Radiotherapy
29
AT-A-GLANCE
■ Radiotherapy is a collection of versatile treatment modalities that includes brachytherapy and external-beam radiation.
■ The clinical effects of radiotherapy include acute and late skin changes:
■ Acute effects include an inflammatory reaction and desquamation.
■ Late effects include fibrotic changes and atrophy of skin adnexa.
■ Radiation-induced malignancy is a rare but serious side effect, which presents at a median of 10 years after treatment.
■ Radiotherapy is indicated for selected benign, proliferative diseases after more conservative measures have failed.
■ Radiotherapy is a valuable option for primary or adjuvant therapy for malignant skin disease.
The first documented use of radiation as a therapeutic treatment was for a cutaneous malignancy, in a patient with squamous cell cancer of the nose, in 1900. Over the next century, radiotherapy was widely used in the treatment of both malignant and benign disorders of the skin, in both adults and children. As the longterm consequences of radiotherapy became evident, particularly the risk of radiation-induced malignancy, its use in the treatment of benign diseases declined, particularly in children. Radiotherapy continues to have a small but important role in the management of benign proliferative diseases of the skin, but is more commonly used as a valuable adjunct or alternative to surgery for both premalignant and malignant lesions.
RADIATION MODALITIES
There are several choices for radiation modalities, some commonly available and others only in specialized centers. The selection is made on the basis of the anatomic location and size of the target, tumor biology, the nature of critical surrounding structures, and availability. In particular, with respect to the cutaneous targets, the depth of the lesion plays a large role in determining the optimal therapy. High-energy photons, in the form of γ- or X-rays, are most commonly produced by a linear accelerator (LINAC) and are available in a spectrum of energies. Incident radiation deposits its energy as it passes through matter, becoming attenuated as a function of depth and the density of the tissue. Higher energy
beams deliver increased doses at depth in tissue, and proportionally less at the surface (often referred to as “skin sparing”). Lower energy radiation deposits the dose primarily at the target surface, sparing deeper tissue. The most commonly available treatment energies in general oncology practice are in the megavoltage range (6 to 18 megavolts),1 depositing their dose at a range practical for the treatment of internal targets in human tissue. Such beams were designed to relatively spare surface structures such as skin in the interest of delivering a higher dose to deeper target structures and sparing the skin from toxicity. This is in contrast to lower radiation energy beams in the kilovoltage range (commonly referred to as “superficial radiation therapy”), which are often more appropriate for cutaneous targets. Figure 200-1A shows the depth dose curves demonstrating the absorption of X-rays as a function of their energy. Orthovoltage X-rays refer to lower-energy photons with maximum energy in the range of 125 to 400 kilovolts, often used in dermatologic applications because the dose at the skin surface is maximized. The dose is then rapidly attenuated as the beam penetrates deeper into soft tissue. Half of the incident energy is absorbed within the first few centimeters, and full dose is only delivered to a depth of a few millimeters. Consequently, the most appropriate use is for very superficial tumors. Importantly, lower doses continue to penetrate fairly deeply, so critical structures can still be exposed to a significant exit dose. Orthovoltage X-rays are produced by specialized treatment units that are far smaller than higher-energy machines. Because of their small size and the lower shielding requirements, they are much easier to install in medical offices or even in portable applications. Grenz rays are even lower-energy X-rays in the range of 5 to 15 kilovolts, and therefore deposit their dose at shallower depths than orthovoltage. Historically, Grenz rays were used to treat superficial, benign skin disease. In these cases, the majority of the target processes occur within 1 mm of the skin surface. Grenz rays are no longer recommended as first-line therapy for routine treatment of benign cutaneous disease. Charged particle therapy is also commonly used in cancer treatment, and includes both electrons, which are commonly available, and protons, which are available at select regional centers. Electrons are the product of the same linear accelerators used to produce megavoltage energy photons. Electron beams are commonly used in dermatologic applications because they deliver a high skin-surface dose and, unlike photons, the deposited dose rapidly falls to negligible values at depth in tissue. Different electron energies can be used to deliver therapeutic doses from 1 to 5 cm deep in tissue, and deeper tissues can be completely spared.
29
Depth dose distributions
Photons: 10 × 10 cm2
120
18 MV 10 MV 6 MV
100
80
DD (%)
60
40
20
0
0
5 10 15 20 25 30
Depth (cm)
A
Electrons: 10 × 10 cm2
120
20 MeV 16 MeV 12 MeV 9 MeV 6 MeV
100
80
DD (%)
60
40
20
0
0 5 10 15 20 25 30
Depth (cm)
B
3688
delivered to deep tumor targets, with less incidental radiation of surrounding normal tissue. Like electrons, protons have a negligible exit dose, but unlike electrons, protons can be delivered to deep targets while sparing the overlying skin.
MODULATION OF EXTERNAL-BEAM RADIATION
Radiation treatment planning involves a complex set of decisions regarding the appropriate radiation modality, radiation energy, beam orientation, patient positioning, and the choice of treatment devices. The choice of device can help increase the radiation dose to targeted structures and block or reduce radiation exposure of normal tissue. “Bolus” is tissue-density material commonly used in radiation treatment of superficial skin malignancies. It can be custom designed in varying thicknesses and applied to the patient’s skin during daily treatment. It serves several potential purposes: for higher-energy X-rays (eg, megavolt energy), or low-energy electrons, the surface dose is low compared to that in deeper tissue. By using the appropriate thickness of bolus, the skin dose can be raised to therapeutic levels (Fig. 200-2). Another function of bolus is to attenuate the incident beam to lower the dose that reaches deeper structures; for example, during treatment of a skin cancer on the
A
29
B
temple, the dose that reaches the underlying brain is decreased. Bolus material also can be used to compensate for complex topography and to smooth the dose distribution for treatment of the skin around the nose and ears (Fig. 200-3). Beams can be shaped by a variety of devices depending on their energy. Megavoltage treatment beams may be shaped by custom-designed, 7-cm thick, lead alloy blocks to conform to the desired shape; most modern linear accelerators have a multileaf collimator (MLC), which contains sliding leaves of tungsten that conform to the desired treatment aperture. Electron-beam radiation is normally blocked with custom-made lead or lead alloy blocks. Orthovoltage radiation is blocked using much thinner custom lead shielding, typically placed on the patient’s skin. Figure 200-4 shows an example of a custom blocking device for superficial radiation. Traditionally, external-beam radiation beams are designed using blocks or static MLCs to conform to a target that is delineated clinically or using CT or other imaging. Multiple beams, beam angles, and energies are chosen to avoid specific normal structures, and the dose is calculated with iterative changes until an acceptable plan was generated. An “inverse planned” method is now increasingly used when the tumor target lies in proximity to a dose-limiting structure. Intensity-modulated radiation therapy incorporates individual radiation beams that are not static; the aperture changes during the treatment to finely adjust beam fluence. This requires a dynamic MLC, in which the leaves slide during beam-on time. During the pretreatment planning phase, the treating physician contours the target volume and those
of the normal tissue organs at risk. Dose constraints for each contoured structure are chosen, and the physician, physicist, and dosimetry staff use dedicated treatment planning software algorithms to optimize the treatment plan. This is a time-intensive, expensive technique that can generate plans to treat complex-shaped tumor targets and spare adjacent, critical, normal tissue structures.
3689
29
MECHANISM OF ACTION
The most common forms of radiotherapy used in clinical practice are X-rays and γ-rays. Both represent photon particles or electromagnetic waves that differ only in the method of their generation: γ-rays are emitted by nuclear reactions, whereas X-rays are emitted by energy transitions in orbital electrons. Ionizing radiation includes that part of the electromagnetic spectrum of sufficient energy to impart energy to target tissue by the ejection of orbital electrons. This is the primary means of energy absorption in human tissue following exposure to therapeutic radiation. As cells are largely composed of water, it is in water molecules that the majority of the ionization occurs, which results in the generation of short-lived free radicals such as hydroxyl radicals. Consequently, the effectiveness of radiation in tissue is dependent upon the availability of oxygen. This is clinically manifest in the reduced radiation response in hypoxic tissue, and is the reason that higher radiation doses are used in the postoperative setting when there is diminished microcirculation. The primary mediator of cell death in response to ionizing radiation, in both tumor and normal tissue, is damage to DNA by indirect ionization by radiationinduced free radicals.2 Indirect DNA damage is characteristic of sparsely ionizing radiation, including not only X-rays, but also commonly used charged particles such as electron and proton therapy. In contrast, densely-ionizing radiation (eg, neutrons, α particles) with a higher linear energy transfer deposit their energy densely along their incident tracks, and more commonly induce double-strand DNA breaks directly, without the intermediate ionization of cellular water. The initial deposition of radiation energy in tissue and the resulting DNA damage occur within thousandths of a second of exposure. The biologic response to DNA damage includes modulation of cell death, differentiation, survival pathways, and activation of DNA repair. These biologic processes occur orders of magnitude more slowly than the initial DNA damage. The ultimate cellular response to radiation can be repair, senescence, differentiation, or cell death. Cell death may occur via apoptosis, a relatively rapid process, but more commonly occurs as mitotic cell death. Misrepair of double-strand DNA breaks generates chromosomal abnormalities, and cells die during failed mitosis, often several generations later.
DOSE AND FRACTIONATION SCHEDULE
The Systéme International d’Unites (SI) unit of radiation dose is the gray (Gy), which is defined as 1 joule (J) of energy absorbed per kilogram of tissue. An alternate unit of absorbed dose, largely replaced by the gray, is the rad (an acronym for radiation absorbed dose); 1 Gy is equal to 100 rads. Dose is specified to the target
3690
volume as defined by the treating radiation oncologist. Most epithelial malignancies are treated to a total dose in the range of 50 to 80 Gy; lymphoid malignancies typically respond to doses of 15 to 40 Gy. Select benign conditions can be treated with lower doses; hypertrophic scars and keloids are commonly prescribed doses in the range of 4 to 20 Gy. Fractionation refers to the delivery of specified radiation dose in temporally separate treatments, and is recommended to both increase the efficacy of effects on target tissue and to allow normal irradiated tissue to repair radiation damage. Thus, the schedule of radiation fractionation can be used to both increase efficacy of the dose to the target and minimize radiation damage to normal tissue. Common fractionation schemes using conventional radiotherapy deliver treatments at intervals ranging from twice daily to once per week. The effectiveness of radiation treatment is highly dependent upon the treatment schedule; both the total number of days over which the treatment is spread and the fraction size. The common daily fraction size is 1.8 to 2 Gy per day, given 5 days per week. Different fractionation schedules can be compared using a mathematical conversion to a biologically effective dose (BED), using a formula that accounts for the number of fractions, fraction size, and the DNA-repair characteristics of the target tissue. Commonly used dose-fractionation schedules for cutaneous malignancies include 60 Gy in 30 fractions, and 48 Gy in 12 fractions. The BED to the tumor is similar, but the dose of 48 Gy in 12 fractions would be expected to have more-severe acute and late side effects.
CLINICAL AND MOLECULAR ASPECTS OF RADIATION DERMATITIS
Skin changes after radiation exposure follow a predictable course dictated by radiation dose, timing, and the biology of the human inflammatory reaction.3 The earliest reaction is erythema that may occur and resolve within hours, and is normally only evident after relatively high-dose exposure. The threshold dose is 2 Gy or greater skin dose, and is not normally noted after daily fractionated treatment of visceral organs with skinsparing megavoltage radiation. This effect is noted in therapeutic courses aimed at cutaneous targets, where the skin receives full dose, or during treatment regimens that use large fraction sizes. Microscopically, there is a vasodilation and a transiently increased capillary permeability that results in mild erythema and edema at 2 to 24 hours following exposure. Prior to the adoption of SI units of radiation dose, skin erythema dose (SED) was used as a crude clinical measure of patient radiation exposure. This transient acute reaction is no longer commonly noted because of the increased use of high-energy, relatively skin-sparing radiation energies, and the increased use of lower fraction sizes. Acute, transient skin erythema is still reported following
interventional diagnostic and therapeutic procedures with prolonged fluoroscopy times. The more sustained, common, and relevant reactions take place over a matter of weeks during and even shortly after fractionated radiation therapy. Acute radiation dermatitis progresses through characteristic stages of severity based on the accumulation of radiation-induced changes to dermal vasculature, appendageal structures, epidermal stem cells, and the activation of inflammatory pathways. Radiation dermatitis is a distinct adverse event graded by the National Cancer Institute’s Common Terminology Criteria for Adverse Events (CTCAE). This scale is graded on severity, and primarily describes the acute reaction of skin exposed to therapeutic radiation. Chronic skin changes may occur months to years after exposure, and include a spectrum of changes characterized by fibrosis and atrophy. Table 200-1 summarizes the common acute and late adverse events attributable to radiation. Grade 1 dermatitis first manifests as faint skin erythema within the treatment area. Erythema is seen in two contexts: first, there may be a transient vasodilation in the hours after a single fraction skin exposure of 2 Gy or higher. More commonly, erythema or hyperpigmentation develops over the first 2 to 3 weeks of fractionated radiation with accumulated exposure. Vasodilation and increasing vascular permeability occur early, and the resulting perivascular inflammation results in clinically characteristic erythema and edema. Moderate-to-brisk erythema is grade 2. With continuing or higher-dose radiation exposure, damage to the basal cells in the epidermis may progress until this stem cell population is lost in localized areas, which results in dry desquamation (CTCAE grade 1). Further damage to the basal layer leads to
29
more widespread desquamation, and the production of a fibrinous exudate resulting from increased arteriole permeability, loss of basement membrane integrity, and edema in the underlying dermis. This is characteristic of moist desquamation. The CTCAE differentiates moist desquamation based on whether it is patchy and localized to areas subject to trauma such as skin folds (grade 2), or confluent and present in a more widespread area (grade 3). Radiation damage to the underlying dermis may lead to ulceration, bleeding, and/or necrosis (grade 4). Skin adnexal cells are relatively radiosensitive and may not regenerate following exposure. The process of epilation begins within days of radiation exposure. Sebaceous glands have similar sensitivity, and eccrine sweat glands become dysfunctional shortly afterward in a fractionated radiation treatment course. Histologically, these glandular structures demonstrate apoptosis, necrosis, and loss of normal mitotic activity. Chronically, there can be fibrotic replacement and loss of the supporting microvasculature. This leads to both acute and chronic hypohidrosis or anhidrosis. Regeneration of areas of desquamation occurs through replacement of epidermal basal cells, either from islands of intact cells within the epidermis or by the migration of such cells from adjacent, uninvolved areas. Normal healing of the radiation wound becomes clinically evident approximately 2 weeks after exposure, consistent with the basal cell turnover time. Widespread confluent moist desquamation (grade 3), or more severe toxicity, such as necrosis of the epidermis or underlying dermis, may not undergo complete regeneration of the structural and adnexal elements. Instead, there can be prolonged inflammation, fibroblast activation, and collagen deposition. This fibrosis is often termed a consequential late effect, because it is a consequence of the severity of the acute reaction. It
ADVERSE EVENT GRADE 1 GRADE 2 GRADE 3 GRADE 4 GRADE 5
Radiation dermatitis
Faint erythema Moderate-to-brisk erythema Moist desquamation (other than skin folds and creases)
Dry desquamation Patchy moist desquamation (mostly confined to skin folds and creases)
Skin necrosis Death
Bleeding induced by minor trauma or abrasion
Ulceration of full thickness of dermis
Moderate edema
Spontaneous bleeding
Alopecia Visible on close inspection Hair loss ≥50% of normal — — —
Atrophy Associated with telangiectasia or pigmentation changes
Striae or adnexal structure loss Ulceration — —
Induration or
Mild, able to pinch
Moderate, able to slide skin
Severe, unable to slide
Generalized,
Death
Induration or fibrosis Mild, able to pinch skin Moderate, able to slide skin but unable to pinch Severe, unable to slide or pinch, limiting self-care
fibrosis
skin
but unable to pinch
Generalized, impaired breathing or feeding
Death
or pinch, limiting self-care
impaired breathing or feeding
3691
29
is in contrast to the more common late fibrosis, which arises following the regeneration of relatively normalappearing skin and can occur years after treatment. Late radiation toxicity occurs months to years following exposure, following a period during which the skin may not exhibit significant abnormalities. The risk and severity of true late skin changes are a function of the irradiation dose and volume. A landmark study of normal tissue radiation tolerance determined that the risk of grade 4 or greater toxicity (ie, ulceration or necrosis) was 5% when 10 cm2 of skin was treated to 70 Gy, or when 30 cm2 was treated to 60 Gy.4 Comorbid medical disease may exacerbate this risk; clinical risk factors associated with increased symptom severity include advanced patient age, diabetes, peripheral vascular disease, and tobacco use.5 The concurrent administration of radiosensitizing drugs significantly increases the severity of acute radiation dermatitis and prolongs healing of the radiation wound. Collagen vascular diseases with a fibrotic cutaneous component (eg, scleroderma and systemic lupus erythematosus) are associated with a pronounced and often debilitating late subcutaneous fibrosis following radiation treatment.6,7 Certain genetic syndromes, particularly inherited defects in DNA damage repair (eg, ataxiatelangiectasia), predispose to a severe, acute, and late radiation response in exposed normal tissue. The late skin toxicity with the most functional consequence is subcutaneous fibrosis. Replacement of the subcutaneous adipose tissue with fibrous tissue leads to loss of normal range of motion, contraction, pain, and poor cosmesis. Even in cases where dermal and subcutaneous fibrosis is not clinically evident, there may be atrophy of skin adnexa. Hair follicles as well as sebaceous and sweat glands may be absent in previously-irradiated skin, because these are not regenerated during normal radiation wound repair. Loss of glandular elements leads to anhidrosis when extensive skin areas are irradiated, such as in totalskin electron therapy. The microvasculature of the dermis and subcutis may exhibit abnormal myointimal proliferation, leading to hypoperfusion. Tortuosity within small vessels and microthrombi result in visible telangiectasia. Irregular regeneration of the basal layer of the epidermis may be evident as dyspigmentation. Paradoxically, there may be a decrease in the population of resident skin fibroblasts in atrophic skin, resulting in loss of the normal collagen structure leading to impaired tissue remodeling, increased skin fragility, and poor wound healing. The pathophysiologic mechanism of late changes, particularly fibrosis, in response to radiation is incompletely understood.8,9 Transforming growth factor-beta (TGF-β) is a secreted protein that serves a complex regulatory role in normal tissue inflammation and remodeling by controlling proliferation, differentiation, and secretory function. TGF-β levels are increased within hours of radiation exposure, and this elevation has been correlated with late fibrotic changes. Abrogation of downstream mediator SMAD3 (Sma- and Mad-related protein 3), a proinflammatory signaling molecule induced in response to TGF-β,
3692
appears to protect tissue from late fibrotic changes after radiation exposure in laboratory models. TGF-β is a complex regulator of inflammation that increases fibroblast proliferation, differentiation, and activation, thereby increasing secretion of extracellular matrix components. TGF-β promotes its own secretion by fibroblasts in a self-amplifying cascade and decreases the production of matrix proteinases. Epithelial cell proliferation is diminished, and there is chemotaxis of mast cells and macrophages. The result is increasing production, processing, and deposition of collagen (fibrosis) and loss of epithelial reconstitution of normal tissue structure. The initiating event in TGF-β activation in response to radiation is poorly understood. Latent TGF-β in the extracellular matrix may be activated by proteolytic enzymes that act in the presence of radiation-induced reactive oxygen species. Other potential sources of TGF-β include endothelial cells, fibroblasts, epithelial cells, and tissue macrophages, which may release TGF-β in direct response to radiation or as a generalized response to tissue damage.
RADIATION RECALL REACTIONS
Radiation recall is a phenomenon that was first described several decades ago. Radiation recall is a cutaneous reaction, in response to specific systemic agents, in the area of previous radiation exposure. The most commonly cited chemotherapeutic agents are anthracyclines, taxanes, and gemcitabine. Other systemic agents implicated in radiation recall reactions include standard chemotherapeutic agents, newer targeted therapeutics, and hormonal agents as well as nononcologic medications; Table 200-2 lists these agents based on case reports. The clinical manifestations of radiation recall occur with the initial administration of the systemic agent— within minutes to days with IV drug, or days to weeks with oral medication. The timing of presentation may be related to the drug dose, and both the severity and timing of the reaction may be related to the prior radiation dose. The duration of the response may range from weeks to months. Interestingly, readministration of the same systemic agent does not consistently lead to recurrence of the phenomenon.10
Although a recall reaction can occur in any organ, skin is the most common site. It occurs in a welldemarcated area defined by the borders of the previous treatment field and can occur despite the lack of any clinically significant skin reaction during the previous radiation treatment. The clinical signs and symptoms mimic an acute radiation dermatitis, ranging from erythema to desquamation and necrosis. A localized maculopapular rash, characteristic of a hypersensitivity reaction, also has been described. The pathogenesis of radiation recall is not well understood. An early hypothesis was that tissue stem cells remained depleted long after radiation, making the tissue more sensitive to cytotoxics. This does not explain,
Agents implicated in inducing a radiation recall reaction include chemotherapy drugs, targeted and hormonal agents, and nononcologic medications.
■Chemotherapy
■Chemotherapy
■Arsenic trioxide
■Arsenic trioxide
■Bleomycin
■Bleomycin
■Capecitabine
■Capecitabine
■Cyclophosphamide
■Cyclophosphamide
■Cytarabine
■Cytarabine
■Dacarbazine
■Dacarbazine
■Dactinomycin
■Dactinomycin
■Daunorubicin
■Daunorubicin
■Docetaxel
■Docetaxel
■Doxorubicin
■Doxorubicin
■Epirubicin
■Epirubicin
■Etoposide
■Etoposide
■Fluorouracil
■Fluorouracil
■Gemcitabine
■Gemcitabine
■Hydroxyurea
■Hydroxyurea
■Idarubicin
■Idarubicin
■Lomustine
■Lomustine
■Melphalan
■Melphalan
■Methotrexate
■Methotrexate
■Paclitaxel
■Paclitaxel
■Vinblastine
■Vinblastine
■Targeted anticancer drugs
■Targeted anticancer drugs
■Bevacizumab
■Bevacizumab
■Pemetrexed
■Pemetrexed
■Hormonal agents
■Hormonal agents
■Tamoxifen
■Tamoxifen
■Nononcologic drugs
■Nononcologic drugs
■Gatifloxacin
■Gatifloxacin
■Isoniazid
■Isoniazid
■Levofloxacin
■Levofloxacin
■Simvastatin
■Simvastatin
however, radiation recall reactions elicited by noncytotoxics or, in some cases, the lack of a reaction to subsequent drug exposure. The clinicopathologic manifestations are best explained by a localized, acquired hypersensitivity reaction. Prior radiation therapy may alter the normal dermal immunologic response by changing basal and stimulated cytokine production. This is consistent with histologic findings of acute inflammation (eg, vasodilation, infiltration of inflammatory cell mediators) in affected tissue. Radiation recall dermatitis responds to treatment with topical or oral corticosteroids.
CLINICAL APPLICATIONS OF RADIATION
BENIGN DISEASE
BENIGN DISEASE
The use of ionizing radiation for benign disease has decreased considerably, because of improvements in alternative therapy and an increasing awareness of the rare, but serious, side effects of radiotherapy.11 Rare
29
but serious side effects include fibrotic changes in the affected skin and, more significantly, a risk of secondary malignancy. It is estimated that the relative risk of malignancy following radiation treatment increases by 10% to 50%; the absolute risk, however, remains very low. These malignancies occur at a median of 10 years following treatment. The risk appears to be greater in younger patients, and in those patients whose treatment was targeted to anatomic areas at highest risk for malignancy (eg, breast or thyroid tissue). For this reason, radiotherapy should be (a) considered in benign disease only after other therapeutic options have been exhausted; (b) avoided when possible in children and young adults; and (c) delivered with attention to sparing radiation exposure to sensitive normal tissue. Radiotherapy is effective for symptomatic treatment of several inflammatory dermatoses, including eczema, psoriasis, and lichen planus, at relatively low-dose exposures (ie, less than 10 Gy of fractionated treatment). Inflammatory dermatoses are rarely treated with radiation, given the number of other antiinflammatory options. Benign lymphoproliferative disorders are sensitive in a similar fashion, and disorders such as lymphomatoid papulosis, lymphoid hyperplasia, and lymphocytoma cutis have an excellent response to radiotherapy. These may be treated with radiation after other options have been exhausted, and are approached using lymphoma regimens. Other benign proliferative processes that can be treated with radiotherapy include keratoacanthomas and hemangiomas. Table 200-3 lists the diagnoses for which radiotherapy may be indicated. A number of large series and one randomized trial have examined the efficacy of localized, lowdose irradiation for the prevention of recurrence of
Benign Malignant
Eczema Squamous carcinoma
Psoriasis Basal cell carcinoma
Lichen planus Melanoma
Benign lymphoid hyperplasia Merkel cell carcinoma
Keratoacanthoma Eccrine and apocrine carcinoma
Keloids/hypertrophic scars
Cutaneous T-cell and B-cell lymphomas
Kaposi sarcoma
Angiosarcoma
Premalignant
Actinic keratoses
Lentigo melanoma
Bowen disease
Erythroplasia of Queyrat
Lymphocytoma cutis
Lymphocytoma cutis
3693
aRadiotherapy is not recommended as first-line therapy for all the listed indications, particularly the benign disorders.
29
hypertrophic scars or keloids following excision.12-14
This should be undertaken after failure of more conservative therapies. The most common treatment regimen is to use kilovoltage X-rays or electrons to a total dose of 10 to 20 Gy delivered over several days. The treatment is usually initiated within 24 to 48 hours of excision. The recurrence risk after surgery and radiation is approximately 20% or less. The use of radiation without excision on existing keloids is not as effective.
MALIGNANT DISEASE
MALIGNANT DISEASE
BASAL CELL CARCINOMA AND SQUAMOUS CELL CARCINOMA
Radiation has been used as primary treatment for basal and squamous cell carcinoma, as an alternative to excision, with local control rates of 90% or greater for small lesions.15 There is concern for progressive late skin atrophy and necrosis decades after radiation, and for this reason surgical excision is usually thought to be a better option in younger patients (ie, those younger than age 55 years). The control rate for primary treatment is a function of tumor size and T stage. For small lesions, radiation is thought to offer local control that approximates the control seen with excision. Radiation is also an effective adjuvant treatment, following excision or Mohs micrographic surgery. The clearest indication for adjuvant treatment is a positive surgical margin; other considerations include tumor depth greater than 4 mm in the case of squamous cell cancer or tumor size greater than 2 cm. Involvement of cartilage or bone is a strong predictor of local recurrence and consensus guidelines recommend adjuvant treatment. Perineural invasion correlates with both local and nodal recurrence following excision and is a relative indication for treatment.16,17 Involvement of large, named nerves should prompt consideration of extension of the clinical target volume to include the proximal nerve tract. Other relative indications for treatment include poorly-differentiated tumors, adenosquamous subtype, and limitations imposed on excision by anatomic location. Patient factors include the presence of neurologic symptoms, implying underlying nerve involvement, and immunosuppressed host status. For squamous cell carcinoma, locally-advanced lesions may have a significant risk of nodal metastasis. In patients being treated adjuvantly or definitively for locally-advanced primaries with risk factors, draining lymphatics should be electively included. Dose fractionation schemes represent a balance between patient convenience and the relative risk of poor cosmesis. A total of 60 to 66 Gy in 2-Gy fractions is appropriate for gross disease, with higher doses indicated for lesions larger than 2 to 4 cm. Published experience with relatively hypofractionated treatment has shown equivalent locoregional control after 45 to 50 Gy in 2.5-Gy fractions, or radiobiologically equivalent doses in fraction sizes of 3 or 4 Gy.
3694
Tumors or postoperative areas that are at superficial depth may be treated with orthovoltage radiation to spare the deeper normal tissue. An alternative is electron therapy with the appropriate bolus to maximize the surface dose. When the target volume is deeper, then megavoltage X-rays, with appropriate bolus, may be required. Target structures such as lymph node basins or nerve tracts, in close proximity to critical normal structures, may require intensity-modulated radiation therapy.
MELANOMA
The role of radiotherapy in the management of localized melanoma has not been conclusively established. Radiotherapy is frequently used for palliation of unresectable lesions, and there is evidence that selected patients at increased risk of local or regional failure may reduce that risk with adjuvant radiation.18 Risk factors predictive of local relapse after wide excision include tumor thickness greater than 4 mm, ulceration, satellitosis, positive surgical margins, mucosal origin, perineural invasion, and desmoplastic histology. Patients with positive lymph nodes at high risk of recurrence after node dissection may benefit from postoperative radiation directed at the nodal basin.19,20
Melanomas are frequently treated with hypofractionated radiation, with fraction sizes of 4 to 6 Gy (ie, 30 Gy in 5 fractions) using megavoltage X-rays. The recurrence risk for melanoma after radiation is significantly higher than that for squamous or basal cell carcinoma.
CUTANEOUS LYMPHOMAS
Cutaneous T-cell lymphomas include numerous subtypes, the most common of which are mycosis fungoides (MF) and anaplastic large-cell lymphoma. MF is exquisitely sensitive to radiotherapy and patients may present with localized or disseminated skin disease. Anaplastic large-cell lymphoma (CD30-positive) is also a common cutaneous T-cell lymphoma, but has a lower incidence than MF. The clinical presentation is also somewhat different, and these cells generally demonstrate a CD4-positive phenotype (which can be seen in MF), and also express cutaneous lymphocyte antigen. As opposed to MF, these cells are typically not epidermotropic and do stain positive for CD30. Lymphomatoid papulosis is also CD30 positive and may be associated with anaplastic large-cell lymphoma. Anaplastic lymphoma kinase is usually not overexpressed in patients suffering specifically from cutaneous lymphoma of the CD30-positive variety, though it may be expressed in patients with noncutaneous anaplastic large-cell lymphoma. There are also a variety of subtypes of cutaneous B-cell lymphoma, but the most commonly encountered are diffuse large B-cell, marginal zone, and follicular center cell. Diffuse large B-cell lymphoma may express CD20 and CD79, and lesions involving the lower extremities may express BCL-2, BCL-6, and MUM-1.
Marginal zone lymphoma can be identified via expression of CD20 and CD79 and often BCL-2, but typically BCL-6 is not noted as a marker in this case. The follicular center cell variant may express CD20 and CD79, but expression of BCL-2 and MUM-1 is unusual. Localized radiotherapy fields may be incorporated into the management of patients with limited disease, but in some cases, patients have extensive areas of skin which are involved and a total skin electron beam therapy (TSEBT) technique may be incorporated for adequate disease control. Localized radiotherapy is typically provided using an electron technique and bolus material is applied to the skin in an effort to maintain an appropriate deposition of dose at the skin surface. Typically the 90% isodose curve is used to provide homogeneous coverage of the skin area in question and margins of 2 to 3 cm radially are incorporated into the treatment plan. Doses of 20 to 30 Gy in 2-Gy fractions are used. With this type of regimen for most cutaneous B-cell lymphomas, the complete response (CR) rate is greater than 95% with 5-year local control of approximately 75%.21,22
Some patients may not be able to logistically receive daily therapy over several weeks, but are in need of palliation of lesions that are bleeding, uncomfortable, unsightly, or impairing function. Such patients may be candidates for an abbreviated regimen of 2 Gy × 2 for a total of 4 Gy, which has been found to provide excellent response rates with reasonable durability in selected patients with low-grade cutaneous B-cell lymphoma.23
TSEBT is significantly more complicated to provide and is typically used in patients suffering from extensive MF. TSEBT provides excellent response rates for patients with various levels of disease and also has been successful in patients with tumors of the skin, assuming that a supplemental boost is provided to the region involved by tumor. MF patches and plaques have an excellent response rate of 100% to TSEBT. The CR rate is variable and decreases with the degree of thickness associated with cutaneous lesions. Historically, the course of therapy is provided over approximately 8 to 10 weeks and, based on a Stanford technique, involves 36 fractions to the total skin using 6 fields with blocking of the eyes, hands, fingernails, and feet based on dosimetric parameters resulting from the individualized treatment program.24 Newer data demonstrating excellent results with only 12 Gy have been published.25 An advantage is that the course is much shorter and toxicities decreased compared with the 36-Gy regimen. The patient is treated in a variety of standing positions. Given its degree of complexity, TSEBT is best performed in centers that have a significant amount of experience with the technique. An important feature to be considered following response to TSEBT is a maintenance program, and such maintenance can be provided in a variety of forms. For MF patients with T1-level and T2-level disease, effective regimens, which have been documented in the literature, include the use of psoralen and ultraviolet A and mechlorethamine. Both cutaneous T-cell and B-cell lymphomas are very sensitive to radiotherapy, and it is generally accepted
29
that all lesions will respond and that localized cutaneous B-cell lymphoma lesions have a CR rate approaching 100%. Cutaneous T-cell lymphoma lesions have CR rates that are also excellent but are more dependent on extent of disease.
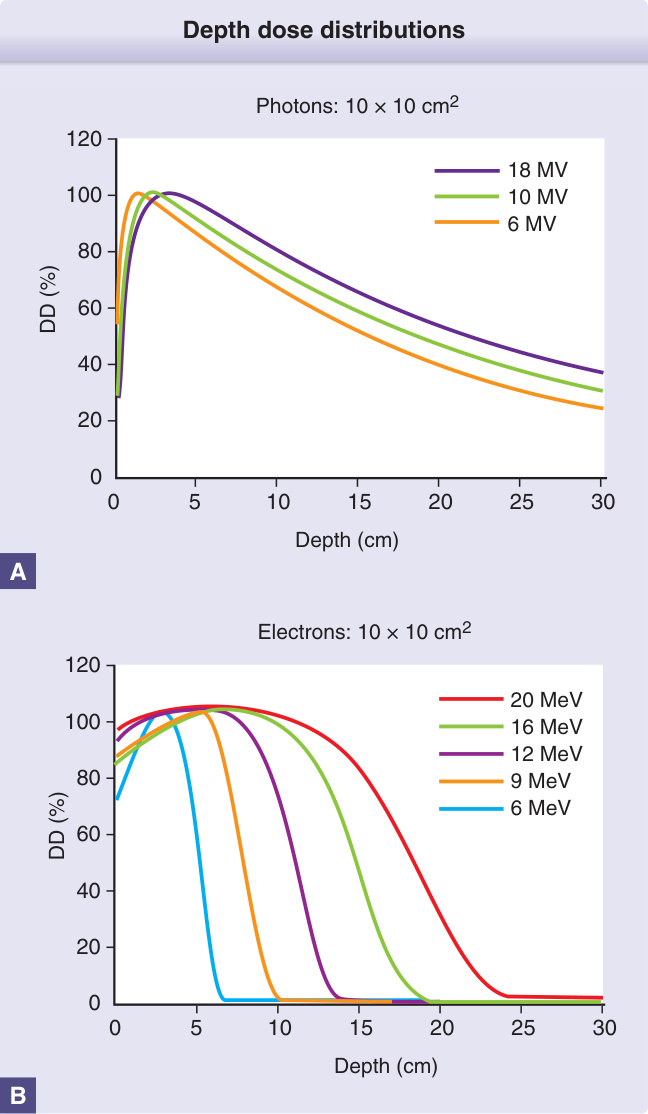
Figure 200-1 Depth dose distributions. A, The percent of the maximum radiation dose (DD) deposited at depth in tissue (in cm), as a function of the photon (X-ray) energy. As photon energy increases, the percent dose at superficial depth decreases, and the percent dose in deeper tissue increases. MV, megavolt. B, A similar relationship for electron therapy. In contrast to photons, the percent dose deposited at both superficial and deep tissue increases with electron energy. Note the difference in scale; electron energy is almost completely absorbed at shallower depths, compared to photons. MeV, million electron volts.
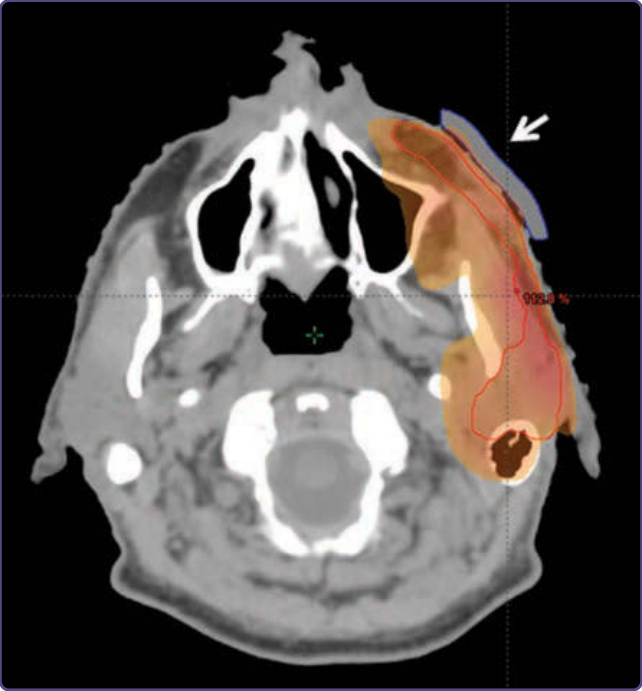
Figure 200-1 Depth dose distributions. A, The percent of the maximum radiation dose (DD) deposited at depth in tissue (in cm), as a function of the photon (X-ray) energy. As photon energy increases, the percent dose at superficial depth decreases, and the percent dose in deeper tissue increases. MV, megavolt. B, A similar relationship for electron therapy. In contrast to photons, the percent dose deposited at both superficial and deep tissue increases with electron energy. Note the difference in scale; electron energy is almost completely absorbed at shallower depths, compared to photons. MeV, million electron volts.
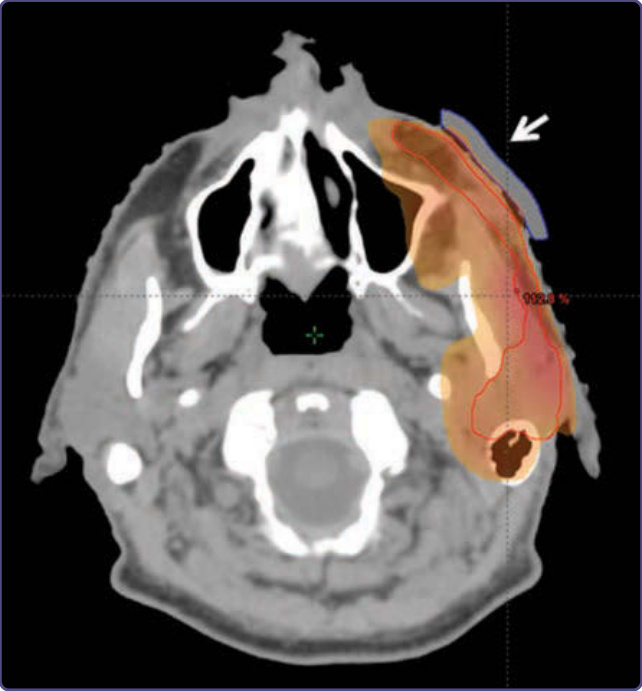
Figure 200-2 Bolus to increase the skin dose. A 61-year-old male underwent resection of a deeply invasive squamous cell carcinoma overlying the zygoma with involvement of parotid lymph nodes and facial nerve. The tumor bed was treated, along with the remaining parotid gland and course of the facial nerve, using megavoltage photons. A tissue-density bolus (white arrow) was placed over the tumor bed to increase the skin dose to 100% in that area.
Figure 200-3 Bolus as a tissue compensator. A deeply invasive basal cell carcinoma was excised from the left nasal ala. A, The patient was immobilized for treatment in a thermoplastic mask. A rectangular, tissue-density box was constructed to overlay the nose and compensate for the irregular tissue contours in this area. B, The patient was treated with right and left lateral megavoltage photon beams, weighted left greater than right. The 100% isodose line (red line) covers the tumor bed (red-shaded area) with full dose at the skin surface and good dose homogeneity.

Figure 200-4 A custom lead shield that would be placed on the patient’s face, with a cutout to allow orthovoltage treatment of a cutaneous malignancy of the left lower eyelid.
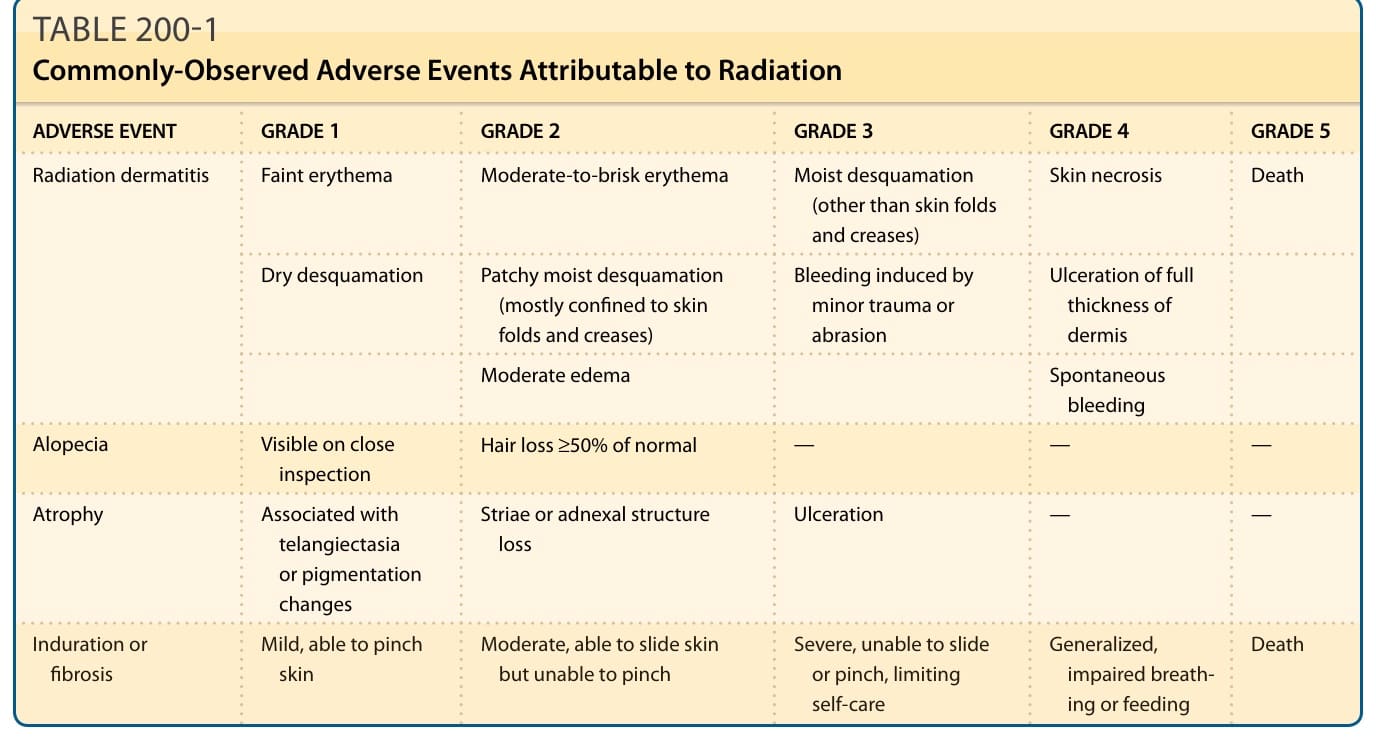
TABLE 200-1 Commonly-Observed Adverse Events Attributable to Radiation
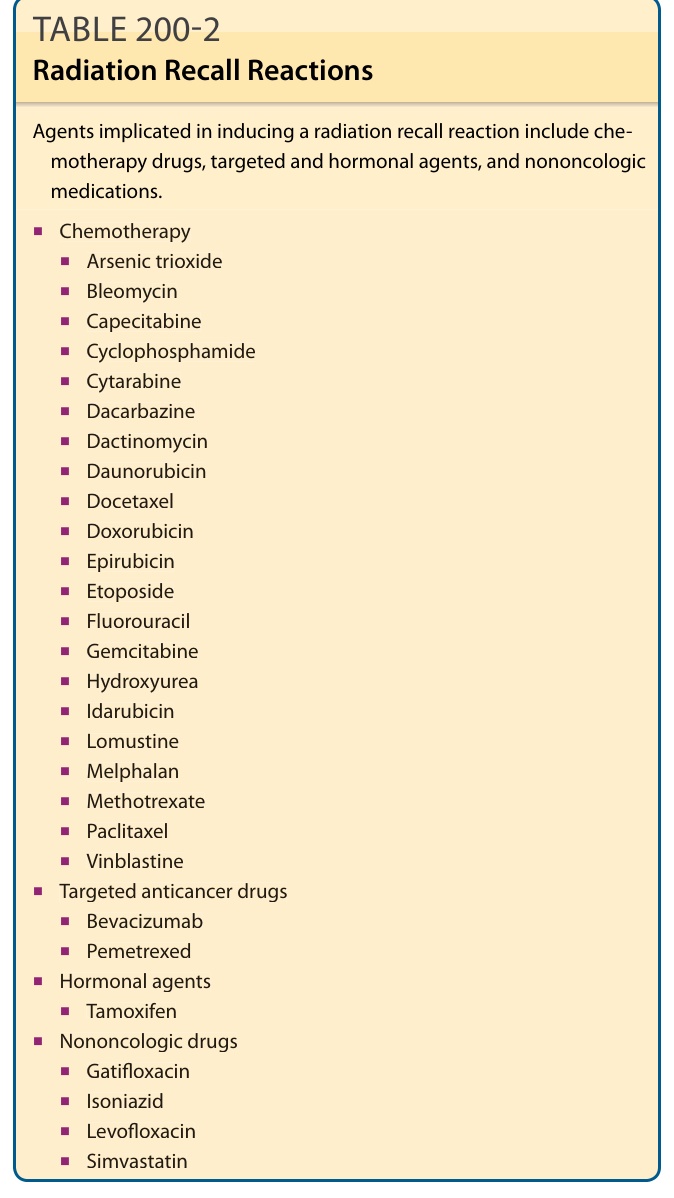
TABLE 200-2 Radiation Recall Reactions
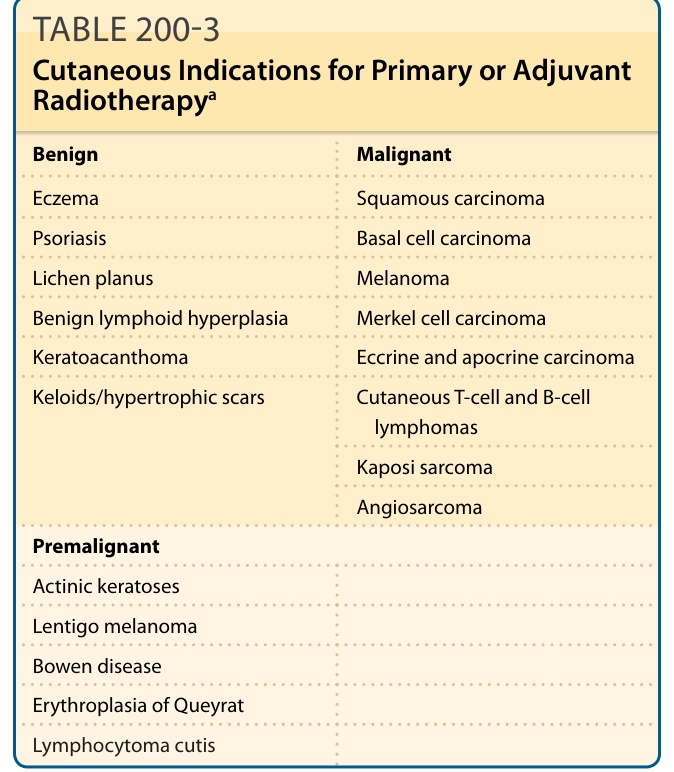
TABLE 200-3 Cutaneous Indications for Primary or Adjuvant Radiotherapya