Chancroid
26
AT-A-GLANCE
■ Chancroid is a sexually transmitted acute ulcerative disease usually localized at the anogenital area and often associated with inguinal adenitis or bubo.
■ Haemophilus ducreyi—a Gram-negative, facultative anaerobic coccobacillus—is the causative agent.
■ Chancroid is disappearing even from most countries where H. ducreyi was previously epidemic, with the exception of North India and Malawi. Nevertheless, recent sporadic case reports from Western Europe have been described, often initially misdiagnosed as genital herpes.
■ Painful, soft ulcers with ragged undermined margins develop 1 to 2 weeks after inoculation (usually prepuce and frenulum in men and vulva, cervix, and perianal areas in women).
■ H. ducreyi facilitates the transmission of HIV.
■ In contrast to a sustained reduction in the proportion of genital ulcer disease caused by H. ducreyi, the bacterium is increasingly found in the South Pacific region and in Africa as a common cause of nongenital cutaneous ulcers especially in children.
■ Laboratory culture of H. ducreyi is problematic, but greater sensitivity can be expected by nucleic acid amplification methods, which are not routinely available.
■ Azithromycin and ceftriaxone are recommended as single-dose treatment, enhancing compliance.
EPIDEMIOLOGY
Until the 1990s chancroid was seen most commonly in developing countries, especially in Africa and Asia, where it was isolated from more than 50% of patients with genital ulcers.1-3 A systematic review analyzed 49 studies (35 were published during 1980-1999 and 14 during 2000-2014) on chancroid.4 During 1980-1999, the percentage of genital ulcers caused by Haemophilus ducreyi ranged from 0% in Thailand and China to 69% in South Africa. During 2000-2014, the percentage of genital ulcers caused by H. ducreyi was low (<10%) except for Malawi with 15% of genital ulcer disease5
and North India with 24% of genital ulcer disease.6 A recent report from Cuba described no infection with H. ducreyi in genital ulcer disease patients.7 In the United States, only 11 cases of chancroid were reported in
2015.8 In Europe, chancroid is restricted to rare sporadic cases, often misdiagnosed as genital herpes.9,10
The distinct decrease in prevalence has followed the introduction by the World Health Organization (WHO) of syndromic management for treating genital ulcer disease.4 Nevertheless, the global epidemiology of H. ducreyi is poorly documented because of difficulties in confirming a microbiologic diagnosis. As a result, this condition may be substantially underdiagnosed.8
Lower-class prostitutes appeared to be a reservoir in all previously reported outbreaks of this disease where men had a markedly higher incidence than women. Male circumcision is associated with a reduced risk of contracting chancroid.11 Several studies in Africa show that chancroid ulcer was an important risk factor for the heterosexual spread of HIV.12,13
In West Africa, it has been shown that 2% of female sex workers carry the organism asymptomatically.14 The duration of infectivity in the absence of treatment is estimated to be 45 days for women. The transmission rate from females to males is not known, in contrast to a reported transmission rate from males to females of 70% per sex act.15 Nonsexual transmission leading to nongenital skin ulcers mostly in children in the Asia Pacific region has been recently reported.16,17 Based on sequencing of whole genomes and defined genetic loci, it appears that the cutaneous H. ducreyi strains (Class II) diverged from the class I genital strains relatively recently.18
CLINICAL FINDINGS
The incubation period is between 3 and 7 days, rarely more than 10 days. No prodromal symptoms are known. The chancre begins as a soft papule surrounded by erythema. After 24 to 48 hours it becomes pustular, then eroded and ulcerated (Fig. 172-1); vesicles are not seen. The edges of the ulcers are often ragged and undermined (Fig. 172-2). The ulcer is usually covered by a necrotic, yellowish-gray exudate (Fig. 172-3), and its base is composed of granulation tissue that bleeds readily on manipulation. In contrast to syphilis, chancroid ulcers are usually tender and/ or painful, not indurated (soft chancre). The diameter varies from 1 mm to 2 cm. Half of the males present with a single ulcer, and most lesions are found on the external or internal surface of the prepuce, on the frenulum, or on the glans (Fig. 172-4). Lesions may spread by extension and autoinoculation, leading to “kissing ulcers” (Fig.172-5) or large serpiginous ulcers involving the groin or thigh. Meatus and shaft of the penis and the anus (Fig. 172-6) are involved less frequently.
Edema of the prepuce is often seen. Rarely, if the chancre is localized in the urethra, H. ducreyi causes purulent urethritis.19
In females, the lesions are mostly localized on the vulva (Fig. 172-7), especially on the fourchette, the labia minora, and the vestibule. Vaginal, cervical, and perianal ulcers also have been described. Extragenital lesions of chancroid have been reported on the breasts, fingers, thighs, and inside the mouth. Trauma and abrasion may be important for such extragenital manifestations. Painful inguinal adenitis (bubo) occurs in up to 50% of patients within a few days to 2 weeks (average: 1 week) after onset of the primary lesion (Fig. 172-8). The adenitis is unilateral in most patients, and erythema of the overlying skin is typical. Buboes can become fluctuant and may rupture spontaneously. The pus of bubo is usually thick and creamy. Buboes are less common in female patients. Besides the common types of chancroid described above, a number of clinical variants have been reported (Table 172-1). Mild systemic symptoms can rarely accompany chancroid, but systemic infection by H. ducreyi has never been observed. The significance of the recent detection of
26
3187
26
3188
Giant chancroid Single lesion extends peripherally and shows extensive ulceration.
Large serpiginous ulcer Lesion that becomes confluent, spreading by extension and autoinoculation. The groin or thigh may be involved (Ulcus molle serpiginosum).
Phagedenic chancroid Variant caused by superinfection with fusospirochetes. Rapid and profound destruction of tissue can occur (Ulcus molle gangrenosum).
Transient chancroid Small ulcer that resolves spontaneously in a few days may be followed 2 to 3 weeks later by acute regional lymphadenitis (French: chancre mou volant).
Follicular chancroid Multiple small ulcers in a follicular distribution.
Papular chancroid Granulomatous ulcerated papule may
Papular chancroid Granulomatous ulcerated papule may resemble donovanosis or condylomata lata (Ulcus molle elevatum).
resemble donovanosis or condylomata lata (Ulcus molle elevatum).
genetic material of H. ducreyi in oesophageal lesions of HIV patients20 is not yet clear.
DIFFERENTIAL DIAGNOSIS
The 3 classic etiologic agents for genital ulceration are (a) H. ducreyi, (b) Treponema pallidum, and (c) herpes simplex. The clinical appearance of the diseases caused by these 3 organisms can be extremely variable in both men and women, making clinical diagnosis of genital ulcer disease with reasonable certainty possible only for a minority of patients.21 The etiology of genital ulcers (Table 172-2)22 also differs considerably by geographic region. In industrialized countries, isolated painful chancres are most likely caused by herpes simplex virus.23 In a high percentage of genital ulcers, no pathogen can be isolated but coinfections with syphilis (Ulcus mixtum) or herpes simplex are not uncommon.24,25
DIAGNOSIS
H. ducreyi appears as small Gram-negative rods. Microscopy may be done on ulcer swabs, but because of low sensitivity and specificity, microscopy is not routinely recommended for diagnosis. A definitive diagnosis of chancroid requires the identification of H. ducreyi on culture media; however, the advent of more-sensitive DNA amplification techniques has demonstrated that the sensitivity of culture of H. ducreyi reaches only 75% at best. Culture is particularly important when testing of antimicrobial susceptibility pattern is needed, such as in cases of therapeutic failure. H. ducreyi will only survive a few hours on the swab, and bedside inoculation of culture plates (2 different selective, enriched culture media) followed by immediate incubation can be done to reduce loss of viable bacteria during transportation.26
DISEASE ETIOLOGIC AGENT
Most Likely Genital herpes Herpes simplex virus Type 1 and Type 2
Syphilis Treponema pallidum
Lymphogranuloma venereum Chlamydia trachomatis serovars L1 to L3
Consider Other bacterial sexually transmitted infection:
Donovanosis (formerly granuloma inguinale) Klebsiella granulomatis (formerly Calymmatobacterium granulomatis)
Other bacterial infections Streptococcus species, staphylococcal and fusospirillary infections, Mycobacterium tuberculosis, Corynebacterium diphtheriae (very rare)
Viral infections:
Acute HIV infection Chronic anogenital ulcers in HIV-positive patients
HIV Cytomegalovirus
Ulcus vulvae acutum Epstein-Barr virus, cytomegalovirus, adenovirus, and others
Genital herpes zoster Varicella-zoster virus
Parasitic infections:
Amebiasis Entamoeba histolytica
Leishmaniasis Leishmania species
Scabies Sarcoptes scabiei
Inflammatory diseases:
Behçet disease
Aphthosis
Crohn disease
Pyoderma gangraenosum
Drug induced:
Fixed drug eruption For example, Trimethoprimsulfamethoxazole
Toxic For example, Foscarnet
Traumatic and selfinduced genital ulcers and neoplasms
Always Rule Out Genital herpes Herpes simplex virus Type 1 and Type 2
Syphilis T. pallidum
HIV infection
HIV infection
Specimens taken for culture also may be used for nucleic acid amplification techniques. These are excellent for demonstrating H. ducreyi in clinical sample material with higher detection rates than culture. Various different in-house polymerase chain reaction methods have
26
■Painful inguinal adenitis (up to 50%)27 (see Fig. 172-8)
■Painful inguinal adenitis (up to 50%)27 (see Fig. 172-8)
■Spontaneous ruptures of inguinal buboes with occurrence of large abscesses and fistula formation (rare)
■Spontaneous ruptures of inguinal buboes with occurrence of large
abscesses and fistula formation (rare)
■Spreading of Haemophilus ducreyi to distant sites (“kissing ulcers” [see Fig. 172-5] and/or extragenital lesions resulting from autoinoculation; the phenomenon of spreading of Hd through autoinoculation occurs in 50% of male patients)
■Spreading of Haemophilus ducreyi to distant sites (“kissing i i ulcers” [see Fig. 172-5] and/or extragenital lesions resulting from autoinoculation; the phenomenon of spreading of Hd through autoinoculation occurs in 50% of male patients)
■Esophageal lesions in HIV patients20
■Esophageal lesions in HIV patients20
■Acute conjunctivitis (very rare)28
■Acute conjunctivitis (very rare)28
■Bacterial superinfection (including anaerobes) leading to extensive destruction (rare)
■Bacterial superinfection (including anaerobes) leading to extensive
destruction (rare)
■Scarring leading to phimosis (rare)
■Scarring leading to phimosis (rare)
■Erythema nodosum (very rare)29
■Erythema nodosum (very rare)29
■Enhanced HIV transmission (3-fold to 10-fold increased risk)
■Enhanced HIV transmission (3-fold to 10-fold increased risk)
been described, some of which have the advantage of simultaneously testing for other relevant pathogens, in particular T. pallidum and herpes simplex virus.26
COMPLICATIONS
In about half of the untreated patients, the course is that of spontaneous resolution without complications. As a consequence of delay in treatment, various complications may occur (Table 172-3).
PROGNOSIS AND CLINICAL COURSE
The disease is usually self-limited. Occasionally, without treatment, genital ulcer and inguinal abscess have been reported to persist for years. Local pain is the most frequent complaint. If no clinical improvement is evident 1 week after the start of therapy, incorrect diagnosis, coinfection with another sexually transmitted infection, concomitant HIV infection, poor compliance, or a resistant strain of H. ducreyi must be considered. Infections do not confer immunity and reinfections are possible. To avoid reinfections, patients must be instructed to use condoms properly.
TREATMENT
Beginning in the 1970s with the emergence of β-lactamase–producing strains of H. ducreyi treatment failures became common. Plasmid-mediated resistance to tetracycline, sulfonamides, chloramphenicol, and aminoglycosides also has been reported.30,31 Little is known about chromosomally mediated resistance in H. ducreyi, but decreased susceptibilities to various antibiotics in the absence of identifiable resistant plasmids suggests such mechanisms.30 Based on in vitro susceptibility, the most active drugs against H. ducreyi are azithromycin, ceftriaxone, ciprofloxacin, and erythromycin. Worldwide, several isolates with intermediate
3189
26
ANTIBIOTICS DOSAGE LIMITATIONS
Azithromycin 1 g orally in a single dose High cost, limited availability
or
Ceftriaxonea 250 mg IM in a single dose Parenterally, may perform less well in HIVpositive patients
or
Ciprofloxacin 500 mg orally twice daily for 3 days High cost, compliance, pregnancy
or
Erythromycin base 500 mg orally q.i.d.
Compliance, GI intoler-
Erythromycin base 500 mg orally q.i.d. for 7 days Compliance, GI intolerance, QT interval prolongation
for 7 days
ance, QT interval prolongation
aWHO recommends as alternative therapy only.
bLautenschlager S, Kemp M, Christensen JJ, et al. 2017 European guideline for the management of chancroid. Int J STD AIDS. 2017;28(4):324-329. Q.i.d., quarter in die sumendus (which is same as q.d.s.)
resistance to either ciprofloxacin or erythromycin have been reported.31 Although no antimicrobial susceptibility data for H. ducreyi have been published for 2 decades, it is still assumed that the infection will respond successfully to treatment with recommended cephalosporin-, macrolide-, or fluoroquinolone-based regimens.32 Table 172-4 lists the regimens recommended by the Centers for Disease Control and Prevention, the WHO, and the European STI Guidelines (2017).26,33,34 Antibiotic combinations (eg, ceftriaxone and streptomycin) showed synergy in an animal model and may be promising to improve single-dose treatment, but clinical evaluation is needed.35 Local treatment consists of antiseptic dressings (eg, povidone-iodine). Suppurative nodes should not be incised; if necessary, they can be punctured to prevent spontaneous rupture and sinus tract formation. A large syringe should be used and the fluctuant buboes entered laterally through normal skin. In patients with phimosis, a circumcision may be necessary when all active lesions have healed. In pregnancy, ceftriaxone is the preferred drug, but azithromycin also can be used.36
Even after correct treatment, relapses occur in approximately 5% of patients and retreatment with the original regimen is recommended. Usually reinfection by an untreated sexual partner is the suspected cause of relapse. HIV infection and lack of circumcision appear to be associated with increased likelihood of infection with H. ducreyi and treatment failure.11 In resourcepoor areas of the world, syndromic management can be recommended, but local epidemiology must be considered.18,34 Flow charts for the management of genital ulcers have been developed that do not require laboratory identification of the causative pathogen.37
3190
If a patient complains of one or more small blisters or an ulcer with a history of recent blisters, then herpes management should be followed. If an isolated small ulcer and painful matted gland is present, lymphogranuloma venereum, chancroid, and syphilis should be treated, and if only an ulcer is present, syphilis and chancroid should be treated.37
RELATION BETWEEN HIV INFECTION AND CHANCROID
During the 1990s, renewed interest in chancroid led to evidence that genital ulcers promote the heterosexual transmission and acquisition of HIV.38-42 During this time it was shown that effective treatment of genital ulcers reduced the incidence of HIV.43
Furthermore, it was shown that concomitant HIV infection has clinically significant effects on the course of the chancroid disease, and failure of single-dose12
or short-course40 therapy for chancroid in men is associated with HIV-1 seropositivity. A wide variation of the clinical picture of chancroid has been observed in HIV-infected patients.40 As in every patient with a sexually transmitted infection, patients with chancroid should also be tested for HIV antibodies and HIVseropositive patients with chancroid should be monitored closely and treated with a multiday regimen.
PREVENTION
The augmentation of the HIV epidemic by H. ducreyi, especially in Africa, has made chancroid control an urgent priority. As a result of the widespread syndromic treatment of genital ulcers combined with behavioral change within communities in response to the global HIV epidemic, chancroid has been nearly eliminated in many countries where it was previously endemic. In the rare case of diagnosis of chancroid nowadays,4,9,10 patients should be advised to abstain from sexual activity until all clinical lesions have cleared. Sexual contacts of the patient (within 10 days of symptom presentation) should be examined and treated regardless of whether symptoms of the disease are present, as asymptomatic carriage of H. ducreyi is possible.14 Antibiotics may provide some protection from reinfection; a single dose of azithromycin lasted as long as 2 months after treatment.44 Chancroid survives in populations in which many men are having sex with a few women. As a result of the dramatic decrease of the incidence of chancroid with only a few exceptions,4 eradication seems to be a feasible public health objective.45
Nevertheless, H. ducreyi should be considered as a cause of chronic limb ulcers in adults, and especially in children, in the Pacific region and Africa.16-18 The reservoir for H. ducreyi cutaneous infection remains to be elucidated.

Figure 172-1 Early sharply circumscribed ulcer in the coronal sulcus.

Figure 172-2 Ragged edges of a soft ulcer.

Figure 172-3 Chancroid with necrotic, yellowish-gray exudates.

Figure 172-4 Isolated small soft chancre on the glans.

Figure 172-5 Spreading of Haemophilus ducreyi by autoinoculation (“kissing ulcer”) from the frenulum to the glans.

Figure 172-6 Anal chancroid.

Figure 172-7 Vulvar chancroid with undermined edges.

Figure 172-8 Small soft ulcer on the internal surface of the prepuce with painful, fluctuant inguinal adenitis (bubo).
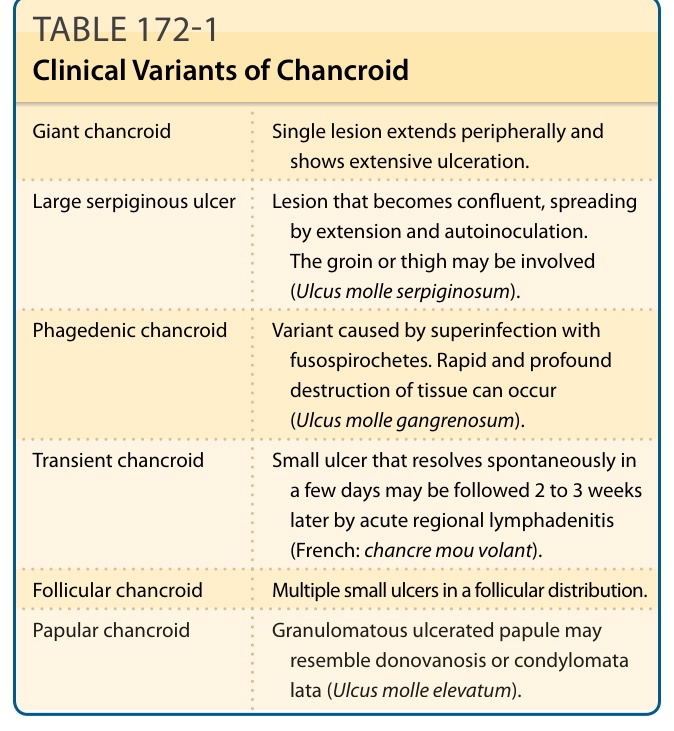
TABLE 172-1 Clinical Variants of Chancroid
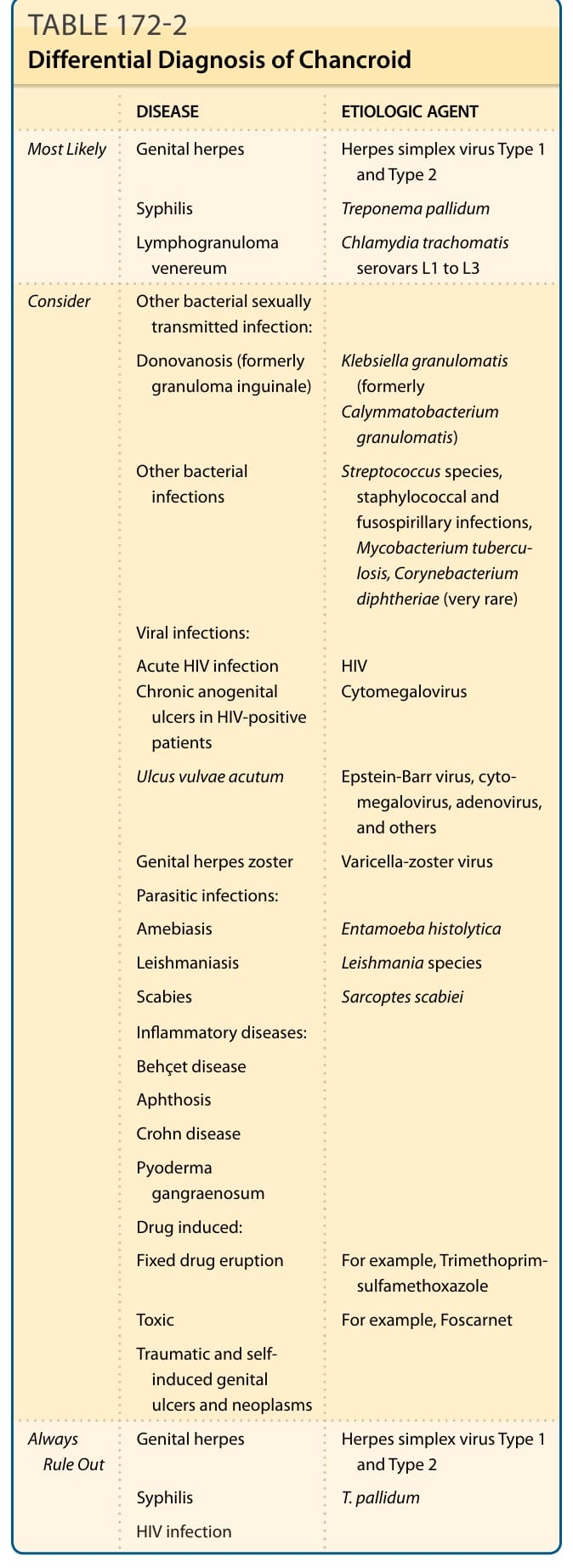
TABLE 172-2 Differential Diagnosis of Chancroid
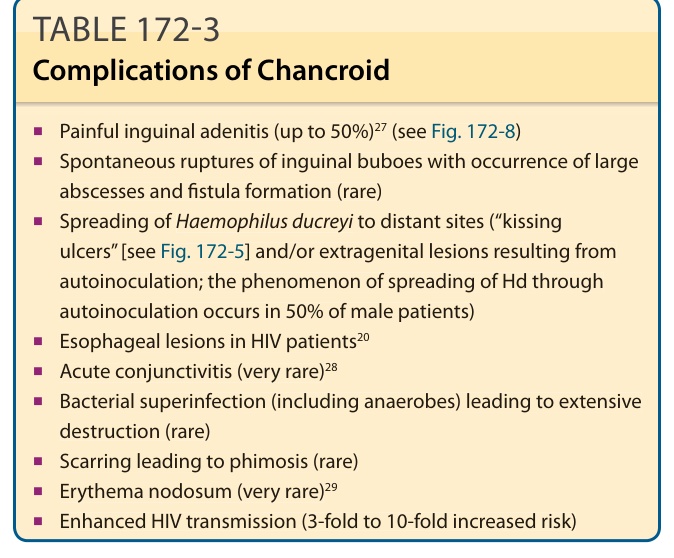
TABLE 172-3 Complications of Chancroid
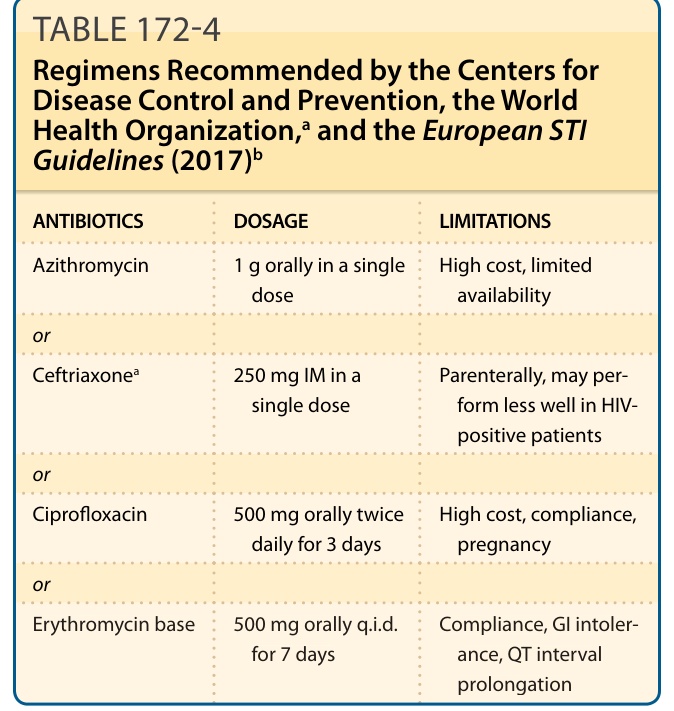
TABLE 172-4 Regimens Recommended by the Centers for Disease Control and Prevention, the World Health Organization,a and the European STI Guidelines (2017)b