Pityriasis Rosea
4
AT-A-GLANCE
■ Common self-limited papulosquamous eruption typically lasting 5 to 8 weeks.
■ Occurs worldwide in all races and age groups, with peak incidence between the ages of 10 and 35 years.
■ Classically begins as an isolated 3- to 5-cm oval plaque on the trunk with a collarette of fine scale just inside the periphery, which plaque is called a herald patch.
■ This is followed by a secondary eruption of similar appearing but smaller lesions on the trunk and proximal extremities, usually with their long axis along the lines of cleavage.
■ Many atypical variants exist in contrast to the pattern described above.
■ Pityriasis rosea can have associated systemic symptoms and pruritus, but many cases are asymptomatic.
■ Etiology is unknown, but it is thought to be a viral exanthem most likely related to infection or reactivation of human herpesvirus (HHV)-6 and/ or HHV-7.
■ Usually only supportive treatment and reassurance is needed, but for severe cases acyclovir may hasten recovery and lessen symptoms.
In 1860, Gibert first used the term pityriasis rosea (PR), meaning pink (rosea) scales (pityriasis).1 PR is most common in teenagers and young adults, and is likely a viral exanthema currently thought to be related to primary infection or reactivation of human herpesvirus (HHV)-6 (HHV-6) and/or HHV-7.2-6 PR is fairly common, self-limited, and not associated with long-term sequelae. It classically begins as an isolated 3- to 5-cm oval plaque on the trunk with a collarette of fine scale just inside the periphery, which plaque is called a herald patch. This lesion is then followed by a secondary eruption of similar appearing but smaller lesions most prominently on the trunk and proximal extremities, usually with their long axis along the lines of cleavage in what is often described as a “Christmas tree” pattern. However, there are many atypical presentations of the herald patch distribution, secondary eruption morphology, and overall rash distribution. PR is commonly asymptomatic, but pruritus and systemic flu-like symptoms may be present. Often only supportive treatment and patient education are needed for management, but in cases with a widespread
eruption, severe pruritus, or significant systemic symptoms acyclovir may be beneficial.
EPIDEMIOLOGY
PR has a worldwide distribution and is found in all races. One institution in the United States found the incidence to be 0.16% (~160 cases per 100,000 personyears).7 Studies in other countries report incidences ranging from 0.75% to 1.17%.8,9 A recent publication combined many of the PR epidemiologic studies from around the world and reported an incidence of 0.64 per 100 dermatologic patients.10 In some studies PR was found to be more common in colder months,7,9 but other studies show no significant seasonal variation.2,11
Studies have demonstrated clustering of cases supporting the hypothesis of an infectious etiology.12,13
There is a slight female preponderance at 1.39:1.10 The peak incidence of PR occurs between the ages of 10 and 35 years, but cases have been reported ranging in age from 3 months to 83 years.7,9,10,14 Relapse is thought to be rare, ranging from 1.8% to 3.7%.7,15
CLINICAL FEATURES
HISTORY
HISTORY
Classic PR typically begins with a solitary lesion on the trunk or less commonly an extremity known as a herald patch. This lesion typically remains isolated on average for 2 weeks in adults and 4 days in children, after which time it is followed by the onset of a secondary eruption of morphologically similar but smaller lesions on the trunk and proximal extremities. The eruption may be preceded by various prodromal symptoms such as malaise, nausea, headache, gastrointestinal, and upper respiratory symptoms. The incidence of these prodromal symptoms varies in the literature from 5% to 69%.14,16 These symptoms can also occur during the eruption. Pruritus is severe in 25%, mild to moderate in 50%, and absent in 25% of patients.17
In contrast to classic PR, Drago and colleagues have reported several variants of PR, such as in pediatric patients (<10 years of age), relapsing, and a persistent form.15,17-20 The relapsing form of PR generally consists of single episode of relapse within 1 year of the initial episode, although multiple relapses have been reported. In this variant, the secondary episodes generally lack a herald patch, are shorter lived, and consist of fewer and more localized lesions than the initial eruption. The persistent form of PR, is defined as having the eruption last for greater than 12 weeks without interruption. It commonly has a herald patch, and oral
manifestations are thought to be more common than in classic PR. When PR presents in the pediatric population it often has a different clinical course compared to classic PR. Thus, the time between the presentation of the herald patch and the secondary eruption is shorter, often lasting only 4 days, in contrast to the more typical 2-week interval. In addition, the average overall duration of the eruption tends to be shorter and on average lasts approximately 16 days.19 Lastly, PR is reported to occur more frequently in pregnant women than in the general population, but otherwise PR during pregnancy presents in a manner similar to classic PR.
CUTANEOUS FINDINGS
CUTANEOUS FINDINGS
The initial classic herald patch presents as a welldemarcated, thin, oval to round plaque that is usually pink, rose colored, erythematous, or, less commonly, hyperpigmented. It frequently has a slightly depressed center and fine collarette of scale within the periphery of the lesion (Figs. 31-1 and 31-2). It most commonly occurs on the trunk (50%) followed by the extremities and neck.2 Atypical locations such as the dorsal feet, face, scalp, and genitalia have been reported. This lesion enlarges over several days usually reaching a diameter greater than 3 cm with a range of 2 to 10 cm. The incidence of the herald patch is reported to be anywhere from 12% to 94%, but is thought to be present in approximately 80% of the cases. Multiple herald patches have been observed with an incidence of 5% (Fig. 31-3). The herald patch may appear concurrently with the more generalized eruption or, less commonly, be the sole manifestation of the disease.2,14
The secondary eruption commonly begins approximately 2 weeks following the onset of the herald
4
patch. However, this interval is described as ranging from a few hours to 3 months.14 This secondary eruption is characterized by multiple, round-to-oval, 0.5- to 1.5-cm macules, papules, and plaques. These lesions are often light pink with a fine collarette of scale and resemble the herald patch in miniature. They are typically found bilaterally and symmetrically on the trunk and proximal extremities (Figs. 31-4 to 31-6). However, these lesions can extend to the distal extremities, and
519
4
520
can been found on the palms and soles. In the classic description, these lesions are aligned with their long axis parallel to lines of cleavage giving a “Christmas tree” distribution on the upper chest and back (Fig. 31-7). This secondary eruption usually occurs in crops every few days over the course of 2 weeks, where it reaches its maximum intensity. Rarely, the secondary eruption is confined to sun-protected skin; in other cases, it is found only on sun-exposed surfaces.14
Many different forms of atypical secondary lesions have been described, including eczematous, papular, follicular, vesicular, urticarial, pustular, and purpuric (Figs. 31-8 and 31-9).2,14,17 These lesions may be the only manifestation of the secondary eruption or they may
Primary and secondary plaques
Herald patch
occur admixed with other morphologies, including the classic type. The vesicular lesions may be arranged in a rosette and are more common in children and young adults.2
Mucosal lesions can occur with PR, and although these lesions are thought to be uncommon, they have been reported in up to 16% of patients with PR.21 The oral lesions can have varying morphologies, including punctate hemorrhagic, ulcerative, erythematous macules, plaques, bullous, and annular lesions.22 Ulcerations are thought to be the most common form. The oral lesions typically occur along with the cutaneous eruption.2 Lymphadenopathy can also be associated with PR particularly when patients have associated flu-like symptoms. There are several atypical variants of PR, such as unilateral, localized, and inverse, which make up approximately 20% of cases.14 Localized PR is often limited to 1 truncal site, whereas unilateral PR does
4
not cross midline. Inverse PR, which is more common in children, is characterized by involvement of the body folds, face, and often distal extremities.2,14 PR in a blaschkoid distribution or with prominent acral involvement has also been reported.23,24
COMPLICATIONS
COMPLICATIONS
PR is not associated with any long-term complications in otherwise healthy individuals. Systemic symptoms, when present, are transient. PR, mostly because of the uncertain etiology, length of disease recovery, and fear of progression, can be associated with the development of anxiety and depression in 30% of cases and does negatively impact quality of life.25 PR in pregnancy deserves special mention as it may be associated with adverse outcomes. In one study where 38 women who developed PR during pregnancy were observed, 13% had a miscarriage; it was noted, however, that the miscarriage rate of the general population is approximately 10%.26 Perhaps of more interest was that in the 8 cases where PR began before 15 weeks of gestation, 5 (62%) resulted in abortion. Of the 33 women who bore children in this study, 9 (27%) had a premature delivery, but none of the infants had birth defects, although hypotonia, weak motility, and hyporeactivity was noted in 6 cases (18%). Based on these findings, women who develop PR during pregnancy, particularly during the first trimester, should be followed carefully for the development of adverse events.
ETIOLOGY AND PATHOGENESIS
PR has long been thought to be caused by an infectious agent. This assumption is based on the findings of case clustering, possible seasonal variation, resemblance to other known exanthems, and the presence of prodromal symptoms in some patients. Over the years there have been numerous investigations into potential causative bacterial, fungal, and viral pathogens, all with largely negative results. However, in 1997, Drago and colleagues found HHV-7 DNA in peripheral blood mononuclear cells, skin, and cell-free plasma of patients with PR suggesting an association.6 Since 1997, multiple studies have been done that support HHV-7 and/or HHV-6 as the likely cause of PR.5,3,27-29 These studies demonstrated the presence of HHV-7, and to a lesser extent HHV-6 DNA and messenger RNA, in both lesional and nonlesional PR skin, in peripheral blood mononuclear cells, and in plasma via real-time polymerase chain reaction, but not in controls. Furthermore serological studies using immunoglobulins M and G against HHV-7 and HHV-6 are in alignment with the findings above. All this evidence suggests PR may be related to infection with HHV-7 and, to a lesser extent, HHV-6. It is not clear if PR is caused by HHV-7 and/or HHV-6 primary infection, reactivation,
521
4
or both. The hypothesis of reactivation is supported by the finding of 7 and HHV-6 DNA in saliva which is a known reservoir of these viruses and the usual mode of transmission.28 However, the antibody profile found by Vag and colleagues was more consistent with primary infection.29 It should be noted that there have also been various studies with results that failed to duplicate the findings of HHV-7 and/or HHV-6 DNA in PR patients, failed to show differences in patients with PR and controls, or, in some cases, found even higher prevalence of HHV-7 and HHV-6 DNA in control individuals.30-35 There are numerous potential reasons for these discordant results. First, HHVs have a very high prevalence in the general population, making it hard to show differences in prevalence between disease states and healthy controls without large numbers. The prevalence of HHV-6 and HHV-7 seropositivity in healthy adults has been found to be 80% to 100%36 and >85%,37 respectively. Also complicating analysis is that HHV-7 may influence and even cause reactivation of latent HHV-6 with subsequent disappearance of active HHV-7 replication.2,30 This could account for the varying percentages of HHV-7 and HHV-6 in the positive studies. Lastly, the varied findings may reflect that PR like other exanthems, such as Gianotti-Crosti syndrome, can be induced by multiple pathogens.30
Overall the pathogenesis of PR is poorly understood and if HHV-7 and HHV-6 are the etiologic agents the mechanisms by which they lead to the clinical findings seen in PR are not known. Several studies have looked into the immunologic aspects of PR. A review of the available literature shows that cell-mediated immunity is important in the pathogenesis of PR.38 Specifically, one study demonstrated that the inflammatory infiltrate of PR was predominantly T cells with an increased CD4-to-CD8 ratio as well as an increased proportion of Langerhans cells, which are common findings in other inflammatory skin conditions thought to be driven by cell-mediated immunity. No significant difference was found between the herald patch and fully developed PR lesions.39 Another study looking specifically at the cytokine profile of PR found increased interleukin-17, interferon-γ, vascular endothelial growth factor, and interferon-inducible protein-10 (CXCL10). Interleukin-17 and interferon-γ in particular were mentioned as evidence that the cytokine profile in PR was not specific for, but consistent with, a viral-induced disease process.40 Lastly, an autoimmune pathogenesis for PR has been investigated, but to date no compelling autoantigens or supporting evidence has been found.38
DIAGNOSIS
The diagnosis of PR is usually clinical, and in the case of classic PR fairly straightforward. The various atypical presentations, however, can pose a diagnostic challenge. A set of clinical diagnostic criteria was proposed in 2003.41,42 In these criteria, the patient had to have 3 essential features and at least 1 of 3 optional
522
features. The 3 essential features were discrete circular or oval lesions, scaling on most lesions, and a peripheral collarette of scale with central clearance on at least 2 lesions. The optional criteria included a truncal and proximal limb distribution with less than 10% of lesions distal to the mid-upper-arm and mid-thighs, distribution of most lesions along the ribs, and a herald patch appearing at least 2 days before the eruption. They also proposed 3 exclusion features, including multiple small vesicles at the center of 2 or more lesions, most lesions on palmar or plantar skin surfaces, and clinical or serological evidence of secondary syphilis.
LABORATORY TESTING
LABORATORY TESTING
Routine blood tests are typically normal in PR. Although various abnormalities, including leukocytosis and an elevated erythrocyte sedimentation rate may be found, blood tests are nonspecific. As such, blood tests are not needed nor are they recommended in the diagnosis of PR.
PATHOLOGY
PATHOLOGY
The histologic features of PR are nonspecific and patients with the classic presentation often do not require skin biopsy as the diagnosis can confidently be made on clinical grounds alone. The epidermal changes seen include parakeratosis which may be focal, multifocal, or confluent; orthokeratosis; mild acanthosis; a thinned granular layer; and spongiosis often with some degree of lymphocyte exocytosis (Fig. 31-10). In the dermis there is typically a superficial perivascular lymphocytic infiltrate and variable extravasated red
blood cells (Fig. 31-11).39 The inflammatory infiltrate is predominantly composed of lymphocytes, neutrophils, histiocytes, and eosinophils can be seen.2,43 There are no consistent differences in the histology of the herald patch versus the secondary lesion, but the herald patch may have a slightly deeper infiltrate with more acanthosis.2
DIFFERENTIAL DIAGNOSIS
Most Likely
■Tinea corporis: Scale is usually at periphery of plaques, plaques usually not oval and distributed along lines of cleavage, positive potassium hydroxide (KOH) examination.
■Nummular dermatitis: Plaques are usually more circular than oval, there are no collarettes of scale, and tiny vesicles are common.
■Guttate psoriasis: Plaques are usually smaller than pityriasis rosea (PR) lesions and do not follow lines of cleavage; scales are thick and silvery. When in doubt, perform a biopsy.
Consider
■Pityriasis lichenoides chronica: More chronic with persistent crops of new lesions, more confluent scale, no herald patch, and more common on extremities.
■Lichen planus: More pruritic, chronic, and with distal extremity involvement. Scale may show classic Wickham striae.
■Seborrheic dermatitis: Look for characteristic face and scalp involvement.
Always Rule Out
Always Rule Out
■Secondary syphilis: History of primary chancre, no herald patch, lesions typically more widespread and classically involve palms and soles. Other features of secondary syphilis, such as condyloma lata, alopecia, mucous patches, and split papules, may be present. Usually there are more severe systemic complaints and lymphadenopathy. If there is any clinical concern, perform a serologic test for syphilis (eg, a rapid plasma reagin).
■Secondary syphilis: History of primary chancre, no herald patch,
lesions typically more widespread and classically involve palms and soles. Other features of secondary syphilis, such as condyloma lata, alopecia, mucous patches, and split papules, may be present. Usually there are more severe systemic complaints and lymphadenopathy. If there is any clinical concern, perform a serologic test for syphilis (eg, a rapid plasma reagin).
■PR-like drug eruption: See the text for an extensive list. A drug history is needed.
■PR-like drug eruption: See the text for an extensive list. A drug his-
tory is needed.
4
seborrheic dermatitis. Nummular eczema generally has more round than oval lesions, typically does not follow the lines of cleavage, and has a predilection for extensor extremities. Seborrheic dermatitis can have truncal lesions similar to PR, but they generally have corresponding lesions on the scalp and/or face. Although guttate psoriasis can be very difficult to distinguish from PR, it also does not follow the lines of cleavage, lacks a larger lesion that could mimic a herald patch, and has a thicker more confluent scale typical of psoriasis. Pityriasis lichenoides has a more chronic and relapsing course, lacks a herald patch, has lesions in various stages, and involves the extremities more than classic PR. Lichen planus is usually more pruritic and chronic than PR, lacks collarette of scale, has a more violaceous color, and often prominently involves the distal extremities. Dermatophyte infection is particularly difficult to distinguish from the herald patch, especially when it presents in the folds, making mycologic investigations, such as potassium hydroxide examination, necessary to distinguish dermatophyte infection from herald patch. Skin biopsy often can help to differentiate the above conditions from PR, particularly in the atypical forms of PR. Another entity commonly in the differential of PR that deserves special mention is secondary syphilis. The rash produced by each of these entities can be identical. Certain features that favor a diagnosis of syphilis include oral lesions, involvement of the palms and soles, and persistent lymphadenopathy. However, as noted above, all these features can be seen in PR, requiring serologic tests, starting with a rapid plasma reagin, to differentiate syphilis from PR. Because of this, some clinicians advocate checking a rapid plasma reagin in every patient suspected of having PR. In addition, one can look for other features of secondary syphilis, such as split papules, a “moth-eaten” appearing alopecia, and condyloma lata. Many medications are also reported to cause a PRlike eruption and there is some debate over whether these cases represent a separate entity or if PR might be drug induced in some instances. Medications reported to cause such eruptions include barbiturates, captopril, clonidine, gold, metronidazole, d-penicillamine, isotretinoin, levamisole, nonsteroidal antiinflammatory agents, omeprazole, and terbinafine.2 PR or PR-like rashes also have been described from the tyrosine kinase inhibitor imatinib and the tumor necrosis factor inhibitor adalimumab.44-46 The development of a PR-like eruption from adalimumab is of particular interest as this medication dampens the T-helper 1 cell response, which is key in the body’s defense against viral infections, and could therefore predispose to both viral infection or reactivation. The drug-induced PR-like eruptions are very similar to classic PR in appearance, but don’t resolve unless the offending agent is stopped, often leaving more marked hyperpigmentation and frequently transitioning to a more lichenoid morphology.2 The histopathology of a druginduced PR-like eruption is also more likely to show interface dermatitis, dyskeratotic keratinocytes, and eosinophils.
523
4
CLINICAL COURSE AND PROGNOSIS
PR typically self-resolves after an average of 45 days, but ranges from 2 weeks to 5 months have been reported.2,17 As previously stated, eruptions lasting longer than 3 months may fit into the proposed category of persistent PR. Upon resolution the only sequela is typically postinflammatory hyperpigmentation or hypopigmentation. As with other inflammatory conditions this dyspigmentation is more common in individuals with a darker skin color. There are no other significant long-term clinical outcomes from PR. As stated above, recurrence can occur, but it is very uncommon. When recurrence does happen, it is usually only once and also does not have any long-term health consequences.
MANAGEMENT
INTERVENTIONS
INTERVENTIONS
As discussed, PR is self-limited and therefore no treatment is necessary in many cases. Also given that many cases of PR have minimal to no symptoms the benefits of any treatment must be weighed against the potential side effects of the intervention on a case-by-case basis. Counseling patients on the natural history of PR and reassurance regarding its self-limited nature is paramount given the anxiety often associated with PR. Although there is no good data to support their use topical steroids and antihistamines are safe and may be helpful for associated pruritus. The macrolide erythromycin has been reported to hasten the clearance of PR.16 In addition, a 2007 Cochrane review found one small, good-quality study that demonstrated benefit from erythromycin.47 However, subsequent studies evaluating the efficacy of the macrolide antibiotics erythromycin and azithromycin failed to show any benefit when compared to placebo.48-50 Acyclovir also has been studied as a potential therapy for PR. Drago and colleagues initially found that treatment with high-dose acyclovir (800 mg 5 times daily) for 1 week led to a 78.6% rate of complete clearance at 2 weeks compared to only a 4.4% rate of complete clearance in the placebo group, but this study was not randomized and the investigators were not blinded.51
Several subsequent trials have all shown that acyclovir at varying doses may hasten the resolution of the rash, improve associated pruritus, and, in some cases, improve associated systemic symptoms.52-55 Therefore, given the low cost and good safety profile of acyclovir and its derivatives, these therapeutic agents may be reasonable to consider in PR patients, particularly in those with significant pruritus, an extensive rash, or significant systemic symptoms. It should be noted that the mechanism of action of acyclovir in the treatment of PR is unclear given that acyclovir’s effect is dependent on thymidine kinase, an enzyme whose gene is
524
not expressed by HHV-7.2 Ultraviolet B phototherapy also is reported to have some benefit in PR clearance time, although results vary on whether or not it helps with the associated pruritus.56,57
PREVENTION
PREVENTION
There is currently no data available on prevention of PR.
ACKNOWLEDGMENTS
The authors acknowledge the contributions of Andrew Blauvelt, the former author of this chapter.
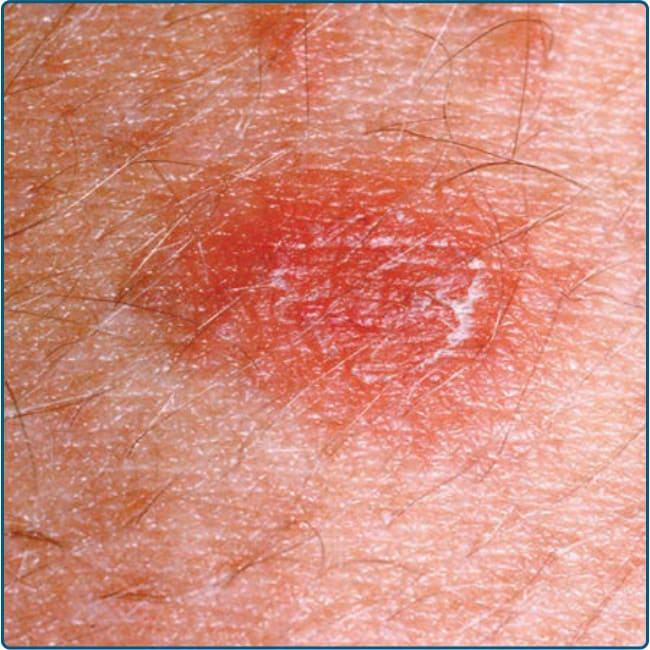
Figure 31-1 A typical primary plaque (herald patch) of pityriasis rosea, demonstrating an oval shape and fine scale inside the periphery of the plaque.

Figure 31-2 A nonscaly purpuric primary plaque (herald patch) of pityriasis rosea.

Figure 31-3 A double herald patch of pityriasis rosea.
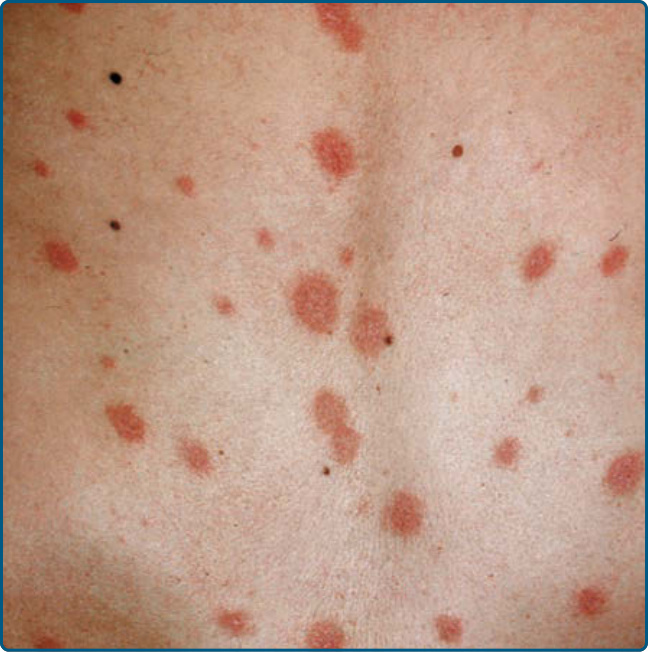
Figure 31-4 Typical distribution of secondary plaques along the lines of cleavage on the back in a Christmas tree pattern.

Figure 31-5 Typical distribution along the lines of cleavage and morphology of the secondary eruption on the back of a 23-week pregnant patient. (Used with permission from Dr. Thy Thy Do and Mr. Harrold Carter.)
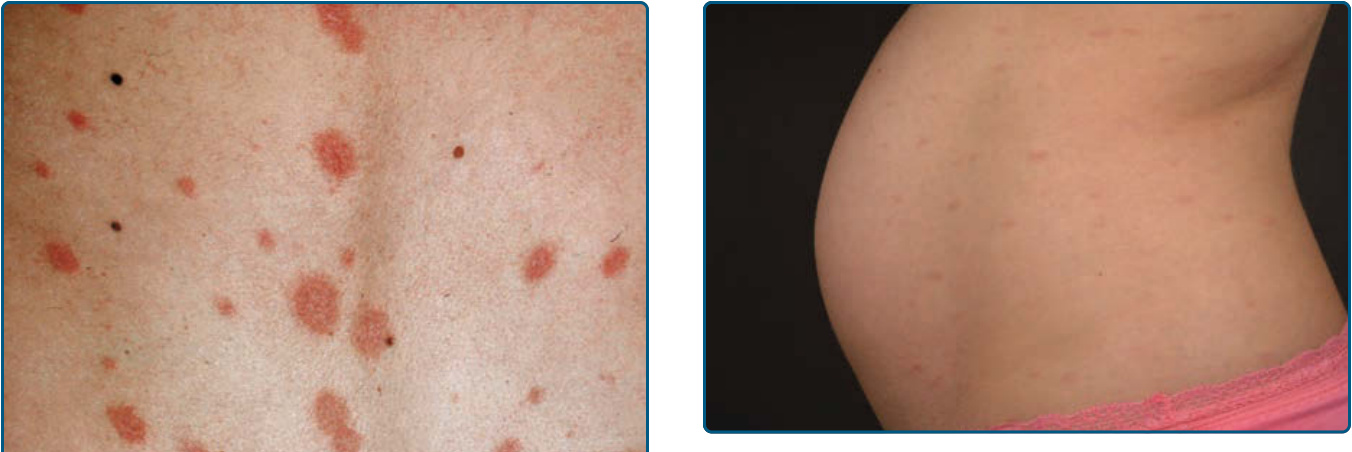
Figure 31-6 Typical distribution along the lines of cleavage and morphology of the secondary eruption on the flank and abdomen of a 23-week pregnant patient. (Used with permission from Dr. Thy Thy Do and Mr. Harrold Carter.)
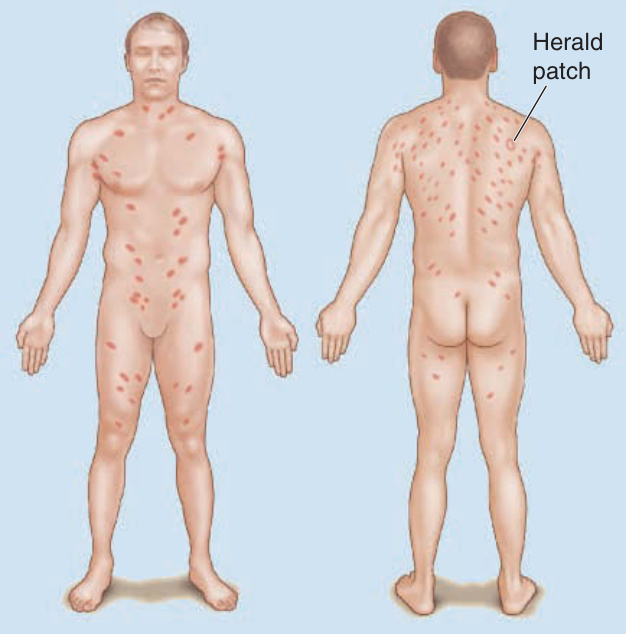
Figure 31-7 Schematic diagram of the primary plaque (herald patch) and the typical distribution of secondary plaques along the lines of cleavage on the trunk in a Christmas tree pattern.

Figure 31-8 Vesicular pityriasis rosea, showing typical primary plaque and secondary papulovesicles. Note Christmas tree distribution.
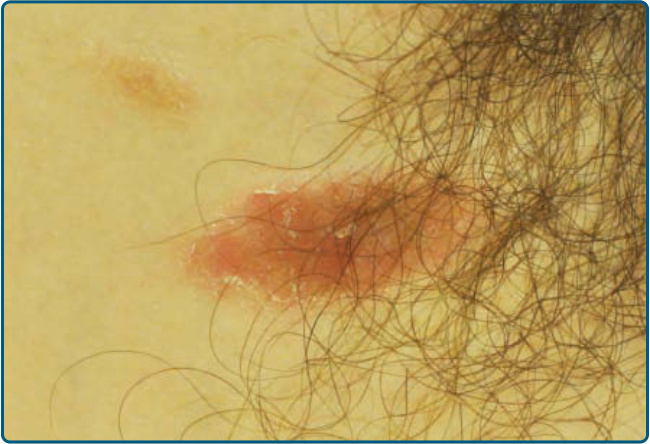
Figure 31-9 Purpuric pityriasis rosea.
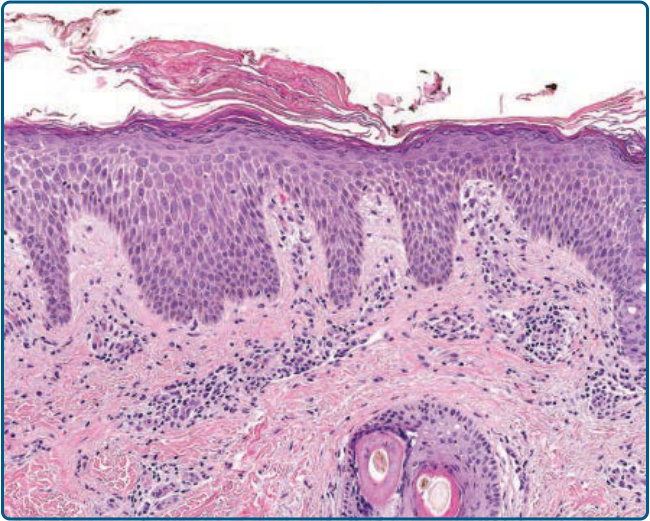
Figure 31-10 Typical epidermal changes seen in pityriasis rosea, including mounded parakeratosis with lift off, mild acanthosis, and spongiosis. (A 4-mm punch biopsy, hematoxylin and eosin stain, ×10 magnification, used with permission from Dr. Paul Harms.)
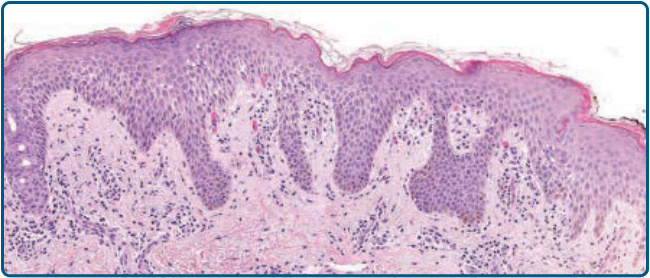
Figure 31-11 Biopsy that highlights the spongiosis, superficial perivascular lymphocytic infiltrate, and red blood cell extravasation typically seen in pityriasis rosea. (A 4-mm punch biopsy, hematoxylin and eosin stain, ×10 magnification, used with permission from Dr. Paul Harms.)
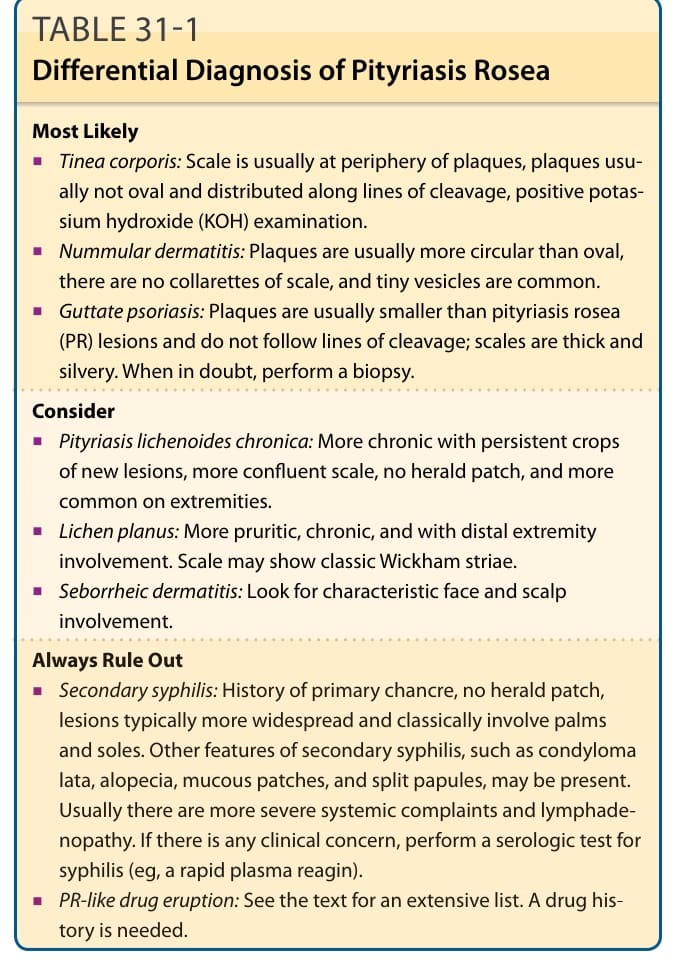
Table 31-1 outlines the differential diagnosis of PR. The differential diagnosis of PR includes various other papulosquamous disorders, including nummular eczema, guttate psoriasis, lichen planus, pityriasis lichenoides, tinea corporis, parapsoriasis, and