Dapsone
28
AT-A-GLANCE
■ Dapsone (4,4′-diaminodiphenylsulfone) is a sulfonamide with unique pharmacologic action.
■ It is used as an antiinfective in particular against Hensen disease and selected fungal infections such as actinomycetoma and rhinosporidiosis. It is also used for the treatment of malaria and as a prophylaxis for toxoplasmosis.
■ It is also an antiinflammatory agents and is effective against dermatitis herpetiformis, erythema elevatum diutinum, linear immunoglobulin A dermatosis and chronic bullous disease of childhood, and bullous eruption of systemic lupus erythematosus.
■ It has antineutrophilic effect and used against collagen vascular and autoimmune diseases and recently topically for acne.
■ It is often used as corticosteroid-sparing agent.
■ Significant side effects to watch for include hemolysis and methemoglobinemia, which are frequently observed in patient with glucose-6- phosphate dehydrogenase (G6PD) deficiency. Dapsone should only be given with great caution and in very special circumstances to patients with G6PD deficiency when the benefits outweigh the risks when constant hemoglobin and monitoring of reticulocyte counts is essential.
■ Other serious side effects include drug hypersensitivity syndrome (sulphone syndrome), Stevens-Johnson syndrome, and agranulocytosis.
■ Dapsone is classified as C Pregnancy Category (ie, risk not ruled out).
INTRODUCTION
Dapsone is 4,4′-diaminodiphenylsulfone,1,2 an aniline derivative belonging to the group of synthetic sulfones. Although dapsone is classified as a sulfonamide, crossreactions occur in only 7% to 22% of sulfa-allergic patients. They are usually mild.3,4
The molecule was synthesized in 1908, but research into dapsone as an antimicrobial agent started only in 1937.5,6 Later it was recognized to possess antiinflammatory effects, and it was investigated predominantly by in vitro studies aiming to get more information on the effect of dapsone on inflammatory effector cells, cytokines, and mediators, such as cellular toxic oxygen metabolism, myeloperoxidase-halogenid system, adhesion molecules, chemotaxis, membraneassociated phospholipids, prostaglandins, leukotrienes,
interleukin-8, tumor necrosis factor-α (TNF-α), lymphocyte functions, and tumor growth. The latter capabilities primarily were used in treating chronic inflammatory disorders. Hence, dapsone has dual functions, combining antimicrobial, antiprotozoal, and antiinflammatory effects resembling those of the nonsteroidal antiinflammatory drugs (NSAIDs).
MECHANISM OF ACTION
DAPSONE AS A BACTERIOSTATIC ANTIBIOTIC AGENT
DAPSONE AS A
BACTERIOSTATIC
ANTIBIOTIC AGENT
Dapsone acts by interfering in the folate biosynthetic pathway. It inhibits the synthesis of dihydrofolic acid by competing with para-aminobenzoic acid for the active site of dihydropteroate synthetase.7,8 It has been used for the treatment of Hensen disease since 1945 (often in combination with other antibiotics, eg, rifampicin and clofazimine). It is also used to treat toxoplasmosis and is used for pneumocystis pneumonia (PCP) prophylaxis in immunocompromised patients in whom it is often prescribed in combination with pyrimethamine and leucovorin. It is also used as chemoprophylaxis for Plasmodium falciparum malaria. In the early 2000s, a topical 5% dapsone gel was reported to be effective against acne without causing clinically significant declines in hemoglobin levels, even in patients with glucose-6-phosphate dehydrogenase (G6PD) deficiency.9 In February 2016, the U.S. Food and Drug Administration (FDA) approved a 7.5% dapsone gel for once-daily application versus twice-daily application of the 5% formulation for acne vulgaris.10 The mechanism of action of topical dapsone here is likely to result from its combined antiinflammatory and antimicrobial activities.
DAPSONE AS AN ANTIINFLAMMATORY AGENT
DAPSONE AS AN
ANTIINFLAMMATORY
AGENT
The antiinflammatory effects of dapsone was studied in animals in the 1970s. Studies showed wide variations in dapsone antiinflammatory properties. The conclusion then was that dapsone can be attributed as an antiinflammatory potential comparable to the NSAIDs. But its exact antiinflammatory mechanism
28
remains unknown. Since then it has been used for its antiinflammatory action on selected dermatologic disorders, especially in those with neutrophilic chemotaxis (eg, dermatitis herpetiformis and leukocytoclastic vasculitis). Dapsone inhibits migration of neutrophils to areas of inflammation by inhibiting neutrophil chemotaxis to the chemoattractant signals F-met-leu-phe6,11 and leukotriene B4 (LTB4).12-14 Dapsone also inhibits the adherence of neutrophils to skin-localized immunoglobulin A (IgA)15 and endothelium.16 Additionally, dapsone inhibits the release of inflammatory mediators, including interleukin (IL)-8,17 prostaglandin D2, and TNF-α.18
Dapsone also inhibit the myeloperoxidase H2O2-halide– mediated cytotoxic system,19,20 likely via the inhibition of the calcium flux necessary for these events.21 Myeloperoxidase is the enzyme in the azurophilic granules of neutrophils and in the lysosomes of monocytes that catalyzes the conversion of hydrogen peroxide and chloride ions into hypochlorous acid, a potent oxidant that causes cell damage.22
The dual antimicrobial and antiinflammatory functions and the long-term usage safety profile of dapsone place it in a unique position as a therapeutic agent different from other drugs. First, its antimicrobial effects can be used in immunocompromised conditions to prevent and treat opportunistic infections in patients (eg, against bacterial and protozoal infection). Second, it is safe for use in long-term treatment (eg, lifelong use in leprosy, long-term intermittent therapy in inflammatory dermatoses). Third, it has unique powerful disease-specific antiinflammatory activities (eg, prompt decrease of pruritus and control of skin lesions in dermatitis herpetiformis to the extent that the disease rapid and dramatic response to dapsone is sometime used as a diagnostic test of the disease).
CHEMISTRY AND PHARMACOLOGY OF DAPSONE
Chemically, dapsone is an aniline derivative. As a sulfone, it shows the structure of a sulphur atom linking to two carbon atoms (Fig. 187-1). The solubility of dapsone varies over a wide range depending on the solvent used (eg, water, 0.2 mg/mL vs methanol, 52 mg/mL). After oral administration, dapsone is almost completely absorbed from the gut with bioavailability exceeding 86%. Peak serum concentrations are attained within 2 to 8 hours. After ingestion of a single 50- to 300-mg dose of dapsone, maximum serum concentrations range from 0.63 to 4.82 mg/L.23,24
Under steady-state conditions, 100 mg/day (the dose most frequently used) results in serum concentrations of 3.26 mg/L (maximum) and 1.95 mg/L (after 24 hours).8,23,24 These dapsone serum concentrations attained in vivo must be kept in mind when interpreting the results of in vitro investigations. After absorption, dapsone undergoes enterohepatic circulation. It is metabolized by the liver but also by
3424
Dapsone structure
C12H12N2O2S
O O
S
NH2 H2N
activated polymorphonuclear leukocytes (PMNs) and mononuclear cells.25 In the liver, dapsone is metabolized primarily through acetylation by N-acetyltransferase to monacetyl-dapsone (MADDS) and through hydroxylation by cytochrome P-450 enzymes, resulting in the generation of dapsone hydroxylamine (DDS-NOH). In fact, administration of dapsone has been used to determine the acetylation phenotype (rapid vs slow acetylator). In terms of both efficacy and induction of adverse effects, the most important issue is the generation of DDS-NOH. This metabolic pathway also occurs in lesional skin of inflammatory dermatoses and is thought to be mediated by activated PMN.25 Dapsone is distributed to virtually all organs and retained in the skin, muscle, kidneys, and liver. Trace concentrations of the drug may be presented in these tissues up to 3 weeks after discontinuation of dapsone treatment. The drug is also distributed into sweat, saliva, sputum, tears, and bile. Dapsone is 50% to 90% bound to plasma proteins, but MADDS is almost completely bound to plasma proteins. It crosses the blood–brain barrier and placenta and is detectable in breast milk.26,27 Cases have been reported in which dapsone therapy of the mother resulted in neonatal hemolysis and cyanosis.28
Approximately 20% of dapsone is excreted as unchanged drug via urine, and 70% to 85% is eliminated as water-soluble metabolites after conjugation with glucuronic acid. This step is mediated by uridine diphosphate glucuronosyltransferase. Additionally, a small amount might be excreted in faeces, including some yet unidentified metabolites. The complex metabolic pathway of dapsone has been reviewed.24,25,29
When dapsone is administered, there is equilibrium between acetylation and deacetylation. Thus, there is the possibility that PMNs in peripheral blood are exposed both to dapsone and its metabolites. These metabolites, such as DDS-NOH, have been shown to be pharmacologically active. However, they are believed
to be responsible for its antiinflammatory mechanisms (eg, inhibition of chemotaxis) but also for a number of side effects. This has been clearly documented for DDS-NOH. Interestingly, Khan and coworkers30
recently demonstrated that human keratinocytes that had been stimulated by various cytokines such as TNF-α, IL-1β, and interferon γ (INF-γ) can produce DDS-NOH as well. Dapsone tablets are available in 25- and 100-mg sizes; therapeutic doses for various conditions range from 25 mg to approximately 400 mg. Dapsone is well absorbed from the gut with peak levels being reached 2 to 6 hours after a single dose. The half-life, approximately 30 hours because of enterohepatic recirculation.24 This allows for once-daily dosing and explains the utility of activated charcoal in reducing drug levels during accidental or intentional overdose.31 Dapsone and its metabolites may be transmitted through human milk, and hemolysis has occurred in nursing infants.27,32,33 No teratogenicity has been observed, but no controlled studies have been performed in humans, and it is classified as Pregnancy Category C.34,35
Topical dapsone in a 5% gel formulation was approved in 2005 for the treatment of acne vulgaris.36,37
Twice-daily application on up to 22% of patients’ body surface area resulted in systemic levels of dapsone and its metabolites that were 100-fold less than oral dapsone at a therapeutic dose. There was no hemolytic anemia or methemoglobinemia, even in patients who were G6PD deficient.9,38-40 Therefore, in 2008, the FDA removed the requirement for pretreatment G6PD testing. Overall, topical dapsone gel has a favorable short- and long-term safety profile. A higher concentration of 7.5% dapsone gel as a oncedaily application has shown to be effective in multiple subgroups of patients.41-44 It was well tolerated, with a low incidence of treatment-related adverse events, with the majority of adverse events being administration site related and mild or moderate in severity.42,45 Topical dapsone has also been shown in a case report to be effective in the treatment of leukocytoclastic vasculitis.46,47
Dapsone is metabolized in the liver. The two major metabolic pathways involve acetylation48,49 and N-hydroxylation.43-45 Dapsone is acetylated polymorphically; that is, some patients rapidly acetylate dapsone to MADDS, but others acetylate dapsone slowly. However, in all patients, MADDS is rapidly deacetylated. Thus, equilibrium between MADDS and dapsone is quickly reached and sustained. Dapsone’s efficacy, half-life, and toxicities appear unrelated to the rate of acetylation, and checking the acetylator phenotype is unnecessary before use of dapsone. The most clinically significant metabolic pathway of dapsone involves hydroxylation of one of the amino groups by cytochrome 2C19,43 3A4, and 2C9 and 2C844 to form dapsone hydroxylamine. Dapsone hydroxylamine is a potent oxidant that is responsible for development of methemoglobinemia, hemolysis, and liver damage.45,47,50,51 Dapsone hydroxylamine is reduced back to dapsone by methemoglobin reductase in erythrocytes and cytochrome b5 reductase and cytochrome P2D in hepatocytes. Reduced levels of
28
Increase Blood Levels of Dapsone (Greater Chance of Adverse Events)
■Probenecid
■Trimethoprim
Reduces Blood Levels of Dapsone (Lowers Effectiveness)
■Rifampicin
Block N-Hydroxylation of Dapsone (Lessening Side Effects)
Block N-Hydroxylation of Dapsone (Lessening Side Effects)
■Cimetidine
■Cimetidine
■Omeprazole
■Omeprazole
these enzymes have been detected in dapsone-treated patients who developed symptomatic methemoglobinemia. Genetic variability in detoxifying enzymes may therefore explain patients’ differential development of methemoglobinemia.52 Recent studies have also shown that dapsone can be hydroxylated by keratinocytes themselves. These hydroxylated metabolites then form drug–protein adducts that generate stress signals, which are delivered to draining lymph nodes. This may be responsible for the pathogenesis of some of the cutaneous side effects of dapsone.53-55
Dapsone is predominantly metabolized by the hepatocytes, but a small study indicated that there is no need to adjust dapsone doses in patients with cirrhosis.56 However, it is prudent to exercise caution when prescribing dapsone in patients with hepatic disease. Probenecid57 and trimethoprim58 have been shown to lead to higher blood levels of dapsone (Table 187-1), hence the need to exercise caution when prescribing them concurrently. Conversely, rifampicin reduces dapsone blood levels by upregulating the P450 system.59 Cimetidine and omeprazole, which block N-hydroxylation of dapsone, have been used to mitigate some of the side effects of dapsone. Cimetidine dosed 400 mg three times a day has reduced methemoglobin levels in reported patients by 27% to 60%.60-63
Dapsone and its metabolites are excreted by the kidneys; therefore, it is important to check renal functions before prescribing dapsone to patients. Dapsone should be avoided in patients with significant renal dysfunction.
MEDICAL INDICATIONS OF DAPSONE
Since its introduction, dapsone has had therapeutic trials and anecdotal successes in a multitude of diseases (Table 187-2). However, there are only a few conditions for which dapsone is considered the drug of choice.
ANTIMICROBIAL ACTION
ANTIMICROBIAL ACTION
Dapsone is most commonly used in combination with rifampicin and clofazimine for the treatment of leprosy.64 It is also used to both treat and prevent PCP,65
3425
28
As an Antiinfective Drug Infections diseases: Hensen disease, malaria, leishmaniasis, nocardiosis, Pneumocystis prophylaxis
As an Antiinflammatory Drug Consistently responsive: dermatitis herpetiformis, erythema elevatum diutinum, linear IgA dermatosis and chronic bullous dermatosis of childhood (idiopathic or drug induced), bullous SLE, prurigo pigmentosa, acropustulosis infantalis
Used as an Adjunctive Combination Treatment Autoimmune blistering diseases: pemphigus (foliaceus, vulgaris and IgA variants), bullous pemphigoid, epidermolysis bullosa acquisita, mucous membrane pemphigoid Neutrophilic dermatosis: subcorneal pustular dermatosis (idiopathic and drug induced), acute febrile neutrophilic dermatosis (Sweet syndrome), pyoderma gangrenosum Autoimmune diseases: rheumatoid papules, relapsing polychondritis, subacute lupus erythematosus, chronic cutaneous lupus erythematosus, lupus panniculitis, vasculitides, cutaneous polyarteritis nodosa, urticarial vasculitis, Henoch-Schönlein purpura, chronic leukocytoclastic vasculitis Others: Behçet disease, acne and related disorders, hidradenitis suppurativa, granuloma faciale, perifolliculitis capitis abscedens et suffodiens, brown recluse spider bites that becomes necrotic, generalized granuloma annulare, chronic idiopathic thrombocytopenia purpura, chronic urticaria, aphthous stomatitis, psoriasis, Melkersson-Rosenthal syndrome, eosinophilic fasciitis, α1-antitrypsin deficiency–related panniculitis, neutrophilic eccrine hidradenitis, insect bite–like reactions in patients with leukemia, erythema multiforme, Rosai-Dorfman disease, idiopathic angioedema, eosinophilic folliculitis (Ofuji disease)
Used in Nondermatologic Disorders Rheumatoid arthritis, eosinophilic fasciitis, immune thrombocytope-
Used in Nondermatologic Disorders Rheumatoid arthritis, eosinophilic fasciitis, immune thrombocytopenia, stroke, asthma, seizure disorders, glioblastoma
nia, stroke, asthma, seizure disorders, glioblastoma
especially in immunocompromised hosts. It is also used for toxoplasmosis in people who are unable to tolerate trimethoprim with sulfamethoxazole.65
ANTIINFLAMMATORY ACTION
ANTIINFLAMMATORY
ACTION
Other indications include dermatitis herpetiformis (in combination with a gluten-free diet),66,67 erythema elevatum diutinum (effective in 80% of early cases of the disease),68,69 linear IgA dermatosis and chronic bullous dermatosis of childhood,70-73 and the bullous eruption of systemic lupus erythematosus.74,75 Patients with these disorders achieve a clinical response within 24 to 48 hours, and their conditions flare over the same time course with drug withdrawal. In 2015, dapsone was reported to be effective against generalized granuloma annulare.76
Other noninfectious conditions in which dapsone has found sporadic success span the spectrum of dermatologic disease (see Table 187-2).75,77-147 As a unifying feature, most of these diseases have granulocytes
3426
(neutrophils or eosinophils) as the predominant infiltrating cell, especially early in the pathologic process. The response to dapsone therapy is not as rapid, regular, or predictable in these diseases. However, dapsone may have a role as a second-line or steroid-sparing agent.
DOSAGES
A therapeutic dose of dapsone varies from 25 mg to 200 mg/day, usually in a single dose. Rarely, patients may require 300 mg/day before a response is seen. The recommended starting dose is between 50 and 100 mg/day to minimize potential pharmacologic adverse effects, in particular hemolysis. If a therapeutic trial of dapsone is successful, the dose of dapsone should be decreased to a point at which lesions recur to be sure that the improvement was indeed caused by dapsone and that there is a continuing need for the drug. Reducing the dose of dapsone to the lowest effective dose is an important means to minimize potential side effects.
TOPICAL DAPSONE
TOPICAL DAPSONE
Topical dapsone (5% gel) is FDA approved for acne vulgaris in adults9,36-40 and adolescents77 up to 12 years old. It has not been reported to cause hemolysis even in patients with G6PD deficiency.9 Clinical trials showed that it can reduce the mean total lesion count by 39% and 49%.9,36,40,77 It can be used in conjunction with other acne medications, including adapalene and benzoyl peroxide gel.78
Topical dapsone, when applied together with benzoyl peroxide, may cause yellow-orange discoloration of the skin; it is washable from skin but may stain clothing.79 Dapsone 7.5% gel has been FDA approved for the treatment of mild to moderate acne vulgaris as a single daily application since 2016.80
ADVERSE REACTIONS FROM DAPSONE (TABLE 187-3)
HEMATOLOGY
HEMATOLOGY
HEMOLYSIS
The commonest side effects of dapsone is doserelated hemolysis. Hemolysis may lead to hemolytic anemia and methemoglobinemia. About 20% of patients receiving dapsone treatment develop hemolysis.22 The side effect is more common and severe in those with G6PD deficiency. G6PD deficiency should be ruled out before initiating therapy in all patients.148
Hemolysis is more profound at the initiation of
Hematology
■Hemolysis
■Methemoglobinemia
Liver
■Toxic hepatitis
■Cholestatic jaundice
■Transaminitis
■Hypoalbuminemia
Skin
■Exfoliative dermatitis
■Erythema multiforme
■Urticaria
■Erythema nodosum
■Morbilliform exanthem
■Scarlatiniform exanthem
■Photosensitivity
Others
■Gastrointestinal upset (nausea)
■Headache
■Fatigue
■Insomnia
■Psychosis
■Peripheral neuropathy
■Motor neuropathy
Life-Threatening Side Effects
Life-Threatening Side Effects
■Dapsone hypersensitivity syndrome
■Dapsone hypersensitivity syndrome
■Hemolysis
■Hemolysis
■Methemoglobinemia
■Methemoglobinemia
■Agranulocytosis
■Agranulocytosis
■Aplastic anemia
■Aplastic anemia
■Hemophagocytic syndrome
■Hemophagocytic syndrome
■Toxic epidermal necrolysis, Stevens-Johnson syndrome194
■Toxic epidermal necrolysis, Stevens-Johnson syndrome194
aItalicized adverse effects are idiosyncratic and not dose dependent.
therapy and is often accompanied by a compensatory reticulocytosis. However, G6PD-deficient patients are less susceptible to methemoglobinemia production, but more susceptible to hemolysis.22 A case of hemolysis in a neonate from dapsone in breast milk has been reported.27,32
METHEMOGLOBINEMIA
Methemoglobinemia is a predictable consequence of dapsone therapy caused by dapsone hydroxylamine’s generation of reactive oxygen species (ROS).149-156
Methemoglobinemia usually occurs only with the intake of oral dapsone; however, a single case of methemoglobinemia has been reported in a patient using topical 5% dapsone.49 Methemoglobin is the form of hemoglobin in which the iron molecule is in the oxidized ferric (Fe3+) state rather than in the ferrous state (Fe2+). As such, the molecule itself is unable to carry oxygen or carbon dioxide.151 The signs and symptoms of methemoglobinemia are those of poor oxygenation, including cyanosis, headache, shortness of breath, chest pain, and fatigue. And although some degree of methemoglobinemia occurs in most
28
patients, symptomatic methemoglobinemia is rare. Symptoms usually occur with methemoglobin levels of 20% to 30%.155,156 Pulse oximetry is a reasonable screening test for methemoglobinemia because a normal value excludes significant methemoglobin levels. However, an abnormal value must be followed up with a direct methemoglobin determination.152-157
Cimetidine, which blocks the hydroxylation of dapsone, has been used intentionally to lower methemoglobin levels in dapsone-treated patients by 27% to 60%.60-63,158 Lipoic acid, a dietary supplement with antioxidant properties, has also been shown in vitro to decrease methemoglobin formation, and 90 mg/day of lipoic acid daily has been suggested for dapsonetreated patients.159
Although G6PD-deficient individuals are at greater risk for hemolytic anemia and methemoglobinemia, the clinician should remember that these events are also seen in patients without G6PD deficiency.160
LIVER
LIVER
Toxic hepatitis and cholestatic jaundice from dapsone have been reported. Hepatitis and jaundice may also occur as part of the dapsone hypersensitivity reaction or syndrome. Dapsone is metabolized by the cytochrome P450 system. Dapsone metabolites produced by the cytochrome P450 2C19 isozyme are associated with the methemoglobinemia side effect of the drug.
SKIN
SKIN
Various skin eruptions from dapsone have been described.161 They include exfoliative dermatitis, erythema multiforme, urticaria, erythema nodosum, morbilliform and scarlatiniform exanthema, and Stevens-Johnson syndrome or toxic epidermal necrolysis. Dapsone-induced photosensitivity is quite rare but usually not dose dependent. When used topically, dapsone can cause mild skin irritation, redness, dry skin, burning, and itching.
OTHER ADVERSE EFFECTS
OTHER ADVERSE EFFECTS
These include nausea, headache, fatigue, insomnia, psychosis, and peripheral neuropathy. Also reported are varied neurologic side effects, including a distal motor neuropathy, most often without a sensory component.162-164 These are usually reversible with dose decrease or discontinuation of dapsone. Checking a patient’s distal motor strength at follow-up visits may alert the clinician to such side effects. Effects on the lung occur rarely and may be serious, although they are generally reversible.165
3427
28
SERIOUS ADVERSE REACTIONS TO DAPSONE
DAPSONE HYPERSENSITIVITY SYNDROME
DAPSONE
HYPERSENSITIVITY
SYNDROME
Hypersensitivity reactions to dapsone occur in some patients. This reaction may be more frequent in patients receiving multiple-drug therapy.166-168 The reaction manifests with a rash and may also present with fever, jaundice, and eosinophilia.169-173 In general, these symptoms occur within the first 6 weeks of therapy and may be ameliorated by corticosteroid therapy. This reaction appears to be more frequent in patients receiving multiple-drug therapy.168 Latencies of the hypersensitivity syndrome after initiation of dapsone treatment were less than 20 days, 24.5%; 21 to 28 days, 35.0%; 29 to 35 days, 20.9%; and more than 36 days, 19.6%. Maximum latency was 20 weeks; 91% and 97% of patients presented with a rash and fever respectively, and 73.7% had lymphadenopathy. Hepatic dysfunction could be detected in the majority of cases, its severity ranging from abnormal liver test results over hepatosplenomegaly and jaundice to hepatic coma. About half of the patients demonstrated hematologic changes (leucocytosis in 56.6%, eosinophilia in 43.8%). After withdrawal of dapsone (and in most cases, steroid therapy), the majority of patients (82.3%) recovered, but nearly 10% had a fatal outcome, hepatic coma being the most frequent cause of death. Early discontinuation of dapsone was associated with a better prognosis.22,174 Corticosteroids have proved helpful, but dosages up to 1g/day of methylprednisolone for 3 days may be required followed by a prednisone taper over 4 to 6 weeks. Clinicians should be alert for rashes that present with fever and other systemic symptoms because these may be manifestations of the dapsone hypersensitivity syndrome.175-190 The incidence of this syndrome ranges from 0.2% to 5% of treated patients.175-178 It is similar to hypersensitivity syndrome seen with some anticonvulsants and other medications.179,180 These syndromes are postulated to be due to drug-allergy-induced immunosuppression53,54,178,179 leading to a reactivation of human herpesvirus 6 (HHV6) or other latent viruses such as cytomegalovirus and Epstein-Barr virus. They develop between 2 and 7 weeks after initiating the medication and inevitably include the triad of fever, rash, and hepatitis. The rash is most often an exfoliative dermatitis,180
but maculopapular and Stevens-Johnson–like lesions have occurred. It is the reactivation of HHV6 that is thought to cause the late flaring of rash, fever, and hepatitis characteristically seen in this class of drug reactions, necessitating such a long steroid taper.178 The hepatitis has a mixed hepatocellular and cholestatic picture with elevations in both transaminases181-186 and alkaline phosphatase.187 Additionally, any other endorgan damage must be managed supportively.175,176
3428
Plasma exchange has also been successfully used in a patient in whom tapering of steroids led to recrudescence of symptoms.190
HEMOLYSIS AND METHEMOGLOBINEMIA
HEMOLYSIS AND
METHEMOGLOBINEMIA
Dapsone therapy is often associated with hemolysis and sometimes methemoglobinemia in a dosedependent fashion.191 These adverse effects are caused by the hydroxylated metabolite, dapsone hydroxylamine, a potent oxidant.45,47,192-197 Within the erythrocytes, dapsone hydroxylamine generates ROS, which oxidize oxyhemoglobin into methemoglobin. Acute methemoglobinemia occurs rarely but may result in dyspnea, anemia, and vascular collapse; in serious cases, it may result in death. The oxidized hemoglobin becomes microscopically visible as Heinz bodies. These Heinz bodies and hydroxylated metabolite/cellular protein adducts may label the red blood cells (RBCs) as senescent, targeting them for removal by the spleen. Glutathione within the erythrocytes is responsible for reversing oxidative damage; however, production of glutathione depends on G6PD. Patients with G6PD deficiency are less tolerant of pharmacologic oxidative stress and are at risk for substantial hemolysis. There are two types of G6PD deficiency that are screened for with the same laboratory assay: “A-type” G6PD deficiency occurs in African Americans and is milder than the type seen in patients of Mediterranean heritage.198
G6PD deficiency should be ruled out before initiating dapsone therapy in all patients.148 Baseline anemias should be worked up before starting patients on dapsone. The frequency of symptomatic anemia is 10%,199
but it might be higher in certain populations such as solid organ allograft recipients (23%).200,201 This higher rate of hemolysis may be attributable to the greater frequency of renal insufficiency in this patient population or a potential interaction with medicines such as sirolimus. If dapsone therapy is efficacious but hemolysis is limiting therapy, coadministration of darbepoetin may allow continuation of drug at therapeutic doses.202,203
AGRANULOCYTOSIS
AGRANULOCYTOSIS
Agranulocytosis is another rare, idiosyncratic side effect and has been estimated to occur in 0.2% to 0.4% of treated patients.148,159,191,204-209 It usually occurs during the first 3 months of therapy. Although usually reversible within days when patients stop therapy, it may be fatal because of superseding infection. Symptoms of agranulocytosis include fever, pharyngitis, dysphagia, and oral ulcerations.148,191 Patients should be warned to seek medical care immediately if these symptoms develop. Recombinant granulocyte colony-stimulating factor has been used to produce a more rapid resolution of agranulocytosis.210
APLASTIC ANEMIA
APLASTIC ANEMIA
Individual case reports of other hematologic sequelae of dapsone include two cases of pure RBC aplasia211 and a single case of hemophagocytic syndrome induced by dapsone.212 Abnormalities in white blood cell formation, including aplastic anemia, are rare yet are the cause of the majority of deaths attributable to dapsone therapy.213-215
INITIATING AND MONITORING OF DAPSONE THERAPY
Before starting patients on dapsone, a targeted history and physical examination to screen for significant preexisting anaemia, cardiopulmonary disease, and peripheral neuropathy should be performed. Laboratory tests (Table 187-4) should include a complete blood cell count and reticulocytes counts to determine baseline white blood cell count, hemoglobin, and reticulocytes. G6PD deficiency should be ruled out, as should significant hepatic or renal dysfunction. After therapy has begun, a white blood cell count with differential and hemoglobin levels and reticulocytes count should be obtained weekly for the first month and then twice a month during the next 2 months.148,191 A drop in hemoglobin of 1 to 2 g/dL should be anticipated and, in the absence of symptoms, should not prompt drug discontinuation. Monitoring reticulocyte counts also provide an estimation of the adequacy of compensation for hemolysis. A profoundly elevated reticulocyte count suggests that erythropoiesis is at its maximum and that further dose increases are not likely to be well tolerated. Even during long-term therapy, complete blood cell counts should be obtained periodically. Checking methemoglobin levels is unnecessary in the absence of symptoms. Patients should also be told to carry a medication card so that in an emergency, treating physicians will know they are taking a drug with hemolytic and methemoglobin-generating potential. It is important
Before Initiation of Therapy
■Glucose-6-phosphate dehydrogenase
■CBC
■Reticulocyte count
■Hepatic function tests
■Renal function tests
During Therapy
During Therapy
■CBC (with WBC differential) weekly for the first month and twice a month for the next 2 months; periodically thereafter
■CBC (with WBC differential) weekly for the first month and twice a
month for the next 2 months; periodically thereafter
■Reticulocyte count weekly for the first month and twice a month for the next 2 months; periodically thereafter
■Reticulocyte count weekly for the first month and twice a month
for the next 2 months; periodically thereafter
CBC, complete blood count; G6PD, glucose-6-phosphate dehydrogenase; WBC, white blood cell.
28
that all patients be made aware of the potential clinical manifestations of adverse events. Especially during the first 3 months of therapy when the risk of agranulocytosis and the dapsone hypersensitivity syndrome is highest, patients should be reminded to seek medical attention immediately for significant fever, pharyngitis, dysphagia, swollen lymph nodes, oral ulcerations, and rash.148,191 Patients with diabetes should also be made aware that dapsone causes falsely low hemoglobin A1c values because of the accelerated RBC turnover; monitoring fructosamine levels avoids this potential confounder.216 It might be suggested to patients who have mild symptoms of anemia or methemoglobinemia to take cimetidine 400 mg three times daily and lipoic acid 90 mg/day to see if these might ameliorate symptoms enough for dapsone administration to continue.60-63,169
Dapsone is contraindicated in patients who are allergic to the drug. It should not be administered to patients with severe anaemia. Dapsone must be used with caution in the following conditions: G6PD deficiency, methemoglobinemia reductase deficiency, severe hepatopathy, cardiac insufficiency or heart failure, and pulmonary diseases as well as comedication with methemoglobinemia-inducing drugs or compounds.
TREATING OVERDOSE
In the case of accidental or intentional dapsone overdose, the clinician should be prepared for significant hemolysis (which may be delayed by up to 9 days because of enterohepatic recirculation) and methemoglobinemia.217-219 Massive intravascular hemolysis seen in dapsone overdose has been linked to optic ischemic injury.220-222 Although dapsone is 50% to 80% protein bound in the circulation, the unbound portion can be dialyzed off, and repeated dialysis has been helpful in the case of overdose.223 Because of dapsone’s enterohepatic recirculation, administration of activated charcoal will reduce drug levels by removing drug from the gut. Methylene blue, 1% solution given 1 to 2 mg/kg slowly intravenously,224,225 can be used to decrease the degree of methemoglobinemia. Methylene blue is a cofactor for methemoglobin reductase after first being reduced by cellular stores of NADPH (nicotinamide adenine dinucleotide phosphate hydrogen) to leukomethylene blue. G6PD-deficient patients should not be given methylene blue because they may have insufficient NADPH, and unreduced methylene blue is its own direct hemolytic agent. Ascorbic acid 1000 mg intravenously every 12 hours has also been used in a case of overdose and certainly could be used until G6PD status is reviewed so that methylene blue can be administered. Ascorbic acid’s effect is caused by its ability to increase methemoglobin reductase activity.218
ACKNOWLEDGMENTS
We acknowledge Joni G. Sago and Russell P. Hall III, who wrote the previous version of this chapter. The new version is adapted from the previous version.
3429
28
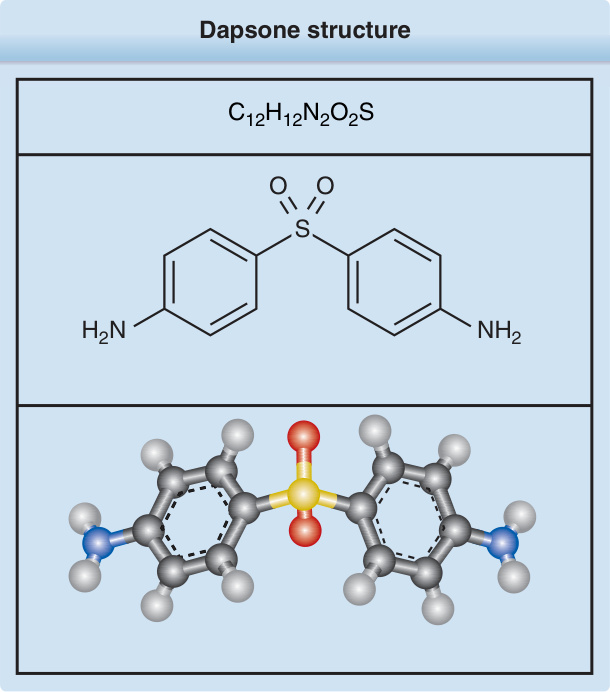
Figure 187-1 Dapsone structure.
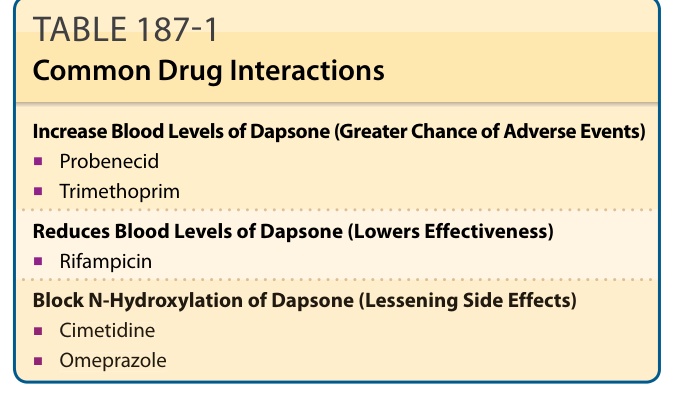
TABLE 187-1 Common Drug Interactions
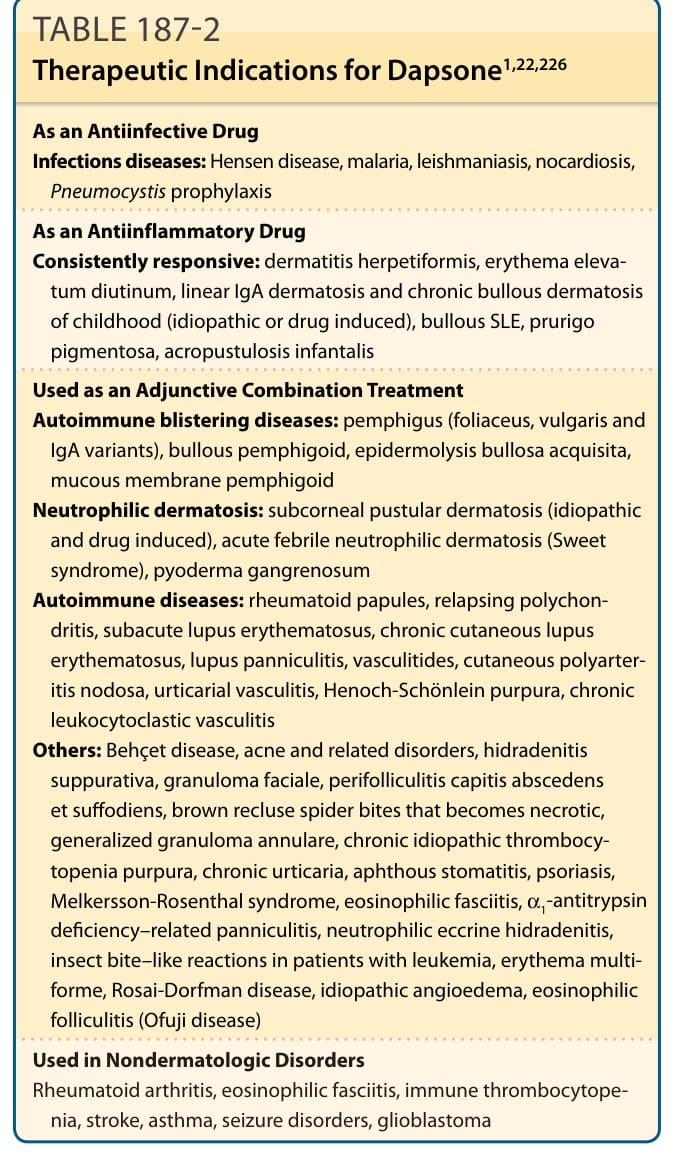
TABLE 187-2 Therapeutic Indications for Dapsone1,22,226
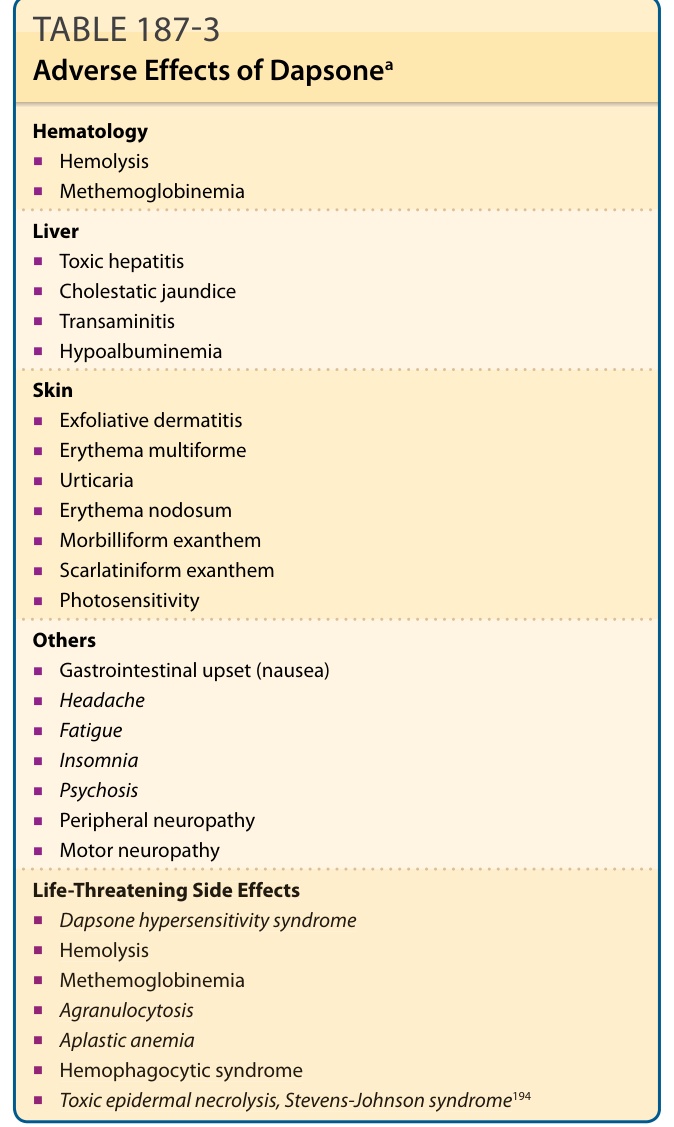
TABLE 187-3 Adverse Effects of Dapsonea
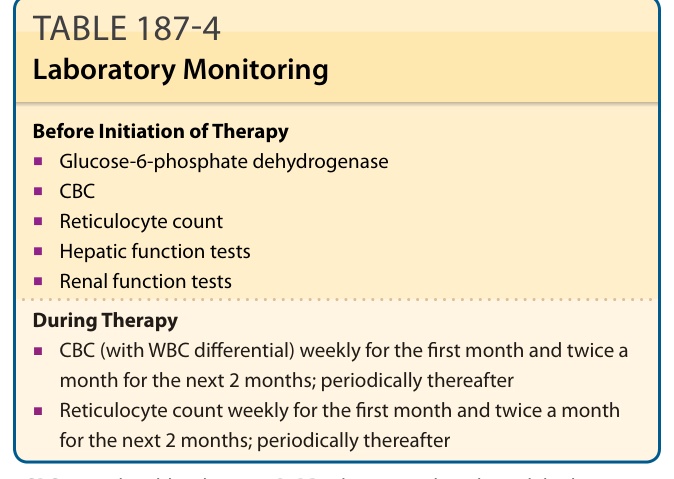
TABLE 187-4 Laboratory Monitoring