Mohs Micrographic Surgery
3
30
AT-A-GLANCE
■ Mohs micrographic surgery is a specialized form of skin cancer excision in which one physician functions as surgeon and pathologist, verifying surgical margins intraoperatively in successive stages.
■ Mohs surgery achieves the highest cure rate and is the treatment of choice for basal cell and squamous cell carcinoma with high risk of recurrence or progression and for tumors in anatomic areas where tissue sparing is critical.
■ Mohs surgery may also be used for treatment of melanoma in situ and other skin cancers in which pathologic margins can be verified on frozen sections.
■ Mohs surgery optimizes functional and cosmetic outcomes after skin cancer removal, has a low rate of postoperative complications, and is highly costeffective for appropriately selected tumors.
INTRODUCTION AND BACKGROUND
Complete surgical removal is the cornerstone of therapy for solid tumors. This is particularly true for nonmelanoma skin cancers, which have a low risk of metastasis. Complete surgical removal may be difficult to achieve, however, for skin cancers with extensive subclinical spread and for lesions adjacent to vital structures such as the eye. Staged excision or intraoperative pathologic examination of margin status have been used to help ensure adequate surgical margins, but these techniques are limited by logistical hurdles in coordination and communication between the surgeon and pathologist, the inability to precisely map areas of positive margins in three dimensional space, and the inherent limitation of standard pathologic specimen processing, which only examines a small, noncontiguous fraction of the surgical margin. In the 1930s and 1940s, Dr. Frederic Mohs developed a novel method of skin cancer excision using zinc chloride paste to chemically fix the tissue in situ on the patient followed by staged excision with rapid pathologic examination of the surgical margins by the operating physician.1 The procedure was originally named chemosurgery because of the use of a chemical fixative (chemotherapy was not used). In his seminal report, Dr. Mohs reported an overall cure rate of 93% in 425 cases of nonmelanoma skin cancer, many of which were advanced lesions not amenable to standard surgical excision.
In the 1970s and 1980s, the use of chemical fixative was gradually replaced with frozen section analysis of unfixed (fresh) tissue, which allowed the procedure to be completed in hours rather than days. Application of the technique grew rapidly in subsequent years, as the superiority of the procedure over other forms of treatment was established in the peer-reviewed medical literature. Today, the technique known as Mohs micrographic surgery (MMS) is used for treatment of approximately one in five skin cancers in the United States.2
It is the standard of care for basal cell carcinoma (BCC) and squamous cell carcinoma (SCC) with a high risk of recurrence or in sensitive anatomic locations or where clinical margins are difficult to ascertain. It is routinely indicated for treatment of other cutaneous malignancy as well. The inherent advantages of complete microscopic surgical margin analysis and precise tumor mapping allow for the highest possible cure rate while maximizing tissue preservation and optimizing cosmetic and functional outcomes. Additionally, because MMS is an office-based procedure, the high cost of hospital-based or ambulatory surgery center treatment is avoided, and patient satisfaction is enhanced.
OPERATIVE TECHNIQUE
The fundamental advantage of MMS is the microscopic analysis of the complete surgical margin, which cannot be accomplished with standard excision and pathologic processing. The thoroughness of the Mohs method is facilitated by the use of tangential, or beveled, excision. With standard excision, the skin is incised with the scalpel blade held perpendicular to the skin, creating a right angle between the peripheral and deep margin (Fig. 204-1A). Although this facilitates optimal wound closure, it prevents histopathologic analysis of the deep and peripheral margins in the same plane. In contrast, with the Mohs technique, incision of the skin is made at a 45-degree angle, creating a beveled, or sloping, surface to the excised specimen (Fig. 204-1B). After tissue is excised with a beveled edge, it is processed for histopathologic analysis with en face sections that are cut parallel to the surgical margin. This is another critical difference from standard excision, in which the excised specimen is most often sectioned perpendicular to the surgical margins in a “bread-loaf” fashion. Perpendicular sections allow for histopathologic examination of the central bulk of the tumor but cannot practically examine the entire surgical margin because each section only visualizes a few micrometers of margin length. Thousands of sections would be required to examine a few centimeters of surgical margin in its entirety, and thus representative sections are often examined at intervals of 1 to 2 mm. This results
30
Comparison of standard versus beveled excision
Peripheral margin
A
Continuous peripheral and deep margin
B
Standard excision
Deep margin
Beveled excision
in examination of less than 1% to 3% of the length of the surgical margin. For many skin cancers with irregular subclinical extension, areas of malignancy may be missed on representative sections, resulting in false-negative margins and potential tumor recurrence (Fig. 204-2A). Beveled excision coupled with en face sections in Mohs surgery examines the entire deep and peripheral surgical margin in a single plane, permitting detection of focal areas of tumor extension as small as a few malignant cells (Fig. 204-2B). This difference is clinically relevant because perpendicular sections at intervals of 1 mm may miss up to 42% of irregular tumor extensions.3
MMS, like every surgical procedure, begins with a consultation between the surgeon and the patient. This allows the surgeon to confirm the pathologic diagnosis of skin cancer before surgery, examine the patient to evaluate tumor location and size, and assess for signs or symptoms of extensive subclinical extension such as paresthesia or motor nerve dysfunction. If there is uncertainty about the pathologic diagnosis (eg, from an inconclusive biopsy) or if malignant invasion of critical
3762
deep structures is suspected, further evaluation may be warranted before surgery. The patient must also be informed of the likely extent of the cancer, the implications for function and cosmesis, expectations for wound healing, and other associated risks and benefits of the procedure. After informed consent has been documented, the procedure can be scheduled or initiated. Mohs surgery is almost universally performed as an office-based procedure under local anesthesia. Facility requirements include treatment rooms equipped to ensure patient comfort, optimal tissue excision, hemostasis, and reconstruction. The on-site histology laboratory for processing, sectioning, and staining the surgical specimens is a fundamental requirement of the Mohs technique. In addition to the surgeon, who also functions as the pathologist in reading intraoperative histopathology specimens, the procedure requires trained nursing staff and a histotechnician experienced in processing frozen sections. Because the procedure relies on accurate interpretation of histopathologic margin status, optimal histologic processing with robust quality control is essential.
3
30
Comparison of standard versus Mohs margin analysis
Perpendicular (bread-loaf) representative sections
A
False-negative surgical margins
Mohs sections complete margin analysis
B
True positive Mohs surgical margin
The Mohs procedure commences with accurate identification of the lesion to be treated (Fig. 204-3A) and confirmation of the site by the patient using a mirror. Photographic records from the time of the diagnostic biopsy may be extremely helpful in cases of patient uncertainty or when wound healing and the passage of time have obscured the precise location of the lesion. The patient is then positioned on the surgical table and the site is infiltrated with local anesthetic. The grossly visible tumor is debulked by curettage or blade if appropriate. The tendency of the semi-sharp curette to dislodge friable tumor aggregates while sparing normal skin helps to define the deep and lateral extent of the tumor. The skin lesion is then excised with a 1- to 2-mm margin around the curettage area, taking care to excise the tissue with a beveled edge at a level deep enough to ensure an adequate margin
below the initial curettage (Fig. 204-3B). This may be at the intradermal, subcutaneous, muscular, or fascial layer, depending on the nature of the cancer and the anatomic site. Before removing the lesion, one or more score marks may be placed across the specimen and onto the surrounding skin to serve as anatomic markers for subsequent stages. Hemostasis is then obtained, a temporary bandage is placed over the wound, and the ambulatory patient waits in a comfortable waiting room while the specimens are processed for histopathologic examination. The excised tissue from the first stage is transported by hand to the adjacent histology laboratory. The tissue is divided into appropriately sized specimens using the score marks made at the time of excision. The anatomic orientation relative to surrounding landmarks on the patient is preserved, each piece is marked with at
3763
30
B A C
D E F
least two colors of indelible ink (to designate laterality or sidedness), and a “map” is drawn to represent the specimen and precisely locate any areas of positive margins (Fig. 204-3C). The tissue is frozen, mounted, and sectioned by the technician with en face sections such that the peripheral and deep margin are visualized on the histopathologic slides (Fig. 204-3D). The slides are then stained, often with standard hematoxylin and eosin stains. Inspection of the slides prepared in this fashion reveals the true surgical margin, and any areas of carcinoma that are noted represent tumor extension to the margin. If present, these areas of persistent malignancy in stage 1 are marked in their precise location on the map in relation to the inked edges (Fig. 204-3E). If carcinoma is detected at the microscopically examined surgical margins, the patient is returned to the procedure room for ongoing staged excision. The fact that the Mohs surgeon functions as the pathologist in
3764
detecting and mapping any areas of positive surgical margins ensures the most focused and precise reexcision when subsequent stages are necessary. These subsequent stages are generally incised with a beveled edge to facilitate complete margin examination and may involve excision of epidermis and dermis from the peripheral margin; subcutis, muscle, fascia, or cartilage from the deep margin; or a combination of these depending on the location and extent of residual tumor (Fig. 204-3F). Subsequent stages are inked, mapped, processed, sectioned, and stained as described earlier, and the surgical margin is again examined microscopically by the surgeon. This iterative process continues until the surgical margins are free of carcinoma and a tumor-free plane has been achieved. When all surgical margins are clear, the patient is evaluated for consideration of immediate surgical repair or healing of the defect by second intent.
The staged nature of Mohs surgery allows optimal flexibility in surgical treatment. Because no a priori assumptions are made about required surgical margins, small lesions can be treated with a minimal surgical defect, and highly invasive lesions, even if not grossly evident, can be completely excised over multiple stages. In general, each stage takes 20 to 45 minutes to process in our laboratory; about half of patients achieve clear margins after a single stage, and approximately 90% are clear after two stages.4 Skin cancers requiring four to six stages are uncommon. It is important to note that the Mohs technique does not examine the central portion of an excised tumor. In selected cases when additional information about histopathologic risk factors such as perineural invasion or poor differentiation is required, the frozen tissue can be thawed and submitted for standard perpendicular section processing through the bulk of the tumor. For the majority of BCCs and SCCs treated with Mohs surgery, this additional pathologic examination is not necessary.
INDICATIONS FOR MOHS SURGERY
BASAL CELL CARCINOMA
BASAL CELL CARCINOMA
BCC is the most common human malignancy, with more than 2 million cases per year in the United States.5
Although BCC rarely leads to metastasis or death, it
A
3
30
can be highly destructive and result in significant morbidity and functional impairment. Given the disproportionate incidence of BCC on anatomically sensitive sites such as the nose, ears, and periocular skin, Mohs surgery has been performed for BCC more than any other skin cancer. Mohs surgery is particularly beneficial for facial BCC because of the tendency of this malignancy to exhibit subclinical extension (Fig. 204-4). Several risk factors have been identified to predict microscopic tumor extension beyond the grossly visible margin of the tumor, including poorly defined clinical margins; diameter greater than 2 cm; and location on the high-risk, or “H” zone of the face, encompassing the nose, eyelids, eyebrows, temples, lips, ear, and periauricular skin.6-8 Histologic subtype of BCC is also a critical determinant of subclinical extension. Although most nodular BCC are completely excised with surgical margins of 4 mm, infiltrative and micronodular subtypes, when excised with the Mohs technique, were found to require surgical margins of 5 to 10 mm for complete clearance and were more likely to require excision of underlying muscle, cartilage, and periosteum.9,10
As it became clear that Mohs surgery could offer superior treatment outcomes for high-risk BCC, systematic studies of the procedure focused on this subgroup of tumors. Dr. Mohs himself published the largest series of cases of BCC of the eyelids: among 1124 primary BCC and 290 recurrent BCC with 5-year follow-up, the cure rates after Mohs surgery were an exceptional 99.4% and 92.4%, respectively.11
B
3765
30
Subsequent studies in thousands of patients have confirmed a long-term recurrence rate of 1% to 4% after Mohs surgery for primary BCC with high-risk features and a higher recurrence rate of 4% to 8% for recurrent BCC, which are likely to have greater subclinical invasion that could be masked by scarring from prior treatment.12,13
The durable cure rates obtained with Mohs surgery are superior to those obtained with standard excision as documented in several retrospective studies and one randomized clinical trial (Table 204-1). A pair of meta-analyses of published data on over ten thousand patients reported that Mohs surgery results in a recurrence rate that is three- to fourfold lower than standard excision,14,15 and a more recent observational study confirmed that although standard excision provides a high rate of cure for cancers on low-risk anatomic locations, Mohs surgery affords at least as high of a cure rate when selectively used on tumors with high-risk features.16 Yet interpretation of these studies is hampered by their retrospective nature and lack of appropriate controls. More recently, 10-year follow up data from a prospective, randomized trial has now provided high-level evidence that Mohs surgery is superior to standard excision for BCC at high risk of recurrence.17
Both primary and recurrent BCC with high-risk features (>1-cm diameter and location on the H zone or with an infiltrative or micronodular histologic pattern) were found to have a more than twofold reduction in recurrence rate after Mohs surgery, although statistical significance was only reached for recurrent BCC. In contrast, small, primary BCC without aggressive histologic features on low-risk anatomic locations such as the trunk are unlikely to have significant benefit from the Mohs technique compared with other forms of surgical treatment.
SQUAMOUS CELL CARCINOMA
SQUAMOUS CELL
CARCINOMA
SCC is the second most common human malignancy, although recent evidence suggests that SCC incidence is increasing and may be approaching that of BCC.5 Like BCC, SCC is effectively treated with Mohs surgery, facilitating identification and complete excision of irregular branches of subclinical tumor extension. Also like BCC, the differential efficacy of Mohs surgery over standard excision is most pronounced for tumors in the H zone of the face, and for tumors greater than 2 cm in diameter or with aggressive histologic features.18 These tumors, as well as those recurring after previous treatment, exhibit an increased propensity for subclinical extension and an increased risk of incomplete excision in the absence of the complete margin assessment of Mohs surgery.19 Particularly on the chronically sun-exposed scalp, SCC may exhibit an infiltrative histology with broad involvement of the fascia and periosteum that is not evident on examination of the skin surface (Fig. 204-5). Overall, the reported rates of recurrence of primary cutaneous SCC are up to 8.1% after standard excision and 3.1% after Mohs surgery.20 The risk of recurrence for previously treated SCC is increased to 23.3% after standard excision and 10.0% after Mohs surgery. Unlike BCC, SCC has a significant risk of regional and distant metastasis, particularly for certain subsets of SCC. Treatment is therefore focused not only on preventing local recurrence but on complete tumor extirpation to prevent metastasis. Four factors that appear most strongly associated with adverse outcomes in SCC are diameter greater than 2 cm, depth of invasion below the subcutaneous adipose, perineural invasion, and
REFERENCE TYPE OF STUDY BCC (n) FOLLOW-UP PERIOD (yr) LOCATION
Primary Basal Cell Carcinoma
RECURRENCE AFTER STANDARD EXCISION (%)
RECURRENCE AFTER MOHS SURGERY (%) P VALUE
van Loo et al17 (2014) Prospective randomized trial 397 10 Facial, high risk 12.2 4.4 0.1
Chren et al16 (2013) Retrospective observational 1127 5 Anya 3.5 2.1 > 0.1
Rowe et al14 (1989a) Meta-analysis 10,276 5 Anyb 10.1 1.0 Not reported
Recurrent Basal Cell Carcinoma
van Loo et al17 (2014) Prospective randomized trial 202 10 Facial, high risk 13.5 3.9 0.023
Rowe et al15 (1989b) Meta-analysis 3531 5 Anyc 17.4 5.6 NR
Rowe et al15
Meta-analysis 3531 5 Anyc 17.4 5.6 NR
(1989b)
aA total of 26% of excisions and 65% of Mohs were in high-risk anatomic sites (nose, eyelids, eyebrows, lips, temple, and ears and periauricular skin); 27% of all lesions were squamous cell carcinoma (SCC), not basal cell carcinoma (BCC).
3766
bData were derived from 12 separate reports; location was not reported (NR).
cData were derived from 9 separate reports; location was not reported.
A
3
30
B
poor histologic differentiation. In a large retrospective review, the presence of one of these factors increased local recurrence from 0.6% (no risk factors) to 5% (one risk factor) and 21% (two or three risk factors), and increased nodal metastasis from 0.1% (no risk factors) to 3% (one risk factor) and 21% (two or three risk factors).21 Importantly, effective local control with Mohs surgery may decrease the risk of subsequent metastasis because SCC with perineural invasion was found to metastasize in 47% of cases after standard excision compared with 8.3% of cases after Mohs surgery.20 Even with complete verification of the histopathologic margin status, however, SCC with perineural invasion or poor differentiation still presents a significant risk of local or regional recurrence. Adjuvant therapy such as radiation may be considered after Mohs surgery to decrease this risk, although high-quality evidence to support the benefit of this approach is lacking. Other risk factors for adverse outcomes of SCC that may benefit from Mohs surgery include host immunosuppression and location on the lip, ear, and temple. SCC arising on penile skin has also been reported to have a high rate of local and regional recurrence, and Mohs surgery is an effective treatment for penile SCC as well.22
SCC in situ can also be effectively treated with Mohs surgery. The reported cure rate for SCC in situ after Mohs surgery is 93.7%, which compares favorably with standard excision.23 Although SCC in situ has been reported to progress to invasive SCC, the risk of progression in
appropriately treated lesions appears to be very low. Moreover, a histopathologic study of depth of invasion of SCC in situ found that in 54 tumors, the maximum depth of invasion was only 0.82 mm.24 Thus, with the exception of high risk lesions such as those within the H zone of the face or lesions with the clinical suggestion of invasive disease, other forms of treatment besides Mohs surgery should be considered for SCC in situ.
MELANOMA
MELANOMA
Dr. Mohs first reported the use of margin-controlled excision for invasive melanoma in 1950 using the chemosurgery approach of in situ tissue fixation with zinc chloride, although this was not widely adopted.25 The transition from in situ fixed tissue to fresh frozen tissue processing for Mohs surgery brought new controversy to the field because it was noted that artifacts introduced on frozen sections complicated the detection of intraepidermal melanocytes and decreased the sensitivity of melanoma detection.26 The more recent development of immunohistochemical stains on frozen sections has brought the potential for more sensitive melanocyte detection and melanoma diagnosis at the microscopic margins but has not resolved the controversy. Currently, Mohs surgery using immunohistochemical stains for melanoma antigen recognized by T cells
3767
30
(MART-1) on rapidly processed frozen sections is the most common technique, although it is only used by a minority of Mohs surgeons, and its use is limited to melanoma in situ and superficially invasive melanoma (Breslow depth <1 mm) with a minimal risk of metastasis. The largest study to date on clinical outcomes with this technique reported a remarkably low 5-year local recurrence rate of less than 1% in more than 2000 melanomas; half of these cases were on the head and neck, 60% were in situ melanoma, and 30% were invasive with a Breslow depth of less than 1 mm.27 Because of concerns about the accuracy of en face frozen sections for melanoma diagnosis and the potential for undetected invasive disease in unexamined tissue from the center of the tumor, other investigators have proposed staged excision with formalin-fixed sections or a combination of perpendicular (bread-loaf) and en face frozen sections during Mohs surgery, both of which can achieve high cure rates of greater than 95%.28,29 Importantly, there has not yet been a direct comparison of Mohs surgery with standard wide excision for superficial melanoma in an appropriately matched cohort of patients, and additional study is required to determine the relative efficacy of these treatments. It is likely that some form of staged excision will provide significant benefit for patients with superficial melanoma on chronically sun-exposed skin because nearly 20% of these tumors will have subclinical extension beyond the recommended 5-mm margin of grossly uninvolved skin.27 Ongoing investigation of the adaptation of the
A
Mohs technique for melanoma treatment illustrates how technologic innovations in tissue processing and staining can be incorporated into surgical treatment, but how these innovations could improve outcomes remains to be determined.
OTHER SKIN CANCERS
OTHER SKIN CANCERS
Dermatofibrosarcoma protuberans (DFSP) is a rare cutaneous malignancy for which Mohs surgery may be particularly effective. DFSP is a slowly progressive tumor that rarely metastasizes but frequently has broad subclinical extension and a historically high recurrence rate after conventional excision. DFSP originates within the dermis or dermal–subcutaneous junction and frequently invades muscle or fascia, requiring accurate assessment of both peripheral and deep surgical margins (Fig. 204-6). The characteristic spindled cells of DFSP can be readily identified on frozen sections, and complete margin assessment with Mohs surgery facilitates identification of the irregular projections of the tumor that may be missed with standard perpendicular section processing. A meta-analysis of published studies on DFSP, none of which were randomized trials, found that whereas local recurrence after conventional excision was approximately 6%, this rate decreased to 1% after Mohs surgery.30 For cases in which Mohs surgery is not practical, staged excision
B
3768
with appropriate pathologic verification of clear margins can also be an effective treatment for DFSP.31
In principle, any solid cancer with contiguous growth (as opposed to discontiguous spread or satellite lesions) that can be identified on frozen histopathologic sections and is accessible from the external surface of the body can be treated with Mohs surgery. Mohs surgery is likely to provide the most therapeutic benefit for tumors with broad and unpredictable subclinical extension, such as microcystic adnexal carcinoma,32 or tumors arising in anatomic locations for which tissue sparing is critical, such as sebaceous carcinoma of the eyelid or extramammary Paget disease (EMPD) of the genitalia. Although EMPD may be multifocal in some cases, a review of published observational studies found that Mohs surgery may result in a lower recurrence rate than standard excision.33 Atypical fibroxanthoma is an uncommon spindle cell cancer of chronically sun-exposed skin with a behavior similar to high-risk cutaneous SCC that is effectively treated with Mohs surgery. The technique has also been used for treatment of adnexal carcinoma, apocrine and eccrine carcinoma, leiomyosarcoma, Merkel cell carcinoma, mucinous carcinoma, and other rare cutaneous malignancies.34
HEALING AND RECONSTRUCTION
Maximal conservation of normal, noncancerous tissue with Mohs surgery facilitates wound healing after
A
3
30
tumor extirpation. With the use of in situ chemical fixation originally described by Dr. Mohs, immediate primary surgical repair was often not feasible because of the residual effects of the chemical fixative. Thus, nearly all of the 440 cases originally described by Dr. Mohs were allowed to heal by second intent, or granulation without surgical repair.1 The continued use of second intent healing for defects after Mohs surgery, even after the transition to non–chemically fixed tissue, was a significant contribution to the surgical literature and established second intent healing as a viable option for selected wounds. Defects resulting from Mohs surgery may be particularly suited to healing without reconstruction because the procedure often creates wounds of shallow depth that may be conducive to second intent healing. This is in contrast to traditional surgical excision, which is routinely performed to the depth of the subcutaneous adipose or connective tissue. Other wounds with reliable functional and cosmetic results after second intent healing include wounds on thin skin such as the eyelid or ear and wounds on concave surfaces such as the medial canthus, anterior surface of the ear, and the temple (Fig. 204-7). Although Mohs surgical defects on convex surfaces such as the nasal tip, malar cheek, and central forehead can also heal with acceptable functional results, the resulting scars in these areas are more likely to be depressed and cosmetically conspicuous. In appropriately selected patients, healing of Mohs surgical defects by second intent results in patient satisfaction that is equivalent to primary surgical repair.35
B
3769
30
A
B
Pathologic verification of complete tumor extirpation after Mohs surgery also facilitates immediate surgical reconstruction because the Mohs technique provides the lowest possible risk of residual or recurrent cancer. As the use of frozen sections replaced in situ chemical fixation and Mohs surgery became the standard of care for anatomically sensitive areas such as the nose, lips, and eyelids, reconstruction with plastic and aesthetic surgical techniques has become an integral part of the technique. In fact, several advances in cutaneous reconstruction were described and popularized by Mohs surgeons, including the use of the buried vertical mattress suture, the modern bilobe transposition skin flap on the nose, and the use of cartilage grafts and multistaged interpolation flaps as office based-procedures under local anesthesia.36-39 Immediate surgical repair with linear closure, skin grafts, or skin flaps from adjacent or interpolated tissue reservoirs is now used more often than second intent healing for Mohs surgical defects and permits optimal restoration of function and cosmesis in critical areas such as the eyelid and nose (Fig. 204-8).
RISKS AND COMPLICATIONS
Although no surgical procedure is without risk, Mohs surgery is a remarkably safe procedure with low complication rates. A multicenter prospective study of adverse events in 20,821 Mohs surgical procedures identified an overall adverse event rate of 0.72% and a serious adverse event rate of 0.02% (4 cases of 20,821).40 The most common adverse events were infections (0.40% event rate), impaired wound healing including dehiscence and necrosis (0.14% event rate), and postoperative bleeding or hematoma (0.11% event rate). The four serious adverse events in this study were all infections requiring hospitalization, and no deaths or life-threatening cardiovascular complications were reported. Smaller studies have confirmed similarly low rates of
3770
complications (minor bleeding in 1.2% and infection in 0.9%) and reported mild postoperative pain scores (mean of 1.99 on a 0–10 scale of pain).41 The use of local anesthetic rather than general anesthesia or conscious sedation, as well as the lack of significant volume shift or cardiovascular stress after cutaneous surgery likely contribute to the safety of the Mohs procedure. The documented safety of office-based Mohs surgery allows the procedure to be performed with minimal risk on a wide range of patients, including octa- and nonagenarians and patients with comorbid conditions including stable cardiac disease. Nevertheless, preoperative evaluation to determine the relative risks and benefits of the procedure and to identify modifiable risk factors is critical. Patients with relatively indolent skin cancers who have limited life expectancy because of another terminal condition may not sufficiently benefit from the procedure to justify even small risks of complications. Patients on anticoagulant therapy such as aspirin, warfarin, or direct factor Xa inhibitors such as rivaroxaban or apixaban have a modestly increased risk of minor bleeding complications (1.7% vs 0.7% in one study41), but this is not a contraindication to Mohs surgery, and patients are generally advised to continue their prescribed anticoagulation therapy during and after surgery. Antibiotic prophylaxis is generally not required before Mohs surgery, with a few notable exceptions. The American Heart Association and American College of Cardiology recommend prophylactic antibiotic therapy only for patients at highest risk of complications of infective endocarditis, including those with prosthetic heart valves, a prior history of infective endocarditis, cardiac transplant recipients with significant valvular disease, and patients with significant cyanotic congenital heart disease. Even in these high-risk patients, antibiotic prophylaxis is only recommended in cases with breach of the oral mucosa; surgical procedures on intact skin or gastrointestinal and genitourinary procedures are not clear indications for antibiotic prophylaxis.42 Patients with total knee or hip replacements may be at increased risk of hematogenous total joint infection after Mohs surgery, and prophylaxis may be considered for these
patients as well. However, there is no evidence to support the use of antibiotic prophylaxis with routine surgical or dental procedures in these patients, and recent guidelines from the American Academy of Orthopedic Surgeons and the American Dental Association do not provide specific recommendations for prophylaxis after prosthetic joint replacement.43 In general, Mohs surgeons use antibiotic prophylaxis sparingly and only in patients at highest risk for hematogenous or surgical site infections.
COST AND APPROPRIATE USE
Mohs surgery is widely used for treatment of nonmelanoma skin cancers and has been shown to be the most effective method of skin cancer eradication. The increasing use of Mohs surgery, however, has prompted concerns about the cost of this procedure relative to other surgical treatments. Cost analysis based on procedure codes and typical reimbursements indicates that the immediate cost of skin cancer treatment, including tumor removal, pathologic examination, and repair of the surgical defect, is approximately 25% greater for Mohs surgery than for standard surgical excision with permanent pathologic section analysis in the outpatient setting.44 This cost differential is reversed, however, when immediate frozen section margin analysis is performed with non-Mohs surgical excision, raising the cost to nearly double that of Mohs surgery. Moreover, when Mohs surgery is limited to high-risk skin cancers or critical anatomic locations such as the H zone of the face, when the use of second intent healing instead of surgical repair is considered with selected Mohs surgery cases, and when the increased rate of recurrence is accounted for with standard surgical excision, the overall costs of Mohs surgery may be 20% to 30% less than standard excision.45
To ensure that Mohs surgery is reserved for clinical scenarios in which the procedure will be most costefficient and provide the greatest benefit over other forms of treatment, the American Academy of Dermatology, the American College of Mohs Surgery, the American Society for Dermatologic Surgery, and the American Society for Mohs Surgery jointly published appropriate use criteria (AUC) in 2012.34 The appropriate use criteria define tumor-specific and patientspecific factors for which Mohs surgery is deemed to be either appropriate, uncertain, or inappropriate in most situations (Table 204-2). A central factor in the AUC is anatomic location, owing to the critical need for tissue sparing with Mohs surgery in certain locations as well as the increased risk of subclinical extension and recurrence of skin cancers in these areas. Highrisk areas include the H zone of the face (eyelids, eyebrows, nose, lips, chin, ears and periauricular skin, and temples; Fig. 204-9), genitalia, hands, feet, ankles, and nipple and areola region. Medium-risk areas are the remainder of the face (cheeks, forehead, and jawline), scalp, neck, and pretibial surfaces. The trunk and the
3
30
CLINICAL DIAMETER (cm)
DIAGNOSIS RISK AREAb
< 0.5 0.6–1 1.1–2 > 2
Primary nodular BCC High A A A A
Medium A A A A
Low I I U A
Primary aggressive BCCc High A A A A
Medium A A A A
Low U A A A
Primary superficial BCC High A A A A
Medium U A A A
Low I I I I
Recurrent BCC (not superficial) Any A A A A
Recurrent superficial BCC High A A A A
Medium A A A A
Low I I I I
Primary SCC without high-risk featuresd High A A A A
Medium A A A A
Low I I U A
Primary SCC with highrisk featuresd Any A A A A
High A A A A
Primary SCC in immunocompromised patient
Medium A A A A
Low U U A A
Recurrent SCC (invasive) Any A A A A
Primary SCC in situ High A A A A
Primary SCC in situ High A A A A
Medium A A A A
Medium A A A A
Low I I U A
Low I I U A
aThe most common clinical scenarios are presented. Each scenario is scored as appropriate (A) or inappropriate (I) for Mohs surgery or uncertain (U).
bHigh-risk area: central face, eyelids, eyebrows, nose, lips, chin, ears and periauricular skin, temples, genitalia, hands, feet, ankles, and nipple and areola. Medium-risk area: cheeks, forehead, scalp, neck, jawline, and pretibial surface. Low-risk area: trunk and remainder of extremities.
cAggressive basal cell carcinoma (BCC) includes pathologic subtypes of infiltrative, morpheaform or sclerosing, micronodular, and metatypical or keratotic or with perineural invasion.
dHigh risk features for squamous cell carcinoma (SCC) include poor differentiation, perineural or intravascular invasion, spindle cell or infiltrative features, Breslow depth >2 mm, and Clark level IV or greater.
remainder of the extremities are considered low-risk areas. The AUC primarily focuses on specific clinical scenarios for BCC and SCC but also notes that Mohs surgery can be appropriate for melanoma in situ and other, more rare tumors. It is important to note that the AUC does not encompass all clinical scenarios nor does it imply that Mohs surgery is required for all tumors deemed appropriate. Individual clinical judgment must always be used to ensure optimal management of cutaneous malignancy, and the AUC are likely to be modified as further research and clinical experience can refine the recommendations.
3771
30
Anatomic risk areas of the head and neck
CONCLUSIONS
Mohs surgery is a specialized form of skin cancer extirpation that relies on staged excision with immediate histopathologic examination of the entire deep and peripheral surgical margin. Mohs surgery is most often used to treat patients with BCCs and SCCs and has been shown to be superior to other forms of treatment for cancers at increased risk of recurrence. The versatility of the Mohs procedure allows for maximal tissue conservation while ensuring complete tumor removal and facilitates optimal wound healing, whether by immediate surgical reconstruction or by second intent. The procedure is the accepted standard of care for appropriately selected cancers as defined by the AUC. Ongoing investigation and technological advances will continue to refine the indications for Mohs surgery, which may include expanded use for superficial melanoma or other less common tumors.
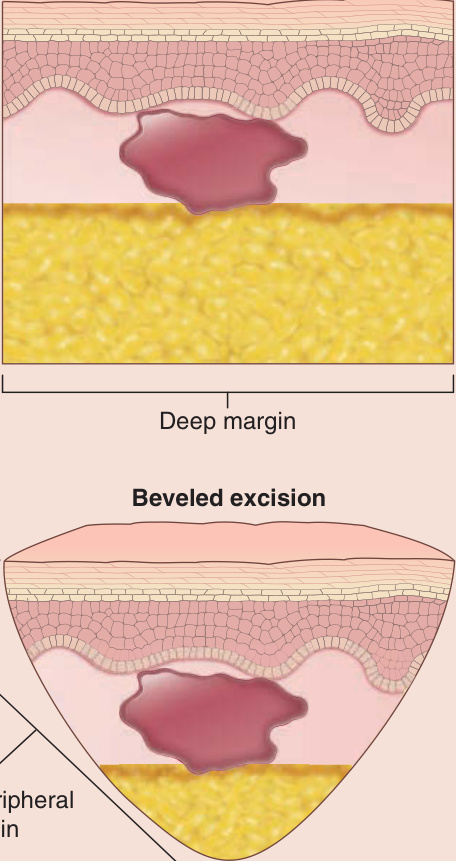
Figure 204-1 Comparison of standard versus beveled excision. A, With standard surgical excision, the incision is made perpendicular to the skin surface with a 90-degree angle between the peripheral and the deep margin. B, With beveled excision, the incision is made at a 45-degree angle with the skin surface, creating a continuous peripheral and deep margin on the same plane.
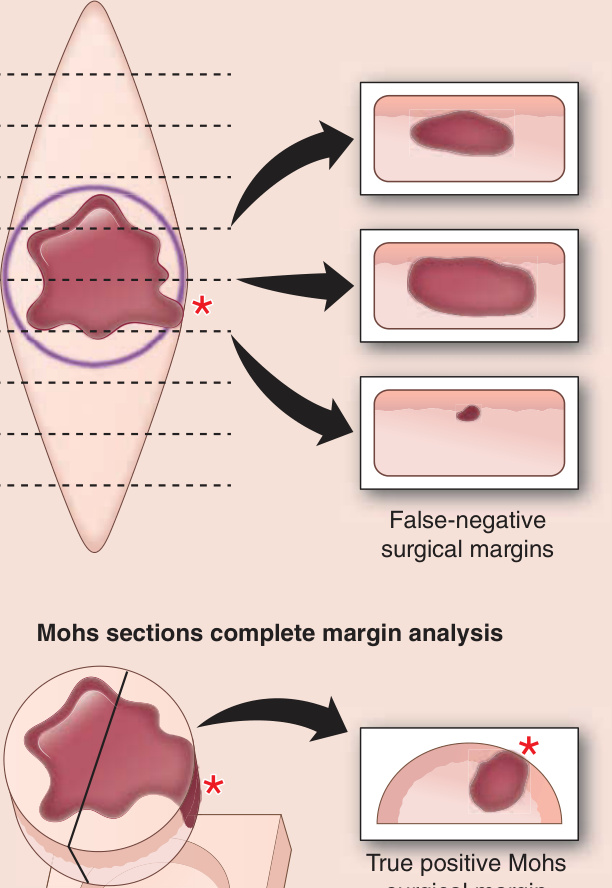
Figure 204-2 Complete margin analysis with Mohs surgical technique. A, With typical perpendicular or “bread-loaf” sections, representative cross sections, indicated by dashed lines, are examined at regular intervals along the excised tissue. Arrows indicate histopathologic visualization of tumor (red) with apparently clear margins in these sections. An irregular projection of tumor (red asterisk) at the margin is not detected in between these sections. B, In Mohs surgery, beveled excision specimens are examined with en face sections, permitting visualization of the entire deep and peripheral margin and identification of any tumor projections at the surgical margin (red asterisk). By definition, any tumor visible with en face sections is present at the surgical margin.
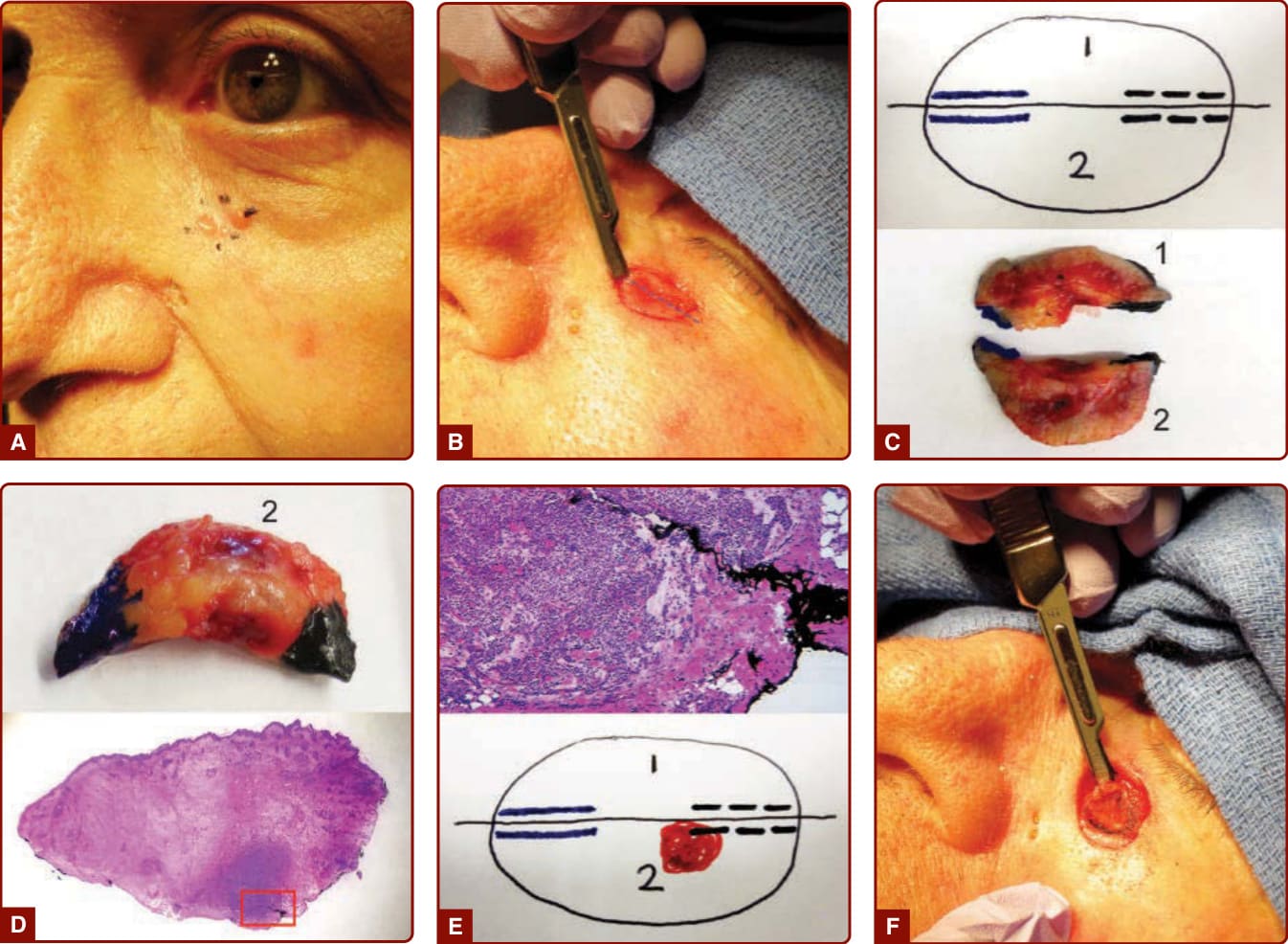
Figure 204-3 Mohs surgery procedure. A, A biopsy-confirmed basal cell carcinoma (BCC) is identified and marked on the left cheek overlying the inferior orbital rim. B, After curettage to remove gross carcinoma and define the clinical margins, the lesion is excised in the first stage with a narrow margin and a beveled edge, holding the scalpel at a 45-degree angle to the skin surface. A score mark (blue dashed line) is made on the excised specimen and extended onto the surrounding skin to preserve anatomic orientation. C, A map is drawn of the excised tissue (upper panel) and the specimen, shown with the epidermal surface facing up, is bisected along the score mark (lower panel). Indelible ink is used to mark the marginal surface blue on the left and black on the right. D, Piece 2 is shown flipped over with the deep marginal surface facing up, revealing the blue and black indelible ink (upper panel). Histopathologic sections are cut from the marginal surface and stained with hematoxylin and eosin (lower panel), revealing the epidermal peripheral margin and the subcutaneous deep margin in a single plane. The red box at the deep margin is shown at higher magnification in panel E. E, Higher magnification reveals persistent BCC at the deep margin near the black ink (upper panel). The area of carcinoma at the margins is marked on the map in red (lower panel). F, The area of residual carcinoma is excised in a second stage, again with a beveled edge to allow complete margin examination. This process is repeated until clear margins are obtained.

Figure 204-4 Basal cell carcinoma (BCC) subclinical extension. An apparently small BCC of the upper lip (A) was found to extend broadly over the cutaneous and mucosal lip and invade into the orbicularis oris muscle (B). Clear margins were obtained after three stages of Mohs surgery and the defect was repaired with a local skin flap.
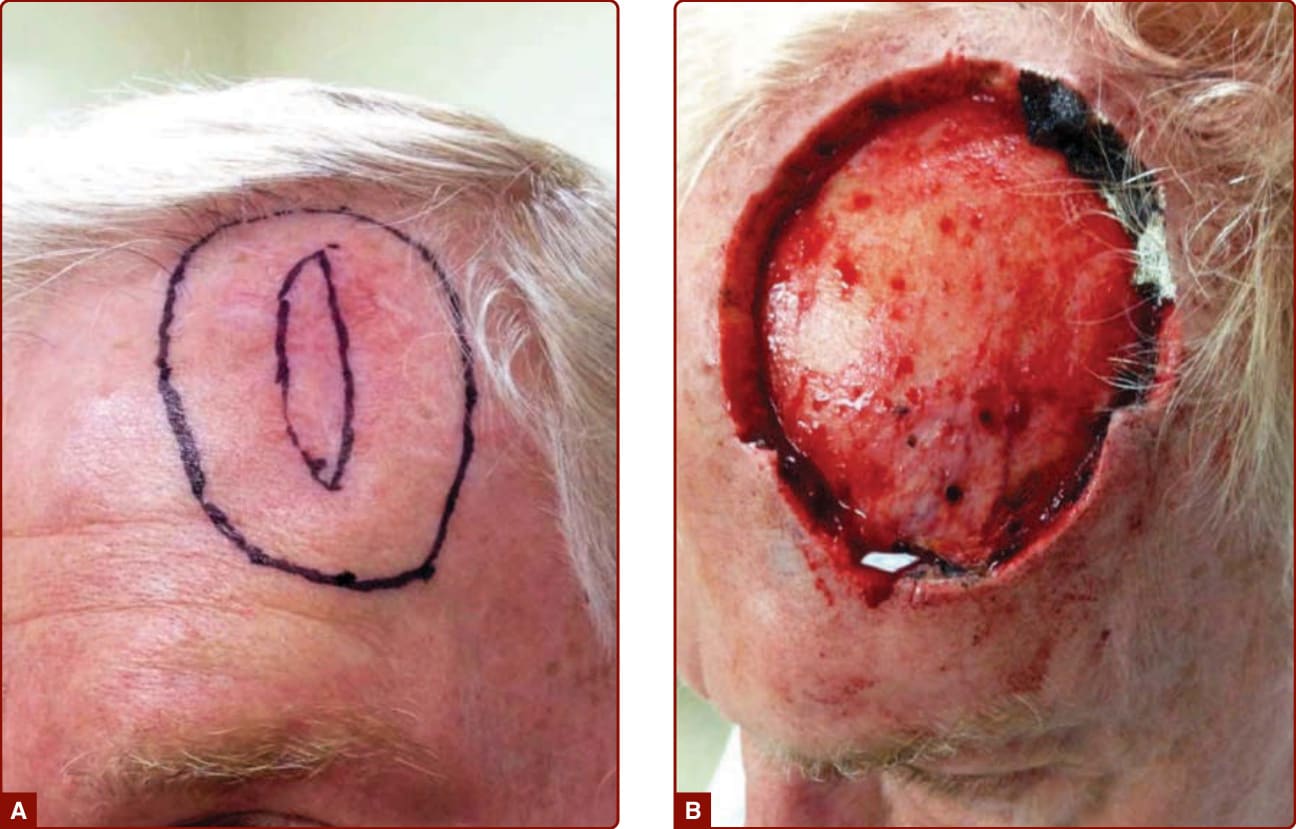
Figure 204-5 Squamous cell carcinoma (SCC) subclinical extension. SCC of the forehead and scalp with infiltrative histology and positive deep and lateral margins after initial excision and linear repair (A). A broad, 2-cm margin was excised as the initial stage of Mohs surgery (outer black line), but carcinoma was found infiltrating the fascia and periosteum at the surgical margins. Clear margins were obtained after the second stage of Mohs surgery. The defect measured 8.4 cm and extended to the exposed frontal bone (B); it was repaired with a delayed full-thickness skin graft.
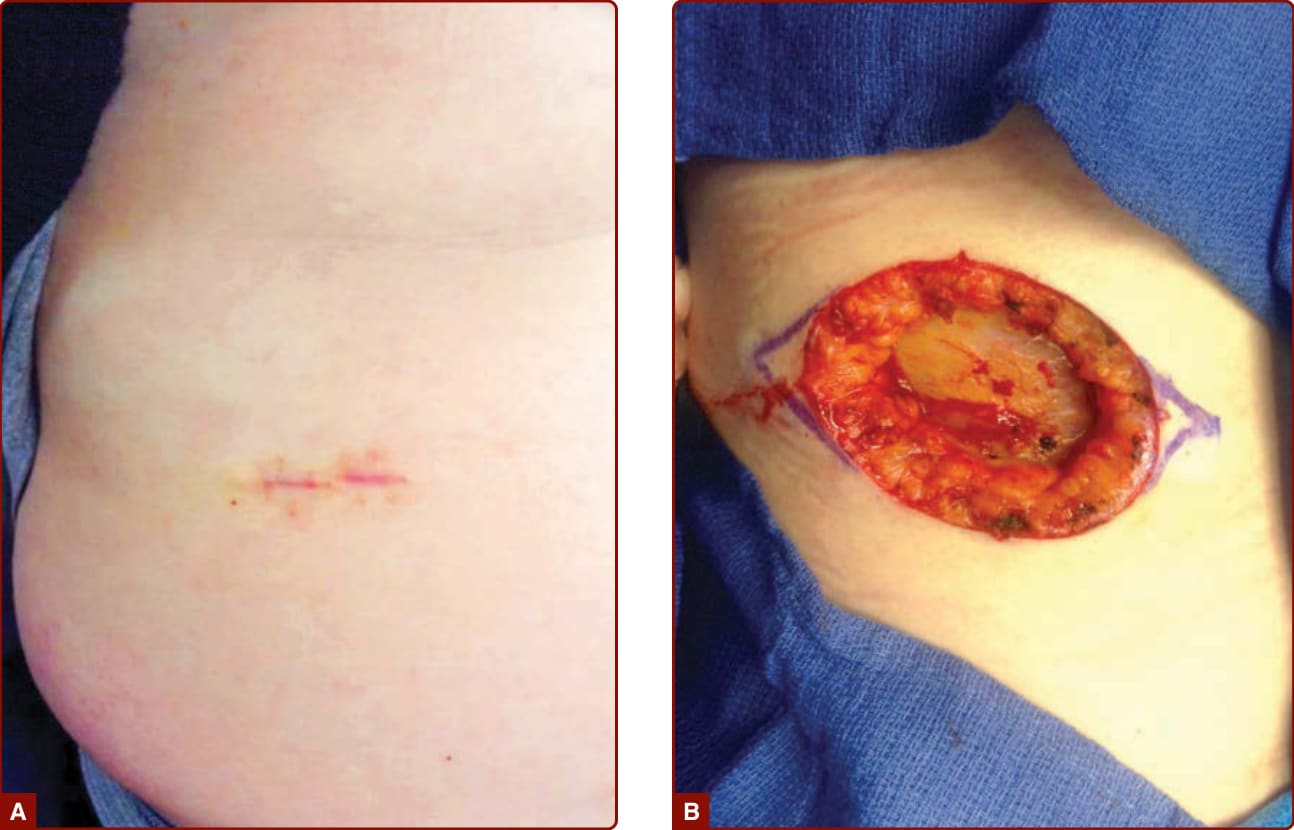
Figure 204-6 Dermatofibrosarcoma protuberans (DFSP). A subtle clinical lesion on the abdomen at the site of a biopsied DFSP (A) was found to extend over a broad area with penetration to the deep subcutis overlying the fascia of the abdominal wall musculature (B). Clear margins were obtained after three stages of Mohs surgery, and the defect was repaired with a linear closure.
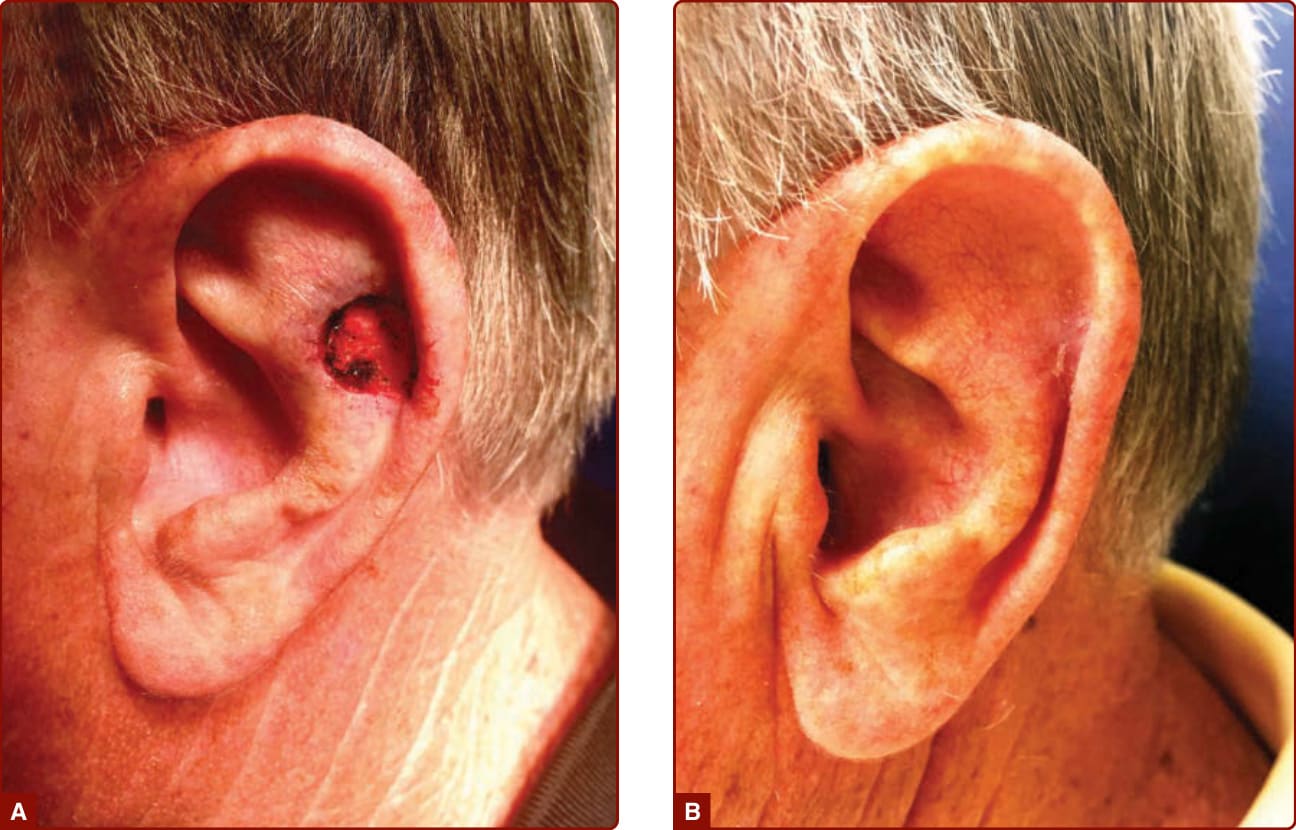
Figure 204-7 Healing by second intent. A 1.6-cm defect of the left scapha and antihelix after Mohs surgical extirpation of a basal cell carcinoma of the ear was allowed to heal by second intent (A). After 6 weeks, the wound is fully healed with an excellent cosmetic and functional result (B).
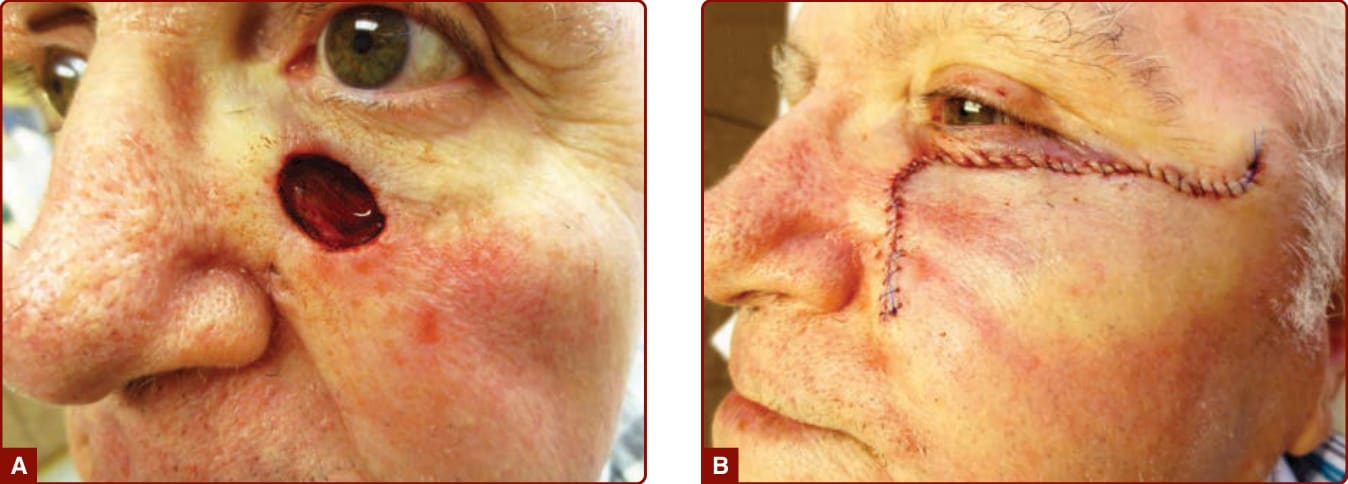
Figure 204-8 Local skin flap reconstruction. After two stages of Mohs surgery, the basal cell carcinoma shown in Fig. 204-3 was completely excised, leaving a 1.6-cm defect of the left cheek and lower eyelid (A). The defect was repaired with an advancement flap from the lateral lower eyelid and temple to avoid distortion of the free margin of the lower eyelid (B).
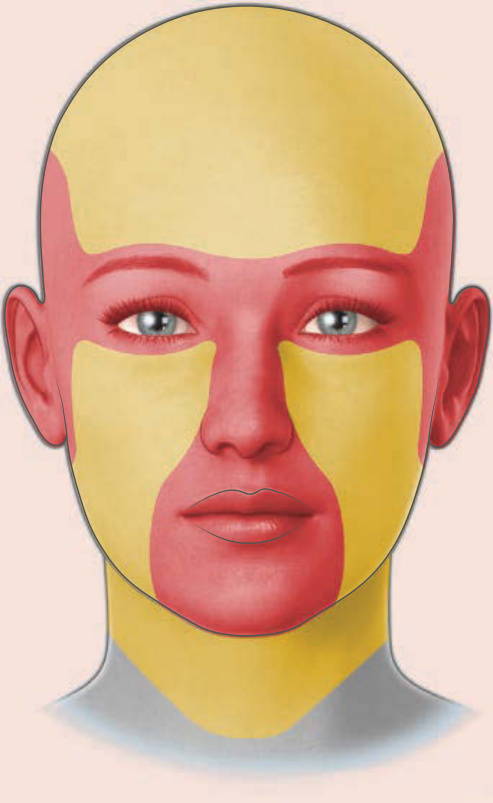
Figure 204-9 Mohs surgery appropriate use criteria anatomic risk areas of the head and neck. High-risk areas on the central face, eyelids, eyebrows, nose, lips, chin, ears, periauricular skin, and temples are shown in red. Medium-risk areas on the cheeks, forehead, scalp, neck and jawline are shown in yellow. Not shown are high-risk areas on the hands, feet, ankles, genitalia, and nipple and areola, as well as medium-risk areas on the pretibial surface.
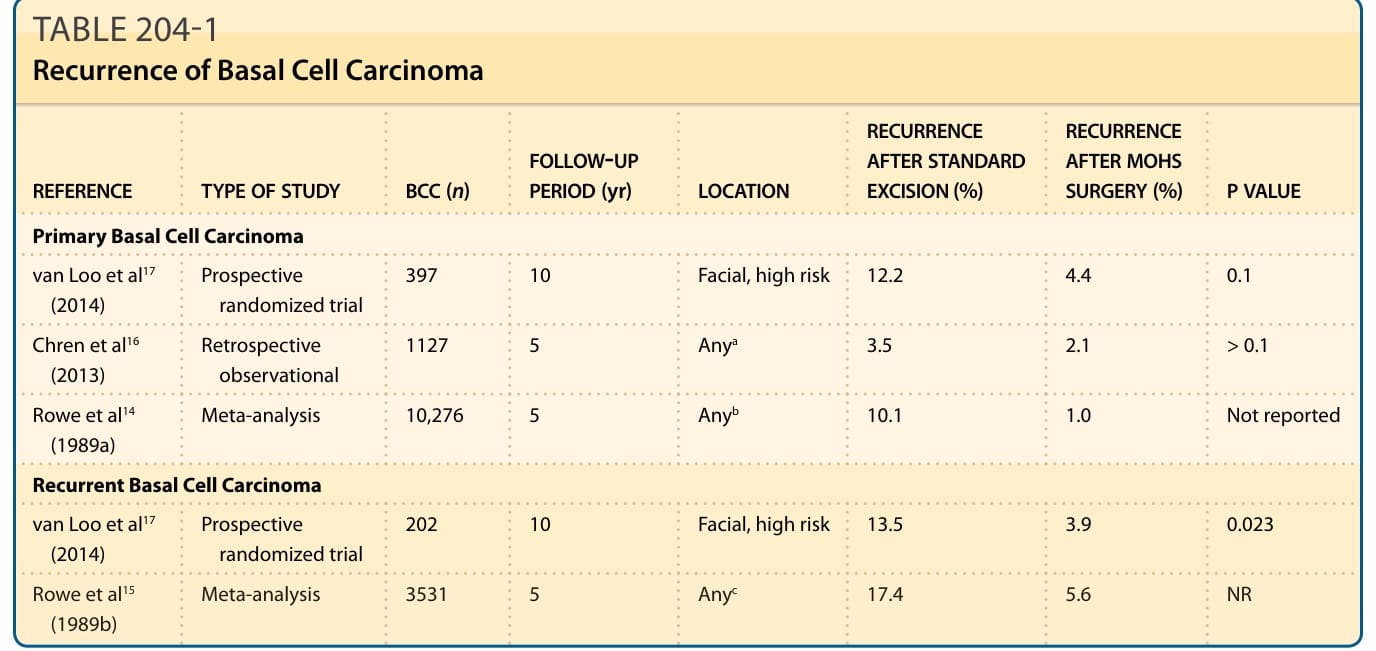
TABLE 204-1 Recurrence of Basal Cell Carcinoma
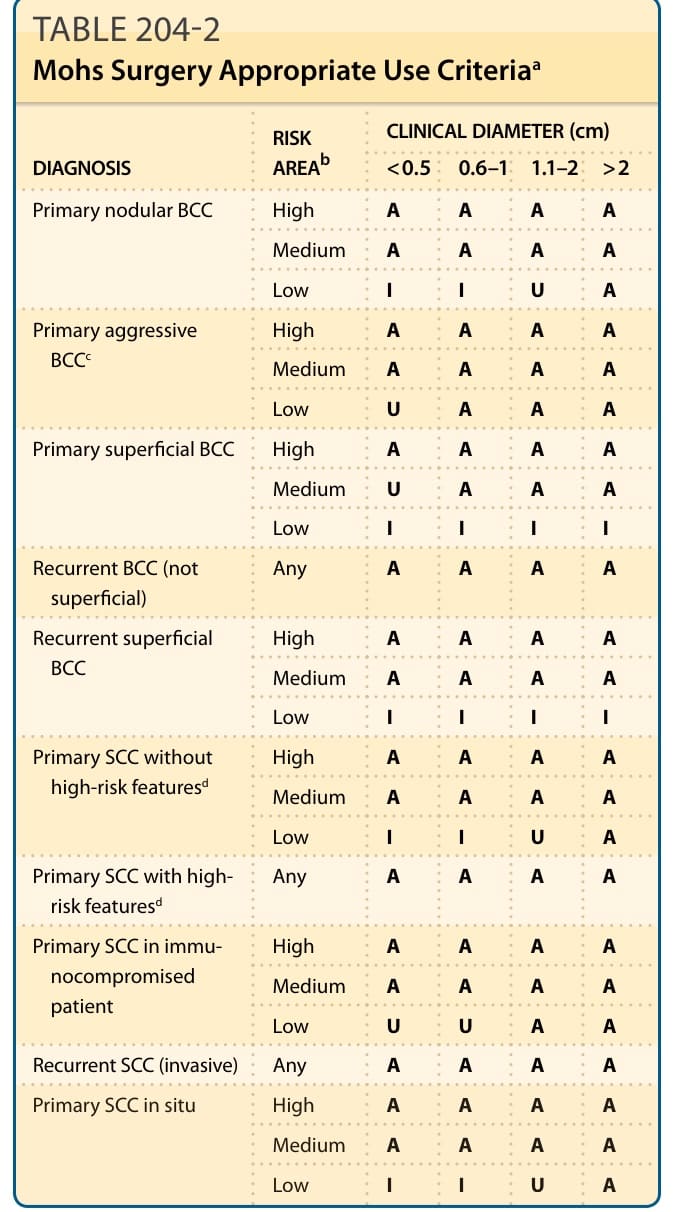
TABLE 204-2 Mohs Surgery Appropriate Use Criteriaa