Glucocorticoids
28
SYSTEMIC GLUCOCORTICOIDS
AT-A-GLANCE
■ Systemic glucocorticoids are potent immunosuppressive and antiinflammatory agents that are frequently used for severe dermatologic diseases.
■ Complications are increased with fluorinated compounds, higher doses, longer duration of therapy, and more frequent administration.
■ Intralesional, IM, IV, topical, and oral routes of administration can be used.
■ Careful monitoring of systemic and cutaneous side effects is an essential component of therapy.
■ Glucocorticoid-induced osteoporosis begins early in treatment and should be aggressively managed in all patients on long-term therapy.
Glucocorticoids are a mainstay of dermatologic therapy because of their potent immunosuppressive and antiinflammatory properties. By understanding the properties and mechanisms of action of glucocorticoids, one can maximize their efficacy and safety as therapeutic agents.
PHARMACOLOGY AND MECHANISM OF ACTION
PHARMACOLOGY AND
MECHANISM OF ACTION
The major naturally occurring glucocorticoid is cortisol (hydrocortisone). It is synthesized from cholesterol by the adrenal cortex. Normally, less than 5% of circulating cortisol is unbound; this free cortisol is the active therapeutic molecule. The remainder is inactive because it is bound to cortisol-binding globulin (also called transcortin) or to albumin. Daily cortisol production is 5 to 7 mg/m2, with a diurnal peak around 8:00 am.1 Cortisol has a plasma half-life of 90 minutes. It is metabolized primarily by the liver, although it exerts hormonal effects on virtually every tissue in the body. The metabolites are excreted by the kidney and the liver. The mechanism of glucocorticoid action involves passive diffusion of the glucocorticoids through the cell membrane, followed by binding to soluble receptor proteins in the cytoplasm.2 This hormone-receptor
complex then moves to the nucleus and regulates the transcription of a limited number of target genes. There are 3 main mechanisms of glucocorticoid action. The first is direct effects on gene expression by the binding of glucocorticoid receptors to glucocorticoidresponsive elements, leading to the induction of proteins like annexin I and MAPK (mitogen-activated protein kinase) phosphatase 1. Annexins reduce phospholipase A2 activity, which reduces the release of arachidonic acid from membrane phospholipids, limiting the formation of prostaglandins and leukotrienes.3-5
The second mechanism is indirect effects on gene expression through the interactions of glucocorticoid receptors with other transcription factors. For example, inhibitory effects on AP-1 and nuclear factor κB, coupled with increased inhibitor of nuclear factor κB (IκB), decreases the synthesis of a number of proinflammatory molecules, including cytokines, interleukins, adhesion molecules, and proteases.6 The third is glucocorticoid receptor–mediated effects on second messenger cascades through nongenomic pathways such as the phosphatidylinositol 3′-kinase (PI3K)-Aktendothelial nitric oxide synthase (eNOS) pathway.7,8
There is usually a delay in the onset of pharmacologic activity of glucocorticoids relative to their peak blood concentrations, which is probably consequent to altering the transcription of genes,7 although some actions appear to be independent of transcription. Some effects of glucocorticoids are too rapid to be mediated by genomic glucocorticoid action,9 which might explain the additive benefits of very-high-pulse glucocorticoids.
CELLULAR EFFECTS OF CORTICOSTEROIDS
Glucocorticoids profoundly affect the replication and movement of cells. They induce monocytopenia, eosinopenia, and lymphocytopenia, and have a greater effect on T cells than on B cells.10 The lymphocytopenia appears to be caused by a redistribution of cells as they migrate from the circulation to other lymphoid tissues. The increase in circulating polymorphonuclear leukocytes is related to demargination of cells from the bone marrow and a diminished rate of removal from the circulation, at least partially mediated by the increase in annexin 111; there also appears to be inhibition of neutrophil apoptosis.12
Glucocorticoids affect cell activation, proliferation, and differentiation. They modulate the levels of mediators of inflammation and immune reactions, as seen with the inhibition of cytokines and tumor
necrosis factor synthesis or release.13,14 Additionally, macrophage functions, including phagocytosis, antigen processing, and cell killing, are decreased by cortisol, and this decrease affects immediate and delayed hypersensitivity.15,16
Glucocorticoids suppress monocyte and lymphocyte function (both Th1 and Th2 cells) more than polymorphonuclear leukocyte function.17 This effect is clinically important because granulomatous infectious diseases, such as tuberculosis, are prone to exacerbation and relapse during prolonged glucocorticoid therapy. The antibody-forming cells, B lymphocytes and plasma cells, are relatively resistant to the suppressive effects of glucocorticoids.
INDICATIONS
INDICATIONS
There is a long list of indications for skin disorders (Table 184-1). In addition, short courses of glucocorticoids may be used for a variety of forms of severe dermatitis, including contact dermatitis, atopic dermatitis, photodermatitis, exfoliative dermatitis, and erythrodermas. The use of glucocorticoids is controversial in the treatment of erythema nodosum, lichen planus, cutaneous T-cell lymphoma, and discoid lupus erythematosus.
DOSING REGIMEN
DOSING REGIMEN
Systemic glucocorticoids can be administered intralesionally, orally, intramuscularly, and intravenously. The route and regimen are determined by the nature and extent of the disease being treated. Intralesional glucocorticoid administration allows direct access to either a relatively few lesions or a particularly resistant lesion. The concentration depends on the site of injection and the nature of the lesion. Lower concentrations are used on the face to prevent atrophy of the skin. In conditions requiring sustained
■Serious blistering diseases (pemphigus, bullous pemphigoid, cicatricial pemphigoid, linear immunoglobulin A bullous dermatoses, epidermolysis bullosa acquisita, herpes gestationis, erythema multiforme, toxic epidermal necrolysis)
■Serious blistering diseases (pemphigus, bullous pemphigoid,
cicatricial pemphigoid, linear immunoglobulin A bullous dermatoses, epidermolysis bullosa acquisita, herpes gestationis, erythema multiforme, toxic epidermal necrolysis)
■Connective tissue diseases (dermatomyositis, systemic lupus erythematosus, mixed connective tissue disease, eosinophilic fasciitis, relapsing polychondritis)
■Connective tissue diseases (dermatomyositis, systemic lupus
erythematosus, mixed connective tissue disease, eosinophilic fasciitis, relapsing polychondritis)
■Vasculitis
■Vasculitis
■Neutrophilic dermatoses (pyoderma gangrenosum, acute febrile neutrophilic dermatosis, Behçet disease)
■Neutrophilic dermatoses (pyoderma gangrenosum, acute febrile
neutrophilic dermatosis, Behçet disease)
■Sarcoidosis
■Sarcoidosis
■Type I reactive leprosy
■Type I reactive leprosy
■Hemangioma of infancy
■Hemangioma of infancy
■Panniculitis
■Panniculitis
■Urticaria/angioedema
■Urticaria/angioedema
28
effects, such as keloids and alopecia areata, longeracting glucocorticoids, such as triamcinolone diacetate (Aristospan), can be administered alone or mixed with the more typically used triamcinolone acetonide (Kenalog). It is best to limit the total monthly dose of Kenalog to 20 mg to ensure that the hypothalamic– pituitary–adrenal (HPA) axis will not be suppressed.18
IM administration of glucocorticoids is associated with variable benefits and challenges. Although IM administration removes concerns for compliance and is not affected by nausea, vomiting, or inability to achieve intravenous access, potential drawbacks include erratic absorption and lack of daily control of the dose. Furthermore, IM injections may result in lipoatrophy or sterile abscesses.19 Long-acting formulations such as triamcinolone acetonide have increased side effects over short-acting formulations, including increased potential of HPA axis suppression. Because this medication produces effects lasting up to 3 weeks, IM administration of triamcinolone acetonide should not be given more than a few times per year to avoid adrenal suppression.19
Intravenous glucocorticoids are used in 2 situations: The first is to provide stress coverage for patients who are acutely ill or are undergoing surgery (see below in section on Adrenal Suppression for discussion on glucocorticoids and surgery) and who have adrenal suppression from daily glucocorticoid therapy. The second is for patients with certain diseases—such as resistant pyoderma gangrenosum, severe pemphigus or bullous pemphigoid, serious systemic lupus erythematosus, or dermatomyositis—so as to gain rapid control of the disease and minimize the need for longterm, high-dose, oral steroid therapy.20 Methylprednisolone is used at a dose of 500 mg to 1 g daily because of its high potency and low sodium-retaining activity. Serious side effects associated with IV administration include anaphylactic reactions, seizures, arrhythmias, and sudden death. Other, less serious adverse reactions include hypotension, hypertension, hyperglycemia, electrolyte shifts, and acute psychosis. Slower administration over 2 to 3 hours minimizes many of the serious side effects. Patients without underlying renal or cardiac disease do not need to be treated in a monitored bed, although vital signs should be monitored regularly during administration.19 It is important to monitor serum electrolytes before and after pulse therapy, particularly when patients are on concomitant diuretic therapy. Prednisone is the most commonly prescribed oral glucocorticoid. The initial dose is most often daily to control the disease process and can range from 2.5 mg to several hundred milligrams daily.
INITIATING THERAPY
INITIATING THERAPY
FUNDAMENTAL PRINCIPLES
Before therapy with glucocorticoids is begun, the benefit that can realistically be expected should be weighed
3383
28
EQUIVALENT DOSE (mg) GLUCOCORTICOID POTENCY HPA SUPPRESSION MINERALOCORTICOID POTENCY PLASMA HALF-LIFE (min) BIOLOGIC HALF-LIFE (h)
Short-acting Glucocorticoids
Cortisol 20 1.0 1.0 1.0 90 8-12
Cortisone 25 0.8
0.8 80-118 8-12
Intermediate-acting Glucocorticoids
Prednisone 5 4.0 4.0 0.3 60 18-36
Prednisolone 5 5.0
0.3 115-200 18-36
Triamcinolone 4 5.0 4.0 0 30 18-36
Methylprednisolone 4 5.0 4.0 0 180 18-36
Long-acting Glucocorticoids
Dexamethasone 0.75 30 17 0 200 36-54
Betamethasone 0.6 25-40
0 300 36-54
Mineralocorticoids
Fludrocortisone 2 10 12.0 250 200 18-36
Desoxycorticosterone
0 20 70
Desoxycorticosterone acetate
0
20 70
acetate
HPA, hypothalamic–pituitary–adrenal axis. From Chrousos G, Pavlaki AN, Magiakou MA. Glucocorticoid therapy and adrenal suppression. [Updated January 11, 2011.] In: De Groot LJ, Chrousos G, Dungan K, et al., eds. Endotext [Internet]. South Dartmouth, MA: MDText.com, Inc; 2000. https://www.ncbi.nlm.nih.gov/books/NBK279156/, with permission. Copyright © 2000-2018, MDText.com, Inc.
against the potential side effects. Alternative or adjunctive therapies should be considered, especially if longterm treatment is contemplated. Coexisting illnesses such as diabetes, hypertension, and osteoporosis need to be considered. The predisposition of the patient to side effects should be included in an assessment of risk.
CHOOSING AMONG GLUCOCORTICOIDS
A number of considerations bear on the choice of glucocorticoids (Table 184-2). First, a preparation with minimal mineralocorticoid effect is usually picked to decrease sodium retention. Second, the long-term oral use of prednisone or a similar drug, with an intermediate half-life and relatively weak steroid-receptor affinity, may reduce side effects. Long-term use of drugs like dexamethasone, which has a longer half-life and high glucocorticoid-receptor affinity, may produce more side effects without additional therapeutic effects. Third, if a patient does not respond to cortisone or prednisone, the substitution of the biologically active form, cortisol or prednisolone, should be considered. However, even in severe liver disease, substitution has not proved to be very important.
EVALUATION BEFORE TREATMENT
To minimize potential problems, the baseline evaluation should include a personal and family history, with
3384
special attention to predisposition to diabetes, hypertension, hyperlipidemia, glaucoma, and associated diseases that could be affected by steroid therapy. Sideeffect-specific evaluation and monitoring recommendations during glucocorticoid therapy are discussed below in the section “Adverse Effects”.
SIDE EFFECTS AND PRECAUTIONS
SIDE EFFECTS AND
PRECAUTIONS
DIET
Diet should be low in calories, fat, and sodium, and high in protein, potassium, and calcium as tolerated, also considering any associated comorbidities. Protein intake is important to reduce steroid-induced nitrogen wasting.21 Use of alcohol, coffee, and nicotine should be minimized. Exercise should be encouraged.
INFECTIONS
Glucocorticoid therapy increases the risk to patients for common and uncommon infections.22 All patients anticipated to be on glucocorticoid doses of 15 mg or greater for 1 month or longer should be screened for tuberculosis with either a tuberculin
SIDE EFFECT PREVENTIVE MEASURES
Hypertension Blood pressure (baseline; repeat with each visit)
Weight gain Weight (baseline; repeat with each visit)
Reactivation of infection Purified protein derivative or interferon-gamma release assay; hepatitis screen; consider Pneumocystis jiroveci pneumonia prophylaxis
Metabolic abnormalities Electrolytes, lipids, glucose (baseline; repeat early after starting therapy; repeat annually; more frequent monitoring with known factors [eg, diabetes, hyperlipidemia])
Osteoporosis Bone density (baseline; repeat annually); instruct about diet, exercise; initiate calcium and vitamin D supplementation; start bisphosphonate for men, postmenopausal women based on bone mineral density evaluation
Eyes Refer for ophthalmologic evaluation and consider more frequent screening if history of cataracts or glaucoma
Peptic ulcer In patients on concomitant nonsteroidal antiinflammatory drugs, initiate prophylaxis with a proton pump inhibitor; with 2 or more risk factors, consider prophylaxis with proton pump inhibitor
Suppression of
Single, early morning doses, preferably every
Suppression of hypothalamic– pituitary– adrenal axis
Single, early morning doses, preferably every other day
hypothalamic– pituitary– adrenal axis
other day
skin test by injecting a purified protein derivative or an interferon-gamma release assay (QuantiFERON- TB Gold In-Tube Test or T-SPOT.TB). Patients with a positive screening test should have chest radiography to evaluate for active tuberculosis. Patients with a negative chest radiograph require treatment for latent tuberculosis. Anergic patients should have a baseline chest radiograph to search for evidence of previous tuberculosis. Of note, glucocorticoids downregulate delayed-type hypersensitivity and may suppress the purified protein derivative response. A positive purified protein derivative in this population is considered 5 mm or more of induration. Attention must also be paid to patients on high doses of glucocorticoids with underlying lung disease, low lymphocyte counts, underlying conditions further contributing to immunosuppression, and/or patients on concomitant cytotoxic therapies, as these patients are at increased risk for development of Pneumocystis pneumonia. Some advocate use of trimethoprim-sulfamethoxazole prophylaxis against Pneumocystis jiroveci for high-risk patients who are on high doses of glucocorticoids. Examination for other covert infections should be based on history and physical examination. For instance, a stool culture for Strongyloides should be performed for those who have lived in tropical countries and for Vietnam veterans.23
28
IMMUNIZATIONS
Immunization with live vaccines can be done if the duration of glucocorticoid use is less than 2 weeks at any dose, if the dose of glucocorticoid is less than 20 mg/day of any duration or less than 2 mg/kg in patients who weigh less than 10 kg, and if long-term alternate-day treatment with short-acting preparations is used. Immunization with live vaccines should not be done for at least 1 month after receiving high doses of glucocorticoids (>20 mg/day) for more than 2 weeks.24
ADRENAL SUPPRESSION
Patients receiving daily glucocorticoid therapy for longer than 3 to 4 weeks must be assumed to have adrenal suppression that requires tapering of the glucocorticoids to allow for recovery of the HPA axis. Prescribers may choose from among a variety of tapering algorithms and may choose to test the HPA axis to guide the need for short-term maintenance therapy at the low end of the taper. If a prescriber chooses to test the HPA axis, it should be done with an 8 am cortisol (to time the test when physiologic cortisol production peaks) prior to taking the daily steroid dose and after tapering that daily dose to a dose less than or equal to the daily physiologic cortisol level (<5 mg prednisone/day; or 15 to 20 mg hydrocortisone/day). If the 8 am plasma cortisol levels are 5 µg/dL or less, then continued glucocorticoid therapy and rechecking of the serum cortisol every 3 to 6 months until levels are higher than 10 µg/dL is required. If levels are 5 µg/dL or higher but 20 µg/dL or less, prescribers may choose to perform further testing, such as a corticotropin-releasing hormone stimulation test; it is reasonable, however, to continue maintenance therapy with a very gradual taper.25 At any point during tapering or within a year of stopping glucocorticoids, a stress caused, for example, by trauma, surgery, diarrhea, or fever can precipitate adrenal insufficiency related to an inadequate stress response. During such situations, it may be necessary to give higher doses of glucocorticoids in divided doses. Patients must be educated about the need for stress coverage and should wear bracelets or carry cards indicating that they are receiving glucocorticoids. Most patients can be maintained on their regular dose of glucocorticoids in preparation for surgery. Prior guidelines for preoperative and perioperative management were based on cortisol response to severity of surgery.26 However, expert opinion demonstrates a shifting paradigm.27,28 Consideration may be given to high-dose glucocorticoids (50 mg hydrocortisone every 8 hours until tolerating oral intake) for patients undergoing major surgical procedures or patients with primary adrenal failure, congenital adrenal hyperplasia, or hypopituitarism.28 Few randomized controlled trials have been done, and data is sparse. Clinicians must remain vigilant for intraoperative hypotension or
3385
28
other signs of adrenal insufficiency for at-risk patients undergoing surgical procedures and treat appropriately if acute adrenal insufficiency is the etiology.
ADVERSE EFFECTS
ADVERSE EFFECTS
Complications associated with systemic glucocorticoid therapy (Table 184-4) increase with higher doses, longer duration of therapy, and more frequent administration.19,29 However, osteoporosis and
Bone health
■Avascular necrosis of bone
■Osteoporosis
Cardiovascular
■Atherosclerosis
■Dislipidemia
■Hypertension
■Sodium and fluid retention
Cutaneous
■Fibroblast inhibition
■Inhibition of wound healing
■Subcutaneous tissue atrophy (striae, purpura, ecchymoses)
Endocrine/Metabolic
■Alterations of fat distribution (typical cushingoid appearance)
■Fatty infiltration of the liver
■Growth failure
■Hyperglycemia and unmasking genetic predisposition to diabetes mellitus
■Secondary amenorrhea
■Suppression of hypothalamic–pituitary–adrenal axis
Gastrointestinal
■GI bleeding
■Intestinal perforation
■Pancreatitis
■Peptic ulcer
Immunity
■Effects on phagocyte kinetics and function
■Immunosuppression, anergy
■Increased incidence of infections
■Suppression of host defenses
Miscellaneous
■Anaphylaxis
■Drug interactions (for example, increased INR on patients on both prednisone and coumadin)
■Hypersensitivity reactions
■Myopathy
■Urticaria
Ophthalmologic
■Cataracts
■Glaucoma
Psychiatric/Mood disturbances
Psychiatric/Mood disturbances
■Depression, mania
■Depression, mania
■Sleep disturbances
■Sleep disturbances
3386
■Thoughts of self-harm
■Thoughts of self-harm
cataracts develop with alternate-day dosing, and avascular necrosis (AVN) can be seen after only short courses of glucocorticoids.
OSTEOPOROSIS
Osteoporosis occurs in 40% of individuals treated long-term with systemic glucocorticoids.30,31 Bone loss occurs most rapidly in the first few months of glucocorticoid use, but continues at a slower rate after that.30,32 Even low doses of prednisone (2.5 mg per day) adversely affect bone and increase vertebral and hip fractures.33
Glucocorticoids have both direct and indirect effects on bone. They decrease bone formation and increase resorption by inhibiting osteoblasts and increasing activity of osteoclasts.30 Indirectly, glucocorticoids increase calcium excretion by the kidney, decrease intestinal calcium absorption, and reduce estrogen and testosterone levels. Any patient anticipated to be on glucocorticoid therapy for 3 months or longer should receive calcium 1200 mg/day and vitamin D 800 International Units/day through diet and supplement.34 Patients with comorbidities, such as patients with sarcoidosis or renal stones, may require close monitoring or adjustment of this recommendation. Clinicians may consider checking vitamin D levels and repleting prior to initiating maintenance therapy. Patients anticipated to be on prednisone 5 mg or more per day for 3 months or longer and all patients considered at high risk for osteoporosis should be evaluated with dual-energy x-ray absorptiometry or by the World Health Organization (WHO)’s fracture risk assessment tool, the FRAX equation (http://www.shef.ac.uk/FRAX/), for consideration of initiation of bisphosphonates. Rare side effects of bisphosphonates include osteonecrosis of the jaw and atypical femoral fractures. Additionally, bisphosphonates are contraindicated in patients with creatinine clearance below 30 mL/min. Oral bisphosphonates are contraindicated for patients who cannot sit upright for 30 minutes after swallowing a pill and for patients with esophageal disorders that impact swallowing, such as achalasia, strictures, reflux, or varices. Initiating bisphosphonates in women of childbearing potential should be considered case-by-case. In general, these women should avoid bisphosphonates in the absence of fragility fractures or ongoing bone loss.35 Long-term use of glucocorticoids and/or highrisk patients may be evaluated for initiation of teriparatide. Secondary causes for osteoporosis should be considered and evaluated in all patients.
AVASCULAR NECROSIS
AVN is manifest by pain and limitation of motion in one or more joints. Various mechanisms have been postulated to explain AVN. Early detection is important because early intervention may prevent progression to degenerative joint disease requiring
joint replacement. Patients should be regularly questioned about pain and limitation of motion of joints. If abnormalities develop, a radiograph, bone scan, or MRI should be ordered. Because radiographs can be normal in AVN, if suspicion for this side effect is high, clinicians should consider evaluation by MRI. If multiple joints may be involved, then a bone scan may be needed. If imaging shows AVN, an orthopedic surgeon skilled in early intervention with core decompression may be able to halt progression of the disease.
CARDIOVASCULAR DISEASE
Glucocorticoid use is associated with an increased risk for ischemic heart disease and heart failure,36,37
although these risks appear to be greatest in patients with iatrogenic Cushing syndrome.38,39 Various mechanisms may contribute to this increased risk for cardiovascular events among patients with hypercortisolism, including hypercortisolisminduced hypertension, increased atherosclerosis, structural changes such as ventricular hypertrophy and myocardial fibrosis, and electrocardiographic changes. However, data is limited. Many studies excluded patients with iatrogenic Cushing syndrome, and comorbidities such as glucose intolerance, weight gain, and dyslipidemia may have resulted in confounding of study results.40-43
Increased cardiovascular risk may persist for years after normalization of the serum cortisol level in Cushing disease.44,45 Although studies primarily address Cushing disease, it is prudent to remain aware of this increased risk for patients on glucocorticoids or with iatrogenic Cushing syndrome, as metabolic syndrome may persist after removal of glucocorticoids contributing to ongoing risk for cardiovascular disease. Cardiovascular risk factors should be aggressively managed. Blood pressure, diet, serum lipids, and glucose levels should be measured serially. Abnormalities should be treated with dietary manipulation and medication as necessary and according to current guidelines.
GASTROINTESTINAL COMPLICATIONS
There is a significantly increased risk for peptic ulcer disease and GI bleeding in patients taking both glucocorticoids and nonsteroidal antiinflammatory agents, although it is unclear whether glucocorticoids independently increase this risk.46-48 In patients on combined therapy with a nonsteroidal antiinflammatory agent and glucocorticoid, prophylaxis with a proton pump inhibitor should be initiated. Prophylaxis should be highly considered in patients with 2 or more risk factors (such as those with a previous history of peptic ulceration or advanced malignant disease).
28
SUPPRESSION OF THE HYPOTHALAMIC–PITUITARY– ADRENAL AXIS AND THE STEROID WITHDRAWAL SYNDROME
The HPA axis is rapidly suppressed after the onset of glucocorticoid therapy. However, if therapy is limited to 1 to 3 weeks, the recovery of the HPA axis is rapid. As noted above, longer daily glucocorticoid therapy is associated with suppression of the HPA axis. Symptoms of adrenal insufficiency include lethargy, weakness, nausea, anorexia, fever, orthostatic hypotension, hypoglycemia, and weight loss. There also exists a steroid withdrawal syndrome, in which patients experience symptoms of adrenal insufficiency despite having an apparently normal cortisol response to adrenocorticotropic hormone. Symptoms most commonly include anorexia, lethargy, malaise, nausea, weight loss, desquamation of the skin, headache, and fever. Less commonly, vomiting, myalgia, and arthralgia occur.49 These patients have adjusted to high levels of glucocorticoids, and symptoms disappear after the glucocorticoids are restarted. This problem can be treated by slower tapering of the glucocorticoids or by temporarily increasing the dose.25,49
PSYCHIATRIC EFFECTS
Mood and cognitive changes are dose dependent and can appear shortly after the start of glucocorticoids. Age and gender appear to be risk factors for specific side effects. Women may be more likely to develop depression, whereas men may be more likely to develop mania.50 The risk of depression, mania, delirium, confusion, and disorientation increases with age, but the opposite is true of suicidal behavior and panic disorder. The incidence of neuropsychiatric events is highest in the first 3 months of therapy. Prednisone doses greater than 80 mg/day place patients at increased risk for steroid psychosis.50
CONCERNS DURING LACTATION AND PREGNANCY
Glucocorticoids cross the placenta, but they are not teratogenic. Even though glucocorticoids are secreted into breastmilk, no adverse effect has been reported among breastfed infants of mothers taking glucocorticoids. Prednisolone instead of prednisone and avoiding breastfeeding for 4 hours after a dose may decrease the amount of drug transferred during breastfeeding.51
ISSUES SPECIFIC TO PEDIATRICS
In the pediatric population, glucocorticoids cause growth suppression and early osteoporosis.52
Glucocorticoids inhibit bone formation, affect calcium and phosphorus metabolism, and interfere with growth hormone via affects on growth hormone secretion, growth hormone receptor expression and signal
3387
28
transduction from growth hormone to target tissuess.52
These effects can be reversed by treatment with growth hormone. Osteoporosis can reverse after glucocorticosteroids are stopped.
TOPICAL GLUCOCORTICOIDS
AT-A-GLANCE
■ Topical glucocorticoids are the most frequently prescribed of all dermatologic drug products.
■ They are effective at reducing the symptoms of inflammation, but do not address the underlying cause of the disease.
■ Topical glucocorticoid research has focused on strategies to optimize potency while minimizing side effects.
■ As with systemic glucocorticoids, careful monitoring of side effects is an essential component of therapy.
MECHANISM OF ACTION
MECHANISM OF ACTION
The mechanism of action, antiinflammatory effects, and immunosuppressive effects are as described in “Systemic Glucocorticoids” above. Topical steroids are also notable for their antiproliferative effect and their vasoconstrictive effect on dermal capillaries.
ANTIPROLIFERATIVE EFFECTS
This effect of topical corticosteroids is mediated by inhibition of DNA synthesis and mitosis, partly explaining the therapeutic action of these drugs in scaling dermatoses.53 They are known to reduce the keratinocyte size and proliferation. Fibroblast activity and collagen formation are also inhibited by topical corticosteroids.54
VASOCONSTRICTION
Topical steroids cause capillaries in the superficial dermis to constrict, thus reducing erythema. The mechanism by which corticosteroids induce vasoconstriction is not yet completely clear. It is thought to be related to inhibition of natural vasodilators such as histamine, bradykinins, and prostaglandins, and possibly via augmentation of vascular tone.55-58 Vasoconstriction assays are used to predict the clinical activity of an agent. These assays have been used to separate the topical corticosteroids into 7 classes based on potency according to the United States’ classification system and 4 classes according to the United Kingdom and France’s classification systems. In the U.S. system,
3388
Class 1 includes the most potent, while Class 7 contains the least potent topical corticosteroids. Table 184-5 lists many of the available topical corticosteroids according to this classification.
Class 1—Superpotent
■Betamethasone dipropionate 0.05% optimized vehicle
■Clobetasol propionate 0.05%
■Diflorasone diacetate 0.05%
■Fluocinonide 0.1% optimized vehicle
■Flurandrenolide 4 µg/cm2
■Halobetasol propionate 0.05%
Class 2—Potent
■Amcinonide 0.1%
■Betamethasone dipropionate 0.05%
■Desoximetasone 0.25%
■Desoximetasone 0.05%
■Diflorasone diacetate 0.05%
■Fluocinonide 0.05%
■Halcinonide 0.1%
■Mometasone furoate 0.1%
Class 3—Potent, Upper Midstrength
■Amcinonide 0.1%
■Betamethasone dipropionate 0.05%
■Betamethasone valerate 0.1%
■Diflorasone diacetate 0.05%
■Fluocinonide 0.05%
■Fluticasone propionate 0.005%
■Triamcinolone acetonide 0.5%
Class 4—Midstrength
■Betamethasone valerate 0.12%
■Clocortolone pivalate 0.1%
■Desoximetasone 0.05%
■Fluocinolone acetonide 0.025%
■Flurandrenolide 0.05%
■Hydrocortisone probutate 0.1%
■Hydrocortisone valerate 0.2%
■Mometasone furoate 0.1%
■Prednicarbate 0.1%
■Triamcinolone acetonide 0.1%
Class 5—Lower Midstrength
■Betamethasone dipropionate 0.05%
■Betamethasone valerate 0.1%
■Fluocinolone acetonide 0.025%
■Fluocinolone acetonide 0.01%
■Flurandrenolide 0.05%
■Fluticasone propionate 0.05%
■Hydrocortisone butyrate 0.1%
■Hydrocortisone valerate 0.2%
■Prednicarbate 0.1%
■Triamcinolone acetonide 0.1%
■Triamcinolone acetonide 0.025%
Class 6—Mild Strength
■Alclometasone dipropionate 0.05%
■Desonide 0.05%
■Fluocinolone acetonide 0.01%
■Triamcinolone acetonide 0.025%
Class 7—Least Potent
Class 7—Least Potent
■Topicals with dexamethasone, flumethasone, hydrocortisone, methylprednisolone, prednisolone
■Topicals with dexamethasone, flumethasone, hydrocortisone,
methylprednisolone, prednisolone
PHARMACOKINETICS
Before choosing a topical glucocorticoid preparation, one must consider patient-related factors such as age, extent and location of body surface area, and presence or absence of inflammation, as well as drug-related factors such as concentration, duration, vehicle, and intrinsic characteristics of the agent. Penetration of the glucocorticoid varies according to the skin site, which, in turn, is related to the thickness of the stratum corneum and the vascular supply to the area. For example, penetration of topical steroids through the eyelids and scrotum is greater than through the forehead and significantly greater than through the palms and soles. Inflamed, moist, and denuded skin also shows increased penetration. Potent topical steroids (Classes 1 and 2) should rarely, if ever, be used in the areas with the highest level of penetration. The target site for topical corticosteroids is the viable epidermis or dermis, and clinical response to a formulation is directly proportional to the concentration of corticosteroid achieved at the target site. Topical corticosteroids are compounded in several formulations and with varying strengths. Treatment adherence in the management of skin conditions is vital, as such, formulations including spray, foam, lotion, hydrogel, and shampoo have been developed to improve patient convenience and acceptance. Both increasing hydration of the stratum corneum and using occlusive dressings may enhance absorption of topical corticosteroids. Expert consensus recommends soak and smear methods for treating atopic dermatitis, which consists of a warm bath followed by a generous application of topical corticosteroids, though evidence from studies remains limited.
INDICATIONS
INDICATIONS
Topical corticosteroids are used for an antiinflammatory activity in inflammatory skin diseases, antimitotic effects, and for their capacity to decrease the synthesis of connective tissue molecules.55 The responsiveness of diseases to topical glucocorticoids varies and thus must be considered when prescribing topical corticosteroids. Diseases can be divided into the 3 categories shown in Table 184-6: (a) highly responsive, (b) moderately responsive, and (c) least responsive.
PEDIATRIC USES
Children and, in particular, infants, are at an increased risk of absorbing topical corticosteroids for several reasons. They have a higher body-surface-area-to-weight ratio, and thus have a higher degree of absorption for the same amount applied as an adult,59 and they also have thinner skin. Infants also may be less able to metabolize potent glucocorticoids rapidly.60 Application of topical steroids to the diaper area results in occlusion of the steroid by the diaper, and increased penetration occurs. As with other skin conditions,
28
Highly responsive
■Atopic dermatitis (children)
■Intertrigo
■Psoriasis (intertriginous)
■Seborrheic dermatitis
Moderately responsive
■Atopic dermatitis (adults)
■Lichen simplex chronicus
■Nummular eczema
■Papular urticaria
■Parapsoriasis
■Primary irritant dermatitis
■Psoriasis
Least responsive
■Allergic contact dermatitis, acute phase
Least responsive ■Allergic contact dermatitis, acute phase
■Dyshidrotic eczema
■Dyshidrotic eczema
■Granuloma annulare
■Granuloma annulare
■Insect bites
■Insect bites
■Lichen planus
■Lichen planus
■Lupus erythematosus
■Lupus erythematosus
■Necrobiosis lipoidica diabeticorum
■Necrobiosis lipoidica diabeticorum
■Palmoplantar psoriasis
■Palmoplantar psoriasis
■Pemphigus
■Pemphigus
■Psoriasis of nails
■Psoriasis of nails
■Sarcoidosis
■Sarcoidosis
selecting the appropriate strength according to the body site, the extent of involvement, and the flare intensity is essential for treatment success. Concerns for atrophy, hypopigmentation, osteoporosis, and telangiectasias are minimized when topical steroids are used in accordance with guidelines.61
High-potency newer formulations of corticosteroids are effective in pediatric atopic dermatitis and may be considered for short courses, although the highest potency steroids may not be recommended by all experts for pediatric use.59,62,63 Rarely, high-potency applications can result in systemic absorption and cutaneous side effects. The low risk for side effects and highly effective treatment modality should be carefully explained to parents to maximize compliance and understanding and minimize undertreatment. Results from numerous surveys demonstrate a “corticosteroid phobia” among patients/caregivers that leads to treatment noncompliance.64-67
GERIATRIC USES
Elderly patients may have thin skin, which allows for increased penetration of topical glucocorticoids. They are also more likely to have preexisting skin atrophy secondary to aging and may be diaper dependent. Similar precautions used in the treatment of infants should be used when treating elderly patients.
USES IN PREGNANCY
Most topical steroids are rated by the U.S. Food and Drug Administration as category C drugs. Best
3389
28
available evidence suggests no significant effects for pregnant women who use mild or moderate topical corticosteroids during pregnancy. A risk for low birth weight is associated with high-potency topical steroids, although the risk is small if used in the short term and increases with heavier use of strong topical corticosteroids.68 However, studies are observational and imprecision was noted in regard to the outcome of low birth weight.69 Topical corticosteroids have not been studied during breastfeeding; however, based on National Institutes of Health recommendations, it is recommended to limit long-term exposure to high-potency corticosteroids while breastfeeding. In addition, use only water-miscible cream or gel products to limit exposure of infants to mineral paraffins while breastfeeding. Topical corticosteroids should be wiped off prior to breastfeeding.51
DOSING REGIMEN
DOSING REGIMEN
The frequency of topical application of corticosteroids was developed in an empirical manner, with most textbooks and physicians recommending twice-daily use. For superpotent corticosteroids once-daily application is considered as beneficial as twice-daily application. Observations suggest once-daily dosing also may be beneficial when using lesser-potency corticosteroids. Tachyphylaxis has been demonstrated in experimental conditions by diminished vasoconstriction, rebound of DNA synthesis, and recovery of histamine wheals after application of topical steroids in patients with a history of long-term topical steroid usage.70 Whether this tachyphylaxis is clinically relevant remains unclear. For example, patient adherence to therapy may explain what could be seen clinically as tachyphylaxis in pediatric eczema treated with appropriate topical corticoisteroids.61
SIDE EFFECTS AND PRECAUTIONS
SIDE EFFECTS AND
PRECAUTIONS
Both local and systemic side effects have been documented with the use of topical corticosteroids. Application of corticosteroids to large surface areas, occlusion, higher concentrations, or more potent derivatives directly increases the risk of systemic absorption and subsequent side effects. Side effect–specific monitoring parameters are discussed below. Under normal conditions, up to 99% of the applied topical corticosteroid is cleared from the skin, and only 1% is therapeutically active. Cutaneous adverse effects can result from the small percentage of percutaneously absorbed corticosteroid or also may result from its transient presence onto the skin. Continued use of topical corticosteroids also may lead to tachyphylaxis, as noted above.
3390
■Initiate lowest potency to sufficiently control disease.
■Initiate lowest potency to sufficiently control disease.
■Topical corticosteroids should be avoided on ulcerated or atrophic skin, and on skin with coexistent infectious dermatoses.
■Topical corticosteroids should be avoided on ulcerated or atrophic
skin, and on skin with coexistent infectious dermatoses.
■Prolonged use of insufficiently potent agent should be avoided.
■Prolonged use of insufficiently potent agent should be avoided.
■Treatment with low to medium potency preparations is recommended for large surface areas.
■Treatment with low to medium potency preparations is
recommended for large surface areas.
■Highly responsive diseases will usually respond to weak steroid preparations, whereas less-responsive diseases require mediumpotency or high-potency topical steroids.
■Highly responsive diseases will usually respond to weak steroid
preparations, whereas less-responsive diseases require mediumpotency or high-potency topical steroids.
■Low-potency, ideally nonhalogenated, preparations should be used on the face and intertriginous areas.
■Low-potency, ideally nonhalogenated, preparations should be
used on the face and intertriginous areas.
■Very potent steroid therapy, frequently under occlusion, is usually required for hyperkeratotic or lichenified dermatoses and for involvement of palms and soles.
■Very potent steroid therapy, frequently under occlusion, is
usually required for hyperkeratotic or lichenified dermatoses and for involvement of palms and soles.
■Because of the increased body-surface-area-to-body-mass-index ratio and increased risk of systemic absorption, high-potency preparations and halogenated–medium-potency preparations, should be avoided in infants and young children, other than for short-term application.
■Because of the increased body-surface-area-to-body-mass-index
ratio and increased risk of systemic absorption, high-potency preparations and halogenated–medium-potency preparations, should be avoided in infants and young children, other than for short-term application.
corticosteroids to prevent side effects should be followed (Table 184-8).54,71
ADVERSE EFFECTS
ADVERSE EFFECTS
Local adverse effects of topical corticosteroid use are more prevalent than systemic reactions.
ATROPHIC CHANGES
Skin atrophy is a prominent and potential cutaneous adverse effect, and involves both the epidermis and dermis. Dermal atrophy develops from the direct antiproliferative effects of topical corticosteroids on
■Highly potent formulations should be used for short periods (2 to 3 weeks) or intermittently.
■Highly potent formulations should be used for short periods (2 to
3 weeks) or intermittently.
■Once disease control is partially achieved, the use of a less-potent compound should be initiated.
■Once disease control is partially achieved, the use of a less-potent
compound should be initiated.
■Reduce frequency of application (eg, application only in the morning, alternate-day therapy, weekend use) once disease control is partially achieved.
■Reduce frequency of application (eg, application only in the
morning, alternate-day therapy, weekend use) once disease control is partially achieved.
■Sudden discontinuation should be avoided after prolonged use to prevent rebound phenomena.
■Sudden discontinuation should be avoided after prolonged use to
prevent rebound phenomena.
■Special guidelines should be followed when treating certain body areas (eg, intertriginous areas) or certain populations (eg, children or the elderly) to prevent the occurrence of local or systemic adverse effects.
■Special guidelines should be followed when treating certain body
areas (eg, intertriginous areas) or certain populations (eg, children or the elderly) to prevent the occurrence of local or systemic adverse effects.
■Close monitoring and further evaluation is recommended if systemic absorption of corticosteroids is suspected.
■Close monitoring and further evaluation is recommended if
systemic absorption of corticosteroids is suspected.
■Use combination therapy when clinically indicated (eg, addition of topical calcineurin inhibitor, tretinoin or calcipotriene).
■Use combination therapy when clinically indicated (eg, addition of
topical calcineurin inhibitor, tretinoin or calcipotriene).
28
STRUCTURAL CLASS A B C D1 D2
Type Hydrocortisone Triamcinolone Acetonide Betamethasone Betamethasone dipropionate Methylprednisolone aceponate
Structure C16—no methyl substitution
C16 methyl substitution C16 methyl substitution C16—no methyl substitution, no halogenation
Probable C21— short-chain ester
C17/21 long-chain ester
Cross-reactions Cross-reacts with D2 Budesonide specifically cross-reacts with D2
Cross-reacts with A and budesonide
Patch-test substance Tixocortol- 21-pivalate Budesonide
Clobetasol-17-propionate Hydrocortisone-17-butyrate
Triamcinolone acetonide
Triamcinolone
acetonide
Adapted from Jacob SE, Steele T. Corticosteroid classes: a quick reference guide including patch test substances and cross-reactivity. J Am Acad Dermatol. 2006;54(4):723-27.
fibroblasts, with inhibition of collagen and mucopolysaccharide synthesis, resulting in loss of dermal support. Reduction of glycosaminoglycan production and changes to structure and proportion has been described, though of note, low-potency therapy may have a lesser effect.72 Levels of hyaluronan, the major glycosaminoglycan in the skin, are also rapidly decreased after short-term glucocorticoid treatment.73,74
Fragmentation and thinning of elastic fibers develop in the upper layers of the dermis, whereas deeper fibers form a compact and dense network. As a result of these atrophic changes, there is vascular dilation, purpura, easy bruising, stellate pseudoscars (purpuric, irregularly shaped, and hypopigmented atrophic scars), and ulceration. Atrophy is more likely to occur with highpotency topical corticosteroids, but this effect has been clinically reversed by reduction of potency.75 Clinicians must consider these findings when prescribing corticosteroids and use appropriate doses, formulations, and durations to minimize risk for skin atrophy and reverse this side effect if it develops.
ACNEIFORM REACTIONS
The development or exacerbation of dermatoses of the face, including steroid rosacea, acne, and perioral dermatitis, is a well-known side effect of topical corticosteroids.76 Although steroids initially lead to the suppression of inflammatory papules and pustules, patients may flare when treatment is withdrawn, thus leading to continued use of greater potency topical corticosteroids. For these reasons, steroid use should be discouraged in the treatment of rosacea and perioral and periocular dermatitis.
OTHER CUTANEOUS EFFECTS
Decreased pigmentation and hypertrichosis are reported with use of topical corticosteroid therapy.76
Patients may also experience a burning sensation primarily on the face after withdrawal from continuous high dose steroid therapy.77 Even though data regarding this reaction is limited, clinicians may consider this in the differential for such reactions.
DEVELOPMENT OF INFECTIONS
Topical corticosteroids may exacerbate and/or mask cutaneous infectious diseases including tinea versicolor, disseminated Alternaria infection, and dermatophytosis. Granuloma gluteale infantum, characterized by reddish-purplish granulomatous lesions on the diaper area, is a well-known complication of diaper dermatitis during treatment with corticosteroids.76
ALLERGIC REACTIONS
Allergic contact dermatitis from steroids should be suspected when dermatitis worsens with corticosteroid therapy, does not lead to improvement, or changes the clinical pattern of disease. In a 6-year retrospective study, 127 patients (10.69%) had an allergic reaction to at least one corticosteroid. Among the 1188 patients, 71 (5.98%) reacted to 1 corticosteroid, 28 (2.36%) to 2 corticosteroids, 6 (0.51%) to 3 corticosteroids, 6 (0.51%) to 4 corticosteroids, and 16 (1.35%) to more than 4 corticosteroids.78 Patients suspected of having an allergy to a topical corticosteroid should undergo patch testing to determine whether the vehicle or the steroid is causing the contact dermatitis.79
If patch testing is unavailable, the clinician should prescribe a Class C steroid (from a classification A through D of steroids according to cross-reactivity in association with allergic contact dermatitis; Table 184-9 outlines the classification of corticosteroids by crossreactivity). Table 184-10 outlines potential allergens in topical corticosteroids.
3391
28
■Formaldehyde-releasing preservatives (imidazolidinylurea/ diazolidinylurea)
■Formaldehyde-releasing preservatives (imidazolidinylurea/
diazolidinylurea)
■Fragrance
■Fragrance
■Lanolin
■Lanolin
■Methylchloroisothiazolinone/methylisothiazolinone
■Methylchloroisothiazolinone/methylisothiazolinone
■Parabens
■Parabens
■Propylene glycol
■Propylene glycol
■Sorbitan sesquioleate
■Sorbitan sesquioleate
SYSTEMIC ADVERSE EFFECTS
Topical glucocorticoids, especially high-potency Class 1 agents, may result in HPA axis suppression and, rarely, other systemic adverse effects. Clinicians should be aware of this possibility when using highpotency topical corticosteroids or when patients report inappropriate use of high-potency corticosteroids.
ACKNOWLEDGMENTS
We would like to thank Isabel C. Valencia and Francisco A. Kerdel, who contributed to the previous version of this chapter in the 8th edition.
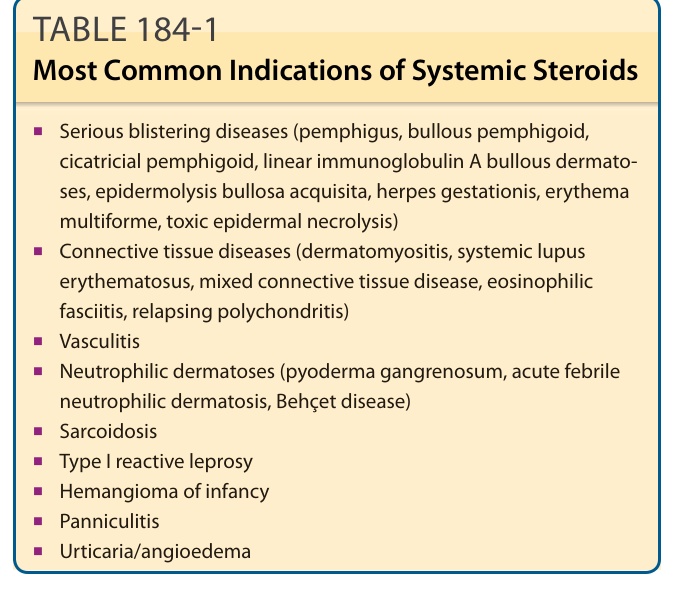
TABLE 184-1 Most Common Indications of Systemic Steroids
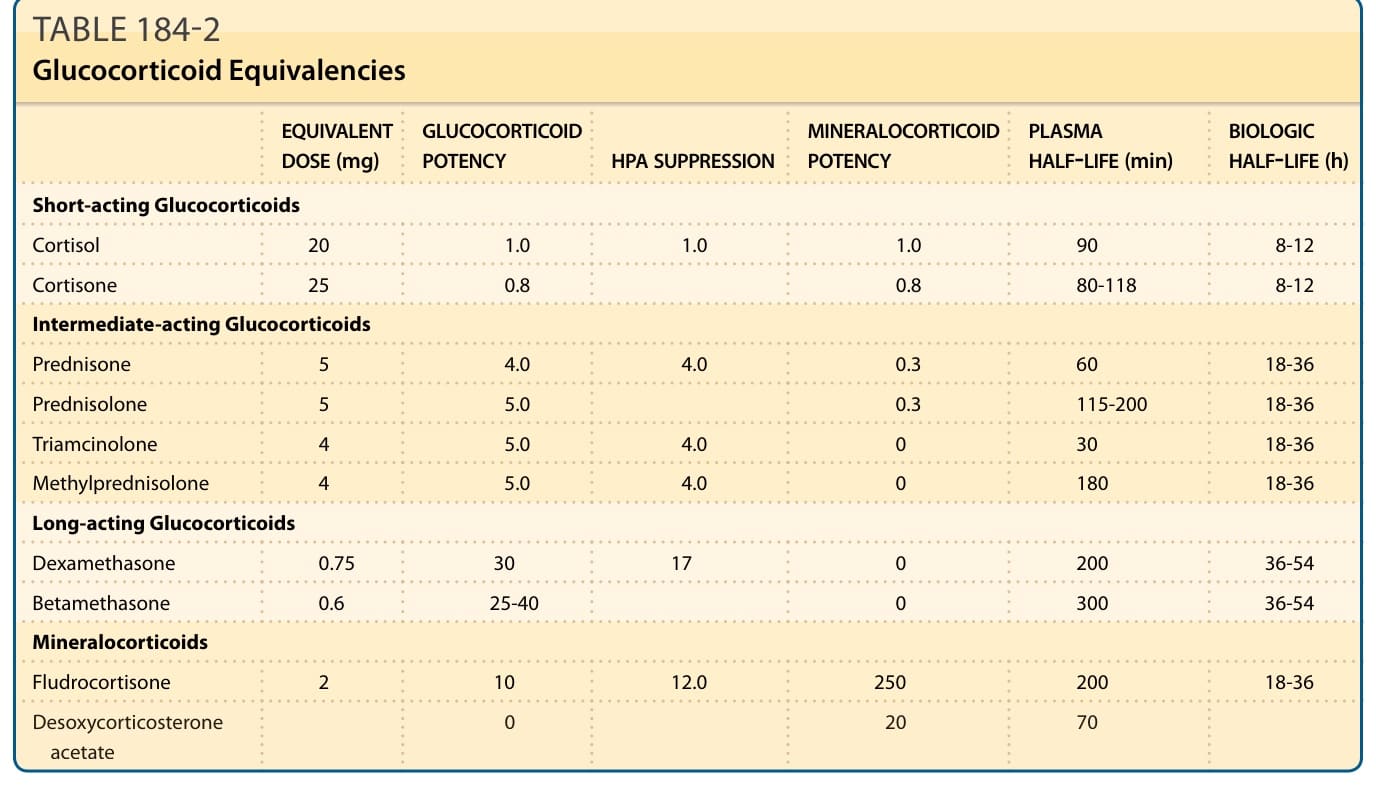
TABLE 184-2 Glucocorticoid Equivalencies
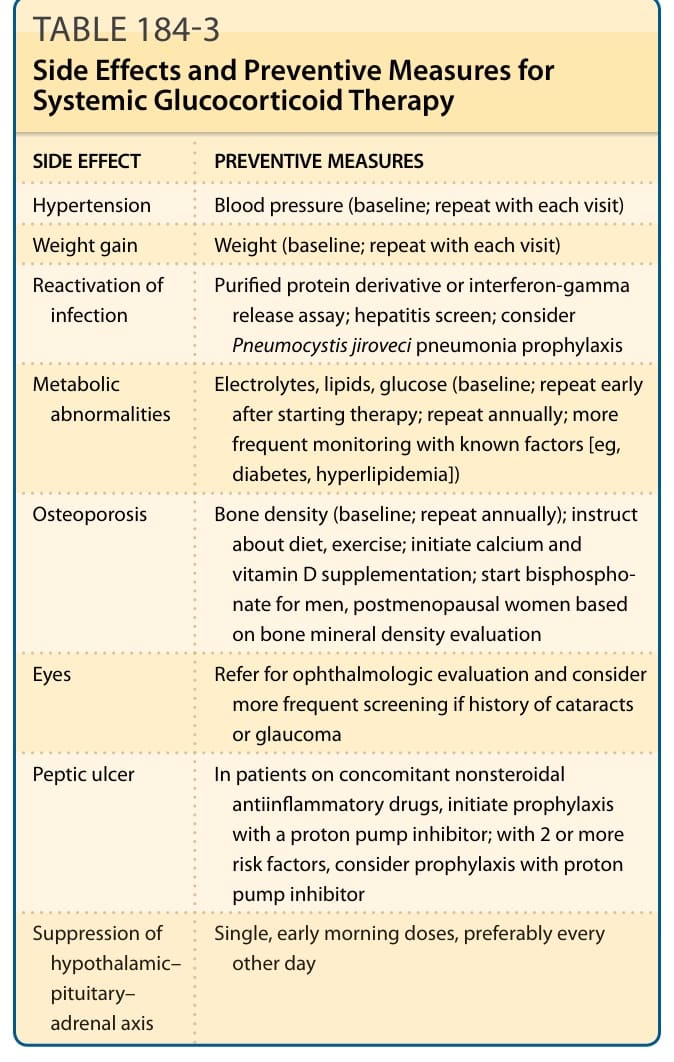
Table 184-3 outlines side effect preventive measures for systemic glucocorticoid therapy.
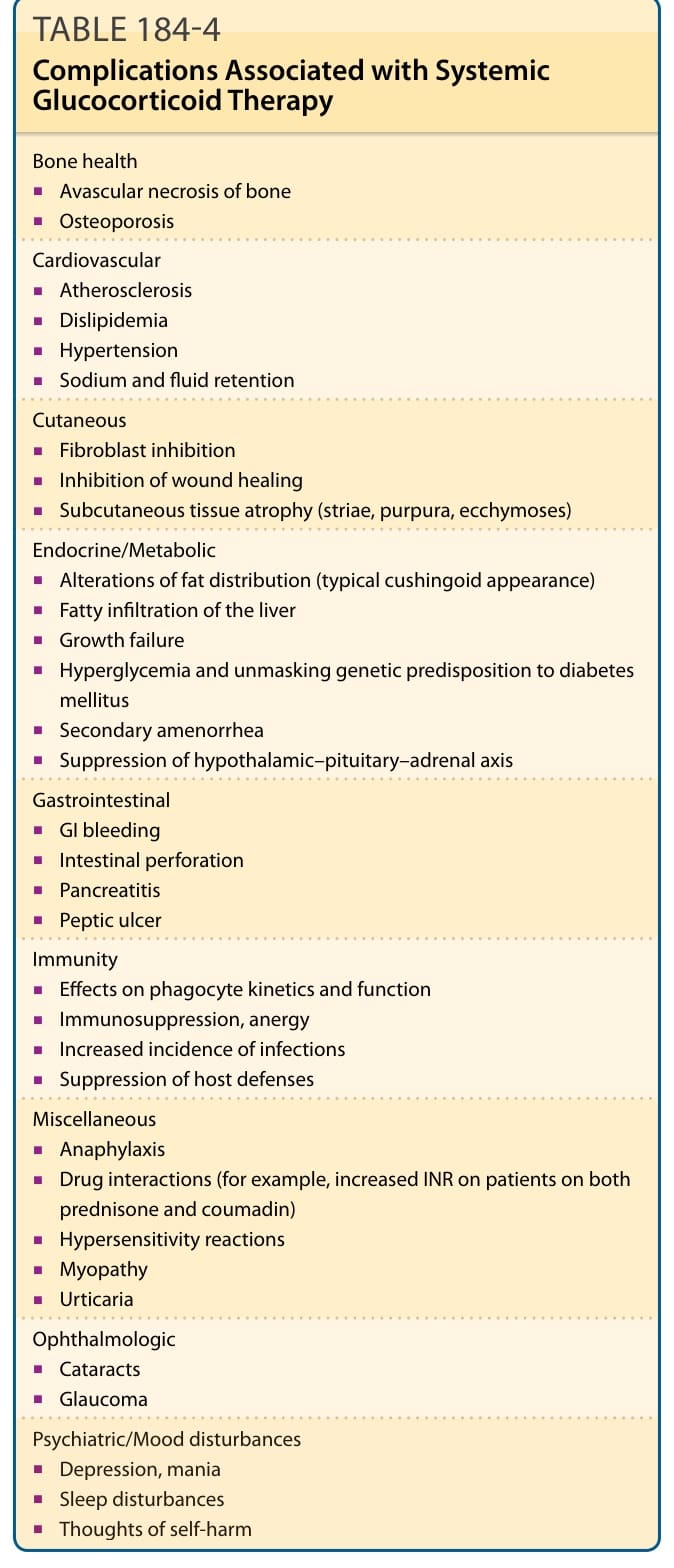
TABLE 184-4 Complications Associated with Systemic Glucocorticoid Therapy
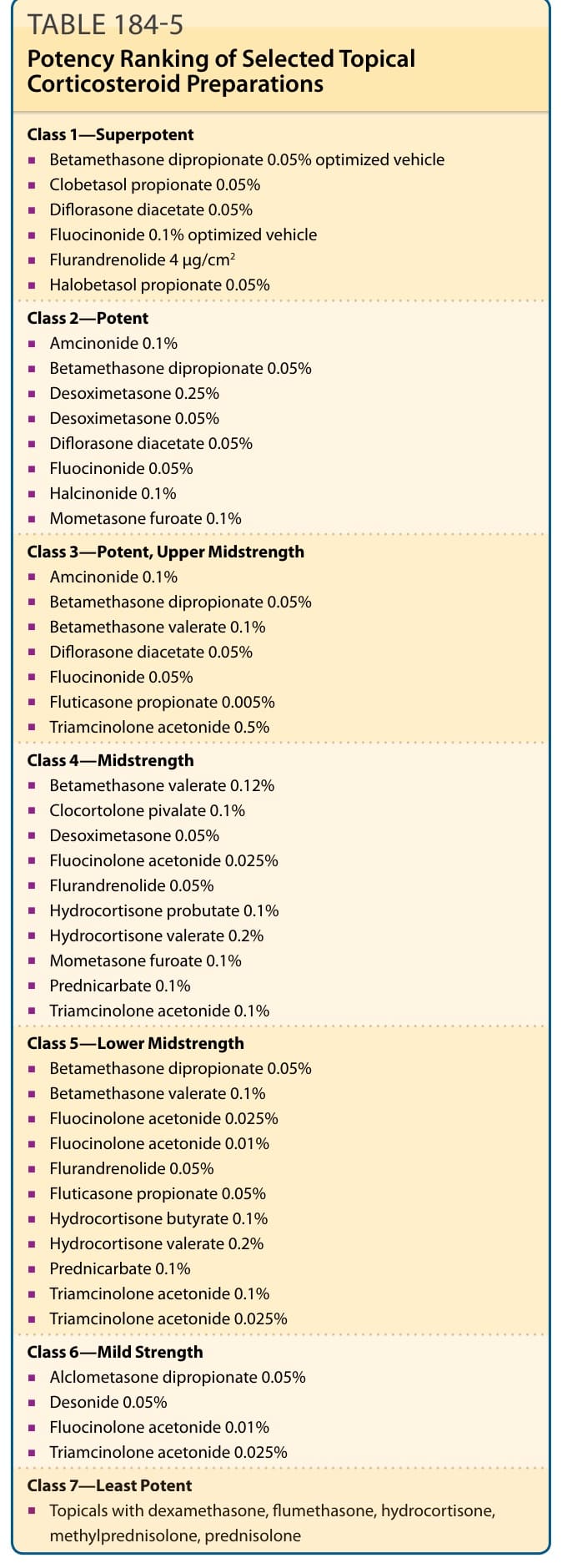
TABLE 184-5 Potency Ranking of Selected Topical Corticosteroid Preparations
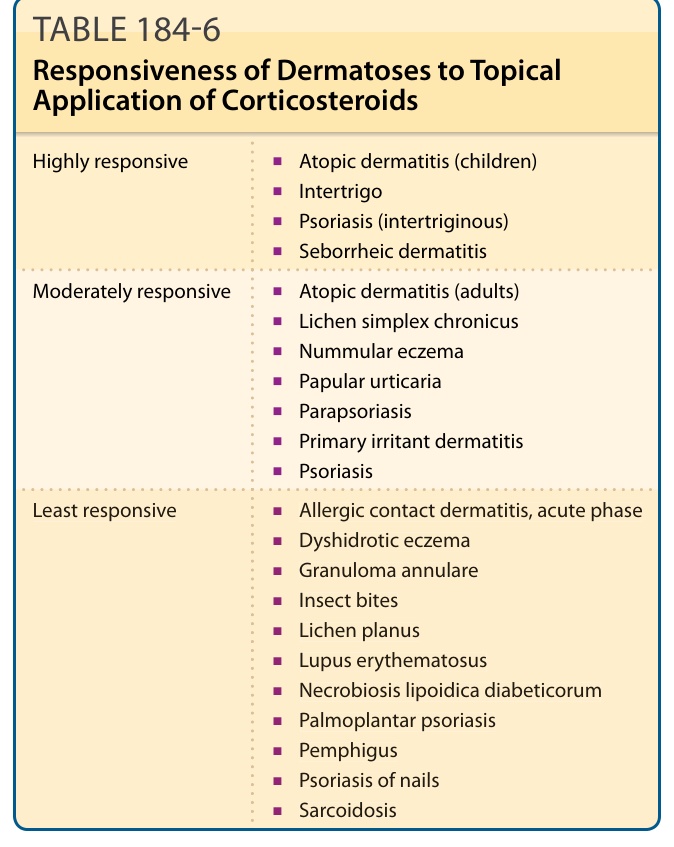
TABLE 184-6 Responsiveness of Dermatoses to Topical Application of Corticosteroids
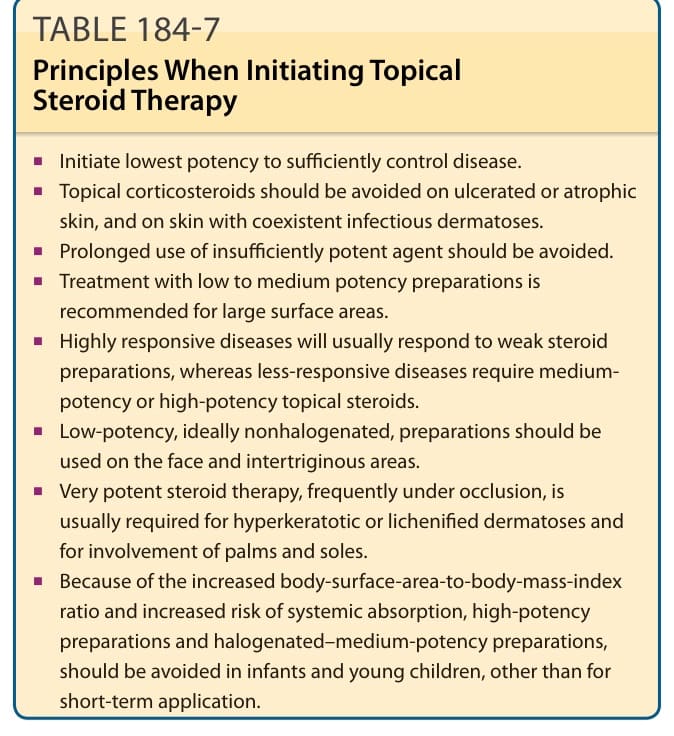
Table 184-7 outlines some general principles that should be remembered when initiating topical corticosteroids.55 Considerations for prescribing topical
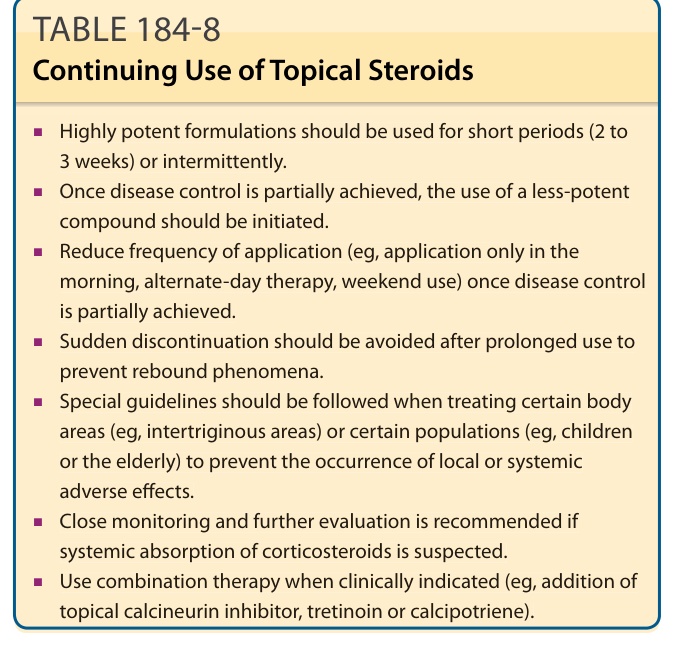
TABLE 184-8 Continuing Use of Topical Steroids
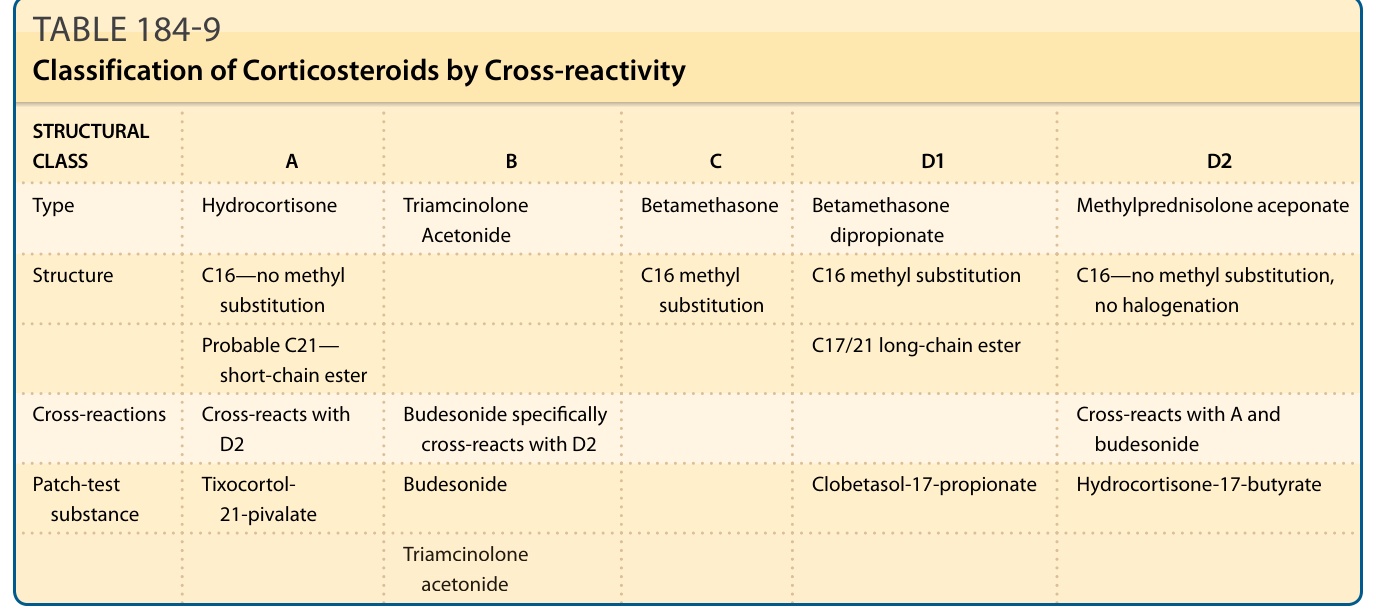
TABLE 184-9 Classification of Corticosteroids by Cross-reactivity
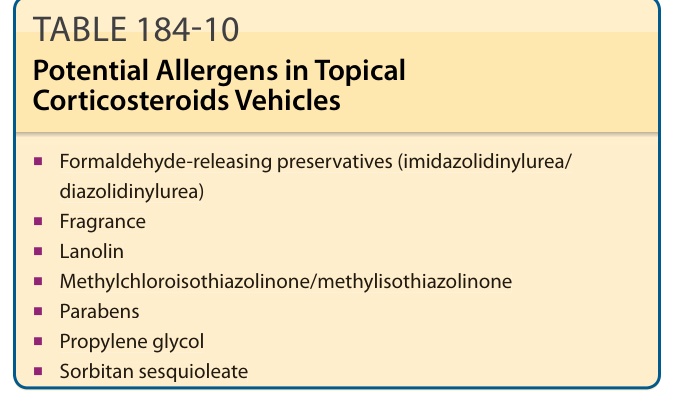
TABLE 184-10 Potential Allergens in Topical Corticosteroids Vehicles