Antiangiogenic Agents
28
AT-A-GLANCE
■ “Direct” antiangiogenic agents act directly on untransformed endothelial cells to prevent proliferation, migration, and survival.
■ “Indirect” antiangiogenic agents inhibit tumorproduced oncogene proteins that promote a proangiogenic state.
■ Antiangiogenic agents are a promising class of drugs because they are effective against slowgrowing tumors.
In 1971, Judah Folkman published a landmark paper hypothesizing that all tumor growth is dependent on angiogenesis and that inhibitors of angiogenesis could be used to treat cancers.1 The ensuing years have proven him correct and have seen the development of new agents that, either alone or in adjunct, have shown promise not only in oncology but in a variety of dermatologic conditions as well.2
Antiangiogenic drugs can be classified as either “direct” or “indirect;” the direct act directly on untransformed endothelial cells to prevent proliferation, migration, or survival, a process that normally occurs upon stimulation by proangiogenic molecules; the indirect act indirectly by inhibition of tumorproduced oncogenic protein products that promote proangiogenic states. Angiogenesis inhibitors as a drug class provide a unique approach to cancer treatment because they are also effective against slow-growing tumors, whereas traditional therapies, such as chemotherapy and radiation, work best on rapidly-dividing cells. In the future, the switch to an angiogenic phenotype may be able to be blocked in clinically undetectable cancers, thereby preventing disease progression using therapies directed, in part, by angiogenesis biomarkers.3,4 Although application of these agents center so far on oncologic and ophthalmologic diseases, promising and new dermatologic indications are sure to come.2
BECAPLERMIN (REGRANEX)
With the rise in incidence of diabetes and the increasingly aging population, chronic wounds have become increasingly prevalent. Treatment of these wounds is particularly challenging because normal woundhealing processes have been disrupted.2
MECHANISM OF ACTION
MECHANISM OF ACTION
Becaplermin (recombinant human platelet-derived growth factor BB) is the first FDA-approved angiogenesis-stimulating therapy. Endogenous plateletderived growth factor (PDGF) is chemotactic for several cell types necessary for wound healing, and is also a mitogen for fibroblasts, the source for extracellular matrix components like glycosaminoglycans and fibronectin. Thus, PDGF is an important factor in the formation of granulation tissue.5
INDICATIONS
INDICATIONS
Becaplermin gel is currently indicated for the treatment of lower extremity, diabetic, neuropathic ulcers which must be adequately vascularized and reach to at least the level of subcutaneous tissue.5-7 Off-label uses include the application of becaplermin to ulcerated hemangiomata, surgical wounds, grafts, pyoderma gangrenosum, calciphylaxis, ulcerated necrobiosis lipoidica, and flaps.8-11 However, cost-effectiveness of this form of therapy in the treatment of diabetic foot ulcers is also outlined.12
CONTRAINDICATIONS
CONTRAINDICATIONS
Becaplermin gel is contraindicated in patients with known cancer within the treatment area or a history of hypersensitivity.2 Efficacy has not been established for pressure and venous stasis ulcers. Efficacy has also
28
Points of action: targets of some antiangiogenic drugs
Normal skin Dysplasia (precancer) Malignancy
Imiquimod induces endogenous IFN
IFN-α/β, Tsp-1, TIMP
VEGF, bFGF
IFN-α/β, Tsp-1, TIMP
Avastin-blocks VEGF-VEGFR-2 interactions
VEGF bFGF
Thalidomide Velcade Curcumin Honokiol inhibit NF-κB
HIF, Akt, NF-κB MAPK
VEGF, bFGF, angiopoietin-2, CRH
MMPs digest basement membrane, releasing growth factors
Tetracycline antibiotics inhibit MMPs
COX-2
Rapamycin
- inhibits translation of VEGF mRNA
- inhibits protein synthesis in endothelial cells
not been evaluated for diabetic neuropathic ulcers that do not extend through the dermis into subcutaneous tissue or for ischemic diabetic ulcers.5
DOSING REGIMEN
DOSING REGIMEN
Becaplermin gel should be applied topically once daily with dose depending on the size of the lesion; generally, every square inch of ulcer requires two-thirds inch of gel from a 15-g tube or one-and-one-third inches of gel from a 2-g tube. After application, the area should be covered with a saline-moistened dressing, then left in place for approximately 12 hours. The dose should be recalculated every 1 to 2 weeks to ensure accurate dosing as the wound changes size. Becaplermin gel should be used in conjunction with standard proper ulcer care.5
MONITORING THERAPY
MONITORING THERAPY
If there is less than a 30% decrease in size after 10 weeks or if the wound has not completely healed after
20 weeks of treatment, the treatment plan should be reevaluated.5
RISKS AND PRECAUTIONS5,13,14
RISKS AND
PRECAUTIONS
5,13,14
■ Because becaplermin gel is nonsterile, it should not be applied to wounds closed by primary intention.
■ An increased rate of mortality because of malignancy has been observed in patients treated with 3 or more tubes of becaplermin gel. Consequently, caution should be used in patients with a known history of malignancy. However, a newer cohort study has shown that such malignancy association is not yet completely established.
■ Pregnancy category: C.
■ The safety and efficacy of becaplermin have not been evaluated in children younger than 16 years of age.
3591
28
COMPLICATIONS (SOME EXAMPLES)5
COMPLICATIONS (SOME
EXAMPLES)
5
■ Rash
■ Hypersensitivity reaction (most often to the paraben or m-cresol components)
■ Ulcer-related complications (incidence was similar in becaplermin vs placebo groups)
BEVACIZUMAB (AVASTIN)
MECHANISM OF ACTION
MECHANISM OF ACTION
Bevacizumab is a recombinant, humanized immunoglobulin G1 monoclonal antibody against vascular endothelial growth factor (VEGF). VEGF is a growth factor that promotes angiogenesis by supporting endothelial cell replication and survival as well as vascular permeability. This potent proangiogenic molecule is upregulated in a majority of human tumors and serves to alter tumor vasculature.2
Binding of bevacizumab to VEGF is direct and specific. The antibody also competitively binds VEGF receptor 1 (VEGFR-1) and VEGFR-2, preventing VEGF from binding to its receptors and initiating the signaling cascade. It also reduces and normalizes tumor vascularity.15 In addition, changes in interleukin (IL)-8 or soluble VEGFR-2 levels at second cycle appear predictive for response.16 Specifically talking about metastatic colorectal cancer, a recent report suggests that NOTCH1 hyperexpression is a detrimental prognostic factor in patients treated with chemotherapy plus bevacizumab.17
INDICATIONS
INDICATIONS
In February 2004, bevacizumab became the first antiangiogenesis drug approved by the U.S. Food and Drug Administration (FDA) for first-line treatment of metastatic colorectal carcinoma when given in combination with intravenous 5-fluorouracil–based chemotherapy. Bevacizumab also has indications for non–small-cell lung cancer, cervical cancer (including metastatic), glioblastoma, ovarian (epithelial), fallopian tube, primary peritoneal cancer (platinum-resistant/sensitive recurrent), metastatic renal cell carcinoma, head and neck squamous cell carcinoma, gastric cancer, and renal carcinoma.18-25 Bevacizumab, in combination either with other antiangiogenic agents or with chemotherapy, even if isolated, is currently being investigated in metastatic melanoma, hemangioendothelioma, angiosarcoma, metastatic colorectal cancer, age-related macular degeneration, retinoblastoma, corneal neovascularization, and ovary tumor.17,18,26-32
Other than a history of hypersensitivity, no known contraindications to bevacizumab therapy exist.18
3592
Bevacizumab-induced inhibition of angiogenesis promotes a more homogeneous intratumoral distribution of paclitaxel, improving the antitumor response.33 In general, bevacizumab prolongs progression-free survival and overall survival, and increases the 1-year survival rate in cancer patients as compared with control therapy.34
COMPLICATIONS (SOME EXAMPLES)18,35,36
COMPLICATIONS (SOME
EXAMPLES)
18,35,36
■ GI perforation with associated intraabdominal abscess or fistula formation.
■ Wound dehiscence (incisions should be healed completely before treatment initiation; drug should be held for at least 28 days prior to elective surgery).
■ Serious hemorrhagic events including hemoptysis, GI bleeding, CNS hemorrhaging, epistaxis, vaginal bleeding, and pulmonary hemorrhage. Use in patients with active hemorrhaging or recent history of hemoptysis is not advised.
■ Arterial thromboembolic events, including cerebral infarction, transient ischemic attacks, myocardial infarction, and angina.
■ Reversible posterior leukoencephalopathy syndrome, a neurologic disorder characterized by headache, seizure, lethargy, confusion, blindness, and other visual or neurologic disturbances, that is diagnosed and confirmed by MRI.
■ Hypertension (monitoring every 2 to 3 weeks during course of treatment is advised).
■ Proteinuria.
■ Infusion reactions.
BORTEZOMIB (VELCADE)
MECHANISM OF ACTION
MECHANISM OF ACTION
Bortezomib is the first proteasome inhibitor to gain FDA approval. This novel class of drugs acts by impairing the ability of the proteasome to degrade a variety of ubiquitinated proteins. Proteasome inhibitors may promote a proapoptotic state by preventing the degradation of tumor-suppressor proteins, such as p53 and inhibitors of nuclear factor κB (NF- κB). NF-κB upregulates the transcription of genes involved in neoplastic progression including VEGF.37 Bortezomib also acts directly to inhibit chemotaxis, capillary formation, and transcription of VEGF, IL-6, insulin-like growth factor-1, ang-1, and ang-2.38,39 Because it has been shown to correlate with NF-κB activity, chemoresistance might also be lessened in the presence of bortezomib. Moreover, bortezomib inhibits the angiogenesis mediated by mesenchymal stem cells.40
INDICATIONS
INDICATIONS
Bortezomib is currently indicated for the treatment of recurrent or refractory multiple myeloma and mantle cell lymphoma.38 Investigational applications include cutaneous T-cell lymphoma, squamous cell carcinoma, and metastatic melanoma.41 It has been reported that the combination of bortezomib, melphalan, dexamethasone, and intermittent thalidomide is an effective regimen for relapsed/refractory myeloma and is associated with improvement of abnormal bone metabolism and angiogenesis.42 Good results can be obtained when bortezomib is combined with bevacizumab to treat temozolomide-resistant malignant gliomas.43
CONTRAINDICATIONS39
CONTRAINDICATIONS
39
■Hypersensitivity to bortezomib, boron, or mannitol.
COMPLICATIONS (SOME EXAMPLES)39
COMPLICATIONS (SOME
EXAMPLES)
39
■ Hypotension
■ Peripheral neuropathy
■ Acute respiratory distress syndrome
■ Blood dyscrasias (neutropenia, thrombocytopenia)
■ Fatigue, malaise, and weakness
■ Cytochrome P450 (CYP) 3A4 drug metabolism interactions
■ Skin rash
CETUXIMAB (ERBITUX)
MECHANISM OF ACTIONS
MECHANISM OF ACTIONS
Cetuximab is a chimeric, human–murine monoclonal antibody against the epithelial growth factor receptor (EGFR), and, as such, competitively inhibits the binding of epithelial growth factor (EGF), transforming growth factor, and other associated ligands. Downstream signaling blockade results in myriad antitumor properties, including decreased proliferation, cellular motility, and invasive potential via downregulation of signaling molecules such as basic fibroblast growth factor (bFGF, a product of keratinocytes) and IL-8.44,45 Angiogenesis is also inhibited through decreased EGFR-mediated VEGF expression. When combined with irinotecan, cetuximab has synergistic antiangiogenesis and antiinvasion activities mediated by downregulation of phosphatidylinositol-3-kinase (PI3K)/Akt and mitogenactivated protein kinase/extracellular signal-regulated kinase (ERK) pathways46; such combination seems to induce a sudden, long-lasting reduction in VEGFcirculating levels, as well as an increase in interferon (IFN)-γ.44 In addition, cetuximab may inhibit tumor growth and angiogenesis induced by ionizing radiation.47
28
INDICATIONS
INDICATIONS
Cetuximab is currently indicated for the treatment of metastatic colorectal carcinoma and squamous cell carcinoma of the head and neck, either alone or in combination with radiation or chemotherapy.48 Additionally, its use in squamous cell carcinoma of the skin is currently under investigation. Given the demonstrated role of EGFR in melanoma, cetuximab may also play an eventual role in melanoma treatment. Be aware, however, that EGFR inhibitors are contraindicated in organ transplantation, as they can stimulate immunity. The subconjunctival use of cetuximab and bevacizumab to inhibit corneal angiogenesis has been reported in the literature.29
COMPLICATIONS (SOME EXAMPLES)48
COMPLICATIONS (SOME
EXAMPLES)
48
■ Serious infusion reactions
■ Acneiform neutrophilic folliculitis—appearance correlates with clinical response
■ Pruritus
■ Electrolyte disturbances
■ Abdominal pain and upset
■ Infections associated with neutropenia
CORTICOSTEROIDS
The role of corticosteroids in angiogenesis is a bit of a mixed picture, with neutral, antiangiogenic, and proangiogenic effects having been observed in various cases. In the setting of uveal melanoma, El Filali and colleagues demonstrated no significant differences in levels of VEGF, PDGF, or thrombospondin 1 (TSP-1) in in vitro models treated with triamcinolone acetate.49
In vivo and in vitro models of prostate cancer have shown potentiation of antiangiogenesis by docetaxel when concurrently exposed to dexamethasone as measured by levels of VEGF, IL-8, and chemokine ligand-1.50 Contrastingly, sequential delivery of dexamethasone followed by VEGF showed an increase in vascularity in a biosensor-model implant into murine subcutaneous fat.51 Whatever the ultimate mechanism and role, the clinical usefulness of steroids as antiinflammatory and antiangiogenic agents is readily apparent.
ERLOTINIB (TARCEVA)
MECHANISM OF ACTION
MECHANISM OF ACTION
Erlotinib is a small-molecule phosphorylation inhibitor that specifically inhibits the EGFR tyrosine kinase. Acting intracellularly, erlotinib downregulates the expression of VEGF via the PI3K/Akt signaling pathway.2 When combined with cisplatin, erlotinib inhibits growth and angiogenesis through c-MYC and hypoxia inducible factor (HIF)-1α in EGFR-mutated lung cancer.52
3593
28
INDICATIONS
INDICATIONS
Erlotinib is currently indicated for the treatment of non–small-cell lung cancer and pancreatic cancer.53
There is an ongoing clinical trial investigating using the combination of erlotinib and bevacizumab in stage 4 melanoma. Other than a history of hypersensitivity, there are no known contraindications.2 Preliminary clinical trials have shown that association of erlotinib with pazopanib, an oral angiogenesis inhibitor, can work perfectly together to obtain better results against angiogenesis.54
COMPLICATIONS (SOME EXAMPLES)53
COMPLICATIONS (SOME
EXAMPLES)
53
■ Acneiform rash
■ GI upset
■ CYP450, CYP1A2, and CYP3A4 drug metabolism interactions
EVEROLIMUS (AFINITOR)
MECHANISM OF ACTION
MECHANISM OF ACTION
Everolimus is another mammalian target of rapamycin (mTOR) inhibitor classified as semisynthetic because it is derived from sirolimus; it has a shorter half life than sirolimus, but better oral bioavailability and less frequent toxic side effects.55 This agent also complexes with FK-binding protein 2 to inhibit mTOR, suppress HIF-1α, and block VEGF-mediated vascular endothelial cell stimulation, bFGF-induced angiogenesis, and T-cell activation and proliferation.56,57 Nevertheless, a few years ago, everolimus was linked with lymphangiogenesis, after causing hyperexpression of prospero homeobox protein 1, podoplanin, VEGFR-C, and VEGFR-3 in chick chorioallantoic membranes treated with it.58
INDICATIONS
INDICATIONS
Everolimus is indicated for the treatment of advanced renal cell carcinoma after failure of sunitinib or sorafenib, and as an agent in drug-eluting stents.59
Everolimus is approved for astrocytoma and breast, neuroendocrine, renal angiomyolipoma with tuberous sclerosis complex, and renal cancers.58,59 Some other commercial brands are also approved for liver and renal transplantation.59 Dermatologic, off-label applications are limited to a case report of its use in psoriasis.60 Recently, it was shown that immune modulatory oligonucleotide, a toll-like receptor 9 agonist, cooperates with everolimus in renal cell carcinoma by interfering with tumor growth and angiogenesis.61
3594
COMPLICATIONS (SOME EXAMPLES)59
COMPLICATIONS (SOME
EXAMPLES)
59
■ Noninfectious pneumonitis
■ Susceptibility to infections
■ Oral ulceration and mucositis
■ Blood dyscrasias
■ Musculoskeletal pain
■ CYP3A4 drug metabolism interactions
IMIQUIMOD (ALDARA)
MECHANISM OF ACTION
MECHANISM OF ACTION
Imiquimod (imidazoquinoline) is both the first immune response modifier and the first topical antiangiogenic agent for dermatologic use. Imiquimod acts by inducing the activation of toll-like receptor 7 in immune cells. Toll-like receptor 7 activation enhances the innate immune response by increasing endogenous IFN and interleukin production, including IFN-α, IFN-β, IFN-γ, IL-10, IL-12, and IL-18; these cytokines also function as endogenous angiogenesis inhibitors.62,63 The upregulation of these cytokines, as well as of other endogenous angiogenesis inhibitors, such as IFN-inducible protein 10, tissue inhibitor of metalloproteinases, and TSP-1, is the basis for imiquimod’s antiangiogenic activity.64 Additionally, imiquimod also downregulates proangiogenic factors such as bFGF and matrix metalloproteinase 9. In vivo, imiquimod has been shown to inhibit angiogenesis in human bowenoid papulosis, hemangioendothelioma, cutaneous melanoma, and murine lung sarcoma cells.64-66 A topical combination therapy of imiquimod and gentian violet for cutaneous melanoma metastases has been reported67; recently, we have observed that such combination can be helpful for plantar warts as well (unpublished data).
INDICATIONS
INDICATIONS
Imiquimod is currently approved for the treatment of clinically typical, nonhyperkeratotic, nonhypertrophic actinic keratosis on the face or scalp, and biopsyconfirmed, primary, superficial basal cell carcinoma located on the trunk, neck, or extremities (maximum tumor diameter of 2 cm) in immunocompetent adults. It is also approved for the treatment of external genital and perianal condyloma acuminata.68 Several studies have shown efficacy in squamous cell carcinoma, lentigo maligna, hemangiomas, Kaposi sarcoma, pyogenic granuloma, discoid lupus erythematosus, and port-wine stain in combination with pulsed-dye laser.69-74 Other than a history of hypersensitivity, there are no known contraindications.2
PHARMACOKINETICS
PHARMACOKINETICS
Imiquimod is only minimally absorbed transdermally, with less than 0.9% of the topical dose being excreted in the urine or feces.68
DOSING REGIMEN68
DOSING REGIMEN
68
■ Actinic keratosis: Patients are to apply the cream 2 times per week to the face or scalp but not both concurrently, preferably before sleeping hours. The area should be washed with a mild soap and water and allowed to dry before application. After approximately 8 hours following application, the area should again be washed with mild soap and water to remove the agent. Treatment should continue for a full 16 weeks, and should not be extended because of missed doses or skip periods.
■ Superficial basal cell carcinoma: Following biopsy confirmation, patients are to apply the cream 5 times per week to the affected area plus 1 cm around the lesion, preferably before sleeping hours. The area should be washed with a mild soap and water and allowed to dry before application. After approximately 8 hours following application, the area should again be washed with mild soap and water to remove the agent.
■ External genital and perianal condyloma acuminate: Patients are to apply the cream 3 times per week to the affected area, preferably before sleeping hours. The area should be washed with a mild soap and water and allowed to dry before application. After approximately 6 to 10 hours following application, the area should again be washed with mild soap and water to remove the agent. Treatment should continue until the lesion(s) completely resolve or until a maximum course of 16 weeks.
RISKS AND PRECAUTIONS68
RISKS AND PRECAUTIONS
68
■ Immunosuppression: The safety and efficacy of imiquimod has not been established in immunosuppressed patients.
■ Photosensitivity: Patients should be instructed to avoid or minimize exposure to sunlight or sunlamps during the treatment course.
■ Pregnancy class: C.
■ Pediatrics: The safety and efficacy of imiquimod has not been established in the treatment of external genital and perianal condyloma acuminate in children younger than 12 years of age, or in the treatment of actinic keratosis or superficial basal cell carcinoma in children younger than 18 years of age.
28
COMPLICATIONS (SOME EXAMPLES)68
COMPLICATIONS (SOME
EXAMPLES)
68
■ Local skin toxicities: Frequency of local skin toxicities include: erythema (97%), flaking/scaling/ dryness (93%), scabbing crusting (79%), induration (78%), edema (71%), erosion/ulceration (54%), vesicles (29%), and weeping or exudates (22%). Patients should be instructed to contact their health care provider if they experience any sign or symptom in the treatment area that restricts or prohibits daily activity or makes continued application of the cream difficult; a rest period of a few days may be necessary. Additionally, to reduce the likelihood of an adverse reaction, the agent should not be applied under occlusion other than porous gauze or cotton underwear. Health care providers should evaluate for possible bacterial superinfection when assessing reactions to imiquimod.
■ Decreased wound healing: Recent wounds should be allowed to heal completely prior to initiating treatment.
■ GI upset.
■ Upper respiratory tract infection, coughing, sinusitis.
■ Musculoskeletal pain.
■ Headache.
INTERFERON-`2b (INTRON A)
IFN-α made history in 1988 as the first antiangiogenic therapy used in humans for the successful treatment of pulmonary hemangiomatosis in a pediatric patient. IFN-α2b is a synthetic cytokine made from the bacterium Escherichia coli transformed with recombinant DNA and has similar actions to its natural endogenous counterpart, IFN-α, a type I IFN produced endogenously by the immune system.2
MECHANISM OF ACTION
MECHANISM OF ACTION
The IFNs act through the Janus kinase–signal transducers and activators of transcription (JAK-STAT) pathway. IFN-α, which is both a direct-on-endothelialcells agent, including impairment of their proliferation and migration75 as a result of delayed progression from the S-phase to the G2-phase of the cell cycle and resulting in the inhibition of Cdc2 kinase activity,76 and an indirect-on-endothelial-cells antiangiogenic agent, was first observed to impair capillary endothelial cell migration. Its properties as an indirect antiangiogenic agent include the ability to decrease tumor cell production of bFGF, which may explain its success in treating hemangiomata.4 Further actions, such as downregulation of IL-8 and VEGF gene expression,75 work together
3595
28
to interfere with both blood vessels and tumor cell proliferation, leading to regression of tumors without necrosis.75 IFN-α has well-known antiviral activity and antitumor activity, which may be mediated in part by upregulating major histocompatibility complex Class I antigen expression, activating natural killer cells, controlling progression through cell-cycle checkpoints, and activating apoptosis.2 In vitro assays also demonstrate ability for IFN-α to inhibit osteoclast differentiation and renal cell carcinoma-induced angiogenesis by reducing calcium-phosphate resorption activity and expression of proteoclastic transcription factor c-Fos; by inhibiting bone endothelial cell proliferation and the expression of FGF-2; and by inhibiting secretion of FGF-2.77
INDICATIONS
INDICATIONS
INF-α2b is currently indicated for the treatment of chronic hepatitis B (which may be chemopreventive against hepatocellular carcinoma), chronic hepatitis C, AIDS-associated Kaposi sarcoma, and condylomata acuminata. It is also indicated in malignant melanoma (adjuvant to surgical therapy in patients who are at high-risk of systemic recurrence; must be administered within 56 days postoperatively), hairy cell leukemia, and follicular lymphoma.78 Off-label uses in dermatology include cutaneous T-cell lymphoma (mycosis fungoides) and basal and squamous cell skin cancers. It also has been used in the treatment of infantile hemangiomas along with corticosteroids or in the event of corticosteroid resistance; however, given rising concerns over the risk of spastic diplegia (especially in children younger than 1 year of age), its usefulness in this setting has been somewhat tempered.79
Early reports had shown that combination therapy of IFN-α and 5-fluorouracil inhibits tumor angiogenesis in human hepatocellular carcinoma cells by regulating VEGF and angiopoietins.76
CONTRAINDICATIONS78
CONTRAINDICATIONS
78
■ Hypersensitivity to IFN-α or any drug components
■ Combination IFN-α and ribavirin therapy in pregnancy or in males whose female partners are pregnant
■ Autoimmune hepatitis
■ Personal history of a hemoglobinopathy (eg, sickle cell disease, thalassemia major)
■ Renal insufficiency (creatinine clearance <50 mL/min)
PHARMACOKINETICS
PHARMACOKINETICS
IFN-α2b comes as a powder that, upon reconstitution, should be used immediately but may be stored up to 24 hours at 2°C to 8°C (36°F to 46°F). It can be given
3596
DISEASE DOSE
Malignant melanoma high-dose regimen Induction: 20 million IU/m2 IV infusion over 20 minutes, 5 consecutive days/ week for 4 weeks
Maintenance: 10 million IU/m2 subcutaneously 3 times/week for 48 weeks
Maintenance: 3 million IU/m2 subcutaneously 3 times/week for 1 year
Malignant melanoma adjuvant low-dose regimen (in clinical trials)
AIDS-related Kaposi sarcoma 30 million IU/m2 subcutaneously or IM 3 times/week until disease progression or maximal response has been achieved after 16 weeks
Condylomata acuminata 1 million IU per lesion (maximum of 5 lesions per course) 3 times/week on alternate days for 3 weeks; may administer additional courses at 12- to 16-week intervals
Hemangiomas 3 million U/m2/day for at least 6 months
Hemangiomas 3 million U/m2/day for at least 6
months
by subcutaneous, IM, IV, or intralesional routes. Its half-life is 3 to 12 hours when given subcutaneously or IM and 30 minutes when given IV. The drug is likely metabolized by the kidneys. Polyethylene glycol IFN- α2b has a 10-fold increase in half life, decreased toxicity, and increased compliance.78,80 Table 195-1 outlines dosing regimens.
COMPLICATIONS (SOME EXAMPLES)78,79
COMPLICATIONS (SOME
EXAMPLES)
78,79
■ Flu-like symptoms (headache, fatigue, fever, chills, tachycardia, myalgia, and anorexia)
■ Depression (new-onset depression or worsening of preexisting depression; patients should be monitored during therapy for severe depression, and therapy should be discontinued if necessary)
■ Sarcoidosis (observed in combination IFN-α- ribavirin therapy)
■ Spastic diplegia (a form of cerebral palsy that is a neuromuscular condition characterized by hypertonia and spasticity in the muscles of the lower extremities; Little disease)
INITIATING THERAPY
INITIATING THERAPY
Hemoglobin, complete blood cell count with differential, electrolytes, liver function tests, thyroidstimulating hormone, chest radiography, and eye examination should be obtained before initiation of
and during therapy on a routine basis. Patients with prior cardiac disease or advanced cancer require a baseline electrocardiogram and routine reevaluation thereafter. Therapy should not be initiated in patients with a history of depression or severe psychiatric disorder because of the risk of worsening psychiatric symptoms and suicide. Patients with thyroid disorders that cannot be corrected with medication should not be treated. The development of spastic diplegia in patients with hemangiomas who are taking IFN seems to correlate with age and severe hypothyroidism (caused by the presence of ectopic thyroxine– degrading enzymes produced by the hemangiomas). Thus, thyroid monitoring is mandatory in all patients with large hemangiomas.78,79
MONITORING THERAPY
MONITORING THERAPY
Treatment should be discontinued if the absolute neutrophil count reaches less than 0.5 × 109/L or the platelet count reaches less than 25 × 109/L. Other symptoms warranting discontinuation include new-onset or worsening eye symptoms, the development of thyroid dysfunction not correctable by medication, and the development of severe depression or other psychiatric disorder during therapy.78
RISKS AND PRECAUTIONS78
RISKS AND PRECAUTIONS
78
■ Pregnancy category: C.
■ Pediatrics: The safety and efficacy in children have not established for any indications other than chronic hepatitides B and C.
PANITUMUMAB (VECTIBIX)
MECHANISM OF ACTION
MECHANISM OF ACTION
Panitumumab is an entirely human monoclonal antibody directed against EGFR. Like cetuximab, it blocks ligand interactions associated with the EGFR (EGF, transforming growth factor) and downstream signaling molecules like VEGF, bFGF, and IL-8; however, because panitumumab is not chimeric, the hypothesized benefit is better overall efficacy and immunologic tolerance.82
INDICATIONS
INDICATIONS
Panitumumab is currently indicated for progressing, metastatic colorectal carcinoma in combination with or as a single agent following chemotherapy.83 No known dermatologic uses or investigations into potential uses
28
exist at this time, but, given its similarity to cetuximab, possible investigations into panitumumab’s usefulness in cutaneous squamous cell carcinoma and melanoma are warranted. Other than a history of hypersensitivity, there are no known contraindications.2
COMPLICATIONS (SOME EXAMPLES)83
COMPLICATIONS (SOME
EXAMPLES)
83
■ Severe dermatologic toxicities (acneiform dermatitis, pruritus, erythema, rash, skin exfoliation, paronychia, dry skin, skin fissures)
■ Photosensitivity
■ Pulmonary fibrosis
■ Electrolyte disturbances
■ Infusion reactions
PEGAPTANIB (MACUGEN)
MECHANISM OF ACTION
MECHANISM OF ACTION
Pegaptanib is a short peptide strand, or aptamer, directed against a specific isomer of secreted VEGF, namely, VEGF165, which is thought to play a particular role in endothelial cell proliferation.84
INDICATIONS
INDICATIONS
Like ranibizumab, pegaptanib is currently indicated for the treatment of neovascular, or wet, age-related macular degeneration85-87; however, no known dermatologic uses or investigations into potential uses exist at this time.2 New reports have presented benefits in other oculovasculopathies, for instance, ischemic diabetic macular edema,88,89 choroidal neovascularization,90 retinal ischemic diseases,91 and myopic choroidal neovascularization.92
CONTRAINDICATIONS85
CONTRAINDICATIONS
85
■Ocular or periocular infection
COMPLICATIONS (SOME EXAMPLES)85
COMPLICATIONS (SOME
EXAMPLES)
85
■ Endophthalmitis, retinal detachment, and traumatic cataract formation associated with intravitreal administration
■ Hypertension
3597
■ Dizziness, headache, and vertigo
28
PROPRANOLOL (HEMANGEOL)
MECHANISM OF ACTION
MECHANISM OF ACTION
The effectiveness of propranolol in the treatment of hemangioma was discovered by chance in 200893 and is considered relatively safe for this usage.94 Given to infants who are at least 5-weeks old, propranolol, a beta-blocker, can be used in the treatment of infantile hemangioma (Fig. 195-2).95,96 Propanolol is not only successfully used for cutaneous hemangioma, but also for liver infantile hemangioma;97 some incomplete responses have been described, such as in focal subglottic hemangioma.98 In general, beta-blockers, whether systemic or topical, have better long-term results when compared to corticosteroids,99-101 but when beta-blockers and corticosteroids are used together, there is a faster positive outcome.102
Propranolol works in the treatment of hemangioma, by blocking both β1- and β2-adrenegric receptors in hemangioma endothelial cells; it also reduces levels without transactivating VEGF-2 signaling, and without promoting G0/G1-phase cell-cycle arrest—indeed, G0/G1-phase cell-cycle arrest has been associated with decreased cyclin D1, CDK-4, CDK-6, phospho- Rb expression, and with cessation of cell proliferation.35 Moreover, propranolol reduces the expression
A
of HIF-1α in a dose-dependent and a time-dependent manner, mainly by acting on β2-adrenegric receptors, in addition to blocking both STAT-3 and proapoptotic Bcl-2 pathways.103 In fact, newer studies point to better results when propranolol is prescribed to infants older than 6 months of age; propranolol also reduces plasma VEGF levels in a posttreatment long-term manner.104
INDICATIONS95
INDICATIONS
95
■ Tremors
■ Angina
■ Hypertension
■ Heart rhythm disorders
■ Treatment and prevention of myocardial infarction
■ Reduction of the severity and frequency of migraine
■ Infantile hemangioma
CONTRAINDICATIONS95
CONTRAINDICATIONS
95
■ Muscle disorder
■ Bronchitis, emphysema, or other breathing disorders
■ Low blood glucose or diabetes
■ Slow heartbeats, low blood pressure
B
3598
■ Congestive heart failure
■ Depression
■ Liver or kidney disease
■ Thyroid disorder
■ Pheochromocytoma
■ Problems with circulation (eg, Raynaud syndrome)
DOSING REGIMEN
DOSING REGIMEN
Chapter 118 provides dosing regimen information for propranolol.
COMPLICATIONS (SOME EXAMPLES)95
COMPLICATIONS (SOME
EXAMPLES)
95
■ Nausea, vomiting, diarrhea, constipation, or stomach cramps
■ Decreased sex drive, impotence, or difficulty having an orgasm
■ Sleep problems (insomnia)
■ Tired feeling
■ Hypoglycemia
■ Asthma attack
RANIBIZUMAB (LUCENTIS)
MECHANISM OF ACTION
MECHANISM OF ACTION
Ranibizumab is an antibody fragment related to bevacizumab that similarly competitively binds VEGF and inhibits its interactions with VEGFR-1 and VEGFR-2; it acts to block endothelial proliferation and survival. Smaller in size than bevacizumab (a full-length antibody), ranibizumab is thought to have better tissue absorption and fewer inflammatory reactions.105
INDICATIONS
INDICATIONS
Ranibizumab is currently indicated for the treatment of patients with neovascular, or wet, age-related macular degeneration, as well as diabetic retinopathy, macular edema, and choroidal neovascularization secondary to pathologic myopia;28,106-108 clinical trials looking into its use in combination with pulsed-dye laser in cutaneous neurofibroma and port-wine stain are ongoing.2
CONTRAINDICATIONS106
CONTRAINDICATIONS
106
■ Ocular or periocular infection
■ Hypersensitivity
28
COMPLICATIONS (SOME EXAMPLES)106
COMPLICATIONS (SOME
EXAMPLES)
106
■ Endophthalmitis and retinal detachment associated with intravitreal administration
■ Increase in intraocular pressures
■ Arterial thromboembolic events
SIROLIMUS (RAPAMUNE)
MECHANISM OF ACTION
MECHANISM OF ACTION
Isolated from the bacterium Streptomyces hygroscopicus, sirolimus is a macrocyclic lactone antibiotic with immunosuppressant, antifungal, and antineoplastic properties. After forming a complex with FK-binding protein-12, sirolimus acts by inhibiting the interaction of the mTOR with its substrates; mTOR is a serine– threonine protein kinase activated by several growth factors whose downstream targets affect cell-cycle control and angiogenesis in normal and neoplastic cells.109
Sirolimus decreases levels of hypoxia HIF-1α and significantly inhibits VEGF-mediated vascular endothelial cell stimulation, bFGF-induced angiogenesis, and T-cell activation and proliferation.110 By suppressing mTOR complex 2, sirolimus also inhibits Akt activation.111 Of the drugs used in the solid-organ transplantation setting, including cyclosporine and tacrolimus, rapamycin has the greatest antiangiogenic activity. To that effect, it may be useful for the prevention of squamous cell carcinoma and lymphoma in the immunosuppressed transplantation population.2
INDICATIONS
INDICATIONS
Rapamycin is currently approved for prophylaxis against renal transplant rejection as well as lymphangioleiomyomatosis.112 Off-label uses in dermatology include the treatment of psoriasis, Kaposi sarcoma, tuberous sclerosis, and angiofibromatosis.113-117 There are also case reports of its efficacy in nephrogenic systemic fibrosis, scleroderma, and dermatomyositis.118-120
Ongoing clinical trials are looking into the usefulness of sirolimus in the prevention of nonmelanoma skin cancer in patients following kidney transplantation, that of topical sirolimus in basal cell nevus syndrome (Gorlin-Goltz syndrome), and in combination with pulsed-dye laser in port-wine stain. Other than a history of hypersensitivity to it or other rapamycin derivatives, there are no known contraindications.2 A new generation of sirolimus-based compounds, phosphorus-containing sirolimus (FIM-A), inhibit the angiogenesis and proliferation of osteosarcomas, as they arrest cells in the G1-phase of the cell cycle, accompanied by reduction of VEGF and HIF-1α; as well as they also inhibit mTORC1 signaling as demonstrated by decreased phosphorylation of p70S6K1 and 4E-BP1.121
3599
28
COMPLICATIONS (SOME EXAMPLES)112,122
COMPLICATIONS (SOME
EXAMPLES)
112,122
■ Systemic toxicities: Complications that may occur include headache, thrombocytopenia, arthralgia, interstitial pneumonitis, and hypercholesterolemia.
■ Cutaneous toxicities: Cutaneous side effects of therapy include angioedema, leukocytoclastic vasculitis, xerosis, and aphthous ulceration, which all resolve with discontinuation of therapy.
■ Increased susceptibility to infections and malignancies.
SORAFENIB (NEXAVAR)
MECHANISM OF ACTION
MECHANISM OF ACTION
Sorafenib is a small-molecule, phosphorylation inhibitor of several tyrosine kinase receptors, including PDGF-β, VEGFR-1, VEGFR-2, VEGFR-3, and RAF kinase,123,124 thereby contributing to RAF/MEK/ERK pathway blockage.125,126 Like sunitinib, sorafenib inhibition of multiple points of downstream signaling by tyrosine kinase receptors results in tumor growth inhibition and regression.2 Furthermore, it has been reported, in preclinical models, that sorafenib blocks tumor growth, angiogenesis, and metastatic potential of osteosarcoma through a mechanism potentially involving the inhibition of the ERK1/ERK2, MCL-1, and ezrin pathways.127
INDICATIONS
INDICATIONS
Sorafenib is currently indicated for the treatment of advanced renal cell carcinoma, unresectable hepatocellular carcinoma, and differentiated thyroid cancer.128
Ongoing clinical trials are looking into the use of sorafenib in the treatment of metastatic melanoma, both alone and in combination with chemotherapy (carboplatin and paclitaxel). Other than a history of hypersensitivity, there are no known contraindications.128
It has been observed in patients who use sorafenib for cancer treatment that progression-free survival was significantly shorter in patients with high levels of Ang-2, granulocyte colony-stimulating factor, hematopoietic growth factor, and leptin.129 Interestingly, expression levels of many angiogenesis-related genes in the cutaneous metastasis of sarcomatoid-changed and rhabdoid features of an advanced renal cell carcinoma were relatively higher than those of the primary sorafenib-resistant tumor.130
A plethora of different sorafenib derivatives with good clinical and in vitro profiles have been presented in recent years. DCT015, a new sorafenib derivate, inhibits tumor growth and angiogenesis in gastric cancer models by inhibiting proliferation, inducing
3600
the morphologic changes of apoptosis, increasing the apoptosis percentage, as well as increasing the sub-G1 population in gastric cancer cells, once it inhibits both MEK/ERK and PI3K/Akt signaling pathways, VEGFinduced migration, and tube formation in human umbilical vein endothelial cells. In addition, DCT015 downregulates VEGF-induced VEGFR-2 phosphorylation with the decreased phosphorylation of the downstream key protein.131 Such suppression of VEGFR-2/ EGFR–mediated angiogenesis can be also observed with NSK-01105, another novel sorafenib derivative, in human prostate tumor growth.132 Another sorafenib derivative, SL1122-37, has greater effects than sorafenib on human hepatocellular carcinoma growth and prevention of angiogenesis.133
COMPLICATIONS (SOME EXAMPLES)128
COMPLICATIONS (SOME
EXAMPLES)
128
■ Dermatologic toxicities (rash, hand–foot syndrome, alopecia, pruritus)
■ Multiple blood dyscrasias
■ Hypertension, cardiac ischemia
■ GI upset, perforation
■ CYP2B6, CYP2C8, and CYP3A4 drug metabolism interactions
■ Nephrotic syndrome134
SUNITINIB (SUTENT)
MECHANISM OF ACTION
MECHANISM OF ACTION
Sunitinib is a small-molecule, phosphorylation inhibitor of several tyrosine kinase receptors, including PDGF-α, PDGF-β, VEGFR-1, VEGFR-2, and VEGFR-3; tumor growth inhibition and tumor regression result due to a variety of downstream mechanisms.55,135,136
INDICATIONS
INDICATIONS
Sunitinib is currently indicated for the treatment of GI stromal tumors, advanced renal cell carcinoma, and pancreatic neuroendocrine tumors.137 Indeed, patients with AA/AC alleles of the VEGFR-1 single-nucleotide polymorphism rs9582036 as well as expression of phosphorylated VEGFR-2 in tumor stroma may carry a good prognosis for sunitinibtreated metastatic renal cell carcinoma.138,139 Clinical trials are ongoing as to the efficacy of sunitinib in metastatic melanoma, but case reports exist of sunitinib efficacy in treating metastatic melanomas, as well as in treating skin ulcers associated with angioosteohypertrophy syndrome (or Klippel-Tré- naunay syndrome, hemangiectatic hypertrophy).140 Other than a history of hypersensitivity, there are no known contraindications.2
COMPLICATIONS (SOME EXAMPLES)137,141
COMPLICATIONS (SOME
EXAMPLES)
137,141
■ Dermatologic toxicities (rash, skin discoloration, hand–foot syndrome, alopecia)
■ Hypertension
■ Adrenal insufficiency
■ CYP3A4 drug metabolism interactions (monitor with concurrent use of CYP3A4 inducers and/or inhibitors)
TEMSIROLIMUS (TORISEL)
MECHANISM OF ACTION
MECHANISM OF ACTION
Like sirolimus, temsirolimus is an mTOR inhibitor that downregulates production of HIF-1α and blocks VEGF-mediated vascular endothelial cell stimulation, bFGF-induced angiogenesis, and T-cell activation and proliferation. The increased water solubility of temsirolimus allows for both oral and IV administration.55
INDICATIONS
INDICATIONS
Temsirolimus is currently indicated for the treatment of advanced renal cell carcinoma142 and is being evaluating in clinical trials for the treatment of metastatic melanoma in combination with either sorafenib or bevacizumab.2 Preliminary data show that metformin, another mTOR inhibitor, might enhance temsirolimus activity.136 Preclinical studies show that good synergistic effect can be obtained by combining temsirolimus and cetuximab in head and neck squamous cell carcinoma,143 in which baseline detection of caspase-3 activity may be useful for early identification of therapy success.144 Promising results may also be obtained when temsirolimus is combined with bevacizumab and cetuximab for solid tumor treatment.145 Other than a history of hypersensitivity to it or other rapamycin derivatives, there are no known contraindications.2
COMPLICATIONS (SOME EXAMPLES)142
COMPLICATIONS (SOME
EXAMPLES)
142
■ Rash
■ Mucositis, GI upset, and bowel perforation
■ Metabolic derangements (hyperglycemia, hyperlipidemia)
■ Interstitial lung disease
■ Renal toxicity
■ CYP3A4 drug metabolism interactions
■ Diarrhea and stomatitis146
■ Fatigue147
28
THALIDOMIDE (THALOMID)
Thalidomide was first released in Europe and several other regions in the late 1950s and quickly became a popular sedative used for the treatment of nausea in pregnancy. It was not approved in the United States at that time because of its questionable safety in pregnancy and emerging evidence of peripheral neuropathy as a side effect; the drug was, however, approved for use in clinical trials in the United States and was given to more than a thousand physicians in the United States for this purpose before its eventual banning. It was soon discovered that thalidomide caused severe embryopathy, resulting in phocomelia, amelia, or other severe birth defects when taken during pregnancy. The tragic experience with thalidomide prompted dramatic changes in drug regulation and approval.2
Recently, it was shown in zebrafish and chickens that thalidomide teratogenicity occurs due to thalidomide binding to the cereblon (CRBN) gene, which inhibits ubiquitin ligase activity.148
In 1965, Sheskin prescribed thalidomide for psychosis in one of his patients and accidentally discovered that thalidomide effectively treated her erythema nodosum leprosum. The FDA approved thalidomide in 1998 for the treatment of erythema nodosum leprosum and currently classifies it as an orphan drug.2
As interest in thalidomide’s ability to treat a wide variety of refractory diseases grows, a promising class of drugs named IMiDs (thalidomide and its derivatives lenalidomide and pomalidomide) or immunomodulatory thalidomide analogs, are under development and investigation. One member of this new class of drugs, lenalidomide (CC-5013, Revlimid), has been approved for the treatment of multiple myeloma, myelodysplastic syndromes, and chronic lymphocytic leukemia. However, Phase III clinical studies of lenalidomide for the treatment of metastatic melanoma did not show a significant effect.149
MECHANISM OF ACTION
MECHANISM OF ACTION
Thalidomide exhibits a wide range of effects in vitro and in vivo. Its mechanisms of action are still unclear, but, exhibiting antineoplastic, immunomodulatory, and antiangiogenic properties, thalidomide downregulates the expression of VEGF, bFGF, and possibly tumor necrosis factor-α, IFN-α insulin-like growth factor-1, NF-κB, IL-6, IL-12, IL-8, and matrix metalloproteinase-2.150-152 Recently, it was described that Slit2/Robo1 endothelial signaling plays a role in angiogenesis, which can be blocked by thalidomide, once it blocks the PI3K/Akt pathway.153 Thalidomide’s antiangiogenic properties may be the basis for its antineoplastic activity, but its myriad other effects likely account for its teratogenicity.154 Apart from its hypnosedative properties, thalidomide’s eventual effects on the immune
3601
28
system result in a reduction in the helper T-cell–to– suppressor T-cell ratio, and a decrease in leukocyte chemotaxis and in monocyte phagocytosis.155 Additionally, human keratinocytes demonstrate increased migration and proliferation when exposed to thalidomide.156
INDICATIONS
INDICATIONS
Thalidomide is currently approved and considered first-line therapy for the acute treatment of the cutaneous manifestations of moderate to severe erythema nodosum leprosum as well as maintenance therapy for prevention and suppression of the cutaneous manifestations of erythema nodosum leprosum recurrence. In combination with dexamethasone, thalidomide is also approved for the treatment of newly-diagnosed multiple myeloma.157 Off-label uses include Kaposi sarcoma, hemangioendotheliomas, severe aphthous stomatitis (especially in patients with AIDS), psoriasis, and a variety of other dermatologic conditions.151
CONTRAINDICATIONS157
CONTRAINDICATIONS
157
■ Pregnancy class: X
■ Hypersensitivity to the drug or its components
PHARMACOKINETICS
PHARMACOKINETICS
Thalidomide has low water solubility and slow absorption from the GI tract, reaching peak plasma levels 0.5 to 4 hours after administration; it is only available in an oral form. A delay in absorption of up to 2 hours may occur if given in conjunction with foods high in fat.157
Thalidomide’s half-life is approximately 5 to 7 hours, with renal clearance estimated to be 1.15 mL/ min. Thalidomide’s main route of elimination remains unknown, but it undergoes nonenzymatic hydrolysis in the serum to a variety of metabolites. Because hepatic metabolism appears to play an insignificant role, thalidomide is unlikely to affect levels of CYPmetabolized drugs such as oral contraceptives. Acetylcholine, prostaglandins, histamine, and serotonin are antagonized by thalidomide in vitro; alcohol, barbiturates, chlorpromazine, and reserpine have enhanced hypnosedative activity in the presence of thalidomide.157
DOSING REGIMEN
DOSING REGIMEN
Because thalidomide may induce drowsiness, guidelines for dosing include initiation at 100 to 300 mg/day
3602
DISEASE DOSE
Erythema nodosum leprosum Initial dose: 100-300 mg/day, preferably 1 hour after the evening meal with a full glass of water Maintenance dose: 50-100 mg/day Tapering recommendations: 50-mg decrements every 2-4 weeks once symptoms subside (usually after 2 weeks); in patients requiring prolonged treatment, attempt tapering schedule every 3-6 months
Severe cutaneous erythema nodosum leprosum reaction
Initial dose: 400 mg/day
Chronic graft-versushost disease Initial dose: 100 mg 4 times daily Maintenance dose: 200 to 400 mg 4 times daily Pediatric dose: 3-9.5 mg/kg twice daily to 4 times daily
Cutaneous lupus erythematosus Initial dose: 400 mg/day Maintenance dose: 25-50 mg/day
Recurrent aphthous stomatitis 100 mg/day
Behçet syndrome Initial dose: 400 mg/day Maintenance dose: 200 mg/day
Behçet syndrome Initial dose: 400 mg/day Maintenance dose: 200 mg/day
with a full glass of water at bedtime or at least 1 hour after the evening meal. Therapy should be continued until improvement is noted, at which point the physician can begin tapering the dose by 50 mg every 2 to 4 weeks. In the case of maintenance therapy, an attempt at tapering should occur every 3 to 6 months (Table 195-2).157
INITIATING THERAPY
INITIATING THERAPY
Thalidomide therapy should be reserved for patients with debilitating, serious diseases that have proven refractory to other therapies. The manufacturer of thalidomide has developed a restricted distribution program called System for Thalidomide Education and Prescribing Safety (S.T.E.P.S.), which requires both prescribers and dispensing pharmacists to be registered. It is mandatory for patients to be informed about the program, adhere to its requirements, and demonstrate in writing an understanding of these warnings. Female patients of childbearing potential (defined by the program as sexually mature women who have not undergone a hysterectomy or who have not been postmenopausal for at least 24 consecutive months) must have a negative pregnancy test (with a β-human chorionic gonadotropin sensitivity of at least 50 mU/mL) within 24 hours of treatment initiation. Patients must use reliable contraception (2 effective methods unless using the abstinence method) for a period of at least 1 month before initiating therapy and must continue
this practice during and for 1 month after therapy is completed. Male patients are required to use latex condoms, including those patients who have had a vasectomy.157
MONITORING THERAPY
MONITORING THERAPY
S.T.E.P.S. requires patient monitoring during therapy. Strict guidelines for pregnancy testing are outlined for males and females of childbearing potential to prevent possible fetal damage. If, during the course of therapy, a patient becomes pregnant, the drug should be stopped immediately and the exposure reported to the FDA and the manufacturer (Celgene; Summit, New Jersey, USA). Patients should then see an obstetrician/gynecologist with experience in reproductive toxicity.157
RISKS AND PRECAUTIONS157
RISKS AND PRECAUTIONS
157
■ Hypersensitivity
■ Bradycardia
■ Stevens-Johnson syndrome and toxic epidermal necrolysis
■ Seizures
■ Pregnancy category: X
COMPLICATIONS (SOME EXAMPLES)
COMPLICATIONS (SOME
EXAMPLES)
■ Teratogenicity: Thalidomide’s embryopathy is well documented. Thalidomide is pregnancy category X, and patients selected for therapy must follow strict contraceptive measures as directed by the program. Thalidomide-induced defects in limb formation may be a consequence of bFGF inhibition, as bFGF induces embryologic limb formation.158
■ Peripheral neuropathy: Thalidomide is neurotoxic and may result in a sensory, symmetrical distal polyneuropathy, which may later evolve to include motor symptoms as well. Neurotoxicity can be permanent. Incidence of peripheral neuropathy in patients receiving thalidomide ranges from 0.5% to 25%. Patients with preexisting peripheral neuropathy should not begin treatment. Baseline nerve conduction studies should be obtained before treatment initiation along with monthly monitoring during the first 3 months decreasing to 6-month intervals thereafter during treatment. A 40% decrease in nerve conduction necessitates treatment discontinuation.157
■ Neutropenia: Because of the risk of neutropenia, baseline measurements should be obtained
28
(including a white blood cell count with differential) and monitored regularly during the treatment course. Treatment should not be initiated in patients with an absolute neutrophil count of less than 750/mm.157
■ Other side effects: Other side effects include drowsiness, orthostatic hypotension, rash, fever, and increases in HIV viral loads.157,159
TRASTUZUMAB (HERCEPTIN)
MECHANISM OF ACTION
MECHANISM OF ACTION
Trastuzumab is a human, monoclonal antibody directed against the human estrogen receptor 2 (HER-2). Blockade of HER-2 results in downregulation of angiopoeitin-1, plasminogen-activator inhibitor-1, VEGF, and transforming growth factor-α but upregulation of TSP-1, an inhibitor of angiogenesis.160
INDICATIONS
INDICATIONS
Trastuzumab is currently indicated for the treatment of HER-2 overexpression, lymph node–positive breast cancer, or breast cancer that is node-negative and is estrogen receptor/progesterone receptor–negative or has 1 high-risk feature,2 sometimes associated with another chemotherapy, such as paclitaxel, doxorubicin, cyclophosphamide, or docetaxel, as well as for treatment of metastatic gastric or gastroesophageal junction adenocarcinoma (in combination with cisplatin and either capecitabine or 5-fluorouracil).161
No known dermatologic uses or investigations into potential uses exist at this time. Other than a history of hypersensitivity, there are no known contraindications.2
COMPLICATIONS (SOME EXAMPLES)161
COMPLICATIONS (SOME
EXAMPLES)
161
■ Cardiomyopathy (requires a baseline measurement of left ventricular ejection fraction and monitoring every 3 months during treatment)
■ Pulmonary toxicities (interstitial pneumonitis, acute respiratory distress syndrome)
■ Worsening of chemotherapy-induced neutropenia
■ Infusion reactions
3603
28
DRUG ANTIANGIOGENIC EFFECTS
ABT-510 Synthetic TSP-1 analog; inhibits actions of VEGF-A, VEGF-C, and bFGF162-166
Calcium dobesilate Binds and antagonizes bFGF167,168
Curcumin (diferuloylmethane) Decreases proangiogenic factors, decreases endothelial cell proliferation, decreases neovascularization169-173
Fulvene-5 Fulvene-5 inhibits Nox4 and NADP-oxidase, as well as downregulates expression of ANG-2174
Gentian violet Triphenylmethane dye; downregulates expression of ANG-2175
Honokiol Inhibits VEGFR-2 autophosphorylation, blocks activation of Rac (necessary for endothelial cell migration and proliferation) in response to vascular endothelial growth factor, interferes with the expression of Bcl-2, caspase-3, and TNF-α176-178
Interleukin-12 Decreases bFGF-mediated angiogenesis, stimulates natural killer cells to exhibit cytotoxicity against endothelial cells, acts through interferon-γ to induce interferoninducible protein 10, an antiangiogenic chemokine, and downregulates matrix metalloproteinase synthesis179
Interleukin-12 Decreases bFGF-mediated angiogenesis,
stimulates natural killer cells to exhibit cytotoxicity against endothelial cells, acts through interferon-γ to induce interferoninducible protein 10, an antiangiogenic chemokine, and downregulates matrix metalloproteinase synthesis179
ANG, angiopoietin; bFGF, basic fibroblast growth factor; NADP, nicotinamide adenine dinucleotide phosphate; TNF, tumor necrosis factor; TSP, thrombospondin; VEGFR, vascular endothelial growth factor receptor.
ACKNOWLEDGMENTS
We thank Ricard L. Berrios, MD, and Jonathan Hofmekler, BSc, who contributed to the equivalent chapter in the 7th edition.
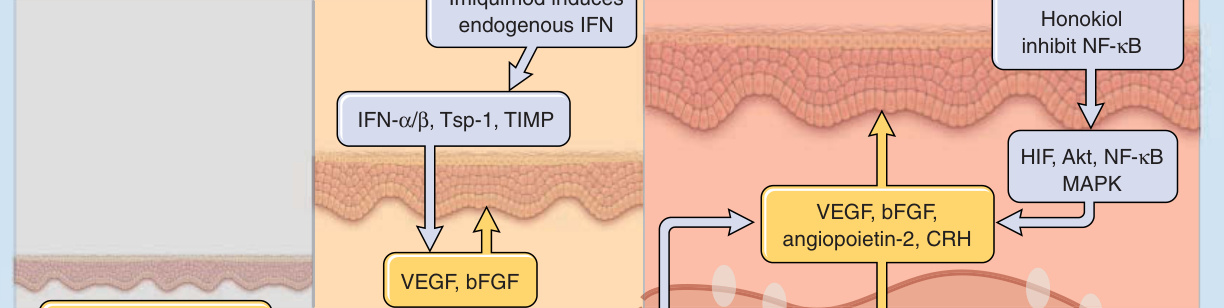
Figure 195-1 better illustrates the mechanisms of action of some of the drugs described in this chapter, helping to elucidate how they work as antiangiogenic agents.

Figure 195-2 Posterior fossa brain malformations, hemangiomas of the face, arterial anomalies, cardiac anomalies, and eye abnormalities (PHACE) syndrome patient whose cranial hemangioma was treated with systemic propranolol. A, Patient before treatment, at age 45 days; (B) same patient at age 5 years. (Images used with permission from Dr. Caroline Romanelli Tiburcio Alves Zelenika, Pontifical Catholic University of Campinas, Campinas/SP, Brazil.)
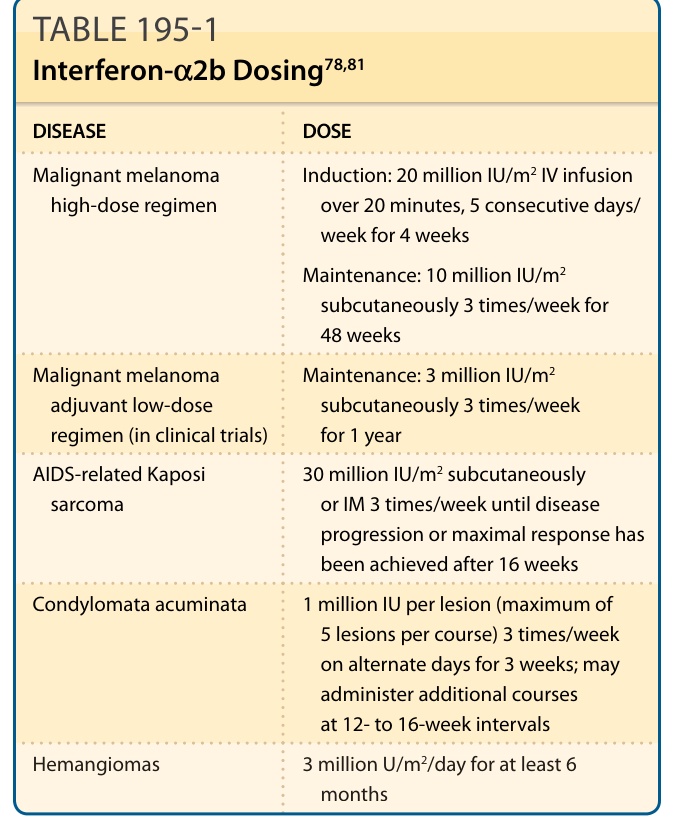
TABLE 195-1 Interferon-`2b Dosing78,81
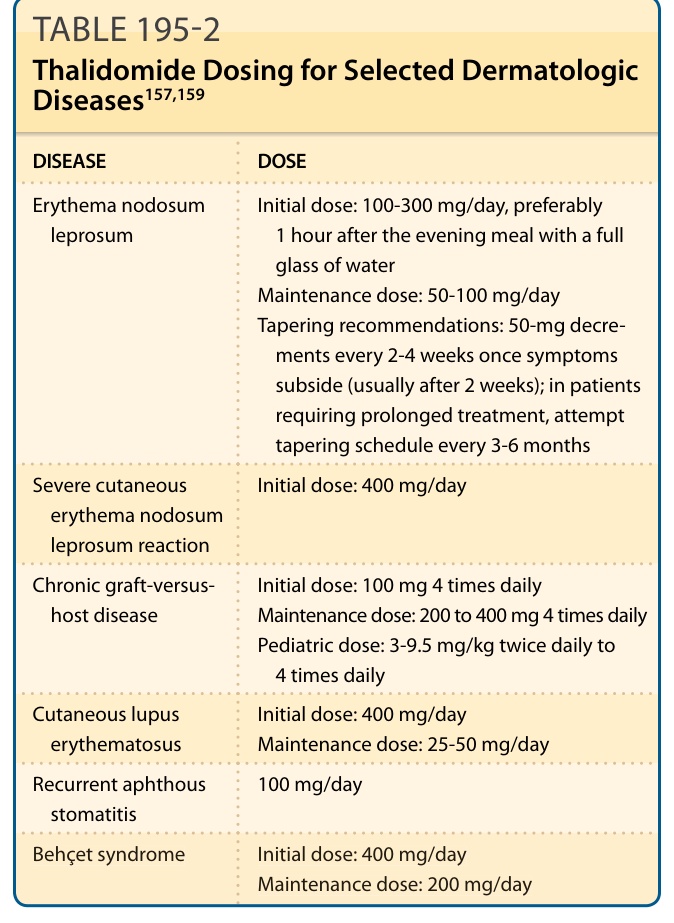
TABLE 195-2 Thalidomide Dosing for Selected Dermatologic Diseases157,159
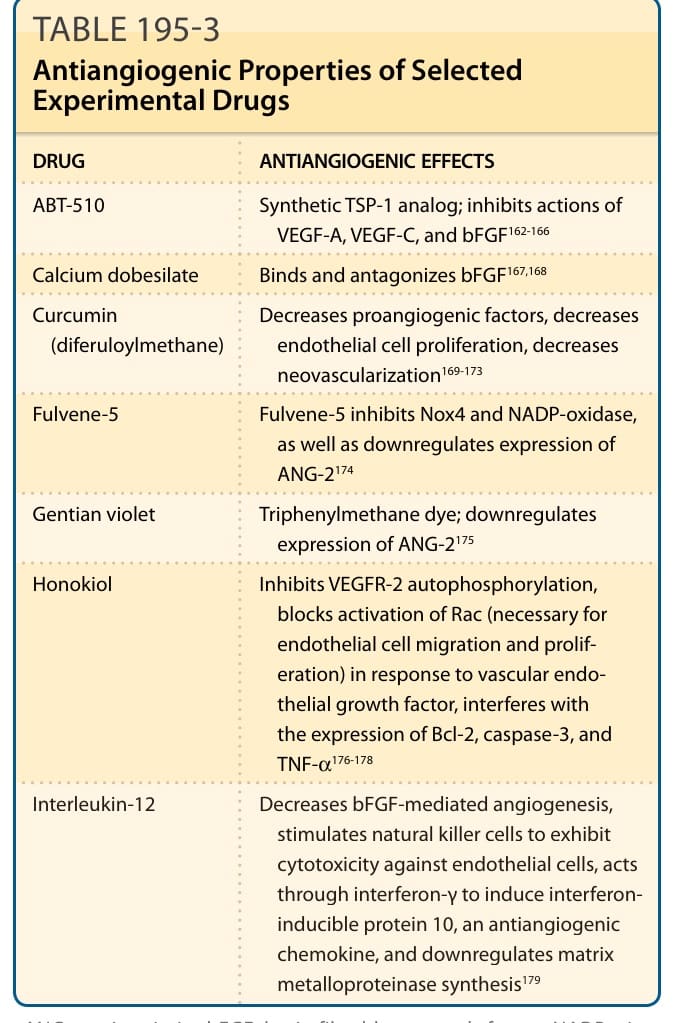
Table 195-3 summarizes the most important aspects of some experimental drugs that are still in experimental use and that may be helpful as antiangiogenic agents in the future.