Soft-Tissue Augmentation
3
31
AT-A-GLANCE
■ Soft-tissue fillers are used for multiple cosmetic and therapeutic indications.
■ A wide variety of injectable soft-tissue fillers are available for clinical use, including biodegradable products such as hyaluronic acid, collagen, calcium hydroxylapatite, and poly-l-lactic acid; products that remain indefinitely in tissue, such as polymethylmethacrylate microspheres, hydrogel polymers, and silicone; and viable autologous fat.
■ Adequate clinician training in the use of these agents is essential for the prevention of adverse events.
As we age, lines, grooves, and creases become more apparent. Superficial rhytides are largely caused by solar damage, characterized by the loss of collagen at the epidermal–dermal junction and an increased elastosis in the reticular dermis. Repetitive facial movement over the years produces pronounced rhytides in the most active areas of the face, such as the forehead, glabella, periorbital and perioral areas, and nasolabial folds. Rhytides tend to appear deeper in the nasolabial and melolabial creases with the compounding feature of soft-tissue atrophy.1
Facial rejuvenation comes in many forms; its primary stake being replacement of soft-tissue volume by an assortment of augmentation techniques. Two major categories are subcutaneous volumizers and dermal fillers. Although subcutaneous volumizers tend to provide more long-lasting results, with improvements in dermal fillers over the past several years, these products have become increasingly popular and are now widely used. When deciding which technique(s) to use in the correction of facial soft-tissue atrophy, an accurate diagnosis of the level(s) of volume loss must be made. In younger patients, dermal fillers may be adequate for treatment, while in a more advanced aging face, a combination of the two above categories may be necessary to obtain optimal results. 1
METHOD AND TECHNIQUE
Dermal filler use began in the mid 1980s and has since become the cornerstone of facial filling in the office setting.1 There are several dermal fillers approved for use in the United States (Table 215-1). Soft-tissue fillers (Table 215-2) are either injected through a sharp needle or blunt cannula. The level of injection into the skin and the length of the needle chosen depend on
the type of filler injected, the properties of the filler, the area injected, and the desired result. Threading is a technique in which the needle is inserted into the skin and the filler is deposited in a linear fashion along the track of the needle as it is being withdrawn. Fanning is a type of threading in which, instead of inserting the needle into a new area each time, the needle is just withdrawn so that a new track can be made radially adjacent to the last. In the “push-ahead” technique, an injection is made in an anterograde direction, so that the injectable material flows from the tip of the needle and hydrodissects the tissues as it flows. This technique is often used in areas where bruising is more likely to occur along the needle track, such as the upper lid and brow. In the depot method of injection, small “pearls” of material are deposited serially, usually along a fold or deep by bone. Crosshatching is an approach used to diffusely cover an area with the injected material. In this method, linear threads are lined up in succession and a second series of rows is then layered at right angles to the first. Some of the more viscous fillers on the U.S. market are injected in a deep subcutaneous bolus through a blunt cannula or large-bore needle. Figure 215-1 illustrates the different injection techniques. Whichever technique is chosen, care should be taken in highly vascular areas to avoid intravascular injection of filling material. With each injection, the plunger of the syringe should be drawn back to check for blood flow, and if it is found, the needle should be withdrawn and repositioned.
COLLAGENS
Once considered the “gold standard” of dermal fillers, collagens (bovine, human, and porcine) are no longer available on the U.S. market.
NONABSORBABLE (PERMANENT) MATERIALS
NONABSORBABLE
(PERMANENT) MATERIALS
One collagen-containing product worth mentioning is polymethylmethacrylate (PMMA microspheres). PMMA is a nonbiodegradable, biocompatible, synthetic polymer that is often used in other medical devices, such as bone cement and intraocular lenses.1
PMMA beads are minuscule, round, smooth particles that are not absorbed by the body. When used as a softtissue filler, these beads are suspended in a gel-like solution that contains cow (bovine) collagen and are injected into the face. A few months after it is injected, the collagen gel breaks down and natural collagen fills
31
TRADE NAME MATERIAL
Restylane Silk Hyaluronic acid with lidocaine
ArteFill (no longer available) Polymethylmethacrylate beads, collagen, lidocaine
Bellafill Polymethylmethacrylate beads, collagen, lidocaine
Fibrel (no longer available) Collagen
Sculptra Poly-L-lactic acid
Sculptra Aesthetic Poly-L-lactic acid
Restylane Injectable Gel Hyaluronic acid
Restylane-L Injectable Gel Hyaluronic acid with lidocaine
Restylane Lyft with Lidocaine Hyaluronic acid with lidocaine
CosmoDerm 1 Human-Based Collagen (no longer available) Collagen
Captique Injectable Gel Hyaluronic acid
Prevelle Silk Hyaluronic acid with lidocaine
Hylaform Modified hyaluronic acid (avian source)
Belotero Balance Hyaluronic acid
Zyplast (no longer available) Collagen
Evolence Collagen Filler (no longer available) Collagen
Radiesse Hydroxylapatite
Elevess Hyaluronic acid with lidocaine
Juvederm Hyaluronic acid
Juvederm Voluma XC Hyaluronic acid with lidocaine
Zyderm Collagen Implant (no longer available) Collagen
Revanesse Versa Hyaluronic acid
Juvederm Vollure XC Hyaluronic acid
Juverderm Volbella XC Hyaluronic acid with lidocaine
Restylane Refyne Sodium hyluronate
Restylane Defyne Sodium hyluronate
Restylane Defyne Sodium hyluronate
out the residual space. This dermal filler is considered semipermanent, and is most often used to treat medium-to-deep rhytides and folds, particularly the nasolabial creases. It is also used by some to fill pitted scars and to augment the lips.
HYALURONIC ACIDS
PATIENT SELECTION
PATIENT SELECTION
Hyaluronic acid–derived fillers are a good choice for patients who desire a long period of correction or more volume enhancement. They are currently approved for augmentation of the nasolabial folds, mid cheeks, and lips, but other common areas of treatment include
3912
the labiomental crease and periorbital areas. Patients often feel that the hyaluronic acid fillers are softer and more natural in appearance than the collagens were, but they need to be warned about the risk of increased erythema, edema, and bruising associated with these products.
FORMULATIONS
FORMULATIONS
Hyaluronic acid is a polysaccharide and a normal extracellular component of most mammalian tissues including the dermis. Hyaluronic acid polymers offer superb biocompatibility and provide the same structural and mechanical properties of normal subcutaneous tissue. Injectable U.S. Food and Drug Administration (FDA)-approved forms include non– animal-derived stabilized hyaluronic acid products made through a bacterial fermentation process and an avian-derived version isolated from cocks’ combs. Brands of injectable hyaluronic acids differ not only in their derivation but also in their concentration of hyaluronic acid per milliliter of product, type of crosslinking or stabilizing agents, viscosity, and particle size. In its native form, hyaluronic acid has a short life span. However, crosslinking increases its longevity. As the proportion and degree of crosslinking increases, the gel becomes more and more like a solid, is more resistant to degradation by enzymes and free radicals, and as such, tends to persist longer in tissue. Injection of crosslinked hyaluronic acid into the deep dermis also has been shown to increase de novo collagen synthesis by fibroblast stretching, resulting in even longerlasting correction.1 Some hyaluronic acid products exist as biphasic gels containing both crosslinked and uncrosslinked particles, and some as monophasic gels containing only crosslinked particles. The biphasic non–animal-derived stabilized hyaluronic acid products are made en bloc initially and then passed through a sieve to create particles ranging in size from 10,000 per mL to 100,000 per mL with a hyaluronic acid concentration of 20 mg/mL. The smaller particle size permits injection through smaller-gauge needles into finer wrinkles and the larger particle size is best for volumetric filling. The small amount of non-crosslinked hyaluronic acid allows for smooth flow with low injection pressures. Monophasic hyaluronic acid gels are produced by varying the amount of high- and low-molecular weight hyaluronic acid, producing a hydrogenous gel. The monophasic product is available in 2 formulations, one containing 24 mg/mL of hyaluronic acid and one containing 30 mg/mL of hyaluronic acid. The crosslinking agent used in both the monophasic and biphasic products is BDDE (1,4-butanediol diglycidyl ether). The avianderived hyaluronic acid, contains 6 mg/mL of hyaluronic acid highly crosslinked with divinyl sulfide. The hydrophilic nature of hyaluronic acid allows it to create larger volumes relative to its mass. This property makes hyaluronic acid fillers especially useful for soft-tissue augmentation. The hyaluronic acid fillers
3
31
FILLER USES TYPE PLACEMENT COMPLICATIONS LONGEVITY
Hyaluronic acid Treatment of medium-todeep folds, lips, acne scars, periorbital hollows, facial contouring
Non–animal-derived stabilized hyaluronic acid
Calcium hydroxylapatite Treatment of deep folds, nipple reconstruction, nasal reconstruction, jawline, malar augmentation
Mid-to-deep dermis or superficial subcutis
Allergic reaction or inflammation, blue discoloration, misplacement, lumps
6 to 12 months
Calcium hydroxylapatite Deep dermis to superficial subcutis Nodules (especially in lips and periorbitally), misplacement with demarcation of product
Poly-L-lactic acid Treatment of HIV lipoatrophy, nasolabial fold, cheek, and temple hollows
6 to 18 months
Poly-L-lactic acid Superficial subcutis Visible and palpable papules 2 years or longer
Autologous fat Pan-facial filling, especially periorbital area Autologous fat Subcutaneous tissue Bumps, vascular occlusive events with injudicious placement
Silicone Treatment of scars, HIV
5 years or longer
Silicone oil Deep dermis Delayed granuloma
Silicone Treatment of scars, HIV lipoatrophy, lips, deep folds
—
Silicone oil Deep dermis Delayed granuloma formation, migration —
lipoatrophy, lips, deep folds
Injection techniques
Threading 1
Direction of needle when injecting
Depot 2
Static needle
Fanning 3
Arrows indicate direction of needle when injecting
Crosshatching 4
Injections are retrograde and overlapping
Push-ahead 5
Static needle
Arrow indicates direction of filler flow
formation, migration
have an excellent tolerability profile and can be used without the need for skin testing.1
ANESTHESIA
ANESTHESIA
As a consequence of their high viscosity, hyaluronic acid products can cause significant discomfort on injection so most hyaluronic acids on the market are combined with lidocaine. As such, it is often beneficial to inject antegrade (in addition to retrograde), as placement of the lidocaine-containing product ahead of the needle tip, can help decrease the associated pain. Topical anesthetic also can be applied before injection. This usually results in adequate anesthesia for periorbital, nasolabial fold, and labiomental crease injections; however, if lips or perioral rhytides are being treated, an ancillary local infiltration of 1% lidocaine or segmental nerve block may be indicated.
TECHNIQUE
Hyaluronic acids should be injected with the patient in a position that elicits the defect or creases to be treated and offers ease of injection to the operator. This is best accomplished by reclining the patient to a 45-degree angle. All the hyaluronic acid products come with a needle in the gauge of choice for ease of injection and preservation of the physical properties of the gel. However, because of their viscoelastic properties, the hyaluronic acids can often be injected through needles tailored to the area or level of injection. For instance, a 32-gauge needle allows for more precise injection of vertical lip rhytides and a 1.5-inch needle may facilitate injection into distal sites. Hyaluronic acids are injected in most areas via threading, depot, or fanning. They
3913
31
A
B
are particularly amenable to crosshatching in areas where a greater density of augmentation is desired. In particular, when hyaluronic acid is injected into the nasolabial fold it is important to span the width of the fold with a serial threading technique and then crosshatch at right angles. This gives structural integrity to the fold and prevents the undesirable result of merely moving the fold medially (Fig. 215-2). In addition, it is often necessary to “suspend” the fold by augmenting the cheek. This is usually done with a deep bolus injection of a high density hyaluronic acid. The labiomental crease can be injected similarly to the nasolabial fold, again blending the product so as not to move the fold medially. Lip injections are made using a depot or threading technique, either along the vermilion border, in the body of the lip, or in a combination of both. Perhaps one of the most exciting off-label applications of hyaluronic acids is the correction of tear trough deformity or suborbital hollows. Injections are made either under the orbicularis oculi muscle near the orbital bone or subdermally above the muscle. Intramuscular injections are to be avoided as the movement in this area increases the risk of lumping of the product. A depot method of injection in which very small amounts of hyaluronic acid are deposited on each pass is preferred, but threading also can be helpful to ensure even blending into neighboring areas. The push-ahead technique is preferred for the sub-brow area. After injection, the periorbital area should be vigorously massaged to disperse the product and minimize aggregation of gel particles. Although periorbital injection of hyaluronic acid results in high levels of patient satisfaction, it is an advanced injection method best left to those with the greatest injecting experience.
POSTPROCEDURE INSTRUCTIONS
POSTPROCEDURE
INSTRUCTIONS
The application of ice immediately after the procedure and periodically throughout the day is recommended after the injection of hyaluronic acid. Patients are
3914
instructed to avoid manipulation of the treated area and extremes of temperature for the first 48 hours after injection. If the lips were treated in a patient with a history of cold sores, then an antiviral medication should be administered prophylactically on the day of the procedure. Patients are instructed to return to the office if they experience any problem such as redness, purulence, or nodule formation.
UNIQUE COMPLICATIONS
UNIQUE COMPLICATIONS
Common side effects of dermal fillers include bleeding or bruising during and following the procedure. Patients should expect some degree of pain during injections. As recommended above, the application of ice to the injection sites can decrease these symptoms. Most additional complications result from improper application of the product. Placement of this clear gel too superficially results in a blue discoloration, known as the Tyndall effect. This occurs as superficial injection allows for more water binding in the dermis, which selectively reflects the blue wavelength of light, making it appear darker than the surrounding skin. Placement of too large an aliquot can result in a noninflammatory bump. Most ill-placed hyaluronic acid can be removed by incising with a 20-gauge needle and expressing the material. An important characteristic of the hyaluronic acid products is their ability to break down with the use of an enzyme known as hyaluronidase. This enzyme breaks the crosslinks by hydrolysis of the glucosamine and glucuronic acid moiety. A few hyaluronidase products are commercially available in the United States in 200 units/mL and 150 units/mL vials. Approximately 15 to 20 units of hyaluronidase can be injected directly into a pea-sized volume of hyaluronic acid, leading to its degradation within minutes to hours. Hyaluronic acid products also contain small amounts of impurities that can cause hypersensitivity reactions; true allergic reactions, however, are exceedingly rare. Patients can react to sterile bacterial proteins or avian
proteins by forming sterile abscesses or granulomatous inflammatory nodules. It has been shown that these nodules, which appear clinically to be granulomas, may in fact be small foci of infection. Treatment with an antistaphylococcal antibiotic is the initial treatment of choice. If no resolution occurs, dilute intralesional corticosteroids can be administered, or hyaluronidase can be injected to cause rapid dissolution of the product.2 It is also important to be aware that excess water absorption by many of the hyaluronic acid fillers can cause immediate swelling that will often decrease over days.
LONGEVITY
LONGEVITY
In general, the longevity of augmentation is greater for the more highly crosslinked or stabilized forms and is also directly proportional to filler viscosity and particle size. Naturally occurring hyaluronic acid is metabolized by lymphatic clearance and is eventually degraded in the liver to carbon dioxide and water. Hyaluronic acid–based products are broken down via isovolemic degradation; they maintain a constant volume throughout their degradation because of their ability to bind water. This property makes possible a very long-lasting product.
BIODEGRADABLE MICROPARTICLE INJECTABLE IMPLANTS
POLY-L-LACTIC ACID
POLY-
-LACTIC ACID
L
PATIENT SELECTION
Poly-l-lactic acid (PLLA) was approved by the FDA in 2004 for correction of HIV-related facial atrophy and is also approved for the cosmetic correction of shallow-todeep contour deficiencies. Currently in the United States, PLLA is well known as a no-downtime, long-lasting filler with a wide range of applications. PLLA’s uniqueness lies in the fact that it is not a direct filling agent but rather a biostimulatory agent, eliciting tissue thickening over the course of many months and many treatment sessions. It is, therefore, the ideal filler for someone desiring a gradual, subtle change. Because PLLA works by initiating a foreign-body tissue response, it is not suited for patients taking immunosuppressive or antiinflammatory drugs, and it appears to work most efficiently in younger patients with robust immune responses. PLLA can be used for volume enhancement in the nasolabial fold, labiomental crease, chin, jawline, buccal hollows, and temples. Some practitioners have found it efficacious for filling for the dorsum of aging hands, however there is a moderate risk of nodule formation in this area. It is not recommended for use in the lips and should be used with care in the periorbital area.
3
31
FORMULATION
PLLA is supplied as a vial (367.5 mg) of freeze-dried powder of synthetic l-polymer of polylactic acid (from the α-hydroxy acid family), sodium carboxymethylcellulose, and mannitol. Injection of PLLA on repeated occasions presumably initiates an immune response that eventually leads to fibroblast activation and collagen deposition. High-level ultrasonographic images taken before and after a series of treatments in study patients confirms the presence of a zone of dermal thickening, but the exact mechanism is unknown.
ANESTHESIA
PLLA must be reconstituted at least 2 hours in advance of use; however, current standard of care is reconstitution at least 8 hours before treatment to fully suspend and hydrate the microparticles of PLLA. The package insert recommends reconstitution with 3 to 5 mL of sterile water, but the consensus of physicians currently using the product is to reconstitute with a minimum of 5 mL of diluent. It is possible to reconstitute the product in advance with 4 mL or more of sterile water and immediately before injection to add 1 mL of 1% lidocaine to the bottle. This tempers the pain on injection. In addition, patients may want to apply a topical anesthetic containing either 4% lidocaine or 20% tetracaine in advance of treatment.
TECHNIQUE
Because of the diffuse panfacial nature of PLLA injections, it is helpful to inject the patient in a supine position. PLLA is injected through a 25- to 26-gauge needle. Because of the risk of particle clumping, the bottle must be agitated frequently throughout the course of treatment. The operator must maintain maximum control over injection amounts, so drawing the material up into 1-mL syringes is highly recommended. The injection technique used when infiltrating PLLA is diffuse crosshatching and threading. Depot deposition of product is not recommended. The principle is to inject PLLA into areas that will eventually display a direct impact from local volume change or affect neighboring areas by filling and suspending tissues upstream. Lower-face injections are performed diffusely over a wide surface area and involve the placement of 0.1-mL linear threads of solution 2 mm apart. The recommended technique is to inject across folds to distend them, rather than filling them directly. No attempt at volumetric correction is made during treatment; rather, the intent is to place the PLLA solution diffusely. The level of injection in the lower face (cheek, nasolabial fold, jawline, labiomental crease, chin) is subdermal (Fig. 215-3). In the upper face (temples and periorbital area) treatment is via diffuse threading of 0.05 mL of PLLA solution under or close to periosteum. No more than 0.5 mL total should be distributed in this fashion. If clogging of the needle occurs, it should be withdrawn and either changed or cleared before proceeding. Many practitioners have found that
3915
31
A
B
the use of long needles (1.5 inches) better facilitates even dispersion of the product.
POSTPROCEDURE INSTRUCTIONS
Immediately after injection, treated areas must be vigorously massaged to distribute the suspension evenly into the tissues. No blebs of material should be palpable. When the practitioner is satisfied that this is the case, the massage may then be continued in a gentler manner by an assistant for the next 5 minutes. Ice is then applied to the face for 20 minutes. The patient may then apply makeup and resume normal activities. The patient should massage the areas of injection for 5 minutes, 5 times a day for 5 days. Because minimal augmentation is achieved in each session, patients are instructed to return at 6-week intervals for additional treatments. The motto “treat, wait, assess” is an important one to follow when using PLLA. Resultant augmentation can take 4 months or longer to occur, so patience is necessary to avoid overcorrection. For the average patient with cosmetic concerns, between 3 and 6 treatments will be required for ample augmentation to occur. For patients with severe lipoatrophy, a minimum of 6 sessions will be required, often with injection of 2 vials per session.
UNIQUE COMPLICATIONS
Superficial injection of PLLA most often results in visible papule formation. Reconstitution with inadequate amounts of fluid may also increase this risk. Delayed formation of subcutaneous papules has been reported in the literature. These papules although palpable are most often nonvisible, asymptomatic, and noninflammatory, and require no treatment. If they are of concern to the patient, an attempt can be made to break apart the papules by injecting sterile water into them or by teasing them apart with a 27-gauge needle. Results of
3916
an 8-year injectable filler safety study found evidence to support a decreased risk of nodules with increasing dilutions.3 Rarely, large visible nodules can be seen as a late-onset side effect. Intralesional cortisone may be of help since they are often inflammatory or granulomatous in nature. Surgical removal is also an option for large unresponsive or deforming nodules.
LONGEVITY
The results from PLLA infiltration are thought to last 2 years or longer, with gradual resorption and breakdown of the product to lactic acid over the course of 2 to 3 years.
CALCIUM HYDROXYLAPATITE
CALCIUM
HYDROXYLAPATITE
PATIENT SELECTION
Patients requiring augmentation of the nasolabial folds, labiomental crease, mandibular ramus, cheeks, or prejowl sulcus, or those with age-related atrophy of the dorsal hands are candidates for treatment with calcium hydroxylapatite (CaHA). CaHA also has been used with success in the correction of atrophic acne scars, in the recontouring of nasal defects, and in nipple reconstruction after failed nipple areolar reconstruction. Because of the risk of nodule formation, CaHA is not recommended for lip augmentation and should be used judiciously in the periorbital area.
FORMULATION
Originally approved for use by the FDA as a radiographic marker and for the correction of oral and
maxillofacial defects and the treatment of vocal cord insufficiency, CaHA has since gained approval for treatment of the nasolabial folds and dorsal hands. All other areas mentioned above are common offlabel uses. The microspheres of CaHA, once injected into the deep dermis, form a scaffold to support the growth of autologous collagen so there is overlap with this product as not only a temporary filler, but also as a biostimulatory agent. CaHA contains smooth spheres of 30% CaHA between 25 and 45 microns and 70% carboxymethylcellulose gel suspension, which serves to hold the microspheres in place until it is resorbed and neocollagenesis takes place.1 CaHA contains no animal or human tissues, so allergy testing is not indicated. This filler is unique in that the standard syringe volume is 1.5 mL of material, making it the largest packaged syringe by volume.1
ANESTHESIA AND TECHNIQUE
Injection of CaHA is quite uncomfortable, so it is almost always necessary to anesthetize the area first with 1% lidocaine. For facial injections, a current popular practice is to mix 0.2 mL of 1% lidocaine with the CaHA via a female–female adapter. This not only provides adequate anesthesia, but also thins the product to allow for smoother injection. Because of its viscosity, CaHA must be injected through a 27- to 28-gauge needle. Placing the patient supine or at 45 degrees, a threading technique is used, with infiltration staying at the dermal–subcutaneous junction in the area of the nasolabial fold and at the deep fat or supraperiosteal region in the areas of the cheek and mandible. CaHA appears to work best if patients undergo retreatment or touchup at 3 months. For injections to the dorsal hands, the patient should be placed in a comfortable position with the hands faced prone on a flat surface. The FDA approved method of injecting CaHA in the hands, involves using 1.3 mL of the CaHA-injectable implant mixed with 0.2 mL of 2% lidocaine HCl. Using a 27-gauge needle, several 0.2- to 0.5-mL aliquots are injected subdermally in the space bound laterally between the first and fifth metacarpals, proximally by the dorsal wrist crease, and distally by the metacarpophalangeal joints. This is followed by gentle massaging of the injected areas to blend the product evenly across the dorsal hand. The number of injection points is left to the discretion of the treating physician, based on the amount of correction needed. No more than 3 mL of the CaHA implant is to be injected per hand. Some clinicians prefer to use cannulas for CaHA injection in the dorsal hands using either a bolus or threading technique.
POSTPROCEDURE INSTRUCTIONS
There can be marked swelling and bruising after the injection of CaHA, so posttreatment icing is recommended. Many physicians advocate immediate postinjection massage but others believe that continued massage is unwarranted.
3
31
UNIQUE COMPLICATIONS
CaHA is not a mucopolysaccharide and therefore does not rely on water binding for its persisting clinical effect and it does not carry the risk of producing the Tyndall effect in the skin. However, if CaHA is injected too superficially or at appropriate levels in thin skin, its opacity can be seen. Because it contains microspheres of CaHA and collagen forms around these particles, these physical properties can lead to more palpability in the soft subcutaneous tissues. The majority of complications with CaHA (nodules) are seen in the lips, but it is possible for nodules lasting 1 to 2 years to occur anywhere the substance is injected. These nodules are supposedly noninflammatory, and often the material can be extruded from a puncture incision. Persistent nodules may have to be surgically removed. Demarcation of product is especially evident in the periorbital area, as is prolonged erythema.
LONGEVITY
In a 12-month, multicenter prospective randomized split face trial comparing CaHA to non–animalderived stabilized hyaluronic acid in the nasolabial folds, CaHA was found to provide significantly greater correction at all time points. In practice, though, longevity appears variable, with effects lasting anywhere between 6 and 18 months.4
AUTOLOGOUS FAT TRANSFER
PATIENT SELECTION
PATIENT SELECTION
Autologous fat transfer (AFT) is a practical option for patients who desire a more dramatic global change in facial appearance. Recent anatomic research suggests that facial fat is delineated in discreet fat compartments that change morphologically over time.5
Therefore, using fat as a filler is done with the intent of restoring the youthful architecture to these fat compartments. This provides broader rejuvenation to the aging face affected by volume loss. Fat is a versatile filler, effective in the periorbital area as well as the lips. Because it is autologous, it is the filler of choice for patients with collagen vascular disease or proven allergic reactions to collagens or hyaluronic acids. AFT is a more involved surgical procedure than the injection of the other fillers previously discussed. There are a subset of patients in whom AFT is not indicated. These patients include those with very low body fat, such as long distance runners, the elderly, and those with HIV-associated lipodystrophy, patients on concomitant anticoagulant treatment, and those who are of poor health.
3917
31
TECHNIQUE
TECHNIQUE
PREPARATION AND ANESTHESIA
For 2 weeks before the initial AFT procedure, the patient must stop taking all nonsteroidal antiinflammatory drugs, vitamin E, ω-3 fatty acid supplements, and ginkgo, ginger, or ginseng supplements. The patient is instructed to begin therapy with an appropriate antistaphylococcal antibiotic starting the day before the procedure. On the day of the procedure, the donor fat site and the face are both washed with an antibacterial soap. The physician then delineates the area to be suctioned with a marking pen. Every attempt should be made to choose a donor site that benefits a patient aesthetically. The outer thighs and hips in women and the flanks in men are usually good sites for fat harvesting. In preparation for fat transfer, a pattern is drawn on the face delineating the areas in which fat is to be placed and highlighting any scars or baseline asymmetry. The patient is then placed on a sterile, draped operating table and the areas requiring fat suctioning are infiltrated with dilute local anesthesia until turgid (tumescent technique; Table 215-3; see Chap. 214). It takes at least 20 minutes for the epinephrine in the tumescent fluid to achieve hemostasis. The face is then anesthetized diffusely with dilute 0.5% lidocaine with epinephrine 1:200,000, and segmental nerve blocks are established where appropriate. For safety, the total lidocaine dose in the tumescent fluid should not exceed 35 mg/kg of body weight.
FAT HARVESTING
Suctioning of the fat used for transplantation should be done by hand with an open-tipped harvesting cannula attached to a 10-mL syringe. After a hole is made with a 1.5-mm punch or No. 11 blade, the cannula is inserted into the deep fat and moved back and forth while the plunger on the syringe is retracted. Fat collection usually occurs quite rapidly and, due to the vasoconstrictive properties of the tumescent fluid, is nearly bloodless. After fat extraction, the syringes may be placed into a centrifuge and spun at 3400 revolutions per minute for 20 seconds or left to stand for 20 minutes to allow separation of the hydrophilic tumescent fluid from the lipophilic fat. The infranate of tumescent fluid should then be decanted before the fatty layer is transferred to 1-mL syringes in preparation for injection into the face. Any supranate of ruptured fat cells (triglycerides and free fatty acids) should be discarded.
■1 L Normal saline
■1 L Normal saline
■50 mg Lidocaine
■50 mg Lidocaine
■0.5 to 1 mg Epinephrine
■0.5 to 1 mg Epinephrine
3918
■12.5 mEq Sodium bicarbonate
■12.5 mEq Sodium bicarbonate
FAT TRANSFER
All AFT to the face is performed with the patient fully supine using an 18-gauge or smaller blunt cannula for infiltration. Incision sites can be made with an 18-gauge needle, a NoKor needle (Becton, Dickinson and Co., USA), or the tip of a No. 11 blade scalpel. Fat is infiltrated in a retrograde manner; that is, fat is injected only as the cannula is withdrawn. Injection is in small aliquots of 0.1 mL or less using a threading or depot method. Placement of fat always starts closest to bone when possible and then proceeds up through muscle and into subcutaneous fat. Fat is deposited in a crosshatched three-dimensional lattice and thus imparts structure as well as augmentation to the tissues. All areas of the face should be addressed to achieve filling both laterally and anteriorly. The goal is to advance tissues forward and elevate them away from the bone, fill in areas of shadow, and restore youthful contours.
POSTPROCEDURE INSTRUCTIONS
POSTPROCEDURE
INSTRUCTIONS
Immediately after the procedure and on-and-off for the next 2 days, ice should be applied to the face. The area suctioned is dressed with absorbent pads, and a snug garment is applied. Incision sites on the body and face are left unsutured. The patient is instructed not to submerge the body in water until all incisions are healed (approximately 1 week). Antibiotics must be continued for 6 days after the initial procedure. Intramuscular triamcinolone may be given to reduce postoperative edema.
UNIQUE COMPLICATIONS
UNIQUE COMPLICATIONS
Postoperative edema and ecchymoses are common and last for approximately 2 weeks. Undercorrection with a gradual decrease in augmentation is common and usually represents a decline in edema rather than absorption of the fat. For this reason, fat transfer should never be recommended as a one-time procedure, but rather as a series of treatments with cumulative augmentation and long-term results. Small, persistent lumps can occur that represent either fat cysts or accumulation of fat. They can be treated, usually to resolution, with intralesional injection of triamcinolone (2 to 4 mg/mL). If a larger fat lump is present, the best option is to feather it into the surrounding tissues with an infiltration cannula. Irregularities can also occur at the harvest site, but operator experience and judicious removal of fat makes this a highly unlikely event. Rarely, infections, such as atypical mycobacteria, can be seen and should be in the differential diagnosis for any nodules occurring up to 1 year following AFT.
A
3
31
B
LONGEVITY
LONGEVITY
Many authors using a standardized, multilevel microinjection technique have published photodocumentation of long-term followup demonstrating persistence of autologous fat (Fig. 215-4).6 When AFT is done with proper technique, the results are permanent. Successful grafting really depends on the precise performance of four important aspects: collecting, processing, injecting and protecting.
INJECTABLE SILICONE
PATIENT SELECTION
PATIENT SELECTION
Injectable silicone is categorically a permanent filler with a wide range of applications. It appears to provide permanent, cosmetically superior augmentation for treatment of HIV lipoatrophy, plantar defects, and scars. Historically, silicone injection has been associated with disfiguring tissue distortions and migration of product. These side effects can almost always be traced to the use of large-volume injections or non–medical-grade silicone. Because of the controversial nature of silicone augmentation, patient selection for cosmetic indications is complex, and use of the procedure should be reserved for those physicians who have extensive experience in the injection of silicone as a filler and who understand the concepts outlined in the “Technique” section. Patients with a known history of autoimmune disease, and those with chronic or active infections should be excluded from treatment.
FORMULATION
FORMULATION
Injectable silicone has both inspired a loyal following and provoked vehement opposition. There is no
approved silicone for soft-tissue skin augmentation. However, off-label uses of ophthalmologic preparations of silicone have been adapted for use, especially in the treatment of HIV-associated lipoatrophy and other clinical conditions of facial volume loss. One formulation, PMS-350, has European approval for treatment of glabellar lines, nasolabial folds, perioral lines, lip augmentation, and scarring disorders. Silicone oil varies in chemical structure, physical properties, purity, sterility, and biocompatibility. Medical-grade silicone oil contains long polymers of dimethylsiloxanes.7 It is noncarcinogenic and does not appear to be associated with arthritic disease in mice. Viscosity of silicone oil is measured in centistokes (cs), which is a unit of kinematic viscosity. After injection, silicone is encapsulated in collagenous fibrous tissue, so that final augmentation is a result of both volume of injected silicone and host tissue response.
ANESTHESIA
ANESTHESIA
Currently available forms of silicone do not contain an anesthetic solution, because such small volumes are injected on each visit an ancillary anesthesia is not often required. If desired, a topical anesthetic agent containing 4% lidocaine or 20% tetracaine may be applied before the procedure.
TECHNIQUE
TECHNIQUE
Improper technique in the injection of silicone oil will almost always guarantee permanent adverse sequelae. Consequently, it is absolutely necessary that a physician considering its use apprentice with an experienced practitioner. Silicone (1000 cs) is highly viscous and must be injected through either a 26-gauge needle on a 1-mL
3919
31
syringe or a 30-gauge needle on a 0.3-mL syringe. Use of a microinjection technique is paramount to success with silicone, so large-bore needles are never to be used. The microdroplet injection technique involves injecting 0.01 mL of silicone oil, with the needle bevel down, into the deep dermis in a depot fashion at 1- to 3-mm intervals. Note that 100 droplets are therefore required to empty a 1-mL syringe. Except in the treatment of HIV cheek atrophy, it is rare to use more than 0.3 mL total per injection session. Treated areas are always undercorrected, and patients are instructed to return for multiple injection sessions at monthly intervals until full augmentation occurs.
POSTPROCEDURE INSTRUCTIONS
POSTPROCEDURE
INSTRUCTIONS
There is very little postoperative discomfort, edema, or ecchymosis after microinjection with liquid silicone. Ice may be applied if needed to lessen the risk of postinjection ecchymosis. Patients may apply makeup and pursue their daily activities as usual after injection.
UNIQUE COMPLICATIONS
UNIQUE COMPLICATIONS
Most authorities on silicone use agree that the incidence of serious complications after the proper use of medical-grade silicone is very low. In an FDA-authorized study involving 1400 patients over a 20-year period, 2 patients experienced serious side effects: one case involved migration of silicone after treatment with large volumes, and the second involved inflammation and necrosis in a patient with concomitant Weber-Christian disease and rheumatoid arthritis. Local granulomatous nodularities can occur many years after the cessation of treatment and are usually preceded by a systemic infection. Treatment regimens for granulomas include intralesional or systemic steroids, minocycline, topical imiquimod and, if necessary, surgical excision.8
LONGEVITY
LONGEVITY
The augmentation derived from liquid silicone injection is permanent. Many authors have published reports of long-term studies, some with 30-year followup, showing persistence of improvement. Patients receiving liquid silicone injections will continue to age, and, for this reason, additional augmentation may be required should neighboring areas of age-related atrophy develop.
3920
COMPLICATIONS ASSOCIATED WITH THE USE OF ALL FILLERS
Vascular occlusion is perhaps the most devastating complication associated with the use of all fillers. This can manifest as local necrosis, CNS infarction, or blindness. Blindness and middle cerebral artery infarction have been described most often after fat transfer, but vascular occlusion with ensuing sequelae has occurred after the use of collagen and hyaluronic acid fillers as well. In theory, the central occlusive events have occurred from high-pressure injections with retrograde flow into arterioles that connect with the internal carotid system. It is, therefore, of utmost importance to keep the needle or cannula moving during withdrawal while depositing filler and to exert as little pressure as possible on the syringe. For similar reasons, when fat transfer is performed, only blunt cannulas should be used for infiltration. Other complications common to the use of all fillers include ecchymosis, edema, extrusion or drifting of the filling substance, foreign-body reactions, pigmentary alteration, injection site scarring, overcorrection, undercorrection, misplacement, and infection.
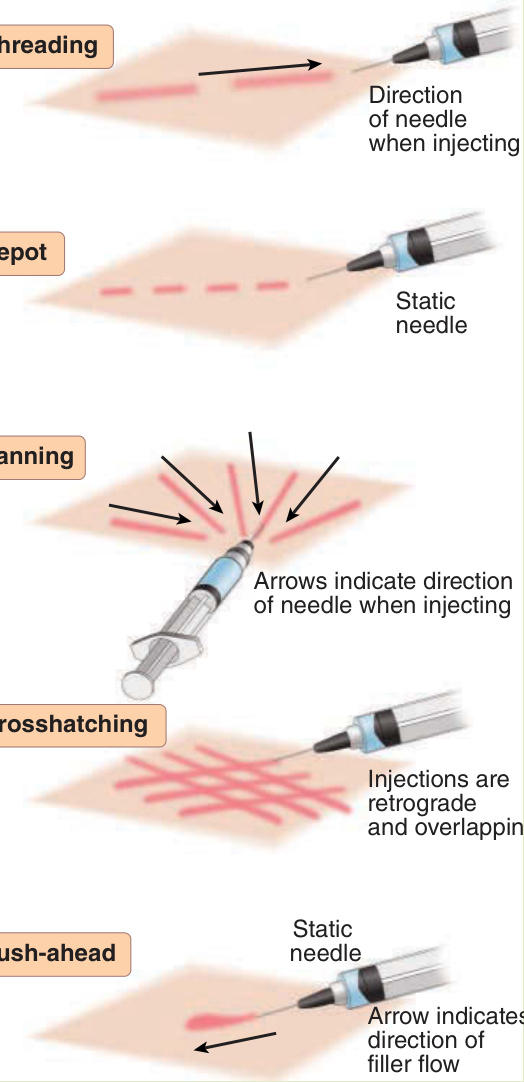
Figure 215-1 Injection techniques.
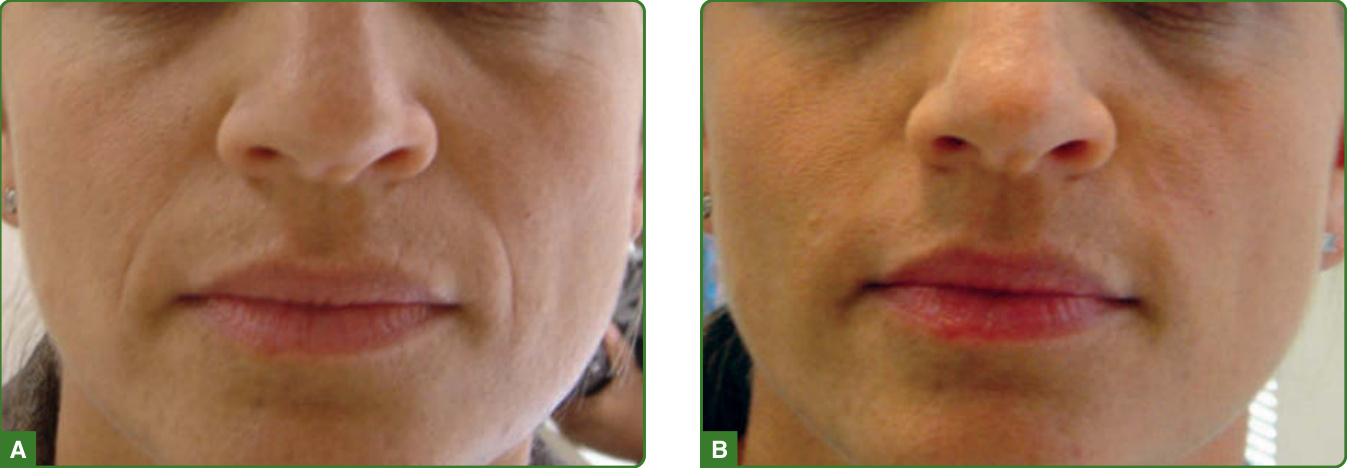
Figure 215-2 Thirty-five-year-old woman before (A) and after (B) infiltration of Restylane into the nasolabial folds.
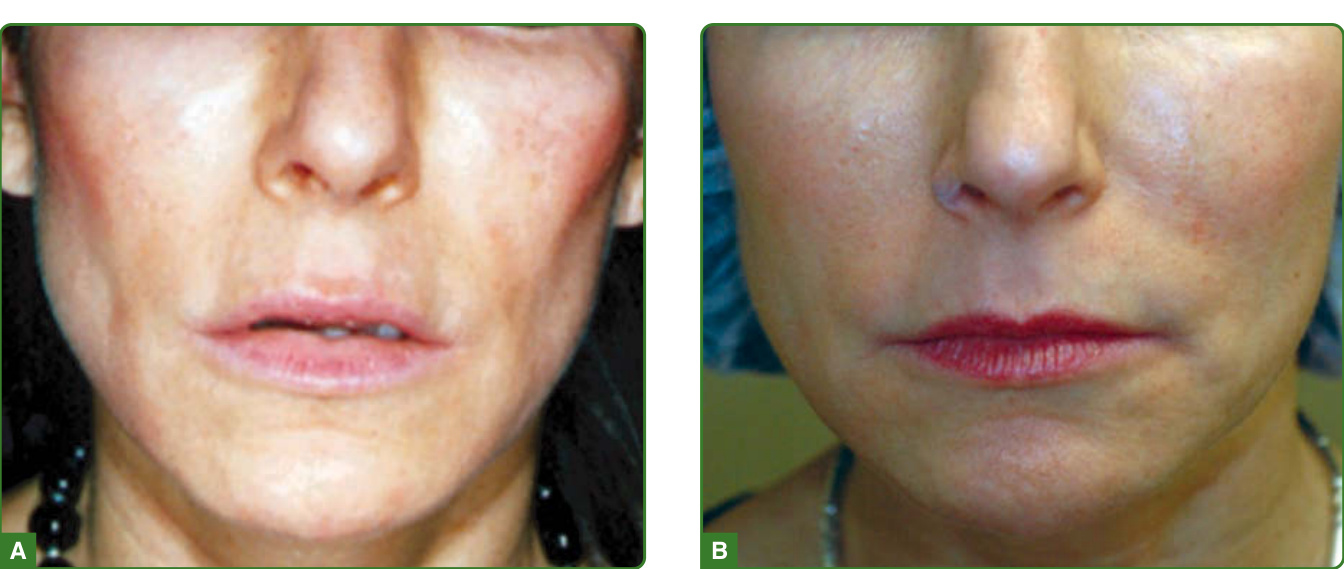
Figure 215-3 Thirty-nine-year-old woman before (A) and 4 months after (B) the last of 2 Sculptra treatments to the lower face.

Figure 215-4 Fifty-five-year-old woman before (A) and 20 months after (B) full-face fat transfer treatment series.
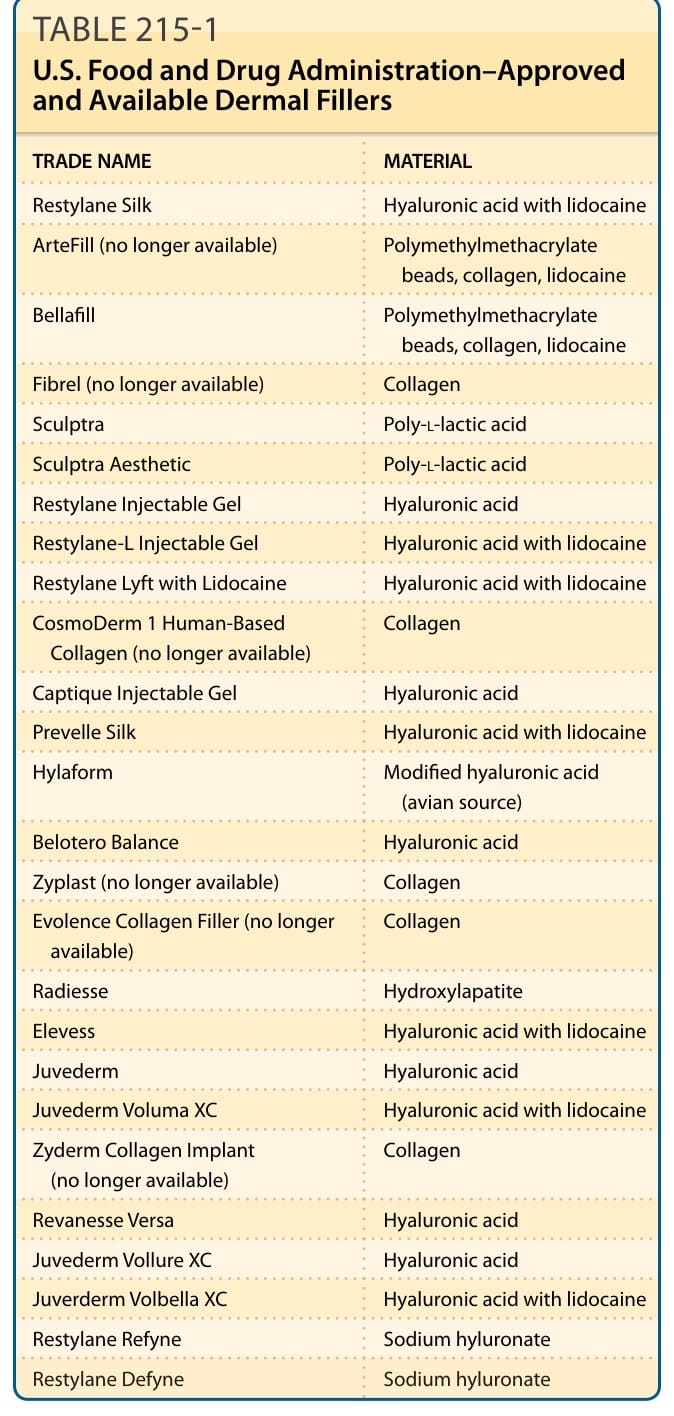
TABLE 215-1 U.S. Food and Drug Administration–Approved and Available Dermal Fillers
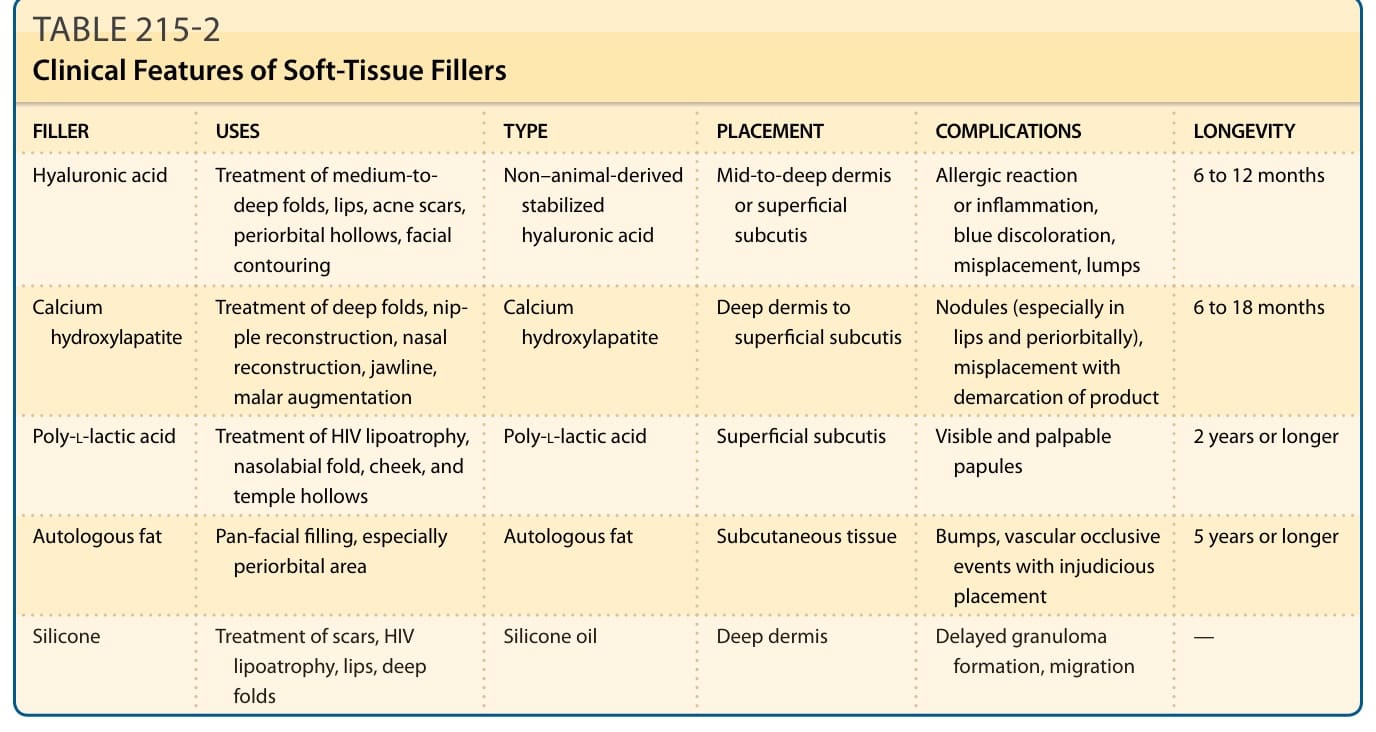
TABLE 215-2 Clinical Features of Soft-Tissue Fillers
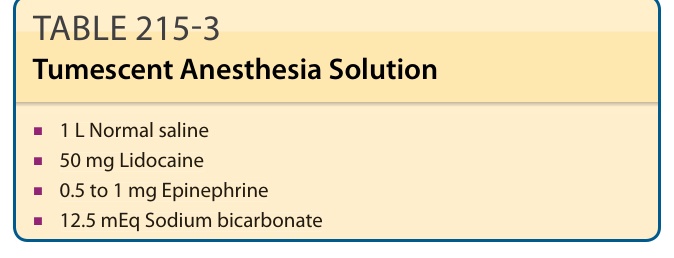
TABLE 215-3 Tumescent Anesthesia Solution