Cryosurgery and Electrosurgery
3
30
AT-A-GLANCE
■ With a boiling point of −195.8 Celsius, liquid nitrogen is the cryogen of choice for treating benign and malignant neoplasms.
■ Melanocytes and fibroblasts are the cells that are most and least sensitive to the destructive effects of cryosurgery.
■ Tumors that require histopathology for diagnosis and recurrent nonmelanoma skin cancers are contraindications for treatment with cryosurgery.
■ Several cryosurgery techniques exist to treat benign and malignant neoplasms.
■ Electrosurgery can be categorized into electrofulguration, electrodessication, electrocoagulation, electrosection, electrocautery, and electrolysis (Table 206-4).
■ Electrosurgical devices have a low risk of interfering with cardiac and non cardiac implanted electronic devices (IEDs).
■ Perioperative and intraoperative safety considerations should be made when performing electrosurgery on patients with IEDs.
■ Curettage and electrodessication is an acceptable definitive treatment for malignant tumors.
CRYOSURGERY
BACKGROUND
BACKGROUND
Cryosurgery refers to the use of extreme cold to destroy cells of abnormal or diseased tissue. The earliest use of a cold refrigerant in medicine is attributed to White, a New York dermatologist, in 1899.1,2 Using a cotton-tipped applicator dipped into liquefied air, he successfully treated warts, nevi, and precancerous and cancerous lesions. In 1907, Whitehouse, another New York dermatologist, reported the use of the spray method in the cryosurgical treatment of skin cancers.3
Cryobiology refers to the study of the effects of subzero temperature on living systems. Tissue destruction from cryotherapy results from direct cell injury, vascular stasis, and the local inflammatory response. Freezing cells convert water to ice (crystallization). Rapid freezing causes intracellular ice crystal formation with the disruption of electrolytes and pH changes, whereas slow freezing causes extracellular ice formation and less cell damage. Therefore, tissue
effects and cell death are most readily achieved when tissue is frozen rapidly.4
During thawing, recrystallization occurs when ice crystals fuse to form large crystals that disrupt cell membranes. As the ice melts further, the extracellular environment becomes hypotonic, causing water to infuse into cells and cause cell lysis.5 The longer the thawing time, the greater the damage to cells because of increased solute effect and greater recrystallization. After freezing, stasis within the vasculature occurs. This loss of circulation and resultant anoxia is a major mechanism of injury from cryosurgery. As the tissue thaws at temperatures higher than 0°C (32°F), a brief hyperemic response ensues with resultant edema and inflammation.5
TARGETS OF CRYOSURGERY
TARGETS OF CRYOSURGERY
CRYOGENS
CRYOGENS
Liquid nitrogen is the cryogen of choice in dermatology. It is easy to store in an insulated unit, easy to use, environmentally friendly, nonflammable, inexpensive, and, at −195.8°C (−320.4°F), has the lowest temperature of all the common cryogens, causing rapid freeze of treated tissue. Other available cryogens include fluorinated hydrocarbons, solid carbon dioxide, and nitrous oxide (Table 206-2). Fluorinated hydrocarbons are used as topical sprays to provide temporary anesthesia before the removal of skin lesions and the administration of vaccinations. Cryogen spray cooling is also used to reduce the pain of laser surgery and eliminate overheating of the epidermis.7
30
CELL TEMPERATURE (çC/çF)
Melanocytes −4 to −7 (24.8 to 19.4)
Keratinocytes −20 to −30 (−4 to −22)
Fibroblasts −30 to −35 (−22 to −31)
Fibroblasts −30 to −35 (−22 to −31)
PERIOPERATIVE CONSIDERATIONS
PERIOPERATIVE
CONSIDERATIONS
PATIENT SELECTION
Cryosurgery is one of several destruction modalities used for benign and malignant skin neoplasms. Several factors, including lesion type, size, depth, border, location, and patient skin type, should be considered when cryosurgery is a treatment choice.
ANATOMICAL SITE PRECAUTIONS
The cryosurgeon should be aware of certain anatomical locations where cryosurgery may lead to complications. Caution should be undertaken when treating lesions overlying nerves, such as the postauricular nerve on the neck or digital nerves on medial and lateral fingers and toes. Damage may result in regional paresthesia or motor dysfunction. In addition, cryosurgery at anatomical sites such as the eyelids, mucosa, nasal ala, and auditory canal, may result in scarring with retraction after treatment. As skin melanocytes are easily prone to destruction by freezing, the cryosurgeon should treat darkly-pigmented skin with caution as cryosurgery may result in hypopigmentation at treated sites.
TREATMENT CONTRAINDICATIONS
Absolute contraindications to cryosurgery include lesions that require histopathology for diagnosis and recurrent nonmelanoma skin cancers. Relative contraindications to cryosurgery include patients with cold urticaria, abnormal cold intolerance, cryoglobulinemia, or cryofibrinogenemia, or tumors with indistinct borders or darkly pigmented features (Table 206-3).
AGENT BOILING POINT (çC/çF)
Freon −40.8/−41.4
Solid CO2 −79.0/−110.2
Nitrous oxide −89.5/−129.1
3792
Liquid nitrogen −195.8/−320.4
Liquid nitrogen −195.8/−320.4
■Lesions that require histopathology for diagnosisa
■Lesions that require histopathology for diagnosisa
■Recurrent nonmelanoma skin cancersa
■Recurrent nonmelanoma skin cancersa
■Cold urticaria
■Cold urticaria
■Abnormal cold tolerance
■Abnormal cold tolerance
■Cryoglobulinemia
■Cryoglobulinemia
■Cryofibrinogenemia
■Cryofibrinogenemia
■Tumors with indistinct borders or darkly pigmented features
■Tumors with indistinct borders or darkly pigmented features
aAbsolute contraindication.
RISKS AND POTENTIAL COMPLICATIONS Pain: In addition to pain during freezing, patients will experience some discomfort several hours posttreatment. Typically, pain is controlled with acetaminophen. Lesions such as periungual warts, digital lesions, or mucous membrane lesions may require stronger analgesics because of intense swelling and throbbing.
Bleeding: Patients on anticoagulant therapy should be warned of bruising resulting from tissue necrosis. If painful hemorrhagic bullae form, they may be drained with an 18-gauge needle inserted into the lateral blister skin. Care should be undertaken not to remove the surface of the bullae, as this tissue acts as a natural wound dressing.
Pigmentation Changes: Hypopigmentation or hyperpigmentation is the most disconcerting complication following cryosurgery. As shown in Table 206-1, pigmented cells are highly susceptible to freezing at temperatures of −4°C to −7°C (24.8°F to 19.4°F). Although pigmentation changes are usually transient, prolonged freezing for longer than 30 seconds may result in permanent pigment loss. Topical steroids, glycolic acids, retinoids, and hydroquinone may aid in reducing the incidence of hypopigmentation.
Nerve Damage: Treatment of lesions overlying nerves, such as the postauricular nerve on the neck or digital nerves on medial and lateral fingers and toes, may result in regional paresthesia or motor dysfunction. Digital neuropathy occurring after cryosurgery of digital warts has been reported.8
Scarring: Fibroblasts are the most resistant to freezing and do not undergo cell death until −30°C to −35°C (−22°F to −31°F). Therefore, most benign and premalignant lesions treated with cryotherapy heal with little scarring. Soft, contracted linear scars resulting from second intention may occur in malignancies treated with cryosurgery.
Alopecia: Freeze times longer than 20 seconds may result in alopecia. This is especially true when treating malignant lesions.
Insufflation of Soft Tissue: During freezing nitrogen gas may escape into perilesional skin,
producing crepitus. Pressure on the crepitated area will expel the gas. The use of a cone surrounding the biopsy site prevents crepitus from occurring.
ANESTHESIA
For the majority of patients, anesthesia is not necessary prior to a cryosurgical procedure. However, cryosurgery is painful, especially in children. For short cryosurgery treatment times, 1% lidocaine with 1:100,000 epinephrine may be locally injected prior to treatment. For longer cryosurgery treatment times, such as treatment of skin neoplasms (up to 30 seconds), local anesthesia is mandatory. Topical anesthesia can be applied approximately 1 hour prior to the procedure to minimize pain. A single-center, double-blinded, randomized, placebo-controlled, parallel-group trial comparing a cream containing 5% lidocaine and 5% prilocaine applied 1 hour prior to cryosurgery for warts, however, did not demonstrate a statistically significant difference in pain during the procedure.9 For longer cryosurgery treatment times, such as treatment of skin neoplasms (up to 30 seconds), 1% lidocaine with 1:100,000 epinephrine can be locally injected prior to treatment.
PERIOPERATIVE CARE
Patients should be given simple verbal and written wound care instructions posttreatment. Edema, vesicles, bullae, and weeping should be expected from treated areas within 24 hours posttreatment. Treated sites may be rinsed with soap and water and patted dry with a towel daily. If actively weeping, the wound site may be bandaged. Benign and premalignant lesion-treated sites heal typically in 1 to 2 weeks, with malignant lesiontreated sites requiring 3 to 4 weeks of healing. Clinically-suspicious actinic keratoses not responsive to cryosurgery should be biopsied to rule out invasive skin cancer.
CRYOSURGERY TECHNIQUES
CRYOSURGERY
TECHNIQUES
There are several cryosurgical techniques that can be used in treating skin lesions. The open spray method is most frequently used. This method uses a handheld cryosurgical unit with fingertip trigger (Fig. 206-1). Patients may be seated or lying on an examination table at an angle. The canister should be held upright when treating the patient as tilting the canister sideways will result in the sudden release of a vapor from the canister. Spray tips with varying-sized apertures are attached to the unit, emitting a stream of liquid nitrogen toward the lesion from a distance of 1 to 2 cm. Although freeze times vary for lesion types, an intermittent spray in a solid, circular, or paintbrush pattern
3
30
is normally used. Longer spray times are required for thicker, keratotic lesions or malignant lesions; shorter times are required for thinner, atrophic, or benign lesions. The intermittent spray helps to localize treatment to the lesion with a small freeze halo, thus minimizing collateral normal tissue damage. This is particularly important when treating lesions around the orbital, nasal, auricular, genital, or periungual regions. As the lesion is treated, a lateral freeze spreads beyond the margins of the lesion. The measurement of the surface radius of the freeze is equal to the central depth of the freeze into the skin.5 Temperature gradients exist within the freeze, with colder temperatures in the middle and warmer temperatures toward the periphery. In general, superficial lesions should have a clinical freeze margin of 2 to 3 mm, and malignant or deeper lesions should have a clinical freeze margin of 5 mm to ensure successful treatment. The closed technique uses a copper cryoprobe that is attached to the cryosurgical unit. Once the metal probe is pressed against a lesion on the skin, the trigger of the unit is squeezed, and liquid nitrogen leaves the unit through a conduit line that maintains it in a closed system. This technique is useful for treating small, well-circumscribed lesions or lesions found in confined locations. Similarly, a metal, cone-sized chamber can be attached to the cryosurgical unit and held in contact with the lesion. This allows liquid nitrogen spray to enter the cone and rapidly freeze the lesion. Another cone apparatus option includes holding an otoscope cover tip against the lesion with one hand while freezing with the cryosurgical unit held in the other hand. Treatment times using the cone method should be decreased because the final temperature at the orifice of the cone is obtained faster, when compared with an open spray.
3793
30
If a cryospray unit is not available, the dipstick technique can be used. First, a small amount of liquid nitrogen is poured into a polystyrene cup or other insulated container. Cotton-tipped swabs are placed tip-down in the container and cooled. Using firm pressure, the cotton tips are placed against the lesion until a 2-mm to 3-mm halo forms around the treated lesion. This method treats lesions on the body where surrounding tissue must be spared, such as periorbital, mucosal, nail, and genital regions. Alternatively, tissue forceps can be placed in the container and allowed to cool. This method is useful for treating filiform lesions such as verrucae and skin tags. The metal forceps cool rapidly, so insulated gloves should be worn while holding the forceps to prevent freeze injury to the practitioner’s fingers.
APPLICATIONS FOR COMMON BENIGN LESIONS
APPLICATIONS FOR
COMMON BENIGN LESIONS
SEBORRHEIC KERATOSIS
The spray technique is an effective modality for treating this common lesion. Although longer freeze times of 10 to 15 seconds with a 1-mm to 2-mm halo are required for these raised growths, too aggressive freezing may result in scarring or hyperpigmentation. For cosmetic purposes and to prevent pigmentation changes, a lighter freeze followed by curettage may be preferential. Forewarn patients that a second treatment may be required, especially for thicker seborrheic keratoses.
VERRUCAE
Warts are a common problem, with a high prevalence in the population.10 Although cryosurgery for warts has sustained a common practice in dermatology, varying techniques have been offered with regard to freezing method, number of freeze–thaw cycles, and frequency of treatment sessions. Cryosurgery using the spray technique is probably the most common method because of its quick, convenient use and ease of obtaining a freeze halo around the lesion (Fig. 206-2). The cotton-tip applicator technique is cheaper and may be less frightening to the patient, particularly if the patient is a child. Care must be undertaken not to cross-contaminate by reintroducing the cotton-tip applicator into a common flask. Combination therapy with cryosurgery also has been advocated to treat verrucae. Berth-Jones and Huchinson11 demonstrated a 52% cure rate at 3 months with the combination of cryotherapy, keratolytic wart paint, and paring. The authors also noted that paring the wart before cryotherapy improved the cure rates for plantar warts, but not hand warts.
SOLAR LENTIGO
As described in Table 206-1, pigmented cells are highly susceptible to freezing. Therefore, these lesions require
3794
a shorter freeze time of 3 to 5 seconds with minimal halo. For darker-skinned individuals, care must be taken not to induce hypopigmentation at treatment sites. Consequently, a test site in a cosmetically less noticeable region may be performed first before treating multiple lesions on sun-exposed areas. In addition, sunscreen with ultraviolet A and ultraviolet B protection should be advocated pretreatment and posttreatment.
KELOIDS AND HYPERTROPHIC SCARS
Treatment of keloids and hypertrophic scars is frequently unsatisfactory. Cryosurgery is a less common but effective means of treating these recalcitrant lesions. Freeze times of 30 seconds are required monthly until flattening is achieved. Zouboulis and colleagues reported a prospective study of 93 keloids and hypertrophic scars treated with 30-second freeze times over 1 to 3 sessions.12 Improved responses were seen in patients treated with 3 or more sessions (79%), compared with subjects treated once or twice (33%).
DERMATOFIBROMA
Dermatofibroma treatment times may require cryosurgery up to 60 seconds because of the fibrotic nature of the lesion and the need to treat cells located in the deep dermis. Torre reported a series of 79 dermatofibromas treated with cryosurgery. Out of the 79 that were followed, 61 were no longer palpable post treatment.13
SEBACEOUS HYPERPLASIA
These benign lesions can be a cosmetic concern for patients. Freeze times of 5 to 10 seconds are required, using the cryoprobe technique with the probe applied directly into the central punctum of the lesion. Patients must be advised that retreatment is frequently necessary.
APPLICATIONS FOR PREMALIGNANT AND MALIGNANT LESIONS
APPLICATIONS FOR
PREMALIGNANT AND
MALIGNANT LESIONS
Cryosurgery appears useful in well-defined lesions for situations where surgery is less favorable, either for technical or cosmetic reasons, or when the patient prefers this treatment option. The goal of cryosurgery is to cure the patient by destroying the lesion in a single treatment.
ACTINIC KERATOSIS
Cryosurgery is an effective modality for the treatment of actinic keratoses (AKs). The open spray technique, using a single freeze–thaw cycle of 8 to 10 seconds, is the treatment of choice. Hypertrophic AKs require longer freeze times, whereas atrophic AKs and AKs on thin-skinned regions require shorter freeze times. A 1-mm to 2-mm freeze margin around the lesion is adequate. For thicker lesions, pretreatment of emollients or curetting may shorten freezing times. Although cryosurgery is widely used in dermatology for treatment of AKs, there are few well-designed studies assessing cure rates. Lubritz and Smolewski14
treated 1018 AKs on 70 patients with cryosurgery with 20- to 45-second thaw times. At 1-year posttreatment, they reported a cure rate of 99%. Another prospective, multicenter study of 421 AKs larger than 5 mm in diameter on the face and scalp demonstrated a complete response of 39% with a 5-second freeze, 69% for a 5- to 20-second freeze, and 83% for a 20-second freeze.15
In patients with diffuse actinic damage, extensive cryosurgery, or cryopeeling, may be useful. Chiarello16
reported cryopeeling was twice as effective as 5-fluorouracil in the reduction of actinic keratoses and the formation of squamous cell carcinomas at 1 and 3 years post-cryopeeling.
BOWEN DISEASE
Ahmed and colleagues17 treated 26 Bowen disease patients using 3-mm clinical margins and spray technique with two 5- to 10-second freeze–thaw cycles. Two years after treatment, 50% of the treated lesions were still present at the same site. The average healing time was 46 days, with lesions on the lower leg taking longer to heal (90 days). Although the cure rate using cryosurgery for Bowen disease was low in this study, the authors did use a lower freeze time to minimize side effects postprocedure.
BASAL CELL CARCINOMA
Several studies have reported treating basal cell carcinomas (BCCs) with cryosurgery with cure rates ranging between 95% and 99%.18-20 Although excellent cure rates have been claimed, few studies have demonstrated histologically that the BCC is no longer present
3
30
posttreatment. Furthermore, there are no good studies comparing cryosurgery with other known treatment modalities, such as Mohs surgery, excision with clinical margins, and electrodesiccation and curettage. Postsurgical cosmetic appearance is a concern to patients. Kokoszka and Scheinfeld21 reported good cosmetic results in their review of the literature. Thissen and colleagues,22 however, compared the cosmetic results of surgical excision compared with cryosurgery for BCCs of the head and neck and concluded that cosmetic results after excision are better than after cryosurgery.
SQUAMOUS CELL CARCINOMA
Similar cure rates to BCCs are evident when treating squamous cell carcinomas (SCCs) with cryosurgery. In a study of 563 primary SCCs, of which most were between 0.5 and 1.2 cm in diameter, Graham and Clark23 reported a cure rate of 97.3%. Treatment technique with cryosurgery for SCCs is the same as for BCCs.
LENTIGO MALIGNA
With proper patient selection, cryosurgery can be an effective treatment option for lentigo maligna because of the sensitivity of melanocytes to cold. With the aid of a Wood lamp, a clinical margin of 5 mm is drawn around the visible borders of the lesion. The lesion is subsequently treated with a double freeze–thaw cycle of 30 to 60 seconds each cycle. Because atypical melanocytes may extend along the length of the hair follicles, treatment must freeze the tissue to this depth. Stevenson and Ahmed24 reviewed cure rates from more than 200 lentigo maligna patients treated with cryotherapy, with an overall recurrence rate of less than 9%. However, the recurrence rates in these studies ranged from 0% to 50%. Advantages of cryotherapy for lentigo maligna include its efficiency and avoidance of large surgical scars. One major disadvantage of cryosurgery is the inability to assess whether the lesion has been completely destroyed. In addition, because no tissue is obtained for definitive confirmation of cancer removal, the chance exists that recurrent melanoma may develop and that it may be invasive. Overlying scars may conceal the cancer.
KAPOSI SARCOMA
Although not commonly used, Tappero and colleagues reported the treatment of Kaposi sarcoma using a double freeze–thaw cycle every 3 weeks.25 An average of 3 treatments were required.
ELECTROSURGERY
Electrosurgery is a technique that uses the transmission of electricity to cut tissue, destroy tissue, and
3795
30
DAMPING VOLTAGE & AMPERAGE CURRENT NUMBER OF TERMINALS DESCRIPTION CIRCUIT LOOP INVOLVES PATIENT
Electrofulguration Damped sine wave High-voltage, low-amperage AC Spark from monoterminal electrode to tissue through air; no direct contact
Least damaging modality; epidermis primarily affected
Yes
Electrodessication Damped sine wave High-voltage, low-amperage AC Direct contact from monoterminal electrode to tissue
Electrocoagulation Moderately damped sine wave
Greater than electrofulguration, but damage is superficial
Yes
Low-voltage, high-amperage AC Direct contact from a biterminal node to tissue
Electrosection Undamped or slightly damped sine wave
Deeper tissue damage than electrofulguration and electrodessication; provides tissue coagulation
Yes
Low-voltage, high-amperage AC Direct contact Cuts tissue with minimal peripheral heat damage
Yes
Electrocautery
Low-voltage, high-amperage DC Heat is transferred from filament to tissue
Protein denaturation and coagulation Noa
Electrolysis
Low-voltage, low-amperage DC Negative electrode is applied to target tissue; acids are produced at the positive electrode
Electrolysis Low-voltage,
DC Negative electrode
low-amperage
Tissue liquefaction
Yes
Tissue liquefaction (negative electrode); tissue coagulation (positive electrode)
Yes
is applied to target tissue; acids are produced at the positive electrode
(negative electrode); tissue coagulation (positive electrode)
aTherefore, this technique is useful for patients with pacemakers or in nonconductive tissues of the body. AC, alternating current; DC, direct current.
cauterize vessels. Variations in current wavelength result in different biologic effects on tissue. For cutaneous procedures, electrosurgery can be categorized into 6 different treatment modalities: electrofulguration, electrodessication, electrocoagulation, electrosection, electrocautery, and electrolysis (Table 206-4).
MODALITIES OF ELECTROSURGERY
MODALITIES OF
ELECTROSURGERY
ELECTROFULGURATION
Electrofulguration uses a damped sine wave, highvoltage, low-amperage alternating current to generate a spark from a monoterminal electrode to the tissue via the air. There is no contact between the electrode and the tissue. This modality is the least tissue damaging of all of the high-frequency electrosurgery techniques, and results in rapid tissue healing. Most of the tissue damage is superficial, primarily involving the epidermis.
ELECTRODESSICATION
Electrodessication uses a damped sine wave, highvoltage, low-amperage alternating current to generate a current from direct contact of a monoterminal electrode
3796
to the tissue. Superficial tissue damage occurs as heat is transferred to tissue, causing cell death. The extent of tissue damage is directly related to electrode contact time with the skin. Although skin injury is greater with electrodessication compared to electrofulguration, most of the tissue damage remains superficial.
ELECTROCOAGULATION
Electrocoagulation uses a moderately damped sine wave, low-voltage, high-amperage alternating current to generate a current from direct contact of a biterminal electrode to the tissue. Tissue damage is deeper than with electrofulguration and electrodessication, providing tissue coagulation through the generation of heat in the tissue. Another distinguishing feature of electrocoagulation is the involvement of the patient within the circuit. This allows the use of a lower voltage and higher amperage to generate more coagulation.
ELECTROSECTION
Electrosection uses an undamped or slightly damped sine wave, low-voltage, high-amperage alternating current to cut tissue with minimal peripheral heat damage. The “Bovie” knife incorporates a blended undamped and damped sine wave that provides both cutting and coagulation at the same time.
ELECTROCAUTERY
Electrocautery uses a heating filament tip connected to a low-voltage, high-amperage direct current, usually a battery. Heat is transferred from the filament to the target tissue, causing protein denaturation and tissue coagulation. There is no electric current transfer to the target tissue, and the patient is not part of the circuit loop. Electrocautery is most used for patients with pacemakers or implantable cardiac defibrillators (ICDs) who are high-risk candidates for receiving electrosurgery. In addition, because patients are not part of the circuit loop, electrocautery is useful for nonconductive tissue areas of the body, such as the cartilage, bone, and nails.
ELECTROLYSIS
Electrolysis uses low-voltage, low-amperage direct current from a negative electrode to the positive electrode. The negative electrode is applied to the target tissue where electrons are released. The electrons interact with the tissue to produce sodium hydroxide and hydrogen gas resulting in tissue liquefaction. Acids are produced at the positive electrode resulting in tissue coagulation. The main use of electrolysis is for hair removal.
PERIOPERATIVE CONSIDERATIONS
PERIOPERATIVE
CONSIDERATIONS
PATIENT SELECTION
Patients commonly present for cutaneous surgery with either a cardiac pacemaker or an ICD. When taking preoperative history for surgery, patients should be asked if they have a device. Although technologic advances, such as titanium shielding, have provided safeguards against electromagnetic interference, electrosurgical devices may cause these cardiac devices to malfunction.
RISKS AND POTENTIAL COMPLICATIONS Interference with Pacemakers/Implantable Cardiac Defibrillators: ICDs deliver an electrical response to an abnormal ventricular rhythm. Some ICDs have a combination of a pacemaker and defibrillator to respond to both bradycardia and tachycardia. Electromagnetic interferences from electrosurgical devices may mimic a cardiac arrhythmia and cause the unit to discharge. Alternatively, the ICD may also respond by inhibiting cardioversion or pacing. Complications resulting from using electrosurgery for cutaneous surgery in patients with pacemakers or ICDs are uncommon. Matzke and colleagues
3
30
published a 3-year retrospective review of 173 patients with pacemakers and 13 patients with ICDs who underwent dermatologic surgery and reported no documented complications from electrosurgery.26 El- Gamal and colleagues reported a rate of 0.8 cases per 100 years of surgical practice from 166 completed surveys from members of the American College of Mohs Surgery and Cutaneous Oncology.27 In this study, the types of interferences reported were skipped beats, reprogramming of a pacemaker, firing of an ICD, asystole, bradycardia, and depletion of pacemaker battery life. Weyer and colleagues28 developed an ex vivo simulation device for assessing disruption of an implanted cardiac device. When electrosurgery was performed using normal (10W) and maximum (30W) power settings, the simulated devices only demonstrated interference at a distance of 1 cm with normal power settings and 3 cm at maximum power settings.
Safety and Recommendations for Patients with Implantable Cardiac Defibrillators: Recommendations have been published for the preoperative and intraoperative management of patients with pacemakers and ICDs during dermatologic surgery.29-33 Patients should be asked when scheduling surgery if they have one of these devices. If present, a preoperative evaluation by the patient’s cardiologist should be arranged before the surgical procedure. For management of patients with pacemakers or ICDs undergoing surgical procedures, consider the following recommendations.
■ Obtain cardiology consultation to determine if any perioperative actions need to be planned.
■ Provide continuous electrocardiography monitoring throughout the procedure.
■ Have advanced cardiac life support staff and crashcart equipment available.
■ Consider the use of alternative means of hemostasis such as patient-applied manual pressure34 or electrocautery.
■ Place the dispersing electrode in a location that directs the current pathway away from the cardiac device.
■ Use a bipolar forceps device to maintain the electrical circuit between the forceps tips.
■ Use minimal power and short electrosurgical bursts of 5 seconds or less.
■ Do not discharge the electrosurgical electrode on the skin directly over the pacemaker power source.
Patients may also present with noncardiac implanted electronic devices (IEDs) such as deep brain stimulators and cochlear implants. Noncardiac IEDs have a battery-powered pulse generator with electrodes that end in the targeted tissue. Risks and recommendations for noncardiac IEDs are similar to cardiac IEDs.35 In some cases, the devices may be turned off, however, the clinical effects on the patient after turning off the device must be taken into consideration.
Burns: There are several situations in which burns may occur with electrosurgery. Thermal injury can
3797
30
occur if there is inadequate contact between the patient and the dispersing electrode plate, when there is inadvertent contact between the dispersing electrode and the patient or surgeon, and if the patient or surgeon may “ground” himself or herself by touching a metal component of the table. Metal jewelry near the electrosurgical site should also be removed.
Fire: Electrosurgical current will ignite flammable substances like alcohol. When prepping the patient before electrosurgery, nonflammable disinfectants such as iodine or chlorhexidine should be used. If an alcohol-based disinfectant is used, the surgical area must be allowed to dry for at least 90 seconds prior to electrosurgery. In addition, electrosurgery should not be used near the presence of nasal cannulas, masks, or endotracheal anesthesia administering oxygen. Finally, care should be taken not to ignite paper surgical drapes in the surgical field.
Channeling: High-frequency electrosurgical current can be conducted along neurovascular bundles, causing pain and tissue damage distant to the local electrosurgical site. Using low-current settings or bipolar forceps may minimize this.
Infection and Mutagenicity: A plume of smoke is generated during electrosurgery. This traveling plume has been shown to contain carbonized tissue and blood, airborne particles, and various chemicals and gases. A review of the literature by Lewin and colleagues36 reported that electrocautery produces a plume of smoke composed of at least 38 chemical contents, including hydrocarbons, phenols, nitriles, fatty acids, carbon monoxide, acrylonitrile, and hydrogen cyanide. In addition, smoke created from treating lesions such as warts may contain bacteria and viruses, such as human papillomavirus, which may transmit infection.37
No known long-term risk for neoplasia or infection is known. The Occupational Safety and Health Administration recommends that surgical smoke be removed and properly filtered by a smoke evacuation system as close to the surgical site as possible.38 Furthermore, protective equipment, such as face shields and respiratory masks, should be worn during electrosurgery.
ANESTHESIA
During electrosurgery, local anesthesia such as lidocaine with epinephrine is required for patient’s comfort.
PERIOPERATIVE CARE
For all treatment groups, wound areas should be covered with a pressure bandage consisting of a topical petroleum product directly on the wound, an overlying nonstick bandage, and firmly applied gauze with adhesive tape.
3798
The pressure bandage is removed 24 to 48 hours posttreatment, and the wound site is cleaned with tap water or saline, gently rinsing over the wound. Petroleum jelly and bandage are changed daily after rinsing, for 3 to 4 weeks or until healed.
ELECTROSURGERY TECHNIQUES
ELECTROSURGERY
TECHNIQUES
EQUIPMENT
Electrosurgical equipment uses either direct or alternating current. In direct current, electrons flow in one direction, whereas in alternating current, electron flow reverses direction. With the exception of electrocautery or electrolysis, electrosurgical units used in dermatologic procedures have high-frequency alternating current. Electrosurgical units can be monopolar or bipolar, referring to the number of tissue-containing tips at the end of a surgical electrode. Monopolar denotes 1 tip, and bipolar denotes 2 tips. Monoterminal refers to the use of a treatment electrode without an indifferent or dispersing electrode. Biterminal refers to the use of both treatment and indifferent electrodes.
POSITIONING
Patients should be supine or prone on the examination table. The dispersing electrode (grounding pad) should be placed in a location that directs the current pathway away from the cardiac device (usually the right lower leg). If a pedal is used, it should be placed near the surgeon’s feet.
ELECTROSURGERY APPLICATIONS
ELECTROSURGERY
APPLICATIONS
HEMOSTASIS
The most common application of electrosurgery is its use in maintaining hemostasis in the operative field. Different techniques of electrosurgery can be used based on the type of electrosurgical unit used during surgical procedures. Coagulation can be achieved using electrofulguration, electrodessication, or electrocoagulation by direct application of the electrode to the bleeding vessel. This provides conduction of heat to the vessel, resulting in tissue coagulation (Fig. 206-3). Alternatively, vessels can be grasped by a forceps or hemostat, followed by application of the active electrode. When electrical current is placed against the metal instrument, heat is transferred from the electrode through the metal tip to the vessel. This technique is
best used when the surgical field cannot be visualized because of bleeding (Fig. 206-4).
ELECTROSURGERY OF BENIGN TUMORS
Electrodessication is an effective treatment modality for papular or plaque-like tumors of the epidermis, such as seborrheic keratoses, verrucae, dermatosis papulosis nigra, molluscum, or flat warts. First, the area around the lesion is anesthetized with lidocaine containing epinephrine. Then, the lesion is touched with the low-power electrode until a gray, superficial, charred layer involves the entire lesion. The charred tissue is removed from the treated lesion by wiping with a sterile gauze or curetting. The process is repeated until the lesion is removed at the level of the surrounding skin. This method results in minimal bleeding and scarring because just the epidermal components are removed.
3
30
CURETTAGE AND ELECTRODESSICATION OF MALIGNANT TUMORS
Curettage and electrodessication (C+D) is a commonly used treatment option for BCCs and SCCs. Certain tumor characteristics, however, should be present to ensure high cure rates and acceptable cosmetic outcome. Tumors should be primary; have distinct clinical borders; be located on sites of low recurrence, such as the trunk, extremities, or non-”H”-zone regions of the face; have a superficial or nodular histologic subtype; and have a diameter of less than 1 cm on the face and less than 2 cm on the trunk and extremities. In addition, C+D is a viable treatment option for patients with high morbidity cofactors that make surgical excision too risky, and for patients who cannot make regular followup visits. Tumors not acceptable for C+D include those with indistinct borders, tumors on the “H”-zone of the face, tumors with an aggressive histologic pattern, tumors with high metastatic potential, and tumors that require histologic diagnosis. For patients with cardiac pacemakers or ICDs, electrocautery may be substituted for electrodessication. The tumor outline should be marked, and lidocaine with epinephrine should be injected to provide adequate local anesthesia (Fig. 206-5). With firm counterpressure, the lesion is then curetted in a checkerboard pattern until the clinical appearance of the lesion is removed (Fig. 206-6). This is followed by electrodessication on high power of the base and periphery of the lesion (Fig. 206-7). This C+D procedure is repeated up to 2 more times until a resultant atrophic defect without clinical evidence of residual tumor is achieved. Some advocate the inclusion of a 2-mm to 4-mm rim of clinically normal skin during the C+D procedure, and individual variations of the protocol are established. If curettage of the BCC extends into subcutis, then an extensive invasion of a BCC has occurred, and excision should be performed. The advantages of treatment with C+D include time efficiency, ease of surgical technique, and minimal posttreatment morbidity. Disadvantages of treating
3799
30
with C+D include nonconfirmation of histologic tumor clearance, practitioner-dependent efficacy, and potentially long (3- to 4-week) healing times via second intention healing. Furthermore, the cosmetic result may show hypopigmentation, atrophy, persistent erythema, and hypertrophic scarring.
OUTCOME ASSESSMENTS OF CURETTAGE AND ELECTRODESSICATION
The 5-year cure rates for C+D have been reported to be 74% to 100% for BCCs39-49 and 96% to 100% for SCCs.39 Although some authors have reported that 20% to 40% of tumors remain immediately following C+D, the 5-year cure rates demonstrate an additional factor may be contributing to the destruction of the
3800
treated malignancy. Some authors have speculated that the inflammatory response or a specific antitumor humoral response following electrosurgery may be responsible for the low recurrence rate.50,51
C+D in combination with other topical treatments may have a synergistic effect in tumor clearance. In a double-blinded, placebo-controlled pilot study by Spencer,52 10 BCCs were treated with C+D and 10 patients were treated with C+D followed by 1 month of daily, topically-applied imiquimod cream. The author reported a substantially reduced frequency of residual BCC and improved cosmetic appearance in the C+Dimiquimod group compared with the C+D-alone group. Another study by Wu and colleagues53 reported excellent efficacy and cosmetic results for nodular BCCs of the trunk and limbs treated with curettage (no electrodessication) followed by daily topical application of imiquimod cream for 6 to 10 weeks. In that study, 32 (94%) of 34 lesions demonstrated no residual histologic evidence of tumor.

Figure 206-1 Actinic keratosis on forehead treated with liquid nitrogen.

Figure 206-2 Warts on hand treated with liquid nitrogen.

Figure 206-3 Electrodessication of bleeding vessel during Mohs surgery.
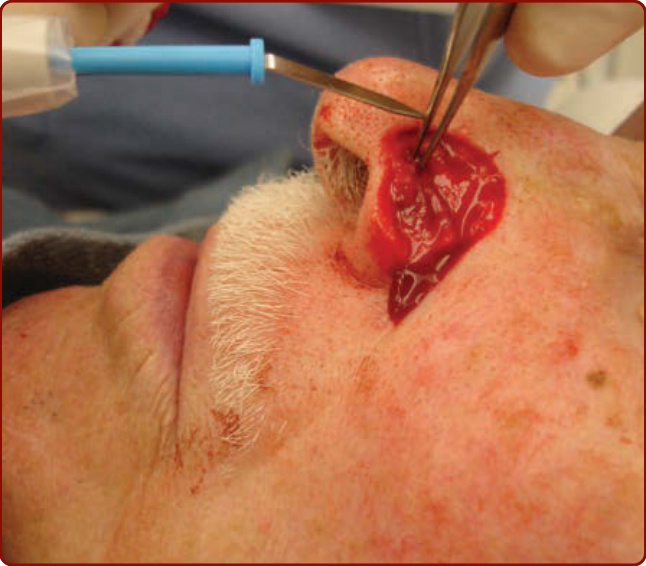
Figure 206-4 Electrocurrent applied to forceps to cauterize bleeding vessel during Mohs surgery.

Figure 206-5 Clinical outline of skin tumor before curettage and electrodessication.

Figure 206-6 Curettage of skin tumor during curettage and electrodessication procedure.

Figure 206-7 Electrodessication of skin tumor during curettage and electrodessication procedure.
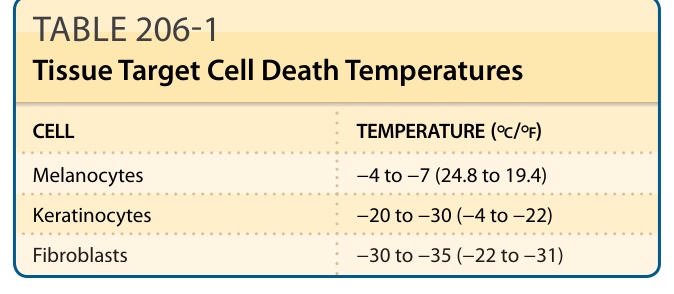
Table 206-1 lists targets of cryosurgery with associated cell death temperatures. Melanocytes are the most sensitive to cryosurgery, with cell destruction at temperatures of −4°C to −7°C (24.8°F to 19.4°F).6 As a result, depigmentation may occur, especially in darkly pigmented individuals. Keratinocytes require longer freezing to temperatures of −20°C to −30°C (−4°F to −22°F) until cell death and are more resistant to cooling effects. Fibroblasts are the most resistant to freezing and do not undergo cell death until −30°C to −35°C (−22°F to −31°F). A temperature of −50°C to −60°C (−58°F to −76°F) is needed for destruction of malignant lesions, whereas lesser degrees of freezing are needed for benign lesions.
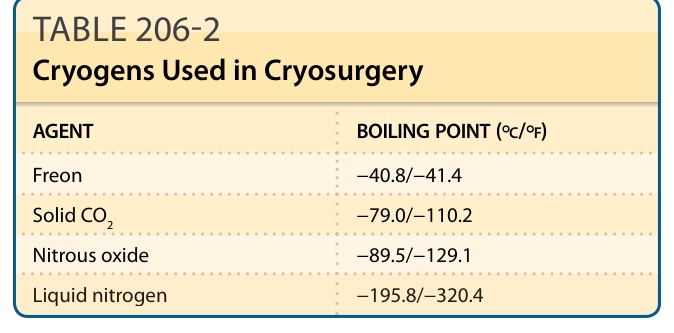
TABLE 206-2 Cryogens Used in Cryosurgery
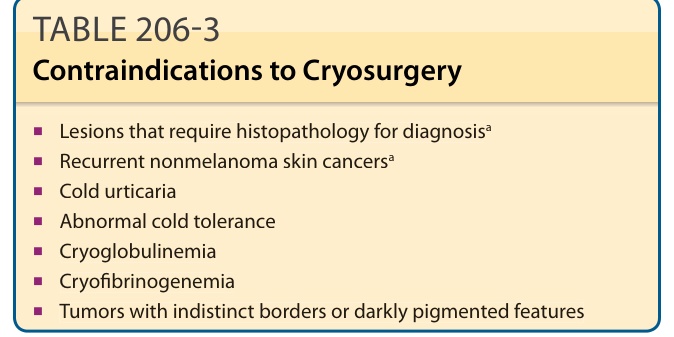
TABLE 206-3 Contraindications to Cryosurgery
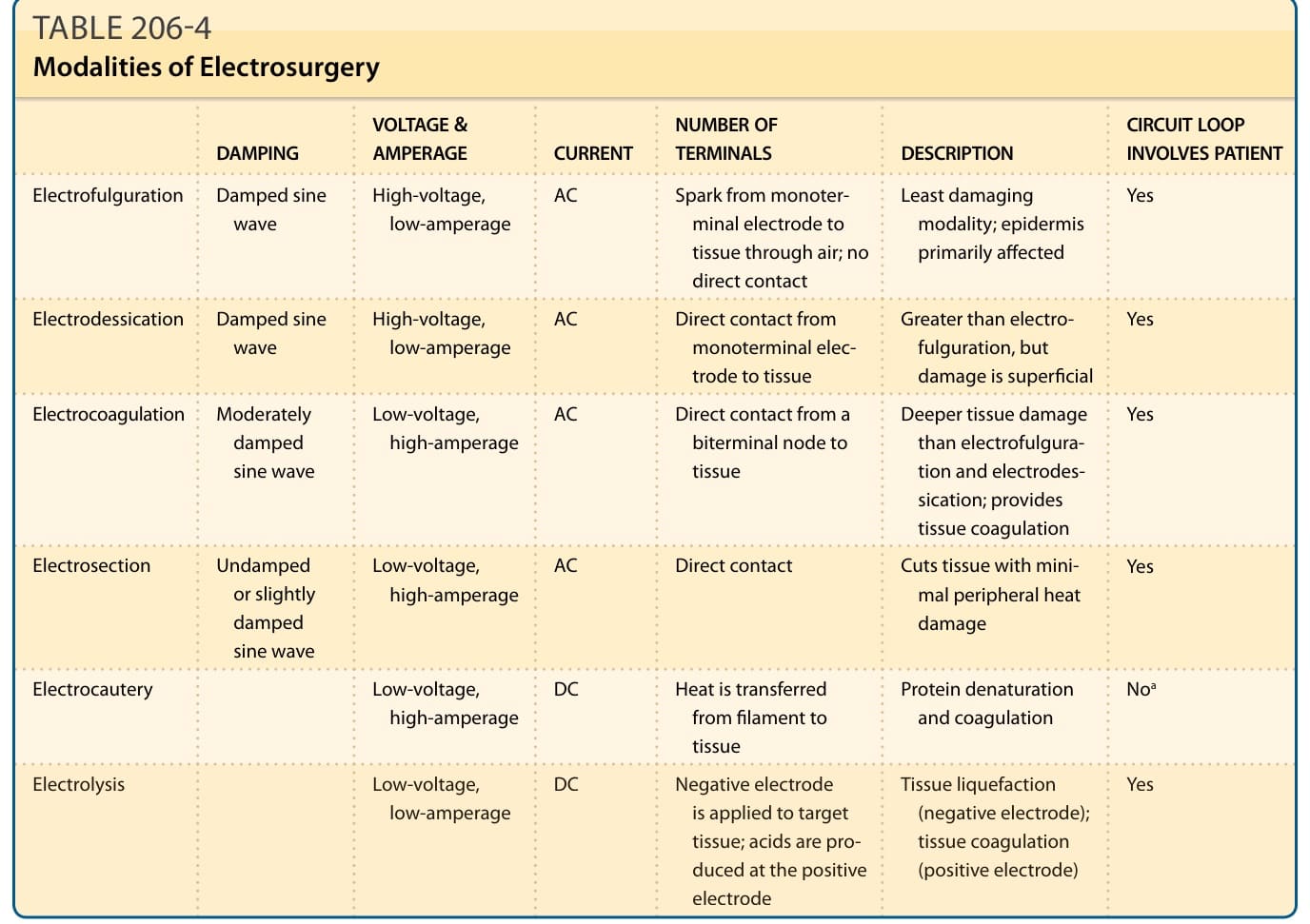
TABLE 206-4 Modalities of Electrosurgery