Seborrheic Dermatitis
3
AT-A-GLANCE
■ Seborrheic dermatitis is a common inflammatory skin disease affecting various age groups.
■ Erythematous, greasy, scaling patches and plaques appear on scalp, face, ears, chest, and intertriginous areas.
■ Severe forms, like generalized erythroderma, rarely occur.
■ Etiology is unclear but may be related to abnormal immune mechanism, Malassezia, sebaceous glands, and individual susceptibility.
■ Treatment is based on symptomatic control.
Seborrheic dermatitis (SD) is clinically characterized by erythematous, scaly patches on sebaceous gland–rich sites, including scalp, face, upper trunk, and intertriginous areas.1 The affected areas present as various appearances from mild pinkish and sometimes greasy scaling to solid adherent crusts. Patients with this condition complain of discomfort, with symptoms of itching and burning, and also have some serious cosmetic problems, leading to psychosocial distress that has a negative impact on their quality of life.2 SD arises in all races and ethnic groups and has a worldwide distribution, but a higher incidence and more-severe forms are observed in AIDS patients and individuals with certain neurologic conditions, such as Parkinson disease.3
CLINICAL FEATURES
GENERAL FEATURES
GENERAL FEATURES
SD usually appears as a chronic and relapsing pattern in adolescents and young adults when the activity of sebaceous glands increases from hormonal effects, with the incidence increasing in patients with older than 50 years of age.4 SD can also affect babies as young as age 2 weeks with peak incidence at 3 months of age, which is called infantile seborrheic dermatitis (ISD; Fig. 26-1). The overall prevalence of SD in general population is between 2.35% and 11.30%, depending on the study.5 A male predominance is observed in all ages without any racial or regional predilection. SD is often influenced by a seasonal impact. It becomes more common and severe in the cold and dry climates, whereas it may be mitigated by sun exposure. However, several cases induced by
treatment of psoralen plus ultraviolet A (PUVA) therapy have been reported.6
The symptoms of SD are mainly chronic, persistent, and recurrent. The red, flaking, and greasy lesions of scalp and face are easily observed, particularly on nasolabial folds (Fig. 26-2); eyebrows, upper eyelid, forehead, postauricular areas (Fig. 26-3); external auditory canal and auricle (Fig. 26-4), with generally symmetrical distribution. SD can appear in other sites, such as occiput and neck. When the sternal area on the chest (Fig. 26-5), upper back (Fig. 26-6), and umbilicus are involved, petaloid or arcuate lesions with fine pink scale can be seen. In contrast, intertriginous areas, including inguinal and axillary regions, show less scale, making SD easily confusable with intertrigo. However, variations of these clinical appearances are common. Scalp involvement is more common in the male patient, in the patient with long disease duration, and in the patient with a history of acne.1 The severity of SD varies from mild erythema and pruritus to severe, oily, thick scale with a burning or tingling sensation. Some patients with SD also may present with Pityrosporum folliculitis and blepharitis. Pityrosporum folliculitis typically manifests as a diffuse papulopustular eruption with peripheral erythema on the trunk and arises more in immunocompromised patients. Seborrheic blepharitis usually appears as a type of anterior blepharitis, inducing flaking and scaling on the eyelids and creating uncomfortable, irritating problems. Characteristically, ISD has a relatively different feature in contrast with SD in older ages. The nonpruritic skin eruption generally affects the frontal or vertex areas (or both areas) of the scalp and the central areas of the face with dry, thick, adherent, and flaking scale, and may be accompanied by erythematous rash on intertriginous folds of the trunk and extremities (Fig. 26-7). The extensive involvement of the scalp, commonly called “cradle cap,” is one of the typical appearances observed in ISD. ISD normally resolves spontaneously within the first 6 to 12 months of life. Extensive and serious conditions should be differentiated from immunosuppressed status.
LEINER DISEASE
LEINER DISEASE
The term Leiner disease was first introduced by Carl Leiner in 1908, to describe infants with desquamative erythroderma, sparse hair, frequent loose stools, and failure to thrive.7 Later, Miller reported other patients with similar clinical features who had generalized SD. Miller also found a lack of opsonization by the serum of the patients.8 Since Miller’s findings it has become
clear that Leiner disease is an umbrella phenotype rather than a single-disease entity, and a variety of immunologic defects have been identified.9 Congenital or acquired deficiencies of C3, C5, and phagocytic activity results in defective opsonization of yeast and bacteria. Association of Leiner disease and Netherton syndrome was also suggested.9 Secondary bacterial infection can bring death to a Leiner disease patient, so appropriate treatment, such as IV hydration, temperature regulation, and antibiotics, is essential. Infusion of fresh-frozen plasma or whole blood can be beneficial in supplementing the deficient factors in a hereditary form of Leiner’s disease.8 The prognosis of Leiner disease depends on the nature of the underlying immunologic abnormality of the patients.
PITYRIASIS AMIANTACEA
PITYRIASIS AMIANTACEA
Asbestos-like scalp, called pityriasis amiantacea, was first described by Alibert in 1832. Pityriasis amiantacea is also called tinea asbestina, tinea amiantacea, keratosis follicularis amiantacea, and porrigo amiantacea. Pityriasis amiantacea is an inflammatory
3
A
B
429
3
condition of the scalp that is characterized by large plates of thick, silvering scale firmly adherent to both the scalp and hair tufts (Fig. 26-8). This can be a localized or diffuse condition, and is attributed to diffuse hyperkeratosis and parakeratosis with follicular keratosis surrounding each hair with a sheath of corneocytes and debris. It is more common in females and it may occur at any age, often without evident causes. Alopecia, which is generally reversible but is sometimes cicatricial, is a common feature of pityriasis amiantacea.10 Concomitant secondary bacterial infection, mostly Staphylococcus aureus, may result in scarring alopecia, so early and appropriate treatment is necessary. The most frequent skin diseases associated with pityriasis amiantacea are psoriasis (35%) and eczematous conditions like SD and atopic dermatitis (34%). Of pediatric patients with pityriasis amiantacea, lesions in 2% to 15% develop into typical psoriasis.11 Pityriasis amiantacea may also manifest as a complication of lichen planus,
430
lichen simplex chronicus, superficial fungal, or pyogenic infection, or as an adverse effect of molecularly targeted therapy such as vemurafenib.12,13 In these cases, therapy should be directed toward the underlying etiology.
3
ASSOCIATIONS OF HIV AND AIDS
ASSOCIATIONS OF HIV
AND AIDS
SD arises in more extensive and refractory patterns in up to 83% of HIV-seropositive and AIDS patients (Fig. 26-9).4 The initial clinical symptom may appear as a butterflylike rash seen in systemic lupus erythematosus. SD is associated with reduction of T-cell function, and gets worse as the CD4+ lymphocyte count decreases, making SD an indicator for evaluating the progression of AIDS.14
ETIOLOGY AND PATHOGENESIS
Many studies to uncover the pathogenesis of SD in adult and adolescent patients have been conducted, but the etiology has not been clearly identified yet.
A
B
431
3
Multifactorial causes, including several endogenous and exogenous predisposing factors, are associated with SD. The role of sebaceous glands in pathogenesis of SD is notable considering time and lesional distribution of SD. The immunologic status of patients or the susceptibility to SD can be an important factor because SD is much more seen in those with certain underlying diseases such as AIDS and Parkinson disease. Malassezia may also be one of the causes of SD as antifungal medications are effective. The relationship of the SD lesions with seasonal fluctuations or sun exposure implies that multiple exogenous factors can contribute to the development of SD.
IMMUNE RESPONSE AND INFLAMMATION
IMMUNE RESPONSE AND
INFLAMMATION
The immune component may be important in the pathogenesis of SD because SD is much more common in immunosuppressed patients. The DBA/2 2C TCR transgenic mouse, which has a defect in expression of CD4+ and CD8+ cells owing to the lack of T-cell progenitor thymocytes, exhibited SD-like eruptions.15
Several studies have focused on the cellular immunity and humoral immunity in SD, but there are some controversies. One study showed a normal CD4+-to- CD8+ ratio, whereas another study demonstrated a decreased CD4+-to-CD8+ ratio in 68% of patients.16 A decrease in the number of B cells in 28% of patients and a rise of the number of natural killer cells in 48% of patients were reported. In addition, 60% of patients showed an increase in CD8+ cells and 70% of patients showed a diminished CD4+-to-CD8+ ratio. Also, it was stated that SD patients had an increased production of immunoglobulin (Ig) A and IgG antibodies in serum.16 However, there was no change in the total amount of antibodies against Malassezia in SD, suggesting that changes to the antibodies are not likely linked with Malassezia.17 The alteration of inflammatory cytokines in patients with SD has been demonstrated by immunohistochemical studies. The production of interleukin (IL)-1α, IL-1β, IL-4, IL-12, tumor necrosis factor-α, and interferon (IFN)-γ was increased in the lesions compared with the normal skin.18 Significantly increased IL-1RA–to–IL-1α and IL-1RA–to–IL-8 ratios, as well as overproduction of histamine, were also shown to occur in SD when compared with healthy controls.19 An investigation of gene expression by DNA microarrays in 15 patients with dandruff showed the reciprocal expression of induced inflammatory genes and repressed lipid metabolism genes compared with nondandruff individuals.20 The expression of induced inflammatory genes was distinctly observed in uninvolved skin of the patients as well, indicating the presence of predisposing factors related to inflammation in patients with SD. Furthermore, inflammation induced by oxidative stress through reactive oxygen species may have a potential role in the pathogenesis of SD.21
432
MICROBIAL EFFECTS
MICROBIAL EFFECTS
Malassezia, normal flora that inhabits human skin, is suggested to be important in SD. This opinion is based on the evidences that the common lesions of SD are related to the distribution of sebaceous glands where Malassezia preferentially colonizes, and that antifungal medications have therapeutic effects on SD. A decline in the number of Malassezia by use of antifungal agents corresponds with the relief of the symptoms.4 Moreover, pityriasis versicolor and Pityrosporum folliculitis, induced by Malassezia, are commonly accompanied by SD. However, there is a lack of difference in Malassezia counts between patients with SD and healthy individuals. In addition, a mycelial form of Malassezia, a pathogenic form observed in pityriasis versicolor, has not been detected in SD.17 These facts propose a complex causative role of Malassezia for SD. The prevalence and types of the most predominant Malassezia species found on SD lesions differ among studies, countries, or parts of body, but Malassezia globosa and Malassezia restricta are considered to be the most important of the 14 Malassezia species identified.4,22 The complete genome sequences of M. globosa and M. restricta have been determined and these genomes encode lipase and phospholipase, making the species lipophilic or lipiddependent.23 The primary role of these enzymes is to metabolize lipid into fatty acids to produce fungal cell walls responsible for virulence, including invasion and dissemination.24 Not all M. globosa or M. restricta strains were found in SD, implying that there may exist specific strains capable of causing the disease.25 Also, an increased amount of Malassezia furfur was observed in patients with SD versus healthy controls.26 The high concentration of M. furfur can disturb protective skin barriers and induce inflammation. Malassezin, generated by M. furfur or M. restricta, can serve as agonists to aryl hydrocarbon receptor, which is involved in the differentiation of T-helper 17 cells and the mediation of contact sensitivity.27
LIPID AND HOST SUSCEPTIBILITY FACTORS
LIPID AND HOST
SUSCEPTIBILITY FACTORS
Several analyses of skin surface lipids in patients with SD or dandruff have shown alterations in those irrespective of HIV status.28 These findings were not consistent with one another, but they introduced the causative relationship between SD and the composition of skin surface lipids. Specifically, irritating free fatty acids, such as oleic acid produced by lipase of M. globosa, could mediate dandruff-like flaking in the dandruff-susceptible individuals with SD but not in nonsusceptible individuals.29 Individual susceptibility is considered to be associated with a disrupted epidermal barrier that allows penetration of the irritating metabolites. The process for Malassezia to reach the aryl hydrocarbon receptor in the granular and spinous
layers also may depend on such defective skin character. This host susceptibility factor could explain the lack of a positive correlation between the number of Malassezia and the severity of dandruff.
EPIDERMAL HYPERPROLIFERATION
EPIDERMAL
HYPERPROLIFERATION
Increased epidermal turnover in SD, which is also shown in psoriasis, implicates SD in a disorder of hyperproliferation, and Malassezia can be considered as one of the incidental outcomes derived from the phenomenon. SD resembles psoriasis in many aspects, both clinically and histologically, and it is sometimes difficult to differentiate the two diseases even after a skin biopsy. There are case reports that keratolytics and antiinflammatory medications were successful in the treatment of the patients with SD whose treatment with amphotericin B had failed.30 This alteration of epidermis may be related with the increased activity of calmodulin and explains the basis of use of cytostatic medications such as azelaic acid.31
NEUROTRANSMITTER ABNORMALITIES
NEUROTRANSMITTER
ABNORMALITIES
SD expressed in Parkinson disease has been thought to result from the elevated levels of sebum allowing the proliferation of Malassezia. Bilateral seborrhea observed in unilateral parkinsonism suggests the changes of sebum levels are presumably triggered by endocrine effects rather than neurotrophic effects. It may be associated with an increased circulating α-melanocyte–stimulating hormone in Parkinson disease.32 Because the severity of SD in Parkinson disease does not correlate with the sebum excretion rate, the sebum accumulation by facial immobility may play a key role. Administration of levodopa can clinically improve the skin symptoms by reducing the sebum production or secretion by restoring the production of melanocyte-stimulating hormone-inhibiting factor. The prevalence of SD is also increased in patients with other neurologic disorders, including mood disorder, Alzheimer disease, syringomyelia, epilepsy, cerebrovascular infarcts, postencephalitis, mental retardation, poliomyelitis, quadriplegia, trigeminal nerve injury, and alcoholism. Indoor lifestyle with less sunlight exposure and hygiene status of the patients may function in this association.4
OTHER FACTORS
OTHER FACTORS
Low humidity and cold temperatures worsen SD, especially in the winter and early spring. Facial trauma (eg, scratching) and PUVA therapy also are aggravating
3
factors.6 Multiple drugs can lead to SD-like eruptions, including griseofulvin, cimetidine, lithium, methyldopa, arsenic, gold, auranofin, aurothioglucose, buspirone, chlorpromazine, ethionamide, haloperidol, IFN-α, phenothiazines, stanozolol, thiothixene, psoralen, methoxsalen, and trioxsalen. The SD-like dermatitis also appears in patients with zinc deficiency (acrodermatitis enteropathica and acrodermatitis enteropathica–like conditions) or biotin deficiency, but the skin eruptions do not respond to zinc or biotin supplementation.33 It is noted that the familial form of SD was reported in an Israeli Jewish family of Moroccan descent, which was caused by autosomal dominant genetic mutation (ZNF750) encoding a zinc finger protein (C2H2).34
DIAGNOSIS
The diagnosis of SD remains a clinical one, based on SD’s characteristic morphology and patterns. Dermoscopy enables the detailed identification of morphologic structures, which is especially helpful in diagnosing SD of the scalp. The typical magnified vascular patterns observed by dermoscopy are twisted loop, red dots and globules, and glomerular vessels in scalp psoriasis, but arborizing vessels and atypical red vessels in SD.35 A skin biopsy is not routinely required, but may be useful when the diagnosis is unclear. The various histopathologic features can be observed depending on the different stages of the disease: acute, subacute, and chronic. Acute and subacute SD may exhibit slight to moderate spongiotic dermatitis with mild psoriasiform hyperplasia, folliculocentric crust containing scattered neutrophils at the tips of the follicular opening, orthokeratosis with focal parakeratosis, and superficial perivascular lymphohistiocytic infiltration. Chronic SD shows a more intense pattern of the foregoing features with minimal spongiosis and markedly dilated superficial vessels. However, the histopathologic picture in chronic cases is sometimes similar to those of psoriasis, and careful attention should be paid to the histopathology reading. HIV-associated SD is histologically distinctive from the ordinary SD, showing very severe patterns such as extensive parakeratosis, leukoexocytosis, necrosis of keratinocytes, and superficial perivascular infiltrate of plasma cells (Table 26-1).36 Lesion scraping for a potassium hydroxide preparation can be beneficial to confirm the diagnosis of accompanied Pityrosporum folliculitis. It should be kept in mind that SD can simultaneously occur with other dermatoses. When SD occurs in infants, the classic diagnostic criteria suggested by Beare and Rook can be used in diagnosing ISD. It is composed of early onset (before 6 months of age); erythematous and scaling rash distributed in the scalp, diaper, or flexural areas; and the relative absence of pruritus.37
Involvement of the diaper area alone is considered as a characteristic sign favoring a psoriasiform type of ISD. Above all, the clinician should remember that there is not a characteristic pathognomonic feature or laboratory test to establish the accurate diagnosis of SD.
433
3
CLASSIC SEBORRHEIC DERMATITIS AIDS-ASSOCIATED SEBORRHEIC DERMATITIS
Epidermis
Limited parakeratosis Rare necrotic keratinocytes No interface obliteration Prominent spongiosis
Widespread parakeratosis Many necrotic keratinocytes Focal interface obliteration with clusters of lymphocytes Sparse spongiosis
Dermis
Thin-walled vessels Rare plasma cells No leukocytoclasis
Many thick-walled vessels Increased plasma cells Focal leukocytoclasis
Thin-walled vessels Rare plasma cells No leukocytoclasis
Many thick-walled vessels Increased plasma cells Focal leukocytoclasis
From Soeprono FF, Schinella RA, Cockerell CJ, Comite SL. Seborrheic-like dermatitis of acquired immunodeficiency syndrome. A clinicopathologic study. J Am Acad Dermatol. 1986;14(2):242-248, with permission.
DIFFERENTIAL DIAGNOSIS
Several diseases should be considered in the differential diagnosis of SD (Tables 26-2 and 26-3), especially as ISD is easily confused with atopic dermatitis, psoriasis, histiocytosis, and scabies; sometimes it is impossible to distinguish among these diseases in infants younger than 3 months of age. Checking family history and pruritus and taking certain laboratory tests including serum IgE levels and multiple allergen stimulation tests may give a clue to whether it is atopic dermatitis or ISD. When the skin eruption arises solely on the scalp, an involvement of frontal hair lines is a distinctive feature for scalp psoriasis.38 Langerhans cell histiocytosis, previously called Letterer-Siwe disease has more generally purpuric lesions and tends to desquamate on the scalp and ulcerate on the folds and the mucosal areas. Severe itching that includes the palms and soles suggests scabies. Intertrigo, contact dermatitis, neonatal erythroderma, and multiple carboxylase deficiency should also be excluded in infants.39
CLINICAL COURSE AND PROGNOSIS
Generally SD in adolescents or adults has a chronic and recurrent relapsing course. Consequently, the primary goal of treatment should be control of symptoms like pruritus, erythema, and scales, rather than cure of disease. Also, patients should be informed that they need to prepare for a future re-outbreak and avoid aggravating factors of SD. However, ISD has a benign, selflimited course; ISD spontaneously disappears by 6 to 12 months of age. Severe exacerbation with exfoliating dermatitis may occur, albeit rarely, but its prognosis is usually favorable. ISD does not progress to adulthood.
434
Scalpa Psoriasis, atopic dermatitis, impetigo, tinea capitisa (mimics dandruff in children)
Face Psoriasis, rosacea, contact dermatitis, impetigo, discoid lupus, sarcoid (petaloid type in African Americans), drug-induced photosensitivity
Ear canal Psoriasis, contact dermatitis
Eyelids Atopic dermatitis, psoriasis, Demodex folliculorum infestation
Chest, back Pityriasis rosea, tinea versicolor, subacute cutaneous lupus, psoriasis vulgaris
Groin, buttock Intertrigo (fungal, Candida, erythrasma), glucagonoma, extramammary Paget disease, zinc deficiency
Intertriginous Inverse psoriasis, candidiasis, erythrasma, contact dermatitis, tinea intertrigo, Langerhans cell histiocytosis (Letterer-Siwe disease in infants)
Generalizedb Scabies, secondary syphilis, pemphigus foliaceus, pemphigus erythematosus, Leiner disease (infants), drug eruption
Erythrodermicc Psoriasis, contact dermatitis, pityriasis rubra pilaris, drug eruption, mycosis fungoides (Sézary syndrome), lichen planus, chronic actinic dermatitis, HIV, Hodgkin disease, paraneoplastic syndrome, leukemia cutis
Erythrodermicc Psoriasis, contact dermatitis, pityriasis rubra
pilaris, drug eruption, mycosis fungoides (Sézary syndrome), lichen planus, chronic actinic dermatitis, HIV, Hodgkin disease, paraneoplastic syndrome, leukemia cutis
aDiffuse scalp dermatitis or inflammatory alopecia in children warrants fungal culture, potassium hydroxide preparation.
bWidespread truncal types warrant scabies prep and rapid plasma reagin to rule out syphilis.
cErythrodermic type should be biopsied.
MANAGEMENT
Basically, using emollients (eg, mineral oil, vegetable oil, or petroleum jelly) can help improve symptoms such as scales. Soft rubbing with a brush or comb aids removing thick, adherent scales, but aggressive scraping should be avoided because it can induce further inflammation. The main recommendations for the firstline treatment of SD are topical medications, including corticosteroids, calcineurin inhibitors, antifungal drugs, and keratolytics. In the case of topical corticosteroids, mild-potency formulations are recommended to be used first because of their cutaneous adverse effects and frequent rebound phenomena. Treatment with corticosteroids is highly effective for reducing erythema, scaling, and pruritus rapidly, resulting in total clearance more often than placebo.40 Topical calcineurin inhibitors (tacrolimus and pimecrolimus) manifest good effects on SD by blocking calcineurin, thus preventing both inflammatory cytokines and a signaling pathway in T-lymphocyte cells. No difference between topical calcineurin inhibitors and topical corticosteroids in total clearance was identified in short-term trials.40 There is no risk of telangiectasia and skin atrophy, so topical calcineurin inhibitors are recommended
3
INFANTILE SEBORRHEIC DERMATITIS “NAPKIN” PSORIASIS ATOPIC DERMATITIS LETTERER-SIWE DISEASE
Occurs in the first few weeks to 3 months Onset at 3 months Onset within first 2 months of life, most within the first year Occurs in newborns; other types of Langerhans cell histiocytosis (LCH) may occur between 1 and 3 years of age
Self-limited, regresses spontaneously Self-limited Severity decreases with age Fatal if untreated; other variants of LCH have differing prognoses
Vertex scalp most commonly affected Diaper commonly affected; scalp and face may be affected Face primarily involved Trunk and scalp involved
Adherent, yellow-brown, greasy scale Macerated, shiny erythema on diaper region Intensely pruritic, erythematous papules with excoriation, vesicles and serous exudate; skin appears dry
Face, neck, trunk, and extremities
Similarly extensive involvement,
Face, neck, trunk, and extremities may be affected with intertriginous sites affected (axillae, groin); isolated diaper lesions more suggestive of seborrheic dermatitis
Similarly extensive involvement, but less scaling on intertriginous sites; diaper region primarily affected
may be affected with intertriginous sites affected (axillae, groin); isolated diaper lesions more suggestive of seborrheic dermatitis
but less scaling on intertriginous sites; diaper region primarily affected
for application to the susceptible regions instead of topical corticosteroids. There are no studies comparing the efficacy of tacrolimus with pimecrolimus in SD. Maintenance therapy with topical calcineurin inhibitors may be useful in preventing the relapse or exacerbation, but their long-term safety has not been verified. Based on the presumed etiologic roles of Malassezia, ketoconazole has been the most heavily investigated topical agent for SD. Several randomized studies have demonstrated that 1% to 2% ketoconazole significantly lowers and improves the severity of SD versus placebo, achieving an equal remission rate with corticosteroids, with nearly 44% fewer adverse events.41 The use of 1% ciclopirox also improved skin symptoms. In single studies for evaluating the short-term efficacy of clotrimazole and miconazole, those had almost equivalent impacts on SD compared with corticosteroids.41
Other topical antifungal agents, such as bifonazole, terbinafine, fluconazole, and zinc pyrithione, are also likely to be useful.4 Dandruff or pityriasis simplex capillitii may be treated by shampoos containing zinc pyrithione, selenium sulfide, ketoconazole, salicylic acid, ciclopirox, and coal tar. Lithium seems to have an antiinflammatory role inhibiting the release of arachidonic acid and restricting availability of free fatty acids essential for the growth of Malassezia.42 Topical lithium has shown good results in total clearance both in HIVnegative patients and in AIDS-associated SD. Topical sulfur, propylene glycol, metronidazole, and benzoyl peroxide wash have also been used. Seborrheic blepharitis should be managed by long-term eyelid hygiene with warm compresses, followed by proper topical antibiotics and topical corticosteroid to reduce the bacterial load and marked inflammation, respectively.43
Aluminum acetate solution can be used to decrease
Slightly raised, rose-yellow papules on trunk that may crust and ulcerate
Forearms and shins (extensors)
Extensive involvement with moist
Forearms and shins (extensors) often affected, axillae are spared; diaper area usually spared
Extensive involvement with moist erythematous plaques and petechial lesions on intertriginous areas; scalp involvement similar to seborrheic dermatitis
often affected, axillae are spared; diaper area usually spared
erythematous plaques and petechial lesions on intertriginous areas; scalp involvement similar to seborrheic dermatitis
the symptoms of seborrheic otitis externa. In cases refractory to topical treatment, systemic therapies can be prescribed for uncontrolled multiple widespread lesions and severe cases. Low doses of systemic glucocorticoids may be used for a short period. Patients should know that SD can be controlled but not eradicated. SD patients treated by glucocorticoids should be informed of the side effects and rebound flares that occur after discontinuation of glucocorticoids. Oral antifungals may be tried for severe and refractory cases. Itraconazole, fluconazole, and pramiconazole have been used with various regimens.44 For example, itraconazole 200 mg/day for the first 7 days of the month for several months is a regimen used to get clinical improvement. The daily administration of isotretinoin 0.1 to 0.5 mg/kg also may be effective in severe cases. The basic principle of treatment is the same for infants. When ISD involves the diaper areas, the use of superabsorbent disposable diapers with frequent changes prevents the aggravation of the symptoms.45
Soap and alcohol-containing compounds are not recommended in cleaning the diaper lesions. Topical medications having antifungal and antiinflammatory activities are effective choices that have a high clinical cure rate. A mild-potency steroid, such as 1% hydrocortisone, is preferred but used with caution because of its adverse effects. In more refractory cases, a midpotency topical steroid, such as 0.1% betamethasone valerate, may be required but usable only for a short time. Keratolytic agents, including salicylic acid and selenium sulfide are dangerous to neonates because of the possibility of its percutaneous absorption. Lotion containing 0.025% licochalcone, an extract from Glycyrrhiza inflata, was shown to have a similar
435
3
effect compared to 1% hydrocortisone.46 If secondary infection with fungi or bacteria is accompanied, appropriate systemic drugs should be prescribed. Dietary controls and vitamin supplementation are not beneficial in ISD. Many researchers have proposed various alternative methods to treat SD as well, in preparation for the antifungal resistance and the adverse effects of existing therapies. Homogeneous mixture of biodegradable elements, such as urea, propylene glycol, and lactic acid, was shown to be highly effective in treatment of SD of the scalp.47 Tea tree oil, derived from nature, was found to be of benefit in improving severity, pruritus, and greasiness in a randomized single-blind study. The antifungal property of tee tree oil, mostly to M. furfur, was established in an in vitro study.48 Narrowband ultraviolet B phototherapy was confirmed as an additional choice and to be both safe and effective in an open-label prospective study. Its role in SD may be associated with its immunomodulatory and antiinflammatory function.49
ACKNOWLEDGMENTS
The author acknowledges the contributions of Chris D. Collins, MD, FAAD, and Chad Hivnor, MD, the former authors of this chapter, and thanks Jungyoon Moon, MD, for his devoted assistance.
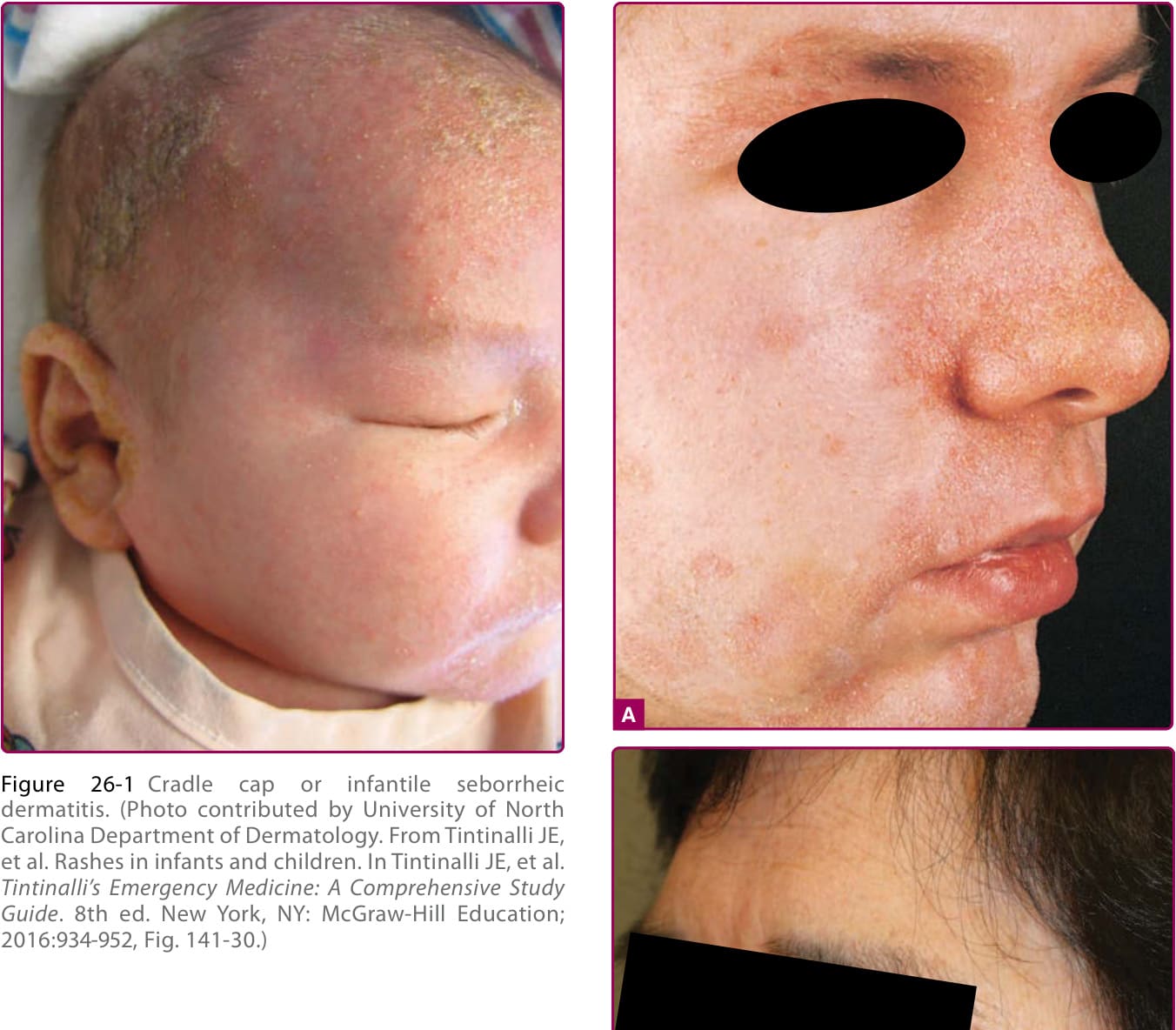
Figure 26-1 Cradle cap or infantile seborrheic dermatitis. (Photo contributed by University of North Carolina Department of Dermatology. From Tintinalli JE, et al. Rashes in infants and children. In Tintinalli JE, et al. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide. 8th ed. New York, NY: McGraw-Hill Education; 2016:934-952, Fig. 141-30.)

Figure 26-2 Seborrheic dermatitis with involvement of (A) nasolabial folds, cheeks, eyebrows, and nose in white person and (B) nasolabial folds in a person of Asian descent.

Figure 26-3 Seborrheic dermatitis of the postauricular area.

Figure 26-4 Seborrheic dermatitis of the ear: external canal, concha bowl, and auricle.

Figure 26-5 Seborrheic dermatitis of the chest.

Figure 26-6 Seborrheic dermatitis of the upper back.

Figure 26-7 Seborrheic dermatitis in an infant. Widespread pattern of seborrheic dermatitis with psoriasiform lesions on the trunk and groin.

Figure 26-8 Pityriasis amiantacea. Masses of sticky silvery scales adhere to the scalp and cause matting of hairs they surround.

Figure 26-9 Wide spread unusual distribution pattern of seborrheic dermatitis in a patient with AIDS. A, Moist patches on the centrofacial region, beard, and scalp. B, Moist lesions on the chest. In patients with AIDS, seborrheic dermatitis responds poorly to conventional therapy.
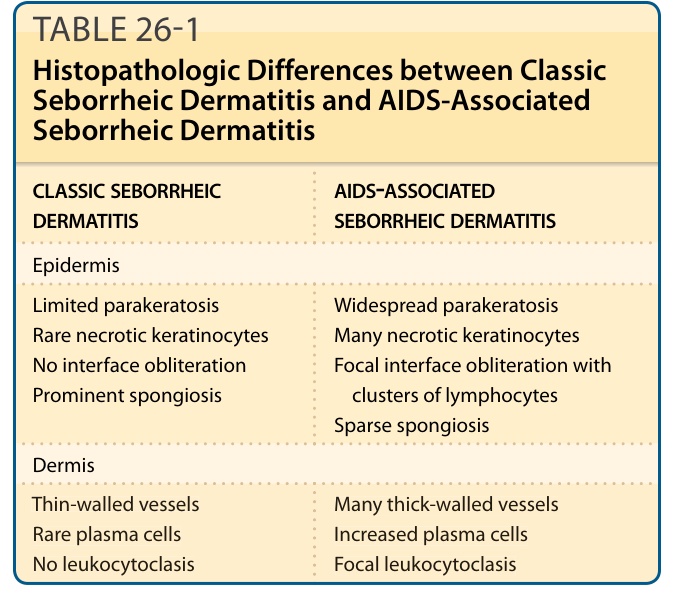
TABLE 26-1 Histopathologic Differences between Classic Seborrheic Dermatitis and AIDS-Associated Seborrheic Dermatitis
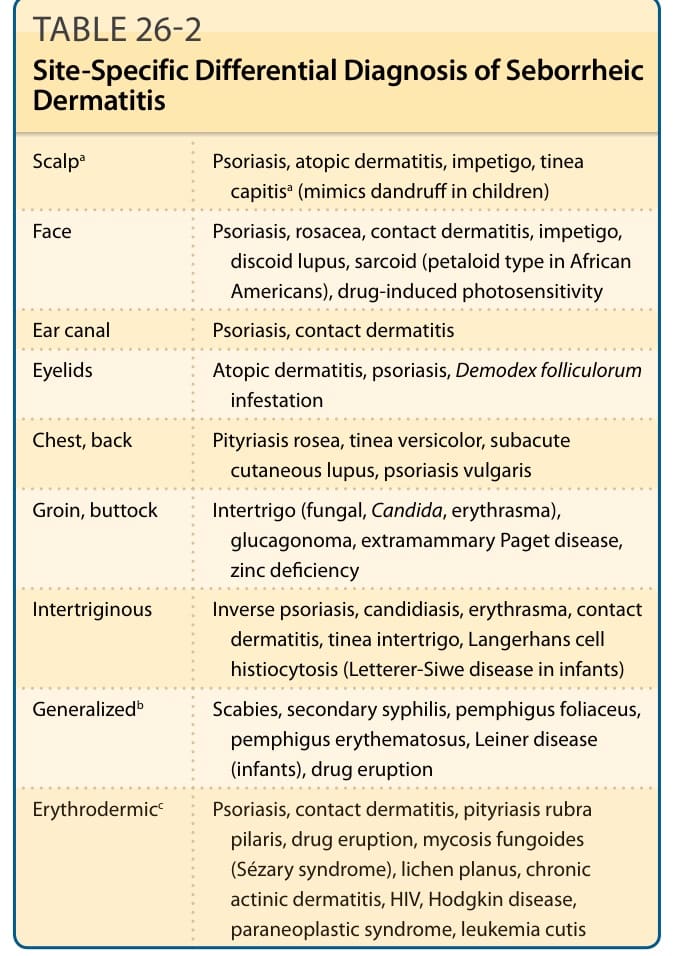
TABLE 26-2 Site-Specific Differential Diagnosis of Seborrheic Dermatitis

TABLE 26-3 Comparison of Infantile Seborrheic Dermatitis with Differential Diagnoses