Hair Transplantation
3
31
AT-A-GLANCE
■ Most patients undergoing surgical procedures for hair loss have either male pattern baldness (MPB) or female pattern hair loss (FPHL).
■ Surgical techniques used to treat hair loss include hair transplantation, alopecia reduction, and transposition flaps. The latter 2 techniques are rarely used currently.
■ Follicular units (FUs) are the building blocks of modern hair transplantation (follicular unit transplanting [FUT]).
■ The 2 main methods of donor harvest are strip harvesting and follicular unit excision (FUE). The latter may be achieved using a variety of techniques and devices.
■ Minoxidil or finasteride may arrest or partially reverse MPB and FPHL, so a trial of treatment is often appropriate prior to surgery, or concurrent with surgery.
■ Additional innovations of potential benefit include bio-enhanced storage solutions and platelet-rich plasma (PRP)
BACKGROUND
Hamilton and Norwood described the degrees of severity of male pattern baldness (MPB) from a mild Type I to a severe Type VII1-3 (Fig. 217-1). Fortunately, a large majority of male patients do not progress past Types VI: Norwood found that at age 79 only 11% of men have Type VII MPB (Table 217-1), and Unger found that among 328 men older than 65 only 13.7% have Type VII MPB4 (Table 217-2). Thus, if one treats all or most patients as if they will develop Type VI MPB, one is being reasonably cautious. Exceptions are individuals with earlier than usual onset of significant degrees of MPB or Diffuse Unpatterned Alopecia especially if there is a family history of Type VII MPB, in which case it is wiser to plan on an evolution to Type VII MPB. Ludwig described 3 degrees of female pattern hair loss (FPHL),5 whereas Olsen developed a distinct classification system based on her observation of a “Christmas-tree” pattern of hair loss6 (Fig. 217-3). According to Hamilton’s study, 79% of postpubertal females develop at least a mild Hamilton/Norwood pattern of hair loss.2 Most female patients do not have a sufficiently large and/or high-density donor area to surgically treat all of the eventually affected alopecic areas. For this reason, some practitioners believe that women are “rarely” candidates for hair restoration
surgery (HRS)—a view promulgated by the media and therefore shared by the general public! However, in the authors’ experience, and in a survey of experts, the opposite appears to be the case.7 A less than optimal donor/recipient ratio does not preclude surgery but does require a treatment plan that focuses on cosmetically strategic areas. In women, this most often corresponds to the frontal area and the part-line, which is usually a 5-mm-wide anteroposterior corridor (Fig. 217-2). The thickened hair in these areas can then be styled in a way that camouflages untreated areas. When this is done, the cosmetic improvement is significant, and patient satisfaction is high.8
In men, the transplantation of areas of MPB should be conceptualized as consisting of 4 areas: (1) a frontal area extending from the proposed hairline to a coronal line drawn perpendicularly between the tragus of each ear; (2) a midscalp area extending from the posterior border of the frontal area to a point where the caudal scalp changes its orientation from parallel to the ground to more or less vertical; (3) a vertex area that consists of the remainder of the alopecic regions; and finally (4) evolving areas of alopecia adjacent to the aforementioned 3 major areas, which on close inspection contain hair that appears likely to be temporary. Commonly, each transplant session treats one of the 3 major areas, plus adjacent evolving areas. Occasionally, the treatment of evolving areas of hair loss is deferred to a later session to transplant a larger proportion of already existing more obvious areas of hair loss. In such cases, sufficient numbers of grafts must be left in reserve to permit the future treatment of these areas, unless an “isolated frontal forelock” is the ultimate goal. In Unger’s study of 328 males older than 65 years, he delineated an area within the zone of rim hair that contained 8 or more hairs per 4-mm circle.4 He referred to this as the “safe” donor area; later to the “safest” donor area (SDA). For most patients, the equivalent of 3 to 5 strips, each of which is 10 mm, can be excised from the SDA during their lifetime. Each of those strips produces 1500 to 2750 follicular units (FUs) (Fig. 217-3), depending on the density of the donor hair. Current methods of follicular unit excision (FUE) allow slight expansion upon Unger SDA, although not as extensively as some practitioners are claiming.
PATIENT SELECTION
During the initial consultation, surgeons must clarify whether the hair loss is temporary or responsive to medical treatment. Dermoscopy may be a very useful method to evaluate the underlying etiology of hair loss.9 A comprehensive discussion of this subject is available elsewhere in this textbook. Provided
31
The Hamilton-Norwood classification of MPB
II I
III III vertex
IV V
VI VII
A
3932
The Norwood classification for Type A variant of MPB
IIa
IIIa
IVa
Va
B
Ludwig’s pattern of hair loss in females
Grade III Grade II Grade I C
3
31
this is not the case, the first step in the surgical evaluation of a patient is to assess the current and anticipated future size of the donor and recipient areas. An accurate assessment of the donor/recipient ratio depends on professional experience, the family history of patterned hair loss, and most importantly the patient’s age. The second step is to evaluate hair characteristics. Table 217-3 lists the hair characteristics of the best hair transplant candidates. Not all of these characteristics are necessary for a satisfactory result, but each one improves the final cosmetic appearance. The authors do not follow any strict rules on patient selection with respect to the stage of hair loss, age, or gender. For example, in regard to the stage of hair loss, it is important to note that the recipient area does not need to be completely alopecic to successfully operate. In fact, there are important advantages to transplanting at an earlier stage of MPB, although treating such areas demands a high degree of skill. Many surgeons have resorted to shaving the recipient areas for ease of surgery; the authors do not find this necessary and it certainly helps patients to seamlessly resume regular life shortly after surgery. Similarly, there are no definite age requirements, although younger patients, especially those under the age of 25, should have more conservative treatment plans. As part of this planning, such patients are encouraged to use medical treatment to delay or partially reverse the progression of MPB. In addition, surgeons should leave enough hair in the SDA to permit at least 1 future surgery in the event of unexpected areas of hair loss. With respect to gender, it is worth mentioning again that women are more often than generally thought acceptable candidates for hair restoration surgery, despite the strong disagreement of a few surgeons. In an effort to discern the consensus opinion, the authors informally polled a group of leading experts in the field. From among this group, a majority (13 of 22) felt that more than 50% of women had enough donor hair to permit at least 1 transplant. In the authors’ opinion, the percentage is even higher provided that the patient’s expectations are commensurate with what is realistically possible given their anticipated eventual donor/recipient ratio and hair characteristics. A strategically planned surgery, with a focus on transplanting the frontal zone and part-line, usually produces a cosmetically significant improvement, and typically leaves female patients very satisfied.10
Although hair transplantation surgery is predominantly used to treat patients with MPB or FPHL, it also can be used to correct surgical scars, (Fig. 217-4), treat congenital areas of hair loss such as temporal triangular alopecia, and change hairlines. With appropriate care, it has also successfully improved areas of cicatricial alopecia such as end-stage central centrifugal cicatricial alopecia or areas of alopecia resultant from radiation therapy. Although predominantly used for the scalp, hair transplantation also can be performed on other sites such as the eyebrows and beard area in select cases.
3933
31
AGE (y)
18–29 30–39 40–49 50–59 60–69 70–79 ≥80
Type I 110 (60%) 60 (36%) 55 (33%) 45 (28%) 29 (19%) 18 (17%) 12 (16%)
Type II 52 (28%) 43 (26%) 38 (22%) 32 (20%) 24 (16%) 20 (19%) 11 (14%)
Type III
14 (6%)
30 (18%) (3V)a 37 (20%) (15V)a 34 (23%) (15V)a 22 (15%) (10V)a 16 (16%) (7V)a 12 (16%) (8V)a
Type IV 4 (3%) 16 (10%) 15 (10%) 21 (9%) 17 (12%) 13 (13%) 9 (12%)
Type V 3 (2%) 10 (6%) 13 (8%) 15 (10%) 22 (15%) 13 (13%) 9 (12%)
Type VI 2 (1%) 4 (3%) 7 (4%) 10 (7%) 19 (13%) 11 (11%) 10 (13%)
Type VII 0 2 (1%) 5 (3%) 4 (3%) 16 (10%) 11 (11%) 14 (17%)
Total 185 (100%) 165 (100%) 165 (100%) 156 (100%) 149 (100%) 102 (100%) 77 (100%)
Total 185 (100%) 165 (100%) 165 (100%) 156 (100%) 149 (100%) 102 (100%) 77 (100%)
aNumbers in parentheses under Type III represent Type III Vertex individuals.
RISKS AND PRECAUTIONS
Before proceeding with surgery, the patient’s physician is contacted to discuss any areas of major medical concern. Basic instruments and supplies needed for surgery are listed in Table 217-4. For safety, the operating room should be equipped with the medications and equipment needed for basic monitoring and advanced life support. Although rarely necessary, the authors prefer operating with an anesthetist or anesthesiologist when patients have significant underlying health risks, including serious cardiovascular conditions, certain respiratory problems, and seizure disorders. Table 217-5 presents a list of significant (but rare) potential intraoperative complications. Whenever possible, the patient should also be free of all medications that may negatively influence bleeding or healing properties. This includes blood
thinners such as acetyl salicylic acid, nonsteroidal antiinflammatory medications, and natural supplements that may create bleeding problems such as garlic, and Ginkgo biloba. Patients are also encouraged to stop alcohol consumption 10 days before surgery as this may prolong bleeding time.
PATIENT POSITIONING
When removing the donor strip, the authors’ patients are placed in a prone position, with their head in a “doughnut” (“prone”) pillow that allows them to breathe comfortably. During the creation of the recipient sites and the insertion of the grafts, patients remain in a semisupine position except when working on the inferior portion of the vertex, in which case a prone position facilitates the work of both the surgeon and technicians.
TYPE
AGE (years)
65–69 70–74 75–79 80+
I 2 (3.6%) 5 (6.2%) 4 (5.5%) 2 (1.7%)
II 9 (16.4%) 7 (8.6%) 7 (9.6%) 12 (10.1%)
III 4 (7.3%) 15 (18.5%) 18 (24.7%) 11 (9.2%)
IV 10 (18.2%) 16 (19.8%) 8 (11.0%) 10 (8.4%)
V 6 (10.9%) 7 (8.6%) 10 (13.7%) 16 (13.4%)
VI 13 (23.6%) 19 (23.5%) 16 (21.9%) 37 (31.1%)
VII 11 (20.0%) 12 (14.8%) 10 (13.7%) 31 (26.1%)
Total 55 (100%) 81 (100%) 73 (100%) 119 (100%)
Total 55 (100%) 81 (100%) 73 (100%) 119 (100%)
Note:
• In age group 65–69, if one excludes Type I and II, 33 of the remaining 44 (75%) have Types III–VI (83.3% Norwood);
• In age group 70–74, if one excludes Type I and II, 57 of the remaining 69 (82.6%) have Types III–VI (82.8% Norwood);
• In age group 75–79, if one excludes Type I and II, 52 of the remaining 62 (83.9%) have Types III–VI;
• In age group 80+, if one excludes Type I and II, 74 of the remaining 105 (70.5%) have Types III–VI (74.0% Norwood).
3934
A
B
RECIPIENT AREA DESIGN11
On the morning of the surgery, a grease pencil is used to outline the treatment area. The frontal recipient area is designed by drawing the proposed hairline.
1 Hair FU
3 Hair FU
2 Hair FU
3
31
■High-density hair in the safe donor area
■High-density hair in the safe donor area
■A mixture of fine and coarse hair
■A mixture of fine and coarse hair
■Minimal contrast between the skin and the hair color
■Minimal contrast between the skin and the hair color
■Wave or curl
■Wave or curl
The midline, anteriormost point of the hairline should be as superior as acceptable to the patient, but nearly always lies within the area in which the vertical forehead changes into the essentially horizontal caudal scalp. The lateral borders are determined by outlining the supratemporal “humps”—semihemispheric areas containing only temporary hair and that are in the superior temporal areas (with the exception of those with existing Type VII MPB). Some of this area may or may not have initially persisting original hair but, regardless, should sooner (or later) usually be transplanted. The lateral ends of the proposed hairline are then joined to the supratemporal humps with a slight flare, to produce a rounded corner that creates a natural shape, but that usually leaves patients with a mature-looking hairline that includes frontotemporal recessions. In some patients, the anterior border of temporal hair is significantly receded, and it may need to be re-created at the same time as the anterior supratemporal humps are being transplanted. The posterior border of the frontal area is completed with an arc that helps create a natural pattern of hair loss in the event that the patient decides not to transplant any further posteriorly, or does not have sufficient donor hair to do so. When transplanting the midscalp, the posterior aspects of the supratemporal humps are included, and the posterior border of the transplant is similarly finished in an arc. For the vertex area, either the entire region or its anticipated eventual periphery can be transplanted, depending on the available donor supply and patient goals. For less experienced surgeons, it may be useful to consider using a premade grid template with 1-cm2
boxes to estimate the surface area of the target treatment area and use this to determine the number of grafts necessary to cover the proposed treatment area. This will also help the surgeon determine the ideal, achievable graft density.
DONOR AREA DETERMINATION
Choosing the optimal location and width of the donor strip is one of the most important decisions made during hair transplanting. For the first surgery, the authors typically choose a donor area that lies in the middle of the densest zone of the fringe hair, and extends into the temporal region in males, but ends posterior to the ears in females. This location is the
3935
31
A
C
B
D
most logical, because hair is progressively lost from the superior and inferior borders of the fringe hair in MPB, and hence this position provides the greatest degree of likelihood that transplanted hair is permanent. Each subsequent harvest includes any scar from prior session(s), as well as donor hair immediately superior and inferior to it. This results in the presence of only 1 scar, regardless of the number of sessions carried out (Fig. 217-5). To determine the location of the densest zone, it is sometimes helpful to wet the hair to determine the superior and inferior margins of current areas that are already thinning somewhat. Another useful adjunct that can be employed is a hand-held densitometer. This allows the practitioner to more objectively quantify the patient’s donor density and estimate the total number of grafts that can be safely obtained from the donor area and help in the surgical planning. Once the donor area is identified, hair in a 10- to 18-mm-wide zone is clipped to approximately 2-mm length and cleansed with alcohol- and typically an iodine-based antiseptic. FUE harvest may be taken from a slightly expanded SDA, but the surgeon still needs to be wary of going too far outside of it. Subsequent harvests will result
3936
in the small punctuate scars becoming more numerous and closer together; thus, the surgeon needs to be particularly careful with choosing extraction sites location and density during the first and any subsequent harvesting in the same areas. To limit this problem, some FUE surgeons recommend “splitting individual multi-hair FU in vivo” with the punch being utilized; this technique has not yet been shown to produce good hair survival in both the recipient and donor areas.
DONOR SITE EXCISION12
Strip harvesting and follicular unit excision are currently the 2 main methods being used by hair restoration surgeons for the purpose of donor harvest (Fig. 217-6). In recent years, there has been a rising tide of hair restoration surgeons who are promoting the “superiority” and benefits of FUE. FUE in our opinion, however, remains optimally indicated in only a select group of patients, whereas strip harvesting remains a method that still has significant and more long-term proven benefits. In particular, the frequent promotion of FUE as
3
31
INSTRUMENTS AND SUPPLIES STRIP HARVESTING FUE
Preoperative Surgical Planning and Setup
■Aluminum rat tail comb
■Curved Metzenbaum scissors
■China marker grease pencil
■Prone pillow
Anaesthesia
■Syringes (various sizes)
■Short-acting local anaesthesia (eg, lidocaine)
■Long-acting local anaesthesia (eg, bupivacaine)
■Epinephrine (1 in 100,000 dilution)
Harvesting Follicular Units
■Double-bladed cutting knife handle
■No. 10 scalpel blade
■No. 15 scalpel blade
■Small curved surgical scissors
■Small straight Iris scissors
■Hyfrecator
■Smoke evacuation system
■Needle driver
■Suture material
■Toothed curved forceps
■Straight Adson forceps
■Stainless steel bowls
■FUE extraction devices (eg, manual punch, motorized device, robotic system)
■Aid to Extraction instrument for FUE
Processing and Storage of Follicular Units
■Stereoscopic microscope with under-lighting
■Clear plastic cutting boards
■Double-sided razor blades
■Razor blade holder
■Divided Petri dishes
■Holding solution (eg, hypothermasol)
■Electric chilling device or ice packs
Recipient Site Creation
■Hypodermic needles (18G, 19G, and 20G)
■Cut to size blades
Graft Insertion
■No. 5 planting jeweler’s forceps
■No. 2 jeweler’s forceps
■Ring graft storage
■Implanters (used either as sharp implanter or for loading into premade sites)
■Magnifying loupes
Other Consumables
Other Consumables
■Gauze
■Gauze
■Telfa pads
■Telfa pads
■Kerlix dressing
■Kerlix dressing
■Povidone-iodine solution
■Povidone-iodine solution
■Hydrogen peroxide solution
■Hydrogen peroxide solution
■Lidocaine toxicity
■Lidocaine toxicity
■Respiratory depression secondary to sedatives or narcotics
■Respiratory depression secondary to sedatives or narcotics
■Excessive intraoperative bleeding
■Excessive intraoperative bleeding
“minimal incision surgery” is completely unwarranted (Table 217-6). Notwithstanding the preceding, it is the authors’ opinion that all good hair restoration practices should include surgeons skilled in both techniques, and be able to offer both option to patients, after taking into account patient long-term donor/recipient area ratios, hair characteristics, and lifestyle.
3937
31
A
3938
C
B
D
DONOR AREA
FUE punch (2000 0.9 mm diameter) STRIP (24-cm strip length)
Total incision length 2πr × 2000 sites 2000 (0.9 mm) diameter (2 × 3.14 × 0.45) × 2000 = 565.2 cm
24 cm × 2 (sides) = 48 cm
Area of scar πr2 × 2000 (3.14) (0.452) × 2000 = 12.72 cm2
Area of scar πr2 × 2000 (3.14) (0.452) × 2000 = 12.72 cm2 24 cm × 0.1 cm (at most) = 2.4 cm2
24 cm × 0.1 cm
(at most) = 2.4 cm2
Typical strip harvesting produces a far smaller total incision length and total area of scar than does typical FUE when a 1 mm diameter punch is used for the latter. (If a 0.9-mm punch or 0.8-mm punch was used, the total incision lengths and area of scars would be, respectively, 565.2 cm and 12.71 cm2 for the 0.9-mm punch and 502.4 cm and 10.048 cm2 for the 0.8-mm punch). Yet FUE is often promoted as “minimal incision surgery”?!!
STRIP HARVESTING
STRIP HARVESTING
Strip harvesting (also called the unified tissue harvest technique) is the most commonly employed method by the majority of hair restoration surgeons for donor harvest. This has been the mainstay for donor harvesting following the old punch graft harvesting methods, and has allowed large numbers of grafts to be taken from the densest region of the “safest donor area” while retaining a single linear scar that is typically unnoticeable when carried out by good hair restoration surgeons.
ANESTHESIA
ANESTHESIA
Oral sedatives (eg, diazepam and lorazepam) are given to the patient approximately half an hour prior to commencing the surgery. In some patients who may have additional anxiety and have difficulty tolerating a prolonged procedure, an anesthetist or anesthesiologist can be employed to facilitate surgery with conscious sedation. Once the donor area is identified and clipped, the surgeon proceeds with administering local anesthesia, usually 1% or 2% lidocaine with 1 in 100,000 epinephrine along the inferior and lateral edges of the clipped donor area. Subsequently, longer-acting anesthesia such as bupivacaine is administered before the initial lidocaine becomes ineffective.
STRIP REMOVAL
STRIP REMOVAL
Effectiveness of the anesthetic block is verified directly prior to strip harvesting. Scalp laxity is clinically assessed to determine the appropriate width
3
31
of the donor strip, which in the authors’ practice is typically 8 to 15 mm wide and is usually wider in the middle section and narrower toward the temporal regions. A prudent decision is to take a slightly narrower strip than the examination suggests is possible, thus permitting a margin of error that will minimize the possibility of a high-tension donor closure, and hence production of a wider than optimal scar. Immediately prior to donor tissue excision, the donor area is tumesced with 10 to 40 mL of normal saline. This increases tissue turgor, thereby minimizing bleeding, but also limiting distortion of the follicle that might otherwise result in FU transection. The authors typically use a single-blade scalpel to cut donor tissue parallel to the exit angle of the hair. Occasionally, if the follicles are particularly long, the superficial epidermis is scored and blunt dissection may be used to increase the depth of incision. The incision begins and ends approximately 2 cm lateral to the ends of the clipped donor area. To reduce the likelihood of “dog ears” forming, the 2 ends are tapered to a 30° angle using a No. 15 scalpel. The depth of the incision can vary significantly. In the first surgery, the blades are placed in high subcutaneous fat, to minimize underlying neurovascular damage. In subsequent surgeries, where fibrous scar tissue has formed deep to the original donor site, the depth of the incision may be increased to permit its removal. This is important because scar tissue is avascular, space occupying, and tethers the edges of the wound, thereby increasing donor closing tension and interfering with wound healing. At the same time, care is observed to prevent the creation of a depression in the tissue. Importantly, the entire strip is removed in 3 sections, each sutured before reassessing scalp laxity in the remaining unharvested section(s). This provides greater control of bleeding and a more accurate guide to the optimal width of the next section of the strip to be excised. Vessels with exuberant bleeding are cauterized using a unipolar hyfrecator. The wound sections are closed either with a single-layer running suture or with a bi-layered closure. The bi-layered closure is typically employed if the authors feel that there is greater than optimal closing tension or if there is hyperlaxity in the scalp. In practice, the authors use an absorbable No. 3.0 PDS II suture for their subcutaneous interrupted sutures, and a No. 2.0 to 4.0 Prolene or Supramid for the superficial closing suture. Other surgeons sometimes close the donor site with staples, but at this point, the authors prefer sutures for greater precision in wound edge approximation, and a more comfortable postoperative patient experience. Occasionally, the authors will employ a “trichophytic closure” to minimize scar visibility in individuals who have previously (and rarely) healed with a wider than usual scar or in patients who wear their hair very short and who have a strong contrast in the color of their skin and hair. In such instances, a very thin slice of the epidermis (<1 mm from the edge) on the inferior wound edge is removed prior to donor closure, using either
3939
31
curved scissors or a bent razor blade. This creates a purposeful controlled transection of the upper portion of hair follicles, and when the 2 edges of the wound are apposed, most of these transected follicles will lie under the line of closure. If properly done, these hairs then grow through the middle of the donor scar, thus reducing the noticeability of scar tissue. The potential disadvantages of a trichophytic closure include temporary folliculitis, an alteration in the direction of hair growing through the scar, and a change in the density of hair follicles within the scar that could be more visible than a thin scar in patients who wear very short hair. It should also be avoided in patients with tighter than average scalps as it results in a minimal increase in wound tension (if the same width strip is taken).
FOLLICULAR UNIT EXCISION
FOLLICULAR UNIT
EXCISION
FUE is an alternative method of donor harvesting and as mentioned earlier is widely gaining popularity among hair restoration surgeons and patients for a variety of reasons; in fact, many young surgeons use only this method of harvesting. Using this technique, each individual FU is harvested directly from the scalp, rather than from a strip of donor tissue.13,14 FUs are excised using a small, sharp cylindrical punch (generally 0.8-1.2 mm in diameter), which superficially incises the skin around each FU. The FU can then be carefully removed with forceps and gentle traction. The donor wounds are left to heal by secondary intention over the course of 7 to 10 days, finally leaving multiple small white scars over the harvested area. On the one hand, this technique offers distinct advantages. Most importantly, it does not leave a
A B
linear scar. The resultant punctate scars are minimally noticeable, even with the hair closely cropped (Fig. 217-7). Thus, this is a useful procedure for individuals who want to wear exceptionally short hairstyles, those who have a tendency to heal with wider scars, and patients with a strong dislike or fear of linear scars. It is also an excellent technique to provide additional grafts after strip harvest surgery is for variable reasons no longer a good option. On the other hand, FUE is associated with important disadvantages. Chief among them, if a patient is destined to develop greater than Type V MPB, and therefore will need more than 6000 transplanted FUs; many of these grafts would need to be harvested from areas outside the boundaries of the SDA (Fig. 217-7). This is because in most patients FUE involves the extraction of every third or fourth FU (depending on patient ages, donor hair density, caliber, color contrast with the skin, etc.), and therefore the donor area would have to be 3 to 4 times as large as the donor area required for strip harvesting and would necessitate extension beyond the SDA. The hair within many of these FUs is therefore less likely to be permanent and may ultimately disappear in the future. Also, as the fringe hair beyond the SDA is progressively lost and/or miniaturized, the small hypopigmented scars from the FUE harvest may become exposed. In a worse-case scenario, overharvesting could result in a moth-eaten appearance that is difficult to rectify. Equally important to consider are the transection rates during graft harvesting. Most hair restoration surgeons who practice both strip harvesting and FUE still find that transection rates are higher for FUE than for strip excision. Although improvement in FUE instrumentation has led to a significant decrease in FUE transection rates compared to its early days, there is still skepticism regarding equivalent transection rates in FUE reported by some practitioners.
3940
In FUE, each FU is at risk of transection when it is extracted blindly from the scalp. In contrast, in strip harvesting, only grafts at the edges of the strip are vulnerable, because other FUs are prepared with magnified, direct visualization (see below). Also, the FU grafts obtained through FUE tend to be more skeletonized with less surrounding supportive tissue. Contrast this with the grafts that are created from strip harvesting, which tend to have more protective tissue surrounding each follicle (Fig. 217-8). This is believed to lend greater protection to the FU and is likely to contribute to higher survival rates and hence better growth from strip harvest surgeries. The use of implanters, which minimize handling of grafts, may help minimize the trauma associated with implanting FUE grafts and improve their survival. As of this writing, there are very few survival studies to assess the growth of FUE grafts, and the few that have been completed indicate lower survival.15
FUE also may be suggested on occasion as a first surgery in the occasional young patient who wants to preserve the option of stopping hair transplants and switching to a short “buzzed look.” The authors most often recommend FUE be used to complement strip harvesting, not to replace it, except in select patients for whom the benefits outweigh the drawbacks. In particular, FUE may be helpful in thinning the bushy temple regions in some patients and it can be utilized to obtain FU for placement into linear scars produced by strip harvesting. This is desirable when the scar is wider than average or when no further strip harvesting is planned. Such an approach combines the main advantage of strip harvesting—the maximization of the number of permanent hairs that can be harvested via the strip method—with the main advantage of FUE, the lack of a linear scar. For this purpose, we recommend that patients with a poorer prognosis (ie, MPB Type VI or VII) start with sessions using strip harvesting followed by FUE. This will maximize the number of available permanent hairs for harvesting over the patient’s lifetime. In some situations, a combination approach with both a strip harvest and FUE also can be carried out on the same day in select patients. This approach is employed when the patient has had previous surgeries that have resulted in a tight, limited donor area due to underlying scarring, as performing FUE around the strip harvest scar can theoretically help in increasing the laxity of the scalp. Additional points of comparison between FUE and strip harvesting are outlined in Table 217-7.
ANESTHESIA
ANESTHESIA
Just like in strip harvesting, oral sedation is given on the morning of the surgery and local anesthesia is employed by way of a ring block around the determined harvest area once this area is shaved and cleansed with usually povidone iodine.
3
31
1 Hair FUGs 2 Hair FUGs 3 Hair FUGs 4 Hair FUGs A
B
C ARTAS
3941
31
Advantages
■Reduced postoperative pain
■Fairly rapid donor healing
■Fewer limits on postoperative activity, which is beneficial for patients who need a quick return to activity
■No suturing required
■Absence of linear scar
■Ideal for patients who prefer to wear their hair short (<2 mm)
■Ability to selectively choose FUs according to desired size or texture
■Ability to utilize body hair in patients with insufficient scalp donor hair
■Ideal for donor scar repair
■Requires a smaller team of technicians
Disadvantages
Disadvantages
■Difficult to obtain large numbers of grafts without exceeding the limits of the safe donor area
■Difficult to obtain large numbers of grafts without exceeding the
limits of the safe donor area
■Higher follicular transection rates
■Higher follicular transection rates
■Skeletonized grafts with potentially lower survival rates due to increased vulnerability and trauma during placing
■Skeletonized grafts with potentially lower survival rates due to
increased vulnerability and trauma during placing
■More difficult postoperative camouflage because hair needs to be shaved short for harvesting of significant number of grafts
■More difficult postoperative camouflage because hair needs to be
shaved short for harvesting of significant number of grafts
■Longer operative times
■Longer operative times
■Scarring of donor area makes subsequent FUE sessions more challenging and limited
■Scarring of donor area makes subsequent FUE sessions more
challenging and limited
INSTRUMENTATION AND ROBOTICS
INSTRUMENTATION AND
ROBOTICS
FUE is a surgeon (and his or her surgical team) AND instrument dependent procedure and there are an increasing number of devices that are being developed to increase both efficiency as well as accuracy of the method. A range of instruments have been developed and marketed, from simple manual FUE punches to motorized FUE devices (with a variety of distinguishing features ranging from whether a sharp or dull tip is employed, to whether the device uses a rotatory head or an oscillatory head) and entire robotic systems.16 The most important properties of the instrument chosen include the amount of surrounding tissue left intact around the grafts, the rate of transection, the size of the resultant punctuate scars, and flexibility in tissue characteristics. It is difficult to find a good objective overview of the benefits and drawbacks of each instrument but, fortunately, as with all innovations, the field continues to evolve.17
BODY FUE
BODY FUE
Body to scalp FUE can be used if the patient has insufficient donor hair in the scalp. The highest growth rates have been observed in hairs harvested from the beard and chest areas. However, the hair in these areas have different growth rates than from scalp and also
3942
has a different curl and caliber/coarseness. Hence, it is not recommended for transplantation into the hairline area, which is more visible and should be created using fine scalp hair. However, the body hair can be mixed posterior to transplanted scalp hair to lend increased density, or to camouflage scars.
GRAFT PREPARATION
STRIP HARVESTING
STRIP HARVESTING
The preparation of grafts from a strip harvest is accomplished using either stereoscopic microscopes or magnifying loupes or glasses. After removal of a donor strip, the first step is “slivering” the donor strip, in which slices, one FU wide, are carefully produced from the strip, much like cutting a loaf of bread into individual slices. These “slivers,” composed of 4 to 10 FUs, are then further divided into individual FUs. FUs naturally occur in clusters of 1 to 4 hairs, with the average white FU containing an average of 2.3 hairs (other races usually have lower hair density, and hairs/FUs as well as different hair characteristics described elsewhere in this chapter). Occasionally, 2 very closely spaced FUs are combined into an individual “follicular family” (FF) small enough to fit into a typical FU recipient site. Compared with larger multi-FU grafts, FUs and FFs are far more susceptible to injury during graft preparation, storage, and insertion.18 Therefore, technicians must have thorough and prolonged training, excellent manual dexterity, and ongoing supervision. The ideal FU has most of its epidermis removed and is tear shaped, with the tapered end near the epidermis and the bulkier end in the subcutaneous tissue (Fig. 217-8A). This results in an FU wherein the dermal and subcutaneous tissue remains surrounding the follicle isthmus, hair bulge, and dermal papilla. The donor tissue is kept moist at all times, and prepared FUs are stored in a sectioned Petri dish filled with a storage solution.19 It is important to ensure that the grafts remain cool throughout the procedure; hence the Petri dish constantly rests on icepacks or an electric chilling device. Within the sectioned dish, FUs are distributed into labeled compartments depending on the number and caliber of hairs. In this way, the individuals planting grafts can immediately find the type of graft that they need for a particular recipient site. Hairs that are partially transected are not discarded, provided that the distal two-thirds or proximal half is intact. They are, however, placed in less cosmetically important regions, because hair growth from these grafts is unpredictable.
FOLLICULAR UNIT EXCISION
FOLLICULAR UNIT
EXCISION
As individual units are harvested directly from the donor area, processing of the grafts typically involves primarily removing damaged follicles from partially
transected FUs, as well as segregating the FU according to number of hair follicles.
GRAFT STORAGE
GRAFT STORAGE
Today, hair transplantation surgery is largely a fullday procedure as larger sessions involving thousands of small grafts have replaced the smaller older sessions involving far fewer and larger grafts. As such, it is important to ensure graft viability by storing them in the best possible way once they are out of the body. The technical team must ensure that the grafts remain moist and chilled from the point of harvesting to the point of graft insertion. Survival of transplanted grafts has been found to decrease over the length of time that they are out of the body, with negative factors being ischemia-induced hypoxemia, adenosine triphosphate (ATP) depletion, and ischemia-reperfusion injury. There are various types of storage media being developed, and practitioners are increasingly using hypothermic tissue–holding solutions (eg, Hypo- Thermosol) to replace intravenous fluids (eg, lactated Ringer). Some practitioners also add liposomal ATP to
A
C
3
31
the holding solution as ATP depletion has been found to negatively influence graft survivability.20
RECIPIENT SITE CREATION22
Recipient sites are created using hypodermic needles or small blades cut to match the size of grafts. Prior to the creation of recipient sites, local anesthesia typically using 1% lidocaine with 1 in 100,000 epinephrine, is administered as a ring block surrounding the area to be treated. As necessary subsequently, a 1 in 50,000 epinephrine solution or normal saline is injected intermittently and superficially into the recipient area to provide better hemostasis. Such infiltration offers the additional advantage of spreading any existing recipient area hairs farther apart, thus minimizing the risk of injury when making incisions. Furthermore, as the solutions dissipate, the recipient sites move closer together, which ultimately produces higher hair density. The authors stress that all incisions should be made at the same angle and direction as any persisting terminal or vellus hairs (Fig. 217-9). Much of the art of hair
B
D
3943
31
transplanting resides in the ability of the surgeon to do this, as both angle and direction vary considerably from patient to patient, and between different areas of the scalp. If one fails to do this, the resultant appearance will be unnatural and preexisting hair in the recipient area can be lethally damaged. Therefore, recipient site creation should be done slowly and carefully to ensure accurate angling and direction (Fig. 217-10). Typically, it will take between 1½ and 2½ hours to make 2000 to 2500 sites, depending on the density of preexisting hair in the recipient area and the amount of bleeding. Recipient sites also can be created in either a perpendicular (coronal) or parallel (sagittal) fashion, relative to the hair direction and angle. The authors typically make most sites in a sagittal fashion and create coronal sites in temporal areas and in eyebrows, where it is ideal and natural to have the transplanted hairs lie flat.
GRAFT DENSITY
GRAFT DENSITY
If hair survival is high, a density of 20 to 30 FUs/cm2
produces very good cosmetic results while preserving donor hair for future areas; consequently, this is the density that the authors prefer (Fig. 217-11). Higherdensity grafting is limited to small cosmetically strategic areas of the recipient area, including an oval area in the anterior midline of the frontal area. Greater density in this particular area gives an impression of higher density across the entire frontal area. The authors believe that it is a significant mistake to create an overly dense hairline, which is not natural, and that better results can be achieved by creating a higher-density area behind the anterior hairline. The hairline should also be created with macro- and micro-irregularities to create a natural appearance and not a too straight and dense line that does not occur in nature.
3944
A
B
A second reason for grafting at 20 to 30 FUs/cm2 is that most studies on hair survival have demonstrated a tendency for unacceptable decreases in hair survival at higher FU densities, especially when the total incision length exceeds 3.0 cm/cm2.21-23 In part, this is because of increased competition for a limited blood supply and also may be because higher densities require smaller recipient sites and, therefore, more graft handling. Although hair survival at high FU densities has improved substantially in the last few years, good cosmetic results can be achieved with 20 to 30 FUs/cm2
(Fig. 217-12), and thus higher densities are reserved for individuals with small areas of alopecia and publicly visible professions. For other individuals, especially younger patients with uncertain long-term donor/ recipient ratios, it is often an inappropriate use of a limited resource. The authors believe that it is important to create a natural appearance with maximal cosmetic improvement using the minimum number of hairs to meet the patient’s density objectives (Fig. 217-13). This approach will allow the hair restoration surgeon to treat more of the alopecic areas that will develop
A
C
3
31
B
D
over the patient’s lifetime, rather than depleting the patient’s finite number of donor grafts by overcommitting to a higher density than is required. With regard to “mega-sessions” of 3000 to 5000 FUs, it should be pointed out that the average recipient site is 1 mm long, and while 1 mm seems quite small, the total length of a 3000-, 4000-, or 5000-graft session is respectively 9.99, 13.33, and 16.67 ft. Obviously, the larger the area treated, the more worrisome any given number of incisions and the resulting vascular damage. It seems reasonable to be cautious about creating 10 to 16 ft of incisions on the scalp until high hair survival rates in such sessions have been confirmed. To determine the optimal size of the recipient site, several grafts containing varying numbers of hairs are tested in different sized incisions. The needle or blade size is adjusted accordingly. In general, the hair restoration surgeon should try to create the smallest recipient sites into which the grafts can be easily placed as this minimizes vascular disruption. Typically, 1-hair FU and fine 2-hair FU fit into sites made with 20-G needles, higher caliber 2-hair FUs fit into 19G sites, and 3- and 4-hair FUs fit into sites made with 18-G needles. On the other hand, the ideal graft fit is one that is
“snug,” and not made too small and tight to require significant handling during insertion. Though a mixture of 1, 2, and 3 or more hairs is used in all areas, in general, sites for 1 or 2 fine-haired FUs are created in the hairline zone, and sites for 2 or 3 coarse-haired FUs are created in areas that need greater hair density.
GRAFT INSERTION
After the recipient sites have been created, the surgeon reviews with their assistants the locations where the various sized FUs should be placed. Usually, 2 or 3 technicians work on a single patient simultaneously. Prior to graft insertion, platelet-rich plasma (PRP) and ACell is injected into the recipient sites and a small amount of the mixture is reserved for bathing grafts in before their placement. A group of grafts is removed from the fluid-filled wells of the Petri dish, placed in a “ring” filled with PRP and ACell on the finger, and from there placed in its recipient site. In this way, grafts are kept constantly moist. The skilled technician minimizes trauma to the follicles by handling only the subcutaneous tissue along the base of the graft rather
3945
31
A
C
B
D
than the grafts themselves. The long axis of each incision tells the technician the direction in which the graft should be inserted, and the graft typically slides in easily at the angle with which the site was made with 1 or 2 swift movements. The recipient area is kept clean by regularly spraying a mixture of saline (90%) and peroxide (10%), and the grafts are left slightly elevated to help in identifying sites that have not yet been filled. At the end of the procedure, grafts are repositioned to the level of the epidermis, or left slightly elevated, but never below the skin surface as this can cause pitting, or depressions, in the perifollicular skin.
HAIR IMPLANTERS
HAIR IMPLANTERS
In some countries, for example Korea, the use of hair implanters has largely replaced the forceps technique of placing grafts. When used properly, hair implanters enhance graft viability by minimizing mechanical trauma to the follicle because the graft is pulled into the device by grasping its hair(s) and the crucial hair bulge and dermal papilla are not touched while loading the implanters as well as during implantation. Furthermore, some implantation devices enable the surgeon to simultaneously place the grafts into the
3946
sites as they are being made by the implanter, thus reducing the overall time for the procedure. Because FUE grafts are both more skeletonized and vulnerable to trauma, some practitioners believe that using hair implanters in FUE cases has a significant advantage since the implanters not only fit more easily into the hollow needle of the implanter than into the skin, but their use also concurrently minimizes graft trauma during handling. Some physicians also find greater success rates when using implanters in Asian patients than in patients of other races. This could be because, as noted earlier, the Asian hair shaft diameter is generally greater than in whites and straighter, making it easier to properly load into the implanter. Implanters will likely develop further and become more important for all types of hair in the near future.
REPAIR SURGERY
The appearance of the recipient area of patients who have easily visible, unnatural grafting from prior surgeries, in particular from multi–follicular unit (MFU) grafting, can be greatly improved with modern hair transplanting techniques, primarily by placing FUs anterior and peripheral to these larger grafts.24 If FUs with too many hairs or too coarse hairs have been inappropriately placed
in the hairline zone, these can be dealt with similarly, by surrounding them with properly selected FUs. For larger grafts, the excision of all or a portion of any larger grafts also may be useful in minimizing “ plugginess,” while providing additional hair that can be transplanted elsewhere in the recipient area (Figs. 217-14 and 217-15). For patients in whom poor planning resulted in the unnatural placement of grafts, for example, a hairline that is too far anteriorly, the grafts can be excised either individually or by employing an “en bloc” excision. In the donor area, multiple rows of scarring can often be reduced by excising a strip of tissue that contains 2 rows of scar tissue and an intervening zone of hairbearing skin. This converts 2 scars into a single scar, while providing additional hair for use in the recipient area. It is important, however, that the removed strip is not so wide as to prevent a tension free closure. Alternatively,
A
B
3
31
A
B
donor scarring can be improved by transplanting FUs, often obtained via FUE, into abnormally wide scars.
SIDE EFFECTS AND COMPLICATIONS
The potential side effects and complications of hair restoration surgery are listed in Table 217-8.25 Below we elaborate on a few of them:
- Edema: Severe postoperative edema is unusual, but can be unsightly if it occurs in the frontal region, or interfere with healing if it occurs in the donor area. The risk is minimized by prescribing perioperative corticosteroids, by proper postoperative patient positioning, and by using ice compresses adjacent to but not on the actual operative sites.
- Infection: Although rare, infection can present as early folliculitis in the recipient area, or more seriously wound dehiscence in the donor area. A number of measures such as prophylactic perioperative antibiotics reduce the risk of superficial surgical site infection.
3947
31
Side Effects
■Minor bleeding
■Scalp hypoesthesia
■Edema
■Crusting
■Pruritus
■Postoperative telogen effluvium
Medical Complications
■Wound Infection
■Wound dehiscence
■Neuralgia and neuromas
■Arteriovenous fistulas
■Central recipient area necrosis
■Folliculitis
Aesthetic Complications
Aesthetic Complications
■Visible scarring
■Visible scarring
■Hypertrophic and keloid scarring
■Hypertrophic and keloid scarring
■Unnatural appearance
■Unnatural appearance
■Poor density
■Poor density
- Bleeding: Minor donor area bleeding can occur in the first few days postoperatively. Usually this resolves with firmly applied pressure, but rarely extra suturing is required.
- Donor area scarring: In the authors’ office, significant attention is given to measures that minimize the likelihood of wide donor scarring: the wound is closed with the absolute minimum of tension; postoperative edema is minimized through the aforementioned measures; and postoperative care is meticulous. Although this prevents wide scars in most patients, intrinsic poor wound-healing characteristics and severe scarring from old surgeries can result in wider than average scars. In such situations, grafts harvested from FUE can be transplanted into the scar, or alternatively trichophytic closures or double-layer suturing can be carried out during subsequent strip excisions.
- Poor density: This may reflect poor hair survival, suboptimal graft distribution, or poor postoperative care. This problem is probably entirely avoidable.
- Postoperative effluvium: This problem may occur in hair-bearing areas in the recipient or donor areas. It is presumably due to the interruption of blood supply and is always temporary. Approximately 10% to 20% of male patients and 50% of females experience some degree of postoperative effluvium.
PATIENT FOLLOWUP
In the authors’ practice, all patients are seen the day after surgery for bandage removal. The hair and scalp
3948
are thoroughly washed and the occasional dislodged graft can be adjusted. Postoperative instructions are also reviewed at this point and a clean cap is used to cover the surgical area before sending the patient home. Unless contraindicated, the patients in our practice are also given a tapering course of oral corticosteroids to minimize postoperative swelling. All patients are seen 8 to 12 days postoperatively to check the surgical area and remove sutures. A followup appointment is also generally booked for 4 to 6 weeks postoperatively to check that healing is progressing along the normal course and again at 9 to 12 months to assess the surgical results and determine any need for further treatment.
ALOPECIA REDUCTION
Alopecia reduction, or scalp reduction, is defined as the excision of an area of alopecia or future alopecia.26
In the past, the technique was used in conjunction with hair transplantation as a means of reducing the size of the prospective recipient area, and thus conserving grafts for cosmetically vital areas of the scalp. Unfortunately, the technique is technically demanding, and the high frequency of medical and aesthetic complications, in inexperienced hands, led to the procedure falling out of favor. Currently, the technique is used to repair aesthetically unsatisfactory hair transplanting, to excise areas of cicatricial alopecia, or for hairline advancement. Despite the cosmetic improvement offered by the procedure, alopecia reduction is rarely used and it does come with its own set of complications. These include postoperative bleeding, infection, nerve damage, persistent hair thinning or loss in the fringe areas, disorientation of hair direction, stretch back, and poor scars which can all be minimized if the procedure is done properly.
CONCLUSION
The evolution of hair transplanting, over the last 10 to 15 years, has resulted in a remarkable increase in the number of patients who are candidates for the procedure and an even more impressive improvement in the naturalness of the results. Unfortunately, these new techniques also require far more skill and patience from not only the surgeon but also their surgical team. Additionally, hair restoration surgeons are not miracle workers, and individuals must be educated as to what they can realistically expect from hair transplanting. When this is done, the reward is nearly always a satisfied and grateful patient.
ACKNOWLEDGMENTS
We would like to acknowledge Dr Mark A. Unger, who contributed to the version of this chapter that was included in the previous edition.
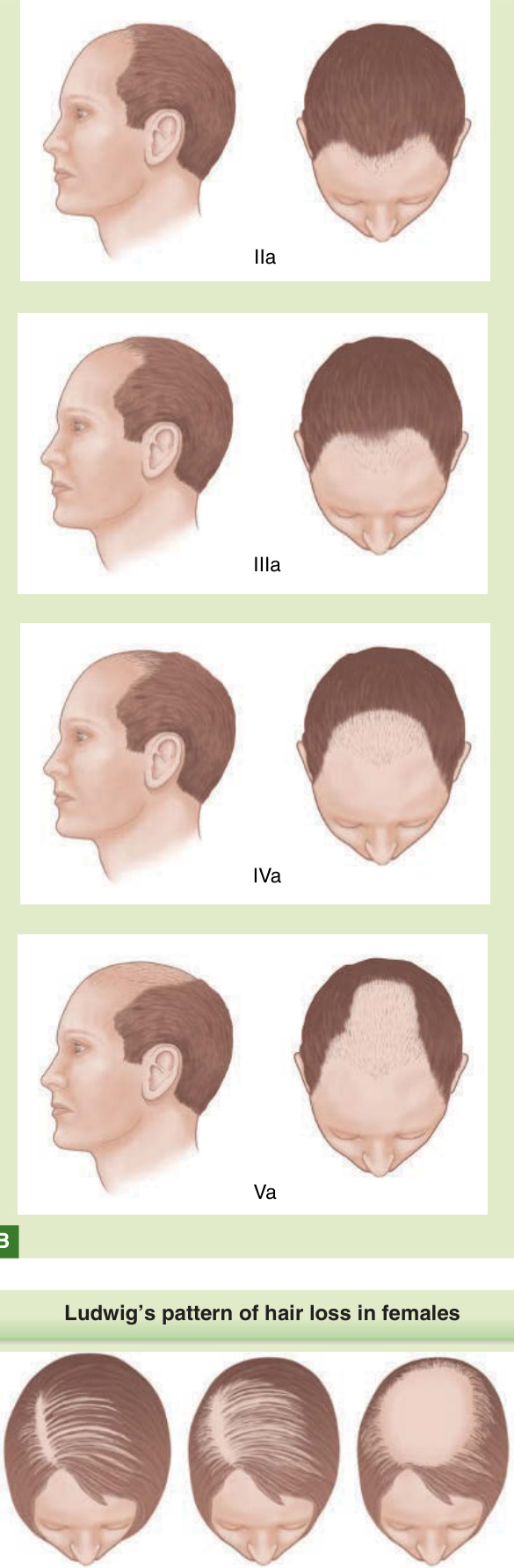
Figure 217-1 A, The Hamilton-Norwood classification of MPB. B, The Norwood classification for Type A variant MPB. C, Ludwig pattern of hair loss in females.

Figure 217-2 A, A 54-year-old female patient with significant hair loss in the hairline and temple regions. B, The same patient 2½ years after a session of 1248 FUs and 264 DFUs. The frontal view shows the effect that can be achieved for the overall appearance.
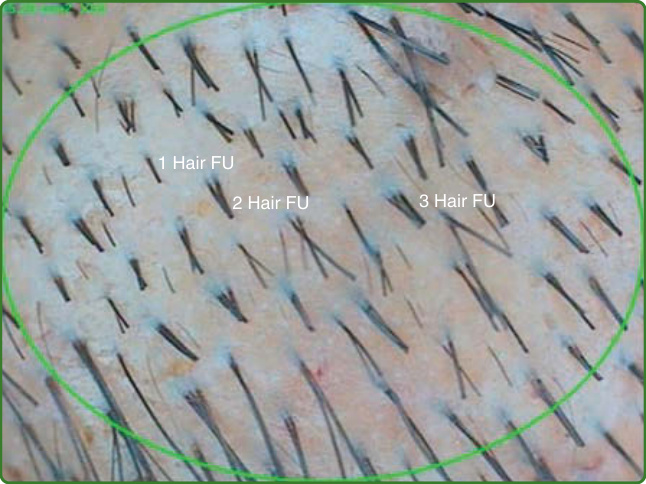
Figure 217-3 A relatively small number of single hairs emerge from the scalp. Most often, hairs grow in small groupings of 2 to 5, as shown in the above photo. These groupings are referred to as follicular units.
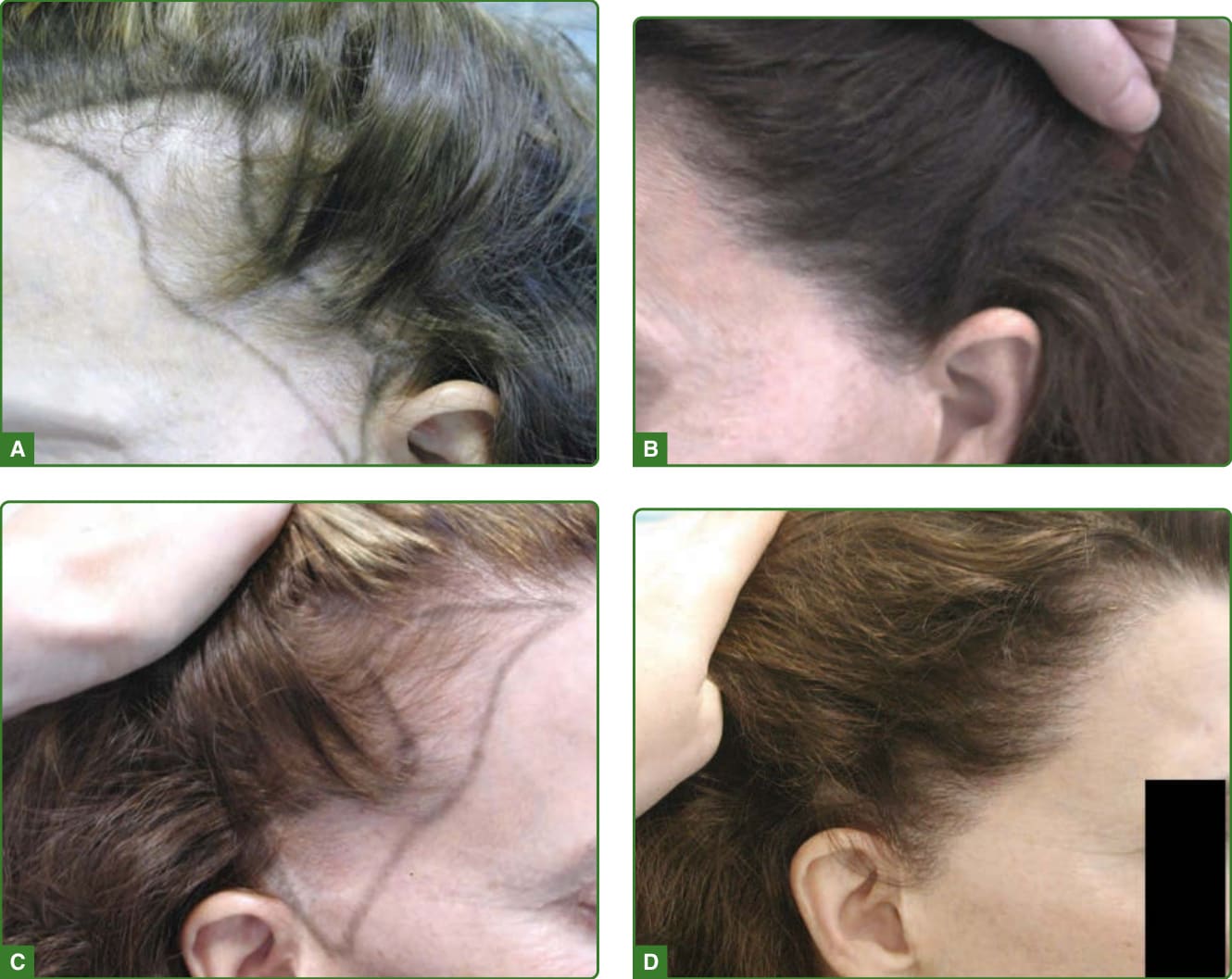
Figure 217-4 Transplanting hair to alopecic areas after a facelift procedure showing before (A and C) and after (B and D) photos.

Figure 217-5 The hair was clipped short in the donor area before the surgery. The narrow scar that can be seen in this photo is the only scar he is going to have as we typically excise any scar from a prior surgery as part of the subsequent donor strips. Scars are usually 0.2 to 1.5 mm wide regardless of the number of strips that have been excised. We believe that this is mainly because we nearly always try to choose strip widths that create wounds that that will close with what we call “minus 1” (-1) to minus 2 (-2) tension, that is, we believe we could have taken a strip that was 1.0 to 2.0 mm wider than what was actually excised.

Figure 217-6 FUE. A, The donor area is shown after suturing. B, The donor area shows the sites of extraction during FUE. C, At 6 months after surgery, the scars are not visible and the overall appearance of the donor is not different from before the FUE. D, Fully healed donor strip.

Figure 217-7 A, This is an intraoperative photo of a patient who had a linear scar from prior conventional strip harvesting, and who was undergoing FUE with the intention of placing grafts within the linear scar, and in areas of alopecia. The FUE was carried out by another surgeon. The round holes are the sites of FU extraction. The superimposed rectangle outlines the safe donor area (SDA). Many of the FUE sites were outside of the SDA, and the hair in these harvested grafts will likely be lost with time as MPB progresses. B, A photo taken 9 months postoperatively demonstrates the most important, immediately recognizable advantage of FUE, namely, the ability for the patient to cut the donor area to any length without visible scarring. The previous linear scar has been effectively concealed with grafting.
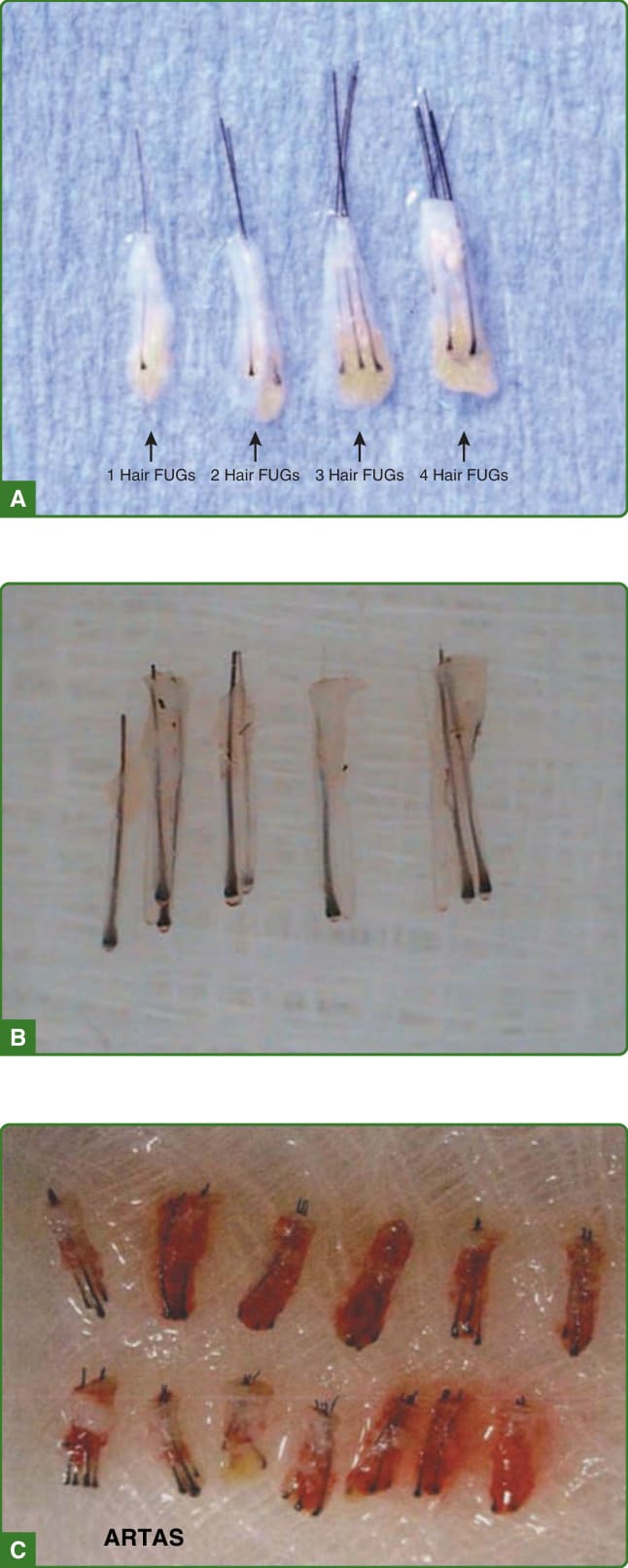
Figure 217-8 Comparison of grafts obtained through 3 different techniques. A, Grafts are harvested using the strip method. The grafts are trimmed into a “ tear drop “ shape preserving the appendages and leaving enough fat tissue to protect the follicle. B, Grafts are harvested by FUE using a motorized punch. Grafts are skeletonized and “naked,” losing their accompanying appendages and devoid of fat tissue for added protection. Note also that there is a more than desired amount of epidermis that needs to be trimmed, which makes the grafts more skeletonized. C, Grafts harvested by FUE using the ARTAS robot.

Figure 217-9 Transplanting hair to areas with preexisting hair. A and C show the areas with preexisting hair before the surgery and the result after transplanting as shown in B and D.
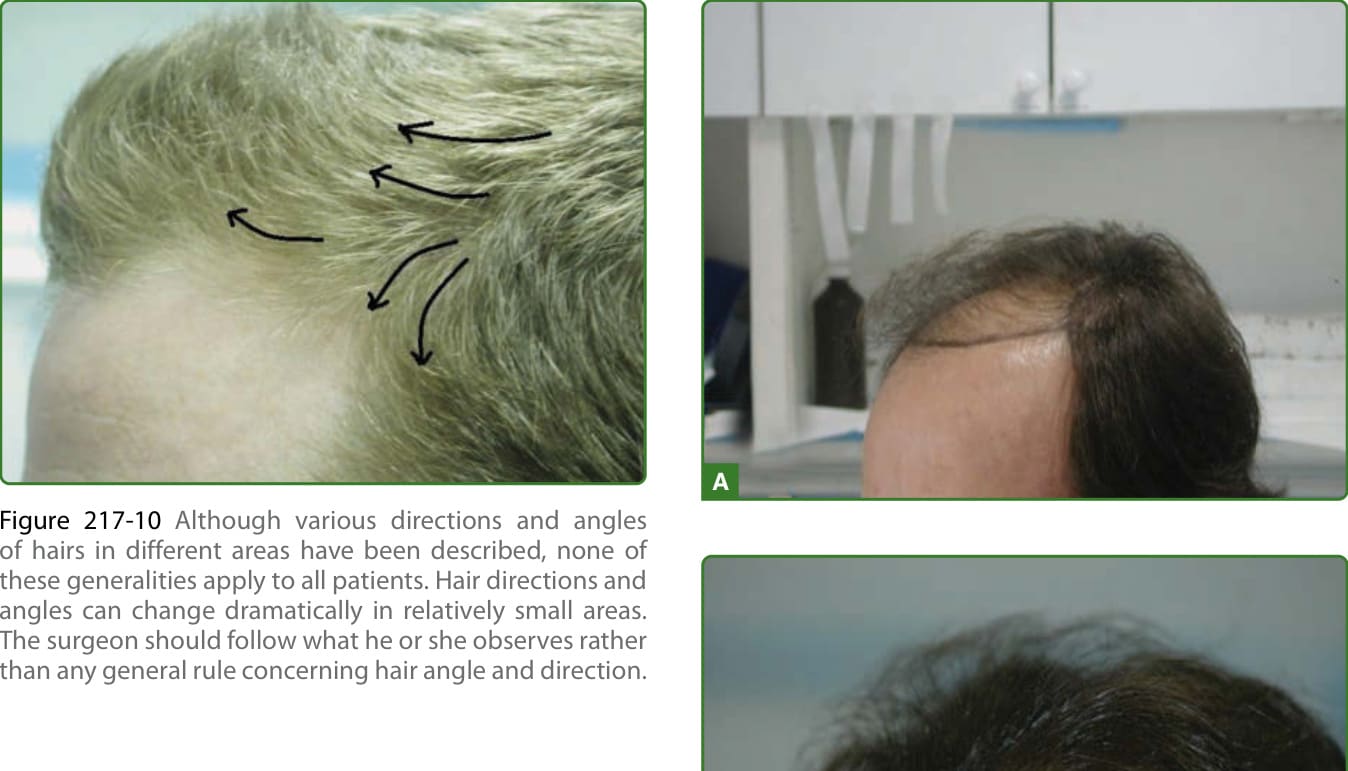
Figure 217-10 Although various directions and angles of hairs in different areas have been described, none of these generalities apply to all patients. Hair directions and angles can change dramatically in relatively small areas. The surgeon should follow what he or she observes rather than any general rule concerning hair angle and direction.

Figure 217-11 A, Before. Objective was more hair but subtle enough to increase likelihood of not being noticed by others. B, 12 months after 1 session at 15 to 20 cm2.

Figure 217-12 A, B, and C, A patient before treatment (A and B) and 9 months after the second of 2 transplants (C)—the first to the frontal area and the second to the midscalp area with a total of 3864 FUs and a relatively low density of approximately 20 to 30 FUs/cm2. D, A frontal view of the same patient taken at the same time as C. Note that the hair appears thicker in this view than in C.
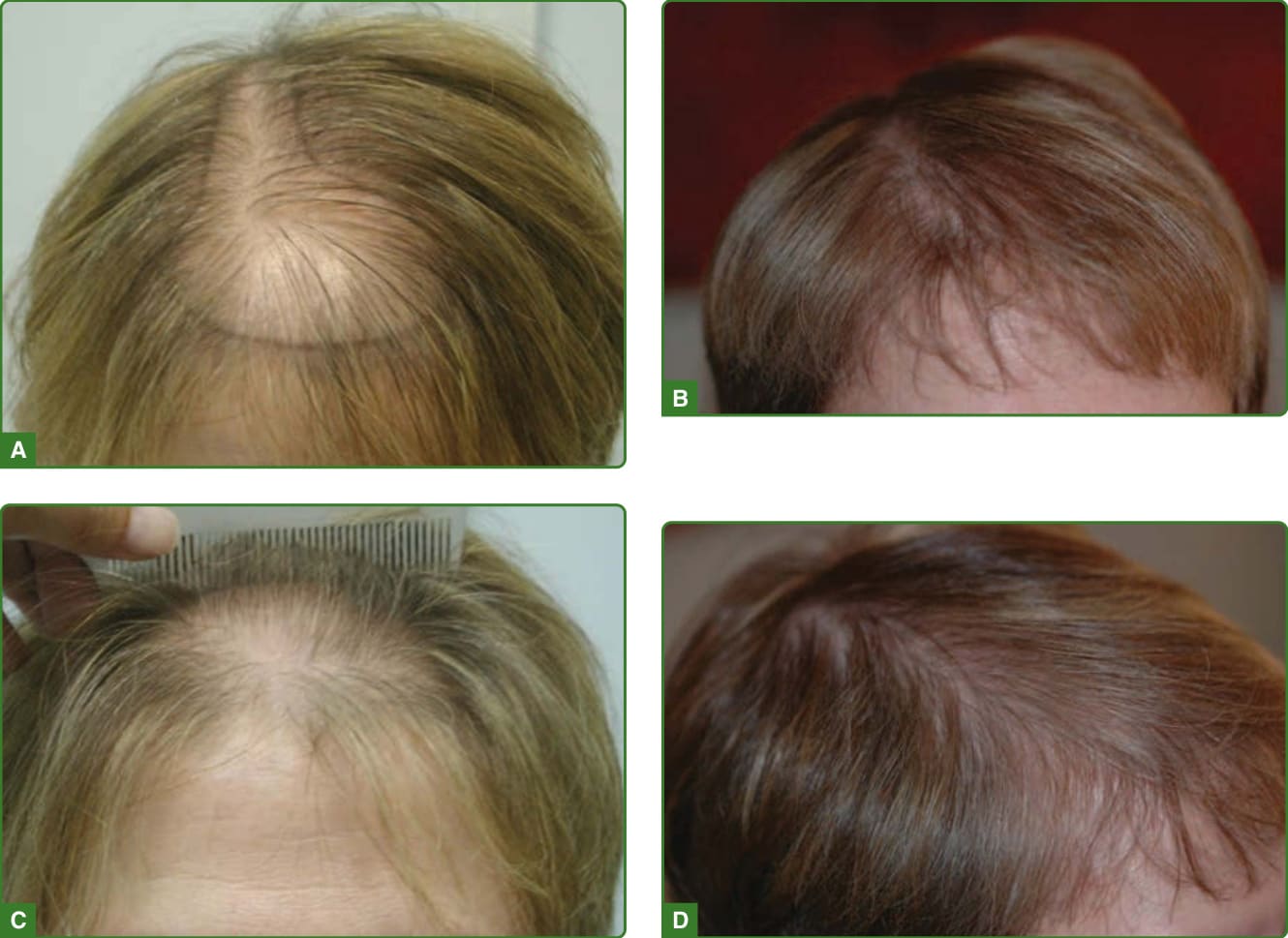
Figure 217-13 The “Christmas tree” pattern of hair loss as described by Olsen. Before surgery and after 1 surgery in a patient with a limited donor density. Concentrating grafts along the part-line and frontal block created an excellent cosmetic improvement.

Figure 217-14 A, This 39-year-old patient had an “FUT” procedure carried out by another physician 3 years before this photograph was taken. A number of errors have been made. These included a failure to transplant into evolving areas of hair loss, and the placement of grafts that contained too many hairs, or too coarse a texture, in the hairline zone. The black crayon outlines the area that we proposed to treat. B, The patient returned 9 months after his first repair consisting of 1973 FUs. A new hairline had been created using finely textured 1- and 2-haired grafts. The rest of the frontal area was repaired by surrounding prior grafts with FUs, and by extending the transplant into adjacent areas of evolving hair loss. A third session, this time to the midscalp, was carried out 2 months after this photo was taken.
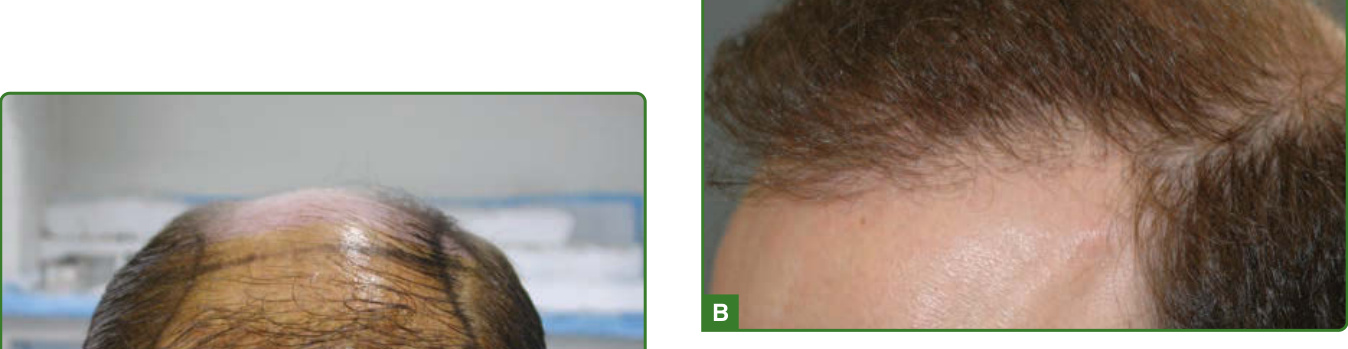
Figure 217-15 A, This patient had a procedure done by another surgeon using round grafts. The grafts contained too many hairs, and too many coarse hairs are seen especially in the hair line zone. Another hair transplant procedure was done using the strip method to correct the hairline and add density to the scalp extending the treatment to areas of possible future loss. B, The patient is seen after 1 year showing refined hairline and increased density of hair and coverage of the scalp.
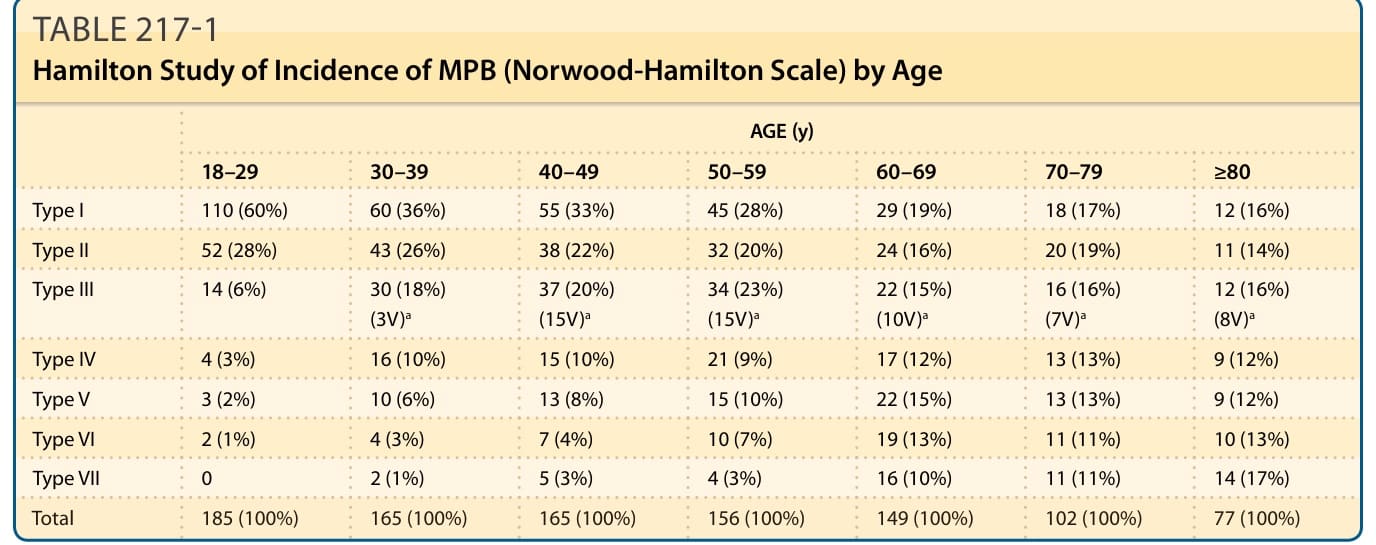
TABLE 217-1 Hamilton Study of Incidence of MPB (Norwood-Hamilton Scale) by Age
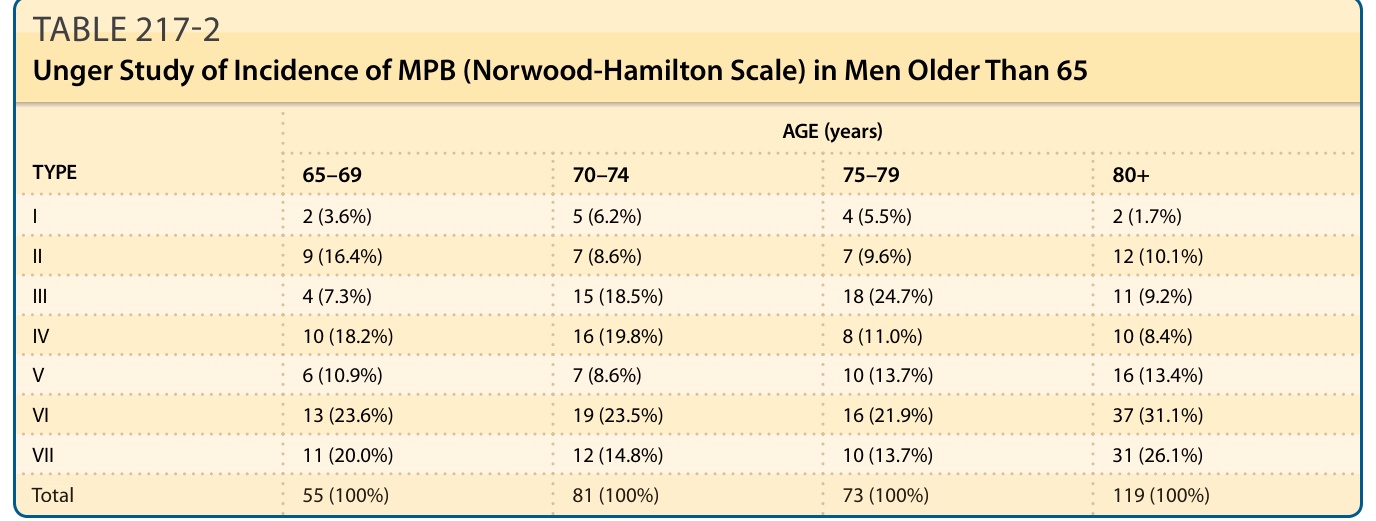
TABLE 217-2 Unger Study of Incidence of MPB (Norwood-Hamilton Scale) in Men Older Than 65
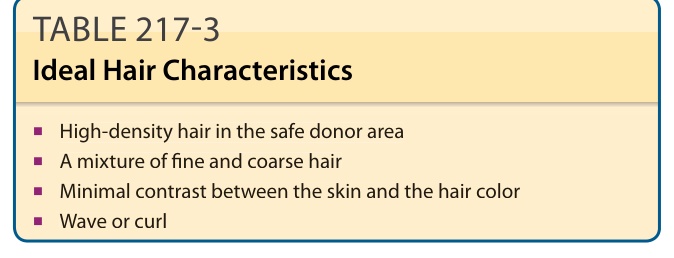
TABLE 217-3 Ideal Hair Characteristics
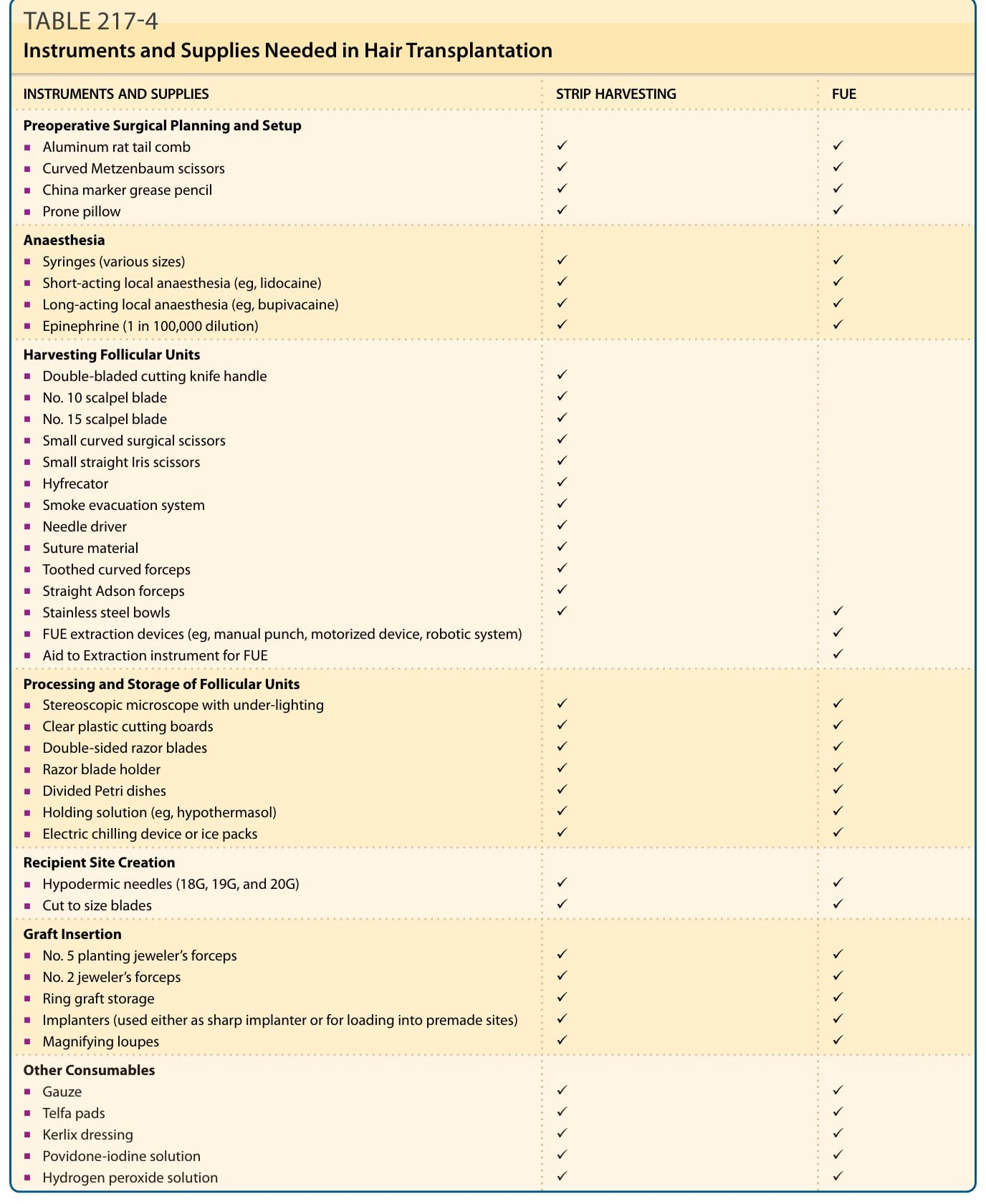
TABLE 217-4 Instruments and Supplies Needed in Hair Transplantation
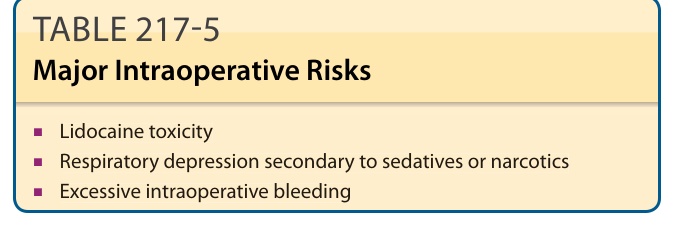
TABLE 217-5 Major Intraoperative Risks
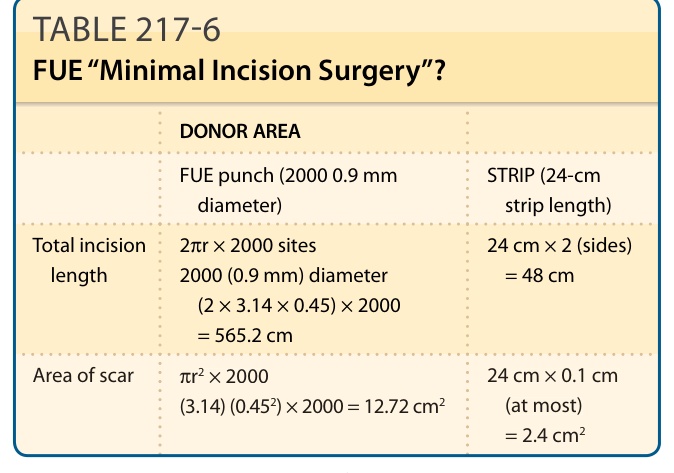
TABLE 217-6 FUE “Minimal Incision Surgery”?
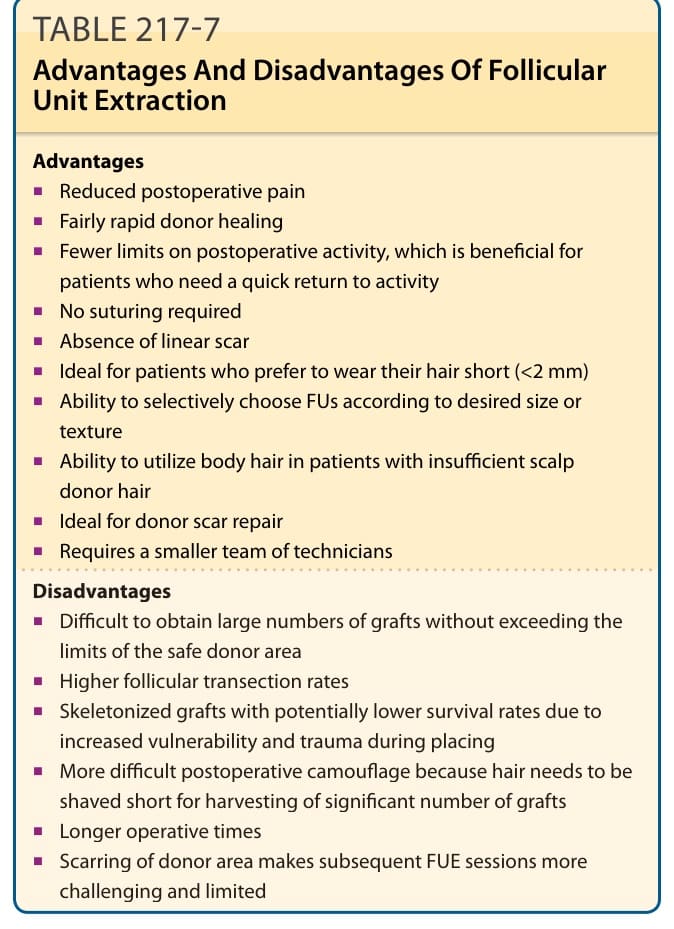
TABLE 217-7 Advantages And Disadvantages Of Follicular Unit Extraction
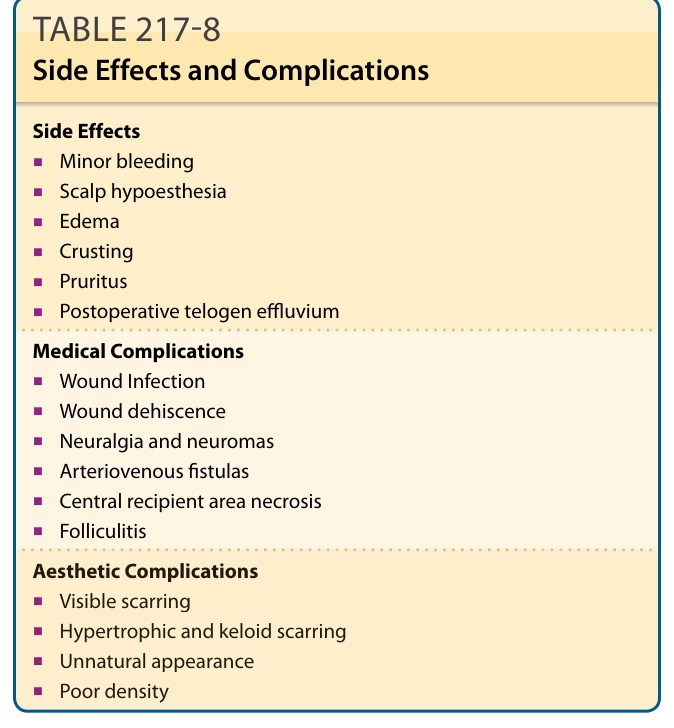
TABLE 217-8 Side Effects and Complications