Atopic Dermatitis
PART3
Dermatitis
AT-A-GLANCE
■ Atopic dermatitis (AD) has a prevalence peak of 15% to 20% in early childhood in industrialized countries.
■ AD has variable rates of remission, with many patients continuing or recurring with symptoms into adulthood.
■ AD is a chronic or chronically relapsing disorder with major features of:
■ Pruritus
■ Eczematous dermatitis (acute, subacute, or chronic) with typical morphology and agespecific patterns
■ Facial and extensor involvement in infancy
■ Flexural eczema or lichenification in children and adults
■ Commonly associated with the following:
■ Personal or family history of atopy (allergic rhinitis, asthma, atopic dermatitis)
■ Xerosis or skin barrier dysfunction
■ Immunoglobulin E reactivity
■ Pathogenesis driven by skin barrier defects (most importantly in the FLG gene), environmental effects and alterations in immunologic responses in T cells, antigen processing, inflammatory cytokines, host defense proteins, allergen sensitivity, and infection.
INTRODUCTION
Atopic dermatitis (atopic eczema, AD) is a chronic inflammatory skin disease primarily beginning in childhood with a variable natural course. Itch is the hallmark symptom of the disease, often unrelenting in severe cases, and leads to sleep disturbance and excoriated, infection-prone skin. Patients with AD often additionally have atopic comorbidities such as allergic asthma and allergic rhinitis and experience a significantly impaired quality of life.
DEFINITIONS AND HISTORICAL PERSPECTIVE
NOMENCLATURE
NOMENCLATURE
The term atopic dermatitis was first coined in 1933 by Sulzberger and Wise and replaced early terms corresponding to probable AD such as tinea muquese, porrigo larvalis, and Hebra’s prurigo. The term atopy was first introduced by Coca and Cooke in 1923 to describe the tendency toward developing allergic hypersensitivity manifested by asthma and hayfever.1 The term atopi is derived from the Greek word atopos meaning “without place,” reflecting the mysterious pathogenic underpinnings of allergic hypersensitivity disease. Wise and Sulzberger coined the term atopic dermatitis in 1933 to describe recurring eczematous skin disease found in patients with a family history of atopic disease.2
3
Importantly, they noted that patients with AD may not have a personal history of other atopic disease. Since this seminal paper, several groups attempted to rename the disease primarily to differentiate AD that has concomitant immunoglobulin E (IgE) sensitization from AD without sensitization, such as atopiform dermatitis and nonatopic eczema. A recent systematic review reveals atopic dermatitis to be the most commonly used name for the disease and proposed the universal use of this term for AD.3 The authors of that paper discourage the use of less specific terms such as eczema, which is a morphological term and includes contact and other eczematous conditions.
DIAGNOSTIC CRITERIA
DIAGNOSTIC CRITERIA
Significant advancement of our understanding of the disease could not be made without a proper disease definition. Early work by luminaries in AD, such as Rajka, Lobitz, and Hanifin, paved the way for the first comprehensive diagnostic criteria for AD—the Hanifin- Rajka criteria.4 The major criteria have been validated and remain the gold standard for AD diagnosis. Similar to AD nomenclature, numerous attempts have been made to refine and shorten the original criteria to make them more useful in clinical practice. The UK Working Party Criteria were developed using modern statistical methods and represent a distilled set of the original criteria useful for population-based epidemiologic study.5 The American Academy of Dermatology consensus diagnostic criteria for pediatric AD are a useful and clinician-friendly guide to AD diagnosis, although no formal validation studies have been published.6
EPIDEMIOLOGY
Since the 1960s, there has been a more than threefold increase in the prevalence of AD.2 AD is a major public health problem worldwide, with a prevalence in children of 10% to 20% in the United States, Northern and Western Europe, urban Africa, Japan, Australia, and other industrialized countries.3 The Global Disease Burden project ranks “dermatitis,” which includes AD, as the highest ranking skin disease in regards to total global disability burden.7 The prevalence of AD in adults is less clear, but recent studies estimate the prevalence to be between 3% to 7% in the United States, Germany, and Japan.8-10 The International Study of Asthma and Allergies in Childhood (ISAAC) Phase Three study confirmed that AD is a disease with high prevalence worldwide, affecting patients in both developed and developing countries.4 There is also an observed female preponderance for AD, with an overall female-to-male ratio of 1.3 to 1.0. Racial and ethnic differences in prevalence also exist with African Americans having a higher prevalence of the disease in the United States.11
Wide variations in prevalence have been observed within countries inhabited by similar ethnic groups,
364
suggesting that environmental factors are critical in determining disease expression. Several studies reveal lower prevalence rates in rural settings compared with urban centers within the same country.12 Other risk factors reported to be associated with AD include exposure to airborne pollution, use of hard water, increased income and education both in whites and blacks, obesity, and increased use of antibiotics.13-17 Climate may also play a role in disease expression with lower humidity and lower ultraviolet (UV) areas displaying higher prevalence rates.18 Climatic factors and pollution levels may also influence symptoms and flares of the disease.19
CLINICAL FEATURES
CUTANEOUS FINDINGS
CUTANEOUS FINDINGS
Acute eczematous lesions are characterized by erythematous papulovesicles, often with pinpoint crusting or frank weeping. More subacute to chronic lesions often display scale, excoriation, and lichenification. Patients with AD may present with only one stage of eczematous lesions, but most often patients have a mixture of both acute and chronic lesions in multiple areas of the body simultaneously or even in the same lesion. Individual eczematous lesions of AD cannot be readily distinguished clinically or histologically from lesions found in other eczematous conditions such as allergic contact dermatitis or nummular dermatitis. Patients with darker skin tones often present with follicular accentuation, flat-topped papules in lichenified areas, and a tendency toward hyperpigmentation in inflamed areas, which can be very distressing for patients. Rarely, patients may also experience a vitiligo-like depigmentation in involved areas that is difficult to distinguish from topical steroid-induced pigment loss. The distribution of eczematous lesions vary according to the patient’s age (Fig. 22-1) and disease activity. During infancy, the AD is generally more acute and primarily involves the face (Fig. 22-2), the scalp, and the extensor surfaces of the extremities (Fig. 22-3).20 The diaper area is usually spared. In older children and in those who have long-standing skin disease, the patient develops the chronic form of AD with lichenification and localization of the rash to the flexural folds of the extremities (Fig. 22-4). AD may subside as the patient grows older, leaving an adult with skin that is prone to itching and inflammation when exposed to exogenous irritants. Chronic hand eczema may be the primary manifestation of AD in many adults (Fig. 22-5). At least one third of patients will have clinical features of filaggrin deficiency such as ichthyosis vulgaris, keratosis pilaris, and hyperlinear palms. These clinical features are associated with genetic defects encoding the filaggrin protein and can identify patients who have a more severe disease course and allergic comorbidities.21
Other less specific but common associated features of AD are listed in Table 22-1. Other specific skin conditions associated with AD include vitiligo and alopecia areata.22
3
Sites of predilection by age
NONCUTANEOUS FINDINGS
NONCUTANEOUS FINDINGS
ATOPIC COMORBIDITIES
There is growing recognition that patients with AD carry a large burden of comorbid conditions. Patients with AD often show signs of T helper 2 (Th2) immune activation, including high levels of total and specific serum IgE, eosinophilia, and a predisposition toward allergic comorbidities. Large population-based studies reveal patients with AD have a higher prevalence of
365
3
food allergy, asthma, and allergic rhinitis. The severity of the skin disease correlates with both the risk and severity of the comorbidity.23 AD is often the first atopic disease to develop, but the diseases can occur in any order and in any combination.24 For example, allergic sensitization may occur before or after AD development25 but does develop in up to 80% of patients. Large collaborative efforts to integrate clinical cohort and “omics” data are underway and suggest Th2-driven pathobiological pathways underlie the multimorbidity seen in AD.26 There are no studies as of yet demonstrating treatment of the skin alone has a positive impact on allergic comorbidities or whether prevention of AD can halt the development of other atopic diseases (“atopic march”).
PSYCHOSOCIAL IMPACT
Numerous studies in pediatric populations and adults reveal AD, especially moderate to severe disease,
366
Major Features Pruritus Rash on face, extensors, or both in infants and young children Lichenification in flexural areas in older children Tendency toward chronic or chronically relapsing dermatitis Personal or family history of atopic disease: asthma, allergic rhinitis, atopic dermatitis
Other Common Findings
Other Common Findings Dryness Dennie-Morgan folds (accentuated lines or grooves below the margin of the lower eyelid) Allergic shiners (darkening beneath the eyes) Facial pallor Pityriasis alba Keratosis pilaris Ichthyosis vulgaris Hyperlinearity of palms and soles White dermatographism (white line appears on skin within 1 minute of being stroked with a blunt instrument) Conjunctivitis Keratoconus Anterior subcapsular cataracts Elevated serum immunoglobulin E Immediate skin test reactivity
Dryness Dennie-Morgan folds (accentuated lines or grooves below the margin of the lower eyelid) Allergic shiners (darkening beneath the eyes) Facial pallor Pityriasis alba Keratosis pilaris Ichthyosis vulgaris Hyperlinearity of palms and soles White dermatographism (white line appears on skin within 1 minute of being stroked with a blunt instrument) Conjunctivitis Keratoconus Anterior subcapsular cataracts Elevated serum immunoglobulin E Immediate skin test reactivity
profoundly impacts the emotional and psychological well-being of a patient. Children with AD display more emotional and behavioral problems compared with normal control participants.27 Population-based studies also find a higher prevalence of attention-deficit hyperactivity disorder (ADHD), anxiety, conduct disorder, and autism in children with AD compared with children without AD.28 Children with more severe disease appear to be particularly at risk. The risk of ADHD in both children and adults appears to be mediated by sleep disturbance, a common consequence of pruritus in AD.29
Anxiety and depression are commonly found comorbidities in adult patients with AD. Between 43% and 57% of patients met thresholds on the Hospital Anxiety and Depression Scale for probable anxiety or depression in phase 3 clinical trials for AD.30 Effective antiinflammatory therapy appeared to alleviate both anxiety and depression symptoms in a significant proportion of adults during these trials.
COMPLICATIONS
COMPLICATIONS
BACTERIAL INFECTION
Superficial Staphylococcus aureus infections are by far the most common infection found in AD. S. aureus colonizes skin lesions in more than 70% of patients with AD with more severe AD having higher rates of colonization.31,32 Studies conflict regarding the prevalence of methicillin-resistant S. aureus (MRSA) in this population but does not appear to be higher than
background colonization rates. Few studies address the rate of true infection from S. aureus, in contrast to colonization. One study from Japan found almost a twofold increase in impetigo in children with AD compared with non-AD control participants.33 The rate of serious infections from S. aureus is also not well characterized in patients with AD, but there are reports in the literature of endocarditis, osteomyelitis, and septicemia.34
Both skin barrier and immune deficits found in AD may explain the propensity to colonization and infection. Inflamed skin increases the expression of fibronectin and fibrinogen, which are S. aureus binding sites.35 The elevated pH and disrupted barrier from excoriation seen in AD skin promotes S. aureus growth. Antimicrobial peptide expression is also blunted in these patients, thought to be secondary to the inhibitory effect of type 2 cytokines.36,37 Type 2 cytokines also augment the killing effect of S. aureus toxins on keratinocytes.38 Blockade of type 2 cytokines in AD appears to reduce skin infections in AD.39
S. aureus colonization likely contributes to skin inflammation; S. aureus toxins activate antigen presenting cells and increase T-cell cutaneous lymphocyte antigen (CLA) expression. Flares of AD correspond to shifts in the microbiome toward larger proportions of S. aureus representation.40 Antibiotic treatment of clinically uninfected skin, however, has not been found to reduce AD severity.41 The use of dilute sodium hypochlorite baths (bleach baths) appears to improve AD severity, but it is uncertain if this is through antiinflammatory and barrier effects rather than antimicrobial ones.42
The decision to treat a S. aureus infection is not straightforward. It is often difficult to distinguish acute crusted AD or excoriation from S. aureus impetiginization, and culturing of lesions does not help in distinguishing between colonization and infection. Culturing is recommended, however, to help guide antibiotic therapy and identify MRSA strains. MRSA has become an increasingly important pathogen in patients with AD.43 Erosive plaques, honey-colored crusting, folliculitis, and persistent or multiple tender pustules are indicators of clinically relevant secondary bacterial skin infection in which antibiotic use would be indicated. Interestingly, topical steroids alone reduce S. aureus counts illustrating the role inflammation plays in S. aureus susceptibility.
VIRAL INFECTION
Patients with AD display an increased susceptibility to common warts and exaggerated clinical presentations to other viral infections such molluscum contagiosum. The most serious virally mediated complication is eczema herpeticum (EH). After an incubation period of 5 to 12 days, multiple itchy, vesiculopustular lesions erupt in a disseminated pattern; vesicular lesions are umbilicated, tend to cluster, and often become hemorrhagic and crusted (Fig. 22-6). Punched-out and extremely painful erosions result. These lesions may coalesce to large, denuded, and bleeding areas that can extend over the entire body and be fatal in some cases.
3
Defects in interferon pathways may explain why some patients develop this potentially devastating complication.44
Although smallpox infections have been eradicated worldwide since the late 1970s, threats of bioterrorism (with smallpox and other infectious agents) have forced nations to reconsider their policies toward initiating vaccination programs. In AD patients, smallpox vaccination (or even exposure to vaccinated individuals) (see Chap. 166) may cause a severe widespread eruption (eczema vaccinatum) that appears very similar to EH. Thus, in patients with AD, vaccination is contraindicated unless there is a clear risk of smallpox. In addition, decisions regarding vaccination of family members should take into consideration the potential of eczema vaccinatum in household contacts. Exaggerated responses to coxsackie virus have also been reported in patients with AD that may resemble EH and has been termed eczema coxsackium.45 Children present with hand and foot vesicles or papules that resemble typical hand, foot, and mouth disease, but lesions tend to be more severe and hemorrhagic and involve additional areas involved with eczema. Despite the sometimes dramatic presentation, the skin rash resolves with no negative sequelae.
FUNGAL INFECTION
It is unclear whether superficial fungal infections are more common in atopic individuals. There has been particular interest in the role of Malassezia sympodialis (Pityrosporum ovale or Pityrosporum orbiculare) in AD. M. sympodialis is a lipophilic yeast (see Chaps. 160 and
161) commonly present in the seborrheic areas of the skin. IgE antibodies against Malassezia furfur are commonly found in AD patients and most frequently in patients with head and neck dermatitis.46 Although there are some case reports of improvement of head and neck AD with antifungal therapy, controlled trials are needed to determine the efficacy of targeting fungi in AD in this subset of patients.
OCULAR PROBLEMS
Eye complications associated with severe AD can lead to significant morbidity. Eyelid dermatitis and chronic
367
3
blepharitis are commonly associated with AD and may result in visual impairment from corneal scarring. Atopic keratoconjunctivitis is usually bilateral and can have disabling symptoms that include itching, burning, tearing, and copious mucoid discharge. Vernal conjunctivitis is a severe bilateral recurrent chronic inflammatory process associated with papillary hypertrophy or cobblestoning of the upper eyelid conjunctiva. It usually occurs in younger patients and has a marked seasonal incidence, often in the spring. The associated intense pruritus is exacerbated by exposure to irritants, light, or sweating. Keratoconus is a conical deformity of the cornea believed to result from chronic rubbing of the eyes in patients with AD and allergic rhinoconjunctivitis. Cataracts were reported in the early literature to occur in up to 21% of patients with severe AD. However, it is unclear whether this was a primary manifestation of AD or the result of the extensive use of systemic and topical glucocorticoids, particularly around the eyes. Indeed, more recent studies suggest that routine screening for cataracts in patients with AD may not be productive unless there is concern about potential side effects from steroid therapy.
HAND DERMATITIS
Patients with AD often develop nonspecific, irritant hand dermatitis. It is frequently aggravated by repeated wetting and by washing of the hands with harsh soaps, detergents, and disinfectants. Atopic individuals with occupations involving wet work are prone to develop an intractable hand dermatitis in the occupational setting, which is a common cause of occupational disability. Less frequently, patients with AD may also develop a recurring chronic palmar or palmoplantar vesicular dermatitis.
EXFOLIATIVE DERMATITIS
Patients with extensive skin involvement may develop exfoliative dermatitis (see Chap. 21). This is associated with generalized redness, scaling, weeping, crusting, systemic toxicity, lymphadenopathy, and fever. Although this complication is rare, it is potentially life threatening. It is usually caused by superinfection, for example, with toxin-producing S. aureus or herpes simplex infection, continued irritation of the skin, or inappropriate therapy. In some cases, the withdrawal of topical or systemic glucocorticoids used to control severe AD may be a precipitating factor for exfoliative erythroderma.
ETIOLOGY AND PATHOGENESIS
OVERVIEW
OVERVIEW
Atopic dermatitis is a complex familial transmitted skin disease caused by interactions among genetic,
368
immune, and environmental risk factors.47 The interindividual variation of these factors compound the heterogeneity of mechanisms leading to AD. AD often occurs in association with asthma, allergic rhinitis, and food allergy. As such, AD may be considered part of a systemic disorder. Genetic and mechanistic studies suggest that two major biologic pathways are responsible for AD: epidermal dysfunction and altered innate or adaptive immune responses to microbes, allergens, stress, and irritants. Discovery of key pathogenic pathways and their associated biomarkers represents an active area of investigation required for the discovery of novel drugs or biologics that will effectively treat severe AD unresponsive to standard medications.
DECREASED SKIN BARRIER FUNCTION
DECREASED SKIN
BARRIER FUNCTION
Atopic dermatitis is associated with decreased in skin barrier function caused by the downregulation of cornified envelope genes (eg, keratin, filaggrin, and loricrin), reduced ceramide levels, increased endogenous proteolytic enzyme activity, and enhanced transepidermal water loss.48 Addition of soap and detergents to the skin raises its pH, thereby increasing activity of endogenous proteases, leading to further breakdown of epidermal barrier function. The epidermal barrier may also be damaged by scratching, exposure to exogenous proteases from house dust mites, and S. aureus. This is worsened by the lack of certain endogenous protease inhibitors in atopic skin. These epidermal changes likely contribute to increased allergen absorption into the skin and microbial colonization. Because epicutaneous sensitization to allergen results in higher level allergic immune responses, decreased skin barrier function could act as a site for allergen sensitization and predispose such children to the development of food allergy and respiratory allergy.
GENETICS
GENETICS
More than 80 genes have been associated with AD.43,49 Of these genes, loss-of-function mutations involving the epidermal barrier protein filaggrin have been most consistently replicated to be a major predisposing factor for AD in European whites and Asians. Of note, the filaggrin gene is found on chromosome 1q21, which contains genes (including involucrin, loricrin, and S100 calcium binding proteins) in the epidermal differentiation complex (EDC), known to be expressed during terminal differentiation of the epidermis. Gene profiling studies have demonstrated downregulation of genes encoding proteins involved in epidermal differentiation, including multiple skin barrier proteins and antimicrobial peptides required for host defense in AD.50 Candidate gene approaches have also implicated
variants in the SPINK5 gene, which is expressed in the uppermost epidermis, where its product, LEKT1, inhibits two serine proteases involved in desquamation and inflammation (stratum corneum tryptic enzyme and stratum corneum chymotryptic enzyme). Stratum corneum tryptic enzyme and stratum corneum tryptic enzyme expression is increased in AD, suggesting that an imbalance of protease versus protease inhibitor activity may contribute to atopic skin inflammation. Other skin barrier genes that have been implicated in AD include LAMA3, TMEM79, filaggrin-2 (FLG2), Late Cornified Envelope-like Proline-rich 1 (LELP1), and claudin-1 (CLDN1). The relative importance of different skin barrier genes and immune responses may vary by race.51 It is interesting, for example, that FLG mutations have currently not been consistently found in African populations; however, loss-offunction mutations in FLG2 are associated with increased risk in African Americans.49
These observations establish a key role for impaired skin barrier function in the pathogenesis of AD because impaired skin barrier formation allows increased transepidermal water loss, and importantly, increased attachment and entry of allergens and chemicals from the environment, resulting in skin inflammatory responses.47 It is important to note that filaggrin mutations and likely other mutations affecting the skin barrier can occur in normal healthy individuals, patients with ichthyosis vulgaris who do not have significant skin inflammation, and only a minority of individuals with AD have filaggrin gene mutations. This suggests that factors other than skin barrier gene mutations are also required for the development of AD. Atopic dermatitis has also been associated with variation of genes involved in innate and adaptive immunity, interleukin-1 (IL-1) family signaling, regulatory T cells, vitamin D pathway, and nerve growth factor pathway.43 Thus, a combination of various genetic factors may influence the development of different AD phenotypes. Patients with filaggrin null mutations often have early onset of AD, severe eczema, and high-level allergen sensitization and develop asthma later in childhood (ie, the so-called atopic march).48,49 In patients with AD susceptible to EH (ADEH+), filaggrin mutations occur in combination with transcriptomic signatures in peripheral blood mononuclear cells (PBMCs) that are distinct from AD without a history of AD (ADEH-). In a recent report, it was demonstrated that unstimulated ADEH+ and ADEH- PBMC had similar transcriptomes.52 However, after stimulation with herpes simplex virus (HSV), PBMCs from ADEH+ had distinct transcriptomic profiles compared with ADEH-, with striking downregulation of antiviral cytokines, including both type I and type III INFs. These results are indicative of defective innate immune responses in ADEH+ subjects. Atopic dermatitis is a complex trait that involves interactions between multiple gene products requiring environmental factors and the immune response, leading to a final clinical phenotype. Chromosome 5q31- 33 contains a clustered family of functionally related cytokine genes—IL-3, IL-4, IL-5, IL-13, and granulocyte macrophage colony-stimulating factor involved
3
in generation of IgE, eosinophilia, and allergic inflammation. Gain-of-function mutations in the alpha subunit of the IL-4 receptor, IL-4, and IL-13 has been significantly associated with AD, providing a rationale for the use of biologicals that interfere with the IL-4 receptor signaling pathway.30 A significant association has also been observed between TSLP gene polymorphisms and AD supporting further evidence for the importance of Th2 polarization in this disease.53
IMMUNOPATHOLOGY OF ATOPIC DERMATITIS
IMMUNOPATHOLOGY OF
ATOPIC DERMATITIS
Based on clinical appearance and duration of illness, AD skin can be characterized as nonlesional AD, acute AD lesions (3 or fewer days after onset), and chronic skin lesions (>3 days’ duration). Nonlesional AD skin may not be normal but characterized by mild epidermal hyperplasia and a sparse perivascular T-cell infiltrate. Dendritic antigen-presenting cells (eg, Langerhans cells (LCs), inflammatory dendritic epidermal cells [IDECs], macrophages) in lesional and, to a lesser extent, in nonlesional skin of AD exhibit surface-bound immunoglobulin E molecules. In acute lesions, there is epidermal spongiosis with an increased infiltration of activated memory T cells bearing the skin-homing CLA. Eosinophils, basophils, and neutrophils are rare. Mast cells are in various stages of degranulation. Chronic lichenified lesions are characterized by a hyperplastic epidermis with elongation of the rete ridges, prominent hyperkeratosis, and minimal spongiosis. There is an increased number of IgE-bearing LCs and in the epidermis, and macrophages dominate the dermal mononuclear cell infiltrate. Mast cells are increased in number but are fully granulated. Neutrophils are absent in AD skin lesions even in the setting of increased S. aureus colonization and infection. Increased numbers of eosinophils are observed in chronic AD skin lesions. Eosinophils are thought to contribute to allergic inflammation by the secretion of cytokines and mediators that augment allergic inflammation and induce tissue injury in AD through the production of reactive oxygen intermediates and release of toxic granule proteins.
CYTOKINE-DRIVEN ATOPIC DERMATITIS SKIN INFLAMMATION
CYTOKINE-DRIVEN
ATOPIC DERMATITIS SKIN
INFLAMMATION
Atopic skin inflammation is orchestrated by the local expression of proinflammatory cytokines.47 A key difference between epidermal keratinocytes found in AD, as compared with normal, skin is the presence of thymic stromal lymphopoietin (TSLP) and IL-33 in AD epidermis. TSLP, along with IL-33, are key cytokines secreted by epithelial cells that induce dendritic
369
3
cells to drive Th0 cells into the Th2 cell differentiation pathway. Nonlesional AD and acute AD skin lesions are predominantly associated with expression of IL-4, IL-5, IL-13, IL-25, IL-31, and IL-33 expression. These type 2 cytokines are present in all stages of AD and can be secreted by multiple cell types, including innate lymphoid type 2 cells, mast cells, and basophils, present in AD skin lesions. This contributes to substantial redundancy in allergic inflammation. As such, cytokine targeting, as opposed to cell targeting, is considered a more effective approach in the treatment of AD. The importance role of type 2 cytokines is that, in animal models, they can recapitulate elevated IgE responses, eosinophilia, skin barrier dysfunction, allergic skin inflammation, and itching observed in clinical AD. Aside from Th2, other cytokine pathways are also activated during the evolution of AD. The IL-22–IL-17 pathway is of particular interest because it, along with IL-4 and IL-13, can inhibit terminal keratinocyte differentiation, including filaggrin expression. Because dendritic cell–derived, IL-23, enhances IL-22–IL-17 cell differentiation, all of these cytokines are being closely examined for their potential role in AD. It is interesting that IL-4 and IL-13 can enhance IL-23 production by dendritic cells. Furthermore, blockade of IL-4 and IL-13 pathway, leading to improvement in AD, is also associated with reduced IL-23 and IL-17 expression in AD skin.54
When acute AD become chronic AD skin lesions, there is an increase in Th1 cytokines such as INF-γ, which potentiates AD skin inflammation. It is noteworthy that experimental studies demonstrate pretreatment with IL-4 and IL-13 dampens responses to interferons and IL-17, suggesting that when the early AD lesion is exposed to IL-4 and IL-13, there is a long-lasting, persistent effect. A recent birth cohort study, however, demonstrated that TSLP could be detected in at-risk infants before the onset of AD, suggesting that the TSLP–Th2- ILC2 pathway plays a critical role in initiation of AD.55 In chronic AD, there is an increased in IL-5, which is involved in eosinophil development and survival. The skin-specific chemokine, cutaneous T cell– attracting chemokine (CTACK; CC chemokine ligand 27 [CCL27]), is highly upregulated in AD and preferentially attracts skin homing cutaneous lymphoid antigen (CLA)+ CC chemokine receptor 10+ (CCR10+) T cells into the skin. CCR4 expressed on skin homing CLA+ T cells can also bind to CCL17 on the vascular endothelium of cutaneous venules. Selective recruitment of CCR4-expressing Th2 cells is mediated by macrophage-derived chemokine and thymus and activation-regulated cytokine, both of which are increased in AD. The severity of AD has been linked to the magnitude of thymus and activation-regulated cytokine levels. In addition, chemokines such as fractalkine, IFN-γ–inducible protein 10, and monokine induced by IFN-γ are strongly upregulated in keratinocytes and result in Th1-cell migration toward epidermis, particularly in chronic AD. Increased expression of the CC chemokines, macrophage chemoattractant protein-4, eotaxin, and RANTES (regulated on activation normal T-cell expressed and secreted) contribute
370
to infiltration of macrophages, eosinophils, and T cells into both acute and chronic AD skin lesions.
IMMUNE EFFECTS ON EPITHELIAL DIFFERENTIATION COMPLEX
IMMUNE EFFECTS
ON EPITHELIAL
DIFFERENTIATION COMPLEX
The dry skin and increased transepidermal water loss in individuals with AD reflect the underlying skin barrier dysfunction and loss of natural moisturizing factors that play an important role in the pathogenesis of AD.47 Only a minority of patients, however, have FLG null mutations. Other genetic variants in the EDC and tight junctions are even rarer. The majority of patients with AD likely have immune-mediated reduction in epidermal terminal differentiation, leading to decreased generation of various epidermal structural proteins, filaggrin breakdown products, epidermal lipids, and antimicrobial peptides. TSLP, IL-4, and IL-13 are the most potent cytokines downregulating filaggrin expression by keratinocytes. IL-17, IL-22, IL-25, and IL-33 can act synergistically with IL-4 and IL-13 to further downregulate expression of epidermal proteins and lipids. This combination of events along with activation of proteases and lipases creates defective epidermal barrier function and alters epidermal acidification and loss of moisturization in AD, thereby contributing to enhanced allergen and microbial penetration met by the host immune response and clinical appearance of AD. The critical role for immune activation in driving AD pathogenesis is supported by the observation that cyclosporin is highly effective in controlling severe AD and reverses the epidermal pathology.56 Clinical studies demonstrating that blockade of IL-4 and IL-13 immune pathways is highly effective in reversing severe AD provides definitive data that in the majority of patients, cytokine activation drives atopic inflammation. Recent studies showing AD immune activation may differ in various races and according to age group suggests the importance of more precise stratification of immune responses with clinical AD subsets.51
BASIS OF PRURITUS IN ATOPIC DERMATITIS
BASIS OF PRURITUS IN
ATOPIC DERMATITIS
Pruritus is a prominent feature of AD, manifested as cutaneous hyperreactivity and scratching after exposure to allergens, changes in humidity, excessive sweating, and low concentrations of irritants. Control of pruritus is important because mechanical injury from scratching can induce proinflammatory cytokine and chemokine release, leading to a vicious scratch–itch cycle, perpetuating the AD skin rash. The mechanisms of pruritus in AD are poorly understood. Allergen-induced release of histamine from skin mast cells is not an exclusive cause of pruritus in AD because H1 antihistamines do not appear to control the
itch of AD.57,58 Recent studies demonstrating a potential role for H4 receptors in skin pathobiology, however, suggests that histamine may play a contributory role. The observation, however, that treatment with topical corticosteroids (TCs) and calcineurin inhibitors is effective at reducing pruritus suggests that the inflammatory cells play an important role in pruritus. Molecules that have been implicated in pruritus include T cell–derived cytokines such as IL-31, stress-induced neuropeptides, proteases such as proteases that can act on protease-activated receptors, eicosanoids, and eosinophil-derived proteins.
DIAGNOSIS
The diagnosis of AD is based on a clinical assessment and guided by the criteria discussed previously. A diagnosis of AD is made only after other conditions such as psoriasis, scabies infestation, seborrheic dermatitis, or contact dermatitis have been considered and ruled out, if necessary, with additional testing. AD not responding to routine skin care or topical antiinflammatory therapy or skin lesions that are atypical in morphology or distribution should prompt the clinician to consider additional diagnoses such as T-cell lymphoma, nutritional deficiencies, or metabolic syndromes. Patients with a history of sinopulmonary infections, severe skin infections, erythroderma, or failure to thrive should be evaluated for immunodeficiency syndromes.
SUPPORTIVE STUDIES
SUPPORTIVE STUDIES
LABORATORY TESTING
Routine potassium hydroxide microscopic evaluation can be used to rule out cutaneous fungal infections that may mimic AD. Mineral oil examination for scabies is warranted if burrows are present or vesicles are present on the palms and soles in infants. If the clinical picture suggests allergic contact dermatitis may be present (eg, atypical distribution, refractory disease), patch testing is warranted. Atopic dermatitis guidelines of care from the American Academy of Dermatology do not recommend routine allergy testing for AD because many patients with AD have detectable antigen-specific IgE to foods and airborne and environmental allergens, especially those with severe disease.59 History-directed skin prick testing or serum-specific IgE antibody testing may be performed to confirm a true type I food allergy if a patient reports a history of immediate-type hypersensitivity symptoms (eg, urticaria, lip swelling, abdominal pain). The Food Allergy Expert Panel sponsored by the National Institute of Allergy and Infectious Disease defined allergy as an “adverse health event”; thus, patients should not be labeled as “allergic” solely based on sensitization alone.60 In patients with AD, positive allergy test results (in the absence of controlled food challenges) poorly predict true type I allergic responses.61 There remains limited
3
evidence that removal of allergens from the diet or environment improves AD outcomes.62,63 Thompson and Hanifin noted that proper AD control with routine therapy reduces parental concern regarding diet as a contributory factor in AD.64 The Food Allergy Expert Panel suggests that children younger than 5 years old with moderate to severe AD be considered for food allergy evaluation for milk, egg, peanut, wheat, and soy if at least one of the following conditions is met: (1) the child has persistent AD despite optimized management and topical therapy or (2) the child has a reliable history of an immediate reaction after ingestion of a specific food.60
Laboratory studies to rule out immunodeficiency associated with eczema include a complete blood count with differential for white blood cell count; lymphocyte phenotyping for T cells, B cells, and natural killer cells; and lymphocyte proliferation assays as well as genomic DNA analysis for pathogenic variants in genes resulting in severe combined deficiency (eg, IL2RG, ADA, IL7R), Omenn syndrome (hypomorphic mutations in RAG1/RAG2 genes) or hyper-IgE (HIE) syndrome (eg, STAT3, DOCK8, SPINK5, TYK2). Small platelets seen on peripheral blood smear are characteristic of Wiskott-Aldrich syndrome. Both elevated serum IgE levels and elevated circulating blood eosinophils can be seen in a number of diseases besides AD, including HIE syndrome but also some immunodeficiencies. Zinc levels to rule out zinc deficiency should be obtained on fasting morning blood and corrected for any concomitant low albumin level.
PATHOLOGY
Biopsy of AD lesions with hematoxylin and eosin staining (Table 22-2) will not allow differentiation among various eczematous processes such as nummular dermatitis or allergic contact dermatitis because all eczematous processes show spongiotic dermatitis on histopathology. Biopsy is helpful to rule out cutaneous T-cell lymphomas (see Chap. 119) and should reveal epidermotropic neoplastic T cells with hyperconvoluted cerebriform nuclei and intraepidermal Pautrier microabscess formation. T-cell receptor gene rearrangement studies will demonstrate clonal rearrangement. Biopsies may not be diagnostic for Sézary syndrome, and diagnostic criteria include an absolute Sezary cell count of 1000 cells/mm3 or greater in peripheral blood, increased CD4/CD8 ratio greater than 10 on flow cytometry analysis, or circulating T-cell clone detected by cytogenetic methods. Histopathology of psoriasis shows characteristic changes that depend on the stage of evolving lesion—initial, developing, or mature (see Chap. 28).
IMAGING
Imaging is not recommended in AD diagnosis except when ruling out specific immunodeficiencies. Chest radiographs will reveal an absent thymus in most forms of severe combined immunodeficiency as well as pulmonary infiltrates from infectious complications.
371
3
NONLESIONAL ATOPIC DERMATITIS ACUTE ATOPIC DERMATITIS (<3 DAYS) CHRONIC SKIN LESIONS (>3 DAYS)
Spongiosis
Mild epidermal hyperplasia, sparse perivascular infiltrate Epidermal spongiosis, increased inflammatory infiltrate Hyperplastic epidermis with elongated rete ridges, prominent hyperkeratosis, minimal spongiosis
Langerhans cells, inflammatory dendritic
Mast cells (degranulating); rare
Langerhans cells, mast cells (fully granulated),
Langerhans cells, inflammatory dendritic epidermal cells, macrophages Mast cells (degranulating); rare eosinophils, basophils, and neutrophils Langerhans cells, mast cells (fully granulated), neutrophils absent, increased eosinophils
epidermal cells, macrophages
eosinophils, basophils, and neutrophils
Chest radiographs or computed tomography scans may reveal extensive infiltrates, cyst-forming pneumonias, and occasionally fungal lesions in HIE syndrome.
DIFFERENTIAL DIAGNOSIS
Because AD is currently not defined by a unique diagnostic biomarker, a number of inflammatory skin diseases, immunodeficiencies, skin malignancies, genetic disorders, infectious diseases, and infestations may share symptoms and signs with AD (Table 22-3). These should be considered in the initial evaluation of a patient presenting with an eczematous rash but also if a patient with a diagnosis of AD is not responding to appropriate therapy. Infants presenting in the first year of life with failure to thrive, diarrhea, a generalized scaling erythematous rash, and recurrent cutaneous or systemic infections should be evaluated for severe combined immunodeficiency syndrome. Omenn syndrome, caused by mutations in RAG1 and RAG2 as well as several other genes, is an autosomal recessive severe combined immunodeficiency that can present with an erythrodermic rash, as well as elevated IgE, eosinophilia, diarrhea, lymphadenopathy, hepatosplenomegaly, and susceptibility to infections.65 The dermatitis can be eczematous though with pachydermia. Other immunodeficiency with eczematous rash includes immune dysregulation, polyendocrinopathy, enteropathy X-linked (IPEX) syndrome.66 IPEX results from mutations of Foxp3, a gene located on the X chromosome that encodes a DNA-binding protein required for development of regulatory T cells. Besides dermatitis, patients typically present with a recalcitrant enteropathy, as well as autoimmune features such as type 1 diabetes, thyroiditis, hemolytic anemia, or thrombocytopenia. Wiskott-Aldrich syndrome is an X-linked recessive disorder characterized by an eczematous rash associated with thrombocytopenia along with
372
neutrophils absent, increased eosinophils
variable abnormalities in humoral and cellular immunity and severe bacterial infections. Hyper-IgE syndrome caused by STAT3 mutations is an autosomal dominant multisystem disorder characterized by recurrent deep-seated bacterial infections, including cutaneous cold abscesses and pneumonias with pneumatocele formation due to S. aureus.67 Although S. aureus is an important pathogen in this disorder, infection with other bacteria, including gramnegative species (eg, Pseudomonas aeruginosa) and nontuberculous mycobacteria and fungi (eg, Aspergillus) may occur, including invasive disease. STAT3 is an essential transcription factor for Th17 T-cell development, and because Th17 T cells play an essential role in protecting against Candida spp., patients with mutations in STAT3 are susceptible to chronic mucocutaneus candidiasis. In infancy, patients may present with a papulopustular eruption of the face and scalp. Other features of HIE syndrome include skeletal abnormalities with coarse facial features and prominent frontal bossing, dental anomalies with retained primary teeth, bone fractures, and osteoporosis. Despite elevated serum IgE levels, patients usually are not atopic. Patients with mutations in the gene encoding dedicator of cytokinesis 8 protein (DOCK8) have an immunodeficiency that accounts for most cases of autosomal recessive HIE.68 These patients have an eczematous dermatitis with recurrent viral infections, including some with central nevous system involvement. Patients may present with recalcitrant warts secondary to human papilloma virus, disseminated molluscum or recurrent herpes simplex infections. Malignancies, including squamous cell carcinomas and lymphomas, are an important cause of death in patients starting in the second decade of life. Another unique feature in patients with DOCK8 is that many have associated food allergies. Patients with tyrosine kinase 2 deficiency can also present with an eczematous rash with high serum IgE and recurrent cutaneous staphylococcal infections.69
Most Likely Contact dermatitis (allergic and irritant) Seborrheic dermatitis Scabies Psoriasis Ichthyosis vulgaris Keratosis pilaris Dermatophytosis
Consider Asteatotic eczema Lichen simplex chronicus Nummular dermatitis Juvenile palmar-plantar dermatosis Impetigo Drug eruptions Perioral dermatitis Pityriasis alba Photosensitivity disorders (hydroa vacciniforme, polymorphous light eruption, porphyrias) Molluscum dermatitis
Less Common or Rare Disorders Predominant in Adolescents and Adults Cutaneous T-cell lymphoma (mycosis fungoides or Sézary syndrome) Human immunodeficiency virus–associated dermatosis Lupus erythematosus Dermatomyositis Graft-versus-host disease Pemphigus foliaceus Dermatitis herpetiformis Photosensitivity disorders (hydroa vacciniforme, polymorphous light eruption, porphyrias)
Less Common or Rare Disorders Predominant in Infants and
Less Common or Rare Disorders Predominant in Infants and Children Metabolic or Nutritional Phenylketonuria Prolidase deficiency Multiple carboxylase deficiency Zinc deficiency (acrodermatitis enteropathica, prematurity, deficient breast milk zinc, cystic fibrosis) Others: biotin, essential fatty acids, organic acidurias Primary Immunodeficiency Disorders
Children Metabolic or c Nutritional Phenylketonuria Prolidase deficiency Multiple carboxylase deficiency Zinc deficiency (acrodermatitis enteropathica, prematurity, deficient breast milk zinc, cystic fibrosis)
Others: biotin, essential fatty acids, organic acidurias Primary Immunodeficiency Disorders
Other diseases to consider in the differential diagnosis of AD include cutaneous T-cell lymphoma, especially in adults without a history of childhood eczema and without other atopic features.70 Mycosis fungoides (discussed in Chap. 119) is the most common form of CTCL, Sézary syndrome is characterized by generalized erythroderma with lymphadenopathy and circulating malignant T cells (Sézary cells). Although contact dermatitis should be considered in the differential diagnosis of AD (see Chap. 24), contact allergy can also complicate AD, especially in patients whose AD appears to worsen with therapy, typically with TCs.71 Allergic contact dermatitis complicating AD may appear as an acute flare of the underlying disease. Eczematous dermatitis has been also reported with human immunodeficiency virus infection as well as with a variety of infestations such as scabies. Other diseases that can be
3
confused with AD include psoriasis, ichthyoses, and seborrheic dermatitis. Although psoriasis can typically be distinguished from AD based on characteristic clinical features (see Chap. 28), inverse (flexural) psoriasis or erythrodermic psoriasis may at times present more of a diagnostic challenge. Zinc deficiency can result from dietary deficiency; excessive losses with diarrhea; or chronic disease, including renal or hepatic as well as inadequate absorption associated with an inherited deficiency of the zinc carrier protein ZIP4 and can present with an eczematous rash with a perioral, acral, or perineal distribution.72
CLINICAL COURSE AND PROGNOSIS
Most AD starting in childhood is mild in severity, and a review of birth cohort studies found that 80% of cases remitted, at least temporarily, by 10 years of age.73
Symptoms of AD, however, may persist or reemerge in adulthood. One primarily pediatric AD cohort found that more than 80% of patients prescribed calcineurin inhibitors reported persistent symptoms into adulthood.74 Risk factors reported to be predictive of a persistent disease course include disease severity, later onset disease, genetic mutations in FLG or FLG-2 genes, and early allergic sensitization.75,76 It is not known whether early or aggressive treatment of AD alters the natural course. For occupational counseling, adults whose childhood AD has been in remission for a number of years may present with hand dermatitis, especially if daily activities require repeated hand wetting.
MANAGEMENT
OVERVIEW
OVERVIEW
Successful treatment of AD requires a systematic, multipronged approach that incorporates education about the disease state, skin hydration, pharmacologic therapy, and the identification and elimination of flare factors such as irritants, allergens, infectious agents, and emotional stressors (Fig. 22-7). Many factors lead to the symptom complex characterizing AD. Thus, treatment plans should be individualized to address each patient’s skin disease reaction pattern, including the acuity of the rash, and the trigger factors that are unique to the particular patient. In patients refractory to conventional forms of therapy, alternative antiinflammatory and immunomodulatory agents may be necessary.
EDUCATION AS INTERVENTION
EDUCATION AS
INTERVENTION
Education may be considered as a therapeutic intervention for the management of atopic dermatitis.77
373
3
Approach to patient with atopic dermatitis
Patient presents with history of pruritic dermatitis
Patient meets Hanifin and Rajka criteria for diagnosis of ADa
General skin care measures:
• Education
• Appropriate skin hydration and use of emollients or skin barrier repair measures
• Avoidance of irritants
• Identification and avoidance of proven allergens
• Antiinflammatory therapy topical steroids, topical calcineurin inhibitorsb, topical PDE4 inhibitor
• Antipruritic interventions (sedating antihistamines, behavioral modification)
• Identification and treatment of complicating bacterial, viral, or fungal infections
• Treatment of psychosocial aspects of disease
• Evaluation for other conditions
Successful outcome?
• Reassess diagnosis of AD
• Consider role of unrecognized infectious agents, allergens, and so on
• Consider poor understanding or nonadherence with treatment plan
• Titration of topical therapy using emollients and skin barrier repair measures, topical steroids, topical calcineurin inhibitors or topical PDE4 inhibitors, as needed intermittently
aSee Table 22-1. bSecond-line therapy per boxed warning.
Successful outcome?
• Consultation with AD specialist
• Consider skin biopsy
• Consider hospitalization
• Consider systemic therapy with FDA-approved biologic (dupilumab) or nonapproved systemic immunosuppressants or UV therapy
Intensive disease education has been shown in randomized, controlled trials to improve subjective quality-of-life and objective eczema severity scores.78 Intensive education may include comprehensive “center-based” patient/family teaching, written “handouts” and care plans, patient and family support groups, and internet-accessed media. Several resources available online are listed in Table 22-4.
374
IDENTIFICATION AND ELIMINATION OF TRIGGERS
IDENTIFICATION AND
ELIMINATION OF TRIGGERS
GENERAL CONSIDERATIONS
Patients with AD are more susceptible to irritants than are unaffected individuals. Thus, it is important to identify and eliminate aggravating factors that trigger
Coping Strategies and Support Groups National Eczema Association (www.nationaleczema.org) Under My Skin: A Kid’s Guide to Atopic Dermatitis (www.undermyskin.com)
Specialized Atopic Dermatitis Care American Academy of Dermatology EczemaNet (www.skincarephysicians.com/eczemanet/index.html) The Eczema Center at Rady Children’s Hospital (www.eczemacenter.org) National Jewish Health (www.njc.org) Northwestern University Eczema Care and Education Center (www.eczemacarecenter.com)
Information on Allergic Triggers
Information on Allergic Triggers American Academy of Allergy, Asthma & Immunology (www.aaaai.org) Food Allergy & Anaphylaxis Network (www.foodallergy.org)
American Academy of Allergy, Asthma & Immunology (www.aaaai.org) Food Allergy & Anaphylaxis Network (www.foodallergy.org)
the itch–scratch cycle. These include soaps or detergents, contact with chemicals, smoke, abrasive clothing, and exposure to extremes of temperature and humidity. Alcohol and astringents found in toiletries are drying. When soaps are used, they should have minimal defatting activity and a neutral pH or slightly acidic pH. New clothing may be laundered before wearing to decrease levels of formaldehyde and other added chemicals. Residual laundry detergent in clothing may be irritating. Using a liquid rather than powder detergent and adding a second rinse cycle facilitate removal of the detergent. Recommendations regarding environmental living conditions should include temperature and humidity control to avoid problems related to heat, humidity, and perspiration. Every attempt should be made to allow children to be as normally active as possible. Certain sports, such as swimming, may be better tolerated than other sports involving intense perspiration, physical contact, or heavy clothing and equipment. Although UV light may be beneficial to some patients with AD, sunscreens should be used to avoid sunburn. However, because sunscreens can be irritants or allergens, care should be used to identify a nonirritating product.
SPECIFIC ALLERGENS
Foods and aeroallergens such as dust mites, animal danders, molds, and pollens have been demonstrated to exacerbate AD in some patients. In patients not responding to routine skin care and topical antiinflammatory therapies, potential allergens can be identified by taking a careful history, looking for immediate or anaphylactic clinical reactions that may trigger the itch–scratch cycle, and carrying out selective skinprick tests or specific serum IgE levels. Negative skin test results or serum test results for allergenspecific IgE have a high predictive value for ruling out
3
suspected allergens. Positive allergy testing results, on the other hand, poorly predicts adverse clinical reactions. Fleischer and colleagues performed food challenges on 125 children with AD who were labeled as having food allergy by allergy testing.61 After oral food challenge, 84% to 93% of the foods being avoided were returned to the children’s diet, when no immediate reactions were observed. Elimination diets, which in some cases can be nutritionally deficient, are rarely, if ever, required. Even in patients with multiple positive skin test results, the majority of patients react to three or fewer foods on controlled challenge. In dust mite–allergic patients with AD, prolonged avoidance of dust mites has not been consistently found to result in improvement of their skin disease.63 Avoidance measures include use of dust mite–proof encasings on pillows, mattresses, and box springs; washing bedding in hot water weekly; removing bedroom carpeting; and decreasing indoor humidity levels with air conditioning. Because there are many triggers contributing to the flares of AD, attention should be focused on identifying and controlling the flare factors that are important to the individual patient. Whereas infants and young children are more likely to have food allergies, older children and adults are more likely to be sensitive to environmental aeroallergens. Contact allergens have been increasingly recognized in AD. One study found that of children with relevant positive reactions, 34% had a diagnosis of AD.77
EMOTIONAL STRESSORS
Although emotional stress does not cause AD, patients often report it exacerbates the illness. AD patients often respond to frustration, embarrassment, or other stressful events with increased pruritus and scratching. Psychological evaluation or counseling should be considered in patients who have difficulty with emotional triggers or concomitant metal health conditions or symptoms contributing to difficulty in managing their disease. It may be especially useful in adolescents and young adults who consider their skin disease disfiguring. Relaxation, behavioral modification, or biofeedback may be helpful in patients with habitual scratching.58
INFECTIOUS AGENTS
Antistaphylococcal antibiotics are often needed in the treatment of patients who are infected with S. aureus. Cephalosporins or penicillinase-resistant penicillins (dicloxacillin, oxacillin, or cloxacillin) are usually beneficial for patients who are not colonized with resistant S. aureus strains. Because erythromycin-resistant Staphylococci are common, erythromycin and newer macrolide antibiotics are usually of limited utility. Topical antimicrobials such as mupirocin, fusidic acid, or more recently retapamulin offers some utility in the treatment of impetiginized lesions. A Cochrane analysis of interventions for impetigo found that topical
375
3
mupirocin and topical fusidic acid are equal to or more effective than oral treatment for patients with limited disease and that fusidic acid and mupirocin are of similar efficacy.79 Patients should be cautioned against using topical antibiotics in an “as-needed” manner that can lead to resistant organisms. Use of neomycin topically can result in development of allergic contact dermatitis because neomycin is among the more common allergens causing contact dermatitis. In patients with extensive superinfection, a course of systemic antibiotics is most practical. MRSA may require culture and sensitivity testing to assist in appropriate antibiotic selection. Baths with dilute sodium hypochlorite (bleach) may also benefit AD patients with superinfected eczema, especially those with recurrent MRSA, although they can occasionally be irritating. Of note, a controlled study of twiceweekly bleach baths for 3 months showed clinical benefit, although skin colonization by S. aureus did not disappear even when combined with intranasal mupirocin 5 days each month.80 Bleach baths may exert their beneficial effect on AD via antiinflammatory mechanisms rather than antimicrobial ones.81
Herpes simplex can provoke recurrent dermatitis and may be misdiagnosed as S. aureus infection or severe eczema. The presence of punched-out erosions, vesicles, or infected skin lesions that do not respond to oral antibiotics should initiate a search for herpes simplex. This can be diagnosed by polymerase chain reaction identification of herpes genetic material, Giemsa-stained Tzanck smear, or direct immunofluorescence of cells scraped from the vesicle base or viral culture. Antiviral treatment for cutaneous herpes simplex infections is of critical importance in the patient with widespread AD because life-threatening dissemination has been reported (EH). Acyclovir, 400 mg three times daily for 10 days or 200 mg four times daily for 10 days by oral administration (or an equivalent dosage of one of the newer antiherpetic medications), is useful in adults with herpes simplex confined to the skin. Intravenous treatment may be necessary for severe disseminated EH. The dosage should be adjusted according to weight in children. Dermatophyte infections can complicate AD and may contribute to exacerbation of disease activity. Patients with dermatophyte infection or IgE antibodies to Malassezia spp. may benefit from a trial of topical or systemic antifungal therapy, although high-quality controlled studies are lacking.
PRURITUS
PRURITUS
The treatment of pruritus in AD should be directed primarily at the underlying causes. Reduction of skin inflammation and dryness with topical glucocorticoids or nonsteroidal antiinflammatory drugs (NSAIDs) and skin hydration, respectively, often symptomatically reduce pruritus. Inhaled and ingested allergens should be eliminated if documented to cause an urticarial skin rash in controlled challenges. Systemic antihistamines
376
act primarily by blocking the H1 receptors in the dermis, thereby ameliorating histamine-induced pruritus. However, histamine is not the primary mediator of itch in AD skin, thus the relative lack of convincing evidence that antihistamines improve pruritus in AD.80
Some antihistamines are also mild anxiolytics and may offer symptomatic relief through tranquilizing and sedative effects. Studies of newer, nonsedating antihistamines show variable results in the effectiveness of controlling pruritus in AD, although they may be useful in the subset of AD patients with concomitant urticaria or concurrent allergic rhinitis. Because pruritus is usually worse at night, the sedating antihistamines, for example, hydroxyzine or diphenhydramine, may offer an advantage with their soporific side effects when used at bedtime. Doxepin hydrochloride has both tricyclic antidepressant and H1- and H2-histamine receptor-blocking effects. It can be used in doses of 10 to 75 mg orally at night or up to 75 mg twice daily in adult patients. If nocturnal pruritus remains severe, short-term use of a sedative or melatonin to allow adequate rest may be appropriate for some patients.82 Treatment of AD with topical antihistamines is generally not recommended because of potential cutaneous sensitization. However, shortterm (1-week) application of topical 5% doxepin cream has been reported to reduce pruritus without sensitization. Of note, sedation is a side effect of widespread application of doxepin cream, and allergic contact dermatitis has been reported.
TOPICAL THERAPY
TOPICAL THERAPY
EMOLLIENTS
Emollients represent the cornerstone of treatment for mild AD and serve as an important flare preventive therapy for all levels of disease severity. Patients with AD have abnormal skin barrier function with increased transepidermal water loss and decreased water content and dry skin (xerosis) contributing to disease morbidity by the development of microfissures and cracks in the skin. These microfissures may serve as portals of entry for skin pathogens, irritants, and allergens. FLG gene mutations or acquired filaggrin protein deficiencies caused by inflammation have also been shown to result in decreased epidermal levels of natural moisturizing factor.83 AD xerosis can become aggravated during the dry winter months and in certain work environments. The daily use of an effective emollient helps to restore and preserve the stratum corneum barrier, decreases the need for topical glucocorticoids and NSAIDs and improves outcomes. Moisturizers are available in the form of lotions, creams, or ointments. Some lotions and creams may be irritating because of added preservatives, solubilizers, and fragrances. Lotions with high water content may be drying because of an evaporative effect and provide few lipids to the skin. Thicker, bland emollients with high lipid content are preferred but are
sometimes not well tolerated because of interference with the function of the eccrine sweat ducts and the induction of folliculitis or itching. In these patients, less occlusive agents should be used. Plain petrolatum is a common lipid base for effective emollients. Petrolatum intercalates into the stratum corneum and appears to upregulate skin barrier and antimicrobial peptide gene expression thought to be beneficial in AD.84 The benefit of emollients with special additives, such as ceramides, is not clear, although one study found the use of a urea-containing moisturizer provided better clinical results than a standard emollient.85
Hydration, by baths or wet dressings, promotes transepidermal penetration of topical glucocorticoids. The optimal bathing regimen for patients with AD is not known, however, and recommendations vary by specialty. Kohn and colleagues found no differences in outcomes in patients applying TCs to wet skin compared with dry skin,86 but the “soak and smear” method is often used in recalcitrant disease.87 Wet dressings or “wet wraps” are recommended for use on severely affected or chronically involved areas of dermatitis refractory to therapy. However, overuse of wet dressings may result in maceration of the skin complicated by secondary infection. Wet dressings or baths also have the potential to promote drying and fissuring of the skin if not followed by topical emollient use. Thus, wet dressing therapy is reserved for poorly controlled AD and should be closely monitored by a physician.
TOPICAL ANTIINFLAMMATORY THERAPY Topical Corticosteroids: According to AD treatment guidelines, TCs are the cornerstone of antiinflammatory treatment in AD.88 Because of potential side effects, many health care practitioners use topical glucocorticoids only to control acute exacerbations of AD. However, studies suggest that after control of AD is achieved with a daily regimen of topical glucocorticoid, long-term control can be maintained in a subset of patients with scheduled intermittent applications of TCs, such as twice-weekly fluticasone, to areas that have healed but are prone to developing eczema.89
Patients should be carefully instructed in the use of topical glucocorticoids to avoid potential side effects. The potent fluorinated glucocorticoids should be avoided on the face, the genitalia, and the intertriginous areas. A low-potency glucocorticoid preparation is generally recommended for these areas and only used intermittently for long-term use. Patients should be instructed to apply topical glucocorticoids to their skin lesions and to use emollients on uninvolved skin. Failure of a patient to respond to topical glucocorticoids is sometimes partly caused by an inadequate supply or inadequate quantity of use. It is important to remember that it takes approximately 30 g of cream or ointment to cover the entire skin surface of an adult once. To treat the entire body twice daily for 2 weeks requires approximately 840 g (2 lb) of topical glucocorticoids.
3
There are seven classes of topical glucocorticoids, ranked according to their potency based on vasoconstrictor assays. Because of their potential side effects, the ultrahigh-potency glucocorticoids should be used daily or twice daily only for very short periods of time (usually 2 weeks) and in areas that are lichenified but not on the face or intertriginous areas. Midpotency glucocorticoids can be used for longer periods of time to treat chronic AD involving the trunk and extremities. Newer formulations of topical steroids include gel formulations without alcohol bases that moisturize skin, and solutions, oils, foams, and shampoos that may be useful on hair-bearing surfaces. Factors that influence topical glucocorticoid potency and the risk of side effects include the molecular structure of the compound, the vehicle, the amount of medication applied, the duration of application, and occlusion, as well as host factors, including age, body surface area and weight, skin inflammation, anatomic location of treated skin, and individual differences in cutaneous or systemic metabolism. Side effects from topical glucocorticoids are directly related to the potency ranking of the compound and the length and frequency of use, so it is incumbent on the clinician to balance the need for a more potent steroid with the potential for side effects. In addition, ointments have a greater potential to occlude the epidermis, resulting in enhanced systemic absorption when compared with creams. Side effects from topical glucocorticoids can be divided into local side effects and systemic side effects resulting from suppression of the hypothalamic– pituitary–adrenal axis. Local side effects include the development of striae, skin atrophy, perioral dermatitis, and acne rosacea. Prolonged daily use of TCs, especially on the face, can also lead to steroid withdrawal syndrome, a condition characterized by severe erythema, swelling, and burning upon TC discontinuation.90 The potential for potent topical glucocorticoid to cause adrenal suppression is greatest in infants and young children. Several topical steroid formulations have been specifically tested for safety and received specific U.S. Federal Drug Administration (FDA) approval for use in younger children such as desonide hydrogel and nonethanolic foam, fluocinolone acetonide oil, and fluticasone 0.05% cream. Mometasone cream and ointment are approved for children aged 2 years and older. Because normal-appearing skin in AD shows evidence of immunologic dysregulation and inflammation, the use of TCs as maintenance therapy to normal-appearing skin has been reported in several controlled studies.91 After control of AD with a oncedaily regimen was achieved, long-term control could be maintained with twice-weekly application of fluticasone to previously involved areas. Given recent insights into skin barrier and immunologic abnormalities and colonization of normal-appearing skin in AD by S. aureus, it is important to appreciate that “proactive therapy” is an attempt to control residual disease, not just application of an active drug to unaffected skin.
377
3
Topical Calcineurin Inhibitors: Topical tacrolimus and pimecrolimus have been developed as nonsteroidal immunomodulators.68 Tacrolimus ointment 0.03% has been approved for intermittent treatment of moderate to severe AD in children aged 2 years and older, with tacrolimus ointment 0.1% approved for use in adults and children 16 years and older; pimecrolimus cream 1% is approved for treatment of patients aged 2 years and older with mild to moderate AD. Both drugs have proven to be effective with a good safety profile for treatment up to 4 years with tacrolimus ointment and up to 2 years with pimecrolimus cream. A frequently observed side effect with topical calcineurin inhibitors (TCIs) is a transient burning sensation of the skin. Importantly, treatment with TCIs is not associated with skin atrophy; thus, they are particularly useful for the treatment of areas such as the face and intertriginous regions. Three-times-weekly “proactive” maintenance therapy using tacrolimus ointment has also been reported in both adults and children with AD.92
Ongoing surveillance and recent reports have not shown a trend for increased frequency of viral superinfections, especially EH. TCIs carry an FDA black box warning for rare cases of skin malignancy and lymphoma have been reported with topical tacrolimus, although a systematic literature review showed a slightly higher risk of lymphoma in patients with AD, with severity appearing to be a risk factor but concluding that TCIs are unlikely to be a significant factor.93
Importantly, a case-control study of a large database that identified a cohort of 293,253 patients with AD found no increased risk of lymphoma with the use of TCIs.93 Margolis and colleagues found no increase in malignancy incidence rates with pimecrolimus cream in a study evaluating more than 26,000 person-years.94
Crisaborole: Crisaborole is a boron-based topical phosphodiesterase 4 (PDE4) inhibitor recently approved for the treatment of mild to moderate AD in patients older than the age of 2 years. PDE4 inhibition is thought to decrease proinflammatory cytokine production by key immune cells that drive chronic inflammatory skin disease. Two identically designed pivotal phase 3 trials revealed crisaborole 2% ointment resulted in clear or almost clear disease (plus a two-step improvement) in 31.4% to 32.8% in the active group compared with 18.0% to 25.4% in the vehicle control groups with these differences being statistically significant.95 No significant adverse events emerged with 4% of patients experiencing burning. Crisaborole represents a safe and efficacious novel nonsteroidal option for the treatment of mild-moderate AD.
Tar Preparations: Coal tar preparations may have antipruritic and antiinflammatory effects on the skin, although not as pronounced as those of topical glucocorticoids. Newer coal tar products have been developed that are more acceptable with respect to odor and staining of clothes than some older products. Tar shampoos can be beneficial for scalp dermatitis and are often helpful in reducing the concentration
378
and frequency of topical glucocorticoid applications. Tar preparations should not be used on acutely inflamed skin because this often results in skin irritation. Side effects associated with tars include folliculitis and photosensitivity. There is a theoretic risk of tar being a carcinogen based on observational studies of workers using tar components in their occupations; however, epidemiologic studies do not confirm similar outcomes when used topically.83
PHOTOTHERAPY
PHOTOTHERAPY
Natural sunlight is frequently beneficial to patients with AD. However, if the sunlight occurs in the setting of high heat or humidity, thereby triggering sweating and pruritus, it may be deleterious to patients. Broadband UVB, broadband UVA, narrowband UVB (311 nm), UVA-1 (340 to 400 nm), and combined UVAB phototherapy can be useful adjuncts in the treatment of AD. Investigation of the photoimmunologic mechanisms responsible for therapeutic effectiveness indicates that epidermal LCs and eosinophils may be targets of UVA phototherapy, with and without psoralen, but UVB exerts immunosuppressive effects via blocking of function of antigen-presenting LCs and altered keratinocyte cytokine production. Photochemotherapy with psoralen and UVA light may be indicated in patients with severe, widespread AD, although studies comparing it with other modes of phototherapy are limited. Short-term adverse effects with phototherapy may include erythema, skin pain, pruritus, and pigmentation. Long-term adverse effects include premature skin aging and cutaneous malignancies (see Chaps. 198 and 199 for detailed discussion of phototherapy and photochemotherapy, respectively).
HOSPITALIZATION
HOSPITALIZATION
Patients with AD who appear erythrodermic or who have widespread severe skin disease resistant to outpatient therapy should be considered for hospitalization. In many cases, removing the patient from environmental allergens or emotional stresses, intense patient education, and assurance of compliance with therapy results in a sustained improvement in their AD. Clearing of the patient’s skin during hospitalization also allows the patient to undergo patch testing or allergen skin testing and appropriately controlled provocative challenges to correctly identify or rule out exacerbating factors.
SYSTEMIC THERAPY
SYSTEMIC THERAPY
The decision to initiate systemic therapies should be based on overall disease severity, response to
topical therapy, adherence to previous topical regimens, impact of the disease on the patient’s quality of life, and understanding the patient’s comorbidities and preferences. Before initiating systemic therapy, other diagnoses should be considered that can mimic or exacerbate AD such as cutaneous T-cell lymphoma, allergic contact dermatitis, scabies, or immunodeficiency syndrome. A biopsy or additional laboratory testing may be needed. What follows are discussions of oral and injectable medications previously studied or commonly used as systemic therapy in AD.96 There are no specific guidelines or comparative effectiveness data to inform guidelines regarding the optimal firstline systemic treatment in AD nor is there a definitive algorithm for treatment.
DUPILUMAB
Dupilumab is a fully human monoclonal antibody targeting the IL-4 receptor alpha subunit. The IL-4 and IL-13 receptors share this subunit; thus, dupilumab blocks cytokine signaling through both of these receptors. Except for oral corticosteroids, dupilumab is the only FDA-approved systemic agent for the treatment of AD at this time. Dupilumab is dosed every other week and delivered as a subcutaneous injection. It is indicated for the treatment of adult patients with moderate to severe AD whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable. In two identically designed phase 3 studies named SOLO 1 and SOLO 2, dupilumab resulted in 36% to 38% of patients reaching clear or almost clear skin after 16 weeks of treatment compared with 9% to 10% in the placebo, group which were statistically significant differences.30 Signs of the disease as measured by the Eczema and Area Severity Index (EASI) reduced by 67% to 72%. Dupilumab treatment led to significant improvement in pruritus, quality of life, and clinically meaningful reductions in anxiety and depressive symptoms. SOLO 1 and 2 were designed as monotherapy, that is, without the concomitant use of TCs. A recent study evaluating the effects of dupilumab in combination with TCs found the addition of TCs to dupilumab to be safe and provides modest increased benefit over monotherapy.97 This combination study named CHRONOS also evaluated outcomes with 1 year of continuous therapy showing a maintenance of benefit with longer term use. To date, there appear to be few adverse effects of dupilumab therapy. Dupilumab does not appear to suppress normal immune responses. A recent analysis found skin infections are reduced with dupilumab treatment.39 Vaccine responses to both T cell–dependent and T cell–independent vaccines were unchanged with treatment.98 Injection site reactions (eg, pain on injection) and conjunctivitis are the most common drug-related adverse effects. The cause of the conjunctivitis is unclear, but it does not appear to be infectious, is usually mild to moderate in severity, and can improve with topical lubricants
3
or antiinflammatory therapy and may spontaneously resolve.
SYSTEMIC GLUCOCORTICOIDS
The use of systemic glucocorticoids, such as oral prednisone, is rarely indicated in the treatment of patients with chronic AD but is commonly used by providers. Some patients and physicians prefer the use of systemic glucocorticoids to avoid the time-consuming skin care involving hydration and topical therapy. However, the dramatic clinical improvement that may occur with systemic glucocorticoids is frequently associated with a severe rebound flare of AD after the discontinuation of systemic glucocorticoids. Short courses of oral glucocorticoids may be appropriate for an acute exacerbation of AD while other treatment measures are being instituted. If a short course of oral glucocorticoids is given, it is important to taper the dosage and to begin intensified skin care, particularly with topical glucocorticoids and frequent bathing followed by application of emollients to prevent rebound flaring of AD.
CYCLOSPORINE
Cyclosporine is a potent immunosuppressive drug that acts primarily on T cells by suppressing cytokine transcription. The drug binds to cyclophilin, an intracellular protein, and this complex, in turn, inhibits calcineurin, a molecule required for initiation of cytokine gene transcription. Multiple studies demonstrate that both children and adults with severe AD, refractory to conventional treatment, can benefit from short-term cyclosporine treatment. Various oral dosing regimens have been recommended: whereas 5 mg/kg has generally been used with success in short- and long-term (1 year) use, some authorities advocate body weight– independent daily dosing of adults with 150 mg (low dose) or 300 mg (high dose) daily of cyclosporine microemulsion. Treatment with cyclosporine is associated with reduced skin disease and an improved quality of life (see Chap. 192 for further discussion). Discontinuation of treatment may result in rapid relapse of skin disease, although some patients may have sustained remission. Elevated serum creatinine or more significant renal impairment, hypertension, and drug–drug interactions are specific side effects of concern with cyclosporine use.
ANTIMETABOLITES
Methotrexate (MTX) is an antimetabolite with potent inhibitory effects on inflammatory cytokine synthesis and cell chemotaxis. MTX has been studied for both pediatric and adult AD patients with recalcitrant disease. One controlled study found MTX to provide an approximate 42% reduction in disease severity scores in adult patients, similar to the active comparator azathioprine.99 A trial in children showed similar responses.100 Side effects of MTX include hematologic
379
3
abnormalities and hepatic toxicity. The long-term risk of occult hepatic toxicity with continued use of MTX is not known, and no guidelines exist regarding the role of liver biopsy or imaging in this patient population. Mycophenolate mofetil is a purine biosynthesis inhibitor used as an immunosuppressant in organ transplantation, which has been used for treatment of refractory inflammatory skin disorders (see Chap. 192). Open-label studies report that short-term oral mycophenolate mofetil, 2 g/day, as monotherapy results in clearing of skin lesions in adults with AD resistant to other treatment, including topical and oral steroids and psoralen and UVA light. Similar results were previously reported in another open study of ten patients with a mean reduction in the SCORAD (SCORing Atopic Dermatitis) index of 68% in all 10 patients.101 The drug was also found to be a reasonably useful flare prevention therapy after induction with cyclosporine.102
The drug has generally been well tolerated with the exception of one patient developing herpes retinitis that may have been secondary to this immunosuppressive agent. Hematologic toxicity has also been observed as have cases of progressive multifocal encephalopathy. The use of the drug during pregnancy has also been associated with pregnancy loss and congenital malformations. Azathioprine is a purine analog with antiinflammatory and antiproliferative effects. It has been used for severe AD, and several controlled trials have been reported in adults and children with modest efficacy. Myelosuppression is a significant adverse effect. Thiopurine methyl transferase levels may predict individuals at risk.
OTHER THERAPIES Interferon-γ: IFN-γ is known to suppress IgE responses and downregulate Th2 cell proliferation and function. Several studies of patients with AD, including a multicenter, double-blind, placebo-controlled trial and two long-term open trials, have demonstrated that treatment with recombinant human IFN-γ results in clinical improvement.103 Reduction in clinical severity of AD correlated with the ability of IFN-γ to decrease total circulating eosinophil counts. Influenzalike symptoms are commonly observed side effects early in the treatment course.
Omalizumab: Omalizumab is a monoclonal antibody targeting IgE and is approved for allergic asthma and chronic urticarial. Even though elevated IgE is present in nearly all patients with AD, case reports of omalizumab’s effect in AD were conflicting. A randomized controlled trial found no clinical effects of omalizumab on AD.104 This study suggest IgE does not play a direct role in AD pathogenesis.
Allergen Immunotherapy: Unlike allergic rhinitis and extrinsic asthma, immunotherapy with aeroallergens has not proven to be efficacious in the treatment of AD. There are anecdotal reports of both disease
380
exacerbation and improvement. A Cochrane review of 12 studies found limited evidence supporting their use in AD, although studies were of low quality.105 Well-controlled studies are still required to determine the role for immunotherapy with this disease.
Extracorporeal Photopheresis: Extracorporeal photopheresis consists of the passage of psoralentreated leukocytes through an extracorporeal UVA light system. Clinical improvement in skin lesions associated with reduced IgE levels has been reported in a few patients with severe, resistant AD who were treated with extracorporeal photopheresis and topical glucocorticoids. One study found the treatment to be comparable to daily 3 mg/kg cyclosporine.106
Probiotics: Several studies have shown perinatal administration of probiotics, especially Lactobacillus rhamnosus strain GG to prevent AD in at-risk children during the first 2 years of life. The efficacy of probiotics to treat AD is less clear. Probiotics are purported to deliver beneficial microbes to the gut of patients, establishing a bacterial milieu that reduces systemic inflammatory responses. A systematic review evaluating 12 trials including 781 participants of probiotic supplementation for AD found little beneficial effect.107
A meta-analysis of seven trials showed no significant difference in eczema severity between probiotic and placebo groups. For both treatment and prevention, more research into subgroups of responders, length of treatment, strain of Lactobacillus, and mechanisms involved is clearly needed.
Chinese Herbal Medications: Several placebocontrolled clinical trials have suggested that patients with severe AD may benefit from treatment with traditional Chinese herbal therapy. However, the beneficial response of Chinese herbal therapy is often temporary, and effectiveness may wear off despite continued treatment. The possibility of hepatic toxicity, cardiac side effects, or idiosyncratic reactions remains a concern. The specific ingredients of the herbs also remain to be elucidated and some topical preparations have been found to be contaminated with corticosteroids. At present, Chinese herbal therapy for AD is considered investigational.
Oral Vitamin D: Vitamin D is thought to normalize immune responses and increase antimicrobial peptide expression in AD. A pilot randomized, double-blind, placebo-controlled study looked at the benefit of oral vitamin D supplementation in children with AD from February to March in Boston.108 Eleven pediatric patients primarily with mild AD were treated with either vitamin D (1000 IU ergocalciferol) or placebo once daily for 1 month. Investigator Global Assessment (IGA) score improved in four of six subjects in the vitamin D group (80%) compared with one of five participants in the placebo group (P = .04). In addition, there was a greater reduction in EASI score in the vitamin D compared with the placebo group, although the difference was not statistically significant. In another small controlled study, 14 healthy participants and 14 participants
with AD were supplemented with 4000 IU/day of oral vitamin D3 (cholecalciferol) for 3 weeks.109 Expression of the antimicrobial peptide cathelicidin was significantly increased in the skin biopsies of AD lesions compared with those in healthy skin or uninvolved AD skin, suggesting a role for oral vitamin D in improving innate immune responses in patients with AD. Since these promising early observations, two larger controlled trials have been performed. A study of 107 Mongolian children with winter-exacerbated AD confirmed previous findings and found a significant improvement in the supplemented children.110 In contrast, a study in 60 adults found no clinical effect of vitamin D supplementation on epidermal antimicrobial expression or clinical scores measured by EASI.111
PREVENTION
PREVENTION
Given the high prevalence and morbidity associated with AD, disease prevention represents the holy grail of AD research. For decades, allergen avoidance remained the primary approach to AD prevention with middling or conflicting results. Food avoidance in pregnant or lactating mothers proved dangerous and food avoidance in infancy likely promoted the development of food allergy. The Learning Early About Peanut Allergy study found early exposure of peanut, rather than delayed exposure, dramatically reduced peanut allergy at age 5 years.112 The 2017 NIAID Expert Panel Addendum Guidelines on prevention of peanut allergy recommend that for children with severe eczema, egg allergy, or both, introduction of solid foods begins at 4 to 6 months of age, starting with solid food other than peanuts, so that the child can demonstrate the ability to consume solid food without evidence of nonspecific signs and symptoms that could be confused with IgE-mediated food allergy.113 A practical consideration for applying this guideline at 4 to 6 months of age is that that infants visit their health care providers for well-child evaluations and infant immunizations at this time. This provides an opportunity for eczema evaluation and, if needed, referral to a specialist for peanut allergy evaluation. Allergy testing in children with severe eczema or egg allergy should be strongly considered before the first peanut protein feeding. The use of hydrolyzed formula for AD prevention has shown a positive effect in studies, including persistence of effect in the German Infant and Nutrition study. A recent Cochrane review, however, concluded that there was no convincing evidence of hydrolyzed formula for the prevention of AD in high-risk infants.114 Probiotics supplements appear to have a protective effect on AD development when delivered both pre- and postnatally.115 The exact strains, dosing, and timing of the intervention is not standardized, nor is the mechanism of action understood. Protecting the skin barrier with emollients early in life in high-risk infants also appears to be promising and reduced the incidence of AD by up to 50% in two small studies.116,117 Larger studies of this approach to AD prevention are ongoing.
3
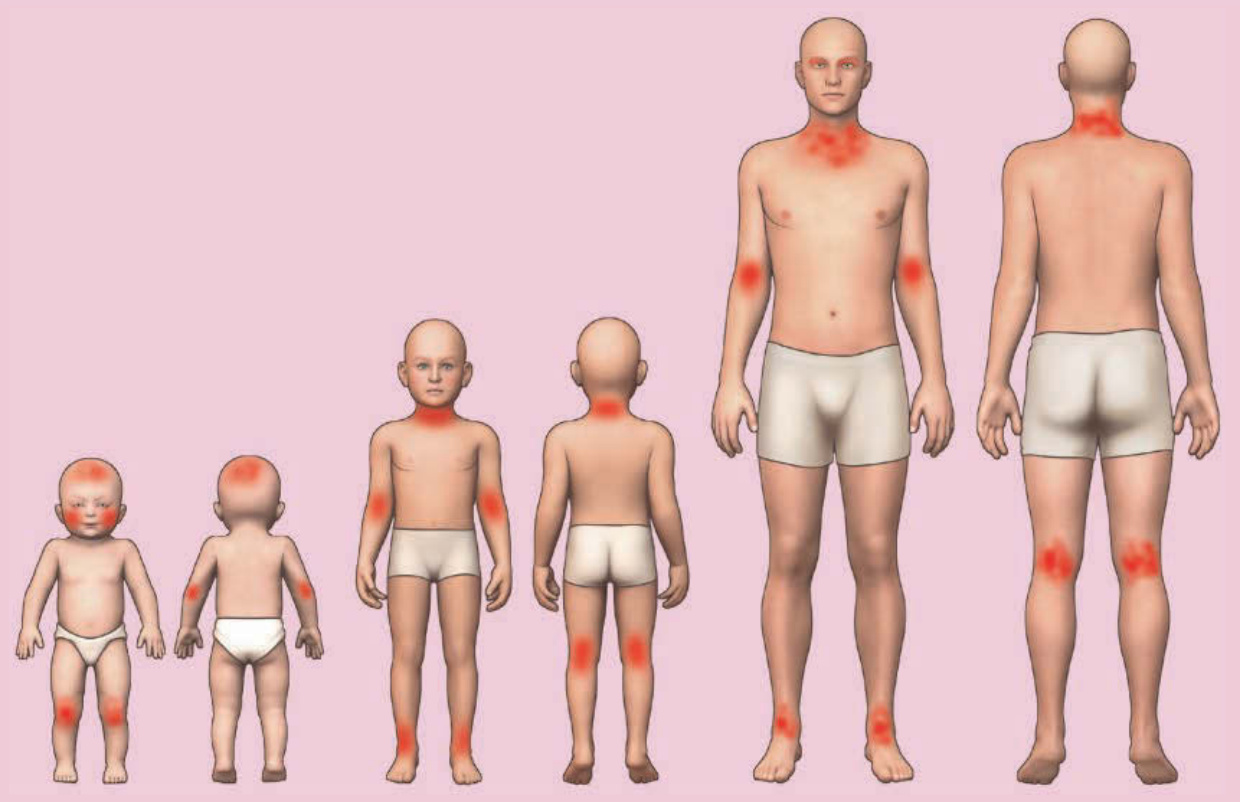
Figure 22-1 Atopic dermatitis progression and distribution: infancy, older childhood, and adulthood.

Figure 22-2 Edematous, erythematous eyelids with lichenification and hyperpigmentation in an adolescent with atopic dermatitis. Note the infraocular (Dennie- Morgan) folds.

Figure 22-3 Itching infant with atopic dermatitis. (Used with permission from Oholm Larsen, MD.)

Figure 22-4 Childhood atopic dermatitis with lichenification of antecubital fossae and generalized severely pruritic eczematous plaques.

Figure 22-5 Typical papules, vesicles, and erosions seen in atopic hand dermatitis.

Figure 22-6 Eczema herpeticum. Typical vesicles and crusting in a patient with disseminated disease.
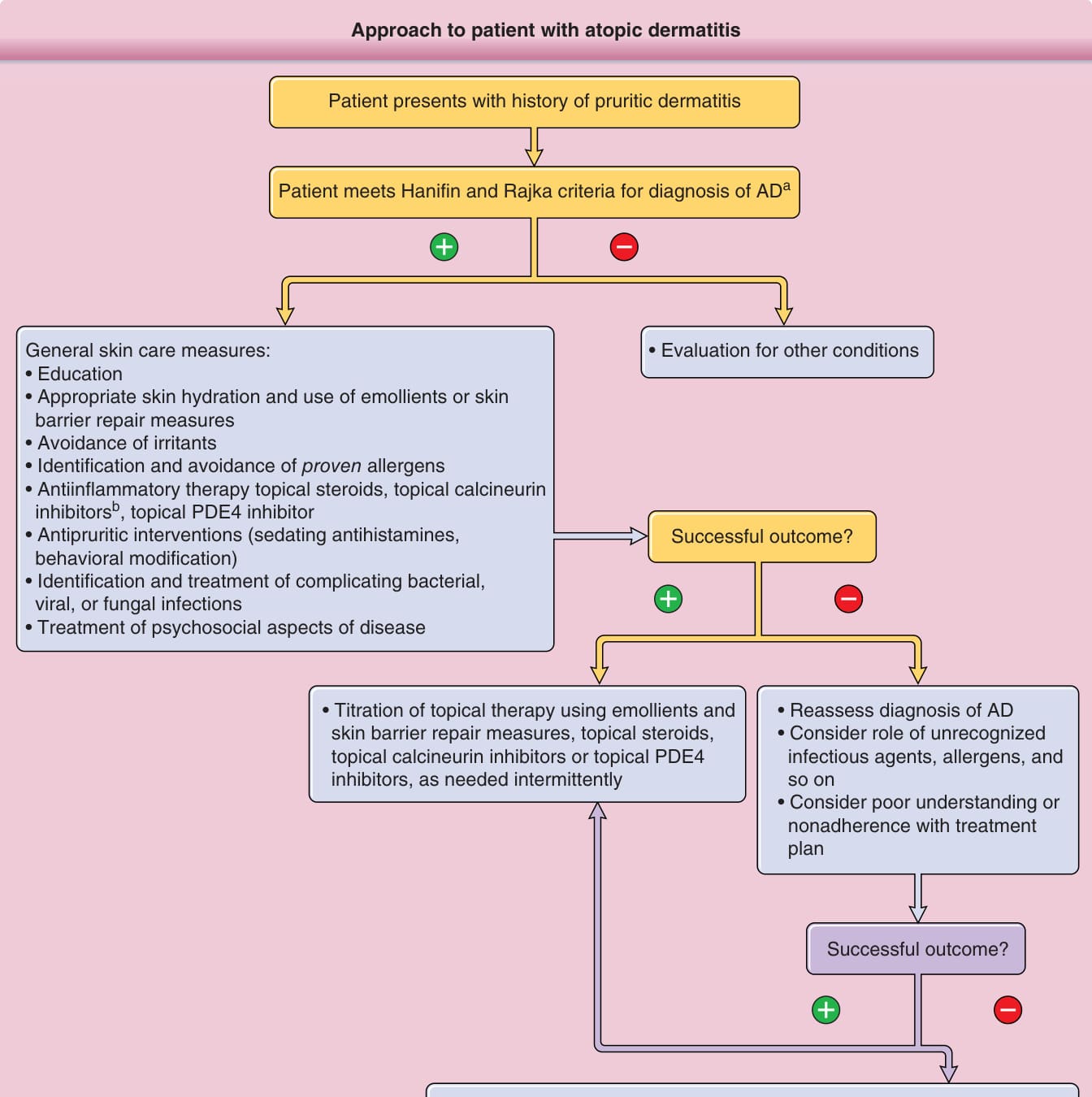
Figure 22-7 Approach to patient with atopic dermatitis (AD). FDA, Food and Drug Administration; PDE, phosphodiesterase; UV, ultraviolet.
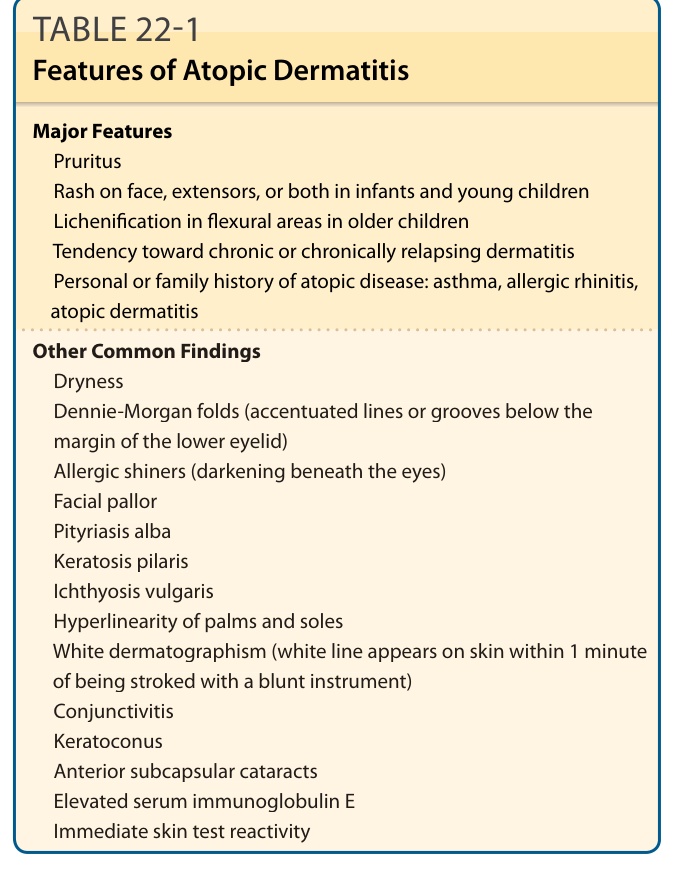
TABLE 22-1 Features of Atopic Dermatitis
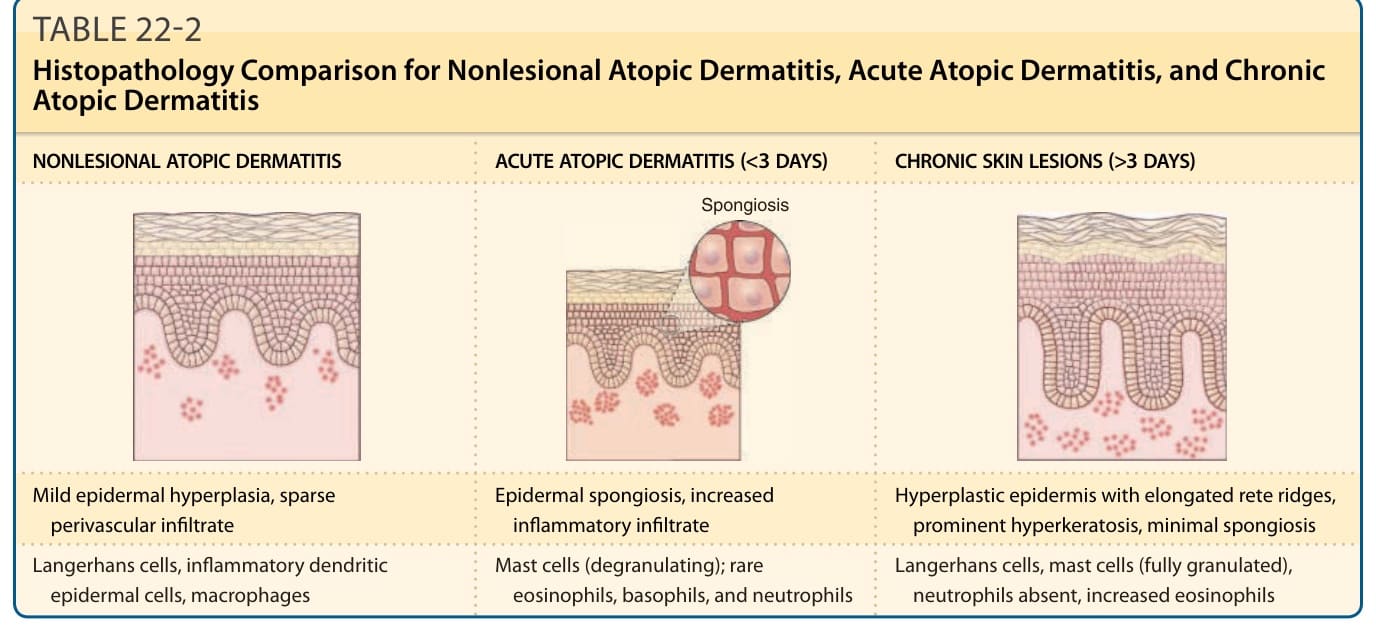
TABLE 22-2 Histopathology Comparison for Nonlesional Atopic Dermatitis, Acute Atopic Dermatitis, and Chronic Atopic Dermatitis
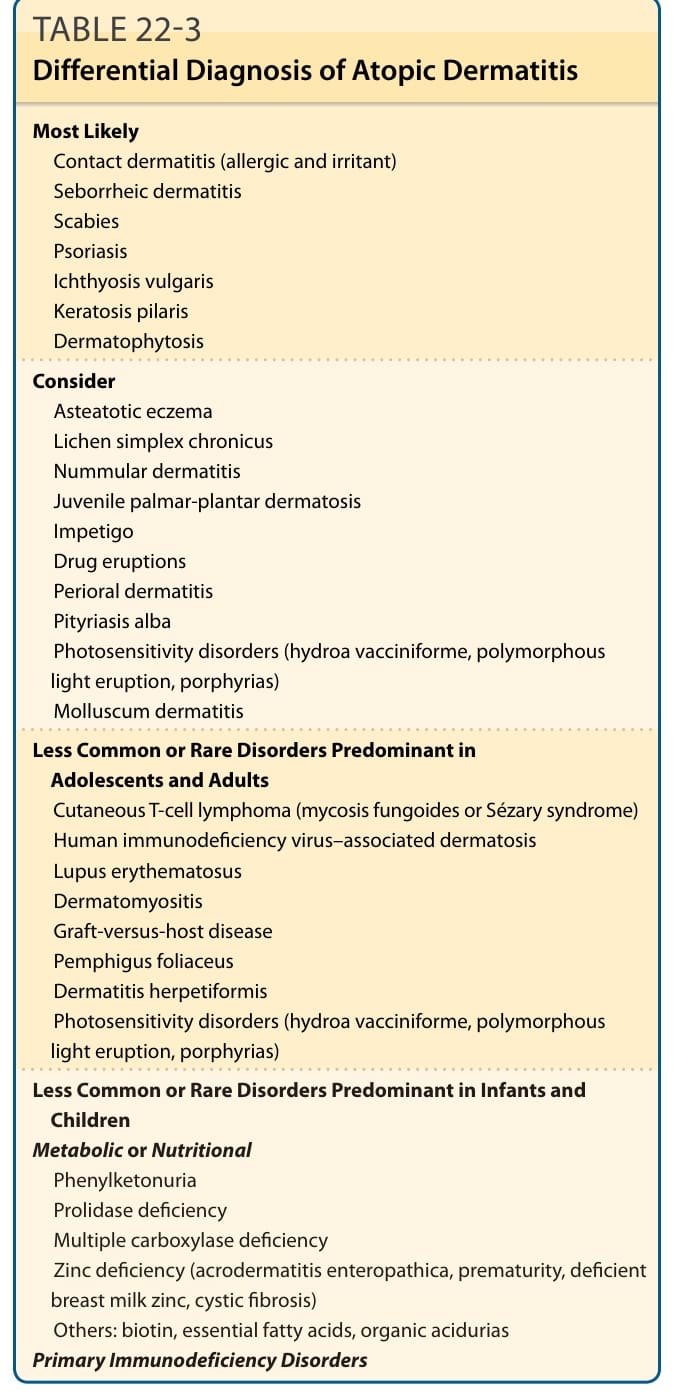
TABLE 22-3 Differential Diagnosis of Atopic Dermatitis
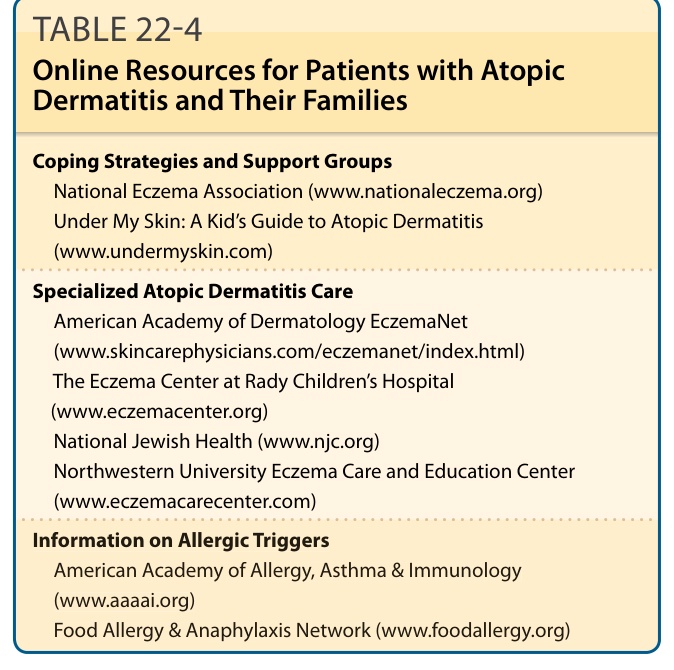
TABLE 22-4 Online Resources for Patients with Atopic Dermatitis and Their Families