Granuloma Inguinale
26
AT-A-GLANCE
■ Granuloma inguinale (GI) is a rare, chronic, progressive ulcerative disease that mainly affects the genital and perigenital skin.
■ GI is primarily contracted through sexual transmission.
■ GI is caused by infection with Klebsiella granulomatis, a gram-negative bacteria.
■ It affects mostly people of lower socioeconomic status living in tropical or subtropical areas.
■ Diagnosis confirmed by demonstrating intracellular Donovan bodies on histology.
INTRODUCTION
Granuloma inguinale (GI), or donovanosis, is a rare chronic ulcerative disease affecting mainly genital and perigenital skin. The microorganism was first identified in 1905 by Donovan, who noted the characteristic Donovan bodies in macrophages. In 1955, the name “donovanosis” was proposed.1 The prevalence of GI has decreased markedly in recent times, and it can now be considered a sporadic disease. Despite its rarity, GI can have an aggressive clinical course so prompt recognition and treatment are necessary.
EPIDEMIOLOGY
GI is typically found in warm, moderately humid tropical and subtropical climates. GI has characteristically been reported in specific endemic areas, including Papua New Guinea, South Africa, parts of India and Brazil, and among the Aboriginal community of Australia.2
Sporadic cases have been reported elsewhere in southern Africa, the West Indies, and South America.3
The disease is very rare in Europe and North America. Since 1989, fewer than 10 cases per year have been reported in the United States.4 Recent epidemiologic data is limited, but overall, the incidence of GI is decreasing, especially in previously endemic areas such as Papua New Guinea and Australia.3,5 The disease has nearly been eradicated from Australia, with only five cases reported in 2004.5 GI is most commonly seen in individuals with lower socioeconomic status and sexually active adults between ages 20 and 40 years. No true race or gender predilection has been determined.
MODE OF TRANSMISSION
Although the mode of transmission is generally thought to be sexual, this is controversial. The consensus that donovanosis is transmitted sexually has been predominant since the middle of the 20th century. The majority of cases of GI occur in patients who have a history of sexual activity, and there is an increased incidence of the disease in age groups with the highest sexual activity. Often individuals with GI have history of sexual contact with sex professionals and concurrent sexually transmitted infections (STIs).6 The predominance of genital lesions and lesions on the cervix only or on the anus in men involved with receptive anal intercourse all favor venereal origin. However, GI has occurred in young children and sexually inactive adults, challenging the idea that all cases are sexually transmitted. Furthermore, transmission rate between sexual partners is lower compared with other STIs.2
The incidence of GI is also relatively low among sex workers and their conjugal partners. In rare cases, transvaginal transmission of GI during delivery can occur.7
CLINICAL FEATURES
The incubation period is uncertain, with estimates ranging between 1 and 360 days.8 Most often the incubation period is stated to be about 2 to 3 weeks, which is based on human experimental data in which lesions appeared on average 50 days after exposure in a group of volunteers.9 GI usually first presents as a single firm papule or subcutaneous nodule that later ulcerates and gradually increases in size. Four clinical types have been described—ulcerogranulomatous, hypertrophic, necrotic, and sclerotic. The most common presentation is the ulcerogranulomatous type, which presents as highly vascular, beefy-red ulcers that are nontender but bleed to the touch (Fig. 174-1). If untreated, the ulcers may extend to adjacent tissues via self-inoculation and form multiple ulcers. These ulcers are often mirror images of each other and have been described as “kissing lesions” (Fig. 174-2). The ulcers of GI may have a smooth border or a hypertrophic or verrucous border resembling condyloma acuminatum in the hypertrophic type (Fig. 174-3). The necrotic type often occurs in long-standing donovanosis and presents as a foul-smelling, deep ulcer with copious gray exudate and extensive destruction to surrounding tissues (Fig. 174-4). In the rare dry sclerotic type, lesions are nonbleeding ulcers that form fibrous band–like scars. The genital region is affected in 90% of cases and the inguinal area in 10%. The most common locations
involved in men are the coronal sulcus, prepuce, and glans penis and in women are the labia minora, fourchette, and perineum.10 Occasionally, GI presents as a mass in the vagina or cervix and can mimic a carcinoma.11 The anus and colon may be involved, especially in homosexual men. GI may spread to the tissue overlying the regional lymph nodes and present as abscess or subcutaneous granuloma called a pseudobubo that later ulcerates.10 The lymph nodes themselves are rarely involved unless there is an overlying bacterial superinfection. Rarely, pseudoelephantiasis of the genitals has occurred because of cicatrization and blockage of the lymph channels.12
Although rare, extragenital lesions account for about 6% of cases. Sites of involvement include the lips,
26
gums, cheek, palate, pharynx, neck, nose, larynx, and chest.6,8,13 Even more rare is disseminated donovanosis with spread to bone (causing osteomyelitis) or liver.14,15
GI takes on an aggressive course during gestation and should be considered in women with atypical lesions living in high-risk areas.16 Although no congenital infections have been reported, there are cases in which the infection was passed to the infant during vaginal delivery. The presentation of exposed infants has varied from otitis media and lymphadenitis to mastoiditis and meningitis.7,17
As with other STIs, patients with GI may be coinfected with HIV. HIV/AIDS-related immune alteration may alter the clinical manifestations of GI.18 The natural history is usually more rapid, extragenital dissemination may occur more frequently, and ulcers may persist for prolonged periods, leading to more tissue
3203
26
destruction. HIV-infected patients with GI also have high failure rates to first-line therapy.19
ETIOLOGY AND PATHOGENESIS
GI is caused by the organism Klebsiella granulomatis, previously called Calymmatobacterium granulomatis. The name was changed after sequencing the phoE and 16S ribosomal RNA genes and demonstrating close homology with Klebsiella pneumoniae and Klebsiella rhinoscleromatis.20 K. granulomatis is a facultative gramnegative, nonmotile, pleomorphic bacteria that resides in the cytoplasm of large mononuclear cells. Although the mature form is encapsulated, it can be unencapsulated and demonstrates a closed safety pin appearance in its immature form.2 Infection leads to a granulomatous inflammatory response, causing local tissue destruction and cutaneous ulceration.
DIAGNOSIS
Clinical suspicion of GI can be confirmed by the demonstration of the characteristic inclusion bodies called Donovan bodies within large mononuclear cells either in smears obtained directly from tissue or biopsy samples (Fig. 174-5). Whereas the cells are 25 to 90 µm in diameter, the Donovan bodies are 0.5 to 0.7 µm by 1 to 1.5 µm and may or may not be encapsulated.3 Rarely, the Donovan bodies are found extracellularly or within neutrophils.21 Both tissue smears and biopsies can be stained with Giemsa, Wright, silver or Gram stains to demonstrate the Donovan bodies. The bodies are more easily visualized with properly done smears than with biopsy. If GI is suspected and multiple swabs are being taken from an ulcer for detection of other organisms, the swab for GI should be taken first so that an adequate amount of cellular material can be obtained. It is also recommended that
A B
the ulcer not be cleaned with topical antimicrobials or saline because this may lead to negative smears.18 The ulcer should be gentle wiped with a cotton swab only before taking the smear. Tissue smears should be prepared by rolling a swab firmly across lesion and then rolling this swab evenly across glass slide to deposit the material. A rapid Giemsa method such as Rapi- Diff can then be used to stain tissue smears for rapid diagnosis. Tissue for biopsy should be taken from the advancing edge of the ulcer. Histologically, the epidermis may exhibit pseudoepitheliomatous hyperplasia or ulcerations (or both) depending on the site biopsied. The dermis often contains a dense mixed inflammatory infiltrate composed of histiocytes, plasma cells, and rare lymphocytes. The hypertrophic and cicatricial forms of GI may exhibit fibrosis. The clusters of Donovan bodies appear as safety pin–like structures inside vacuolated cytoplasms of large mononuclear cells. Neither cultures nor serology play a major role in diagnosis. K. granulomatis is difficult to culture and store; however, successful culture has been accomplished by two laboratories using human peripheral blood mononuclear cells and in HEp-2 cells.22,23 A polymerase chain reaction (PCR) test using a colorimetric detection system has been developed but is currently only in use for research purposes.24 No commercial PCR test for GI is available currently. Serologic tests have been developed but are not reliable.
DIFFERENTIAL DIAGNOSIS
The clinical differential diagnosis of GI includes several other disorders that cause genital ulcers. Distinguishing features of GI ulcers include the lack of pain, beefy-red appearance, and presence of “kissing lesions.” Table 174-1 reviews the most common differential diagnoses (organized by clinical presentation of genital ulcers, necrotic lesions, or extragenital involvement).
3204
DISORDER CONSIDERATIONS
Genital Ulcers
Primary syphilis Chancre: painless, punched-out, pink ulcer with nonpurulent clean base and indurated raised border; usually hard and firm
Secondary syphilis Condyloma lata: present as pale, white, moist warty plaque but may rarely ulcerate
Lymphogranuloma venereum Initially presents as an asymptomatic, genital papule or pustule or a symptomatic ulceration; later inguinal buboes form
Chancroid Painful ulcers, often yellow in color, with surrounding erythema and painful lymphadenopathy
Condyloma acuminatum White, gray, or skin-colored warty papules or may be giant cauliflower-like lesions
Malacoplakia Solitary or multiple soft papules and nodules, often in urinary tract
Long-Standing Necrotic Lesions
Squamous cell carcinoma Important to rule out malignancy in longstanding necrotic lesions, especially those that do not respond to conventional therapy
Genital amebiasis Painful genital ulcers with or without genitourinary discharge
Chronic herpes simplex in immunosuppressed
May present with chronic nonhealing genital ulcers with exuberant granulation tissue or with more verrucous growth
Extragenital Involvement
Leishmaniasis Often starts as nonhealing papule or nodule that enlarges slowly and may develop central ulceration or raised, indurated border
Paracoccidiomycosis Red painful plaques and nodules on oral and nasal mucosa
Pyoderma gangrenosum Painful solitary nodule or pustule than transforms into ulcer with dusky, undermined border
Cutaneous
Tuberculous chancres: firm shallow ulcer with
Cutaneous tuberculosis Tuberculous chancres: firm shallow ulcer with granular base; may also have dissemination to organs such as liver or bone
tuberculosis
granular base; may also have dissemination to organs such as liver or bone
CLINICAL COURSE AND PROGNOSIS
Treatment has been shown to halt progression of lesions, and healing typically proceeds inward from the ulcer margins. GI shows no tendency for spontaneous healing. If left untreated, GI may disseminate to internal organs, including the liver, ovaries, and uterus or to bone. If not correctly diagnosed, systemic dissemination can be fatal.20 If left untreated, genital complications include genital swelling that may progress to pseudoelephantiasis, phimosis, paraphimosis, and progressive tissue destruction that may lead to destruction of the whole penis or other involved organs.25 Another
26
major risk of untreated GI is the presence of painless ulcers that bleed easily upon contact greatly increases the risk of HIV transmission. Development of carcinoma is another serious but rare complication that is predicted to occur in 0.25% of cases. A recent case report demonstrated coexisting squamous cell carcinoma and GI in an HIV-infected patient.25 Malignancies should always be ruled out in cases of long-standing ulcers not responsive to treatment. Despite these complications, if proper treatment is initiated early in the course of disease, the prognosis is generally good.
MANAGEMENT
The optimal way to manage a possible case of GI is to establish diagnosis as soon as possible so appropriate antibiotics and specific patient education can be given. The patient should be educated about the complications of untreated GI and the risk for acquiring other STIs, including HIV. Several antimicrobial regimens have proven effective, but only a limited number of controlled trials have been published. Prolonged therapy is usually required to permit granulation and reepithelialization of the ulcers. It should be noted that standard treatment regimens used for other STIs such as chancroid may not be adequate in both dose and duration for GI, highlighting the importance of appropriate diagnosis. Table 174-2 outlines the most current treatment recommendations by both the Centers for Disease Control and World Health Organization.26,27 Duration of treatment should be for at least 3 weeks and until complete healing is achieved. The addition of another antibiotic to these regimens, specifically an aminoglycoside (gentamicin 1 mg/kg IV every 8 hours), can be considered if improvement is not evident within the first few days of therapy. The addition of aminoglycosides is particularly important in patients who are pregnant or HIV positive, given the aggressive clinical course in these subsets of patients. Children with GI should receive a short course of azithromycin 20 mg/kg. Children born to mothers with GI should receive prophylaxis with a 3-day course of azithromycin 20 mg/kg once daily.28
Relapse may occur 6 to 18 months after apparently effective therapy, thus requiring follow-up by the physician. Long-standing cases may be complicated by secondary bacterial infections or by fistula and abscess formation, which require surgical intervention and render antibiotic treatment alone ineffective.29 Patients with GI should be screened for other STIs, notably HIV and syphilis. Although donovanosis is uncommon in partners of index cases, all sexual contacts in the previous 6 months should be examined. Treatment of sexual partners is not necessary unless they develop signs and symptoms of GI.
ACKNOWLEDGMENTS
The authors acknowledge the contributions of Abdul- Ghani Kibbi, Ruba F. Bahhady, and Myrna El-Shareef, the former authors of this chapter.
3205
26
CDC (2015) WHO (2003)
Recommendationsa Azithromycin 1 g orally once weekly or 500 mg/day Azithromycin 1 g orally once; then 500 mg/day or Doxycycline 100 mg orally twice daily
Alternatives Doxycycline 100 mg orally twice daily or Ciprofloxacin 750 mg orally twice daily or Erythromycin base 500 mg orally four times daily or Trimethoprim-sulfamethoxazole one double-strength (160 mg/800 mg) tablet orally twice daily
Erythromycin 500 mg four times daily or Tetracycline 500 mg four times daily or Trimethoprim 80 mg/sulfamethoxazole 400 mg, 2 tablets, twice daily for a minimum of 14 days
Pregnancy Macrolide antibiotic (azithromycin or erythromycin) as dosed above
Pregnancy Macrolide antibiotic (azithromycin or erythromycin) as dosed above
aDuration of treatment with any regimen is for at least 3 weeks and until all lesions have completely epithelialized. CDC, Centers for Disease Control and Prevention; WHO, World Health Organization.

Figure 174-1 Granuloma inguinale, ulcerogranulomatous type. Beefy red, ulcerated plaque that bleeds easily. (Used with permission from A. Eichmann, MD.)

Figure 174-2 Granuloma inguinale, kissing lesions. Two adjacent ulcers that are essentially mirror images of each other. (Used with permission from Shukrallah Zaynoun, MD.)

Figure 174-3 Granuloma inguinale. Long-standing hypertrophic lesion causing significant destruction to surrounding tissue. (Reproduced with permission from the Graham Library of Wake Forest Department of Dermatology.)

Figure 174-4 Granuloma inguinale. Large ulcerative lesion with destruction to surrounding tissues.
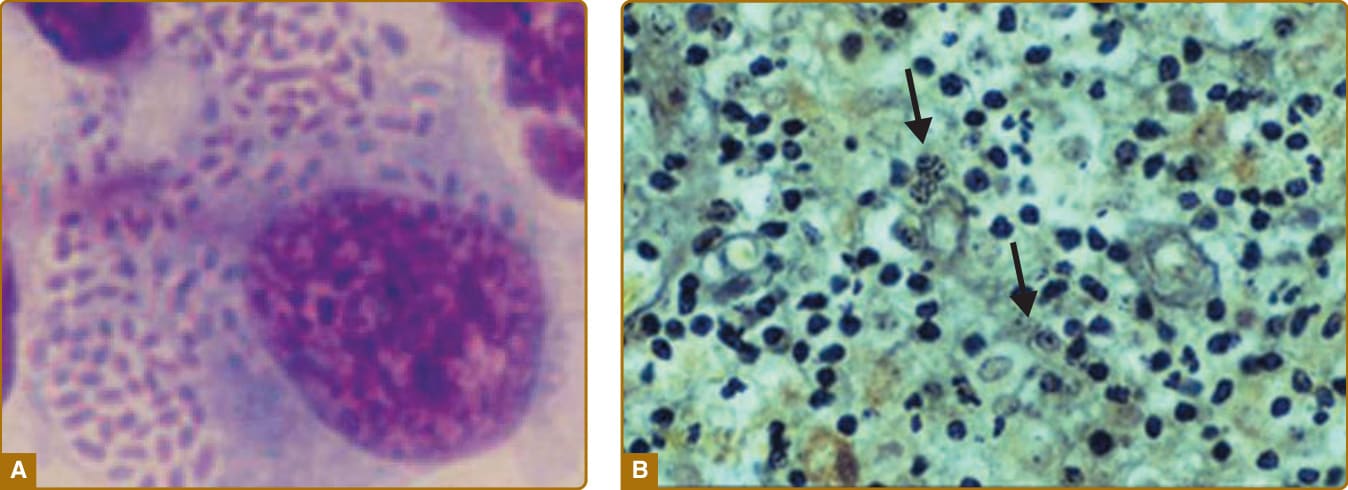
Figure 174-5 Granuloma inguinale. A, Large, mononuclear cell demonstrating multiple Donovan bodies. B, Donovan bodies (arrows) readily stained with Giemsa stain (Image A, From O’Farrell N. Donovanosis. In: Longo, DL, Fauci AS, Kasper DL, et al, eds. Harrison’s Principles of Internal Medicine. 18th ed. New York: McGraw-Hill; 2012:1321; with permission.)
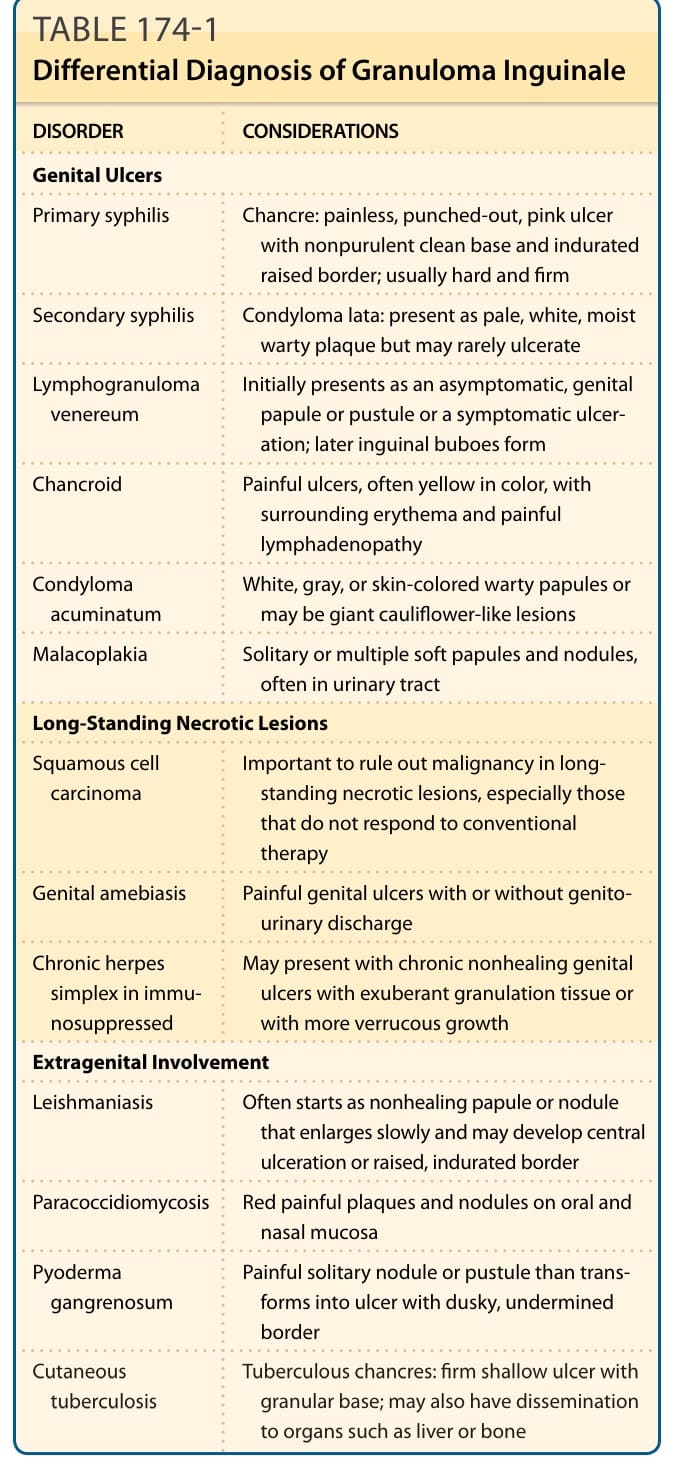
TABLE 174-1 Differential Diagnosis of Granuloma Inguinale
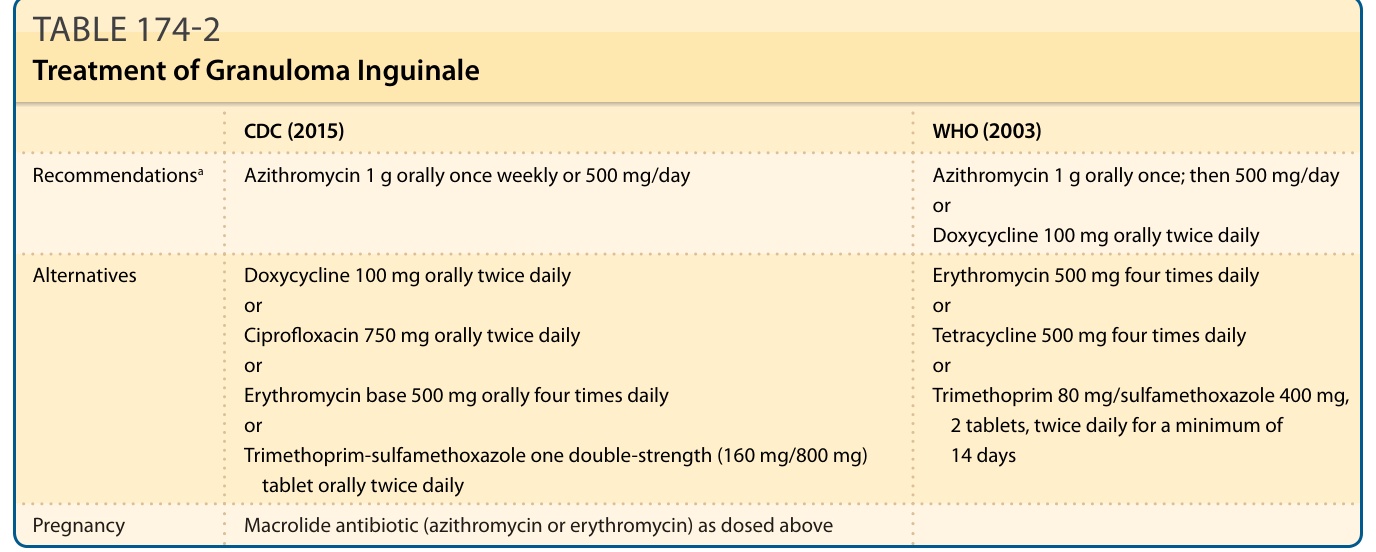
TABLE 174-2 Treatment of Granuloma Inguinale