Cutaneous Surgical Anatomy
PART30
Dermatologic Surgery
AT-A-GLANCE
■ The superficial musculoaponeurotic system (SMAS) is a fibromuscular layer connecting the facial muscles. Incisions and undermining within the subcutaneous fat above SMAS will not result in damage to motor nerves.
■ When planning reconstruction, the surgeon should consider cosmetic units, junctional lines, and resting skin tension lines to optimize the final aesthetic result.
■ The three branches of the trigeminal nerve (cranial nerve V) provide sensory innervation to the face.
■ The three main danger zones are areas where the temporal and marginal mandibular branches of the facial nerve and spinal accessory nerve lie superficial and can be easily injured. Damage to the temporal branch of the facial nerve may result in an ipsilateral eyebrow ptosis and obscuring of the superolateral visual field. The marginal mandibular branch of the facial nerve is vulnerable to damage along the inferior edge of the body of the mandible. Damage to the marginal mandibular branch of the facial nerve results in an asymmetrical smile. The spinal accessory nerve lies in the posterior triangle of the neck and may be identified by Erb’s point.
■ The rich vascular supply to the face from both the external and internal carotid ensures the reliable healing potential and viability of flaps and grafts in head and neck surgery.
INTRODUCTION TO CUTANEOUS SURGICAL ANATOMY
Factors such as the increasing incidence of skin cancer, the desire to maintain a youthful appearance in an aging population that is living longer, and the financial pressure to perform procedures in less invasive and more cost-effective ways have made surgery a cornerstone of the practice of dermatology. Knowledge of anatomy is critical for a number of reasons, including communicating precisely with colleagues, performing safe and efficient procedures, achieving aesthetic and functional reconstruction, understanding the lymphatic drainage, and anticipating metastatic spread of cutaneous malignancies. Because the vast majority of these procedures are performed on the head and neck, this chapter focuses on the anatomy of this critical region. This chapter focuses on five important concepts in head and neck anatomy, which are
■ The superficial musculoaponeurotic system (SMAS)
■ Topography and cosmetic units
■ Free margins
■ Relaxed skin tension lines (RSTL)
■ Facial motor nerves susceptible to damage during dermatologic surgery
30
THE SUPERFICIAL MUSCULOAPONEUROTIC SYSTEM
An important concept in understanding head and neck anatomy is the SMAS, a layer of superficial fascia that envelopes and links the facial expression muscles with each other and with the overlying skin. It stretches over the cheeks between the temporalis and frontalis muscles above and the platysma muscle below. The SMAS also attaches to the orbicularis oculi muscles anteriorly and the trapezius muscle posteriorly and includes the fascia of the forehead and galea of the scalp. Most of the superficial muscles of the scalp and face insert into the skin either directly through fibrous bands running in the subcutaneous tissue or indirectly by attachment to the SMAS, which in turn is attached to the skin. In the lateral areas of the face, the SMAS is organized and more visible but becomes less discrete medially. Because of its attachment to the skin superficially and muscles deep, the SMAS coordinates a wide range of facial expressions. In addition, the SMAS is an important landmark because most major arteries and nerves run within or deep to it. Dissection above the SMAS allows the dermatologic surgeon to safely avoid neurovascular structures.
TOPOGRAPHIC ANATOMY AND COSMETIC UNITS
Cosmetic units are zones of tissue that share cutaneous features such as color, texture, pilosebaceous quality, pore size, and degree of actinic exposure. These cosmetic units are demarcated by junction lines that can be discrete (eyebrows) or subtle (nasofacial sulcus). The forehead, temples, eyelids, nose, cheeks, upper and lower lips, chin, and ears represent the major cosmetic units of the face. Cosmetic units can also be further divided into subunits. Because of the tissue similarity, it is often best to reconstruct a surgical defect within a cosmetic unit or subunit or borrow tissue from nearby units. In addition, scar lines can be hidden easily in junction lines between the cosmetic units. Scars that cross cosmetic units are more noticeable and cosmetically less pleasing. The more complex regions of the face that have multiple subunits include the nose, ears, and lips (Figs. 201-1 and 201-2). Topographic anatomy and cosmetic units help localize areas of the face accurately for purposes of communication with colleagues and to perform the surgery itself. For instance, it is more helpful to describe a lesion on the face if it is said to be located on the “left nasal sidewall” versus left nose or “right triangular fossa” versus right ear. The subunits of the nose include the glabella (the area between the eyebrows), the root (the deep sulcus below the glabella and uppermost portion of the nose), the dorsum or bridge (the area overlying
3698
Cosmetic units and landmarks of the face
Glabella
Root
Nasofacial sulcus
Dorsum
Lateral side wall
Columella
Tip
Philtral crest Melolabial fold Cupid’s bow
Ala nasi
Philtrum
Vermilion
Mental crease
the nasal bone), lateral sidewalls (the sides of the nose), the nasal tip, the nasal ala (the nostril), the alar groove and nasolabial crease (the grooves that demarcate the alae superiorly from the lateral nasal sidewall and alae inferiorly from the lip, respectively), and the columella (the mobile linear structure separating the alae inferiorly) (see Fig. 201-1). The lateral surface of the ear is rimmed by the helix, a curved cartilaginous structure that begins at the crus just above the external auditory canal and continues around the ear to end at the fleshy lobule. The central concavity within which the external auditory meatus lies is the concha. The concha is divided by the crus of the helix into a superior portion; the cymba; and an inferior portion, the cavum. The posterior border of the concha is formed by another cartilaginous structure called the antihelix. Superiorly, the antihelix originates from two legs (crus is Latin for leg): (1) the
Landmarks of the external ear
Crura of antihelix
Triangular fossa
Scapha
Crus of helix
Concha -Cymba -Cavum
External auditory meatus
Helix
Tragus
Intertragic notch
Antihelix
Antitragus Lobule
superior crus and (2) inferior crus. The region between the crura is referred to as the triangular fossa. The groove between the helix and antihelix is the scaphoid fossa. The triangulated cartilaginous structure just anterior to the auditory canal is called the tragus, and just posterior to this is the triangulated end of the antihelix, referred to as the antitragus. The inferior region between the tragus and antitragus is the intertragic notch (see Fig. 201-2). The cutaneous upper lip has a concave depression in the center, called the philtrum, which is bounded by two ridges, the philtral crests. There is a prominent crease, the mental crease, which divides the cutaneous lower lip from the chin. The boundary between the red mucosal surface of the lips and the cutaneous surface is called the vermillion border. The raised contoured area of the inferior portion of the philtrum is a critical aesthetic landmark known as the Cupid’s bow (see Fig. 201-1).
FREE MARGINS
A free margin is any anatomical structure that can be easily distorted when tension is placed on it. The eyelid margin, alar rim, lip vermillion, and helical rim are free margins. When these regions become distorted, the resulting asymmetry can cause cosmetic and functional concerns. An ectropion can result in epiphora, as well as conjunctival and corneal exposure leading to corneal scarring. An eclabium may result in altered speech, an asymmetrical smile, or drooling. The nasal ala does not have cartilage and is composed of fibrofatty tissue, thus making it quite vulnerable to distortion when tension is placed on it. It is important for dermatologic surgeons to appreciate the tension vectors during wound closure to avoid free margin distortion.
RELAXED SKIN TENSION LINES
RSTLs are another characteristic of the face that help guide surgical reconstruction and allow the structural camouflage of scar lines. RSTLs are creases on the face that form over time because of factors such as loss of elastic tissue tone, lengthening of the collagenous fibrous septae that connect the dermis to the underlying facial muscles, development of excessive skin, gravity, and ultraviolet radiation exposure (see Fig. 201-3). RSTLs are most obvious on the face because unlike other muscles in the body that connect tendons and bones, facial muscles attach to the overlying skin. These lines can be induced by facial muscle movement in young people but inevitably become more pronounced with age. RSTLs usually run perpendicular to the underlying muscles. In most situations, the long axis of the excision should be placed parallel to the RSTL because they are often in the direction of the least tension for a scar. It is preferable to design flaps such that the majority of the scar lines fall within the RSTL.
3
30
Relaxed skin tension lines of the face
FACIAL MOTOR NERVES SUSCEPTIBLE TO DAMAGE DURING DERMATOLOGIC SURGERY
There are three main danger zones that are critical to understand while performing surgical procedures on the head and neck. Each of these zones involves a motor nerve and the muscles it innervates. These are the temporal and marginal mandibular branches of the facial nerve (cranial nerve VII) and the spinal accessory nerve (cranial nerve XI) (Table 201-1). These will be discussed in more detail below. It is important to confirm the baseline function of these nerves and muscles before performing a procedure in these areas so that it can be readily determined whether an injury occurred during surgery. The facial nerve exits the skull through the stylomastoid foramen near the earlobe and immediately gives off the posterior auricular branch, which provides motor innervation to the occipital and posterior auricular muscles. It then enters the parotid gland at the midpoint of a line connecting the tragus with the angle of the mandible. Within the parotid gland, the facial nerve divides into the temporofacial and cervicofacial rami from which five branches arise. The well-known mnemonic “to Zanzibar by motor car” can be used to remember the five main branches: (1) temporal, (2) zygomatic, (3) buccal, (4) mandibular, and (5) cervical. After leaving the parotid gland, the branches of the facial nerve lie deep to the SMAS and enter the
3699
30
Paralysis of trapezius, winging of the scapula, shoulder drop, inability to shrug the shoulder, difficulty with arm abduction, chronic shoulder pain
ula, shoulder drop, inability to shrug the
shoulder, difficulty with arm abduction,
Parotid gland
Mastoid process
Mastoid process
= Danger zones for undermining
Cervical branch
al mandibular branch
Angle of jaw
Angle of jaw
atic branches
al branches
l’s tubercle
l branches
is muscle
Tempora
Zygoma
Frontali
Margina
Whitnall
Bucca
Inferior border of the mandible, as the nerve crosses the angle of the mandible at the inferoanterior border of the masseter
midpoint of the posterior border of
Facial nerve as it crosses the middle third of the zygomatic arch
the sternocleidomastoid
Depressor anguli oris, depressor labii inferioris, mentalis, part of orbicularis oris
Temporal branch of the facial nerve Frontalis, upper fibers of the orbicularis oculi, corrugator supercilii, anterior and superior auricular muscles
Danger Zones of the Face
Marginal mandibular branch of the facial nerve
chronic shoulder pain
Proximal third of stemocleidomastoid
omastoid
apezius
Distal third of trapezius
al third
Spinal accessory nerve
ssory
rd of
of tra
Dista
Spinal acces
Proximal thir
stemocleido
nerve
Mid point of sternocleidomastoid
Mid point of
ernocleidomastoid
Erb’s point
Erb’s point
ste
muscles of facial expression from their deep surface. The branches of the facial nerve are therefore well protected during surgical procedures that are no deeper than fat. However, it is important to note that there can be minimal thickness of the fat layer at certain sites such as the temple and at other sites in older adult patients. The two branches of the facial nerve most susceptible to injury during dermatologic surgery are the temporal branch as it crosses the zygomatic arch and the marginal mandibular branch along the inferior border of the mandible. The buccal and zygomatic branches form an interconnecting network across the midface, and although damage to these nerves may occur during surgical procedures, any injury is less debilitating than an injury to the temporal nerve because of the multiple rami in the buccal and zygomatic branches. Damage to the cervical branch is of minimal clinical importance because it innervates the platysma muscle, which also receives nerve fibers from the marginal mandibular nerve.
TEMPORAL BRANCH OF THE FACIAL NERVE
TEMPORAL BRANCH OF
THE FACIAL NERVE
The temporal (or frontal) branch of the facial nerve innervates the frontalis, the upper fibers of the orbicularis oculi, the corrugator supercilii, and the anterior and superior auricular muscles. After emerging from the parotid gland, the nerve travels diagonally across the temple, where it lies between the superficial temporal fascia (a component of SMAS) and the deep temporal fascia. The temporal branch of the facial nerve divides into three to five rami as it crosses the middle third of the zygomatic arch. At this point, the nerve is most superficial and susceptible to damage and it is critical in this area to undermine just beneath the dermis in the superficial fat above the fascia. The approximate course of the temporal branch of the facial nerve can be projected on the skin by a line drawn from the earlobe to the lateral edge of the eyebrow and another line from the tragus to just above the and behind the highest forehead crease (Fig. 201-4). Damage to the temporal branch of the facial nerve results in cosmetic and functional loss. Flattening of the forehead with diminished visibility of wrinkles and skin tension lines becomes easily noted. Over time, as the denervated muscle atrophies, patients develop eyebrow and eyelid ptosis, which may lead to visual field disturbance. A brow lift and blepharoplasty may be required to correct this problem.
MARGINAL MANDIBULAR NERVE
MARGINAL MANDIBULAR
NERVE
The marginal mandibular branch of the facial nerve exits the parotid gland at the angle of the jaw. It divides into two or more rami and travels anteriorly along the
3
30
Danger zone for the temporal nerve
ramus of the mandible to supply the depressor anguli oris, the depressor labii inferioris, the mentalis, and part of the orbicularis oris. As it crosses the angle of the mandible at the inferoanterior border of the masseter, the marginal mandibular nerve is covered only by skin, subcutaneous fat, and fascia, which may be thin in this location, particularly in older adults. Damage to the marginal mandibular nerve results in contralateral and upward pull on the mouth while the affected ipsilateral side of the mouth is fixed in a grimace with a lip droop.
SPINAL ACCESSORY NERVE
SPINAL ACCESSORY NERVE
The posterior triangle of the neck is defined by the posterior border of the sternocleidomastoid, the anterior border of the trapezius, and the clavicle. The spinal accessory nerve enters the posterior triangle of the neck from under the posterior border of the sternocleidomastoid, roughly at its midpoint. It then crosses the floor of the posterior triangle, before leaving the posterior triangle under the trapezius. In the posterior triangle of the neck, the spinal accessory nerve occupies a relatively superficial location between the superficial and prevertebral layers of the deep cervical fascia. One can anticipate the location of the spinal accessory nerve by drawing a line connecting the angle of the mandible with the mastoid process. A vertical line is then drawn from the midpoint of this line 6 cm inferiorly. The point at which this line intersects the
3701
30
posterior border of the sternocleidomastoid muscle is Erb’s point. This landmark indicates the location of several important sensory nerves, including the transverse cervical, lesser occipital, and great auricular nerves, but most important, the point at which the spinal accessory nerve emerges from behind the sternocleidomastoid. Injury to the spinal accessory nerve leads to the paralysis of the trapezius with winging of the scapula, shoulder drop, inability to shrug the shoulder, difficulty with abducting the arm, and chronic shoulder pain.
SENSORY NERVES
The trigeminal nerve (cranial nerve V) provides the majority of the sensory innervation of the face (Figs. 201-5 and 201-6 and Table 201-2). It exits the skull via three foramina located bilaterally in the midpupillary line, the supraorbital, infraorbital, and mental foramina. The first branch, the ophthalmic nerve (V1), has several branches that supply the innervation to the superior portion of the face: the supraorbital, supratrochlear, infratrochlear, external nasal, and lacrimal nerves. The supraorbital (lateral) and supratrochlear (medial) nerves supply the forehead and anterior scalp and are branches of the frontal nerve (the largest branch of the ophthalmic nerve). They exit from two
Sensory distribution of the trigeminal nerve
Opthalmic V1
Maxillary V2
Mandibular V3
Innervation of the face
Supratrochlear nerve
Supraorbital nerve
Zygomaticotemporal nerve
Auriculotemporal nerve
Lacrimal nerve
Zygomaticofacial nerve
Infratrochlear nerve
Infraorbital nerve
Buccal nerve
Great auricular nerve
External nasal nerve
Mental nerve
Temporal branch
Zygomatic branch
Buccal branch
Mandibular branch
Cervical branch
3702
BRANCH AREA INNERVATED
V1 (Ophthalmic Nerve)
Supraorbital (lateral) nerve Forehead, anterior scalp
Supratrochlear (medial) nerve Forehead, anterior scalp
Infratrochlear nerve (nasociliary) Glabella, nasal root, nose bridge
External nasal nerve (dorsal nasal) Anterior ethmoidal nerve, dorsal nose
Lacrimal nerve Upper eyelid
V2 (Maxillary Nerve)
Zygomatic nerve Zygomaticofacial Lateral canthus
Zygomaticotemporal Anterior temporal region
Infraorbital nerve Eyelid, superior cheek
V3 (Mandibular Nerve)
Auriculotemporal Most of the temple, temporoparietal scalp, anterior ears, external ear canal, tympanic membrane
Buccal Buccinators, buccal mucosa, gingiva
Mental Lower lip, chin
Mental Lower lip, chin
notches along the orbital rim: (1) the supraorbital foramen or notch laterally and (2) the supratrochlear notch medially. The infratrochlear branch (of the nasociliary nerve) supplies the glabella, nasal root, and bridge. The external nasal branch (or the dorsal nasal nerve) is a branch of the anterior ethmoidal nerve of the nasociliary branch of V1. The external nasal branch supplies the dorsal nose and provides the anatomical explanation of Hutchinson sign that can occur in some cases of herpes zoster of the ophthalmic nerve. Vesicles on the nasal tip indicate that the eye may be involved because the nasociliary branch of V1 sends branches both to the nasal tip and the cornea. The lacrimal branch supplies sensation to the upper eyelid. The second branch of the trigeminal nerve is the maxillary nerve (V2). The maxillary nerve supplies sensation to the lateral nose, lower eyelid, superior cheek, and anterior temple. The maxillary nerve gives off two main branches that supply the skin of the face. The zygomatic branch of the maxillary nerve gives rise to the zygomaticofacial nerve, which exits the skull through the lateral zygomatic bone and supplies a small area of the lateral canthus. In addition, the zygomatic branch also gives rise to the zygomaticotemporal nerve, which exits the skull through the anterior temporal fossa and supplies skin of the anterior temporal region. The largest branch of the maxillary nerve is the infraorbital nerve that exits the skull through the infraorbital foramen of the maxilla. This supplies sensation to the eyelid and superior cheek.
3
30
The third branch of the trigeminal nerve is the mandibular nerve (V3). Its branches provide sensory innervation to the lower lip, chin, mandibular and preauricular cheek, anterior ear, and central temporal scalp. The mandibular nerve gives off three major cutaneous branches: the (1) auriculotemporal, (2) buccal, and (3) mental nerves. The auriculotemporal nerve innervates most of the temple, the temporoparietal scalp, the anterior ears, parts of the external ear canal, and the tympanic membrane. The buccal nerve lies deep to the parotid gland and supplies the skin over the buccinators, the buccal mucosa, and the gingiva. The mental nerve exits through the mental foramen and is a continuation of the inferior alveolar nerve. The mental nerve supplies sensation to the lower lip and chin.
MUSCLES OF FACIAL EXPRESSION
The scalp has two muscles overlying it, the frontalis anteriorly and the occipitalis posteriorly. These muscles are joined by a thick fascia centrally over the scalp, the galea aponeurotica. The frontalis muscle also covers the forehead and elevates the eyebrows. The eyebrows move medially and downward with contraction of the corrugator supercilii muscles. The procerus lies between the supercilii muscles and draws the skin of the forehead inferiorly to create the horizontal creases at the root of the nose. The orbicularis oculi muscle surrounds the eye and consists of an orbital and palpebral portion. The orbicularis oculi muscle serves to close the eyes with the palpebral part with both reflexive and voluntary control and the orbital part with voluntary control. The central sphincter-like muscle around the mouth is the orbicularis oris. This muscle helps purse the lips to form certain sounds and whistle. The lip depressors are depressor anguli oris, depressor labii inferioris, and the mentalis. The lip elevators are the zygomaticus major, zygomatic minor, levator anguli oris, levator labii superioris, and levator superioris alaeque nasi. The risorius helps retract the corner of the mouth. The buccinators and masseter muscles help with mastication (Fig. 201-7).
VASCULAR ANATOMY
The blood supply of the face is almost entirely derived from branches of the external carotid artery (Fig. 201-8). Just posterior and medial to the angle of the mandible, the facial artery branches off the external carotid artery. The facial artery continues anteriorly and superiorly toward the angle of the mouth, giving off the inferior labial artery and superior labial arteries that supply the lips. The continuation of the facial artery in the nasofacial sulcus is called the angular artery. The angular artery continues superiorly to enter the orbit immediately over the medial canthal tendon, where it anastomoses with the ophthalmic artery, a branch of the internal carotid artery. After giving off the facial artery, the external carotid artery then passes deep to
3703
30
Muscles of facial expression
Epicranial aponeurosis (galea aponeurotica) Frontalis muscle
Procerus muscle
Corrugator supercilii muscle
Orbital portion
Orbicularis oculi muscle
Palpebral portion
Levator labii superioris alaeque nasi muscle
Levator labii superioris muscle
Zygomaticus minor muscle
Zygomaticus major muscle
Levator anguli oris muscle
Risorius
Buccinator muscle
Orbicularis oris muscle
Depressor anguli oris muscle
Depressor labii inferioris muscle
Mentalis muscle
Vascular supply of the face
Superficial temporal artery
Superior labial artery
Inferior labial artery
3704
Supraorbital artery
Supratrocholear artery
Dorsal nasal artery
Angular artery
Facial artery
External carotid
the sternocleidomastoid muscle and enters the body of the parotid gland, where it gives off the posterior auricular artery that supplies the postauricular scalp, the maxillary artery, and the superficial temporal artery. The terminal branch of the maxillary artery exits the infraorbital foramen with the infraorbital nerve as the infraorbital artery to supply the lower eyelids and infraorbital cheek. The terminal branches of the internal carotid artery are the ophthalmic artery branches, the supraorbital artery, and the supratrochlear artery. The supraorbital artery emerges from the supraorbital foramen, whereas the supratrochlear artery emerges more medially. The internal and external carotid systems join in two places: (1) where the supratrochlear branch and the dorsal nasal artery anastomose with the angular artery and (2) where the forehead branches of the supraorbital and supratrochlear arteries anastomose with branches of the superficial temporal artery. The veins of the face are parallel and lie posterior to the arteries. Unlike the veins of the trunk and extremities, facial veins have no valves. This allows blood to flow in either direction. Thus, in the central face where there are anastomoses between branches of the ophthalmic vein and of the angular vein, infection has easy access to travel along the ophthalmic vein to the cavernous sinus. The angular vein also communicates with the deep facial vein and pterygoid plexus.
3
30
LYMPHATICS
The lymphatic vessels of the face generally drain from superficial to deep and medial to lateral and caudad. Although the general drainage patterns are described here, variations can occur. The posterior scalp drains to the postauricular and occipital nodes. The lateral and superior face, the forehead, and the lateral eyelids drain to the parotid nodes. The medial and inferior face, including the medial eyelids and lateral lips, drain to the submandibular nodes. The middle twothirds of the lower lip and the chin drain to the submental nodes. These nodes can be optimally palpated by performing a bimanual examination with a gloved hand feeling through the floor of the mouth. The lymph nodes of the head and neck eventually drain into a terminal series of nodes (deep cervical nodes) and finally into the lateral internal jugular chain.
ACKNOWLEDGMENTS
We acknowledge and are grateful to Brent Pennington, MD, coauthor of the previous edition of this chapter.
3705
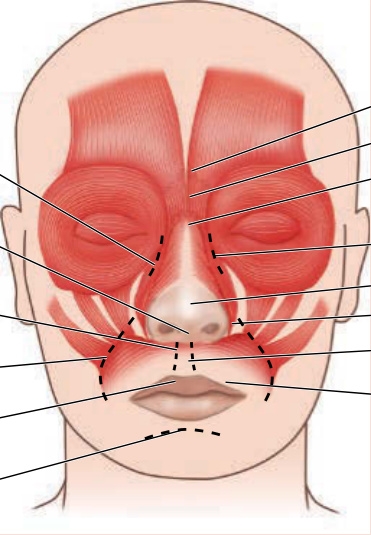
Figure 201-1 Cosmetic units and landmarks of the face.
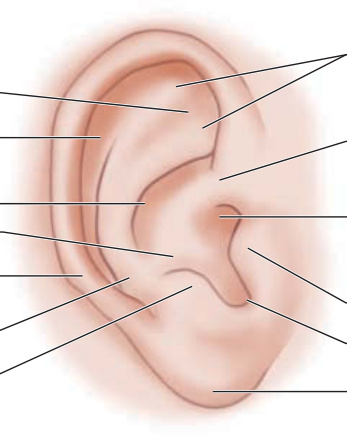
Figure 201-2 Landmarks of the external ear.
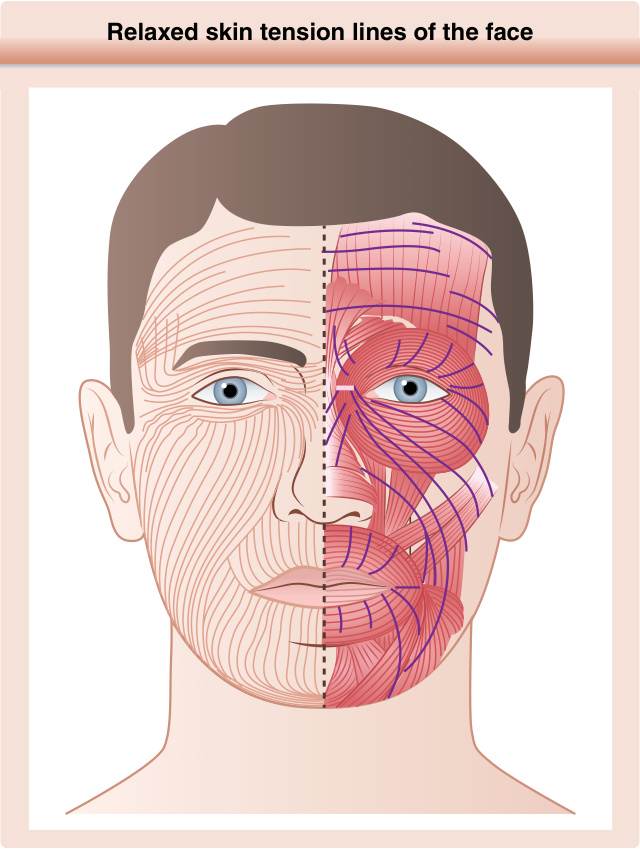
Figure 201-3 Relaxed skin tension lines of the face.
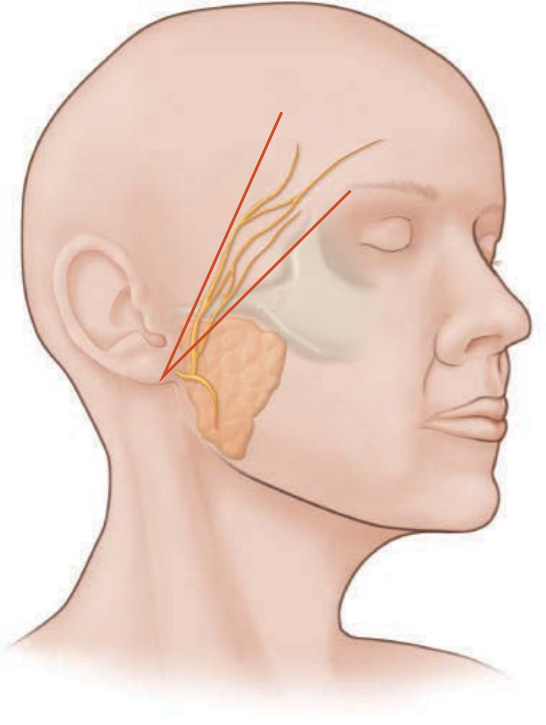
Figure 201-4 Danger zone for the temporal nerve.
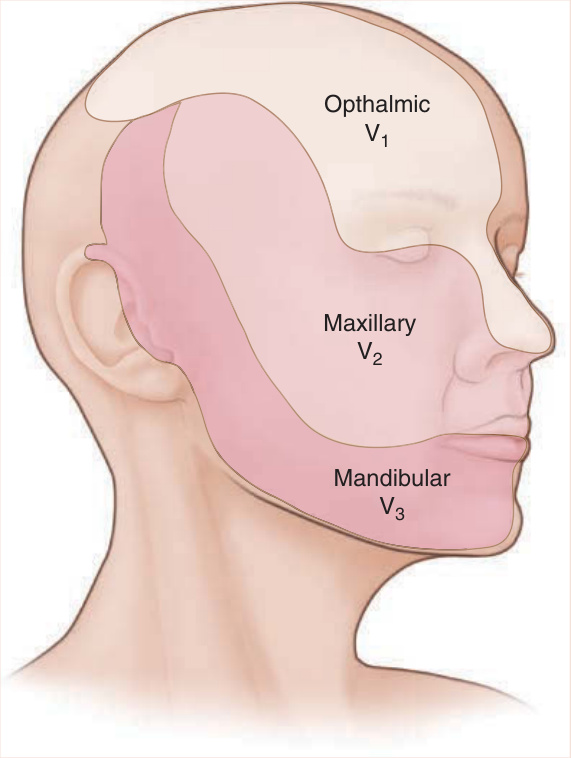
Figure 201-5 Sensory distribution of the trigeminal nerve.
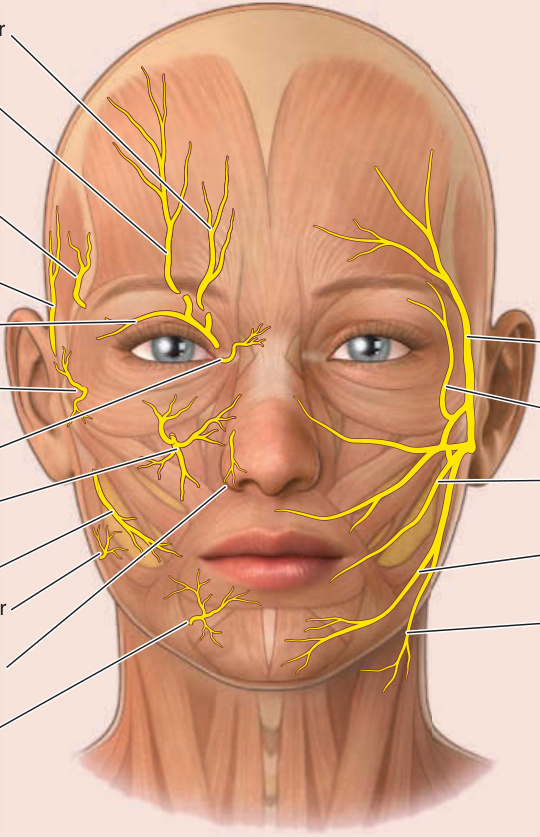
Figure 201-6 Nerves in the face. A, Sensory nerve supply to the skin of the face. B, Branches of the seventh cranial nerve to muscles of facial expression.
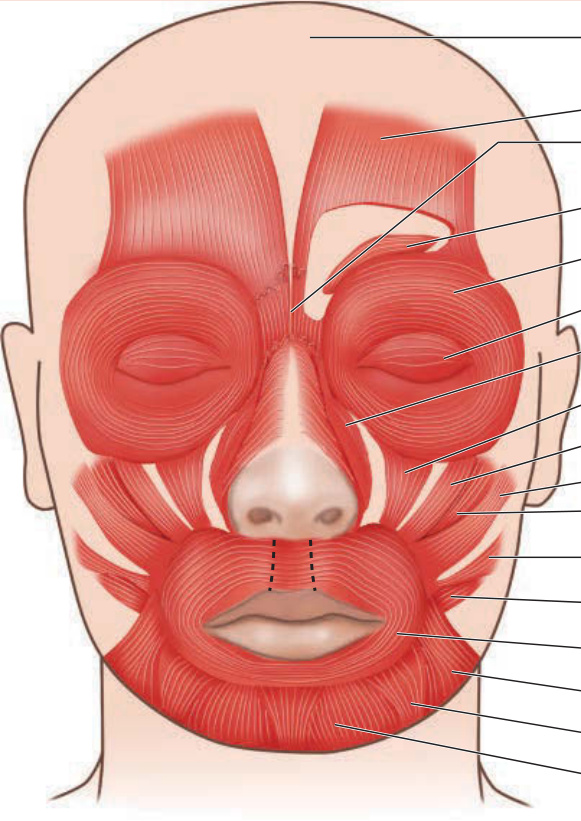
Figure 201-7 Muscles of facial expression.
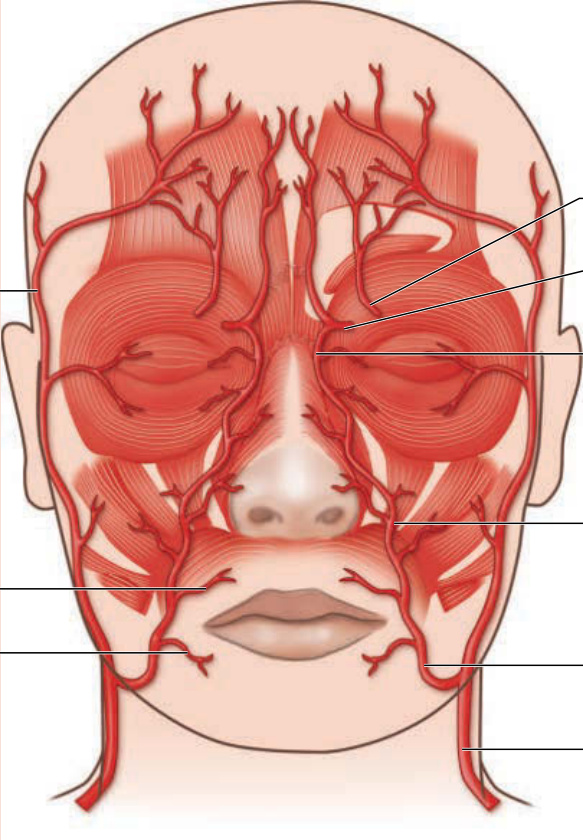
Figure 201-8 Vascular supply of the face.
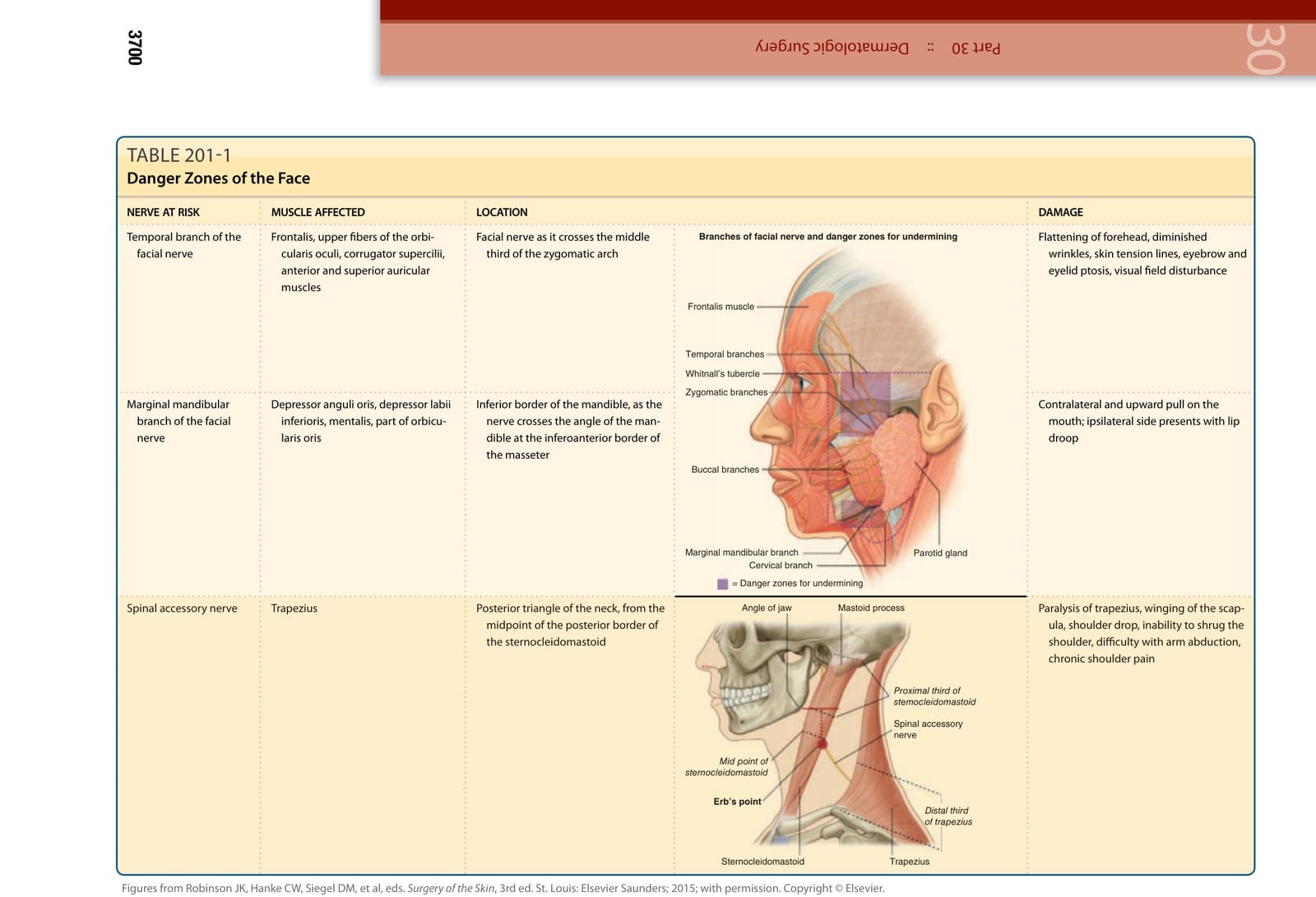
TABLE 201-1
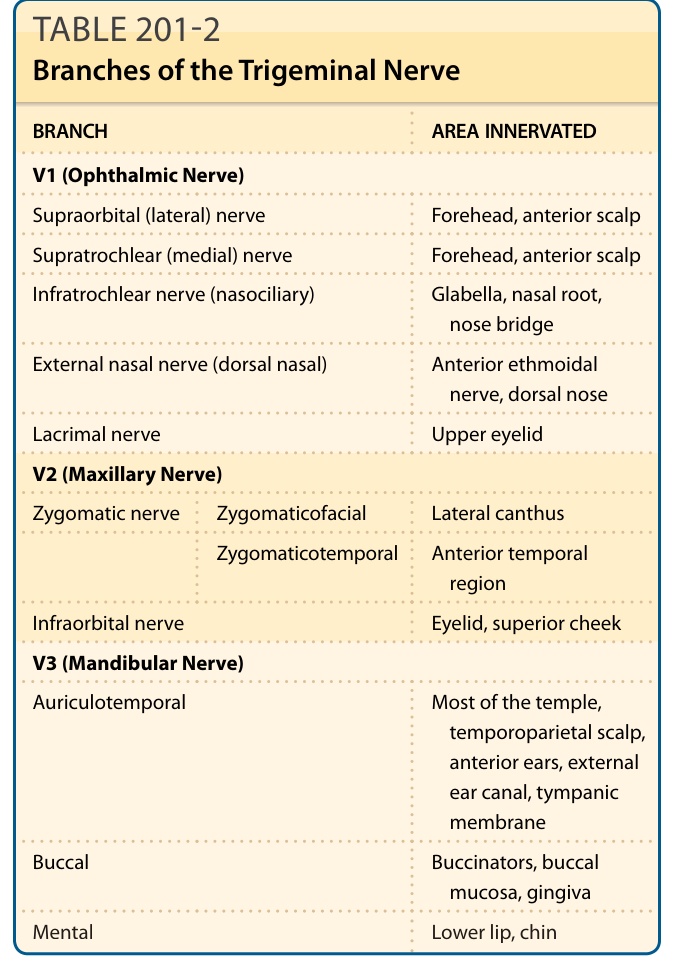
TABLE 201-2 Branches of the Trigeminal Nerve