Nail Surgery
30
AT-A-GLANCE
■ Nail surgery requires careful patient selection to prevent unnecessary complications.
■ The technique used for anesthesia depends on the type of surgery. Distal digital block with ropivacaine 2 mg/mL is usually the best option.
■ Partial nail avulsion allows the exploration and/or the treatment of a subungual lesion or the removal of a pathologic nail plate. Total nail plate avulsion should be discouraged to prevent nail bed shrinking and distal embedding.
■ Nail biopsies are performed to determine the histopathologic features of a lesion or to clarify an uncertain clinical diagnosis.
■ Lateral longitudinal biopsy is the best technique for inflammatory disorders or lateral longitudinal melanonychia.
■ Punch biopsy less than 3 mm in the distal matrix does not produce serious dystrophy.
■ Tangential shave excision is the best option for superficial matrix tumors such as wide longitudinal melanonychia or superficial epithelial benign tumors.
BACKGROUND
The main objectives of nail surgery are to aid diagnosis by biopsy, to treat infection, to alleviate pain, to remove local tumors, and to ensure the best cosmetic results in acquired and congenital abnormalities.
PERIOPERATIVE CONSIDERATIONS
PATIENT SELECTION
PATIENT SELECTION
Providing the patient with an exact illustration of the operation is helpful to give the patient insight into the procedure and its expected outcome. A thorough discussion regarding postoperative morbidity is essential.
RISKS AND PRECAUTIONS
RISKS AND PRECAUTIONS
Preoperative photographs as well as any taken during surgery may be useful medicolegally. Careful history taking may reveal systemic disease such as diabetes
mellitus, blood dyscrasia, vascular disease, vascular collagen disease (scleroderma), allergy, chronic pulmonary disease, or immune impairment. Any of these may at times be relative contraindications to surgery, may be associated with severe complications (infection, necrosis), or may call for alteration of the technique to be used. Surgery of the nail is not recommended in patients with high-risk conditions. A history of concurrent use of drugs may be relevant, because these drugs may affect anesthesia (eg, monoamine oxidase inhibitors or phenothiazines), prolong bleeding (eg, aspirin and anticoagulants), delay healing (eg, glucocorticoids), or have toxic effects on the nail apparatus (eg, retinoids). There may be a history of allergy to lidocaine or mepivacaine or to parabens contained in both as a preservative. A magnifying lens and dermoscopy are useful to observe the color, surface, and structure of the periungual tissue and to compare the unaffected contralateral digit. It may be necessary to probe to localize pain, to obtain a radiograph to rule out underlying bone involvement, or to ask for ultrasonography and MRI when a tumor is suspected. The basic requirements for nail surgery include a detailed knowledge of the anatomy and physiology of the nail apparatus on the part of the surgeon. Full aseptic conditions, regional block anesthesia, and local hemostasis are indispensable.
ANATOMY1 (CHAP. 8)
ANATOMY
(CHAP. 8)
1
The nail plate is the permanent product of the nail matrix. Its normal appearance and growth depend on the integrity of the perionychium and the bony phalanx (Fig. 205-1). The nail is a semihard horny plate covering the dorsal aspect of the tip of the digit. The nail is inserted proximally in an invagination that is practically parallel to the upper surface of the skin and laterally in the lateral nail grooves. This pocketlike invagination has a roof, the proximal nail fold, and a floor, the matrix from which the nail is derived. The matrix extends approximately 6 mm under the proximal nail fold, and its distal portion is only visible as the white semicircular lunula. The general shape of the matrix is a crescent, concave in its posteroinferior portion. The lateral horns of this crescent are more developed in the great toe and are located at the coronal plane of the bone. The ventral aspect of the proximal nail fold encompasses both a lower portion, which continues the matrix, and an upper portion (roughly three-quarters of its length), called the eponychium (Fig. 205-2). The germinal matrix forms the bulk of the nail plate. The proximal element forms the superficial third of the nail plate, whereas
Sagittal section of the nail unit
Proximal nail fold
Extensor tendon Eponychium Nail matrix
Cuticle Lunula
Lateral nail fold
Nail plate
Middle phalanx Flexor tendon Terminal phalanx
Nail bed Hyponychium
the distal element provides its inferior two-thirds. The ventral surface of the proximal nail fold adheres closely to the nail for a short distance and forms a gradually desquamating tissue, the cuticle, made of the stratum corneum of both the dorsal and the ventral sides of the proximal nail fold. The cuticle seals and protects the nail cul-de-sac. The nail plate is bordered by the proximal nail fold, which is continuous with the similarly structured lateral nail fold on each side. The nail bed extends from the lunula to the hyponychium. It has parallel, longitudinal rete ridges. In contrast to the matrix, the nail bed has a firm attachment to the nail plate. Colorless but translucent, this highly vascular connective tissue, containing glomus organs, transmits a pink color through the nail. Avulsion of the overlying nail plate denudes the nail bed. Distally, adjacent to the nail bed, lies the hyponychium, an extension of the volar epidermis under the nail plate, which marks the point at which the nail separates from the underlying tissue. The distal nail groove, which is convex anteriorly, separates the
Origin of nail layers
Superficial (dorsal) nail plate Sublingual keratin (ventral nail)
Eponychium
Proximal matrix
Lunula Nail bed (sterile matrix)
Deep nail layer
Intermediate matrix
3
30
hyponychium from the fingertip. The circulation of the nail apparatus is supplied by 2 digital arteries that course along the digits and give off branches to the distal and proximal arches. The sensory nerves to the distal phalanx of the 3 middle fingers are derived from fine, oblique, dorsal branches of the volar collateral nerves. Longitudinal branches of the dorsal collateral nerves supply the terminal phalanx of the fifth digit and also the thumb. Among its multiple functions, the nail provides counterpressure to the pulp that is essential to the tactile sensation involving the fingers and to the prevention of hypertrophy of the nail bed.
INSTRUMENTS AND DRAPING
INSTRUMENTS AND
DRAPING
The instruments used in nail surgery are, in general, the same as those used in cutaneous surgery with the addition of the instruments listed in Table 205-1. Draping is accomplished by means of a sterile surgical drape or a sterile glove on the involved hand. The tip of the glove is cut off on the finger that is to undergo surgery. The remaining open finger of the glove is then rolled back down the digit. This exsanguinates the digit and provides a tourniquet when it reaches the proximal part of the finger. Disinfection is extremely important to avoid contamination of the wound with consecutive infection. Isopropyl alcohol scrub and chlorhexidine have proven to be superior to povidone iodine washing.
ANESTHESIA
ANESTHESIA
Local anesthesia should be administered while the patient is reclining or in a supine position. Lidocaine 1% or 2% is widely used because the incidence of allergy to this agent is very low as well as for its low cost. Buffered 2% lidocaine and ropivacaine are characterized by quick absorption and near instantaneous anesthesia. Applying Emla or LMD under occlusion 2 hours prior to the injection may lessen the pain especially in children. For anxious patients, administering a fast-acting benzodiazepine orally (midazolam, alprazolam or diazepam) 2 hours
■Nail elevators
■Nail elevators
■Single- or double-pronged skin hooks
■Single- or double-pronged skin hooks
■Double-action nail splitter (bone rongeur)
■Double-action nail splitter (bone rongeur)
■Clippers, splitting scissors, English nail splitter
■Clippers, splitting scissors, English nail splitter
■Pointed scissors (Gradle scissors), curved iris scissors
■Pointed scissors (Gradle scissors), curved iris scissors
■Small-nosed hemostats
■Small-nosed hemostats
■Disposable biopsy punches
■Disposable biopsy punches
■Penrose drains
■Penrose drains
3775
■Luer-Lok syringe, 30-gauge needles
■Luer-Lok syringe, 30-gauge needles
30
before anesthesia can considerably reduce the fear of the injection.2 Ropivacaine 2 mg/mL is another agent that can be used and offers the advantage of a rapid onset and a long duration, usually between 8 and 12 hours. The use of local anesthesia in conjunction with epinephrine for surgery on digits is no longer contraindicated and offers the advantage of vasoconstriction and thus a less bloody surgical field. However, caution is warranted for patients with risk factors predisposing for local circulatory insufficiency. Buffering and warming the local anesthetic coupled with a slow rate of injection and small needle size, all drastically reduce the pain of injection. Buffering is accomplished with the use of 1 part 7.5% bicarbonate with 9 parts. Anesthetics are administered via a 30-gauge needle for fingernails or a 27-gauge needle for toenails on a Luer-Lock syringe using either a proximal digital block or, better, a distal digital block (wing block) procedure. Other techniques, such as median distal anesthesia or transthecal block, have not replaced the classic routes of anesthesia. Although emergencies related to minor surgery occur rarely, the ready availability of resuscitative equipment and expertise is essential.
PROXIMAL DIGITAL BLOCK
This is the more traditionally used block. Although less painful than the distal block procedure, the anesthesia takes 5 to 10 minutes to become established. The hand is laid down flat, with the fingers spread, so that 1 to 2 mL of anesthetic can be administered by a dorsal injection, with a thin needle inserted and directed tangentially to the sides of the bony phalanx at the base of the involved finger and as far as the lateral side of the flexor tendon (Fig. 205-3). A tourniquet effect may inadvertently be produced by injecting more than 5 mL of anesthetic and should be avoided. The absence of blood reflux in the syringe should be verified before injection if a nondental syringe is used. When the operation is strictly localized to a lateral region, a block limited to the nerves ipsilateral to the lesion suffices, as in the case of a partial distolateral nail avulsion.
Proximal digital block
Dorsal View Volar View
3776
DISTAL DIGITAL BLOCK
The distal digital block procedure is more painful than the proximal block procedure, but anesthesia occurs immediately. As such, it is our preferred method of anesthesia in the absence of a digital bacterial infection. For a distal digital block, the needle is inserted just behind the junction of the proximal nail fold and a lateral nail fold and a few 10ths of a milliliter of anesthetic is injected, which whitens the region. The injection is continued by aiming the needle toward the pad. One then returns to the initial area to inject the proximal fold transversely. Finally, at the junction of the proximal fold with the lateral fold on the opposite side, one proceeds as described earlier (Fig. 205-4). The anesthesia is almost immediate, and when the procedure is done correctly, injections rarely have to be extended to the distal area of the finger. Median distal administration is relatively simple and quick (Fig. 205-5). The needle is introduced at a 30° angle into the middle of the proximal nail fold and advanced distally into the underlying matrix. Anesthetic is injected slowly as the needle pierces first the nail plate, then the matrix, and finally the adjacent nail bed. The nail plate is soft and offers little resistance. Blanching confirms the delivery of anesthetic to the nail matrix and bed. Pain is brief and anesthesia nearly instantaneous. This method is suitable for most procedures performed on the proximal half of the nail unit. It is not suitable for matricectomy or complete nail avulsion.
TRANSTHECAL BLOCK
The flexor tendon sheath may be used as an avenue for introducing anesthetic to the core of the digit. Through centrifugal anesthetic diffusion all 4 digital nerves are anesthetized rapidly. This technique involves palmar percutaneous injection of 2 mL of lidocaine or ropivicaine into the potential space of the flexor tendon sheath at the level of the palmar flexion crease using a 3-mL syringe and a 25-gauge hypodermic needle. Postoperative pain may be more severe than with other techniques.
Distal digital block
REGIONAL BLOCKS AND GENERAL ANESTHESIA
These are used mainly in more extensive and painful surgeries or in circumstances under which it is useful to have anesthesia of more than 1 digit at the same time. For instance, it may be appropriate in the surgical treatment of numerous warts and in the infiltration of more than 1 finger with triamcinolone in the treatment of nail unit psoriasis. General anesthesia is also indicated for nail rotation of congenital malalignment of the big toe nail in children.
TOURNIQUETS
TOURNIQUETS
Most nail surgery procedures are undertaken with strict surgical ischemia to avoid bleeding and enable a correct visualization of the operative field. Use of the digital tourniquet is relatively safe and efficacious. For brief intraoperative hemostasis (eg, nail avulsion, punch biopsy of the nail bed), squeezing the sides of the digits is effective. If a prolonged bloodless field is required, a Penrose drain may be placed around the base of the digit and secured with a hemostatic clamp for use as a tourniquet. It is preferable not to leave it on for more than 15 to 20 minutes. The tourniquet application can be interrupted for a few minutes during longer procedures. Although it seems intuitive, it is essential to never forget the tourniquet on, as several cases of digital necrosis following forgotten tourniquet have been reported.3
To facilitate establishment of a bloodless field, the use of an exsanguinating tourniquet is recommended1
3
30
Exsanguinating tourniquet
before anesthesia. A wide Penrose drain is wound tightly in loops that overlap in a distal to proximal fashion, with an exposed loose end left distally (Fig. 205-6). This “milks” the blood from the digit. The loose end is then grasped and the drain unwound, again from distal to proximal, until the nail unit is exposed with the final proximal loop. In the absence of contraindication, the addition of epinephrine to lidocaine, for example, may reduce the need for a tourniquet and produce better and longer pain control perioperatively.
DRESSING AND POSTOPERATIVE CARE
DRESSING
DRESSING
At the end of the operation, either the digit is cleansed with sterile 10% hydrogen peroxide solution and sprayed with a colorless disinfectant or an antiseptic with hemolytic action is applied. The nail area is then covered with an antiseptic or antibiotic ointment on gauze or pads. Dressing must be done in a way that takes into account oozing, pain, and sensitivity. A bulky dressing provides a cushion against local trauma. Compressive dressing is mandatory and must not be removed in the first 48 hours following the procedure. The compression must be applied to the distal part of the digit and not proximally to avoid a tourniquet effect. Then, the dressings should be changed every other day or daily if there is infection. Several layers of sterile gauze should be kept in place by Micropore (2.5-cm) tape placed first on the dorsal aspect of the finger or toe, then on the ventral aspect, and last on the lateral edges in a U shape (a circular dressing should never be applied in the first week). Finally, use of an X-span tube dressing or Surgitube will give the patient more freedom to use the hand, but care must be taken that dressings do not constrict
3777
30
blood flow. During the first 48 hours, the arm must be kept in a sling. Stitches are removed after 7 to 12 days. When the feet are treated, daily chlorhexidine baths precede the care just described. For all operations involving the toes, the patient should wear an appropriate shoe or sandal after the dressing has been applied. The patient should be recumbent for 24 to 48 hours, with the foot elevated to 30°.
POSTOPERATIVE COMPLICATIONS
POSTOPERATIVE
COMPLICATIONS
BLEEDING
Bleeding seen after the tourniquet is removed is not worrisome as the compressive dressing will stop it. In case of persistent bleeding, 35% aluminium chloride solution or an oxidized cellulose application (Gelfoam) should be applied. Alternatively, an extra injection of lidocaine + epinephrine bilaterally will stop the bleeding through compression of the vessels.
PAIN
Pain threshold varies based on the procedure and from patient to patient. CO2 laser vaporization of warts and chemical matricectomy are the least painful procedures whereas larger excisions require the use of more potent postoperative painkillers. While the dressing is being put in place, the patient must be told what precautions to take. Providing a supply of moderately potent oral analgesics will help the patient feel in control of any pain. Elevating the extremity during the first 48 hours is advised to prevent swelling and decreases the experienced postoperative pain. Weak opioids can be prescribed in the presence of moderately perceived pain as well as nonsteroidal antiinflammatory drugs while strong opioids are restricted to intense pain. Pulsating pain beginning after 36 to 48 hours may indicate an infection, which should be treated according to the results of bacterial culture of the organism. Any bulky dressing that is blood stained after 24 hours should be changed.
DYSESTHESIA
DYSESTHESIA
Occurrence of postoperative long-term dysesthesia after nail surgery is well known. Complete or partial resolution may be noted after 6 to 12 months.
INFECTION
Prophylactic antibiotic treatment is mandatory for patients with prosthetic valve and in prevention of joint prosthesis infection. Peripheral vascular disease and young age (in childhood, the nail matrix is extremely fragile and behavior is less sanitary) are
3778
further indications. Tetanus toxoid for lesions of the toes should be discussed and advised especially in farmers, for example. If there are ragged surfaces to the nail, which makes thorough preoperative cleaning difficult, antibiotics may prevent wound infection. Postoperative infection may be caused by preoperative colonization or infection. Culture of preoperative swab specimens will indicate the best choice of drug after initial coverage with a broad-spectrum antibiotic. Attention to detail is important. Carelessness may result in serious infectious complications in the soft tissue and occasionally in bone. Routine or preoperative nail cleansing softens the nail plate and keeps contamination to a minimum. In the event of an infection, broad-spectrum antibiotics should be initiated.
ACQUIRED NAIL MALALIGNMENT4
Development of malalignment of the nail plate may result from lateral longitudinal biopsy in excess of the routine 3 mm.
RELAPSE
Relapse will depend on the nature of the lesion treated. Warts, ingrown nails, and myxoid cysts can be difficult to eradicate.
RESIDUAL DYSTROPHY
Residual dystrophies are not unusual when surgery involves the proximal area of the matrix. Nail spicules can be observed after lateral longitudinal excision, lateral matricectomies, or total removal of the nail apparatus.
UNPREDICTABLE COMPLICATIONS
■ Necrosis can result from too tight stiches.
■ Hypertrophic scars and keloids are rare.
■ Implantation epidermoid cysts may occur in operation scars.
■ Reflex sympathetic dystrophy now known as “Complex regional pain syndrome” Type I is rare. It presents with pain sensitive and motor disturbances along with autonomic and even soft tissue trophic changes.
NAIL AVULSION
A nail avulsion consists of separating the nail plate from its underlying attachments. It allows the exploration and/or the treatment of a subungual lesion or the removal of a pathologic nail plate. The nail is strongly adherent to its underlying bed and less adherent at the level of the distal matrix and the lateral nail folds. An avulsion is therefore easier to perform either a proximal or lateral approach. The
removal of the nail plate can be carried out using distal or proximal approaches. In both techniques, inserting the blunt instrument back and forth between the horny layer of the proximal nail fold and the nail plate loosens the proximal nail fold adherence. Anesthesia is mandatory except in case of preexisting onycholysis.
DISTAL APPROACH
DISTAL APPROACH
In the more commonly used distal approach, a Freer septum elevator or a dental spatula is inserted between the nail plate and nail bed (Fig. 205-7A). The nail is separated from its nail-bed attachment using
3
30
proximal force applied in anterior–posterior movements so as not to injure the longitudinal ridges of the nail bed. The detachment is completed by firmly pushing the instrument into the posterolateral corners of the nail plate. Then, one of the lateral edges is grasped with a sturdy hemostat, and extracted with an upward and circular movement to accomplish the removal of the nail plate.
PROXIMAL APPROACH
PROXIMAL APPROACH
The advantage of a proximal approach for nail avulsion is to prevent an injury to the distal nail bed and hyponychium through the insertion of the Freer septum. The
Distal and proximal nail avulsion
B1: proximal
distal
B2: proximal
B3: proximal
A B
C1: proximal partial avulsion
C
C2: proximal partial avulsion
3779
30
spatula is then used to reflect the proximal nail fold, and is delicately inserted under the base of the nail plate where adherence is normally weak (Fig. 205-7B). The instrument is advanced distally following the natural cleavage plane, and this operation is repeated on the entire width of the subungual region. After the last attachments are freed, the nail plate is easily pulled out. Total surgical removal should be discouraged, however, because the distal nail bed may shrink and become dislocated dorsally. In addition, the loss of counterpressure produced by the removal of the nail plate allows expansion of the distal soft tissue, and the distal edge of the regrowing nail then embeds itself. In patients at high risk, nonsurgical removal of the nail plate should be considered when necessary. This can be accomplished by applying 40% urea paste directly to the nail after protecting the surrounding skin. Urea acts on the bond between nail keratin and diseased nail plate, sparing only the normal nail tissue.
PARTIAL NAIL AVULSION
PARTIAL NAIL AVULSION
The problems that can arise after total nail avulsion may be overcome by partially avulsing the nail. Partial distal avulsion requires only separation of the
A
3780
nail from the distal nail bed. This procedure can be performed under local anesthesia in selected patients, when, for instance, a fungal infection is of limited extent. An affected portion of the nail plate may be removed in one session, even when the disease has reached the deeper regions of the subungual tissue beneath the proximal nail fold. Commonly, an English anvil nail splitter or a double-action bone rongeur is used for this procedure. Partial surgical section of the lateral and/or medial segment of the nail plate may be sufficient for the treatment of distal lateral subungual onychomycosis (Fig. 205-7C). In the toe, this procedure leaves enough normal nail to counteract the upward forces exerted on the distal soft tissue when walking, and this will prevent the appearance of a distal nail wall. In proximal subungual onychomycosis, removal of the nonadjacent base of the nail plate, cut transversely, leaves the distal portion of the nail in place (Fig. 205-8), which decreases discomfort. Similarly, an acute paronychia that does not respond to appropriate antibiotics within 48 hours should be treated surgically by removing the base of the nail plate. Moreover, in cases of nail matrix procedures, a partial proximal avulsion prevents damaging the distal nail while allowing for an excellent visualization of the matrix and the cul-de-sac. The proximal nail plate is usually cut at its proximal third, lifted up, and always pulled back into its initial position at the end of the procedure.
B
TRAP DOOR NAIL AVULSION
TRAP DOOR NAIL
AVULSION
This technique minimizes trauma in nail surgery when accessing the nail bed and matrix. Trap door nail plate avulsion entails separation of all periungual attachments except for that between the dorsum of the nail and the ventral aspect of the proximal nail fold. Both are then reflected en bloc in the manner of a trap door, utilizing the same oblique incisions normally made for reflection of the PNF alone. A partial medial trap door nail avulsion is also recommended for medial longitudinal excision.
NAIL BIOPSIES
Biopsies are performed to determine the histopathologic features of a lesion or to clarify an uncertain clinical diagnosis. Techniques depend on the location of the lesion.
LATERAL LONGITUDINAL BIOPSY OR LATERAL FUSIFORM EXCISION
LATERAL LONGITUDINAL
BIOPSY OR LATERAL
FUSIFORM EXCISION
It gives information of the entire nail organ and therefore represents the best technique for the diagnosis of inflammatory disorders as lichen planus or psoriasis when all the subunits of the nail apparatus are involved. Lateral longitudinal biopsy is also advised when longitudinal melanonychia3 is located in the lateral part of the nail plate (Fig. 205-9). An elliptical incision may be made on either side of the nail plate and proximal nail fold. For the most part, the incisions parallel the lateral edge of the nail plate. Beginning in the lateral nail groove, the incisions should include a 3- to 4-mm nail segment reaching to the bone. (See
3
30
Video 205-1 at mhprofessional.com/fitzderm9evideos) This ensures that a full-thickness fragment of the matrix with its lateral horn is obtained. Slightly curved iris scissors are useful for separating the tissue from the bone. Starting at the tip of the digit, one proceeds proximally while maintaining contact with the bony phalanx. Backstitches for the lateral nail folds avoid their flattening. It is helpful, especially for thick toenails, to soften the nail before the procedure by soaking it in warm water for 5 minutes.
BIOPSY OF THE DISTAL NAIL MATRIX 5-7
A 3-mm punch biopsy may be performed through the nail plate into the distal matrix. Three millimeters is the maximum size that does not produce serious dystrophy, although even biopsies of this size can cause such effects if carried out in the most proximal portion of the nail matrix. When a punch biopsy is used to sample longitudinal melanonychia of less than 3 mm in width, the circumferential incision is made around the origin of the band, through the nail plate (Fig. 205-10A). This area may be distal enough to be reached by pushing back the cuticle (Fig. 205-10B), but if it is more proximal, the proximal nail fold may have to be reflected using a posterolateral incision. The next step is to remove the proximal third of the nail plate (Figs. 205-10B and C), while leaving the cylinder of tissue containing the origin of the longitudinal melanonychia still in place. This technique allows the surgeon to inspect the surrounding nail matrix and bed with a magnifying lens to determine whether the pigment extends around the punch incision (Figs. 205-10C and D) and facilitates the removal of the cylinder of biopsy tissue with a Gradle scissors. (See Video 205-2 at mhprofessional.com/fitzderm9evideos.) For transverse biopsy (Fig. 205-11), 2 small oblique incisions are made on each side of the proximal nail fold. The fold is then reflected to expose the matrix area. The proximal third of the nail plate is avulsed. Then, the lesion is removed by excising an elliptical or crescent-shaped wedge of tissue with the convex portion of the crescent paralleling the anterior border of the lunula. When longitudinal melanonychia lies within the midportion of the nail plate, the potential for postoperative dystrophy is great, and selection of the optimal biopsy method is difficult (Fig. 205-12) (Haneke’s releasing flap technique derived from Schernberg’s releasing flat method). It is important to establish the matrix origin (proximal or distal) of longitudinal melanonychia preoperatively, because the more proximal the origin, the greater the risk of nail dystrophy.5 The origin of pigmentation may be determined by dermoscopy of the free edge of the nail.8
Tangential matrix biopsy (Fig. 205-13) for wide longitudinal melanonychia is a good option. Cutting, then reclining the proximal portion of the nail plate (1), after reflecting the proximal nail fold (2), the pigmented lesion is exposed. An incision is made around
3781
30
A B
C D
the lesion, followed by its tangential removal. Finally, the proximal nail plate is replaced and the oblique incisions of the proximal nail fold are maintained by micropore. This technique is claimed to give the best cosmetic results.
NAIL BED BIOPSY
Biopsy (Fig. 205-14) may be useful in any pathologic condition involving the nail bed. Punch biopsy is done with a 3- or 4-mm-diameter punch, which is driven perpendicularly into the nail plate in a circular
3782
motion down to the bone. However, it is not always easy to extract the cylinder cut with an area this small. One useful technique is to perforate the nail plate with a 6-mm punch without injuring the underlying tissue (Fig. 205-14A). The covering nail is then detached by using the tip of the scalpel to remove the disk of nail, and the biopsy is performed easily by using the 4-mm punch to the bone. The tissue can then be released from its tether with fine scissors. It is advisable to replace the 6-mm disk of nail keratin, after cleaning with 10% hydrogen peroxide, to cover the hole. If the nail plate is thick, rotating grinders can
Transverse biopsy of the nail matrix
Haneke’s releasing flap technique for longitudinal melanonychia within the midportion of the nail plate
Reflected proximal nail fold
(1) (2)
3
30
Nail bed biopsy
6 mm 6 mm 4 mm
4 mm
A
4 mm 6 mm
B
be used to thin it down and facilitate the transungual biopsy.
PROXIMAL NAIL FOLD BIOPSY
A 2- to 3-mm punch may be used for biopsy of a tumor. A blister may be completely removed by shave biopsy using half a razor blade (Fig. 205-15). Excision of a 3-mm crescent-shaped tissue segment in the proximal region of the lateral nail folds may be helpful in the evaluation of collagen disease.
Proximal nail fold shave biopsy
Razor blade
Small blisters
Biopsy site
3783
30
APPLICATION TO THE DIFFERENT TISSUES OF THE NAIL APPARATUS
NAIL MATRIX PROCEDURES
NAIL MATRIX PROCEDURES
When surgery involves the nail matrix, there are 3 primary approaches, including (1) a reduction in its width or (2) its length for removal of tumors, for instance, by using a cold steel procedure or (3) a 2- to 3-mm punch biopsy. In contrast to these 3 procedures, complete matricectomy, that is, ablation of the nailforming tissue, is rarely performed because the nail is permanently lost (Fig. 205-16). After reduction of the nail matrix width, one is left with a narrower nail and after reduction of the length, with a diminution in the thickness of the nail. Reduction of the matrix width is a useful and/or necessary procedure in the following major circumstances: need for lateral-longitudinal biopsy, lateral nail splitting, benign or malignant tumor in the lateral third of the nail apparatus, longitudinal melanonychia in a lateral location, ingrown nail, racquet nail. Destruction of lateral horn of the matrix can be performed surgically for lateral tumors or chemically with a solution of 88% phenol, 80% trichloroacetic acid, or 10% sodium hydroxide for nail splitting, ingrowing nail, or racquet nail (cf infra). Reduction of the matrix length is necessary only in limited cases: to obtain a transverse elliptical biopsy
Matricectomy
Nail matrix Proximal nail fold
Lateral nail fold
Cuticle
Hyponychium
A
Nail plate Nail bed
Lunula
B
3784
specimen, to treat tumors that are 3 mm wide or larger, and to thin thick nails in patients with dystrophic congenital and/or hereditary disorders.
NAIL MATRIX TUMORS
NAIL MATRIX TUMORS
If the tumor is located within the lateral third of either portion of the nail, especially when it is close to the lateral margin, the best method is the technique recommended for lateral longitudinal nail biopsy, that is, the removal of the lateral portion of the nail with the defect. If the tumor is located in the middle region, the proximal nail fold is carefully freed from the underlying nail plate, obliquely incised at both sides, and reflected to expose the whole matrix area. For distal matrix tumors, excision is performed as a transverse biopsy except for very superficial epithelial tumors or wide longitudinal melanonychia that can be removed by tangential shave excision. (See Video 205-3 at mhprofessional. com/fitzderm9evideos.) For tumors located underneath the matrix, incision should be done parallel to the anterior border of the lunula. If the tumor is located to the proximal nail matrix and too deep to allow a tangential excision, an alternative approach is the formation of a Schernberg nail bed–matrix flap with an L-shaped incision of the lateral aspect of the finger (Fig. 205-17). A technique slightly modified by E. Haneke.
NAIL ABLATION AND ISOLATED MATRICECTOMY
Nail ablation (Fig. 205-16A) is the definitive removal of the entire nail organ and matricectomy (Fig. 205-16B), the complete extirpation of the nail matrix, which results in permanent nail loss. The principle of nail ablation is the complete removal of the nail unit
Schernberg’s releasing flap technique
with hyponychium, nail bed, matrix, and lateral and proximal nail folds. Except for treatment of malignant tumors of the nail apparatus, nail ablation is rarely indicated. It may be necessary in the case of an excessively painful nail treated several times without success, but this should be an exception. Scalpel excision is strongly advocated whenever the surgical specimen needs histopathologic examination. If periungual pigmentation is associated with longitudinal melanonychia or if the latter is wider than 6 mm or the full thickness of the nail is pigmented, a large portion of the matrix would necessarily be involved. Under these circumstances, the underlying disease process is unlikely to be benign. The entire portion of the involved nail apparatus has to be excised en bloc. The defect from nail ablation (Fig. 205-18B) may be covered with a free graft (split-thickness, full- thickness, reversed dermal graft), which usually takes on the bone in this particular location. A cross-finger flap is an alternative to a free graft. The use of the skin from the intermediate phalanx of a neighboring finger is more convenient for the patient than skin from the thenar area of the palm. If only permanent nail matrix removal is necessary, the procedure is less extensive. In cases in which pathologic examination of the removed tissue is unnecessary, phenol cautery, rather than scalpel excision, is the preferred technique for matricectomy. Most patients return to normal ambulation and activity as early as 1 day after the operation.
Nail ablation
Nail matrix Proximal nail fold
Lunula Lateral nail fold
Cuticle
Hyponychium
Nail plate Nail bed
A
Defect to heal by secondary intention, grafting, or cross-finger flap
B
3
30
NAIL-BED PROCEDURES
NAIL-BED PROCEDURES
Nail-bed surgery is performed for biopsy, removal of tumors, and treatment of subungual hematoma or nail dystrophies such as onychogryphosis. If a larger nail bed fragment is needed, fusiform biopsy with a major longitudinal axis can be performed after partial avulsion of the lateral half of the nail (Fig. 205-14B; see Video 205-4 at mhprofessional.com/fitzderm9evideos) or after total avulsion if the fragment is central. After excision, the nail bed is undermined to facilitate reapproximation of both sides. The suture needle is used generously on these fragile subungual tissues. The wound is stitched with 6-0 resorbable thread. It is sometimes useful to make relaxing incisions at the most lateral margins of the nail bed.
SUBUNGUAL HEMATOMA
In cases of subungual hematoma, acute trauma with severe pain is always remembered by the patient. Depending on the site and intensity of the injury, the hematoma may be visible almost immediately or it may grow out from under the proximal nail fold within a few weeks. When the hematoma is partial (less than 25% of the visible portion of the nail), it should be drained with a pointed scalpel or by hot paperclip cautery over the center of the dark spot (Fig. 205-19). This will produce relief from pain. Sometimes the nail sloughs as the new nail regenerates beneath the old one. Small hematomas may be included in the nail, but they cannot be degraded to hemosiderin, and results of the Prussian blue test will be negative. Therefore, to demonstrate the nature of the blackish pigment, scrapings are boiled in a small test tube with Hemostix, which gives a positive benzidine result. A hematoma involving more than 25% of the visible portion of the nail is a sign of significant nail bed injury. A radiograph is mandatory, because the phalanx may be fractured. The nail plate
Treatment of partial hematoma
3785
30
is carefully removed and the hematoma evacuated. Traumatic nail bed laceration or wounds need a surgical approach to avoid delayed complications. Nail bed lacerations can be sutured after thorough cleaning with antiseptics, using 6-0 resorbable monofilament material. The avulsed nail plate should be put back to cover the wound and then kept in place by suturing to the lateral nail folds or the fingertip. Nail bed defects larger than 4 mm can be repaired using a split- thickness graft taken either from the nail bed of the same digit or from the nail bed of a great toe. The torn nail bed should be sutured with 6-0 resorbable thread, and large bites of tissue should be taken so that the suture material does not pull through when it is tied. The nail plate is cleaned, shortened, and slightly narrowed, and then replaced with sutures into the lateral nail folds. The stitches are left in for 2 weeks. Chronic hematomas are usually painless and are caused mainly by repeated microtrauma from either ill-fitting footwear or sporting activities. A notch is made with a scalpel blade at the distal and proximal border of the pigmented spot. Observation over a 3-week period will demonstrate whether the nail grows independently of the pigmentation or with it. However, chronic hematoma may resemble subungual melanoma and pose a distressing problem, and nonmigrating hematoma should be ruled out.
PROXIMAL NAIL FOLD PROCEDURES
PROXIMAL NAIL FOLD
PROCEDURES
RECALCITRANT CHRONIC PARONYCHIA
Presence of a foreign body (eg, hair) under the proximal nail fold is the main cause of recalcitrant chronic paronychia. The disorder manifests as a red swelling that is painless except when pressed, with secondary retraction of the paronychial tissue whose cuticle has disappeared and with recurrent episodes of acute paronychial inflammation. For crescentic excision, a Freer septum elevator is inserted under the proximal nail fold to protect the matrix and extensor tendon. A No. 15 Bard-Parker blade is used to excise, en bloc, a crescent-shaped full-thickness skin segment, 4 mm at its greatest width that extends from one lateral nail fold to the other. Use of a beveled incision prevents accidental damage to the proximal nail matrix and the most proximal portion of the proximal nail fold, which is responsible for the normal shine of the nail plate (Fig. 205-20). In patients who experience repeated acute flares associated with chronic paronychia, additional removal of the base of the nail is useful. The drawback of this technique is that the PNF is usually slightly retracted giving rise to a longer nail. This can be avoided by reclining the PNF in order to remove the fibrous under surface and suture it back to its original position.9
3786
Crescentic excision of the proximal nail fold
3-4 mm
TUMORS OF THE PROXIMAL NAIL FOLD
Different techniques can be used to treat tumors of the proximal nail fold, depending on the nature of the tumor, its location, and the length of its long axis. Crescentic excision is useful for small distal tumors. The crescent should not exceed 4 mm at its greatest width. Tumors of the proximal nail fold that are situated in a median position and have a longitudinal axis longer than 4 to 5 mm can be excised with a wedge of proximal nail fold whose base is located at the free margin and whose apex points proximally (Fig. 205-21A). Two relaxing lateral incisions are then made in the proximal nail fold to allow suturing of the wedge-shaped defect after the undersurface of the proximal nail fold has been released from the nail plate (Fig. 205-21B). The resulting symmetric narrow defects on both sides heal rapidly by secondary intention. A small tumor on the lateral part of the proximal nail fold may be treated using a wedge-shaped excision
Tumor removal from proximal nail fold
A B
A B C
(Fig. 205-22). Only one lateral relaxing incision is made at the opposite region of the proximal nail fold. To obtain better healing of the secondary defect, which is wider than in the procedure using 2 relaxing incisions, the surgery may be supplemented by making a relaxing crescent-shaped incision in the proximal nail fold. A dorsal flap can be raised from the proximal nail fold by using 2 dorsolateral incisions and a horizontal one proximal to the cuticle. This gives complete exposure of subcutaneous tumors.
RECONSTRUCTION OF THE PROXIMAL NAIL FOLD
Reconstruction of the proximal nail fold may be necessary after any injury (accident, burn, avulsion caused by rapidly rotating belts and sanders, etc.). If the irregular tissue is excised, it is sometimes possible to recreate the distal curve of the proximal nail fold, which may produce a nearly perfect restoration. The proximal nail fold also may be restored by using 2 long, narrow, V-shaped transposition flaps from the lateral aspects of the terminal phalanx.
LATERAL NAIL FOLD PROCEDURES
LATERAL NAIL FOLD
PROCEDURES
A 2- to 4-mm punch can remove a tumor of the lateral nail fold (Fig. 205-23). Benign tumors may be removed by taking an elliptical wedge of tissue from the lateral nail fold and lateral nail wall. Malignant tumors, such as in Bowen disease, are treated by excision of the whole lateral nail fold or by Mohs micrographic surgery followed by healing by second intention.
INGROWN NAIL
Ingrown nail is a condition that occurs mainly in the great toe. It is created by impingement of the nail plate into the dermal tissue distally or into the distolateral
3
30
Biopsy techniques involving the lateral nail fold
Punch biopsy
Eliptical biopsy Shave biopsy
nail groove. Irrespective of the initial cause, the condition finally presents with a nail bed that is too narrow for its nail plate. Logical treatment is therefore aimed at correcting this disparity.
DISTAL TOENAIL EMBEDDING
DISTAL TOENAIL
EMBEDDING
Surgical avulsion or the loss of the toenail from trauma, such as tennis toe, may initiate the pathology. The distal subungual tissues released from the physiologic counterpressure of the nail plate become hypertrophic, and the newly formed nail plate abuts this distal wall. To treat the condition, a crescentic wedge-shaped excision is made around the distal phalanx (Fig. 205-24). The wedge should be 4 mm at its greatest width and must be dissected from the bone. The defect is closed with 5-0 monofilament sutures, which should be removed after 12 to 14 days.
Surgical treatment for distal nail bedding
3787
30
RETRONYCHIA
RETRONYCHIA
Retronychia represents proximal regrowth of the nail that occurs when the nail embeds backwards into the proximal nail fold. This condition involves usually big toenails but also, rarely, fingernails. There is a thickening of the proximal portion of the yellowish nail plate as well as a painful paronychia. There is an embedding of the nail into the proximal nail groove following an acute insulte of fingers or toes. There is a characteristic triade: disruption of the linear nail growth, subacute paronychia, with lifting at the rear of the nail due a double or triple-layered proximal nail plate associated with frequent xanthonychia. A longitudinal overcurvature may be seen. Proximal granulation tissue, inflammatory subungual exsudate and onycholysis are often observed. Ultrasound shows the pathognomonic sign: the shortening of the distance between the proximal edge of the nail and the distal interphalangial joint. Surgical treatment consists of avulsing the nail showing superimposed layers of keratin (Fig. 205-25).10,11
JUVENILE (SUBCUTANEOUS) INGROWN NAILS
JUVENILE
(SUBCUTANEOUS)
INGROWN NAILS
Juvenile or subcutaneous embedded nail is the most common type of ingrown nail. The nail is usually embedded medially, but both sides are often affected. In an effort to relieve the pain, the patient often tries to cut off the offending corner under the inflamed and swollen soft tissue. The remaining portion gives rise to a nail spicule piercing the epithelium of the lateral nail groove, which produces secondary infection and excessive granulation tissue. Treatment at the early stage must be conservative but demands a high degree of patient compliance. The foot is soaked in warm water with povidone-iodine soap; then, under local anesthesia, the nail spicule is removed and a wisp of cotton wool is placed between
The scheme on retronychia
3788
the nail and the lateral nail groove. It should be moistened repeatedly with a disinfectant. For definitive cure, surgical excision or, better, chemical suppression of the lateral horn of the nail matrix permanently narrows the nail. The lateral fifth of the nail plate is freed with a nail elevator from the proximal nail fold and the subungual tissues. It is then cut longitudinally with an English nail splitter or nail-splitting scissors and extracted using a sturdy hemostat. The lateral matrix horn is cauterized with a freshly made solution of liquefied phenol (88% solution) (Fig. 205-26). Above all, a bloodless field is needed, because blood inactivates phenol. Hemostasis is therefore accomplished with a tourniquet, and the blood is carefully cleaned from the space under the proximal nail fold using sterile gauze. The surrounding skin is protected with petroleum jelly. The phenol is rubbed onto the matrix epithelium for 30 seconds, 3 times with a cotton-tipped swab that is changed each time. Postoperative pain
A
Phenolization of the lateral matrix horn
B
is minimal because phenol has a local anesthetic action and is antiseptic. The matrix epithelium is sloughed off, and oozing is usual for 2 to 6 weeks. Daily warm foot baths with povidone-iodine soap accelerate healing. Besides phenol and 10% sodium hydroxide, 80% trichloracetic acid also has been performed for partial matricectomy. The wound almost always heals within 2 weeks without prolonged exudative discharge. Pain is mild but transient.
PINCER NAIL12
PINCER NAIL
12
Overcurvature of the nails may affect the great toe alone or all the digits. This condition may be so painful that even contact with a bedsheet becomes unbearable. When the condition is mild, the nail brace technique aims at correcting the inward distortion of the nail by maintaining continuous tension on the nail plate. A stainless steel wire brace is fitted to the nail plate. A series of adjustments adapted to the gradual decrease of curvature is made over a period of 6 months and results in a painless correction of the pincer nail. Because the underlying bone pathology remains untreated, however, relapse is usual. Therefore, the definitive cure—the use of phenol cautery on the lateral matrix horns—is undoubtedly the simplest effective treatment modality.
HYPERTROPHY OF THE LATERAL NAIL FOLD
HYPERTROPHY OF THE
LATERAL NAIL FOLD
Hypertrophic lateral nail folds are usually the result of long-standing ingrown nails. Inflammation may range from the subclinical to the severe. For treatment, approximately one-fifth of the nail digging into the lateral nail fold is removed. Then an elliptical wedge of tissue is taken from the lateral nail wall of the toe, down to the bone (Fig. 205-27). Suturing of the defect pulls the lateral nail fold away from the offending lateral nail edge. In severe cases, this procedure may be combined with phenol cautery of the lateral horn of the matrix. In contrast to adult-acquired hypertrophy of the lateral nail fold, congenital lateral hypertrophic lips disappear progressively and spontaneously within 12 months.
CONGENITAL MALALIGNMENT OF THE GREAT TOENAIL13
CONGENITAL
MALALIGNMENT OF THE
GREAT TOENAIL
13
In congenital malalignment of the nail of the great toe, typically the nail is malaligned laterally, with transverse furrows on a thick brownish or greenish nail.
3
30
Surgical treatment of hypertrophy of adult lateral nail fold
A B
In 50% of cases, this condition corrects itself without therapy before the age of 10. If the appearance is extreme, surgery diminishes the risk of permanent dystrophy. Treatment requires rotation of a bulky nail unit flap, including the entire nail, nail bed, and matrix (Fig. 205-28). This demands creation of an external Burow’s triangle. An eccentric crescent-shaped excision is made to undermine the nail unit, with the maximum width located on the internal side of the foot, corresponding to the side to which the nail needs to be redirected. This crescent ends on each side 3 to 4 mm behind the most proximal part of the proximal nail fold. The nail bed and the matrix are then undermined and lifted until the fibers of the extensor tendon are visible on its bony insertion, and the dorsal expansion of the lateral ligament of the distal interphalangeal joint is cut. Suturing the edges of the excised triangle together reduces the loss of cutaneous substance. The nail unit
Surgical treatment of congenital malalignment of the nail of the great toe
A B
3789
30
is rotated inwardly, because the maximum cutaneous resection is mostly distal and medial.
NONINVASIVE TREATMENT FOR INGROWN NAILS
NONINVASIVE TREATMENT
FOR INGROWN NAILS
Anchor taping, acrylic affixed gutter splint sculptered nail and others have obtained good results for treating ingrown nails, especially in children. Most ingrown nail cases are noninvasively cured by the combination of anchor-taping and acrylic affix gutter splint methods and do not require invasive surgery.14
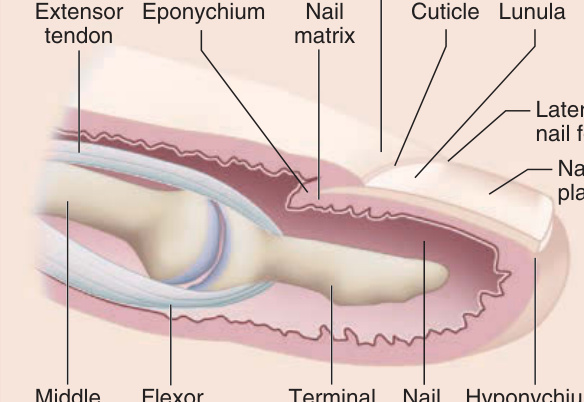
Figure 205-1 Sagittal section of the nail unit.
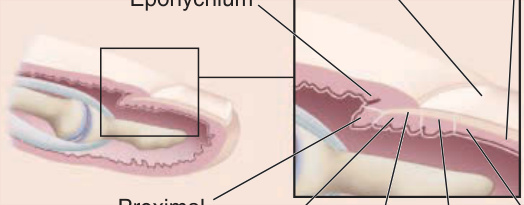
Figure 205-2 Origin of the nail layers. (Used with permission from P. Kechijian, MD.)
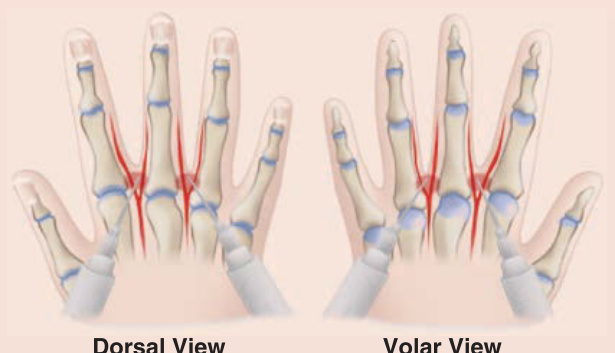
Figure 205-3 Proximal digital block.

Figure 205-4 Distal digital block.

Figure 205-5 Median distal block.

Figure 205-6 Exsanguinating tourniquet.
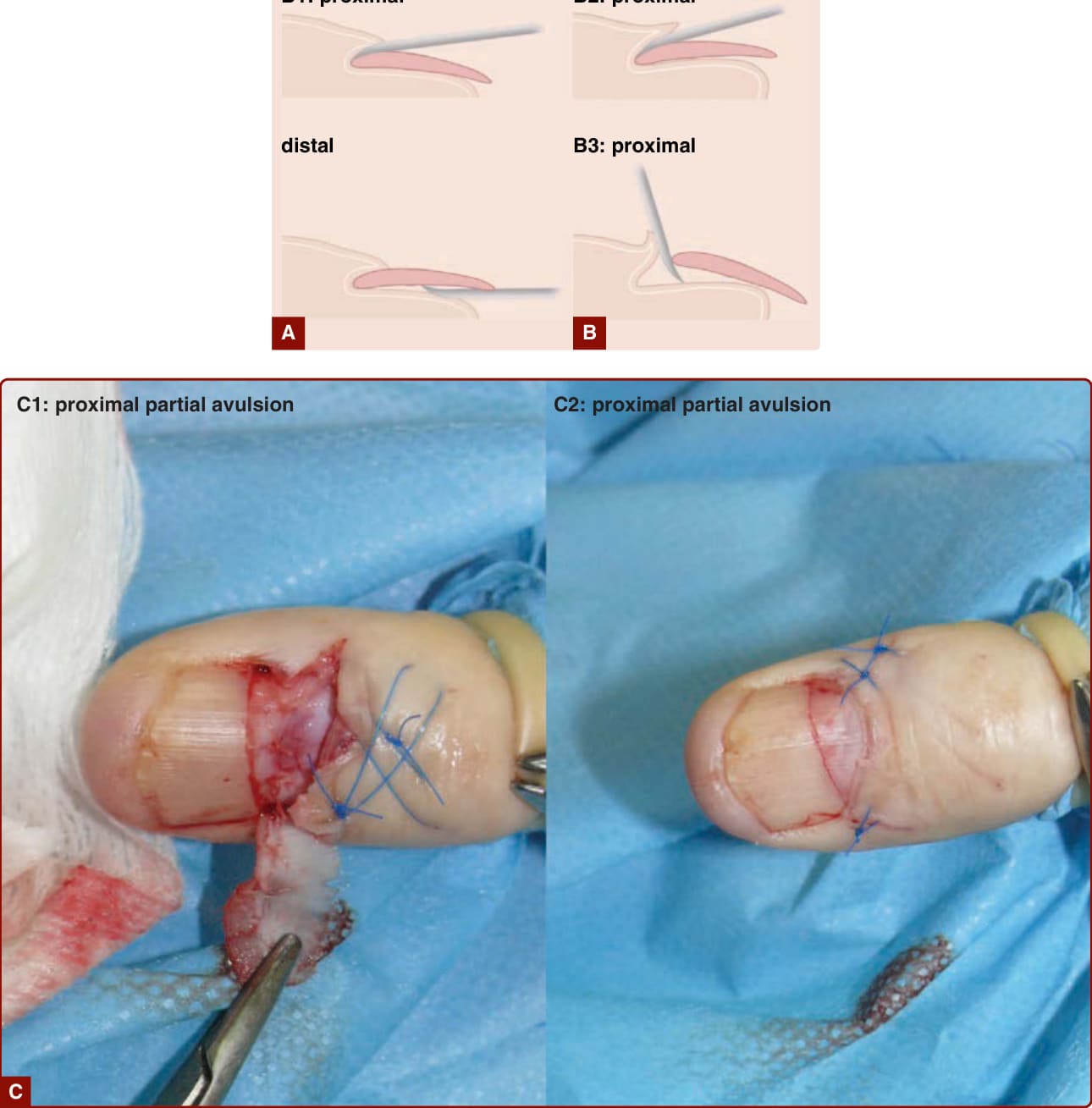
Figure 205-7 A, Distal nail avulsion. B, Proximal nail avulsion. C, Partial avulsions.
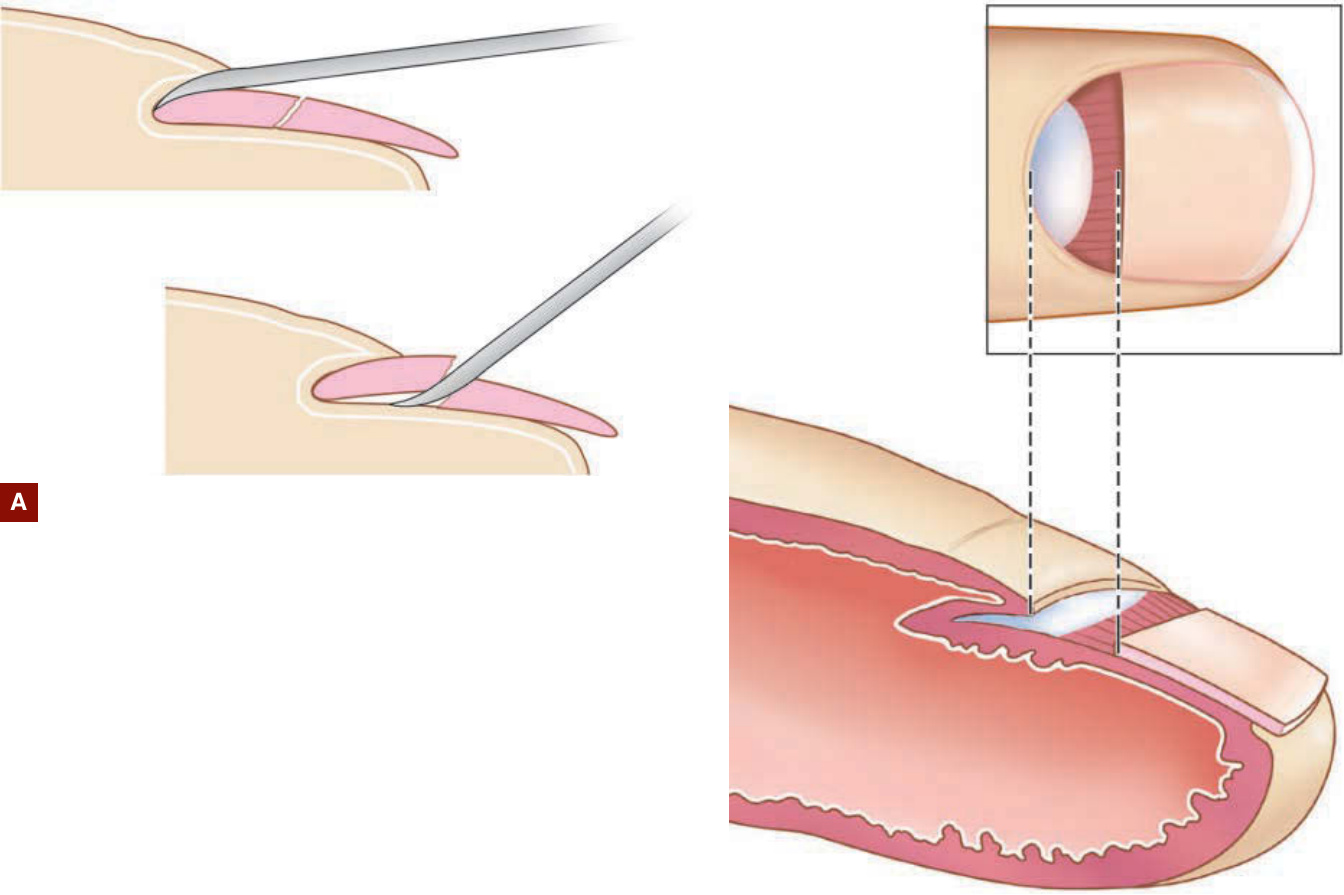
Figure 205-8 A and B, Technique of removal of the base of the nail plate.

Figure 205-9 Lateral longitudinal biopsy of longitudinal melanonychia located within the lateral third of the nail plate.
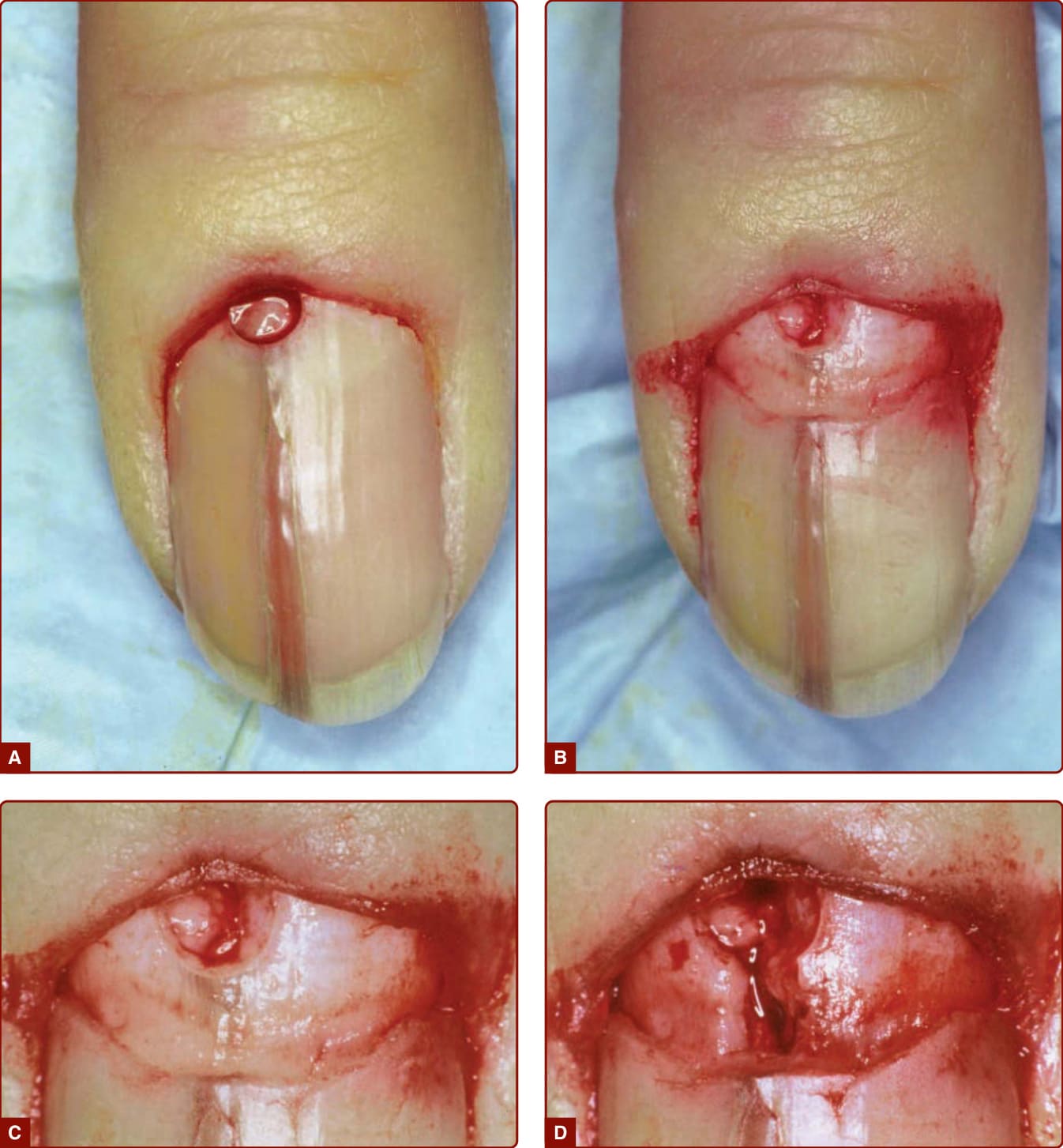
Figure 205-10 A, Punch biopsy of longitudinal melanonychia of width less than 3 mm. B–D, Removal of the base of the nail plate (B) to allow easy removal of the biopsied cylinder of matrix tissue (C), and pigment left distally (D).
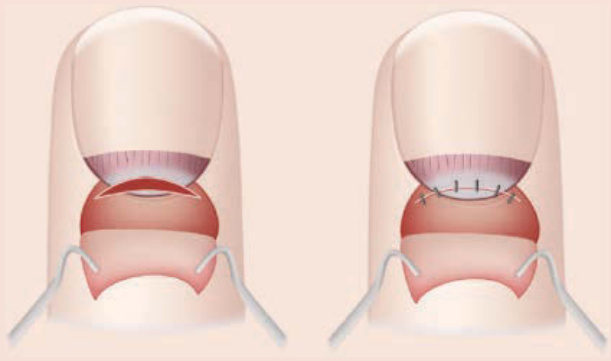
Figure 205-11 Transverse biopsy of the nail matrix.

Figure 205-12 Haneke’s releasing flap technique for longitudinal melanonychia within the midportion of the nail plate.
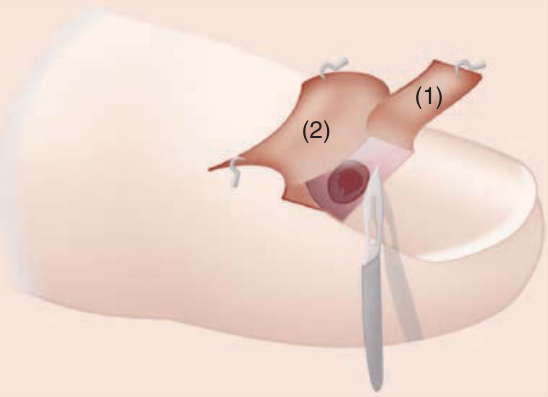
Figure 205-13 Reflected proximal nail fold and removal of the proximal portion of the nail plate exposing the pigmented lesion. Around the latter is made an incision followed by its tangential removal Haneke’s matrix tangential biopsy technique.
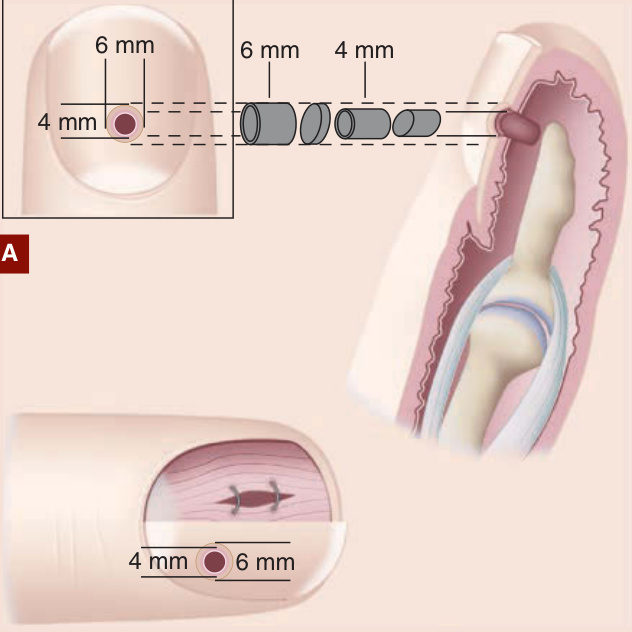
Figure 205-14 Nail bed biopsy. A, Punch biopsy. B, Fusiform biopsy.
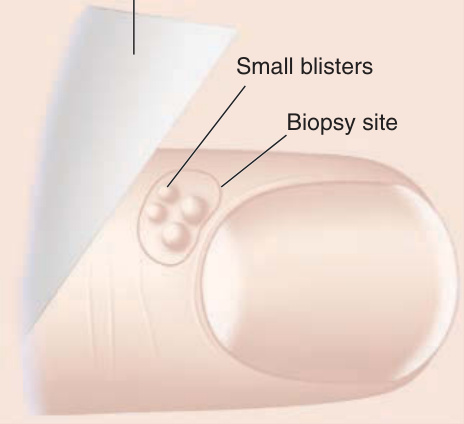
Figure 205-15 Proximal nail-fold shave biopsy.
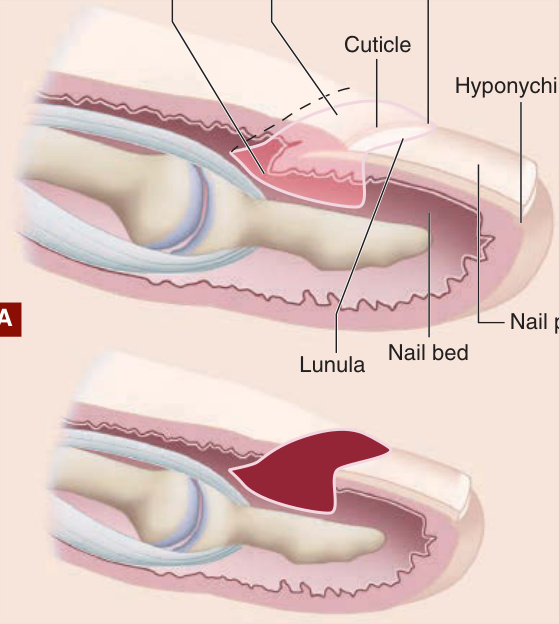
Figure 205-16 Matricectomy. A, Area of excision. B, Remaining defect.
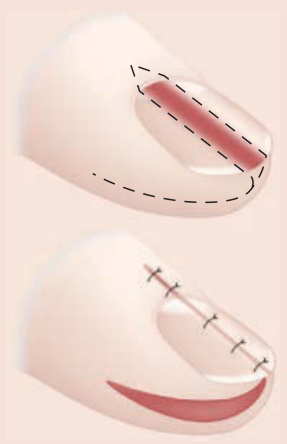
Figure 205-17 Schernberg’s releasing flap method.
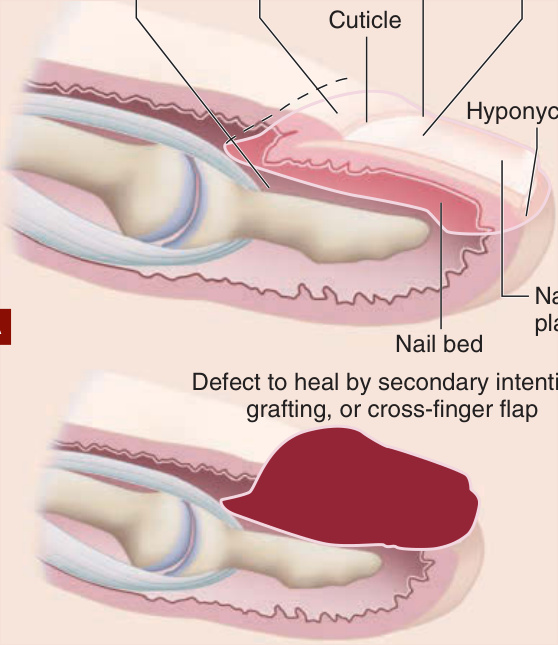
Figure 205-18 Nail ablation. A, Area of excision. B, Remaining defect.
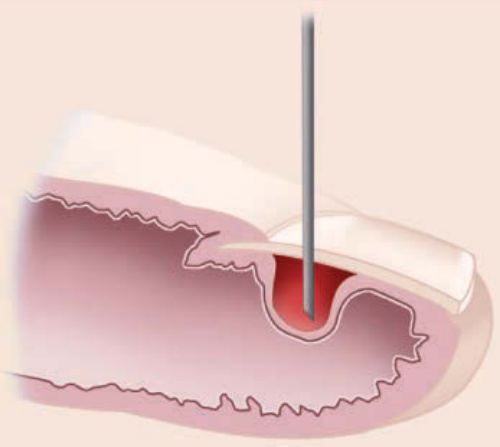
Figure 205-19 Treatment of partial hematoma.
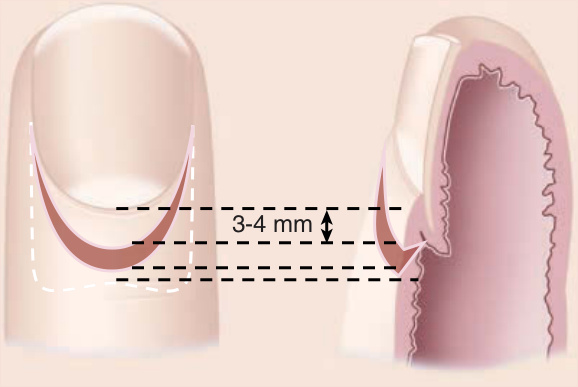
Figure 205-20 Crescentic excision of the proximal nail fold.

Figure 205-21 A, Tumor of the proximal nail fold situated in a median position. B, Suturing of the defect after relaxing lateral incisions are made and the proximal nail fold has been released from the nail plate.
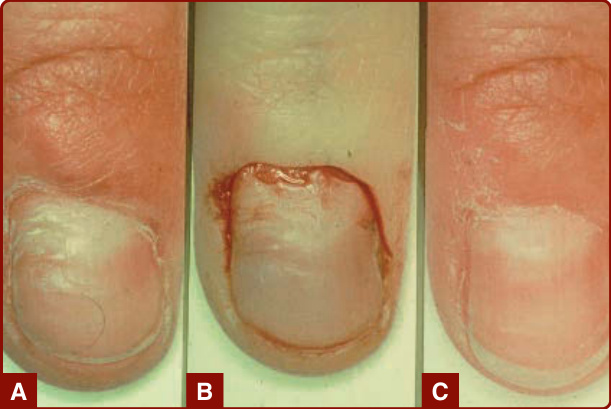
Figure 205-22 A, Irregular shape of the distal border of the proximal nail fold. B, Crescenting wedge-shaped excision of the proximal nailfold. C, Two months after healing.
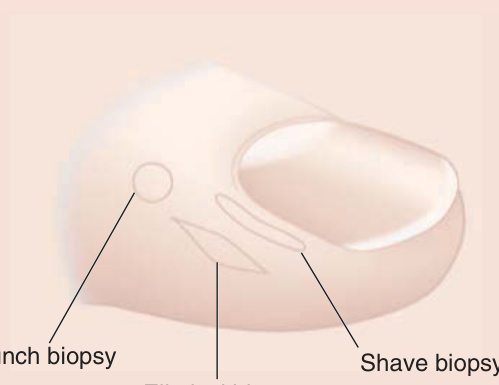
Figure 205-23 Biopsy techniques involving the lateral nail fold.

Figure 205-24 Surgical treatment for distal nail embedding.
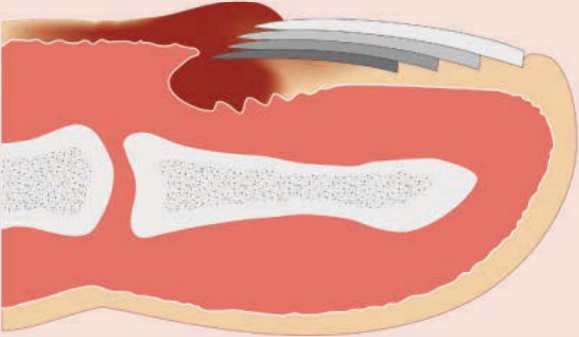
Figure 205-25 The scheme on retronychia.

Figure 205-26 A, Juvenile ingrown nail with excessive granulation tissue. B, Phenolization of the lateral matrix horn.
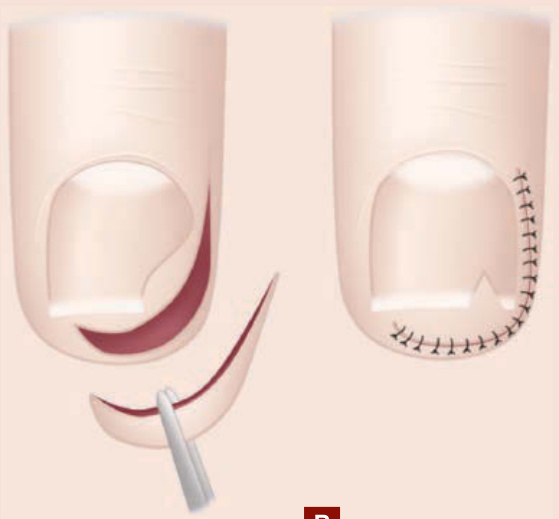
Figure 205-27 Surgical treatment of hypertrophy of adult lateral nail fold.
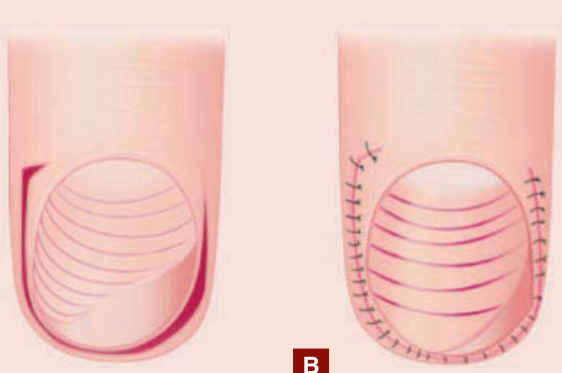
Figure 205-28 Surgical treatment of congenital malalignment of the nail of the great toe.
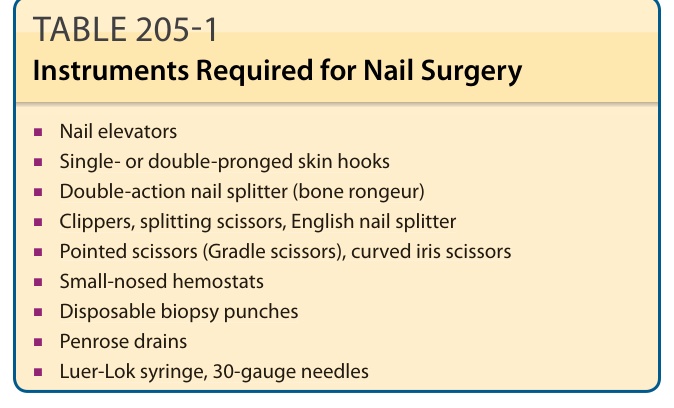
TABLE 205-1 Instruments Required for Nail Surgery