Lichen Planus
PART5
Lichenoid and Granulomatous Disorders
AT-A-GLANCE
■ Lichen planus is an idiopathic T cell–mediated process without a clear autoantigen.
■ The worldwide prevalence of lichen planus is approximately 1%.
■ The lesions are well-marginated, flat-topped, red-violet polygonal papules.
■ The distribution is symmetrical and grouped lesions affect the flexural aspects of the arms and legs.
■ Variants are based on configuration, morphology of lesion, and site of involvement.
■ Histology shows basal keratinocyte damage with a lymphocyte-rich interface reaction.
INTRODUCTION
Lichen planus (Greek leichen, “tree moss”; Latin planus, “flat”) is a common inflammatory condition that can affect any ectodermal-derived tissue. Both Hebra and Erasmus Wilson described a similar inflammatory papulosquamous eruption, lichen ruber and lichen planus, respectively, which likely represented the same entity.1 Weyl and Wickham elaborated upon the morphology of lichen planus, and Gougerot and Burnier described disease involvement of mucosal sites.2-4 Although no single feature of lichen planus is a sine qua non, classic lichen planus is typified clinically by “the four Ps”—(1) purple, (2) polygonal, (3) pruritic, and (4) papules—and histologically by a brisk lymphocytic interface reaction.
PATHOGENESIS
The pathogenesis of lichen planus is unknown. Many contributing factors are implicated and include infectious, immune, metabolic, and genetic causes. It is
evident that specific immunologic mechanisms control the development of lichen planus. T cell–mediated pathologic alterations involving proinflammatory and counterregulatory mechanisms function in the pathogenesis of lichen planus. No consistent alterations in immunoglobulins have been shown in lichen planus, and humoral immunity most likely is a secondary response in immunopathogenesis. Cell-mediated immunity, on the other hand, plays a major role in lichen planus. One consistent feature of lichen planus is CD4-positive T-helper (CD4-Th) cells in the dermis despite disease chronicity and CD8-positive T- cytotoxic (CD8-Tc) cells in close proximity to damaged basal keratinocytes.5 Based on these observations and insights from other lichenoid tissue reactions (LTRs), such as graft-versus-host-disease (GVHD), modern theories encompass three major stages: antigen recognition, lymphocyte activation, and keratinocyte apoptosis. A fourth stage, resolution, is a new and emerging facet of the disease to further understand the pathogenesis of lichen planus.
ANTIGEN RECOGNITION
ANTIGEN RECOGNITION
The CD8-Tc cell is the effector cell of lichen planus; however, the initial antigen recognition and CD8-Tc stimulation may be driven by the initial interaction between the CD4-Th cell with the Langerhans cell (LC). The targeted antigen(s) and trigger(s) for lichen planus remains unknown. However, in other similar diseases, such as lichenoid GVHD, the target antigens are alloantigens. In oral disease, a lichen planus– specific antigen associated with major histocompatibility complex (MHC) class I on keratinocytes has been reported.6
It is unknown if this antigen is unique to oral lichen planus and if this antigen is an autoreactive peptide or an exogenous antigen. Circulating antibodies have also been identified in multiple studies without a clear
5
target antigen.7,8 A small but significant population of CD 56–positive CD 16–negative natural killer (NK) cells are observed early in the disease course of lichen planus.9 These cells express chemokine receptor-3 (CXCR-3) and chemokine (c-c) motif ligand (CCL) -5 and -6 and release interferon-γ (IFN-γ) and tumor necrosis factor-α (TNF-α).9 Taken together, NK cells may migrate to the site of inflammation and provide an early stimulating signal for the recruitment of CD4- Th and CD8-Tc cells. The CD4-Th population is localized to the dermis with scattered cells in the epidermis. CD4-Th cells colocalize with the LCs. LCs are the principal antigenpresenting cells of the epidermis and they upregulate MHC class II receptors in lichenoid disease, which allows for an interaction between CD4-Th cells and keratinocytes.10 In particular, CD4-positive LCs are seen in close approximation with the HLA-DR– positive keratinocytes.11 In addition, the CD4-Th cells have restricted V-β gene expression, which suggests antigen-specific oligoclonal T-cell expansion.12,13 Upon costimulation by LCs, CD4-Th cells release inflammatory cytokines, including IFN-γ, which leads to CD8- Tc activation and additional oligoclonal expansion.14
Taken together, these findings suggest an integral role of LCs, keratinocytes, and CD4 T helper cells in antigen presentation as well as the initiation and propagation of the Th1 response via the production of IFN-γ. The nature of antigenic stimulation is not known. Contact sensitizers such as metals could act as haptens and elicit an immunologic response. Enhanced lymphocyte reactivity to inorganic mercury, a component of dental amalgam, has been found in patients with oral LTRs. Low-grade chronic exposure to mercury, and possibly to other metals such as gold, may stimulate a lymphocytic reaction that manifests as lichen planus. A list of contact chemicals and drugs that can elicit lichenoid reactions is discussed in the section “Drug- Induced Lichen Planus.” With more widespread use of biologics, specifically TNF-α inhibitors, for the treatment of various chronic inflammatory diseases, cases of TNF- α associated LTRs have been identified and implicate dysregulated cytokine production, including the upregulation of type I IFN.15 Microbial mediators in the development of lichen planus have elicited recurring debate. Although provocative, no conclusive evidence has molecularly linked lichen planus to any of the following infections or colonization: syphilis, herpes simplex virus 2, human immunodeficiency virus (HIV), amebiasis, chronic bladder infections, hepatitis C virus (HCV), Helicobacter pylori, or human papillomavirus (HPV).
LYMPHOCYTE ACTIVATION
As mentioned in the prior section, following antigen recognition, CD8-Tc cells are activated and undergo oligoclonal expansion. A cascade of both pro- and antiinflammatory cytokines is released, including interleukin (IL)-2, -4, and -10; IFN-γ; TNF-α; and transforming growth factor-β1 (TGF-β1).16,17 In lichen
528
planus, the balance between lymphocyte activation, downregulation, and the cytokine milieu determines the disease phenotype. IFN-γ plays a central role in lichen planus. IFN-γ induces the expression of inflammatory chemokines such as chemokine ligand (CXCL)-9, -10, and -11.18-20
CXCR-3, their matching receptor, is predominantly expressed on the surface of IFN-γ–producing CD4-Th cells.19-22 Peroxisome-proliferator-activated receptor γ (PPARγ) inhibits CXCL-10 and -11, and its loss may be an underlying driver result in scarring alopecia.23,24
IFN-γ increases peripheral blood mononuclear cell (PBMC) binding to HLA-DR–positive keratinocytes.19
Intercellular adhesion molecule 1 and vascular cell adhesion molecule expression is also enhanced by IFN-γ.21 Therefore, IFN-γ is fundamentally involved in the upregulation of cellular adhesion molecules and subsequent migration of lymphocytes to the dermal– epidermal junction (DEJ).25,26
KERATINOCYTE APOPTOSIS
CD8-Tc cells are likely the terminal effector cells in lichen planus. They colocalize with apoptotic keratinocytes and have in vitro cytotoxic activity against autologous keratinocytes.6,27 The cytotoxic effects of the CD8-Tc cells can be inhibited by blockade of the MHC class I domain.6 The exact mechanism of apoptosis in lichen planus remains unknown. The possible mechanisms include granzyme B release, TNF-α–TNF-α R1 receptor interaction, and Fas–Fas-L interaction. Granzyme B and granulysin are expressed at 100- to 200- fold higher levels in lichen planus relative to normal skin.28 Granzyme B, excreted by CD8-Tc cells, activates caspase-3 and promotes apoptosis.29 TNF-α upregulates the expression of matrix metalloproteinase-9 (MMP-9) in lesional T lymphocytes of oral lichen planus and leads to disruption of the basement membrane and damage to basilar keratinocytes.30 MMP-9 levels correlate with the phenotype, with high levels correlating with ulcerative disease.31 Taken together, MMP-9 likely disrupts the basement membrane homeostasis, blocking normal cell survival signaling and leads to apoptosis and cell death. Fas–Fas-L expression is elevated in oral lichen planus, correlates with disease progression, and likely contributes to apoptosis of keratinocytes.32-34
RESOLUTION
Lichen planus tends to be a self-resolving disease; however, there is a paucity of research into the resolution phase of disease. T-regulatory cells are seen in oral lichen planus and correlate with disease subtype and activity.35,36 Studies in acute GVHD have shown the central role of T-regulatory cells in disrupting dendritic cell (DC) and allogeneic T-cell interactions37
and prevents disease development. DCs have a complex role in lichen planus and are involved in T-cell migration, as well as, the modulation of inflammatory signals.38,39 Fas-L, granzyme B, and perforin can be expressed by keratinocytes, allowing for apoptosis
of lymphocytes.40,41 Further understanding of the resolution phase of LTRs should lead to development of novel targeted therapies.
GENETIC AND EPIGENETIC REGULATION
The immune system targets various naturally occurring, but potentially deleterious, antigens (ie, viruses and bacteria, malignant cells, and exogenous contactants).42 However, the generation of an immune response to exogenous antigens poses a risk for the development of cross-reactivity to self-antigens.43,44
Genetic polymorphisms have been implicated in the risk of development of lichen planus, including HLA, immune signaling molecules and receptors (IFN-γ, TNF-α, TNF-α R2, IL-4, IL-6, and IL-18), oxidative stress, prostaglandin E2 synthesis, formation of transglutaminase, thyroid hormone synthesis, prothrombin, and nuclear factor kappa B (NF-κB) as well as epigenetic regulation of genes by micro-RNA (miRNA)-146a and -155.45 These polymorphisms may regulate the activity of proinflammatory mediators and lead to aberrant signaling. Gene expression profiling of lichen planus, identified the expression of the CXCR-3 ligand, CXCL-9, as the most specific marker for lichen planus.46 In addition, keratinocytes were confirmed as a source of type I IFNs (-α and -β).46
EPIDEMIOLOGY
The exact incidence and prevalence of lichen planus are unknown. Additionally, most large, epidemiologic studies of lichen planus focus on the prevalence of oral disease or cutaneous disease and few include the ectodermal (skin, hair, nail, and mucous membranes) spectrum of lichen planus. Therefore, the 1% prevalence of lichen planus in the general population should be interpreted with caution.47 The prevalence of lichen planus varies geographically with a range from 0.1% to 4%. Nearly two thirds of cases of lichen planus present between the ages of 30 and 60 years with a peak onset between 55 and 74 years.48 lichen planus is less common at the extremes of age. There is no clear sexual or racial predilection in lichen planus; however, the age of onset is earlier in women.47-49
Childhood lichen planus accounts for only 1% to 5% of the total lichen planus cases in the general population. In Pacific Indians, childhood lichen planus is more common and accounts for nearly 20% of all cases.50 In the United States, childhood lichen planus may be slightly more common in African Americans. Much like adult lichen planus, there is no clear sexual predilection in childhood lichen planus. The peak onset of disease is between 8 and 12 years of age.50-53
Fewer than 100 cases of familial lichen planus have been reported. However, a strong family history has been reported in 1.5% of adult cases and 3.8% of pediatric cases.50,54 Familial forms are characterized by early onset, widespread and often erosive or
5
ulcerative disease, mucosal involvement, and frequent relapses.55,56 The atypical nature of familial lichen planus has led some to consider it a unique dermatosis. Multiple HLA haplotypes have been reported in familial lichen planus, including HLA-B27, Aw19, -B18, and -Cw8. In nonfamilial cases, HLA-A3, -A5, -A28, -B8, -B16, and Bw35 are more common.57 HLA-B8 is more common in patients with oral lichen planus alone, and HLA-Bw35 is more common with cutaneous lichen planus alone.
CLINICAL FEATURES
Although lichen planus most commonly involves the skin and oral mucosa, any ectodermal-derived tissue may be affected, including hair, nails, internal and external genitalia, eyes, and esophagus. For this reason, a detailed history and physical examination is required to guide appropriate therapy, referrals, and monitoring. The skin lesions of lichen planus typically develop over the course of weeks. The disease duration is dependent on the location of the lesions, lesion morphology, and histologic pattern.
CUTANEOUS FINDINGS
CUTANEOUS FINDINGS
The classic cutaneous lesions of lichen planus are wellmarginated, dull red-violet, flat-topped, polygonal papules. The papules are grouped and often coalesce into plaques. Wickham striae, fine, white and adherent reticulate scale, are noted in well-developed lesions (Fig. 32-1). Wickham striae are highly characteristic in lichen planus and are more easily visualized with dermoscopy. The characteristic clinical and
529
5
dermoscopic features of lichen planus correlate with the characteristic histological findings of lichen planus. Wickham striae correlate with orthokeratosis, epidermal thickening, and an increased granular layer. The dull red-violet color correlates with the combination of vascular dilation and pigment incontinence. The lesions of lichen planus are often symmetrically distributed over the over the extremities. The most common areas of involvement are the flexural wrists, arms, and legs. The proximal thighs, trunk, and neck are other common sites of involvement. Involvement of the face and palms are atypical for classic lichen planus. Inverse lichen planus (discussed below) commonly involves the axillae, groin, and inframammary region. Lichen planus tends to be extremely pruritic. The degree of pruritus appears to directly correlate with the extent of involvement with the most symptomatic disease in generalized lichen planus. One major exception is hypertrophic lichen planus, which often affects limited areas, such as the lower extremities, and is extremely pruritic. In the acute setting, lichen planus exhibits an isomorphic (Koebner) phenomenon in which trauma induces disease (Fig. 32-2). This phenomenon is now explained by trauma-induced exposure of plasmacytoid DCs to endogenous peptides, such as cathelicidin LL-37, and endogenous antigens, such as DNA and RNA, which stimulate the release of type I IFNs (-α and -β), which propagates disease.58
Lichen planus usually heals with postinflammatory
530
hyperpigmentation, which is more common in darker skinned individuals. Hypopigmentation is uncommon in lichen planus, and its presence should prompt consideration of an alternative diagnosis. Frequent reports of childhood lichen planus have come from the Indian subcontinent.50-52 The explanation of such a phenomenon may be multifactorial, including genetic susceptibility, infectious exposure, and social stigma associated with pigmentary changes. In support of the social implications of pigmentary changes, the largest study of childhood lichen planus in the United States found a predominance in African American children.53 The clinical and histological features of childhood lichen planus are similar to adult lichen planus with skin and oral involvement in 42% to 60% and 17% to 30% of cases, respectively.50-53 However, hair involvement and nail involvement is rare in 2% to 6% and 0% to 19% of cases, respectively.50-53
CLINICAL VARIANTS
CLINICAL VARIANTS
Many variations in the clinical presentation of lichen planus have been described and are most easily categorized by the configuration of lesions, the morphologic appearance, and the site of involvement (Table 32-1). Although there may be significant variation in the presentation of specific subtypes of lichen planus, there are often morphological clues of an LTR. The underlying mechanisms driving these clinical variants are unknown; however, akin to psoriasis, these variations are likely caused by genetic polymorphisms and environmental stimuli.
CONFIGURATION Annular Lichen Planus: Annular lesions occur in approximately 10% of lichen planus and commonly develop as an arcuate grouping of individual papules of lichen planus that coalesce to form a ring or expand centrifugally with a central clearing. Annular lesions are more common on the penis and scrotum (Fig. 32-3). Additionally, large lesions often appear annular because of central resolution and hyperpigmentation with an active, raised rim. Actinic lichen planus is seen in subtropical zones on sun-exposed, dark-skinned young adults and children, is frequently annular in shape.
Linear, Blaschkoid, and Zosteriform Lichen Planus: Papules of lichen planus may develop in a linear pattern secondary to trauma. Rarely, in fewer than 0.2% of lichen planus cases, the eruption may follow lines of Blaschko. Similar to other segmental diseases, the etiology is thought to be related to postzygotic, somatic mutations in susceptibility-associated genes.59 Zosteriform and linear lichen planus were thought to be the same disease; however, a recent study of zosteriform lichen planus found varicella zoster antigens exclusively in zosteriform lichen planus suggesting either a viral trigger of disease or an isotopic
SUBTYPES MOST COMMON SITES OF INVOLVEMENT
Cutaneous Lichen Planus
Actinic Sun-exposed areas
Annular Male genitalia, intertriginous areas
Atrophic Predominately on lower extremities, may occur on other areas of the body
Erosive Soles of the feet
Guttate Trunk
Hypertrophic Anterior legs, ankles, interphalangeal joints
Linear Lower extremities
Follicular Trunk and proximal extremities
Papular Flexural surfaces
Bullous Feet
Pigmentosus Sun-exposed areas
Pigmentosus inversus Intertriginous and flexural areas
Nail Fingernails > toenails
Palmoplantar Malleoli Palms Soles
Lichen planopilaris Classic: vertex scalp Frontal fibrosing alopecia Graham-Little-Piccardi-Lasseur syndrome
Mucosal Lichen Planus
Oral
Reticular Buccal mucosa and mucobuccal folds
Atrophic Attached gingiva
Hypertrophic Buccal mucosa
Erosive Lateral and ventral tongue Buccal mucosa
Bullous Posterior and inferior areas of the buccal mucosa
Plaque-like Dorsum of tongue and buccal mucosa
Vulvovaginal Vaginal introitus, clitoral hood, labia minora, labia majora, vagina
Esophageal Proximal esophagus Proximal and distal esophagus Distal esophagus
Special Forms
Drug induced Sun-exposed areas, lacks oral involvement
Lichen planus–lupus erythematosus overlap
Distal extremities, sun exposed
Lichen planus
Extremities
Lichen planus pemphigoides Extremities
pemphigoides
Adapted with permission from Gorouhi F, Davari P, Fazel N. Cutaneous and mucosal lichen planus: a comprehensive review of clinical subtypes, risk factors, diagnosis, and prognosis. Scientific World Journal. 2014;2014:742826.
response related to underlying resident memory cells.60 Therefore, the term linear lichen planus should only be used when dermatomal lines are not followed. It is important to differentiate linear and zosteriform lichen
5
planus from other segmental diseases, including lichen striatus, linear epidermal nevus, inflammatory linear and verrucal epidermal nevus, linear psoriasis, and linear Darier disease.
MORPHOLOGY OF LESIONS Hypertrophic Lichen Planus: Hypertrophic lichen planus occurs most commonly on the anterior shins and interphalangeal joints (Fig. 32-4). Additionally, hypertrophic lichen planus tends to be highly pruritic, refractory to treatment, and associated with relapse. The primary lesions are thickened, elevated, purple-red, hyperkeratotic plaques and nodules. Verrucal lesions may develop, which can simulate keratinocyte carcinomas, rupioid psoriasis, rupioid syphilis, reactive arthropathy, and cutaneous lupus erythematosus. The lesions of hypertrophic lichen planus may show follicular accentuation, elevation, and chalklike scale. Chronic venous insufficiency is commonly among individuals with hypertrophic lichen planus.
Atrophic Lichen Planus: The atrophic variant of lichen planus is characterized by oligo-lesional disease with well-marginated, blue-white papules or plaques with central atrophy.49 Early lesions are often a few millimeters in diameter but may coalesce into larger plaques. Atrophic lichen planus is most common on the proximal lower extremity and trunk. The two clinical entities in the differential diagnosis are lichen sclerosus et atrophicus and mycosis fungoides (MF). The histopathology may be subtle and has led some to believe that atrophic lichen planus occurs in late-stage resolved disease and is not a true variant of lichen planus.
Vesiculobullous Lichen Planus: Vesiculobullous lesions in lichen planus are rare. They occur secondary to an exuberant inflammatory response and an exaggerated Max-Joseph space. This is in contrast to lichen planus pemphigoides, which has classic lesions of lichen planus separated from lesions of bullous pemphigoid and positive bullous pemphigoid
531
5
antibodies (BP 180 and 230) and immunofluorescence. Vesiculobullous lesions on the skin are more common on the lower extremities (Fig. 32-5) and tend to occur in acute flares of lichen planus. The disease course is similar to that of classic lichen planus. Oral vesiculobullous disease is often symptomatic and leads to erosion and ulceration.
Erosive and Ulcerative Lichen Planus: Erosive and ulcerative cutaneous disease is more common on the feet (Fig. 32-6) and oral cavity and is associated with significant pain and scarring.61 Patients often
532
have other ectodermal involvement, which aids in the diagnosis. Scarring alopecia and loss of the toenails are common. Squamous cell carcinoma (SCC) has been described in chronic lesions of ulcerative oral lichen planus.
Follicular Lichen Planus: Follicular lichen planus may occur alone or in association with other cutaneous or mucosal forms of lichen planus.62 Follicular lichen planus occurs most commonly on the scalp and occurs in three distinct variants, including lichen planopilaris, frontal fibrosing alopecia, and Gram-Little- Piccardi- Lassueur syndrome (GLPLS) (see the discussion of lichen planus of the scalp). Rare reported cases of lichen planus follicularis tumidus, which is characterized clinically by pruritic, red-violet pseudo-tumoral facial and posterior auricular plaques with yellow cysts.63 Lichen planus follicularis tumidus cases often have signs of lichen planus elsewhere. The diagnosis of lichen planus follicularis tumidus should be made with caution and folliculotropic MF, and cutaneous lupus erythematosus should be considered in the differential diagnosis.
Lichen Planus Pigmentosus: Lichen planus pigmentosus is characterized by hyperpigmented, dark-brown macules in sun-exposed and flexural folds (Fig. 32-7). Lichen planus pigmentosus is more common in darker skinned individuals. Histologically, there are epidermal atrophy, a lymphocyte poor LTR, and pigment incontinence. Lichen planus pigmentosus and ashy dermatosis, or erythema dyschromicum perstans, have significant overlapping features and likely represent a phenotypic spectrum based on genetic and environmental factors.
Actinic Lichen Planus: Actinic lichen planus was first described in subtropical countries.64 Actinic lichen planus affects young individuals of Middle Eastern descent and is most common in the spring and summer months.65-68 There is a predilection for the face;
however, the dorsal hands, arms, and nape of the neck are also affected.68 The primary lesions are annular well-marginated, hyperpigmented brown-violet, flattopped, plaques with a slightly rolled border.66 The lesions are minimally symptomatic, and more classic lesions of lichen planus may be seen in non–photoexposed areas. The histopathology is characterized by a more brisk LTR relative to lichen planus pigmentosus, vacuolar changes, and pigment incontinence.68
SITE OF INVOLVEMENT Lichen Planus of the Scalp: Lichen planopilaris, or follicular lichen planus, is a distinct clinical and histologic entity with a female predominance. There are three distinct follicular variants of lichen planus on the scalp, including lichen planopilaris, frontal fibrosing alopecia, and GLPLS. In classic lichen planopilaris, individual keratotic follicular papules form plaques on the scalp with associated scarring alopecia. Classic lichen planopilaris affects the vertex scalp and consists of diffuse erythema with perifollicular hyperkeratosis and livid erythema (Fig. 32-8A).69 Dermoscopy can aid in the diagnosis of early scarring lichen planopilaris. Dermoscopic features of lichen planopilaris include absence of follicular opening, cicatricial white patches, peripilar casts and perifollicular scale, blue-gray dots, perifollicular erythema, and polytrichia (two or three hairs) (Fig. 32-8B).70 Most active lesions are found within the hair-bearing areas at the edge of the alopecic patch. The scarring alopecia may be unilesional or multifocal with severe cases resulting in near-total scalp involvement. Lichen planopilaris, as well as frontal fibrosing alopecia and GLPLS, often has a significant psychological impact on affected individuals. Frontal fibrosing alopecia was once considered an uncommon condition characterized by progressive
5
A
B
C
533
5
frontotemporal recession caused by inflammatory destruction of the hair follicles (Fig. 32-8C). Up to 75% of women with frontal fibrosing alopecia report concomitant loss of the eyebrows, which tends to be noninflammatory.71 The number of cases of frontal fibrosing alopecia has increased dramatically in recent years. Leave-on facial products, including sunscreen, and positive patch test results to fragrances are more common in individuals with frontal fibrosing alopecia.72 Frontal fibrosing alopecia is more common in postmenopausal women but can occur in younger women as well. The disease is characterized by slow progression of frontal hairline recession over years. GLPLS is a rare subtype characterized by cicatricial alopecia of the scalp, nonscarring alopecia of the axilla and groin, and follicular papules on the trunk and extremities.73
Pseudopelade of Brocq is a rare clinical syndrome of scarring alopecia and fibrosis, in which distinct pathologic features are absent. It is generally accepted that pseudopelade of Brocq is the end stage of follicular fibrosis caused by a primary inflammatory dermatosis such as lichen planus, lupus erythematosus, pustular scarring forms of folliculitis, fungal infections, scleroderma, and sarcoidosis.
Mucosal Lichen Planus: Lichen planus can affect any mucosal surface and most commonly involves the mouth or genitalia. Its prevalence is estimated at approximately 1% of the adult population.47
Oral involvement occurs in approximately 60% to 70% of patients with lichen planus and may be the only manifestation in 20% to 30% of patients.49,54,74-76 Multiple types of oral lichen planus have been described, including reticular, plaque-like, atrophic, papular, erosive or ulcerative, and bullous forms (Fig. 32-9). The reticular form of oral lichen planus is the most common and is often asymptomatic. The buccal mucosa is the most common site of involvement followed by the tongue and gingiva. Erosive and ulcerative oral lichen planus is most on the tongue, is extremely painful, and thus is commonly reported in the literature.77 Gingival involvement may take the form of gingival stomatitis
A B
or desquamative gingivitis and is the sole manifestation in 8% of oral lichen planus. On the other hand, oral lichen planus is the most common cause of desquamative gingivitis, accounting for 75% of cases.78
Oral lichenoid reactions (OLRs) are similar clinically and histologically to oral lichen planus; however, with an identifiable cause. Differentiating these two entities clinically is often difficult. OLRs are usually seen on the buccal mucosa adjacent to amalgam dental fillings (Fig. 32-10).79 Patch tests frequently show positive reactions to mercury, gold, and other metals.80-82 Interestingly, patients with an OLR, no cutaneous lichen planus, and negative patch test results often improve with removal of amalgams.83 This brings into question if amalgams are a bona fide hapten response or represent a special site irritant reaction, which leads to koebnerization.84,85
A unique lichenoid eruption has been described on the tongues of individuals with HIV. This reaction is characterized by bilateral reticular keratotic or atrophic changes of the buccal mucosa and lichenoid atrophic patches over the dorsal tongue.86 The eruption usually follows zidovudine or ketoconazole intake and may therefore represent a unique drug hypersensitivity in the setting of immunosuppression. Esophageal lichen planus is rare and most often affects the proximal esophagus. Esophageal lichen planus is most common in middle-aged women.87
Nearly all cases of esophageal lichen planus have preceding or concomitant oral lichen planus.88 Clinical clues of progressive dysphagia and odynophagia in the setting of oral lichen planus should prompt a gastroenterology referral for endoscopy. Endoscopic findings can include lacy white papules, pinpoint erosions, desquamation, pseudomembranes, and stenosis. Esophageal stricture is common and often requires multiple dilations. Histologically, esophageal lichen planus shows parakeratosis, epithelial atrophy, and lack of hypergranulosis.87 Esophageal lichen planus often requires systemic immunosuppression with oral corticosteroids. Malignant transformation has been described; therefore, regular surveillance with gastroenterology is required.87,89
534
Male genitalia are involved in 25% of cases of lichen planus (see Fig. 32-3). The glans penis is most commonly affected with annular lesions. Anal lesions of mucosal lichen planus present with leukokeratosis, hyperkeratosis, fissuring, and erosions (Fig. 32-11). Vulvar and vaginal lichen planus is present in 25% to 60% of patients with oral lichen planus.74,90 Erosive and atrophic disease is most commonly reported in the literature. Clinically, the condition is often asymptomatic unless erosions develop, and then burning, itching, pain, and abnormal discharge become common.91
Clinical examination often shows patches of leukoplakia or erythroplakia, sometimes with erosions, and occasionally, as a more generalized desquamative vaginitis. Vaginal adhesions and labial agglutination may result. Vulvovaginal gingival syndrome is a distinct triad of vulvar, vaginal, and gingival disease. Vulvovaginal gingival syndrome is characterized by erythema and erosions of the gingivae and tongue and desquamation and erosions of vulva and vagina.92
Other cutaneous sites of involvement include skin
5
(40%), scalp (20%), nails (13%), and esophagus (15%).93
Vulvovaginal gingival syndrome is associated with significant long-term sequelae with nearly 90% of individuals developing fibrosis and stricture.93 Class II HLA DBQ1∗0201 allele has been found in 80% of individuals with vulvovaginal gingival syndrome with a relative risk of 3.71.93 Given the multifocal involvement and chronic nature of vulvovaginal gingival syndrome, early institution of aggressive topical and systemic immunosuppression as well as a multidisciplinary approach is needed for optimal outcomes. Conjunctival lichen planus may manifest as cicatricial conjunctivitis. Histologically, irregular thickening with reduplication of the basement membrane is seen. Conjunctival lichen planus often a diagnostic challenge with significant overlap with cicatricial pemphigoid. In cases with severe oral and ocular disease and a lichenoid infiltrate on biopsy, one should also consider paraneoplastic autoimmune multiorgan syndrome and paraneoplastic and cicatricial pemphigoid in the differential diagnosis. Direct immunofluorescence, indirect immunofluorescence, and serologies for autoantibodies are often helpful to distinguish conjunctival lichen planus from cicatricial pemphigoid and paraneoplastic autoimmune multiorgan syndrome.94,95 Longterm sequelae include corneal scarring, symblepharon, blindness, and lacrimal duct stenosis.96
Otic lichen planus is another rare manifestation of lichen planus affecting the external auditory canal and the tympanic membrane. Otic lichen planus is more common in women, often has concomitant disease at multiple body sites, and can lead to progressive hearing loss.97 Otic lichen planus should be considered in the differential diagnosis in a patient with mucosal or cutaneous lichen planus with persistent, unexplained otorrhea or external auditory canal stenosis.
Lichen Planus of the Nails: Nail involvement occurs in 10% to 15% of lichen planus patients.98 Lichen planus limited to the nails is uncommon and, in many cases, is followed by the development of more typical cutaneous or mucosal lesions of lichen planus. Nail involvement in children with lichen planus is rare and affects approximately 5%.50-53 There are three major forms of nail lichen planus: classic nail lichen planus (described later) (Fig. 32-12A), 20-nail dystrophy (Fig. 32-12B), and idiopathic atrophy of the nails. The most common findings of nail lichen planus are diffuse nail involvement with thinning, longitudinal ridging, and distal nail splitting (onychoschizia). Other findings include onycholysis, longitudinal striation with a “sandpaper-like quality” (onychorrhexis), subungual hyperkeratosis, and atrophic or absent nail plates (anonychia). Dermoscopy can aid in the early diagnosis of nail lichen planus because early nail pitting may be present before the development of more classic disease.99 Disease with prominent inflammation can result in nail loss and scarring. Pterygium or forward growth of the eponychia with adherence to the proximal nail plate is a classic finding in nail lichen planus involving the matrix. Dorsal pterygium is an irreversible process and, if present as the primary clinical findings, will likely
535
5
A
B
not improve with treatment. Involvement of the nail bed results in elevation of the nail plate and nail splitting. Trachyonychia, or uniform roughness of the nails, often affects all 20 nails and follows an indolent course. Idiopathic atrophy of the nails is characterized by an abrupt onset and rapidly progressive thinning of the nails with subsequent loss and scarring with or without dorsal pterygium. The latter two forms of nail lichen planus are more common in children.100 The differential diagnosis of isolated nail lichen planus includes psoriasis, alopecia areata, atopic dermatitis, and rarely immunobullous diseases.
Inverse Lichen Planus: The inverse pattern of lichen planus is rare and is characterized by red-brown, discrete papules and flat-topped plaques. Inverse lichen planus commonly affects the flexural areas, including the axillae, inframammary region, and groin. The antecubital and popliteal areas may be rarely involved. The findings of inverse lichen planus are often isolated and involvement of other ectodermal-derived tissues is uncommon. Inverse lichen planus has been most commonly reported in whites, Asians, and recently Tunisians.101 Unlike lichen planus pigmentosus, there is an absence of
536
involvement in sun-exposed areas, and some prefer the term lichen planus pigmentosus inversus.
Palmoplantar Lichen Planus: Palmoplantar lichen planus is a rare, difficult-to-diagnose form of lichen planus. Approximately 25% of individuals with palmoplantar lichen planus have other areas of cutaneous involvement, most commonly on the anterior shin and malleoli in those with plantar disease.102 Palmoplantar lichen planus is characterized by pruritic, red-purple, scaly plaques with or without hyperkeratosis. Because of the thickness of palmar and plantar skin, Wickham striae are absent. Four patterns of palmoplantar lichen planus are seen: plaque type, punctate, diffuse keratoderma, and ulcerated. Lesions are commonly seen on the internal plantar arch on the feet (see Fig. 32-5) and the thenar and hypothenar eminence on the hands (Fig. 32-13). Yellow, compact keratotic papules or papulonodules are seen on the lateral margins of the fingers and hand surfaces. Involvement of the fingertips is uncommon and, if present, raises the possibility of a primary or concomitant dermatitis. The lesions often appear callus-like with a faint purple hue and an inflammatory halo. The differential diagnosis includes psoriasis, warts, calluses, porokeratosis, hyperkeratotic dermatitis or eczema, tinea, or secondary syphilis.
SPECIAL FORMS Drug-Induced Lichen Planus: Lichen planus–like or lichenoid drug eruptions are a group of cutaneous reactions identical or similar to lichen planus. Lichenoid drug eruptions have been reported after ingestion, contact, or inhalation of certain chemicals (Table 32-2).103 They may be localized or generalized with eczematous papules and plaques. The degree of desquamation is variable. They often manifest with hyperpigmentation and alopecia. Wickham striae are rare. The eruption is often symmetrical on the trunk and extremities with less common flexural
Most Likely
■Gold salts
■β-Blockers
■Antimalarials
■Diuretics (thiazides, furosemide, spironolactone)
■Penicillamine
■Immune checkpoint inhibitors (pembrolizumab, nivolumab, ipilimumab)
Less Likely
■Angiotensin-converting inhibitors
■Calcium channel blockers
■Sulfonylurea
■Nonsteroidal antiinflammatory drugs
■Ketoconazole
■Tetracycline
■Phenothiazine
■Sulfasalazine
■Carbamazepine
■Lithium
■Antituberculosis agents
■Iodides
■Radiocontrast media
■Radiotherapy
■Antipsoriatic therapy: etanercept, infliximab, adalimumab
■TNFα inhibitors (etanercept, infliximab, adalimumab, certolizumab)
Contact Inducers of Lichen Planus
■Color film developers
■Dental restoration materials
■Musk ambrette
■Nickel
■Gold
Photo Inducers of Lichen Planus and Lichenoid Drug Eruption
■5-Fluorouracil
■Carbamazepine, chlorpromazine, diazoxide
■Ethambutol
■Pyritinol
■Quinine
■Quinidine
■Tetracycline
■Thiazide
■Furosemide
Inducers of Oral Lichen Planus and Lichenoid Drug Eruption
Inducers of Oral Lichen Planus and Lichenoid Drug Eruption
■Allopurinol
■Allopurinol
■Angiotensin-converting inhibitors
■Angiotensin-converting inhibitors
■Cyanamide
■Cyanamide
■Dental restoration materials
■Dental restoration materials
■Mercury, silver, gold
■Mercury, silver, gold
■Ketoconazole
■Ketoconazole
■Nonsteroidal antiinflammatory drugs
■Nonsteroidal antiinflammatory drugs
■Penicillamines
■Penicillamines
■Sulphonylureas
■Sulphonylureas
■Interferon-α and ribavirin
■Interferon-α and ribavirin
involvement (Fig. 32-14). Involvement of the mucous membranes is rare and is associated with specific drugs and chemicals. A photodistributed pattern is implicated with specific drugs and chemicals as well. One new class of drugs with a high rate of lichenoid drug eruption is immune checkpoint inhibitors, ipilimumab, pembrolizumab, and nivolumab, which target
5
A
B
CTLA-4 and programmed cell death-1. Lichenoid drug eruptions are some of the most common side effects with this drug class, affecting 17% of patients.104,105
The latency period for the development of a lichenoid drug eruption varies from months to more than 1 year.
537
5
The time of onset depends on the dosage, host response, previous exposure, and concomitant drugs. The resolution of the lichenoid drug eruption is variable, and most resolve in 3 to 4 months. Exceptions are gold-induced lichenoid drug eruption, which can require years for resolution. For many drugs, the severity and extent of disease affect the rate of clearance. Occasionally, the lichenoid drug eruption may intermittently recur. Genetic susceptibility is likely important, especially in recurrent cases and cases involving immune- modulating drugs, such as INF-α, ipilimumab, pembrolizumab, and nivolumab. Lichenoid contact dermatitis may result from contact with compounds such as color film developers, dental restorations, amalgams (silver, mercury, gold), and aminoglycosides (see “Mucosal Lichen Planus”).106,107
Oral lichenoid eruptions are most commonly related to dental restorations metals such as mercury, silver, and gold.79-81,108
Lichen Planus–Lupus Erythematosus Overlap: This rare variant of lichen planus is characterized by features of lichen planus and lupus erythematosus.109,110 Lesions of lichen planus–lupus erythematosus overlap are red-violet, atrophic patches and plaques with hypopigmentation, telangiectasia, and minimal scale. The dorsal aspect of the extremities, specifically the hands and nails, are most commonly affected and patients often develop anonychia (Fig. 32-15). Classic features of lichen planus and lupus erythematosus are absent. Some individuals go on to
538
develop systemic lupus erythematosus. Laboratory studies may find a weakly positive antinuclear antibody, and traditional histology and immunofluorescence show overlapping features of lichen planus and lupus erythematosus. The disease course of lichen planus–lupus erythematosus overlap is often prolonged and refractory to treatment.
Lichen Planus Pemphigoides: Lichen planus pemphigoides has features of lichen planus and bullous pemphigoid (Fig. 32-16). The pathogenesis is unclear but is believed to result from the liquefactive degeneration of keratinocytes caused by a brisk LTR and the subsequent exposure of autoantigens, which result in antibody formation. Some have argued that lichen planus pemphigoides is simply lichen planus and bullous pemphigoid in coexistence. However, there are key clinical and serologic features that differentiate true lichen planus pemphigoides from concomitant lichen planus and bullous pemphigoid. First, lichen planus commonly affects individuals in the fifth to seventh decades of life and bullous pemphigoid most commonly after the seventh decade, but lichen planus pemphigoides is most common in younger individuals in the four to fifth decades of life. Additionally, lichen planus pemphigoides blisters may occur on top of lichenoid lesions as well as normal-appearing skin.
The prognosis of lichen planus pemphigoides is good and is response to conventional therapy.111 Last, the Medical College of Wisconsin domain 4 (MCW-4) of bullous pemphigoid antigen 180 (BPAG180) appears to be unique for lichen planus pemphigoides.112 The major consideration in the differential diagnosis is bullous lichen planus, which can be differentiated on serologies and immunofluorescence. Drug-induced lichen planus pemphigoides has been described.113
Keratosis Lichenoides Chronica (Nekam Disease): Keratosis lichenoides chronica (KLC), or Nekam disease, is a rare dermatosis that has distinct clinical and histologic features. Clinically, KLC is distinct from lichen planus and is characterized by lichenoid, keratotic papules and plaques in a seborrheic distribution with characteristic linear or reticulate pattern.114 Additional sites of involvement include the palms and soles. The individual lesions tend to be folliculo- and infundibulocentric. The eruption is often asymptomatic and refractory to treatment. Histologically, KLC is characterized by a brisk LTR and often shows parakeratosis with neutrophils in the crust.115 The diagnosis of KLC should be made with caution because other diseases such as lichen planus, lichen simplex, and lupus erthematosus (LE) may manifest a similar reaction pattern.115
Lichenoid Graft versus Host Disease: Chronic GVHD is traditionally considered that occurring 100 days after transplant and may manifest as a dermatitic, sclerodermoid, or lichenoid eruption, which can be indistinguishable from lichen planus. A newer consensus definition of GVHD focuses in on both clinical and chronological features, including classic acute GVHD, persist, recurrent, or lateonset acute GVHD occurring after 100 days, classic chronic GVHD, and overlap syndromes.116 GVHD is caused by immunocompetent donor cells attacking fast dividing tissue such as the liver, gastrointestinal tract, and skin. Although the mechanism is incompletely understood, the various forms of GVHD appear to be pathogenically distinct. Because there is a better understanding of GVHD relative to lichen planus and a clear driver of an autoantigen stimulating an allogeneic immune response, we will discuss the mechanism briefly. Whereas acute GVHD is driven by Th2 cytokine signaling, chronic GVHD is driven by Th1/ Th17 signaling and increased numbers of IFN-γ– and IL-17–producing cytotoxic CD8-positive T cells.117 Supporting this theory, mice deficient of IL-17 receptors are unable to develop GVHD.118 Additionally, exciting new research with therapeutic potential points to the possible role of IL-17 blockade in the transdifferentiation of Th17 cells into CD4-positive T-regulatory cells.119 Similar targets may be useful in refractory lichen planus. Clinically, lichenoid GVHD is characterized by classic lichenoid papules with prominent follicular involvement of the head and neck as well as oral involvement.120 Onycholysis and cicatricial alopecia may be prominent features. Histopathologically,
5
lichenoid GVHD is often indistinguishable from lichen planus; however, satellite cell necrosis, plasma cells, and eosinophils may be subtle clues to the diagnosis.121
Lichenoid Keratosis: Lichenoid keratosis often consists of a single, nonpruritic, brown to red, scaling flat-topped plaque on sun-exposed skin of the extremities.122 Lichenoid keratosis is easily differentiated clinically from lichen planus. These lesions can be histologically identical to lichen planus; however, they may have some differentiating features such as parakeratosis or a remnant lentigo, seborrheic keratosis, or actinic keratosis.
Lichenoid Dermatitis: Lichenoid dermatitis describes a reaction pattern with nonclassic lichenoid features as well as spongiosis. A study of 62 patients with lichenoid dermatitis had an alternative diagnoses with further clinical, serologic, and histopathological analysis. The differential diagnosis of lichenoid dermatitis includes dermatitis, drug eruption, lupus erythematosus, lichen planus, and cutaneous T-cell lymphoma.123 Additional features, specifically granuloma formation, expand the differential diagnosis to include drug eruptions (including pseudolymphoma in 31%), hepatobiliary disease, endocrinopathy ( diabetes mellitus and thyroiditis), rheumatoid arthritis, Crohn disease, and infection (in 28%).124
RELATED FINDINGS
See Table 32-3. Lichen planus is associated with liver diseases such as autoimmune chronic active hepatitis, primary biliary cirrhosis (PBC), and postviral chronic, active hepatitis. The association of PBC is observed regardless of the use of penicillamine. Hepatitis C virus (HCV) and lichen planus are associated in certain endemic regions (East and Southeast Asia, South America, the Middle East, and Southern Europe) but not in others (North America, South Asia, and Africa).125,126 The prevalence of HCV is 16% to 29% in
Hepatitis C virus Autoimmune chronic active hepatitis Primary biliary cirrhosis Postviral chronic, active hepatitis Dyslipidemia Metabolic syndrome Hypothyroidisma
Hepatitis C virus Autoimmune chronic active hepatitis Primary biliary cirrhosis Postviral chronic, active hepatitis Dyslipidemia Metabolic syndrome Hypothyroidisma
Lichen sclerosus et atrophicusb
Lichen sclerosus et atrophicusb
Systemic lupus erythematosus Sjögren disease Dermatomyositis Vitiligo Alopecia areata
Systemic lupus erythematosus Sjögren disease Dermatomyositis Vitiligo Alopecia areata
539
aLichen planopilaris.
bOral lichen planus.
5
southern European patients with lichen planus.127,128 In patients with oral lichen planus and liver disease, there are significantly higher rates of HCV in selected populations (78% versus 3%). There is no clear association of HCV with pure cutaneous lichen planus.129 There may be specific unidentified genetic factors contributing to this co-occurrence because large studies on HCV have not found lichen planus to be a common finding.130 The heterogeneity of HCV and oral lichen planus may be related to the human leukocyte antigen-DR6 (HLA- DR6) haplotype, which is found in endemic regions of both diseases.131,132 There is no strong link between hepatitis B virus (HBV) and lichen planus.133
Patients with lichen planus have been reported to have higher rates of dyslipidemia and to harbor more cardiac risk factors than healthy individuals.134-136
Metabolic syndrome appears to be more common in individuals with oral lichen planus.137 Thyroid dysfunction, most commonly hypothyroidism, is found in up to 34% of patients with lichen planopilaris.138 Lichen sclerosus et atrophicus is seen in up to 16% of patients with oral lichen planus; however, there is no associated risk of oral lichen planus in individuals with lichen sclerosus et atrophicus.90,139 Recent population studies have found an association between lichen planus and autoimmune diseases, including systemic lupus erythematosus, Sjögren disease, dermatomyositis, vitiligo, and alopecia areata, in the Taiwanese population.140
Cases of lichen planus in association with internal malignancy may represent a manifestation of paraneoplastic autoimmune multiorgan syndrome.
MALIGNANT TRANSFORMATION
There has been considerable controversy as to whether oral lichen planus inherently harbors malignant potential.77,141 It is currently believed that the risk of malignant transformation is low. Risk factors that increase the likelihood of developing oral cancer are long-standing disease, erosive or atrophic types, tobacco use, and possibly esophageal involvement. Additionally, oncogenic subtypes of HPV, including type 16, are more common in oral lichen planus and may account, in part, for the malignancy risk.142
The reported rates of SCC development have varied: 0.8% of oral lichen planus in the United States, 1.9% in the United Kingdom, 0.6% in China, and 1% in the Swedish population.77,143-145 The majority of these cases are in situ carcinoma or with a microinvasive pattern. The most common site for cancer is the tongue (Fig. 32-17) followed by the buccal mucosa, gingiva, and, rarely, the lip. Clinically, the lesions appear as indurated, nonhealing ulcers or exophytic lesions with a keratotic surface. Red atrophic plaques could also be seen and often correlate with in situ disease. Advanced cases may result in nodal metastases and even death. No overall increased risk of malignancy has been observed in cutaneous lichen planus.145 There are rare case reports of cutaneous SCC arising in long-standing
540
lesions of lichen planus. Risk factors include: hypertrophic or verrucous lichen planus, location on the lower extremity, a history of arsenic or x-ray exposure, and long-standing disease (average, 12 years).145
DIAGNOSIS
The diagnosis of lichen planus is largely clinical. However, in cases with atypical or overlapping clinical features, a histopathologic diagnosis may be required. In cases of vesiculobullous disease or erosive disease, immunofluorescence (DIF), indirect immunofluorescence (IIF), and enzyme-linked immunosorbent assay (ELISA), may be needed to differentiate from immunobullous diseases. Laboratory testing is not required and is largely focused in upon associated morbidities and should be part of age-specific screening for risk reduction of diseases such as thyroid and cardiac disease.
SUPPORTIVE STUDIES
SUPPORTIVE STUDIES
LABORATORY TESTING
See Table 32-4. No specific abnormalities of laboratory analyses are seen in lichen planus. The total white blood cell count and lymphocytes may be decreased. This could be related to cytokine activation and local trafficking of cells to skin or other tissue compartments. In cases of oral disease, allergic contact dermatitis should be ruled out because oral contact stomatitis can appear identical to lichen planus.80,146-148 Sensitivity to mercury, gold, chromate, flavoring agents, acrylate,
Complete blood count Patch testinga
Complete blood count Patch testinga
Lipid panel Thyroid function testsb
Lipid panel Thyroid function testsb
Antithyroid peroxidase antibodies Antithyroglobulin antibodies Hepatitis C virus testingc
Antithyroid peroxidase antibodies Antithyroglobulin antibodies Hepatitis C virus testingc
aParticularly for oral lichen planus.
bFor lichen planopilaris.
cFor endemic areas; oral lichen planus.
and thimerosal are common sensitizers. Avoidance of these clinically relevant sensitizers results in amelioration of disease. Dyslipidemia is more common in patients with lichen planus compared with control participants and should be tested as part of normal, preventative care.134,135,137,149 Additionally, in cases of lichen planopilaris, one should consider testing for associated thyroid abnormalities, including thyroid-stimulating hormone, antithyroid peroxidase antibodies, and antithyroglobulin antibodies.138
HCV testing is controversial in lichen planus and testing should be considered in those with oral disease, risk factors for HCV (elevated liver function, intravenous drug use, a history of blood transfusion prior to 1992, and high risk sexual behaviors) as well as those in endemic areas (East and Southeast Asia, South America, the Middle East, and Southern Europe) having a prevalence of greater than 7%.150
PATHOLOGY
The two major pathologic findings in lichen planus are basal epidermal keratinocyte damage and a lichenoidinterface lymphocytic reaction. Classic changes are seen in established cutaneous lesions.151 Classic lichen planus is characterized by a dense, continuous, and bandlike lymphohistiocytic infiltrate at the DEJ (Fig. 32-18). The heavy infiltrate can result in effacement of the DEJ. Parakeratosis and eosinophils are absent. The epidermal changes include hyperkeratosis, wedge-shaped areas of hypergranulosis, and elongation of rete ridges that resemble a sawtooth pattern. Multiple apoptotic cells or colloid-hyaline (Civatte) bodies are seen at the DEJ. Eosinophilic colloid bodies are present in the papillary dermis. Eosinophils are absent in classic lichen planus and are seen in two thirds of lichenoid drug eruptions and are seen in significant numbers in 20.6% of cases of hypertropic lichen planus.152-154 Melanin pigmentation is invariably present and is more pronounced in older, waning lesions in dark-skinned individuals and lichen planus pigmentosus. Separation of the epidermis in small clefts (Max Joseph cleft formation) is seen in 20% of cases. Late disease is characterized by an atrophic epidermis, effacement of the rete ridges, occasional colloid
5
A
B
bodies, dermal fibrosis, and melanophages. When few colloid bodies are present, distinguishing from poikiloderma may be very difficult. Hypertrophic lichen planus is characterized by hyperkeratosis, acanthosis, papillomatosis, and thickened collagen bundles in the dermis (Fig. 32-19). Hypertrophic lichen planus can be mistaken for SCC; therefore, good clinical pathological correlation is needed to avoid inappropriate treatment.155 As mentioned earlier, eosinophils are more commonly seen in hypertrophic lesions.152
Mucosal lesions tend to have less specific changes, and genital disease can often be inconclusive. Parakeratosis and an absent granular layer are common at mucosal sites, and plasma cells are often prominent. Lichen planopilaris is characterized by a perifollicular, lymphohistiocytic inflammatory reaction with perifollicular fibrosis, scarring, and follicular atrophy. The initial inflammation is at the level of the isthmus and infundibulum and spares the lower segment.156
541
5
A
B
DIF studies are focused on oral disease and show a positive finding in 62% to 75% of cases with numerous apoptotic cells at the DEJ (60%) staining with immunoglobulin M (IgM) and, occasionally, with IgG and IgA (Fig. 32-20).157 Shaggy deposition of fibrinogen at the DEJ is seen in 55% to 70% of cases.157,158 The criterion for lichen planus requires basement membrane zone fibrinogen and colloid bodies with one or more conjugate(s) (Mayo Clinic criteria).157 Multiple immunoglobulin (IgG, A, and M) conjugates and granular, basilar deposition of immunoglobulins are more common in LE, and the diagnosis of lichen planus should be suspect when multiple conjugates are present.159
DIF of oral lichen planus (sensitivity of 61% and specificity of 96%) is inferior to both hematoxylin and eosin (sensitivity of 84% and specificity of 93%) and clinical impression (sensitivity of 74% and specificity of 87%).157 These findings emphasize the importance of clinical examination and routine histology in classic lichen planus. DIF has a role in atypical disease and is a
542
A
B
prerequisite for the diagnosis of ulcerative and vesiculobullous lichen planus variants. The location of the biopsy is critically important in lichen planus and varies by lichen planus subtype. The optimal location for biopsy of cutaneous lichen planus is on the proximal trunk with avoidance of the distal extremities.158 Dermoscopic-driven biopsies of lichen planopilaris showing the key features of perifollicular erythema and scaling led to definitive diagnosis in 95% of cases.160 Biopsies for nail disease should be guided by dermoscopy and should focus on the underlying structures involved. The presence of trachyonychia and pitting should guide a matrix biopsy, chromonychia, nail plate fragmentation, splinter hemorrhage, onycholysis, and subungual debris should guide a nail bed biopsy.99 For DIF, the highest
sensitivity is on the mouth floor and the ventral side of the tongue. The oral biopsy specimen for DIF may be taken up to 1 cm from the lesion (including glabrous skin) without a decrease in sensitivity and should not be split.158,161,162
DIFFERENTIAL DIAGNOSIS
The differential diagnosis of lichen planus is quite broad. A more practical approach is to look at the age of the individual, morphology of the primary lesion, and site of involvement (Table 32-5).
CLINICAL COURSE AND PROGNOSIS
Most cutaneous lichen planus resolves within one to 2 years and may be associated with relapses. Recurrence is seen in up to 20% of cases but is more common in generalized cutaneous disease.54,163 The duration of disease depends on the extent and site of involvement. In general, generalized disease tends to resolve more quickly. Disease duration, in ascending order, is generalized cutaneous, nongeneralized cutaneous,
Morphology and Age Classic: psoriasis, lichenoid drug eruption, lichen simplex chronicus, chronic cutaneous lupus, graft-versus-host disease, secondary syphilis, pityriasis rosea, mycosis fungoides Annular: granuloma annulare, tinea corporis Linear: nevus unius lateris, lichen striatus, linear epidermal nevus, psoriasis, Darier disease Hypertrophic: lichen simplex chronicus, prurigo nodularis, lichen amyloidosis, Kaposi sarcoma, squamous cell carcinoma, psoriasis Atrophic: lichen sclerosus, cutaneous lupus erythematosus, poikiloderma, mycosis fungoides, morphea Vesiculobullous: lichen planus pemphigoides, epidermolysis bullosa pruriginosa, pemphigus vulgaris, bullous pemphigoid, bullous amyloidosis Follicular: lichen nitidus, lichen spinulosa, follicular psoriasis, pityriasis rubra pilaris Childhood: lichen nitidus, lichen striatus, pityriasis lichenoides, papular acrodermatitis of childhood, annular lichenoid dermatitis of youth, mycosis fungoides, frictional lichenoid eruption
Special Sites Nail: psoriasis, onychomycosis, alopecia areata, atopic dermatitis Genital: psoriasis, seborrheic dermatitis, fixed drug eruption Palms and soles: secondary syphilis, erythema multiforme Scalp: cicatricial alopecia, lupus erythematosus, inflammatory
Special Sites Nail: psoriasis, onychomycosis, alopecia areata, atopic dermatitis Genital: psoriasis, seborrheic dermatitis, fixed drug eruption Palms and soles: secondary syphilis, erythema multiforme Scalp: cicatricial alopecia, lupus erythematosus, inflammatory folliculitis, alopecia areata, cicatricial pemphigoid, keratosis follicularis spinulosa decalvans Mucosal: pemphigus vulgaris, cicatricial pemphigoid, bullous pemphigoid, epidermolysis bullosa acquisita, paraneoplastic autoimmune multiorgan syndrome or paraneoplastic pemphigus, candidiasis, lupus erythematosus, leukokeratosis, secondary syphilis, traumatic patches, chronic ulcerative stomatitis, erythema multiforme
folliculitis, alopecia areata, cicatricial pemphigoid, keratosis follicularis spinulosa decalvans Mucosal: pemphigus vulgaris, cicatricial pemphigoid, bullous
pemphigoid, epidermolysis bullosa acquisita, paraneoplastic autoimmune multiorgan syndrome or paraneoplastic pemphigus, candidiasis, lupus erythematosus, leukokeratosis, secondary syphilis, traumatic patches, chronic ulcerative stomatitis, erythema multiforme
5
cutaneous and mucosal, mucosal, hypertrophic, and lichen planopilaris.164 The mean duration of oral disease is 5 years, and hypertrophic and scalp disease are often unremitting. In higher Fitzpatrick skin types, postinflammatory changes manifest as significant, persistent pigmentary abnormalities.
TREATMENT
The treatment of lichen planus is challenging and discouraging for both physicians and patients. Because of its ability to affect multiple ectodermal-derived tissues, lichen planus may require a multidisciplinary approach with dermatologists, dentists, gynecologists, and occasionally otolaryngologists, gastroenterologists, and ophthalmologists. The goal of therapy is to minimize morbidity and improve the patient’s quality of life. Treatment options and the potential risks of therapy should be weighed against the extent and severity of disease. Potentially exacerbating drugs should be discontinued, trauma minimized, and microbial overgrowth reduced. The basic concepts in the treatment of lichen planus have remained largely unchanged over the past decade. The therapies are mainly divided into skindirected and systemic agents. The therapies for various ectodermal tissues are also similar. Nearly all of these agents act in a manner to suppress the immune response. To date, there are no disease-specific medications for lichen planus. However, Janus kinase (JAK) inhibitors target CD8-Tc cells and represent a potential, disease-specific treatment of lichenoid diseases, including lichen planus.165 JAK inhibitors have been successful in treating refractory dermatomyositis, alopecia areata, and vitiligo.166-168 This section provides a brief overview of the general approach to therapy for lichen planus and its variants of lichen planus.
CUTANEOUS LICHEN PLANUS
CUTANEOUS LICHEN
PLANUS
SKIN-DIRECTED THERAPIES Topical Corticosteroids: Despite few clinical trials, high-potency topical corticosteroids are considered first-line therapy for limited cutaneous lichen planus. Occlusion may be necessary to increase penetration in cases of hypertrophic lichen planus. The sole randomized controlled trial in cutaneous lichen planus comparing calcipotriene to betamethasone valerate (twice daily for 12 weeks) found no difference between treatments.169 If no response is observed with twice daily application for 2 to 4 weeks, changing to a higher potency corticosteroid or intralesional injections should be considered.170
Topical Calcineurin Inhibitors: There are no trials using topical calcineurin inhibitors in cutaneous lichen planus. However, clinical data in oral lichen
543
5
planus suggest that topical calcineurin inhibitors may be the most effective topical therapy for lichen planus. Application of tacrolimus 0.1% ointment is as effective as 0.05% clobetasol.171 Because of cost, topical calcineurin inhibitors are a second-line topical agent and are often used in conjunction with topical steroids in refractory cases of limited cutaneous lichen planus. The combination of topical corticosteroids and calcineurin inhibitors often allows one to taper topical corticosteroids and minimize the possibility of steroid atrophy. Intralesional Corticosteroids: Intralesional corticosteroids (5 to 10 mg/mL injected on a monthly basis) can be highly effective in resistant and hypertrophic lichen planus. However, one should use caution to prevent excessive trauma to avoid Koebnerization. Because of the risk of relapse, intralesional corticosteroids should always be combined with topical therapy or an additional corticosteroid-sparing agent. Phototherapy: Phototherapy has been used successfully in many inflammatory diseases of the skin. Ultraviolet B (UVB) exposure of dendritic cells (DCs) impairs their interaction with T cells, alters cytokine expression, and leads to T-cell suppression and apoptosis.172,173 UVB three times weekly until remission with taper after remission over 3 to 6 weeks has a 70% remission rate, and 85% of the patients remained in remission at 34 months.174 A short course of oral corticosteroids in combination with UV light therapy is highly effective for generalized cutaneous lichen planus. Narrow-band UVB (311 nm) is as effective in lichen planus and has largely supplanted UVA, psoralen plus UVA (PUVA), and UVB phototherapy.175
SYSTEMIC THERAPIES
Systemic medications are often needed for severe, more protracted lichen planus. Oral corticosteroids are often first systemic treatments. Second-line, corticosteroid-sparing agents are sulfasalazine, metronidazole, acitretin, antimalarials (hydroxychloroquine and chloroquine), methotrexate, mycophenolate mofetil (MMF), and azathioprine (less preferred second-line agent). Because of its side effect profile, cyclosporine is considered a third-line corticosteroid-sparing agent. Within the second-line agents, particular agents are more effective for specific variants of lichen planus, which is outlined later. In general, drugs that target lymphocytes more specifically (methotrexate, MMF, and azathioprine) are of higher utility in refractory and ulcerative disease, but drugs acting indirectly on lymphocytes (sulfasalazine and metronidazole) or cellular differentiation (acitretin) are more effective for generalized disease and hypertrophic disease, respectively. Systemic Corticosteroids: Systemic corticosteroids for cutaneous lichen planus have only been reported in one study with a 90% response rate and 32% relapse rate at 6 months.176 Lichen planus is often responsive to 0.3 mg/kg to 1 mg/kg of oral prednisone within 4 to 6 weeks of treatment and requires a
544
4- to 6-week taper. In our clinical experience, systemic corticosteroids are highly effective and serve a role in attaining rapid disease control but are associated with high rates of relapse upon discontinuation. Therefore, oral should always be combined with topical therapy or an additional corticosteroid-sparing agent. Long-term monotherapy with oral corticosteroids is not recommended.
Sulfasalazine: Sulfasalazine (initial dose, 1 g/day with an increase every 3 days by 0.5 g to a maximum of 2.5 g/day) has the highest level of evidence of efficacy for lichen planus with an 83% improvement in skin lesions of generalized lichen planus and a 91% improvement in itch at 6 weeks in the therapy group.177,178 Agranulocytosis and elevated liver function tests can occur with sulfasalazine; therefore, it is important to monitor these laboratory tests during drug initiation.
Metronidazole: An open-labeled study of oral metronidazole (250 mg three times daily for 12 weeks) showed a 74% response rate at 3 months of follow-up.179
Alternate dosing (500 mg twice daily for 20 to 60 days) has also been reported to be successful.180 In our experience, metronidazole is more effective in generalized cutaneous lichen planus. Because of its side effect profile, metronidazole is often considered the first-line nonimmunosuppressive systemic agent; however, one should caution patients as well as monitor for possible sensory peripheral neuropathy.181
Acitretin: A double-blind, placebo-controlled trial of acitretin (30 mg/day for 8 weeks) showed marked improvement in 64% of individuals.182 Mucocutaneous side effects and hyperlipidemia were common. In our experience, acitretin is highly effective for hypertrophic lichen planus. Topical retinoids are of limited value in cutaneous lichen planus.
Antimalarials: Chloroquine has been reported effective in cutaneous lichen planus.183,184 Hydroxychloroquine has been reported effective in oral lichen planus, lichen planopilaris, and actinic lichen planus.185-190 However, given its favorable side effect profile, hydroxychloroquine (200 to 400 mg [up to 6.5 mg/kg ideal body weight] for 6 to 12 months) is often used as a second-line agent in cutaneous lichen planus and the first-line agent in actinic lichen planus.
Methotrexate: Methotrexate has been shown to be of benefit for more recalcitrant disease as well as in specific forms of disease, including hypertrophic lichen planus and lichen planopilaris. Recent, nonrandomized, prospective data have shown methotrexate (15 to 20 mg weekly for 4 to 24 weeks) to be highly efficacious with complete responses in 58% to 91% of cases.191-193 Methotrexate is useful and cost effective and is a preferred second-line systemic agent.
Mycophenolate Mofetil and Azathioprine: Both oral MMF and azathioprine are used commonly in refractory cutaneous lichen planus. MMF, 2 to 3 g/day in divided doses is effective in refractory
cases; however, the clinical responses are delayed and adjuvant oral corticosteroids are often required during initiation.194 Azathioprine has been reported effective in refractory lichen planus; however, because of its suppressive effects on T and B lymphocytes and its tolerability issues, we reserve this as a less preferred second-line agent.195
Cyclosporine: Cyclosporine has been reported effective at doses of 3 to 10 mg/kg/day; however, lower doses of 1.0 mg/kg/day to 2.5 mg/kg/day are likely to achieve disease remission.196 Frequent relapses of lichen planus after discontinuation of cyclosporine, as well as its long-term side effects, limit its use in chronic lichen planus.
Other Therapies: TNF-α inhibitors, apremilast, trimethoprim–sulfamethoxazole, griseofulvin, itraconazole, terbinafine, tetracyclines, laser, IFN, alitretinoin, thalidomide, and low-dose heparin have also been reported.
ORAL LICHEN PLANUS
ORAL LICHEN PLANUS
The cornerstone of treatment in oral lichen planus is good oral hygiene with regular professional dental cleanings.197 Minimizing other exacerbating factors such as contact allergens, drug reactions, reducing oral microbes, and minimizing trauma can reduce disease severity as well as frequency of flares. Replacement of dental amalgams and gold dental restorations can be beneficial, even in patients with negative patch testing results.84,85 Gingival lesions may respond less favorably. However, removal and restoration should be individualized based on the severity of disease as well as the index of suspicion of the level of involvement of the metal or prosthesis.
SKIN-DIRECTED THERAPIES Topical Corticosteroids: Topical steroids are first-line therapy in oral lichen planus with overall clinical responses on the order of 70% to 80%. The use of occlusive materials, such as Orabase, may alleviate pain associated with ulcerative lesions. Although few direct comparisons between topical corticosteroids in lichen planus exist, the most beneficial are likely: 0.1% triamcinolone acetonide in Orabase, 0.025% to 0.05% clobetasol-17-propionate in Orabase, and 0.1% fluocinonide gel.198,199 However, only clobetasol and fluocinonide have demonstrated a clear benefit over placebo.200 Higher potency corticosteroids as well as more occlusive preparations lead to faster healing times.201-203 However, the clinician and patient must weigh the benefit of an occlusive ointment or Orabase with the difficulty of application and potential for noncompliance. In general, topical corticosteroids should be applied two to six times daily based on the severity of disease. One therapeutic approach is to initiate high to ultrapotent steroid gel three times daily after meals
5
to all affected areas followed by tacrolimus ointment twice daily. The corticosteroids are tapered every 2 to 4 weeks to a maintenance dose of two to three times weekly, and tacrolimus is continued twice daily. The major complications of topical corticosteroids are fungal infections and, in general, higher rates of fungal infections are seen with more potent topical corticosteroids. Therefore, concomitant therapy with oral chlorohexidine gluconate mouthwash, topical anticandidal medications, or prophylactic oral fluconazole is recommended.202,204
Topical Calcineurin Inhibitors: Pimecrolimus 1% cream is effective in curing the erosive lesions of oral lichen planus but is ineffective at symptomatic control.198,205 Meta-analysis has found tacrolimus 0.1% ointment one to four times daily to be more effective than clobetasol propionate ointment.198 Cyclosporine in various preparations has been found to be less effective than both clobetasol and triamcinolone.198,206
Because of cost, commercially available calcineurin inhibitors and increasing restrictions on compounding, we would recommend topical cyclosporine as a third-line topical agent. Transient burning with usage of topical calcineurin inhibitors is common and overlap therapy with topical corticosteroids may alleviate the burning sensation.
Retinoids: Topical tretinoin 0.05% to 0.1% gel applied twice daily may be effective in oral lichen planus; however, because of issues of irritation, this is a third-line topical agent and is often used in conjunction with topical corticosteroids.207,208
Intralesional Corticosteroids: Intralesional triamcinolone 0.5 mL of 40 mg/mL on a weekly basis for 4 weeks is effective in oral lichen planus.209 More dilute concentrations, 10 mg/mL, injected every 1 to 4 weeks, in conjunction with topical corticosteroids, is highly effective. However, because of the discomfort of injection and few well-controlled studies, intralesional therapies are reserved after exhausting topical therapies.
SYSTEMIC THERAPIES
The approach to systemic therapies in oral lichen planus is similar to that of cutaneous disease. A few exceptions are the larger reported series of MMF and hydroxychloroquine in refractory oral lichen planus, the efficacy and dual benefit of oral acitretin, and the high levels of iatrogenic candida infections. In general, the hierarchy of therapy is the same; however, one should always consider the increased risk of oral SCC in erosive and refractory oral lichen planus and more heavily weigh the risks of immunosuppression against the benefits of disease control. Based on this, drugs such as acitretin, with its antiproliferative effects, and less immunosuppressive agents such as hydroxychloroquine and methotrexate are preferred.
Oral Corticosteroids: Systemic steroids are one of the most effective treatment for oral lichen planus and can provide rapid improvement in acute exacerbations.
545
5
However, there are no randomized clinical trials for systemic corticosteroids. Both clinical experience as well as prospective studies indicates that oral corticosteroids 1.5 to 2 mg/kg tapered over 3 to 6 weeks are highly effective.210,211 Based on evidence in other erosive and blistering dermatologic diseases, doses greater than 1 mg/kg of corticosteroids add little clinical benefit and dramatically increase side effects. Studies using pulsed betamethasone, 5 mg on 2 consecutive days weekly for 3 months, showed a more rapid response but no clear long-term advantage over topicals.212 Oral therapy should be done concomitantly with topical therapy or systemic steroid-sparing agents because patients often flare upon discontinuation. Oral candidiasis is a common complication of oral corticosteroids, and prophylaxis should be used.
Oral Retinoids: Oral acitretin is effective in oral lichen planus; one study of severe lichen planus found that 30 mg/day for 8 weeks resulted in remission in two thirds of cases.182 Acitretin can be effective at lower doses of 25 mg 3 to 7 days per week; however, oral lichen planus often recurs after the discontinuation of therapy; therefore, adjuvant topical therapy is often necessary. In a pilot study, oral alitretinoin dosed at 30 mg/day for up to 24 weeks reduced the severity of disease by 50% in 4 of 10 patients with severe oral lichen planus.213
Antimalarials: Hydroxychloroquine (200 to 400 mg [up to 6.5 mg/kg ideal body weight] for 6 months) is effective as a monotherapy in oral lichen planus.186 Despite its long half-life, improvement in erythema and pain may be seen within 1 to 2 months and reduction in erosions in 3 to 6 months.186
Methotrexate: Methotrexate at 2.5 to 7.5 mg weekly with adjuvant topical therapies is effective for severe, refractory oral lichen planus.214 Based on reports in cutaneous lichen planus and in clinical practice, 10 to 15 mg weekly is more efficacious without an increase in side effects. The benefits of methotrexate can be seen within 4 to 8 weeks of initiation. Both methotrexate and MMF are first choices as a corticosteroid-sparing agent. Whereas MMF and methotrexate are preferred with erosive disease, oral retinoids are preferred with noneroded and hyperkeratotic disease. Given its low cost and relatively fast onset, methotrexate is often our preferred second-line systemic agent.
Mycophenolate Mofetil: MMF at 2 to 3 g/day in divided doses led to remission in 6 of 10 patients with severe oral lichen planus.215 Of note, the clinical improvement of oral lichen planus using MMF can be gradual, often over 3 to 6 months, and adjuvant topical or oral corticosteroids are often necessary. Because of its tolerability and safety, MMF is considered a secondline systemic agent.
Cyclosporine: Cyclosporine has been reported effective in a report of two patients.196 The dosages of cyclosporine are outlined in the prior section on cutaneous
546
lichen planus therapies. Because of its long-term side effect profile and because there is no clear evidence that cyclosporine is superior to methotrexate or MMF in oral lichen planus, it is a third-line systemic agent.
Other Therapies: Additional therapies have been reported, including mesalazine, antibiotics, hydroxychloroquine, griseofulvin, thalidomide, and azathioprine, as well as parenteral alefacept, extracorporeal photopheresis, laser therapy, and PUVA therapy have all been reported as efficacious. However, these therapies often have attendant side effects or do not show clear efficacy. They are reserved as third-line corticosteroid-sparing therapies, and the risks and benefits of therapy should be considered before institution.
LICHEN PLANOPILARIS AND FRONTAL FIBROSING ALOPECIA
LICHEN PLANOPILARIS
AND FRONTAL FIBROSING
ALOPECIA
There are no randomized controlled trials in lichen planopilaris and only one controlled study. Therefore, many of the therapies in lichen planopilaris are based on expert opinion.216 Lichen planopilaris has three major subtypes; however, for therapeutic purposes, they will be divided into lichen planopilaris and frontal fibrosing alopecia. These clinically distinct entities also appear to be responsive to different therapies.217
When considering therapeutic modalities, the psychosocial effects of irreversible, scarring alopecia should be taken into account. Although the pathogenesis of lichen planopilaris is unknown, there is destruction of the bulge region, which leads to scarring. Recent studies have indicated a deficiency of PPARγ, which may lead to loss of immune privilege and scarring alopecia.24 However, targeting of PPARγ with pioglitazone has shown mixed results with cessation of disease progression in 14% to 73% of cases.218,219
LICHEN PLANOPILARIS Skin-Directed Therapies: First-line therapies for lichen planopilaris are mid to high potency topical corticosteroids with an average 53% response rate.156,217,220 There are only limited data to determine the efficacy of topical calcineurin inhibitors, but its efficacy in cutaneous and oral lichen planus makes it common second-line topical therapy.
Systemic Therapies: Hydroxychloroquine (6.5 mg/kg of ideal body weight for 6 to 12 months) is the second most commonly used drug and showed a good response in 23% of cases.185,217 There have been several negative studies using hydroxychloroquine, and there is good evidence that although clinical evidence of inflammation is decreased, progressive scarring of follicles continues.216 Based on these findings, we advocate against hydroxychloroquine as a monotherapy. Oral corticosteroids at 1 mg/kg/day for 15 days with
taper over 4 months and cyclosporine 300 mg/day for 3 to 5 months are the third most commonly used drugs with a good response in 60% of cases.156,217,220,221 However, because of its side effect profile, cyclosporine has been largely supplanted by methotrexate and MMF. Relapse is common upon discontinuation of these medicines; therefore, topicals or intralesional therapy should be used concomitantly. A commonly used combinational regimen of oral doxycycline 100 mg twice daily, MMF 2 to 3 g/day, and intralesional steroids 10 mg/mL monthly basis had marked improvement in one third of cases in 6 to 12 months.220,222-224
Therapeutic Approach: One approach is superpotent topical corticosteroids, clobetasol, twice daily for 1 month, daily for 3 months, and every other day for 3 months.221 Intralesional corticosteroids, hydroxychloroquine, and doxycycline (often in combination) can be added if there is no effect at 1 to 3 months, recognizing that hydroxychloroquine monotherapy is ineffective. Other immunosuppressive agents can then be added in severe, refractory, and rapidly progressive cases, including prednisone in combination with methotrexate or MMF, and cyclosporine monotherapy may be used with the above skin-directed therapies.
FRONTAL FIBROSING ALOPECIA Skin-Directed Therapies: High-potency topical corticosteroids have been shown to be ineffective in frontal fibrosing alopecia, for 93% of cases, but intralesional corticosteroids (10 to 20 mg/mL injected every 3 to 6 months) led to partial improvement in 60% of cases.217,221,225,226
Systemic Therapies: Oral 5 α-reductase inhibitors, such as finasteride (2 mg to 5 mg/day dose for 12–18 months) or dutasteride (0.5 mg every 1 to 7 days) for 12 months), are most commonly used and most effective drugs, and they result in a good response in 45% to 47% of cases.217,225,227-230 The largest study of frontal fibrosing alopecia to date found that androgenetic alopecia (AGA) was concurrently present in 40% of the women and 67% of the men.226 Therefore, the benefit seen with antiandrogens may be due to the component of AGA. Hydroxychloroquine has been reported effective in approximately 30% of cases; however, many of the studies had concomitant topical therapy with immune modulators and minoxidil.71,217 Other reported therapies (eg, systemic prednisone, hormone replacement, topical calcineurin inhibitors, topical minoxidil, cyclosporine, and MMF) have only been reported in small series and have highly variable response rates.
Therapeutic Approach: Based on the above evidence, many hair experts will use as first-line therapy an oral 5-αreductase inhibitor, intralesional corticosteroids, and occasionally topical minoxidil. For severe, rapidly progressive cases, corticosteroids in combination with MMF or methotrexate and cyclosporine monotherapy may be used in conjunction with these therapies.
5
NAIL LICHEN PLANUS
NAIL LICHEN PLANUS
Nail lichen planus can be extremely difficult to treat, and 20-nail dystrophy and atrophic nails are often nonresponsive. The goal of therapy should be to reduce the number of inflammatory cells within the nail and to prevent irreversible pterygium. A therapeutic approach should be very similar to cutaneous lichen planus. Ultrapotent topical and intralesional corticosteroids (5 to 10 mg/mL injected on a weekly basis) are firstline therapies. Systemic therapies should be reserved for cases manifesting significant compromise of function and causing debilitating pain. Additional therapies such as hydroxychloroquine has also been reported.187
ACKNOWLEDGMENTS
Steven A Nelson, MD, David J DiCaudo, and Collin Costello

Figure 32-1 Lichen planus. Flat-topped, polygonal, sharply defined papules of violaceous color, grouped and confluent. The surface is shiny and reveals fine white lines (Wickham striae). Note the hyperpigmentation of resolving lesions. (Used with permission from Mayo Foundation for Medical Education and Research, all rights reserved.)

Figure 32-2 Koebnerization. Linear pattern with a Koebner response adjacent to clustered papules on the flexural wrist. (Used with permission from Mayo Foundation for Medical Education and Research, all rights reserved.)

Figure 32-3 Annular lichen planus. Violaceous, annular lesions involving the corona and body of the penis. (Used with permission from Mayo Foundation for Medical Education and Research, all rights reserved.)

Figure 32-4 Hypertrophic lichen planus. Well-marginated, acanthotic and papillomatous, dull-violet plaques are noted over the anterior shin. Areas of postinflammatory hyperpigmentation as well as superficial varicosities, signifying venous stasis, are noted. (Used with permission from Mayo Foundation for Medical Education and Research, all rights reserved.)

Figure 32-5 Vesiculobullous lichen planus. Vesicles and bullae with violaceous-erythematous papules and plaques on the foot. (Used with permission from Mayo Foundation for Medical Education and Research, all rights reserved.)

Figure 32-6 Erosive–ulcerative lichen planus. Erosions, ulcers, and granulation tissue and scarring of toes, interdigital web spaces, and soles. (Used with permission from Mayo Foundation for Medical Education and Research, all rights reserved.)

Figure 32-7 Lichen planus pigmentosus. Multiple, wellmarginated, hyperpigmented, dark-brown macules located along the neck, with sparing of the face. The macules coalesce to form a slightly retiform pattern. This patient had involvement of the intertriginous regions and negative patch testing results. (Used with permission from Mayo Foundation for Medical Education and Research, all rights reserved.)
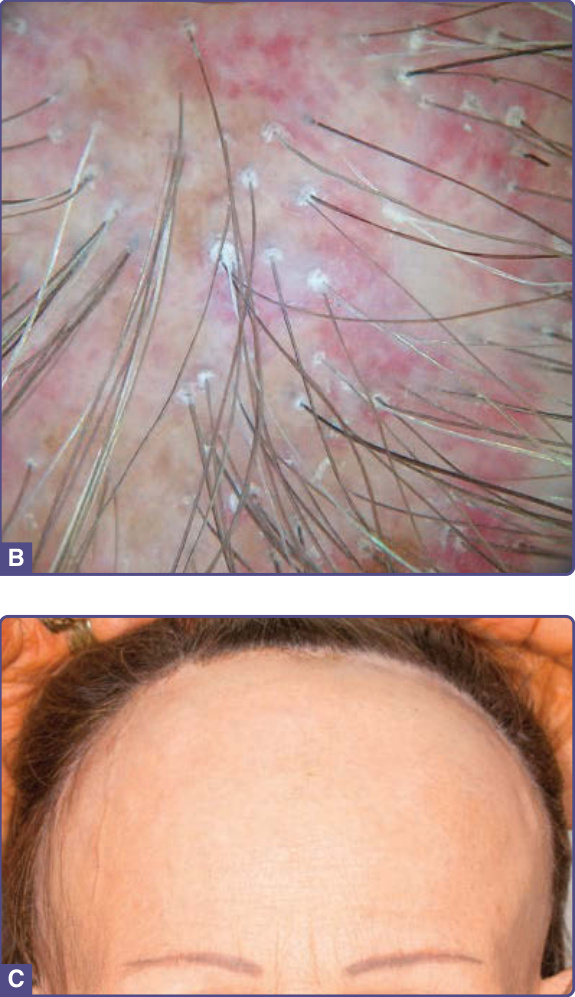
Figure 32-8 Follicular lichen planus. Lichen planopilaris. A, Posterior scalp scarring alopecia with perifollicular erythema and scaling. B, Dermoscopy showing white scarred patches, peripilar casts, perifollicular scale and erythema, and polytrichia. Frontal fibrosing alopecia. C, Frontal scalp with scarring alopecia, perifollicular erythema, and scaling. Note the complete loss of the eyebrows bilaterally.
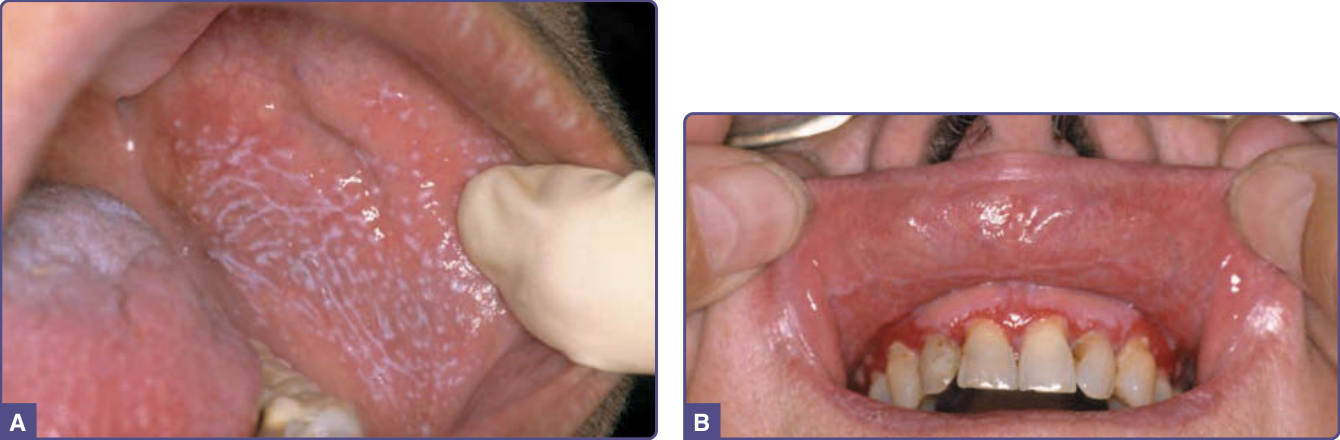
Figure 32-9 Mucosal lichen planus. A, Reticulate oral lichen planus with the typical lace-like, whitish reticulated pattern of oral lesions is seen on the buccal mucosa. B, Erosive oral lichen planus with painful erosions on the gingiva. (Used with permission from Mayo Foundation for Medical Education and Research, all rights reserved.)

Figure 32-10 Oral lichenoid tissue reaction. Reticulate oral lichenoid eruption with typical lace-like, reticulated pattern concentrated along the lower buccal mucosa and in close approximation to the underlying dental amalgams. (Used with permission from Mayo Foundation for Medical Education and Research, all rights reserved.)

Figure 32-11 Mucosal lichen planus. Perianal leuko- and hyperkeratosis with hypertrophic, folded violaceous epithelium, fissures, and a healing biopsy site. (Used with permission from Mayo Foundation for Medical Education and Research, all rights reserved.)

Figure 32-12 Nail lichen planus. A, Classic nail lichen planus showing longitudinal ridging and splitting of all nails (onychorrhexis) with distal splitting (onychoschizia). Additionally, the third finger shows dorsal pterygium at the lateral aspect of the nail bed with loss of the nail (anonychia). B, Twenty-nail dystrophy showing longitudinal ridging of all nails (trachyonychia) and atrophic nails. (Used with permission from Mayo Foundation for Medical Education and Research, all rights reserved.)

Figure 32-13 Palmar lichen planus. Callus-like keratotic papules with a faint purple hue and an inflammatory halo are concentrated over the thenar and hypothenar eminence bilaterally. Note the relative sparing of the distal fingertips. (Used with permission from Mayo Foundation for Medical Education and Research, all rights reserved.)
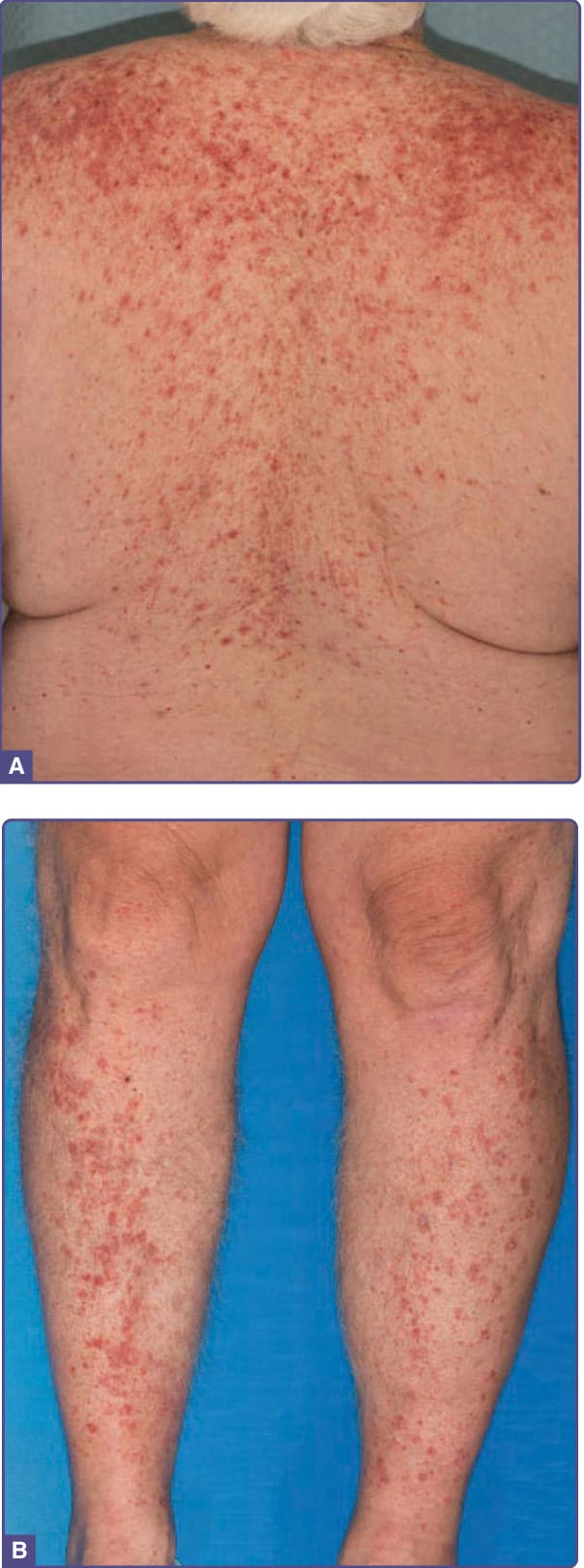
Figure 32-14 Lichenoid drug eruption. A, and B, Symmetrical, generalized, eczematous papules and plaques over the trunk and anterior shins. Wickham striae are absent, and there is sparing of the flexural surfaces. (Used with permission from Mayo Foundation for Medical Education and Research, all rights reserved.)

Figure 32-15 Lichen planus–lupus erythematosus overlap syndrome. Lichenoid lesions over the dorsal hand and forearm. Direct immunofluorescence showed evidence of lupus erythematous. (Used with permission from Mayo Foundation for Medical Education and Research, all rights reserved.)

Figure 32-16 Lichen planus pemphigoides. Erythema, erosions, and bullae over the distal shin with histology showing a lichenoid tissue reaction and direct immunofluorescence showing features of bullous pemphigoid. Indirect immunofluorescence result also was positive. (Used with permission from Mayo Foundation for Medical Education and Research, all rights reserved.)
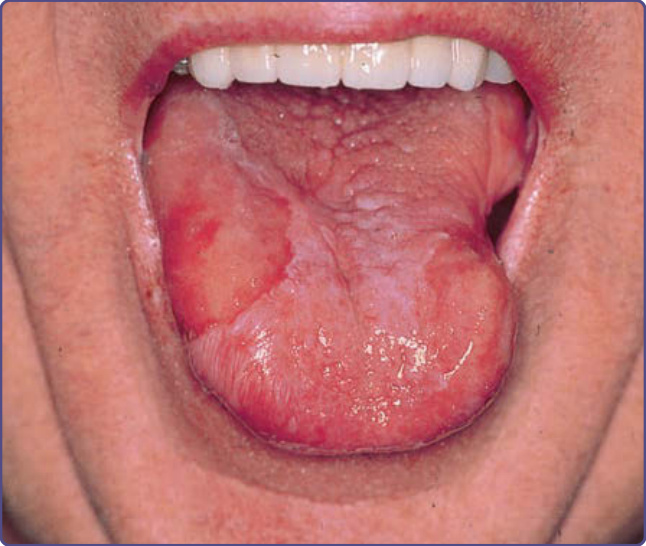
Figure 32-17 Lichen planus and squamous cell carcinoma (SCC). Long-standing oral lichen planus with scarring of the tongue. Well-circumscribed erythroplakia and erosions of the right lateral tongue was biopsied and confirmed SCC. (Used with permission from Mayo Foundation for Medical Education and Research, all rights reserved.)
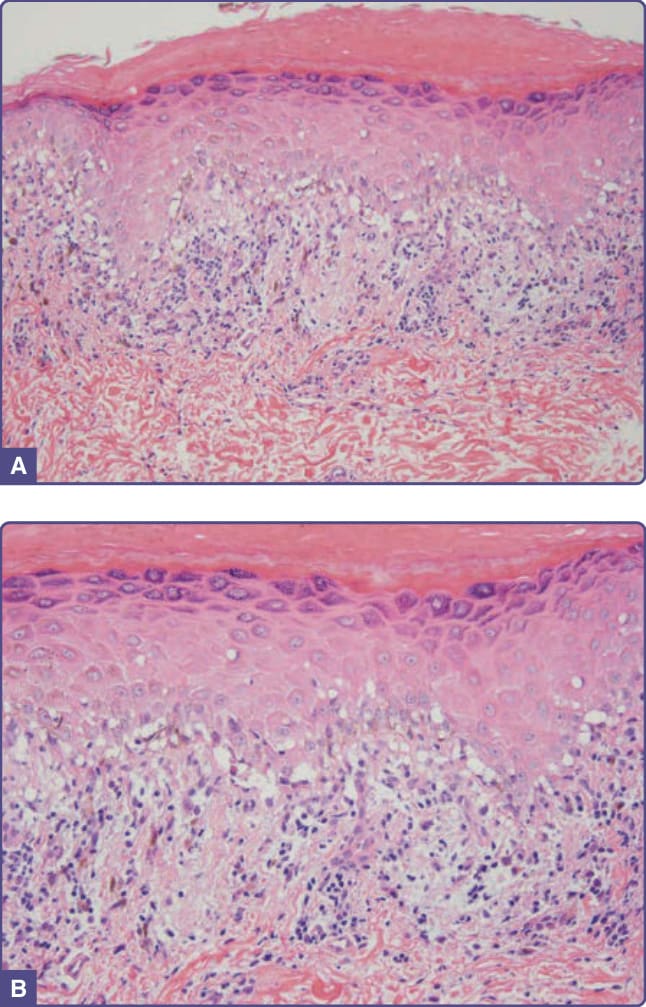
Figure 32-18 Lichen planus. A, The characteristic findings of lichen planus with compact orthohyperkeratosis, wedgeshaped hypergranulosis, sawtoothed rete ridges, and a lichenoid infiltrate. (Hematoxylin and eosin [H&E] × 100.) B, Dense, lichenoid lymphocytic infiltrate with scattered apoptotic keratinocytes and pigment incontinence. A small Max-Joseph space is noted centrally. (H&E × 200.) (Photo contributors: David J. DiCaudo, MD and Steven A. Nelson, MD. Used with permission from Mayo Foundation for Medical Education and Research, all rights reserved.)
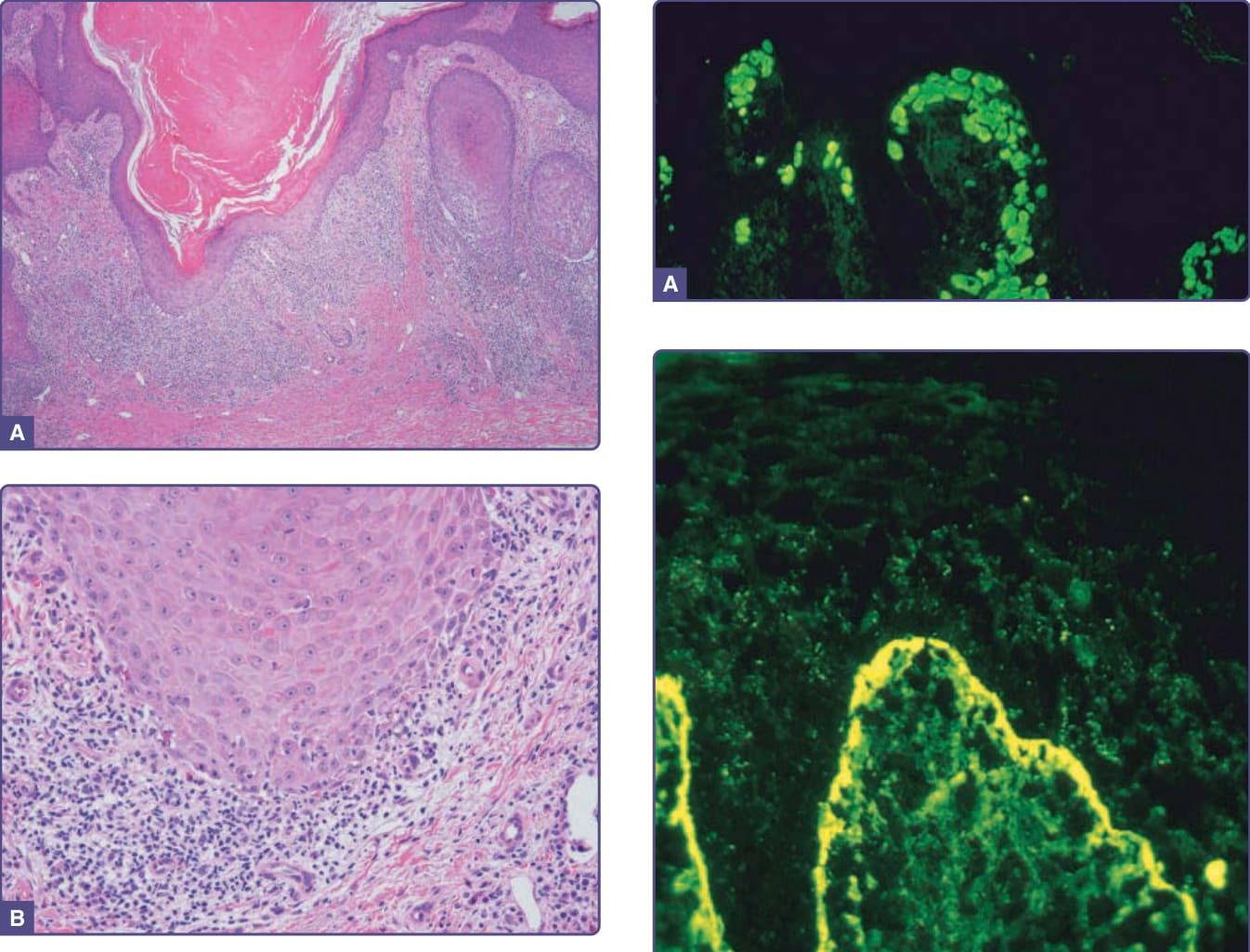
Figure 32-19 Hypertrophic lichen planus. A, The characteristic findings of hypertrophic lichen planus with hyperkeratosis, acanthosis, and papillomatosis. ( Hematoxylin and eosin [H&E] × 40.) B, Dense, lichenoid lymphocytic infiltrate with scattered apoptotic keratinocytes and eosinophils. (H&E × 200.) (Photo contributors: David J. DiCaudo, MD and Steven A. Nelson, MD. Used with permission from Mayo Foundation for Medical Education and Research, all rights reserved.)
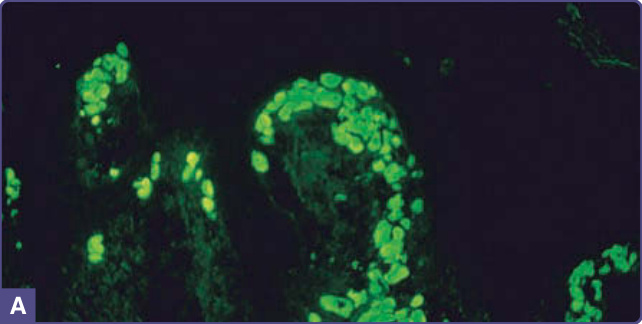
Figure 32-20 Lichen planus. Direct immunofluorescence. A, Fibrinogen/fibrin, shaggy pattern at the dermal– epidermal junction. B, Numerous immunoglobulin M-positive cytoids at the dermal–epidermal junction. (Used with permission from Mayo Foundation for Medical Education and Research, all rights reserved.)
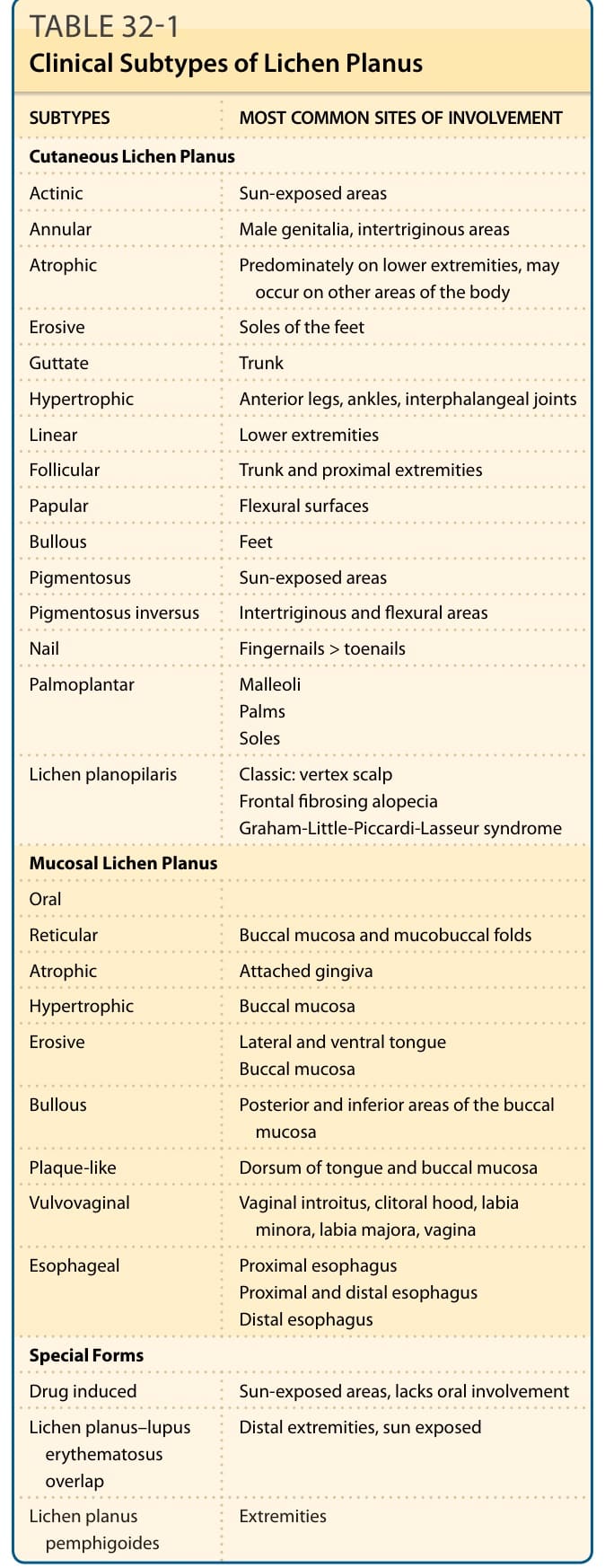
TABLE 32-1 Clinical Subtypes of Lichen Planus
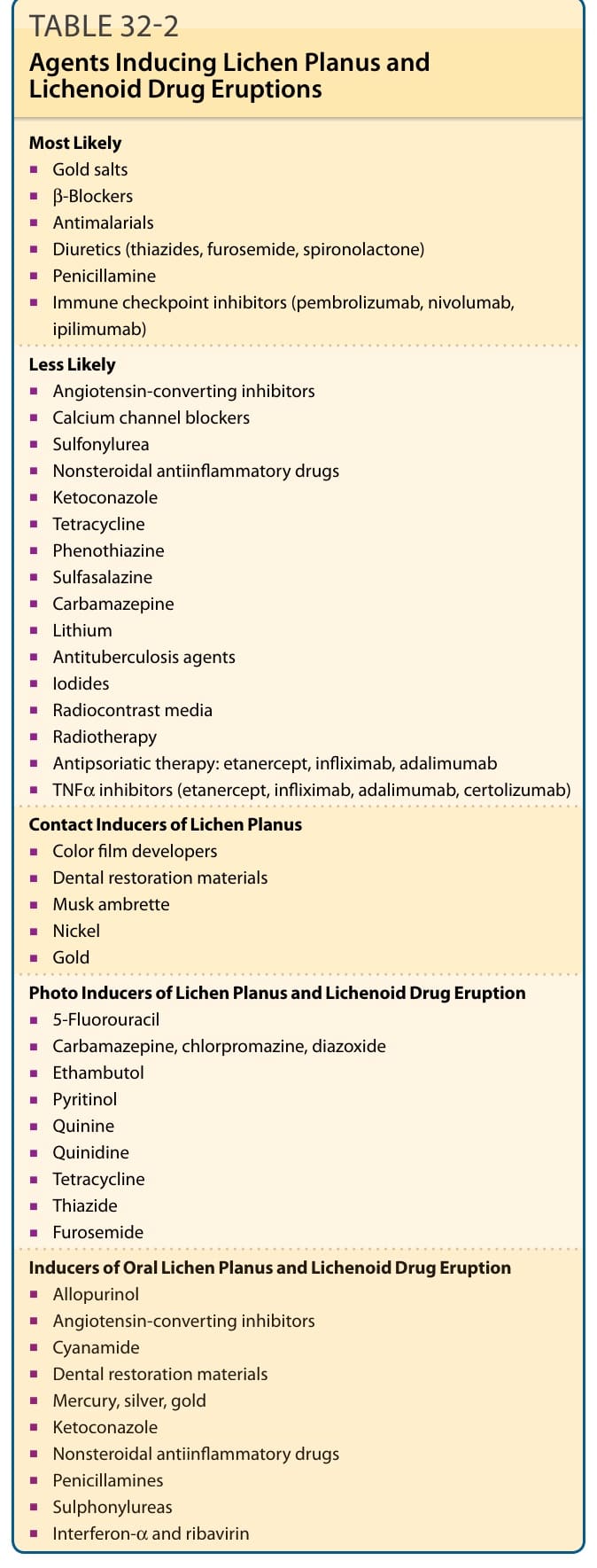
TABLE 32-2 Agents Inducing Lichen Planus and Lichenoid Drug Eruptions
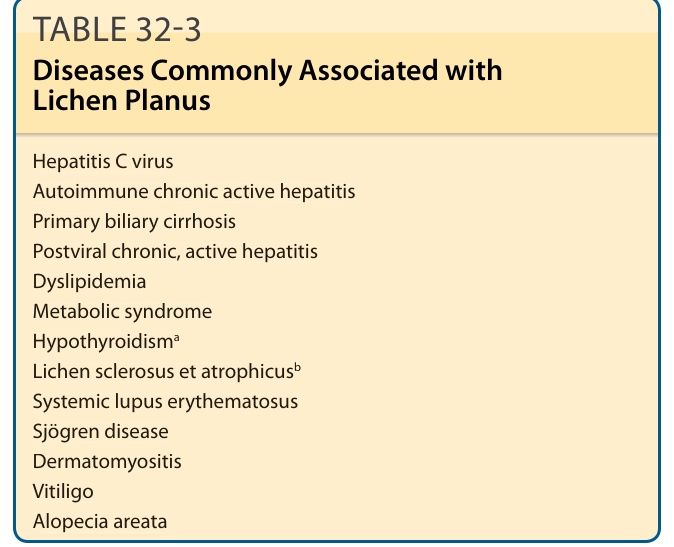
TABLE 32-3 Diseases Commonly Associated with Lichen Planus
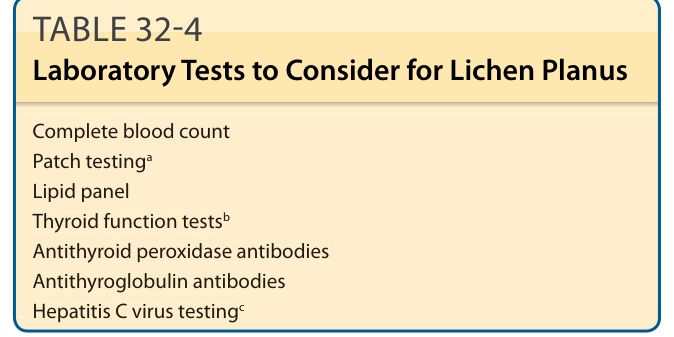
TABLE 32-4 Laboratory Tests to Consider for Lichen Planus
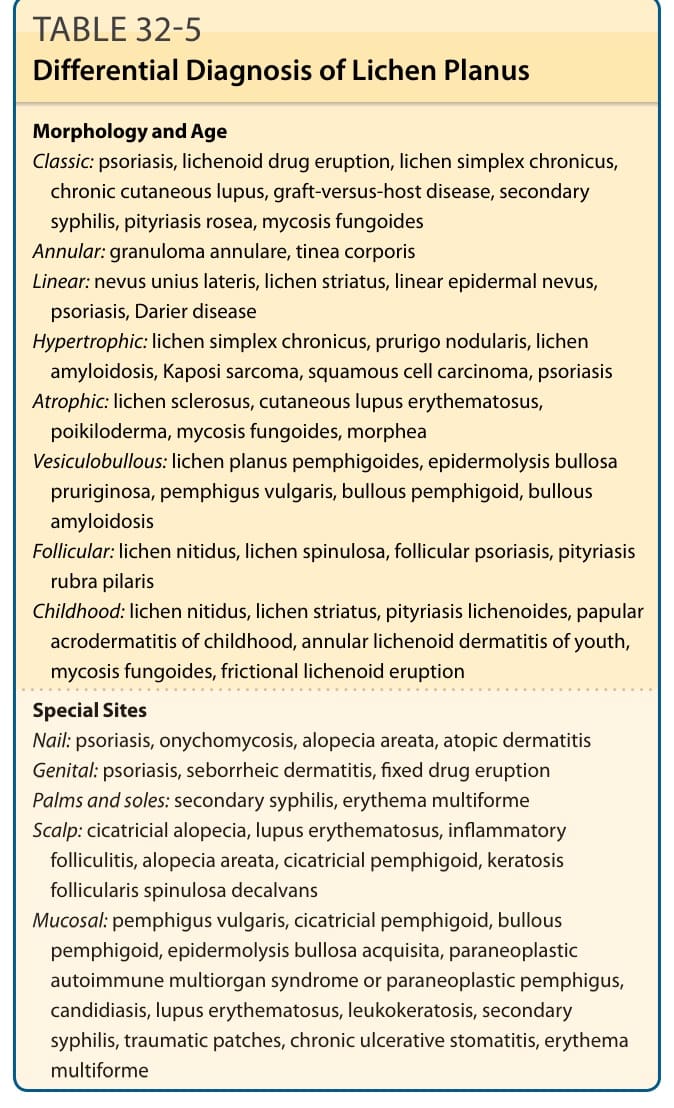
TABLE 32-5 Differential Diagnosis of Lichen Planus