Botulinum Toxin
3
31
COMMERCIAL MARKET
When Drs. Jean and Alastair Carruthers made the critical leap from ophthalmologist Dr. Alan Scott’s seminal use of botulinum as an alternative to strabismus surgery to the cosmetic use of the toxin to treat the glabellar frown lines, no one could have predicted the explosive growth of this agent in the commercial market.1 On April 15, 2002, the US Food and Drug Administration (FDA) approved Allergan, Inc.’s Botox Cosmetic∗ (botulinum toxin type A) for “temporary improvement in the appearance of moderate-to-severe glabellar lines in adult men and women 65 or younger.” This was the first elective cosmetic indication for which any commercially available botulinum toxin in the US market had been approved. The toxin had previously been approved and was marketed as Botox® for the treatment of strabismus, blepharospasm, and cervical dystonia but existing offlabel cosmetic use of the toxin had already propelled annual sales to 1 billion per year by the end of 2009. The last half of 2015 and first half of 2016 produced 3 billion annual market for Botox®
and Botox Cosmetic® in 2017-2018. Allergan’s product in the US market has equaled the brand name equity of Pfizer’s product Viagra® (sildenafil citrate). “Botox” is now part of the daily vernacular, used to refer to a class of biologic neurotoxins in much the same way as the well-known trademarks Coke® and Kleenex® are used to refer to carbonated beverages and facial tissue. The clinical utility of the neurotoxin is so widely known today that the word Botox has become a generic term in the public mind for all agents used in cosmetic neurotoxin therapy, although the term is properly reserved for Allergan’s trademarked commercial version of the type A neurotoxin complex. In April 2009, the FDA approved a third commercial neurotoxin, a serotype A product, Dysport® (Ipsen [UK]/Medicis [US]) to join Allergan’s Botox®/Botox Cosmetic® and a previously approved serotype B product, Myobloc® (Solstice Neurosciences [US]). In July 2011, the FDA approved a fourth commercial neurotoxin for the US market, a serotype A product, Xeomin® (Merz Pharma GmbH [Germany]). To emphasize the noninterchangeability of these biologic toxins, the FDA in August 2009 required the manufacturers to
∗It is the editors’ policy not to use trade names in this book. However, in certain instances, the editors had to depart from this policy to avoid confusion.
adopt new drug names: onabotulinumtoxinA (Botox®/ Botox Cosmetic®), abobotulinumtoxin A (Dysport®), rimabotulinum toxin B (Myobloc®), and incobotulinum toxin A (Xeomin®). Another serotype A toxin in development in 2011, at the time the last edition was written, was called PurTox® (Mentor [US]). This toxin is purportedly a “naked” toxin, that is, without complexing proteins, and probably with a molecular weight similar to that of Xeomin®. Johnson & Johnson acquired Mentor in 2009 and decided in 2014 to walk away from the neurotoxin portion of their investment represented by PurTox®. The development of this toxin is apparently at an end, all production having ceased, and with some of the intellectual property reportedly having been sold off. The 16-million manufacturing facility that Mentor had built in Madison, Wisconsin, was deemed redundant by Johnson & Johnson and was donated to a private–public research foundation based at University of Wisconsin. In 2014, Allergan spent 65 million (with potential milestone bonuses of another $180 million) to acquire worldwide licensing rights (exclusive of Korea) for the neurotoxin products produced by Medy-Tox [Korea], which are marketed outside the United States under the names Meditoxin® or Neuronox®. The Medy- Tox product is produced in liquid form. Some clinicians have suggested that the liquid formulation may provide a stable, prefilled syringe as a convenience for those practitioners who would like to avoid the required dilution of the lyophilized forms of botulinum toxin such as Botox Cosmetic® and Dysport®. Others speculate that Allergan simply made this licensure agreement to stave future competition for Botox®
in the US commercial space. Korea has been the center of another commercial botulinum toxin product, Botulax®, which was released in Korea and Japan in 2010. It has been used for blepharospasm and glabellar lines. It is an A-type toxin that has a molecular weight of about 900 kDa, similar to Allergan’s product, with the accessory complexing protein structure wrapped around the central 150-kDa core toxin like Botox®. Botulax® is made by Hugel Pharma and is made from the Clostridium strain CBFC26. The American company ALPHAEON (Irvine, CA) acquired Evolus, Inc (Santa Barbara, CA) in 2013 and, as a result of that acquisition, entered into licensure agreement with Daewoong Pharmaceutical (Seoul, Korea) to develop a 900-kDa A toxin for the US and other international markets. This toxin is named Evosyal® and has been known as either DWP-450 or Nabota® in the Korean markets. Evosyal® has completed Phase II and III trials in the US and is awaiting FDA approval.
31
Another serotype of A toxin in use outside of the United States (Asia, South America) is Hengli®/ Prosigne® (Lanzhou [China]). The hurdles to entry into the US market, particularly given the FDA’s rigorous manufacturing standards, may ultimately forestall entry of the Chinese product into the US market. At the time of this writing, there are no particular plans reportedly afoot to bring Hengli® into the US market.
RECENT DEVELOPMENTS
An A-type toxin manufactured by Revance Therapeutics (Newark, CA), daxibotulinumtoxinA, was initially formulated as a topical gel (RT001™) and then as formula for injection (RT002™). Although early Phase II trials showed promise for the topical formulation in the treatment of hyperhidrosis and crow’s feet, in June 2016, the company announced that the RT001 phase 3 trial for crow’s feet had failed to meet its primary endpoints and that future efforts would center on the phase 3 trials of the injectable RT002 for glabellar lines and Phase II trials for cervical dystonia. Earlier, Phase II trials of the RT002 injectable suggested a statistically significant increase in duration of action that would merit confirmation studies in phase 3. In January 2016, Allergan announced the purchase of Anterios, Inc, a biopharmaceutical firm that purported to have a proprietary technology that permits delivery of neurotoxins through the skin. The transport system, called NDS™, was apparently developed with intellectual property from the University of Massachusetts, and involves surrounding the target molecule with nano-particles that permit movement of the molecule across the skin barriers. The topical A-type toxin, ANT-1207, has completed Phase II clinical trials in lateral canthal lines, acne, and hyperhidrosis in March 2016, but results were unpublished at the time of this writing. An additional formulation of A-type toxin in liquid form, AI-09, is in preclinical development as an injectable form of the A toxin.
PHARMACOLOGY
TOXIN STRUCTURE
TOXIN STRUCTURE
Botulinum neurotoxins are currently categorized into 7 distinct serotypes: A, B, C1, D, E, F, and G.2 The molecules vary in their biosynthesis, size, cellular sites of action, binding kinetics, duration of effect, and stability. The serotypes currently commercially available, serotypes A and B, are derived from different strains of Clostridium botulinum. They both have 150-kDa dichain polypeptides with a heavy chain and light chain linked by disulfide bonds. During biosynthesis, the molecules of A and B can be surrounded by proteins to form a neurotoxin complex, ranging from 500 to 900 kDa (Fig. 216-1). Xeomin® (incobotulinumtoxin A) consists of the 150-kDa dichain without accessory proteins.
3922
Botulinum complex
MECHANISM OF ACTION
MECHANISM OF ACTION
The toxin enters the nerves by binding to surface protein receptors and undergoing endocytosis into internalized vesicles. The light chain is released into the nerve cytosol, and the SNARE (soluble N-ethylmaleimidesensitive factor attachment protein receptor) protein complex is cleaved to inhibit exocytosis of the neurotransmitters such as acetylcholine (Fig. 216-2). Type A toxin cleaves SNAP-25 (synaptosome-associated protein of 25 kDa), whereas type B cleaves VAMP (vesicleassociated membrane protein), also called synaptobrevin (Fig. 216-3). These proteins are necessary for the release of acetylcholine from vesicles within the cytoplasm of the motor nerve endings. The binding characteristics of each serotype dictate the locus of action on the intracellular SNARE protein complex (Table 216-1). The end result is a chemodenervation of the cholinergic neurons, either motor nerves or autonomic nerves, leading to localized absence of skeletal muscle activity or autonomic control of target organs such as the eccrine sweat glands. The way in which the nerves escape the effect of the neurotoxin is partially understood.3 The chemodenervated nerve endings develop collateral sprouting near the primary terminus of the nerve. These sprouts eventually make proximate contact with the targets, either muscle or gland, and begin to overcome the loss of neurotransmitter at the end organ synaptic junctions. Once these sprouts have reestablished chemical contact with their targets, muscles resume activity and glands begin to secrete. Simultaneously, the original
Botulinum toxin binding
Motorneuron
LC
HN HC
1
2
3
ACh
B, D, F, G
VAMP Assembled SNARE complex
4
C A, C, E
ACh
Secretory vesicle
SNAP-25
Syntaxin
AChR
Muscle
chemodenervated terminal nerve ending begins to degrade the blocked SNARE proteins and develop new proteins to resume the chemical exocytosis of acetylcholine. While these repairs are under way, and while the original terminal nerve ending reacquires communication with the target organ, the collateral sprouts begin to slowly resorb until anatomically nothing is left but the original terminal ending with restored junctional activity. Four commercially available preparations of botulinum neurotoxin were on the market in the United States and Europe in late 2016, and one was pending approval (Table 216-2). All but one are serotype botulinum toxin A, and one is a serotype botulinum toxin B. The products differ in their methods of manufacture, commercial form, and biologic profiles. Various other toxins are available outside of the US or are in current development. These are summarized, compared, and contrasted in Table 216-3. The units by which these products are described are not interchangeable because of the nature of the assays
3
31
used to determine their potency. The mouse assays used differ in the diluents used and are not comparable. There is no such thing as a standard neurotoxin unit; hence, there is no “International Unit” for neurotoxin. Thus, there is no way of standardizing neurotoxin units to compare serotype A products to each other, let alone to other serotype B products. Although the molecule complexes are unique, similar uses are based on clinical observations. For example, in the glabellar frown line pivotal trials, 20 units of Botox® or Xeomin® and 50 units of Dysport® were used.4 Botox® is generally diluted with either 1.0, 2.0, or 2.5 mL of saline per 100 units, producing concentrations of either 10 units per 0.1 mL, 5 units per 0.1 mL, or 4 units per 0.1 mL, respectively. Xeomin® is diluted with 2.5 mL per 100-unit vial. Allergan’s pivotal trial used the 4 unit per 0.1 mL dilution. Dysport® is usually diluted with 1.5 mL of saline per 300-unit vial producing a concentration of 10 units in 0.05 mL as used in the pivotal trial. Notice that the Dysport® pivotal trial used injection volumes that were half those used in the Allergan trial: 0.05 mL (10 U) per injection point (Dysport®) versus 0.1 mL (4 U) per injection site (Botox®). It is unclear whether such differences in volume may contribute to behavioral differences between the 2 products in terms of diffusion and persistence. At some point, a larger volume might increase diffusion but probably decrease persistence since less drug would saturate the receptors in a given area. The use of sterile saline with preservative ( benzyl alcohol) as a diluent appears to lessen the sting of injection with Botox® and Dysport®. Myobloc®, the B serotype, causes more discomfort on injection because of its low pH, but it is stable in liquid form at room temperature for many months. In addition to the drug name changes, which the FDA required of the manufacturers in 2009, the agency instituted a Risk Evaluation and Mitigation Strategy (REMS), and a boxed warning for these products that warned of the possibility of spread distant from the injection site with potentially life-threatening consequences. Emphasizing the noninterchangeability of these commercial products, the FDA wished to minimize the possibility of medication errors as well as draw attention to the need for tailoring specific doses of each toxin product to specific situations.
IMMUNOLOGY
IMMUNOLOGY
The possibility of antibody-mediated resistance appears to be largely theoretical. Original Botox® batch No. 79-11, widely used in ophthalmology and neurology for years, produced rare cases of nonresponse in the treatment of torticollis and blepharospasm. Newer batches introduced in 1997, No. 91223US and No. BCB2024, have significantly less protein load. Although cases of primary nonresponse may be rarely encountered, immunologic resistance to Botox® and Botox Cosmetic® does not appear to be clinically relevant in dermatology, even at the dosages used to treat
3923
31
Sites of action of the different botulinum serotypes on the SNARE complex
Vesicle
BoNT/G TeNT BoNT/B BoNT/D
VAMP
BoNT/A
BoNT/C
BoNT/E
SNAP-25
BoNT/F
Plasma membrane Syntaxin
hyperhidrosis, which can average 400 units per treatment session. In addition, the treatment interval does not appear to be a significant factor in clinical resistance for the newer batches and at the smaller dosages used in cosmetic facial treatment, although exposure to the toxin at increasingly shorter intervals may theoretically be associated with development of neutralizing antibodies. In clinical practice, the reality of induced resistance on the basis of development of neutralizing antibodies is extremely rare, a fact bolstered by the
SEROTYPE INTRACELLULAR PROTEIN
A SNAP-25
B VAMP/synaptobrevin
C1 SNAP-25 and syntaxin
D VAMP/synaptobrevin
E SNAP-25
F VAMP/synaptobrevin
G VAMP/synaptobrevin
G VAMP/synaptobrevin
SNAP-25, synaptosome-associated protein of 25 kDa; SNARE, soluble N-ethylmaleimide-sensitive factor attachment protein receptor; VAMP, vesicle-associated membrane protein.
3924
difficulty in trying to purposefully induce resistance to the toxin through repeated vaccination.
INDICATIONS
Botulinum toxin is used in cosmetic dermatology primarily for the treatment of dynamic expression lines in the upper third of the face (the glabellar brow furrow, horizontal frontalis forehead lines, periocular rhytides aka crow’s feet) and for the treatment of axillary hyperhidrosis. Less common and therapeutically more challenging indications are platysmal banding in the neck, perioral rhytides, marionette lines at the corners of the mouth from the action of the depressor anguli oris, shaping the lower face with masseter volume reduction, postsurgical synkinesis in the lower face, and palmar/plantar and forehead/scalp hyperhidrosis.
TREATMENT
GLABELLAR LINES (BROW FURROWS)
GLABELLAR LINES
(BROW FURROWS)
A firm understanding of the underlying facial anatomy is the sine qua non of successful aesthetic therapy with botulinum toxin. Depending on the muscle
3
31
PROPRIETARY NAME BOTOX® BOTOX® COSMETIC DYSPORT® XEOMIN® MYOBLOC® RT001 TOPICAL RT002 INJECTABLE
Non-proprietary Name (FDA) Onabotulinumtoxin A Abobotulinumtoxin A Incobotulinumtoxin A Rimabotulinumtoxin B Daxibotulinumtoxin A
First approval 1989 (US) 2002 (US) 1991 (UK) 2010 (US) 2000 (US) Pending
Manufacturer Allergan (US) Ipsen (UK) Merz (Germany) Solstice Neurosciences (US) Revance Therapeutics (US)
Commercial US Yes Yes Pending US Yes Pending US
Serotype A A A B A
Strain Hall (Allergan) Hall Hall Bean Hall
Process Crystallization Chromatography Chromatography Chromatography Chromatography
Excipients HSA (500 µg) Sodium chloride HSA (125 µg) Lactose HSA (1 mg/vial) Sucrose (5 mg/vial) HSA (500 µg/mL) Sodium succinate Sodium chloride
HSA
Receptor/Target SV2/SNAP-25 SV2/SNAP-25 SV2/SNAP-25 Syt II/VAMP SV2/SNAP-25
Complex molecular weight uniformity ∼900 kDa homogeneous ∼500 kDa heterogeneous ∼150 kDa ∼700 kDa homogeneous ∼150 kDa
Stabilization Solubilization pH
Vacuum dried Normal saline ∼ 7
Lyophilization Normal saline ∼ 7
Vacuum dried Normal saline ∼ 7.4
Solution N/A 5.6
Lyophilization Normal saline ∼ 7
Package (units per vial) 100, 200 300, 500 100 2500/5000/10,000 50
∼5 (100-U vial) 4.35 (500-U vial) 0.6 (100-U vial) 25/50/100 1 (100-U vial)
Neurotoxin protein per vial (ng/vial) ∼5 (100-U vial) 4.35 (500-U vial) 0.6 (100-U vial) 25/50/100 1 (100-U vial)
Neurotoxin protein
per vial (ng/vial)
mass present and the degree of atrophy from prior treatment, 20 to 35 units of Botox® or Xeomin® or 50 to 75 units of Dysport® may be placed in 5 separate injection points to treat the corrugators and procerus muscle in the average brow (Fig. 216-4). A 30-gauge, 31-gauge, or even 32-gauge needle and a tuberculin or diabetic syringe are used to minimize the trauma of the intramuscular injections. The corrugator injections are placed (1) just at or above the medial brow and (2) in or just medial to the midpupillary line, at least 1 cm above the bony orbital rim (see Fig. 216-4). The fifth injection is placed in the procerus at the midline at a point just above the horizontal creases created in the glabella at the bridge of the nose. Figure 216-5 shows the results of the procedure. Based on earlier experience with ophthalmologic periocular injections for treatment of muscle spasms, patients have been instructed to remain upright for 2 to 3 hours to limit the incidence of eyelid ptosis, which occurs with diffusion of the toxin down into the levator muscles of the lid (Fig. 216-6). With operator experience, the incidence of ptosis after injection of the brow should be less than 2%. Temporary stimulation of Müller muscle in the lid can be achieved with 0.5% apraclonidine or 2.5% phenylephrine eyedrops or even naphazoline hydrochloride 0.025%/pheniramine maleate 0.3% eyedrops (Naphcon A® available over the counter)
(see Fig. 216-6). These will produce 2 to 3 mm of elevation of the lash margin, and administration may be repeated at intervals of 4 to 6 hours as needed until the distant diffusion effect of the botulinum toxin on the levator muscle disappears, usually in 2 to 3 weeks.
HORIZONTAL FOREHEAD LINES
HORIZONTAL
FOREHEAD LINES
The frontalis is treated at the horizontal equator of the forehead or above to avoid inactivation of the lower third of the frontalis muscle, which is responsible for suspension and movement of the eyebrows (see Figs. 216-4 and 216-7). Twelve to 20 units of Botox® or 20 to 50 units of Dysport® are placed in 4 or 5 divided doses equidistantly along the forehead equator. If too large a dose is applied or injection sites are placed too low, brow ptosis and loss of brow arch are produced, which leads to an unpleasant, heavy sensation in the brow as well as an aesthetically unattractive appearance in females. Unlike in the treatment of eyelid ptosis, there is no comparable adrenergic agent available to reverse brow ptosis induced by botulinum, and the patient
3925
31
PROPRIETARY NAME PURTOX® MEDITOXIN® NEURONOX® DWP-450, EVOSYAL®, NABOTA® BOTULAX® HENGLI®/ PROSIGNE® ANT-1207 TOPICAL AI-09 INJECTABLE
Non-proprietary Name (FDA) Not named Licensed to Allergan Outside Korea Outside US only Outside US only Outside US only In trials US
First approval No approval 2006 (Korea) 2013 (Korea) 2010 (Korea, Japan) 1993 (China) Pending US
Manufacturer Mentor (J&J) (US) Medy-Tox (Korea) Daewoong Pharma (Korea), Alphaeon (US), Evolus, Inc. (US)
Hugel Pharma (Korea) Lanzhou (China) Anterios (US) Acquired by Allergan 2016
Commercial US No approval No Pending No No Pending
Serotype A A A A A A
Strain Hall Hall Hall Clostridium CBFC26 Hall Hall
Process Chromatography Chromatography Chromatography Chromatography Crystallization Chromatography
Excipients HSA Trehalose HSA (500 µg) Sodium chloride HSA (500 µg) Sodium chloride HSA (500 µg) Sodium chloride Porcine gelatin 5 mg Dextran 25 mg Sucrose 25 mg
Unpublished; Proprietary NDS technology
Receptor/target SV2/SNAP-25 SV2/SNAP-25 SV2/SNAP-25 SV2/SNAP-25 SV2/SNAP-25 SV2/SNAP-25
∼150 kDa ∼150 kDa ? ∼150 kDa 900 kDa ∼500 kDa heterogeneous ? 150 kDa
Complex molecular weight uniformity
Stabilization Solubilization pH
Lyophilization Normal saline ∼7
Lyophilization Lyophilization Freeze Dried 6.5 ± 0.5 Lyophilization Liquid
Package (units per vial) 100 50/100 100 50/100/200 100 Unpublished
Neurotoxin
1 (100-U vial) ? ? <2.5 / <5.0 / <10 ? Unpublished
Neurotoxin protein per vial (ng/vial)
1 (100-U vial) ? ? <2.5 / <5.0 / <10 ? Unpublished
protein per vial (ng/vial)
must wait several weeks for the effect to wear off. In a patient who has never received botulinum toxin before, it is wise to separate the glabellar area from the forehead area and to wait a couple of weeks between treating the two to avoid the possibility of overtreatment and brow ptosis. Many patients find even the smallest drop in brow position very bothersome, and great care should be taken to avoid this complication of aesthetic treatment.
LATERAL CANTHAL LINES (CROW’S FEET)
LATERAL CANTHAL LINES
(CROW’S FEET)
The rhytides at the corners of the eye respond favorably to injections of toxin; however, patients frequently confuse true crow’s feet rhytides with the dynamic expression lines that appear across the malar eminence laterally in conjunction with smiling and contraction of the zygomaticus muscles. Toxin may successfully ameliorate true crow’s feet, which radiate directly
3926
from the lateral canthus and are associated with contraction of the orbicularis oculi muscles by themselves. But the “smile lines” that appear over the malar eminence often lie in wait for the unwary injector. Placing toxin at or below the malar eminence in an attempt to weaken these lines may lead to paralysis of the zygomaticus muscles and a drooping corner of the mouth that cannot spontaneously be raised, so that the patient may acquire a poststroke appearance. To safely approach crow’s feet, the toxin is usually placed at 1 to 3 injection points approximately 1 cm lateral to the lateral canthus. Some practitioners place all of the drug at one point, and others distribute the dose evenly among 3 points. Typical doses range from 10 to 18 units of Botox® or 25 to 30 units of Dysport®
depending on the estimate of muscle mass and activity. Great care must be taken to make the injections into the skin only, raising wheals or blebs that can be gently massaged down. Intramuscular injection in this area will reliably produce unwanted bruising because of the rich venous plexus underlying the skin in this region. The toxin will readily diffuse from the blebs into the underlying orbicularis muscle, relaxing
Sites of injections on the forehead
the grip on the overlying skin and smoothing out the wrinkles. As previously mentioned, care must be taken to avoid injecting too low down onto the malar eminence, where diffusion may affect the zygomaticus major muscle and disrupt the symmetrical movement of the corner of the mouth in smiling. The patient being treated for crow’s feet should have good lower eyelid tarsal tone to avoid the appearance of senile ectropion from too much laxity of the lower eyelid. Pretreatment of the crow’s feet area is very useful as an adjunctive technique before laser resurfacing. It prevents the problem of rhytides being readily re-formed by repeated squinting during the postoperative healing period, in which case the resurfacing may give rise to more noticeable lines than existed before the resurfacing.
COMBINATION THERAPY
COMBINATION THERAPY
As clinical experience accumulated with these commercial botulinum toxin products, experts in softtissue augmentation soon recognized that a synergy exists between soft-tissue fillers and neurotoxins.5
Concomitant with the rise in the use of botulinum neurotoxin for cosmetic applications, the marketplace
3
31
for soft-tissue augmentation expanded with the introduction of injectable hyaluronic acid gels (Chap. 215). These agents provided the first new directions in cosmetic therapy since the introduction of solubilized bovine collagen in the mid-1970s. The ability to control both muscles of expression and their secondary lines and folds, and to repair age-related volume changes in subcutaneous tissue has revolutionized minimally invasive cosmetic techniques. Many patients have eagerly embraced simultaneous treatment with both fillers and botulinum toxin to achieve a natural look and forego more traditional incisional surgery.6 As an example, patients frequently combine treatment of the upper third of the face (glabellar frown lines, horizontal forehead lines, and crow’s feet) with volume restoration of the lower and middle face (lip enhancement, filling of nasolabial fold and marionette lines, chin and cheek augmentation) (Chap. 215).
HYPERHIDROSIS
HYPERHIDROSIS
Focal axillary hyperhidrosis is successfully treated with botulinum toxin by using Minor starch-iodine test to map out the extent of surface area in the axillary vault
3927
31
that is affected. Anesthesia may be achieved with a eutectic mixture of local anesthetics but is usually not needed because of the relative insensitivity of the axillary skin. Doses of 2.5 to 4.0 units of Botox® are placed every 1 to 2 cm as intradermal injections in axillary skin. Reliable anhidrosis is produced within 72 hours and will last for 8 to 12 months with doses of 50 to 100 units of Botox®
per axilla (Fig. 216-8). The duration of effect appears to be dose related, and doses of up to 200 units (Dysport®) per axilla have been reported to produce dryness for up to 29 months.7 Aside from insignificant bruising from the needle trauma, there are no apparent side effects. Compensatory hyperhidrosis is not a clinically significant side effect, probably because of the relatively small surface area of the axillary vaults in contrast to the much larger surface areas affected by the surgical interruption of the nerves that occurs with endoscopic cervical sympathectomy, where compensatory hyperhidrosis is a real concern in up to a third of patients treated. Palmar hyperhidrosis (Fig. 216-9) is more challenging to treat because of (1) the more limited diffusion of the toxin in palmar skin, (2) the pain on injection, and (3) the generally predictable incidence of temporary weakness in the hand. Anesthesia is achieved with regional wrist blocks of the median, ulnar, and radial nerves using lidocaine 1% to 2% without epinephrine. Approximately, 100 to 150 units of Botox®
are needed to treat a single palm, divided into 50 to 60 intradermal injections of 2 to 3 units each. Onset of anhidrosis peaks in 5 to 7 days and is accompanied by
3928
minor weakness of the intrinsic muscles of the hand, which makes tasks requiring strength and stability (eg, pushing a button through a buttonhole) difficult to perform. The weakness usually subsides within 3 weeks, whereas the anhidrosis persists for several months. There is wider variation in response to palmar treatment than to axillary treatment, with anhidrosis lasting from 4 to 12 months, which probably reflects the technical difficulties in achieving even dispersion of the toxin through the palmar skin.
SIDE EFFECTS AND COMPLICATIONS
Minor needle trauma and bruising on injection with a 30-gauge needle are insignificant short-term complications of botulinum toxin injection, and use of a smallergauge needle (31 gauge or 32 gauge) will minimize needle trauma. Minor discomfort can be made more tolerable in some patients by pretreating the injection site areas with topical anesthetic and using sterile saline with preservative as a diluent, which greatly reduces the sensation of injection.
3
31
The more problematic complications to consider are eyelid ptosis, which can occur after injections in the glabellar brow (see Fig. 216-6); brow ptosis from overzealous treatment of the frontalis muscle; transient lid edema from periocular injections; headaches after injections anywhere in the upper third of the face; and palmar weakness after injections for hyperhidrosis. Antibody-mediated resistance appears to be an exceedingly rare event and of little clinical consequence in cosmetic dermatologic uses of botulinum toxin. Although millions of doses have been given as of this writing, there is no well-documented evidence of the development of immunologic resistance in patients treated with cosmetic doses. Resistance continues to be observed in patients treated for cervical dystonia, albeit at much lower rates than in the early years, probably because of the lower protein content of current formulations. Eyelid ptosis is thought to be best avoided by carefully placing the midbrow injections at a minimal distance of 1 cm from the superior orbital rim, keeping the injection rate slow and gentle, and having the patient avoid prone positions and sleeping for 2 hours after injection. Restricting injections to the upper two-thirds of the frontalis and reducing doses to the minimum necessary to produce the desired clinical effect may minimize brow ptosis. Unopposed muscle groups may trigger headaches as a rebound phenomenon after facial injections of botulinum toxin, but their etiology is unclear. Usually nonsteroidal anti-inflammatory agents are sufficient to treat them, unless the patient experiences migraines, in which case the patient’s usual migraine medication will be required. In hyperhidrosis, palmar weakness is a predictable consequence of injecting the palms. It is transient and dealt with by clear preinjection counseling. There is no similar effect of any clinical significance in either the axillae or the feet.
3929
31
COSMETIC USES “OFF-LABEL”
At the present time, the only FDA-approved indications for cosmetic botulinum toxin are the glabellar frown lines and the lateral canthal lines or crow’s feet. But clinicians have described a variety of different anatomic locations that can benefit from carefully dosed botulinum toxin. These include the horizontal lines on the forehead (frontalis muscle),8,9 the vertical rhytides of the upper lip (orbicularis),10,11 the rhytides from nasalis muscles (“bunny lines”),12 the melomental folds at the corners of the mouth (depressor anguli oris),13,14
the deep mental crease on the chin and pebbly or peau d’orange chin (mentalis),15 hypertrophy of the masseters (squared lower face),16,17 and horizontal neck lines and bow-string bands of the neck (platysma).18,19 The techniques and doses for these indications have been widely discussed, but few have been systematically studied.
SUMMARY
The development of botulinum toxin treatment has brought great creativity and capability to cosmetic dermatologic therapy. Further evolution will occur as new serotypes come to market and greater therapeutic synergies evolve as developers of soft-tissue augmentation systems strive to achieve similar effect and elegance. The high degree of efficacy and safety in the use of botulinum toxins in cosmetic dermatology has produced a great level of satisfaction in patients and physicians alike.
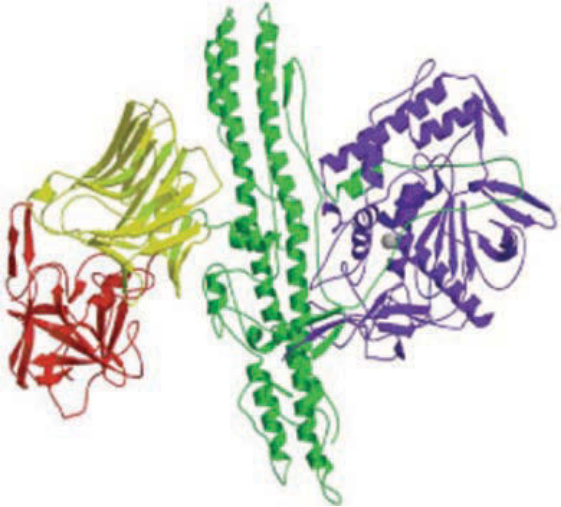
Figure 216-1 Schematic of the botulinum complex showing the binding domain with the N-terminus (yellow) and the C-terminus (red), together with the translocation domain (green) and the light chain (blue). (Used with permission from Turton K, Chaddock JA, Acharya KR. Botulinum and tetanus neurotoxins: structure, function and therapeutic utility. Trends Biochem Sci. 2002;27:554. Copyright © Elsevier.)
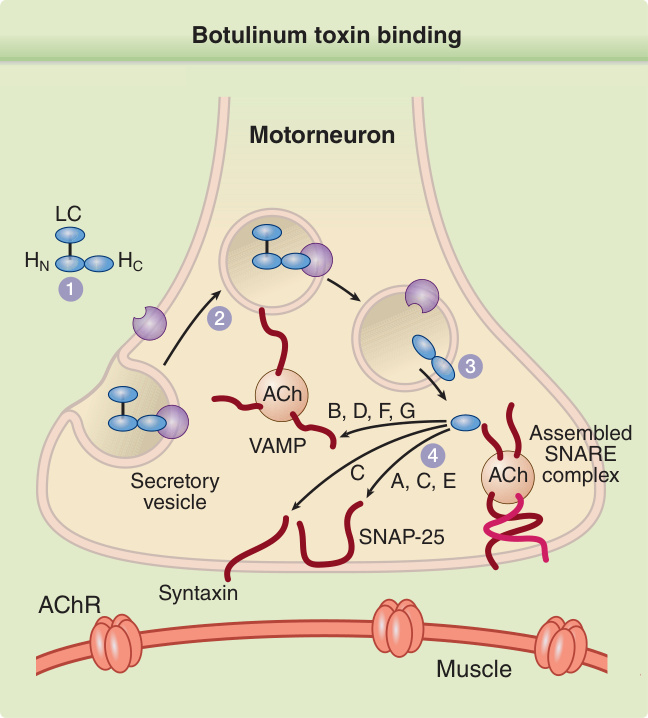
Figure 216-2 The heavy-chain domain of the botulinum neurotoxin complex binds to the plasma membrane receptor (1), and the complex is internalized (2). The lightchain fragment is then released into the cytoplasm (3), where it cleaves the SNARE (soluble N-ethylmaleimidesensitive factor attachment protein receptor) protein complex at a site determined by the neurotoxin serotype (4). This disruption of the SNARE complex prevents exocytosis of acetylcholine (ACh) into the synaptic space of the neuromuscular junction n. A through G, neurotoxin serotypes; AChR, acetylcholine receptor; LC, light chain; HC, heavy chain C-terminus; HN, heavy chain N-terminus; SNAP-25, synaptosome-associated protein of 25 kDa; VAMP, vesicleassociated membrane protein. (Used with permission from Turton K, Chaddock JA, Acharya KR. Botulinum and tetanus neurotoxins: Structure, function and therapeutic utility. Trends Biochem Sci. 2002;27:555. Copyright © Elsevier.)
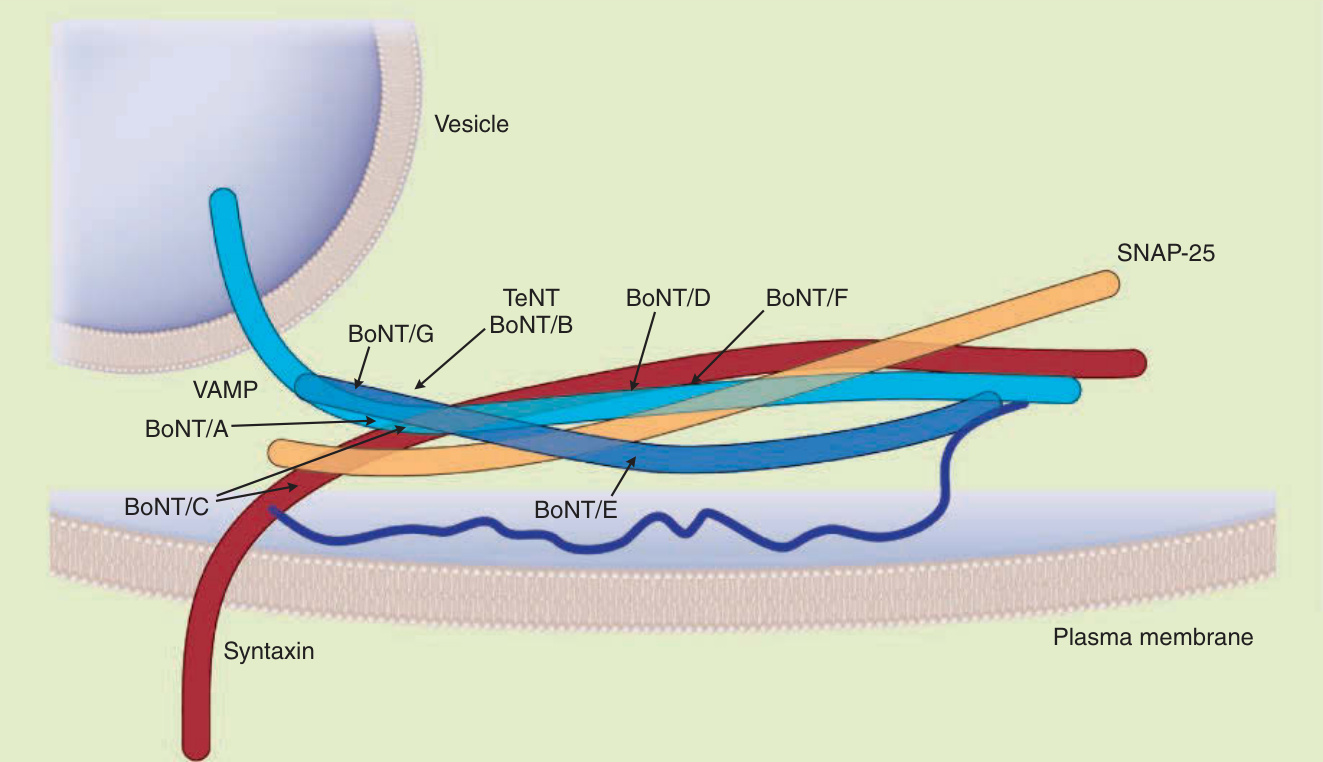
Figure 216-3 Schematic representation showing the sites of action of the different botulinum serotypes on the intracellular protein complex known as the SNARE (soluble N-ethylmaleimide-sensitive factor attachment protein receptor) proteins responsible for exocytosis of acetylcholine from the nerve. Botulinum A serotype cleaves SNAP-25 ( synaptosome-associated protein of 25 kDa). Other serotypes impact VAMP (vesicle-associated membrane protein), synaptobrevin, or syntaxin. BoNT/A through BoNT/G, botulinum neurotoxin serotypes A through G; TeNT, tetanus neurotoxin.
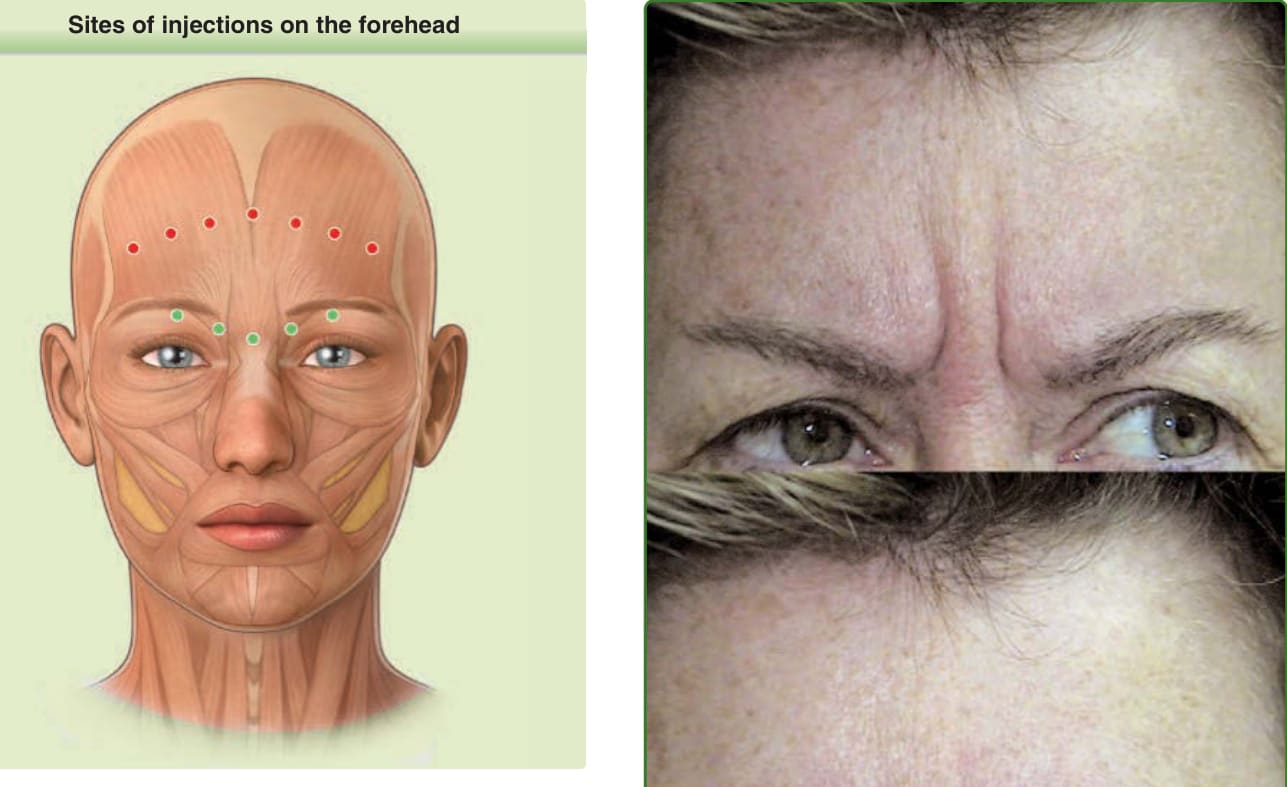
Figure 216-4 Sites of injections on the forehead. The corrugator and procerus muscles are weakened by carefully positioning 5 injections of botulinum toxin of 5 units each (Botox®) (green circles). If Dysport® is used, 10 units would be placed in the 3 central injection points but the lateral corrugator injection points (represented by the red circles) are a little medial and slightly higher than the lateral injection points used for Botox,® in most cases, according to Ascher.15 Forceful knitting of the brow is prevented. To weaken the frontalis muscle, injections are placed in 5 or more divided doses along the forehead equator (red circles).

Figure 216-5 Before botulinum toxin treatment of the corrugator and procerus muscles (upper panel) and 1 week after treatment (lower panel).
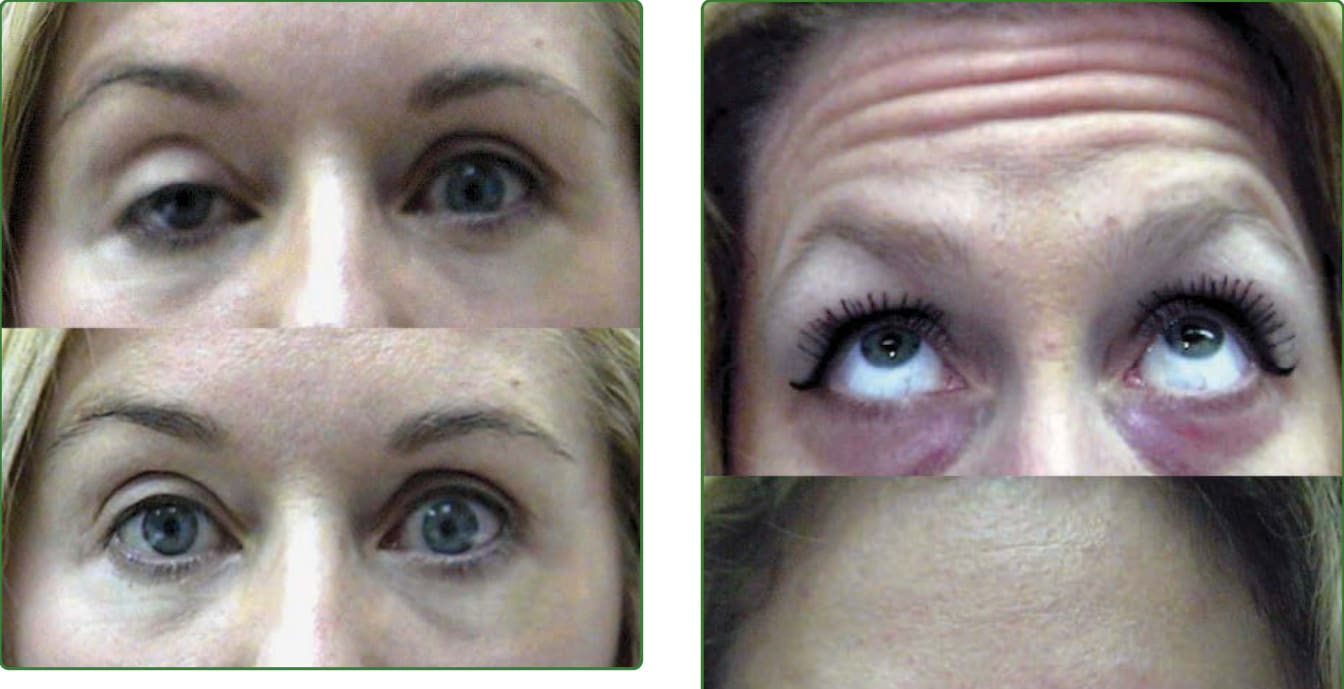
Figure 216-6 Patient who developed ptosis of the right upper eyelid due to diffusion of the botulinum toxin from the area above the midbrow down into the levator muscle of the upper eyelid. The lower photograph shows the patient approximately 1 minute after instillation of 2 drops of apraclonidine 0.5% ophthalmic solution into the right eye. Direct adrenergic stimulation of Müller muscle occurs, which lifts the lid temporarily. The drops may be administered every 4 hours as needed. The botulinum-induced ptosis resolves spontaneously, usually in 3 weeks or less.

Figure 216-7 The upper half of the frontalis muscle is weakened by injecting 4 or 5 sites equidistantly along the equator of the forehead with a total of 16 to 20 units of Botox® or 30 to 50 units of Dysport®. Patient is shown before treatment (upper panel) and 1 week after treatment (lower panel).

Figure 216-8 Minor starch-iodine test is used to demonstrate the area of axillary sweating (top panel). The pattern of intradermal botulinum toxin injections is shown with the starchiodine material in place to highlight the injection points (middle panel). One week later, the treated axilla shows a negative result on the starch-iodine test (bottom panel).

Figure 216-9 Hands showing response to Minor starch-iodine test. The left hand was not treated. The right hand received 100 units of intradermal Botox® 1 week before the photograph was taken.
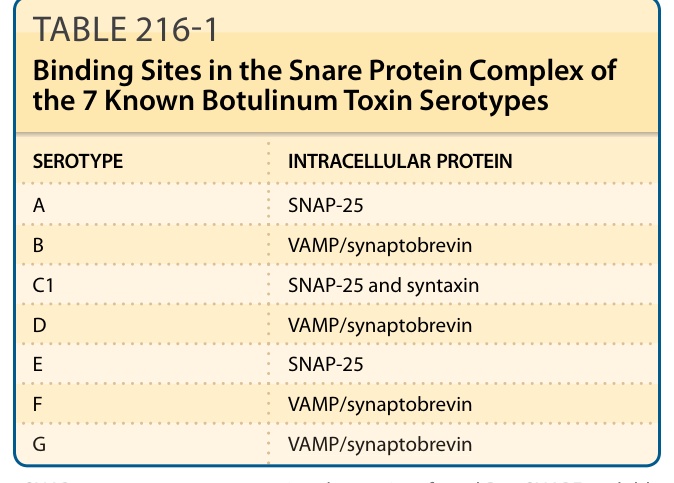
TABLE 216-1 Binding Sites in the Snare Protein Complex of the 7 Known Botulinum Toxin Serotypes
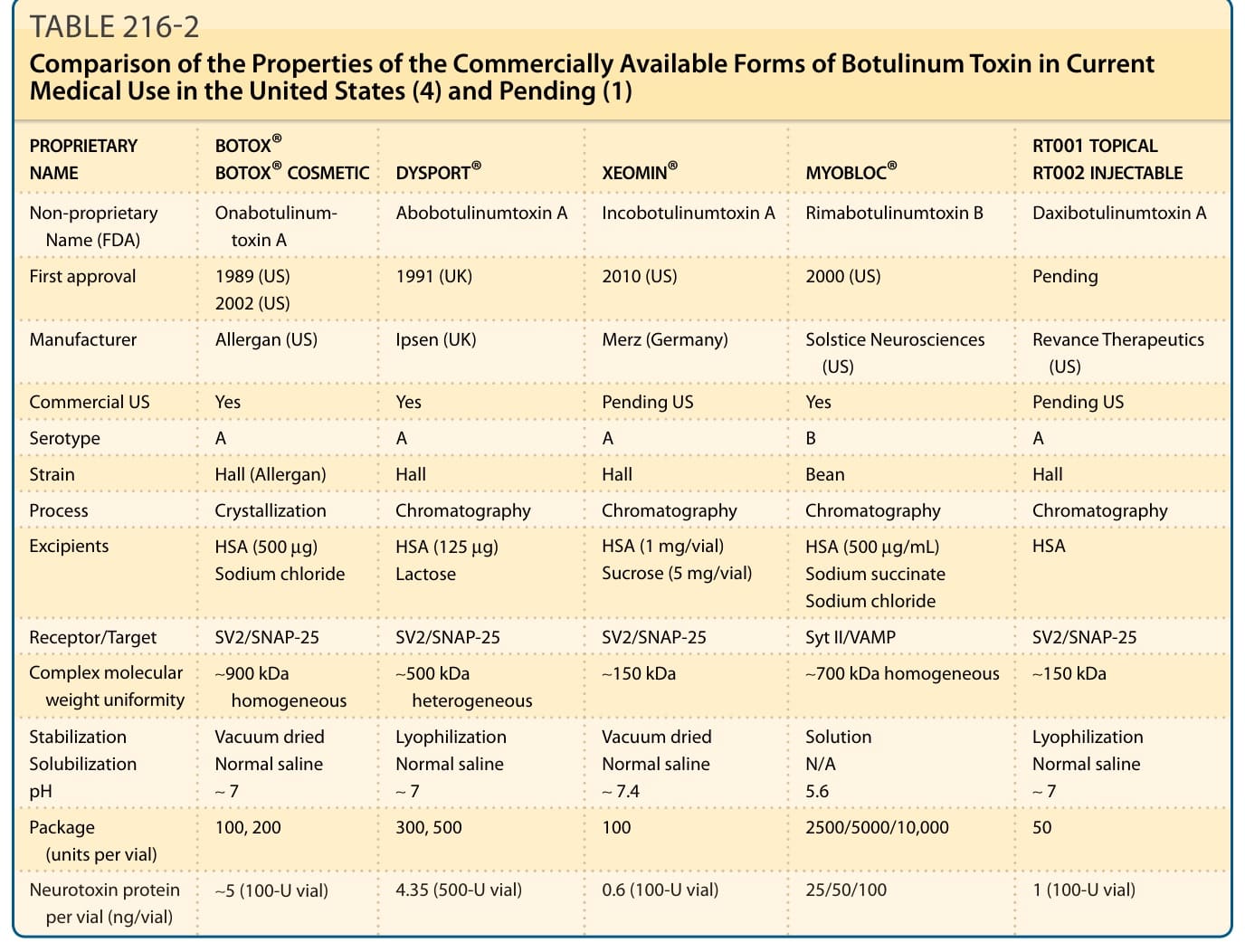
TABLE 216-2 Comparison of the Properties of the Commercially Available Forms of Botulinum Toxin in Current Medical Use in the United States (4) and Pending (1)
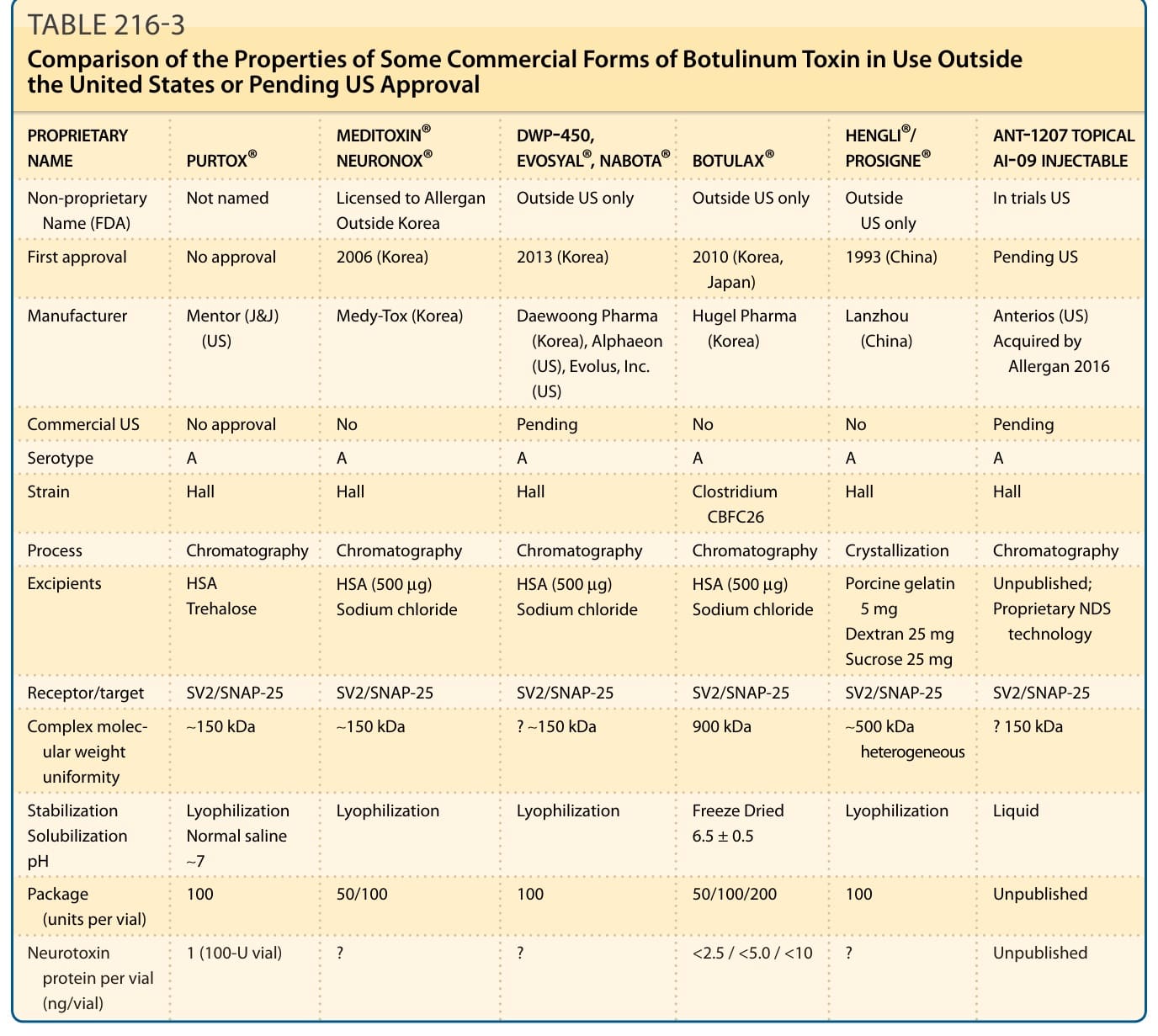
TABLE 216-3 Comparison of the Properties of Some Commercial Forms of Botulinum Toxin in Use Outside the United States or Pending US Approval