Irritant Dermatitis
3
AT-A-GLANCE
■ Irritant dermatitis from wet-to-dry cycling is common in cold seasons.
■ Decreasing the duration and frequency of contact with irritants may improve symptoms of irritant contact dermatitis (as opposed to allergic contact dermatitis which requires complete avoidance to clear).
■ Innate immune signals from irritant dermatitis predispose to allergic dermatitis (allergic contact and atopic dermatitis).
■ Emollients accelerate recovery and may help prevent the complication of allergic dermatitis in infants.
■ Emollients used on normal skin over long intervals may predispose to irritant dermatitis.
■ Hardening, or disappearance of symptoms, often occurs with continued irritant exposure without any treatment.
■ Future understanding of ways to promote hardening could reduce the impact of allergic contact dermatitis and atopic disease which complicate irritant dermatitis.
INTRODUCTION
Irritant contact dermatitis is sometimes encountered as a primary diagnosis, but it is most important for its critical role in predisposing to atopic and allergic contact dermatitis. When acute irritant dermatitis is the sole diagnosis, patients are often able to self-diagnose. There is obvious temporal relationship because irritant dermatitis manifests within hours of the causative exposure, and resolves within days of cessation of exposure. In contrast, allergic contact dermatitis may manifest days after exposure and persist for weeks. Consequently, accurate self-diagnosis of contact dermatitis is more common with irritant contact dermatitis than allergic contact dermatitis. The combination of straightforward selfdiagnosis and shorter duration makes the presentation of irritant dermatitis for dermatologic consultation less common than that of allergic contact dermatitis. T cells produce the inflammation of atopic and allergic contact dermatitis as part of the adaptive immune response. The adaptive response is influenced by upstream innate immune response. Irritant dermatitis provides the innate immune signals that predispose to allergic contact and atopic dermatitis. Therefore, the importance of irritant contact dermatitis is less
recognition and treatment as a primary diagnosis, but its role in downstream dermatitis mediated by the adaptive immune response. Study of barrier disruption and the resulting innate immune signals should help us develop strategies to prevent irritant dermatitis so as to prevent more severe and disabling allergic and atopic dermatitis.
DEFINITIONS
DEFINITIONS
Dermatitis is an inflammatory disruption of the epidermis related to physical or immunologic provocation. Dermatitis and eczema are often used interchangeably.1 Dermatitis appears as spongiosis histologically. There is impairment of the barrier functions of the skin, which results in increased transepidermal water loss. As Fig. 25-1 illustrates, dermatitis is usually multifactorial. Irritant dermatitis results in barrier disruption which may predispose to higher concentrations of bacteria and yeast, and these microorganisms may stimulate immune response.2-4 Immune signals from barrier disruption also predispose to allergic contact dermatitis to chemical antigens,5 as discussed later in “Complications.” Irritant dermatitis begins with damage to keratinocytes, which then release danger signals that promote recruitment of inflammatory cells. In severe cases, necrotic keratinocytes are evident. Irritant dermatitis is caused by physical damage to the epidermis and is temporally more immediate after provocation than the delayed hypersensitivity response leading to allergic contact dermatitis. Many variables influence expression of irritant dermatitis including climate and season, occlusion, frequency of exposure to the irritant, and concentration of the irritant. Dermal injury producing scarring can result from corrosive chemicals that coagulate protein and cause cutaneous scars. Corrosive chemicals are not further discussed in this chapter. Irritant chemicals by definition do not cause scarring when in contact with the skin for less than 4 hours.6 Rarely, scarring can result from secondary infection of dermatitis, but not from uncomplicated dermatitis. Hand dermatitis is a common site for irritant contact dermatitis. Repeated wetting and drying of the skin causes fissuring, especially if drying is rapid because of low ambient humidity. Contact with an allergen often results in allergic contact hand dermatitis complicating irritant contact dermatitis. Consequently, the definition of pure irritant contact dermatitis is one of exclusion. Irritant hand dermatitis has been defined as “A documented exposure of the hands to an irritant, which is quantitatively
3
Dermatitis becomes increasingly multifactorial with chronicity
Rapid repeated exposure to detergent and water
Vulvodynia with positive patch tests to candida2
Occupational hand dermatitis to rubber gloves used for wet work
Allergic dermatitis to poison ivy or epoxy resin Head/neck dermatitis caused by Malassezia3
Irritant dermatitis
Allergy to bacteria/yeast Allergy to chemicals
Childhood-onset dermatitis with food and staphylococcal hypersensitivity4
likely to cause contact dermatitis. No relevant contact allergy (no current exposure to allergens to which the patient has reacted positive in patch test).”7
HISTORICAL PERSPECTIVE
HISTORICAL PERSPECTIVE
In the past, homemakers did more wet work, such as washing dishes by hand, and were often diagnosed with “dishpan hands.” Today, irritant dermatitis in its pure form is commonly described as “chapping” or rough, cracked, sore skin. Compared to prior decades, this more commonly occurs from frequent hand hygiene as required for health care workers, or from exposure to wind and cold during outdoor sports and exercise. Patient history is very helpful when distinguishing acute irritant dermatitis from acute allergic contact dermatitis. When chronic, irritant and allergic contact dermatitis cannot reliably be differentiated clinically or histologically. A detailed clinical history and often patch testing are required to diagnosis allergic contact dermatitis (Table 25-1). The classification of hand dermatitis as purely irritant may depend on the absence of relevant positive
patch tests to indicate allergic contact dermatitis. The percentage of cases identified as irritant varies between clinics as the number of patch tests used varies. Many cases are classified as irritant hand dermatitis with allergic or atopic hand dermatitis.7
The lack of a diagnostic test for irritant dermatitis makes it very difficult to comment on prevalence over time.8 Irritant contact dermatitis in its pure form is probably a less-common reason for presentation to a dermatologist now than in the past. This may be because of decreased prevalence resulting from technology reducing the amount of wet work required for homemaking, or improved patient access to medical information, and/or improved formulations of products such as emollients and diapers.
EPIDEMIOLOGY
CLIMATE
CLIMATE
Climate influences the rapidity of wet-to-dry cycles. In low ambient humidity, water evaporates rapidly causing uneven surface change, whereas slow drying in
415
3
IRRITANT CONTACT DERMATITIS ALLERGIC CONTACT DERMATITIS
Acute Sharp, strictly confined to the site of exposure Spreading from site of exposure to the periphery; usually tiny papules; may become generalized
Margination and site
Chronic Ill-defined Ill-defined, spreads
Evolution Acute Rapid (few hours after exposure) Not so rapid (12-72 hours after exposure)
Causative agents
Dependent on concentration of agent and state of skin barrier; occurs only above threshold level
Relatively independent of amount applied, usually very low concentrations sufficient, but depends on degree of sensitization
Incidence May occur in practically everyone Occurs only in the sensitized
Incidence
May occur in practically everyone Occurs only in the sensitized
From Wolff K, Johnson R, Saavedra AP, Roh EK. Fitzpatrick’s Color Atlas and Synopsis of Clinical Dermatology, 8th ed. New York, NY: McGraw-Hill; 2017, Table 2-3, p. 29, with permission.
higher humidity conditions results in a smoother surface. Irritant contact dermatitis can occur from cumulative irritancy from wet-to-dry cycles with or without exposure to irritant chemicals, including detergents and solvents. Wet-to-dry cycles are a common cause of irritant dermatitis in the setting of genetic predisposition to impaired barrier, as in atopic dermatitis where perioral chapping occurs in infants from drooling. Occupational hand dermatitis in the setting of wet work is more common in cold seasons when humidity indoors is low.9
GENDER
GENDER
Women are more likely than men to have hand dermatitis, presumably because of greater wet work exposure. Occupational hand dermatitis is often multifactorial, with both an irritant and an allergic contact component, for example, in hairdressers and machinists.10 Women reported more itching compared to men in one large study where the severity of hand dermatitis was similar in men and women.11
Frequency of hand washing is a risk factor for irritant hand dermatitis. Women are more likely than men to perform higher-risk wet tasks such as hairdressing, and are more likely to wash their hands frequently when away from work.11 Irritant hand dermatitis increased coincident with campaigns to improve hand hygiene in health care workers to decrease hospitalacquired infections.12
ATOPIC DERMATITIS
ATOPIC DERMATITIS
Some people with atopic dermatitis have a genetic barrier defect. In some racial cohorts, this is caused by a mutation leading to defective filaggrin, which weakens the protein milieu that binds corneocytes together in the stratum corneum and decreases natural moisturizing factor.13 In a study comparing patients with atopic dermatitis to healthy controls, the atopic dermatitis patients
416
had greater reactivity to the irritant detergent sodium lauryl sulfate,14 and in a prospective study of workers evaluated for irritant contact dermatitis, atopic patients were more likely to discontinue work.15
In contrast, in a population of health care workers with no history of dermatitis severe enough to warrant physician evaluation, a history of childhood flexural dermatitis did not predispose to lower the irritancy threshold to various concentrations of sodium lauryl sulfate, although irritant response to sodium lauryl sulfate did correlate with development of wintertime irritant hand dermatitis.16 The latter observation suggests that there are individual risk factors for irritant hand dermatitis in addition to atopic dermatitis in a population of healthy hospital workers.
SPECIFIC EXPOSURES
SPECIFIC EXPOSURES
OCCUPATIONAL EXPOSURES
In the setting of dermatologic consultation for occupational hand dermatitis, allergic contact dermatitis may be more commonly diagnosed than irritant contact dermatitis.17 Irritant contact dermatitis is more commonly diagnosed than allergic contact dermatitis10 in studies where larger numbers of workers are assessed. The greater prevalence of irritant dermatitis in the working population compared to the dermatologic consultation cohort may reflect the relative ease of self-diagnosing irritant contact dermatitis, and its comparative lesser severity compared to allergic contact dermatitis, such that many workers do not seek medical consultative care for irritant contact dermatitis.
CONDITION IRRITANT
3
Agriculture workers Artificial fertilizers, disinfectants, pesticides, cleaners, gasoline, diesel oil, plants, and grains
Artists Solvents, clay, plaster
Automobile and aircraft industry workers Solvents, cutting oils, paints, hand cleansers
Bakers and confectioners Flour, detergents
Bartenders Detergents, wet work
Bookbinders Solvents, glues
Butchers Detergents, meat, waste
Cabinet makers and carpenters Glues, detergents, thinners, solvents, wood preservatives
Cleaners Detergents, solvents, wet work
Coal miners Dust (coal, stone), wet conditions
Construction workers Cement
Cooks and caterers Detergents, vegetable juices, wet work
Dentists and dental technicians Detergents, hand cleansers, wet work
Dry cleaners Solvents
Electricians Soldering fluxes
Electroplaters Acids, alkalis
Floor-layers Solvents
Florists and gardeners Manure, artificial fertilizers, pesticides, wet work
Hairdressers Permanent wave solutions, shampoos, bleaching agents, wet work
Hospital workers Detergents, disinfectants, foods, wet work
Homemakers Detergents, cleansers, foods, wet work
Jewelers Detergents, solvents
Mechanics Oils, greases, gasoline, diesel fuel, cleaners, solvents
Metal workers Cutting oils, solvents, hand cleansers
Nurses Disinfectants, detergents, wet work
Office workers Solvents (photocopiers, adhesives)
Painters Solvents, thinners, wallpaper adhesives, hand cleansers
Photography industry workers Solvents, wet work
Plastics workers Solvents, acids, styrene, oxidizing agents
Printers Solvents
Rubber workers Solvents, talc, zinc stearate, uncured rubber
Shoemakers Solvents
Tannery workers Acids, alkalis, reducing and oxidizing agents, wet work
Textile workers Fibers, bleaching agents, solvents
Veterinarians and slaughterhouse workers Disinfectants, wet work, animal entrails and secretions
Veterinarians and slaughterhouse workers Disinfectants, wet work, animal entrails and secretions
Wet work (water or water plus detergent) is the most common occupational irritant. From What occupations are at risk? OSH Answers, Canadian Centre for Occupational Health and Safety (CCOHS), October 15, 2008. https://www.ccohs.ca/ oshanswers/diseases/dermatitis.html. Reproduced with the permission of CCOHS, 2016.
may develop a type of irritant dermatitis characterized by perifollicular papules and pustules.18 Workers exposed to oil often use solvents to remove oil from the skin that further aggravates the irritant dermatitis. Plants and insects less commonly cause irritant dermatitis, but when they do cause irritant dermatitis, it may appear in areas other than the hands. An example is an outbreak of irritant dermatitis from blister beetles in Thai military recruits.19
Fiberglass dermatitis can cause irritant contact or airborne irritant dermatitis. Airborne irritant dermatitis is characterized by eyelid and other flexural involvement of exposed skin.20
NONOCCUPATIONAL EXPOSURES
417
3
Solvents including water
Detergents
Disinfectants
Anti-wrinkle medicaments
Anti-wrinkle medicaments
is commonly seen with the use of retinoids and benzoyl peroxide. Diaper rash is another common example of irritant dermatitis that can occur with wet-to-dry cycles and irritation from stool. Irritant diaper dermatitis has decreased with use of superabsorbent and lessocclusive disposable diapers.21
EXPOSURE TO RUBBING OR STRETCHING THE SKIN
Friction from sporting equipment, such as shin guards, rubbing against skin can cause irritant dermatitis. The friction is worsened by perspiration, and the resulting dermatitis may be complicated by allergic contact dermatitis to rubber chemicals or textile dyes in the shin guard. Athletes may also develop contact dermatitis from dye in clothing that reaches skin as a result of liberation from the fabric by perspiration and friction. Testing to materials obtained from the patient’s own sporting equipment in addition to relevant commercial patch test series increases the sensitivity of patch testing for allergic contact dermatitis caused by sporting equipment.22,23 Irritant dermatitis may be mitigated by use of powder that absorbs perspiration and reduces friction. Friction blisters are an acute skin injury that can be occupational or avocational, such as from raking leaves. Stasis dermatitis occurs when swollen lower legs experience barrier disruption caused by stretching. Lymphatic obstruction accentuates inflammation in mice when challenged with the irritant croton oil. When challenged with the sensitizer dinitrofluorobenzene, mice with lymphatic obstruction had more swelling than those without, but also had lower levels of the inflammatory signals interferon-γ, tumor necrosis factor-α, and the chemokines CXCL9 and CXCL10 than did mice without lymphatic obstruction, suggesting that the increased swelling is a consequence of fluid retention rather than accentuated allergic contact dermatitis.24
CLINICAL FEATURES
CUTANEOUS FINDINGS
CUTANEOUS FINDINGS
Epidermal disruption is the primary finding in irritant dermatitis, as opposed to allergic contact dermatitis which displays proportionately more dermal inflammatory infiltrate. Irritant contact dermatitis is
418
characterized by redness, fissuring, oozing, and pain. Figure 25-2 shows chronic irritant contact dermatitis with epidermal thickening and pigment change. Figure 25-3 shows an irritant patch test created by applying sodium lauryl sulfate 2.5% under occlusion. Note that there is scorched appearing skin surface without much induration. Irritant dermatitis, like this patch test, usually demonstrates more epidermal than dermal inflammation. As Fig. 25-4 shows, severe acute irritant dermatitis can also produce blisters. Allergic contact dermatitis can occur with irritant dermatitis and is more likely to present with the symptoms of itch and more likely to demonstrate induration. Figure 25-5 shows an allergic patch test result. Note that there is more induration than epidermal change.
FLEXURAL ACCENTUATION
Flexural accentuation is an important sign of irritant dermatitis. Common areas for irritant dermatitis are folds in the eyelid, neck, antecubital fossae, volar wrist, and intertriginous regions. In the cases of irritant hand dermatitis and of diaper rash, irritant dermatitis is more apparent in finger webs and creases (Fig. 25-6) and intertriginous folds,
3
respectively, where irritants concentrate, and is worsened by increased pH from soaps and feces, respectively. Irritant cleansers cause predominantly flexural dermatitis where the concentration of irritant is highest because of occlusion.25 Figure 25-7 shows flexural accentuation of acute dermatitis in a patient who inadvertently applied a cleanser, mistaking it for an emollient, to the entire surface of both legs. Retinoid dermatitis also preferentially involves folds such as the nasolabial fold. This is often noted several days after starting cutaneous application, as retinoids produce a delayed irritant reaction.26 Figure 25-8 shows irritant dermatitis on the neck in a patient who began applying tretinoin daily to the neck after tolerating long-term use on the face.
419
3
NONCUTANEOUS FINDINGS
NONCUTANEOUS FINDINGS
Hand dermatitis, which always has an irritant component, is associated with anxiety and obsessivecompulsive traits, but not with depression, compared to healthy controls.27 Contact dermatitis leads to substantial costs and lower work productivity in adults, which may lead to financial harm.28
ETIOLOGY AND PATHOGENESIS
RISK FACTORS
RISK FACTORS
WET WORK, DETERGENTS, AND GLOVES
Occupational hand dermatitis is common in wet workers. Irritation from water is synergistic with irritation from detergent. Solvent exposure is also synergistic with detergent exposure.29
Glove use can protect skin from water and detergents, but perspiration or leakage of moisture around the cuff can occlude moisture under the glove causing maceration from perspiration. Rapid drying of the retained moisture when the glove is removed causes even more damage to the epidermis. Figure 25-9 shows a patient with underlying hand dermatitis who aggravated the dermatitis by wearing occlusive gloves. In healthy human controls with no history of atopic dermatitis who were exposed to repeated half-hour intervals of water occlusion over 4 days, the detergent sodium lauryl sulfate and the alcohol
420
n-propanol both caused more irritation at the test sites than they did on previously unoccluded skin. The detergent was more irritating than the alcohol solution by visual inspection of the skin, measure of transepidermal water loss, and measured decrease in natural moisturizing factor levels.30 A review of the effects of glove occlusion similarly concluded that using waterproof gloves predisposed the skin to more-severe irritation from detergents used for hand hygiene.31
ATOPIC DERMATITIS
Filaggrin mutations are associated with early-onset dermatitis,32 which is often considered to be “atopic dermatitis.” As children become more active, flexural areas develop frictional irritant dermatitis, which leads to allergic contact dermatitis in many cases. Patch testing should be considered in cases of chronic flexural dermatitis.33
PATHOGENESIS
PATHOGENESIS
STEP 1: EPIDERMAL INSULT
The barrier function of the epidermis can be diminished by solvents that remove lipids from the upper epidermal layers, or by desiccation of the stratum corneum from repeated rapid drying. Genetic factors, such as filaggrin mutations, lower the threshold for epidermal damage to include even minor friction.
STEP 2: DANGER SIGNALS
Damaged keratinocytes release danger signals termed alarmins that are analogous to pathogen associated molecular patterns that defend against infections. Examples of candidate alarmins include defensins and uric acid, which may be operative in psoriasis and other inflammatory skin diseases in addition to dermatitis. In fact, the signals from epidermal trauma that drive koebnerization in psoriasis may be different than those in dermatitis and may explain the differences in downstream cytokines that explain the inverse relationship between psoriasis and autoimmune disease and allergic dermatitis.34
These danger signals can bind toll-like receptors and promote inflammatory pathways such as nuclear factor-κB that link to the adaptive immune response leading to allergic dermatitis.35
STEP 3: POTENTIAL FOR ALLERGIC SENSITIZATION
Chemical allergens and microorganisms stimulate the innate immune system, and toll-like receptors play an important role in mediating both irritant and subsequent allergic contact dermatitis.36
Irritant dermatitis predisposes to allergic sensitization to antigens that would not normally cause allergic contact dermatitis on noninflamed skin. Potent sensitizers that can cause allergy on previously noninflamed skin are dependent on their inherent irritant properties. Athymic mice, as an example of intact innate response without adaptive response, mount a neutrophil response and some diminished T-helper (Th)1/Th2 cell response to the sensitizer oxazolone, while FcγR knockout mice, as an example of intact adaptive response without innate response, have a greatly diminished response when sensitized and rechallenged with oxazolone.37
COMPLICATIONS
COMPLICATIONS
ALLERGIC CONTACT DERMATITIS
Allergic contact dermatitis is dependent on irritant dermatitis either in the context of previously inflamed skin or the inherent irritant properties of the sensitizer. Toll-like receptors in a mouse model trigger an innate response that begins the education of the adaptive immune response36 and are well-positioned to initiate an inflammatory response to microorganisms on the skin.
IMMUNE RESPONSE TO LESS- POTENT ALLERGENS, INCLUDING THE MICROBIOME
Childhood-onset dermatitis, also known as atopic dermatitis, is associated with inflammatory responses to common organisms such as Staphylococcus aureus, Malassezia sympodialis, and Alternaria. These organisms may exist as part of a biofilm that concentrates microorganisms and their antigens and may lead to an allergiclike immunologic response to these organisms.38 Figure 25-10 shows a positive patch test to M. sympodialis yeast in a patient with adult-onset dermatitis of the neck and upper torso (Fig. 25-11). The immune response to microbial allergens is distinct from allergic contact dermatitis to potent
3
conventional sensitizers that function as their own irritants on normal-appearing skin. Weakly potent antigens such as propylene glycol, defined as negative in the guinea pig local lymph node assay,39 are more likely to cause contact allergy in patients with barrier disruption triggering “danger signals.” In general, patients with ongoing innate immune signals from either genetic barrier dysfunction or wet work become sensitized to less potent allergens as measured by the local lymph node assay.40
Patients without preexisting irritant dermatitis are more likely to become sensitized to potent antigens that likely create their own innate signal, such as poison ivy. Innate signal from disrupted skin barrier, together with the irritant signal of a potent antigen, may drive dendritic cells into the dermis and promote immunologic tolerance.41 This is consistent with the observation that patients with atopic dermatitis are less likely to exhibit dermatitis to the potent allergen in poison ivy that is also a strong irritant.
FOOD ALLERGY
Infants with irritant dermatitis around the mouth from drooling are at risk for allergic contact sensitization from food contact with the inflamed skin. Foods are generally weak allergens and do not sensitize noninflamed skin. If initial food exposure is on mucosa, tolerance develops.42 This likely explains the higher incidence of peanut allergy in the Unites States where initial peanut exposure is often by self-feeding peanut butter as opposed to the 10-fold lower incidence Israel where initial exposure is to soft baked peanut bambas, which are placed into the mouth directly.
421
3
Patients with atopic dermatitis often, but not always, have only a transient Th1 response to cutaneous contact sensitization. This might explain the tendency for atopic dermatitis to improve as children get older. These patients also develop a more persistent Th2 skewed response43 that might contribute to the atopic march. Figure 25-12 shows the typical perioral inflammation seen with infantile dermatitis that can be complicated by contact sensitization and food allergy with delayed and immediate type hypersensitivity (the atopic march). Although there is no prospective study to confirm the recommendation, new foods should logically be introduced when there is no perioral irritant dermatitis and fed with an infant feeding spoon directly into the mouth rather than being self-fed, which results in substantially more skin contact.
DIAGNOSIS
SUPPORTIVE STUDIES
SUPPORTIVE STUDIES
PATCH TESTING
Patch testing is needed to exclude a component of allergic contact dermatitis. Sensitivity of patch testing is dependent on obtaining a detailed history of personal and occupational exposures and then testing to all potential allergens based on this history. Occupational exposures almost always require specialty patch test series tailored to occupation, and often require dilution of the worker’s own products to an appropriate patch test concentration and vehicle.
LABORATORY TESTING
LABORATORY TESTING
Transepidermal water loss (TEWL) is a measure of the ability of the skin to maintain homeostasis of fluids
422
in the body. In addition to the stratum corneum, tight junctions between living keratinocytes contribute to skin barrier function and provide defense between microbial pathogens and their ligands including tolllike receptors.44 TEWL is a measure of barrier function and increased TEWL indicates increased permeability to antigens.45 TEWL is not routinely tested in clinical practice but is used in research studies of irritant contact dermatitis.
PATHOLOGY
PATHOLOGY
All forms of dermatitis show intercellular edema, or spongiosis, of the epidermis. In the acute phase, there is more fluid which correlates with the clinical presence of vesicles, bullae, and crusting. With chronicity, the stratum corneum exhibits hyperkeratosis, and there is less spongiosis. Figure 25-13 shows the features of subacute dermatitis. In very chronic dermatitis, there is even less spongiosis, no crusting, and elongation of the rete ridges in the epidermis and dermal fibrosis.
IMAGING
IMAGING
Confocal microscopy has been studied to help differentiate irritant from allergic contact dermatitis in vivo, but this is not currently used in practice.46
DIAGNOSTIC ALGORITHM
DIAGNOSTIC ALGORITHM
Diagnosis of irritant dermatitis begins with a detailed history of potential irritants, temporal course of symptoms, and examination for evidence of flexural accentuation. In patients with severe inflammation and itch, allergic contact dermatitis needs to be investigated with appropriate testing. An example is shown in Table 25-4 for a patient with complaint of itching and redness of the hands
3
TIMING TEST COUNSELING
Contact urticaria Itchy hives begin within minutes of exposure and resolves within hours; when chronic, skin findings may resemble dermatitis
Allergic contact dermatitis to rubbera Itchy dermatitis begins hours to days after exposure and resolves over weeks
Irritant contact dermatitis exacer-
Inflammation begins within hours
Irritant contact dermatitis exacerbated by occlusive gloves Inflammation begins within hours and resolves within days of glove avoidance; becomes more chronic over time
bated by occlusive gloves
and resolves within days of glove avoidance; becomes more chronic over time
Avoid latex if positive
Skin prick to latex glove or antigen specific immunoglobulin E (sensitivity 50%-90%); if negative, 15-minute wear test of latex finger cot47
Patch test to a series including rubber accelerators and antioxidants, and to pieces of glove as is
Avoid natural and synthetic rubber gloves containing allergens; use vinyl or allergen-free chemically resistant gloves depending on exposure needs
If patch tests are negative, proceed
Wear cotton under occlusive
If patch tests are negative, proceed with counseling for irritant dermatitis, but consider the possibility of an allergen not patch tested
Wear cotton under occlusive gloves; change gloves frequently; reduce exposure to hand washing
with counseling for irritant dermatitis, but consider the possibility of an allergen not patch tested
gloves; change gloves frequently; reduce exposure to hand washing
aIrritant dermatitis is often the precursor of allergic dermatitis, such that counseling for irritant dermatitis is usually appropriate in addition to counseling for confirmed allergic dermatitis.
after wearing rubber gloves for wet work where irritant contact dermatitis, contact urticaria, and allergic contact dermatitis are considered. Contact urticaria to latex is an example of a contact allergen that is more common in atopic patients and where the allergic contact sensitization has a more persistent Th2 than Th1 response.
DIFFERENTIAL DIAGNOSIS
Irritant dermatitis occasionally mimics other inflammatory dermatoses such as the “mechanic’s hands” sign seen in dermatomyositis (see Chap. 62). The more common clinical dilemma is differentiating irritant dermatitis as the sole explanation for cutaneous inflammation as opposed to irritant dermatitis complicated by allergic disorder. The allergens that cause sensitization depend on the type and degree of irritant dermatitis that is present at the time of sensitization. More research in this area is needed to develop appropriate patch test series. Table 25-5 demonstrates the concept.
The likelihood of sensitization to a moderate to highly potent antigen may be greater in patients with a subclinically decreased irritancy threshold as detected by response to a low concentration patch test to sodium lauryl sulfate.48 Wet workers are more likely to be sensitized to moderately potent allergens such as rubber accelerators.40 The prevalence of eczema and food allergy is higher in children born in autumn or winter months,49 supporting the relationship between climate and irritant dermatitis caused by drooling and sensitization to food on inflamed skin. However, maternal immune factors related to season may also contribute to prevalence of eczema based on immune markers in cord blood that vary by season.50
Patch test series are currently grouped by commonality of exposure rather than skin condition at time of sensitization, which is often not known. As discussed in the section “Immune Response to Less Potent Allergens”, strong sensitizers function as their own irritant and can sensitize noninflamed skin. Most allergens on standard screening series are strong or medium potency allergens and therefore fail to detect the weaker potency allergens
TYPE OF PREEXISTING IRRITATION EXAMPLE POTENCY OF ALLERGEN EXAMPLE OF ALLERGENS
Normal skin or subclinical decreased irritancy threshold Positive patch test to low concentration sodium lauryl sulfate48 Strong Poison ivy; epoxy resin
Moderate Irritant hand dermatitis from wet work40 Medium Rubber chemicals; formaldehydereleasing preservatives
Severe Infantile perioral dermatitis from drooling in cold season49 Weak Foods; vitamin E; propylene glycol
Severe Infantile perioral dermatitis from
drooling in cold season49
Weak Foods; vitamin E; propylene
423
glycol
3
that sensitize patients with preexisting severe irritant contact dermatitis. As a result, allergic contact dermatitis caused by weakly potent allergens in the setting of irritant contact dermatitis is not well studied and the prevalence as well as recommendations for type and frequency of patch testing are not established.
CLINICAL COURSE AND PROGNOSIS
HARDENING
HARDENING
Irritant dermatitis often resolves despite continued exposure to the irritant; this is known as hardening. The process is incompletely understood, which makes it difficult to know which patients will go on to develop chronic irritant hand dermatitis.51 In a prospective experiment, participants challenged with repeated higher concentrations of sodium lauryl sulfate were more likely to harden than those challenged with lower concentrations or distilled water. Only about half of all participants hardened. Those who hardened and those who did not had similar measurements of hyperkeratosis and ceramide content of the stratum corneum.52
This area represents a tremendous knowledge gap. Hardening is the ideal response to unavoidable chronic irritant exposure. Understanding how to promote hardening could reduce the impact of allergic complications of irritant dermatitis including allergic contact dermatitis and atopic diseases.
MANAGEMENT
INTERVENTIONS
INTERVENTIONS
TOPICAL PREWORK PRODUCTS
British standards for occupational contact dermatitis suggest that the term prework cream replace barrier cream to avoid the suggestion that creams can replace more effective barrier equipment such as protective gloves.53 These creams, designed for application prior to irritant exposure, may be modestly effective in some circumstances. A systematic review of barrier creams revealed considerable variation in methodology. The reviewers point out that participants were often tested on the forearm or back, rather than the hand, which is the most frequently affected site. Friction and multiple flexures on the hands may increase the risk of irritation at this site.54 Barrier creams may not be applied in the same quantity in the workplace as in the studies. Barrier creams were more effective for preventing irritation from the detergent sodium lauryl sulfate and the alkaline sodium hydroxide than against the solvent toluene.55
424
MEDICATIONS
Given the weak evidence for the most commonly used treatments, avoidance of irritants is the best treatment option. Although not clearly effective for prevention of hand dermatitis, use of emollients is recommended for treatment of hand dermatitis, even though some emollients appear to increase the penetration of allergen and irritants, and it is not clear which emollients are best in specific settings.56 Only some emollients, usually with high lipid content, including petrolatum, accelerate barrier repair in experimentally induced irritant and allergic contact dermatitis.57
Topical corticosteroids are frequently used, but chronic use may impair barrier function by thinning the epidermis.26 Topical immunomodulators may be of some benefit but are not consistently more effective than vehicle alone.26
Although rarely needed for purely irritant dermatitis, phototherapy and systemic immunosuppressive medications are often used for multifactorial dermatitis, such as hand dermatitis. Alitretinoin is considered second-line therapy for chronic hand dermatitis in Europe,56 but is not available in the United States as of 2018.
COUNSELING
There is weak evidence that nurse-led counseling improves disease severity, but not quality of life, in patients with contact dermatitis of the hands.58 Patients may increasingly prefer technology-assisted counseling, such as by telemedicine, as opposed to travel to a clinic, although traveling to a clinic is still needed for diagnostic testing, including patch testing. Decreasing the frequency of exposure may allow a worker to continue with their job.59 Alcohol-based hand sanitizers should substitute for hand washing whenever allowed, especially in cold seasons when indoor heating lowers ambient humidity.56
Gloves: Avoidance of irritants, including use of water-resistant gloves for wet work, is the best strategy to prevent and treat irritant dermatitis. In people without other irritant factors, that is, no history of childhood onset dermatitis to suggest genetically impaired barrier function, no use of irritant chemicals at work, infrequent wet work, occlusive gloves are well tolerated. However, occlusion alone can cause inflammation in skin that is already irritated.60 Figure 25-14 shows a patient with atopic dermatitis where polyethylene film alone applied to the skin for 24 hours caused visible inflammation as did the adjacent 3 patch tests to sodium lauryl sulfate. Occlusive gloves should be used for wet work but only worn for the shortest time possible. In persons with preexisting irritant dermatitis, cotton gloves are recommended under occlusive gloves if the duration of glove usage is longer than 10 minutes.56
People who itch with occlusion often also report itching with perspiration. The same factors that contribute
to irritant dermatitis under gloves also cause irritation under bandages that mimic allergic contact dermatitis to adhesive.61
Patients who itch with occlusion generally prefer foam, lotion, or cream vehicles for topical products as they find ointments to cause itching.
TREATMENT ALGORITHM
TREATMENT ALGORITHM
Dermatitis should be treated as soon as it is recognized, as chronic dermatitis has a worse prognosis than acute dermatitis. All irritants should be avoided for weeks beyond visual recovery. There was lowered irritancy threshold lasting longer than 10 weeks after visual recovery from experimentally induced dermatitis from sodium lauryl sulfate applied 15 times to forearm skin over 3 weeks.62
The British guidelines for occupational contact dermatitis suggest referral to a dermatologist knowledgeable about patch testing for occupational contact dermatitis if there is no improvement 3 months after initial evaluation for dermatitis and if there is suspicion for allergic contact dermatitis or changes to job duties are contemplated.53
PREVENTION OF IRRITANT DERMATITIS
PREVENTION OF IRRITANT
DERMATITIS
A systematic review published in 2010 found no significant evidence to prove efficacy of gloves, barrier creams, emollients, or worker education programs in preventing occupational irritant hand dermatitis.63
Barrier creams were discussed in the section “Topical Pre-Work Products” earlier. There are studies that show some emollients may provide some degree of prevention when used prior to developing dermatitis rather than as intervention for dermatitis. A study of normal volunteers who washed their hands 15 times daily with an antiseptic soap to mimic hand hygiene in health care workers found that 3 of 5 emollients decreased visible irritation and TEWL compared to no emollient.64
Duration of application prior to exposure may influence the degree to which it provides protection from
3
an irritant. An emollient applied 15 minutes prior to exposure to sodium lauryl sulfate (SLS) prevented irritation as measured by TEWL, but daily use of the same emollient increased irritation after sodium lauryl sulfate exposure. This suggests that hydrated skin may be more susceptible to irritants and that prolonged use of emollients may actually increase the risk of irritant contact dermatitis.65
PREVENTION OF COMPLICATIONS
PREVENTION OF
COMPLICATIONS
In regard to prevention of atopic dermatitis as a complication of irritant dermatitis resulting from genetic barrier deficits, a randomized controlled trial of daily application of emollients in infants from 3 weeks to 6 months of age showed a significant benefit in favor or emollients compared to no emollients. Thirteen percent of the control group used emollients despite randomization to the nonemollient group, and the authors did not comment on seasonal comparability of the control groups during this year-long study in cities in Oregon and the United Kingdom. Cream-based emollients were favored by parents in this study over oil- and ointment-based emollients.66
Another study of daily versus occasional application of petroleum jelly to infants from birth to 32 weeks of age showed lower incidence of dermatitis in the daily application group, but no significant decrease in sensitization to egg white as measured by antigen-specific immunoglobulin E to egg at 32 weeks of life.67
Prevention of both irritant contact dermatitis and its complications is understudied as discussed in the section “Clinical Course and Prognosis” on hardening. We do not know the components of emollients least likely to cause allergic contact dermatitis in various populations, the ideal pH of emollients, or the effect of various types of emollients on potentially inflammatory components of the microbiome.
SCREENING
SCREENING
Screening with a questionnaire to assess risk factors and visual assessment of health care worker’s hands in Toronto revealed a 72% prevalence of mostly mild and some moderate hand dermatitis. Risk factors included handwashing frequency and duration of wearing gloves, but not age or gender.68
Screening may help identify early cases of irritant hand dermatitis, which is important because there is a delay in obtaining diagnostic patch testing from onset of symptoms ranging from 2 to 5 years. The delay is attributable to patient factors including hope that the condition will go away and anxiety over obtaining care, and to access, with most patients seeing a primary care physician first and then waiting for an
425
3
appointment with dermatologist and then again after referral to a patch test expert.69
Given the association between chronicity and poor prognosis, screening may reduce societal burden of disease. However, reduced burden of disease will occur only with advances in treatment and improved understanding of ways to prevent complications.
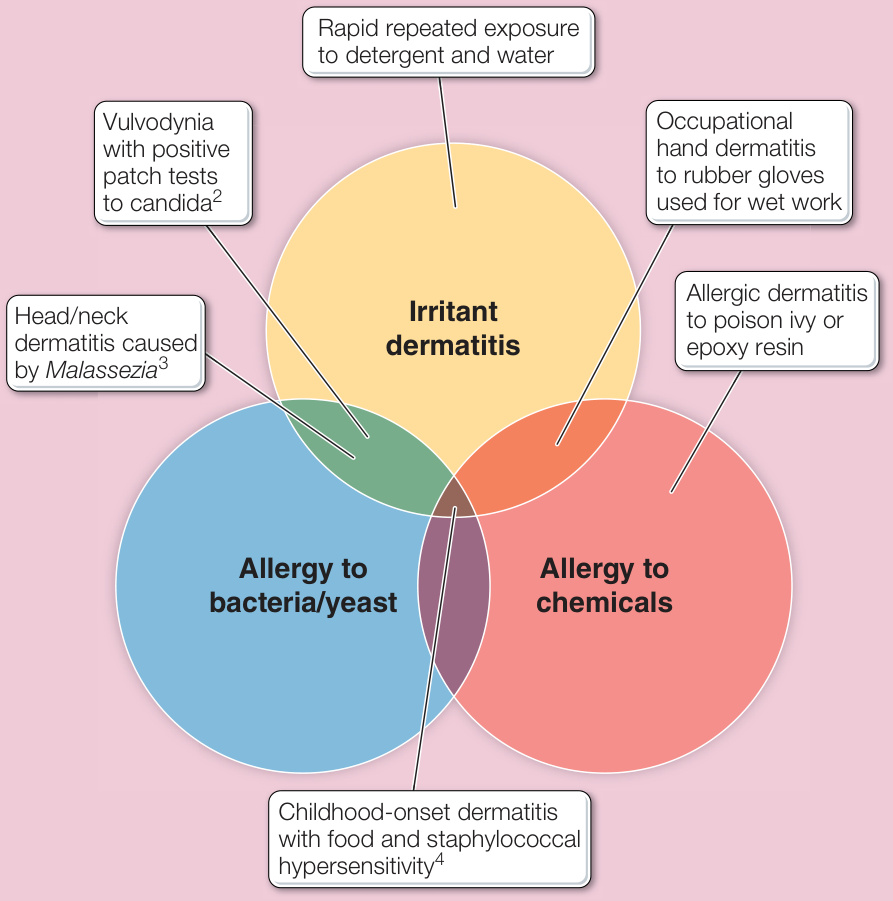
Figure 25-1 Irritant dermatitis leads to barrier disruption that promotes immune response to bacteria and yeast, as well as to chemicals in contact with the skin. Dermatitis often results from a combination of causative factors. Examples are shown here for various combinations of causative factors.

Figure 25-2 Thickened skin with pigment changes in areas of chronic friction on the dorsal hands caused by occupation. This is an exception to the usual finding of accentuation in flexural areas, because the frictional exposure was to the dorsal surface of the hands only.

Figure 25-3 Irritant dermatitis from a patch test with sodium lauryl sulfate. Note the scorched appearance of the skin with more surface change than papules.

Figure 25-4 Bullous irritant patch test response with blister but no surrounding induration.

Figure 25-5 Allergic dermatitis from a patch test to gold; there are multiple papules and an indurated base.

Figure 25-6 Mild wintertime irritant dermatitis in a health care worker. Note the accentuation of the chapping in the flexural areas.
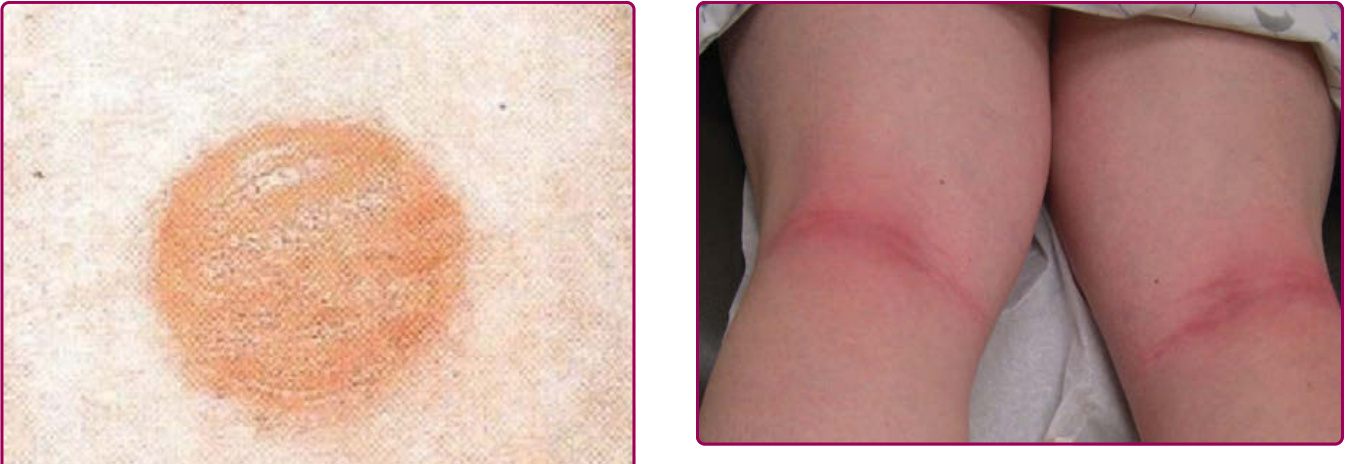
Figure 25-7 Acute irritant dermatitis in a patient who mistook a body wash for an emollient and applied the body wash at bedtime. The patient awoke with inflammation primarily in the flexural areas despite application to the entire leg.

Figure 25-8 Topical retinoid-induced irritant dermatitis on the neck.

Figure 25-9 Irritant macerated dermatitis from wearing a wet cotton glove under an occlusive glove.

Figure 25-10 Positive patch test to Malassezia sympodialis yeast in an adult patient with dermatitis of the anterior axillary line and neck.

Figure 25-11 Distribution of dermatitis seen in patients with sensitivity to Malassezia sympodialis.

Figure 25-12 Infantile dermatitis that likely began as irritant dermatitis from drooling and in this case was complicated by allergic contact dermatitis to an emollient cream confirmed by patch testing.
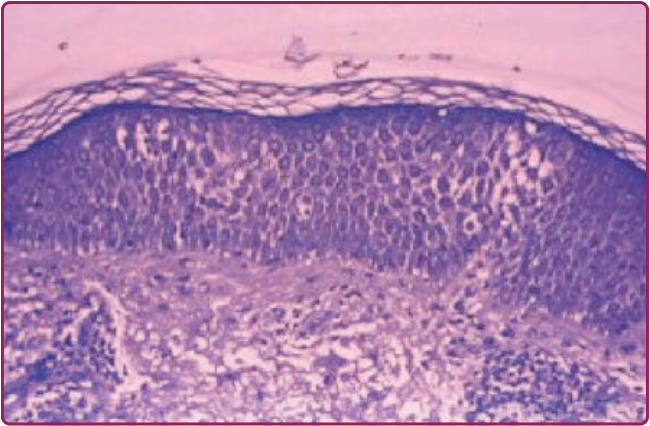
Figure 25-13 Subacute spongiotic dermatitis as seen in irritant and in allergic contact dermatitis.

Figure 25-14 Inflammation from a rectangular piece of polyethylene film applied to atopic skin for 24 hours and compared to 3 round chambers containing sodium lauryl sulfate applied to the same subject for 24 hours.
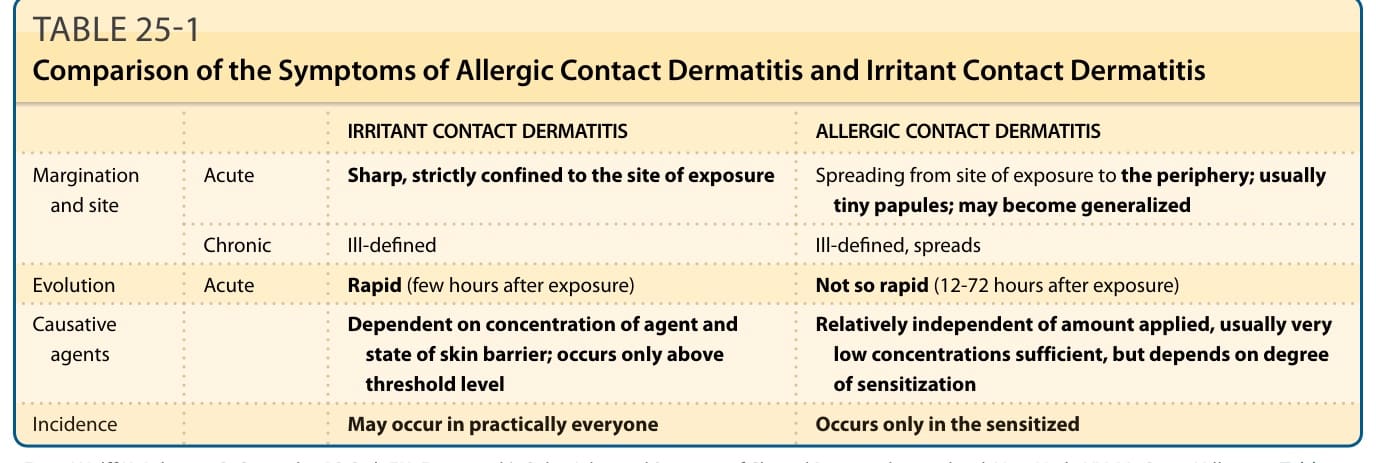
TABLE 25-1 Comparison of the Symptoms of Allergic Contact Dermatitis and Irritant Contact Dermatitis
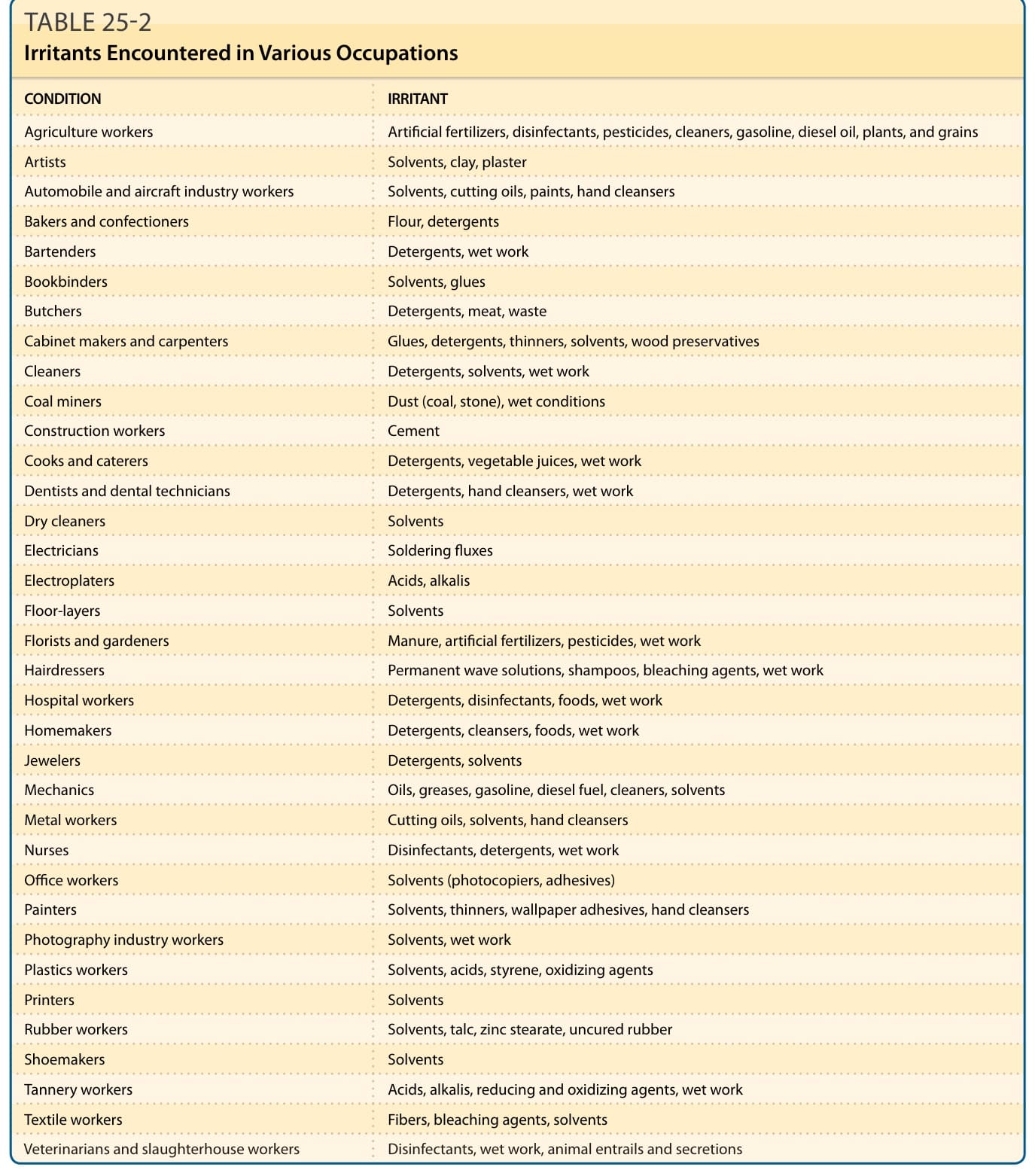
Table 25-2 lists common irritants by occupation. These are rarely important diagnostically, as patients self-identify and avoid most irritants. Water—from wet work, drooling, and sweating—is the most important irritant that provokes irritant dermatitis leading to allergic contact and atopic dermatitis because it is difficult to avoid. Oil dermatitis occurs in workers whose hands and forearms have prolonged contact with oil and who
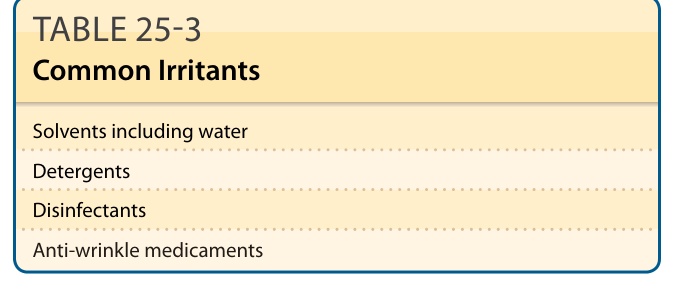
Table 25-3 shows common irritants encountered outside of work. Medicaments may cause irritation, which
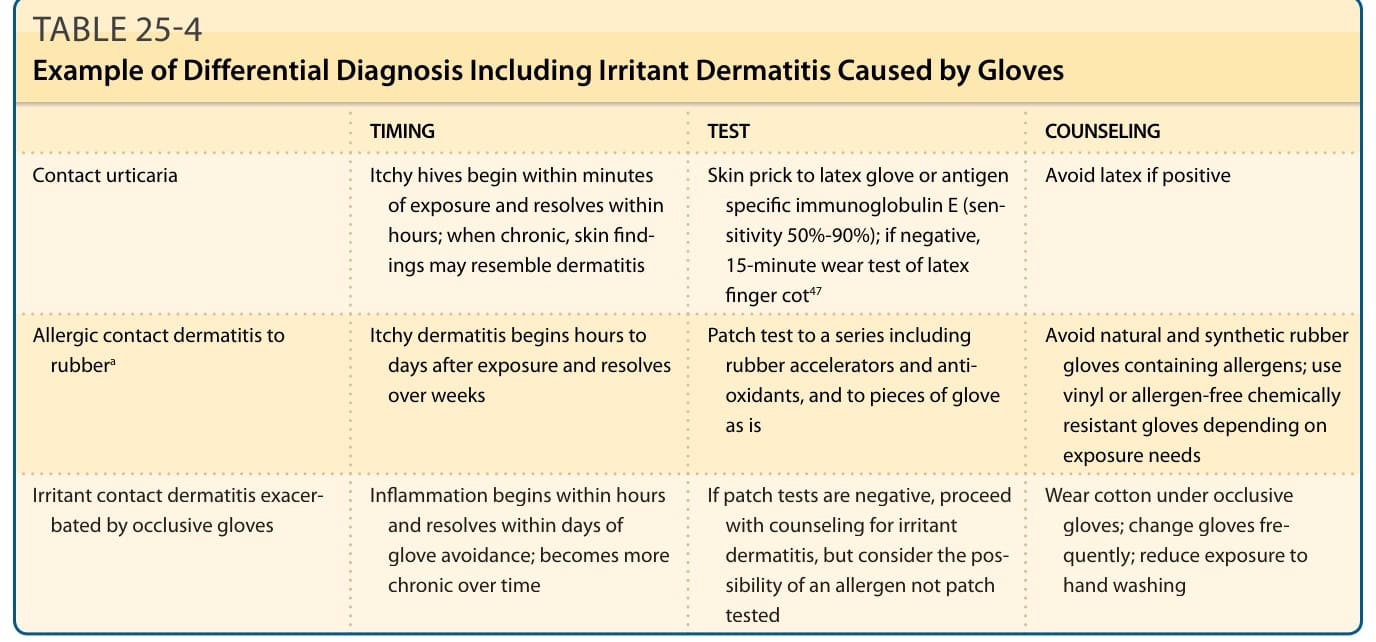
TABLE 25-4 Example of Differential Diagnosis Including Irritant Dermatitis Caused by Gloves
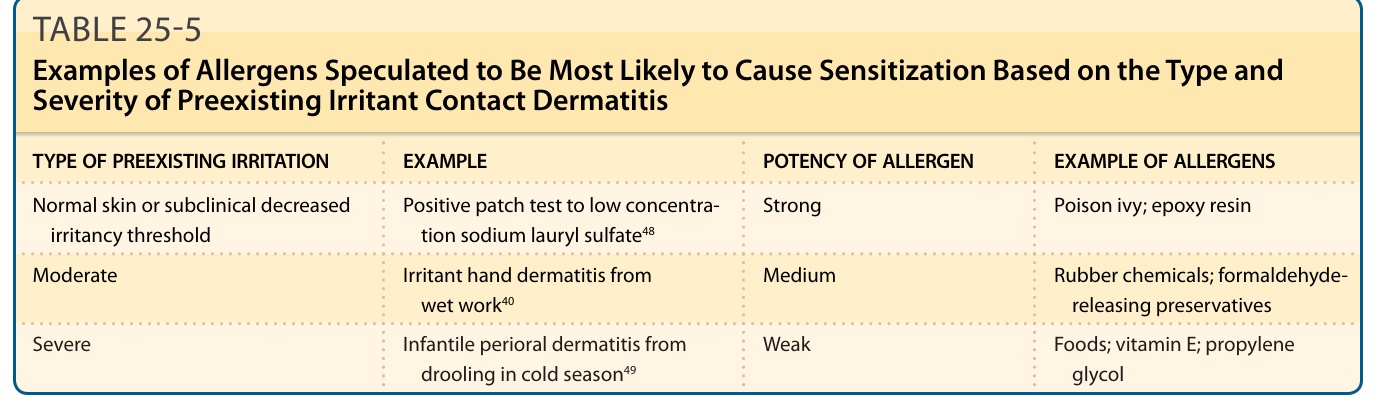
TABLE 25-5 Examples of Allergens Speculated to Be Most Likely to Cause Sensitization Based on the Type and Severity of Preexisting Irritant Contact Dermatitis