Helminthic Infections
27
AT-A-GLANCE
■ Helminthic infections are a major cause of morbidity and mortality, particularly in tropical and developing countries.
■ The majority of infected individuals has a low worm burden and is asymptomatic.
■ Dermatologic symptoms and cutaneous findings may be associated with or present features of many helminthic infections.
■ Returned travelers and immigrants from endemic areas may differ in the dermatologic manifestations of helminthic infection.
■ Migratory lesions, subcutaneous masses, papular eruptions, urticaria, and pruritus are the most common presenting symptoms of helminthic infections.
■ Cutaneous larva migrans is the most common helminthic dermatosis identified.
■ Recognition of skin findings or helminthic infections and an appropriate epidemiologic history can guide appropriate investigations and effective therapy.
Helminths (worms) are variably sized multicellular parasites that can infect a wide range of mammals, including humans. Those causing human disease belong to 3 groups: nematodes (roundworms), trematodes (flukes), and cestodes (tapeworms); trematodes and cestodes are collectively referred to as platyhelminths (flatworms). A variety of helminths can infect humans and cause cutaneous findings (Table 177-1).1,2
This chapter focuses on those helminths that are notable for causing dermatologic disease.
EPIDEMIOLOGY
Globally, helminthic infections are among the most common diseases of humans. However, the true prevalence of helminthiases is difficult to determine, particularly as the majority of infected individuals harbor relatively few worms and are asymptomatic. Large worm burdens and symptomatic disease affect a relatively small proportion of those who are infected. While some helminths such as Enterobius vermicularis and Toxocara canis are found worldwide, others are more geographically restricted. Most infections occur in developing tropical or subtropical countries, where environmental conditions are conducive to the completion of the life cycle of many helminths, and the requisite animal hosts and vectors for ongoing
transmission exist. In addition, the high population density, poverty, and poor sanitation commonly found in these areas further facilitate the transmission of these diseases. Knowledge of the geographic distribution of specific helminths is important for the clinician, and will help to direct appropriate investigations and management. Helminthic infections are less prevalent in temperate and northern climates, although some diseases are endemic even in these regions. In developed countries and colder climates, helminthic diseases are more often imported by travelers to or immigrants from endemic areas. Less frequently, helminthic infections in developed nations can be locally acquired (eg, trichinellosis resulting from improperly prepared food) or transmitted via person-to-person spread (eg, enterobiasis).
SKIN DISEASES IN TRAVELERS
SKIN DISEASES IN
TRAVELERS
Dermatologic disorders are the third most common illness in travelers.3 Observational studies over the past decade have consistently demonstrated that between 10% and 23% of travelers develop a dermatologic condition during or after travel.4-11 These figures cannot be generalized to all travelers, however, as studies included only individuals assessed in specialty (travel and tropical medicine) clinics and may also have been subject to geographic biases (because of the specific populations studied and/or the destinations of these individuals). Infections, including tropical skin diseases, are common causes of dermatoses among travelers. Insect bites, allergic reactions, and other rashes are among the most prevalent noninfectious dermatologic diagnoses in travelers. Of the helminthic skin infections, cutaneous larva migrans (CLM) is by far the most commonly reported in travelers and accounts for up to 25% of all skin diseases in this group.7-11 Most other helminthic infections that may be associated with dermatologic findings are relatively rare in travelers.
SKIN DISEASES IN IMMIGRANTS AND REFUGEES
SKIN DISEASES IN
IMMIGRANTS AND
REFUGEES
The prevalence of dermatologic conditions in immigrants and refugees has not been exhaustively studied,5,6,9,10 but in general they appear to occur no more frequently than in travelers. These observations are subject to the same biases noted above. The helminths that cause skin findings in this population, and the clinical presentations,
27
Nematodes (Roundworms)
Trematodes (Flukes)
Filariae
bLymphedema with filarial infections.
cDisseminated strongyloidiasis.
Cestodes (Tapeworms)
aFocal or localized edema.
may differ from those in travelers, however. For example, filarial infections are more commonly encountered in individuals who have resided in endemic areas for prolonged periods rather than in travelers, because they usually require repeated exposures to insect vectors for effective transmission to occur. Strongyloidiasis is also more prevalent in immigrants from endemic areas, particularly southeast Asia, and often presents with eosinophilia and few, if any, abdominal symptoms; most are asymptomatic. Onchocerciasis rarely occurs in short-term (at least 1 month) visitors to endemic areas and characteristically presents as an acute dermatitis with a hyperimmune response manifested by pruritus and rash (Fig. 177-1), despite low parasite loads. In contrast, infected immigrants more commonly have chronic onchodermatitis, with chronic skin changes, including atrophy, hypopigmentation, and lichenification, and onchocercal nodules (Fig. 177-2).
27
LIFE CYCLE AND TRANSMISSION OF HELMINTHS
LIFE CYCLE AND
TRANSMISSION OF
HELMINTHS
All helminths have complex life cycles that include maturation from eggs (or other infective forms) to larvae (or other immature forms) to adults. Human disease results from ingestion of eggs or other infective forms, or, alternatively, exposure of the skin to infective forms (larvae or cercariae) by direct contact or via the bite of an insect vector. Humans may be the primary hosts for some helminths (eg, Strongyloides stercoralis), or may be incidental or accidental hosts (eg, avian schistosomes, animal hookworm, and T. canis). Helminths that are well adapted to humans can mature from the infective stage into adult forms in the human host; infection generally persists for the life span of the adult worm, which in some cases can be for many years. In contrast, animal helminths cannot mature into adult forms in humans (who in this setting are therefore “dead-end” hosts), although infection can still cause tissue damage and clinical findings. In general, helminths do not multiply in the human host. Most helminths (with the notable exception of S. stercoralis) are incapable of completing an entire life cycle in the human host, and depend on the environment (eg, soil, water), plants, or other animal hosts or insects, for their survival. Consequently, transmission of infection requires the presence of appropriate environmental conditions, specific intermediate hosts (in whom only the asexual reproductive cycle occurs), and/or specific insect vectors, explaining in large part the localized geographic distributions of many helminthic diseases. Examples of helminthic diseases acquired by ingestion of infective forms (eggs or metacercariae) in contaminated food or water include Ascaris lumbricoides and Fasciola hepatica. In ascariasis, swallowed eggs are consumed, larvae are released within the GI tract, and migrate through the portal–systemic circulation to the lungs, from which they are swallowed. Skin disease, such as urticaria, may occur during the larval migration phase. Once in the GI tract, larvae mature into adult worms where sexual reproduction may take place; either eggs or adult worms can be shed in stool. Eggs must mature in soil before releasing infective larvae. In fascioliasis, infective metacercariae ingested on watercress excyst in the small intestine and migrate through the intestinal wall and peritoneum to their target tissue, the biliary tract, where they become adults. Again, skin findings typically occur as immature forms migrate. Eggs produced by adult flukes are passed in feces and become infective for humans only after maturation in a suitable (intermediate) snail host. Schistosomiasis results from penetration of intact skin by infective cercariae. Dermatologic findings in early disease manifest either at the time of cercarial penetration (swimmer’s itch or cercarial dermatitis), or during migration of immature forms (schistosomulae)
3253
27
from the skin and through tissue to the venous systems of their target organs (bladder or bowel, depending on the infecting species), where they mature into adults. Sexual reproduction leads to the release of eggs into the local circulation. En route to the bladder or bowel, eggs may sometimes become trapped in ectopic tissues, including skin, where they cause a granulomatous reaction. Eggs hatch in fresh water, releasing cercariae that must undergo further maturation in one of several intermediate snail hosts in order to infect humans. Infection can also result from penetration of intact skin by larvae, as exemplified by human hookworm infection. Larvae then migrate to the circulatory system where they are carried to the lungs, penetrate the alveoli and ascend the bronchial tree, are swallowed, and enter the GI tract. Skin findings may occur during larval migration to the lungs. Maturation into adult worms occurs in the small intestine, where they reproduce and release eggs into stool. Under the appropriate environmental conditions, eggs mature into infective larvae in soil. In contrast, larvae of animal hookworms (eg, Ancylostoma braziliense) cannot mature beyond the larval stage in humans and tunnel aimlessly in the skin before the infection eventually extinguishes itself. Larvae also can be introduced through intact skin by insect bites (eg, in filarial infections). The insect vector and the target tissue both vary according to the infecting species; cutaneous disease may be seen during either migration of larval forms through tissue, or as a result of adult worms in tissue. Microfilariae (larvae) released from mature adult worms are taken up by an insect during a subsequent blood meal, and then undergo maturation to infective forms within the insect before being introduced into another human host.
CLINICAL FEATURES
APPROACH TO THE PATIENT
APPROACH TO THE PATIENT
With the exception of CLM, most travelers and immigrants who present with dermatologic complaints will not have a diagnosis attributable to a helminthic infection. However, clearly these must be considered if the epidemiologic and exposure history and clinical findings are consistent with a helminthic infection, as these are treatable infections that have important clinical implications, such as disseminated strongyloidiasis in an immunocompromised host. As with all diseases of travelers and immigrants, a thorough history is essential in order to direct the clinician toward the correct diagnosis. The history should focus on aspects related to travel (or residence in endemic areas), general medical conditions, and medications. In addition, specific details of the dermatologic complaints must also be obtained. Finally, the clinician should be knowledgeable about (or know how to find out about) outbreaks of disease that may have been ongoing during an individual’s travel or residence in a given area.
3254
EXPOSURE HISTORY: TRAVEL AND AREAS OF RESIDENCE
The travel history (or history of residence in endemic areas) must be thorough in order to elucidate likely exposures to helminths. Specific details may be more readily obtained in recently returned travelers than immigrants, although immigrants are much more likely to be aware of local and endemic diseases (albeit often by local names). Details to be obtained include the exact dates, durations, and locations of travel or residence; purpose of travel; activities or occupations, inquiring specifically about those that would increase exposure to specific helminths; dietary intake; a history of similar signs and symptoms in other family members or fellow travelers; and the use of preventive measures. The exact destinations of travel (urban versus rural), not only the country or countries visited, are important to obtain. While some diseases may be endemic throughout a world region or area, the prevalence of others may vary greatly, sometimes within a given country. For example, onchocerciasis and loaisis are endemic in Central and West Africa, but generally not in other parts of Africa; and both infections are found only in rural areas, unlike bancroftian filariasis (Wuchereria bancrofti) that is often transmitted in urban centers. The risk of disease may not be present in all areas of a country in which a disease is considered to be endemic; for example, schistosomiasis is found in Brazil, but predominantly in the eastern and northeastern regions. Duration of travel or residence in an endemic area (and hence duration of exposure) is relevant for some diseases; schistosomiasis can be acquired after a single exposure to infective cercariae in freshwater, whereas filariasis is often acquired only after numerous bites, and therefore is rare among short-term travelers to endemic areas. The purpose of travel is also correlated with the likelihood of exposure to specific pathogens. Rural and adventure travelers are more likely to be exposed to helminthic infections than are business travelers, travelers whose itineraries are limited to urban areas, and those whose travels are of shorter durations. Certain activities and occupations will place individuals at greater risks of helminthic infections while abroad. Examples of common exposures and associated diseases include barefoot walking or walking in open shoes (sandals) (eg, CLM; strongyloidiasis); freshwater swimming in Africa (eg, schistosomiasis); and dietary indiscretions such as consumption of salads or undercooked or contaminated meat or fish (eg, ascariasis, echinococcosis, fascioliasis, gnathostomiasis). Although direct exposure to animals is not a risk factor for helminthic infections, the risk of CLM is greater in areas with a higher prevalence of stray dogs and cats. For those infections that are vector borne, such as filarial infections transmitted by mosquitoes, black flies and deer flies, the use of preventive measures such as appropriate clothing, insect repellent and bed nets can reduce the risk of infection.
GENERAL MEDICAL HISTORY
In addition to the travel history, a general medical history should be obtained. Skin findings may be related to underlying medical conditions, or to any associated treatment for these. The differential diagnosis of skin lesions in a returned traveler or immigrant also includes noninfectious disorders such as contact dermatitis (including to jewelry), drug eruptions, and photosensitivity reactions (that may be precipitated by travel-related medications such as doxycycline). A list of prescription and nonprescription medications or supplements should be obtained, in particular those that may have been started recently and/or prescribed abroad, as well as any recent use of topical medications or products.
DERMATOLOGIC HISTORY
The dermatologic history should include details regarding the initial presentation, morphology, and anatomic distribution of skin lesions; the progression and duration of lesions; time of onset relative to potential exposures; and any associated local and systemic signs and symptoms. While some manifestations of helminthic infections, such as urticaria or maculopapular eruptions, are nonspecific, the differential diagnosis of helminthic dermatoses can often be narrowed based on the description and morphology of the lesion(s) present. For
27
some diseases such as CLM, skin findings are virtually pathognomonic and the diagnosis can be established by history and careful examination of skin lesions, often without the need for additional investigations.
CUTANEOUS FINDINGS OF HELMINTHIC INFECTIONS
CUTANEOUS FINDINGS OF
HELMINTHIC INFECTIONS
Skin lesions caused by helminthic infections can assume a variety of morphologies. The most commonly encountered problem is that of migratory skin lesions. CLM is the most common cause of migratory lesions in general. Subcutaneous nodules, papular eruptions, and urticaria and pruritus are also common manifestations of helminthic infections.
MIGRATORY SKIN LESIONS
Migratory lesions can be caused by multiple helminths. Migratory lesions can be linear (serpiginous) or may be more ill-defined areas of erythema and swelling, and may be painless, painful, or pruritic. Table 177-2 lists the most common helminthic causes of migratory lesions, as well as characteristic features of these lesions. Serpiginous and linear lesions are most commonly caused by CLM (most frequently caused by A. braziliense
HELMINTH MORPHOLOGY OF LESION DESCRIPTION MOST COMMON LOCATION
Ancylostoma braziliense, Ancylostoma caninum Serpiginous (cutaneous larva migrans [CLM]) Typically 1 to 3 serpiginous lesions, 3 mm wide and up to 20 cm in length; intensely pruritic, may be vesicobullous; movement up to several cm per day
Ancylostoma duodenale, Necator americanus (human hookworm)
Feet, buttocks
Serpiginous Pruritic tracks from larval migration Feet
Dracunculus medinensis Localized area of edema or swelling with movement beneath
Moving mass may be seen just before emergence of adult worm through skin Feet
Fasciola hepatica Migratory subcutaneous swellings Erythematous, painful, pruritic subcutaneous nodules may have a migratory component; larval track marks also may be seen Abdomen, back, extremities
Loa loa Migratory subcutaneous swelling or serpiginous Migration of adult worm across conjunctivae or under skin Skin, eye
Gnathostoma spinigerum Serpiginous (CLM) Migration of larvae can cause creeping eruption; movement 1 cm per hour Trunk, upper body
Migratory subcutaneous swellings (eosinophilic panniculitis)
Intermittent single or multiple erythematous swellings; may be migratory, pruritic or painful; last 1 to 4 weeks, with recurrences in different anatomic areas after variable asymptomatic periods
Thighs
Paragonimus westermani Migratory subcutaneous swellings or nodules Firm migratory swellings or nodules, may be migratory; slightly tender and slightly mobile, up to 6 cm in diameter; swellings contain immature flukes
Lower abdomen, inguinal region
Spirometra mansonoides, others (sparganosis) Migratory subcutaneous swellings Slow growing, typically painful swellings that may be migratory; may be pruritic Abdomen, lower extremities
Strongyloides stercoralis
Serpiginous (larva currens) Movement at 5 to 10 cm per hour; intensely pruritic, transient,
Buttocks, groin,
Strongyloides stercoralis (larva currens) Serpiginous (larva currens) Movement at 5 to 10 cm per hour; intensely pruritic, transient, but recurrent Buttocks, groin, trunk, thighs
(larva currens)
but recurrent
3255
trunk, thighs
27
and Ancylostoma caninum; see also “Cutaneous Larva Migrans Syndrome”). Usually 1 to 3 (or more) erythematous, serpiginous, and intensely pruritic lesions caused by intradermal larval migration are present (Fig. 177-3). Serpiginous skin lesions in S. stercoralis infection, a pathognomonic manifestation of strongyloidiasis known as larva currens, typically present as recurrent, transient, and rapidly moving skin lesions (Fig. 177-4). Larval migration may occur at rates of 5 to 10 cm per hour, and the lesions usually disappear within hours only to recur over subsequent weeks to years. Linear migratory lesions also can be seen occasionally in human hookworm infection (Ancylostoma duodenale and Necator americanus) at the site of larval penetration, and in gnathostomiasis (usually relatively slow migration at 1 cm per hour). Linear migratory lesions also can be seen in loaiasis, and result from movement of the adult worm (not larvae) in tissue, typically under the skin or also across the bulbar conjunctivae (Fig. 177-5).
3256
Migratory subcutaneous swellings and nodules are characteristic of infections caused by Loa loa, Fasciola, Gnathostoma, and Paragonimus, and in sparganosis (Spirometra spp.). Lesions may be painful or pruritic. Migratory swelling resulting from the movement of adult worms is also seen in dracunculiasis, in which movement within a bullous, vesicular, or edematous lesion on the foot is often noted prior to eruption of the skin lesion and egress of the adult worm (Fig. 177-6). Since the implementation of a global eradication and drinking water monitoring program in endemic
countries, cases of dracunculiasis have decreased dramatically and the disease has almost been eliminated.
SUBCUTANEOUS NODULES AND MASSES
Subcutaneous and soft-tissue masses may have variable characteristics, including overlying erythema, pain or tenderness, and pruritus. They may be single or multiple, and fixed or mobile. Table 177-3 lists the more common etiologies of nodular lesions. Solitary nodules or masses are found in echinococcosis, filariasis caused by Brugia malayi and W. bancroftii (both of which may cause scrotal masses in men from lymphatic obstruction), dirofilariasis, and coenurosis (Taenia multiceps). Multiple nodules are typical of cysticercosis (Taenia solium infection), in which small, painless subcutaneous or intramuscular nodules are present, although single nodules can also occur. Subcutaneous cysticercosis, reported commonly in infected individuals in older case series, currently occurs in less than 10% of cases. Most other helminths that manifest
27
as subcutaneous nodules or masses may present with single or multiple lesions. Painless nodules are most characteristic of coenurosis, cysticercosis, dirofilariasis, echinococcus, and onchocerciasis. Painful nodules are seen in paragonimiasis and sparganosis. Transient painful lesions that resolve and subsequently recur in different anatomic areas are characteristic of Gnathostoma infection and loiasis. Fixed lesions are typical of cysticercosis, echinococcosis, and onchocerciasis.
PAPULAR AND MACULAR LESIONS
Papules and macules occur in relatively few helminthic infections (Table 177-4). Papular lesions may occur at sites of skin penetration by infective larvae or cercariae in CLM and schistosomiasis. In CLM, papules are typically in the feet or buttocks, similar to the distribution of migratory lesions. In schistosomiasis, exposure to infected freshwater (for avian or human schistosomes) or salt water (avian schistosomes) may cause pruritus, which is followed rapidly by a papular eruption in previously sensitized individuals. Chronic
HELMINTH DESCRIPTION OF NODULAR LESION MOST COMMON LOCATION
Brugia malayi Hydrocele/scrotal mass caused by lymphatic obstruction Scrotum
Dirofilaria spp. Single erythematous, well-defined, firm nodule or mass, usually 1 to 5 cm in diameter; usually asymptomatic but may be tender; rarely may be migratory
Head and neck, breasts, extremities, scrotum
Dracunculus medinensis Edematous lesion/mass may be seen just before emergence of adult worm through skin; movement underneath lesion due to movement of adult worm Feet
Echinococcus spp. Firm subcutaneous (or muscular) nodules or masses; usually single but may be multiple; may feel fluctuant; nontender. Rarely with fistulization and inflammation of skin (Echinococcus multilocularis). True cutaneous lesions are rare
Abdomen
Gnathostoma spinigerum Intermittent single or multiple erythematous swellings; may be migratory, pruritic or painful; last 1 to 4 weeks, with recurrences in different anatomic areas after variable asymptomatic periods
Trunk, upper body, thighs
Loa loa Calabar swellings–localized angioedema, 5 to 20 cm in diameter, usually lasting 2 to 4 days but recurrent; caused by migration of adult worms Eyelid, upper extremities, periarticular regions (especially knee, wrist)
Mansonella perstans Calabar swellings–localized swellings lasting 1 to 4 days, recurrent Face, upper extremities (especially forearms), hands
Onchocerca volvulus Well-defined, fixed, painless nodules containing adult worms in deep dermis and subcutaneous tissue Over bony prominences including skull (South America), ribs, iliac crest (Africa), others
Paragonimus westermani Firm swellings or nodules, may be migratory; slightly tender and slightly mobile, up to 6 cm in diameter; swellings contain immature flukes Lower abdomen, inguinal region
Spirometra mansonoides, others (sparganosis) Slow growing, typically painful swellings that may be migratory; may be pruritic Abdomen, lower extremities
Taenia multiceps, others (coenurosis) Solitary subcutaneous (or muscular) nodule, usually 2 to 6 cm in diameter; painless Trunk (especially intercostal regions), anterior abdominal wall; head, neck, extremities less commonly
Taenia solium (cysticercosis) Painless, fixed, well-circumscribed rubbery subcutaneous nodules in 50% of patients with cysticercosis; may be single or multiple; average size 2 cm in diameter
Trunk, extremities
3257
Wuchereria bancrofti Hydrocele/scrotal mass caused by lymphatic obstruction Scrotum
Wuchereria bancrofti Hydrocele/scrotal mass caused by lymphatic obstruction Scrotum
27
HELMINTH DESCRIPTION MOST COMMON LOCATION
Ancylostoma braziliense, Ancylostoma caninum (CLM) Pruritic erythematous papule(s) within days of larval penetration; may be vesicular; also papular larva migrans Feet, buttocks
Ancylostoma duodenale, Necator americanus (human hookworm) Ground itch: in sensitized individuals, pruritic papular lesions at sites of larval entry; may be vesicular Feet, hands
perstans, Mansonella streptocerca Multiple pruritic papules; hypopigmented and hyperpigmented macules and lichenification may be present Upper chest (M. streptocerca)
Onchocerca volvulus Acute: multiple pruritic papules, may become vesicular or pustular; may be erythematous and edema may be present Face, trunk, extremities
Chronic: intensely pruritic, flat papules (3 to 9 mm) or macules, may be hyperpigmented or lichenified Shoulders, buttocks, waist, extremities
Schistosoma spp. (avian) Erythematous papular or maculopapular lesions, may be vesicular or urticarial; intensely pruritic; onset within 24 hours of saltwater or freshwater exposure, lasts 1 to 3 weeks
Any surface exposed to water
Schistosoma spp. (human) Acute: erythematous papular and urticarial lesions in previously sensitized individuals; onset within hours of freshwater exposure, lasting 1 week Any surface exposed to water
Chronic: bilharziasis cutanea tarda; slightly pigmented, 2- to 4-mm, firm, pruritic,
Chronic: bilharziasis cutanea tarda; slightly pigmented, 2- to 4-mm, firm, pruritic, oval papules or papulonodular lesions, may be verrucous or polypoid; may appear in crops; caused by granulomatous reaction to eggs in skin
Trunk, especially
Trunk, especially periumbilical region; buttocks, genitalia
oval papules or papulonodular lesions, may be verrucous or polypoid; may appear in crops; caused by granulomatous reaction to eggs in skin
papular lesions (bilharziasis cutanea tarda) may be present in chronic schistosomiasis. Papular lesions also may be manifestations of acute or chronic infection with Onchocerca volvulus, and have been reported in disseminated and chronic strongyloidiasis.
HELMINTH COMMENTS
Nematodes (Roundworms)
periumbilical region; buttocks, genitalia
URTICARIA AND PRURITUS
Pruritus (Table 177-5) may be present in the absence of skin findings, either as a primary symptom of infection (eg, filariasis caused by Mansonella perstans or O. volvulus),
Ancylostoma braziliense, Ancylostoma caninum Pruritus and urticaria after skin penetration and during larval migration
Ancylostoma duodenale, Necator americanus (human hookworm) Pruritus and urticaria after skin penetration and during larval migration
Ascaris lumbricoides Pruritus and urticaria during larval migration (with Loeffler syndrome)
Enterobius vermicularis Pruritus ani
Filariae
Loa loa Pruritus and urticaria
Mansonella ozzardi, Mansonella perstans, Mansonella streptocerca Pruritus occurs early, may be only symptom
Onchocerca volvulus Pruritus and urticaria in acute or chronic disease
Gnathostoma spinigerum, others Pruritus and urticaria during larval migration
Strongyloides stercoralis Pruritus and urticaria after skin penetration and during larval migration, including chronic infection; pruritus ani
Toxocara canis, Toxocara cati Pruritus and urticaria during larval migration
Trichinella spiralis Pruritus and urticaria during larval migration
Trematodes (Flukes)
Fasciola hepatica Urticaria during migration of adult flukes
Paragonimus westermani Urticaria during larval migration
Schistosoma spp. (human and avian) Transient urticaria with pruritus within 24 hours of exposure to cercariae; urticaria with
Schistosoma spp. (human and avian) Transient urticaria with pruritus within 24 hours of exposure to cercariae; urticaria with Katayama fever (acute schistosomiasis)
3258
Katayama fever (acute schistosomiasis)
or before the onset of skin lesions (eg, schistosomiasis). Pruritus is a common feature of many helminthic infections, with the noteworthy exceptions of lymphatic filariasis (eg, caused by Brugia spp. and W. bancrofti) and tapeworm infections. Pruritus ani is characteristic of strongyloidiasis and enterobiasis (pinworm infection). Urticaria are often present in the acute phase of infection, during which larvae or other immature forms actively invade human tissues. Helminths that infect humans by penetration of skin may cause a local urticarial rash at the sites of penetration. Migration of immature forms in the circulation may cause a generalized hypersensitivity reaction; urticaria is common during this phase of infection by many helminths (see Table 177-5). Chronic spontaneous urticaria, recurrent episodes of wheals, and/or angioedema lasting 6 weeks or longer, is associated with parasitic infections, including T. canis and Anisakis simplex.12
LOCALIZED EDEMA
Although edema or swelling may be an associated feature of many helminthic skin lesions, localized edema may is highly suggestive of the presence of certain infections. Eyelid edema in particular may be seen in gnathostomiasis and loiasis (Calabar swelling), and violaceous periorbital edema is characteristic of trichinosis. Limb edema is highly suggestive of lymphatic filariasis (caused by Brugia spp. and W. bancrofti). Rarely, limb edema (“gros bras camerounais”) may occur with acute onchocerciasis.13
CHANGES IN SKIN TEXTURE OR PIGMENTATION
Hypopigmentation of skin can be a feature of chronic infection caused by O. volvulus (“leopard skin”), M. perstans, and Mansonella streptocerca. Hypopigmented macules are the most common cutaneous findings in streptocerciasis. In onchocerciasis, depigmentation is characterized by perifollicular pigmentation within macular or minimally depressed areas, with yellow-brown hypopigmentation, and is particularly noticeable in dark-skinned individuals. Hyperpigmentation can also occur with mansonellosis caused by M. streptocerca, as well as in chronic schistosomiasis and onchocerciasis. Lichenification is a feature of onchocerciasis (“sowda” in Arabic), and to a lesser extent mansonellosis; hyperpigmented plaques eventually coalesce and become lichenified over time, particularly over the lower extremities and in young adults in Yemen and Sudan. Verrucous lesions may be seen in chronic schistosomiasis (bilharziasis cutanea tarda). Ichthyosis also may be present in chronic onchocerciasis.
OTHER CUTANEOUS MANIFESTATIONS
Petechiae may be present with trichinellosis and are frequently seen in disseminated strongyloidiasis, in
27
which they are particularly prominent on the trunk. Vesicles or bullae may be seen at the site of larval skin penetration in up to 15% of patients with CLM, in human hookworm infection, and occasionally in dracunculiasis, onchocerciasis, and strongyloidiasis. Ulcers are uncommon findings in most helminthiases, with the exception of dracunculiasis; multiple ulcers are common. Ulcerative genital lesions, particularly in women, may occasionally be present in schistosomiasis and tend to occur more often with acute disease (eg, in travelers). Erythema nodosum is rare in helminthic infections, but has been described as a clinical finding with hookworm infection, visceral larva migrans, sparganosis, and lymphatic filariasis. It also has been reported in 1 patient in conjunction with ascariasis,14 although erythema nodosum in this patient may also have been caused by concomitant Chlamydia pneumoniae pneumonia. Erythema multiforme has been reported in CLM. Eosinophilic panniculitis has been documented in gnathostomiasis and toxocariasis. Eosinophilic cellulitis (Wells syndrome) may occur in ascariasis, onchocerciasis, and toxocariasis. Eosinophilic folliculitis has been rarely described in CLM and in toxocariasis. Exfoliative dermatitis of the affected limb may occur during the resolution phase of acute adenolymphangitis or following secondary bacterial-mediated cellulitis in W. bancrofti infection.
INTERVAL BETWEEN EXPOSURE AND ONSET OF SYMPTOMS
The time of onset of skin disease (and other key symptoms) relative to travel and likely exposures can be helpful in establishing a diagnosis (Table 177-6). Some infections, such as cercarial dermatitis in schistosomiasis or CLM, become evident within hours to days of exposure, whereas others may not present until months to years after infection.
PROGRESSION AND DURATION OF SKIN LESIONS
Skin lesions resulting from helminthic infections can persist for variable durations (see Table 177-6). For helminths that cause infection by penetration of skin, local dermatologic findings last only for a short time during infection by human helminths, but may persist longer with animal helminths (eg, CLM). During the chronic phase of infection, however, the duration of cutaneous manifestations varies depending on the infecting helminth. For infections in which skin findings are the result of inflammatory reactions to larvae (eg, onchocerciasis) or eggs (eg, schistosomiasis) in tissues, clinical manifestations can persist for the life span of the adult worms, which in some cases may be years. Even with appropriate therapy for chronic infections, chronic skin changes may not resolve completely.
3259
27
SPECIES TYPICAL INTERVAL BETWEEN EXPOSURE AND ONSET OF CUTANEOUS SYMPTOMS (RANGE) TYPICAL DURATION OF SYMPTOMS (RANGE)
Nematodes (Roundworms)
Ancylostoma braziliense, Ancylostoma caninum Usually 1 to 5 days, typically within 1 month 2 to 14 weeks, rarely longer (up to 2 years)
Ancylostoma duodenale, Necator americanus (human hookworm) Ground itch: 1 to 2 days Urticaria: 1 to 3 weeks 1 to 2 weeks
Ascaris lumbricoides Urticaria: 10 to 14 days Several weeks
Dirofilaria spp. Subcutaneous nodules: several months
Dracunculus medinensis Edema, vesicle or bulla formation, ulceration with worm protrusion: 1 year Several weeks
Enterobius vermicularis Pruritus ani: weeks to months 30 to 45 days (self-limited) or until treated
Filariae
Brugia malayi, Brugia timori Hydrocele: years Years
Loa loa Calabar swelling, urticaria: >6 months to years Adult worm migration: years Several days to weeks Years
Mansonella ozzardi, Mansonella perstans, Mansonella streptocerca Pruritus, dermatitis, hypopigmentation: unknown Years
Onchocerca volvulus Onchodermatitis: months to years Onchocercoma: years Years Years
Wuchereria bancrofti Hydrocele: years Years
Gnathostoma spinigerum, others Creeping eruption: 1 to 2 days Migratory masses: 3 to 4 weeks Up to 3 months 1 to 2 weeks, but recur for years
Strongyloides stercoralis Larva currens: months to years Chronic urticaria, larva currens: years Petechiae, purpura (in disseminated disease): variable
Hours, but recur for years Years —
Toxocara canis, Toxocara cati Urticaria: weeks to months Years
Trichinella spiralis Eyelid edema, petechiae: 1 to 3 weeks 2 to 3 weeks
Trematodes (Flukes)
Fasciola hepatica Urticaria: 6 to 12 weeks (with abdominal pain, fever, weight loss) Several weeks to months
Paragonimus westermani Urticaria: 2 days to 2 weeks Subcutaneous nodules: 2 to 3 weeks Several weeks Years
Schistosoma spp. (human and avian) Swimmer’s itch: <24 hours Urticaria: 2 weeks to months Bilharzia cutanea tarda: years
Cestodes (Tapeworms)
Days to 3 weeks 2 to 10 weeks Years
Echinococcus granulosis, Echinococcus multilocularis Years Years
Spirometra mansonoides, others (sparganosis) 20 days to 3 years Years
Taenia multiceps, others (coenurosis) Months to years Years
Taenia solium (cysticercosis) Variable—months to years Years
Taenia solium (cysticercosis) Variable—months to years Years
NONCUTANEOUS FINDINGS
NONCUTANEOUS FINDINGS
Apart from the skin, symptoms of helminthic infections tend to most frequently involve the respiratory, GI, and neurologic systems, and the eye. Disease may also occur in many other tissues as a consequence of aberrant migration of larvae and adult worms. Because the skin lesions of many helminthic infections tend to occur in acute (larval) infection, and nondermatologic symptoms often result from the presence
3260
of adult helminths or their products of reproduction, it is important to appreciate that skin findings often precede other manifestations of disease. However, dermatologic and nondermatologic symptoms may coexist in some acute infections, as well as in chronic infections.
PULMONARY DISEASE
Loeffler syndrome, a hypersensitivity syndrome consisting of dyspnea, wheezing, cough, and fever, typically
results from larval migration through lung tissue and may be seen in infection caused by human hookworms, Ascaris, and Strongyloides. Because these symptoms are a result of larval migration, they begin shortly after infection and may occur coincidentally with an urticarial rash. Loeffler syndrome typically lasts for 1 to 2 weeks. Diffuse pulmonary infiltrates and nodules may be seen during larval migration in acute schistosomiasis (Katayama syndrome) that occurs several weeks after exposure.15
Other pulmonary symptoms are generally not simultaneous with dermatologic symptoms, occurring after larvae have matured into adult forms. Hemoptysis is uncommon; among helminthic infections it is most frequently a feature of paragonimiasis, but also can be a symptom of echinococcal disease and disseminated strongyloidiasis. Pulmonary nodules may be seen in dirofilariasis, a zoonotic filariasis transmitted by mosquitoes, in conjunction with subcutaneous swellings and ocular lesions. Pleural effusions also occur rarely, and in helminthic infections are more likely to be eosinophilic. The most common parasitic etiology is Paragonimus, but effusions also can be caused by a variety of other helminths.16
GASTROINTESTINAL DISEASE
Abdominal pain is most commonly seen in ascariasis and human hookworm infection, after dermatologic manifestations have resolved, and in strongyloidiasis. Abdominal pain in strongyloidiasis is typically epigastric. Because S. stercoralis can complete its entire life cycle within the human host, larvae and adult worms may coexist simultaneously, and thus abdominal symptoms may be coincident with larva currens and pruritus ani. Right-upper-quadrant abdominal pain also may be a manifestation of acute fascioliasis, caused by larval penetration of the hepatic capsule; urticaria also may be present during this phase. Diarrhea can be a symptom with heavy Strongyloides or Schistosoma infections, and rarely hookworm infection. Hepatitis may be seen in acute fascioliasis. Liver masses or abdominal masses may be the presenting symptom of echinococcosis; hypodense liver lesions are commonly seen in fascioliasis as well. Hepatomegaly is one of the classic findings of visceral larva migrans (toxocariasis), typically occurring in children and usually in conjunction with fever, respiratory symptoms (wheezing) and occasionally urticaria. Hepatomegaly also has been reported as a finding of several other helminthiases including fascioliasis. Granulomatous hepatitis may also cause hepatomegaly, and is most commonly encountered in schistosomiasis (the result of granuloma formation around eggs in the periportal circulation), but also can be a feature of ascariasis (eggs), strongyloidiasis (larvae), and toxocariasis (larvae). Biliary disease may be a result of either occlusion of the biliary tract by adult worms or flukes (eg, ascariasis, fascioliasis) or from compression of the biliary tract by a mass lesion (eg, echinococcosis). Hepatic fibrosis can be a complication of chronic schistosomiasis.
27
NEUROLOGIC DISEASE
Helminthic infections most commonly affecting the CNS include neurocysticercosis and strongyloidiasis. Seizures, typically focal but sometimes generalized, are the most common presentation of neurocysticercosis. Neurocysticercosis should be considered in the presence of subcutaneous cysticercosis. The clinical presentation of neurocysticercosis is determined by the number, size, and location of intracranial lesions, as well as the viability of cysts (dying cysts produce more inflammation and are more likely to be associated with seizures). Globally, neurocysticercosis is among the most common causes of seizure disorders. Seizures may also occur with infection caused by Schistosoma spp. and Paragonimus, and in sparganosis. Meningitis can be seen in strongyloidiasis. S. stercoralis larvae may be visualized in cerebrospinal fluid, but more commonly meningitis is a result of Gram-negative bacteremia caused by enteric organisms that are carried across the bowel mucosa during larval penetration in disseminated disease; abdominal petechiae or purpura are often present. Eosinophilic meningitis or meningoencephalitis may be a feature of cysticercosis, gnathostomiasis, paragonimiasis, schistosomiasis, toxocariasis, angiostrongyliasis, baylisascariasis, and, less commonly, strongyloidiasis, among others.17 Mass lesions or cysts can be caused by Echinococcus spp., Paragonimus, Taenia spp. causing coenurosis, and Toxocara. In schistosomiasis, intracranial infection is most commonly associated with Schistosoma japonicum infection and may result from the development of granulomas around ectopic eggs. Other CNS manifestations of helminthic infections, including brain abscesses, transverse myelitis and myelopathy, and intracranial hemorrhage, may occasionally be seen.
OCULAR DISEASE
Although ocular involvement is most frequently associated with infections caused by Loa loa and O. volvulus (river blindness), disease involving the conjunctiva, sclera, and all chambers of the eye can be occasional features of many helminthic infections. Onchocerciasis is a major cause of blindness worldwide. Ocular symptoms and findings are often related to the presence of larvae or microfilariae migrating through and causing inflammatory reactions in various chambers of the eye and the retina. Onchodermatitis is common in chronic infection, and skin findings and eye disease may be present simultaneously. Ocular disease is also one of the most frequent presentations of sparganosis. Conjunctivitis is the typical ocular manifestation of gnathostomiasis and sparganosis, but also has been reported in a variety of other infections. Keratitis is most commonly present in onchocerciasis and coenurosis. Uveitis is characteristic of onchocerciasis and schistosomiasis. Retinitis or chorioretinitis may be present in onchocerciasis and toxocariasis. Migration of adult worms through the eye may be seen in loiasis and dirofilariasis, and less commonly in fascioliasis and gnathostomiasis,
3261
27
and gives rise to a foreign-body sensation in the eye. Granulomatous nodules in the eye or conjunctivae may be present in toxocariasis, schistosomiasis and M. perstans infection. Eyelid swelling (Calabar swelling) may be the result of infection by Loa loa and M. perstans.
LYMPHADENOPATHY
Lymphadenopathy is an uncommon finding in helminthic infections, with the exception of filarial infections. Regional lymphadenopathy can be present with lymphatic filariasis (caused by infection with Brugia spp. and W. bancrofti), as well in loiasis, M. streptocerca infection, and onchocerciasis. Generalized lymphadenopathy may be present in lymphatic filariasis, and in acute schistosomiasis (Katayama fever).
OTHER SYMPTOMS
Fever and urticaria can be features of Loeffler syndrome, which may be the initial manifestation of infection due to A. lumbricoides, human hookworm, S. stercoralis, and in toxocariasis. Fever in acute trichinellosis usually occurs in conjunction with other symptoms including myalgias, cough, facial edema, and splinter hemorrhages in the nails. Fever is also a finding in acute schistosomiasis (Katayama fever) and fascioliasis, and also may be present in other helminthiases, typically during larval migration. Gram-negative sepsis may occur in disseminated strongyloidiasis, a result of translocation of enteric bacteria as Strongyloides larvae penetrate the intestinal lumen; a petechial or purpuric eruption, particularly on the trunk, has been well reported in disseminated strongyloidiasis (see section “Strongyloidiasis”).
COMPLICATIONS
COMPLICATIONS
Secondary complications including excoriation and secondary superinfection are not uncommon, especially when pruritic lesions are present. Skin changes, such as lichenification and pigment changes, as noted above, may be persistent. Other significant complications of specific cutaneous helminthic diseases are discussed below.
ETIOLOGY AND PATHOGENESIS
Cutaneous manifestations can be seen at every phase of the helminth life cycle in humans: by larvae or cercariae during skin penetration; during larval migration and tissue invasion; and because of the presence of eggs and adult worms in skin and soft tissues. Skin lesions also may occur during either early (acute) or chronic infection. The pathogenesis of skin lesions in helminthic infections is varied. Direct penetration of skin may lead to a localized immune response, as seen in CLM or cercarial dermatitis. Migration of helminths can cause a generalized immune response (urticaria, maculopapular
3262
eruptions), particularly from migration of larvae or immature forms (eg, with Ascaris or Toxocara infection); a local inflammatory reaction to adult worms or eggs may also develop, as occurs with cutaneous nodules caused by O. volvulus and in schistosomiasis and cysticercosis, or subcutaneous swellings caused by Loa loa and Gnathostoma. Skin changes can also result from disruption of the normal skin structures because of lymphedema, as with filarial infections. Finally, illdefined systemic immune reactions, such as erythema nodosum or erythema marginatum, rarely reported manifestations of several helminthic infections, also may be present. Skin findings of helminthic infections do not generally result from hematogenous spread of parasites, in contrast to many bacterial and viral infections. Helminths induce a dramatic expansion of the T helper 2 (Th2) lymphocyte subset, with elevated levels of immunoglobulin E (IgE), peripheral eosinophilia, and an increase in tissue mast cells. It is unclear whether these Th2-derived responses are important in the protective immune response against the parasite or are responsible for immune-mediated pathology, or both.12 Despite high levels of IgE and other features of Th2 cell activation, allergic responses are rarely observed in infected individuals except during the invasive phase of infection, when pruritus and/or urticaria may occur. Infected hosts have evolved elaborate immune evasion strategies to permit long-lived helminthic infections, including the induction of tolerance to parasite antigens.
DIAGNOSIS
The definitive diagnosis of most helminthic infections rests on identification of 1 or more of the various stages of the helminth (eg, larvae, eggs, adult worms) in tissue specimens, blood, or excretions (stool or urine). Occasionally, adult worms may be observed during medical procedures (eg, endoscopy or surgery). In many helminthic infections causing skin disease, however, cutaneous findings occur during the larval migration phase, and hence precede the presence of adult worms and the production of eggs or larvae that may not be detectable for weeks or months. The diagnosis of a helminthic infection is therefore often difficult during the penetration and acute phase of the disease; the diagnosis may be suspected because of associated epidemiologic and clinical findings. In chronic infection, the diagnosis can be established based on the identification of parasite eggs or larvae, or occasionally adult worms, but the sensitivity of stool examination can also vary depending on the parasite.
SUPPORTIVE STUDIES
SUPPORTIVE STUDIES
Results of routine blood tests, including eosinophilia, are neither sensitive nor specific for diagnosing helminthic infections. While most hematologic
and biochemical tests are nonspecific, the presence of eosinophilia can suggest specific diseases when combined with clinical findings and/or the exposure history, and should prompt additional investigations.18,19
Diagnosis of helminthic infections also may be aided by results of ancillary investigations (eg, chest radiography; abdominal imaging).
LABORATORY TESTING Eosinophilia: Eosinophilia, defined as an absolute eosinophil count of greater than 500 eosinophils per mm3, is not typical of infections caused by most pathogens other than helminths; helminth antigens are effective stimuli for inducing eosinophilia. Levels of eosinophils in the blood can be affected by host factors, including the response to other bacterial, viral, or fungal coinfections (which lower eosinophil counts), the use of systemic steroids (which lower eosinophil counts), and an immunosuppressed state. In helminthic infection, eosinophil counts vary according to the stage of infection and the infecting helminth. Tissue invasion is the key factor in the development of eosinophilia. For example, eosinophilia is not a feature of intestinal lumen-dwelling helminths, except during the larval migration phase for those helminths in which this occurs; in contrast, helminthic infections in which adults, larvae, or eggs persist in tissues are typically associated with eosinophilia. Eosinophil counts are usually normal during the penetration phase and reach their highest levels (often markedly elevated) during the invasive phase of the cycle. Eosinophilia often accompanies the urticarial rash during the invasive stage of infection; thereafter, the eosinophil count often decreases slowly and may fluctuate more or less above the normal value during the chronic phase of infection. However, the detection of helminthic infection in returned travelers who present with asymptomatic eosinophilia is often very low. A transient hypereosinophilia may be also observed approximately 10 days after the start of effective antihelminthic treatment, and eosinophilia may persist for one to two months after successful helminth eradication.
Additional Laboratory Tests: Other laboratory tests may be abnormal but may not aid with establishing a specific diagnosis. Other than leukocytosis, which may reflect only the presence of eosinophilia, hematologic studies obtained when skin lesions are present are unlikely to be helpful. Evidence of disseminated intravascular coagulation may be present in disseminated strongyloidiasis. Iron-deficiency anemia is a feature of established hookworm infection, but occurs well after the resolution of cutaneous disease. Biochemical testing may reveal abnormal liver function tests and enzymes in acute fascioliasis and toxocariasis, when urticaria may be present. Granulomatous
27
DISEASE COMMENTS
Ascariasisa
Marked eosinophilia in early infection
Ascariasisa
Marked eosinophilia in early infection
Cysticercosis Dirofilariasis Dracunculiasis Fascioliasisa
Cysticercosis Dirofilariasis Dracunculiasis Fascioliasisa
Marked eosinophilia in early infection Eosinophilia may be marked especially in loiasis and with pulmonary symptoms
Marked eosinophilia in early infection Eosinophilia may be marked especially in loiasis
Filariasisa
Filariasisa
and with pulmonary symptoms
Gnathostomiasisa
Gnathostomiasisa
Hookworm infection (CLM)a
Hookworm
Can be marked during larval migration
Can be marked during larval migration
infection (CLM)a
Paragonimiasisa
Paragonimiasisa
Marked eosinophilia in early infection Especially during early infection (Katayama fever)
Marked eosinophilia in early infection Especially during early infection (Katayama fever)
Schistosomiasisa
Schistosomiasisa
Sparganosis Strongyloidiasisa
Sparganosis Strongyloidiasisa
Eosinophilia may be moderate in chronic infection
Eosinophilia may be moderate in chronic infection
Toxocariasis (VLM)a
Toxocariasis (VLM)a
aMarked eosinophilia (eosinophil count >3000/mm3) may be present. CLM, cutaneous larva migrans; VLM, visceral larva migrans.
hepatitis may be associated with a disproportionately elevated alkaline phosphatase. Most biochemical tests are otherwise nonspecific and are of limited use in determining the correct diagnosis.
Serology: Serologic assays are available for many helminthic infections, but vary greatly in their sensitivity and specificity. Their utility is also limited by cross-reactivity of tests among the various helminths, especially with filarial antibodies. Another significant limitation to serologic testing relates to the delayed appearance of antibodies after acute infection. Antibody production typically begins during the invasive (acute) phase of disease, when skin lesions are clinically apparent, but titers may be negative at this time. Serologic tests may not become positive for 2 months or more after the onset of infection. Although the presence of antibodies often supports or establishes the clinical diagnosis, antibodies may reflect prior infection and do not necessarily imply active or acute disease, and titers often remain positive for years after helminthic infections have been eradicated. The exception is strongyloidiasis, where a decrease in antibody titer is often used as a test of cure.
Molecular Testing: Molecular testing by polymerase chain reaction is highly sensitive and specific, and may be especially useful in the diagnosis of mixed infections.20,21 However, its use is limited by the technical requirements of testing and cost, and it is not readily available in many diagnostic laboratories in North America.
Pathology: Additional diagnostic tests may include pathologic examination of tissue specimens or blood (for microfilariae), or microscopic examination of other specimens (eg, bronchoscopy specimens in disseminated strongyloidiasis).
3263
27
RADIOLOGIC INVESTIGATIONS
RADIOLOGIC
INVESTIGATIONS
Symptomatic patients with Loeffler syndrome and acute schistosomiasis will typically have diffuse patchy infiltrates or nodules on chest radiographs; urticaria may be present at this time. Radiologic findings consistent with acute respiratory distress syndrome may be present in disseminated strongyloidiasis. Chest radiographs also may be abnormal in paragonimiasis (cystic lesions, pleural effusion). Pleural effusions may be present in infection caused by other helminths, as previously noted. A solitary pulmonary nodule may be noted in dirofilariasis. Abdominal imaging (ultrasonography, CT, or MRI) should be directed by abdominal symptoms and is suggestive of a diagnosis in relatively few helminthic infections. Septated hepatic cysts are characteristic of cystic echinococcosis, whereas in alveolar hydatid disease hepatic lesions are usually solid. Hepatic masses or nodules (hypodense lesions up to 10 mm in size) may be visualized on ultrasonography or CT scan in fascioliasis. Tracts or tunnels representing migration of immature flukes through the liver also may be noted in fascioliasis. Imaging studies of the CNS are diagnostic in neurocysticercosis, in which CT or MRI usually reveals parenchymal cysts and occasionally intraventricular or subarachnoid cysts. In cerebral gnathostomiasis, worm-like tracts have been noted.
MANAGEMENT
Treatment varies depending on the specific diagnosis. Recommended and alternate therapies for treatment of helminthic infections causing cutaneous findings can be found in recent reviews and guidelines.22
SPECIFIC HELMINTHIC DISEASES OF MAJOR IMPORTANCE
The sections that follow describe key features of the most important helminthic infections. CLM syndrome and enterobiasis (pinworm infection) are encountered relatively frequently by clinicians in developed countries. In comparison, filariasis and schistosomiasis are uncommon, but may lead to chronic dermatologic complications. Strongyloidiasis, also seen relatively infrequently, must be considered in the appropriate clinical context; failure to diagnose and treat the infection may have significant clinical consequences for immunocompromised patients in particular, in whom disseminated strongyloidiasis carries a significant mortality risk. For these reasons, these 5 infections are described below.
3264
CUTANEOUS LARVA MIGRANS SYNDROME
CUTANEOUS LARVA
MIGRANS SYNDROME
The terms CLM and creeping eruption are often used interchangeably when referring to disease caused by animal hookworms. Even though CLM is the most common cause of creeping eruption,23 technically CLM refers to a syndrome in which the larvae of any animal nematode infect humans and in which the infected human is a deadend host. These nematodes include animal hookworms (mostly from dogs and cats), Gnathostoma species, and agents of zoonotic filariases including Spirurina type X, Pelodera strongyloides, and zoonotic Strongyloides species. By definition, CLM syndrome does not include diseases in which creeping eruption is the result of: (a) nonlarval forms of parasites (eg, dracunculiasis, loiasis); (b) larval forms of human nematodes such as S. stercoralis (larva currens); or (c) larval forms of trematodes such as Fasciola gigantica. Creeping eruption refers to the clinical finding (sign) of a migratory serpiginous lesion, but does not denote the etiology of the lesion. Hookworm-related CLM (creeping verminous dermatitis, sand-worm eruption, plumber’s itch, duck hunter’s itch), is most commonly caused by animal hookworms, and in particular A. braziliense. Other skinpenetrating hookworm larvae that produce similar disease include A. caninum, Uncinaria stenocephala (hookworm of European dogs), and Bunostomum phlebotomum (hookworm of cattle). A. caninum causes eosinophilic enteritis as well as cutaneous disease. Cats and dogs are hosts for Ancylostoma ceylanicum and A. caninum. Clinically, the hallmark of CLM is a creeping eruption. The different helminthic diseases causing creeping eruption can often be distinguished based on the epidemiologic and exposure history, the characteristics of the cutaneous trail(s) (location, number, width and length, rate of movement) (see Table 177-2), and the duration of symptoms (see Table 177-6), in addition to other clinical and laboratory findings. The correct diagnosis is required for appropriate treatment.
EPIDEMIOLOGY
Hookworm-related CLM is widely distributed but is most commonly found in tropical and subtropical areas, especially the southeastern United States, Caribbean, Africa, Central and South America, India, and Southeast Asia. Contact with sand or soil contaminated with animal feces is required for infection to occur; infection can be prevented by avoiding skin contact with fecally contaminated soil.
CLINICAL FEATURES
Infection results from direct skin penetration by infective larvae of animal hookworms. Larvae migrate up to several centimeters a day, usually between the stratum germinativum and stratum corneum, and induce a localized eosinophilic inflammatory reaction.
27
DISEASE PRIMARY THERAPY (ADULT DOSES) ALTERNATE THERAPY (ADULT DOSES) COMMENTS
Cutaneous larva migrans Albendazole 400 mg by mouth daily × 3 days Ivermectin 200 µg/kg daily × 1 to 2 days Thiabendazole, topical 10% Albendazole, topical
Enterobiasis Albendazole 400 mg by mouth once Mebendazole 100 mg once Pyrantel pamoate 11 mg/kg (maximum: 1 g) once
Treatment should be repeated 2 weeks after the first treatment, regardless of the agent used. Treatment of household contacts recommended
Filariasis Endosymbiotic Wolbachia bacteria may play a role in filarial development and host response for all filariasis except loiasis. Doxycycline 100 to 200 mg by mouth daily × 6 to 8 weeks can reduce Wolbachia and block microfilariae production Antihistamines or glucocorticoids may be required to reduce the allergic reaction secondary to microfilariae disintegration during the treatment of filarial infections In patients with microfilariae in the blood, diethylcarbamazine (DEC) may cause severe allergic or febrile reactions. When microfilariae are present, it is advisable to start with a low dose and escalate (eg, 50 mg on day 1; 50 mg thrice daily on day 2; 100 mg by mouth thrice daily on day 3; then full dose)
Brugia malayi, Brugia timori DEC 2 mg/kg by mouth thrice daily × 12 days In chronic disease, elevation of the affected limb, compression stockings, good skin care, treatment of superficial fungal and bacterial infections are important. Surgical treatment can sometimes be considered
Loa loa DEC 3 mg/kg by mouth thrice daily × 21 days Surgical removal of adult worm may be required
Mansonella ozzardi Ivermectin 200 μg/kg by mouth once Ivermectin reduces microfilarial burden. DEC is ineffective. Doxycycline may be effective
Mansonella perstans Doxycycline 100 to 200 mg daily × 6 to 8 weeks DEC, mebendazole. and ivermectin are ineffective
Mansonella streptocerca DEC 2 mg/kg by mouth thrice daily × 12 days Ivermectin 150 μg/kg by mouth once
Onchocerca volvulus Ivermectin 150 μg/kg by mouth once, then every 6 months until asymptomatic
DEC must not be used as rapid killing of worms can cause ocular side effects
Wuchereria bancrofti DEC 2 mg/kg by mouth thrice daily × 12 days Single-dose combination of albendazole 400 mg plus either ivermectin 200 µg/kg or diethylcarbamazine 6 mg/kg is effective in suppressing W. bancrofti microfilaremia. Chronic disease: see Brugia spp.
Schistosomiasis
Systemic steroids (eg, prednisone) may be helpful during acute disease
Schistosoma haematobium, Schistosoma intercalatum, Schistosoma mansoni
Praziquantel 40 mg/kg/day in 1 or 2 doses × 1 day Oxamniquine 15 mg/kg by mouth once (S. mansoni only)
Oxamniquine unavailable in the United States, and is generally not as effective as praziquantel, but has been effective in some areas when praziquantel is less effective. In East Africa, increase oxamniquine dose to 30 mg/kg. In Egypt and South Africa, increase oxamniquine dose to 30 mg/kg/day × 2 days. Oxamniquine is contraindicated in pregnancy
Schistosoma japonicum, Schistosoma mekongi Praziquantel 60 mg/kg/day in 2 or 3 doses × 1 day
Strongyloidiasis Ivermectin 200 μg/kg/day × 2 days Albendazole 400 mg by mouth
In immunocompromised patients or
Strongyloidiasis Ivermectin 200 μg/kg/day × 2 days Albendazole 400 mg by mouth twice daily × 7 days In immunocompromised patients or disseminated disease, it may be necessary to prolong or repeat therapy. Combination therapy (ivermectin plus albendazole) may be indicated in disseminated disease
DEC, diethylcarbamazine.
twice daily × 7 days
disseminated disease, it may be necessary to prolong or repeat therapy. Combination therapy (ivermectin plus albendazole) may be indicated in disseminated disease
3265
27
In contrast to human hookworm infection, animal hookworm larvae cannot mature beyond the larval stage in humans; they are unable to invade deeper tissues and die after days to months. Typical skin lesions appear 1 to 5 days after exposure. The characteristic lesion of hookworm-related CLM is an erythematous, raised, and vesicular, linear, or serpentine cutaneous trail that progresses at a rate of 2 to 3 cm per day (see Fig. 177-6). Vesicular, papular or bullous lesions may be seen at the site of larval skin penetration in up to 15% of patients with CLM (Fig. 177-7). Lesions are approximately 3 mm wide and may reach 15 to 20 cm in length. They can be single or multiple, are intensely pruritic, and may be painful. The hookworm larvae advance a few millimeters to a few centimeters daily. The most common anatomic sites (usually 3 to 4 cm from the penetration site) include the feet (see Fig. 177-3) and buttocks (Fig. 177-8), although other
3266
sites may be affected. Excoriation and impetiginization are uncommon (10% of cases). Skin lesions usually last between 2 and 8 weeks, but have been reported to last for as long as 2 years. Systemic signs and symptoms (wheezing, dry cough, urticaria) are rare. A less frequent but well-reported clinical presentation is that of hookworm folliculitis, consisting of 20 to 100 eosinophilic follicular papules and pustules confined to a particular area of the body, usually the buttocks. Patients with folliculitis usually also have creeping eruption. Papular lesions without CLM (papular larva migrans) are a less-common presentation. Other cutaneous signs related to the subcutaneous migration of helminth larvae have been occasionally described, such as urticaria and panniculitis.
DIAGNOSIS
The diagnosis of hookworm-related CLM is based on clinical findings. Hookworm folliculitis also can be diagnosed clinically when creeping eruption is also present; if not, skin biopsy may be required. Histopathologic findings include larvae trapped within the follicular canal, the stratum corneum, or the dermis, together with an inflammatory eosinophilic infiltrate.24 Skin scrapings in patients with folliculitis may reveal live and dead larvae when examined by light microscopy with mineral oil.
MANAGEMENT
Both albendazole (400 mg by mouth daily for 3 days) and ivermectin (200 µg/kg daily for 1 or 2 days) are effective therapies for hookworm-related CLM25,26 (see Table 177-8). Treatment of hookworm folliculitis may require repeated treatments. Topical therapy with thiabendazole, 10% albendazole, or ivermectin also may be used, but may be less effective than oral therapy. Thiabendazole is often not readily available. Because larvae have usually migrated beyond the end of the visible skin lesion and their location cannot be reliably determined, surgical excision or cryotherapy is not recommended.
ENTEROBIASIS (PINWORM INFECTION)
ENTEROBIASIS (PINWORM
INFECTION)
EPIDEMIOLOGY
Enterobiasis (threadworm, pinworm, or seatworm infection; oxyuriasis) is caused by E. vermicularis. It is among the most widely distributed helminthic infections and is found worldwide. Transmission is by the fecal–oral route; infection results from ingestion of E. vermicularis eggs (eg, by contact with contaminated fomites or via contaminated fingers) and rarely by inhalation and ingestion of aerosolized eggs in dust. The highest rates of infection are among children. Infection can be prevented by treatment of infected cases and good personal hygiene.
CLINICAL FEATURES
Nocturnal anal and perianal pruritus is the primary clinical feature. The worm may be seen around the anus. The skin may become impetiginized, and cellulitis may occur as a complication. Women may rarely develop vulvovaginitis; vulvar granuloma and an association with Bartholin cysts also have been described. Nondermatologic extraintestinal manifestations are rare but have been reported. Epidemiologically, enterobiasis is often associated with an intestinal protozoan, Dientamoeba fragilis, which may produce GI upset. A recent study detected D. fragilis DNA on washed pinworm ova.27
DIAGNOSIS
The diagnosis is established by identification of E. vermicularis eggs in the perianal area, most effectively by the sticky-tape method. A piece of tape, sticky side out, can be attached to a wooden tongue depressor and firmly pressed against the perianal skin immediately on waking in the morning, before defecation or bathing. The tape is removed and placed sticky side down on a slide, and examined under a microscope. Sensitivity of this method is 70% with 3 specimens and increases to almost 100% with 7 specimens. Eggs are found in stool in only 10% to 15% of infections. Occasionally, the adult worm (white, up to 4 mm in length) is found in the perianal area, vulva, vagina, or underclothes. When ectopic sites are involved, the parasite may be identified in tissue sections.
DIFFERENTIAL DIAGNOSIS
The differential diagnosis includes strongyloidiasis, atopic dermatitis, contact dermatitis, and neurodermatitis.
MANAGEMENT
Enterobiasis is self-limited if reinfection does not occur. Treatment with 1 dose of albendazole 400 mg, mebendazole 100 mg, or pyrantel pamoate 11 mg/kg, is effective (see Table 177-8). Treatment of household members is also recommended, as household transmission is common. Treatment should be repeated once, 2 weeks after the first course of therapy, as medications are relatively ineffective against developing larvae and newly ingested eggs. Specific personal hygiene measures are also important for eradication of infection; these include wearing underwear and pajamas to sleep, bathing in the morning, keeping fingernails short, changing underwear daily and bedsheets weekly, and dusting the environment to remove eggs.
FILARIASIS
FILARIASIS
Filarial infections have been broadly grouped into 3 categories of disease based on the location of disease:
27
lymphatic, cutaneous, and body cavity. Morbidity is almost entirely attributable to those species that cause lymphatic disease, and to a lesser extent cutaneous disease. Body cavity infection, caused by Mansonella ozzardi, is usually asymptomatic and is not discussed further.
EPIDEMIOLOGY
Lymphatic filariasis is caused mainly by W. bancrofti (bancroftian filariasis), which causes 90% of disease, and B. malayi (Malayan filariasis), which accounts for only 10% of all cases.28 Infection caused by Brugia timori is rare. Lymphatic filariasis is widely distributed in both urban and rural areas of tropical and subtropical areas, with the largest number of infections occurring in India, South Asia, East Asia, and the Pacific Islands, and sub-Saharan Africa. W. bancrofti is also endemic in northern parts of South America (Guyana, Surinam, and some coastal regions of Brazil). In developed countries, infections are seen primarily in immigrants and persons with prolonged visits to endemic areas. Infection is transmitted to humans by mosquitoes, and can be prevented by avoidance of mosquito bites. The incubation period is usually 5 to 18 months, during which time microfilariae migrate to the lymphatic system, mature into adults, mate, and release microfilariae (larvae); occasionally symptoms develop within 3 months of exposure. Lymphatic filariasis is first acquired in childhood, often with as many as one-third of children in endemic areas infected before the age of 5 years.29 The characteristic symptoms typically occur years after infection and the prevalence of clinical disease increases after age 20 years in endemic areas. Adult worms live an average of 10 to 15 years, and microfilariae probably 6 to 12 months. Cutaneous filariasis is caused by Loa loa, M. perstans, M. streptocerca, and O. volvulus. Loiasis is endemic in rural areas of Central and West Africa, affecting an estimated 3 to 13 million residents. Loa loa is transmitted by the day-biting Chrysops fly; infection can be prevented by avoiding bites from Chrysops in endemic areas, diethylcarbamazine chemoprophylaxis, and treatment of infected humans to reduce the source of parasites. Symptoms usually begin an average of 24 months after exposure, but can begin as early as 4 months or as late as a decade or more after infection. The adult worm can live longer than 20 years in the human host. Infection caused by both M. perstans and M. streptocerca is often asymptomatic. M. perstans is endemic in sub-Saharan Africa, as well as parts of Central and South America, where it is transmitted by Culicoides midges. Like lymphatic filariasis, infection during childhood is common, and reinfection may occur.30 In highly endemic areas, the prevalence of infection may be as high as 80%. M. streptocerca is endemic in forested areas of West and Central Africa. Transmission is also by infected midges. Onchocercosis (river blindness; erysipelas de la costa in Mexico and Guatemala; sowda in Arabic speaking areas; craw-craw in West Africa) is concentrated in rural areas of equatorial Africa and the Arabian peninsula,
3267
27
and in Latin America. Onchocerciasis is transmitted by black-flies of the genus Simulium. In the human, infective larvae mature to adult worms that are encapsulated in fibrous tissue and reside in nodules in the subcutaneous tissue and deep fascia. The incubation period is usually 1 to 2 years with a range of months to several years, although microfilariae may first appear 3 to 15 months after exposure; symptoms may precede microfilaremia but often develop only after months or years of infection. Microfilariae can survive in humans for up to 2 to 3 years, and adult worms for 10 to 15 years. The primary means of preventing onchocerciasis are through vector control and mass treatment with ivermectin of the population in endemic areas.
CLINICAL FEATURES Lymphatic Filariasis (Brugia malayi, Brugia timori; Wuchereria bancrofti): Clinical manifestations may be acute, chronic, or recurrent. Initial infection may be subclinical but may also cause recurrent lymphangitis with characteristic retrograde progression (beginning in the affected lymph node and moving distally), lymphadenitis, orchitis, epididymitis, or, occasionally, fever. Lymphangitis typically recurs 6 to 10 times per year, with each episode lasting 3 to 7 days. The affected body part clinically appears normal between early episodes, although during the resolution of the acute phase of W. bancrofti filariasis, there may be extensive exfoliation of the skin of the affected limb. Intermittent fevers and adenolymphangitis can recur for the lifetime of the adult worm. Travelers (>1 month) to endemic areas less frequently acquire infection but may present with more intense inflammatory reactions to filarial parasites. The findings may include lymphangitis, lymphadenitis, groin pain from the associated lymphatic inflammation, urticaria, and peripheral eosinophilia. Chronic disease with sequelae of lymphatic obstruction (lymphedema, elephantiasis, hydrocele, and chyluria) becomes evident 10 to 15 years after infection. The skin over the involved area can become hypertrophic, verrucous, and fibrotic with redundant skin folds (Fig. 177-9). Fissures, ulceration, secondary bacterial infection, and gangrene may occur. The lower extremity, scrotum, and penis are most commonly affected, and less frequently the upper extremity, breast, and vulva are involved. Although antiparasitic treatment does not reverse the late findings of scarring and lymphatic obstruction, a 6-week course of doxycycline can reduce mild-to-moderate lymphedema independent of active filarial infection by reducing vascular endothelial growth factor.31
The differential diagnosis for lymphatic filariasis includes acute infection that can resemble bacterial lymphangitis and other causes of nodular lymphangitis (eg, sporotrichosis, leishmaniasis). Other causes of lymphedema and elephantiasis must also be considered during evaluation of chronic disease.
Cutaneous Filariasis: Loaisis (Loa loa): The characteristic finding of loiasis is the Calabar swelling (Fig. 177-10), a localized area of angioedema caused
3268
by migration of adult worms through subcutaneous tissues. Calabar swellings usually begin years after infection, typically around joints of the upper extremities, generally last 2 to 4 days, and may be associated with pruritus or pain. They range in size from 5 to 20 cm in diameter and may recur in different locations. Fatigue, myalgias, arthralgias, and fever are rare. Adult worms may be seen moving across the bulbar conjunctiva of the eye (see Fig. 177-5) and eyelid. Pruritus may also occur. High-grade peripheral eosinophilia, leukocytosis, and elevated IgE levels are often present. The differential diagnosis includes other causes of migratory and nodular skin lesions (see Tables 177-2 and 177-3).
Cutaneous Filariasis: Mansonelliasis (Mansonella perstans, Mansonella streptocerca): Cutaneous manifestations of M. perstans infection include Calabar-like swellings, typically in the
forearms, hands and face, and pruritus with or without a papular rash. The exact interval between infection and onset of symptoms is unclear. Pruritus, papular lesions, and hypopigmented, hyperpigmented, or lichenified macules, typically found on the upper chest, are seen with M. streptocerca infection. Eosinophilia is often present in Mansonella infections, but also may be from the high prevalence of coinfection with other filarial or helminthic infections.
Cutaneous Filariasis: Onchocerciasis (Onchocerca volvulus): Individuals with onchocerciasis may be asymptomatic. Clinical manifestations most commonly involve the skin and eye. Heavy infections can result in blindness from chronic keratitis or retinitis. Six different patterns of skin changes have been described in onchocerciasis: acute and chronic papular onchodermatitis (see Fig. 177-1), lichenified onchodermatitis, atrophy, depigmentation, and onchocercal nodules (see Fig. 177-2). More than one pattern of skin involvement may be present simultaneously, or one pattern of skin involvement may evolve into another pattern. Pruritus is the most prominent and persistent symptom of infection. Acute papular onchodermatitis most often involves the face, extremities, and trunk, and includes widespread small pruritic papules, vesicles and pustules, sometimes with associated erythema and edema. Short-term visitors to endemic regions typically present with acute pruritus and rash (see Fig. 177-1),32 and demonstrate immune hyperresponsiveness despite low levels of parasites33; skin nodules and eye involvement are usually absent. After exposures in forested areas of West and Central Africa, travelers and expatriates may have an acute form of onchocerciasis characterized by acute pruritic and erythematous swelling of a limb known as gros bras camerounais13 or onchocerciasis-associated limb swelling.34
The skin lesions of chronic papular onchodermatitis are macules and lichenoid papules varying in size from 3 to 9 mm in diameter. Pruritus is common, and postinflammatory hyperpigmentation may be present. The most commonly affected anatomic areas are the buttocks, shoulders, and waist (see Fig. 177-1). Palpable asymptomatic onchocercal nodules containing the adult worm involve the deep dermis and subcutaneous tissue (see Fig. 177-2), and occur over bony prominences such as the skull, iliac crest, knee, rib, sacrum, scapula, and trochanter. Diagnosis is made by finding microfilariae in the skin by biopsy or skin snips (superficial 2- to 4-mm snips of the upper dermis placed in saline and incubated for 24 hours; the fluid is then examined for microfilariae). Peripheral eosinophilia and elevated IgE levels are common findings. The differential diagnosis for onchocercal nodules includes other parasitic causes of nodules (see Table 177-3) and epidermal inclusion cysts. Acute onchodermatitis may resemble miliaria, insect bites, scabies or eczema. Chronic onchodermatitis may resemble a chronic or lichenoid eczema or atopic dermatitis. Skin changes resembling lichenified onchodermatitis can be
27
the result of conditions causing significant pruritus or rubbing. Atrophic changes resemble those associated with aging. Onchocercal depigmentation may be confused with postinflammatory hypopigmentation or depigmentation.
DIAGNOSIS
Eosinophilia, sometimes high-grade, and elevated IgE levels are common in filarial infections. Diagnosis rests primarily on demonstration of microfilariae in blood (for lymphatic filariasis, loiasis, and cutaneous filariasis caused by Mansonella species; note that daytime blood specimens are appropriate for all except bancroftian filariasis, which requires nocturnal specimens for diagnosis) or in skin snips (for Mansonella and Onchocerca infections). However, persons with active filarial infection may not be microfilaremic. Microfilariae may not appear in blood until 5 to 6 months after infection in loiasis. Diagnosis also can be established through identification of the adult worm. Filarial serology is often very sensitive but is nonspecific because of cross-reaction with other helminthiases. A positive serologic test for bloodborne species should be followed by both a blood examination for larvae and test for filarial antigen, to confirm whether serology represents an active infection or a previous one. Infiltrates may be present on chest radiography in individuals with lymphatic filariasis and tropical pulmonary eosinophilia, an aberrant immune response to the infection. Inguinal lymph node ultrasonography may show active adult worms (“filarial dance sign”), more commonly seen in men than in women. Lymph node biopsy is contraindicated.
MANAGEMENT
Management of filariasis depends on the infecting species. Table 177-8 summarizes treatment of filariasis.
SCHISTOSOMAL INFECTIONS
SCHISTOSOMAL
INFECTIONS
EPIDEMIOLOGY
Cercarial dermatitis (swimmer’s itch) occurs worldwide and may be acquired by contact with infective cercariae of many species of nonhuman schistosomal parasites in both freshwater and salt water. Attack rates during outbreaks usually range from 55% to 100% of those exposed, with highest attack rates in those with a history of previous cercarial dermatitis. An estimated 200 million people worldwide have schistosomiasis (bilharziasis) and over half a billion live in endemic areas. Infection can be caused by Schistosoma haematobium, Schistosoma intercalatum, Schistosoma japonicum, Schistosoma mansoni, and Schistosoma mekongi. Humans are the only important reservoir
3269
27
for S. haematobium, which is prevalent in Africa and the Middle East. Schistosoma mansoni is endemic in the same areas, as well as parts of the Caribbean and South America; S. intercalatum in central Africa; S. japonicum in China, Indonesia, and the Philippines; and S. mekongi primarily in Cambodia and Laos. Infection can be acquired after a brief exposure in an endemic area, often in travelers,35-37 typically after swimming, wading, rafting, or bathing in slowmoving freshwater in endemic areas. Attack rates in nonimmune, exposed persons (eg, travelers) can be as high as 100%. Cutaneous manifestations can be seen at every phase of the infection.
CLINICAL FEATURES
Clinical findings of cercarial dermatitis are confined to the skin and are usually distributed on skin surfaces exposed directly to water. Pruritus may begin while swimming, followed rapidly by the appearance of an erythematous macular rash that persists for several hours. Ten to 15 hours after exposure, papules, vesicles, and urticaria develop. Marked pruritus is characteristic. Symptoms peak 48 to 72 hours after exposure, and gradually resolve spontaneously over the next several weeks. Cercariae of S. haematobium, S. intercalatum, S. japonicum, S. mansoni, and S. mekongi can penetrate intact skin within 30 seconds to 10 minutes and may elicit a local inflammatory response (penetration phase). The first exposure to cercariae typically results in erythema and pruritus that resolve within hours. In those previously sensitized, a pruritic, erythematous, papular, and urticarial rash develops, usually lasting 1 week. Migration of the larvae (schistosomulae) usually occurs 2 to 6 weeks after exposure and leads to an acute parasitic hypersensitivity reaction with circulating immune complexes. This invasive phase (Katayama fever or acute schistosomiasis) has historically been described with S. japonicum (Katayama fever, sensu stricto), S. mansoni, and, to a lesser extent, with S. haematobium. Symptoms of acute schistosomiasis are most prominent in primary infection in nonimmune persons and include fever, fatigue, myalgia, cough, and headache that may persist for several weeks. Abdominal symptoms and diarrhea also may be present. Urticaria, purpura, subungual hemorrhages, and edema of the face, the extremities, genitals, and trunk may be seen during the invasive phase. Chronic infection may be asymptomatic, or associated with abdominal pain (S. mansoni, S. japonicum) or hematuria (S. haematobium). Chronic dermal schistosomiasis (bilharziasis cutanea tarda) may begin after years of infection and result from a granulomatous inflammatory reaction to the deposition of eggs in the dermis (Fig. 177-11), which may continue for the life span of the adult worm (10 years or more). It is seen primarily in persons who have lived in endemic regions. Lesions are skin-colored or slightly pigmented, 2- to 4-mm firm, pruritic, oval papules that appear in crops and clusters, typically on the trunk and especially the periumbilical region, and remain unchanged without treatment. Lesions also appear in
3270
the genital and buttocks areas, especially on the vulva in women and the scrotum and penis in men. Chronic lesions may also include painless, skin-colored, pink, or brown eroded papules and warty, vegetative, polypoid lesions that may be ulcerated and necrotic, with fistulous tracts. Chronic skin disease can be complicated by lymphedema and elephantiasis, secondary bacterial infection, and squamous cell carcinoma.
DIFFERENTIAL DIAGNOSIS
The differential diagnosis of acute schistosomiasis includes other causes of urticaria. Bilharziasis cutanea tarda of the genitals and buttocks must be differentiated from syphilis, condyloma latum, condyloma acuminatum, other granulomatous diseases, malignancy, and hemorrhoids.
DIAGNOSIS
Cercarial dermatitis is largely a clinical and epidemiologic diagnosis. In schistosomiasis, prominent eosinophilia may be present in early infection, especially during the invasive phase, and subsequently fluctuates more or less above the normal value during the chronic phase. Onset of eosinophilia may lag behind appearance of clinical symptoms. Acute disease can be suspected based on the history of exposure and cercarial dermatitis, although many patients do not develop the dermatitis. Identification of eggs in the stool or urine occurs only after the acute phase of infection, generally 2 to 3 months after the onset of infection. Similarly, serology does not become positive until approximately 2 months after infection.
MANAGEMENT
Cercarial dermatitis is self-limited and does not require specific therapy. Table 177-8 outlines management of schistosomiasis.
STRONGYLOIDIASIS
STRONGYLOIDIASIS
EPIDEMIOLOGY
Strongyloidiasis is caused by S. stercoralis, which is endemic to Africa, Asia, Southeast Asia, and Central and South America. Disease is also found in the Caribbean, and to a much lesser extent in Europe, Japan, Australia, and parts of the southern United States. Humans are the only hosts. Infection caused by Strongyloides fuelleborni, found sporadically in Africa and Papua New Guinea, is relatively rare. The prevalence of infection can be high in endemic areas, as well as among institutionalized mentally impaired persons, in former prisoners of war, and in refugees and immigrants from endemic areas. Most infected persons have low worm burdens and are persistently infected for life, often with minimal or no symptoms. The life cycle of Strongyloides helminths differs from that of most other helminths in that an entire parasite life cycle may be completed within the human host. Infection typically results from penetration of skin or mucous membranes by infective larvae, usually from soil; the risk of infection is high for persons with frequent soil contact (eg, walking barefoot) in warm, moist areas contaminated by human feces. Filariform larvae travel via the circulatory system to the lungs where they penetrate the alveoli, ascend the trachea, are swallowed, and then mature into adult worms in the small intestine. Although sexual reproduction does take place within the intestine, adult females are also parthenogenetic (capable of reproduction without males). Eggs are deposited in the intestinal mucosa, hatch, and release rhabditiform larvae, which are excreted in the stool to begin another “free-living” cycle, developing into adults in soil where they reproduce sexually and give rise to infective filariform larvae. However, rhabditiform larvae in the bowel may also transform directly into filariform larvae (the “parasitic cycle”) that penetrate the perianal skin and/ or intestinal mucosa and enter the circulation, and begin another cycle of infection (autoinfection). In the appropriate clinical setting this may lead to disseminated disease (hyperinfection syndrome). Appropriate sanitation and avoidance of soil contact by skin in endemic areas reduce the risk of infection. Persons with a history of prior residence or activities that place them at an increased risk for strongyloidiasis should be evaluated for presence of the infection, and should be treated even if asymptomatic. This is especially important in persons who receive or will receive immune suppressing therapy.
27
CLINICAL FEATURES
Cutaneous manifestations may be seen at any phase of infection. Following skin penetration, an urticarial eruption or larva currens may develop. Larva currens, a migratory serpiginous and intensely pruritic lesion caused by intradermal migration of larvae, can be differentiated from CLM by the high rate of movement (up to 5 to 10 cm per hour). Larva currens typically disappears within a few hours, only to recur over the course of weeks to years. Perianal larva currens may be present (see Fig. 177-4) and is pathognomonic of chronic infection. Lesions on the buttocks and in the perianal region result from larvae exiting the GI tract and reinfecting the host by penetrating the perianal skin. Persons chronically infected with Strongyloides may also experience pruritus ani and chronic urticaria, which may be complicated by prurigo nodularis or lichen simplex chronicus. The dermatologic manifestation of hyperinfection and disseminated strongyloidiasis is a rapidly and progressively diffuse petechial and purpuric eruption, often with a reticular pattern, typically involving the trunk and proximal extremities (Fig. 177-12).38,39 The “thumbprint sign,” a unique pattern of periumbilical purpura resembling multiple thumbprints,40 also may be seen. During the invasive phase of the infection, transient pulmonary manifestations (cough, wheezing, infiltrates) are manifestations of pulmonary migration and may be associated with urticaria. Chronic strongyloidiasis gives rise to nonspecific GI complaints (epigastric pain, nausea, vomiting, diarrhea, constipation, malabsorption, weight loss).
COMPLICATIONS
Hyperinfection syndrome is the most severe complication, typically occurring in the presence of impaired cellular immunity as seen with use of systemic steroids but also with other immunocompromised states, including human T-cell lymphotropic virus (HTLV)-1
3271
27
infection. Interestingly, HIV infection is not associated with an increased risk of disseminated disease. Insidious GI symptoms may be present in hyperinfection syndrome. Pulmonary disease is the most common extraintestinal manifestation of hyperinfection syndrome and is characterized by diffuse pulmonary infiltrates with dyspnea, cough, wheezing, or hemoptysis. Diarrhea and abdominal pain occur frequently, with inflammation leading to small-bowel-wall edema; ileus may develop in late stages. In uncontrolled hyperinfection, filariform larvae also penetrate organs not normally involved in the life cycle, including the urinary tract, liver, brain, and skin. The finding of filariform larvae in stool may be an early sign of hyperinfection even in those with minimal symptoms. Gram-negative bacillary infections including bacteremia, peritonitis, meningitis and sepsis may result from the concurrent migration of bacteria and larvae across the bowel wall. The mortality rate for disseminated disease is approximately 50%.
DIAGNOSIS
Peripheral eosinophilia is present in up to 80% of patients with intestinal disease. Eosinophilia may be high grade during larval migration, but is rarely a feature of disseminated infection (although pulmonary eosinophilia may be noted in the latter), and may be absent in patients on systemic steroids and who are otherwise severely immunocompromised. In chronic disease, the eosinophil level fluctuates and is often mildly elevated (mild to moderate increase) but may be normal. Hence, the absence of eosinophilia does not rule out strongyloidiasis. The diagnosis of larva currens is based on its characteristic clinical features. The identification of larvae in the stool, small bowel contents, and, rarely, in other body fluids confirms the diagnosis. Larvae first appear in the stool 2 to 4 weeks after exposure. Multiple stool examinations are often necessary to make the diagnosis; a single stool specimen may fail to detect larvae in up to 70% of cases, although sensitivity approaches 100% with 7 consecutive stool samples. Although the agar plate method is a very good test that has a sensitivity of 90%,41 it is not readily available. A stool sample is placed on solid bacterial medium, incubated, and subsequently examined for bacterial tracks created by larvae dragging enteric bacteria as they migrate across the plate. Serology has become the test of choice, with a sensitivity of approximately 90%, but lacks specificity and may cross-react with other helminthic infections (in particular filariasis, ascariasis, and acute schistosomiasis). However, because strongyloidiasis is potentially fatal, and most individuals are not infected with other helminths, except in the tropics, the lack of sensitivity is not clinically relevant. Because studies show that antibody levels drop significantly over the first year following successful therapy, serology is often used as a test of cure.42 Skin biopsy of the larva currens eruption often fails to reveal larvae, whereas they may be visualized in biopsy specimens of purpuric and petechial lesions with hyperinfection.
3272
MANAGEMENT
Treatment of strongyloidiasis in asymptomatic individuals is often successful. Ivermectin 200 µg/kg daily for 2 days is the recommended therapy (see Table 177-8). Albendazole 400 mg twice daily for 7 days appears to be a less-effective alternative, although data are more limited; the drug is not approved by the U.S. Food and Drug Administration for this indication. In contrast, patients with disseminated disease may require prolonged or repeated courses of therapy; some experts also suggest that combination therapy with ivermectin and albendazole be used in this setting. Patients with concurrent HTLV-1 infection may require lifetime therapy, given intermittently, owing to the inability of the host to eliminate the parasite. If possible, immunosuppressant therapy should be discontinued in those with hyperinfection. For patients in whom strongyloidiasis is suspected epidemiologically or clinically and who require immunosuppression therapy, Strongyloides therapy should be given “on spec” if the diagnosis cannot be ruled out in a timely manner prior to initiating immunosuppressants.
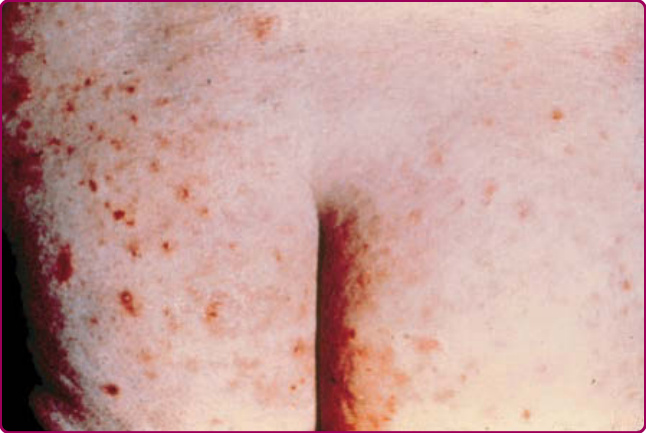
Figure 177-1 Onchocercal dermatitis. (Used with permission from Herman Zaiman, MD.)
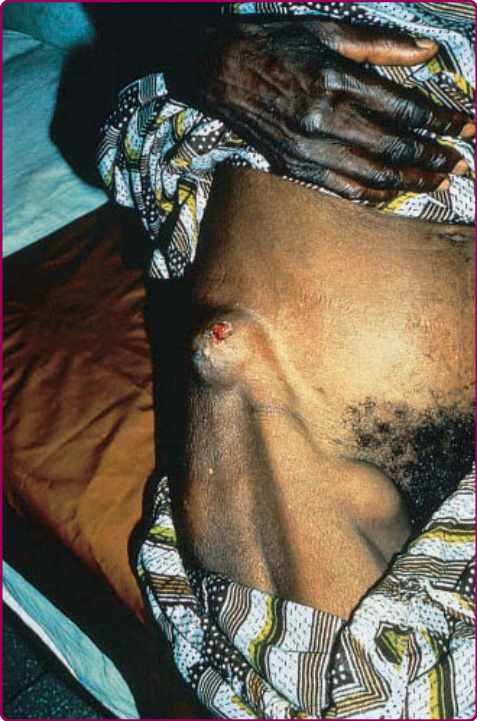
Figure 177-2 Onchocercal nodule over iliac crest. (Used with permission from Jay S. Keystone, MD, FRCPC.)
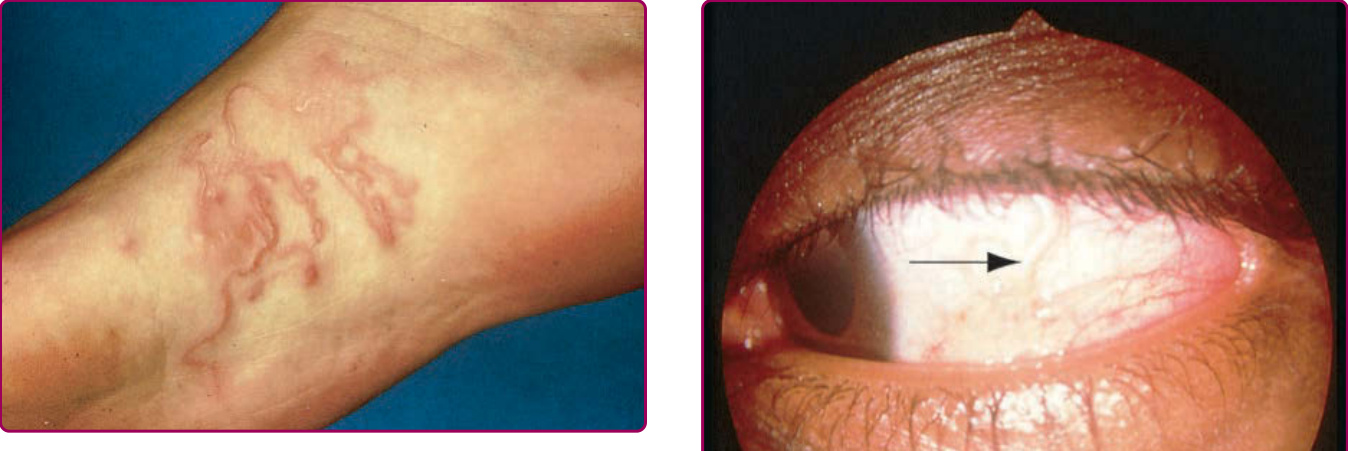
Figure 177-3 Cutaneous larva migrans. (Used with permission from Jay S. Keystone, MD, FRCPC.)

Figure 177-4 Larva currens in chronic strongyloidiasis. Multiple serpiginous, inflammatory lesions are visible on the buttocks.
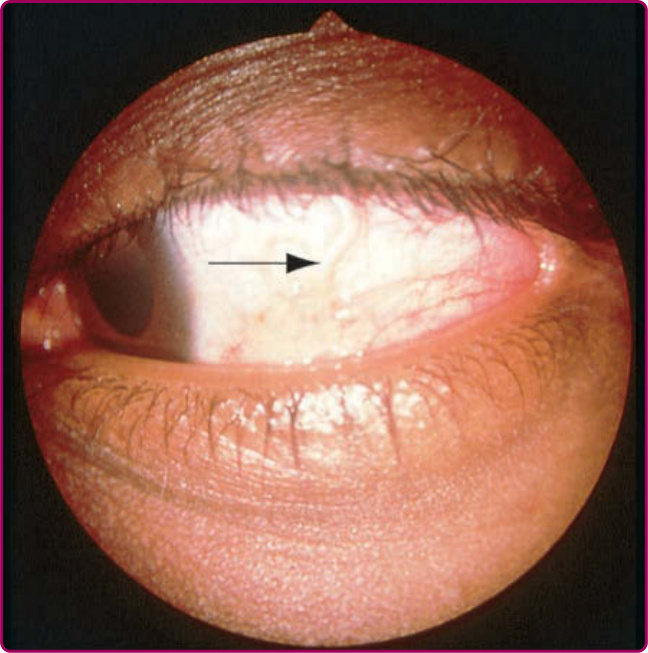
Figure 177-5 Loiasis. Adult worm crossing bulbar conjunctiva of the eye (arrow). (Used with permission from Murray Wittner, MD, PhD.)

Figure 177-6 Dracunculiasis. (Used with permission from Jay S. Keystone, MD, FRCPC.)

Figure 177-7 Cutaneous larva migrans with vesicular and bullous lesions. (Used with permission from Jay S. Keystone, MD, FRCPC.)

Figure 177-8 Cutaneous larva migrans of the buttocks. (Used with permission from Jay S. Keystone, MD, FRCPC.)

Figure 177-9 Lymphatic filariasis. (Used with permission from Jay S. Keystone, MD, FRCPC.)

Figure 177-10 Calabar swelling in loiasis. (Used with permission from Jay S. Keystone, MD, FRCPC.)

Figure 177-11 Ectopic deposition of Schistosoma mansoni eggs.

Figure 177-12 Disseminated strongyloidiasis, with nonpalpable purpura on the abdominal wall. (Reprinted with permission from Grossman ME, Roth J. Cutaneous Manifestations of Infection in the Immunocompromised Host. Baltimore, MD: Lippincott, Williams & Wilkins; 1995.)
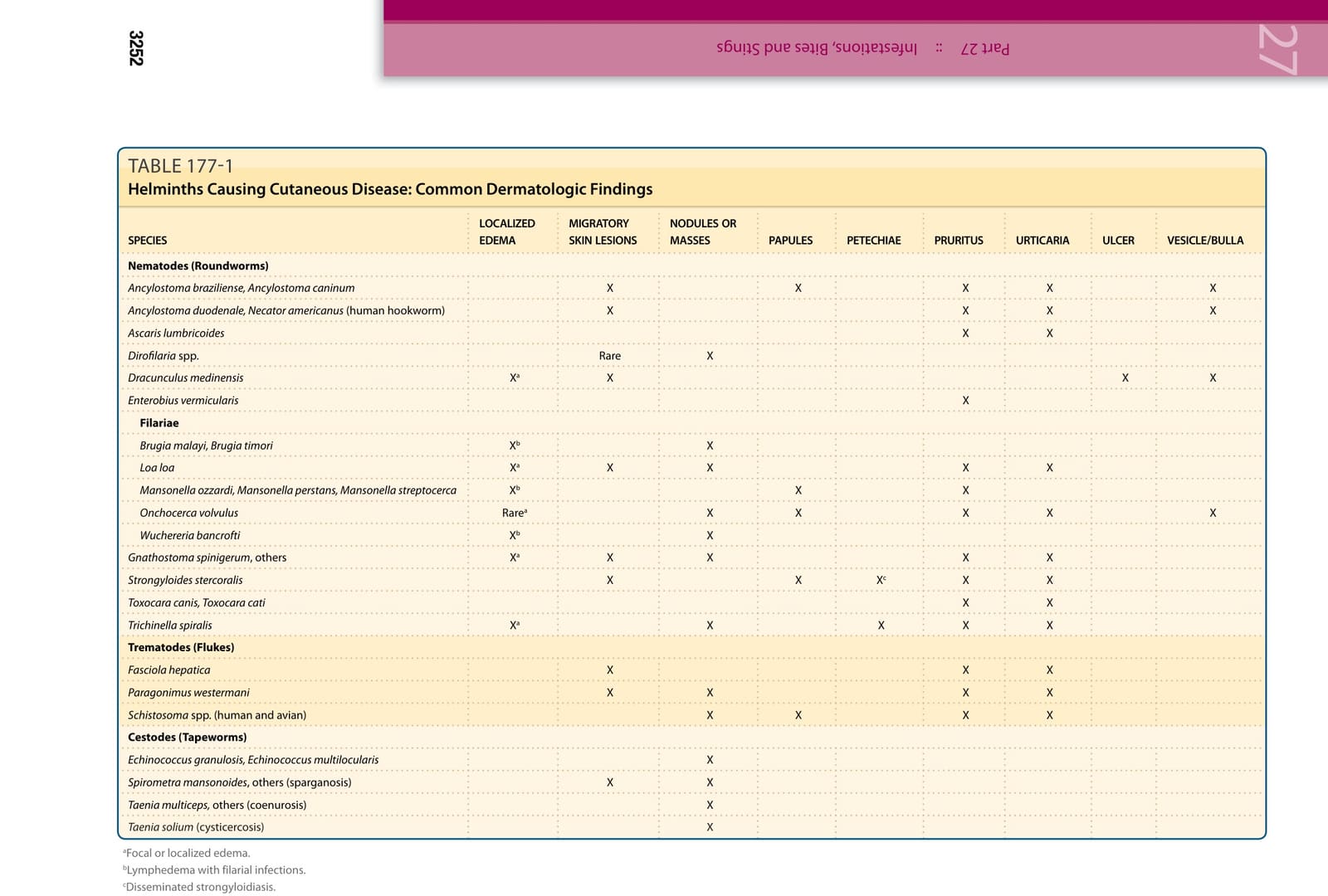
TABLE 177-1
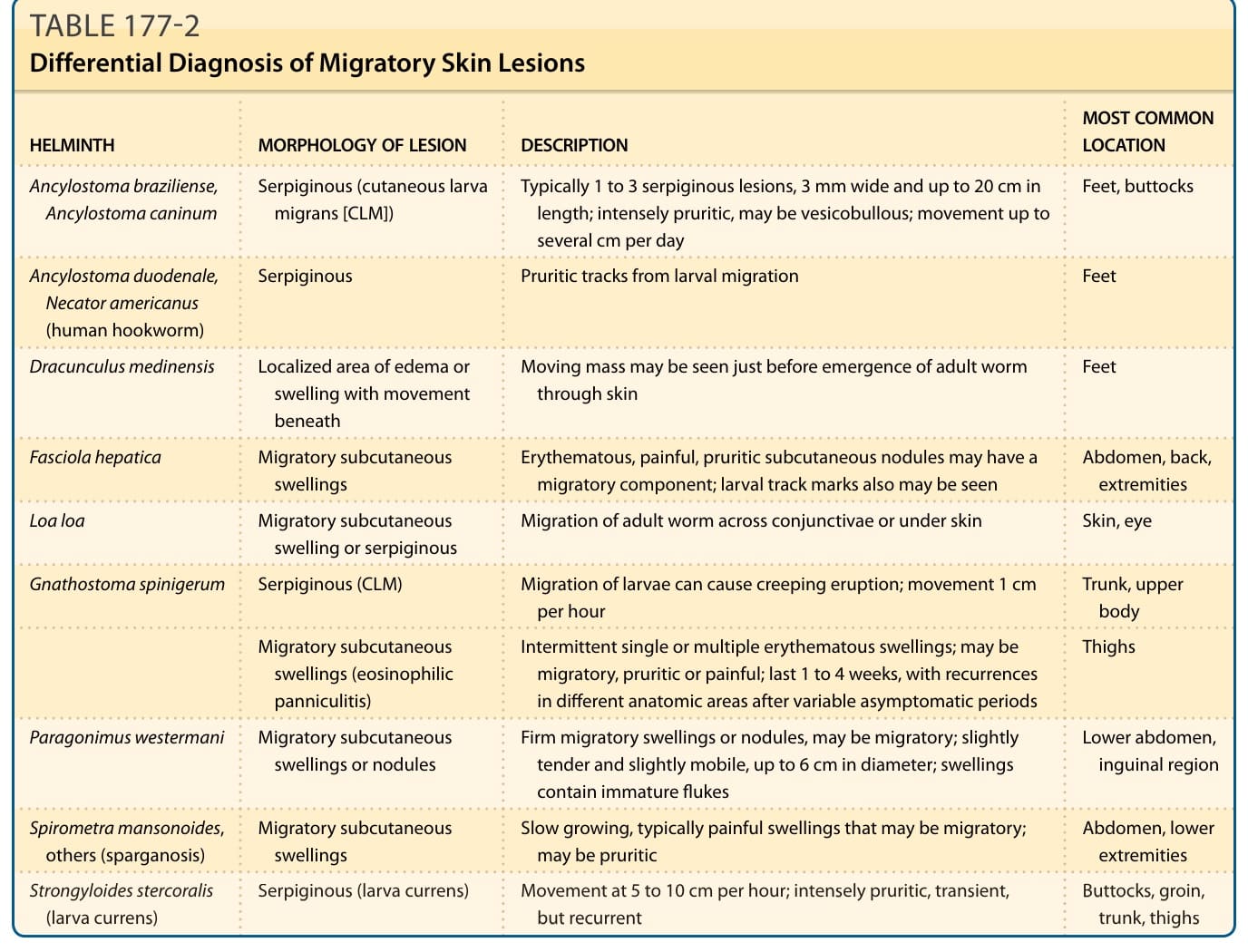
TABLE 177-2 Differential Diagnosis of Migratory Skin Lesions
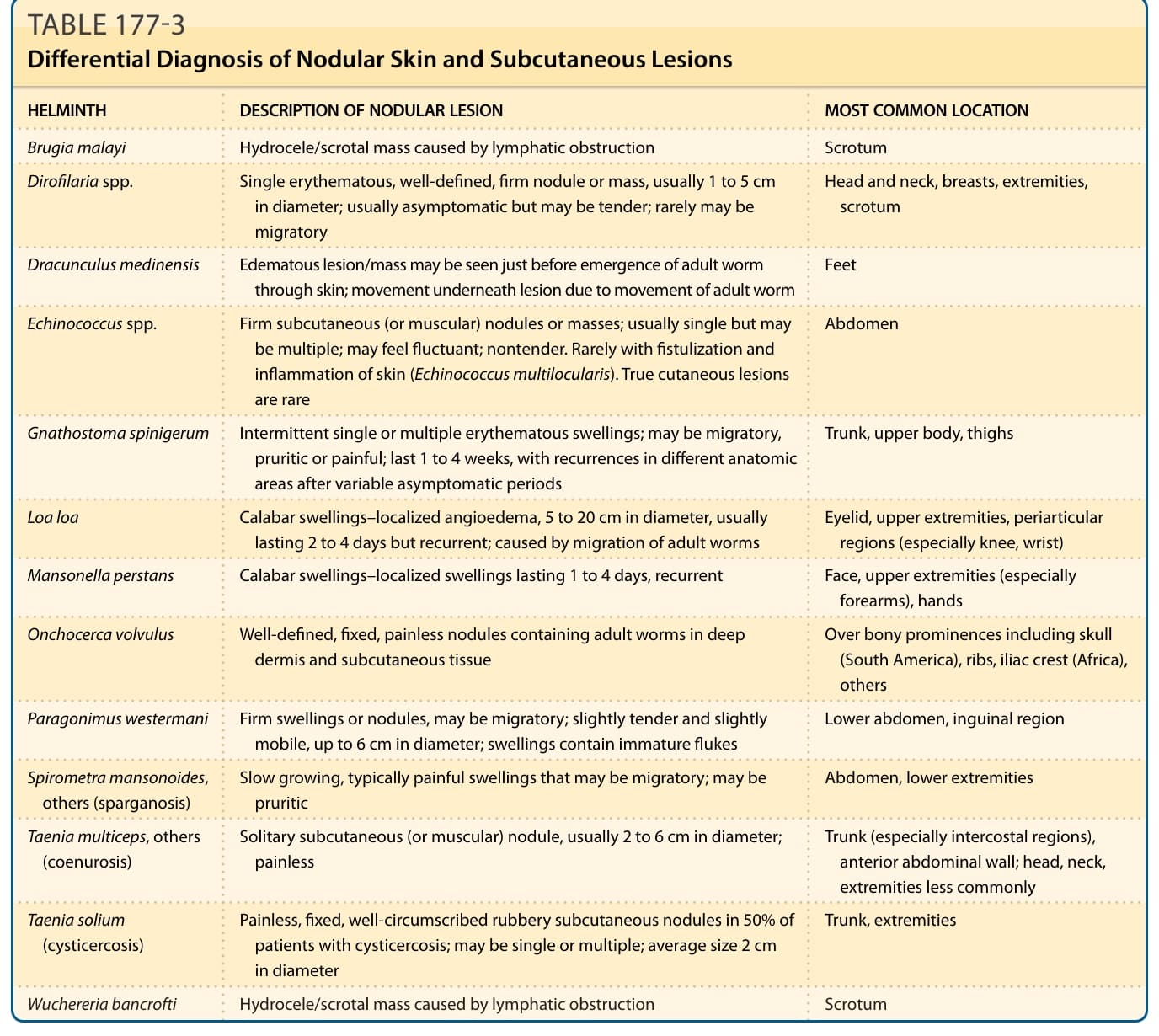
TABLE 177-3 Differential Diagnosis of Nodular Skin and Subcutaneous Lesions
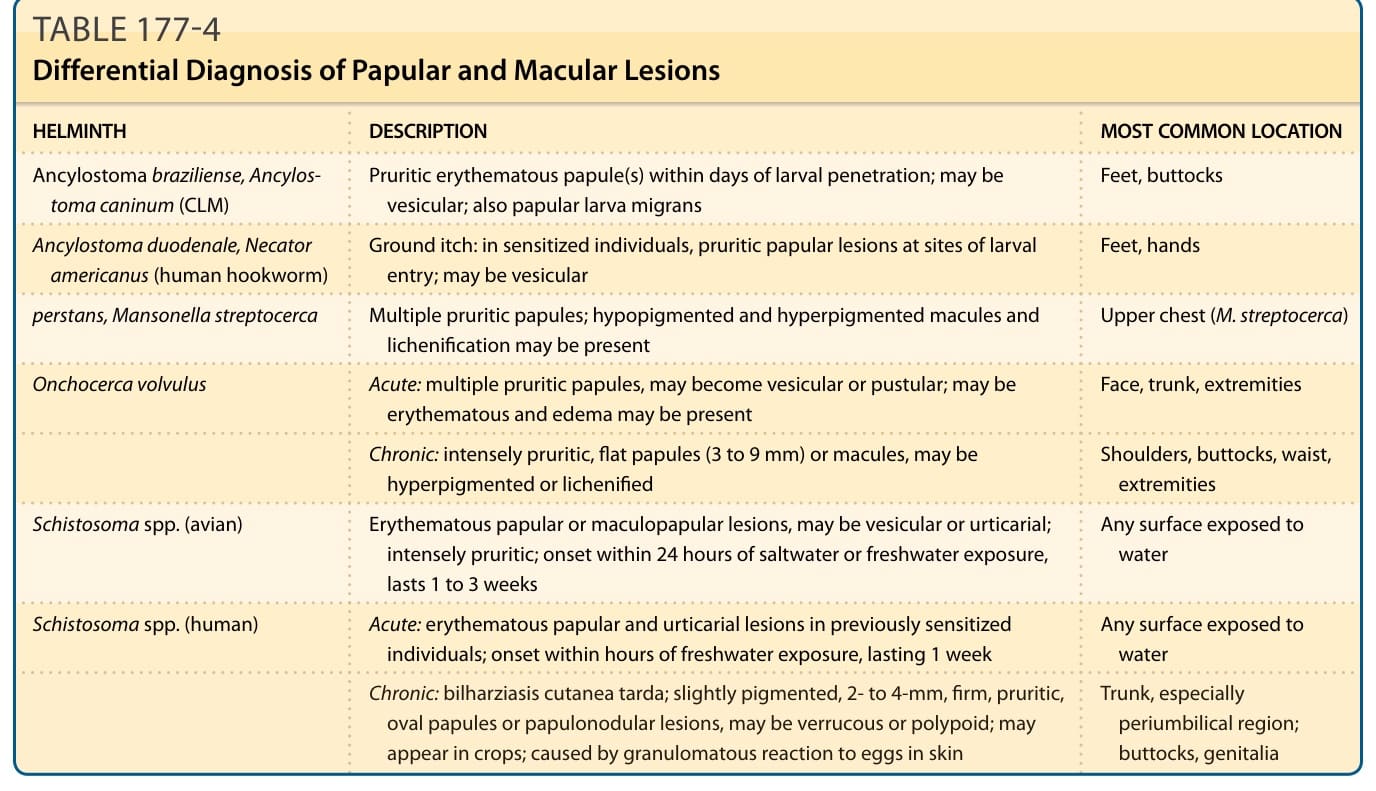
TABLE 177-4 Differential Diagnosis of Papular and Macular Lesions
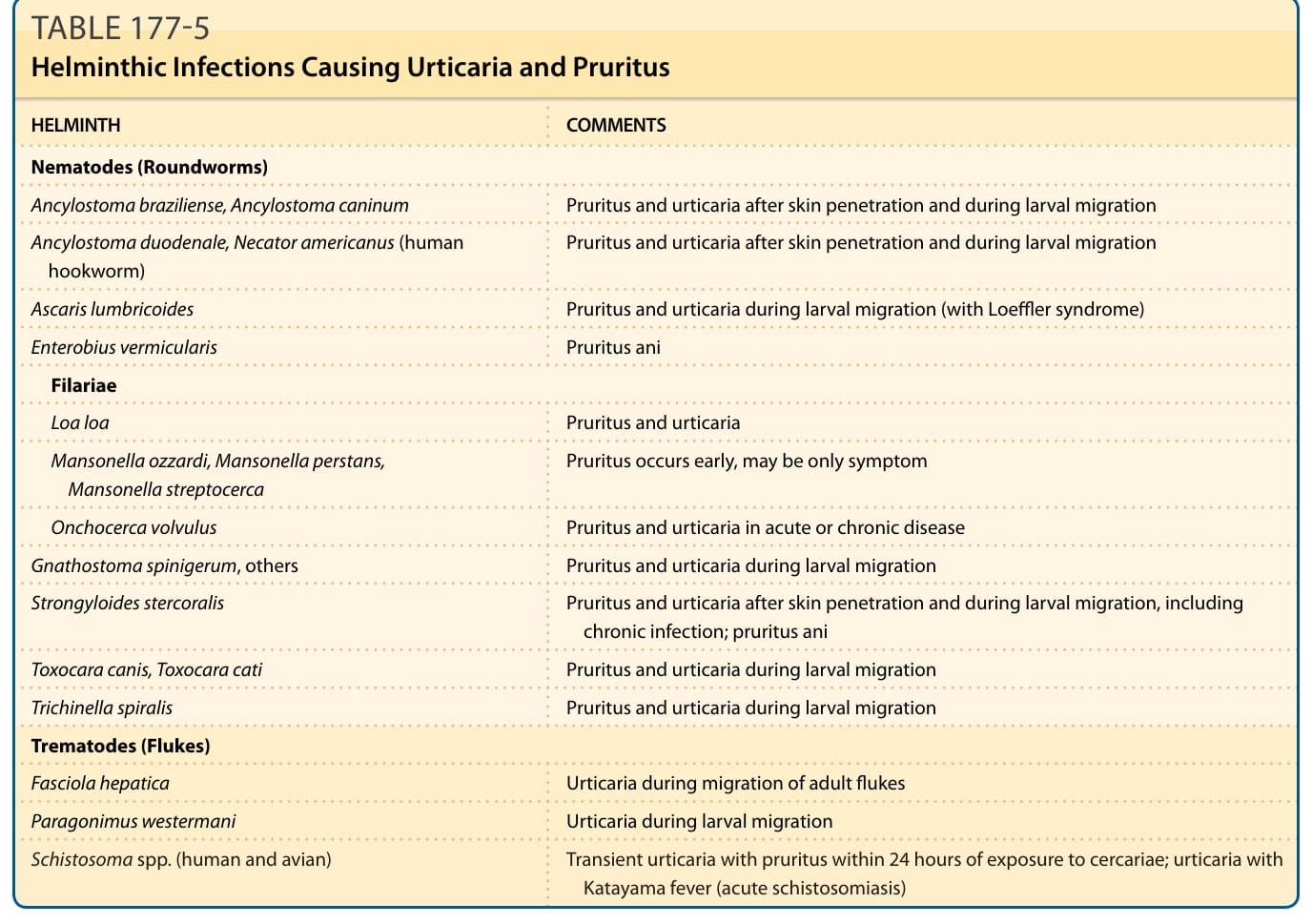
TABLE 177-5 Helminthic Infections Causing Urticaria and Pruritus
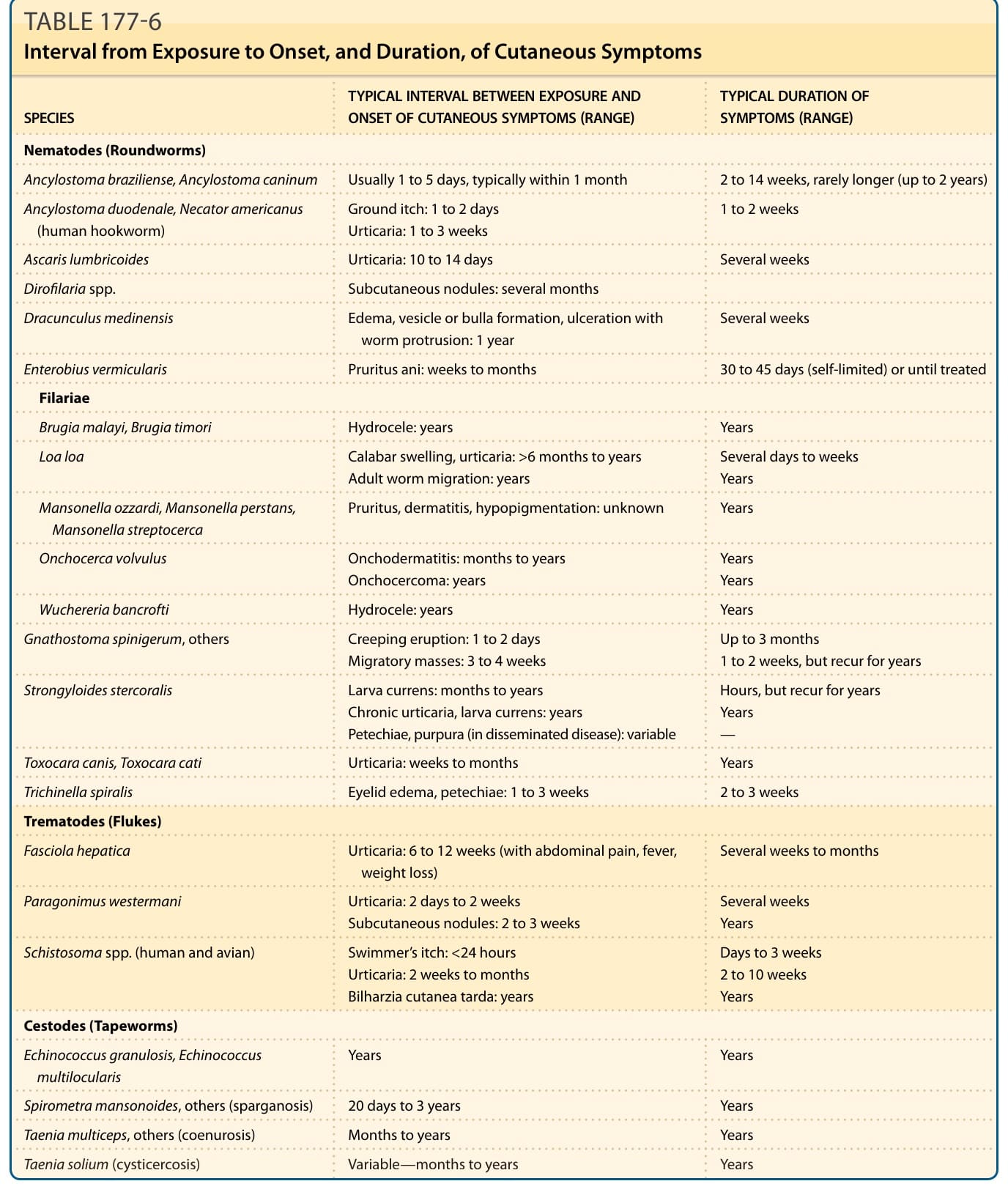
TABLE 177-6 Interval from Exposure to Onset, and Duration, of Cutaneous Symptoms
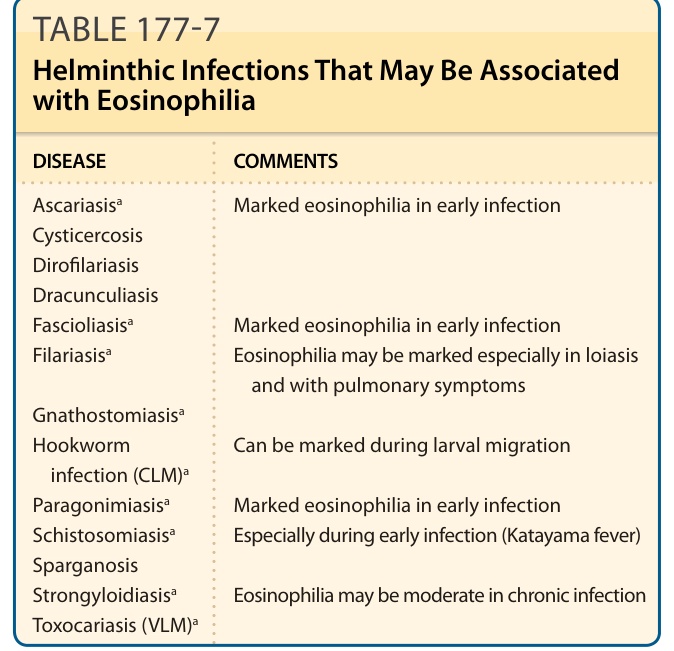
Table 177-7 lists the helminths that typically cause eosinophilia. Severe or high-grade eosinophilia (an eosinophil count of >3000/mm3) is suggestive of infection caused by relatively few of these parasites (Table 177-7).
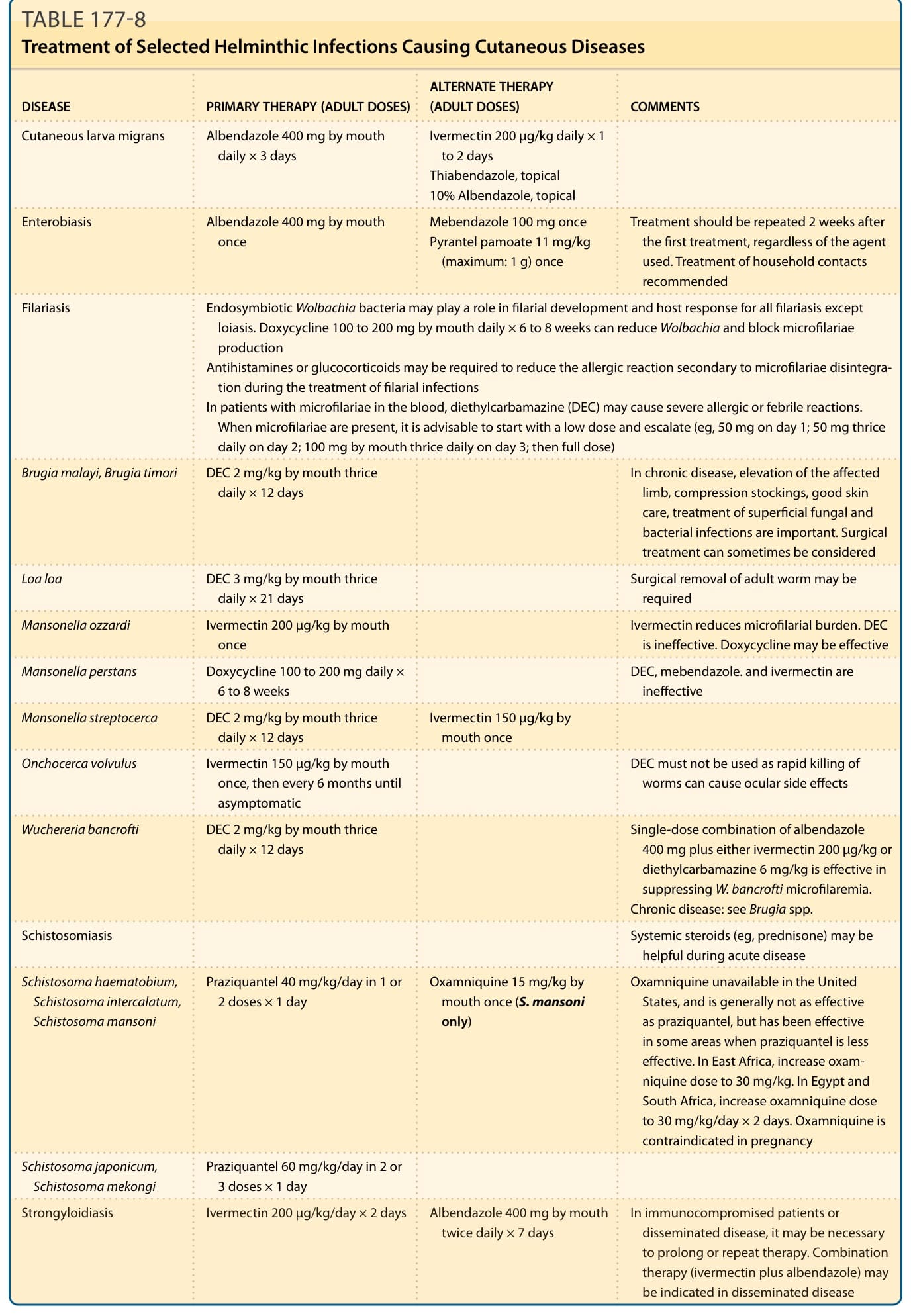
Table 177-8 lists treatment of selected infections that are discussed in detail below.