Occupational Skin Diseases
3
AT-A-GLANCE
■ Occupational skin diseases are the second most common occupational illness accounting for approximately 15% of occupational illnesses.
■ The vast majority of occupational skin diseases are occupational contact dermatoses (irritant contact dermatitis and allergic contact dermatitis), with approximately 80% of cases occurring on the hands.
■ Workers in the natural resources and mining, manufacturing, and education and health services have the highest rates of reported skin diseases and disorders.
■ Occupational exposures (ultraviolet radiation and chemical carcinogens) can have a significant role in skin cancer development, which is a major public health concern.
■ Personal protective equipment should be the last consideration in addressing occupational skin hazards.
INTRODUCTION
BACKGROUND
BACKGROUND
Occupational skin diseases (OSDs) are a category of skin conditions caused or aggravated primarily by workplace factors. Occupational skin diseases are common and also contribute to significant economic costs. An estimate as high as $1 billion is associated with the burden of workplace skin diseases in the US annually.1,2
In addition, OSDs may have unique implications. Federal agencies such as the Occupational Safety and Health Administration (OSHA) have mandated criteria for recording occupationally related injuries and illnesses by the employer, and the determination of work-relatedness may result in the involvement of a workers’ compensation system. Thus, a thorough knowledge of contributing factors to OSDs is vital for the timely treatment and prevention of these skin conditions to return patients and employees back to work.
HISTORICAL PERSPECTIVE
HISTORICAL PERSPECTIVE
Occupational skin diseases have existed throughout history. Even in antiquity, the Roman poet Virgil (70-19 BCE) described the cutaneous manifestations of Bacillus anthracis exposure in sheepmen.3 However, it was centuries later that the Italian physician Bernardino Ramazzini (1633-1714), recognized as “the Father of Occupational Medicine,” would document his pioneering observations of various occupational diseases in De Morbis Artificum Diatriba (Diseases of Workers). In regard to OSDs, Ramazzini observed leg ulcers in fishermen, fissures and inflammation of the hands in laundrywomen, and skin eruptions in grain workers among others.4 Although Ramazzini described associations between occupation and disease, further work identifying the causal relationship between the 2 has been the impetus for labor laws and reform. One classic example was the identification of scrotal cancer in chimney sweepers by Sir Percivall Pott (1714-1788), a British surgeon. Pott recognized that chronic exposure to soot (polycyclic aromatic hydrocarbons) lodged in the rugae led to scrotal cancer; and, in 1788, Pott’s work led to the first of many Chimney Sweeps Acts passed in Britain.5
EXPOSURE CLASSIFICATION
EXPOSURE CLASSIFICATION
The etiology of occupational injuries and illnesses, including OSDs, can be classified by the following exposures:
■ Chemical: organic and inorganic compounds, elemental substances
■ Mechanical: friction, pressure, vibration
■ Physical: ionizing and nonionizing radiation, thermal stress
■ Biologic: bacteria, viruses, fungi, parasites, insects, plants, animals
The vast majority of OSDs are attributed to chemical agents; however, mechanical, physical, and biologic exposures must be considered in the differential diagnoses as multiple concurrent exposures can often occur in the workplace.
∗Disclaimer: The contents of this publication are the sole responsibility of the authors and do not necessarily reflect the views, opinions or policies of the Uniformed Services University of the Health Sciences (USUHS), the Department of Defense (DoD), or the Departments of the Army, Navy, or Air Force. Mention of trade names, commercial products, or organizations does not imply endorsement by the U.S. Government.
OCCUPATIONAL DISEASE SPECTRUM
OCCUPATIONAL DISEASE
SPECTRUM
Of all the work-related dermatologic diseases, occupational contact dermatitis (OCD) comprises 90% to 95% of OSDs.6 The remaining 5% to 10% of OSD cases consist of a wide variety of diseases. Some of these include immunologic and nonimmunologic contact urticaria, occupational skin cancers, vibration white finger, and infections. Table 27-1 lists common categories of OSDs.
EPIDEMIOLOGY
In the United States, the Bureau of Labor Statistics (BLS) publishes annual data on occupational injuries and illnesses. Among private industry, nonfatal occupational injuries and illnesses accounted for nearly 3 million cases in 2014. Nonfatal occupational illnesses only consisted of 4.9% of the total cases, but of these, 15.2% were skin diseases.7 The distribution of nonfatal occupational illness cases is depicted in Fig. 27-1. Additionally, the rate of reported OSDs declined in 2014 among all industries from the previous year from 3.2 to 2.6 cases per 10,000 full-time workers.7 However, limitations in BLS epidemiologic data may considerably underestimate the true incidence of OSDs by as much as 10 to 50 times.2,8 Moreover, BLS categorizes wounds and bruises separately under injuries, which is not reflected in the aforementioned rates. In comparison, several studies of European countries including those with active nationwide notification programs for OCD reported incidence rates between 5 and 19 cases per 10,000 full-time workers per year for OCD alone.9-13
When comparing OSD among industries in the United States, education and health services accounted for the highest total skin disease cases (6100) followed by the manufacturing industry (4400) in 2014.7 However, the highest incidence rate occurred in the natural resources and mining industries. With only 1000 total cases, natural resources and mining had an incidence rate of 5.5 cases per 10,000 full-time workers, with education and health services following behind with 4 cases per 10,000 full-time workers.7
The total distribution of OSDs by industry is demonstrated in Fig. 27-2. The total cases of OSD has declined over the last decade, and a corresponding decline in the incidence of OSD cases involving days away from work also has been observed, potentially reflecting not only better prevention measures but improved early management.14 In 2014, among all OSDs, skin infections resulted in the longest duration away from work (median = 6 days) while wounds and bruises had the highest incidence rate involving days away from work (9.1 cases per 10,000 full-time workers).7
3
OCCUPATIONAL CONTACT DERMATITIS
Occupational contact dermatitis refers to any irritation of the skin arising from direct exposure to an exogenous agent and can be further divided into 2 general categories based on exposure, etiology, and pathophysiology of the resulting skin disease. These are irritant contact dermatitis (ICD) and allergic contact dermatitis (ACD). Occupations at increased risk for OCD are listed in Table 27-2. Specifically, ICD results from a nonimmunologic reaction to a chemical, physical, or mechanical irritation of the skin causing cutaneous inflammation via a direct cytotoxic effect from an agent. Anyone may develop an ICD, and those with compromised skin barrier such as atopic dermatitis, xerosis, or light colored skin are at higher risk.15
In contrast, ACD is a reaction to a substance by a type IV, delayed hypersensitivity reaction. This cellmediated, immune reaction requires prior sensitization to an allergen, which is usually a low-molecular weight chemical that acts as a hapten. Only a small percentage of people will develop ACD after contact from various haptens. For perspective, more than 57,000 chemicals have been known to cause skin irritation (ICD), whereas only about 3700 chemicals have been identified as true skin allergens.16 Table 27-3 provides a comparison of ICD and ACD characteristics. As would be expected, the vast proportion of OCD occur on the hands (80%).16
IRRITANT CONTACT DERMATITIS
IRRITANT CONTACT
DERMATITIS
BACKGROUND
Irritant contact dermatitis occurs when the normal epidermal barrier is disrupted by an irritant and is often concentration or duration dependent, with no previous substance exposure necessary to elicit an effect. Effects may be visible within minutes to a few hours. Wet work tasks have been identified as the most common occupational exposure leading to contact dermatitis though other frequent causes include exposure to soaps, petroleum products, cutting oils, coolants, and solvents (Fig. 27-3).21 The exposed hands are the most commonly involved sites for ICD given their interaction with the environment and opportunities for irritant exposure. Though there is no readily available diagnostic test for ICD, a careful history in addition to the patient’s clinical presentation are usually sufficient in making the diagnosis.
CLINICAL FEATURES
Irritant contact dermatitis, unlike ACD, is not a distinct clinical entity. The clinical pictures of ICD is
439
3
ORGANISM OCCUPATION TREATMENT
Bacterial Infections
Staphylococcus sp., Streptococcus sp. Meat packers, construction workers, farm workers, nurses, athletes, hairdressers, manicurists
Impetigo, cellulitis, furuncles, and abscesses
Topical: mupirocin 2%, retapamulin 1%, fusidic acid 1% Systemic agents: dicloxacillin, cephalexin, erythromycin, clindamycin, TMP-SMXa
Anthrax Bacillus anthracis Workers in contact with goat hair, wool, hides Penicillin, doxycycline (naturally occurring anthrax); Fluoroquinolone (suspected weaponized anthrax)
Fish tank granuloma Mycobacterium marinum Fisherman, fish market worker Doxycycline, ethambutol, minocycline, rifampicin
Erysipeloid Erysipelothrix rhusiopathiae Fishermen, butchers, farmers, veterinary surgeons, poultry dressers Penicillin, ampicillin, ceftriaxone, fluoroquinolone
Pitted keratolysis Corynebacterium sp. Barefooted laborers, soldiers, miners Prophylactic measures; benzoyl peroxide cleanser; topical clindamycin, erythromycin solutions, miconazole, fusidic acid
Brucellosis Brucella sp. Slaughterhouse workers, farmers, veterinarians, meat packers, livestock breeders, laboratory workers.
Doxycycline combined with streptomycin OR gentamicin OR rifampin
Tularemia Francisella tularensis Laboratory workers, farmers, veterinarians, sheep workers, hunters, cooks, meat handlers, landscapers
Fungal and Yeast Infectionsb
Tinea pedis Trichophyton rubrum; E. floccosum, T. mentagrophytes/ interdigitale
Aminoglycoside, fluoroquinolone, doxycycline
Miners, military personnel, athletes, laborers Topical: allylamines, imidazoles; Systemic agents: terbinafine, itraconazole, fluconazole
Candida, other yeast infections Candida albicans Waitresses, bartenders, food handlers Topical: imidazoles, nystatin; Systemic agents: fluconazole
Other superficial mycoses
Trichophyton verrucosum Exposure to cattle, farm buildings, and straw Topical: allylamines, imidazoles; Systemic agents: terbinafine, itraconazole, fluconazole)
Trichophyton mentagrophytes/ interdigitale
Cattle, domestic animal exposure Topical: allylamines, imidazoles; Systemic agents: terbinafine, itraconazole, fluconazole
Microsporum canis Domestic animals, esp. cats Systemic agents: terbinafine, itraconazole, fluconazole
Microsporum nanum Pigs Topical: imidazolesc
Sporothrix schenckii Gardeners, forestry workers, nursery workers, miners, farmers Systemic agents: itraconazole, terbinafine
Deep mycoses
Histoplasma capsulatum Workers with exposure to demolition, excavation activities Systemic agents: itraconazole; amphotericin B
Chromoblastomycosis Farmers, outdoor workers Systemic agents: itraconazole, terbinafine, amphotericin B
Phaeohyphomycosis Farmers, outdoor workers Surgical excision
Eumycetoma Farmers, outdoor workers Itraconazole, voriconazole
Viral Infections
Herpetic whitlow Herpes simplex virus Dental workers Acyclovir, valacyclovir, famciclovir
Orf/ecthyma contagiosum Parapoxvirus Veterinarians, sheep herders, farmers Supportive care, antibiotic coverage if secondary infection is suspected
Pseudocowpox/ milker’s nodule Paravaccinia virus Farmers, veterinarians, fresh meat handlers Symptomatic treatment; surgical curettage for large lesions
Human papilloma virus
Human papilloma
Butchers Destructive modalities (cryotherapy, curettage, electrodessica-
Human papilloma virus Human papilloma virus (HPV)-7 Butchers Destructive modalities (cryotherapy, curettage, electrodessication), podophyllotoxin, topical 5-fluorouracil, cantharidin, caustics and acids, imiquimod
(HPV)-7
virus
tion), podophyllotoxin, topical 5-fluorouracil, cantharidin, caustics and acids, imiquimod
aDose and duration, as well as antibiotic option dependent on clinical manifestation of the infection, sites affected, and methicillin-sensitivity of the causative organism.
bDose and duration of treatment are dependent on the clinical manifestation of the infection, as well as the sites affected.
cRoller JA, Westblom TU. Microsporum nanum infection in hog farmers. J Am Acad Dermatol. 1986;15(5 Pt 1):935-939.
440
Distribution of nonfatal occupational illnesses, 2014
Poisoning, 1%
Respiratory conditions, 8.4%
Hearing loss, 12.7%
Other illness, 62.7%
Skin diseases, 15.2%
Total of 144,720 cases
dependent on time-effect and dose relationship.22
For instance, a severe acute response to a strong noxious irritant may present with necrosis or ulceration, whereas chronic lesions often present
3
with lichenification, scaling, hyperpigmentation, or fissuring. ICD presentations may be categorized as follows, although no standard case definition exists for the spectrum of ICD16,23:
■ Acute
■ Irritant reaction
■ Cumulative
■ Traumatic
■ Asteatotic dermatitis
■ Pustular and acneiform
■ Subjective
Even with these categories, it is important to recognize that ICD and ACD can both have similar clinical manifestations as acute, subacute, and chronic skin conditions. Acute Irritant Contact Dermatitis: Acute ICD manifests when the skin is exposed to a potent irritant or caustic chemical from an accident at work. The irritant reaction quickly reaches a peak, then starts to heal; this is called a decrescendo phenomenon. Because of the short lag time (minutes to hours after exposure) and the clear association between exposure and skin symptoms, the diagnosis can be easily made. However, it may be difficult when the patient is unaware of an exposure, and consequently, an acute ACD should be considered in the differential diagnosis. Because acute ACD is a delayed sensitization reaction, it is characterized by the crescendo phenomenon that is a transient increase of symptom intensity despite removal of the allergen. Symptoms of acute ICD include burning, soreness, and stinging of the skin. These lesions are restricted to
Distribution of skin diseases and disorders by industry, 2014
7
Cases in 1000 Incidence per 10,000 full-time workers
6
5
4
3
2
1
0
Trade, Transportion, and Utilities
Construction
Natural Resources and Mining
Manufacturing
Information
Education and Health Services
Other Services, Except Public
Professional and Business Services
Leisure and Hospitality
Financial Activites
441
3
OCCUPATION IRRITANTS ALLERGENS
Agricultural workers Fertilizers, germicides, dust, diesel, gasoline, oils, pesticides, plants, solvents, wet-work Pesticides, animal feeds, barley and oats, fungicides, germicidal products, cement, plants, veterinary medications, wood dust, preservatives, wool
Bakers Acids, flour, spices, soaps and detergents, oven cleaners, essential oils, yeast, enzymes Ammonium persulfate; benzoyl peroxide; dyes; essential oils; enzymes; flavors; flour; some fruits
Construction workers Acids, fibrous glass, concrete, solvents, hand cleaners Cement, chromium, chromium compounds, cobalt, epoxy resins, nickel, resins, rubber allergens, wood dust
Cooks Wet work, soaps and detergents, vegetable and fruit juices, raw meat and fish, spices, sugar and flour, heat Flavors and spices, formaldehyde, garlic, sodium metabisulfite (antioxidant for vegetables)
Cosmetologists Soaps and detergents, bleaches, solvents, permanent wave solutions, shampoos, wet-work Dyes, amine-based products including parphenylene diamine, glyceryl monothioglycolate (perming solution), rosin, preservatives, rubber allergens, ethylmethacrylate, methylmethacrylate
Dentists and dental technicians
Wet work, adhesives (epoxy and cyanoacrylates), essential oils, orthodontic plasters, amalgam mixtures, solvents
Dental impression material, eugenol, anesthetics, mercury, disinfectants, methacrylates, latex, rubber accelerators
Florists Wet work, soaps and detergents, fertilizers, herbicides, pesticides, mechanical and chemical plant irritants Plants, pesticides, insecticides
Health care workers Wet work, soaps and detergents, alcohol, ethylene oxide, medications Latex gloves, anesthetics, antibiotics and antiseptics, phenothiazines, formaldehyde, glutaraldehyde, chloroxylenol
Housekeepers Wet work, soaps and detergents, cleaners, polishes, oven cleaners, disinfectants Potassium dichromate, preservatives, rubber accelerators, latex
Machinists Solvents, coolants, cutting oils, degreasers, acids, corrosion inhibitors, heat, soaps and detergents, metal filings and swarf
Additives/preservatives in cutting fluids, chromium, nickel
Automobile mechanics Abrasive skin cleaners, diesel, gasoline, greases, oils, solvent, transmission fluid, motor oils Chromium, cobalt, epoxy resin; nickel
Painters Paints, solvents, adhesives, paint removers, paintbrush
Turpentine, thinners, chromium, formaldehyde, epoxy products,
Painters Paints, solvents, adhesives, paint removers, paintbrush cleaners, soaps and detergents Turpentine, thinners, chromium, formaldehyde, epoxy products, polyester resins
cleaners, soaps and detergents
the areas where the irritant damages the skin, which may result in erythema, edema, bullae, or necrosis with sharply demarcated borders. An asymmetric pattern may hint at an exogenous cause. Acute ICD has a good prognosis with appropriate and symptomatic management. Acids and alkaline
polyester resins
are the most frequent potent culprits giving rise to an acute ICD. A common example can be seen in construction workers developing chemical burns when alkaline concrete fluid spills into work boots or soaks through garments.24 Also, several agents causing chemical burns warrant brief mention as they require
IRRITANT ALLERGIC
Onset Within minutes for strong irritants, up to days/weeks with weak irritants Within 24-96 h in sensitized individuals
Resolution Improves after 3-6 weeks away from exposure May improve within days after exposure; some cases persist
Histology Spongiotic dermatitis Spongiotic dermatitis
Mechanism Nonimmune, sensitization not required; epidermal barrier disruption, epidermal cellular damage, pro-inflammatory mediators released from keratinocytes17-19
Immune-mediated, sensitization required; Antigen-activated primed T cells; sensitization phase typically takes 10-14 d20
Agent Concentration dependent Not concentration dependent
Atopy Predisposition Variable
Diagnosis Clinical Patch testing
Diagnosis Clinical Patch testing
442
Modified from Belsito DV. Occupational contact dermatitis: etiology, prevalence, and resultant impairment/disability. J Am Acad Dermatol. 2005;53:303-313.
more specific therapies. These agents are summarized in Table 27-4.
Irritant Reaction Contact Dermatitis: Irritant reaction contact dermatitis is a subclinical irritant dermatitis in workers whose hands are excessively wet, including hairdressers, bartenders, and metal workers. On the hands, scaling and erythema are first identified under rings before spreading over fingers to hands and forearms. The thinner
3
skin of the dorsum of the hand is usually affected, though irritants can also cause vesiculation resembling pompholyx. Frequently, irritant reaction contact dermatitis heals spontaneously with hardening of the skin, but may progress to cumulative irritant dermatitis.
Cumulative Irritant Contact Dermatitis: Cumulative ICD is a consequence of multiple subthreshold insults to the skin with insufficient time between insults to allow complete restoration of the skin barrier function.28 It may result from the frequent repetition of one agitating factor but is more commonly the result of a variety of stimuli, each beginning before recovery from the foregoing stimulant. Clinical symptoms develop only when the damage exceeds an individually determined manifestation threshold. Patients with sensitive skin (ie, atopics) have a decreased irritant threshold or a prolonged restoration time, leading to earlier development of cumulative ICD. The threshold is not a fixed value for an individual but may decrease with disease progression. Therefore, in patients with cumulative ICD, even limited irritant exposure may sustain the condition. Cumulative ICD is associated with weak irritants rather than potent irritants with exposures occurring not only at work but also at home. The link between exposure and disease is frequently not obvious to the patient, and therefore, the diagnosis may be considerably delayed. These patients often complain of pruritus and pain due to fissuring of the hyperkeratotic skin with notable lichenification and chapping. In contrast to acute irritant dermatitis, the lesions are less sharply demarcated (Fig. 27-4).
CHEMICAL TREATMENT BASICS (THEN TRANSPORT TO HOSPITAL EMERGENCY DEPARTMENT FOR FURTHER EVALUATION AND TREATMENT)
Burning metal fragments of sodium, potassium, and lithium
Extinguish with Class D fire extinguisher (containing sodium chloride, sodium carbonate or graphite base) or with sand; cover with mineral oil; extract metal particles mechanicallya
Hydrofluoric acid Flush with running water; then administer calcium gluconate gel (2.5%) followed by intralesional injection, if needed
White phosphorus Remove particles mechanically; wash with soap and water; then apply copper (CuSO4) sulfate in water for several minutes, remove black copper phosphide, and wash with water. Vigorous water irrigation and removal of phosphorus particles mechanically; the use of a Wood lamp (ultraviolet light) results in the fluorescing of the white phosphorus and may facilitate its removal. A brief rinse with 1% copper sulfate solution may be helpful. Copper sulfate combines with phosphorus to form a dark-copper phosphide coating on the particles that makes them easier to see and debride, and also impedes further oxidation. However, copper sulfate can cause hemolysis and hemoglobinuria, and should be used with caution.25 More recently Kaushik and Bird recommend vigorous water washing rather than using copper sulfate.26
Phenolic compounds Decontaminate with undiluted 200- to 400-Da molecular weight polyethylene glycol (PEG), which can be located in the chemical section of hospital pharmacies, followed by copious water irrigation. Isopropanol or glycerol may be substituted if PEG is not available.27 Initial soap and water washing followed by treatment with polyethylene glycol 300 or 400 or ethanol (10%) in water.
Bromine or iodine Wash frequently with soap and water followed by treatment with 5% sodium thiosulfate.
Bromine or iodine Wash frequently with soap and water followed by treatment with 5% sodium thiosulfate.
443
aUse of water to extinguish burning metal fragments is contraindicated because of the formation of highly alkaline hydroxides.
3
Traumatic Irritant Contact Dermatitis: Traumatic ICD may arise after acute skin trauma, such as lacerations, burns, or acute ICD. The latter is seen frequently after use of harsh cleansers, and inquiring if patients have cleansed their skin with strong soaps or detergents is warranted. The syndrome is characterized by eczematous lesions and delayed healing. Continued use of the irritant may cause the condition to persist, and full resolution may not occur for many months after discontinuation of exposure. When warranted, harsh soaps should be replaced by an appropriate soap. Soap is used to emulsify an unwanted material on the skin. Typically, a specific cleanser for the substance that is to be removed can be identified and should be “harmless” yet effective.
Asteatotic Dermatitis: Also known as exsiccation eczematid ICD, asteatotic eczema, winter dermatitis, or eczema craquelé, asteototic dermatitis is a unique variant seen predominantly in elderly individuals with a history of extensive usage of soaps and cleansing products.29 This leads to dry-appearing skin with ichthyosiform scaling, and patients experiencing intense pruritus. It is a condition mainly occurring in low-humidity, winter months.30
Pustular and Acneiform Irritant Contact Dermatitis: Pustular and acneiform ICD result from exposure to specific irritants such as croton oil, mineral oils, tars, greases, and naphthalenes. This syndrome should always be considered when acneiform lesions develop in postadolescent patients who never had teenage acne. The pustules are sterile and transient.
Subjective Irritant Contact Dermatitis: Although not well understood, subjective ICD is characterized by the lack of objective clinical signs as individuals complain of a sensation of burning or stinging (sensory irritation) after contact with certain
444
chemicals.31 Though no visible cutaneous irritation is generally observed, these reactions are usually dose-related and have been observed with chemicals such as lactic acid, which can be found in cosmetic products.32
ALLERGIC CONTACT DERMATITIS
ALLERGIC CONTACT
DERMATITIS
BACKGROUND
Although it has been widely reported that 80% of all OCD cases are caused by ICD, there is broad variation in the distribution of ACD versus ICD among reports of OCD in the literature.16,33 For instance, the North American Contact Dermatitis Group (NACDG) reported significantly more occupational ACD (60%) than ICD (32%).34 A myriad of reasons may contribute to the disparate rates and include differences in the types of industries being studied in a geographical area, the age and sex distribution of evaluated patients, selection biases inherent among patients referred to tertiary dermatologic centers, the ability of the health care provider to fully assess the worker by patch testing, and existing national regulations and notification systems.35
CLINICAL FEATURES
Clinically, both ICD and ACD can have similar manifestations of pruritus, pain, erythema, swelling, xerosis, formation of wheals or blisters as well as lichenification. They both can manifest as an acute, subacute, or chronic condition. Health care workers are reported to be one of the most commonly affected professions with identified allergens, including glutaraldehyde, formaldehyde, quaternium-15, and thiuram mix.36 Other professions frequently affected include machinists, construction workers, homemakers/house cleaners, food handlers, custodians, stock handlers, cosmetologists, and laboratory technicians (Fig. 27-5).35 Major occupational contact allergens are listed in Table 27-5.
CONTACT URTICARIA AND IMMEDIATE CONTACT REACTIONS
Contact urticaria (CU) is a transient wheal and flare reaction from direct contact with a chemical or protein agent. Lesions appear within minutes to an hour and resolve within hours after exposure. Contact urticaria is categorized as either nonimmunemediated or immune-mediated.38 Additionally, CU of uncertain mechanism also has been recognized
and demonstrates features of both nonimmune and immune-mediated CU.
NONIMMUNOLOGIC CONTACT URTICARIA
NONIMMUNOLOGIC
CONTACT URTICARIA
BACKGROUND AND CLINICAL FEATURES
Nonimmunologic contact urticaria (NICU), though less well understood in regard to pathogenesis, is caused by a wide array of agents in exposed individuals who develop a reaction without previous sensitization. Nonimmunologic contact urticaria is the most common type of contact urticaria, remains localized, and is less severe than immunologic contact urticaria (ICU) reactions. Additionally, in contrast to ICU, NICU reactions are not inhibited by H-1 antihistamines, but oral or topical nonsteroidal antiinflammatory medications are effective, suggesting a role of prostaglandins in the pathogenesis of these lesions.39 Classification of NICU agents are reviewed in Table 27-6.40
Cobalt Chromate Cosmetics and fragrances Epoxies Nickel Plants Preservatives Resins Acrylics
Cobalt Chromate Cosmetics and fragrances Epoxies Nickel Plants Preservatives Resins Acrylics
3
CATEGORIES EXAMPLES
Animals Caterpillars, arthropods, corals
Foods Pepper, mustard, thyme
Fragrances and flavorings Cinnamic aldehyde, balsam of Peru, cinnamic acid
Medicaments Witch hazel, benzocaine, camphor
Metals Cobalt
Plants Nettles, seaweed
Preservatives and disinfectants Benzoic acid, formaldehyde, sorbic acid
Miscellaneous Butyric acid, pine oil, turpentine
Miscellaneous Butyric acid, pine oil, turpentine
Data from Basketter D, Lahti A. Immediate contact reactions. In: Johansen DJ, Frosch JP, Lepoittevin JP, eds. Contact Dermatitis. 5th ed. Berlin: Springer; 2011:137-153.
IMMUNOLOGIC CONTACT URTICARIA
IMMUNOLOGIC CONTACT
URTICARIA
BACKGROUND AND CLINICAL FEATURES
Immunologic contact urticaria (ICU) is a type I hypersensitivity reaction mediated by allergen-specific immunoglobulin E (IgE) and seen in individuals previously exposed to the specific agent. Atopic individuals are particularly at risk. ICU can spread beyond the cutaneous localized contact point and the level of spread is categorized in a staging system presented in Table 27-7.41
Contact urticaria from latex gloves is the prototypical example of ICU. Beginning in the early 1980s, a combination of factors including the use of latex gloves for universal precautions in light of the increasing prevalence of HIV and viral hepatitis contributed to an alarming number of individuals with type I
STAGING SYSTEM
Stage 1 Localized urticaria, dermatitis, or nonspecific symptoms (itching, tingling, burning, etc.)
Stage 2 Generalized urticaria
Stage 3 Urticaria and rhinoconjunctivitis, asthma, or GI symptoms
Stage 4 Anaphylaxis
Stage 4 Anaphylaxis
445
Adapted from Wang CY, Maibach HI. Immunologic contact urticaria—the human touch. Cutan Ocul Toxicol. 2013;32:154-160.
3
hypersensitivity from latex rubber.42 As the natural rubber latex (NRL) allergy epidemic was identified in the United States and Europe, various organizations and agencies recommended several prevention strategies, including reduction of protein content in gloves (to reduce allergenicity) and providing latex-free alternatives, which helped reduce the incidence of latex allergies.43,44 Apart from health care workers, occupations commonly affected by ICU from NRL include kitchen workers, cleaners, others who wear NRL, as well as those with occupations involved in manufacturing rubber bands, surgical gloves, and latex dolls. It is important to note that NRL can also cause a type IV hypersensitivity reaction (ie, ACD), which accounts for the majority of allergic reactions (>80%) to NRL.45,46
Furthermore, virtually any food is capable of eliciting an ICU response and is the second most common cause of ICU. Foods such as potato, carrot, apple, tomato, shellfish, seafood, and meats are well documented, and recent literature has highlighted the problem of wheat allergens among bakers.41 Additional causes include preservatives, fragrances, disinfectants, antibiotics, topical medicaments, epoxy resin hardeners, formaldehyde in clothing, several woods, and birch pollen.
CONTACT URTICARIA OF UNCERTAIN MECHANISM
CONTACT URTICARIA OF
UNCERTAIN MECHANISM
BACKGROUND AND CLINICAL FEATURES
This type of reaction may occur with substances that produce a CU and a generalized histamine-type reaction but lacks a direct or immunologic basis for the reaction. It is most commonly caused by ammonium persulfate in bleaching hair boosters and typically has a sudden onset characterized by erythema, edema, severe pruritus, urticaria, and occasionally syncope with wheezing and dyspnea.
OTHER OCCUPATIONAL SKIN DISEASES BY EXPOSURE CATEGORIES
CHEMICAL EXPOSURES
CHEMICAL EXPOSURES
A significant proportion of chemical exposures result in OCD. However, there are also several exposures that lead to unique skin manifestations such as acne.
ACNE Background and Clinical Features: Different forms of acne have been observed in several work settings associated with certain chemical exposures.
446
Machinists with skin exposed to industrial or cutting oils can develop oil acne not only in oil-soaked clothing regions but in other areas exposed to potential airborne oil mists.47 Additionally, coal tar plant workers, roofers, and road and construction workers exposed to coal tar oils, creosote, and pitch can develop comedonal acne particularly on the face and malar regions.48
These compounds also contain polycyclic aromatic hydrocarbons (PAH), which are carcinogenic as well. Exposures to certain dioxins, naphthalenes, biphenyls, dibenzofurans, azobenzenes, and azoxybenzenes also have been associated with one of the more notable forms of acne, chloracne.49 Chloracne from these chemical exposures are typically characterized by multiple closed comedones and straw-colored cysts primarily over the malar crescents and retroauricular folds that may also involve the neck, trunk extremities, buttocks, scrotum, and penis. Specifically, a potent inducer of chloracne includes 2,3,7,8-tetrachlorodibenzo-p-dioxin (TCDD), which was a contaminant in some batches of Agent Orange used during the Vietnam War as well as a by-product in other industrial processes.
MECHANICAL EXPOSURES
MECHANICAL EXPOSURES
The skin is exposed to various forms of mechanical insults on a daily basis, and numerous occupations involving repetitive tasks may lead to mechanical trauma of the skin. Friction, pressure, pounding, and vibration of the skin may create changes ranging from calluses and blisters to myositis, tenosynovitis, osseous injury, nerve damage, lacerations, shearing of tissue, or abrasions. Lacerations, abrasions, tissue disruption, and blisters additionally pave the way for secondary infection by bacteria, or less often, fungi, parasites, and viruses. Though the skin is well adapted to cope with such insults, the time allowed for adaptation determines the reaction of the skin. The effects on the skin manifestations induced by the trauma are modified by age, gender, humidity, sweating, nutritional status, infection, preexisting skin disease, as well as genetic and racial factors.50
Certain occupations are prone to having distinct mechanically induced skin dermatoses. For instance, musicians may develop lesions in areas of chronic rubbing specific to the instrument being played (harpist’s finger, fiddler’s neck, guitar nipple, cellist’s chest, flautist’s chin). Athletes who experience repetitive trauma while running or shearing forces from quick changes in directional movements may develop black heel or talon noir as well as blisters and jogger’s toe. A relatively new group of skin disorders has been described with prolonged computer use with either repetitive trauma (mousing callus) or prolonged pressure (computer palms).51 Fiberglass may cause a mechanical irritation by penetration into the skin in those who work with the man-made fibers, often causing a pruritic eruption that may resemble scabies. Plants may also induce mechanical irritant dermatitis from delicate hairs (trichromes) or hairs with
barbs (glochids). The irritation is caused by both the mechanical action of the oxalate crystal and subsequent penetration of plant toxin or enzyme into the skin.52 Onycholysis has been reported from repetitive pressure leading to total or partial anoxia of the distal finger tips in housewives and slaughter house workers who skin cattle.53,54
The use of vibration-producing tools can induce painful vascular spasms in the fingers and hands known as white finger or vibration-induced white finger (VWF), which is a secondary type of Raynaud phenomenon.55
In addition to neurovascular, soft tissue, fibrous, and bone injury to the hands and forearms, workers who use pneumatic riveters, chippers, chainsaws, drills, and hammers are at greater risk of suffering from VWF, especially in cold climates. Vibration frequencies between 30 and 300 Hz are most strongly associated with VWF and smoking is a known risk factor. Continued improvements in design of modern equipment has helped to reduce vibration and decrease the prevalence of these symptoms. In today’s society with increasing automation, less frequent manual operation of tools, and better protective gear, mechanically induced occupational skin lesions have greatly decreased in prevalence.30
PHYSICAL EXPOSURES
PHYSICAL EXPOSURES
Physical agents such as extremes in temperatures, ionizing, and nonionizing radiation are well-known causes of occupational skin disease.
THERMAL STRESS Background and Clinical Features: Heat may cause burns, hyperhidrosis, erythema, and telangiectasias. Workers in hot environments such as farmers and construction workers may develop miliaria in areas of chronic rubbing with clothing, leading to symptoms of pruritus, papule formation, and even a small risk of heat exhaustion due to an inability to maintain normal homeostasis through sweating. Relief may be obtained with wearing loose clothing and cooling the skin. Erythema ab igne also has been observed in repeated, prolonged exposure to heat and in those using laptops on their laps for extensive periods of time. In addition, preexisting skin conditions and diseases may be aggravated by heat exposure, such as rosacea, herpes simplex, and acne vulgaris. Work-related burn injuries often result in hospitalizations with extensive treatment. Hot grease burns may be seen in kitchen workers, roofers may incur hot tar burns, and flammable and explosive liquids are known to cause most industry-related burns. Specific occupations are associated with higher rates of burn injuries, with welders having the highest incidence rates for all burn injuries.56 Cooks, laborers, food service workers, mechanics, and nurse aides are also occupations at higher risk. One report noted that
3
almost one third of all hospitalized burn injuries were work-related, highlighting the impact of this occupational hazard.57
Cold exposure may lead to Raynaud phenomenon. Frostbite is another common cold injury that may be seen affecting acral body surface areas such as the nose, ears, fingers, and toes of firemen, construction workers, postal workers, and military personnel. Individuals engaged in winter sports, refrigeration workers, icemakers, liquefied gas makers, ski patrolmen, and mountain rescue workers are also at risk.
IONIZING AND NONIONIZING RADIATION Background and Clinical Features: Occupational skin cancers are more common than generally recognized, although it is difficult to obtain an accurate estimate of their prevalence. Ultraviolet radiation (UV), both natural and artificial, is the most important cause for all types of skin cancer to include melanoma, squamous cell carcinoma, and basal cell carcinoma.58 It is estimated that avoiding this risk factor alone could prevent more than 3 million cases of skin cancer each year.59
Occupational skin cancer is characterized by long induction periods, often decades, with the first manifestations often not seen until many years after the occupational exposure.60 Outdoor workers, loosely defined as individuals who work outdoors for 3 or more hours on a typical workday, are at high risk of harmful UV exposure and development of skin cancer.61 These may include workers in industries such as agriculture, building and construction, fishing, transport, and landscaping as well as physical education teachers and police officers. Other professions at risk include pilots and cabin attendants. A meta-analysis identified twice the rate of melanoma in pilots and cabin crew compared with the general population.62 Because UV radiation is recognized to increase by 10% to 12% for every 1000 m in elevation, airline crews have the potential for increased UV exposure by as much as 2 to 3 times at cruising altitude.63 One study identified that pilots and cabin crew flying for approximately 56 minutes at cruising altitude receive the same amount of UV-A as that from a 20-minute tanning bed session.64
As 90% of squamous cell carcinoma and basal cell carcinoma and two-thirds of melanomas may be attributed to excessive UV radiation exposure, the aim of primary skin cancer prevention is to limit UV radiation exposure.60 Three measures successful in the prevention of skin cancer in outdoor workers include regular use of sunscreen, protection from direct UV radiation by suitable clothing, and changes in behavior with awareness of health and diseases resulting from exposure to UV radiation. Even with recommended strategies to use protective measures such as wide-brimmed hats, longsleeve shirts and pants, sunscreen, and avoiding peak UV times (10 am to 3 pm), many studies have shown inadequate use of sun protection measures by outdoor
447
3
workers.65 An Australian study of construction workers discovered that only 10% of workers were using adequate sun protective measures.66 This highlights the continued need for an increase in skin cancer awareness and safe sun practices in individuals with high levels of work-related UV radiation exposure. To determine the role of the workplace in the development of skin cancer and actinic skin damage, one must take into consideration not only detailed occupational history with job descriptions from earliest worker employment but also nonoccupational activities, hobbies, and outdoor recreational pursuits from a worker’s past. Ionizing radiation, such as X-rays, can also cause skin cancer, primarily squamous cell carcinoma and less often basal cell carcinoma. High levels of acute exposure may lead to acute radiation dermatitis observed as erythema, itching, and cutaneous inflammation. Higher doses may manifest as skin blisters, hemorrhage, and even necrosis (Fig. 27-6). Delayed sequelae from exposure may result in chronic radiation dermatitis with skin atrophy, abnormal pigmentation, keratinization disorders, increasing sclerosis, telangiectasias, hair loss, and xerosis due to loss of sebaceous glands. Ionizing radiation sources may be found in a wide range of occupational settings, and examples include health care facilities, nuclear weapon production facilities, nuclear reactors and their support facilities, and various manufacturing settings.67
BIOLOGIC EXPOSURES
BIOLOGIC EXPOSURES
BACKGROUND
A number of infectious agents are responsible for occupational skin disease, especially in occupations that involve contact with animals. With greater awareness
448
and implementation of public health measures, many historically prominent infections have greatly diminished in the general population. However, certain infectious agents are still observed in at-risk occupational groups such as health care workers, military personnel, farmers, and forestry workers. These infections, in turn, may affect the productivity of a worker and ultimately the employer when conditions favor disease transmission.
BACTERIAL INFECTIONS Staphylococcus and Streptococcus: Staphylococci and streptococci are gram-positive bacteria that can contaminate minor lacerations, burns, puncture wounds, or abrasions leading to impetigo, cellulitis, furuncles, and abscesses. Though all occupations may be at risk, they are prevalent in meat packers, construction workers, farm workers, and those working in close contact with other infected individuals, for example, nurses, athletes, hairdressers, and manicurists. Epidemics of methicillin-resistant Staphylococcus aureus infections that have been difficult to control have been documented in professional football players in the United States.68
Anthrax: Anthrax, though endemic in parts of Africa and Asia, is rare in the United States and predominantly a cutaneous infection (Woolsorter disease) found in occupations in which workers handle imported goat hair, wool, and hides contaminated with the spores from the bacterium Bacillus anthracis.69 Only 49 anthrax-related epidemiologic investigations were conducted by the U.S. Centers for Disease Control and Prevention between 1950 and 2001, with most involving agricultural settings or textile mills.70 Because of the highly infectious nature of its spores and recent world events including the 2001 bioterrorism anthrax attacks in the United States, Bacillus anthracis is also considered a high-priority pathogen by several U.S. government agencies for its potential as a bioterrorist agent.
Fish Tank Granuloma: Mycobacterium marinum is an acid-fast, nontuberculous mycobacterium that was first isolated in 1926 from salt water fish carcasses in the Philadelphia aquarium.71 It is responsible for fish tank granuloma (also known as swimming pool granuloma), a distinct infection presenting as a warty nodule or plaque usually at a point of trauma, often 6 weeks after exposure. Individuals with fish- or water-based occupations and hobbies are most at risk. Vectors of the infection include fresh or salt water fish, shellfish, snails, water fleas, or dolphins.72,73
Erysipeloid (Fish-Handler Disease): The gram-positive bacterium Erysipelothrix rhusiopathiae is responsible for the acute infection of erysipeloid, which is almost always an occupational disease. Human infection is associated with handling of decaying animal products such as fish, shellfish, mammals, and poultry. Infection occurs when a worker has a predisposing insult to the skin, such as an abrasion or cut that allows entry of the bacteria. A localized sharply
demarcated bright red to violaceous infection, often involving the hands, then ensues. Occupations at risk include fisherman, butchers, farmers, veterinary surgeons, and poultry dressers.74
Pitted Keratolysis: Pitted keratolysis is a rather common dermatologic condition caused by grampositive bacterium (usually Corynebacterium species) that infects the stratum corneum of the plantar skin, leading to malodor, hyperhidrosis, and sliminess of the skin. Though well documented among bare-footed laborers, such as paddy farmers in the tropics, it is also observed in soldiers, miners, and laborers as a result of occlusive, protective shoe-wear that creates a warm and moist environment for the bacteria. Because of pain while marching and walking, the condition may cause reduced operational deployability when observed in military personnel.75 A study of 144 US Marine volunteers in combat in Vietnam during monsoon months discovered that 49% of soldiers were affected with this condition.76
Brucellosis: Brucellosis is a worldwide zoonosis caused by gram-negative bacterium of the genus Brucella that is primarily a disease of animals in which humans are an accidental host.77 Occupationally, the disease is contracted through inhalation of contaminated aerosols, contact with conjunctival mucosa, or entry of bacteria through cuts in the skin as a result of contact with infected animals or their products.78
Occupations at highest risk include slaughterhouse workers, farmers, veterinarians, meat packers, livestock breeders, and laboratory workers. Nonoccupational sources of exposure include ingestion of infected milk or milk products. Brucellosis is a multisystem disease that presents with symptoms such as fevers, night sweats, myalgia, weight loss, and arthralgia but has a propensity for more serious chronicity. Skin manifestations are generally infrequent and have been reported to affect anywhere from 1% to 14% of those infected.79
Cutaneous findings of brucellosis are often nonspecific, and findings include disseminated papular and nodular eruptions, nodosum-like erythema, extensive purpura, diffuse macular and papular rash, chronic ulcerations, and abscesses.80
Tularemia: Tularemia is a potentially severe zoonosis caused by Francisella tularensis, a gram-negative bacterium transmitted by ticks, fleas, deerflies, as well as by ingestion, inhalation, or direct contact with infected tissues. The most common presentation of tularemia is the ulceroglandular form, where an ulcer arises at the site of inoculation and regional lymphadenopathy develops. The more severe, though less common, pneumonic form may develop after inhalation of the bacteria. Historically, tularemia has been reported among laboratory workers, farmers, veterinarians, sheep workers, hunters, cooks, and meat handlers; however, recent literature supports an increased risk in landscapers, particularly for the pneumonic form of the disease. Health care workers in tularemia-endemic areas should consider a diagnosis of tularemia in landscapers who have fever or pneumonia.81
3
FUNGAL AND YEAST INFECTIONS
A wide variety of mycoses may be responsible for occupational dermatoses including most kinds of dermatophytoses, candidiasis, and even deep mycoses. Tinea pedis is a common infection of the general population but certain workers are at even greater risk of infection as a result of humid, occlusive footwear such as miners, military personnel, athletes, and laborers.25 Zoophilic dermatophytes such as Trichophyton verrucosum are associated with cattle, farm buildings, and straw; Trichophyton mentagrophytes may be transmitted by cattle and domestic animals; Microsporum canis is identified in domestic animals, especially cats; and, Microsporum nanum may be found in pigs.26,27,82 Thus, occupations at risk for these zoophilic dermatophytes include slaughterhouse workers, veterinarians, farmers, and pet shop workers. Bartenders, waitresses, and food handlers are prone to developing candida skin infections as a result of their wet work, which provides a favorable environment for the yeast in macerated skin near the nails and between the digits. Prevention is key through proper drying of the skin and wearing protective gloves. Inoculation of Sporothrix schenckii via puncture wounds from thorns, splinters, sticks, and sphagnum moss can lead to sporotrichosis. Those at risk include gardeners, forestry workers, nursery workers, miners, and farmers. Since the late 1990s, there has been an epidemic of sporotrichosis associated with transmission by cats in Rio de Janeiro, Brazil, thus adding veterinarians as an at-risk occupation.83
Other subcutaneous and deep mycoses known to be responsible for OSDs include histoplasmosis, with at-risk occupations being construction workers and farmers who participate in demolition, soil-disrupting activities, and excavation in endemic areas. Chromoblastomycosis, phaeohyphomycosis, and eumycetoma (Madura foot) are subcutaneous mycoses that are all acquired as a result of penetrating trauma to the skin.84 Farmers and outdoor workers are most at risk for these chronic and challenging mycoses.
VIRAL INFECTIONS Herpes Simplex Virus: The high prevalence and infectious nature of herpes simplex virus (HSV) makes it an occupational hazard among health care workers, particularly for dental practices, where HSV can be easily spread by direct (lip) or indirect (finger) contact, especially when a lesion is present in the patient.85
Orf (Ecthyma Contagiosum): Orf, or ecthyma contagiosum, is a zoonotic infection caused by a parapoxvirus that commonly infects sheep and goats and is transmitted to humans through contact with infected animals or fomites. Veterinarians, sheep herders, and farmers are most at risk, though it has been reported in children after visiting petting zoos and livestock fairs.86
Pseudocowpox (Milker Nodule): Milker nodule, also known as pseudocowpox, is an occupational
449
3
viral infection transmitted by direct contact from infected cows’ udders to farmers, veterinarians, and also fresh meat handlers. Painful nodules similar to orf develop on exposed sites, become crusted, and then spontaneously resolve. Prevention consists of treating the cows’ mastitis as well as using preventive measures such as gloves, soap, water, and disinfectants before and after handling these animals.87
Human Papilloma Virus: Viral warts causes by human papilloma virus (HPV) have been well documented in butchers and meat and fish handlers. Though these warts may be due to many different serotypes of HPV, HPV-7 (Butcher wart virus) is almost exclusive to this group of workers.88 Recent innovations in dermatology as well as other medical specialties in the treatment of HPV-induced diseases have brought up questions regarding the controversial nature of the risk of nasopharyngeal HPV in health care personnel. However, a recent study supports a low HPV transmission risk of oral and nasal HPV in employees performing CO2-laser evaporation of genital warts or loop electrode excision procedure (LEEP) of cervical dysplasia by gynecologists, though more studies are likely needed to further assess this relatively new occupational risk.89
Bloodborne Pathogens: The 3 bloodborne viruses that are known to pose a serious occupational threat to health care workers include hepatitis B virus (HBV), hepatitis C virus (HCV), and HIV. Although infections by these bloodborne pathogens generally do not exhibit acute skin findings, untreated and prolonged viral burden may have skin manifestations as well as other systemic dysfunctions. Acquisition of infection from body fluids and accidental puncture wounds are known routes of risk to health care personnel. Though safer needle devices for performing procedures and universal infection control precautions are in place, they will not completely eliminate the risk, and prophylactic treatment will remain an important component of prevention efforts.90
DIAGNOSIS OF OCCUPATIONAL SKIN DISEASES
PATCH TESTING AND ALLERGIC CONTACT DERMATITIS
PATCH TESTING AND
ALLERGIC CONTACT
DERMATITIS
Patch testing is the gold standard in diagnosing ACD and is pivotal in helping to determine the etiology of OSDs when assessing contact dermatitis. Early evaluation and diagnosis of ACD has been associated with decreased health care costs and improved disease course and quality of life of the patient.91 Taking a careful exposure and occupational history is pivotal in
450
guiding appropriate selection of allergens to be tested. Testing is performed using commercially prepared allergens, which are mixed in petrolatum or water and sold in individual syringes or vials. Allergens are grouped in series, such as the rubber, metals, glues and adhesives series, or by profession, such as the dental, hairdressers’, or bakers’ series. The TRUE Test® is a prepackaged, ready-to-apply kit that now consists of 3 adhesive panels of 35 allergens and allergen mixes that are reported to be responsible for the majority of cases of ACD. The North American Contact Dermatitis Group (NACDG) standard screening tray includes a greater range of allergens and is also widely used among other commercially available series. It may be necessary to test products from the workplace, as not all allergens may be included in the panel used. However, a basic principle is to never test an unknown substance or test with known irritants such as solvents, cements, and soaps. Patch testing should be performed by a trained provider, who has access to a wide range of allergens for testing purposes and experience in interpreting results. The successful management of ACD requires a meticulous and dedicated physician who is able to not only recognize and treat the skin disease but also has an understanding of the ramifications of the results in regard to the patient’s occupation and potential legal aspects of workers’ compensation boards.
SKIN PRICK TESTING AND CONTACT URTICARIA
SKIN PRICK TESTING AND
CONTACT URTICARIA
In contrast to patch testing, skin prick testing (SPT) is an allergy test used for the identification of IgE-mediated immediate hypersensitivity reactions (eg, immunologic contact urticaria). The skin prick introduces a small amount of allergen into the epidermis eliciting a localized response in the form of a wheal and erythema at the site of testing when positive. In regard to OCD, the test is used to help make a diagnosis when contact urticaria is suspected. Conventionally, it is also used for diagnosing other type I immediate hypersensitivity reactions in patients with rhinoconjunctivitis, asthma, atopic eczema, and food allergy. Specifically for ICU, a diagnostic algorithm is illustrated in Fig. 27-7. Of note, alternatives similar to SPT include scratch testing and scratch-chamber testing, which may be used for nonstandardized allergens because routine use in place of SPT is not recommended.92
RADIOALLERGOSORBENT TESTING AND CONTACT URTICARIA
RADIOALLERGOSORBENT
TESTING AND CONTACT
URTICARIA
Blood tests may be used to help measure the amount of allergen-specific antibodies present in the blood and guide the diagnosis in regards to an allergy. For
Diagnostic algorithm for evaluation of contact urticaria
Suspected allergen
Open test* application on normal skin
If results are negative
Open test* application to previously affected skin
If results are negative
Positive results at any stage of evaluation warrant discontinuation of further testing
Patch test† on normal skin
If results are negative
Patch test† on previously affected skin
If results are negative
Skin prick testing
3
instance, the radioallergosorbent test (RAST) measures serum-specific IgE, though it has become outdated and is now often replaced with the more sensitive enzymelinked immunosorbent assay (ELISA) tests that do not require radioactivity. In 2010 the United States National Institute of Allergy and Infectious Diseases recommended that the RAST measurements of specific IgE for the diagnosis of allergy be abandoned in favor of testing with more sensitive fluorescence enzymelabeled assays.95
OTHER DIAGNOSTIC TESTING
OTHER DIAGNOSTIC
TESTING
Depending on the potential exposure based on occupational history and clinical examination, other diagnostic modalities may be used to make a definitive diagnosis. Common procedures in nonoccupational settings such as skin scraping with potassium hydroxide (KOH) preparation and skin biopsies can similarly be utilized in the occupational setting. In addition, several other biomonitoring methods may be employed particularly for certain occupational exposures. For example, exposure to arsenic can be detected in the blood, hair, nails, and urine; however, measuring arsenic in the urine provides the most reliable indicator of exposure. In addition, when measuring arsenic in the urine, it is important to request speciation to determine the specific amounts of organic versus inorganic arsenic. Inorganic arsenic, elemental arsenic, and arsine gas are the toxic forms leading to adverse health effects. Organic arsenic (eg, arsenobetaine), on the other hand, is relatively benign and can be found in seafood, which can significantly elevate total arsenic levels up to 72 hours after ingesting a seafood meal. Furthermore, although beryllium sensitization can be detected through patch testing, laboratory testing of the blood is also commonly used in the occupational setting. The beryllium lymphocyte proliferation test (Be-LPT) exposes the separated white blood cells drawn from a venipuncture to a beryllium solution and measures the proliferation of these white blood cells. In one large study of more than 12,000 individuals, the sensitivity and specificity of the Be-LPT were 68.3% and 96.9%, respectively.96 Identifying sensitization to beryllium is paramount because sensitized workers can develop chronic beryllium disease (CBD), a permanent and potentially progressive granulomatous restrictive lung disease. Observational studies suggest that early treatment of clinically apparent CBD is associated with improved pulmonary function, radiographic findings, respiratory symptoms, and functional status.97 When beryllium sensitization is initially suspected, additional testing in conjunction with temporary or permanent work restriction may be recommended.
451
3
MANAGEMENT
Treatment of OSDs is dependent on the initial cause and is practically the same as that for skin diseases of nonoccupational origin. Identifying the specific cause(s) of the patient’s disease and outlining the appropriate steps to avoid exposure and recurrences is an important role to be played by the provider. As most occupational skin disorders are preventable, patients should be educated on the appropriate preventive measures. Employers should work with their employees to mitigate hazards through the hierarchy of controls (Fig. 27-8), with the last resort for prevention being protective clothing and topical barriers, if practical. Ideally, medical providers and occupationally related disciplines including industrial hygiene should work with employers to eliminate or substitute known hazards. However, if elimination or substitution is unrealistic, engineering controls should be considered that protect workers through physically isolating hazardous processes. Other methods to help reduce exposure include administrative controls, which include alterations in work cycles to decrease exposure time to hazards.
RISK FACTORS
RISK FACTORS
Understanding risk factors for OSDs is important for potential prevention of disease. Risk factors may be endogenous and beyond the control of the individual, such as age, gender, race and genetics. Or, risk factors may be exogenous and potentially modifiable, including specific occupations and duties, work practices and environment, experience level of the worker, and protective measures used. In regard to age, reports have indicated that older individuals have reduced reactivity to irritants.98
Hierarchy of controls
Elimination
Substitution
Engineering
Administrative
PPE
452
However, research on age and development of ACD is less clear, with studies showing mixed results.99
Several studies have also shown that occupational ICD is seen more commonly in females. At the same time, many epidemiologic assessments may be biased by chemical exposure patterns and specific genderrelated occupations, which may give a perception that females are more reactive to irritants than males, and this difference is not necessarily supported by direct comparative testing.98 Females may be more predisposed to developing ACD, but again, this is likely related to exposure patterns and not to intrinsic skin characteristics.100 Racial differences in dermatologic response to chemical agents also have been described, with some evidence that Asian skin may be more reactive and black skin less reactive than white skin.101
Increasing research on genetic factors has found genetic susceptibility markers associated with ICD and ACD. For ICD and ACD, alterations in production of pro-inflammatory cytokines interleukin (IL)-1alpha, IL-1beta, IL-8, tumor necrosis factor (TNF-alpha), and anti-inflammatory IL-1 have been associated with increased risk.102 Additionally, mutations in the filaggrin gene have been shown to affect skin barrier functions and contribute to the development of atopic dermatitis and potential susceptibility towards contact dermatitis. Maceration and other skin disease that disrupt the skin barrier can enhance penetration of both irritants and allergens. Atopic dermatitis is known to increase the susceptibility of skin to irritants but not to allergens.102 Consequently, workers with atopic skin disease are more likely to develop OSDs when also exposed to wet work conditions (defined as exposure of skin to liquid for more than 2 hours per day, use of occlusive gloves for more than 2 hours per day, or frequent handwashing).103 And studies of polymorphisms in genes encoding for metabolic enzymes, such as N-acetyltransferases, suggest a role in developing ACD.102
Certain industries and occupations also appear to pose a higher risk of developing occupational dermatoses. Based on the 2010 Occupational Health Supplement of the National Health Interview Survey (NHIS) that sampled 17,524 adults who had worked in the preceding 12 months, the period prevalence of occupational dermatitis was highest in arts, entertainment, and recreation (12.6%) followed by health care and social assistance (12.5%) and accommodation and food services (12.4%) industries after adjusting for age, sex, and race/ethnicity.104 Similarly, occupational categories (defined by the Standard Occupational Classification) identified with the highest prevalence of reported dermatitis included life, physical, and social sciences (18.2%) and art, design, entertainment, sports, and media (15.1%).104 In contrast, the overall prevalence rate among the surveyed current/recent workers for dermatitis was 9.8%. Other exogenous risk factors beyond industry and occupation may include chemical concentration, exposure duration, and use of personal protective equipment (PPE). The use of PPE, including gloves
and clothing, can often limit hazardous exposures; however, if used improperly, it may actually increase permeation and penetration of irritants and allergens. Furthermore, the PPE itself may directly irritate the skin or contain allergens (eg, latex gloves), so correct use of PPE is paramount. Although handwashing is generally encouraged, excessive hygiene measures and use of soaps and detergents can lead to ICD.
HEALTH RISK ASSESSMENT
Although occupational dermatologic hazards exist in many workplaces, the risks to workers are often variable and depend on a multitude of factors. In the occupational environment, this probability is evaluated through a methodical approach known as a health risk assessment. Health risk assessments encompass 4 main components: (1) hazard identification, (2) doseresponse relationship, (3) exposure assessment, and (4) risk characterization.
HAZARD IDENTIFICATION
HAZARD IDENTIFICATION
The initial step to identify workplace hazards should incorporate knowledge from industries involving similar work practices and recognize potential injuries and illnesses that can result from related exposures. Hazardous chemicals, in particular, legally require Safety Data Sheets (SDSs, formerly known as Material Safety Data Sheets [MSDSs]), which display not only chemical properties but also adverse health effects, protective equipment necessary for safe handling, and first aid measures for acute exposure treatment among others.105 Employers must have SDSs readily available to employees for all hazardous chemicals in the workplace.
DOSE-RESPONSE RELATIONSHIP
DOSE-RESPONSE
RELATIONSHIP
The dose-response assessment helps delineate relative threshold concentrations of an exposure that results in adverse health effects. For many OCDs, the adverse effects are often dose-dependent with exposure. However, it is important to recognize health conditions (eg, atopic dermatitis) that can contribute to adverse health effects (eg, ICD) at lower exposure doses.
EXPOSURE ASSESSMENT
EXPOSURE ASSESSMENT
Because not all OCDs are purely from direct dermal exposures, careful assessment should be taken to determine the potential routes of exposure in the particular workplace. The work task duration and frequency should also be noted as adverse health effects
3
can not only be dose-dependent but time-dependent as well. Furthermore, monitoring is often performed since certain toxic substances have legal permissible exposure limits (PELs) enforced by OSHA. One important caveat is that PELs do not necessarily represent safe limits. The National Institute for Occupational Safety and Health (NIOSH) and American Conference of Governmental Industrial Hygienists (ACGIH) provide recommended exposure limits that are based on adverse health effects.
RISK CHARACTERIZATION
RISK CHARACTERIZATION
By analyzing the collected data from hazard identification, dose-response assessments, and exposure evaluations, an overall level of risk can be assigned to the evaluated hazards. Some assessors use a risk matrix incorporating toxicity and probability of exposure to determine risk level, but regardless of the method, a safe margin of error should be in place to buffer a higher risk hazard misclassified in a lower risk category. Ultimately, risk characterization also allows recommendations on control measures, if necessary, which may include substitution of chemicals, changes in ventilation, addition of local exhaust, alterations in work cycles, and donning of PPE.
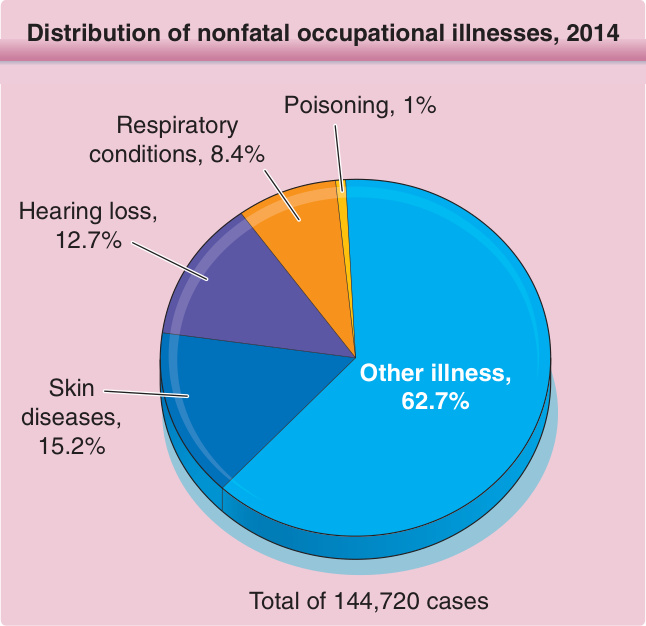
Figure 27-1 Distribution of nonfatal occupational illnesses. Distribution of nonfatal occupational illness cases by category of illness; private industry; 2014. Less than 5% of injury and illness cases reported among the private industry establishments in 2014 were illnesses. More than 60% of illness cases were categorized as “all other illnesses,” which includes such things as repetitive motion cases and other systemic diseases and disorders. (Data from U.S. Bureau of Labor Statistics: 2014 Survey of Occupational Injuries & Illnesses.)
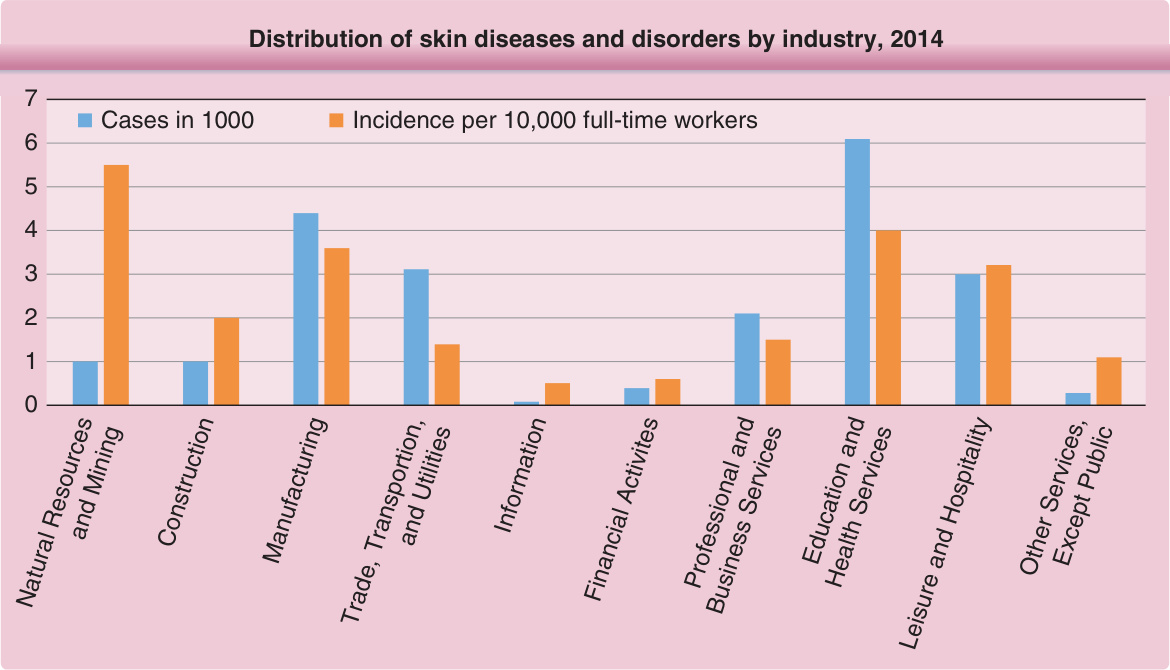
Figure 27-2 Distribution of skin diseases and disorders by industry. Distribution of skin diseases or disorders by private industry; 2014. Natural resources and mining excludes farms with fewer than 11 employees. Data for mining include establishments not governed by the Mine Safety and Health Administration rules and reporting, such as those in Oil and Gas Extraction and related support activities. (Data from U.S. Bureau of Labor Statistics: 2014 Employer-Reported Workplace Injuries & Illnesses.)

Figure 27-3 Acute irritant contact dermatitis on the hand caused by an industrial solvent. There is massive blistering on the palm.

Figure 27-4 Irritant contact dermatitis in a construction worker who works with cement. Note the hyperkeratosis, scaling, and fissuring. There is also minimal postulation. Note that right (dominant working) hand is more severely affected than left hand.

Figure 27-5 Hand dermatitis due to mercaptobenzothiazole in corrosion inhibitors at work and subsequent use of nitrile gloves containing mercaptobenzothiazole.

Figure 27-6 Finger injury from overexposure to an industrial gamma radiation source. (From Sahin C, Cesur C, Sever C, Eren F. Finger injury from over-exposure to an industrial gamma radiation source. Burns. 2015;41:e8-e10, with permission. Copyright © Elsevier.)
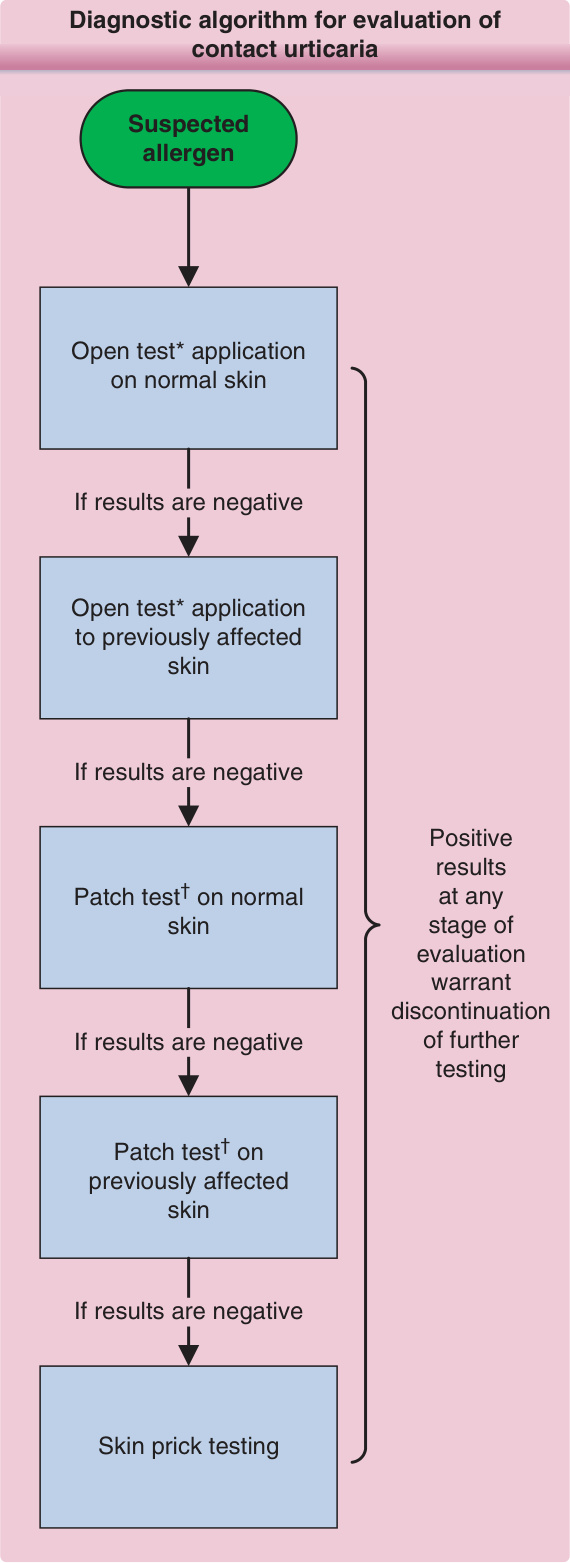
Figure 27-7 Diagnostic algorithm for evaluation of contact urticaria.92,93,94 ∗Open test: application of the substance in a vehicle (petrolatum, ethanol, water) is applied over a 3 × 3-cm area and usually read at 20-, 40-, and 60-min intervals. Immunologic contact urticaria usually presents earlier (15-20 min), whereas nonimmunologic contact urticaria may be delayed (45-60 min) after application. †Patch should be removed after 15-20 min after application and interpreted at similar intervals to the open test.38 Appropriate resuscitation equipment and medications should be readily available when testing for contact urticaria.
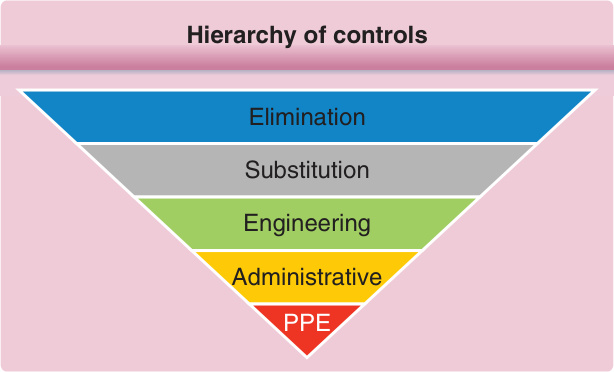
Figure 27-8 Hierarchy of controls. The hierarchy of controls highlights the major categories of mitigating hazards. The most protective to least protective are (1) complete elimination of the hazard, (2) substitution to a nonhazardous or lesser hazardous substance, (3) engineering controls to prevent exposure to the employee, (4) administrative controls to limit the duration of potential exposure, and (5) donning personal protective equipment (PPE).

TABLE 27-1 Common Occupational Skin Diseases
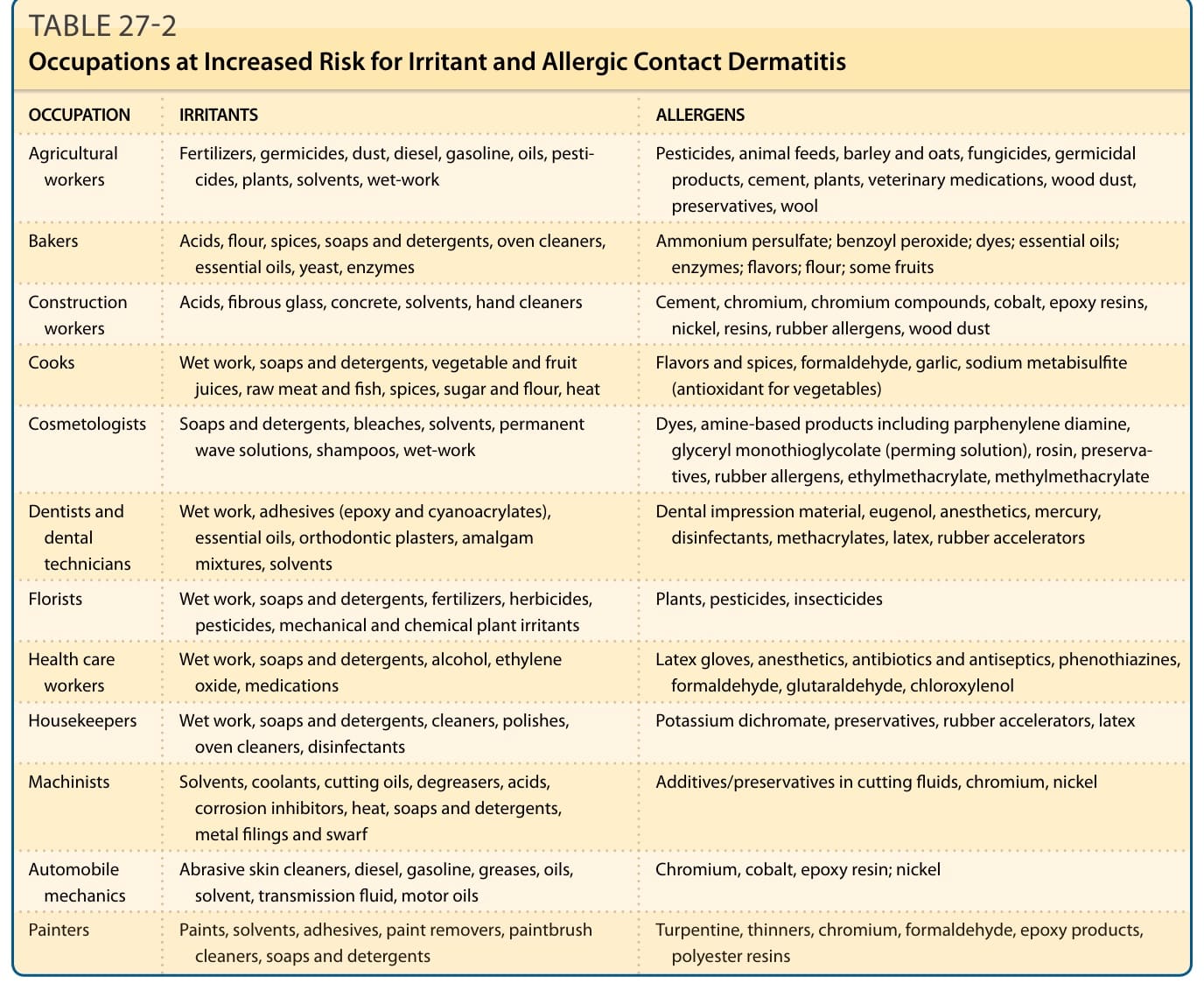
TABLE 27-2 Occupations at Increased Risk for Irritant and Allergic Contact Dermatitis
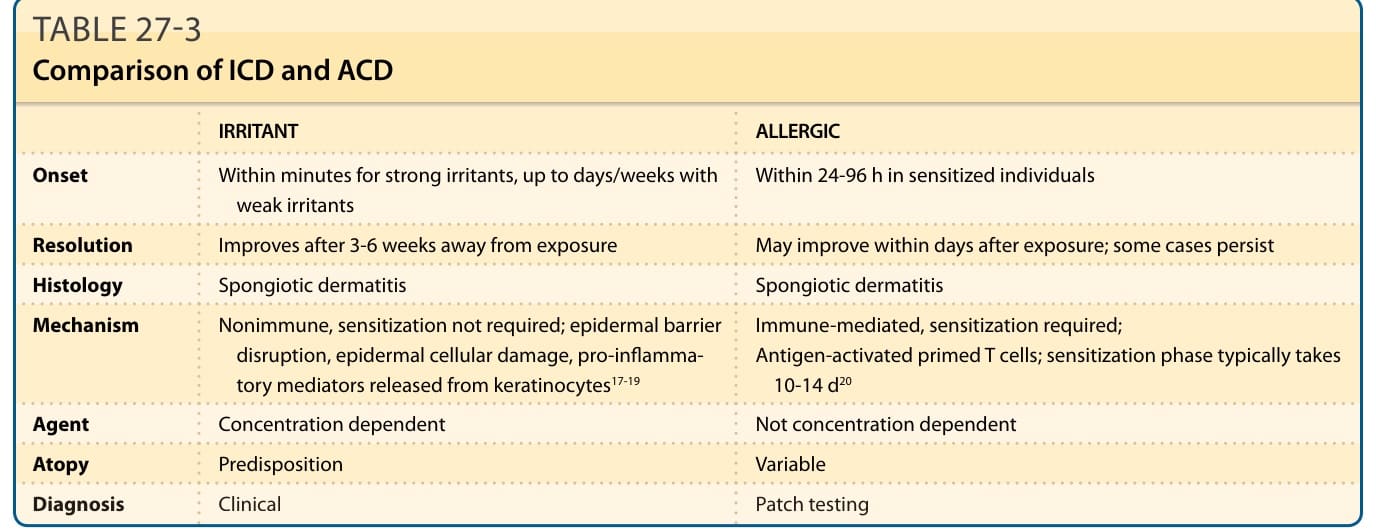
TABLE 27-3 Comparison of ICD and ACD
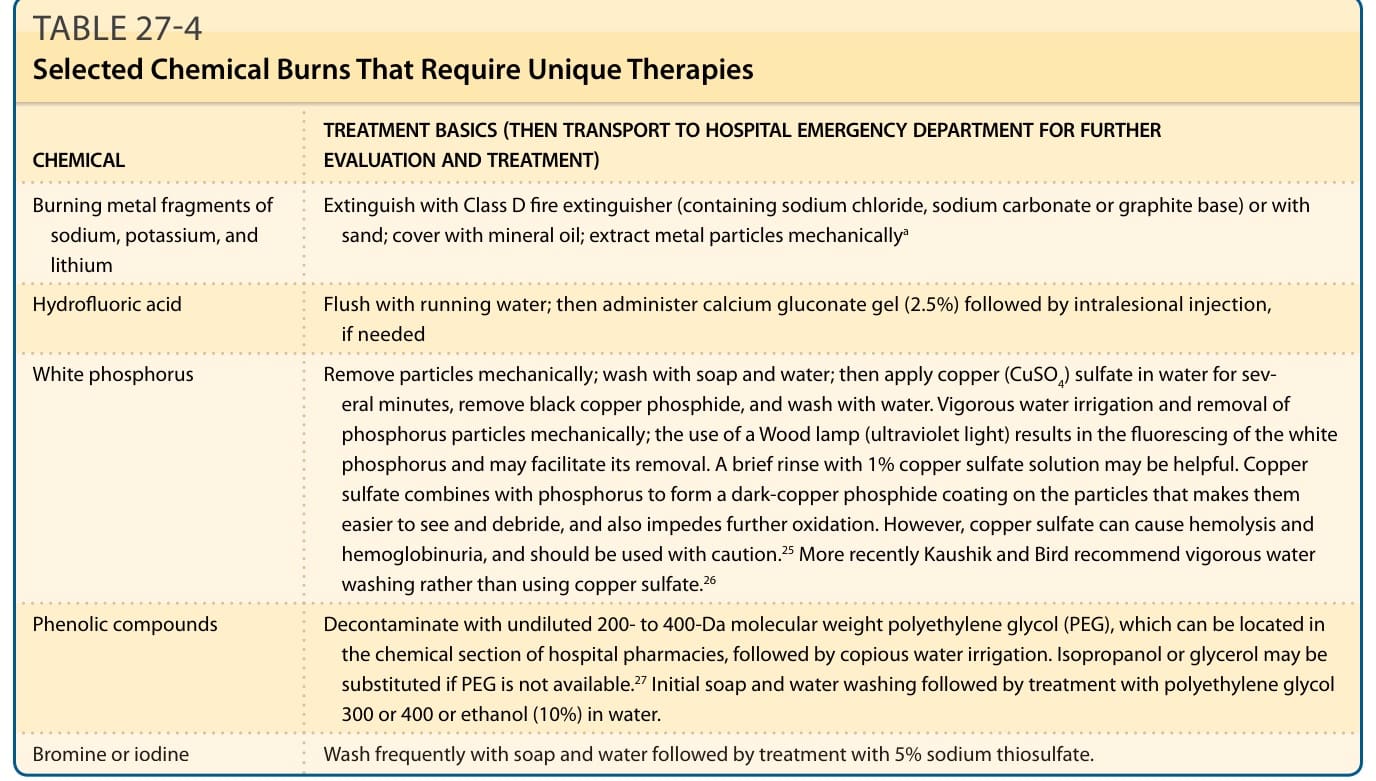
TABLE 27-4 Selected Chemical Burns That Require Unique Therapies
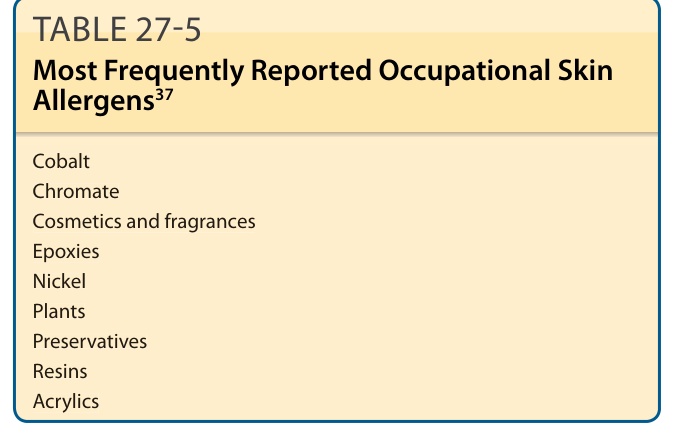
TABLE 27-5 Most Frequently Reported Occupational Skin Allergens37
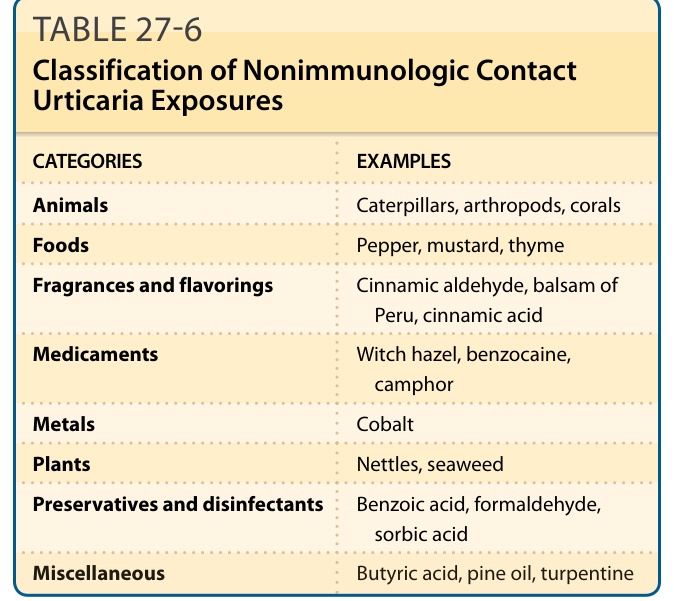
TABLE 27-6 Classification of Nonimmunologic Contact Urticaria Exposures
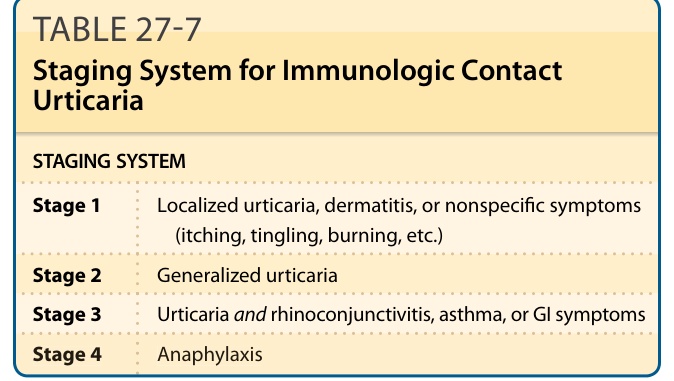
TABLE 27-7 Staging System for Immunologic Contact Urticaria