Lyme Borreliosis
27
AT-A-GLANCE
■ Lyme disease is caused by Borrelia burgdorferi, a tickborne spirochete.
■ Clinical course can be prolonged and may involve multiple organ systems.
■ The most common cutaneous finding is the erythema migrans rash. Other cutaneous manifestations include lymphocytoma and acrodermatitis chronica atrophicans, which are only seen in European disease.
■ Diagnosis is typically made on clinical identification of the erythema migrans rash and/or serologic testing.
■ Early treatment with antibiotics (doxycycline, amoxicillin, or cefuroxime) is highly successful.
HISTORICAL PERSPECTIVE
Lyme borreliosis, or Lyme disease, is the most commonly reported arthropod-borne illness in both the United States and Europe.1 The disease acquired its name from epidemiologic investigations in the 1970s of cases of oligoarticular arthritis among children in and around the town of Lyme, Connecticut.2 Certain features, including the tight clustering of cases in a heavily wooded area, and a rash that preceded arthritis that occurred predominantly in the summer, were suggestive that this was an arthropod-borne infectious disease. In 1981, Burgdorfer isolated a new spirochetal bacterium, Borrelia burgdorferi, from the midgut of the Ixodes dammini tick (now Ixodes scapularis).3 Recovery of the organism from cutaneous lesions, cerebrospinal fluid, and blood specimens of patients with Lyme disease in both the United States4,5 and Europe6-8 definitively linked the disease with B. burgdorferi. Subsequently, additional genospecies causing Lyme disease were recognized. The original North American genospecies was designated B. burgdorferi sensu stricto and other species (including the 2 most prominent genospecies in other parts of the world, Borrelia garinii and Borrelia afzelii) were considered part of the B. burgdorferi sensu lato group. Recently, a change in the genus of Lyme disease causing Borrelia to Borreliella has been proposed to recognize significant differences with relapsing fever Borrelia. Borreliella encompasses all the genospecies that were originally designated as part of the sensu lato group. However, this has not been fully accepted so we will continue to use the Borrelia designation conventions.
EPIDEMIOLOGY
Lyme disease occurs in the northern hemisphere in North America, Europe and Asia. The prevalence of strains differs between the continents, with B. burgdorferi being the predominant species in North America, B. garinii and B. afzelii being predominant in Asia, and all three present in Europe. Disease is often focal with high rates in some countries/states but not others. In Europe, the incidence is highest in the Austria, Belgium, Estonia, Lithuania, The Netherlands, Slovenia, and Sweden, with approximately 120,000 reported cases per year in Europe. The disease is less common in Asia, but has been reported in Russia, China, Korea, and Japan. In the United States, the majority of the cases are reported from the Northeast and mid- Atlantic areas and the North Central part of the country. There is also a smaller foci of disease in the Northwestern United States. Lyme disease Borrelia are transmitted by ticks in the Ixodes ricinus group. In the United States, the major tick vector is I. scapularis. Ixodes pacificus serves as the vector in the western United States. The white-footed mouse is the primary amplifying host of B. burgdorferi, with other small mammals, such as voles, shrews, chipmunks, and birds, playing a lesser role. B. burgdorferi sensu stricto is by far the dominant genospecies in the United States, although there have been recent reports of other species causing human disease (Borrelia bissettii, Borrelia mayonii).9-11
In Europe, the disease is transmitted by the I. ricinus tick, which feeds on more than 300 species of animals. Birds, shrews, voles, and other small mammals serve as the major amplifying hosts of Borrelia species in Europe.12 Three genospecies constitute the majority of human-infecting organisms in Europe: B. burgdorferi sensu stricto, B. afzelii, and B. garinii. Ixodes persulcatus is the main vector of B. burgdorferi in Asia. Human infections are less common throughout most of Asia and correspondingly, less is understood about the epidemiology. I. persulcatus is only known to transmit B. garinii and B. afzelii. B. burgdorferi has an enzootic cycle that involves the Ixodes ticks and small mammals and birds, as noted above. Ixodes ticks undergo 4 stages during a 2-year cycle: egg, larva, nymph, and adult. There is no transovarial (ie, transmission of disease from the adult tick to the larva via the eggs) passage of B. burgdorferi. Ticks must acquire the bacterium by taking a blood meal from an animal that can maintain the living organism. Once acquired, there is transstadial transmission ( passage from one stage in the tick lifecycle to the next). The majority of human transmission is from infected nymphal stage ticks, although infected adult ticks are also able to transmit disease.
27
In the United States, the incidence and range of the organism has steadily grown over the last several decades. Deer, which do not get infected with B. burgdorferi but can transport infected ticks, and birds are thought to be the primary drivers in dispersal of infected ticks into new areas. In the United States, the Centers for Disease Control and Prevention initiated surveillance for Lyme disease in 1982, and the Council of State and Territorial Epidemiologists made Lyme disease a nationally notifiable disease in 1991. From 1992 to 2006 the number of cases reported annually doubled, from 9908 cases to 19,931 cases.13 By 2015, the number of new cases reported annually in the United States was 34,390.12 In 2015, accounting for unreported cases, the Centers for disease control and prevention estimated that the incidence of Lyme disease in the U.S. was approximately 300,000 cases per year.14,15 During the period 2005 to 2014, approximately 96% of reported cases occurred in 14 states located in the Northeastern, mid-Atlantic, and North Central regions: Connecticut, Delaware, Maine, Maryland, Massachusetts, Minnesota, New Hampshire, New Jersey, New York, Pennsylvania, Rhode Island, Vermont, Virginia, and Wisconsin (Fig. 179-1).16 Disease in many of the states with low incidence represents travelers infected during travel to more endemic regions. In the United States, Lyme disease is slightly more prevalent in males (53.1%) than in females, and whites are disproportionately represented at 94.1% of cases. Two-thirds of cases of have onset in the summer months of June, July, and August. There
is a bimodal age distribution of Lyme disease in the United States, with peaks at ages 5 to 9 years (8.6 cases per 100,000 population) and 55 to 59 years (7.8 cases per 100,000 population).13
CLINICAL FEATURES
CUTANEOUS FINDINGS
CUTANEOUS FINDINGS
EARLY CUTANEOUS FINDINGS Erythema Migrans: Lyme disease initiates with movement of bacteria from the tick to the patient during tick attachment. Bacteria first multiply locally in the skin. The erythema migrans (EM) rash, which is typically the first symptom to develop with infection, begins 3 to 30 days (average: 7 days)17 after completion of tick feeding. EM is thought to be present in 70% to 80% of those individuals infected, with estimates reported to be as high as 90% in patients diagnosed with Lyme disease.5,17,18 EM rash is a result of the host inflammatory response to the nascent infection. The histopathologic description of EM is a superficial and deep perivascular infiltrate of eosinophils at the center of the lesion and plasma cells, lymphocytes, and histiocytes peripherally (Fig. 179-2).19 Immunohistochemical studies indicate the infiltrate to be composed of CD4+ T lymphocytes, with the exception of those seen
Cases of Lyme disease reported to Centers for Disease Control and Prevention in 2014
1 dot placed randomly within county of residence for each confirmed case
3288
in association with HIV infection in which the infiltrate is mainly CD8+ T lymphocytes, reflective of the CD4 lymphopenia of HIV infection.20 The organism can be readily cultured from biopsy of the EM lesion and can be seen in tissue samples by immunofluorescence.21
Solitary EM rash typically occurs at the site of the tick bite, although in many cases, a definite history of a tick bite at the site of the lesion is not obtained.22
Certain areas on the body are more likely to sustain tick bites long enough to allow for transmission of the spirochete, which is typically thought to require a minimum of 36 hours. Ticks may go unnoticed in the popliteal fossa, the groin, axilla, back, and on the head; likewise EM rash may also go unobserved in these areas. In small children, solitary EM rash occurs more often on the head and neck than in older children or adults, where these areas are seldom affected.18
EM rash is classically described as a large (>5 cm), expanding, erythematous, round or oval lesion, with the longer axis along the lines of least skin tension (Langer lines) and central clearing, often with a darker punctate center at the site of the tick bite (so-called Bull’s-eye rash) (Figs. 179-3 and 179-4). However, this classic appearance only occurs in a minority of cases. In one observational study of 118 microbiologically proven cases of Lyme disease, only 9% of EM rash had this appearance, whereas 59% had a homogeneous appearance.23 In another study of 14 patients with microbiologically proven Lyme disease, 10 (71%) of 14 EM rashes lacked the classic central clearing (Fig. 179-5).24 Central clearing may be more common in B. garinii than with B. burgdorferi. Strle and others compared characteristics of culture-proven EM rash from B. garinii in Slovenia and B. burgdorferi in the United States. Central clearing was found in 71% of those with B. garinii versus 35.3% with B. burgdorferi (p = 0.0002) (Table 179-1).25
The lesion in itself is usually asymptomatic, but approximately 30% to 50% of patients report mild tingling, itching, or burning.25,26 Systemic manifestations,
27
reported in approximately 50% of patients, may appear before, during, or after the classic lesion.27,28
Uncommon presentations of EM rash include forms with marked central necrosis, EM of minimal size (size of the ring less than 5 cm at initial presentation) (2%), and the vesicular variant (5%).29-31
The bacteria can disseminate from the inoculation site as early as 3 days after the presence of the original EM lesion. The most common manifestation of hematogenous dissemination of the spirochete are multiple EM rashes, which are scattered over the body. These are randomly distributed and do not represent multiple localized infections at individual tick bite sites. The appearance of multiple EM lesions appears to have become less common, as Lyme disease is more widely recognized and treated early in the disease process. As of this writing, it is estimated that multiple EM lesions occur approximately 10% to 18% of the time in those infected with B. burgdorferi.5,32,33 Secondary EM lesions
3289
27
are generally smaller than the primary EM lesions, but are otherwise indistinguishable, either visually or histologically (Figs. 179-6 to 179-8).
LATE CUTANEOUS FINDINGS
There are several dermatologic findings of Lyme disease that occur months to years after the initial infection. The majority of these are reported only in European infections and have not been seen in North American or Asian cases of disease.
Acrodermatitis Chronica Atrophicans: Observed mainly in elderly patients in Europe, acrodermatitis chronica atrophicans (ACA) has an insidious onset and appears to have a predilection for females.34 Rare cases of ACA have been reported in children.35 The time interval from the spirochete inoculation to the onset of symptoms of ACA is extremely difficult to evaluate. Most patients do not recall the
CHARACTERISTICS
FREQUENCY (%) LYME—U.S. (N = 79)
FREQUENCY (%) LYME—EUROPE (N = 231)
Patients: Median Age (years) (range in years) Male Female
38 (16-76) 62% 38%
46.7 (15-83) 43% 57%
Median diameter at presentation 13 cm 26 cm
Multiple EM lesions 18% 6%
“Bull’s-eye” or central
37% 71%
“Bull’s-eye” or central clearing 37% 71%
clearing
Data from Nadelman RB, Nowakowski J, Forseter G, et al. The clinical spectrum of early Lyme borreliosis in patients with culture-confirmed erythema migrans. Am J Med. 1996;100(5):502-508; and Strle F, Nelson JA, Ruzic-Sabljic E, et al. European Lyme borreliosis: 231 culture-confirmed cases involving patients with erythema migrans. Clin Infect Dis. 1996; 23(1):61-65.
3290
specific tick bite that initiated the disease.8,36 That the spirochete can survive for decades is favored by reports indicating recovery of the spirochete from biopsies of skin from ACA patients even after 20 years.8
An inflammatory phase characterizes the early clinical stages of this biphasic disease.37 The inflammatory phase presents as a bluish-red discoloration on the extensor aspect of fingers, hands, joints, and lower extremities (Fig. 179-9). Joints usually involved include the elbows and knees. Infiltrated purple bands of varying widths may be observed adjacent to involved joint(s). Associated findings include a cushion-like (“doughy”) swelling of the dorsum of the hands and feet.37 The extremities are most commonly involved, although extensive lesions on the trunk also have been documented. Lesions typically extend from the distal to the proximal portion of the extremity involved. Although the erythema and swelling initially vary in intensity (“waxes and wanes”), swelling of the posterior aspect of the lower extremities is believed by some to be particularly indicative of Lyme disease.38
Cutaneous atrophy characteristic of the later clinical stage is not an obligatory sequel to the inflammatory phase of ACA.37 Rarely, coexistence of both kinds of lesions at different sites in the same patient has been
27
documented. The atrophic phase is characterized by lesions with a “cigarette paper-like” appearance and a prominence of superficial veins (Fig. 179-10). CNS and peripheral nervous system involvement also have been documented in approximately 45% of patients with ACA. Thirty percent to 45% of patients suffer from a polyneuropathy, often most pronounced in the limb with cutaneous involvement.39 Chronic joint and bone involvement, attributed to persistence of spirochetes in cutaneous lesions, is most often seen in patients with longstanding ACA or an untreated lesion of EM or ACA and is typically restricted to the extremity involved. The characteristic symptom, exhibited in approximately one-third of patients in one study, was a swollen or painful foot and heel.39 Other symptoms include subluxation of small joints, bursitis, arthritis, and cortical thickening of bone. Solitary or multiple fibrotic lesions near joints, particularly in the olecranon area, may develop in some patients.37
All 3 species of B. burgdorferi that infect humans have been found in ACA lesions.40 Histopathologic features of biopsied lesions vary with the clinical phase of ACA. In inflammatory lesions, 3 layers are typically described: an atrophic epidermis, a zone of uninvolved papillary dermis, and a layer of inflammatory cells composed of lymphocytes and plasma cells.41 The presence of plasma cells in the infiltrate is documented mainly from studies from Europe, as American reports indicate that few or no plasma cells are found.36 The infiltrate may be deep with extension into the subcutis.38 Occasionally, interface dermatitis has been reported. Unusual findings include the presence of vacuoles, either singly or in groups, at different levels of the dermis.42 Although some believe these represent mature adipocytes, others believe them to be an expression of lymphedema, given that they are mainly observed from biopsies of markedly edematous sites. In favor of the expression-of-lymphedema hypothesis is the absence of such vacuoles from the same site after treatment.
3291
27
Phenotypic studies indicate the lymphocytes in the infiltrate are mainly of the CD4 phenotype, favoring the concept that ACA is a T-cell–mediated immune response.43 Further in support of this theory is the expression of adhesion molecules, such as intracellular adhesion molecule-1, on endothelial cells, lymphocytes, and basal keratinocytes in the inflammatory infiltrate.44 Chronicity of the lesions may be partially explained by downregulation of major histocompatibility complex class II molecules on Langerhans cells.45
Cutaneous Scleroborrelioses: Sclerotic skin lesions clinically indistinguishable from primary lichen sclerosus et atrophicus or morphea develop not only in association with other dermatoborrelioses ( approximately 10% of patients with ACA and borrelial lymphocytoma [see below]) but also in the absence of other cutaneous manifestations of Lyme disease.29,46,47
Periarticular (“ulnar”) fibrous nodules described in association ACA, may also occur in the absence of dermatoborrelioses.48 They usually present as hard nodules on the elbows and knees, and on the lateral aspect of the digits near joints, and have been reported to be provoked by trauma, surgery, and electromagnetic radiation.49
Uncommon sclerotic disorders associated with Lyme disease include progressive facial hemiatrophy (Parry-Romberg syndrome) and eosinophilic fasciitis (Shulman syndrome) (see Chap. 64).50 In support of an infectious etiology is the clinical similarity of the cutaneous lesions, positive history of tick bite, and, in rare cases, antiborrelial serologic evidence and positive culture and polymerase chain reaction (PCR) from lesions.51,52 Eosinophilic fasciitis associated with borrelial infection has been termed borrelial fasciitis, reflective of the infectious nature of these lesions.52 However, patients with borrelial fasciitis lack the peripheral blood eosinophilia typical of patients with Shulman disease. A unifying feature of lichen sclerosus et atrophicus– like and morphea-like scleroborrelioses is the abundance of plasma cells in the inflammatory infiltrate.37 Unusual histologic findings include a scleromyxedema-like picture with increased dermal mucin and fibroblast proliferation.48
Histopathologic examination of a periarticular fibrous nodule reveals relatively well-circumscribed nodules of broad hyalinized bundles of collagen with macrophages and plasma cells.49,53 Adjacent capillaries may be occluded by similar deposits. Progressive facial hemiatrophy and eosinophilic fasciitis show variable dermal sclerosis, loss of appendages, and a perivascular infiltrate composed predominantly of lymphocytes and plasma cells with scattered histiocytes.38 In borrelial fasciitis, eosinophilic infiltration of the fascial planes is not as impressive as in “idiopathic” Shulman disease.50
Cutaneous Atrophoborrelioses: Atrophic lesions indistinguishable from primary anetoderma (see Chap. 70) may also occur in the absence of other dermatoborrelioses.37,54 When associated with ACA, these lesions are usually seen at the periphery of an extensive lesion.55
3292
Biopsy specimens from atrophic or anetodermalike skin lesions show abnormal elastic tissue fibers in association with a perivascular infiltrate of lymphocytes with occasional histiocytes, neutrophils, or eosinophils.37 Spirochetes are found with difficulty in histologic sections.
Cutaneous Lymphoborrelioses (B-Cell and T-Cell Lymphoid Hyperplasias): Lymphocytic infiltrates associated with Borrelia are the least common of the cutaneous hallmarks of Lyme disease (1%) and may present either as single borrelial lymphocytoma (lymphadenosis benigna cutis) or as multiple lesions.38 The coexistence of lymphocytoma with other dermatoborrelioses led to the suggestion of a unifying causative organism, favored by the development of EM-like lesions following passive inoculation of an infiltrate from a lesion of lymphadenosis benigna cutis.8,56 Lymphocytoma has been reported solely in Europe. However, all 3 species of B. burgdorferi sensu lato are associated with lymphocytoma, so it is unclear whether the lack of U.S. cases is related to strain differences.40
More common in children than in adults, lymphocytoma clinically presents as a nodulopapular lesion in the ear lobes (Fig. 179-11) and scrotum in children and the nipple-areolar area (Fig. 179-12) in adults.29 The precise reason for this predilection is not known but is believed to be tissue temperature related.38 As with the other dermatoborrelioses, most patients are not aware of a preceding tick bite. The incubation period varies anywhere from a few weeks to 10 months. The duration of an untreated solitary lesion can vary from months to years ( average: 5 years). Spontaneous resolution may occur, but typically lesions resolve more rapidly with antibiotic therapy.39 Lesions of multiple lymphocytomas can be entirely subcutaneous, may last for decades, and typically have no specific site predilection or associations with other dermatoborrelioses. Direct evidence of an infective etiology has been provided from studies demonstrating the presence of
fragmented spiral forms suggestive of B. burgdorferi in lesions of benign lymphocytic infiltrates,57 and has been confirmed by immunofluorescence using species-specific monoclonal antibodies. Spirochetes may be cultured directly from biopsy specimens or B. burgdorferi DNA may be detected by PCR. High titers of antiborrelial antibodies have been reported in more than 50% of patients with lymphadenosis benigna cutis solitaria.56 The common denominator in patients with Borrelia-associated lymphoma appears to be a high titer of antibodies, typical of the chronic stage of the infection, against B. burgdorferi.56
Discoid lesions “starting as small papules and expanding peripherally with central clearance” that wax and wane also have been described in association with borrelial infection.57 The name given for these lesions is benign lymphocytic infiltrates of the skin ( Jessner-Kanof) (see Chap. 120). More common in men, they tend to be located on the face, neck, and upper trunk. Annular lesions clinically resembling EM also have been described. Several reports suggest an association of lowgrade cutaneous B-cell lymphoma with B. burgdorferi infection.58,59 Clinical presentation of Borrelia- ssociated B-cell lymphoproliferative disease is varied and consists of multiple ill-defined, slowly progressive plaques and nodules presenting on the trunk, extremities, or both, of usually older patients. The highest frequency of infection with Borrelia has been found in marginal zone lymphoma (20% to 52%), followed by follicular center lymphoma (15% to 26%) and diffuse large B-cell lymphoma (15% to 16%; see Chaps. 119 and 120).58,60 That antigenic drive by Borrelia may be a pathogenic factor in more than 1 subtype is supported by the association of B. burgdorferi with multiple subtypes of cutaneous B-cell lymphoma. Demonstration of the organism in the skin before development of overt cutaneous B-cell lymphoma serves to confirm the temporal progression of B. burgdorferi– associated B-cell lymphoproliferative disease. Clinical regression of marginal zone lymphoma after eradication of B. burgdorferi argues in favor of a benign process.59,61,62
27
Histopathologic findings of benign B-cell– and T-cell–dominant hyperplasias are essentially similar to benign lymphoid hyperplasias secondary to an arthropod bite, vaccination, or other causes (see Chap. 120). Definitive classification of Borreliaassociated B-cell lymphoma is confounded by the immunohistochemical profile: expression of CD5 and CD10 (common acute lymphoblastic leukemia antigen), antigens typically associated with centrocytic lymphoma, are absent in Borrelia-associated B-cell lymphoma.58
Other Cutaneous Lesions: Other cutaneous lesions reported in patients with documented Lyme disease include panniculitis, vasculitis, granuloma annulare, erythema multiforme, and a syphilis-like papulosquamous eruption, but B. burgdorferi has not been directly recovered from any of these lesions (Table 179-2).
NONCUTANEOUS FINDINGS
NONCUTANEOUS FINDINGS
After the initial inoculation into skin and resultant EM lesion, B. burgdorferi quickly disseminates to other parts of the body causing site-specific manifestations. Common areas for dissemination include the central and peripheral nervous system, the heart and the joints. Often in early Lyme disease there are multiple, nonspecific symptoms in addition to rash. The frequency of these symptoms appears to vary depending on the genospecies is involved (Table 179-3).
NERVOUS SYSTEM MANIFESTATIONS
B. burgdorferi can cause neurologic disease in 10% to 15% of patients in the United States who have not received antibiotics. Meningitis, cranial neuropathy, and radiculopathy are the most common neurologic manifestations and can manifest as soon as 1 week after EM.63 Facial palsy is the most characteristic neuropathy of early Lyme disease in the United States, occurring in 40% to 50% of patients with borrelial neurologic involvement, usually within 4 weeks after onset of EM. Bilateral facial palsy should immediately raise suspicion for Lyme disease, as it is uncommon in most other causes of facial palsy. Involvement of other cranial nerves has been reported, but is relatively rare.63 The triad of lymphocytic meningitis, cranial palsy (often facial), and radiculoneuritis, known as Bannwarth syndrome, is pathognomonic for Lyme disease. It is frequently reported in Europe but is rare in the United States.64,65 It is thought that B. garinii causes meningitis and radiculopathy more frequently than B. burgdorferi.66 Acute or subacute myelitis leading to spastic paraparesis and cerebrospinal fluid pleocytosis, mononeuritis, and a Guillain-Barré–like syndrome may also occur in early disseminated disease.67,68 Late neurologic manifestations include encephalomyelitis, encephalopathy, and chronic polyneuropathies.69,70
3293
27
ONSET DIAGNOSIS/DIFFERENTIAL DIAGNOSIS
Common Manifestations
Erythema migrans Weeks to months (early) Arthropod bite, erythema multiforme granuloma annulare, urticaria, erysipelas, brown recluse spider bite, fixed drug eruption
Acrodermatitis chronica atrophicans Months to years (late) Venous insufficiency, lichen sclerosus, scleroderma, physiologic age-related atrophy, corticosteroid-induced atrophy
Uncommon Manifestations
Cutaneous scleroborrelioses Months to years (late)
■Morphea
■Primary morphea
■Lichen sclerosus et atrophicus
■Primary lichen sclerosus et atrophicus
■Periarticular fibrous nodules
■Rheumatoid nodule, gouty tophi
■Progressive facial hemiatrophy
■Primary progressive facial hemiatrophy/Parry-Romberg syndrome
■Eosinophilic fasciitis
■Primary eosinophilic fasciitis/Shulman syndrome
Cutaneous atrophoborrelioses Months to years (late)
■Anetoderma
■Primary anetoderma
Cutaneous lymphoborrelioses Months to years (late)
■B-cell dominant (including B-cell lymphoma)
■Arthropod bite reaction, response to vaccination, granulomas, neoplasm
■T-cell dominant
■Pityriasis lichenoides, polymorphous light eruption
Other cutaneous lesions Weeks to months to years (early or late)
■Panniculitis
■Erythema nodosum
■Granuloma annulare
■Insect bite reaction
■Erythema multiforme
■Drug eruption
■Syphilis-like papulosquamous eruption
■Secondary syphilis
■Syphilis-like papulosquamous eruption ■Secondary syphilis
CARDIAC MANIFESTATIONS
Cardiac involvement occurs in anywhere from 1% to 10% of untreated patients in the United States71,72
and in 0.3% to 4% of European patients.73,74 The wide ranges probably reflect the fact that in recent years, Lyme disease is recognized and treated sooner,
SYMPTOM OR LABORATORY ABNORMALITY
FREQUENCY (%) LYME U.S. (N = 79)
FREQUENCY (%) LYME EUROPE (N = 231)
FREQUENCY (%) B. MAYONII (N = 6)
Fatigue 54 10 67
Arthralgia 44 25 17
Myalgia 44 11 67
Headache 42 20 83
Neck stiffness/ meningeal signs 35 1 50
GI symptoms 26 0.4 67
Regional lymphadenopathy 23 7 N/A
3294
Fever 16 4 83
Fever 16 4 83
resulting in lower incidence than in the past. It usually occurs within several weeks after the onset of infection, although it can occur as early as 1 week and as late as 7 months into the infection.71,75 Within the heart, B. burgdorferi has a predilection for the atrioventricular node, resulting in atrioventricular block. Acute myopericarditis and left ventricular dysfunction can also occur, but are usually self-limited and mild, only sometimes resulting in transient cardiomegaly or pericardial effusion.76 B. burgdorferi has been isolated from endomyocardial biopsy samples from several European patients with chronic dilated cardiomyopathy, a complication observed less frequently in the United States.77,78 In the United States, there have been cases of cardiac sudden death where autopsies have revealed myocarditis caused by undiagnosed Lyme disease.72
MUSCULOSKELETAL MANIFESTATIONS
Early musculoskeletal manifestations of B. burgdorferi infection are typically nonspecific. Inflammatory arthritis is the most frequent clinical sign of late-disseminated Lyme disease in the United States, occurring in approximately 60% of patients with untreated or incompletely treated infection.62,79 It usually presents 1 or more months
after the onset of Lyme disease as asymmetric monoarthritis or oligoarthritis of large joints, most often of the knee. Migratory arthralgia is also relatively common, especially during disseminated Lyme disease. Bouts of arthritis are generally frequent and short at first, becoming longer and less frequent with time, each lasting from several days to 1 year.79
OTHER MANIFESTATIONS OF LYME DISEASE
Ophthalmic complications in the form of conjunctivitis, keratitis, iridocyclitis, retinal vasculitis, chorioiditis, and optic neuropathy are rare manifestations of Lyme disease. They are thought to be the direct result of tissue inflammation by B. burgdorferi and are usually associated with other signs and symptoms of disease. The eye also may be affected by extraocular manifestations of Lyme disease, such as cranial nerve pareses and orbital myositis. Findings in other organ systems (GI, lymphatic, respiratory, urinary, and genital) have been reported, but the associations with borrelial infection are loose.
PERINATAL LYME DISEASE
Studies in both human and animal models indicate that B. burgdorferi can cross the placenta during the initial spirochetemia, but evidence of a fetal immune response or an adverse neonatal outcome are not definitively established. Several studies have found no link between maternal infection with Lyme and subsequent birth defects.80-84
LYME DISEASE IN CHILDREN
Other than differences in localization of EM lesions (more typically in the head and neck), pediatric Lyme disease is similar to that of adults. Of note, however, optic nerve involvement may lead to blindness in children.85
COMPLICATIONS
COMPLICATIONS
All manifestations of Lyme disease resolve over time, even in the absence of antibiotic therapy. Antibiotic therapy can hasten resolution of some (EM, arthritis), but not all (facial palsy, radiculitis) manifestations, and antibiotic therapy can clearly abort late manifestations. Coinfection with B. burgdorferi and either (or both) of Babesia microti or Anaplasma phagocytophilum occurs at different frequencies depending on the geographic location, and may alter the clinical presentation of Lyme disease in some patients. Some studies suggest more-severe disease in patients who are coinfected, but this remains uncertain.86-89
A small number of patients have symptoms that persist for years despite appropriate antibiotic therapy.
27
Up to 10% of patients with Lyme arthritis who are treated with appropriate antibiotics may have continued arthritis that persists for years.90,91 Arthritis in these patients does typically respond to immunosuppressive agents (methotrexate, anti–tumor necrosis factor therapies), which has led to suggestions that these patients may have an autoimmune syndrome. Molecular mimicry of borrelial antigens with host proteins has been proposed as one possible mechanism, but this remains unproven.92,93
There are many reports of patients who continue to have symptoms beyond a standard treatment course for Lyme disease of 2 to 4 weeks, including profound fatigue, depression, myalgia, polyarthralgias without arthritis, and paresthesias, as well as neurocognitive difficulties involving memory, concentration ( particularly auditory), and decreased mental flexibility (ie, impaired verbal fluency) after infection with B. burgdorferi.92 This syndrome is often referred to as posttreatment Lyme disease syndrome. The linkage of these symptoms with B. burgdorferi infection remains controversial and several large epidemiologic studies have shown that patients who have contracted Lyme disease are no more likely to suffer from these symptoms than persons in the general population.94-96 There are numerous studies demonstrating that longerthan-standard courses of antibiotics for Lyme disease do not improve long-term symptoms.97-99 However, prolonged courses of antibiotics for Lyme disease do have serious adverse effects.100,101 At this time, courses of antibiotics exceeding the standard duration are not recommended.
ETIOLOGY AND PATHOGENESIS
RISK FACTORS
RISK FACTORS
The risk of acquiring Lyme disease is almost completely dependent on exposure to the tick vector in areas where Lyme disease is prevalent. These areas are detailed in section “Epidemiology”. Avoidance of environments where ticks are likely to be found is an effective strategy to prevent disease. Other methods to reduce the risk of acquiring Lyme disease and coinfecting organisms are found in section “Prevention”.
PATHOGENESIS
PATHOGENESIS
B. burgdorferi sensu lato, the agent of Lyme borreliosis, belongs to the eubacterial phylum of Spirochaetales, which are vigorously motile, corkscrew-shaped bacteria. Recently, it has been proposed that B. burgdorferi sensu lato be renamed as Borreliella burgdorferi to distinguish it from relapsing fever Borrelia. Here we will continue to use the Borrelia designation. The borrelial genome is made up of a linear chromosome and more than 20 circular and linear plasmids, the largest number
3295
27
known for any bacteria.102,103 Some of the plasmids can be considered minichromosomes, as they are required for survival of the organism. Among the interesting characteristics of the organism are the large number of lipoproteins (more than 150) encoded by the genome. Borrelia lack biosynthetic machinery to produce many essential nutrients (eg, amino acids, fatty acids), suggesting that B. burgdorferi is highly dependent on its hosts for obtaining crucial nutrients.102,103
Ixodes ticks have a 2-year, 3-stage (larval, nymphal, and adult) life cycle. Larval ticks acquire B. burgdorferi organisms by taking a blood meal from an infected animal and maintain the infection during the subsequent molting to the nymphal and adult stages. B. burgdorferi remain dormant in the tick’s midgut between feedings.104 Each tick life stage takes 1 blood meal: larval ticks feed in late summer, nymphal ticks feed the subsequent spring and early summer, and adult ticks feed in the fall and early winter.104 The major reservoirs for B. burgdorferi are small rodents and birds that are fed on by larval and nymphal ticks. Adult ticks feed on larger mammals (eg, deer) that are not important reservoirs for B. burgdorferi but are an important feeding source for adult ticks. Reductions in deer populations can lead to significant decreases in the tick population.105
Humans are incidental hosts not important in maintaining B. burgdorferi in the wild. Most cases of human illness occur in the late spring and summer months when the nymphs are most active and human outdoor activity is greatest. Of clinical relevance, certain Ixodes ticks are vectors of other tick-borne illnesses in addition to Lyme disease: I. scapularis ticks in the United States and I. ricinus ticks in Europe may transmit B. microti (a red blood cell parasite), A. phagocytophilum (formerly referred to as the agent of human granulocytic ehrlichiosis) and Borrelia miyamotoi (a relapsing fever type Borrelia).86,102,103 I. ricinus in Europe and I. persulcatus in Asia are also vectors of tick-borne encephalitis virus, whereas I. scapularis transmits a related Powassan family virus (deer tick virus).106,107 Patients who have been bitten by Ixodes ticks may be coinfected with multiple organisms. B. burgdorferi rapidly adapt to different host environments by changing protein expression.104 There are multiple levels of control of gene expression but 2 of the major regulators of borrelial gene expression are the histidine kinase-1 (HK1)/response regulator-1 (Rrp1) pathway and the Response regulator-2 (Rrp2)/ RNA polymerase, sigma S (RpoS)/RNA polymerase, sigma N (RpoN) pathway. The HK1/Rrp1 pathway becomes activated as bacteria exit a mammalian host and enter a tick host. The Rrp2/RpoS/RpoN system becomes activated as the bacteria readies itself for entry into a mammalian host. Other regulatory factors such as BosR, a Fur-like transcription factor, and RpoD, a sigma factor, also help to control expression of genes upon tick feeding and transition to the mammalian host. Genes upregulated by Rrp2/RpoS/RpoN include those that may assist with immune evasion and cellular adhesion, as well as genes identified as essential for establishment of initial infection whose functions are unknown.
3296
At the tick bite site, the spirochete is injected along with tick saliva into the skin. The presence of the tick salivary protein, Salp15, on the surface of the spirochete is instrumental in helping the organism evade the mammalian immune system during early infection.108
After a latency period of 3 days to 1 month, the organism spreads through the skin. The immune response to the bacteria causes the characteristic EM rash. The bacteria enter the blood circulation and disseminate hematogenously. This generally occurs within days to weeks after infection. This dissemination is caused by both host and pathogen factors. For instance, it has been found that in North America, infection with certain strains of B. burgdorferi, such as OspC type A (RST 1), are particularly likely to result in hematogenous spread of the organism.109 Host proteases, such as plasmin and matrix metalloproteinases, may assist the bacteria as it moves through tissues. With its ability to establish long-term infection in mammalian hosts, several important factors in escaping immune defenses have been identified. Motility is a critical element of B. burgdorferi survival.110 B. burgdorferi move very quickly within tissues and have been clocked at up to 4 µM/s which is faster than neutrophils or macrophages can travel. Another important element is antigenic variation. B. burgdorferi have the ability to change the antigenic composition of a dominant protein expressed during mammalian infection, VlsE, through recombination into a portion of the gene from silent cassettes.106,107 Finally, B. burgdorferi have been shown to express proteins that bind a host complement inhibitory protein, factor H. Binding of factor H by specific B. burgdorferi has been shown in vitro to help it evade complement mediated killing.111-113 However, the importance of individual factor H–binding proteins in vivo is not known, possibly a consequence of redundancy among the proteins.
DIAGNOSIS
Physical findings, a history of potential exposure, known tick bites, or symptoms consistent with the typical multisystem presentation of Lyme disease can all be helpful in making a diagnosis. In the presence of classic EM or of Bannwarth syndrome, the diagnosis of Lyme disease can be made on clinical grounds alone. Diagnostic conundrums arise in presentations that involve other compatible skin, cardiac, neurologic, or musculoskeletal symptoms in the absence of a history of EM or tick exposure. In these cases, laboratory testing can aid in making the diagnosis.
DIRECT DETECTION OF BORRELIA BURGDORFERI
DIRECT DETECTION OF
BORRELIA BURGDORFERI
The gold standard for diagnosis of most infectious diseases is culture. However, the need for specialized media and the slow growth of the organism make it impractical in most clinical settings. B. burgdorferi can
be readily cultured from biopsies of EM and ACA,21 but rarely grows in synovial fluid in patients with Lyme arthritis or cerebrospinal fluid samples in patients with meningitis.7,114 Studies also have demonstrated that the organism can be recovered from the blood in up to 50% of untreated adult patients with multiple EM.115 However, cultures are generally insensitive in patients with extracutaneous manifestations of Lyme borreliosis, particularly in later-stage disease. PCR assays are very sensitive in detecting B. burgdorferi DNA in skin biopsy and synovial fluid specimens from patients with EM and Lyme arthritis, respectively.116 PCR testing for B. burgdorferi DNA has not been approved by the U.S. Food and Drug Administration (FDA), and its main use is in detecting B. burgdorferi in synovial fluid where Lyme arthritis is suspected. In this setting its sensitivity is between 70% and 85%,116-118 but a positive test does not necessarily mean there are living organisms.
SEROLOGIC DIAGNOSIS OF LYME DISEASE
SEROLOGIC DIAGNOSIS OF
LYME DISEASE
Immunologic diagnosis is the main laboratory modality used to support a clinical diagnosis of Lyme disease. In the United States, the FDA has approved more than 70 different immunoassays for Lyme disease—mainly enzyme-linked immunoabsorbent (ELISA) and Western immunoblot assays.119 ELISA tests use whole-cell lysates of B. burgdorferi sensu lato or purified B. burgdorferi antigens to capture either anti-B. burgdorferi immunoglobulin (Ig) G and/or IgM antibodies present in a given sample. Although relatively sensitive, ELISA tests are associated with a high rate of false-positive results.120,121 Patients with autoimmune diseases (lupus, rheumatoid arthritis), Epstein-Barr virus, bacterial endocarditis, and other tick-borne diseases appear to be at an increased risk for false-positive IgM serologic testing; syphilis, Helicobacter pylori, systemic lupus erythematosus, ehrlichiosis, and babesiosis cause false-positive IgG serologic testing.120,121 A newer ELISA test that uses only a small peptide of the constant region of B. burgdorferi VlsE protein appears to have greater specificity than traditional whole-cell ELISA testing. This test, also known as the C6 peptide test, measures only IgG antibody, but IgG antibody to the C6 peptide develops early in the course of disease and the sensitivity of the assay in patients with early disease has been equivalent to that seen with IgM whole-cell ELISA tests.121,122 Western immunoblot assays are more specific because they enable detection of antibodies to individual components of B. burgdorferi. Currently, there are no widely accepted standard tests or criteria for serodiagnosis of Lyme disease in either Europe or Asia, in part because of the presence of multiple strains of B. burgdorferi that have only partial antigen cross-reactivity. Because of its limitations, particularly high falsepositive results within the general population, serologic testing should be initiated based on the pretest
27
probability of disease and serve only to support a clinical diagnosis.7 It is most helpful in patients with an intermediate pretest probability of Lyme disease— namely those who reside in endemic areas and who present with signs and symptoms consistent with, but not diagnostic of, Lyme disease (eg, facial palsy, arthritis, or atrioventricular nodal conduction abnormalities in the absence of an EM lesion). Patients who reside in areas of high endemicity and have clear EM lesions should be diagnosed on clinical grounds alone without laboratory testing. Testing should be avoided in patients with low suspicion for disease (patients not living in endemic areas, or with nonspecific systemic symptoms, or after a tick bite) as the rates of falsepositive tests greatly outnumber true positive tests in this setting. Figure 179-13 shows one algorithm for the workup of patients presenting with an eruption suspicious for EM. Once the decision is made to obtain serologic testing, current recommendations are for 2-stage testing, starting with a highly sensitive ELISA test first.123 If the ELISA is negative, the likelihood of Lyme disease is low, and further testing is not generally recommended. However, if the test is positive or indeterminate, a Western immunoblot assay with high specificity should be used to confirm the results. The specificity of this 2-step approach is thought to be 99% to 100% in late-stage Lyme disease.119 If testing is negative early in the course of disease, the tests can be repeated in 3 to 4 weeks (antibiotic therapy, if given very early, may abort antibody development). It is important to note that in patients with disease untreated for longer than 1 month, IgM testing should not be performed. A positive IgM Western blot with a negative IgG Western blot in this setting is considered a negative result owing to the high false- positivity rate of IgM testing. Misuse or misinterpretation of the IgM tests is a major factor in over diagnosis of Lyme disease. Seronegativity in patients suspected of having late Lyme disease practically excludes the diagnosis.124 Finally, because IgG and IgM antibody titers may persist for years despite antibiotic therapy, persistent seropositivity is not in itself an indication of treatment failure, nor is it proof of recent infection or reinfection. Currently, there is no test that allows confirmation of successful clearance of the organism after treatment. Some recent studies suggest that the use of 2-step testing for Lyme disease may result in underdiagnosis of Lyme disease. The performance of traditional ELISA tests against nonisogenic genotypes of B. burgdorferi is reduced and results in lower sensitivity in patients infected with these strains early in the course of disease.119 The C6 antibody test appears to function better across genotypes of B. burgdorferi sensu stricto and with the European strains B. garinii and B. afzelii. Newer strategies using the C6 ELISA as the second step (dual enzyme immunoassay), replacing Western blot testing125 or using a C6 band in the second step Western blot IgG test126 show promising results but require further confirmation before they can be recommended.
3297
27
Approach to patient with erythema migrans
Solid or ring-shaped erythema
Consistent with EM (and endemic region or recent travel to endemic region) Possibly consistent with EM
Endemic region or recent travel to endemic region
No other sx or nonspecific sx >2 wka
Test
Nonendemic region and no travel to endemic region
Other symptoms suspicious for LDb
Observe Consider alternate dx
Treat Treat
1st step test (ELISA, C6)
Western blot
Treat
Observe Consider alternate dx Consider repeat test in 2-4 wk
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
The differential diagnosis of Lyme disease is dependent upon the specific manifestation. Early, nonspecific systemic symptoms (fevers, myalgia, headache, lymphadenopathy) have often been described as “viral-like” and cannot be distinguished from many infectious and noninfectious causes of these types of symptoms. EM is the most distinctive clinical manifestation of infection. The differential diagnosis for EM includes cellulitis or erysipelas, tinea, insect bites, fixed drug eruptions, and erythema multiforme. EM can usually be distinguished from other conditions by its size, onset, duration, local symptoms (eg, itching, pain at site) or presence of systemic symptoms. A newer inclusion in the differential diagnosis is another tickassociated disease called southern tick-associated rash illness (STARI). STARI is associated with the bite of a different tick, Amblyomma americanum, but the causative agent has not been identified. Most cases of STARI have occurred in the southern United States where Lyme disease is uncommon. However, as A. americanum has spread northward and Lyme disease has expanded southward, there is now overlap in the geographic regions where STARI and Lyme occur. STARI is typically a self-limited disease that does not require treatment.
3298
MANAGEMENT
Antibiotic treatment is indicated for all stages of Lyme disease, even though most manifestations resolve over time without therapy. Patients may not be asymptomatic at the time of completion of the antibiotic course but this is not an indication for extending length of therapy; symptoms generally continue to improve steadily over time. Of note, Jarisch-Herxheimer reactions (fevers, chills, and worsening arthralgia and
27
DIAGNOSTIC ENTITY DESCRIPTION DISTINGUISHING FEATURES TO DIFFERENTIATE FROM ERYTHEMA MIGRANS
Single Lesions
Cellulitis, erysipelas Erythematous painful, spreading rash, often with associated edema, most commonly on lower extremity Generally painful, seldom round or ovoid
Hypersensitivity to tick bite Red papule at bite site with surrounding pruritic erythema, edema, urticaria Typically pruritic, seldom exceeds 5 cm
Tinea corporis Erythematous, annular lesions Scaly, often with tiny vesicles at the border
Contact dermatitis Acute erythematous rash which may form papules, vesicles, scale; in chronic cases lichenification, fissuring and erosions may occur
Generally in areas exposed to jewelry, clothing, often with unusual patterns; often pruritic
Southern tick-associated rash illness (STARI) Clinically indistinguishable from erythema migrans rash Generally occurs in the South and Southwestern United States, but the geographic range is spreading to overlap with Lyme disease
Multiple Lesions
Urticaria Multiple, small, localized cutaneous edema with blanching erythema, generally pruritic Usually presents as a pruritic, erythematous wheal; lesions generally last for minutes to hours
Tinea corporis Erythematous, annular lesions Scaly, often with tiny vesicles at the border
Pityriasis rosea Multiple, small 2- to 4-cm oval lesions, often preceded by a larger “Herald patch” Scaly, often appear in a classic “Christmas tree” pattern, generally on the trunk
Erythema annulare centrifugum Expanding erythematous, annular, migrating lesions Generally chronic, with waxing/waning course
Erythema multiforme Circular, erythematous plaques, generally not exceeding
Acral distribution, may involve mucous membranes;
Erythema multiforme Circular, erythematous plaques, generally not exceeding 3 cm, sometimes with wheal with dark center; lesions often become confluent
Acral distribution, may involve mucous membranes; sometimes follows herpes simplex virus or Mycoplasma pneumoniae infection
3 cm, sometimes with wheal with dark center; lesions often become confluent
myalgia) are sometimes reported after the initial dose of antibiotics; the reaction is thought to be caused by host reaction to the dying organisms. The Infectious Disease Society of America has published guidelines for the treatment of all manifestations of Lyme disease,127 although many of the recommendations are based on expert opinion and not on rigorously controlled clinical trials. Treatment patterns differ in different countries, but no data suggest differences in either the efficacy of specific antibiotics or in the optimal duration of therapy between patients in North America and Europe. Treatment of all of the cutaneous manifestations of Lyme disease should initially be with oral antibiotics. Doxycycline is generally considered as first-line therapy, because it has excellent penetration into the CNS and is also effective against A. phagocytophilum, the agent of human granulocytic ehrlichiosis. Doxycycline should be used in children and pregnant women.128
Cefuroxime is an alternative first-line agent. These 3 agents have been found to be equally effective.129-131
Macrolides are second-line agents and should only be used in those who cannot tolerate the other agents. If macrolides are used to treat Lyme disease, close monitoring and follow up should take place.127 Duration of therapy for EM is generally recommended to be 10 to 14 days; a randomized, double-blinded, placebo-controlled study showed similar outcomes in patients with EM treated with either a 10-day or a 20-day course of oral doxycycline.131-133
sometimes follows herpes simplex virus or Mycoplasma pneumoniae infection
IV antibiotics (ceftriaxone, cefotaxime, or penicillin G) may be recommended for patients with cutaneous manifestations that are accompanied by neurologic disease (meningitis, encephalopathy) or high-degree heart block. However, multiple recent studies suggest that outcomes for treatment of neurologic disease with either oral doxycycline or IV ceftriaxone are similar. IV antibiotics are also sometimes used for patients with refractory ACA or arthritis.
PREVENTION
PREVENTION
Prevention of Lyme disease on a personal level can be approached in many ways, including avoidance of environments where ticks which can carry B. burgdorferi are likely to reside. However, in some areas of the United States with a high prevalence of Lyme disease, avoidance may not be possible, as ticks are found in and around human habitations.
3299
27
REPELLANTS AND ACARICIDES
The evidence for performing tick checks and bathing after engaging in activities where exposure to ticks is expected is mixed.135,136 However, these are simple and reasonable measures and removal of crawling or even attached ticks can prevent disease as it is thought that there is minimal transmission of spirochetes before
36 hours of attachment and feeding.127 Under certain conditions (see footnote for Table 179-5) if an attached tick is found, a single dose of oral doxycycline may be recommended as prophylaxis against the development of Lyme disease.137
There are several commercially available products marketed as insect repellants that have activity in preventing tick bites. The active ingredients, DEET
CLINICAL FINDING ANTIBIOTIC DURATION ALTERNATIVE REFERENCES
Prophylaxisa Doxycycline 200 mg × 1 dose
Watchful waiting 127,137
Skin Manifestations
Erythema migrans Doxycycline 100 mg by mouth twice daily Amoxicillin 500 mg by mouth three times daily Cefuroxime axetil 500 mg by mouth twice daily
10 days 14 days 14 days
Azithromycin 500 mg by mouth daily for 7-10 days 131-133
Acrodermatitis chronica atrophicans See regimen for erythema migrans 21 days
127
Borrelial lymphocytoma See regimen for erythema migrans 14-21 days Azithromycin 500 mg by mouth daily for 7 to 10 days 127
Musculoskeletal Manifestations
Lyme arthritis Doxycycline 100 mg by mouth twice daily 28 days Amoxicillin 500 mg by mouth 3 times daily × 28 days Cefuroxime axetil 500 mg by mouth twice daily × 28 days
Failure/recurrence after initial treatment Doxycycline 100 mg by mouth twice daily or Ceftriaxone 2 g IV daily
Cardiac Manifestations
Lyme carditis Nonhospitalized Doxycycline 100 mg by mouth twice daily Amoxicillin 500 mg by mouth 3 times daily Cefuroxime axetil 500 mg by mouth twice daily Hospitalizedb
Ceftriaxone 2 g IV daily until stable/discharge, then complete course with antibiotics listed above for nonhospitalized
Neurologic Manifestations
127
28 days
Amoxicillin 500 mg by mouth 3 times daily × 28 days Cefuroxime axetil 500 mg by mouth twice daily × 28 days
127
14-28 days
127
14-21 days 14-21 days
Cranial neuropathy/ radiculopathy Doxycycline 100 mg by mouth twice daily or 200 mg by mouth daily 14 days Amoxicillin 500 mg by mouth three × daily for 14 days Cefuroxime axetil 500 mg by mouth twice daily for 14 days
Meningitis Nonhospitalized Doxycycline 100 mg by mouth twice daily Hospitalizedc
Meningitis Nonhospitalized Doxycycline 100 mg by mouth twice daily Hospitalizedc
Ceftriaxone 2 g IV dailyd
Ceftriaxone 2 g IV dailyd
aProphylaxis should only be offered when all of the following conditions are met114: The attached tick can be reliably identified as an adult or nymphal Ixodes scapularis Tick that is estimated to have been attached for >36 hours Prophylaxis can be started within 72 hours
127, 144-148
14 days
Penicillin G 18 to 24 million units IV divided in 6 daily doses (every 4 hours)
14 days
Penicillin G 18 to 24 million units
127, 144-149
127, 144-149
IV divided in 6 daily doses (every 4 hours)
14 days
14 days
bEcologic information indicates that the local rate of infection of these ticks with Borrelia burgdorferi is >20%; and Doxycycline treatment is not contraindicated.
cHospitalization recommended for patients who are symptomatic, who have first-degree atrioventricular block with PR interval exceeding 30 msec, or with second- or third-degree atrioventricular block
dMany European studies have shown that oral doxycycline is as efficacious as IV beta-lactam therapy in treating Lyme meningitis. Some U.S. experts are similarly using oral doxycycline for this indication, although no U.S. studies have been reported at the time of the preparation of this manuscript. Consider deescalation to oral doxycycline upon discharge from the hospital to complete therapy.
3300
(N,N-diethyl-meta-toluamide), IR3535, paramenthane- 3,8-diol (PMD, which is refined from the oil of lemon eucalyptus), and picaridin are generally considered to have the greatest efficacy. However, because the duration of efficacy of each of these agents for repelling ticks is less than 2 hours, they require frequent reapplication. DEET has been in use for 70 years and has a strong safety record. DEET-treated clothing has been demonstrated to provide up to 92% protection against tick bites when applied to military clothing.138
Acaricides have potent acaricidal and insecticidal properties. The efficacy in actually reducing human infection with Lyme disease and other tick-borne illnesses through applying pyrethrins to the environment (such as spraying residential lawns) has been unclear. Recently, however, a large, randomized, double-blinded, placebocontrolled trial was conducted over 2 years in 3 states in the Northeast. The trial showed a 63% decrease in the number of ticks found, but no difference in tick-borne infections, based on both self-report and medical record review, by applying pyrethrins to the environment.139 Certain pyrethrins, such as permethrin, can be applied to clothing as an effective acaricide against some species of ticks which carry Lyme disease.140
VACCINATION
An effective human vaccine against Lyme disease was developed against the outer-surface protein A antigen and introduced in the United States in 1998. This was shown to reduce the risk of infection by approximately 76% in those who were vaccinated.141 However, a series of factors lead to its voluntary withdrawal from the market in 2002, a result of low demand.142,143 There is currently no human vaccine available against Lyme disease. Vaccination for dogs is currently available.
ACKNOWLEDGMENTS
This chapter is based on a previous version of the chapter written by Drs. Meera Mahalingam, Jag Bhawan, Daniel Eisen, and Linden Hu.
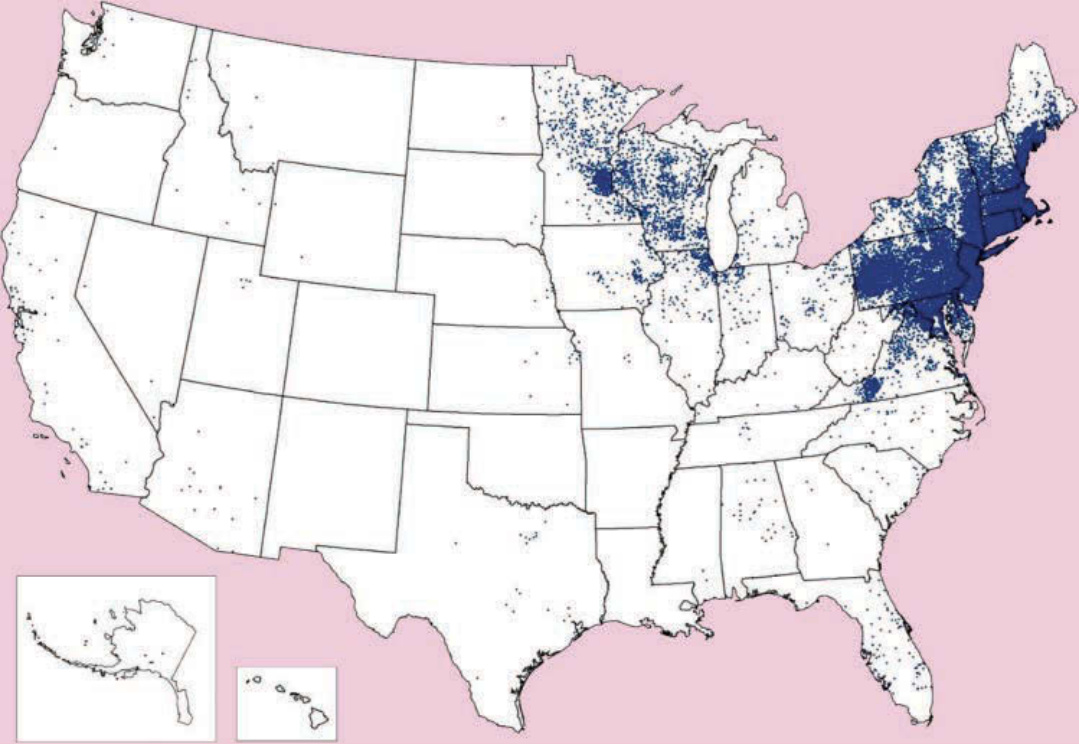
Figure 179-1 Cases of Lyme disease reported to Centers for Disease Control and Prevention in 2014. Cases shown indicate the county or residence of the infected individuals, and do not necessarily indicate where the infection occurred.
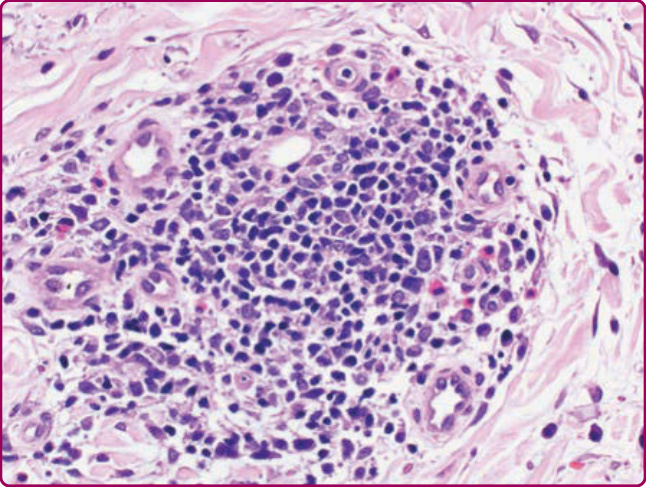
Figure 179-2 Histopathology of erythema migrans. Dense nodular perivascular lymphoid cell infiltrate with many plasma cells and few eosinophils in a biopsy from a later stage of erythema migrans. (Hematoxylin and eosin stain, ×40 magnification.)

Figure 179-3 Erythema migrans with the classic “bull’seye” appearance with a dark center, surrounding area of clearance, and a darker, advancing border. While this represents the classic appearance, it occurs only in a minority of cases.

Figure 179-4 Erythema migrans lesion. Note the relative central clearing. This lesion lacks the darker punctate center sometimes found in the classic “bull’s-eye” lesion. (From Clark RP. Tickborne infections. In: McKean S, Ross J, Dressler D, et al, eds. Principles and Practice of Hospital Medicine. 2nd ed. New York NY: McGraw-Hill; 2017, with permission.)

Figure 179-5 Erythema migrans. Note the lack of central clearance. This is the most common form of EM rash in the United States, appearing as an expanding, homogeneous, round or oval erythematous rash.

Figure 179-6 Disseminated erythema migrans. These are often smaller than the primary EM rash noted at the site of the tick bite.

Figure 179-8 Disseminated erythema migrans. The lesion on the left is elongated, almost linear in appearance, whereas the one on the right is almost elliptical, with a “bull’s-eye” morphology.

Figure 179-9 Acrodermatitis chronica atrophicans. Note the classical “tissue paper–like” cutaneous atrophy. (Image used with permission of Franc Strle, MD.)

Figure 179-10 Acrodermatitis chronica atrophicans with bluish-red discoloration and cutaneous atrophy as evidenced by the “tissue paper” appearance of the dorsum of the right hand. (Image used with permission of Franc Strle, MD.)

Figure 179-11 Borrelial lymphocytoma in a young adult with an erythematous nodulopapular lesion of the ear lobe. (Image used with permission of Franc Strle, MD.)

Figure 179-12 Borrelial lymphocytoma involving the left nipple. (Photograph used with permission of Franc Strle, MD.)
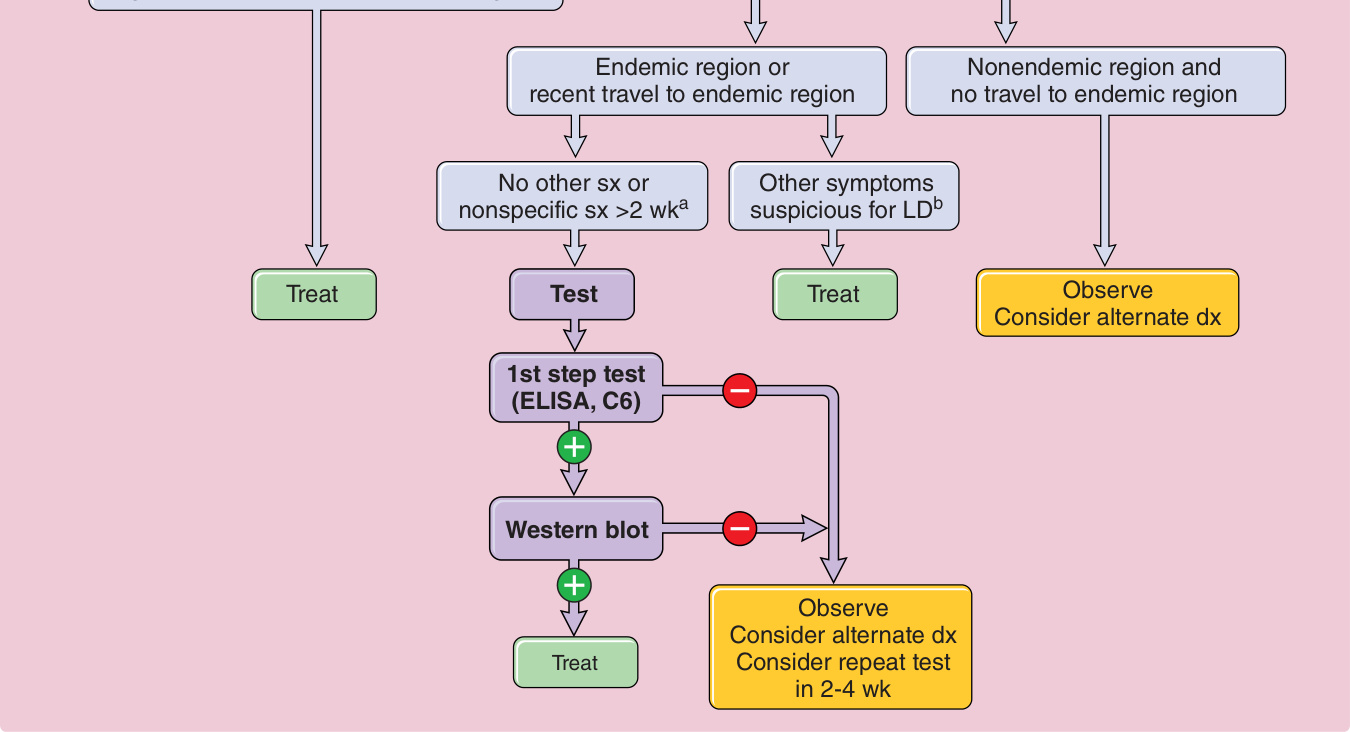
Figure 179-13 Approach to patient with erythema migrans (EM). aFever, chills, fatigue. bBell palsy, radiculoneuritis, meningitis, arthritis. dx, Diagnosis; ELISA, enzyme-linked immunosorbent assay; LD, Lyme disease; sx, symptoms.
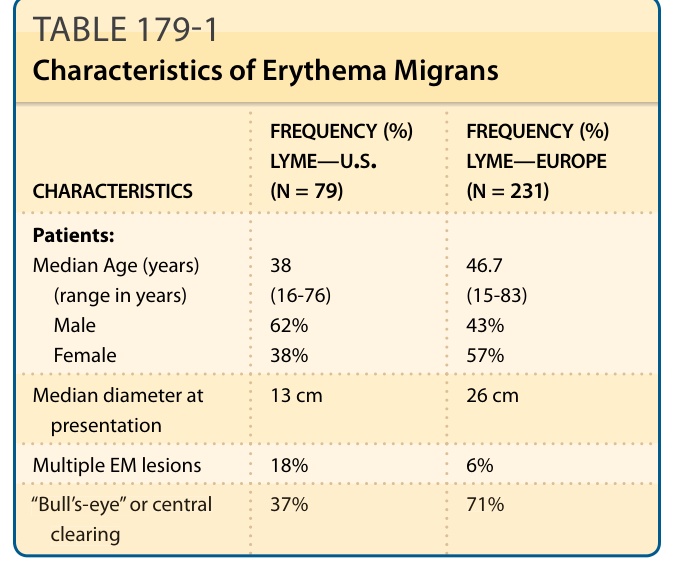
TABLE 179-1 Characteristics of Erythema Migrans
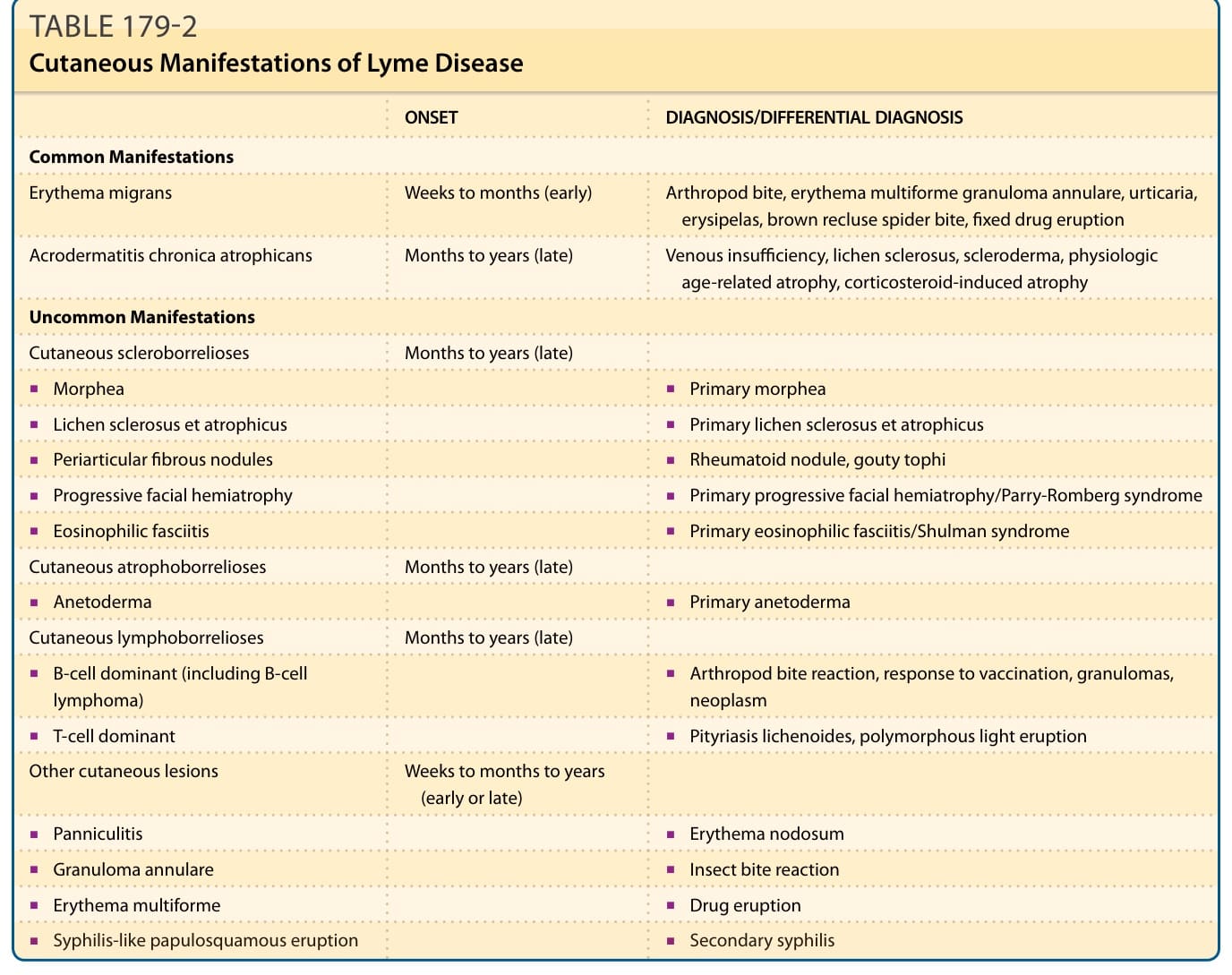
TABLE 179-2 Cutaneous Manifestations of Lyme Disease
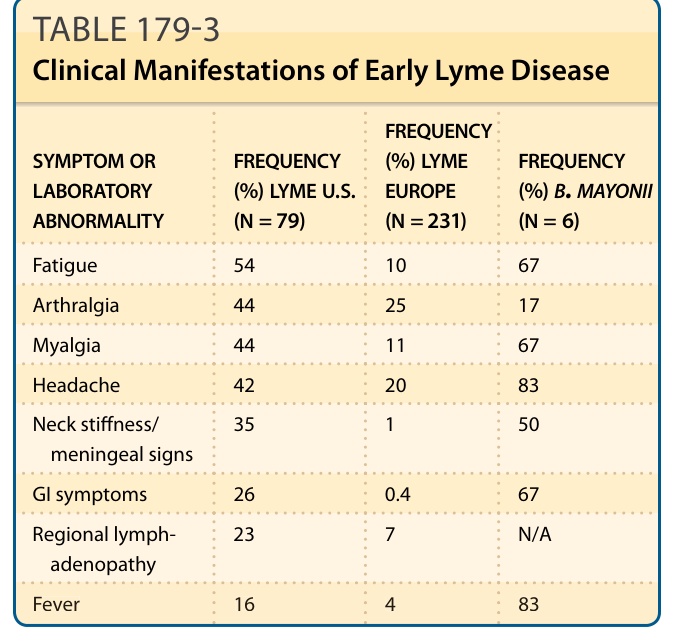
TABLE 179-3 Clinical Manifestations of Early Lyme Disease
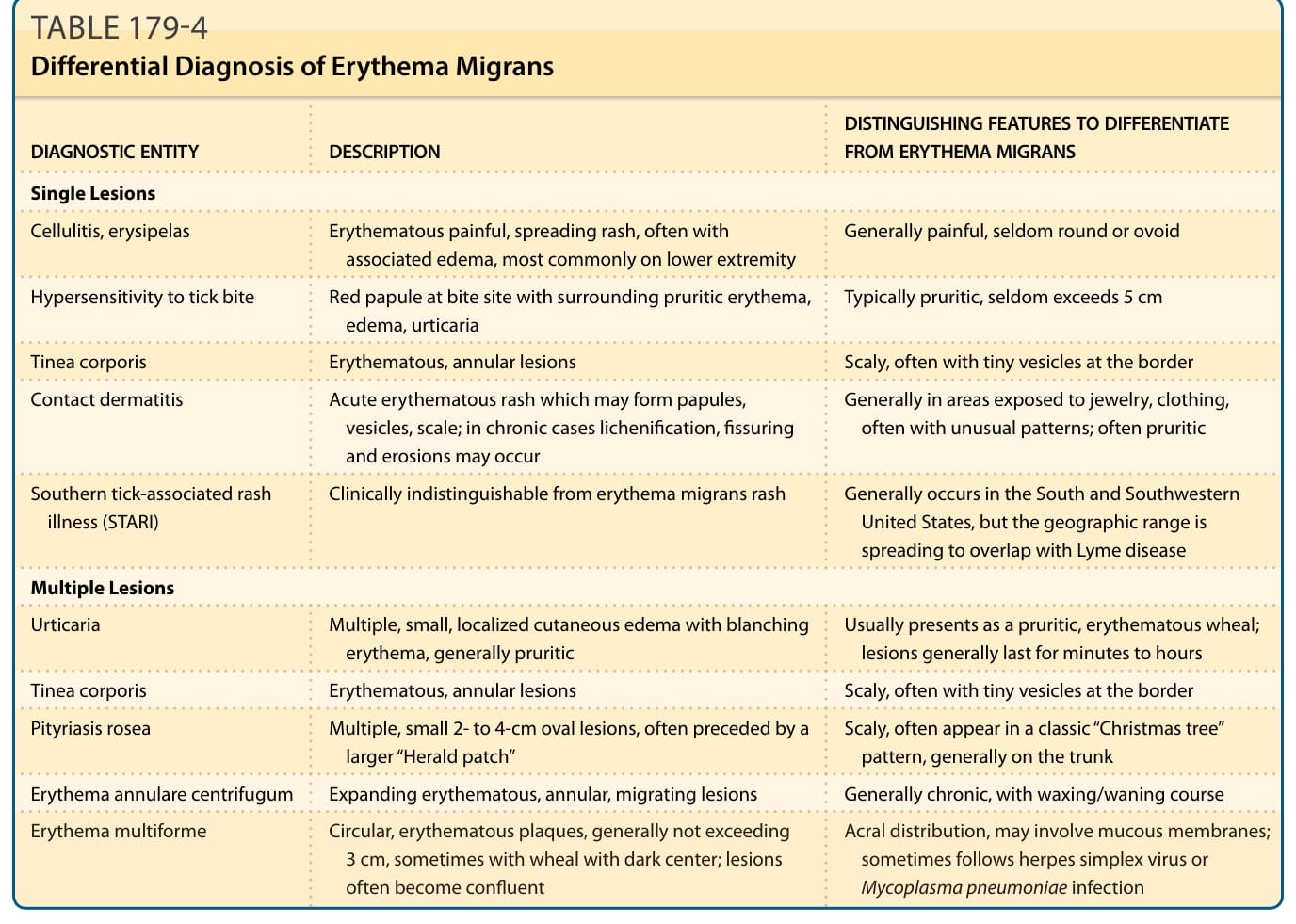
Table 179-4 lists the differential diagnoses for other cutaneous manifestations of Lyme disease. For many of the cutaneous manifestations of borreliosis, the clinical and histologic appearances are insufficient to make a definitive diagnosis. Obtaining a good clinical history is important. Lesions of ACA are notoriously overlooked or misinterpreted. In those with a relevant clinical history, the onset appears to be related to an untreated lesion of EM and/or neurologic manifestations. In one study, a history of EM months to years earlier on the same side was found in approximately 18% of patients.45 Serologic testing is typically positive in patients with ACA, but are more variable with other cutaneous manifestations.47 Direct identification of the spirochete in the affected skin by immunofluorescence, culture or PCR is often necessary to make a definitive diagnosis.
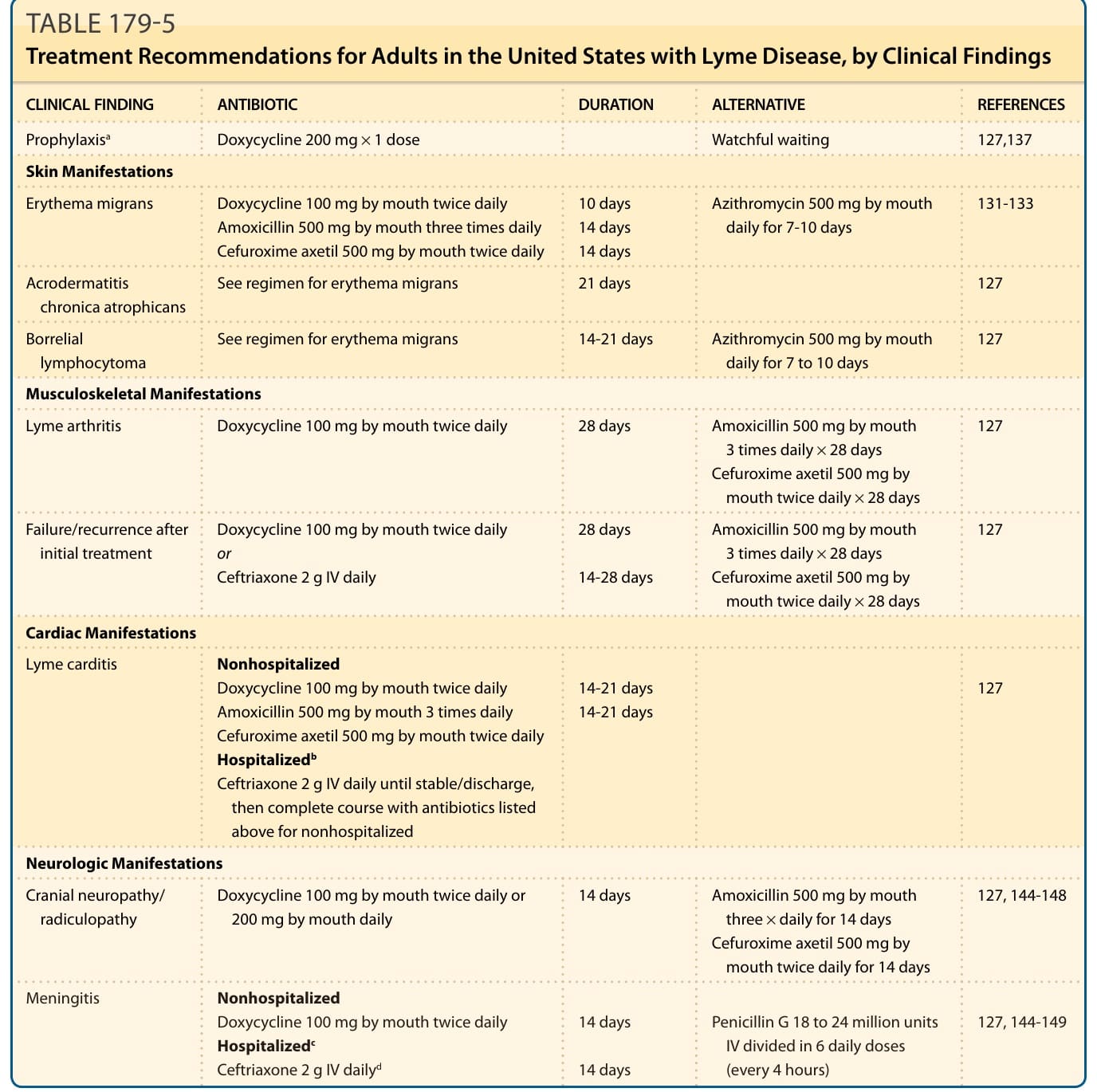
Table 179-5 outlines the choice of antibiotics and duration of treatment of the major cutaneous and noncutaneous manifestations of Lyme disease. Treatment of patients with nonspecific fibromyalgialike disease after infection with B. burgdorferi is controversial. There are multiple controlled trials showing no benefit to prolonging therapy with currently recommended oral or IV antibiotics.127,134