity of the putative antigen(s) triggering the immunologic cascade is unknown. Infectious agents and environmental antigens and have been investigated.
RISK FACTORS
RISK FACTORS
Infectious agents such as mycobacteria,43 Propionibacterium acnes,44 and Chlamydia45 are associated with sarcoidosis. However, patients with sarcoidosis improve with immunosuppressive agents, which argues against a purely infectious etiology. Mineral dusts, including silica, iron,46 and titanium,47 are associated with sarcoidosis. Firefighters and persons with wood burning stoves are documented as having an increased risk of developing sarcoidosis.48,49 Lifelong nonsmokers are more likely to develop the disease50
than smokers. Genetics play a major role in determining susceptibility to sarcoidosis. Relatives of an affected person are more likely to develop disease than is the general population.51 Numerous studies in various ethnic groups show a relationship between HLA antigens
5
Proposed immunopathogenesis of sarcoidosis
Antigen
HLA class II molecule
TCR
IL-12
Macrophages Dendritic cells T lymphocytes (CD4)
IFN-γ, IL-2
IL-12
Th1 response
TNF-α, IL-1β
Granulomatous inflammation
and the development of disease, protection from disease, good prognosis, bad prognosis, acute disease, chronic disease, and various phenotypic expressions of sarcoidosis. Additionally, mutations in genes related to the immune system, including those encoding TNF, lymphotoxin α, and the IL-23 receptor, are associated with different presentations of sarcoidosis, including erythema nodosum, cardiac sarcoidosis, and uveitis.52-55
The interplay of antigenic and genetic risk factors suggests that there may be multiple causes of sarcoidosis. Perhaps patients have to experience a specific interaction between one or several exposures and be genetically programmed to one or several immunologic responses. Each putative antigen may be associated with a specific HLA class II molecule and T-cell receptor and/or other polymorphisms of the many molecules of the human immune system.
577
5
DIAGNOSIS
DIAGNOSIS
The diagnosis of sarcoidosis requires a compatible clinical picture, histologic demonstration of noncaseating granulomas, and exclusion of other diseases capable of producing similar histology or clinical features. As sarcoidosis is a diagnosis of exclusion, the diagnosis can never be confirmed with 100% certainty.56 Often the diagnosis is assumed when the clinical presentation is typical for the disease and is not explained by an alternative cause. The presence of noncaseating granulomas in a single organ system does not conclusively establish the diagnosis of sarcoidosis because sarcoidosis is, by definition, a systemic disease that involves multiple organs.57
Isolated skin granulomas should not be assumed to represent sarcoidosis, and efforts must be made to exclude alternative diagnoses. Although confirmation of sarcoidosis requires proof of granulomatous involvement in at least 2 separate organs, histologic confirmation is not necessarily required in the second organ.58
Certain disease presentations are so specific for the diagnosis of sarcoidosis (eg, Lofgren syndrome, Heerfordt syndrome, and asymptomatic bilateral hilar adenopathy) that the diagnosis may be accepted without a tissue biopsy. For example, asymptomatic bilateral hilar lymphadenopathy noted on chest radiograph is relatively specific for sarcoidosis. Some clinical, imaging, and laboratory tests are recommended when a diagnosis of sarcoidosis is considered. These tests screen for involvement of various organ systems (Table 35-2).
■History (occupational and environmental exposure, symptoms)
■History (occupational and environmental exposure, symptoms)
■Physical examination
■Physical examination
■Posteroanterior chest radiograph
■Posteroanterior chest radiograph
■Pulmonary function tests: spirometry, DLCO, and KLCO
■Pulmonary function tests: spirometry, DLCO, and KLCO ■Peripheral blood counts: white blood cells, red blood cells, platelets
■Peripheral blood counts: white blood cells, red blood cells, platelets
■Serum chemistries: calcium, liver enzymes (alanine aminotransferase, aspartate aminotransferase, alkaline phosphatase), creatinine, and blood urea nitrogen
■Serum chemistries: calcium, liver enzymes (alanine aminotransfer-
ase, aspartate aminotransferase, alkaline phosphatase), creatinine, and blood urea nitrogen
■Urine analysis
■Urine analysis
■Electrocardiogram
■Electrocardiogram
■Routine ophthalmologic examination
■Routine ophthalmologic examination
■Tuberculin skin test
■Tuberculin skin test
DLCO, diffusing capacity of lung for carbon monoxide; KLCO, diffusing capacity per liter alveolar volume. Adapted with permission of the American Thoracic Society. Copyright © 2017 American Thoracic Society. Originally from American Thoracic Society/European Respiratory Society: Statement on sarcoidosis. Joint Statement of the American Thoracic Society (ATS), the European Respiratory Society (RS) and the World Association of Sarcoidosis and Other Granulomatous Diseases (WASOG) adopted by the ATS Board of Directors and the ERS Executive Committee, February 1999. Am J Respir Crit Care Med. 1999;160:736. The American Journal of Respiratory and Critical Care Medicine is an official journal of the American Thoracic Society.
578
A physical examination and routine ophthalmologic examination should be performed in addition to testing. A history to assess for risk of other granulomatous diseases by occupational and environmental (eg, exposure to tuberculosis, endemic fungi, and beryllium exposure) should be performed.
LABORATORY TESTING
LABORATORY TESTING
Recommended tests to evaluate for system disease include pulmonary function tests, complete blood count, comprehensive metabolic panel, urine analysis, electrocardiogram, and tuberculosis testing (QuantiFERON-TB gold tuberculosis assay or tuberculin skin test). The epithelioid cell of the sarcoidal granuloma secretes angiotensin-converting enzyme.59
Consequently, serum angiotensin-converting enzyme (SACE) levels reflect the total granuloma burden in sarcoidosis. However, elevated SACE levels are insufficiently specific for the diagnosis of sarcoidosis to rest on it alone, and insufficiently sensitive to exclude the diagnosis.60 SACE levels are elevated in all granulomatous diseases, including infectious ones. Initial SACE levels are not different between patients who deteriorate and those who improve,61
so they should not be used to determine treatment. Serial SACE levels may be useful for monitoring the course of sarcoidosis, but this test is not presently routinely used.
IMAGING
IMAGING
A posteroanterior chest radiograph is abnormal in more than 90% of patients with sarcoidosis. Staging of pulmonary radiographs is as follows:
Stage 0: normal Stage I: bilateral hilar and/or paratracheal adenopathy Stage II: adenopathy with pulmonary infiltrates Stage III pulmonary infiltrates only Stage IV: pulmonary fibrosis
Bilateral hilar adenopathy is noted in 50% to 85% of cases. Pulmonary parenchymal infiltrates are seen in 25% to 60% of cases. Asymptomatic hilar adenopathy on chest radiograph almost always represent sarcoidosis.62 It has been suggested that histologic confirmation of sarcoidosis may not be required in asymptomatic patients provided the physical examination, complete blood count, and routine blood tests are all normal and there is no prior history of malignancy.63 Although chest computed tomography reveals more thoracic disease than can be appreciated on chest radiography, there is insufficient evidence that computed tomography has a clinical role in the management of pulmonary sarcoidosis.64 Characteristic round, punched out,
lytic, cystic lesions may be found in radiographs of the hands and feet. The mechanism of gallium-67 uptake in sarcoidosis is incompletely understood. It is thought that inflammatory processes cause hyperemia and increased capillary permeability of gallium. Gallium also accumulates in macrophages and, to a lesser extent, in T lymphocytes, which are major participants in the granulomatous inflammation of sarcoidosis. Sarcoidosis may cause gallium uptake in thoracic and extrathoracic sites, although typically not in areas of skin involvement. Gallium scanning has not been found useful for monitoring the clinical course of sarcoidosis, but it may have a role in identifying organs with sarcoid involvement. The presence of panda sign (bilateral lacrimal and parotid gland uptake) and lambda sign (bilateral hilar and right paratracheal uptake) on gallium-67 scanning is highly specific for sarcoidosis and may obviate the need for invasive diagnostic procedures. However, these signs are both positive in only a small percentage of sarcoidosis patients. Organ activity has been detected by gadolinium enhancement on nuclear magnetic resonance imaging. Magnetic resonance imaging is useful in detecting neurosarcoidosis and monitoring therapeutic response. Fluorodeoxyglucose positron emission tomography scanning is more sensitive in revealing granulomatous inflammation than gallium-67 scanning and in monitoring response to treatment.65,66
PATHOLOGY
PATHOLOGY
The epithelioid granuloma of sarcoidosis usually contains a compact collection of mononuclear phagocytes. The granulomas typically are surrounded by a paucity of lymphocytes (“naked granulomas”), but varying degrees of lymphocytic inflammation may be present (Fig. 35-14). Epithelioid cells, which are themselves transformed monocytes, are commonly present within the sarcoidal granuloma. Multinucleated giant
5
cells of the Langerhans type result from the fusion of epithelioid cells. Although central fibrinoid necrosis is not uncommon, gross necrosis is not a characteristic feature of sarcoid granulomas and suggests an alternative diagnosis, such as tuberculosis, fungal infection, or vasculitis.59 Mycobacterial and fungal diseases must always be considered as alternative diagnoses; therefore, stains and cultures for mycobacteria and fungi should be routinely performed. Reaction to foreign bodies such as beryllium, tattoo pigment, and paraffin can have similar histologic findings. Although there are often distinguishing features from sarcoidosis, granuloma annulare, necrobiosis lipoidica, rheumatoid nodules, cheilitis granulomatosa, and annular elastolytic giant cell granuloma may have cutaneous granulomas and are in the differential diagnosis. A clinically important aspect of the pathology of sarcoidosis involves the development of fibrosis. Dense bands of fibroblasts may encase the ball-like granulomas. This fibrotic response can produce tissue destruction and organ dysfunction that cannot be successfully reversed with therapy.
DIAGNOSTIC ALGORITHM
DIAGNOSTIC ALGORITHM
Approach to patient with sarcoidosis
The diagnosis of sarcoidosis
Biopsy: NCG
Classical clinical syndrome:
Exclude other granulomatous diseases
Löfgren syndrome Heerfordt syndrome Asymptomatic bilateral Hilar adenopathy on CXR Lambda + panda sign on gallium scan +Kveim test
Document systemic involvement: clinical evidence of a second organ involved
579
5
Histologic and Clinically Similar Conditions
Histologic and Clinically Similar Conditions
■Deep fungal infections can be granulomatous and clinically resemble sarcoid like blastomycosis, histoplasmosis and others
■Deep fungal infections can be granulomatous and clinically resem-
ble sarcoid like blastomycosis, histoplasmosis and others
■Annular elastotic giant cell granuloma
■Annular elastotic giant cell granuloma
■Granuloma annulare
■Granuloma annulare
■Lupus vulgaris
■Lupus vulgaris
■Atypical mycobacterial infection
■Atypical mycobacterial infection
■Cheilitis granulosa
■Cheilitis granulosa
■Foreign-body reactions (eg, tattoo, soft-tissue fillers, ruptured hair follicles/cyst)
■Foreign-body reactions (eg, tattoo, soft-tissue fillers, ruptured hair
follicles/cyst)
■Rheumatoid nodules
■Rheumatoid nodules
■Necrobiosis lipoidica
■Necrobiosis lipoidica
■Granulomatous rosacea
■Granulomatous rosacea
■Cutaneous Crohn disease
■Cutaneous Crohn disease
■Blau syndrome
■Blau syndrome
■Granulomatous syphilis
■Granulomatous syphilis
■Granulomatous cutaneous T-cell lymphoma
■Granulomatous cutaneous T-cell lymphoma
■Melkersson-Rosenthal syndrome Clinically Similar Conditions Without Similar Histologic Findings
■Melkersson-Rosenthal syndrome Clinically Similar Conditions Without Similar Histologic Findings
■Amyloidosis of the skin
■Amyloidosis of the skin
■Cutaneous xanthomas
■Cutaneous xanthomas
■Syndromes with multiple adnexal tumors and/or dermal tumors (eg, Cowden syndrome, Brooke-Spiegler)
■Syndromes with multiple adnexal tumors and/or dermal tumors
(eg, Cowden syndrome, Brooke-Spiegler)
DIFFERENTIAL DIAGNOSIS
Granulomatous syphilis, granulomatous cutaneous T-cell lymphoma, annular elastotic giant cell granuloma, fungal infections, Blau syndrome, granuloma annulare, lupus vulgaris, atypical mycobacterial infections, foreign-body reactions (eg, tattoo, soft-tissue fillers, ruptured hair follicles/cyst), rheumatoid nodules, necrobiosis lipoidica, cheilitis granulosa, and granulomatous rosacea are in the differential diagnosis. Histologic findings are very different, but clinically, syndromes with multiple adnexal tumors, amyloidosis of the skin, and cutaneous xanthomas may resemble cutaneous sarcoidosis (Table 35-3).
CLINICAL COURSE AND PROGNOSIS
The granulomatous inflammation of sarcoidosis can remit spontaneously or with therapy. Therefore, the general prognosis of sarcoidosis is good.57 Pulmonary sarcoidosis resolves, improves, or stabilizes in 60% to 90% of patients without treatment.67 Remissions often occur within the first 6 months after diagnosis, although it may take 2 to 5 years.68 The prognosis is generally favorable for liver and peripheral lymph node sarcoidosis as well. Skin lesions may resolve with or without scarring or pigmentary changes. The development of fibrosis causes almost all significant impairment from sarcoidosis. This is probably the result of hyalinization of granulomatous inflammation. Host response and inadequate treatment
580
may be to blame for the propensity for a brisk fibrotic response. In addition to permanent scarring of the skin from fibrosis, cutaneous lesions may ulcerate or destroy adjacent bone and cartilage. Lupus pernio lesions most commonly leave permanent scarring and destruction. In the United States, three-fourths of the sarcoidosis deaths are related to pulmonary involvement. Sarcoidosis of the heart and central nervous system accounts for most of the remaining deaths.69
There is no current laboratory tests or radiologic findings that can reliably predict the outcome of sarcoidosis. Skin lesions are not a reliable indicator of prognosis, but several useful associations have been documented. Patients with cutaneous lesions area more likely to have chronic systemic sarcoidosis than patients without skin involvement.70 Erythema nodosum with fever and arthralgia portends a good prognosis.71 Patients with Lofgren syndrome have a more than 80% rate of spontaneous remission, generally within 4 to 6 weeks.2 Lupus pernio indicates chronic disease and is associated with upper respiratory tract involvement, pulmonary fibrosis, and bony cysts.2 African descent, higher stage chest radiograph (greater than stage I), age older than 40 years, splenic involvement, disease duration longer than 2 years, and forced vital capacity less than 1.5 L are associated with a worse prognosis.57
MANAGEMENT
Sarcoidosis often spontaneously remits, and therapy may be associated with significant side effects. Consequently, monitoring patients for development of progressive irreversible damage is a reasonable strategy. Clinicians should treat cutaneous sarcoidosis when the lesions are cosmetically unacceptable for the patient or they are scarring and infiltrative as in lupus pernio. Other appropriate reasons to initiate therapy include pulmonary symptoms, worsening pulmonary function, neurologic involvement, ocular involvement, symptomatic cardiac disease, evidence of hepatic synthetic dysfunction, and splenomegaly.
THERAPY DIRECTED AT THE SKIN
THERAPY DIRECTED
AT THE SKIN
Cutaneous sarcoidosis, including lupus pernio, may be improved with prolonged application (at least 2 weeks) of class I topical steroids such as clobetasol ointment. Intralesional injections of triamcinolone (strength 3 to 10 mg/mL) are more effective. Both therapies can cause skin atrophy and hypopigmentation. Topical tacrolimus may be effective for skin disease and does not pose the same adverse effects, but is not generally as effective.72,73
SYSTEMIC CORTICOSTEROIDS
SYSTEMIC CORTICOSTEROIDS
Systemic corticosteroids are the most reliable immediate initial therapy for sarcoidosis. Treatment of cutaneous disease is usually initiated with 40 to 60 mg/day of prednisone equivalent with tapering of therapy over a month to doses of 10 to 20 mg/day. The recommended initial dose of pulmonary sarcoidosis is 20 to 40 mg of prednisone equivalent/day.74 Cardiac and neurologic sarcoidosis may require higher initial doses, up to 60 to 80 mg of prednisone equivalent/ day.74 The corticosteroid dosage typically is tapered 0.1 to 0.2 mg/kg over a few months.74 It is unusual for pulmonary disease to require a maintenance dose of more than 15 mg of prednisone equivalent/day, but cutaneous, cardiac, and neurologic disease may require higher doses. An attempt should be made
AGENT DOSE/COMMENT
5
to taper the dose within 9 to 12 months of the initiation of therapy.74 Life-threatening arrhythmias are an exception to this rule, and placement of an internal defibrillators may be indicated.75-77
If patients cannot be successfully weaned from corticosteroids, a variety of immunosuppressive medications can be used as steroid-sparing agents. Most immunosuppressive are inadequate as monotherapy. Table 35-4 lists the appropriate doses for treatment of sarcoidosis.
METHOTREXATE
METHOTREXATE
Methotrexate is the most studied steroid-sparing agent. The drug requires careful monitoring of liver function tests and blood cell counts. Folic acid can
Topical steroids and intralesional steroids Localized skin lesions Class I ultrapotent steroids (eg, clobetasol 0.05% ointment) BID for 2-4 weeks then BIW Intralesional triamcinolone 2.5-10.0 mg/mL
Topical tacrolimus Tacrolimus 0.1% ointment BID Localized skin lesions
Systemic corticosteroids Prednisone (or equivalent) 20-40 mg/day then taper Consider higher doses for cardiac, neurologic involvement
Methotrexate 10-25 mg/week Monitor complete blood count, liver function tests >1.5 g cumulative dose consider liver biopsy or procollagen III peptide testing Consider adjunctive folate 1 mg/day
Hydroxychloroquine 200-400 mg/day Yearly ophthalmologic screening
Chloroquine 250-1000 mg/day Yearly ophthalmologic screening
Tetracycline Minocycline 200 mg/day Doxycycline 200 mg/day Primarily for nonlupus pernio skin disease
Broad-spectrum antibiotics CLEAR (combined levofloxacin, 500 mg/day; ethambutol, 25 mg/kg/day up to 1200 mg; azithromycin, 250 mg/day; and rifampin, 10 mg/kg/day or up to 300 mg/day) for 8 weeks
Infliximab 5 mg/kg IV q6weeks Screening/monitoring for tuberculosis Consider adjunctive low-dose methotrexate to prevent antidrug antibody formation
Adalimumab 40 mg weekly beginning at week 4 following a 160-mg dose at week 0 and an 80-mg dose at week 2
Pentoxifylline 400 mg TID
Leflunomide 100 mg/day for 3 days loading, then 10 mg/day; can increase to 20 mg/day; monitor complete blood count and liver function tests
Thalidomide 50-200 mg/day QHS dosing as sedating Peripheral neuropathy common monitoring necessary
Melatonin 20 mg/day for 1 year then 10 mg/day for 1 year QHS dosing
Cyclophosphamide 500-1000 mg IV q3-4weeks; monitor complete blood count and urinalysis; stop if hematuria develops Reserved for life-threatening disease because of carcinogenicity
Cyclophosphamide 500-1000 mg IV q3-4weeks; monitor complete blood count and urinalysis; stop if hematuria develops Reserved for life-threatening disease because of carcinogenicity
581
5
be given in conjunction with methotrexate to alleviate side effects. Patients with sarcoidosis may develop cirrhosis, even if their liver function tests are normal. Liver biopsies should be considered in patients after 1 to 2 g of total therapy. Typical doses of methotrexate for cutaneous disease are 10 to 25 mg/week. Cutaneous improvement may be noted within 1 month, but maximal therapeutic benefit often does not occur until at least 6 months after the initiation of treatment.
ANTIMALARIALS HYDROXYCHLOROQUINE/ CHLOROQUINE
ANTIMALARIALS
HYDROXYCHLOROQUINE/
CHLOROQUINE
Antimalarial drugs are useful for sarcoidosis affecting the joints and skin, and hypercalcemia.78,79
Antimalarial agents area not highly effective for pulmonary disease, and often take several months to be effective. Chloroquine has a higher potential of causing retinal damage than hydroxychloroquine, but patients taking either drug must have regular ophthalmologic exams. Hemolytic anemia may occur and patients with glucose-6 phosphate dehydrogenase deficiency may have a higher rate of anemia, but with usual dermatologic doses the deficiency is not an absolute contraindication for usage of hydroxychloroquine.
CYCLOPHOSPHAMIDE
CYCLOPHOSPHAMIDE
Cyclophosphamide is effective for many forms of sarcoidosis. However, because of its significant sideeffect profile, including carcinogenic potential, cyclophosphamide is reserved for severe or potentially life-threatening disease.
ANTIBIOTICS
ANTIBIOTICS
Minocycline and doxycycline (doses of 100 mg twice daily) have been reported to improve skin sarcoidosis in case series. These drugs may take up to 2 years to be effective.80 Tetracyclines modify the immune response by suppressing activity of macrophages and T lymphocytes.81 Several months of the CLEAR (combined levofloxacin, 500 mg/day; ethambutol, 25 mg/kg/day up to 1200 mg; azithromycin, 250 mg/day; and rifampin, 10 mg/kg/day or up to 300 mg/day) regimen has also shown some effectiveness, and clinical trials are currently ongoing to better assess the usefulness of this regimen.82
582
TUMOR NECROSIS FACTOR ANTAGONISTS
TUMOR NECROSIS
FACTOR ANTAGONISTS
TNF is a cytokine that is secreted in macrophages associated with sarcoidal granulomas.18 Antagonists of TNF have been shown to be useful for the treatment of sarcoidosis. Pentoxifylline,83 thalidomide,84
infliximab,85 and adalumimab85 are the most studied. Infliximab appears to be particularly useful for the treatment of lupus pernio,86 and it may be superior to the other TNF antagonists, as a study of etanercept failed to show benefit for sarcoidal uveitis.87 Paradoxically, administration of these drugs for other conditions has been rarely associated with the development of sarcoidosis.88
OTHER AGENTS
OTHER AGENTS
Azothioprine,89 mycophenolate mofetil,90 leflunomide,91 and cyclosporine92 have been reported to be useful for the treatment of systemic sarcoidosis in small case series. Melatonin,93 allopurinol,94 isotretinoin,95
and fumaric acid esters96 have been reported to be effective for cutaneous sarcoidosis.
PROCEDURES
PROCEDURES
Phototherapy and photodynamic therapy have been used to mitigate cutaneous sarcoidosis.97 Electrodessication, pulse-dye laser, carbon dioxide laser therapy, and reconstructive surgical procedures have all been used successfully to improve the cosmetic disfigurement of cutaneous disease.
TREATMENT ALGORITHM
TREATMENT ALGORITHM
PREVENTION/SCREENING
PREVENTION/SCREENING
Prevention and screening for this elusive disease are not currently practical or available.
ACKNOWLEDGMENTS
Thanks to Marc Judson, MD for his continued guidance in all things related to sarcoidosis.
5
Treatment algorithm for cutaneous sarcoidosis
Cutaneous sarcoidosis without significant systemic dysfunction
Erythema Nodosum
Specific Lesions
Asymptomatic Not disfiguring
Treatment based on symptoms No treatment or NSAID or Prednisone
No treatment/monitor
Localized/ Mild disease
Inadequate response
Topical high potency steroids or intralesional steroids
Inadequate response
Add topical tacrolimus
Inadequate response
Brief course <1 month prednisone if not contraindicated
Inadequate response
Antimalarials or Methotrexate or Tetracycline antibiotic or Pentoxylfylline or Melatonin
Symptomatic or disfiguring
Assess extent/severity of disease
Lupus pernio severe/extensive
Corticosteroids (prednisone 40-60 mg/day) + Steroid-sparing agent Methotrexate Antimalarials + Intralesional to prominent areas +
Good response
Inadequate response
Taper steroids slowly over several months. Then taper steroid-sparing agent slowly over several months.
Add TNF-α inhibitor Adaluminmab or Infliximab with low dose methotrexate to prevent antibody formation.
Good response
Inadequate response
Inadequate response Good response
Taper very slowly over months Try alternative
Inadequate response
Good response
Add low-dose prednisone
Consider experimental, surgical, or more toxic therapies (eg, Cytoxan, Apremilast, Laser)
583
5

Figure 35-1 Perioral papular lesions.

Figure 35-2 Periorbital papular lesions.

Figure 35-3 Diascopy revealing “apple-jelly” coloration.
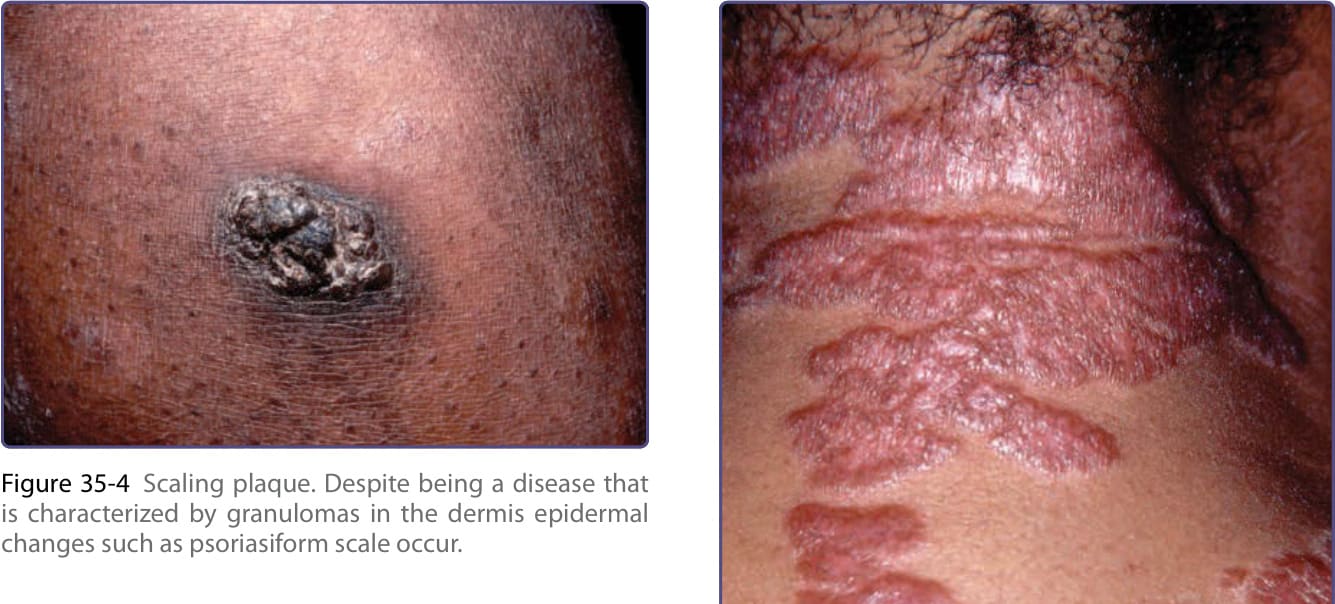
Figure 35-4 Scaling plaque. Despite being a disease that is characterized by granulomas in the dermis epidermal changes such as psoriasiform scale occur.

Figure 35-5 Dermal plaque. Notice there are no epidermal changes in this example of cutaneous sarcoidosis.

Figure 35-6 Plaques on neck.
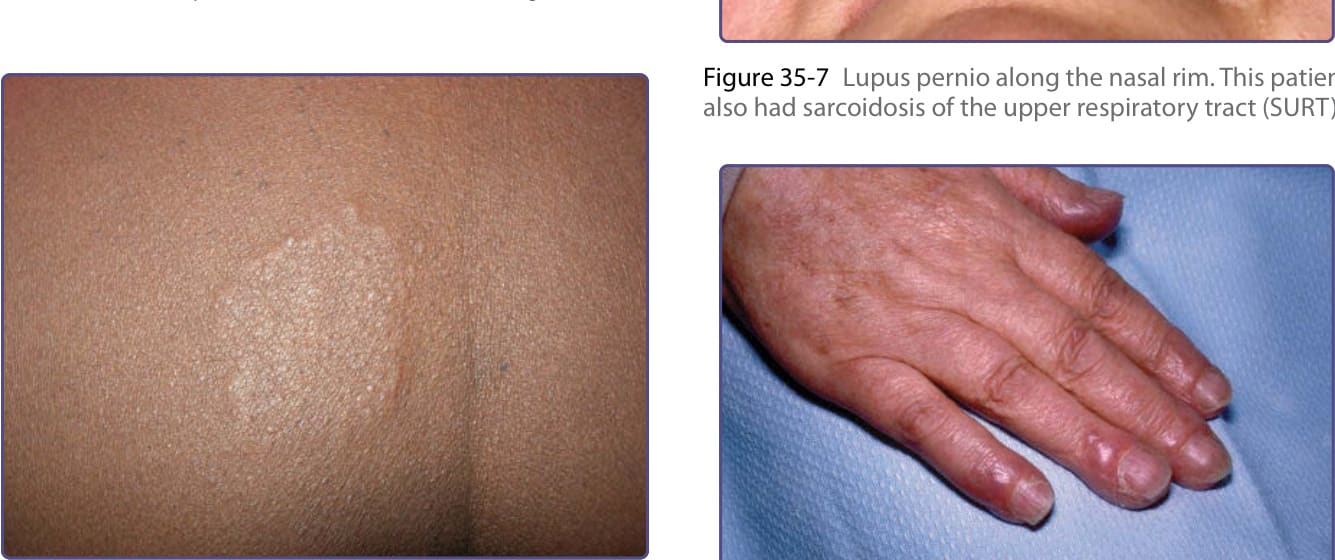
Figure 35-7 Lupus pernio along the nasal rim. This patient also had sarcoidosis of the upper respiratory tract (SURT).

Figure 35-8 Lupus pernio of the digits.

Figure 35-9 Scar sarcoid arising in an excision site.

Figure 35-10 Hypopigmented macules.
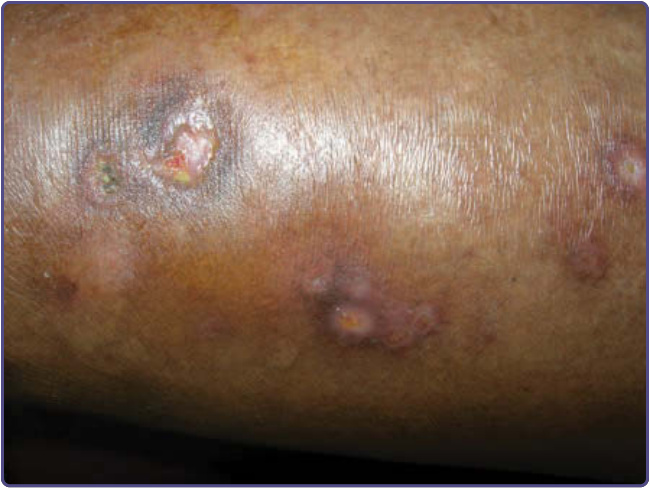
Figure 35-11 Ulcerative lesions on the leg.
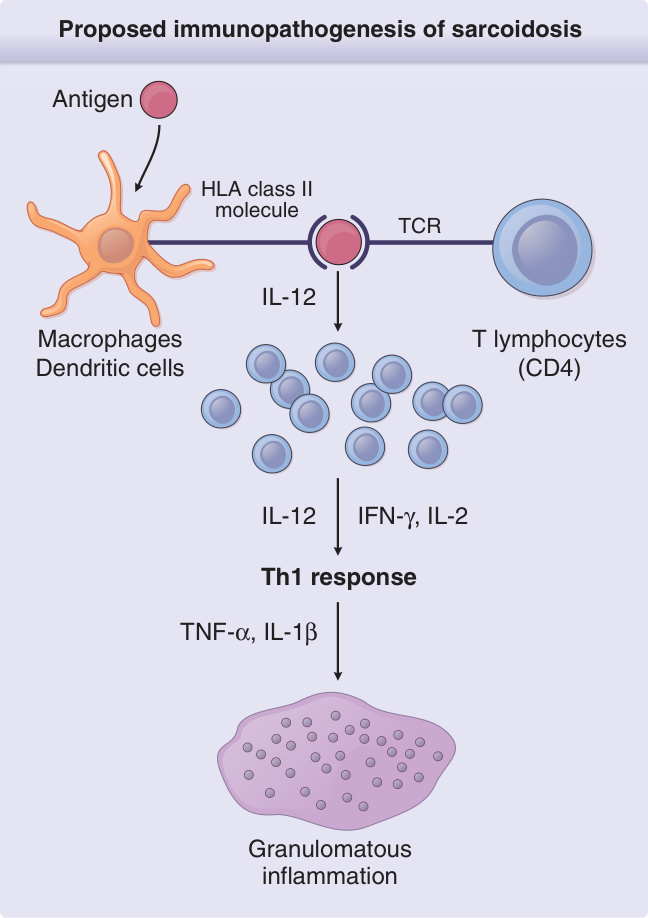
Figure 35-13 Proposed immunopathogenesis of sarcoidosis. An antigen, presently unknown, is engulfed and processed by an antigen-presenting cell (macrophage or dendritic cell). The processed antigen is presented to a T-cell receptor (TCR) of a T lymphocyte via an HLA class II molecule. Once the HLA receptor and TCR have bound the processed antigen, numerous lymphokines and cytokines of the T-helper cell subtype 1 (Th1) class are released that lead to T-cell proliferation, recruitment of monocytes, and eventual granuloma formation. A few of these lymphokines and cytokines are shown, with those released by the antigen-presenting cells on the left and those released by lymphocytes on the right. IFN, interferon; IL, interleukin; TNF, tumor necrosis factor.
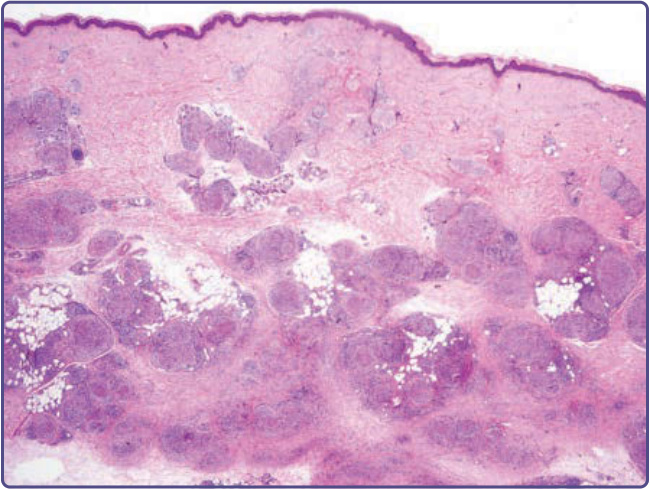
Figure 35-14 Histology of cutaneous sarcoidosis with “naked” granulomas.
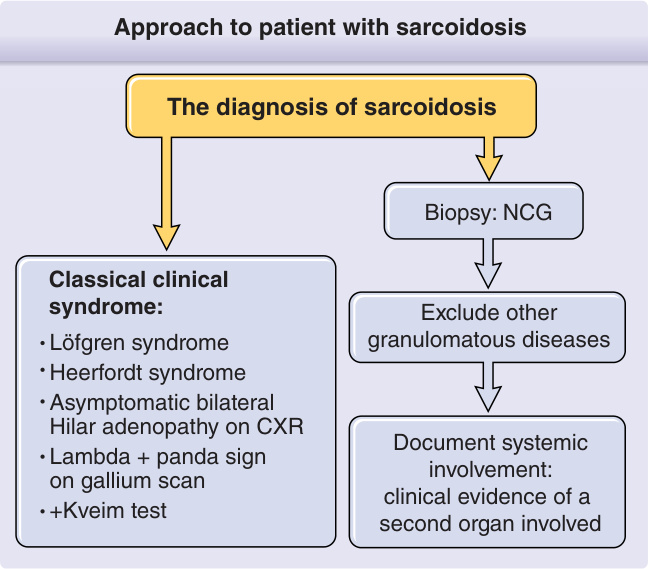
Figure 35-15 shows an algorithm for diagnosing whether a patient has sarcoidosis.
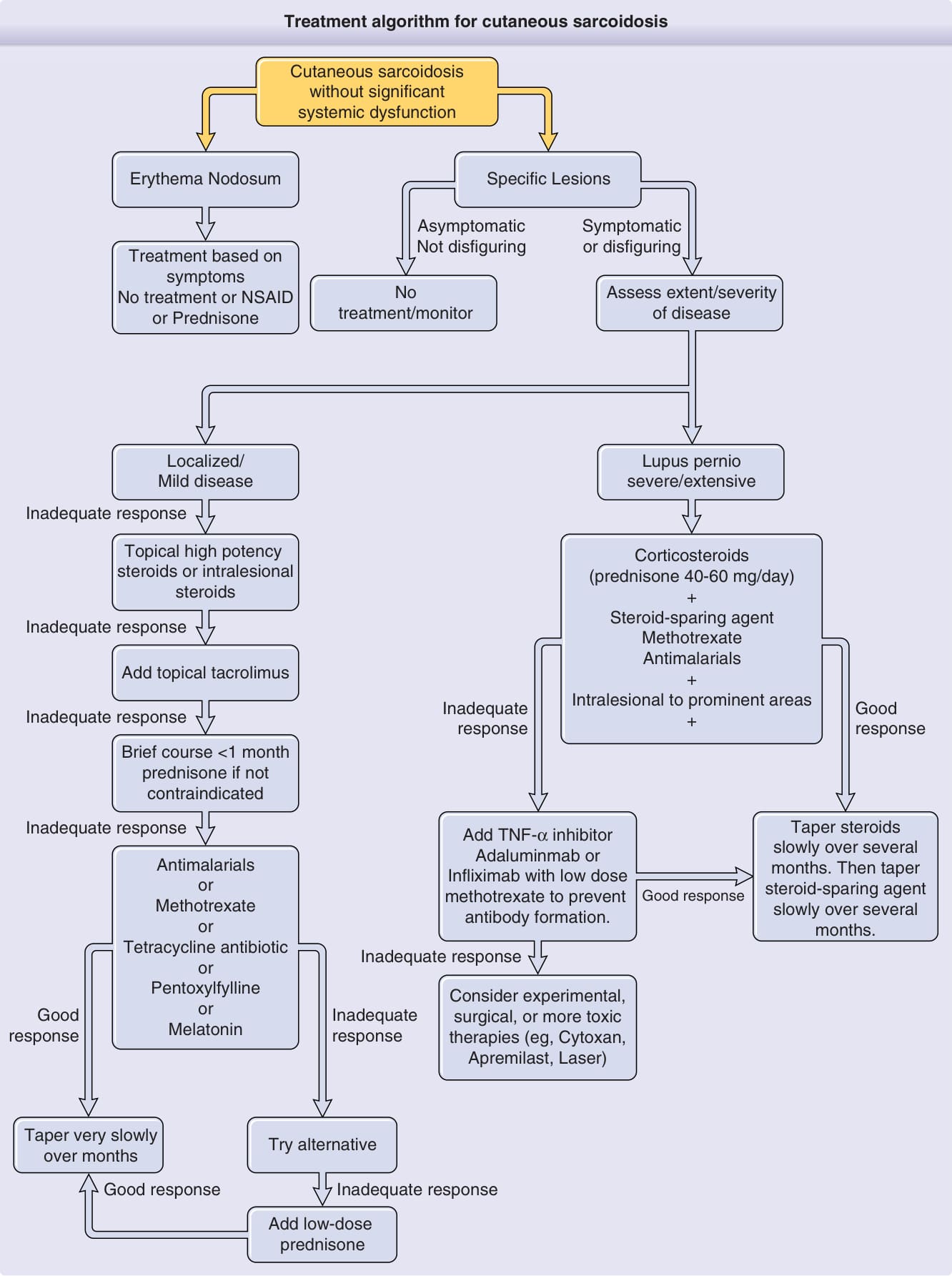
Figure 35-16 presents a treatment algorithm for cutaneous sarcoidosis.
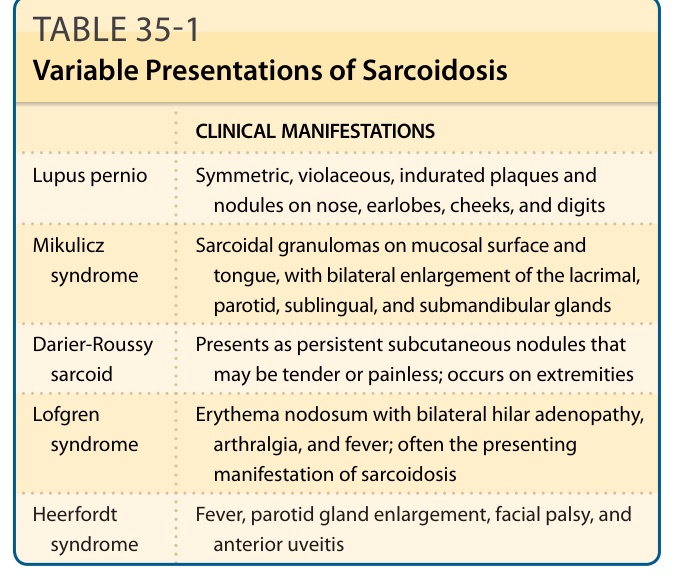
Table 35-1 summarizes the variable presentations of sarcoidosis.
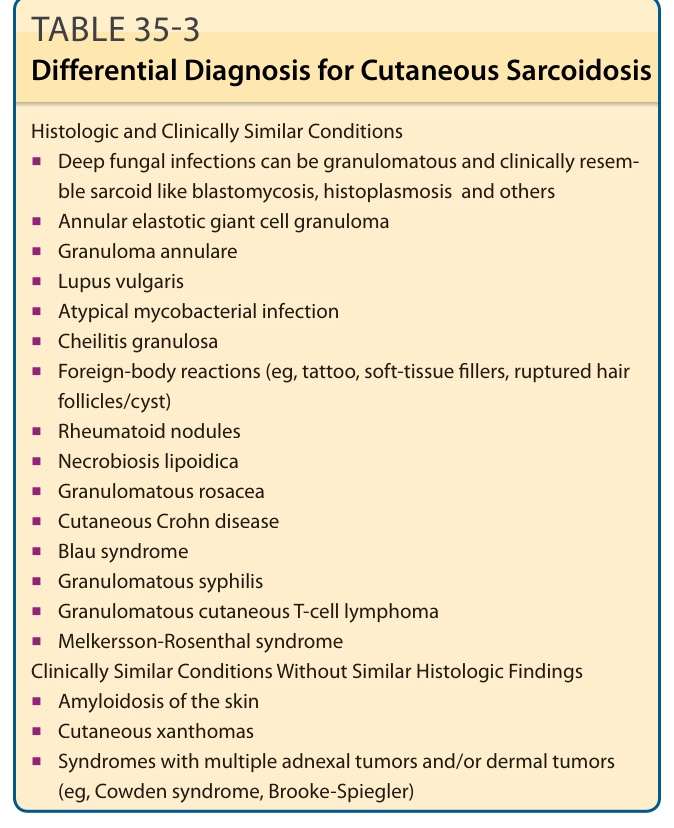
TABLE 35-3 Differential Diagnosis for Cutaneous Sarcoidosis
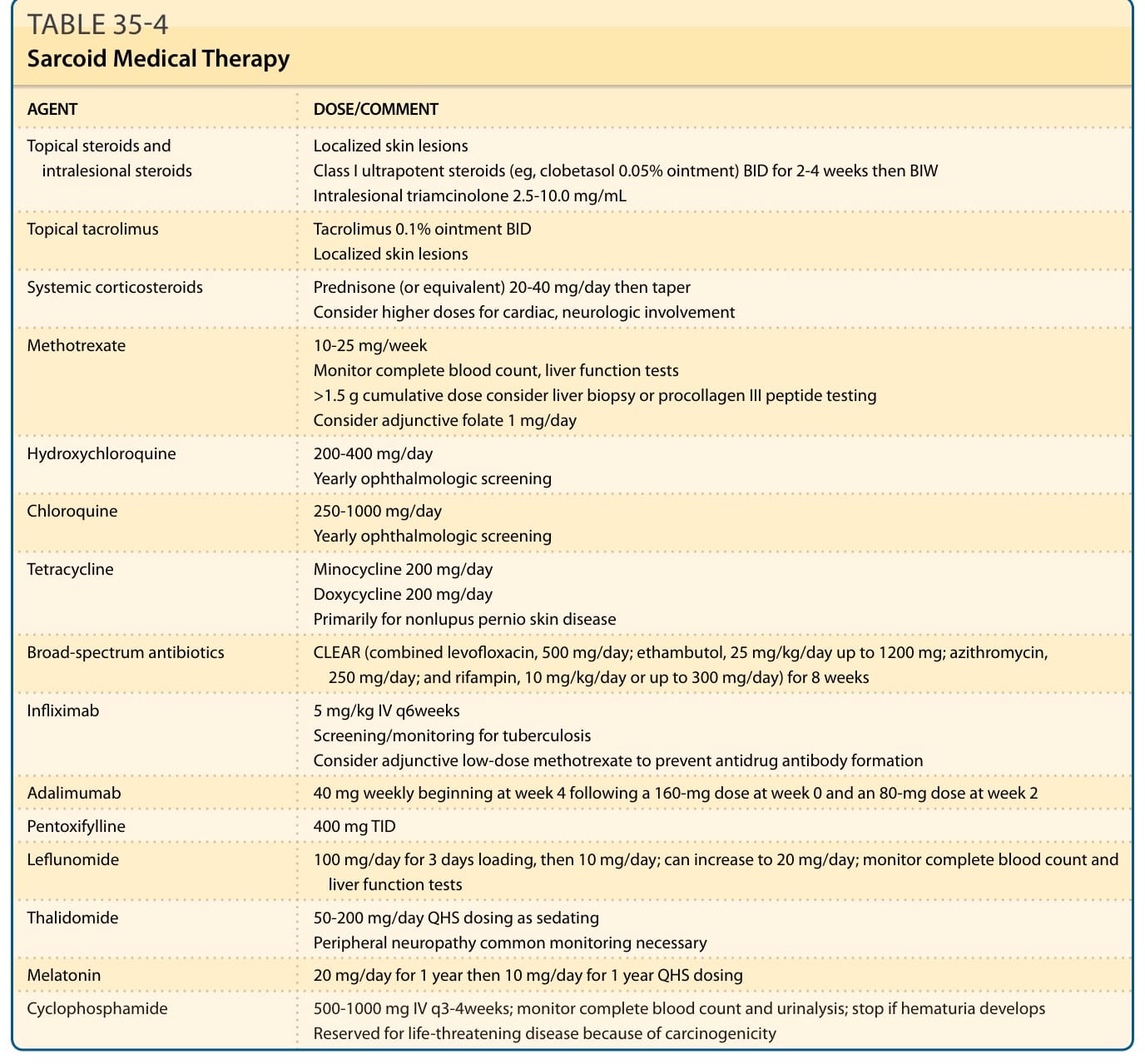
TABLE 35-4 Sarcoid Medical Therapy