Phototherapy
PART29
Physical Treatments
AT-A-GLANCE
The main wavelengths used for phototherapy include broadband ultraviolet B (BB-UVB), narrowband UVB (NB-UVB), ultraviolet A (UVA) 1, and UVA for psoralen photochemotherapy (PUVA); these have different depths of penetration and interact with a specific range of molecules rendering unique photobiologic properties with respect to potency, side effects, and diseases in which they are effective. Targeted therapy devices can deliver distinct wavelengths of ultraviolet radiation to only lesional skin. Such devices that can deliver wavelengths of UVR at or close to those that are most effective at clearing localized atopic dermatitis, psoriasis, vitiligo, and cutaneous T-cell lymphoma have been evaluated, and are being used clinically. Sunburn-like reactions are the most common short term adverse effect of phototherapy. UVB phototoxicity usually peaks at 12 to 24 hours and PUVA reaction manifests at 24 to 48 or even 72 hours. Importantly, except for PUVA therapy for which formal long term follow up studies established an increased risk of lentigines, squamous cell carcinoma, and possibly melanoma, other forms of phototherapy appear to be remarkably safe.
MECHANISMS OF PHOTOTHERAPY
Phototherapy is the use of ultraviolet radiation or visible light for therapeutic purposes. Its beneficial effects in vitiligo were first recognized thousands of years ago in India
and Egypt and its activity is now well-established for a variety of other dermatologic conditions. The enduring appeal of phototherapy is based on its relative safety coupled with an ongoing interest in its molecular and biologic effects. The expanded use of phototherapy for dermatologic and nondermatologic conditions can be attributed to the following factors: identification of photosensitizers with unique photochemical properties; development of novel methods for the delivery of light to cutaneous and noncutaneous surfaces; and manufacture of light sources that emit selective wavelengths of radiant energy. The main phototherapeutic devices that are in use today (aside from lasers, high-output incoherent light sources, and visible light sources employed for photodynamic therapy) include broadband ultraviolet B (BB-UVB), narrowband UVB (NB-UVB), ultraviolet A (UVA) 1, and UVA for psoralen photochemotherapy (PUVA). Ideally, these devices used for therapeutic ultraviolet radiation (UVR) should be safe, efficient, and cost-effective. Therefore, understanding the basic principles of these devices is important for dermatologists and other providers using phototherapy for the management of dermatologic diseases.1,2
The distinct wavelengths of UVR used for phototherapy have different depths of penetration and interact with a specific range of molecules. As a consequence, each form of phototherapy has unique photochemical and photobiologic properties with respect to potency, side effects, and diseases in which they are effective (Fig. 198-1). Most UVB radiation (290 to 320 nm) is absorbed superficially by the epidermis and superficial dermis (Fig. 198-2). In white skin, less than 10% of UVB radiation is transmitted beyond 14 microns.3 This particular wavelength of radiant energy produces many different types of DNA damage, including pyrimidine dimers and 6,4-pyrimidine-pyrimidone photoproducts. These by-products are thought to be particularly important for both UVB’s efficacy and toxicity.4 UVB also causes
29
Summary of effects from ultraviolet A (UVA), psoralen and ultraviolet A (PUVA), or ultraviolet B (UVB) treat
Mast cells Immune system
Mast cell membrane stabilization
Increased IL-10
Decrease histamine release
Phototherapy (UVA, PUVA, UVB)
Melanocytes
Collagen Keratinocytes
Stimulates cytokeratins 15 and 19
Increased ROS
Acanthosis
Thickening of stratum corneum
Increased IL-1, IL-6
Increased cyclooxygenase-2
Mast cell apoptosis
Increased prostaglandin E2
Melanogenesis
Increased MMP-1
Decreased dendritic cell activity
Decreased PGD2
T-cell apoptosis in lymphoid infiltrates
Decreased CD54 expression
Inhibition of effector T-cell activation
Diminished cellmediated immune response
Effective in mast cell–mediated diseases
Effective in T-cell hyperactive conditions
Collagen degradation
Skin “hardening”
Repigmentation
Effective in some disorders of hypo- or depigmentation
Effective in sclerotic skin diseases
Atopic dermatitis
Telangiectasis Macularis eruptiva perstans
Psoriasis
Lichen planus
Cutaneous T-cell lymphoma
Urticaria pigmentosa
Effective in some photodermatoses
Localized and systemic scleroderma
Polymorphic light eruption
Vitiligo
Postinflammatory hypopigmentation
Solar uritcaria
Graft-versus-host disease
Actinic prurigo
3636
UVA and UVB penetration in human skin
UVB (290-320 nm) UVA (320-400 nm)
14 microns
140 microns
photochemical changes in trans-urocanic acid, converting it into the cis form of the molecule. Urocanic acid is a breakdown product of histidine and is present in large amounts in the stratum corneum. Originally considered to be a natural photoprotectant, there is now substantial evidence that cis-urocanic acid is a mediator of UVB-induced immunosuppression.5 In addition, urocanic acid levels can also affect vitamin D production. Specifically, upon NB-UVB exposure, there is an accompanied increase in hydroxyvitamin D synthesis that inversely correlates with the baseline levels of trans-urocanic acid.6 A third direct target of UVB radiation is the amino acid tryptophan. UVB converts tryptophan into 6-formylindololo[3,2-b]carbazole, which binds to the intracellular aryl hydrocarbon hydroxylase receptor, initiating a series of events that culminates in activation of signal transduction pathways. One such pathway results in expression of cyclooxygenase-2, an enzyme required for synthesis of prostaglandin E2.7
Finally, there is evidence that UVB exposure leads to the generation of reactive oxygen intermediates, which has downstream effects such as DNA damage in the form of 8-oxo-deoxyguanosine, lipid peroxidation, activation of signal transduction pathways, and stimulation of cytokine production.8
In contrast to UVB radiation which has a relatively superficial depth of penetration, UVA radiation (320 to 400 nm) can reach the mid- or lower dermis to a depth of 140 microns (see Fig. 198-2).3 It is therefore more effective than UVB for skin diseases in which the cutaneous pathology lies deeper than the superficial dermis. Like UVB, UVA radiation can produce pyrimidine dimers in DNA, but, on a per-photon basis, it is much less effective at doing so.9 In most situations, the major biologic effects of UVA radiation are from the generation of reactive oxygen intermediates.10 Following UVA exposure, reactive oxygen intermediates are formed in mitochondrial enzyme complexes during oxidative
29
phosphorylation. Although the skin contains antioxidants, reactive oxygen intermediates formed during phototherapy exceed the amount that can be neutralized by endogenous photoprotective activities. UVAinduced oxidants are capable of harming DNA, lipids, structural and nonstructural proteins, and organelles such as mitochondria. The generation of oxidants following UV exposure also has been implicated in photoaging of the skin and skin cancer. Interestingly, animal studies show that exposure to UVA’s longer wavelength (UVA1, 340-400 nm) has immunoprotective properties via the generation of heme oxygenase-1, which exerts antioxidant and antiinflammatory effects while also decreasing UVB-induced damage.11
In psoralen photochemotherapy, psoralen photosensitizers are activated by UVA radiation, and the depth of penetration of PUVA is the mid-dermis. The major photochemical effect of psoralen photochemotherapy is damage to DNA. Psoralen photochemotherapy– induced changes in DNA differ from those of UVB and UVA without psoralens.12 Psoralens used for photochemotherapy have 2 double bonds that can absorb UVA radiation. When administered to an individual, these compounds intercalate with DNA. Following UVA exposure, they form a single adduct with DNA and then become a bifunctional adduct, crosslinking the DNA strands in the double helix, when a second photon is absorbed. There is also some evidence that photochemotherapy augments the production of reactive oxygen intermediates such as singlet oxygen. This effect has been implicated in induction of the cyclooxygenase enzyme and activation of arachidonic acid pathways.13
EFFECTS ON THE IMMUNE SYSTEM
EFFECTS ON THE
IMMUNE SYSTEM
The photoimmunologic effects of phototherapy are thought to provide an explanation, at least in part, for phototherapy’s efficacy in cutaneous diseases in which T-cell hyperactivity predominates (eg, psoriasis, atopic dermatitis, lichen planus). Under normal circumstances, both effector and regulatory T cells are generated, with the overall intensity of the immune response dependent on the relative proportion of effector and regulatory T-cell populations that are present. UVB exposure inhibits activation of effector T cells, whereas it leaves the development of regulatory T cells unaltered.14 Consequently, the equilibrium of effector and regulatory T cells is biased toward a diminished cell-mediated immune response. This perturbation in the balance of effector and regulatory T cells reflects disruption of the activities of dendritic cells within the skin, the major function of which is to present antigen to T-lymphocytes. This is a result of the direct effects of UVB on dendritic cells and indirectly through the production of interleukin (IL)-10 and prostaglandin E2, both of which diminish the capacity of dendritic cells to present antigen to effector T cells leading to suppressed T-cell responses.15 Increased levels of IL-10 have been found after UVB, UVA1, and PUVA exposure. Prostaglandin E2 production occurs through
3637
29
UVB effects on keratinocytes16-18; UVB is an inductive stimulus for cyclooxygenase-2, which is important for prostaglandin E2 production. UV exposure also significantly lowers levels of immunomodulatory factors such as prostaglandin D2, possibly reflecting a loss of Langerhans cells from the epidermis upon UV exposure.19
Other immunosuppressive soluble mediators that are reported to be increased following UVB exposure include agonists of the platelet activating factor receptor,20 melanocyte-stimulating hormone, and calcitonin gene–related peptide.21 In addition, in the setting of inflammation, FoxP3-positive regulatory T cells can convert into IL-17–producing cells and lose FoxP3. UVB radiation, however, increases FoxP3 expression by binding the transcription factor, p53, and stabilizing the FoxP3-positive regulatory T-cell population.22,23
The epidermal growth factor–like growth factor amphiregulin influences the activity of regulatory T cells and basophil-derived amphiregulin is implicated in mediating UVB-induced immune suppression in murine models, which supports the notion that growth factors have immunomodulatory properties relevant to skin biology and disease.24,25
PUVA has effects that are similar to UVB with respect to antigen-presenting cells within the skin, the balance between effector and regulatory T cells, and the production of soluble immunosuppressive mediators.14 However, there is limited information on the effect of UVA1 on antigen-presenting cells and on effector and regulatory T cells. In acute skin lesions of atopic dermatitis, UVA1 appears to increase IL-4 and thymus-regulated and activation-regulated chemokine messenger RNA expression, but has little effect on expression of human beta defensin-1, thymic stromal lymphopoietin, IL-5, IL-10, IL-13, or IL-31.26,27
In addition to its actions on cutaneous antigenpresenting cells, phototherapy causes cell death by apoptosis of T cells in cutaneous lymphoid infiltrates. This has been demonstrated for UVA1 phototherapy in the lymphocytic infiltrate in atopic dermatitis,28 and for NB-UVB in psoriasis.29 Another immunologic effect of phototherapy is on expression of CD54 (intercellular adhesion molecule-1) and other adhesion molecules. Intercellular adhesion molecule-1 is not normally present on epidermal keratinocytes, but can be induced in a variety of inflammatory skin conditions. It facilitates T-cell binding to keratinocytes, through its interaction with lymphocyte function–associated antigen-1 that is present on T cells. Because UVB, UVA1, and PUVA all interfere with keratinocyte expression of CD54, this effect of phototherapy may contribute to phototherapy’s efficacy in diseases that have increased keratinocyte CD54 expression.14
EFFECTS ON MAST CELLS
EFFECTS ON MAST CELLS
Both UVA1 and PUVA have deleterious effects on mast cells, although the mechanisms of action differ.30,31
PUVA is not cytotoxic for mast cells, and because of
3638
this, there is little reduction in mast cell concentrations in the dermis. However, PUVA does stabilize mast cell membranes and, as a result, limits the release of histamine and other mediators when these cells are stimulated to degranulate.31 In contrast, chronic therapy with UVA1 results in apoptosis of mast cells with a marked reduction in their concentrations that can last for several months.30 Both PUVA and UVA1 have been employed to treat selective mast cell–mediated diseases.
EFFECTS ON COLLAGEN
EFFECTS ON COLLAGEN
One of the downstream effects of UVA-induced generation of reactive oxygen intermediates is activation of matrix metalloproteinase (MMP)-1,32,33 the major biologic activity of which is degradation of collagen. UVA radiation increases the production of IL-1 and IL-6, which are stimuli for MMPs.34 PUVA also increases MMPs.35 These effects of UVA1 and PUVA on MMP-1 and collagen degradation provide the rationale for its use in sclerotic skin diseases.
EFFECTS ON KERATINOCYTES
EFFECTS ON
KERATINOCYTES
UVB, PUVA, and UVA all cause acanthosis of the epidermis and thickening of the stratum corneum.36
This effect accentuates light scattering and increases its absorption by the upper levels of the epidermis. Therefore, phototherapy treatment doses must be progressively increased so that an equivalent number of photons can reach the lower levels of the epidermis and dermis where therapeutic targets lie. Alternatively, this attribute of phototherapy has been exploited for the management of chronic photosensitivity disorders because this “hardens” the skin, permitting individuals afflicted with these disorders to tolerate greater amounts of sun exposure.
EFFECTS ON MELANOCYTES
EFFECTS ON
MELANOCYTES
Exposure to UVR is also known to stimulate melanogenesis,37 which is, at least in part, a consequence of DNA damage and/or its repair.38-41
Experimental studies have shown that treatment of melanocytes with DNA repair enzymes increases the melanin content of melanocytes,42 and application of small fragments of thymidine dinucleotides to guinea pig skin produces a tanning response.39-41 The stimulatory effects on melanogenesis decrease the efficacy of phototherapy unless the doses of UVR are gradually
increased, but in patients with some photosensitivity disorders, this biologic effect can be exploited therapeutically, allowing them to tolerate greater amounts of ambient sun exposure. Narrowband UVB and PUVA are also employed to repopulate vitiliginous skin with melanocytes. The mechanism by which phototherapy stimulates repigmentation of vitiliginous skin is incompletely understood, but may involve stimulation of hair follicle melanocyte proliferation and migration.43 Cytokines and other inflammatory mediators released from other cells, such as keratinocytes, are thought to stimulate inactive melanocytes in the outer root sheath of hair follicles to proliferate, mature, and migrate to repopulate the interfollicular epidermis.44 Increased expression of cytokeratins 15 and 19, markers for stem cell activation in the follicular and interfollicular epithelium, is also seen in response to phototherapy.45
PHOTOTHERAPY DEVICES
In an ideal situation, the wavelengths that are most effective for the treatment (ie, the action spectrum) for every dermatologic condition would be known and there would be a device capable of delivering those wavelengths specifically to lesional skin. For some skin diseases, such as psoriasis, great strides have been made toward this ideal; targeted therapy using devices that can deliver wavelengths of UVR at or close to those that are most effective at clearing psoriatic plaques have been evaluated and are being used clinically. Unfortunately, for most dermatologic conditions this information is still unknown. However, the increased availability of improved phototherapy devices and novel treatment approaches is providing new options for patients and clinicians. In addition, as studies are conducted that use phototherapy, there is a better understanding of how best to use these technologies. Many different types of phototherapy devices exist and more are currently under development. Phototherapy devices are varied and can be booth-like devices that patients enter to receive their treatment, smaller stationary devices that can deliver UVR to a specific anatomic region (such as the hands and/or feet) while sparing uninvolved areas, or handheld devices that can be maneuvered to deliver UVR to lesional skin. The type of device used needs to be individually tailored to a given patient. Some patients may have trouble standing for the required amount of time needed for therapy, whereas others may have difficulty maneuvering themselves. It is important to note that phototherapy can be delivered in the setting of a dermatology practice or in the home. Numerous changes are being made to phototherapy devices to make them safer and more convenient. For example, a “digital phototherapy device” has been developed that integrates a camera, computer hardware and software, a digital mirror device, and other components that only delivers UVR specifically to diseased skin while sparing surrounding normal skin.46,47
29
BASIC PRINCIPLES OF PHOTOTHERAPY DEVICES AND TYPES OF LAMPS
BASIC PRINCIPLES OF
PHOTOTHERAPY DEVICES
AND TYPES OF LAMPS
Phototherapy devices generate light by the conversion of electrical energy into electromagnetic energy. Filters and fluorophores are used to modify the output such that the desired wavelengths are emitted. There are several types of lamps (or bulbs) used to generate therapeutic UVR. These include incandescent lamps, arc lamps, and fluorescent lamps. Incandescent lamps generate UVR by passing an electric current through a thin tungsten filament, which, in turn, generates heat and light. Because much of the electrical energy is converted to heat, these lamps are relatively inefficient light sources and have relatively short life spans. By sealing the tungsten filament in a quartz envelope that contains a halogen (bromine or iodine), the filament can be made to emit more energetic photons without reducing the longevity of the bulb. These lamps are called quartz halogen lamps and can emit wavelengths within the UV, visible, and infrared ranges. In clinical dermatology, these lamps are employed primarily in situations that require visible light such as phototesting and photodynamic therapy. Arc or gas discharge lamps were the first effective artificial UVR sources used for phototherapy. Arc lamps take advantage of the fact that when a high voltage is passed across 2 electrodes in the presence of a gas, the electrons of the gas atoms become excited. The “arc” of an arc lamp refers to the electric arc generated when the gas is ionized (ionized gas is also known as plasma) by a high electric current. When the gas electrons return to their ground state, light is emitted. The type of gas incorporated into the lamp determines the wavelengths that are emitted (ie, spectral output). The output of arc lamps can be modulated by altering the gas pressure within the bulb such that at high pressures, the peak wavelength output broadens. High-pressure arc lamps typically contain mercury or xenon gas, whereas low-pressure arc lamps use fluorescent material. In addition to altering the gas pressure to modify the spectral output of arc discharge lamps, the addition of metal halides broadens the output spectrum such that it becomes nearly continuous across the UV spectrum. For example, when mercury arc lamps are operated at high pressures, they have output emission peaks (so-called mercury lines) seen at 297, 302, 313, 334, and 365 nm. In contrast, if a metal halide is added to the mercury, the output between these peaks is increased and is thus more continuous. The use of optical filters can then further refine the output of these lamps such that only the desired wavelengths are emitted. The advantage of metal halide lamps is the high output that allows for shorter treatment times. However, they are costlier and more difficult to operate than fluorescent lamps. One example of a metal halide lamp currently in clinical use is the UVA1 light source.
3639
29
Fluorescent lamps are the most commonly used sources of therapeutic UVR. These lamps take advantage of the fact that chemicals called phosphors (a specific type of chromophore also called a fluorophore) absorb and then reemit light. The light that is reemitted is of lower energy (and thus longer wavelength) than the inciting light. Using this principle, the ultraviolet C irradiation (which peaks at 254 nm) generated from a low-pressure mercury lamp can be converted to the longer UVB and UVA wavelengths of light that are desirable for phototherapy. The final output of a fluorescent lamp is dictated by the specific phosphor of the bulb. An important advance in photodermatology came with the development of a modified fluorescent lamp that emits largely at 311 nm.48 Broadband UVB and UVA light sources used for PUVA are other examples of fluorescent lamps. Because different forms of phototherapy are used to treat different diseases, it is important and practical to divide devices based upon wavelength. Devices that deliver BB-UVB, 311-nm NB-UVB, UVA (for use in psoralen photochemotherapy), and UVA1 (340 to 400 nm) are available in the United States and in most other countries. In addition to differing by spectral output, phototherapy devices range in the surface area that they are designed to treat (whole body, localized regions, or only lesional skin). Devices used for large body surface areas resemble booths, which patients enter for each treatment. These devices come in a variety of styles, from round cylinders to folding units that can be unfolded for treatments and then collapsed while not in use. Devices have been developed to treat more limited areas (such as the palms and soles) and are substantially smaller in size. Finally, targeted therapy uses devices that can deliver therapeutic UVR only to lesional skin range in size from small handheld units to larger devices with a handheld wand attached.
BROADBAND AND NARROWBAND ULTRAVIOLET B
BROADBAND AND
NARROWBAND
ULTRAVIOLET B
Originally used for psoriasis therapy, artificial sources of BB-UVB have been used therapeutically since the early 20th century. In particular, UVB combined with the topical application of coal tar (as developed initially by William Goeckerman) had been a mainstay of psoriasis treatment for many decades.49 With the development and availability of NB-UVB, some dermatologists have concluded that BB-UVB is obsolete.50
However, BB-UVB is still widely used in the United States for a variety of conditions. The most commonly employed devices that deliver BB-UVB use fluorescent lamps. These devices emit UVR over a broad spectral range. Approximately twothirds of the output is in the UVB range and the rest is primarily in the UVA. Because wavelengths within the UVB spectrum have higher energy than those within
3640
the UVA, the UVA component generally contributes little to the therapeutic efficacy, assuming the patient is not taking a photosensitizing medication. BB-UVB and NB-UVB devices are specifically designed to limit output below 290 nm (ie, in the ultraviolet C range). The wavelengths that most efficiently clear psoriasis are approximately around 313 nm.51 In contrast, wavelengths less than 300 nm are the most efficient at causing erythema and nonmelanoma skin cancer. Based on this knowledge, light sources, termed NB- UVB, have been produced.48 These light sources emit only wavelengths between 308 and 313 nm, and have largely supplanted BB-UVB UV radiation sources for phototherapy. Although originally employed to treat psoriasis, they are now used to treat several other inflammatory skin diseases as well. The initial starting dose of both BB-UVB and NB- UVB is determined in one of two ways (Tables 198-1 and 198-2). In the first, the minimal erythema dose (MED) is determined by exposing six 1-cm2 areas of skin on the inner aspect of the forearm or lower back to gradually increasing amounts of UV radiation from the same device that will be used for phototherapy. Twenty-four hours later, the UV-exposed areas of skin are examined and phototherapy is initiated at 50% to 70% of the smallest UV dose that results in uniform erythema over the entire area (ie, the MED). A semiautomated handheld device to determine MED has shown high correlation with the conventional method with low interobserver variability. This may be a faster, more reproducible alternative to conventional MED testing.52 Alternatively, the initial dose of phototherapy is established empirically based on Fitzpatrick skin phototype (Tables 198-1 and 198-2). Subsequent exposures are given 2 to 5 times per week and the dose is
I. MED based
A. MED determination Expose 1-cm2 areas on the lower back or inner aspect of the forearm to 200, 400, 600, 800, 1000, 1200 mJ/cm2; read at 24 hours B. Initial exposure: 50% to 70% of MED C. Subsequent exposures: 2 to 5 times per week Increase UV dose by 10% to 20% with each treatment II. Skin phototype based Initial exposure based on Fitzpatrick skin phototype; subsequent exposures as above
SKIN PHOTOTYPE INITIAL NB-UVB DOSE (MJ/CM2) MAXIMUM DOSE (MJ/CM2)
I 130 2000
II 220 2000
III 260 3000
IV 330 3000
V 350 5000
VI 400 5000
VI 400 5000
MED, minimal erythema dose; NB-UVB, narrowband ultraviolet B. Modified from Menter et al1 and Krutmann et al.374
I. MED based
A. MED determination Expose 1-cm2 areas on the lower back or inner aspect of the forearm to 20, 40, 60, 80, 100, 120 mJ/cm2; read at 24 hours B. Initial exposure: 50% to 70% of MED C. Subsequent exposures: 2 to 5 times per week Increase UV dose by 25% with each treatment for the first 10 treatments; 10% per treatment thereafter II. Skin phototype based Initial exposure based on Fitzpatrick skin phototype; subsequent exposures as above
SKIN PHOTOTYPE INITIAL BB-UVB DOSE (MJ/CM2)
I 20
II 25
III 30
IV 40
V 50
VI 60
VI 60
MED, minimal erythema dose; BB-UVB, broadband ultraviolet B. Modified from Menter et al1 and Krutmann et al.374
increased at each treatment, assuming the patient has not developed an erythema response. If an erythema response has occurred, then, depending on its severity, the dose is either reduced or the treatment is delayed (Tables 198-1 and 198-2). Interestingly, NB-UVB is considerably less photoadaptive in comparison to BB- UVB, demonstrating the importance of wavelength on epidermal thickening and need for higher subsequent MEDs when treated with BB-UVB in comparison to NB-UVB.53 The maximum NB-UVB dose that should be administered is 2000 to 5000 mJ/cm2, depending on the photoreactive skin type. If patients miss treatments, dosage modifications should be made to avoid a phototoxic response (see Table 198-5).
PSORALEN AND ULTRAVIOLET A
PSORALEN AND
ULTRAVIOLET A
PUVA photochemotherapy combines the oral ingestion or topical application of psoralens with exposure to UVR in the UVA range. Although psoralens and sunlight had been employed for thousands of years for the treatment of vitiligo, it was not until 1947 that PUVA in its modern form was described, initially for the treatment of vitiligo, and subsequently for the treatment of psoriasis.54
Three forms of psoralen are used in photochemotherapy regimens: 8-methoxypsoralen (8-MOP), 5-methoxypsoralen (5-MOP), and 4,5′,8-trimethylpsoralen. In the United States, only 8-MOP is available. There are 2 oral formulations of 8-MOP, a micronized form that is typically given at a dose of 0.6 mg/kg 120 minutes
29
prior to UVA exposure or a dissolved form that is given at a dose of 0.4 to 0.6 mg/kg 90 minutes before UVA exposure. Because the dissolved preparation is absorbed faster and yields higher and more reproducible serum levels, it is more commonly employed in PUVA phototherapy regimens. The most common sources of radiation for PUVA therapy are UVA fluorescent lamps, which have a maximum emission at 352 nm, near the absorption maximum for psoralens. For oral PUVA therapy, UVA radiation is usually initiated at a dose that corresponds to either the skin phototype or to 50% to 70% of the minimum phototoxic dose (Table 198-3). The minimum phototoxic dose is determined by having the patient take the dose of the oral psoralen to be used for the photochemotherapy treatment and exposing six 1-cm2
areas of skin to the gradually increasing doses of UVA. The minimum phototoxic dose is evaluated 72 hours after UVA exposure and is the lowest amount of UVA that produces a uniform erythema over the entire area. In the United States, it is more common to initiate therapy based on the skin phototype (Table 198-3). Treatments are usually given 2 to 4 times per week, avoiding consecutive days. The amount of UVA that is to be given is increased with each treatment. UVA dose modifications are made if an erythema response develops or if treatments are missed (Table 198-3). Delivery of psoralens in bathwater is popular in some areas of the world because it provides a uniform drug distribution over the skin surface, is associated
I. Psoralen dose 8-MOP micronized 0.6 mg/kg; 120 minutes before UVA 8-MOP dissolved 0.4-0.6 mg/kg; 90 minutes before UVA MPD based
A. MPD determination Expose 1 cm2 areas on the lower back or inner aspect of the forearm to 0.5, 1, 2, 3, 4, 5 J/cm2 UVA; read 72 hours after UVA exposure B. Initial exposure: 50% to 70% of MPD C. Subsequent exposures: 2 to 4 times per week Increase UVA dose per table entries each week (not each exposure) II. Skin phototype based
A. Initial exposure based on Fitzpatrick skin phototype; subsequent exposures as above
SKIN PHOTOTYPE INITIAL PUVA DOSE (J/CM2) DOSE INCREASES (PER WEEK AFTER THE FIRST WEEK)
I 0.5 0.5
II 1.0 0.5
III 1.5 1.0
IV 2.0 1.0
V 2.5 1.5
VI 3.0 1.5
VI 3.0 1.5
8-MOP, 8-methoxypsoralen; MPD, minimum phototoxic dose; PUVA, psoralen and ultraviolet A; UVA, ultraviolet A. Modified from Menter et al1 and Krutmann et al.374
3641
29
I. Psoralen dose 8-MOP dissolved in bath water for a final concentration of 1 mg/L Bath water is at body temperature (37°C [98.6°F]) Duration of bath is 15 to 20 minutes II. UVA Exposure
I. Psoralen dose 8-MOP dissolved in bath water for a final concentration of 1 mg/L Bath water is at body temperature (37°C [98.6°F]) Duration of bath is 15 to 20 minutes II. UVA Exposure
A. MPD Determination
A. MPD Determination Expose 1-cm2 areas on the lower back or inner aspect of the forearm; read 72 hours after UVA exposure Skin phototype I or II: 0.5, 1, 2, 3, 4, and 5 J/cm2 UVA Skin phototype III or IV: 1, 2, 4, 6, 8, or 10 J/cm2 UVA B. UVA exposure immediately after bathing C. Initial exposure: 30% of MPD D. Subsequent exposures: 2 times per week
Increase UVA dose by 20% each week
Expose 1-cm2 areas on the lower back or inner aspect of the forearm; read 72 hours after UVA exposure Skin phototype I or II: 0.5, 1, 2, 3, 4, and 5 J/cm2 UVA Skin phototype III or IV: 1, 2, 4, 6, 8, or 10 J/cm2 UVA B. UVA exposure immediately after bathing C. Initial exposure: 30% of MPD D. Subsequent exposures: 2 times per week Increase UVA dose by 20% each week
8-MOP, 8-methoxypsoralen; MPD, minimum phototoxic dose; PUVA, psoralen and ultraviolet A; UVA, ultraviolet A. Modified from Menter et al1 and Krutmann et al.374
with very low psoralen plasma levels, and results in a rapid elimination of free psoralens from the skin. This form of psoralen delivery circumvents GI side effects and possible phototoxic hazards to the eyes that are associated with the oral form. Skin psoralen levels are highly reproducible, and photosensitivity lasts for no more than 2 hours. Bath PUVA consists of 15 to 20 minutes of whole-body immersion in solutions of 1 mg 8-MOP per liter of body temperature bathwater (Table 198-4). 5-MOP and trimethylpsoralen are also employed for bath PUVA. Irradiation is performed immediately after bathing, as photosensitivity decreases rapidly. Bath PUVA is started at 30% of the minimum phototoxic dose. Treatments are typically given twice weekly. Guidelines for bath, local immersion, and other topical PUVA forms have been published by the British Photodermatology Group.55
A cost-effectiveness analysis of data collected across 4 centers in Scotland revealed that courses of both bath PUVA and other topical PUVA treatments were consistently more expensive than oral PUVA.55 This is related predominantly to the increased nursing time required. More recently, cream PUVA has been developed which can be used to treat local and more widespread disease.55A Thirty minutes following the application of a psoralen-containing cream, patients are exposed to UVA irradiation.
AVOIDANCE AND MANAGEMENT OF PHOTOTOXIC REACTIONS
AVOIDANCE AND
MANAGEMENT OF
PHOTOTOXIC REACTIONS
Sunburn-like reactions are the most common shortterm adverse effect of phototherapy. UVB phototoxicity usually peaks at 12 to 24 hours and PUVA reaction
3642
REASON FOR MODIFICATION MODIFICATION OF DOSE
No erythema Increase by 25%
Erythema with no pain No increase
Erythema with pain Hold treatment until symptoms subside
Erythema with pain and blistering Hold treatment until symptoms subside and then reduce dose by 50% from last dose
Modification of Phototherapy Dose for Missed Treatments
<1 week No increase in dose
1 to 2 weeks Decrease dose by 50% (BB-UVB) or 25% (NB-UVB or PUVA)
2 to 3 weeks Decrease dose by 75% (BB-UVB) or 50% (NB-UVB or PUVA)
3 weeks Restart at initial exposure dose
3 weeks Restart at initial exposure dose
BB-UVB, broadband ultraviolet B; NB-UVB, narrowband ultraviolet B; PUVA, psoralen and ultraviolet A. Modified from Menter et al1 and Krutmann et al.374
manifests at 24 to 48 or even 72 hours. Severe burns over a large portion of the skin surface produce systemic toxicity with fever and malaise in addition to pain. Severe PUVA burns, which extend well into the dermis, can lead to epidermal sloughing and are an indication for admission to a burn care hospital facility. To avoid exacerbating a still-developing PUVA burn it is recommended that PUVA treatments not be given on consecutive days. Table 198-5 specifies the UVB or UVA dose adjustments in the event of a burn reaction during phototherapy. A burn reported by the patient at the next visit, even if no longer visible, should be managed in the same manner as a stillvisible reaction. Burns over limited body areas, such as just the face or breasts, can be managed by local application of an appropriate sunscreen before or part way through subsequent treatments, especially if the area is not affected by the disease being treated. However, care must be taken to consistently protect the same area(s) to avoid a sudden full treatment to previously shielded skin. Repeated UV-irradiated skin develops tolerance to subsequent exposures, allowing and, indeed, mandating progressively larger doses for optimal therapeutic effect. However, this tolerance is rapidly lost when exposures cease, requiring downward adjustments of dose after as little as 1 week (see Table 198-5) to avoid burns.
ULTRAVIOLET A1
ULTRAVIOLET A1
Because of its longer wavelength, UVA1 phototherapy (340 to 400 nm) can penetrate deeper into the skin than UVB or shorter-range UVA called UVA2
(ie, 320 to 340 nm). The first report describing a device capable of emitting UVA1 occurred in 1981.56 It was not until 1992 when the therapeutic benefit of UVA1 was demonstrated for atopic dermatitis that greater interest in its therapeutic properties occurred.57,58
Initially, one obstacle to the widespread use of firstgeneration UVA1 devices was the intense heat that they produced. Although not widely available in the United States, these light sources are useful for the management of a variety of dermatologic conditions for which other forms of phototherapy are not helpful.59,60
UVA1 is administered 3 to 5 times per week. Three dosing regimens have been used: low dose (10 to 30 J/cm2), medium dose (40 to 70 J/cm2), and high dose (130 J/cm2). In general, patients are started at 20 to 30 J/cm2 and increased to the full dose within 3 to 5 treatments. The risk of burns is far less than with UVB or PUVA therapy.
TARGETED PHOTOTHERAPY
TARGETED PHOTOTHERAPY
Targeted phototherapy is also called focused phototherapy, concentrated phototherapy, and microphototherapy. Unlike the previously described phototherapy devices that expose both lesional and uninvolved skin to UVR, targeted phototherapy delivers therapeutic doses of UVR only to lesional skin. Several devices are available to deliver targeted phototherapy, including both monochromatic (1 wavelength) and polychromatic systems. As of this writing, there is also a new therapeutic device in development that provides digital UV phototherapy that can be used to institute either targeted UVA or UVB therapy.47 There are several advantages to targeted phototherapy. These devices spare normal skin, thereby allowing higher fluences to be delivered to diseased skin while decreasing the risk of acute and chronic side effects to normal skin. Targeted therapy can be used on treatment-resistant lesions and in difficult anatomic locations (such as the scalp, chin, and nails). The handheld nature of a targeted phototherapy device may have increased feasibility for young children compared to receiving treatments in a phototherapy booth that can be large and intimidating. The limitations of targeted phototherapy are device expense and that it may not be practical to treat for patients with greater than 10% to 20% body surface area involvement. Targeted phototherapy devices have been used to administer targeted therapy to patients with psoriasis, vitiligo, and cutaneous T-cell lymphoma.61,62 Monochromatic light sources, which include excimer lasers, monochromatic UVA1 lasers,63 and nonlaser devices known as monochromatic excimer light devices, have been developed for this purpose. They differ in several respects. Lasers typically treat smaller areas, but can emit higher amounts of radiation over a shorter period. In contrast, monochromatic excimer light devices deliver monochromatic irradiation to a larger area
29
but with a lower power density. There are also several devices that emit polychromatic UVA or UVB (BB-UVB or NB-UVB) to targeted areas. These devices typically use fiberoptic systems coupled with UVB-generating sources. They have spot sizes from 1 to 3 cm. In addition, these devices have multiple delivery programs and automatic calibration which makes treatment with predetermined dosages possible. These devices are smaller, less expensive, and have fewer maintenance problems than lasers.64,65 Treatment protocols with targeted phototherapy vary depending on the type of device that is employed. A novel cream that selectively filters solar UVB may be a cheaper and more convenient alternative to traditional phototherapy in certain cases. This cream has been shown to improve symptoms of chronic pruritus after 3 months of treatment (3 sessions per week).66
SAFETY OF PHOTOTHERAPY
Safety principles are common to most phototherapy devices. Equipment should be checked on a regular basis by the clinical staff or the manufacturer’s engineer, since bulb output may change over time and internal dosimetry components may fail. While phototherapy is usually delivered without incident, the risk of overtreatment is real, although the exact incidence of adverse events attributable to phototherapy is unknown and varies depending on the device. Importantly, except for PUVA therapy for which formal longterm followup studies established an increased risk of lentigines, squamous cell carcinoma, and possibly melanoma, other forms of phototherapy appear to be remarkably safe.62,67 Newer therapies, such as NB-UVB and UVA1 appear to be relatively safe especially compared to nonphototherapeutic options for the same diseases.
ULTRAVIOLET B
ULTRAVIOLET B
Repeated exposure of the skin to UV irradiation does result in cumulative actinic damage regardless of the source. With respect to nonmelanoma skin cancer, most studies show that there is little risk beyond that associated with habitual sun exposure with either BB-UVB or NB-UVB phototherapy.68,69 More than 300 BB-UVB treatments is associated with a modest, but significant, increase in squamous cell carcinoma (SCC) and basal cell carcinoma.70 However, the carcinogenic risk of a single PUVA treatment is approximately 7 times greater than a single UVB treatment.71 As a result of its safety profile and efficacy, NB-UVB has emerged as a leading therapy for a number of skin diseases. Several studies also show that long-term exposure to BB-UVB combined with topical tar preparations is not associated with an increased risk of SCC.72
3643
29
PSORALEN AND ULTRAVIOLET A
PSORALEN AND
ULTRAVIOLET A
ACUTE SIDE EFFECTS
Potential side effects of PUVA include drug intolerance in addition to the adverse reactions resulting from the combined action of psoralens plus UVA radiation. Oral 8-MOP may cause nausea (10% of patients) and vomiting, which occasionally necessitates discontinuation of treatment. These side effects are more common with liquid preparations than with crystalline preparations, probably because of higher psoralen serum levels. The nausea may be minimized or avoided by instructing the patient to take 8-MOP with milk, food, or ginger, or to divide the dose into 2 portions, taken approximately 30 minutes apart. Other reported effects include nervousness, insomnia, and depression. With 5-MOP, nausea is rare, even with doses up to 1.8 mg/kg/body weight. Following exposure to UVA, approximately 10% of patients undergoing PUVA therapy will experience pruritus. In most cases, this can be alleviated by bland emollients. Some patients with severe pruritus require systemic treatment. A stinging pain may rarely occur; the mechanism for this is unknown. These symptoms are usually unresponsive to antihistamines, and, in most instances, subside when the treatment is discontinued. Mild and often transient focal erythema after PUVA therapy occurs frequently. Any area showing erythema with tenderness or blistering should be shielded during subsequent UVA exposures until the erythema has resolved. As noted above, erythema appearing within 24 hours may signal a potentially severe phototoxic reaction, and may worsen progressively over the next 24 hours, as peak erythema with PUVA characteristically occurs at least 48 hours after the treatment. In that situation, patients should be protected from further UVA exposures and sunlight, and should be monitored closely until the erythema has resolved. Very rare side effects of PUVA include polymorphous light eruption-like rashes, acneiform eruptions, subungual hemorrhages caused by phototoxic reactions of the nail beds, onycholysis, and occasionally hypertrichosis of the face. These disappear when treatment is discontinued. Analysis of laboratory data in several large studies revealed no significant abnormal findings in patients receiving PUVA over prolonged periods of time.73-75
CHRONIC ACTINIC DAMAGE
Chronic exposure to PUVA may result in skin changes that resemble photoaging, which is aggravated by chronic natural sun exposure. PUVA lentigines are small brown macules with irregular borders and uneven pigmentation76 and are histologically characterized by proliferation of large melanocytes.77 In contrast to solar lentigines, melanocytes in PUVA lentigines often display an increased size of melanosomes, clustering and binucleation with nuclear hyperchromatism, and
3644
cellular pleomorphism. BRAF (v-raf murine sarcoma viral oncogene homolog B) mutations have been found to be present in PUVA lentigines,78 but the full significance of this is not yet understood, as both cutaneous malignant melanoma and benign melanocytic nevi often have BRAF mutations.79-82 The presence of these lesions is directly related to the number of PUVA treatments and total UVA dose that has been administered. The absence of PUVA lentigines serves as a useful indicator of a lower risk of PUVA malignancy.83
CARCINOGENESIS
Cutaneous malignancies are the major concern of long-term and repeated PUVA treatments. The risk of nonmelanoma skin cancer and possibly malignant melanoma increases in a dose-dependent manner. In laboratory animals, 8-MOP and 5-MOP have unequivocally induced skin cancer at levels of drug and UVA irradiation comparable to those used in PUVA therapy.84 Cancer development is thought to stem from both DNA damage and downregulation of the immune system. The PUVA Follow-up Study, which evaluated 1380 patients who began PUVA treatment for psoriasis in 1975 and 1976 has documented major health events in these individuals in a prospective manner. Overall, patients who were treated with at least 337 PUVA treatments exhibited a 100-fold increased risk of SCC compared to that expected from population incidence rates.85 Moreover, almost 4% of patients with SCC developed metastases, most commonly originating in the genital area. There is uncertainty about PUVA being the sole factor as many of the patients in the long-term followup studies also had significant exposure to sunlight and to treatments with carcinogenic potential, including arsenic, UVB, and methotrexate. The risk of developing SCC with PUVA may be further potentiated by the use of cyclosporine and for this reason cyclosporine is contraindicated in individuals who have been treated with PUVA.86 Oral retinoids used concurrently with PUVA, on the other hand, reduce the risk of SCC.87
Individuals treated with PUVA are at increased risk of cutaneous malignancies of the genitalia, and this has led to standard protection of the genitalia during phototherapy.88 The risk is dose-dependent, with a 90-fold increased risk of genital tumors among patients exposed to high doses of PUVA compared with that expected in the general population. Men treated with high-dose exposures to both PUVA and topical tar/UVB have the greatest risk of genital tumors.88,89 There is currently no standardized regimen for genital shielding. Commonly used protective agents include commercially available pouches for genital shielding, surgical masks, paper towels, blue surgical towels, and underwear. The efficacy of these materials has been studied, and surgical masks were found to provide insufficient protection against UV irradiation, most likely because of increased porosity (looser weave) and decreased mass.90
The relationship between PUVA and melanoma also has been examined in detail. The PUVA Follow-Up Study has provided evidence that individuals with at least 250 treatments and at least 15 years from the first PUVA treatment were at increased risk of developing melanoma.91 Patients who developed a phototoxic reaction more easily were at higher risk for melanoma than those with darker skin.92 As a result of those studies, a personal or family history of melanoma or a history of more than 200 PUVA treatments is considered to be a relative contraindication to further PUVA therapy.92
In patients employing PUVA therapy in combination with methotrexate for at least 36 months, the incidence of lymphoma was more than 7 times higher than that of cohort members earlier in the study who had not taken methotrexate.93
OPHTHALMOLOGIC EFFECTS
UVA is absorbed in the lens and in the presence of UVA, psoralens can bind protein, DNA, and RNA. Because the lens never sheds its cells, protein-bound 8-MOP accumulates in the lens, increasing the risk of irreversible opacification.94 There have been reports of various ocular problems in patients on PUVA including cataracts,95,96 conjunctival hyperemia,97 and decreased lacrimation.97
A 25-year prospective study98 sought to evaluate the effect of PUVA on the eyes. Participants were instructed to use UVA-blocking eyewear when outside or looking outside through window glass during daylight for a minimum of 12 hours, although current labeling calls for 24 hours of eye protection. This study found no relationship between increasing numbers of PUVA sessions and visual impairment or cataracts, and demonstrates that increasing exposure to PUVA does not increase cataract risk among middle-aged and older persons using eye protection as practiced by this cohort.98 Other smaller studies also have found no increase in cataract formation or visual impairment.99-102
ULTRAVIOLET A1
ULTRAVIOLET A1
UVA1 phototherapy is generally well tolerated.103,104 Reported side effects include intense tanning, erythema, pruritus, urticaria, tenderness, a burning sensation, polymorphous light eruption, eczema herpeticum, and bacterial superinfection.59,60,105 However, because UVA1 phototherapy has only been available since the 1990s’, the long-term effects are still under investigation.
SPECIAL CONSIDERATIONS
SPECIAL CONSIDERATIONS
HIV
The safety of phototherapy and photochemotherapy in HIV-positive patients has been debated. UVR may activate HIV by the induction of nuclear factor κB,106-108
29
and UVB therapy increases HIV-1 gene expression in the skin.109-111 However, BB-UVB phototherapy does not appear to affect plasma HIV levels nor does it have an effect on CD4 counts.110,112,113 In general, phototherapy is thought to be safe for HIV patients.114 A consensus statement published by the American Academy of Dermatology in 2010 concluded that for moderate to severe psoriasis in HIV-positive patients, phototherapy and antiretrovirals are the recommended first-line therapeutic agents.115
CHILDREN
NB-UVB is now preferred to PUVA in children for most skin conditions, because of concern about PUVA side effects, including phototoxicity, carcinogenicity, photoaging, and the potential development of cataracts.
PREGNANCY
NB-UVB in a high mean cumulative dose (>118.16 J/cm2 in 36 treatments) and BB-UVB (110 to 220 mJ/cm2 in 7 to 22 treatments) can cause a proportionate decrease in serum folic acid levels. Although there are no specific guidelines, dermatologists should consider measuring folic acid levels intermittently, especially during the first trimester.116-118
ELDERLY
Phototherapy should be considered in patients older than 65 years of age if there are no physical and cognitive disabilities impairing use of phototherapy. However, it is important to be aware that UVB-induced erythema lasts longer and peaks later in the elderly.119
Also, photoadaptation may be decreased in the elderly secondary to decreased epidermal turnover, melanocyte number, and tanning response. Hence, it is important to consider initiating phototherapy at a lower dose and increasing dose levels more slowly to limit the number of phototoxic events.120
MISCELLANEOUS
Patients who have had arsenic exposure are at increased risk for cutaneous malignancies and should avoid phototherapy. Transplantation patients have a much higher risk of skin cancer compared to the general population because of the medications they are taking to prevent rejection of their transplanted organ. Consequently, there is a relative contraindication to phototherapy in transplantation patients. Photosensitizing medications should theoretically be avoided during phototherapy treatment, although in practice many patients receive phototherapy while taking tetracycline, hydrochlorothiazide, or other photosensitizing drugs without adverse consequences. There are reports of an association between chronic use of voriconazole and the development of aggressive cutaneous malignancies, including melanoma.121-123
3645
29
NB-UVB/ BB-UVB PUVA UVA1
Aquagenic pruritus − + −
Atopic dermatitis + + + (acute flares)
Cholestatic pruritus + − −
Chronic graft-versus-host disease + + +
Chronic hand eczema + + +
Chronic urticaria + +/− +/−
Cutaneous T-cell lymphoma + + +
Granuloma annulare − + +
Indolent systemic mastocytosis + + −
Lichen planus + + −
Localized and systemic scleroderma − + +
Lymphomatoid papulosis − + +
Perforating disorders + + −
Photodermatoses + + −
Pityriasis lichenoides + + −
Pruritus of chronic renal failure + − −
Pruritus of polycythemia vera + + −
Psoriasis + + −
Telangiectasis macularis eruptiva perstans − + +
Urticaria pigmentosa − +/− +
Vitiligo NB-UVB + −
Vitiligo NB-UVB + −
BB-UVB, broadband ultraviolet B; NB-UVB, narrowband ultraviolet B; PUVA, psoralen and ultraviolet A; UVA, ultraviolet A.
DISEASES AMENABLE TO PHOTOTHERAPY
PHOTOTHERAPY OF PSORIASIS
PHOTOTHERAPY
OF PSORIASIS
BROADBAND AND NARROWBAND ULTRAVIOLET B
Both BB-UVB and NB-UVB have been employed to treat psoriasis. Their presumptive mechanisms of action in this disease include its effects on DNA, antimicrobial actions that may alter the microbial flora of the skin,124 induction of anti-inflammatory and
3646
immunosuppressive cytokines,125-127 augmentation of vitamin D levels,128,129 alterations in antimicrobial peptides,129 modulation of vascular endothelial growth factor expression,130 restoration of Th17/Treg imbalance as well as function,131 suppression of Type I interferon signaling,132 a reduction in C-reactive protein,133
and decrease in serum plasmin.134
Clinical trials48 supporting the research findings51
that wavelengths in the range of 313 nm are most effective at clearing psoriasis have led to broad use of NB-UVB for psoriasis (Fig. 198-3). NB-UVB has thus become first-line therapy for chronic plaque psoriasis, and is considered to be superior to conventional BB-UVB with respect to both clearing and remission times.48,135 The difference in efficacy may be related to more efficient clearing of T cells by NB-UVB from the epidermis and dermis of psoriatic plaques compared with conventional BB-UVB.29 The end point of phototherapy is complete clearance of all psoriatic skin lesions. Psoriasis, however, is a chronic disease and the remission induced by UVB phototherapy is often shortlived. In a randomized, prospective, multicentered trial, investigators found that continuing UVB phototherapy, after initial clearing, contributes to control of the disease and is justified for many patients.136 The frequency of UVB treatments is reduced while maintaining the last dose given at the time of clearing. NB- UVB can be used safely in pregnancy and in children. Other agents (topical and oral) combined with UVB phototherapy may clear psoriatic skin lesions in a shorter period of time. Combined therapies may thus allow for fewer treatments and potentially less photoaging and fewer other risks. Often combination regimens are administered when phototherapy alone is no longer effective. Oral retinoids, such as acitretin,137 increase efficacy, particularly in patients with chronic plaque-type psoriasis.138-140 Addition of oral acitretin to either NB-UVB or the Goeckerman regimen (see next paragraph) reduces the total number of treatments necessary.141 Although fewer sessions may be required with combination therapy, the rate of relapse may be slightly higher. Methotrexate (15 mg/week) administered 3 weeks before starting NB-UVB can also enable quicker results in fewer phototherapy sessions.142 Biologic therapies are being evaluated in conjunction with phototherapy. Treatment with NB-UVB significantly accelerated the clearance of psoriatic lesions in patients responding slowly to etanercept.143
BB-UVB and NB-UVB phototherapy can be combined with topical agents to achieve higher clearance rates, longer disease-free intervals, and a lower risk of side effects. The Goeckerman regimen consists of the application of tar-containing topical agents with subsequent UV irradiation. The use of liquid carbonis detergens with NB-UVB is one example of a modified form of this regimen. The regimen is safe, convenient, effective, and leads to a more rapid improvement of psoriasis than light therapy alone.144 The antipsoriatic vitamin D analogs calcipotriol and calcitriol, used in conjunction
A
29
B
with NB-UVB, provide additional benefit compared to either the drugs or the phototherapy alone.145-150
Application of calcipotriol prior to phototherapy leads to unwanted degradation of vitamin D3, and calcipotriene increases the MED in patients, suggesting that it has a photoprotective effect.151 For these reasons, when used in combination with phototherapy, vitamin D analogs must be applied after the light treatment. Tazarotene 0.1% gel has an additive or synergistic effect when combined with NB-UVB.152 Because retinoids can cause photosensitivity, it is common practice to initiate phototherapy at 50% to 75% of the usual starting dose when tazarotene is used with UVB.153 Topical bexarotene gel 1% also has been combined with NB-UVB for the treatment of psoriasis and has greater efficacy than either alone.154 By decreasing scatter from scales in the stratum corneum, lubricants improve transmission of UVB, and a combination of topical lubricants with UVB therapy increases efficacy.155-157
The use of topical salicylic acid with UVB has not been found to increase the efficacy of UVB phototherapy because it blocks UVB penetration.157A
TARGETED PHOTOTHERAPY
Targeted phototherapy using a monochromatic 308- nm excimer laser or monochromatic excimer light is effective and safe for psoriasis. A large, multicenter
study found that fewer patient visits were required with targeted phototherapy compared to conventional phototherapy.158 The use of monochromatic excimer compared to cream PUVA has been found to have equivalent efficacy for palmoplantar psoriasis.159
Calculating the dose that induces blistering on a psoriatic plaque and treating the plaques at just below that dose can lead to clearance in significantly fewer sessions.160
PSORALEN AND ULTRAVIOLET A PHOTOCHEMOTHERAPY
Oral PUVA has consistently induced remission of psoriasis in clinical studies.73,161,162 At least a 75% improvement in the Psoriasis Area and Severity Index score can be expected after 12 weeks of PUVA treatments in 60% of patients.161 In some studies, oral PUVA has been observed to be more efficacious in clearing plaque psoriasis than NB-UVB, and the duration of remission is more prolonged,162 whereas other studies have found the 2 treatments to be comparable, particularly when NB-UVB is administered 3 times per week.163-166 It must be noted here that unlike drug administration, the success of PUVA and phototherapy generally depends in large part on physician-determined patient-specific subtle modifications of the regimen, such as dose increments between treatments, that optimize therapeutic response while avoiding burns or other adverse
3647
29
effects. Hence, the response to phototherapy may vary greatly among studies and among practitioners. Additionally, polymorphisms in genes encoding glutathione S-transferases are associated with PUVA sensitivity and these may have implications for treatment response.167
Repeated exposures are required to clear PUVAresponsive diseases, with gradual increments in dose as pigmentation and epidermal thickness increase. Upon clearing, patients are often transitioned to maintenance therapy, during which the frequency of treatments is gradually reduced. There are various maintenance algorithms. One regimen consists of 1 month of twice-weekly treatments, at the last UVA dose used for clearing, followed by another month of once-weekly exposures. A combination of PUVA and methotrexate can reduce the duration of treatment, number of exposures, and total UVA dose required for clearing. It is also effective in clearing patients unresponsive to PUVA alone.168 This combination appears to be safe if used during the clearing phase. However, long-term methotrexate, defined as 36 or more months of use, in combination with PUVA may increase the risk of lymphoma.93
The combination of cyclosporine with PUVA is not recommended because of the greatly increased risk of squamous cell carincoma.86 There are no published clinical trials combining PUVA with biologic agents. PUVA therapy is more efficacious when combined with a daily oral retinoid (etretinate, acitretin, isotretinoin; 1 mg/kg), a treatment regimen that has been referred to as RePUVA. The addition of an oral retinoid can bring patients into remission, even if they have not responded to PUVA alone.169 The oral retinoid is typically administered 5 to 10 days before initiating PUVA, and is continued throughout the clearing phase. RePUVA can often reduce the number of PUVA exposures by one-third and the total cumulative UVA dose by more than one-half. Oral retinoids when combined with PUVA have been shown to reduce the risk of SCC by 30%, although it does not alter the incidence of basal cell carcinoma.87 The mechanism of the synergistic action of retinoids and PUVA is unknown, but has been postulated to result in part from accelerated desquamation that optimizes the optical properties of the skin. Topical tazarotene gel 0.1% combined with oral PUVA accelerates the response to treatment.170
This may decrease exposure to UVA and thus the long-term hazards associated with PUVA therapy. Because of the photosensitizing effect to tazarotene, it is recommended that PUVA therapy be initiated at slightly lower doses than usual.153 Topical tazarotene plus PUVA bath therapy is also clinically and statistically superior to vehicle plus PUVA bath therapy.171
The application of salicylic acid in petrolatum just before PUVA therapy is not recommended as it may hinder the penetration of UVA.172 When calcipotriol
3648
is used with PUVA, it should not be applied within 2 hours of phototherapy.
TOPICAL AND BATH PSORALEN AND ULTRAVIOLET A FOR PSORIASIS
Application of 8-MOP in creams, ointments. or lotions followed by UVA irradiation is effective in clearing psoriasis, but may result in nonuniform distribution on the skin surface. This may induce unpredictable phototoxic erythema reactions and irregular patches of cosmetically unacceptable hyperpigmentation. Furthermore, the application of the medication is potentially labor intensive. For these reasons, topical psoralens are used most commonly in psoriasis for limited plaque psoriasis and palmoplantar disease.
PHOTOSENSITIVE PSORIASIS
Interestingly, UVA and UVB are both capable of triggering or aggravating psoriatic plaques in predisposed patients. This phenomenon appears to be linked to certain genetic traits, female gender and susceptibility to photosensitive disorders such as polymorphous light eruption. In predisposed individuals, there is a tendency toward creating a microenvironment that is inflammatory rather than immunosuppressive upon exposure to UVR, resulting in worsening of psoriatic disease.173 However, even though there are anecdotal reports of developing polymorphous light eruption secondary to NB- UVB treatment for psoriasis, NB-UVB can still be a viable treatment option in these patients. The strategy is to temporarily discontinue phototherapy until the lesions resolve and to restart at a much lower NB-UVB dose. NB-UVB should be increased slowly, which allows for treatment of psoriatic plaques with simultaneous photohardening that leads to resolution of polymorphous light eruption.174
PHOTOTHERAPY OF ATOPIC DERMATITIS
PHOTOTHERAPY OF
ATOPIC DERMATITIS
NARROWBAND ULTRAVIOLET B
Studies evaluating NB-UVB as a treatment for severe atopic dermatitis have shown that it improves severity scores, reduces potent topical steroid use, and provides a long-term benefit for most patients.175-178 Compared with bath PUVA, using half-body UVB versus UVA comparisons, NB-UVB and bath PUVA are both highly effective. Most patients, however, prefer NB-UVB. Relief of pruritus usually occurs in the first
2 weeks, prior to visible resolution of the cutaneous lesions.179 Additionally, improvements can be maintained months after phototherapy is stopped. NB-UVB can also be used sequentially following cyclosporine, to avoid relapse of disease.180
There is little information regarding the use of NB- UVB in children, and long-term data on the safety of this therapy are still needed. However, those studies that have examined NB-UVB for atopic dermatitis and other skin diseases in children have found that it is well-tolerated and produces excellent responses with no serious side effects.181-185 When side effects are mentioned, erythema is the most common182; other adverse reactions, such as herpes simplex reactivation, are rarely reported.183 In some cases, UVA combined with NB-UVB appears to provide added benefit.186
Long-term studies in animal models evaluating the carcinogenic potential of tacrolimus (0.03% and 0.1%) and pimecrolimus 1% did not find an increase in the incidence of UV-induced skin tumor growth.187 There are no studies evaluating the safety or efficacy of combined phototherapy with topical calcineurin inhibitors for atopic dermatitis in humans.
EXCIMER LASER AND ATOPIC DERMATITIS
The 308-nm xenon-chloride monochromatic excimer light has been evaluated in localized atopic dermatitis and has been shown to be efficacious in reducing its severity, and in diminishing its pruritus with lasting results.70,188-190 In extensive atopic dermatitis, this treatment is impractical, but it is particularly useful for atopic dermatitis involving the hands,70 and in situations in which there is an interest in limiting the use of topical steroids.
PSORALEN AND ULTRAVIOLET A
Oral PUVA is highly effective for the treatment of atopic dermatitis.191-194 In contrast to psoriasis, the number of treatments required for clearance of atopic dermatitis may be relatively high. Additionally, a rebound effect may occur in a high percentage of patients if the phototherapy is not combined with other therapies or if maintenance therapy is not instituted.191 Bath PUVA is also used for atopic dermatitis, primarily in Europe, and is a very effective treatment.195-197
ULTRAVIOLET A1
UVA1 phototherapy is a highly effective, nonsteroidal, therapeutic alternative for treatment of acute exacerbations of atopic dermatitis and is almost devoid of uncomfortable side effects.57,103,105,198 Doses of UVA1 (60 to 130 J/cm2 per day) over a 3-week period reduce the clinical severity of atopic dermatitis. However, effectiveness is short term and is followed by recurrence of
29
symptoms in a majority of patients.104,199 In one study, NB-UVB provided a greater therapeutic effect than UVA1 for chronic atopic dermatitis.200
PHOTOTHERAPY OF CUTANEOUS T-CELL LYMPHOMA
PHOTOTHERAPY OF
CUTANEOUS T-CELL
LYMPHOMA
PSORALEN AND ULTRAVIOLET A
PUVA photochemotherapy has been a successful therapeutic option for cutaneous T-cell lymphoma (CTCL) since the 1970s’.201,202 Complete clearing may be induced when malignant cells are confined to the epidermis and the superficial dermis, within the depth of UVA penetration. For the clearing phase, treatment schedules and dosimetry are essentially the same as for psoriasis. The treatment consists of 3 phases: a clearing phase, a maintenance phase, and monitoring off therapy. Maintenance therapy is not standardized; patients benefit most from individualized schedules.203 Therapy is discontinued after a variable period of time and patients are monitored. Relapses tend to respond as well as initially when PUVA is resumed. Patients with tumor-stage CTCL (IIB or greater) exhibit a high rate of early recurrences, which require permanent maintenance treatment. In these cases, PUVA typically is combined with other modalities to produce complete responses. Prolonged remissions have been observed with combinations of PUVA and interferon-α2a204 or low-dose interferon-α2b.205 In later stages of CTCL, PUVA has been employed as a palliative treatment, reducing the tumor-cell burden and acting synergistically with other treatments.202 For example, there has been success combining PUVA and oral bexarotene for the treatment of advanced CTCL (Sézary syndrome).206
Bathwater PUVA therapy with 8-MOP is a valuable phototherapeutic alternative, which can be considered for patients in whom systemic psoralen cannot be used. Excellent responses have been reported in patients with early stage mycosis fungoides207 and in children.208 There is also evidence of efficacy in patients with superficial folliculotropic mycosis fungoides.209 Cream PUVA with 8-MOP as a form of targeted UV therapy can be considered in patients with high risk of skin cancer.46
NARROWBAND ULTRAVIOLET B
NB-UVB may be as effective as PUVA for early stage CTCL.210-218 Some authors advocate starting with NB- UVB because of its more favorable safety and sideeffect profile.211 Clinical remissions are reported to last for 3216 to 24.5211 months; maintenance therapy tends to prolong remission.217 NB-UVB also has been used successfully in conjunction with oral bexarotene.219
3649
29
PHOTOTHERAPY OF VITILIGO
PHOTOTHERAPY
OF VITILIGO
PUVA and NB-UVB are two of the leading treatments for vitiligo. NB-UVB decreases IL-17 and IL-22 levels that are usually elevated in vitiligo and also increases FoxP3-expressing cells, restoring the balance between Th17 and regulatory T cells.220 It also appears to restore the balance of oxidant and antioxidants relieving oxidative stress that is considered to play a role in the pathogenesis of vitiligo.221 When employed for vitiligo, NB-UVB is typically administered 3 times per week.222
The earliest sign of response to therapy is perifollicular repigmentation. Cosmetically acceptable treatment success, defined as greater than or equal to 75% repigmentation, has been achieved in 12.5%223 to more than 75%224,225 of patients. Factors that predict how a patient will respond to NB-UVB include ethnic background, skin phototype, the areas treated,224-230 and the type of vitiligo.228 There does not appear to be an association between response to treatment and patients’ sex, age, family history of vitiligo, or the extent of body surface involvement.229-231 Patients who show early initial repigmentation are more likely to have a higher percentage of final repigmentation.223,229 In individuals with Fitzpatrick skin types IV and V, vitiliginous areas have been noted to repigment slightly darker than the surrounding skin. This resolves after a few months, resulting in a cosmetically acceptable outcome.222,229
Although data is somewhat limited, relapse rates may be anywhere from 25% to 84% after 1 year.229,232,233
Those who relapse tend to respond to another course of phototherapy. When NB-UVB is used in combination with topical tacrolimus 0.3% ointment, the therapeutic efficacy is higher than with NB-UVB alone.234 This synergistic effect is mediated through upregulation of MMP-2 and MMP-9 resulting in enhanced melanocyte migration.235
However, combination therapy is not effective in typical UV therapy–resistant sites such as the hands and feet.236 Pseudocatalase cream has been used in conjunction with NB-UVB. Whether pseudocatalase increases the efficacy of NB-UVB is controversial.237-239 In difficult-to-treat areas, laser dermabrasion in combination with topical steroids and NB-UVB twice weekly has been significantly more effective than just topical steroids and NB-UVB. Despite significant improvement in repigmentation rates, the procedure is poorly tolerated because of pain and there are risks of delayed wound healing and hypertrophic scarring.240 A novel approach using afamelanotide, an analog of melanocyte-stimulating hormone, combined with NB-UVB has shown significant improvement compared to NB- UVB monotherapy especially in patients with Fitzpatrick skin types IV through VI.236
Targeted phototherapy with a 308-nm excimer laser also is reported to be effective in vitiligo and should be considered first-line therapy in localized vitiligo.241-245
Sessions are performed 2 to 3 times weekly, with the ultimate rate of repigmentation dependent on the total
3650
number of sessions rather than the frequency.246,247 The treatments are well-tolerated and side effects are minimal. Excimer laser achieved the same grade of repigmentation as NB-UVB, but at a lower total cumulative dose.248 Because the laser is monochromatic, it can deliver higher energy exclusively to the affected areas while minimizing side effects. Similar to standard NB-UVB therapy, lesions on the face, neck, and trunk respond better than those on the extremities. The hands and feet have the least-favorable outcome.241,244,249-252
Combining a topical antioxidant gel with the excimer laser appears to have higher efficacy in terms of repigmentation than excimer laser alone.253 Monochromatic excimer light also is effective in patients with vitiligo, even if they have not previously responded to NB-UVB.61
Although PUVA was first used for vitiligo, it is used less often for that indication since the introduction of NB-UVB. Responses have been achieved in up to 70% of patients.254 Combination therapy of PUVA and a medium-potency topical corticosteroid is 3 times more effective than either treatment alone.255 In contrast to NB-UVB and PUVA, UVA1 does not cause repigmentation and only accentuates the difference in color between normal and vitiliginous areas by tanning the normal skin.
SCLEROTIC SKIN DISEASES
SCLEROTIC SKIN DISEASES
LOCALIZED AND SYSTEMIC SCLERODERMA
UVA1 has been reported to decrease lesional skin thickness, improve skin elasticity, reduce sclerotic plaques, and increase passive range of motion in localized scleroderma.256-258 There have been varying opinions as to the best dose and treatment regimen.259-261 In most studies, UVA1 has been administered at a dose of 60 to 130 J/cm2 5 times per week, although lower doses (20 J/cm2) also have been reported to be effective. When doses of 20 J/cm2 and 70 J/cm2 were compared, the higher dose caused greater improvement.259 However, when 130 J/cm2 was administered 3 times per week, the tanning response produced by the UVA1 treatments interfered with its ability to soften the sclerodermatous patches, implying that medium dose and less-frequent treatments would be more effective.261 The recurrence after successful UVA1 treatment was dependent on the duration of morphea prior to treatment rather than morphea subtypes, Fitzpatrick skin type, or medium-to-high-dose regimens implying that a medium-high dose of UVA1 is adequate in terms of prevention of recurrence.262
The mechanism of action is at least partly through induction of MMP-1,263 and downregulation transforming growth factor-β through the SMAD (Sma- and Mad-related protein) signaling pathway.264-266 UVA1 downregulates human beta-defensin, IL-6, and IL-8, which correlates with clinical improvement.267
UVA1 also has been used to treat acrosclerosis in patients with systemic scleroderma.268 Marked improvement was noted with softening of affected skin and increased finger movement. It also improved microstomia.269 Oral and topical PUVA also have been used for this disease, with improvement in range of motion and contractures.270 Oral PUVA has been used to treat disabling, extensive morphea in children.271-274
GRAFT-VERSUS-HOST DISEASE
In chronic graft-versus-host disease, NB-UVB has been employed as a second-line treatment in children275 and adults276 who are resistant to or have relapsed on standard immunosuppressive regimens. Oral PUVA,277-281 topical PUVA,282,283 and UVA1284-286 also have been employed. Bath PUVA in combination with isotretinoin is another option for sclerodermoid graft-versus-host disease.287 If phototherapy is to be employed for these patients, it is important to examine the patients regularly, as they already have an increased risk of skin cancer from their immunosuppressive therapies. There are anecdotal reports of successful treatment of sclerotic graft-versus-host disease with NB-UVB treatment.288
OTHER SCLEROTIC SKIN DISEASES
UVA1 has led to modest improvement in the degree of induration, and, at times, in mobility of the hands and legs in nephrogenic systemic fibrosis.121,289 Total treatments have ranged from 22 treatments (with a cumulative dose of 1855 J/cm2) to 50 treatments (3850 J/cm2). There are also anecdotal reports of its use in scleredema, vulvar lichen sclerosis and stiff skin syndrome, as well as radiation-induced morphea.60
PRURITUS
PRURITUS
UVB phototherapy is an option for the pruritus associated with chronic renal failure. Approximately 80% to 90% of patients improve within 2 to 5 weeks.290-292 If symptoms recur, they commonly respond to retreatment with UVB. For this disorder, phototherapy works on a systemic level rather than locally, because BB- UVB exposure to one-half of the body improves pruritus in both the exposed and unexposed sites.291 Some patients respond well to BB-UVB, but are less responsive to NB-UVB.293
Phototherapy is considered by some to be the most effective treatment for cholestatic pruritus.294-296 UVB phototherapy also has been combined with cholestyramine.297
PUVA has resulted in improvement in aquagenic pruritus in several patients, but maintenance treatments may be required.298-300
Treatment with NB-UVB 3 times a week,301 UVA in combination with UVB,302 and PUVA303-305 have been reported to improve the pruritus associated with polycythemia vera.
29
NB-UVB, BB-UVB, and PUVA have been used safely and effectively to treat eosinophilic folliculitis in HIVpositive patients.306-310
CHRONIC URTICARIA
CHRONIC URTICARIA
NB-UVB should be considered in patients who have failed first-line antihistamine regimens. It appears to be effective and well-tolerated. BB-UVB has a higher relapse rate. The observed efficacy of NB-UVB may be partly from the greater penetration into the dermis and relatively larger systemic immunosuppressive effects of NB-UVB in comparison to BB-UVB. PUVA or UVA therapy shows some efficacy but results are inconsistent.311
PHOTODERMATOSES
PHOTODERMATOSES
NB-UVB312-314 and oral PUVA315,316 are useful methods for preventing outbreaks of moderate to severe polymorphous light eruption. “Hardening” is obtained by exposing the individual to low levels of phototherapy while, at the same time, placing them prophylactically on oral corticosteroids to prevent the rash. Proposed mechanisms by which phototherapy induces tolerance to sunlight include thickening of the stratum corneum, hyperpigmentation, and cutaneous immune modulation by normalizing UV-induced inflammatory cytokines such as IL-1β,317 restoring impaired neutrophil chemotaxis,318 increasing regulatory T cells,319 and transiently decreasing Langerhans cells in the epidermis while increasing the mast cell recruitment into the papillary dermis.320 Although NB-UVB is currently used more commonly than PUVA, PUVA has the advantage of a rapid and intense pigment induction at relatively low UVA doses that usually remain well below the threshold for eliciting an outbreak. Approximately 10% of patients will develop typical polymorphous light eruption lesions during the initial phase of PUVA, but these usually disappear with continued treatment. Phototherapy is typically initiated 1 month before the first anticipated intense sun exposure, such as a sunny midwinter vacation. Once “hardening” has been induced, it must be maintained by frequent exposure to ambient sunlight. Novel home UVB low-intensity phototherapy devices that can be used each day for 6 minutes have shown better acceptance by patients while providing the same efficacy as a BB-UVB hospital treatment.321
Lesions of solar urticaria also can be prevented with phototherapy. The regimen involves induction of tolerance by repeatedly exposing the patient to graded doses of the causative wavelengths.322-324 Successful treatment has been achieved with repeated exposures to NB-UVB,325 UVA, or PUVA.322,324-327 PUVA may result in a response of greater duration. A condensed type of phototherapy called “rush hardening” also has been used.328 In rush hardening patients are exposed to quarter- or half-body UVA irradiation at 50% of the determined minimal urticarial dose with hourly increases in body surface area irradiation and dose.328 “Hardening”
3651
29
or “desensitization” has been reported to occur in as few as 3 days. The most important parameter in rush hardening is to determine the minimal urticarial dose and action spectra immediately before starting therapy and initiating the treatment at a dose lower than the minimal urticarial dose to minimize exacerabations.329 The disadvantage of this modality is that tolerance is lost quickly if the treatments are not continued every few days. For unexplained reasons, UVA1, which has effects on mast cells, is not particularly effective in preventing solar or other forms of urticaria. Chronic actinic dermatitis and actinic prurigo are other photosensitive disorders that are reported to benefit from controlled, low doses of UV irradiation.190,330,331
In contrast to polymorphous light eruption, an extended duration of treatment is often required for chronic actinic dermatitis.
OTHER DISEASES
OTHER DISEASES
LICHEN PLANUS
NB-UVB therapy has been used for recalcitrant lichen planus and is typically administered 3 times per week on nonconsecutive days. A complete response in 70% of patients has been reported after an average time of 10 weeks.332-334 Improvement in pruritus can be expected before disappearance of skin lesions. Oral and topical PUVA335 are other alternatives. In general, lichen planus tends to be more resistant to PUVA than psoriasis when treated with a similar schedule. A regimen of RePUVA may accelerate clearing, but has been reported to cause transient hyperpigmentation.336
NB-UVB produces similar outcomes, but some have reported a better initial clinical response with PUVA.337
Followup of patients who have cleared on PUVA shows that the disease reoccured at a higher frequency compared to non-PUVA group, raising the possibility that the treatment may prolong the disease.335 Although exceedingly rare, PUVA has been reported to induce lichen planus338 and lichen planus pemphigoides339
in patients undergoing the therapy for other skin diseases. In a small series, the excimer laser has successfully treated erosive oral lichen planus.340 However, the longterm effects of this form of radiant energy on the oral mucosa, which may also have been exposed to tobacco products, are unknown. Consequently, phototherapy for oral lichen planus should not be a first-line therapy for this form of the disease.
CHRONIC HAND ECZEMA
NB-UVB and local bath PUVA have been successful treatments for dyshidrotic eczema and chronic palmoplantar eczema.341-343 Bath PUVA may be less effective in smokers with dyshidrotic eczema.344 Oral PUVA is preferable for patients with hyperkeratotic eczema and bath PUVA is more beneficial for dyshidrotic eczema,345 although oral PUVA also is effective for dyshidrotic eczema.346
3652
Localized UVA1 has been used for dyshidrosis347,348 and has the same efficacy when compared to cream PUVA for chronic vesicular dyshidrotic eczema.347 Because the long-term effects of UVA1 are unknown, it has been recommended that courses of localized UVA1 phototherapy be performed no more than twice annually.
PITYRIASIS LICHENOIDES
NB-UVB and BB-UVB are safe and effective for both pityriasis lichenoides chronica349,350 and pityriasis lichenoides et varioliformis acuta.351 A complete response has been reported to occur with NB-UVB in 65% of pityriasis lichenoides et varioliformis acuta patients and a partial response in the rest.351 NB-UVB also led to a complete response in more than 85% of pityriasis lichenoides chronica patients.
LYMPHOMATOID PAPULOSIS
Oral PUVA has been used for patients with lymphomatoid papulosis,352,353 but relapse may occur upon cessation of therapy.353 Bath PUVA is effective in lymphomatoid papulosis in children.354,355 Some patients have also responded to targeted phototherapy with the 308-nm excimer laser.356 UVA1 (60 J/cm2) also has been employed,357 but relapses are common.
TELANGIECTASIA MACULARIS ERUPTIVE PERSTANS
Oral PUVA is reserved for telangiectasia macularis eruptiva perstans patients with severe disease, because other therapies, such as laser treatment, may be safer longterm, and because the response is often temporary.358-360
URTICARIA PIGMENTOSA
UVA1 phototherapy ameliorates both the objective and subjective symptoms of urticaria pigmentosa in adult patients, and long-term remission can be achieved in many cases.30,361,362 Although lesions may not respond completely with UVA1 therapy, the symptoms of pruritus are often relieved. Urinary histamine levels also decrease in response to UVA1. In some patients, systemic manifestations, such as diarrhea and migraine headaches, also have been reported to improve. In 1 patient with bone marrow infiltration, mast cell numbers decreased continuously after high-dose UVA1, which may have resulted from modulation of soluble cytokine production by UVA1-treated skin.30 PUVA does not decrease mast cell numbers, which may explain its limited benefit in many patients.363
INDOLENT SYSTEMIC MASTOCYTOSIS
In a small case series, NB-UVB phototherapy resulted in complete and long-term remission of cutaneous lesions and pruritus after approximately 40 total treatments and a total median cumulative dose of 51.4 J/cm2.364
Even though the number of treatments needed to achieve improvement in symptoms was lower with PUVA therapy, the average total exposure was higher with PUVA. In the case series, serum tryptase levels trended downward in patients receiving phototherapy and potentially may be used as a surrogate marker for response in some patients.365
GRANULOMA ANNULARE
Patients with widespread granuloma annulare treated with PUVA have had complete clearance of their disease.366 Maintenance therapy may result in prolonged disease-free intervals. Bath and cream PUVA also is reported to be useful for granuloma annulare.367-369
Although the mechanism of action of PUVA in granuloma annulare is unclear, selective elimination of pathogenic cells may be one explanation. UVA1 phototherapy provides good or excellent results in the majority of patients, but discontinuation of treatment is followed by early reoccurrence of disease.370 There are anecdotal reports of NB-UVB successfully treating disseminated granuloma annulare.371
PERFORATING DISORDERS
There has been some success in treating perforating disorders with NB-UVB phototherapy.372 There are anecdotal reports that PUVA also is effective.373 Patients are treated 2 to 3 times weekly, with lesions and symptoms clearing after 10 to 15 treatments. The mechanism by which improvement occurs is unknown.
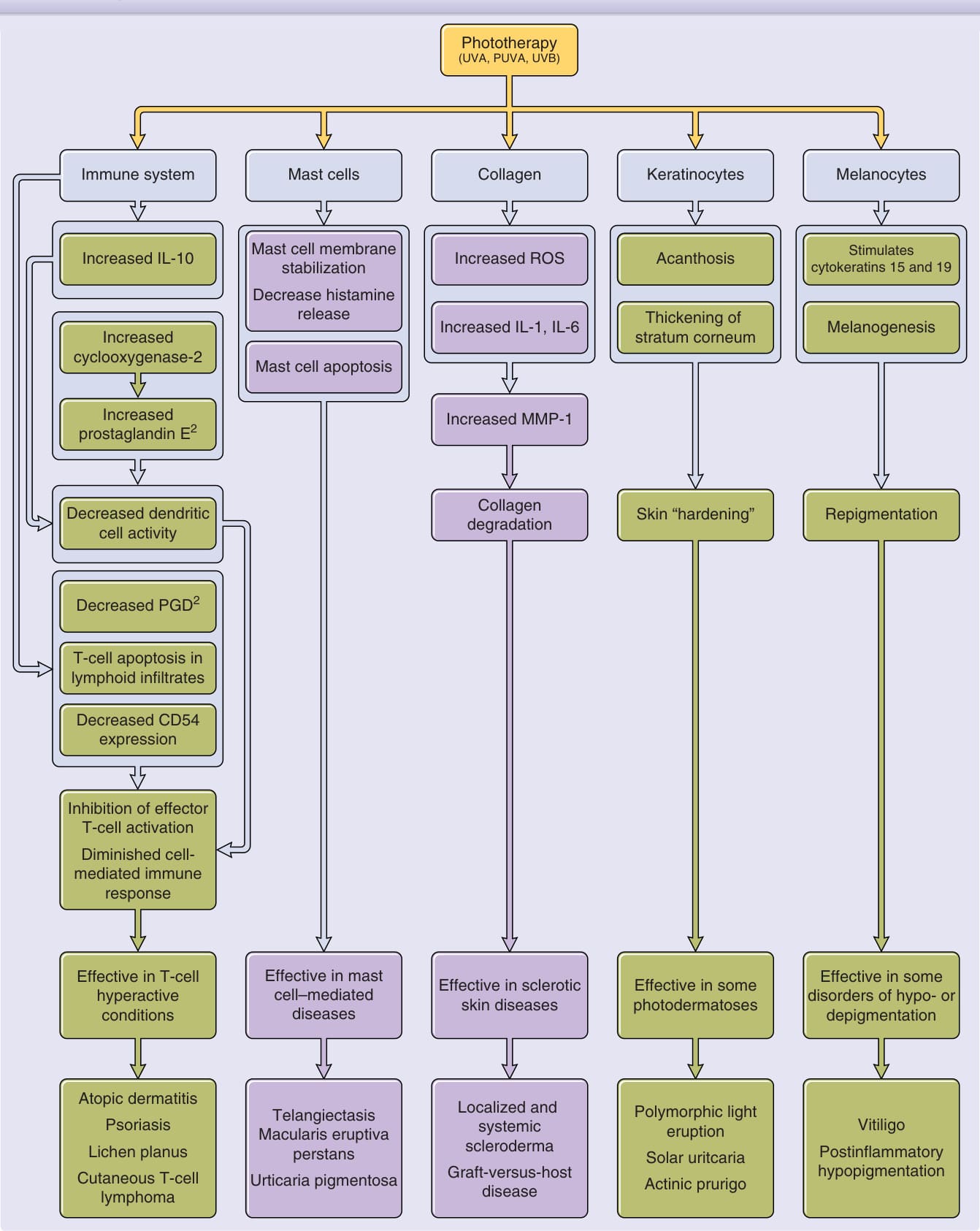
Figure 198-1 Summary of effects from ultraviolet A (UVA), psoralen and ultraviolet A (PUVA), or ultraviolet B (UVB) treatment. Detailed discussion in text. Boxes in purple indicate effects of either UVA and/or PUVA only, boxes in green indicate effects of both UVB and UVA and/or PUVA. The bottom two rows of boxes indicate clinical relevance of and application of skin changes induced by phototherapy. IL, interleukin; MMP, matrix metalloproteinase; PGD2, prostaglandin D2; ROS, reactive oxygen species.
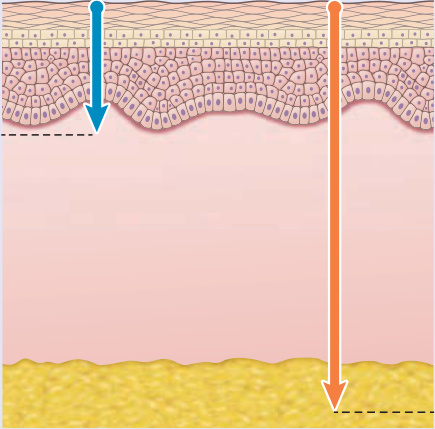
Figure 198-2 Depth of penetration in human skin for ultraviolet B (UVB) and ultraviolet A (UVA).

Figure 198-3 A, Psoriasis prior to narrowband ultraviolet B (NB-UVB) phototherapy. B, At the completion of NB-UVB therapy. (Photos used with permission from Herbert Hönigsmann, MD.)
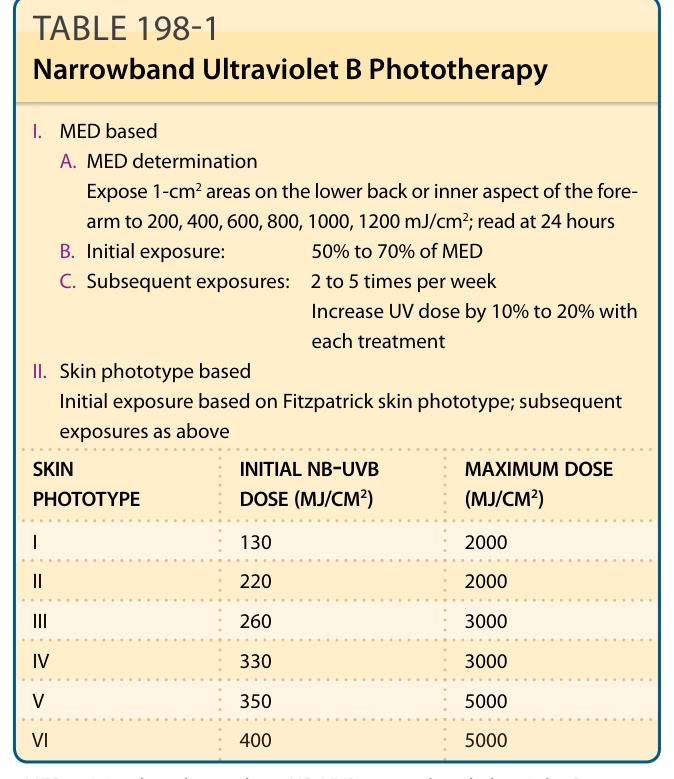
TABLE 198-1 Narrowband Ultraviolet B Phototherapy
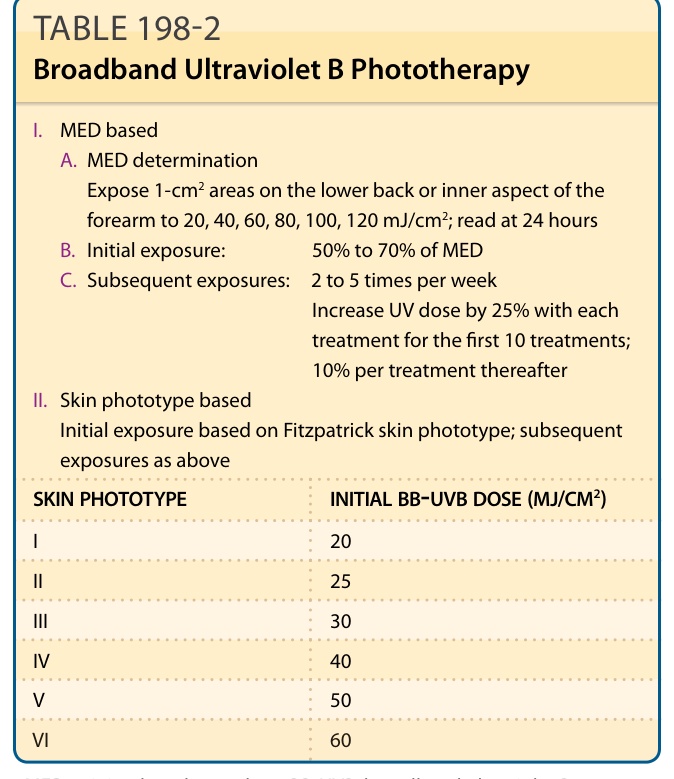
TABLE 198-2 Broadband Ultraviolet B Phototherapy
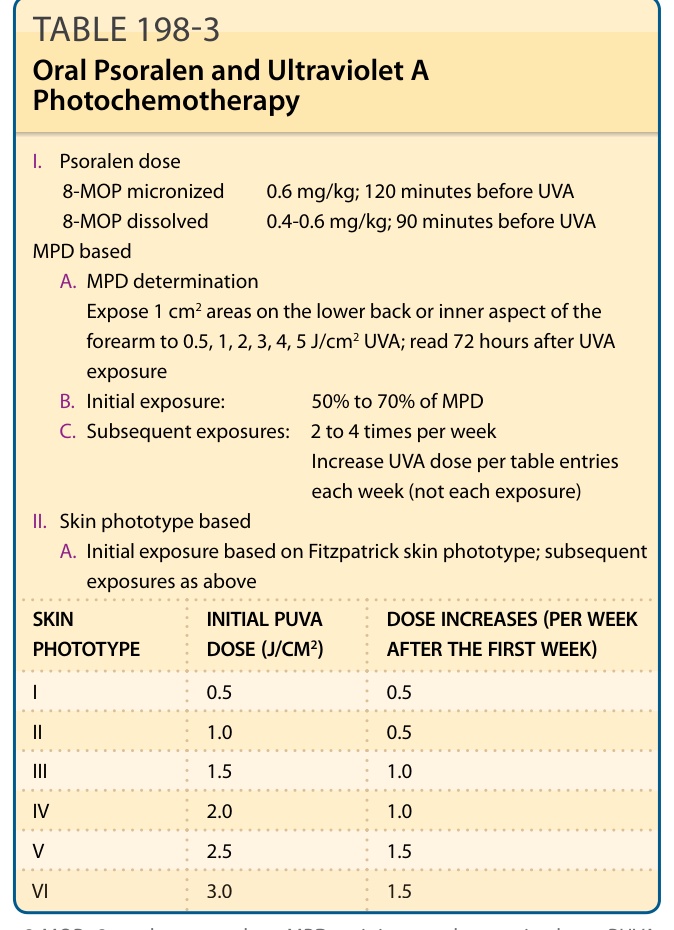
TABLE 198-3 Oral Psoralen and Ultraviolet A Photochemotherapy
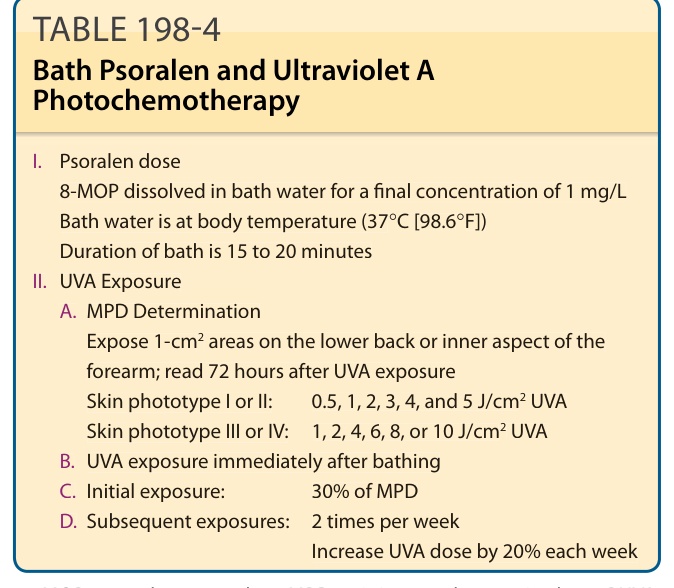
TABLE 198-4 Bath Psoralen and Ultraviolet A Photochemotherapy
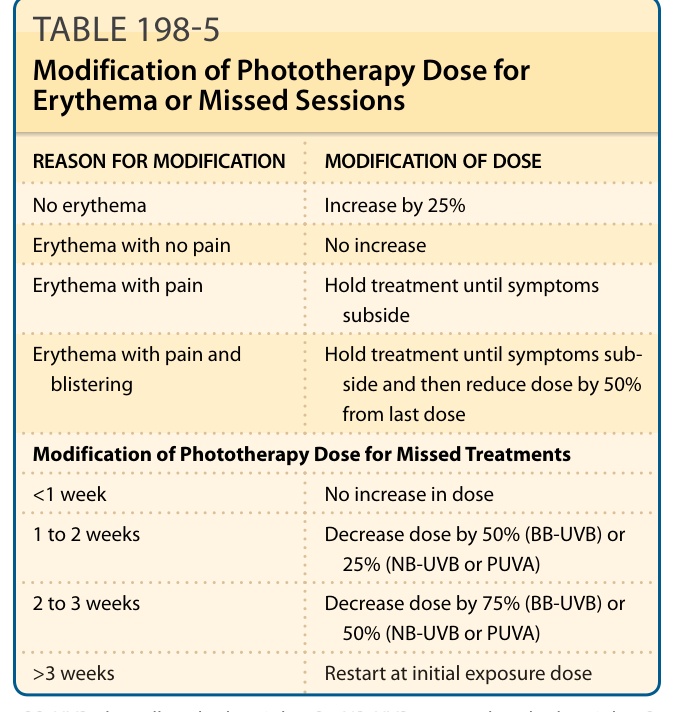
TABLE 198-5 Modification of Phototherapy Dose for Erythema or Missed Sessions
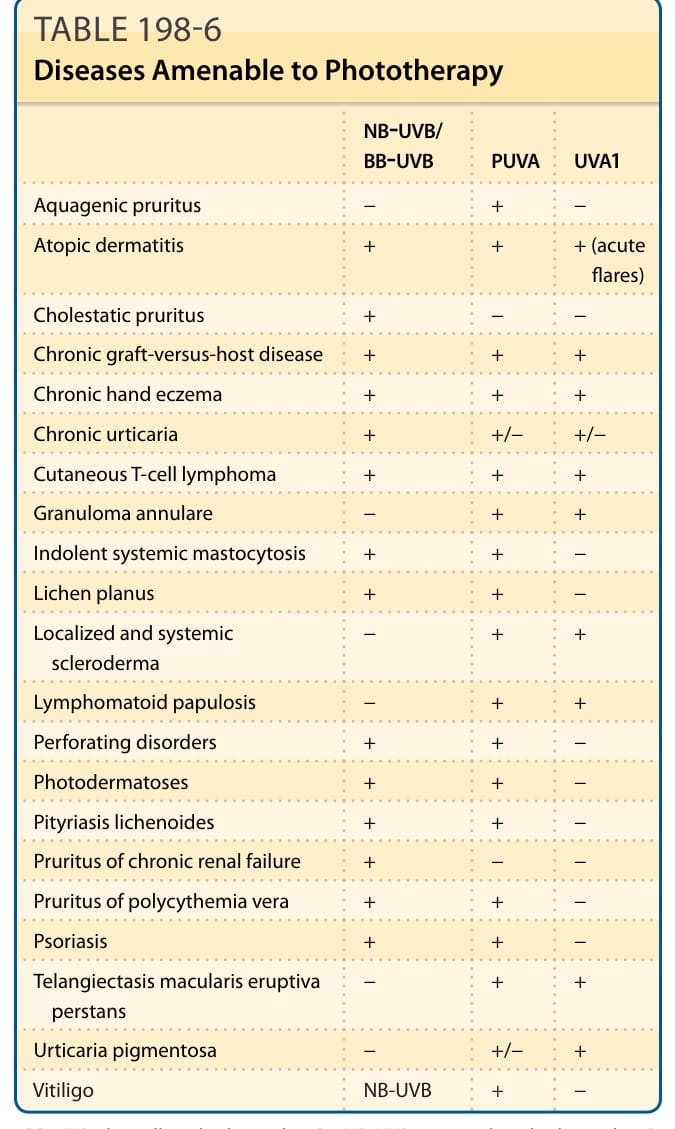
TABLE 198-6 Diseases Amenable to Phototherapy