Psoriasis
PART4
Psoriasiform Disorders
AT-A-GLANCE
■ Worldwide occurrence; affects 2% to 3% of Americans; prevalence ranges from 0.1% to 3% in various populations.
■ A chronic disorder with polygenic predisposition combined with triggering environmental factors such as trauma, infection, or medication.
■ Erythematous scaly papules and plaques; pustular and erythrodermic eruptions occur.
■ Most common sites of involvement are the scalp, elbows, knees, hands, feet, trunk, and nails.
■ Psoriatic arthritis occurs in 10% to 25% of patients; pustular and erythrodermic forms may be associated with fever.
■ Pathology of fully developed lesions is characterized by uniform elongation of the rete ridges, with dilated blood vessels, thinning of the suprapapillary plate, and intermittent parakeratosis. Epidermal and perivascular dermal infiltrates of lymphocytes, with neutrophils occasionally in aggregates in the epidermis.
INTRODUCTION
DEFINITION
DEFINITION
Psoriasis is a common, immunologically mediated, inflammatory disease characterized by skin inflammation, epidermal hyperplasia, and increased risk of a painful and destructive arthritis as well as cardiovascular morbidity and psychosocial challenges. The economic and health burden of this constellation of pathologies is very substantial, yet its cause remains unknown.
HISTORICAL PERSPECTIVE
HISTORICAL PERSPECTIVE
More than 2000 years ago, Hippocrates used the terms psora and lepra for conditions that can be recognized as psoriasis. Later, Celsus (ca. 25 bc) described a form of impetigo that was interpreted by Robert Willan (1757–1812) as being psoriasis. Willan separated two diseases as psoriasiform entities, a discoid lepra Graecorum and a polycyclic confluent psora leprosa, which later was called psoriasis. In 1841, the Viennese dermatologist Ferdinand von Hebra (1816–1880) unequivocally showed that Willan’s lepra Graecorum and psora leprosa were one disease that had caused much confusion because of differences in the size, distribution, growth, and involution of lesions.
EPIDEMIOLOGY
PREVALENCE
PREVALENCE
Psoriasis is universal in occurrence. However, its reported prevalence in different populations varies considerably, from 0.91% in the United States to 8.5% in Norway.1 The prevalence of psoriasis is lower in Asians, and in an examination of more than 25,000 Andean Indians, not a single case was seen.2 Psoriasis appears to be equally common in males and females.
AGE OF ONSET
AGE OF ONSET
Psoriasis may begin at any age, but it is uncommon before the age of 10 years. It is most likely to appear between the ages of 15 and 30 years. Possession of certain human leukocyte antigen (HLA) class I antigens, particularly HLA-Cw6, is associated with an earlier age of onset and with a positive family history.
4
This finding led Henseler and Christophers3 to propose that two different forms of psoriasis exist: type I, with age of onset before 40 years and HLA associated, and type II, with age of onset after 40 years, although many patients do not fit into this classification.
GENETIC EPIDEMIOLOGY
GENETIC EPIDEMIOLOGY
The concordance rate for psoriasis in monozygotic twins ranges from 35% to 73%.4 This variability and the fact that these rates do not approach 100% support a role for environmental factors. Thus, the mode of inheritance for psoriasis is best described as multifactorial (ie, polygenic plus environmental factors). Interestingly, the overall prevalence of psoriasis,1 and the concordance of psoriasis in both monozygotic and dizygotic twins decreases with decreasing distance from the equator. These observations suggest that ultraviolet (UV) light exposure may be a major environmental factor interacting with genetic factors in psoriasis.
CLINICAL FEATURES
CUTANEOUS FINDINGS
CUTANEOUS FINDINGS
PLAQUE-TYPE PSORIASIS
The classic lesion of psoriasis is a well-demarcated, raised, red plaque with a white scaly surface (Fig. 28-1). Lesions can vary in size from pinpoint papules to plaques that cover large areas of the body. Under the scale, the skin has a glossy homogeneous erythema, and bleeding points appear when the scale is removed, traumatizing the dilated capillaries below (the Auspitz sign) (Fig. 28-2). Psoriasis tends to be a symmetric eruption, and symmetry is a helpful feature in establishing a diagnosis. Unilateral involvement can occur, however. The psoriatic phenotype may present a changing spectrum of disease expression even within the same patient. The Koebner phenomenon (also known as the isomorphic response) is the traumatic induction of psoriasis on nonlesional skin; it occurs more frequently during
A B C
D E F
458
A
B
flares of disease and is an all-or-none phenomenon (ie, if psoriasis occurs at one site of injury, it will occur at all sites of injury) (Fig. 28-3). The Koebner reaction usually occurs 7 to 14 days after injury, and from 25% to 75% of patients may develop trauma-related Koebner phenomenon at some point during their disease. Psoriasis vulgaris is the most common form of psoriasis, seen in approximately 90% of patients. Red, scaly, symmetrically distributed plaques are characteristically localized to the extensor aspects of the extremities; particularly the elbows and knees, along with scalp, lower lumbosacral, buttocks, and genital involvement (see Fig. 28-1). Other sites of predilection include the umbilicus and the intergluteal cleft. The extent of involvement varies widely from patient to patient. Lesions may extend laterally and become circinate because of the confluence of several plaques (psoriasis gyrata). Occasionally, there is partial central clearing, resulting in ringlike lesions (annular psoriasis) (Fig. 28-4). This is usually associated with lesional clearing and portends a good prognosis. Other clinical variants of plaque psoriasis have been described depending on the morphology of the lesions, particularly those associated with gross hyperkeratosis (see Fig. 28-4). Rupioid psoriasis refers to lesions in the shape of a cone or limpet. Ostraceous psoriasis, an infrequently used term, refers to a ringlike, hyperkeratotic concave lesion, resembling an oyster shell. Finally, elephantine psoriasis is an uncommon form characterized by thickly scaling, large plaques, usually on the lower extremities. A hypopigmented
4
A
B
ring (Woronoff ring) surrounding individual psoriatic lesions may occasionally be seen and is usually associated with treatment, most commonly UV radiation or topical corticosteroids (see Fig. 28-4). The pathogenesis of the Woronoff ring is not well understood but may result from inhibition of prostaglandin synthesis.
GUTTATE (ERUPTIVE) PSORIASIS
Guttate psoriasis (from the Latin gutta, meaning “a drop”) is characterized by eruption of small (0.5–1.5 cm in diameter) papules over the upper trunk and proximal extremities (Fig. 28-5). It typically manifests at an
459
4
A
B
C D
A B
C D
460
early age and as such is found frequently in young adults. This form of psoriasis has the strongest association to HLA-Cw6,5 and streptococcal throat infection frequently precedes or is concomitant with the onset or flare of guttate psoriasis.6 However, antibiotic treatment has not been shown to be beneficial or to shorten the disease course.7 Patients with a history of chronic plaque psoriasis may develop guttate lesions, with or without worsening of their chronic plaques.
SMALL PLAQUE PSORIASIS
Small plaque psoriasis resembles guttate psoriasis clinically but can be distinguished by its onset in older patients, by its chronicity, and by having somewhat larger lesions (typically 1–2 cm) that are thicker and scalier than in guttate disease. It is said to be a common adult-onset presentation of psoriasis in Korea and other Asian countries.8
INVERSE PSORIASIS
Psoriasis lesions may be localized in the major skin folds, such as the axillae, the genitocrural region, and the neck. Scaling is usually minimal or absent, and the lesions show a glossy sharply demarcated erythema, which is often localized to areas of skinto-skin contact (Fig. 28-6). Sweating is impaired in affected areas.
ERYTHRODERMIC PSORIASIS
Psoriatic erythroderma affects all body sites, including the face, hands, feet, nails, trunk, and extremities (Fig. 28-7). Although all the symptoms of psoriasis are present, erythema is the most prominent feature, and scaling is different compared with chronic stationary psoriasis. Instead of thick, adherent, white scale, there is superficial scaling. Patients with erythrodermic psoriasis lose excessive heat because of generalized vasodilatation, and this may cause hypothermia.
A B
4
Patients may shiver in an attempt to raise their body temperature. Psoriatic skin is often hypohidrotic because of occlusion of the sweat ducts, and there is an attendant risk of hyperthermia in warm climates. Lower extremity edema is common secondary to vasodilation and loss of protein from the blood vessels into the tissues. High-output cardiac failure and impaired hepatic and renal function may also occur. Psoriatic erythroderma has a variable presentation, but two forms are thought to exist. In the first form, chronic plaque psoriasis may worsen to involve most or all of the skin surface, and patients remain relative responsive to therapy. In the second form, generalized erythroderma may present suddenly and unexpectedly or result from nontolerated external treatment (eg, UVB, anthralin), thus representing a generalized Koebner reaction. Generalized pustular psoriasis (see later) may revert to erythroderma with diminished or absent pustule formation. Occasional diagnostic problems may arise in differentiating psoriatic erythroderma from other causes.
PUSTULAR PSORIASIS
Several clinical variants of pustular psoriasis exist: generalized pustular psoriasis (von Zumbusch type), annular pustular psoriasis, impetigo herpetiformis, and two variants of localized pustular psoriasis— pustulosis palmaris et plantaris and acrodermatitis continua of Hallopeau. In children, pustular psoriasis can be complicated by sterile, lytic lesions of bones and can be a manifestation of the SAPHO syndrome (synovitis, acne, pustulosis, hyperostosis, osteitis).
Generalized Pustular Psoriasis (von Zumbusch): This is a distinctive acute variant of psoriasis that is usually preceded by other forms of the disease. Attacks are characterized by fever that lasts several days and a sudden generalized eruption of sterile pustules 2 to 3 mm in diameter (Fig. 28-8). The pustules are disseminated over the trunk and extremities, including the nail beds, palms, and soles.
461
4
A
B
C
The pustules usually arise on highly erythematous skin, first as patches (see Fig. 28-8) and then become confluent as the disease becomes more severe. With prolonged disease, the fingertips may become atrophic. The erythema that surrounds the pustules often spreads and becomes confluent, leading to erythroderma. Characteristically, the disease occurs in waves of fevers and pustules. The cause of generalized psoriasis von Zumbusch type is unknown. Various provoking agents include infections, irritating topical treatment (Koebner phenomenon), and withdrawal of oral corticosteroids.9 This form of psoriasis is usually associated with prominent systemic signs and can potentially have life-threatening complications such as hypocalcemia, bacterial superinfection, sepsis, and dehydration. Severe pustular psoriasis can be difficult to control and requires a potent treatment regimen with rapid onset of action to avoid lifethreatening complications.
Exanthematic Pustular Psoriasis: Exanthematic pustular psoriasis tends to occur after a viral infection and consists of widespread pustules with generalized plaque psoriasis. However, unlike the von Zumbusch pattern, there are no constitutional symptoms, and the disorder tends not to recur. There is an overlap between this form of pustular psoriasis and acute generalized exanthematous pustulosis, a type of drug eruption.
462
Annular Pustular Psoriasis: Annular pustular psoriasis is a rare variant of pustular psoriasis. It usually presents in an annular or circinate form. Lesions may appear at the onset of pustular psoriasis, with a tendency to spread and form enlarged rings, or they may develop during the course of generalized pustular psoriasis. The characteristic features are pustules on a ringlike erythema that sometimes resembles erythema annulare centrifugum. Identical lesions are found in patients with impetigo herpetiformis, an entity defined by some as a variant of pustular psoriasis occurring in pregnancy. Onset in pregnancy is usually early in the third trimester and persists until delivery. It tends to develop earlier in subsequent pregnancies. Impetigo herpetiformis is often associated with hypocalcemia.9 There is usually no personal or family history of psoriasis.
Pustulosis Palmaris et Plantaris: Palmoplantar pustular psoriasis (PPPP) is a rare variant of pustular psoriasis that is localized to the palms and soles. It may coexist with chronic plaque psoriasis with approximately 27% of patients having concomitant chronic plaque psoriasis.10 It differs from chronic plaque psoriasis both in terms of genetic predisposition11 and transcriptional changes.12 Therefore, many authors make a distinction between palmoplantar pustulosis (PPP) and PPPP, in which chronic plaque psoriasis is present, although the lesions of PPPP and PPP
A
B
4
C
D
E
are indistinguishable by themselves both clinically and transcriptionally.12 Pustulosis palmaris et plantaris is more common in females (about 78%) with a median age of onset of 47 years.10 Psoriatic arthritis (PsA) can be seen with pustulosis palmaris et plantaris, with a prevalence of 13% to 25%.10 Smoking is strongly associated with pustulosis palmaris et plantaris, and about 80% of patients are tobacco smokers at the time of presentation.10
Acrodermatitis Continua of Hallopeau: Acrodermatitis continua of Hallopeau, also known as dermatitis repens, is an extremely rare localized sterile pustular eruption of the fingers and toes.13 It typically involves the distal portions of the fingers and
toes and may occur after minor trauma or infection. Pustules often coalesce to form lakes of pus and nail loss is common. Over time, sclerosis of the underlying soft tissues and osteolysis of the distal phalanges may occur. Similar to pustulosis palmaris et plantaris, it is more common in middle-aged women. Evolution of acrodermatitis continua into generalized pustular psoriasis has been described.13
SEBOPSORIASIS
A common clinical entity, sebopsoriasis presents with erythematous plaques with greasy scales localized to seborrheic areas (scalp, glabella, nasolabial folds,
463
4
perioral and presternal areas, and intertriginous areas). In the absence of typical findings of psoriasis elsewhere, distinction from seborrheic dermatitis is difficult. Sebopsoriasis may represent a modification of seborrheic dermatitis by the genetic background of psoriasis and is relatively resistant to treatment. Although an etiologic role of Pityrosporum remains unproven, antifungal agents may be useful.
NAPKIN PSORIASIS
Napkin psoriasis usually begins between the ages of 3 and 6 months and first appears in the diaper (napkin) areas as a confluent red area with appearance a few days later of small red papules on the trunk that may also involve the limbs. These papules have the typical white scales of psoriasis. The face may also be involved with red scaly eruption. Unlike other forms of psoriasis, the rash responds readily to treatment and tends to disappear after the age of 1 year.
LINEAR PSORIASIS
Linear psoriasis is quite rare. The psoriatic lesion presents as linear lesion most commonly on the limbs but may also be limited to a dermatome on the trunk. This may be an underlying nevus, possibly an inflammatory linear verrucous epidermal nevus (ILVEN) because these lesions resemble linear psoriasis both clinically and histologically. The existence of a linear form of psoriasis distinct from ILVEN is controversial.
NAIL CHANGES
Nail changes are frequent in psoriasis, being found in up to 40% of patients,14 and are rare in the absence of skin disease elsewhere. Nail involvement increases with age, with duration and extent of disease, and with the presence of PsA. Several distinct changes have been described and can be grouped according to the portion of the nail that is affected (Table 28-1). Nail pitting is one of the commonest features of psoriasis, involving the fingers more often than the toes (Fig. 28-9). Pits range from 0.5 to 2.0 mm in size and can be single or multiple. The proximal nail matrix forms the dorsal (superficial) portion of the nail plate, and psoriatic involvement of this region results in pitting caused by defective keratinization. Other alterations in the nail matrix resulting in deformity of the nail plate (onychodystrophy) include leukonychia, crumbling nail, and red spots in the lunula. Onychodystrophy has a stronger association with PsA than other nail changes.14 Oil spots and salmon patches are translucent, yellow-red discolorations observed beneath the nail plate often extending distally toward the hyponychium caused by psoriasiform hyperplasia, parakeratosis, microvascular changes, and trapping of neutrophils in the nail bed.15 Unlike pitting, which is also seen in alopecia areata and other disorders, oil spotting is considered to be nearly specific for psoriasis. Splinter hemorrhages result from capillary bleeding underneath the thin
464
NAIL SEGMENT INVOLVED CLINICAL SIGN
Proximal matrix Pitting, onychorrhexis, Beau’s lines
Intermediate matrix Leukonychia
Distal matrix Focal onycholysis, thinned nail plate, erythema of the lunula
Nail bed “Oil drop” sign or “salmon patch,” subungual hyperkeratosis, onycholysis, splinter hemorrhages
Hyponychium Subungual hyperkeratosis, onycholysis
Nail plate Crumbling and destruction plus other changes secondary to the specific site
Proximal and lateral nail folds Cutaneous psoriasis
Proximal and lateral nail folds Cutaneous psoriasis
Modified from Del Rosso JQ, et al. Dermatologic diseases of the nail unit. In: Scher RK, Daniel CR, eds. Nails: Therapy, Diagnosis, Surgery, 2nd ed. Philadelphia: WB Saunders; 1997; with permission. Copyright © Elsevier.
suprapapillary plate of the psoriatic nail bed. Subungual hyperkeratosis is caused by hyperkeratosis of the nail bed and is often accompanied by onycholysis (separation of the nail plate from the nail bed), which usually involves the distal aspect of the nail. Anonychia is total loss of the nail plate. Although nail changes are rarely seen in the localized pustular variant of pustulosis palmaris et plantaris, anonychia can be seen in other forms of pustular psoriasis.
HAIR AND SEBACEOUS GLANDS
Alopecia is not a common observation in scalp psoriasis clinically; however, both scarring and non-scarring forms of scalp alopecia have been reported (reviewed by Rittie and coworkers16). A recent study of nonscalp psoriasis demonstrated that psoriasis plaques have markedly fewer visible hairs than adjacent uninvolved or normal skin, without loss of hair shafts, and suggested that this might be related to sebaceous gland atrophy, which is profound in psoriasis.16
NONCUTANEOUS FINDINGS
NONCUTANEOUS FINDINGS
GEOGRAPHIC TONGUE
Geographic tongue, also known as benign migratory glossitis or glossitis areata migrans, is an idiopathic inflammatory disorder resulting in the local loss of filiform papillae. The condition usually presents as asymptomatic erythematous patches with serpiginous borders, resembling a map. These lesions characteristically have a migratory nature. Geographic tongue has been postulated to be an oral variant of psoriasis because these lesions show several histologic features of psoriasis, including acanthosis, clubbing of the rete
A
4
B
C D
ridges, focal parakeratosis, and neutrophilic infiltrate. Although the prevalence of geographic tongue is increased in psoriatic patients, this is a relatively common condition that is seen in many nonpsoriatic individuals, so its relationship to psoriasis needs further clarification.
PSORIATIC ARTHRITIS
Arthritis is a common extracutaneous manifestation of psoriasis seen in up to 40% of patients. It has a strong genetic component, and several overlapping subtypes exist. This condition is discussed in Chap. 65.
COMPLICATIONS
COMPLICATIONS
CARDIOVASCULAR MORBIDITY
Patients with psoriasis have an increased morbidity and mortality from cardiovascular events, particularly those with severe and long duration of psoriasis skin disease.17 Risk of myocardial infarction is particularly elevated in younger patients with severe psoriasis,18 and vascular inflammation as detected by
18F-fluorodeoxyglucose–positron emission tomography computed tomography (PET/CT) correlates directly with the extent of cutaneous involvement.19
In a recent study of 1.3 million German health care recipients, metabolic syndrome was 2.9-fold more frequent among patients with psoriasis, and the most common diagnoses were hypertension (35.6% in psoriasis vs 20.6% in control participants) and hyperlipidemia (29.9% vs 17.1%).20 Patients with psoriasis have also been shown to be at increased risk for rheumatoid arthritis (RA), Crohn’s disease, and ulcerative colitis20
as well as Hodgkin’s lymphoma and cutaneous T-cell lymphoma.21
PSYCHOSOCIAL RAMIFICATIONS
Psoriasis is emotionally disabling, carrying with it significant psychosocial difficulties. Emotional difficulties arise from concerns about appearance, resulting in lowered self-esteem, social rejection, guilt, embarrassment, emptiness, sexual problems, and impairment of professional ability.22 The presence of pruritus and pain can aggravate these symptoms. Psychological aspects can modify the course of illness; in particular, feeling stigmatized can lead to treatment noncompliance and worsening of psoriasis. Likewise, psychological stress
465
4
can also lead to depression and anxiety. The prevalence of suicidal ideation and depression in patients with psoriasis is higher than that reported in people with other medical conditions and the general population. A comparative study reported reduction in physical and mental functioning comparable with that seen in cancer, arthritis, hypertension, heart disease, diabetes, and depression.23 According to one survey, 79% of patients with severe psoriasis reported a negative impact on their lives.24
ETIOLOGY AND PATHOGENESIS
DEVELOPMENT OF LESIONS
DEVELOPMENT OF LESIONS
Detailed light, electron microscopic, immunohistochemical, and molecular studies of involved and uninvolved skin of newly appearing and established psoriatic lesions provide a useful framework for relating the many cellular events that take place in a psoriatic lesion. They are illustrated schematically in Fig. 28-10 and with actual photomicrographs in Fig. 28-11. The normal-appearing skin of psoriatic patients has long been known to manifest subclinical morphologic and biochemical changes, particularly involving lipid biosynthesis.25 In the initial pinheadsized macular lesions, there is marked edema, and mononuclear cell infiltrates are found in the upper dermis,26 usually confined to the area of one or two papillae. The overlying epidermis soon becomes spongiotic, with focal loss of the granular layer. The venules in the upper dermis dilate and become surrounded by a mononuclear cell infiltrate. Similar findings have been described in early macules and papules of psoriasis and in the uninvolved skin of guttate psoriasis.27
The clinical margins of somewhat larger lesions (0.5–1.0 cm) manifest doubling of epidermal thickness, increased metabolic activity of epidermal cells, and increased mast cells and dermal macrophages with increased mast cell degranulation, as well as increased dermal T cells and dendritic cells (DCs). Toward the center of these evolving lesions, there are increasing bandlike epidermal thickness, parakeratosis, and capillary elongation, as well as perivascular infiltration of lymphocytes and macrophages without exudation into the epidermis. Squamous cells manifest enlarged extracellular spaces with only a few desmosomal connections, and parakeratosis is typically mounded or spotty. More mature lesions of psoriasis manifest uniform elongation of rete ridges, with thinning of the epidermis overlying the dermal papillae.25 Epidermal mass is increased three to five times, and many more mitoses are observed, frequently above the basal layer. About 10% of basal keratinocytes are cycling in normal skin, but this value rises to 100% in lesional psoriatic skin.28 Widening of the extracellular spaces between keratinocytes persists but is less prominent than in developing lesions and is more uniform than
466
the typical spongiosis of eczematous skin lesions. The tips of the rete ridges are often clubbed or fused with adjacent ones, with thin, elongated, edematous papillae containing dilated, tortuous capillaries. Parakeratosis, with accompanying loss of the granular layer, is often horizontally confluent but may alternate with orthokeratosis. The inflammatory infiltrate around the blood vessels in the papillary dermis becomes more intense but still consists of lymphocytes, macrophages, DCs, and mast cells. Unlike the initial lesion and the transitional zone, lymphocytes are observed in the epidermis of the mature lesion. Neutrophils exit from the tips of a subset of dermal capillaries (the “squirting papillae”), leading to their accumulation in the overlying parakeratotic stratum corneum (Munro’s microabscesses) and, less frequently, in the spinous layer (spongiform pustules of Kogoj). Collections of serum can also be seen in the epidermis and stratum corneum.25
IMMUNOPATHOGENESIS OF PSORIASIS
IMMUNOPATHOGENESIS
OF PSORIASIS
LYMPHOCYTES
T cells play an essential role in psoriasis as demonstrated in 1996, when it was shown that psoriasis could be induced by injecting activated autologous T cells into uninvolved psoriatic skin transplanted onto severe combined immunodeficient mice.29 Early studies suggested that at least some T-cell responses are antigen specific because oligoclonal expansions of both CD4+ and CD8+ T cells have repeatedly been identified in psoriatic lesions.30 However, more recent studies using deep T-cell receptor (TCR) sequencing indicate most of the T cells in normal, uninvolved and lesional psoriatic skin are polyclonal with approximately equal diversity31 and thus may accumulate in response to the cytokine environment of the lesion. There is virtually no evidence for B-cell involvement or antibody-mediated processes in psoriasis. The bestcharacterized T cells are the CD4+ and CD8+ subsets. Predominantly of the memory phenotype (CD45RO+), these cells express the cutaneous lymphocyte antigen, a ligand for E-selectin, which is selectively expressed on skin capillaries and therefore provides them with access to the skin.32 Whereas CD8+ T cells are predominantly located in the epidermis, CD4+ T cells are predominantly located in the upper dermis. Epidermal T cells, particularly CD8+ cells, appear to have a critical role in development of psoriatic plaques as either blocking the entry of these cells into the epidermis,33 or neutralization of CD8+ T cells34 prevents development of psoriasis in a xenograft model. The cytokine profile of psoriatic lesions is rich in interferon (IFN)-γ, indicative of T helper 1 (Th1) polarization of CD4+ cells, and T cytotoxic 1 (Tc1) polarization of CD8+ cells (Fig. 28-12). Two other subsets of CD4+ T cells, stimulated by interleukin (IL)-23 and
Development of psoriatic lesions
A
L L L L
T L
B
L
L L
L
DC
4 4
Mc
C
L L
8
8 8 MP
4
Mc
DC
4
4
4
MP
DC
MP
4
Mc Mc
MP
4
4
D
Neu
8
8 8
8
MP
DC
Mc
4
L
8
8
4
L
Mc
4
8 8
DC
L
4 4
DC
4
MP
4
DC
MP
Mc Mc
4
Mc
MP
Mc
4
467
4
A
Uninvolved distant Uninvolved near edge
Activated edge Plaque center
B
characterized by production of IL-17 (Th17, ∼20% of T cells) or IL-22 (Th22, ∼15% of T cells), have been shown to play a major role in maintaining chronic inflammation in psoriasis35 (Fig. 28-13) as well as other autoinflammatory conditions. In addition to IFN-γ–producing Tc1 cells, CD8+ T-cells producing IL-17 (Tc17) and IL-22 (Tc22) are found in psoriasis, most of which localize to the epidermis. These T-cell subsets have considerable functional plasticity and conversions of Tc17 to Tc1 and Th17 to Th1 have been described. Regulatory T cells (Tregs) suppress immune responses in an antigen-specific fashion and are responsible not only for downregulating successful responses to pathogens but also for the maintenance of immunologic tolerance. Several different populations
468
of Tregs exist, but the best characterized one is the CD4+ CD25+ subset.36 Tregs manifest impaired inhibitory function and failure to suppress effector T-cell proliferation in psoriasis.37 Other “unconventional” lymphocytes implicated in the pathogenesis of psoriasis include natural killer (NK) cells, NK-T cells, γδ T-cells, mucosal-associated invariant T (MAIT) cells, and innate lymphoid cells (ILCs). These populations also represent important sources of IL-17, IFN-γ, tumor necrosis factor (TNF), and other cytokines.38,39
MYELOID CELLS
T cells in psoriatic lesions are in constant communication with DCs, which have a role in both the priming of
4
The cytokine network in psoriasis
Cathelicidin hBD2 LL37 IL-36
TGF-α AREG
IL-20 IL-19 IL36
TNF-α
IL-18
IL-8 / hBD2 chemokines
IL-17 IL-22 IL-26
DC
DC
IL-23
TNF-α
CD4+
CD
IL-12
IFN-γ
IL-12
IL-23
IL-12
p35
p40
TNF-α
CD8
IL-17 IL-22 IFN-γ
IL-7 IL-15
KCs
IL-17 IL-22
ILC3
IFN-γ
CD4+
Th17/Th22
Th1
Etanercept Adalimumab Infliximab Golimumab Certolizumab
IFN-f TNF-`
Th1
Th17 Th1 plasticity
IFN-f
Ustekinumab Cyclosporine RORyt inh
DC
p40 p19 IL23R
IL-23
Guselkumab Risankizumab Tildrakizumab
TNF-` IL-22 IL-17
Th17
Brodalumab Secukinumab Ixekizumab
adaptive immune responses and the induction of selftolerance (see Chap. 11; Fig. 28-13). Several subsets of DCs have been defined, and many of these are found in markedly increased numbers within psoriatic lesions.40 However, the specific role of each subset is still somewhat unclear. As noted earlier, macrophages are prominent in developing psoriasis lesions, with neutrophils appearing somewhat later. Studies in a mouse model that was used to implicate macrophages suggested
that neutrophils may be unnecessary for lesional development.41 However, neutrophils are likely to play a major role in pustular psoriasis by amplifying the local inflammatory reaction through secretion of proteases such as cathepsin G, elastase, and proteinase-3. These proteases are capable of processing inactive IL-36 family cytokines (IL-36α, IL-36β, and IL-36γ) secreted by keratinocytes into their active forms. When activated, IL-36 cytokines are strong activators of keratinocytes,
469
4
The inflammatory and genetic network in psoriasis
Epidermal differentiation
Interferon and antiviral signaling
LCE3Bdel SERPINB8 KLF4 KLF13 TP63
IFNLR1 RUNX3 STAT2 SOCS1 TYK2
IKBKE IFIH1 DDX58 TRIM65 RNF114
Autoinflammatory response
Th17 differentiation / IL-17 responses
IL36RN CARD14 AP1S3
TRAF3IP2 KLF4 NFKBIZ ETS1 IRF4
Tc1/Tc17
Predisposing factors Disease initiation Disease maintenance
Environment Microbes Smoking Trauma Stress Drugs
Neutrophil
β-Defensins 1and 2 S100A7-9 Chemokines
Keratinocyte activation and proliferation
Trigger Stressed cells
IL-36 Genotype
Nitric oxide TNF-α
IL-1β IL-6
IL-1β IL-6 TNF-α
60 genetic loci
LL-37
DNA-LL-37 complexes
Tonsil
Activation
DC DC
Crypt
Interferon-α
Dermal DC Plasmacytoid DC
Interferon-γ TNF-α
IL-17A
CXCR3 CCR6
Lymph
node
Th1
DC
Th17
IL-12 IL-1
T-cell
IL-23
Antigen presentation Putative autoantigens
HLA-Cw6 ERAP1 ERAP2 MICA Antigen
LL37 ADAMTSL5 KRT17 T resident memory
HLA-Cw6
T-cell migration
IL-17A IL-17F IL-22
Autoantigens
TCR
Tc17
Tc1/Tc17
Tc1/ Tc17
Tc1
Th17
CD45RO
DC
VLA-1
Th17
Oxidative response
Tc1 Tc1
Th2
NOS2 O2 –
TIP DC
CCL19
Tc1 Tc1
Chemokines
Macrophage
TNF/ NF-jB signaling
KGF-1/2 TGF-β
TNIP1 TNFAIP3 NFKBIZ NFKBIA REL UBE2C3
IKBKE
CCR4
TNFSF15 CHUK ZC3H12C CARD14
Putative autoantogen presentation TNF-α TGF-β IL-1α
Th1
Th17
T-cell development
TNFRSF9 DENND1B B3GNT2
IL4/IL13 TAGAP ELMO1
ZNF683 KLRK1/ KLRC4
RUNX1 FASLG IL31
Fibroblast
Effector cells recirculate and migrate into skin tissue Collagen and proteoglycans
UBE2L3
IL-23 signaling
IL23R TYK2 IL23A STAT3 IL12B
470
4
Proposed model integrating the genetics and immunology of psoriasis
LCE3B/LCE3C
ERAP1
PSMA6
HLA-Cw6
KC DC
Tc17 Tc17
NF-κB
DEFB CNV
TRAF3IP2
IL-17R Th2
Th22
IL-17
IL4/IL13
IL23R
Th1 Th17
IFN-γ
IL23A
IL12B
Th17
NOS2
Th17
DC
Tc1 Tc1
DC
TLR ligands
TNF-α
TNFAIP3
TNIP1
NFKBIA
FBXL19
NF-κB
leading to secretion of chemotactic proteins, particularly neutrophil chemokines, thereby amplifying and sustaining the inflammatory process.
KERATINOCYTES
Comprising the bulk of the epidermis and its appendages, keratinocytes are a major producer of proinflammatory cytokines, chemokines, and growth factors, as well as other inflammatory mediators such as eicosanoids and mediators of innate immunity such as cathelicidins, defensins, and S100 proteins. Psoriatic keratinocytes are engaged in an alternative pathway of keratinocyte differentiation called regenerative maturation.42 Regenerative maturation is activated in response to immunologic stimulation. Besides keratinocytes, other skin-resident cell types, such as endothelial cells and fibroblasts, are also likely participants in the pathogenic process.40
GENETICS OF PSORIASIS
GENETICS OF PSORIASIS
In recent years, many genetic variants contributing to psoriasis susceptibility have been identified, initially
through linkage studies and more recently through genome-wide association studies (GWAS). An overview of the major genetically-implicated pathways in psoriasis is provided in Fig. 28-14, and a list of genetic loci identified to date is provided in Table 28-2.
MAJOR HISTOCOMPATIBILITY COMPLEX GENES
Overall, the major histocompatibility complex (MHC) accounts for the bulk of the overall genetic risk for psoriasis. Thus, although 63 currently known Europeanorigin signals explain 28% of the genetic heritability of psoriasis, MHC signals alone contribute 11.2% of the 28%, or about 40% of the detectable heritability.43
The major genetic signal for psoriasis in the MHC is HLAC∗0602, which encodes HLA-Cw6 protein.44,45
HLA-Cw6 presents antigens to CD8+ T cells, which are MHC class I restricted and comprise about 80% of the T cells in the epidermis of psoriatic lesions (Fig. 28-15). CD8+ T cells selectively traffic to the epidermis because they express integrin α1β1, which binds to Type IV basement membrane collagen33 as well as integrin αEβ7, which binds to keratinocyte E-cadherin.46
471
4
ERAP1, LNPEP 5q15 ● ● 20953187, 20953190, 23143594 Both genes encode endoplasmic reticulum aminopeptidases involved in trimming HLA class I-binding peptide precursors for antigen presentation. ERAP1 acts as a monomer or ERAP1/2 heterodimer. Epistasis with HLA class I in AS and Behçet disease.
TP63 3q28 ●
25903422 Encodes a member of the p53 family of TFs; essential for epidermal development in mice; mutations associated with ectodermal dysplasia, cleft lip or palate, and others; epidermal overexpression results in an AD-like phenotype
IL12B 5q33.3 ● ● 17236132, 19169254, 19169255, 20953186, 20953190
4
(Continued)
IRF4 6p25.3 ●
23143594 Encodes a TF that regulates IL17A promoter activity and Th17-mediated colitis in vivo; stabilizes the Th17 phenotype through IL-21; associated with pigmentation, RA, lymphoma, leukemia, and schizophrenia
HLA-C, HLA-B, HLA-A, HLA-DR 6p21.33 ● ● 19169254, 19169255, 19680446, 20953190, 25087609
4
RPS6KA4, PRDX5 11q13.1 ●
22482804 RPS6KA4: serine/threonine kinase that phosphorylates CREB1, ATF1, and histone H3 to regulate genes involved in inflammation PRDX5: a protective antioxidant enzyme
BRAP, MAPKAPK5 12q24.12 ●
29553248 BRAP: sequesters BRCA1 to the cytoplasm MAPKAPK5: tumor suppressor activated by MAPKs in response to cell stress and inflammatory cytokines; phosphorylates HSP27
IL23A, STAT2 12q13.3 ●
19169254 IL23A: encodes p19 subunit of IL-23, which acts on memory CD4+ T cells to induce STAT4 and IFN-γ STAT2: transcriptional activator; complexes with STAT1 in response to IFN
NFKBIA, PSMA6 14q13.2 ● ● 20953189, 20953190, 24070858 NFKBIA: moves between cytoplasm and nucleus to inhibit NF-κB; mutations associated with ectodermal dysplasia with T-cell immunodeficiency PSMA6: encodes a proteasomal subunit involved in cleavage of MHC class I peptides
4
(Continued)
CARD14 17q25.3 ● ● 23143594, 24212883 A caspase recruitment domain-containing protein of the MAGUK family, members of which act as scaffold proteins in cell adhesion, cell polarity, and signal transduction; interacts with BCL10 to activate NF-κB and promote apoptosis
4
RNF114, SNAI1 20q13.13 ●
18364390, 23143594 RNF114: ubiquitin-protein ligase that degrades the inhibitor of CDKN1A to induce G1-to-S phase transition SNAI1: zinc finger transcriptional repressor involved in mesodermal development
POLI, STARD6, MBD2 18q21.2 ●
23143594 POLI: DNA polymerase involved in DNA repair and in mutation of immunoglobulin genes STARD6: homologous to STAR proteins involved in sterol transport MBD2: methyl-CpG binding protein that can repress or activate transcription
AD, atopic dermatitis; AKT, serine/threonine kinase 1; AP-1, activator protein-1; APC, anaphase-promoting complex; AS, ankylosing spondylitis; ATF1, activating transcription factor-1; BMI, body mass index; CBL, Casitas B-lineage Lymphoma; CD, Crohn’s disease; CREB1, cAMP responsive element binding protein 1; DC, dendritic cell; dsDNA, double-stranded DNA; GPCR, G-protein coupled receptor; HLA, human leukocyte antigen; HPV, human papillomavirus; IKKε, I-κB kinase epsilon; IL, interleukin; IFN, interferon; iNOS, inducible nitric oxide synthase; JAK, Janus kinase; KC, keratinocyte; KIR, killer immunoglobulin-like receptor; LCE, late cornified envelope; MAGUK, membrane-associated guanylate kinase; MAPK, mitogen-activated protein kinase; MHC, major histocompatibility complex; MS, multiple sclerosis; NF-κB, nuclear factor kappa B; NK, natural killer; PDZ, post-synaptic density, Dlg1, and ZO-1 protein; PKB, protein kinase B; PsA, psoriatic arthritis; PsC, purely cutaneous psoriasis; RA, rheumatoid arthritis; REL, proto-oncogene c-REL; RELA, proto-oncogene, NF-κB subunit; RIP, receptor-interacting kinase; SCC, squamous cell carcinoma; SLE, systemic lupus erythematosus; STAT, signal transducer and activator of transcription; T1D, type 1 diabetes; T2D, type 2 diabetes; TCR, T-cell receptor; TF, transcription factor; TGF, transforming growth factor; Th, T helper; TNF, tumor necrosis factor; TRAF, TNF receptor-associated factor; TYK2, tyrosine kinase 2; UC, ulcerative colitis; UV, ultraviolet; RIPKs, receptor-interacting protein kinase.
Functionally, epidermal invasion by CD8+ T cells correlates with lesional development in a xenograft model of psoraisis.47 Further emphasizing the importance of MHC class I antigen presentation, several other MHC class I risk variants are associated with psoriasis independently of HLA-Cw6 in both European-origin45
and Chinese populations.48 The fact that oligoclonal T-cell expansions are found in CD8+ T-cells in psoriatic skin30 suggests that in the epidermis, CD8+ T cells “interrogate” peptides bound to HLA-Cw6 on the surface of dendritic antigen-presenting cells (APCs) and expand in response to one or more specific antigens (see Figs. 28-14 and 28-15). The nature of these antigens remains a topic of active investigation. Besides candidate antigens described in previous editions of this chapter, three recent publications have implicated additional candidate autoantigens in psoriasis, including the antimicrobial protein LL37,49 neolipid antigens generated by mast cell phospholipase and presented by the MHC -like class I antigen-presenting protein CD1a,50 and the melanocyte
4
antigen ADAMTSL5. Of these, the ADAMTSL5 antigen is of genetic interest because it is presented specifically by HLA-Cw6.51 Of note, recent immunohistochemical data suggest that expression of ADAMTSL5 may not be limited to melanocytes.52 Although much remains to be learned about specific autoantigens, the observations that multiple HLA alleles are implicated genetically and that expanded TCR rearrangements are usually oligoclonal in nature suggest that multiple autoantigens may be involved in the pathogenesis of psoriasis. CD4+ T cells predominate in the dermis of psoriasis lesions and are also clonally expanded in psoriasis. CD4+ T cells are also required for the development of psoriasis lesions from uninvolved skin in a xenograft model.53 This is consistent with the identification of genetic signals in the MHC class II region in both European-origin45 and Chinese48 populations. Although CD4+ and CD8+ memory T cells can traffic among the skin, lymph nodes, and blood, increasing evidence indicates that when initially activated in the cutaneous environment, they spend most of their time
Proposed role of HLA-Cw6 in the pathogenesis of psoriasis
Crosspresentation of antigens
8
Activation and proliferation of memory T cells in dermis
4
CD8 T cell
4
Cα Cβ
T-cell receptor CD8
Vα
Vβ
HLA-Cw6-Ag
TCR
8
Cytokines sublethal injury?
Ag
Activation and proliferation of naive T cells in lymph nodes
8
Lymphatics
Dermal blood vessels
Antigen
α2 α1
HLA-Cw6
α3 β2m
Keratinocyte or DC
4
477
4
in the skin site at which they were activated, as resident memory T cells.32 This would be consistent with the behavior of psoriatic plaques, which tend to recur in the same body sites after therapeutic or spontaneous improvement.
NON-MAJOR HISTOCOMPATIBILITY COMPLEX GENES
Over the past decade, GWAS have identified 86 genomic regions that are associated with psoriasis at genome-wide significance (see Table 28-2). Eleven of the 86 known psoriasis risk loci are shared by European and Chinese populations, 55 loci have been established for Europeans only, and 20 loci have been established for Chinese only. Sixteen loci have also been established as susceptibility loci for PsA and 12 for purely cutaneous psoriasis.45,54,55 Perhaps surprisingly, most of the genetic signals identified in psoriasis thus far do not affect the structure of a protein and instead are regulatory in nature.43 Moreover, because of topologic looping of DNA in chromatin, the regulatory signals affected by genetic variation may lie at a substantial distance from the causal gene being regulated. Thus, the “candidate genes” listed in Table 28-2 cannot simply be assumed to be the causal genes underlying the observed associations. However, there is strong bioinformatic evidence indicating that the genes underlying these psoriasis genetic signals are disproportionately involved in immunity and host defense, including functions such as lymphocyte differentiation and regulation, type I IFN and pattern recognition, nuclear factor kappa B (NF-κB) signaling, and response to viruses and bacteria.43 Correspondingly, psoriasis signals are enriched in regulatory elements active in several T-cell subsets, including CD8+ T cells, and CD4+ T-cell subsets, including Th0, Th1, and Th17.43 Thus, there can be little doubt that “psoriasis genes” are involved in various aspects of immunity and host defense even if many of them remain to be formally identified. Most of the non-MHC associations identified thus far fall into several interconnected functional axes: IL-23–IL-17 signaling, interferon signaling, NF-κB signaling, DC–macrophage function, and keratinocyte responses (see Fig. 28-14 and Table 28-2).
IL-23–IL-17 Signaling: Three strong regions of association map near genes involved in IL-23 signaling: IL12B (encoding the p40 subunit of IL-23 and IL-12), IL23A (encoding the p19 subunit of IL-23), and IL23R (encoding a subunit of the IL-23 receptor). These associations are further supported by the impressive efficacy of biologics targeting the p40 subunit common to IL-12 and IL-2356 as well as the p19 subunit,57 which is unique to IL-23. IL-23 signaling promotes the survival and expansion of IL-17–expressing T-cells, which protect epithelia against microbial pathogens.58 Ankylosing spondylitis (AS) is another HLA class I–associated autoimmune disorder that is clinically associated with inflammatory bowel disease59 and genetically associated with IL23R.60 PsA shares a number of clinical similarities with AS, and is genetically associated with
478
IL12B, IL23A, and IL23R (see Chap. 65). Other candidate genes relevant to this signaling axis include TRAF3IP2 encoding Act1; a ubiquitin ligase coupling IL-17 receptors to downstream signaling pathways; RUNX3, which encodes a transcription factor (TF) required for development of Th17 cells; NFKBIZ, a TF whose expression is stimulated by IL-17 via Act161; and IRF4, encoding a TF that regulates IL-17A promoter activity.
Interferon Signaling: Although the IFNG gene does not itself map to a psoriasis susceptibility region, its product IFN-γ is secreted by activated Th1 cells and stimulates DC to produce IL-23.62 This may explain why Th1 and Th17 cells are co-localized in psoriasis lesions and many other sites of inflammation.62 Another psoriasis susceptibility region contains the IL4 and IL13 genes. In addition to biasing T-cell differentiation away from Th1 and toward Th2, IL-4 inhibits Th17 cell development.63 Moreover, treatment of psoriasis with IL-4 resulted in significant clinical improvement by selective silencing of IL-23 in APCs.64 Other psoriasis genetic signals suggest involvement of Type I IFN signaling in disease pathogenesis, including associations with DDX58 encoding RIG-I and IFIH1 encoding MDA5. Each of these proteins bind viral nucleic acids and activate the mitochondrial antiviral signaling protein (MAVS), leading ultimately to activation of type I IFNs and IFN-stimulated genes as well as NF-κB.65 TYK2 encodes Tyk2, which also prominently involved in downstream type I IFN signaling and mediates responses to several other cytokines.66
NF-jB Signaling: Several psoriasis-associated genomic regions contain genes involved with controlling signaling through the TF NF-κB. TNF-α is a major activator of NF-κB signaling, and these associations are clinically reinforced by the dramatic therapeutic response of psoriasis to anti-TNF biologicals (see Treatment). TNFAIP3 and TNIP1, respectively, encode A20 and ABIN-1, which interact with each other to regulate the ubiquitin-mediated destruction of IKKγ/ NEMO, a central nexus of NF-κB signaling.67 TNFAIP3 is genetically associated with RA, and both TNFAIP3 and TNIP1 are associated with systemic lupus erythematosus (SLE). The polymorphisms implicated in RA and SLE show no association with psoriasis, suggesting that each of these diseases is driven by different variants of the TNFAIP3 gene. CHUK encodes IKK-α, which activates NF-κB via degradation of IκBα, and NFKBIA encodes IκBα, which inhibits NF-κB signaling by sequestering it in the cytoplasm. Other notable candidate genes in this category include FASLG encoding Fas ligand (CD95), a transmembrane protein of the TNF family; REL and NFKB1, both of which encode members of the NF-κB family; TNFSF15 encoding TL1, a TNF-inducible cytokine that activates NF-κB; IKBKE encoding IKK-ε, which functions downstream of viral sensors to activate NF-κB; and CARD14 encoding CARMA2, which activates NF-κB via interactions with BCL10. Notably, CARD14 has been identified as the causative gene in the PSORS2 locus, initially identified in a large pedigree by linkage analysis.68
Dendritic Cell and Macrophage Function: Besides the MHC, two other regions of association contain genes whose products function in antigen presentation: PSMA6, which encodes a proteasomal subunit involved in MHC class I antigen processing, and ERAP1, an IFN-γ–inducible aminopeptidase that trims peptides for optimal binding to the MHC class I peptide groove. Macrophages and inflammatory DCs are major sources of IL-23, TNF-α and inducible nitric oxide synthetase (iNOS). Psoriasis risk variants are present in NOS2 (encoding iNOS) and ZC3H12C encoding the zinc-finger protein MCPIP3, both of which are important for macrophage function.
Keratinocyte Responses: Although the TNF-α and IL-23–Th17 axes described above converge strongly at a physiological level to stimulate production of innate inflammatory mediators such as hBD2 by keratinocytes,69 relatively few psoriasis-associated regions contain genes that are thought to function primarily in keratinocytes. The most well-established association is an insertion-deletion (indel) polymorphism of the late cornified envelope genes LCE3B and LCE3C, which was independently discovered in European-origin70 and Chinese71 populations. Located in the epidermal differentiation complex (EDC), these genes are expressed very late in keratinocyte terminal differentiation and are markedly overexpressed in psoriasis, wound healing, and epidermal stress.72 Notably, the LCE3B/3C indel is associated with cutaneous psoriasis but not with PsA.54 Another psoriasis risk variant resides near the KLF4 gene, which is a TF required for establishment of skin barrier function. TRAF3IP2- and NFKBIZ –encoded proteins are known to function in IL-17 responses of epidermal cells, and several genes implicated in the pathogenesis of generalized or PPPP are primarily expressed in the epidermis, including IL36RN, AP1S3, and CARD14.
OTHER RISK FACTORS
OTHER RISK FACTORS
OBESITY
It has been demonstrated that obese individuals are more likely to present with severe psoriasis. However, obesity does not appear to have a role in defining the onset of psoriasis.73
SMOKING
Heavy smoking (>20 cigarettes daily) has been associated with more than a twofold increased risk of severe psoriasis.74 Unlike obesity, smoking appears to have a role in the onset of psoriasis.73
INFECTIONS
An association between streptococcal throat infection and guttate psoriasis has been repeatedly confirmed.
4
Streptococcal throat infections have also been demonstrated to exacerbate preexisting chronic plaque psoriasis,75 and tonsillectomy has been shown to lead to long-term improvement in psoriasis,76 particularly in HLA-Cw6 carriers.77 Severe exacerbation of psoriasis can be a manifestation of HIV infection. The prevalence of psoriasis in HIV infection is no higher than in the general population, indicating that this infection is not a trigger for psoriasis but rather a modifying agent. Psoriasis is increasingly more severe with progression of immunodeficiency but can remit in the terminal phase. This paradoxical exacerbation of psoriasis may be caused by loss of Tregs and increased activity of the CD8 T-cell subset.78 Psoriasis exacerbation in HIV disease may be effectively treated with antiretroviral therapy. Psoriasis has also been associated with hepatitis C infection.
DRUGS
Medications that exacerbate psoriasis include antimalarials, β blockers, lithium, nonsteroidal antiinflammatory drugs (NSAIDs), IFNs-α and -γ, imiquimod, angiotensin-converting enzyme inhibitors, and gemfibrozil. Imiquimod acts on plasmacytoid dendritic cells (pDCs) and stimulates IFN-α production, which then strengthens both innate and Th1 immune responses.79
Exacerbations and onset of psoriasis have been described in patients receiving TNF inhibitor therapy. The majority of these patients have PPP, but about one third develop chronic plaque psoriasis.80 New-onset psoriasis has also been described after the anti-IL-6 treatment tocilizumab. Lithium has been proposed to cause exacerbation by interfering with calcium release within keratinocytes, whereas β blockers are thought to interfere with intracellular cyclic adenosine monophosphate levels.81 The mechanisms by which the remaining medications exacerbate psoriasis are largely unknown.
DIAGNOSIS
An algorithm for the diagnosis and treatment of psoriasis is presented in Fig. 28-16.
PATHOLOGY
PATHOLOGY
Although histopathologic examination is rarely necessary to make the diagnosis of psoriasis, it can be helpful in difficult cases. The histopathologic manifestations of guttate and chronic plaque psoriasis have already been described (see Development of Lesions).
LABORATORY TESTING
LABORATORY TESTING
Laboratory abnormalities in psoriasis are usually not specific and may not be performed in all patients.
479
4
Diagnosis and treatment algorithm for patients with psoriasis
Diagnosis not obvious
Not psoriasis See DDx
Clinical impression
Features supporting a diagnosis of psoriasis – Symmetry of lesions – Extensor distribution – Auspitz sign – Sharply demarcated lesions – Silvery scale
Psoriasis Biopsy
Erythrodermic/ pustular psoriasis – Acitretin – Cyclosporine A – PUVA, NB-UVB – Methotrexate – Anti-TNF agents – Anti-IL17A agents – Anti-p40 (ustekinumab) – Systemic steroids*
Severe, >30% BSA
Day treatment center – Modified Goeckerman Systemic Tx First line – Methotrexate – Acitretin – Apermilast – Biologicals – Etanercept – Adalimumab – Infliximab – Ustekinumab – Secukinumab – Ixekizumab Second line – FAE – Cyclosporine A – Other agents: – Hydroxyurea – 6-thioguanine – Cellcept – Sulfasalazine
Guttate psoriasis – No treatment – NB-UVB – Topical treatment – Vitamin D3 analog – Topical steroids
Chronic plaque psoriasis
Moderate, >10% BSA
Mild,<10% BSA
Phototherapy First line – NB-UVB – BB-UVB Second line – PUVA – Excimer – Climatotherapy
Topical Tx First line – Emollients – Glucocorticoids – Vitamin D3 analogs Second line – Salicylic acid – Dithranol – Tazarotene – Tar
480
In severe psoriasis vulgaris, generalized pustular psoriasis, and erythroderma, a negative nitrogen balance can be detected, manifested by a decrease of serum albumin. Patients with psoriasis manifest altered lipid profiles, even at the onset of their skin disease.82 Whether these differences in lipid profile can explain or are contributing to an increased incidence of cardiovascular events in psoriasis remains to be seen. The serum uric acid is elevated in up to 50% of patients and is mainly correlated with the extent of lesions and the activity of disease. There is an increased risk of developing gouty arthritis. Serum uric acid levels usually normalize after therapy. Markers of systemic inflammation, including C-reactive protein, α2-macroglobulin, and erythrocyte sedimentation rate, can be increased. However, such elevations are rare in chronic plaque psoriasis uncomplicated by arthritis. Increased serum immunoglobulin (Ig) A levels and IgA immune complexes, as well as secondary amyloidosis, have also been observed in psoriasis, and the latter carries a poor prognosis.
DIFFERENTIAL DIAGNOSIS
A schema for the differential diagnosis of psoriasis is presented in Table 28-3.
4
CLINICAL COURSE AND PROGNOSIS
NATURAL HISTORY
NATURAL HISTORY
It is useful to determine the age at onset and the presence or absence of a family history of psoriasis because a younger age of onset and positive family history have been associated with more widespread and recurrent disease.3,14 In addition, the physician should inquire about the prior course of the disease because major differences exist between “acute” and “chronic” disease. In the latter form, lesions may persist unchanged for months or even years, but acute disease shows sudden outbreak of lesions within a short time (days). Likewise, patients have great variability in regard to relapses. Some patients have frequent relapses occurring weekly or monthly, but others have more stable disease with only occasional recurrence. The frequently relapsing patients tend to develop more severe disease with rapidly enlarging lesions covering significant portions of the body surface83 and may require more rigorous treatment than those with more stable disease. The physician should also inquire about joint complaints. Although osteoarthritis is extremely common and can coexist with psoriasis, a history of onset of joint symptoms
PSORIASIS VULGARIS GUTTATE ERYTHRODERMIC PUSTULAR
Most Likely
Most Likely
Most Likely
Most Likely
■Discoid/nummular eczema
■Pityriasis rosea
■Discoid/nummular eczema
■Pityriasis rosea
■Cutaneous T-cell lymphoma (CTCL)
■Pityriasis lichenoides chronica
■Cutaneous T-cell lymphoma (CTCL)
■Pityriasis lichenoides
■Tinea corporis Consider
■Tinea corporis Consider
chronica
■Lichen planus Consider
■Lichen planus Consider
■Pityriasis rubra pilaris
■Pityriasis rubra pilaris
■Seborrheic dermatitis
■Small plaque parapsoriasis
■Seborrheic dermatitis
■Small plaque parapsoriasis
■Subacute cutaneous lupus erythematosus
■Pityriasis lichenoides et varioliformis acuta
■Subacute cutaneous lupus
■Pityriasis lichenoides et
erythematosus
varioliformis acuta
■Erythrokeratoderma (the fixed plaques of keratoderma variabilis or progressive symmetric erythrokeratoderma
■Lichen planus
■Erythrokeratoderma (the fixed
■Lichen planus
■Drug eruption Always Rule Out
■Drug eruption Always Rule Out
plaques of keratoderma variabilis or progressive symmetric erythrokeratoderma
■Secondary syphilis
■Secondary syphilis
■Inflammatory linear verrucous epidermal nevus
■Inflammatory linear verrucous
epidermal nevus
■Hypertrophic lichen planus
■Hypertrophic lichen planus
■Lichen simplex chronicus
■Lichen simplex chronicus
■Contact dermatitis
■Contact dermatitis
■Chronic cutaneous lupus erythematosus/discoid lupus erythematosus
■Chronic cutaneous lupus erythema-
tosus/discoid lupus erythematosus
■Hailey-Hailey disease (flexural)
■Hailey-Hailey disease (flexural)
■Intertrigo (flexural)
■Intertrigo (flexural)
■Candida infection (flexural) Always Rule Out
■Candida infection (flexural) Always Rule Out
■Bowen disease or squamous cell carcinoma in situ
■Bowen disease or squamous cell
carcinoma in situ
■Extramammary Paget disease
■Extramammary Paget disease
Most Likely
Most Likely
Most Likely
Most Likely
■Drug-induced erythroderma
■Impetigo
■Drug-induced erythroderma
■Impetigo
■Eczema
■Superficial candidiasis
■Eczema
■Superficial candidiasis
■CTCL or Sézary syndrome
■Reactive arthritis syndrome
■CTCL or Sézary syndrome
■Reactive arthritis syndrome
■Pityriasis rubra pilaris
■Superficial folliculitis Consider
■Pityriasis rubra pilaris
■Superficial folliculitis Consider
■Pemphigus foliaceus
■Pemphigus foliaceus
■Immunoglobulin A pemphigus
■Immunoglobulin A pemphigus
■Sneddon-Wilkinson disease (subcorneal pustular dermatosis)
■Sneddon-Wilkinson disease
(subcorneal pustular dermatosis)
■Migratory necrolytic erythema
■Migratory necrolytic erythema
■Transient neonatal pustular melanosis
■Transient neonatal pustular
melanosis
■Acropustulosis of infancy
■Acropustulosis of infancy
■Acute generalized exanthematous pustulosis
■Acute generalized exanthema-
tous pustulosis
481
4
before the fourth decade or a history of warm, swollen joints should raise the suspicion of PsA (see Chap. 65). Guttate psoriasis is often a self-limited disease, lasting from 12 to 16 weeks without treatment. It has been estimated that one third to two thirds of these patients later develop the chronic plaque type of psoriasis.84 In contrast, chronic plaque psoriasis is in most cases a lifelong disease, manifesting at unpredictable intervals. Spontaneous remissions, lasting for variable periods of time, may occur in the course of psoriasis in up to 50% of patients. The duration of remission ranges from 1 year to several decades. Erythrodermic and generalized pustular psoriasis have a poorer prognosis, with the disease tending to be severe and persistent.
MANAGEMENT
GENERAL CONSIDERATIONS
GENERAL CONSIDERATIONS
TOPICAL STEROIDS VITAMIN D ANALOGUES TAZAROTENE CALCINEURIN INHIBITORS
Mechanism of action Bind to glucocorticoid receptors, inhibiting the transcription of many different AP-1– and NF-κB–dependent genes, including IL-1 and TNF-α
Bind to vitamin D receptors, influencing the expression of many genes; promote keratinocyte differentiation
Dosing 10,000-fold range of potency; high-potency steroids are applied to affected areas twice daily for 2–4 wk and then intermittently (weekends)
Calcipotriene, 0.005%, to affected areas twice daily; often used alternating with topical steroids (ie, vitamin D analogues on weekdays; topical steroids on weekends)
Metabolized to tazarotenic acid, its active metabolite, which binds to retinoic acid receptors; normalizes epidermal differentiation, exhibits a potent antiproliferative effect, and decreases epidermal proliferation
Bind to FKBP and inhibit calcineurin, decreasing the activation of the transcription factor, NF-AT, with resultant decrease in cytokine transcription, including IL-2
Available in 0.05% and 0.1% formulations, both as cream and gels; apply every night to affected area
Application to affected areas twice daily
Efficacy Very effective as short-term treatment Efficacy is increased by combination with topical steroids; can be combined with various other therapies
Safety Suppression of the hypothalamic–pituitary– adrenal axis (higher risk in children); atrophy of the epidermis and dermis; formation of striae; tachyphylaxis
Efficacy is increased by combination with topical steroids
Effective for treatment of facial and flexural psoriasis but minimally for chronic plaque psoriasis
Development of irritation at the site of application is common; isolated reports of hypercalcemia in patients who applied excessive quantities
When used as monotherapy, significant proportion of patients develop irritation at the site of application
Burning sensation at the site of application; case reports of development of lymphoma
Contraindications Hypersensitivity to the steroid, active skin infection Hypercalcemia, vitamin D toxicity Pregnancy, hypersensitivity to tazarotene Use only with caution for treatment of children younger than 2 yr of age
Remarks and long-term use Long-term use increases risk of side effects Calcipotriol is well tolerated and continues to be clinically effective with minimum of adverse effects in long-term use
Pregnancy
Combination of steroid with tazarotene may reduce atrophy seen with superpotent topical steroids; if added during phototherapy, the UV doses should be reduced by one third
Because of anecdotal reports of association with malignancy, this class of medications recently received a black-box warning by the FDA
C C X C
Pregnancy Category C C X C
Category
AP, activator protein; FDA, Food and Drug Administration; FKBP, FK506-binding protein; IL, interleukin; NF-AT, nuclear factor of activated T cells; NF-κB , nuclear factor kappa B; UV, ultraviolet.
482
4
NARROWBAND UVB (NB-UVB; 310–331 NM) BROADBAND UVB (BB-UVB) PSORALEN AND UVA LIGHT (PUVA) EXCIMER LASER (308 NM)
Dosing Dosage based on either the Fitzpatrick skin type or MED; determine MED; initial treatment at 50% of MED followed by three to five treatments weekly; lubricate before treatment Treatments 1–20: increase by 10% of initial MED Treatments ≥21: increase as ordered by physician Maintenance therapy after >95% clearance: once a week for 4 wk; keep dose the same once every two weeks for 4 weeks; decrease dose by 25% once every 4 weeks, 50% of highest dose
The dose of energy delivered is guided by the patient’s skin type and thickness of plaque; further doses are adjusted based on response to treatment or development of side effects; treatment usually given twice weekly
The dosage may be administered according to the Fitzpatrick skin type; initial treatment at 50% of MED followed by three to five treatments weekly Treatments 1–10: increase dose by 25% of initial MED Treatments 11–20: increase by 10% of initial MED Treatments ≥21: increase as ordered by physician
Efficacy >70% improvement in a split-body study after 4 wk of treatment; 9 of 11 patients showed clearance; more effective than BB-UVB
Dose based on MPD is recommended; if MPD testing is impractical, a regimen based on skin type may be used Initial dose: 0.5–2.0 J/cm2, depending on skin type (or MPD) Treat twice weekly, increments of 40% per week until erythema, and then maximum 20% per week No further increments when 15 J/cm2 is reached
47% improvement in a split-body study after 4 wk; only 1 of 11 patients showed clearance
Safety Photodamage, polymorphic light eruption, increased risk of skin aging and skin cancers but lower than that for PUVA
Induces remission in 70%–90% of patients; less convenient than NB-UVB but may be more effective
High response rates In one study, 85% of patients showed ≥90% improvement in PASI after an average 7.2 wk of treatment; another study showed >75% improvement in 72% of patients in an average of 6.2 treatments
Photodamage, polymorphic light eruption, increased risk of skin aging and skin cancers
Contraindications
Absolute: photosensitivity disorders
Photodamage, premature skin aging, increased risk of melanoma and nonmelanoma skin cancers, ocular damage; eye protection required with oral psoralens
Erythema, blisters, hyperpigmentation, and erosions; long-term side effects not yet clear but likely similar to NB-UVB
Absolute: photosensitivity disorders
Relative: photosensitizing medications, melanoma, and nonmelanoma skin cancers
Absolute: light-sensitizing disorder, lactation, melanoma Relative: age <10 yr, pregnancy, photosensitizing medications, nonmelanoma skin cancers, severe organ dysfunction
Absolute: photosensitivity disorders
Relative: photosensitizing medications, melanoma, and nonmelanoma skin cancers
Remarks Effective as a monotherapy, but
Relative: photosensitizing medications, melanoma, and nonmelanoma skin cancers
Coal tar (Goeckerman regi-
Remarks Effective as a monotherapy, but coal tar (Goeckerman regimen), anthralin (Ingram regimen), or systemic therapies may increase effectiveness in resistant cases
<200 total treatments
Normal skin is spared
Normal skin is spared from unnecessary radiation exposure because therapy is selectively directed toward lesional skin.
Coal tar (Goeckerman regimen), anthralin (Ingram regimen), or systemic therapies may increase effectiveness in resistant cases
coal tar (Goeckerman regimen), anthralin (Ingram regimen), or systemic therapies may increase effectiveness in resistant cases
<200 total treatments (or <2000 J/ cm2 UVA) are recommended; combination with oral retinoids can reduce cumulative UVA exposure
men), anthralin (Ingram regimen), or systemic therapies may increase effectiveness in resistant cases
(or <2000 J/ cm2 UVA) are recommended; combination with oral retinoids can reduce cumulative UVA exposure
from unnecessary radiation exposure because therapy is selectively directed toward lesional skin.
MED, minimal erythema dose; MPD, minimal phototoxic dose; PASI, Psoriasis Area and Severity Index; UVA, ultraviolet A; UVB, ultraviolet B.
disease. One study found that 40% of patients felt frustrated with the ineffectiveness of their current therapies, and 32% reported that treatment was not aggressive enough.24 As psoriasis is a chronic condition, it is important to know the safety of a treatment
during long-term use. In most treatments, the duration of a treatment is restricted because of the cumulative toxicity potential of an individual treatment, and in some instances, treatment efficacy may diminish with time (tachyphylaxis). Some treatments,
483
4
Absolute: pregnancy during or within 3 years after termination of acitretin, breastfeeding Absolute: patients with chronic disease of the GI tract or renal disease; pregnant or lactating women; malignancy (or history of)
Interferes with intracellular redox regulation, inhibiting NF-κB translocation; skews the T-cell response toward a Th2-like pattern
Initiate at 25–50 mg/day and escalate and titrate to response Initiate at low dose and escalate dose weekly; after treatment response is achieved, the dose should be individually adjusted; maximum dose, 1.2 g/day
Baseline LFTs, CBC, lipids, pregnancy test; repeat LFTs, CBC, lipids every week for 1 mo and then every 4 wk; pregnancy test every month for women; spinal radiography if symptoms
Hepatotoxicity; chronic use may lead to hepatic fibrosis; fetal abnormalities or death, myelosuppression, pulmonary fibrosis, severe skin reactions; rarely, severe opportunistic infections
Baseline CBC and LFTs; monitor CBC and LFTs weekly until target dose is achieved; then every 4–8 wk96; liver biopsy every 1.5 g (high risk) to every 3.5–4.0 g (low risk) of cumulative dose or use procollagen III assay
Absolute: pregnancy, lactation, bone marrow dysfunction, alcohol abuse Relative: hepatic dysfunction, hepatitis, renal insufficiency, severe infections, reduced lung function
Mechanism of action Binds cyclophilin, and the resulting complex blocks calcineurin, reducing the effect of the NF-AT in T cells, resulting in inhibition of IL-2 and other cytokines
Monitoring BP; obtain baseline CBC, CMP, magnesium, uric acid, lipids, UA; repeat tests every 2–4 wk; then every month along with BP
Dosing
High-dose approach: 5 mg/kg/day; then tapered Low-dose approach: 2.5 mg/kg/day; increased every 2–4 wk up to 5 mg/kg/day; tapering is recommended on discontinuation
With appropriate monitoring, long-term use appears to be safe Retinoids have been combined with PUVA and occasionally with UVB in an attempt to minimize the side effects and to improve therapeutic response
Absolute: hypersensitivity to sulfasalazine, sulfa drugs, salicylates, intestinal or urinary obstruction, porphyria; precaution in patients with G6PD deficiency
Starting dose: 500 mg three times a day. If tolerated after 3 days, increase dose to 1 g three times a day. If tolerated after 6 wk, increase dose to 1 g four times a day.
Baseline CBC, CMP, and G6PD; repeat CBC and CMP weekly for 1 mo, then every 2 wk for 1 mo, then monthly for 3 mo, and then every 3 mo
Antiinflammatory agent; inhibits 5-lipoxygenase, molecular mechanism unclear
Headache, nausea and vomiting, which occur in approximately one third of patients; rashes, pruritus, and hemolytic anemia (associated with G6PD deficiency)
GI, including constipation, diarrhea, nausea and vomiting, bleeding; myelosuppression, leukopenia; headaches, HTN, peripheral edema; infectious disease, lymphoma
Purine analog that interferes with purine biosynthesis, thereby inducing cell cycle arrest and apoptosis A noncompetitive inhibitor of inosine monophosphate dehydrogenase, blocking de novo purine biosynthesis; selectively cytotoxic for cells that rely on de novo purine synthesis (ie, lymphocytes)
Baseline CBC, CMP, LFTs; repeat baseline tests weekly during dose escalation and then every 2 wk; hold if WBC count ≤ 4.0 × 109/L, platelet count is <125 × 109/L, or hemoglobin <110 g/L
Safety Bone marrow suppression, macrocytosis; teratogenicity and mutagenicity; dermatologic side effects: lichen planus–like eruptions, exacerbation of postirradiation erythema, leg ulcers, and dermatomyositis changes
Mechanism of action Inhibits ribonucleotide diphosphate reductase, which converts ribonucleotides to deoxyribonucleotides, thus selectively inhibiting DNA synthesis in proliferating cells
Monitoring Baseline CBC, CMP, LFTs; repeat baseline tests weekly for 4 wk; then every 2–4 wk for at least 12 wk; then repeat tests every 3 mo; hold dosage if WBC count <2.5 × 109/L, platelet count is <100 × 109/L, or severe anemia
Contraindications
Absolute: prior bone marrow depression (leukopenia, thrombocytopenia, anemia), pregnancy, lactation Relative: renal abnormalities
4
(Continued)
4
Monitoring No laboratory monitoring is required Baseline CBC, CMP, LFTs, lipids; repeat baseline tests monthly; lymphocyte count <500 cell/mm3, ANC <500 cells/mm3, discontinue drug; if ANC between 500 and1000 cells/mm3 or Hgb decrease >2 g/dL or <8 g/dL interrupt dosing until ANC >1000 cell/mm3 or Hgb has normalized
In a study of 1861 patients, 5 mg twice-a-day dosing led to approximately 55% and 30% PASI-75 and PASI-90 response, respectively, and 10 mg twice-a-day dosing had approximately 70% and 45% PASI-75 and PASI-90 responses, respectively (week 28)
Absolute: do not initiate in patients with lymphocyte count <500 cell/mm3, ANC <1000 cells/mm3, or Hgb <9g/dL Relative: infections, risk of GI perforations, history of malignancy and lymphoproliferative disease
Efficacy In a study of 274 treated patients, 28.8% and 55.5% of patients achieved PASI- 75 and PASI-50 response at week 16, respectively
Pregnancy
160-mg injection at week 0 followed by 80 mg at weeks 2, 4, 6, 8, 10, and 12; then 80 mg every 4 wk
PASI-75 at week 12 achieved in 87% of patients; PASI-90 in 68% and PASI-100 in 38% of patients
Humanized monoclonal antibody that specifically targets IL-17A
Infections; hypersensitivity reactions; exacerbation of IBD
Infections, particularly nasopharyngitis; exacerbation of IBD; hypersensitivity reactions; patients should not receive live vaccines while on treatment
150- to 300-mg injections at weeks 0, 1, 2, 3, and 4 (loading dose) followed by injections every 4 wk
Fully human recombinant monoclonal antibody that specifically targets IL-17A
PASI-75 at 16 wk, 71% PASI-75 at week 12 in the range of 77%–82% PASI-90 52%–59% and PASI-100 24%–29% for 300-mg dosing
IV infusions over 2 hr; 5–10 mg/kg at weeks 0, 2, and 6 Initial dose of 80 mg followed by 40 mg given every other week starting 1 week after the initial dose
Injection site reactions, infections, lupus-like syndrome, worsening heart failure, cytopenias, neurologic events; live vaccinations should not be given
Fully human recombinant monoclonal antibody that specifically targets TNF-α
PASI-75 at 10 wk, 82% (5 mg/kg) and 91% (10 mg/kg); at wk 26 (after a single course), 57% of patients maintained PASI-50, and 50% maintained PASI-75
Infusion-related reactions, infections, worsening of MS, malignancy, or lymphoproliferative disease, worsening heart failure; lupus-like symptoms (anti-dsDNA positive); live vaccinations should not be given
Chimeric monoclonal antibody that has high specificity, affinity, and avidity for TNF-α
Serious infections, exacerbation of MS, pancytopenia, malignancy, worsening congestive heart failure; lupus-like symptoms (anti-dsDNA positive); live vaccinations should not be given
Efficacy PASI-75 at 12 wk, 67%; 71%–78% at wk 28 PASI-75 at 12 wk, 34% and at 24 wk, 44% for the 25-mg twice-weekly vs 49% and 59% for 50-mg twice-weekly dosing
25- to 50-mg injections SC twice weekly; commonly given as 50 mg twice weekly for 12 wk followed by 50 mg weekly For pediatric patients, recommended dosing is 0.8 mg/kg weekly with a maximum of 50 mg per week
Human recombinant, soluble TNF-α receptor; binds TNF-α and neutralizes its activity
Safety Serious infections, increased risk of malignancy, reversible posterior leukoencephalopathy syndrome; live vaccinations not recommended
Mechanism Binds p40 (the common subunit of IL-12 and IL-23); blocks Th1 and Th17 differentiation and proliferation
Dosing SC injections; weight-based dosing Individuals weighing <100 kg (220 lb): 45 mg Individuals weighing >100 kg: 90 mg Injections at wk 0 and 4 and then every 12 wk
4
Clinical trials have shown maintenance of efficacy beyond 60 wk of treatment
Similar to other TNF-α inhibitors Clinical trials have shown maintenance of effi- cacy beyond 52 wk of treatment
As intermittent therapy; large databases in patients with other immunologic diseases indicate relative safety
PASI response continues to increase to wk 24; large databases in patients with other immunologic diseases indicate safety
4
■Special caution needs to be exercised when treating women of childbearing potential and during pregnancy.
■Special caution needs to be exercised when treating women of
childbearing potential and during pregnancy.
■Medications such as methotrexate and oral retinoids should be avoided or used with extreme caution and then only along with appropriate contraception.
■Medications such as methotrexate and oral retinoids should be
avoided or used with extreme caution and then only along with appropriate contraception.
■In selected cases, isotretinoin rather than acitretin may be the preferred agent because of its much shorter half-life.
■In selected cases, isotretinoin rather than acitretin may be the pre-
ferred agent because of its much shorter half-life.
■Because methotrexate is fetotoxic and an abortifacient and retinoids are potent teratotoxins, the use of these agents is absolutely contraindicated in pregnancy.
■Because methotrexate is fetotoxic and an abortifacient and reti-
noids are potent teratotoxins, the use of these agents is absolutely contraindicated in pregnancy.
■Many women experience improvement or remission during periods of pregnancy, thus decreasing the need for the more potent agents.
■Many women experience improvement or remission during peri-
ods of pregnancy, thus decreasing the need for the more potent agents.
■If treatment is needed, emollients and other topical agents are firstline agents, often in association with ultraviolet B phototherapy.
■If treatment is needed, emollients and other topical agents are first-
line agents, often in association with ultraviolet B phototherapy.
■Many of the topical agents, such as topical steroids and calcipotriene, are Pregnancy Category C agents, and caution should be exercised with their use.
■Many of the topical agents, such as topical steroids and calcipot-
riene, are Pregnancy Category C agents, and caution should be exercised with their use.
■Several of the biologic agents are Pregnancy Category B and can be used in pregnancy. Likewise, cyclosporin A may be considered because it is Pregnancy Category C and is nonteratogenic.
■Several of the biologic agents are Pregnancy Category B and can
be used in pregnancy. Likewise, cyclosporin A may be considered because it is Pregnancy Category C and is nonteratogenic.
■Systemic psoralen and ultraviolet A light has been used on occasion in selected cases and appears to be safe.
■Systemic psoralen and ultraviolet A light has been used on occa-
sion in selected cases and appears to be safe.
such as calcipotriol, methotrexate (MTX), and acitretin, can be regarded as appropriate for continuous use.85 These treatments maintain efficacy and have low cumulative toxicity potential. In contrast, topical corticosteroids, dithranol, tar, photo(chemo) therapy, and cyclosporin are not indicated for continuous chronic use, and combinatorial or rotational treatments85 are suggested. However, patients with stable chronic plaque psoriasis who respond well to local treatments may not require a change of treatment.85 In cases of itchy or pruritic psoriasis, treatments with an irritative potential, such as dithranol, vitamin D3 analogues, and photo(chemo) therapy, should be used cautiously; treatments with potent antiinflammatory effects, such as topical corticosteroids, are more appropriate.85 In patients with erythrodermic and pustular psoriasis, treatments with an irritant potential should be avoided, and acitretin, MTX, or short-course cyclosporin are the treatments of first choice.85 See Table 28-8 for special considerations in the treatment of women of childbearing potential.
TOPICAL TREATMENTS
TOPICAL TREATMENTS
See Table 28-4. Most cases of psoriasis are treated topically.86 Because topical treatments are often cosmetically unacceptable and time consuming to use, noncompliance is on the order of 40%.87 In most cases, ointment formulations are more effective than creams but are less cosmetically
488
acceptable. For many patients, it is worth prescribing both cream and ointment formulations—cream for use in the morning and ointment for nighttime. Topical agents are also used adjunctively for resistant lesions in patients with more extensive psoriasis and who are concurrently being treated with either UV light or systemic agents.88 It is worth noting that around 400 g of a topical agent is required to cover the entire body surface of an average-sized adult when used twice daily for 1 week.
CORTICOSTEROIDS
Glucocorticoids exert many, if not all, of their myriad effects by stabilizing and causing nuclear translocation of glucocorticoid receptors, which are members of the nuclear hormone receptor superfamily. Topical glucocorticoids are commonly first-line therapy in mild to moderate psoriasis and in sites such as the flexures and genitalia, where other topical treatments can induce irritation. Improvement is usually achieved within 2 to 4 weeks, with maintenance treatment consisting of intermittent applications (often restricted to the weekends). Tachyphylaxis to treatment with topical corticosteroids is a well-established phenomenon in psoriasis. Long-term topical corticosteroids may cause skin atrophy, telangiectasia, striae (Fig. 28-17), and adrenal suppression. Another concern is that when topical steroids are discontinued, patients may reflare, sometimes worse than it was before treatment.88 This class of agents is discussed in detail in Chap. 184.
VITAMIN D3 AND ANALOGUES
Vitamin D exerts its actions by binding to the vitamin D receptor, another member of the nuclear hormone receptor superfamily. Vitamin D3 acts to regulate cell growth, differentiation, and immune function, as well as calcium and phosphorous metabolism. Vitamin D has been shown to inhibit the proliferation of keratinocytes in culture and to modulate epidermal differentiation. Furthermore, vitamin D inhibits production of several proinflammatory cytokines by psoriatic T-cell clones, including IL-2 and IFN-γ. Analogues of vitamin D that have been used for the treatment of skin diseases are calcipotriene, (calcipotriol), tacalcitol, and maxacalcitol. In short-term studies, potent topical corticosteroids were found to be superior to calcipotriene. When compared with shortcontact anthralin or 15% coal tar, calcipotriene was the more effective agent. The efficacy of calcipotriene is not reduced with long-term treatment. Calcipotriene applied twice daily is more effective than oncedaily use. Hypercalcemia is the only major concern with the use of topical vitamin D preparations. When the amount used does not exceed the recommended 100 g/week, calcipotriene can be used with a great margin of safety. Vitamin D analogues are often used in combination with or in rotation with topical corticosteroids in an effort to maximize therapeutic effectiveness while minimizing steroid-related skin atrophy.
A
C D
4
B
ANTHRALIN (DITHRANOL)
Dithranol (1,8-dihydroxy-9-anthrone) is a naturally occurring substance found in the bark of the araroba tree in South America. It can also be synthesized from anthrone. Dithranol is made up in a cream, ointment, or paste. Dithranol is approved for the treatment of chronic plaque psoriasis. Its most common use has been in the treatment of psoriasis, particularly on plaques resistant to other therapies. It can be combined with UVB phototherapy with good results (the Ingram regimen). Most common side effects are irritant contact dermatitis and staining of clothing, skin, hair, and nails. Anthralin possesses antiproliferative activity on human keratinocytes along with potent antiinflammatory effects. Classic anthralin therapy starts with low concentrations (0.05%–0.1%) incorporated in petrolatum or zinc paste and given once daily. To prevent auto-oxidation, salicylic acid
(1% to 2%) should be added. The concentration is increased weekly in individually adjusted increments up to 4% until the lesions resolve. Scalp psoriasis should be treated with great caution as anthralin can stain hair purple to green.
COAL TAR
The use of tar to treat skin diseases dates back nearly 2000 years. In 1925, Goeckerman introduced the use of crude coal tar and UV light for the treatment of psoriasis. Its mode of action is not understood, and because of its inherent chemical complexity, tar is not pharmacologically standardized. It was recently suggested that carbazole, a coal-derived chemical, is the main active ingredient in tar.89 Coal tar can be compounded in creams, ointments, and pastes at concentrations of 5% to 20%. It is often combined with salicylic acid (2%–5%), which by its keratolytic action
489
4
leads to better absorption of the coal tar. Occasionally, patients become sensitized, and a folliculitis may occur. Furthermore, it has an unwelcome smell and appearance and can stain clothing. Coal tar is carcinogenic.
TAZAROTENE
Tazarotene is a third-generation retinoid for topical use that reduces mainly scaling and plaque thickness, with limited effectiveness on erythema. It is thought to act by binding to retinoic acid receptors. It is available in 0.05% and 0.1% gels, and a cream formulation has been developed. When this drug is used as a monotherapy, a significant proportion of patients develop local irritation. Efficacy of this drug can be enhanced by combination with mid- to high-potency glucocorticoids or UVB phototherapy. When used in combination with phototherapy, it lowers the minimal erythema dose (MED) for both UVB and UVA. It has been recommended that UV doses be reduced by at least one third if tazarotene is added to phototherapy.
TOPICAL CALCINEURIN INHIBITORS
See Chap. 192. Tacrolimus (FK-506) is a macrolide antibiotic, derived from the bacteria Streptomyces tsukubaensis, which, by binding to immunophilin (FK506 binding protein), creates a complex that inhibits calcineurin, thus blocking both T-lymphocyte signal transduction and IL-2 transcription. Pimecrolimus is also a calcineurin inhibitor and works in a manner similar to tacrolimus. In a study of 70 patients with chronic plaque psoriasis treated with topical tacrolimus, there was no improvement beyond that seen for placebo. However, for treatment of inverse and facial psoriasis, these agents appear to provide effective treatment.90 The main side effect of these medications is a burning sensation at application site. Anecdotal reports of lymph node or skin malignancy require further evaluation in controlled studies, and these drugs currently carry a U.S. Food and Drug Administration (FDA) “black box warning.”
SALICYLIC ACID
Salicylic acid is a topical keratolytic agent. Its mechanism of action includes reduction of keratinocyte adhesion and lowering the pH of the stratum corneum, which results in reduced scaling and softening of the plaques, thereby enhancing absorption of other agents. Therefore, salicylic acid is often combined with other topical therapies such as corticosteroids and coal tar. Topical salicylic acid decreases the efficacy of UVB phototherapy,88 and systemic absorption can occur, particularly in patients with abnormal hepatic or renal function and when applied to more than 20% of the body surface area. No placebo-controlled studies have been performed to verify the efficacy and safety of salicylic acid as a monotherapy.
490
BLAND EMOLLIENTS
Between treatment periods, skin care with emollients should be performed to avoid dryness. Emollients reduce scaling, may limit painful fissuring, and can help control pruritus. They are best applied immediately after bathing or showering. The addition of urea (up to 10%) is helpful to improve hydration of the skin and remove scaling of early lesions. The use of liberal bland emollients over a thin layer of topical prescription treatments improves hydration while minimizing treatment costs.
PHOTOTHERAPY
PHOTOTHERAPY
See Table 28-5 and Chap. 198. Phototherapy of psoriasis with artificial light sources dates back to 1925 when Goeckerman introduced a combination of topical crude coal tar and subsequent UV irradiation. In the 1970s, it was shown that broadband UVB radiation alone, if given in doses that produce a faint erythematous reaction, could clear the milder clinical forms of psoriasis. Major steps forward were the introduction of photochemotherapy with psoralen and UVA light (PUVA) in the 1970s and narrowband UVB (311–313 nm) in the 1980s.91
The mechanism of action of phototherapy appears to involve selective depletion of T cells, predominantly those that reside in the epidermis.78 The mechanism of depletion may involve apoptosis, accompanied by a shift from a Th1 to a Th2 response in lesional skin.
ULTRAVIOLET B LIGHT
Ultraviolet B (UVB) light is in the range of 290-320 nm. The initial therapeutic UVB dose lies at 50% to 75% of the MED. Treatments are given two to five times per week. Because peak UVB erythema appears within 24 hours of exposure, increments can be performed at each successive treatment. The objective is to maintain a minimally perceptible erythema as a clinical indicator of optimal dosing. Treatments are given until total remission is reached or until no further improvement can be obtained with continued treatment.92 The main side effects of UVB phototherapy are summarized in Chap. 198. Narrowband (312 nm) UVB (NB-UVB) phototherapy is superior to conventional broadband UVB with respect to both clearing and remission times. Although early studies found NB-UVB to be as effective as PUVA, a controlled trial found that PUVA was more effective, albeit less convenient.93 On clearing, treatment is either discontinued, or patients are subjected to maintenance therapy for 1 or 2 months. During this period, the frequency of UVB treatments is reduced while maintaining the last dose given at the time of clearing.91,92 Systemic drugs, such as retinoids, increase the efficacy of UVB light, particularly in patients with chronic and hyperkeratotic plaque–type psoriasis.
PSORALEN AND ULTRAVIOLET A LIGHT
PUVA is the combined use of psoralens (P) and longwave UVA radiation. The combination of drug and radiation results in a therapeutic effect, which is not achieved by the single component alone. Remission is induced by repeated controlled phototoxic reactions. A detailed account of PUVA therapy and its short- and long-term side effects is to be found in Chap. 199.
EXCIMER LASER
See Chap. 208. Supraerythemogenic fluences of UVB and PUVA are known to result in faster clearing of psoriasis; however, the limiting factor for the use of such high fluences lies with the intolerance of the uninvolved surrounding skin as psoriatic lesions can often withstand much higher UV exposures. The monochromatic 308-nm excimer laser can deliver such supraerythemogenic doses of light (up to 6 MED, usually in the range of 2–6 MEDs) focally to lesional skin. The dosing is guided by the patients’ skin type and thickness of the plaque with subsequent doses based on the response to therapy or development of side effects.92 In a study on 124 patients, 72% of study participants achieved at least 75% clearing in an average of 6.2 treatments delivered twice weekly.94 This treatment is commonly used for patients with stable recalcitrant plaques, particularly of the elbows and knees.
CLIMATIC THERAPY
It is well known that going to a sunny climate can improve psoriasis, although a small proportion of patients actually deteriorate. Patients should be warned not to overexpose themselves in the first few days because sunburn may progress to psoriasis (Koebner phenomenon). The best-studied effects are from the Dead Sea area,95 and the therapeutic effects may be attributed, at least partially, to its unique climate. Because it is situated 400 m below sea level, the evaporation of the sea forms an aerosol that stays in the atmosphere above the sea and surrounding beaches. This aerosol screens out the majority of the UVB rays but not the UVA. This mixture of UV light appears to be sufficient to clear psoriasis but without sunburn. Thus, patients can stay on the shores of the Dead Sea for long periods of time with a greatly reduced risk of sunburn. This treatment is carried out over a period of 3 to 4 weeks, and improvements comparable to NB-UVB or PUVA treatments are observed. The main disadvantages are time and expense.
SYSTEMIC ORAL AGENTS96-98
SYSTEMIC ORAL
AGENTS
96-98
See Table 28-6.
4
METHOTREXATE
Methotrexate is highly effective for chronic plaque psoriasis and is also indicated for the long-term management of severe forms of psoriasis, including psoriatic erythroderma and pustular psoriasis.96 For mechanisms of action, see Chap. 190. When first used for the treatment of psoriasis, MTX was thought to act directly to inhibit epidermal hyperproliferation via inhibition of dihydrofolate reductase (DHFR). However, it was found to be effective at much lower doses (0.1–0.3 mg/kg/wk) in the management of psoriasis, PsA, and other inflammatory conditions such as RA. At these concentrations, MTX inhibits the in vitro proliferation of lymphocytes but not proliferation of keratinocytes. It is now thought that the main mechanism of antiinflammatory action of MTX is inhibition of (AICAR [5-aminoimidazole-4-carboxamide ribonucleotide] transformylase), an enzyme involved in purine metabolism. This leads to accumulation of extracellular adenosine, which has potent anti-inflammatory activities.99 Consistent with a DHFR-independent mechanism of action, concomitant administration of folic acid (1–5 mg/day) reduces certain side effects, such as nausea and megaloblastic anemia, without diminishing the efficacy of anti-psoriatic treatment. The very long half-life of MTX may account for its efficacy after weekly administration and may help to explain why its onset of action is rather slow (therapeutic effects usually require 4–8 weeks to become evident). MTX is renally excreted and should therefore not be administered to patients with impairment in renal function because MTX side effects are generally dose related. Short-term toxicity and long-term concerns are discussed in Chap. 190. Recent guidelines98
suggest that patients be divided into two separate groups based on their risk factors for liver injury: The low risk patients follow the American College of Rheumatology guidelines and are not asked to undergo liver biopsy until they have reached a cumulative MTX dose of 3.5 to 4.0 g. In contrast, patients with one or more risk factors continue to follow the previous, more stringent guidelines requiring baseline liver biopsy either before treatment or after 2 to 6 months of treatment and then at each cumulative MTX dose of 1.0 to 1.5 g.98 The risk factors include current or past alcohol consumption, persistent abnormalities of liver function enzymes, personal, or family history of liver disease, exposure to hepatotoxic drugs or chemicals, diabetes mellitus, hyperlipidemia, and obesity. Some groups have recommended the use of amino terminal type III procollagen peptide assay for screening of liver fibrosis. Another well-known side effect of MTX is myelosuppression, especially pancytopenia, which usually occurs in the setting of folate deficiency. Leucovorin calcium (folinic acid) is the only antidote for the hematologic toxicity of MTX. When an overdose is suspected, an immediate leucovorin dose of 20 mg should be given parenterally or orally, and subsequent doses should be given every 6 hours. Pneumonitis can develop, and mucosal and skin ulcerations have also been reported in patients treated with MTX.
491
4
Discontinuation of MTX treatment is required in the event of hepatotoxicity, hematopoietic suppression, active infections, nausea, and pneumonitis. MTX is also teratogenic and should therefore not be prescribed for women who are pregnant or breastfeeding. Several classes of drugs, including NSAIDs and sulfonamides, may interact with MTX to increase toxicity.
ACITRETIN
Acitretin is a second-generation, systemic retinoid that has been approved for the treatment of psoriasis since 1997 and is discussed in Chap. 185. The clinical forms most responsive to etretinate or acitretin as monotherapy include generalized pustular and erythrodermic psoriasis.100 Acitretin induces clearance of psoriasis in a dose-dependent fashion. Overall, higher starting doses appeared to clear psoriasis faster. The mechanism of action of retinoids for psoriasis is not fully understood. The optimal initial dose of acitretin for psoriasis is reported at 25 mg/day, with a maintenance dose of 20 to 50 mg/day. Adverse effects, such as hair loss and paronychia, occur more frequently with higher initial dose (ie, ≥50 mg/day). Most patients relapse within 2 months after discontinuing etretinate or acitretin. Acitretin should be discontinued if liver dysfunction, hyperlipidemia, or diffuse idiopathic hyperostosis develops.
APREMILAST
Apremilast is a small-molecule inhibitor of phosphodiesterase (PDE)-4, which degrades cyclic adenosine monophosphate (cAMP) intracellularly. The inhibition of PDE4 increases intracellular levels of cAMP resulting in increased activity of the TF CREB (cAMP response element-binding protein), while inhibiting NF-κB signaling. To reduce risk of gastrointestinal (GI) symptoms the drug is titrated over a period of 1 week, starting at 10-mg dosing at day 1 and ending in 30-mg twice-a-day dosing on day 6, which is maintained for the duration of treatment. Adverse effects include GI symptoms such as diarrhea, nausea, and headaches. Worsening of depression has been described, and the drug should be used with caution in individuals with history of depression or suicidal thoughts or behaviors.
TOFACITINIB
Tofacitinib is an oral Janus kinase (JAK) inhibitor. Janus kinases are a family of four tyrosine kinases (JAK1, JAK2, JAK3, and TYK2) and have a role in downstream signaling of multiple proinflammatory cytokines, including IL-2, IL-4, IL-9, IL-13, IL-21, type I and II IFN signaling, IL-6, and to a lesser extent IL-12 and IL-23.101 At the time of this writing, tofacitinib is only approved for RA, but several clinical trials in psoriasis have been completed using either 5 mg twice a day or 10 mg twice a day.102,103 Patients should be screened for tuberculosis before initiation, and patients need to be
492
monitored for changes in hemoglobin, leukopenias, or lipid abnormalities. Increased incidences of viral infections, particularly herpes zoster, have been reported in patients with RA taking tofacitinib.
CYCLOSPORIN A
Cyclosporin A (CsA) is a neutral cyclic undecapeptide derived from the fungus Tolypocladium inflatum gams. Its mechanism of action and side effects are discussed in Chap. 192. The only formulation approved for treatment of psoriasis is available as an oral solution or in capsules. It is highly effective for cutaneous psoriasis and can also be effective for nail psoriasis (see Fig. 28-9). CsA is particularly useful in patients who present with widespread, intensely inflammatory, or frankly erythrodermic psoriasis. The dosage ranges from 2 to 5 mg/kg/day. Because the nephrotoxic effects of CsA are largely irreversible, CsA treatment should be discontinued if kidney dysfunction or hypertension occurs. CsA-induced hypertension may be treated with calcium antagonists such as nifedipine. The most common adverse effects noted in patients using CsA for short periods of time are neurologic, including tremors, headache, paresthesia, or hyperesthesia. Long-term treatment of psoriasis with low-dose CsA was found to increase risk of nonmelanoma skin cancers. However, unlike organ transplant patients treated with higher doses of CsA, there is little or no increased risk of lymphoma.
FUMARIC ACID ESTERS
Fumaric acid was first reported in 1959 to be beneficial in the systemic treatment of psoriasis104 and is licensed in Germany for the treatment of psoriasis. Because fumaric acid itself is poorly absorbed after oral intake, esters are used for treatment. The esters are almost completely absorbed in the small intestine, and dimethylfumarate is rapidly hydrolyzed by esterases to monomethylfumarate, which is regarded as the active metabolite. The mode of action in psoriasis is not fully understood.104 Patients with severe concomitant disease, chronic disease of the GI tract, chronic kidney disease, or with bone marrow disease leading to leukocytopenias or leukocyte dysfunction should not be treated. Likewise, pregnant or lactating women and patients with malignant disease (including positive history of malignancy) should be excluded from treatment. Prolonged therapy (up to 2 years) to prevent relapse in psoriasis patients with high disease activity is possible. Another therapeutic option is short-course intermittent therapy. Fumaric acid esters (FAEs) are given until a major improvement is achieved and are then withdrawn. If a patient remains lesion-free during prolonged treatment, the FAE dose should be gradually decreased to reach the individual’s threshold.104 Therapy with FAEs can be stopped abruptly because rebound phenomena have not been observed.
SULFASALAZINE
Sulfasalazine is an uncommonly used systemic agent in the management of psoriasis. In the only prospective double-blind study on the efficacy of sulfasalazine in psoriasis, moderate effects were seen, with 41% of the patients showing marked improvement, 41% with moderate improvement, and 18% with minimal improvement after 8 weeks of treatment.105
SYSTEMIC STEROIDS
See Chap. 184 In general, systemic steroids should not be used in the routine care of psoriasis. When systemic steroids are used, clearance of psoriasis is rapid, but the disease usually breaks through, requiring progressively higher doses to control symptoms. If withdrawal is attempted, the disease tends to relapse promptly and may rebound in the form of erythrodermic and pustular psoriasis. However, systemic steroids may have a role in the management of persistent, otherwise uncontrollable, erythroderma and in fulminant generalized pustular psoriasis (von Zumbusch type) if other drugs are ineffective.
MYCOPHENOLATE MOFETIL
See Chap.192 Mycophenolate mofetil is a prodrug of mycophenolic acid, an inhibitor of inosine-5′-monophosphate dehydrogenase. Mycophenolic acid depletes guanosine nucleotides preferentially in T and B lymphocytes and inhibits their proliferation, thereby suppressing cell-mediated immune responses and antibody formation. The drug is usually well tolerated with few side effects. Few studies have been done on this medication for psoriasis, but in a prospective open-label trial on 23 patients with dosage between 2 to 3 g/day, a 24% reduction of the Psoriasis Area and Severity Index (PASI) was seen after 6 weeks, with 47% improvement at 12 weeks.
6-THIOGUANINE
6-Thioguanine is a purine analog that has been highly effective for psoriasis. Apart from bone marrow suppression, GI complaints, including nausea and diarrhea, can occur, and elevation of liver function test results is common.96 Isolated instances of hepatic venoocclusive disease have been reported.
HYDROXYUREA
Hydroxyurea is an antimetabolite that has been shown to be effective as monotherapy, but nearly 50% of patients who achieve marked improvement develop bone marrow toxicity with leukopenia or thrombocytopenia. Megaloblastic anemia is also common but rarely requires treatment.96 Cutaneous reactions affect
4
most patients treated with hydroxyurea, including leg ulcers, which are the most troublesome.106
BIOLOGIC TREATMENTS
BIOLOGIC TREATMENTS
See Table 28-7 and Chap. 193. Based on the continuous progress in psoriasis research and advances in molecular biology, a new class of agents—targeted biologic therapies—has emerged. These agents are designed to block specific molecular steps important in the pathogenesis of psoriasis or have been transferred to the psoriasis arena after being developed for other inflammatory diseases. Currently, three types of biologics are approved or are in development for psoriasis: (1) recombinant human cytokines, (2) fusion proteins, and (3) monoclonal antibodies, which may be fully human, humanized or chimeric. Because of the risk of the development of antibodies to mouse sequences, humanized or fully human antibodies are preferred for clinical use. Using internationally acknowledged safety and efficacy endpoints, the overall utility and benefit of biologics have been demonstrated based on the percentage of patients achieving at least a 50% improvement in PASI (PASI-50), a 75% improvement in PASI (PASI-75), the impact of treatment on quality of life, and safety and tolerability. Many of these agents have antipsoriatic activity roughly comparable to that of MTX and lack its risk of hepatotoxicity. However, they are far more expensive and carry risks of immunosuppression, infusion reactions, and antibody formation, and their long-term safety remains to be evaluated. In the opinion of the authors, use of biologic agents should be reserved for treatment of moderate to severe psoriasis that is either unresponsive to MTX or in patients for whom the use of MTX is contraindicated.
TUMOR NECROSIS FACTOR-α ANTAGONISTS
The clinical application of TNF antagonists in inflammatory diseases has exploded on the clinical realm in a manner reminiscent of the discovery of the activity of corticosteroids. TNF-α is a homotrimeric protein that exists in both transmembrane and soluble forms, the latter resulting from proteolytic cleavage and release. It is still unclear which form is more important in mediating its proinflammatory activities or the relative importance of the two p55- and p75-kd TNF-α–binding receptors. Currently, five anti-TNF biologics are available in the United States. Infliximab is a chimeric monoclonal antibody that has high specificity, affinity, and avidity for TNF-α. An example of an excellent treatment outcome with infliximab is shown in Fig. 28-17. Etanercept is a human recombinant, soluble, TNF-α receptor-Fc IgG fusion protein that binds TNF-α and neutralizes its activity. Adalimumab and golimumab are fully human recombinant IgG1 monoclonal antibodies and
493
4
specifically targets TNF-α. Certolizumab pegol is a polyethylene glycol (PEG) Fab′ fragment of a humanized TNF inhibitor monoclonal antibody. The pegylation is thought to reduce immunogenicity of the drug and prolongs serum half-life without compromising activity. Currently, golimumab and certolizumab pegol are only FDA approved for PsA. Clinical trials have shown that each of these agents is well tolerated and appears suitable for long-term use in chronic plaque psoriasis. However, like all the targeted biologic therapies, they carry risks of immunosuppression. Clinical studies have found infliximab and adalimumab to be slightly more effective than etanercept in the treatment of psoriasis. It is likely that the differential effects of these agents are associated with selectivity in their ability to perturb these receptor–ligand interactions. It is known that infliximab, adalimumab, golimumab, and etanercept bind TNF differently; whereas infliximab and adalimumab bind to both soluble and membrane-bound TNF, etanercept binds primarily to soluble TNF. Binding to membrane-bound TNF can induce a dose-dependent increase in apoptosis of T cells, but the relevance of this mechanism in psoriasis has not been evaluated. New onset of psoriasis has been described several times in patients on these agents for other conditions such as Crohn disease or RA. These paradoxical reactions are characterized by increased production of IFN-α.107
INTERLEUKIN-12 AND INTERLEUKIN-23 ANTAGONISTS
Ustekinumab is a human monoclonal antibody that binds the shared p40 subunit of IL-12 and IL-23 and prevents interaction with their receptors. This treatment blocks IL-12, which is critical for Th1 differentiation, but its inhibitory effect on IL-23 may be more important. As described earlier, IL-23 supports chronic inflammation mediated by Th17 and Th22 cells. Clinical studies have found ustekinumab to be slightly more effective than etanercept in the treatment of psoriasis,108 but direct comparison with infliximab or adalimumab has not been reported. Several agents specifically targeting the p19 subunit of IL-23 are currently in development and appear to be highly effective, consistent with a key role for IL-23 in psoriasis pathogenesis.57,109,110
INTERLEUKIN-17A ANTAGONISTS
Two IL-17A antagonists are currently approved for the treatment of psoriasis. Secukinumab is a fully human antibody, and ixekizumab is a humanized antibody that binds and neutralizes IL-17A. IL-17A is a critical cytokine in the pathogenesis of psoriasis, and biologics targeting IL-17A are among the most effective drugs available for the treatment of psoriasis.111-113
Brodalumab, a fully human antibody targeting the IL-17 receptor α chain, is also highly effective114 and has recently been FDA approved for use in psoriasis after screening for depression and suicidal ideation.
494
COMBINATION TREATMENTS
COMBINATION
TREATMENTS
Combination treatment may increase efficacy and reduce side effects, so it may result in a more substantial improvement, or alternatively, may permit reduced doses to reach the same improvement as compared with monotherapy.85 Data on combination of biologics with other systemic or topical agents are not yet widely available, but some combinations commonly used in the treatment of inflammatory arthritides, such as a combination of MTX and anti-TNF agents, may be appropriate for treatment of recalcitrant psoriatic disease.
TREATMENT OF PALMOPLANTAR PUSTULAR PSORIASIS
TREATMENT OF
PALMOPLANTAR PUSTULAR
PSORIASIS
Palmoplantar pustular psoriasis (including PPP and PPPP) tends to be difficult to treat and is often unresponsive to treatments used for chronic plaque psoriasis. Given its rarity, randomized controlled trials are lacking. Phototherapy, cyclosporine, and topical steroids are the treatments with the most welldocumented efficacy.115 Tonsillectomy has been used to treat pustulosis palmaris et plantaris, and in a cohort of 116 Japanese patients, clinical improvement was seen in 109 (94%).116 Notably, given its strong association with smoking, smoking cessation provides substantial clinical improvement.117
PREVENTION
There is no known prevention for psoriasis.

Figure 28-1 A–F. Chronic plaque psoriasis located at typical sites. Note the marked symmetry of the lesions. (Used with permission from Dr. Johann Gudjonsson and Mr. Harrold Carter.)

Figure 28-2 A, Auspitz sign. B, Note the point of bleeding after the scale is removed. (Used with permission from Dr. Johann Gudjonsson and Ms. Laura Vangoor.)

Figure 28-3 Koebner phenomenon. A, Psoriasis appearing in keratome biopsy sites 4 weeks after biopsy. B, Flare of psoriasis on the back after a sunburn. Note sparing of sun-protected areas. (Image A, used with permission from Mr. Harrold Carter. Image B, used with permission from Dr. James Rasmussen.)

Figure 28-4 Unusual forms of plaque-type psoriasis. A, Annular psoriasis on the flank. B, Rupioid psoriasis in an infant. Note the cone-shaped lesions. C, Psoriatic patient undergoing modified Goeckerman therapy (ultraviolet B light, coal tar, and topical steroid), demonstrating Woronoff rings. D, Elephantine psoriasis of the lower extremities. Note psoriatic involvement of toenails. (Used with permission from Dr. Johann Gudjonsson, Mr. Harrold Carter, and Ms. Laura Vangoor.)

Figure 28-5 Guttate psoriasis, involving the thigh (A), hands (B), and back (C and D). The patient in D went on to develop chronic plaque psoriasis. (Used with permission from Drs. Johann Gudjonsson and Trilokraj Tejasvi, Mr. Harrold Carter, and Ms. Laura Vangoor.)

Figure 28-6 Flexural psoriasis. A, Well-demarcated, beefy-red, shiny plaques. B, Infant with “napkin psoriasis.” (Used with permission from Dr. Johann Gudjonsson and Mr. Harrold Carter.)

Figure 28-7 Erythrodermic psoriasis. A, This patient rapidly developed near-complete involvement and complained of fatigue and malaise. Note the islands of sparing. B and C, This patient had total-body involvement with marked hyperkeratosis and desquamation. (Used with permission from Mr. Harrold Carter and Dr. Johann Gudjonsson.)

Figure 28-8 Pustular psoriasis. A and B, von Zumbusch-type generalized pustular psoriasis. Note the tiny pustules, 1 to 2 mm in diameter, on erythematous skin. C and D, localized pustular psoriasis of the leg and foot, respectively. E, Resolving pustular psoriasis. Note the extensive areas of desquamation. (C–E used with permission from Dr. Johann Gudjonsson, Dr. Trilokraj Tejasvi, and Neena Khanna.)

Figure 28-9 Nail psoriasis. A, Distal onycholysis and oil drop spotting. B, Nail pitting. C, Subungual hyperkeratosis. D, Onychodystrophy and loss of nails in a patient with psoriatic arthritis. (Used with permission from Dr. Johann Gudjonsson, Dr. Allen Bruce, and Mr. Harrold Carter.)
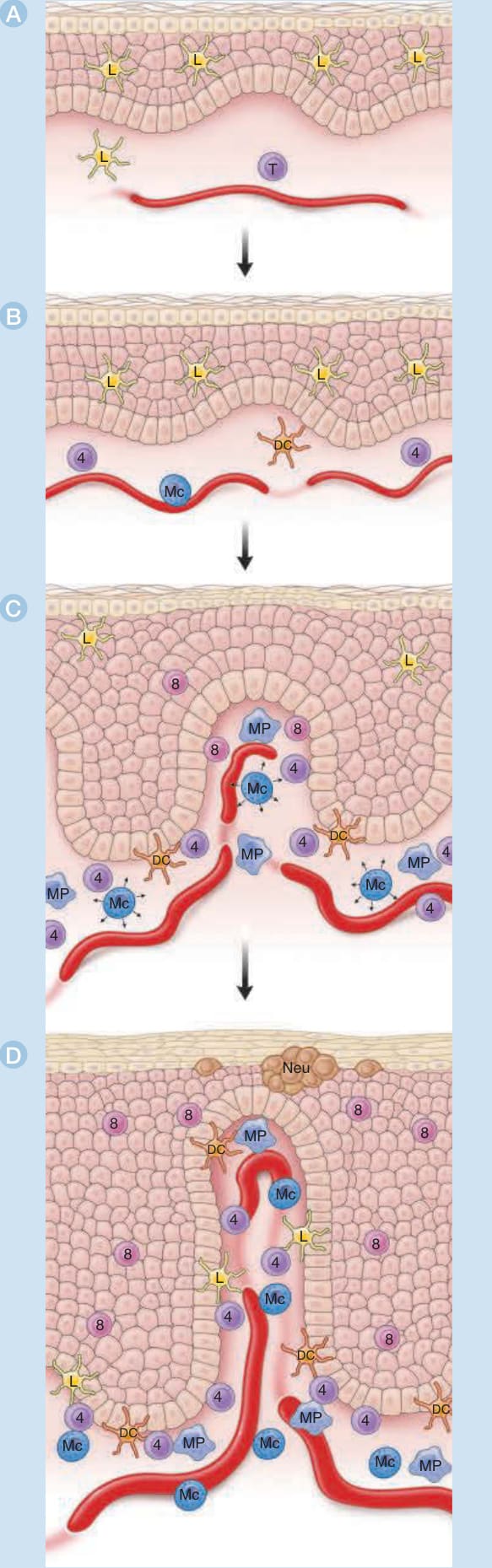
Figure 28-10 Development of psoriatic lesions. Normal skin from a healthy individual (A) contains epidermal Langerhans cells, scattered immature dendritic cells (D), and skin-homing memory T cells (T) in the dermis. Normalappearing skin from a psoriatic individual (B) manifests slight capillary dilatation and curvature and a slight increase in the numbers of dermal mononuclear cells and mast cells (Mcs). A slight increase in epidermal thickness may be present. The transition zone of a developing lesion (C) is characterized by progressive increases in capillary dilatation and tortuosity, numbers of mast cells, macrophages (MPs), and T cells and mast cell degranulation (arrowheads). In the epidermis, there are increasing thickness with increasingly prominent rete pegs, widening of the extracellular spaces, transient dyskeratosis, spotty loss of the granular layer, and parakeratosis. Langerhans cells (L) begin to exit the epidermis, and inflammatory dendritic epidermal cells (I) and CD8+ T cells (8) begin to enter the epidermis. The fully developed lesion (D) is characterized by fully developed capillary dilatation and tortuosity with a 10-fold increase in blood flow, numerous macrophages underlying the basement membrane, and increased numbers of dermal T cells (mainly CD4+) making contact with maturing dermal dendritic cells (D). The epidermis of the mature lesion manifests markedly increased (∼10-fold) keratinocyte hyperproliferation extending to the lower suprabasal layers, marked but not necessarily uniform loss of the granular layer with overlying compaction of the stratum corneum and parakeratosis, increased numbers of CD8+ T cells, and accumulation of neutrophils in the stratum corneum (Munro’s microabscesses).
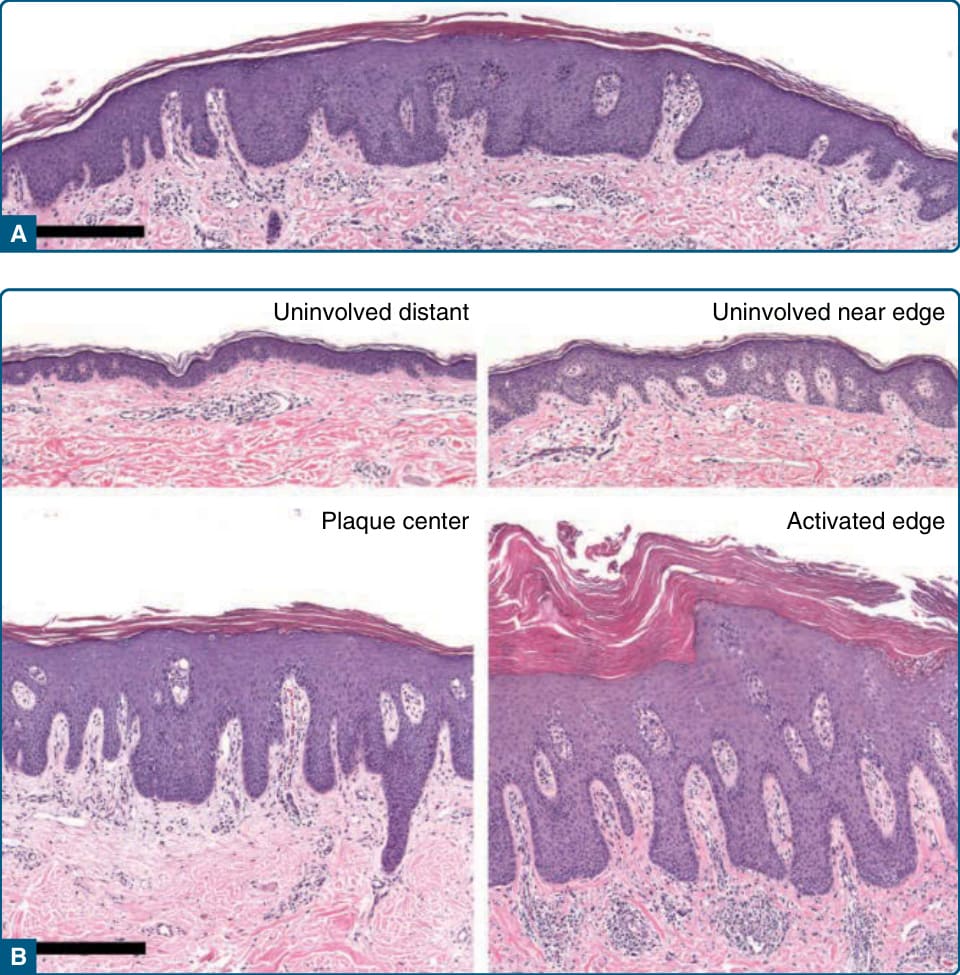
Figure 28-11 Histopathology of psoriasis. A, Pinpoint papule of psoriasis. In the transition from the edges to the center of the lesion, note progressive thickening of epidermis with elongation of rete pegs, increasing dilation and tortuosity of vessels, and increasing mononuclear cell infiltrate. Also note the transition from basket-weave to compact stratum corneum with loss of granular layer in the center of the lesion. (Four-mm punch biopsy, hematoxylin and eosin, scale bar, 100 µM.) B, Comparison of uninvolved versus involved skin. Four 4-mm biopsies were taken from the same individual sampled in A on the same day. “Uninvolved distant” skin was taken from the upper back 30 cm from the nearest visible lesion of psoriasis. The “uninvolved near edge” skin was taken 0.5 cm from the edge of a 20-cm plaque, which had been present for several years, according to the patient. “Center plaque” skin was taken from a relatively inactive (less red and scaly) area in the center of this plaque. “Involved edge” skin was taken from an active (more red and scaly) area about 1 cm inside the edge of the same plaque. In comparing “uninvolved distant” with “uninvolved near-edge” skin, note that the latter manifests increased thickness and early elongation of the rete pegs, dilation and early tortuosity of blood vessels, and increased numbers of mononuclear cells in the upper dermis, many of which are in a perivascular location. In this patient, “uninvolved near-edge” skin also manifests an increased frequency of dyskeratotic keratinocytes, a finding that has been noted previously at the periphery of psoriatic lesions.53 In comparing less active with more active areas of the plaque, note that the more active area manifests increased dermal mononuclear infiltrate, increased hyperkeratosis and parakeratosis, and Munro microabscesses. (Four-mm punch biopsies, hematoxylin and eosin, scale bar, 100 µM.)
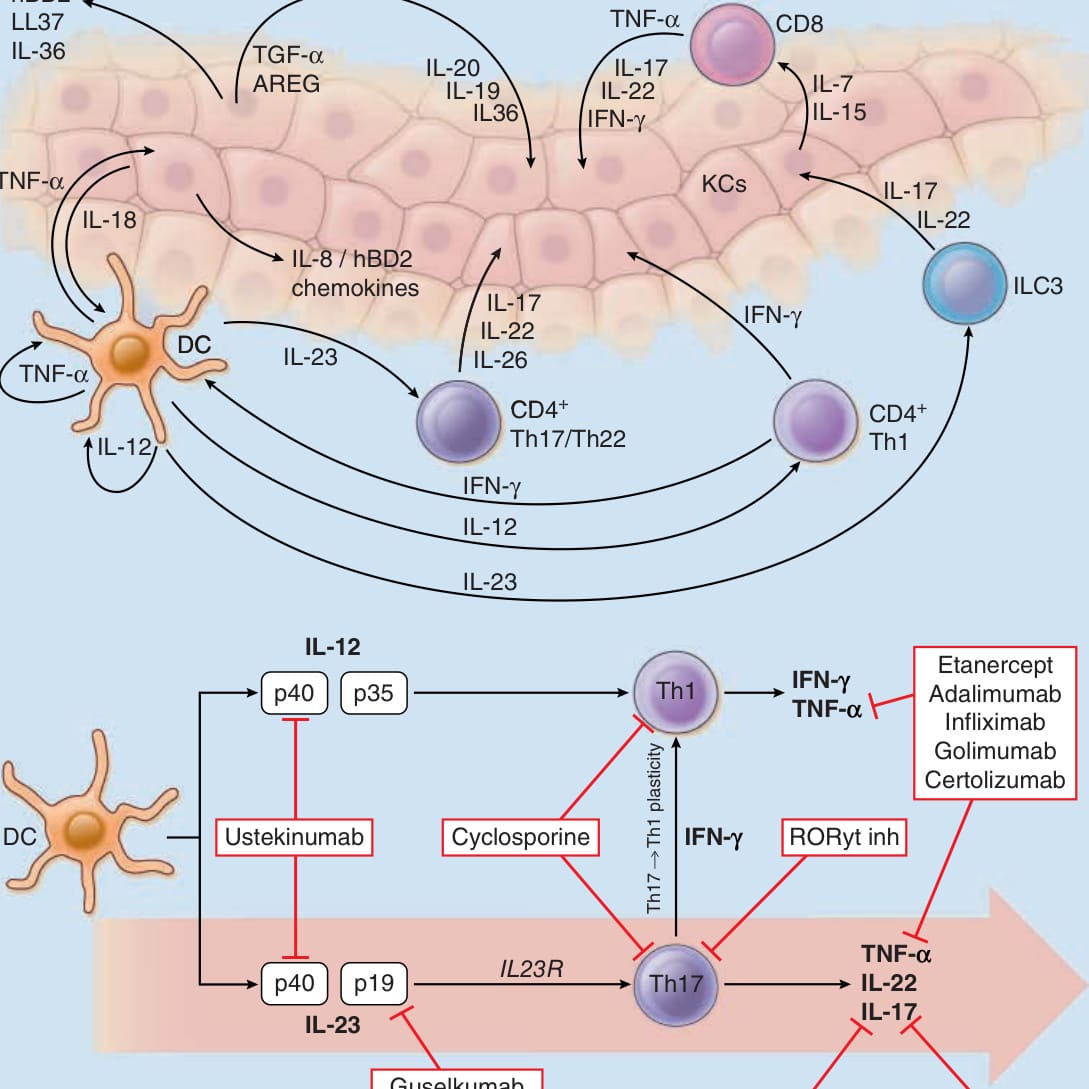
Figure 28-12 The cytokine network in psoriasis. Interferon (IFN)-γ is produced by T helper (Th) 1 cells and tumor necrosis factor (TNF)-α is produced by activated T cells and dendritic cells (DCs). IFN-γ amplifies the production of interleukin (IL)- 23 by DC. In turn, IL-23 maintains and expands subsets of CD4+ T cells, called Th 17 and Th22 cells, which are characterized by production of IL-17 and IL-22, respectively. ILC3 also contribute to IL-17 in psoriatic skin. CD8+ T cells are predominantly found in the epidermis, and their entry into the epidermis is necessary for lesion development. IL-17, TNF-α, IFN-γ, and IL-22 synergistically promote activation of the innate keratinocyte defense response involving secretion of antimicrobial peptides such as human-β-defensin 2 (hBD-2), cathelicidin (LL37), IL-8 and other chemokines, and growth factors such as transforming growth factor (TGF)-α, amphiregulin (AREG), IL-19, and IL-20. Keratinocytes also produce IL-7 and IL-15, which influence the survival and turnover of CD8+ T cells; IL-18, which via IL-12 causes DCs to further increase the production of IFN-γ by T-cells; and IL-36 family cytokines, which attracts leukocytes, including neutrophils. Notably, the majority of available systemic therapeutic agents that have shown high therapeutic efficacy in psoriasis target the IL-12–Th1 and IL-23–Th17 axes.
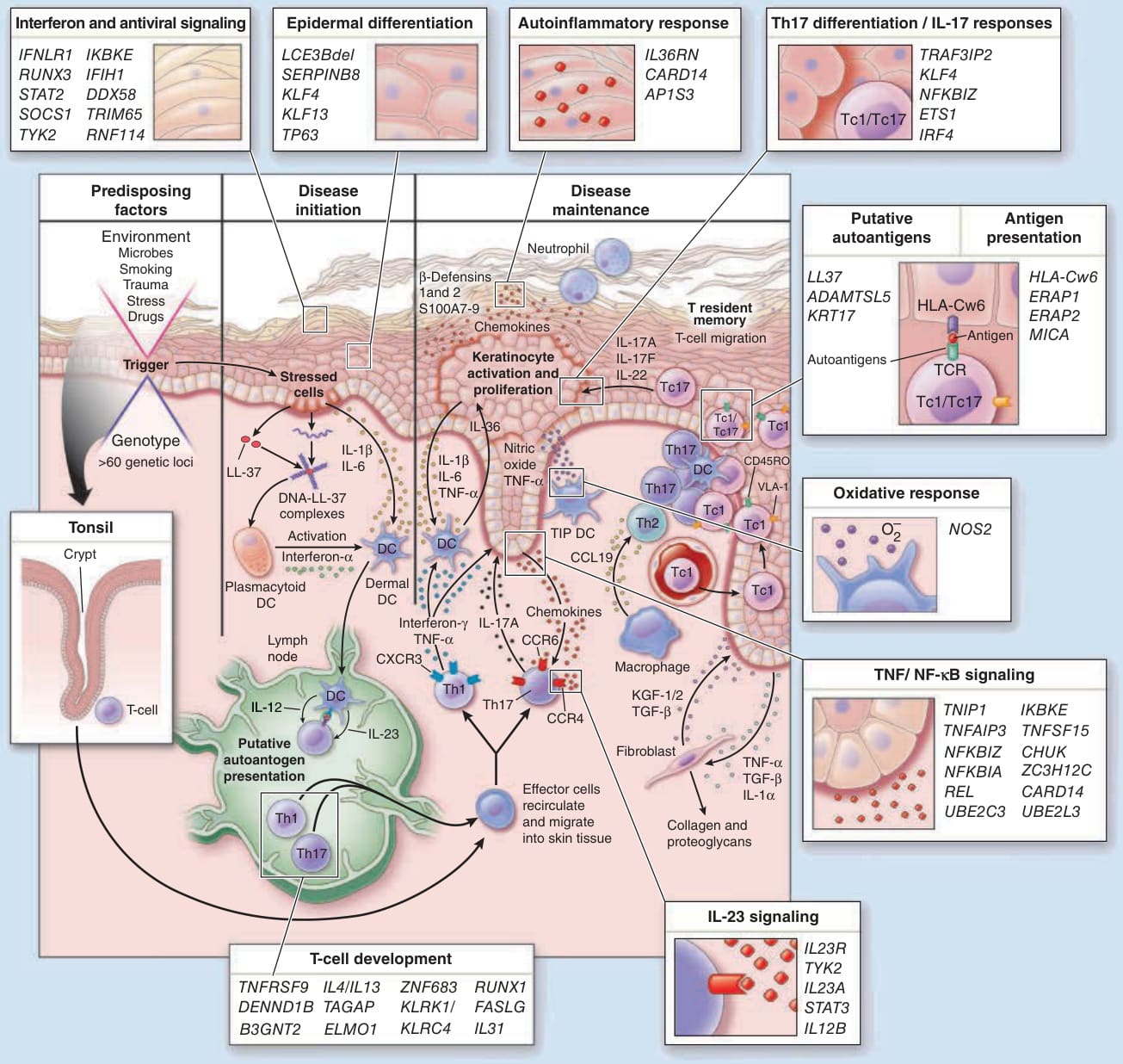
Figure 28-13 The inflammatory and genetic network in psoriasis. Psoriasis is initiated and maintained by interactions between intrinsic genetic susceptibility factors and external environmental factors, with the cutaneous immune system playing a central role. Initiation (triggering) of psoriasis lesions can occur in the skin (Koebnerization) or in the tonsils (streptococcal pharyngitis). In the context of environmental challenge, dendritic cells (DCs) are activated by “danger signals” released by damaged keratinocytes such as nucleic acids, S100 proteins, cathelicidins, and β-defensins; microbial products such as bacterial lipopolysaccharide; and proinflammatory cytokines such as interleukin (IL)-1, IL-36, and IL-8 induced in damaged keratinocytes. Through secretion of the key cytokines IL-12 and IL-23, activated DCs drive polarization and expansion of “T1” (T helper [Th] 1 and Tc1), “T17” (Th17 and Tc17) lymphocytes, which acquire skin-homing properties. Activated T1 and T17 cells secrete pro-inflammatory mediators including interferon (IFN)-γ, tumor necrosis factor (TNF)-α, IL-22, and IL-17, which act in a synergistic manner to amplify keratinocyte responses in the vicinity of the initial insult. To this end, keratinocytes increase their production of inflammatory mediators, including IL-1, IL-36, and a large number of chemokines, including IL-8 (CXCL8), CXCL9, and CXCL10. Cytokine-activated keratinocytes also release larger amounts of the various “danger signals” such as S100 proteins, cathelicidins, and β-defensins, many of which also have antimicrobial and chemotactic properties. This amplified inflammatory circuit recruits in chemotaxis and recruitment other inflammatory cells, including macrophages, DC, neutrophils, and other T-cell subsets, which act in synergy to maintain the disease process. Injured keratinocytes also produce growth factors such as TGF-α, amphiregulin (AREG), fibroblast growth factor (FGF), and nerve growth factor (NGF) to promote structural integrity, as well as T-cell growth factors, including IL-7 and IL-15. Key aspects of this process, which continue to be topics of active investigation, include the role of specific antigens in initiation versus maintenance of psoriasis and the mechanism of psoriatic epidermal hyperplasia. As indicated in the highlighted boxes, genetic variation influences multiple steps in this process, including INF and antiviral signaling, epidermal response, IL-23 signaling, cellular responses to IL-17 and TNF via NF-κB and other intracellular signaling pathways, autoinflammatory response, oxidative responses, and antigen presentation, T-cell development. Details on the role of specific candidate genes in this process can be found in Table 28-2.
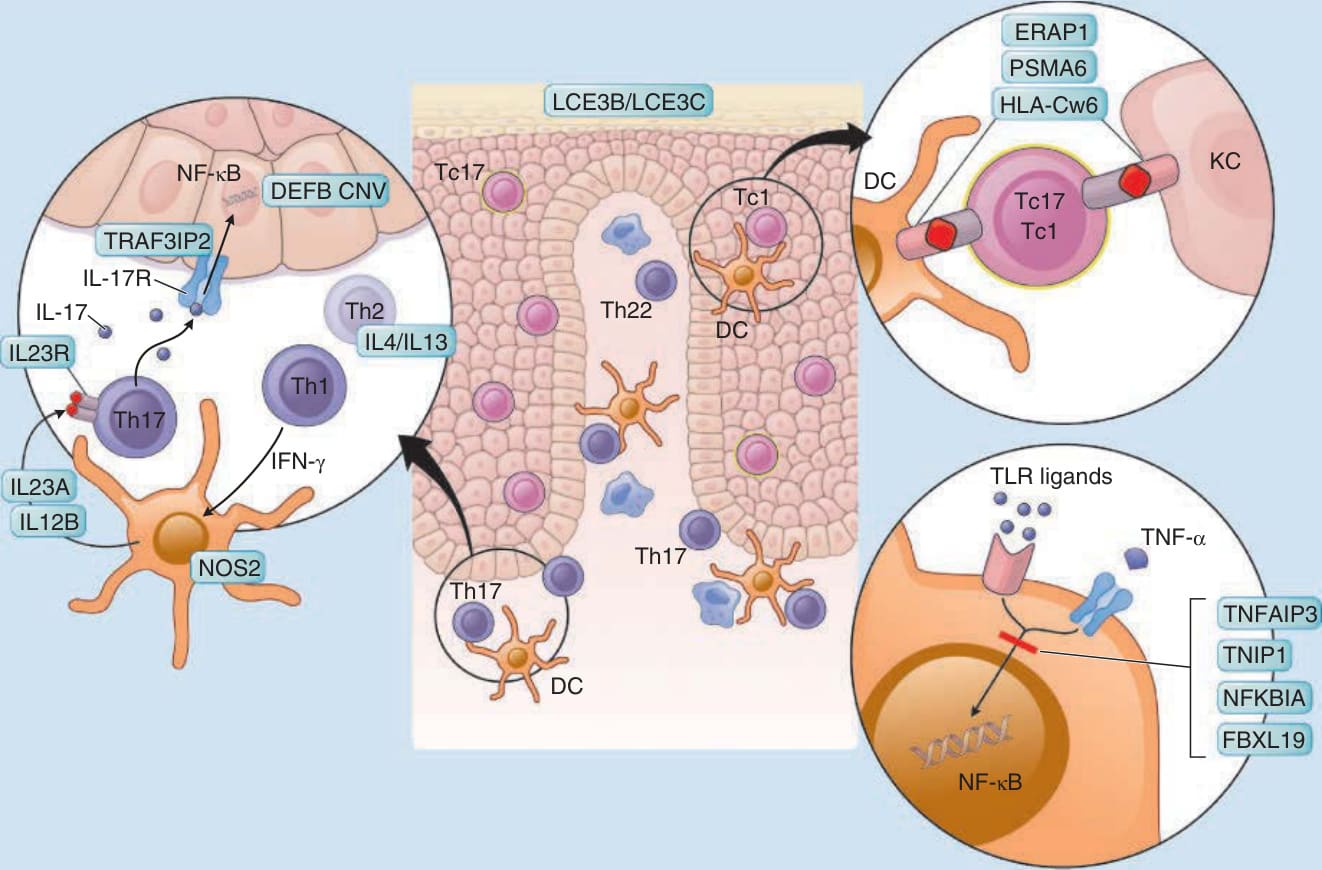
Figure 28-14 Proposed model integrating the genetics and immunology of psoriasis. Whereas the majority of the CD8+ T-cells (green) are located in the epidermis, CD4+ T cells (purple) predominate in the dermis along with antigen-presenting cells and dendritic cells (DCs) (blue) and macrophages (Mφs) (orange). Confirmed association signals are indicated by the likely candidate genes they contain. Not all known psoriasis loci are depicted in this figure; please see text and Table 28-2 for additional details. Th, T helper; TLR, toll-like receptor. (Adapted from Nair RP et al. Psoriasis bench to bedside: genetics meets immunology. Arch Dermatol. 2009;145(4):462-464, with permission. Copyright © 2009 American Medical Association. All rights reserved.)
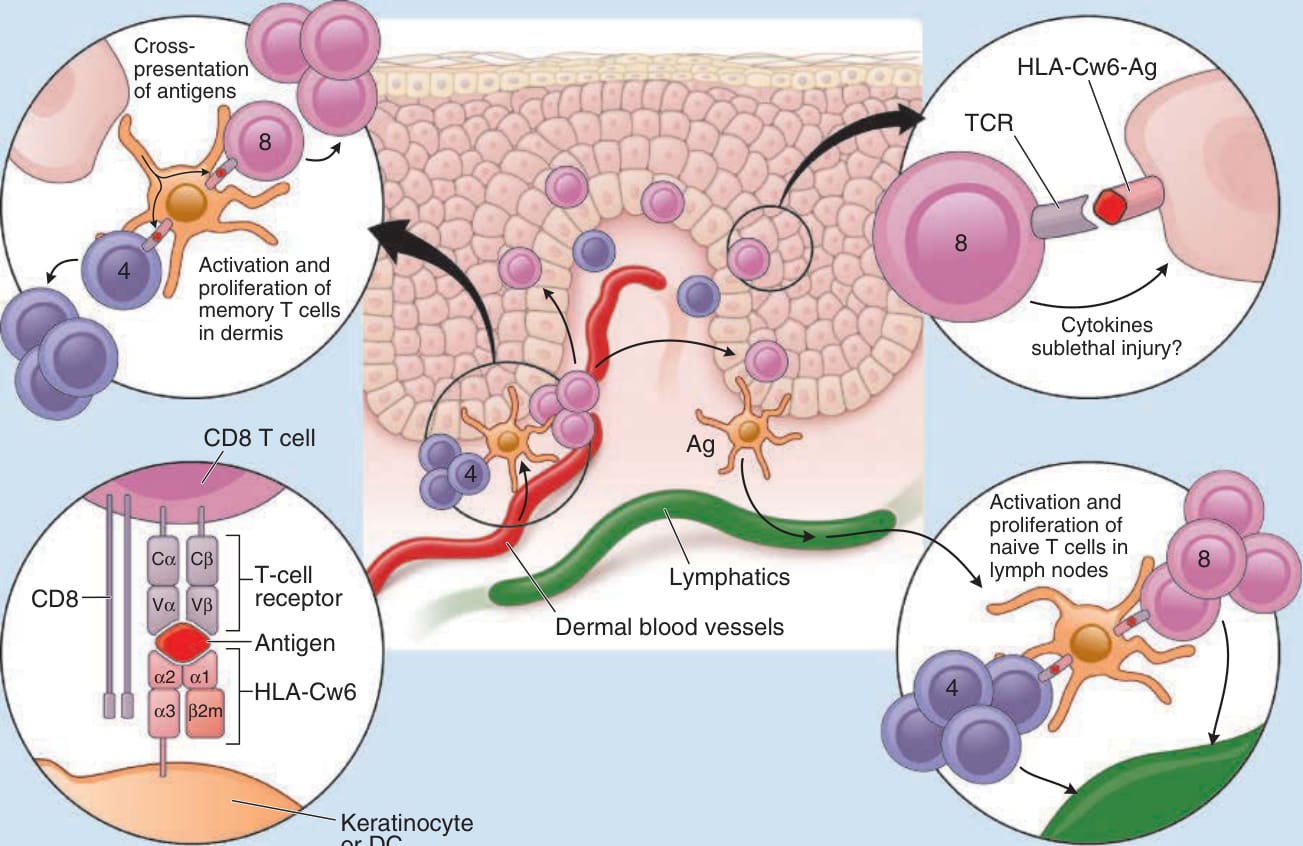
Figure 28-15 Proposed role of HLA-Cw6 in the pathogenesis of psoriasis. Antigen (Ag) in the binding pocket of human leukocyte antigen (HLA)-Cw6 interacts with a T-cell receptor (TCR). The role of HLA-Cw6 in psoriasis is likely to be twofold. HLA-Cw6 is active in cross-presenting peptides on the surface of dendritic cells (DCs), allowing activation and clonal expansion of antigen-specific CD8+ T cells. This process is dependent on CD4+ T-cell help for cross-presentation of intracellular antigens and is likely to happen both in the dermis (activation of resident memory T cells) and local lymph nodes (activation of naïve T cells). Subsequently, the activated CD8+ T cells are able to migrate into the epidermis, where they encounter HLA-Cw6 on the surface of DCs or keratinocytes presenting those same pathogenic peptides. Because these T cells express perforin, they may directly damage keratinocytes in the traditional cytotoxic manner. Activated CD8+ T cells may also trigger the local release soluble factors, including cytokines, chemokines, eicosanoids, and innate immune mediators, which could further increase local inflammation and stimulate keratinocyte proliferation.
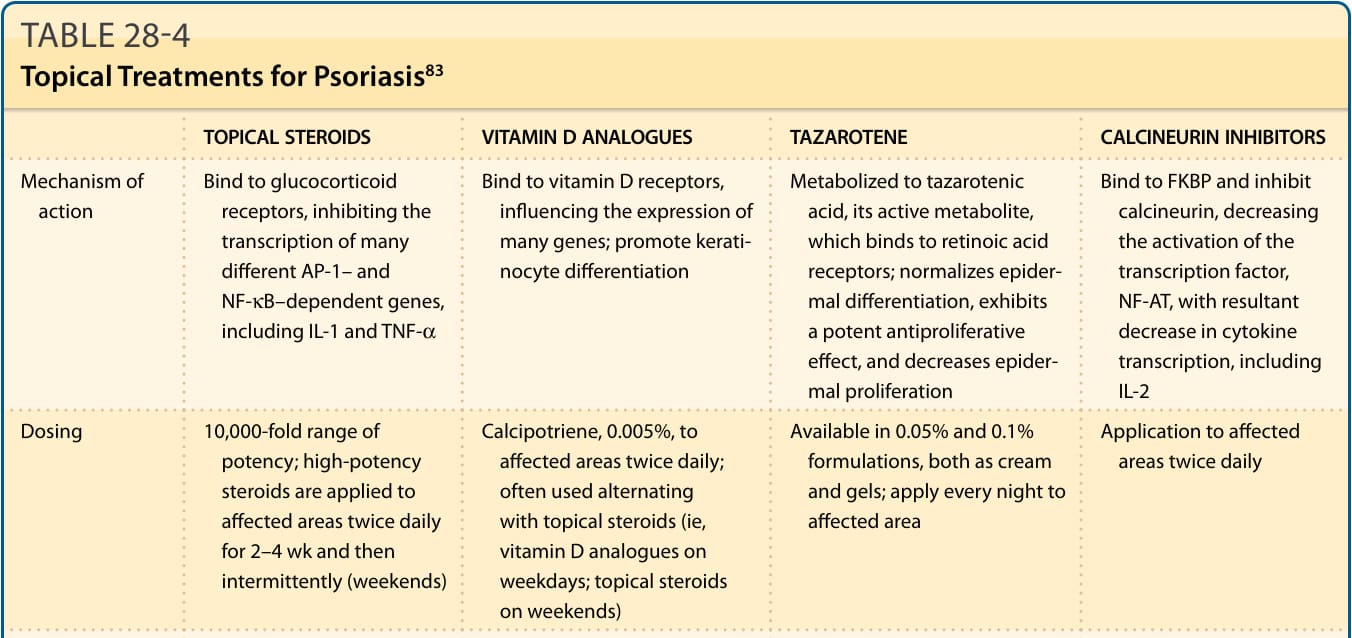
Figure 28-16 Diagnosis and treatment algorithm for patients with psoriasis. The diagnosis of psoriasis is usually based on clinical features. In the few cases in which clinical history and examination is not diagnostic, biopsy is indicated to establish the correct diagnosis. The majority of psoriasis cases fall into three major categories; guttate, erythrodermic/pustular, and chronic plaque, of which the latter is by far the most common. Guttate psoriasis is often a self-limited disease with spontaneous resolution within 6 to 12 weeks. In mild cases of guttate psoriasis, treatment may not be needed, but with widespread disease, ultraviolet B (UVB) phototherapy in association with topical therapy is very effective. Erythrodermic/ pustular psoriasis is often associated with systemic symptoms and necessitates treatment with fast-acting systemic medications. The most commonly used drug for erythrodermic and pustular psoriasis is acitretin. In occasional cases of pustular psoriasis, systemic steroids may be indicated (asterisk). Dotted arrows indicate that guttate, erythrodermic, and pustular forms often evolve into chronic plaque psoriasis. Therapeutic choices for chronic plaque psoriasis are typically based on the extent of the disease. Among the main treatment regimens (topical treatment, phototherapy, day treatment centers, and systemic treatments), first- and second-line modalities are indicated by the solid and dashed lines, respectively. Individuals with conditions that limit their activities, including painful palmoplantar involvement and psoriatic arthritis, may require more potent treatments irrespective of the extent of affected body surface area. Likewise, psychological issues and the impact on quality of life should be taken into consideration. Within each treatment regimen, first-line and second-line choices are grouped. Cyclosporin A is not considered a first-line long-term systemic treatment because of its side effects, but short-term treatment can be helpful for induction of remission. If patients have incomplete response to or are unable to tolerate individual first-line systemic medications, combination regimens, rotational treatments, or use of biologic therapies should be considered. BB-UVB, broadband UVB; BSA, body surface area; DDx, differential diagnosis; FAE, fumaric acid ester; NB-UVB, narrowband UVB; PUVA, psoralen and ultraviolet A light; tx, therapy.
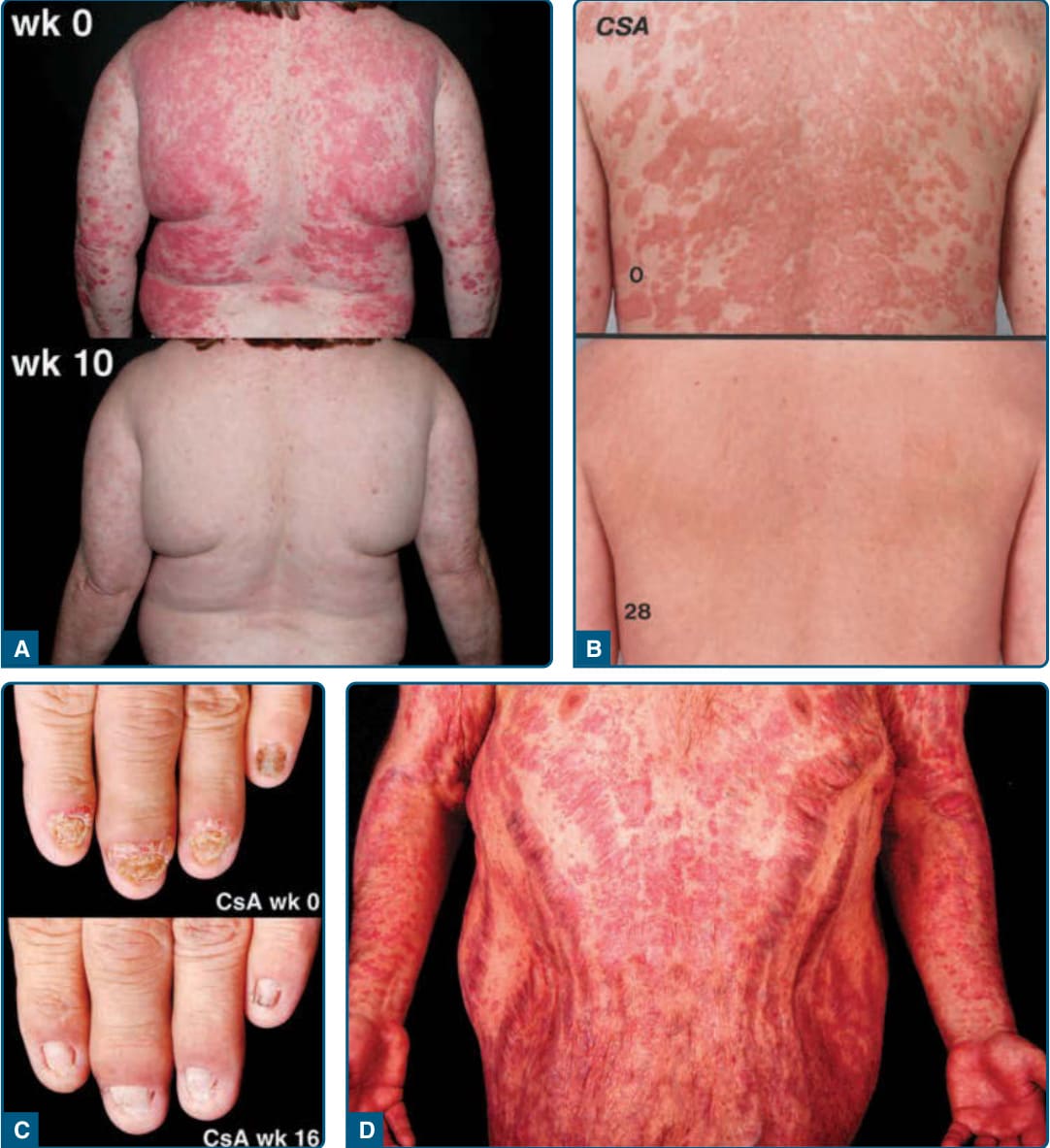
Figure 28-17 Positive and negative outcomes of psoriasis treatment. A, Near-complete improvement of psoriasis after 10 weeks of infliximab therapy. B, Marked improvement after 28 days of oral cyclosporin A (CsA) treatment. C, Marked reduction in nail dystrophy after 16 weeks of CsA treatment. D, Severe atrophy with striae distensae after several years of treatment with potent topical steroid creams. (Images used with permission from Mr. Harrold Carter.)
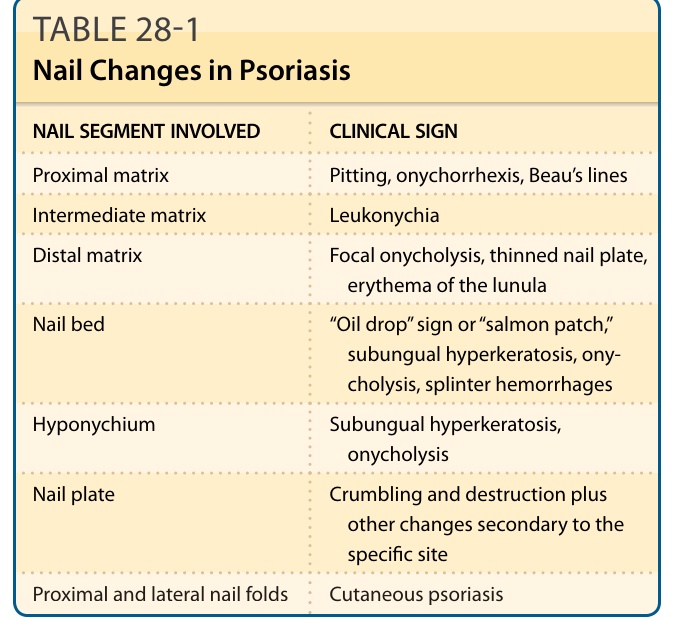
TABLE 28-1 Nail Changes in Psoriasis
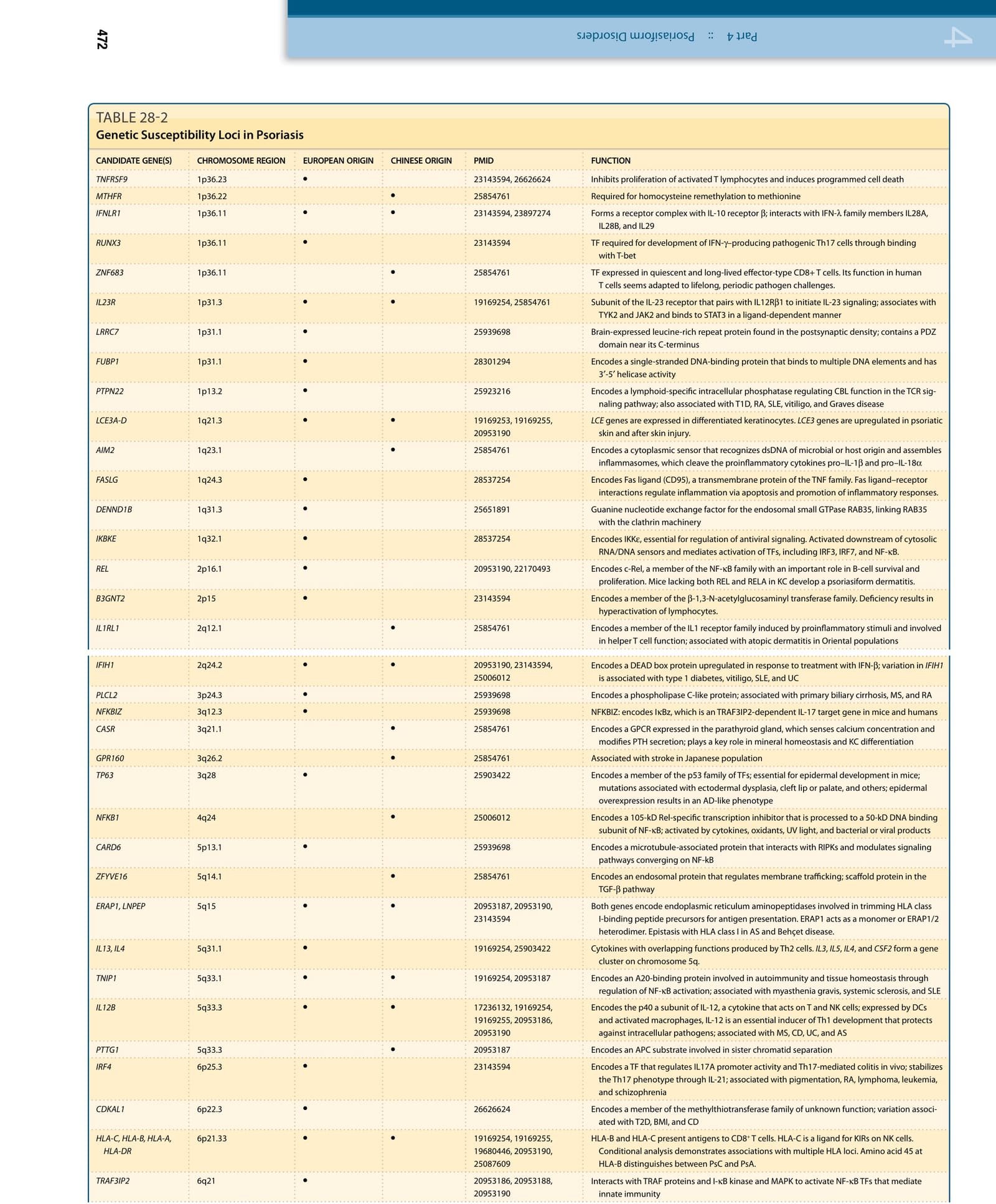
TABLE 28-2
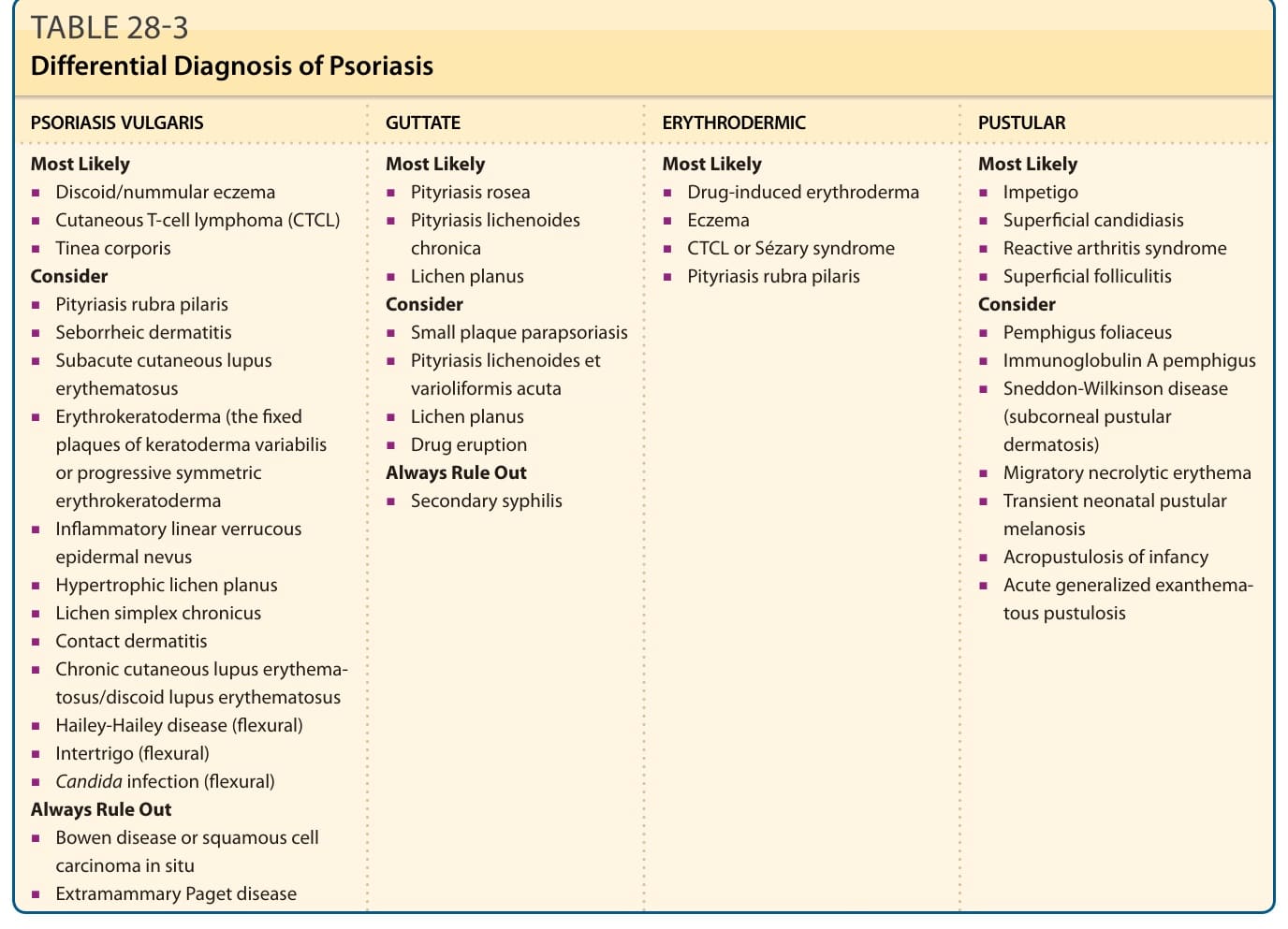
TABLE 28-3 Differential Diagnosis of Psoriasis
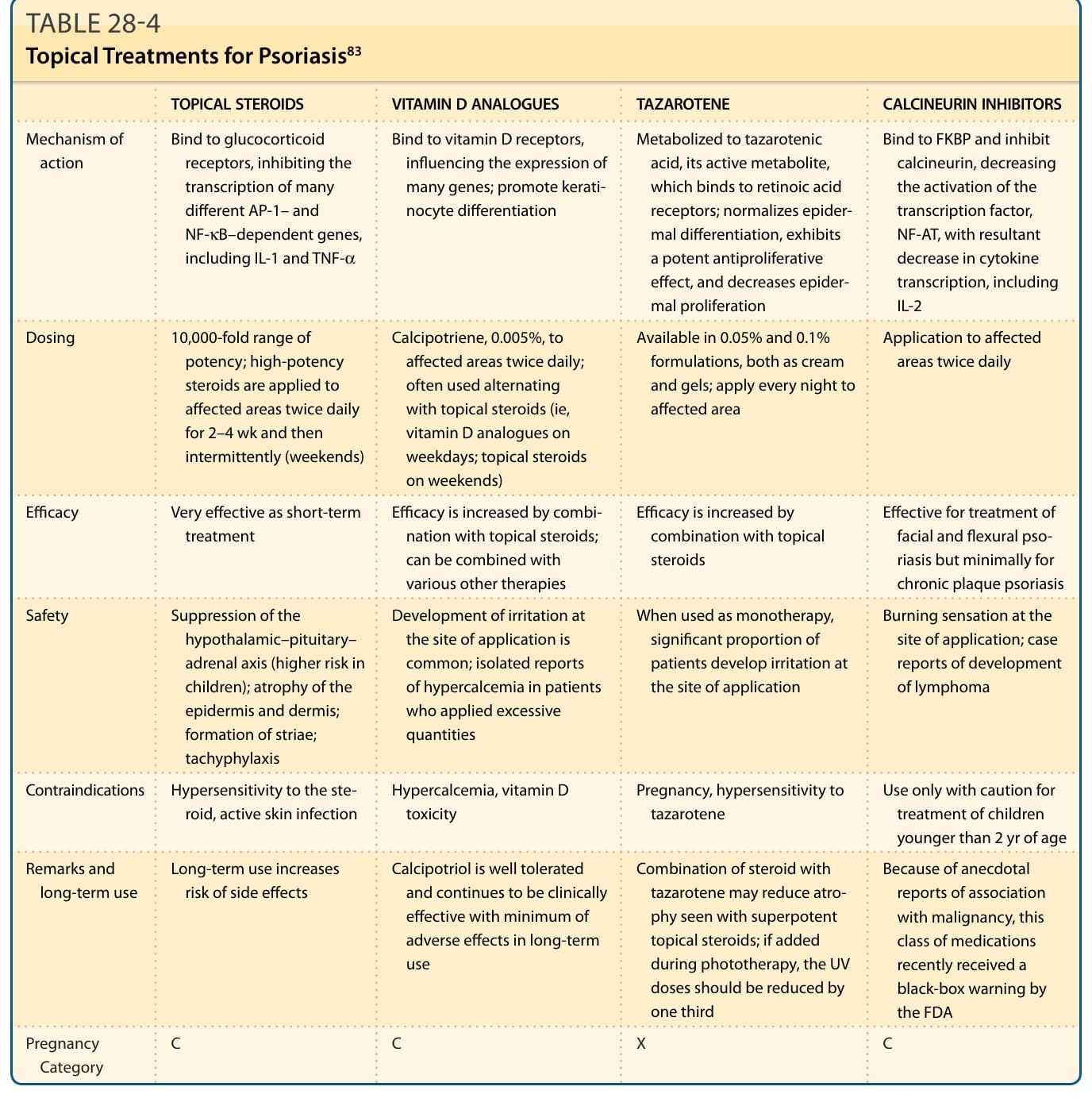
TABLE 28-4 Topical Treatments for Psoriasis83
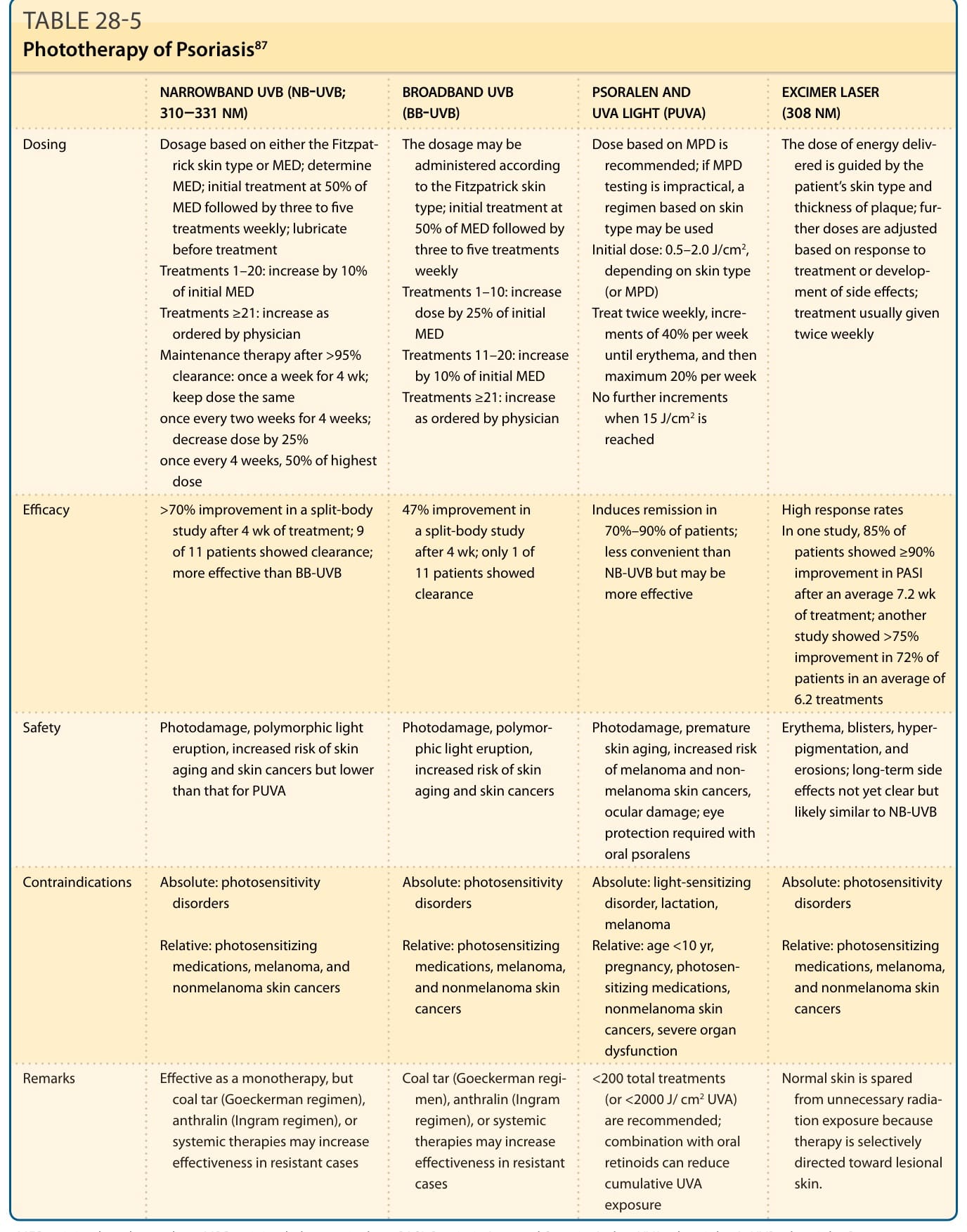
TABLE 28-5 Phototherapy of Psoriasis87
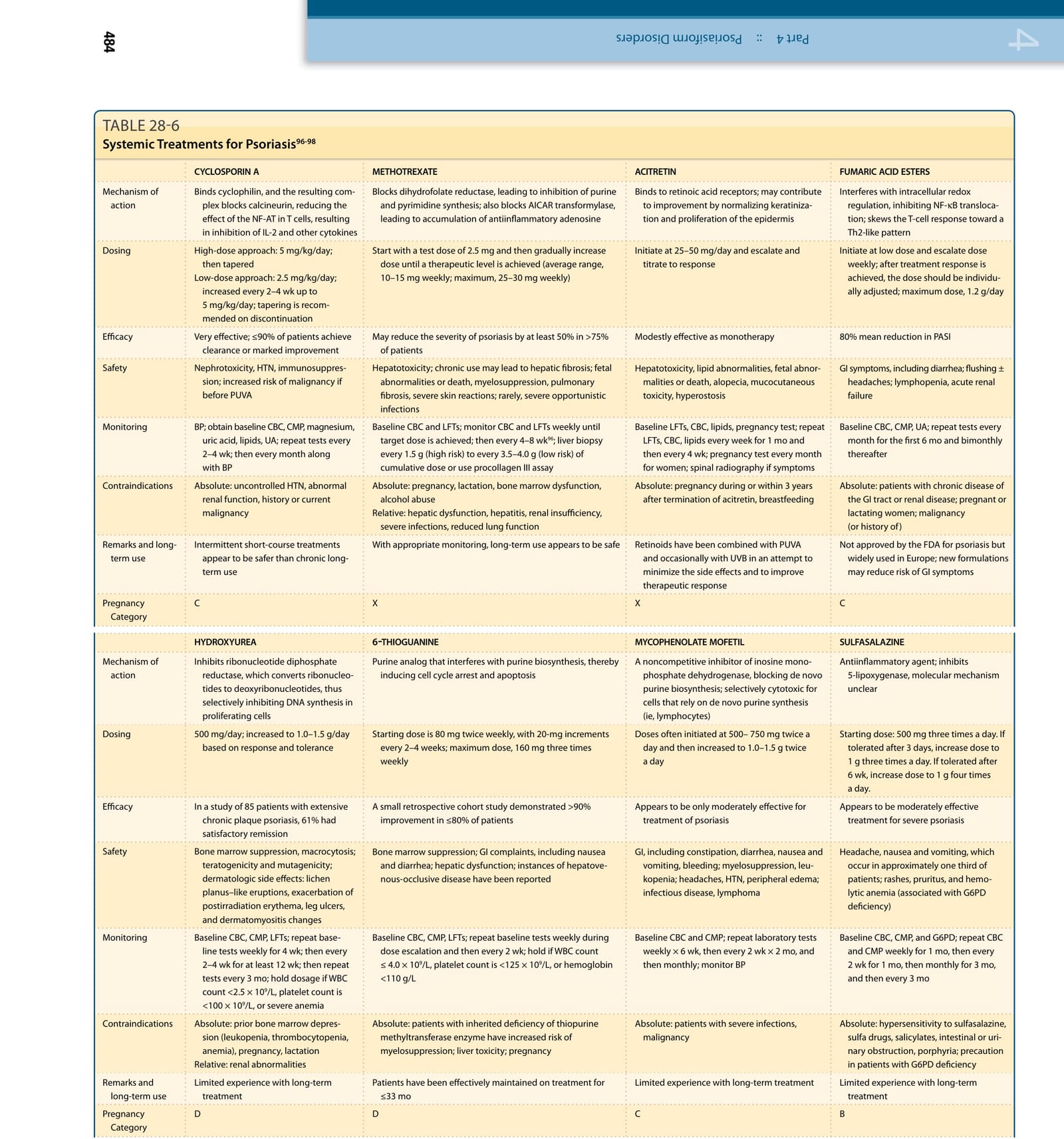
TABLE 28-6
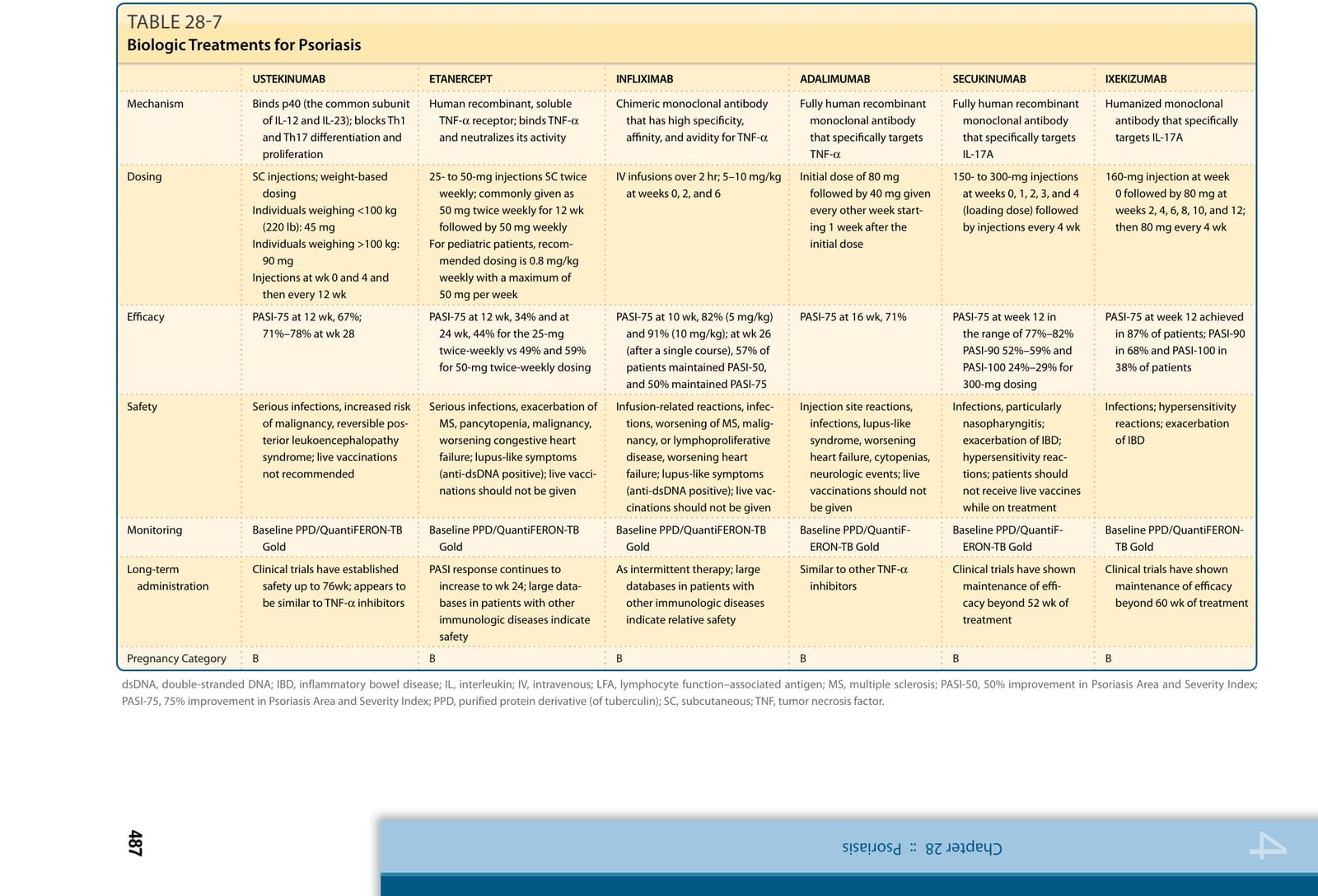
TABLE 28-7
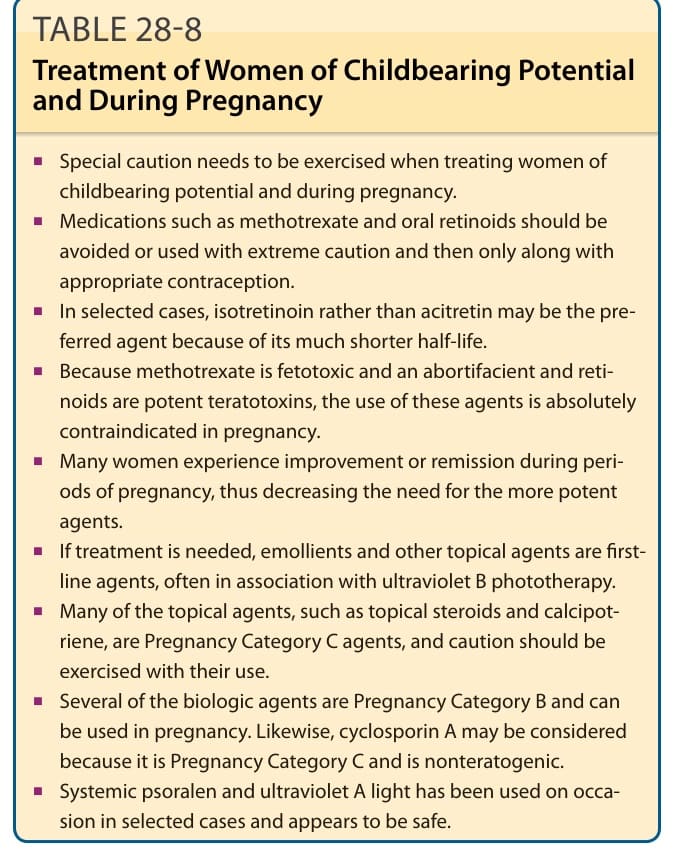
TABLE 28-8 Treatment of Women of Childbearing Potential and During Pregnancy