Endemic (Nonvenereal) Treponematoses
26
INTRODUCTION
The endemic treponematoses are infectious diseases caused by microorganisms that are closely related to Treponema pallidum, the causative agent of syphilis. This group of entities includes (1) pinta, caused by Treponema carateum; (2) yaws, caused by T. pallidum ssp. pertenue; and (3) bejel, caused by T. pallidum ssp. endemicum. Although all these entities are caused by Treponema species, there are important differences between the endemic treponematoses and syphilis, including a nonvenereal form of transmission, an endemic occurrence in very specific geographic areas, a tendency to affect children rather than sexually active adults, and a less likely risk for congenital transmission to occur. In common with syphilis, every endemic treponematosis goes through an early stage (including primary and secondary), a period of latency, and a late stage. Significant morbidity is associated with progression of the disease, mainly affecting the skin, bone, and cartilage, leading to significant disfigurement, pain, disability, and social isolation, causing more suffering to already disadvantaged populations living in poverty. From an epidemiologic point of view, global efforts commanded by the World Health Organization (WHO) from 1952 through 1964 resulted in more than 50 million individuals who were treated for endemic treponematosis, with special attention to yaws. The global incidence of endemic treponematoses was reduced significantly, by 95%, from 50 million cases worldwide to a merely 2.5 million cases.1 However, after all the efforts of such campaign, the sustainability of the control program was transferred to local primary care systems in endemic areas. Because of waning and poor commitment in such surveillance programs, there has been a resurgence in the incidence of the endemic treponematoses. A recent study estimates that at least 89 million people are living in yaws-endemic areas.2 The WHO now recognizes all endemic treponematosis as neglected tropical diseases.3 The current WHO goal is to eliminate yaws by 2020; stricter and more sensitive surveillance programs are required to reach such goal. Table 171-1 shows a quick comparison among the three diseases.
PINTA
AT-A-GLANCE
■ Pinta is a chronic infectious and contagious disease recognized by the World Health Organization as a neglected tropical disease.
■ It is the most benign form of endemic treponematosis, with clinical manifestations limited to the skin, including vitiligo-like achromic lesions as well as hyperpigmented lesions.
■ It affects people of all ages.
■ It is neither sexually transmitted nor congenitally acquired.
■ Treatment includes single or divided dose of longacting benzathine penicillin (1.2 MU for adults; 0.6 MU for children).
INTRODUCTION
INTRODUCTION
DEFINITIONS
Pinta, also known as azula (blue), carate, and mal de pinto (pinto sickness), is the most benign of the endemic treponematosis because it affects only the skin. The word pinta comes from Spanish for painted, spot, or mark.4
The etiologic agent of pinta, Treponema carateum, cannot be distinguished morphologically or serologically from the not-yet-cultivable T. pallidum subspecies that cause venereal syphilis, yaws, and bejel.1,2
HISTORICAL PERSPECTIVE
Pinta is considered the first treponematosis to occur in humans. It was described in Aztec and Caribbean Amerindians in the early years of the 16th century.5,6
Initially, it was thought that a pathogenic fungus caused pinta. However, two observations suggested otherwise. First, laboratory studies of pinta patients’
26
FEATURE PINTA YAWS BEJEL
Etiology Treponema carateum Treponema pallidum ssp. pertenue Treponema pallidum ssp. endemicum
World distribution, main areas Probably present focally in Brazilian and Venezuelan green forest Papua New Guinea, Solomon Islands, and Ghana African Sahel and Saudi Arabia
Climate conditions Tropical green forest Tropical humid Hot and dry climate
Population affected Children and adults Mostly children Mostly children
Transmission Close contact Close contact Close contact and fomites
Primary lesion Evident, can be multiple, several locations One to several, lower extremities Rarely evident
Predominant lesion Vitiligo-like and hyperchromic lesions Exudative, papillomatous or papulosquamous lesions Moist lesions near mucosal surface or intertriginous areas
Nonskin involvement None Periositis, osteitis Periositis, osteitis
Nonskin involvement None Periositis, osteitis Periositis, osteitis
sera showed that result for the Wassermann test, an early serology test for syphilis (STS), was positive in the majority of cases. Second, treatments that were effective against syphilis (ie, mercury and arsenicals) were also effective against pinta.7 In 1938, Armenteros and Triana (Cuba)6 recognized Treponema carateum as the causative agent of pinta. Leon Blanco, in Mexico, reproduced the disease by inoculating exudates on himself and human volunteers in 1942. The same author also demonstrated that patients with late-stage pinta could not be reinfected, but patients whose early-stage pinta had been cured could be reinfected.8,9
Padilha-Gonçalves established that pinta was a different treponematosis from syphilis or yaws.10,11
EPIDEMIOLOGY
EPIDEMIOLOGY
Most patients acquire the infection during childhood. There is no difference between the two sexes. The indigenous population is the most affected.3
In the 1950s, pinta existed in Mexico, Central America, and the northern countries of South America. The WHO then considered the disease endemic in 15 Latin American countries, including Brazil, Colombia, Ecuador, Peru, and Venezuela. Lower numbers of cases were seen in Bolivia, Dominican Republic, El Salvador, Guatemala, Haiti, Honduras, and Nicaragua. The disease was occasionally seen in Cuba, Guadeloupe, Panama, Puerto Rico, and the Virgin Islands.12
The last report of cases from Colombia was in 1977.12
Although Cuba had reported its last case in 1975, in 1998, a patient who had lived in Cuba for 7 years was diagnosed with pinta in Austria.13 In 1982 and 1983, clinical evidence of pinta was discovered in 20% of the examined inhabitants of a remote village of Panama.14
In Brazil, the disease was supposed to be extinct until 1975, when 265 new cases of pinta were diagnosed among Indians from Baniwas, Canamari, Paumari, and Tikuna ethnic groups.4,5,15 These Indians lived in small communities on the banks of the Amazon river, including the Içana, Juruá, Purus, and
3174
upper Negro rivers as well as in some tributaries of the western Amazon river. Since 1979, no further cases of pinta have been reported to the WHO from previously Brazilian endemic areas.5,15
Because of the lack of surveillance data, the current prevalence of pinta is unknown; it is believed that the disease still exists in very isolated communities in remote rural areas of Mexico and South America, especially in a few scattered areas in the Brazilian Amazon rainforest. Nonpublished cases have been reported affecting the Yaruro community in Venezuela by R. Hernandez-Perez (FB, personal communication), near the border with Brazil. There is no proof of a spontaneous cure for the disease; because cell-mediated immunity is not completely effective, the infection persists indefinitely. Patients may harbor subclinical disease and be contagious for a long time. It has been said that pinta was man’s best friend: it follows him to the grave.12
CLINICAL FEATURES
CLINICAL FEATURES
CUTANEOUS FINDINGS
The disease is classified into two different clinical stages, the primary and late stages. The primary stage is characterized by two phases, an early phase or initial period, and a secondary phase or period of cutaneous dissemination. According to Padilha-Gonçalves,10,11 the initial period appears 7 to 20 days after the treponema inoculation. The primary lesions consist of one to several erythematous scaly papules (Fig. 171-1) affecting most commonly the face, upper and lower extremities, or other exposed areas. These lesions tend to grow in extension, producing erythematosquamous or erythematous, hyperpigmented plaques, varying in size and shape (arciform, circinate, polycyclic, and serpiginous) (Fig. 171-2). Generally, the lesions are asymptomatic, but eventually patients may complain of pruritus (Fig. 171-3). Regional lymphadenopathy is common. During early infection, the STS
26
result may be negative for antibodies to nontreponemal (cardiolipin) and treponemal antigens. Within 6 months to 2 to 3 years of the first lesions’ appearance, hypochromic, erythematous, or erythematohypochromic patches appear, initiating the period of cutaneous dissemination (secondary phase). Those lesions present variable degrees of hyperkeratosis.5,12 The lesions are small and occasionally nummular in morphology. They gradually enlarge and coalesce, affecting large areas of the body; the centers of the lesions look like normal skin. These lesions are referred to as pintides and are initially red to violaceous and later become slate-blue, brown, gray, or black. Lesions from different periods may be present in a single patient, giving a polymorphic clinical picture.1,3,4
The late or tertiary stage, which appears 2 to 5 years after the first lesion, is characterized by the appearance of achromic patches, especially over body prominences, such as the dorsum of the hands, wrist, elbows, anterior aspect of the tibia, ankles, and dorsal and plantar areas of the foot. In this period, large hypochromic areas commonly appear on the upper extremities, trunk, and thighs. One may observe cutaneous atrophy, achromic dotlike lesions, and multiple hyperchromic lesions, producing a mottled pattern. The presence of hypochromic patches with irregular borders and hypochromic macules is quite frequent on buttocks (Fig. 171-4). Curiously, the groin, genital area, and the inner and upper parts of the thighs are often spared. Another very important aspect of the late phase of pinta is the appearance of hyperchromic and hyperkeratotic patches most commonly on exposed areas of the upper and lower extremities. On the palmar surfaces, hyperpigmented and achromic patches associated with hyperkeratosis are usually observed (Fig. 171-5). Plantar hyperkeratosis is quite frequent. In some patients, even with a prolonged history of the disease, the cutaneous lesions may be confined to a limited area of the body.5,12
NONCUTANEOUS FINDINGS
There is no evidence of involvement of other organs, even after many years of evolution.2,5,8
3175
26
COMPLICATIONS
Although early pinta lesions heal within several months after specific treatment, the therapy cannot reverse the skin changes of late pinta that can stigmatize those who were infected.8 Unlike the other treponematoses, neither destructive skin and bone lesions nor cardiovascular and neurologic manifestations are seen in patients with pinta.3
3176
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
The disease is caused by T. carateum, an organism that is morphologically and antigenically identical to the etiologic agents of syphilis and yaws.3,12,15 However, T. carateum has not been propagated in experimentally infected animals and has not been characterized genetically.16
The disease is found in warm and humid environments and is usually acquired during early childhood. Pinta is thought to spread mostly via direct contact with an infected person, although it is said that transmission may occur via fomites. The treponema enters the skin through small cuts, scratches, or other skin damage. The only known reservoir is human beings.3,12,15
DIAGNOSIS
DIAGNOSIS
LABORATORY TESTING
Dark-field microscopy can be used to identify viable spirochetes from lesion swabs; however, in most settings where pinta is still prevalent, this technique is not routinely available. Therefore, serology remains the cornerstone of diagnosis. The T. pallidum particle agglutination (TPPA) and hemagglutination (TPHA) assays are used to detect Treponema-specific antibodies; when the result is positive, it usually remains positive for life. The venereal disease research laboratory (VDRL) and rapid plasma reagin (RPR) tests are nonspecific tests. Although these tests are less specific, they are more accurate to reflect disease activity than TPPA or TPHA, with titers falling rapidly after successful treatment.3 However, serologic techniques cannot distinguish pinta from syphilis or any of the other nonvenereal treponematoses.
PATHOLOGY
The histopathologic examination is important for the diagnosis of pinta. The primary lesions are characterized by mild acanthosis and spongiosis, with lymphocyte migration and vacuolar degeneration of the basal cell layer, but in the dermis, the changes consist of a slight lymphohistiocytic and plasmocytic infiltrate and mild vascular reaction.5,15 The hypochromic lesions from the secondary phase present with moderate hyperkeratosis, acanthosis, and spongiosis, plus a superficial infiltrate around the thickened vessels. In the erythematous and squamous lesions, acanthosis, hyperkeratosis, and spongiosis are seen in the epidermis plus a lymphohistiocytic infiltrate in the dermis with edema and vascular proliferation in the papillary dermis. In the achromic lesions, there are hyperkeratosis, atrophy of the epidermis, and complete absence of melanin in the basal layer but some perivascular
Primary Stage
■Tinea
■Psoriasis
■Erythema dyschromicum perstans
■Tinea versicolor
■Eczema
■Leprosy
■Cutaneous tuberculosis
Late Stage
Late Stage
■Vitiligo
■Vitiligo
inflammatory infiltrate. It is possible to demonstrate the presence of treponema in the epidermis through special stains such as Warthin-Starry, in all lesions, except for those that are already achromic.4,6,12
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
See Table 171-2.
CLINICAL COURSE AND PROGNOSIS
CLINICAL COURSE AND
PROGNOSIS
Primary and secondary lesions of pinta may resolve spontaneously. However, despite treatment, patients may present with lifelong late lesions.3,12,15
MANAGEMENT
MANAGEMENT
MEDICATIONS
The recommended treatment for pinta, irrespective of the stage of the disease, is a single or divided dose of long-acting benzathine penicillin (1.2 MU for adults; 0.6 MU for children), which renders the lesions noninfectious in less than 24 hours. Within a few days, the hypochromic and erythematosquamous lesions disappear. Later, the hyperpigmented and recent achromic lesions disappear. The old achromic patches do not usually respond to the treatment and persist for life, giving a vitiligo-like clinical aspect in some patients.5,12,17
PREVENTION AND SCREENING
At present, the WHO has not developed a specific strategy for the control or eradication of pinta. However, it has launched a campaign to eradicate yaws by 2020. The strategy is based on mass treatment of endemic communities with an oral dose of azithromycin, a macrolide antibiotic with demonstrated efficacy
26
against yaws.1,2,7,18 If T. carateum is sensitive to azithromycin, this treatment strategy could have a concomitant effect on pinta in areas of Latin America where yaws and pinta may be coendemic.7
YAWS
AT-A-GLANCE
■ Yaws is the most prevalent of the endemic treponematosis.
■ It is most commonly seen in children.
■ Countries with the largest number of cases are Papua New Guinea, the Solomon Islands, and Ghana.
■ Primary lesions are either papillomatous or ulcerated lesion on the lower extremities.
■ Secondary lesions are multiple, bilateral, and symmetrical. They are either moist and papillomatous (raspberry-like) or dry and papulosquamous.
■ Eroded or hyperkeratotic palmoplantar lesions with fissuring induce a crablike gait (crab yaws).
■ Periostitis and dactylitis are common.
■ Penicillin and azithromycin are both effective in the treatment of patients with yaws.
INTRODUCTION
INTRODUCTION
DEFINITION
Yaws is an infectious disease caused by T. pallidum ssp. pertenue. The term yaws probably originates either from the Carib word yaya (sore) or from the African word yaw (berry). The clinical appearance of a typical lesion of yaws, resembling a raspberry, explains also one of the names given to the disease, framboesia tropica (framboesia is the French word for raspberry). Other names used to refer to the same disease include pian, buba, bouba, parangui, and paru.
HISTORICAL PERSPECTIVE
Yaws was the 17th century term used by the Dutch physician Willen Piso when he wrote one of the first clinical descriptions of the disease in South America. In 1679, Thomas Sydenham described classical yaws in African slaves and thought it was the same disease as syphilis. In 1905, Castellani found spirochetes in the ulcers of patients with yaws from Ceylon.18
Some phylogenetic analyses identify yaws as the oldest of the treponemal diseases and suggest that syphilis and bejel evolved subsequently. The Unitarian hypothesis proposed by Hudson stated that syphilis, as a venereal disease, arose from yaws brought to
3177
26
Europe by the slave trade. However, recent genetic studies by Gray and Mulligan19 support the idea of a parallel evolution of the three subspecies of T. pallidum responsible for yaws, syphilis, and bejel.
EPIDEMIOLOGY
EPIDEMIOLOGY
The geographical distribution of yaws has changed dramatically since the 1950s following the very successful programs developed by the WHO and UNICEF to eradicate the disease. Those programs were directed to identify active disease as well as latent disease and to treat them with long-acting penicillin. Furthermore, the programs were also intended to establish alert systems for early detection of any new cases. In 1950, yaws was still present in tropical and subtropical areas around the world, including Central and South America, most of Central Africa, India, Southeast Asia, and the Western Pacific region. Since then, the map has changed drastically; the disease has almost disappeared from the Americas. Ecuador was the last country reporting elimination of the disease; Guyana reported residual cases in 2003. India also reported elimination of the disease by the year 2003. The number of affected African countries has diminished, and the disease is now confined to few countries of East Central Africa. On the contrary, yaws is still clearly present in Western Pacific countries, such as Papua New Guinea, the Solomon Islands, and Vanuatu. A recent systematic review published in 2015 identified 256,343 cases reported to the WHO in 13 endemic countries in the 2010 to 2013 period.2,3 The prevalence of active disease in such endemic areas ranged from 0.31% to 14%, and the prevalence of latent disease ranged from 2.4% to 31%. Near 84% of reported cases came from three countries, Papua New Guinea, the Solomon Islands, and Ghana.
CLINICAL FEATURES
CLINICAL FEATURES
CUTANEOUS FINDINGS
Yaws is transmitted by direct skin contact with an infectious lesion and facilitated by abrasion or erosion of the skin. Children are most commonly affected, up to 15 years of age, with a peak incidence between 6 and 10 years. The disease affects people living in rural communities under poor sanitary condition in tropical areas of the world with an average temperature over 27°C (80°F) and heavy rainfall. The primary lesion of yaws is usually a papule that develops 21 days (range, 9 to 90 day) after initial contact. The papule evolves into a proliferative, exudative, papillomatous lesion 2 to 5 cm in diameter or evolves into a crusted, nontender ulcer, most commonly located on the legs. Genital location is extremely uncommon. This primary lesion is known under different names, including “mother yaws,” “maman pian,” or “buba
3178
madre” (Fig. 171-6A). Even if left untreated, the lesion resolves spontaneously over a 3- to 6-month period, leaving a pigmented scar. A patient may have primary and secondary lesions simultaneously.20
Secondary lesions appear after 1 to 2 months (up to 24 months). They represent hematogenous and lymphatic spreading to the skin and bone. In the skin, the lesions can be exudative, proliferative, and papillomatous (Fig. 171-6B) (pianomes in French) or dry
A
B
C
and papulosquamous (pianides in French). The exudative papules (pianomes or frambresiomas) are usually generalized, bilateral, and symmetrical, from a few millimeters to 2 cm in diameter, soft, wet, red yellowish in color, with either a moist surface or a crust. By resembling raspberries, they are the most representative lesions of yaws. They can affect scalp and folds; in the latter location, they may resemble condyloma lata of syphilis. Mucosal lesions tend to be located around natural orifices, presenting as a bilateral exudative, angular cheilitis (Fig. 171-6C). The dry, papulosquamous papules (pianides) are multiple and generalized, and they can have annular or discoid morphology, with a squamous collaret (tinea yaws), grouped in a corymbose pattern. On the face, lesions may resemble psoriasis or seborrheic dermatitis. Multiple, florid lesions are associated with the wet seasons; they become scarce and restricted to intertriginous areas in dry climate. On the palms and soles, the lesions can be also exudative papules or papulosquamous plaques, keratodermic, with a tendency to form fissures (Fig. 171-7). Because the acral lesions are tender or painful, patients develop a peculiar gait, known as crab yaws. Pianic onychia is a paronychia that originates from hyperkeratotic lesions in the nail folds.21
All secondary yaws resolves, either spontaneously or after treatment, healing with or without scarring. If left untreated, the patient will enter the latent phase and remain as such for the rest of her or his life. Relapsing yaws tend to localize in perioral, perianal, and axillary areas. Relapses may occur for as long as 5 years after the initial infection. About 10% of untreated patients progress to the tertiary sate. Late-stage lesions are subcutaneous gummatous nodules with massive tissue destruction and necrosis, sometimes resulting in large serpiginous ulcerations, followed by debilitating deformity and contractures. The most common manifestations associated with this state are a result of simultaneous involvement of the skin and bone structures .The complete destruction of the nasal cartilage and the collapse of the nasal pyramid results in a deformity known as gangosa (Fig. 171-8). Pintoid dyschromia and palmoplantar hyperkeratosis have been described at this late stage (Fig. 171-9).
26
In areas of reduced transmission, because of climate condition or after mass treatment, a milder form of disease can be seen, associated with few lesions (attenuated yaws).
NONCUTANEOUS FINDINGS
Arthralgia, generalized lymphadenopathy, headaches, and malaise are common, as well as asymptomatic cerebrospinal fluid changes. The most important noncutaneous findings refer to the involvement of osteoarticular structures. In secondary yaws, early osteoperiostitis of fingers (dactylitis) or long bones (forearm, fibula, and tibia) might result in nocturnal bone pain swelling. Early bone changes can be visualized on radiography, and the
3179
26
thickened periosteum can be palpated clinically; a fusiform swelling of a finger affecting the two proximal phalanges is a common expression of this dactylitis (ghoul hand). The average number of bones involved is three, with common involvement of hand and feet. A specific hypertrophic bone exostosis of the paranasal area known as goundou is rarely seen nowadays. In late yaws, besides the destructive central face involvement known as rhinopharyngitis obliterans or gangosa, patients may also develop a saddle-nose deformity, bowing of the tibia, or sabre shins. Another manifestation includes the presence of juxtaarticular nodes. Opposite of tertiary syphilis, late yaws is not associated with cardiovascular or neurologic disease. Optic atrophy, however, has been reported in the tertiary stage.21 T. pallidum spp. pertenue is not associated with congenital transmission.
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
T. pallidum ssp. pertenue is a spiral-shaped, gram-negative bacteria that belongs to the family Spirochaetaceae, closely related to other subspecies of T. pallidum, from which it is morphologically and serologically identical. T. pallidum ssp. pertenue is 10 to 15 µm long and has a diameter of 0.2 µm; it is not seen on regular microscopy but can be seen on dark-light microscopy. A cytoplasmic membrane enclosed by a loosely associated outer membrane surrounds the bacterium. Some proteins of this outer membrane are able to induce opsonic activity.18 Treponema has a characteristic corkscrew motility and can swim efficiently in gel-like media or environment, such as the connective tissue, a factor that contributes to its virulence. The microorganism multiplies very slowly, at a rate of 1 every 30 to 33 hours. It does not grow on culture media but can be isolated and reproduced in experimental animals, such as rabbits and golden hamsters. In vitro assays based on Treponema protein synthesis have demonstrated that T. pallidum ssp. pertenue is sensitive to penicillin, tetracycline, and erythromycin. T. pallidum ssp. pertenue is 99.8% identical in its genomic sequence to T. pallidum ssp. pallidum. Established differences between the two microorganisms include a one pair base difference in the tpp15 gene, one nucleotide difference in the gpd gene, a base pair deletion in the tpr gene, sequence variation in the arp gene, and sequence variation of the intergenic spacer IGR19.18
The microorganism enters the skin by small abrasions. After penetrating the epidermis, it reaches the extracellular matrix and attaches to fibronectin-coated surfaces. After minutes, the spirochetes reach lymph nodes and disseminate extensively in hours. The lymph node enlarges and teems with treponemas for several weeks. In the skin, the initial reaction is mainly neutrophilic and later composed mainly of plasma
3180
cell. T. pallidum ssp. pertenue is seen as extracellular clusters in upper regions of the epidermis on immunohistochemistry staining. The immune response to the microorganism is both humoral and cellular. The organism, because of its low metabolic rate, is able to maintain infection with few viable cells, avoiding the stimulation of the immune system in the latent state. Adults rarely develop new skin lesions, suggesting that untreated individuals can develop immunity to reinfection.
DIAGNOSIS
DIAGNOSIS
The diagnosis is easy in the endemic areas, although attenuated yaws may be more challenging. Health care workers not familiar with the disease may need laboratory methods to confirm the diagnosis
LABORATORY TESTING
Treponemas can be detected in a wet preparation using dark-field microscopy. However, the scarce availability of the method in rural setting makes it unpractical. The best diagnostic aid is serology testing using the same techniques as in syphilis. Nontreponemal agglutination tests, such as the RPR and the VDRL, can be used for diagnosis and followup after treatment, as they are used in syphilis. False positives can be seen in patients with other tropical diseases such as malaria and leprosy, as well as in rheumatic diseases. Results of treponemal tests, such as TPHA, TPPA, and fluorescent treponemal antibody absorption (FTA-ABS) are also positive, but as in syphilis, they remain positive forever and are not useful for follow-up. The new rapid diagnostic test, including the immunochromatographic strips developed for syphilis, are also very useful and easy to use in the primary care setting. Differential diagnosis with syphilis itself might be tricky; real-time polymerase chain reaction remains, in such cases, the technique of choice, although it is expensive and limited to research centers. In such cases, epidemiologic and clinical data need to be carefully evaluated to establish the correct diagnosis.
PATHOLOGY
The histologic findings of yaws is quite similar to those of syphilis and include epidermal hyperplasia, focal spongiosis, and a dermal infiltrate. Some authors describe an early accumulation of neutrophils in the epidermis,18 but others state that is mainly plasmocytic from the beginning.1 Plasma cells predominate in all evolved lesions. An important difference with syphilis is that yaws does not induce vascular changes or endothelial proliferation. The same immunohistochemistry staining used in syphilis is quite useful in yaws by demonstrating the spirochetes in large numbers at the epidermal level.
IMAGING
Radiographic studies are particularly valuable in cases of periostitis and bone involvement; onion layering periosteal reaction and loss of clarity of the cortex are seen on plain radiographs (Fig. 171-10). Bowing of the tibia, destructive osteitis of facial bones (such as seen in gangosa), and the hypertrophic periostitis and exostosis seen in gondou are quite evident on radiology studies.
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
See Table 171-3.
CLINICAL COURSE AND PROGNOSIS
CLINICAL COURSE AND
PROGNOSIS
Primary and secondary lesions may resolve spontaneously. Up to 10% of patients in a latent stage may evolve into the most disfiguring, disabling late stage after 5 years of an untreated infection.
MANAGEMENT
MANAGEMENT
MEDICATIONS
Single-dose, long-acting penicillin has been the treatment of choice for yaws and the base of the successful eradication program. A dose of 1.2 million units for patients older than 10 years and a dose of 0.6 million units for those younger than 10 years is still the recommended regimen. Cure rates are above 95% for early active yaws.
26
Primary Lesion
■Leishmaniasis
■Tropical phagedenic ulcer
■Ecthyma
■Tuberculosis
■Buruli ulcer
■Sickle cell anemia
Secondary Lesions
■Eczema
■Psoriasis
■Syphilis
■Disseminated leishmaniasis
■Superficial mycosis
■Infective dermatitis of HTLV-1
■Leprosy
■Impetigo
■Pyoderma vegetans
Facial Lesions
■Leishmaniasis
■Lupus vulgaris
■Leprosy
■Paracoccidioidomycosis
■Rhinoscleroma
■Rhinosporidiosis
■Rhinoentomophthoromycosis
■T-NK lymphomas
Pintoid Lesions
Pintoid Lesions
■Vitiligo
■Vitiligo
■Pinta
■Pinta
HTLV, human T-lymphotropic virus; T-NK, it is a type of extranodal lymphoma caused by a proliferation of Natural Killer cells or T lymphocytes.
One oral dose of azithromycin (30 mg/kg, to a maximal dose of 2 g) is considered as effective as penicillin. Since 2012, the WHO considers the one single dose of azithromycin equivalent to the standard penicillin regimen. Oral tetracyclines, doxycycline, and erythromycin are considered alternative drugs for adults who are allergic to penicillin; erythromycin is the choice for children younger than 12 years of age. Oral therapy with azithromycin has many advantages over intramuscular penicillin therapy. When it is used in massive control programs, it can be administrated by less skilled health workers, and there is a reduced risk of anaphylaxis. However, a higher potential risk of developing resistance does exist when macrolides are used. In such cases, follow-up is recommended, allowing early retreatment with penicillin when needed. The effectiveness of therapy is expressed by several facts. Yaws lesions become noninfectious in 24 hours after therapy. Joint pain disappears in 24 to 48 hours. All clinical lesions resolve within 2 to 4 weeks after therapy. However, therapy will not resolve the destruction and deformities seen in the tertiary stage, thus justifying the importance of early intervention. RPR and VDRL testing titers decrease to a minimum within 6 to 12 months and become negative or remain at low titers in the next 2 years.
3181
26
PREVENTION AND SCREENING
The success of the WHO eradication effort in the 1950s was followed by a loss of continuity of such a program. The responsibility of maintaining the program was rapidly transferred to primary care systems that were either too weak or nonexistent in many endemic areas; this lack of continuity translated into a resurge of yaws in the past decades. Of note, the success of this program in India and Ecuador remain an exception because both countries have now been declared free of yaws. One of the conclusions of the 1950s efforts was the importance of subclinical or latent cases as a source of reinfection. The initial program was directed to treat active disease cases; resurveys of the treated communities showed that all new cases were individuals in the latent stage who did not receive treatment. In 2012, the WHO endorsed the commitment to eradicate yaws by the year 2020. This time, the strategy includes some variations. Surveys are directed to detect precisely the villages and communities affected by yaws. Oral azithromycin instead of intramuscular penicillin is the treatment of choice. The aim of the program is the treatment of the whole community, which will be repeated if the first attempt did not cover 90% of the population. The follow-up surveillance program will include passive and active search of new cases, tracing and treating contacts, intensive information and educational efforts, and monthly reporting of case (including no new cases) and yearly serologic surveys in children younger than 5 years. Indeed, improvement of education and sanitary conditions in affected communities are important factors that will facilitate the success of the eradication program.18
BEJEL
AT-A-GLANCE
■ Bejel is most commonly seen in children.
■ Transmission routes include direct contact and fomites by sharing utensils.
■ Countries and regions with the largest number of cases are the African Sahelian countries and Saudi Arabia (dry, hot climates).
■ Primary lesions are not easily identified or seen.
■ Secondary lesions are represented by moist plaques on mucosal and perioral areas, mimicking condyloma lata or angular stomatitis.
■ Gummas and gangosa represent tertiary lesions.
■ Involvement of the nasopharynx and larynx is common.
■ Periostitis and saber shins may be seen.
3182
■ The treatment of choice is penicillin.
INTRODUCTION
INTRODUCTION
DEFINITIONS
The name bejel has been coined from Arabic and is the term used for nonvenereal (endemic) treponematoses. Other names have been used to designate the disease, including njovera in Zimbabwe, belesch or bishel in Saudi Arabia, and dichuchwa in Botswana. The causative agent is the spirochete T. pallidum ssp. endemicum. Bejel is a disease of countries of dry and arid climate and is often found in isolated communities with poor hygiene. The disease mainly involves children from 2 to 15 years of age, but it can also be seen in adults belonging to nomadic people. This treponematosis is likely transmitted not only by nonvenereal direct mucosal or skin contact but also by sharing utensils and drinking vessels. Bejel is therefore often considered as a “familial” disease.
HISTORICAL PERSPECTIVE
Endemic syphilis or bejel has been described in many European countries since the 16th century. The first description appeared in 1575 in Brno, Czech Republic, where it was called morbus Brunogallicus. It was associated with the use of communal bath and bloodletting. A similar disease was described in southwest Scotland and received the name of sibbens or sivvens. In Croatia in the 1800s, an entity named morbus Skrljevo sharing similar clinical features with nonvenereal syphilis was commonly seen and clearly associated with poverty and poor hygiene. The republic of Bosnia and Herzegovina were a site of endemic syphilis for centuries. By the 20th century, additional cases were seen in Russia and Bulgaria. Europe was able to eliminate the disease basically by improving sanitary conditions, and the few persistent endemic areas disappeared with the massive use of penicillin in the 1950s.22
EPIDEMIOLOGY
EPIDEMIOLOGY
As with the other endemic treponematosis, bejel was once described as endemic in many areas of the world, such as Northern Europe, the Balkans, Russia, Mongolia, the near East, the eastern Mediterranean, and southern and northern Africa, affecting mainly those living in poverty. Improvements in the social and economic status in many of these populations have led to a marked reduction in the prevalence of the infection, even preceding the massive campaigns efforts of the 1950s by the WHO. However, there are still areas of the world where the disease is yet prevalent, mostly in the Near East (rural areas of Saudi Arabia) and the African Sahel, the geographic area between the southern border of the Sahara desert and the Sudanese sabana. In the 1980s, bejel was reported in Burkina
Faso and Mali. In the 1990s, cases were reported in Niger and Mauritania. It is an interesting observation that bejel predominates in countries with dry climate, but in the nearby countries with more humid climates, yaws is the predominant disease.1
Few additional cases have been reported in Turkey, Mozambique, and, most recently, Iran but only as isolated cases.23
CLINICAL FEATURES
CLINICAL FEATURES
CUTANEOUS FINDINGS
The main population affected are children younger than 15 years of age. Overcrowding, poor sanitary conditions, and poor personal hygiene seem to facilitate the infection. Distinctly in bejel, the primary lesion is infrequently observed. When the lesion has been noted, it is described as a painless and superficial mucosal ulceration in the mouth or the nasopharynx. An anecdotal report of a primary lesion in the nipple of a nursing woman has been reported that tended to simulate the genital primary chancre of syphilis. The secondary lesions are quite similar also to what is seen in syphilis in the oral mucosae, tonsils, tongue, lips, and nasopharynx. They are oval, almost painless patches, with a whitish, slightly elevated cap. Lesions of angular stomatitis can be part of bejel, similar to what is seen in yaws. Patients also may have generalized, nonitchy skin eruptions, generalized lymphadenopathy, and laryngitis. Condylomata lata-like lesions (Fig. 171-11) may also be present in mucosal and intertriginous areas. On hairless skin, circinate papules may appear (Fig. 171-12). The secondary lesions take 6 to 9 months to heal, and then the disease enters the latency period. The tertiary stage may develop earlier than in yaws, as early as 6 months or taking several years to show. The lesions are gummas that can progress to very destructive ulcerations. They may heal spontaneously, but leave significant scars, surrounded by
26
hyperpigmentation. Involvement of central face and nasal cartilage and bone may result in the picture of gangosa, as described in yaws.
NONCUTANEOUS FINDINGS
Patients with bejel may develop the same osteitis and periostitis of long bones and hands seen in patients with yaws. Such patients will complain of nocturnal pain. The bone changes may evolve into saber tibias, although it is said that such involvement is less severe than in yaws. Neurologic and cardiovascular involvement, as well as congenital transmission are all said to be rare in bejel, but there is a report that mentioned uveitis, optic atrophy, and choroidal atrophic scar. An attenuated form of bejel, manifested mainly as leg pain and radiographic evidence of periostitis. has been described in Saudi Arabia.1
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
The disease is caused by T. pallidum ssp. endemicum. The microorganism is morphologically identical to all spirochetes of the genus Treponema. There is a 99.7 genome sequence identity with the genome of T. pallidum ssp pallidum24; its genome size is 1137.7 kbp. As the other endemic treponematosis, acquiring the disease during childhood and a direct transmission through the skin seem to be the classical scenario. However, bejel is the disease in which more emphasis should be put on the risk of transmission by fomites transported in utensils and drinking vessels.
DIAGNOSIS
DIAGNOSIS
Most cases of bejel are diagnosed on the basis of clinical findings. Among all the nonvenereal treponematosis,
3183
26
bejel is the one with which the differential diagnosis with venereal syphilis might be tricky.
LABORATORY TESTING
Results of the nontreponemal agglutination tests, such as the RPR and VDRL, as well as the most specific treponemal tests, TPHA, TPPA and FTA-ABS, are positive, as in yaws. Clear distinction with venereal syphilis is most difficult and should be based on a careful history and evaluation of the mother and siblings, as illustrated by a recent case seen in Canada.25 In a small number of cases, the final diagnosis may require molecular studies that, unfortunately, are only available in research centers.
PATHOLOGY
The cutaneous lesions show a superficial dermal lymphoplasmacytic infiltrate. In early lesions, epidermal changes such hyperplasia and spongiosis are expected. Treponemas can be then visualized with the aid of immunohistochemistry. Additional findings that may be seen include a lichenoid pattern of the infiltrate and endothelial swelling in superficial capillary plexus, as in venereal syphilis. Tuberculoid granulomas are described occasionally.20
IMAGING
Periostitis as well as bone involvement can be seen on radiographs, very much as they are seen in yaws.
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
See Table 171-4.
Primary and Secondary Cutaneous Lesions
■Syphilis
■Condyloma acuminatum
■Molluscum contagiosum
■Seborrheic dermatitis
■Psoriasis dermatophytosis
Tertiary Gummatous Lesions
■Syphilis
■Gummas of tuberculosis
■Deep fungal infections
■Rhinosporidiosis
■Rhinoscleroma
Mucosal and Perioral Lesions
Mucosal and Perioral Lesions
■Syphilis
■Syphilis
■Angular cheilitis
■Angular cheilitis
■Herpes simplex
■Herpes simplex
3184
■Aphthous disease
■Aphthous disease
MANAGEMENT
MANAGEMENT
MEDICATIONS
Penicillin remains the treatment of choice for bejel. As in yaws, the WHO recommends 1.2 million units of benzathine penicillin for treatment of all stages in adults; half the dose is used in children younger than 10 years. Strategies for eradication are the same as proposed by the WHO in the case of yaws. Accessibility to health care for deprived populations is an important part of any future effort to control and elimination of bejel.
ACKNOWLEDGMENTS
Figures 171-6A to C and 171-8 to 171-12 were obtained by one of the authors (KE) while working at the NGOs Centre René Labusquière and the Réseau Dermatrop, from patients from Mali, Senegal, and Ghana.

Figure 171-1 Pinta. Early phase in a Tikuna Indian presenting with an erythematous scaly plaque on the abdomen.

Figure 171-2 Pinta. Early phase in a Tikuna Indian presenting with multiple erythematosquamous papules.

Figure 171-3 Lichenification and dyschromic changes in early pinta.

Figure 171-4 Dissemination period in a Tikuna child and his mother. The child (the pictures shows his back, held by the mother) presents with hypochromic scaly patches, and the mother shows achromic lesions on the elbows (late pinta).

Figure 171-5 Vitiligoid and hyperchromic changes in late pinta.
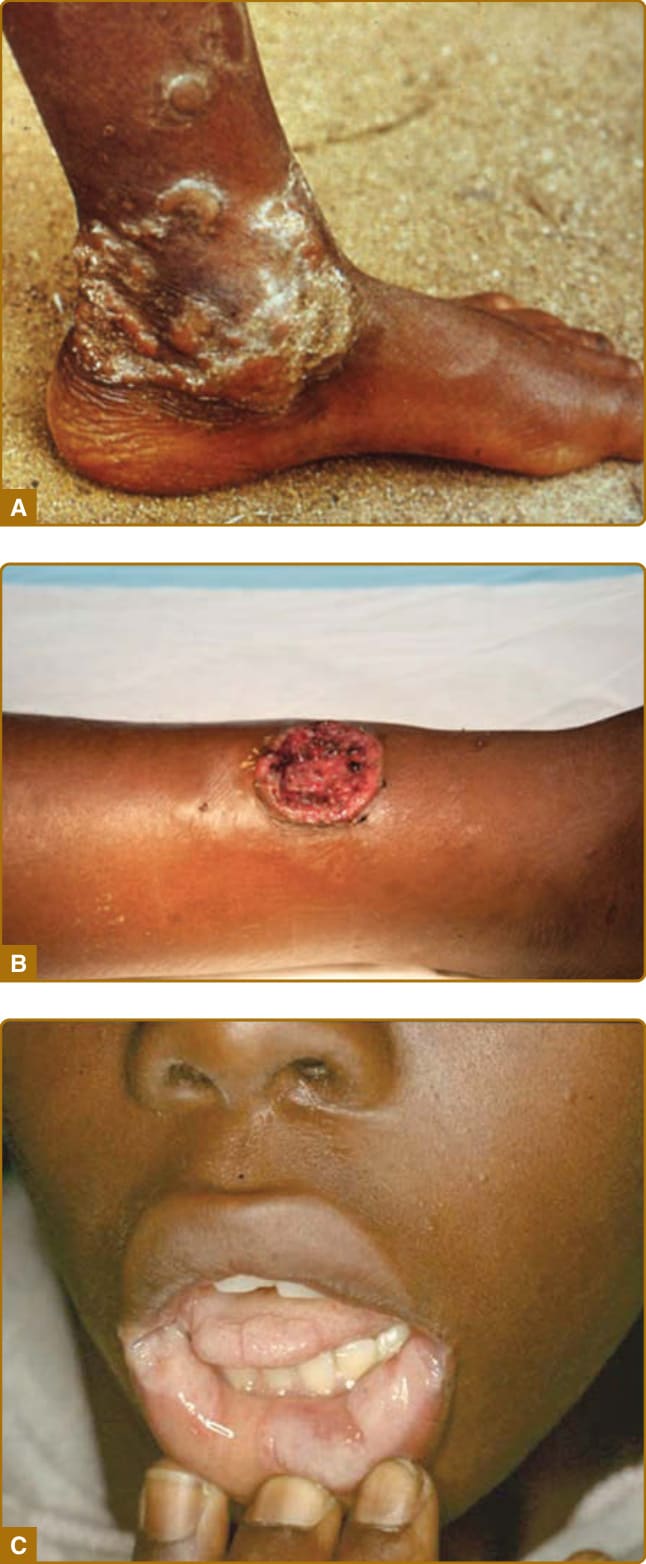
Figure 171-6 A, Primary lesion in yaws, also known as maman pian. B, The secondary, exudative lesion, known as pianome. C, Mucosal and perioral lesion of yaws, quite similar to the mucosal condylomas of syphilis.

Figure 171-7 Crab yaws: plantar keratoderma with fissuring.
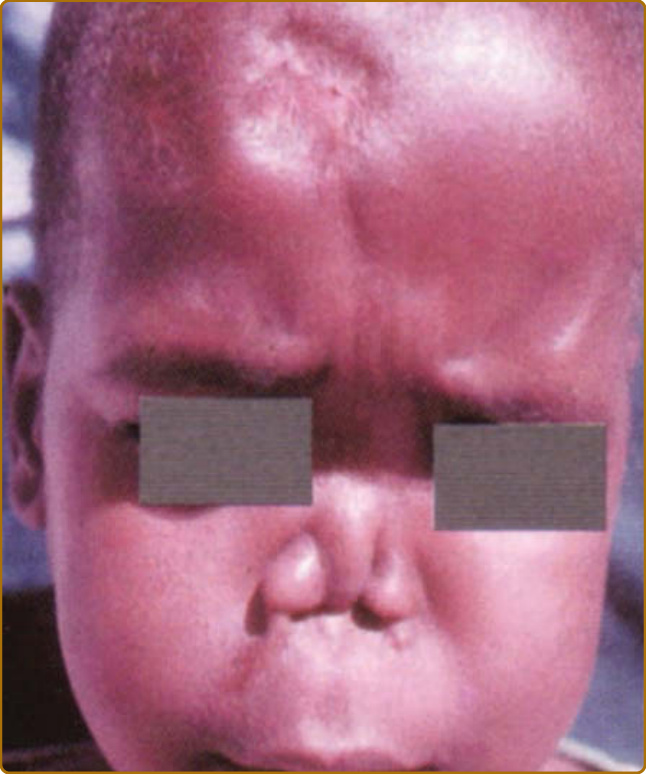
Figure 171-8 Gangosa seen in yaws. See the significant destruction of nasal cartilage.

Figure 171-9 Pintoid dyschromia and hyperkeratosis seen in late yaws.

Figure 171-10 Radiographic evidence of periosteitis of yaws.

Figure 171-11 Cheilitis and angular stomatitis, representing secondary lesions of bejel.

Figure 171-12 Dry and exudative lesions of bejel.
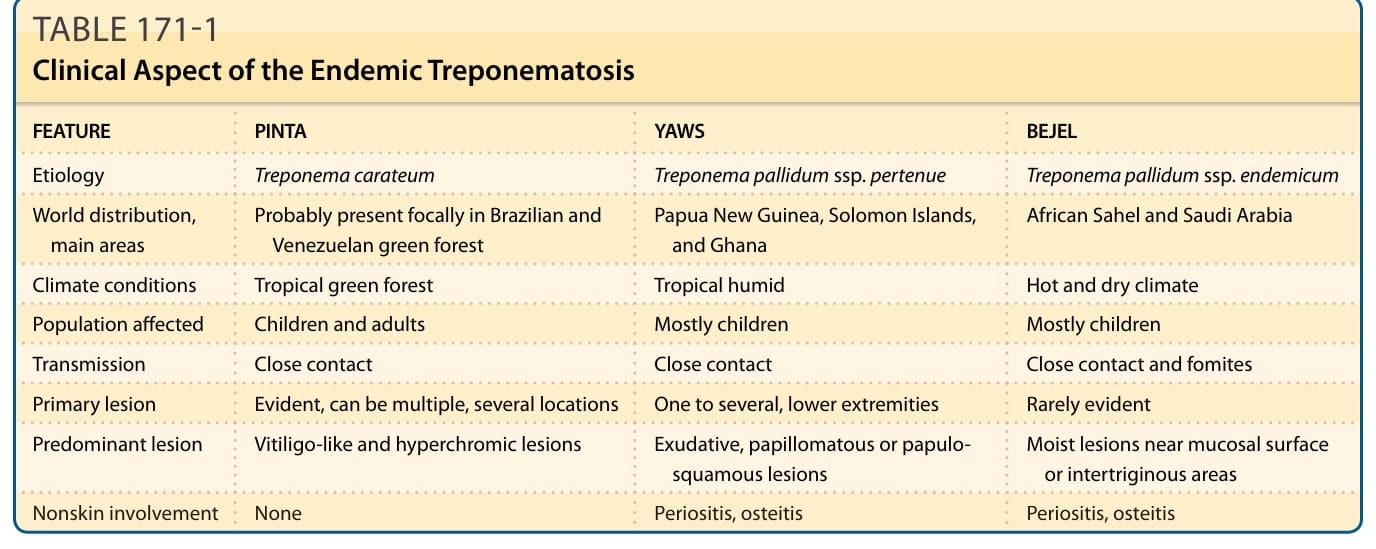
TABLE 171-1 Clinical Aspect of the Endemic Treponematosis
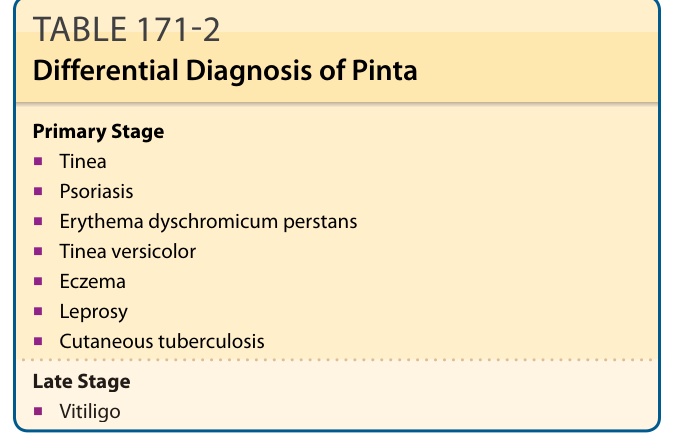
TABLE 171-2 Differential Diagnosis of Pinta
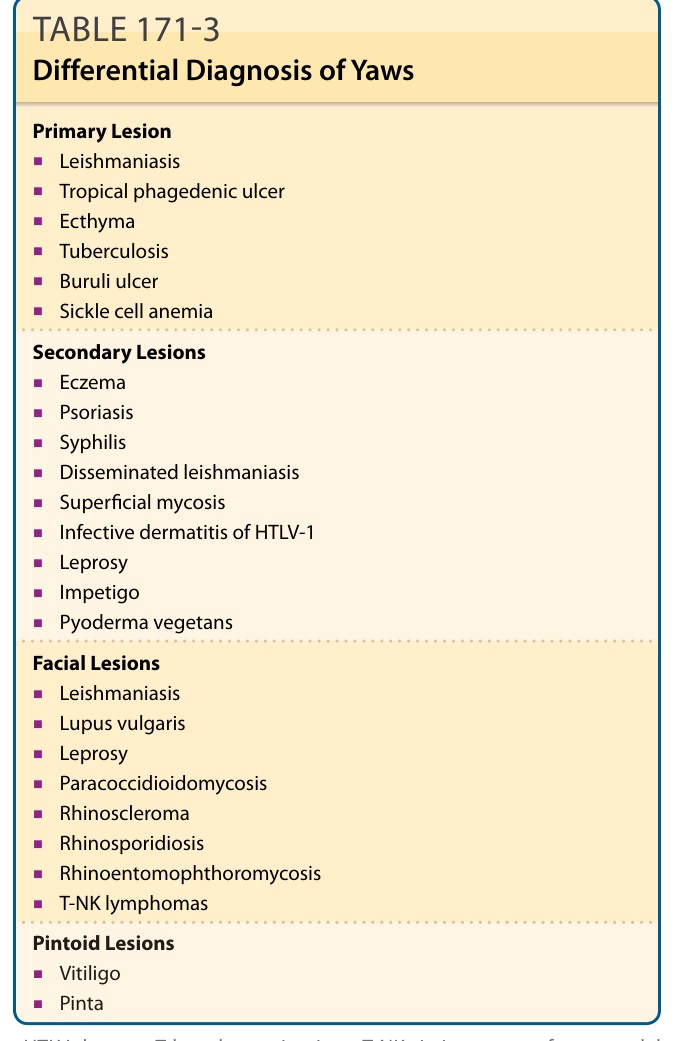
TABLE 171-3 Differential Diagnosis of Yaws
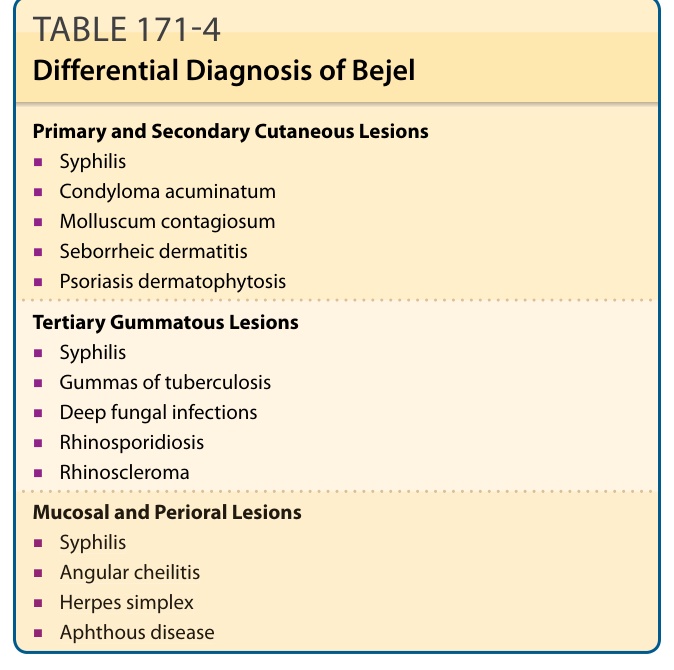
TABLE 171-4 Differential Diagnosis of Bejel