Antihistamines
28
AT-A-GLANCE
■ H1 antihistamines are first-line therapy for chronic idiopathic and physical urticarials.
■ H1 agents may be useful in treating conditions with histamine-associated pruritus.
■ Limited evidence supports the use of H1 in the treatment of atopic dermatitis.
■ Certain special patient populations, including children, the elderly, and patients with renal or hepatic impairment, may require dosage adjustments when using antihistamines.
■ H2 antihistamines may be a useful adjunct to H1 antihistamine therapy in refractory cases of chronic idiopathic urticaria/angioedema.
Histamine is a low-molecular-weight amine that is synthesized from l-histidine by histidine decarboxylase, an enzyme expressed by numerous cells throughout the body. Histamine exerts its effects through 4 different receptors that play a role in embryonic development, cellular growth and proliferation, hematopoiesis and immunity, inflammation, and wound healing. This amine is an important neurotransmitter in the CNS and is produced in neurons located in the tuberomammillary nucleus of the posterior hypothalamus. Nerves arising from this area regulate the sleep–wake cycle, endocrine homeostasis, cognition and memory. Histamine also exerts anticonvulsant effects. Histamine is metabolized by 2 major pathways: diamine oxidase and histamine methyl transferase.1,2
Histamine receptors are heptahelical transmembrane molecules that transmit extracellular signals to intracellular second messengers via G proteins. These receptors have constitutive activity, and thus are able to trigger downstream events in the absence of ligand stimulation. Active and inactive states of histamine receptors exist in equilibrium and can be shifted to a greater proportion of active or inactive states by histamine and antihistamines, respectively.3,4 Both H1 and H2 histamine receptors are widely expressed on neurons, smooth muscle, epithelium, endothelium, and multiple immune cells. H2 receptors also exist on gastric mucosal parietal cells; consequently, occupation by specific H2 antihistamines inhibits gastric acid secretion. H3 and H4 receptors have more limited expression in the body with H3 receptors occurring primarily on histaminergic neurons and immune cells, whereas H4 receptors are highly expressed in the bone marrow and on peripheral hematopoietic cells.2,5
H1 ANTIHISTAMINES
The first H1 antihistamines were introduced in the 1940s after groundbreaking work by Bovet in the 1930s. The H1 antihistamines—diphenhydramine, chlorpheniramine, and promethazine—all became available for clinical use during this time, and these and other agents were the primary source of antihistamine therapy until the 1980s when less-sedating, second-generation antihistamines were developed. First-generation antihistamines are divided into 6 groups on the basis of chemical structure: (a) ethylenediamines, (b) ethanolamines, (c) alkylamines, (d) phenothiazines, (e) piperazines, and (f) piperidines. The presence of multiple aromatic or heterocyclic rings and alkyl substituents enhances the lipophilicity of these compounds, permitting penetration of the blood–brain barrier, thereby leading to sedation. Second-generation antihistamines are less capable of accumulating in the CNS, and thus are less sedating. Compared to first-generation antihistamines, these second-generation agents also have the added advantage of longer half-lives, thus requiring for less-frequent dosing. Today, more than 45 H1 antihistamines exist worldwide as prescription and nonprescription medications, and are used for the treatment of allergic reactions, urticaria, pruritus, nausea, vertigo, sleep, and anxiety.4,6
MECHANISM OF ACTION
MECHANISM OF ACTION
H1 antihistamines are inverse agonists that reversibly bind and stabilize the inactive form of the H1 receptor, thereby favoring the inactive state (Table 189-1). By means of the H1 receptor, H1 antihistamines decrease the production of proinflammatory cytokines, the expression of celladhesion molecules, and chemotaxis of eosinophils and other immune cells (Fig. 189-1).1,4 H1 antihistamines may also decrease mediator release from mast cells and basophils through inhibition of calcium ion channels. In addition to binding to histamine receptors, first-generation H1 antihistamines also act on muscarinic, α-adrenergic, and serotonin receptors, as well as cardiac ion channels. Some of the more significant side effects associated with first-generation H1 antihistamines, such as urinary retention, hypotension, and cardiac arrhythmias, are mediated through these nonhistamine receptors. Many of the low-sedating, second-generation H1 antihistamines are chemically derived from firstgeneration agents.1,2 For example, cetirizine is a metabolite of hydroxyzine and loratadine is related to azatadine. The second-generation H1 antihistamines bind noncompetitively to the H1 receptor, and thus are not easily displaced by histamine. They
28
■Both H1 and H2 antihistamines are inverse agonists that reversibly bind and stabilize the inactive form of the histamine receptor, thereby favoring the inactive state.
■Both H1 and H2 antihistamines are inverse agonists that reversibly
bind and stabilize the inactive form of the histamine receptor, thereby favoring the inactive state.
■First-generation H1 agents are relatively lipophilic, which enhances penetration of the blood–brain barrier and leads to sedation.
■First-generation H1 agents are relatively lipophilic, which enhances
penetration of the blood–brain barrier and leads to sedation.
■First-generation H1 antihistamines may interact with other drugs metabolized by the hepatic cytochrome P450 system leading to drug–drug interactions.
■First-generation H1 antihistamines may interact with other drugs
metabolized by the hepatic cytochrome P450 system leading to drug–drug interactions.
■Second-generation H1 antihistamines have poor penetration of the blood–brain barrier and thus are less sedating.
■Second-generation H1 antihistamines have poor penetration of the
blood–brain barrier and thus are less sedating.
■Second-generation H1 antihistamines bind selectively to peripheral H1 receptors and have fewer CNS effects.
■Second-generation H1 antihistamines bind selectively to peripheral
H1 receptors and have fewer CNS effects.
■Second-generation H1 antihistamines require less hepatic metabolism and thus are less likely to interact with other medications.
■Second-generation H1 antihistamines require less hepatic metabo-
lism and thus are less likely to interact with other medications.
■There is no evidence of tolerance or tachyphylaxis to first-generation or second-generation antihistamines.
■There is no evidence of tolerance or tachyphylaxis to first-genera-
tion or second-generation antihistamines.
dissociate slowly, and have a longer duration of action than first-generation H1 antihistamines. As a result of the selectivity of second-generation antihistamines for the H1 receptor and their reduced lipophilicity, these agents are far less likely to cause sedation and have fewer side effects than the first-generation antihistamines.1,3,6
Some low-sedating H1 antihistamines affect cell trafficking in the skin and other tissues, presumably by modulating the release of inflammatory mediators
and the expression of adhesion molecules. In a skin chamber model, cetirizine administration reduced eosinophil influx after allergen challenge; however, similar effects have not been seen in the nasal mucosa following allergen exposure. In vitro studies demonstrate that cetirizine inhibits eosinophil, monocyte, and T-lymphocyte chemotaxis to N-formyl-methionylleucyl-phenylalanine and platelet-activating factor.7 H1 antihistamines may also modulate the expression of cellular adhesion molecules such as antigeninduced intercellular adhesion molecule 1 that exists on keratinocytes, Langerhans cells, and endothelial cells These antihistamines also may influence the release of inflammatory mediators from leukocytes.8
In vitro, desloratadine and emedastine inhibit platelet-activating factor–induced eosinophil chemotaxis, tumor necrosis factor-α–induced eosinophil adhesion, and spontaneous and phorbol myristate–induced superoxide generation.9,10
PHARMACOKINETICS
PHARMACOKINETICS
FIRST-GENERATION H1 ANTIHISTAMINES
After oral administration, the sedating effects of firstgeneration H1 antihistamines can be observed within
Mode of action of H1 antihistamines
H1 antihistamines
?
Inhibition of preformed mediator release
Superoxide radical release
Histamine Prostaglandin D2 Platelet-activating factor Thromboxanes Tryptase Kinins Cytokines
Arachadonic acid metabolites
Via H1 receptor
Release proinflammatory products Expression of cell-adhesion molecules
Cytokine release
Granule products
ICAM-1 VCAM-1
TNF-α GMCSF IL-1β IL-6 IL-8
Eosinophililic cationic protein
Chemotaxis of eosinophils and inflammatory infiltrate
Neutrophil elastase
↓ Inflammation
3452
30 minutes to 1 hour and generally persist for 4 to 6 hours. However, sedation may last for 24 hours or longer for some agents in some individuals. For example, after the oral administration of a single dose, the serum half-lives of brompheniramine, chlorpheniramine, and hydroxyzine exceed 20 hours in adults. First-generation H1 antihistamines are metabolized by hepatic cytochrome P450 (CYP) enzyme 3A4, forming glucuronides before excretion in urine.1,4
The potency and relative concentration of H1 antihistamines in the skin can be compared by their inhibition of the cutaneous wheal-and-flare response induced by intradermal histamine. First-generation H1 antihistamines are typically administered in divided doses at intervals of 4 to 8 hours (see section “Dosing Regimens”), although once-daily dosing may suffice for agents with longer serum half-lives. In placebocontrolled, double-blind studies, there is no evidence of tolerance or tachyphylaxis to these antihistamines over a 3-month period. Interestingly, despite the relatively short half-lives of first-generation antihistamines, suppression of allergen-induced whealand-flare reactions may persist for up to 7 days after discontinuation.1,4
Topical H1 antihistamine formulations for dermatologic use are available, although these preparations tend to be less effective and are associated with the potential for delayed allergic contact reactions.
SECOND-GENERATION H1 ANTIHISTAMINES
Most second-generation, H1 antihistamines are low sedating. They are administered once or twice daily and generally achieve peak plasma concentrations within 1 to 2 hours, These drugs achieve higher concentrations in the skin than first-generation antihistamines, and a single dose can suppress the wheal-and-flare reaction from 1 to 24 hours. Regular use prolongs this effect; for example, 6 days of daily cetirizine use results in 7 days of wheal-and-flare suppression.11-15
The second-generation antihistamines—loratadine, acrivastine, mizolastine, ebastine, and oxatomide—are metabolized in the liver via the hepatic enzyme CYP 3A4. Cetirizine, fexofenadine, levocabastine, desloratadine, and levocetirizine undergo minimal hepatic metabolism, which reduces the likelihood of interactions with other drugs. In general, most of these antihistamines are excreted in the urine and thus dosages need to be adjusted for patients with renal insufficiency.1,4
In healthy adults, cetirizine and levocetirizine reach peak concentrations approximately 1 hour after administration, with elimination half-lives of 6.5 to 10 hours. Fexofenadine generally reaches a peak concentration at 2 to 3 hours, with an elimination half-life of 14 hours.5 While dosage adjustments are recommended for patients with decreased creatinine clearance, this is usually unnecessary for patients with hepatic disease because fexofenadine undergoes minimal hepatic metabolism.1,4 Loratadine’s half-life ranges on average from 8 to 24 hours, depending on hepatic
28
function. Ebastine, which is metabolized to form its carboxylic acid metabolite, and carebastine, has a half-life of 15 hours.1,4 In a single-dose study, normal subjects were treated with cetirizine (10 mg), fexofenadine (60 mg), or loratadine (10 mg) prior to repeated intradermal histamine injections over 24 hours. In the study, cetirizine proved to be more potent than fexofenadine, which was more effective than loratadine in suppressing these histamine reactions.16 Similar studies also have demonstrated that levocetirizine (5 mg) and fexofenadine (180 mg) are more potent than desloratadine (5 mg) in suppressing histamine’s effects in the skin.17 Pharmacogenetics may also influence drug metabolism and clearance of antihistamines. In a series of pharmacokinetic studies, approximately 7% of all subjects and 20% of African Americans were slow metabolizers of desloratadine. Comparable differences may exist for other H1 antihistamines.4,18
INDICATIONS
INDICATIONS
Studies comparing the efficacy of second-generation antihistamines, on the other hand, are numerous. Double-blind, placebo-controlled, or parallel studies, have demonstrated that low-sedating H1 antihistamines (cetirizine, loratadine, fexofenadine, desloratadine, levocetirizine, acrivastine, mizolastine, azelastine, ebastine, and oxatomide) are superior to placebo in the treatment of urticaria and angioedema.20-26 Trials comparing different second-generation antihistamines with one another have not shown any one agent to be consistently superior, although cetirizine and levocetirizine have fared best overall in comparative trials.1,26-29
Even though both first-generation and secondgeneration H1 antihistamines are used to treat pruritus in patients with atopic dermatitis, their efficacy
■Acute urticaria
■Acute urticaria
■Chronic idiopathic urticarial
■Chronic idiopathic urticarial
■Physical urticarias and dermatographism
■Physical urticarias and dermatographism
■Pruritus associated with histamine release
■Pruritus associated with histamine release
3453
■Symptoms of mastocytosis
■Symptoms of mastocytosis
28
has not been proved by rigorous clinical trials. In the 18-month Early Treatment of the Atopic Child study, cetirizine afforded a steroid-sparing benefit to children with severe atopic dermatitis, but no consistent benefit was observed in children with moderate disease.30,31 A meta-analysis of 16 studies conducted from 1966 through 1999 failed to demonstrate a major role for either first-generation or second-generation H1 antihistamines in the treatment of atopic dermatitis.31
Mastocytosis represents an uncontrolled proliferation of tissue mast cells, and histamine is believed responsible for many of the symptoms associated with this disorder; H1 antihistamines are commonly used to treat symptomatic mastocytosis patients.32-34 In general, higher doses of H1 antihistamines than normally employed for allergic disorders may be necessary for symptom control in mastocytosis patients. For example, fexofenadine 360 mg in the morning and cetirizine 40 mg at night may be necessary for some symptomatic mastocytosis patients.
DOSING REGIMENS
DOSING REGIMENS
The H1 antihistamines are considered first-line therapy in the treatment of CIU and physical urticarials, and may be useful in treating other conditions in which histamine-driven pruritus is a major feature. The lowest effective dosage is preferred to minimize dose-related side effects, such as sedation. Table 189-3 outlines the dosing regimens for H1 antihistamines. After several days of therapy, the dosage may be increased if symptom control is inadequate. Occasionally, gradual escalation of dosing permits the development of tolerance to sedation, which allows higher dosages to be used to treat certain conditions, such as refractory CIU. Doses up to 4 times
that normally recommended for second-generation H1 antihistamines may be necessary in the treatment of some CIU patients.19,35 In a retrospective study of 368 CIU patients treated with either first-generation or secondgeneration H1 antihistamines, 276 (75%) increased their dose by 2 to 4 times the normal recommended dose. Half of these patients experienced a clinical benefit from the medication increase. Those patients treated with secondgeneration H1 antihistamines also experienced less sedation and other side effects compared to patients treated with first-generation H1 agents.35
Ingestion of the medication with food may alleviate the GI discomfort that sometimes can accompany antihistamine use. Patients, however, should be advised to avoid taking fexofenadine with antacids because this can interfere with drug absorption. Individuals with comorbid conditions, such as hepatic or renal disease, may require lower dosages as a result of impaired metabolism or excretion of these drugs. Certain special patient populations, including children, the elderly, and pregnant or breastfeeding women, may also need antihistamine dosage adjustments (Table 189-4). Therapeutic end points are usually dictated by improvement in histamine-related signs and symptoms (eg, severity of pruritus; wheal number, size, and frequency). As for drug toxicity, no particular monitoring beyond the usual surveillance for adverse effects is required in most cases. Because of reports of hepatotoxicity, some sources recommend periodic liver transaminase evaluation when cyproheptadine is prescribed.1,4,6
RISKS AND PRECAUTIONS
RISKS AND PRECAUTIONS
Sedation is the most commonly reported problem, primarily with first-generation H1 antihistamines
DRUG FORMULATION DOSAGE CONDITIONS REQUIRING DOSAGE ADJUSTMENT
First-generation H1 Antihistamines
Chlorpheniramine
2-, 4-, 8-, 12-mg tablet Adult: 4 mg thrice daily, 4 times daily; 8-12 mg twice daily Hepatic impairment
2 mg/5 mL syrup Age 6-11 years: 2 mg q4-6h
Cyproheptadine
4-mg tablet Adult: 4 mg thrice daily, 4 times daily Hepatic impairment
2 mg/5 mL syrup Age 7-14 years: 4 mg twice daily, thrice daily
Diphenhydramine
25-, 50-mg tablet Adult: 25-50 mg q4-6h Hepatic impairment
12.5 mg/5 mL syrup Age 6-12 years: 12.5-25 mg q4-6h
50 mg/15 mL syrup Age <6 years: 6.25-12.5 mg q4-6h
6.25 mg/5 mL syrup
12.5 mg/5 mL syrup
Hydroxyzine
10-, 25-, 50-, 100-mg tablet Age ≥6 years: 25-50 mg q6-8h or at bedtime Hepatic impairment
10 mg/5 mL syrup Age <6 years: 25-50 mg daily
Tripelennamine 25-, 50-, 100-mg tablets Adult: 25-50 mg q4-6h Hepatic impairment
3454
(Continued)
28
(Continued)
DRUG FORMULATION DOSAGE CONDITIONS REQUIRING DOSAGE ADJUSTMENT
Second-generation H1 Antihistamines
Acrivastinea 8-mg tablet Adult: 8 mg thrice daily Renal impairment
Azelastine
2-mg tabletb Adult: 2-4 mg twice daily Renal and hepatic impairment
0.1% nasal spray Age 6-12 years: 1-2 mg twice daily
2 sprays/nostril twice daily
Cetirizine
5-, 10-mg tablet Age ≥6 years: 5-10 mg daily Renal and hepatic impairment
5 mg/mL syrup Age 2-6 years: 5 mg daily
Age 6 months to 2 years: 2.5 mg daily
Desloratadine
2.5-, 5-mg tablet Age ≥12 years: 5 mg daily Renal and hepatic impairment
5 mg/mL syrup Age 6-12 years: 2.5 mg daily
Age 1-6 years: 1.25 mg daily
Age 6-12 months: 1 mg daily
10-mg tablet Age ≥6 years: 10-20 mg daily Renal impairment
Ebastineb
Age 6-12 years: 5 mg daily
Age 2-5 years: 2.5 mg daily
Fexofenadine
30-, 60-, 120-, 180-mg tablet Age ≥12 years: 60 mg daily, twice daily; 120-180 mg daily Renal impairment
Age 6-12 years: 30 mg daily, twice daily
Levocetirizine 5-mg tablet Age ≥6 years: 5 mg daily Renal and hepatic impairment
Loratadine
10-mg tablet Age ≥6 years: 10 mg daily Renal and hepatic impairment
5 mg/mL suspension Age 2-9 years: 5 mg daily
Mizolastineb 10-mg tablet Adult: 10 mg daily Hepatic impairment
Mizolastineb 10-mg tablet Adult: 10 mg daily Hepatic impairment
aAvailable in the United States only as a fixed-dose combination with pseudoephedrine hydrochloride, 120 mg.
bNot currently available in the United States.
(Table 189-5).1,4 The sedative effect is much more pronounced with first-generation H1 antihistamines, especially in the ethanolamine and phenothiazine groups, and is less marked with the alkylamine group antihistamines. The use of first-generation H1 antihistamines is associated with an increase in occupational injuries and automobile accidents.36 Sedating H1 antihistamines are sometimes used for their somnolent effects at night; however, these agents actually delay the onset of rapid eye movement sleep, leading to poor sleep quality and impaired memory, attention capabilities, and sensory-motor performance the following day.37
Other CNS effects of sedating antihistamines include
■Risks
■Risks
■History of cardiac arrhythmias, particularly ventricular arrhythmias
■History of cardiac arrhythmias, particularly ventricular
arrhythmias
■First trimester of pregnancy
■First trimester of pregnancy
■Prostatic hypertrophy
■Prostatic hypertrophy
■Contraindications
■Contraindications
■Narrow-angle glaucoma
■Narrow-angle glaucoma
■Concomitant use of monoamine oxidase inhibitors
■Concomitant use of monoamine oxidase inhibitors
dizziness, tinnitus, disturbed coordination, inability to concentrate, blurred vision, and diplopia. Stimulatory CNS effects, which occur especially with the alkylamine group, include nervousness, irritability,
■Sedationa
■Sedationa
■Other CNS disturbancesa
■Other CNS disturbancesa
■Dizziness
■Dizziness
■Tinnitus
■Tinnitus
■Blurred vision
■Blurred vision
■Irritability or nervousness
■Irritability or nervousness
■Insomnia
■Insomnia
■Tremor
■Tremor
■GI complaints (rare)a
■GI complaints (rare)a
■Nausea and vomiting
■Nausea and vomiting
■Diarrhea or constipation
■Diarrhea or constipation
■Anorexia
■Anorexia
■Anticholinergic effectsa
■Anticholinergic effectsa
■Dry mucous membranes
■Dry mucous membranes
■Urinary retention
■Urinary retention
■Postural hypotension
■Postural hypotension
■Cardiac arrhythmias (particularly prolongation of the QT interval, ventricular arrhythmias, torsades de pointes) (rare)a
■Cardiac arrhythmias (particularly prolongation of the QT interval,
ventricular arrhythmias, torsades de pointes) (rare)a
■Hypersensitivity reactions (rare)
■Hypersensitivity reactions (rare)
3455
aMore common in first-generation H1 antihistamines.
28
insomnia, and tremor.1,4 Most second-generation H1 antihistamines, except for cetirizine and levocetirizine, are low sedating and thus better tolerated than firstgeneration agents.37-41 Although far less soporific than its parent compound hydroxyzine, cetirizine causes sedation in approximately 10% to 15% of users, and appears to be dose dependent.38,39 At doses of 10 mg and 20 mg, cetirizine occupies 12% and 25% of H1 receptors in the human brain, respectively, as assessed by positron emission tomography scan.40 Fexofenadine and loratadine/desloratadine, on the other hand, are least likely to enter the brain, and consequently have few if any CNS effects.4,41
Anticholinergic side effects are much more common with first-generation H1 antihistamines as they have an affinity for cholinergic receptors.4,42,43 These anticholinergic side effects include dry mucous membranes, urinary retention and hesitancy, postural hypotension, dizziness, erectile dysfunction, and constipation. These effects are often associated with the ethanolamine, phenothiazine, and piperazine groups. The anticholinergic effects of H1 antihistamines preclude their use in patients with narrow-angle glaucoma and require close monitoring in patients with prostatic hypertrophy.4,42 Most secondgeneration H1 antihistamines are selective for H1 receptors, and thus lack these anticholinergic side effects.1,4,41
GI complaints, including anorexia, nausea, vomiting, epigastric distress, diarrhea, and constipation, are uncommon side effects. The administration of these agents with food frequently reduces/eliminates these symptoms.1,6
Arrhythmias, particularly prolongation of the QT interval and torsades de pointes, are the most serious, but fortunately rare, cardiac side effects.1,6 These dosedependent effects are mediated through blockade of potassium channels unrelated to the H1 histamine receptor. Transient hypotension may develop after intravenous therapy, especially if the drug is administered rapidly.43 Two early second-generation H1 antihistamines, terfenadine and astemizole, were removed from the world market because of risk of QT interval prolongation and torsades de pointes. Other secondgeneration agents have an approximately 1000-fold lower affinity for cardiac ion channels than terfenadine and astemizole. Evidence for ventricular arrhythmias have been extensively investigated and found to be absent in the newer second-generation H1 antihistamines currently available in the United States.4,5,42
The occurrence of cutaneous reactions after the administration of oral H1 antihistamines is extremely uncommon. Reported reactions include eczematous dermatitis, allergic contact dermatitis, urticaria, petechiae, fixed drug eruptions, and photosensitivity. Some of these reactions may be secondary to excipients in the drug.44
DRUG INTERACTIONS
DRUG INTERACTIONS
The H1 antihistamines may interact with other drugs metabolized by the hepatic CYP system, such as imidazole antifungals, cimetidine, and macrolide
3456
antibiotics.4,6 The first-generation H1 antihistamines— diphenhydramine, chlorpheniramine, clemastine, promethazine, hydroxyzine, and tripelennamine— inhibit the hepatic enzyme CYP 2D6 in vitro.45,46 In vivo, diphenhydramine has been noted to increase levels of other drugs metabolized by the CYP 2D6 system, including metoprolol and venlafaxine. Firstgeneration H1 antihistamines are contraindicated for patients receiving monoamine oxidase inhibitors as these medications may interfere with the metabolism of monoamine oxidase inhibitors.6,46,47
Central depressive effects may be accentuated when sedating H1 antihistamines are combined with alcohol or other CNS depressants such as benzodiazepines. These interactions are generally not observed with second-generation H1 antihistamines. In rare circumstances, antihistamines of the phenothiazine group may block and reverse the vasopressor effect of epinephrine. If individuals receiving a phenothiazine require a vasopressor agent, norepinephrine or phenylephrine should be used.1,6,42
SPECIAL PATIENT POPULATIONS
SPECIAL PATIENT
POPULATIONS
CHILDREN
Many of the sedating and low-sedating H1 antihistamines can be safely used in children with appropriate dosing. Children may be more susceptible to certain side effects, such as excitation and insomnia, especially with first-generation H1 antihistamines. Acute poisoning may develop with first-generation agents, but this is rare. Hallucinations, ataxia, incoordination, athetosis, and convulsions are the major features. The second-generation H1 antihistamines cetirizine, levocetirizine, and loratadine have been extensively studied in children from 6 to 36 months of age with long-term safety profiles equal to placebo.4,48,49
ELDERLY
Caution should be used when treating elderly patients who may have renal insufficiency, cardiac disease, chronic hepatic disease, and/or CNS or balance comorbidities with first-generation H1 antihistamines. Older individuals may be more susceptible to anticholinergic effects, particularly urinary retention and hesitancy, constipation, and postural hypotension.4,6,42
PREGNANT WOMEN
There are limited guidelines for the use of H1 antihistamines in pregnant women. Most H1 antihistamines are classified as U.S. Food and Drug Administration (FDA) pregnancy category B or category C. Based on earlier reports linking H1 antihistamines to fetal malformations, particularly cleft palate defects, these agents have been
customarily avoided in the first trimester of pregnancy. However, newer studies, including a metaanalysis of 200,000 first-trimester exposures to first-generation antihistamines, did not demonstrate an increased risk of congenital malformations.50 In a prospective trial, astemizole administered to pregnant women was not associated with intrauterine growth retardation or perinatal complications, and the rate of congenital abnormalities was identical to the control group and general population.51-53
BREASTFEEDING WOMEN
No formal studies have been performed on the safety of H1 antihistamines during breastfeeding. Theoretically, these drugs may diminish milk supply via anticholinergic effects. Clemastine, diphenhydramine, promethazine, triprolidine, cetirizine, loratadine, fexofenadine, desloratadine, and levocetirizine are all known to be excreted in breastmilk; however, their effects on the nursing infants has not been studied. When antihistamine therapy is necessary for the nursing mother, second-generation agents, which have fewer side effects and toxicities, are preferred.4,6,52
H2 ANTIHISTAMINES
MECHANISM OF ACTION
MECHANISM OF ACTION
H2 antihistamines also are inverse agonists and include cimetidine, ranitidine, famotidine, and nizatidine. These agents bind to H2 receptors located throughout the body, including epithelial cells, endothelial cells, and chondrocytes, as well as lymphocytes, neutrophils, eosinophils, monocytes, mast cells and dermal dendritic cells. In addition to their association with gastric acid secretion, H2 receptors, and thus H2 antihistamines, appear to play some role in antigen presentation, cellular recruitment, cutaneous vascular permeability, and local release of inflammatory mediators.54 These complex immune events, however, remain poorly defined.
PHARMACOKINETICS
PHARMACOKINETICS
H2 antihistamines are rapidly absorbed from the GI tract with peak levels occurring between 1 and 2 hours after administration. They are eliminated primarily unchanged through renal excretion with only 10% to 35% undergoing hepatic metabolism. The half-life of cimetidine in plasma is 2 hours, and approximately 70% is excreted unchanged in the urine.54,55 The plasma half-life of ranitidine is 2 to 3 hours in healthy adults, and longer in elderly individuals and those with liver or kidney disease.55,56 Famotidine has a plasma half-life of 3 to 8 hours, but may exceed 20 hours in patients with renal failure.57 Nizatidine has a plasma half-life of 1 to 2 hours, and its duration of action is up to 10 hours.51 The oral bioavailability of nizatidine is not affected by food and this antihistamine is primarily
28
■Acute allergic reactions
■Acute allergic reactions
■Chronic urticaria (as a second-line agent)
■Chronic urticaria (as a second-line agent)
■Systemic symptoms associated with mastocytosis (especially GI related)
■Systemic symptoms associated with mastocytosis
(especially GI related)
eliminated by the kidneys within 16 hours. In general, H2 antihistamines have limited penetration of the blood–brain barrier.55-58
INDICATIONS IN DERMATOLOGY
INDICATIONS IN
DERMATOLOGY
There are few data from controlled studies supporting the use of H2 antihistamines to treat dermatologic conditions (Table 189-6). Several studies demonstrate that H2 antihistamines have a limited role in blocking histamineinduced wheal-and-flare reactions in the skin. Compared to H1 antihistamines alone, the addition of an H2 antihistamine further reduces this reaction by only 5% to 15%.59 Most often, H2 antihistamines are used in combination with H1 agents in refractory cases of CIU and angioedema. In a double-blind crossover study, greater reductions in pruritus and wheal number, size, and severity were observed when cimetidine was combined with hydroxyzine versus hydroxyzine alone.59 Similar observations have been made for when cimetidine was combined with chlorpheniramine.60 Combination H1 and H2 antihistamine therapy also may be helpful in reducing GI symptoms associated with mastocytosis.34 High doses of cimetidine also have been reported successful in the treatment of verruca vulgaris in some individuals.61
INITIATION OF THERAPY
INITIATION OF THERAPY
For treatment of dermatologic conditions, H2 antihistamines are generally used following an unsuccessful trial of H1 antihistamines alone. In most cases, treatment with H2 antihistamines may be initiated without any particular laboratory screening. The inhibition of the hepatic CYP system and the potential for drug interactions is usually the greatest concern, and patients’ medication lists should be reviewed carefully before initiating therapy. Ranitidine is less inhibitory of the CYP system than cimetidine and may be the preferred H2 antihistamine in situations in which drug interactions are a particular concern.56 Also, patients with decreased creatinine clearance may require dosage adjustments.62 In patients taking the cardiac drug dofetilide, cimetidine is contraindicated because of the risk of prolongation of the QT interval and life-threatening cardiac arrhythmias.63 Therapeutic end points for H2 antihistamines are determined by improvements in
3457
28
DRUG FORMULATION DOSAGE CONDITIONS REQUIRING DOSAGE ADJUSTMENT
Cimetidine
100-, 200-, 300-, 400-, 800-mg tablet Adult: 400-800 mg twice daily Renal or hepatic impairment
300 mg/5 mL syrup
200 mg/20 mL syrup
Ranitidine
75-, 150-, 300-mg tablet Adult: 75-150 mg twice daily Renal impairment
15 mg/5 mL syrup Pediatric: 5-10 mg/kg/day divided in 2 doses
150-mg granules
Famotidine
10-, 20-, 40-mg tablet Adult: 20-40 mg twice daily Renal impairment
40 mg/5 mL syrup Age 1-16 years: 1 mg/kg/day
Divided in 2 doses, up to 40 mg twice daily
Nizatidine 150-, 300-mg capsule Age ≥12 years: 150 mg daily, twice daily Renal impairment
15 mg/5 mL syrup
15 mg/5 mL syrup
histamine-related signs and symptoms (eg, pruritus; flushing, wheal size/frequency/intensity). Table 189-7 lists the dosing regimens for H2 antihistamines.
RISKS AND PRECAUTIONS
RISKS AND PRECAUTIONS
In general, H2 antihistamines are safe and rarely cause significant side effects. However, in patients with hepatic or renal disease, there is a greater risk for adverse effects. H2 antihistamines may have CNS effects, including confusion, headache, and dizziness (Table 189-8). These effects seem to be partly dose-related. Other, less-common side effects include drowsiness, malaise, muscular pain, diarrhea, and constipation. There are rare reports of granulocytopenia.56-58 For patients with a history of thrombocytopenia, a complete blood count
■CNS disturbances
■CNS disturbances
■Confusion
■Confusion
■Dizziness
■Dizziness
■Drowsiness
■Drowsiness
■Headache
■Headache
■GI effects
■GI effects
■Abdominal pain
■Abdominal pain
■Diarrhea or constipation
■Diarrhea or constipation
■Increased transaminases and hepatitis (rare)
■Increased transaminases and hepatitis (rare)
■Nausea or vomiting
■Nausea or vomiting
■Gynecomastia
■Gynecomastia
■Hematologic (rare)
■Hematologic (rare)
■Anemia
■Anemia
■Thrombocytopenia
■Thrombocytopenia
■Hypersensitivity to H2 (uncommon)
■Hypersensitivity to H2 (uncommon)
■Drug interactions
■Drug interactions
■Cardiac effects (with concomitant administration of dofetilide; dofetilide use is therefore a contraindication)
■Cardiac effects (with concomitant administration of dofetilide;
3458
dofetilide use is therefore a contraindication)
may be warranted once H2 antihistamine therapy is initiated, because thrombocytopenia has been reported as an idiosyncratic effect in a few individuals.64 By their suppression of gastric acid secretion, H2 antihistamines may facilitate oral infections and increase the risk of pneumonia in immunocompromised individuals.65 As a class, these drugs may mask symptoms of gastric carcinoma. Also, cimetidine and ranitidine inhibit alcohol dehydrogenase activity, which can lead to increased blood alcohol levels.56
Uncommon side effects of cimetidine include gynecomastia with or without elevated prolactin levels in men; galactorrhea with elevated prolactin levels in women; and loss of libido, impotence, and reduction of sperm counts in young men.56 Modest elevations in serum creatinine levels and hepatic transaminase levels have been reported and are reversible after the drug is withdrawn.56,66 Rare dermatologic adverse effects, including alopecia and urticarial vasculitis, also have been reported.66-68
Ranitidine does not bind to androgen receptors and unlike cimetidine, does not enhance cell-mediated immune responses.56 Ranitidine may affect the cardiovascular system by altering parasympathetic and sympathetic control functions. This altered cardiac sympathovagal balance may lead to a susceptibility to arrhythmias, particularly bradyarrhythmias, after intravenous infusion.68
Famotidine and nizatidine are associated with few side effects. They cause less inhibition of the CYP system, and therefore have fewer reported drug interactions.57,58
DRUG INTERACTIONS
DRUG INTERACTIONS
Through inhibition of the CYP system, cimetidine increases the serum levels of numerous drugs, including some commonly prescribed medications.68,69
Cimetidine increases levels of warfarin potentially leading to an increased risk of bleeding. This agent
also interacts with cardiac drugs, including β blockers, calcium channel blockers, amiodarone, and antiarrhythmic agents. As already mentioned, cimetidine use is contraindicated in patients taking dofetilide. Both cimetidine and ranitidine also can reduce the urinary excretion of procainamide and quinidine. Other common drugs with which cimetidine interacts are phenytoin, benzodiazepines, metformin, sulfonylureas, and selective serotonin reuptake inhibitors.56,68,69
Although ranitidine interacts with other medications less frequently than cimetidine, significant interactions with fentanyl, metoprolol, midazolam, nifedipine, theophylline, and warfarin have been observed. Ranitidine may decrease the absorption of diazepam and reduce its plasma concentration by 25%.56
SPECIAL PATIENT POPULATIONS
SPECIAL PATIENT
POPULATIONS
CHILDREN
Of the H2 antihistamines, ranitidine and famotidine have pharmacokinetics that have been relatively well studied in children, and these drugs have acceptable safety profiles with appropriate dosing. Cimetidine and nizatidine are not recommended for children for uses other than reducing gastric acidity. One adverse effect unique to children is an uncommon but drug class– wide risk of necrotizing enterocolitis in neonates.70
ELDERLY
Older patients may require a reduction in dosage to accommodate decreased renal function, as well as careful review of medication lists. Elderly patients also appear more susceptible to H2 antihistamine–induced CNS disturbances, such as confusion and dizziness.56-58
PREGNANT WOMEN
The H2 antihistamines are classified as FDA pregnancy category B drugs. Cimetidine, ranitidine, famotidine, and nizatidine are all excreted in breastmilk; however, the potential effects on the nursing infant have not been studied.56-58
OTHER THERAPEUTIC AGENTS WITH ANTIHISTAMINIC ACTIVITY
TRICYCLIC ANTIDEPRESSANTS
TRICYCLIC
ANTIDEPRESSANTS
Tricyclic antidepressants bind to both H1 and H2 receptors. The tricyclic antidepressant most commonly used in dermatology is doxepin, which is 800 times more potent
28
than diphenhydramine.71 Oral doxepin has been used successfully in the treatment of refractory CIU, physical urticarials, and pruritus associated with systemic conditions.72,73 In a double-blind, crossover study, doxepin proved more efficacious than diphenhydramine in the treatment of CIU.72 Topical doxepin cream has proven effective for the treatment of pruritus in patients with atopic dermatitis and lichen simplex chronicus.73
Sedation is the most common adverse effect with both oral and topical doxepin, although some patients may develop tolerance with regular use.72-74 Oral doxepin has been classified by the FDA as a pregnancy category C drug; topical doxepin is classified as a pregnancy category B drug.74 Use of both oral and topical forms is contraindicated during breastfeeding. The safety and efficacy of doxepin therapy in children younger than age 12 years has not been established. This drug also should be used with caution in elderly patients, who may be more susceptible to its anticholinergic effects, including urinary retention and blurred vision. Doxepin should not be used concurrently with monoamine oxidase inhibitors, and all patients with underlying depression should be closely monitored for signs of suicidal ideation when initiating therapy. Doxepin also can cause a sudden increase in intraocular pressure and should not be used in patients with glaucoma.71-74 Although doxepin has the potential to alter myocardial function, several studies have shown this medication to be safe in depressed patients with and without underlying heart disease.75
KETOTIFEN
KETOTIFEN
Ketotifen, a benzocycloheptathiophene derivative, is an H1 antihistamine with additional mast cell– and basophil-stabilizing properties.3,76,77 Ketotifen has been used successfully in the treatment of CIU, physical urticaria, and symptoms associated with mastocytosis.76-79
In a double-blind trial in CIU patients, ketotifen alleviated pruritus more effectively than clemastine or placebo.79 Studies comparing ketotifen with lowsedating H1 antihistamines have not been performed. Sedation and atropine-like side effects have been reported with this medication.80 There are no studies evaluating the safety of ketotifen in pregnant or breastfeeding women. Ketotifen is available in the United States only as an ophthalmic solution.80
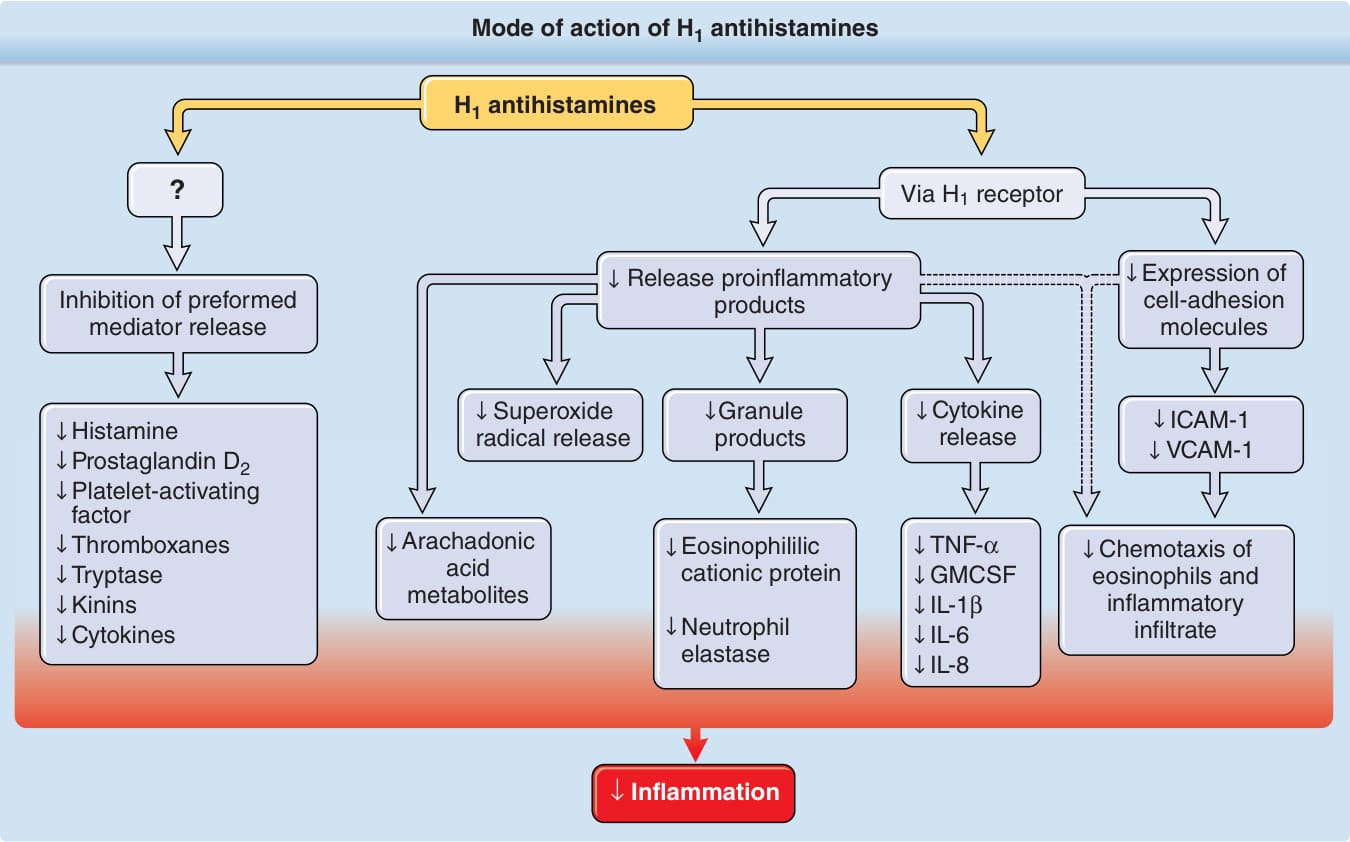
Figure 189-1 Mode of action of H1 antihistamines. By means of the H1 receptor, H1 antihistamines inhibit the release of preformed mediators and decrease the production of proinflammatory cytokines, the expression of cell-adhesion molecules, and chemotaxis of eosinophils and other cells. ↓, Decreased; GMCSF, granulocyte-macrophage colonystimulating factor; ICAM-1, intercellular adhesion molecule 1; IL, interleukin; TNF-α, tumor necrosis factor-α; VCAM-1, vascular cellular adhesion molecule 1.
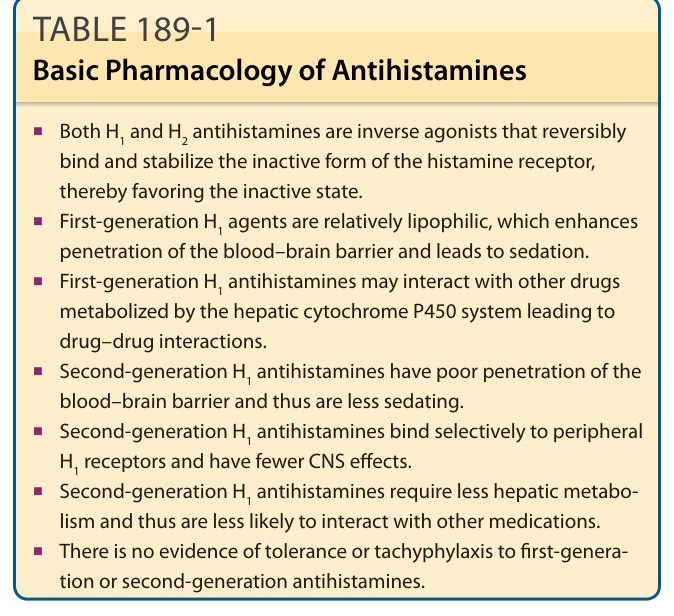
TABLE 189-1 Basic Pharmacology of Antihistamines
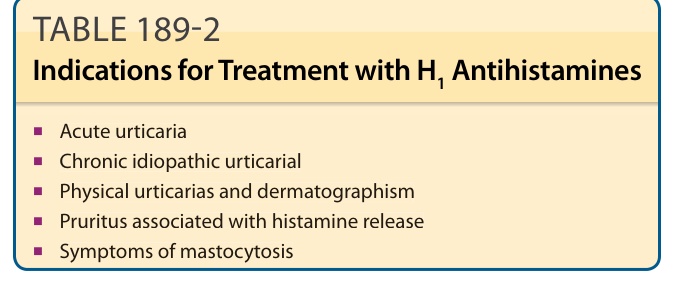
Table 189-2 outlines the indications for treatment with H1 antihistamines. H1 antihistamines appear to be effective in treating up to 50% of patients with chronic idiopathic urticaria (CIU), angioedema, and dermatographism. They are not as effective in treating physical urticarias, hereditary and acquired angioedema, urticarial vasculitis, and pruritus unrelated to histamine. Comparative studies of different groups of first-generation H1 antihistamines are few; however, in general, these agents appear to have equal efficacy in the treatment of CIU. If an agent from one class of H1 antihistamines proves ineffective, then an agent from another antihistamine group should be considered.4,19
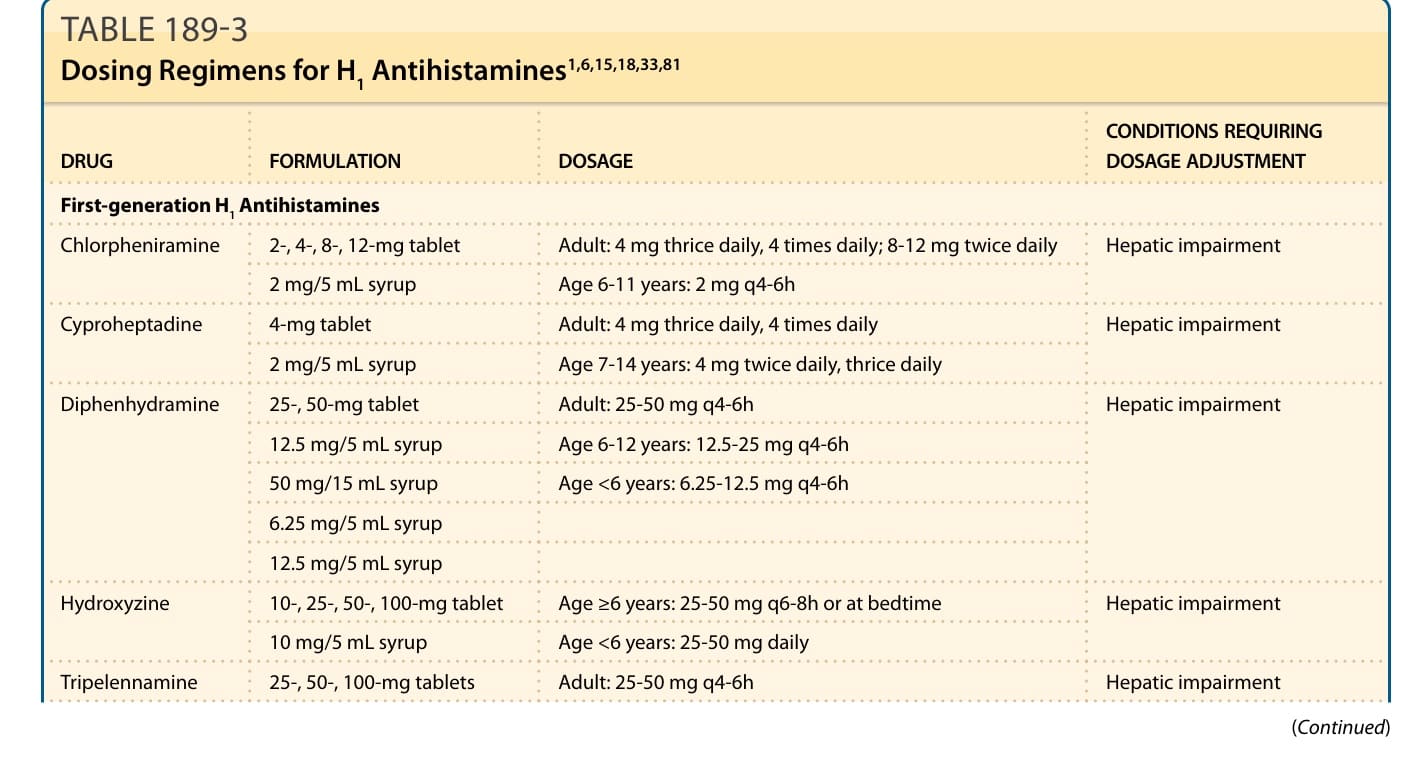
TABLE 189-3 Dosing Regimens for H1 Antihistamines1,6,15,18,33,81
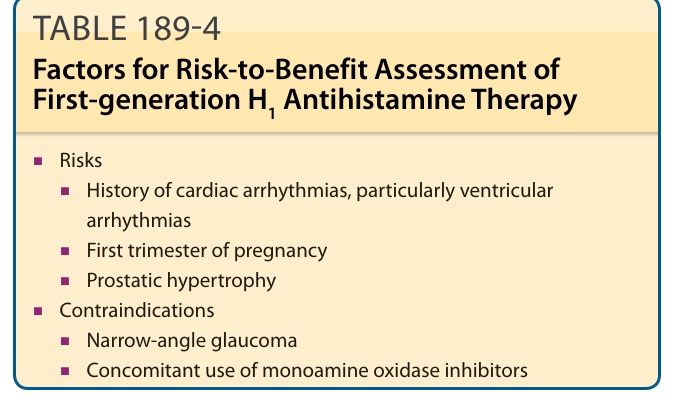
TABLE 189-4 Factors for Risk-to-Benefit Assessment of First-generation H1 Antihistamine Therapy
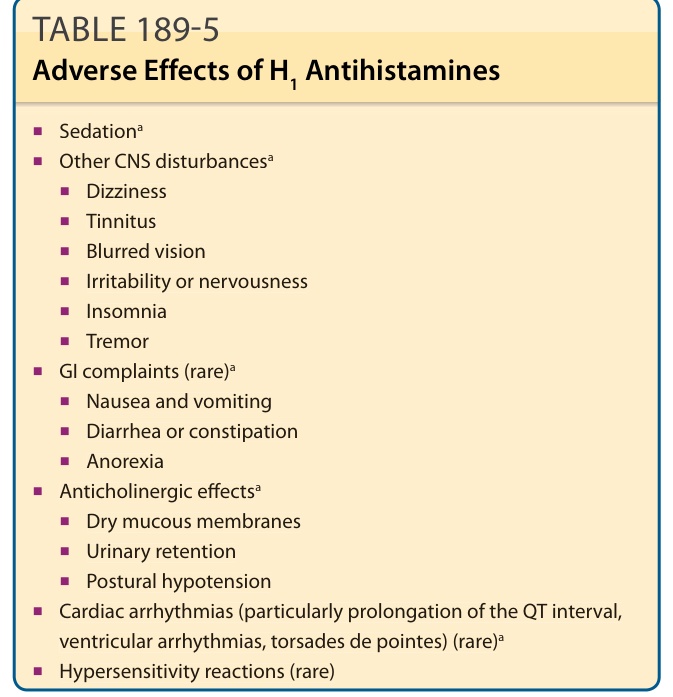
TABLE 189-5 Adverse Effects of H1 Antihistamines
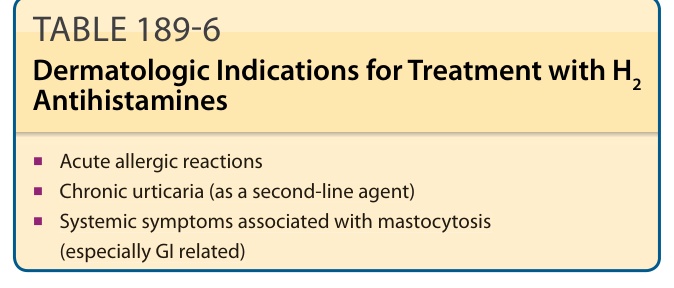
TABLE 189-6 Dermatologic Indications for Treatment with H2 Antihistamines
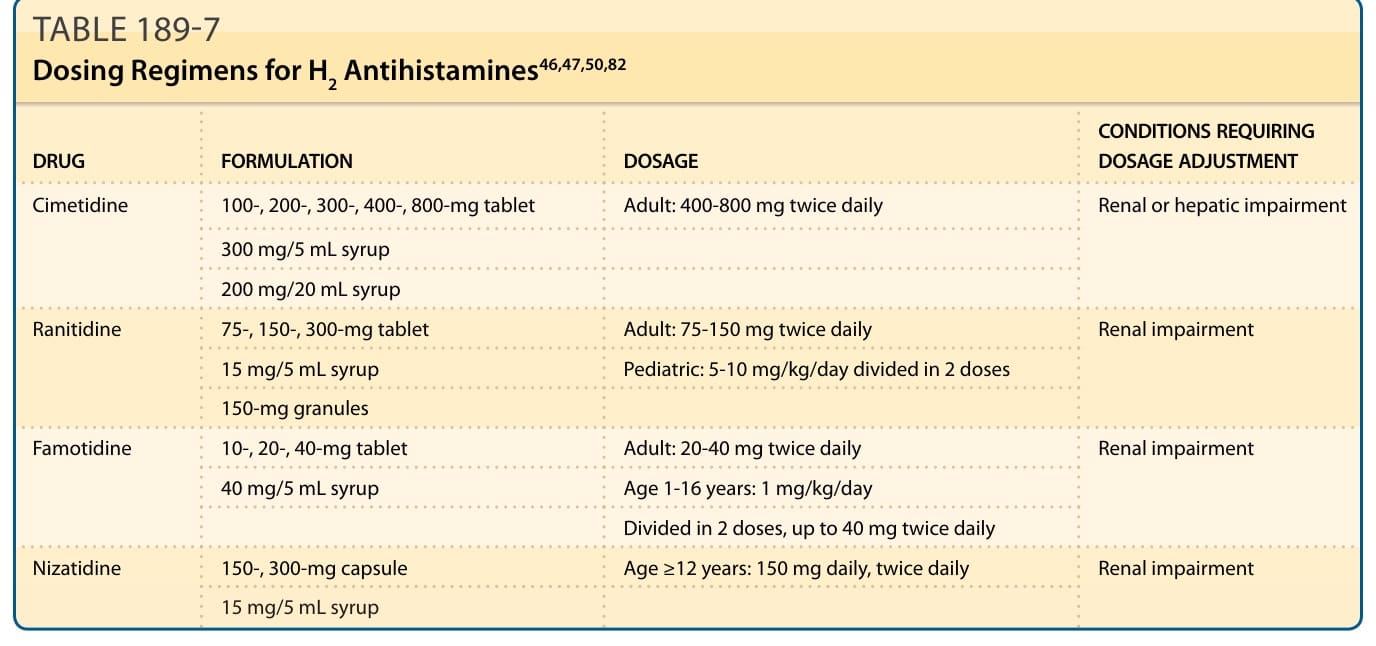
TABLE 189-7 Dosing Regimens for H2 Antihistamines46,47,50,82
TABLE 189-8 Adverse Effects of H2 Antihistamines