Syphilis
PART26
Sexually Transmitted Diseases
AT-A-GLANCE
■ A disease caused by the spirochete Treponema pallidum subspecies pallidum that is almost exclusively sexually transmitted.
■ In the United States, syphilis disproportionately affects men who have sex with men and African American heterosexual communities.
■ The most common and recognizable manifestations are usually cutaneous.
■ Syphilis passes through 4 distinct clinical phases:
■ Primary stage, characterized by a chancre.
■ Secondary stage, characterized typically by skin eruption(s) with or without lymphadenopathy and organ disease.
■ A latent period of varied duration, characterized by the absence of signs or symptoms of disease, with only reactive serologic tests as evidence of infection.
■ Tertiary stage, with cutaneous, neurologic, or cardiovascular manifestations.
■ Neurosyphilis and ophthalmic syphilis can occur at any stage.
■ The recommended treatment for most types of syphilis is benzathine penicillin G, with dose and administration schedule determined by disease stage.
■ Any patient diagnosed with syphilis should be tested for other sexually transmitted infections, including HIV.
DEFINITIONS
Syphilis is a sexually transmitted infection caused by Treponema pallidum subspecies pallidum. Many of its manifestations are cutaneous, making it of
interest and importance to dermatologists, especially as morbidity from syphilis rises in the developed world and continues in the developing world.
HISTORICAL PERSPECTIVE
Whether syphilis arose in the New World, the Old World, or both remains a controversial subject.1-3
Pandemics of syphilis began in the Old World in Naples, Italy, 1 year after Columbus returned from the New World.2,4,5 Syphilis earned the monicker “great pox,”5 to distinguish it from another virulent disease with cutaneous manifestations, smallpox. The disease takes its name from a poem, called Syphilis, Sive Morbus Gallicus (Syphilis, or the French Disease), written in 1530 by Giralomo Fracastoro, a physician and poet of Verona. Part of the poem recounts the story of a shepherd, named Syphilus, who, as punishment for angering Apollo, was afflicted with the disease known as syphilis.4 Other names besides Morbus Gallicus and the Great Pox by which the disease has been known include lues, the Great Mimic, the Great Masquerader, the Great Imitator, and the Neapolitan disease.4 The cause of syphilis, the bacterium T. pallidum, was discovered by Schaudinn and Hoffman in 1905.6 Darkfield microscopy was pioneered in 1906 by Landsteiner, and serologic testing for syphilis was pioneered in 1910 by Wasserman.5
Because of the skin manifestations, syphilis historically has been of major interest to dermatologists, who were leaders in syphilis research and treatment in Europe and the United States, especially in the prepenicillin era.7-12 One of the leading American dermatology journals, currently called Archives of Dermatology, was before 1955 called Archives of Dermatology and Syphilology. An editorial explaining
26
the jettisoning of “Syphilology” from the journal’s title stated:
The diagnosis and treatment of patients with syphilis is no longer an important part of dermatologic practice. The papers on syphilis that are now submitted to the Archives are few and far between. Few dermatologists now have patients with syphilis; in fact, there are decidedly fewer patients with syphilis, and so continuance of the old label, “Syphilology,” on this publication seems no longer warranted.
Elsewhere in the world, however, the link between dermatology and syphilology (and other sexually transmitted diseases) remains stronger.13,14
Treatments for syphilis in the prepenicillin era included burning sores with hot irons, rubbing mercury-containing ointments (calomel) on lesions, administering mercury orally, and treating with arsenicals, including salvarsan (also called “606” or arsphenamine), which was the first systemic treatment and was discovered by Ehrlich and Hata in 1909.5 Arsenical and other heavy metal-based therapies required multiple injections for at least a year, and were highly toxic. Recognition that T. pallidum was heat sensitive led the Viennese psychiatrist Julius Wagner von Jauregg to develop syphilis malariotherapy in 1917,15 an accomplishment for which he received the Nobel Prize in Medicine in 1927.16 That therapy involved inoculating syphilis patients with malaria, allowing them to experience, optimally, between 10 and 12 febrile episodes, and then treating them with quinine.10,16-18 The treatment reportedly led to complete or partial remission of neurosyphilis (general paresis) in a substantial proportion of patients, although it killed an estimated 10% of those receiving the therapy.17
Two studies have provided the most insight into the natural history of syphilis. The first was a retrospective study of approximately 2000 persons with syphilis in Oslo, where mercury treatments standard in other places were not used.18 The second was the infamous Tuskegee syphilis study, in which 399 black men from Alabama who had late syphilis were prospectively followed from 1932 to 1972.19 The men were denied treatment for syphilis, even after the discovery of the effectiveness of penicillin for the disease. There were multiple other serious ethical lapses in the study. The aftermath of the study led to major changes in ethical requirements for conducting clinical research in the United States.20
Of historical interest, persons said to have suffered from syphilis include Ivan the Terrible, Henry VIII, Henri de Toulouse-Lautrec, and Al Capone,5 among many others.21 Osler, aware of the high prevalence and protean manifestations of syphilis, has been quoted as saying, “He who knows syphilis knows medicine.”5 By the early 1930s, it was estimated that approximately 10% of Americans had syphilis, with 500,000 new infections and 60,000 cases of congenital syphilis per year.22 In 1937, Surgeon General Thomas Parran, keenly interested in syphilis, published a book, titled Shadow on the Land,23 that focused on the substantial public health harms of the then-prevalent disease.22 Parran developed and implemented a national program for syphilis
3146
prevention and control, emphasizing screening, treatment, community involvement, and education.22,24
Penicillin was first used to treat syphilis in 1943, and became widely available in the postwar era.5 As a result of effective treatment, syphilis incidence then declined sharply in the 1950s, followed by a modest rebound through the mid-1980s. In the late 1980s and early 1990s syphilis reemerged in the United States in the South and in large cities, disproportionately affecting black Americans, and associated with crack cocaine and commercial sex workers.2,25 The waning of the crack epidemic and development of the National Plan to Eliminate Syphilis from the United States, released in 1999 by the Centers for Disease Control and Prevention (CDC), resulted in declining rates in heterosexuals.26 However, since the late 1990s, there has been a dramatic increase in incidence in men who have sex with men in the United States and other developed countries.
EPIDEMIOLOGY
In 2000 and 2001, the rate of reported primary and secondary syphilis in the United States was the lowest it had been since reporting began in 1941, at 2.1 cases per 100,000 population. Unfortunately, syphilis incidence in the United States has been increasing steadily since 2001; the rate of primary and secondary syphilis (which is indicative of incident infection) was 6.3 cases per 100,000 population in 2014, the highest rate reported since 1994.27 The current syphilis epidemic in the United States has been primarily driven by increasing cases among gay, bisexual, and other men who have sex with men (MSM). Of 19,999 reported cases of primary and secondary syphilis in 2014, 12,226 (61.1%) were among MSM and 3,407 (17.0%) were among men without information about the gender of the sex partner. Among male cases with information on gender of sex partner, 82.9% occurred in MSM.27 Incidence of syphilis and other sexually transmitted infections among MSM had declined during the AIDS epidemic, and the subsequent increased incidence among MSM has been attributed to a number of factors, including a decrease in safe sex practices resulting from successful HIV treatments, use of the internet to meet sex partners, serosorting (ie, attempting to choose sex partners who share the same HIV status), and an increase in use of recreational drugs, including methamphetamine and erectile dysfunction medicines.2,28,29 Studies that led to the approval, in 2012, for the use of oral antiretroviral medications for pre-exposure prophylaxis to prevent HIV acquisition in high-risk individuals generally did not report increased sexual risk behavior or acquisition of sexually transmitted infections.30
However, how widespread rollout of preexposure prophylaxis may affect syphilis rates, particularly in MSM, remains to be seen.31 The epidemics of HIV and syphilis in the United States MSM population have been intimately linked. Not only are a high proportion of patients coinfected (in 2014, 51.2% of cases
of reported primary and secondary syphilis among MSM were also HIV-positive),27 but incident syphilis infection also is associated with a significantly increased risk of HIV acquisition.32-34 All patients diagnosed with syphilis should be tested for the other sexually transmitted infections, including HIV. Conversely, all patients diagnosed with HIV should also be tested for the other sexually transmitted infections, including syphilis.35
Although rising syphilis incidence in the United States is primarily attributable to cases in MSM, the general male and female populations are affected as well. During 2013-2014, the primary and secondary syphilis rate increased 14.4% in men and 22.7% in women.27 The increase in women has been particularly concerning because of a concomitant rise in reported cases of congenital syphilis. In 2015, the CDC released a report warning of a 38% increase in reported cases of congenital syphilis between 2012 and 2014. Although rates in all ethnic groups increased, the rate of congenital syphilis in blacks remained approximately 10 times the rate among whites in 2014.36
Rates of primary and secondary syphilis nationwide are highest in persons 20 to 29 years old. There is a major health disparity; blacks are disproportionately affected by primary and secondary syphilis, with rates in 2014 more than 5 times higher than rates among non–Hispanic whites overall.27
Recently, there has been an increase in reported cases of ocular syphilis. Between December 2014 and March 2015, 12 cases of ocular syphilis were reported from San Francisco, California, and Seattle, Washington. Several of these patients suffered severe sequelae, including permanent vision loss. Subsequent case finding indicated more than 200 cases reported over the past 2 years from 20 states. As a result, in October 2015, the CDC released a clinical advisory calling for vigilance and careful screening for visual complaints in any patient at risk for syphilis.37,38
Internationally, morbidity from syphilis remains substantial. Each year an estimated 12 million new cases of syphilis occur, and 1 million pregnancies are complicated by syphilis.2
CLINICAL FEATURES
When considering syphilis in the differential diagnosis in a patient, clinicians should take into account the epidemiology and routes of transmission of the disease. This requires taking a complete sexual history. Patients should be asked about partners (including gender and number of recent sexual partners), sexual practices (including anatomic exposure site and use of condoms), and past history of sexually transmitted infections. Effective interviewing skills characterized by respect and a nonjudgmental attitude are critical to obtaining an accurate assessment of behavioral risk.35
Untreated syphilis is characterized by multiple distinct stages of disease, each of which is associated with
26
Contact (one-third become infected)
↓ (10-90 days)
Primary (chancre)
↓ (3-12 weeks)
Neurosyphilis can occur (including ocular syphilis)
Secondary (mucocutaneous lesions, organ involvement)
↓ (4-12 weeks)
Early latent → Relapsing (1/4) (1 year from contact)
↓
Late latent (more than 1 year)
Continue late latent
Tertiary (one-third)
Continue late latent (two-thirds) Tertiary (one-third)
■Late benign (16%)
■Late benign (16%)
(two-thirds)
■Cardiovascular (10%)
■Cardiovascular (10%)
■Neurosyphilis (5% to 10%)
■Neurosyphilis (5% to
10%)
different clinical (including cutaneous) manifestations. Table 170-1 outlines the natural history of syphilis.
EXPOSURE AND INCUBATING SYPHILIS
EXPOSURE AND
INCUBATING SYPHILIS
Syphilis in adults is almost exclusively sexually acquired, when a person comes in contact with infectious lesions of syphilis on another person. Of note, these lesions are only present during primary or secondary syphilis, so the infection is considered sexually transmissible solely in these stages. Importantly, patients with early latent syphilis (within the first year of infection) can relapse into secondary syphilis and become infectious again.16 Infectious lesions of syphilis in adults, which include chancres, condyloma lata, and mucous patches, can be present anywhere on the body but are typically located in or around the genital, anal, or oral area. Direct contact with infectious lesions during oral, vaginal, or anal sex, or during other sexual activities, can result in inoculation and infection. Lesions on keratinized skin (eg, secondary syphilis palmoplantar lesions and maculopapular rash on the trunk) typically do not contain sufficient treponemes to be infectious, and prophylaxis for persons exposed to noninfectious lesions such as those is neither necessary nor indicated. Infectious lesions of congenital syphilis include discharge from rhinitis (“snuffles”) and bullous lesions on the skin. Nonsexually acquired syphilis rarely occurs39 and when it does, it is usually via blood transfusion (of unscreened blood),40 accidental inoculation in an occupational setting (eg, laboratory or health care worker)41
or nonoccupational setting (eg, tattooing),42 or through exposure in utero.43 Transmission to the fetus may occur at any stage of maternal infection, although it is far more likely in the early stages of disease.16,44
3147
26
Estimates of the risk of acquisition (“transmission efficiency”) of syphilis following sexual exposure to a person with infectious syphilis are varied and have been derived in 2 types of sources.45 The first source are data from 3 prospective placebo-controlled trials of prophylactic treatment, in which 9%,46 28%,47 or 63%48
of sexual contacts to syphilis acquired syphilis. The second source is from studies of persons identified as sex contacts in contact-tracing interviews of persons diagnosed with syphilis, in which 18% to 88% of contacts acquired syphilis.45 Nevertheless, the relatively high estimates of syphilis acquisition following exposure underscores the importance of prompt treatment and testing of sexual contacts, as discussed ‘Disease Reporting and Management of Persons Exposed to Syphilis’ section. Persons recently exposed to and infected with syphilis who have yet to manifest signs or symptoms of the disease are said to have incubating syphilis.
PRIMARY SYPHILIS
PRIMARY SYPHILIS
Primary syphilis is the first stage of syphilis, and is characterized by the appearance of 1 or more chancres. Treponemes in the cerebrospinal fluid (CSF) can be demonstrated in up to 30% of primary and secondary syphilis cases.49 There may be overlap of secondary syphilis or even neurosyphilis manifestations with primary syphilis.
CUTANEOUS FINDINGS
At the inoculation site, a chancre develops after an incubation period that ranges from 10 to 90 days (average: 3 weeks). The chancre starts as a dusky red macule that evolves into a papule and then a roundto-oval ulcer (Figs. 170-1 to 170-4). The typical chancre, also called a Hunterian chancre or ulcus durum (hard ulcer), ranges in diameter from a few millimeters to 2 cm and is sharply demarcated with regular, raised borders that are indurated, giving the lesion a cartilaginous feel. The base is usually clean, and the chancre is classically painless. Pain can be reported,50 and
3148
multiple chancres have been reported in 32% to 47% of cases.51 The absence of any of the typical features of a chancre does not rule out syphilis, however. Variations in clinical presentation can result from the number of spirochetes inoculated, the patient’s immune status, concurrent antibiotic therapy, and impetiginization.52-54
Because they are typically painless, patients might not be aware of chancres, especially if painless and located in areas that are not visible, such as the ventral uncircumcised penis, anus, vagina, cervix, or oral cavity.55,56
Common genital locations for a chancre in men include the glans, the coronal sulcus, and the foreskin.57,58 Retraction of the foreskin when a chancre is present on the underside causes the foreskin to flip suddenly, a sign known as the dory flop, after the movement of a dory, a small wooden fishing boat, which flips suddenly when overturned.57 The dory flop sign can help distinguish chancres from other nonindurated causes of genital ulcer disease, such as herpes simplex virus infection and chancroid, that present without the induration that leads to the sudden flip of the foreskin. Uncommon presentations include giant necrotic chancre, phagedenic chancre (a deep, bright-red, necrotic ulcer with a soft base and exudate, resulting from secondary bacterial infection associated with immunosuppression), phimosis resulting from
adherence of a chancre on the foreskin to the glans, endourethral ulcers leading to swelling or serosanguinous discharge, and balanitis.56,58
Common genital locations in women include the cervix, labia majora, labia minora, fourchette, urethra and perineum (see Fig. 170-4).58,59 Chancres in women, especially labial ones, can be more edematous than indurated.58 Edema indurativum is a unilateral labial swelling with rubbery consistency and intact surface, indicative of a deep-seated chancre. Extragenital chancres occur where there may be exposure, and are most frequent in the oropharyngeal cavity.60,61 Syphilis can be transmitted via either receptive or active oral sexual exposure, and is seen in both heterosexual and MSM.62,63 Oral lesions are often larger and may lack the indurated borders that are more typical in keratinized tissues (Fig. 170-5). Anal sex can lead to development of chancres in the perianal (Fig. 170-6) or anal areas that can be difficult to detect on routine physical examination.50,64 Digital or other65,66 contact with the oral, genital, or anal areas, or receiving a bite (eg, on the nipple during sex)67 can also lead to infection and chancre on the exposed area. The chancre heals in 3 to 6 weeks without treatment and 1 to 2 weeks with treatment. Scarring typically does not occur, although thin atrophic scars may occur.55
Coinfection with herpes simplex virus or Haemophilus ducreyi, the causative organism of chancroid, can be present in rare cases.68-70 Relapses of primary syphilis,
26
called monorecidive syphilis or chancre redux, arise in the setting of untreated or inadequately treated syphilis and are rare.71
NONCUTANEOUS FINDINGS
In 60% to 70% of cases of primary syphilis, painless regional lymphadenopathy arises 7 to 10 days after the chancre appears, especially when the chancre’s location is genital. Unilateral lymphadenopathy is more common earlier in the course of disease, with bilateral involvement later in the course.71
SECONDARY SYPHILIS
SECONDARY SYPHILIS
Secondary syphilis is essentially an infectious vasculitis, characterized by localized or diffuse mucocutaneous lesions, often with generalized lymphadenopathy, in the presence of laboratory evidence from tissues or sera consistent with syphilis.72 Cutaneous and mucosal locations are most common.73
Infectious
■Aphthous ulcer
■Chancroid
■Erosive candidal vulvitis or balanitis
■Granuloma inguinale
■Herpes simplex
■Lymphogranuloma venereum
■Vaccinia
Noninfectious
Noninfectious
■Basal cell carcinoma
■Basal cell carcinoma
■Behçet disease
■Behçet disease
■Fixed-drug eruption
■Fixed-drug eruption
■Squamous cell carcinoma
■Squamous cell carcinoma
3149
■Traumatic erosion or ulcer
■Traumatic erosion or ulcer
26
CUTANEOUS FINDINGS
Lesions of secondary syphilis, classically called syphilids or, when affecting the skin, syphiloderms,58 typically erupt 3 to 12 weeks after the chancre appears (up to 6 months after exposure). In some cases lesions of the secondary syphilis develop while the chancre is still present,51,53 with overlap more common among HIVinfected persons.53 Rash is present in nearly all cases of secondary syphilis, although the specific type of rash varies.51,52,74 Erythematous macules (roseola syphilitica) or maculopapules are commonly present symmetrically on the trunk and extremities in 40% to 70% of cases (Fig. 170-7), with papular, papulosquamous, or lichenoid presentations less common.51,74 A white scaly ring on the surface of papulosquamous lesions, called the Biett collarette (Fig. 170-8), is characteristic of, but
3150
not pathognomonic for, syphilis. The face is typically spared in these generalized syphilids, although seborrheic dermatitis–like lesions around the hairline, termed the Crown of Venus or corona veneris, can form a crown-like pattern.55 Lesions are not usually pruritic,58
although pruritus was reported in up to 40% of patients in one study.58 The presentation of the rash overall can be subtle or florid, or can develop from subtle macules to more florid papules over time.75 Erythematous to copper-colored round papules or macules, well demarcated and sometimes with an annular scale, are present on the palms and soles in nearly 75% of cases (Figs. 170-9 to 170-12) and classically cross the palmar creases.51 Plantar lesions can be variously mistaken for calluses (clavi syphilitici). Plantar lesions can also extend to the lateral and posterior aspects of the foot (Fig. 170-13). Other dermatologic manifestations include a patchy nonscarring alopecia, described as moth-eaten (see Fig. 170-11) or, less commonly, a diffuse alopecia of the scalp. Loss of lateral third of the eyebrows can occur. Annular papules and plaques can be present around the mouth and nose, in a presentation colloquially referred to as “nickels and dimes”
26
(Fig. 170-14).58 Papules and plaques, sometimes annular and occasionally papulosquamous, also can be present on the penis and scrotum (Fig. 170-15). Mucous patches are white-to-yellow erosions on the tongue that efface lingual papillae (Fig. 170-16).58
Confluence of mucous patches on the tongue has been termed plaques fauchée en prairie. Mucous patches can be present elsewhere in the oral cavity (Fig. 170-17), on other mucous membranes (such as on the genitalia), or at the corners of the mouth, where they appear as “split papules,” with an erosion traversing the center (Fig. 170-18). Mucous patches are teeming with
3151
26
spirochetes and, hence, highly infectious. Also highly infectious are condyloma lata, which present as moist, flat, well-demarcated papules or plaques with macerated or eroded surfaces in intertriginous areas, commonly in the labial folds in females or in the perianal region in all patients (Figs. 170-19 to 170-21).58
However, any moist intertriginous area of the body can harbor condyloma lata, including the axillae, web spaces between toes, and the folds under breasts, umbilicus (Fig. 170-22) or an abdominal panniculus. Mucous patches and condyloma lata have been reported in 8% and 17% of patients with secondary
3152
syphilis, respectively.51 Malignant lues is a rare manifestation that presents as crusted or scaly papules and plaques that can ulcerate or become necrotic, with an oyster shell-like surface (Fig. 170-23). These lesions, described as rupioid, are often seen in association with high nontreponemal titers and systemic symptoms.76 Nail changes including fissuring, onycholysis, Beau lines, and onychomadesis have been reported.55
Less-common presentations of secondary syphilis include hyperkeratotic, lichenoid, nodular, follicular, pustular, frambesiform, and corymbose eruptions and palmoplantar keratodermas (Figs. 170-24 to 170-26).56,77-80 With the exception of mucous patches and condyloma lata, cutaneous manifestations of secondary syphilis do not contain a substantial number of treponemes and, therefore, are not typically infectious. The maculopapular rash of secondary syphilis can resemble almost any generalized or localized maculopapular eruption (Table 170-3); mucous membrane lesions resemble mucosal manifestations of other dermatoses, and syphilitic hair loss has to be separated from other etiologies of alopecias.
26
Without treatment, the secondary stage typically recedes 4 to 12 weeks after it appears. Scarring typically does not occur, although pigmentary changes (leukoderma colli syphiliticum or, if on the neck, “necklace of Venus”) can result55 from inhibition of melanogenesis. Dermal atrophy, possibly related to elastin degradation, may occur. Absence of syphilids in cinnabar-containing red tattoos has been reported as well, possibly resulting from the antitreponemal effect of mercury in cinnabar.81
NONCUTANEOUS FINDINGS
In addition to neurosyphilis (including ocular syphilis),82 discussed in section “Neurosyphilis” patients with secondary syphilis may experience systemic symptoms that include sore throat, malaise, headache, weight loss, fever, musculoskeletal aches, pruritus, and hoarseness.74 Pharyngitis and tonsillitis,83
laryngitis,84 gastritis,85 hepatitis,85 renal disease (membranous glomerulopathy),86 and periostitis87 have all been reported in secondary syphilis, as have hematologic abnormalities including lymphopenia, anemia, and elevated erythrocyte sedimentation rate.88 Lymphadenopathy is common, and is often bilateral and symmetric in distribution.58
3153
26
LATENT SYPHILIS
LATENT SYPHILIS
The secondary stage is followed by an asymptomatic stage with no clinical findings, with seroreactivity by definition the only evidence of infection. So-called latent syphilis is a diagnosis of exclusion, after primary, secondary, and tertiary syphilis (including neurosyphilis) have been ruled out. Asymptomatic patients who have acquired syphilis within the last year are classified as having “early latent” infection.35
The distinction between early latent and asymptomatic syphilis acquired more than 1 year ago (often termed late latent syphilis), is important for 2 reasons. First, up to 25% of patients with early latent syphilis may relapse into secondary syphilis, leading to possible sexual transmission.16 Second, clinical management of patients with early latent syphilis differs from management of patients with late latent syphilis.16,35 The treatment of early latent syphilis is the same as that
Most Likely
■Drug eruption
■Pityriasis rosea
■Psoriasis
■Viral eruption
■Differential for condyloma lata: Condyloma acuminata
Consider
Consider
■Balanitis
■Balanitis
■Cutaneous T-cell lymphoma
■Cutaneous T-cell lymphoma
■Dermatophytosis
■Dermatophytosis
■Eczema
■Eczema
■Erythema multiforme
■Erythema multiforme
■Granuloma annulare
■Granuloma annulare
■Lichen planus
■Lichen planus
■Lupus erythematosus
■Lupus erythematosus
■Sarcoid
■Sarcoid
■Vasculitis
■Vasculitis
3154
■Vulvitis
■Vulvitis
of primary and secondary (collectively termed early syphilis), whereas late syphilis requires an extended therapeutic course.35
Persons who acquired syphilis during the preceding year can be diagnosed with early latent syphilis. A patient can be classified as having early latent syphilis if, within the year preceding discovery of the reactive serologic test, the patient had 1 of the following:
- Documented seroconversion or a sustained (longer than 2 weeks) fourfold or greater increase in nontreponemal test titers;
- Unequivocal symptoms of primary or secondary syphilis;
- A sex partner documented to have primary, secondary, or early latent syphilis; or
- Reactive nontreponemal and treponemal tests if the patient’s only possible exposure occurred within the previous 12 months.35
To make a diagnosis of early latent syphilis based on the first or third criterion above, clinicians often need, and should seek, the assistance of the local health department. Because syphilis diagnoses and results of reactive serologic tests for syphilis are reportable in every state and territory of the United States, local or state health departments compile (or attempt to compile) records of all syphilis diagnoses and reactive serologic titers for persons residing in the jurisdiction. Clinicians can contact the “reactor desk” of their local or state health jurisdiction, where syphilis diagnostic and titer histories are maintained, to inquire about a patient’s titer history and prior diagnoses and treatments, so that a patient can be staged as having early latent syphilis according to the first criterion above. Public health workers can also search diagnostic and titer histories in their databases for the names of sex partners identified by seroreactive patients, to enable staging patients with early latent syphilis under the third criteria above. Patients in whom the duration of infection cannot be established based on the criteria reference above should be assumed to have late latent syphilis and must be managed accordingly. Latent syphilis may remain indefinitely or progress to the tertiary stage.
TERTIARY SYPHILIS
TERTIARY SYPHILIS
Late manifestations of syphilis are rarely seen. However, historically, on the basis of information from the Oslo and Tuskegee studies, approximately one-third of patients with untreated latent syphilis progress to tertiary syphilis, typically after 15 to 40 years, while the other two-thirds remain in latency.16 Tertiary syphilis manifestations may include gummas (granulomatous, erosive, nodular lesions which most commonly affect the skin and bones), and cardiovascular syphilis.35 Although neurosyphilis can occur at any stage of disease (see “Neurosyphilis” later), late manifestations of neurosyphilis are also considered to be a manifestation of tertiary syphilis.
CUTANEOUS FINDINGS
The signs and symptoms of syphilis that occur after secondary syphilis that do not involve the cardiovascular or nervous systems have historically been referred to as late benign syphilis. Lesions of late benign syphilis are caused by delayed-type hypersensitivity responses to the small number of treponemes present in the involved tissue or organ.54 The hallmark of late benign syphilis is the gumma, a granulomatous nodular lesion with variable central necrosis, which most commonly affect the skin or mucous membranes (80% of gummas).54 Gummas are nontender pink to dusky-red nodules or plaques that vary in size from millimeters to many centimeters in diameter. They favor sites of previous trauma and may arise anywhere on the body, but are more common on the scalp, forehead (Fig. 170-27), buttocks, and presternal, supraclavicular, or pretibial areas. The nodule is initially firm but develops a gummy consistency from accumulation of necrotic tissue. Gummas may grow both horizontally and vertically, and many assume geometric configurations. Small ulcers and abscesses may be present within the lesions. As the central gumma heals, new lesions may develop on the periphery, forming scalloped borders. In contrast to noduloulcerative lesions, gummas are deeper and more destructive (Fig. 170-28). Tissue necrosis eventuates in cylindrical, punched-out ulcers with clean granulomatous bases covered with adherent yellow-white slough (Fig. 170-29). The ulcer may enlarge, remain unchanged, or heal spontaneously, even as the gumma enlarges. Superficial gummas heal with atrophic scars, whereas deeper lesions
26
leave thickened, pitted, ridged scars. Pseudochancre redux refers to a solitary gumma of the penis. Gummas involving the mucous membranes typically affect the palate, nasal mucosa, tongue, tonsils, and pharynx. The lesions ulcerate and can be disfiguring, as when they cause a saddle-nose deformity from destruction of nasal cartilage and bone, or perforation
3155
26
A
B
of the nose or palate (Fig. 170-30).54 Gummas do not heal without appropriate antibiotic therapy, but in the setting of appropriate therapy respond briskly, leaving scars.16 Chronic interstitial glossitis can develop even after penicillin treatment and may undergo malignant degeneration (Fig. 170-31). Other manifestations of late benign syphilis affecting the skin include granulomatous nodular and noduloulcerative lesions and psoriasiform plaques.55
Nodular and noduloulcerative lesions are superficial, firm, painless, dull-red, shiny, flat nodules that range in size from several millimeters to 2 cm. They appear in a grouped configuration, can coalesce into large plaques or ulcerate, and can resemble granuloma annulare.89,90 Psoriasiform plaques are most commonly seen on the arms, back, and face.
3156
NONCUTANEOUS FINDINGS
Besides the skin and mucous membranes, gummas can affect practically any organ, but especially the bones, as well as the liver, heart, brain, stomach, and upper respiratory tract.16 When they involve critical organs such as the brain, gummas can have serious complications.91
Historically, cardiovascular manifestations of tertiary syphilis affected 10% to 40% of those infected and were thought to be responsible for most deaths caused by syphilis.16 Syphilis typically causes syphilitic aortitis, leading to aortic regurgitation in 10% of individuals with untreated disease,92 and can also cause coronary ostial stenosis and saccular aneurysm.93 T. pallidum DNA has been detected in an aortic aneurysm, demonstrating that infection of the aorta leads to direct damage to the tissue.94
Consider
■Deep fungal infections
■Granulomatosis with polyangiitis (Wegener polyangiitis)
■Leishmaniasis
■Lupus vulgaris
■Lymphomas
■Metastatic carcinoma
■Psoriasis
■Sarcoid
■Sarcomas
■Vasculitis
■Vasculitis
NEUROSYPHILIS
NEUROSYPHILIS
Infection of the CNS by T. pallidum can occur during any stage of infection. “Neuroinvasion,” in which T. pallidum disseminates to CSF and meninges, occurs very early in syphilis.95 Neuroinvasion can be transient, with the body clearing the infection, or more sustained, in which case it is called asymptomatic neurosyphilis, defined by CSF abnormalities. Asymptomatic neurosyphilis, if discovered, is usually treated to prevent progression to symptomatic neurosyphilis, although benefits of treatment for asymptomatic neurosyphilis are not well documented. Early symptomatic neurosyphilis typically manifests as meningitis, resulting in meningismus, fever, or cranial nerve abnormalities (especially cranial nerves II, III, IV, VI, VII, and VIII), or meningovasculitis, resulting in meningitis with stroke, usually affecting the portion of the brain supplied by the middle cerebral artery.95 Uveitis is the most common ophthalmic manifestation of early neurosyphilis (see “Ocular Syphilis” below), presenting as eye pain, redness, and photophobia, and sensorineural hearing loss is the most common manifestation of otologic syphilis. Ophthalmic and otologic manifestations of early neurosyphilis are managed in the same way as neurologic manifestations.35,95
Early symptomatic neurosyphilis is not uncommon. A review of syphilis cases among HIV-infected men in 4 large U.S. cities during 2002 to 2004 showed that almost 2%, including persons at each stage of infection, had symptomatic early neurosyphilis. Ocular abnormalities were most common among those affected, followed by other cranial nerve involvement, acute meningitis, other syndromes (headache, altered mental status, or both), and cerebrovascular accidents. Of those with symptomatic early neurosyphilis, nearly one-third had persistent neurologic deficits 6 months after receiving appropriate treatment.96
The 2 syndromes commonly associated with late neurosyphilis are general paresis of the insane, also known as dementia paralytica, and tabes dorsalis.95 General paresis presents as a rapidly progressive dementia, accompanied by personality changes. Tabes dorsalis presents with sensory ataxia and bowel and bladder dysfunction, resulting from damage to the posterior columns of the spinal cord. Tabes dorsalis can be accompanied by an Argyll Robertson pupil (which accommodates, but does not react to, light) and optic atrophy. These syndromes are now very rare in the developed world. Clinicians diagnosing a person with syphilis should perform a neurologic review of systems and perform a neurologic examination. According to CDC recommendations, indications for CSF examination in persons with syphilis include neurologic, ophthalmic, or otologic signs or symptoms; evidence of active tertiary syphilis; or treatment failure. HIV infection in-and-of-itself is not an indication for CSF examination.35
26
OCULAR SYPHILIS
Although the syndromes may not always overlap, ocular syphilis has generally been considered to be a subset of neurosyphilis, and as per CDC recommendations should be clinically managed as such.35 Given the recent increase in reported cases, clinicians should be careful to ask about eye symptoms in evaluating any patient suspected to have syphilis. Ocular syphilis may occur during any stage of infection, and may involve almost any portion of the eye. Chancres or gummas of the conjunctiva, conjunctivitis, and scleroconjunctivitis; syphilitic interstitial keratitis; anterior, posterior, and pan uveitis; multiple retinal complications including retinal detachment, cataracts, and glaucoma, as well as optic nerve involvement (including papillitis, retrobulbar neuritis, optic atrophy, optic nerve gumma, and various stroke syndromes) are among the clinical syndromes that have been described. Furthermore, multiple manifestations of syphilis can be observed in the eye, such as pupillary abnormalities (including the Argyll Robertson pupil), palsies of the third, fourth and sixth nerve, usually from syphilitic basilar meningitis, and focal gummas along the nerves, brainstem infarction, or syphilitic aneurysmal compression or hemorrhage that may involve the optic and oculomotor nerves. Syphilitic basilar meningitis or gummas may cause a chiasmal syndrome with bitemporal hemianopia. Finally, eyelid chancres or condyloma lata of the eyelids have been described, although these do not directly involve the eye.37,97-99
CONGENITAL SYPHILIS
CONGENITAL SYPHILIS
Congenital syphilis results from infection in utero with T. pallidum. Transplacental fetal infection can occur at any time during pregnancy and at any stage of maternal infection.100 Probability of transmission of infection depends on the stage of infection in an untreated mother, ranging from 70% to 100% in primary syphilis, 40% for early latent syphilis, and 10% for late latent syphilis.101 Because infection is spread hematogenously, a chancre is not present on the fetus or infant.100 In 30% to 40% of cases, congenital syphilis results in stillbirth.43 Of infants who survive, two-thirds are asymptomatic at delivery and only later develop symptoms.100
Clinical findings in symptomatic infants are similar to congenital infections caused by cytomegalovirus, toxoplasmosis, herpes simplex virus, rubella, and other infections.43 The most prominent manifestations of early congenital syphilis, defined as syphilis in a child younger than 2 years of age, include fever, rash, hepatosplenomegaly, and persistent rhinitis (“snuffles”).100 Hydrops fetalis (edema), lymphadenopathy, neurosyphilis, leukocytosis, thrombocytopenia, periostitis, and osteochondritis also may be present, with the pain associated with osteochondrotic lesions causing the infant to refuse to move the affected anatomic area (“pseudoparalysis of
3157
26
Parrot”).43,100 If present at delivery, the rash is usually bullous (“syphilitic pemphigus”; Fig. 170-32) and very infectious.100 Rash that presents at 2 weeks or more after birth, however, is typically maculopapular, with small copper-red lesions similar to lesions of secondary syphilis most commonly affecting the hands and feet.43 Desquamation and crusting can then occur.102 Other cutaneous lesions present can include condyloma lata (Fig. 170-33), mucous patches, fissures around the lips, nares, or anus, and petechiae from thrombocytopenia.43 The skin of the syphilitic neonate is often dry and wrinkled and, in newborns with fair skin, may have a café-au-lait hue (Fig. 170-34). Late congenital syphilis is defined as disease occurring in a child who is at least 2 years old that typically manifests over the first 2 decades of life.43 Many manifestations of late congenital syphilis result from damage caused during early infection and are not reversible with treatment. Those manifestations include scars (rhagades; Fig. 170-35) resulting from cutaneous fissures; a saddle-nose deformity, resulting from destruction of nasal cartilage; frontal bossing (Olympian brow), thickening of the sternoclavicular portion of the clavicle (Higoumenakia sign), anterior bowing of the midtibia (saber shins), and scaphoid scapula, all resulting from chronic periostitis; and
3158
peg-shaped notched central incisors (Hutchinson teeth; Fig. 170-36) and mulberry molars, resulting from syphilis vasculitis in developing tooth buds. Other manifestations include eighth nerve deafness and eye abnormalities, including interstitial keratitis, glaucoma, or corneal scarring. The Hutchinson triad refers to Hutchinson teeth, interstitial keratitis, and eighth nerve deafness.43
Of note, as with any sexually transmitted disease, the diagnosis of syphilis in a child beyond the neonatal period should raise the question of child abuse.35
SYPHILIS AND HIV INFECTION
SYPHILIS AND HIV
INFECTION
Chap. 168 discusses cutaneous manifestations of the HIV. The interaction of syphilis and HIV infection is complex.29 The clinical presentation of syphilis varies in minor ways between HIV-infected and HIV-uninfected persons.29 HIV-infected persons are more likely to present with more than 1 chancre and with larger and deeper chancres in primary syphilis,53,103 and are more likely to manifest signs of secondary syphilis while at least 1 chancre is present.53,104 Atypical and aggressive presentations of syphilis in HIV-infected persons might also be more common, although those presentations are not thought to be unique to HIV coinfection.29,103
Some studies have shown syphilis to transiently increase HIV viral load and decrease CD4+ T-cell count during infection, with resolution following treatment.105-111 Those changes might facilitate HIV transmission by HIV-infected patients coinfected with syphilis.29,109 An effect of syphilis on progression to AIDS or mortality has not been found.112 Syphilis also is associated with HIV acquisition,113 and all persons presenting with syphilis who are not known to be infected with HIV should be tested for HIV.35 The disruption of epidermal or mucosal barriers caused by syphilis ulcers, and the migration to these lesions of inflammatory cells that are targets for HIV are 2 biologic mechanisms that might account for the synergy between the 2 infections. Common behavioral factors (eg, lack of condom use) also likely contribute to risk of coinfection. All HIV-infected persons entering HIV care should have a serologic test for syphilis, which should be repeated yearly thereafter in all those who are sexually active, or more frequently (every 3 to 6 months) if indicated (depending on risk behaviors).114 HIV infection also is associated with repeat syphilis infection.115
Because of its effect on the immune system, HIV infection is thought to increase risk of neurosyphilis.29,95 This is based on studies correlating abnormal CSF findings with advanced HIV disease116 and failure to normalize CSF–VDRL (Venereal Disease Research Laboratory)
26
test results in the presence of HIV infection,117 especially with lower CD4 cell counts. Additionally, HIV-infected persons with syphilis can experience “neurorelapse,” meaning the development of neurosyphilis following appropriate treatment for primary, secondary, or early latent syphilis, and declines in nontreponemal titers consistent with cure.95
HIV infection can sometimes complicate serologic diagnosis of syphilis and subsequent followup, as unusual serologic responses have been observed in HIV-infected persons with syphilis.35 False-negative serologic test results in the setting of the prozone phenomenon118 and seronegative syphilis119 have been reported. Also, serofast reactions (ie, persistently reactive nontreponemal test results, even following appropriate treatment) can occur.120 When syphilis is suspected clinically and serology is nonreactive, skin biopsy can be useful diagnostically, as can darkfield microscopy35,121 or polymerase chain reaction (PCR)- based assays for T. pallidum,68 if available. CDC treatment recommendations for syphilis do not depend on HIV infection status, and are supported by limited data indicating that outcomes are not improved with more intense or prolonged treatment.29,35,122 Titers might decline more slowly in appropriately treated HIV-infected persons,29,35,123 particularly in those who have lower titers on initial diagnosis.124 Compared with HIV-uninfected persons, HIV-infected persons with primary or secondary syphilis should have more frequent followup (Table 170-5).35
ETIOLOGY AND PATHOGENESIS
T. pallidum subspecies pallidum is a motile, spiralshaped bacterium for which humans are the only natural host.16 T. pallidum ranges in size from 5 to 16 µm in length and is 0.2 to 0.3 µm in diameter.121 The bacterium is surrounded by a cytoplasmic membrane, which is itself enclosed by a loosely associated outer membrane. Between those membranes lies a thin layer of peptidoglycan, which provides structural stability and houses endoflagella, organelles that are responsible for T. pallidum’s characteristic corkscrew motility. Microscopically the bacterium is indistinguishable from other pathogenic treponemes that cause nonvenereal diseases, including T. pallidum subspecies endemicum (bejel), T. pallidum subspecies pertenue (yaws), and T. pallidum subspecies carateum (pinta). The T. pallidum genome, sequenced in 1998,125 is 1.14 Mb in length, relatively small for a bacterium.16
The bacterium has very limited metabolic capabilities, making it reliant on host pathways for many of its metabolic needs.16,73 T. pallidum does not survive more than a few hours to days outside its host and cannot be cultured easily in vitro for sustained periods, complicating efforts to understand the organism.16,73 Instead, it must be propagated in mammals, with rabbits the preferred species because, following testis inoculation, rabbits, unlike mice, experience disease
3159
26
STAGE OF DISEASE HIV STATUS OF PERSON RECOMMENDED TREATMENT a
Primary or secondary HIV-uninfected Benzathine penicillin G, 2.4 million units, administered IM in a single dose
HIV-infected Benzathine penicillin G, 2.4 million units, administered IM in a single dose
Early latent HIV-uninfected Benzathine penicillin G, 2.4 million units, administered IM in a single dose
HIV-infected Benzathine penicillin G, 2.4 million units, administered IM in a single dose
Late latent (>1 year), or latent of unknown duration
HIV-uninfected Benzathine penicillin G: 3 doses of 2.4 million units IM given at 1 week intervals
HIV-infected Benzathine penicillin G:
HIV-infected Benzathine penicillin G: 3 doses of 2.4 million units IM given at 1 week intervals
3 doses of 2.4 million units IM given at 1 week intervals
aInitial treatment is the same for HIV-uninfected and HIV-infected persons.
ALTERNATIVE TREATMENT FOR PENICILLIN-ALLERGIC PERSONS (NONPREGNANT WOMEN ONLYb)
TIME FRAME TO EXPECT FOURFOLD DECLINE IN TITERd
SCHEDULE FOR FOLLOWUP AFTER TREATMENTc
Doxycycline 100 mg orally twice daily for 14 days 6 and 12 months 6 to 12 months
Doxycycline 100 mg orally twice daily for 14 days 3, 6, 9, 12, and 24 months 6 to 12 months
Doxycycline 100 mg orally twice daily for 14 days 6, 12, and 24 months after treatment 12 to 24 months
Doxycycline 100 mg orally twice daily for 14 days 6, 12, 18, and 24 months 12 to 24 months
Doxycycline 100 mg orally twice daily for 28 days 6, 12, and 24 months after treatment 12 to 24 months
Doxycycline 100 mg orally
6, 12, 18, and
12 to 24 months
Doxycycline 100 mg orally twice daily for 28 days 6, 12, 18, and 24 months 12 to 24 months
twice daily for 28 days
24 months
b Pregnant women must not be treated with doxycycline. If allergic to penicillin, pregnant women must be desensitized and then treated with benzathine penicillin G.
c Some persons (eg, men who have sex with men or women who become pregnant) should be screened appropriately in addition to being followed at the recommended intervals to assess clinical and serologic response to treatment.
d If titers have not declined fourfold after the stated time frame, consider reinfection or treatment failure (including treatment failure because of neurosyphilis). If at any time after treatment signs or symptoms of syphilis appear, also consider those same possibilities.
manifestations.16,73 T. pallidum divides slowly, taking from 30 to 50 hours in vitro. That slow reproduction rate has important implications for treatment, which must be present in the body for a long period to assure effectiveness against the bacterium.16
Following inoculation, T. pallidum attaches to host cells, including epithelial, fibroblast-like, and endothelial cells, likely by binding to fibronectin, laminin, or other components of host serum, cell membranes, and the extracellular matrix.16 It can invade rapidly into the bloodstream—within minutes of inoculation, based on rabbit models—and can cross many barriers in the body, such as the blood–brain barrier and the placental barrier, to infect many tissues and organs. That dissemination leads ultimately to manifestations of syphilis distant from the site of the initial chancre(s) in an infected person and in a developing fetus.16
T. pallidum lacks virulence factors common to many other bacteria, including lipopolysaccharide endotoxin.16 It does, however, produce a brisk immune response, mediated by membrane lipoproteins,126 that begins shortly after infection. Infection at all stages leads to infiltration by lymphocytes, macrophages, and plasma cells.73 CD4+ T cells predominate in chancres,
3160
and CD8+ T cells predominate in lesions of secondary syphilis.73 Infection leads also to elaboration of T-helper (Th)-1 cytokines, including interleukin-2 and interferon-γ, although downregulation of the Th1 response during secondary syphilis, coincident with the peaking of antibody titers,73 might contribute to the organism’s ability to evade the host immune response.54,127 Subtyping studies of T. pallidum have linked certain strains of the organism to neurosyphilis.128
The humoral immune response begins with production of immunoglobulin (Ig) M antibodies approximately 2 weeks after exposure, followed 2 weeks thereafter by IgG antibodies.126 IgM, in addition to IgG, continues to be produced during infection and can lead to immune-complex formation.126 Antibody titers peak during bacterial dissemination in secondary syphilis.73
Some antibodies cross-react with other treponemal species, and some are specific for T. pallidum subspecies pallidum. The immune response is somewhat active against the organism, helping block attachment of the organism to host cells, conferring passive immunity in rabbit models, and enhancing phagocytosis in vitro.73
The immune response is sufficient to prevent syphilis reinfection in persons who have untreated syphilis.
In other words, in what is called the law of Colles or chancre immunity, persons with untreated syphilis will not experience another episode of primary syphilis as long they remain untreated.73 However, the immune response is insufficient to eradicate T. pallidum from the host. In addition to suppressing the Th1 response, the organism is thought to evade those host defenses by taking harbor in immune-privileged tissues (eg, CNS, eye, and placenta), failing to be present in sufficient quantities (eg, during latent infection) to trigger a host response, varying its surface proteins during infection through gene conversion, and overcoming host attempts to prevent bacterial access to iron, which is necessary for bacterial growth.16,73 The immune response is also inadequate to prevent reinfection after a person is cured of syphilis, although it might modify the course of reinfection. Compared with persons with syphilis for the first time, for example, reinfected persons may be more likely to be asymptomatic.129
The immune response is also likely responsible for the tissue damage caused in syphilis.16 Damage to axons located near the site of a chancre might explain why that lesion, although ulcerative, is typically painless.130
Interest in a vaccine for syphilis continues, with focus on using outer membrane protein antigens to elicit an immunoprotective response.131 However, a number of barriers to vaccine development exist. Those include variability in outer membrane protein antigens, the limited number of antigens on T. pallidum to which immunoprotective antibodies could bind, the possibility that the formation of a host protein coat around T. pallidum might prevent antibody binding, and a potential lack of commercial incentive to produce a vaccine.131
DIAGNOSIS
Diagnosis of syphilis depends on clinical suspicion combined with laboratory testing to directly or indirectly detect infection with T. pallidum. Of note, in cases where clinical suspicion for syphilis is high, clinicians should not wait for the results of laboratory testing before administering appropriate treatment. Clinicians should also remember that serologies can be negative in up to 30% of patients with primary syphilis.132
DIRECT DETECTION OF T. PALLIDUM
DIRECT DETECTION OF
T. PALLIDUM
Direct detection of T. pallidum, provides definitive evidence of infection, and is particularly important in primary syphilis, given that serologies may be negative. However, these tests, including darkfield microscopy, which has been a mainstay of diagnosis for decades, are rarely available outside of specialized settings.133
DARKFIELD MICROSCOPY
When available, darkfield microscopic examination is the diagnostic test of choice in chancres, moist lesions
26
of secondary syphilis (condylomata lata and mucous patches), and the discharge from rhinitis in congenital syphilis. Darkfield examination (Fig. 170-37) will often be positive before serologic tests become reactive.134
Importantly, because nonpathogenic treponemes are normally present in the oral cavity and can be mistaken for T. pallidum, darkfield microscopy cannot be used to test oral lesions.135 The number of T. pallidum organisms in secondary syphilis lesions except for mucous patches and condyloma lata is generally not sufficient to allow darkfield diagnosis. Universal precautions must be used when collecting and handling darkfield specimens, as lesions of syphilis suitable for darkfield examination are very infectious. Darkfield specimens are prepared by removing crusts from the surface of the lesion, cleaning the surface of the lesion with a sterile saline-soaked gauze, squeezing the base of the lesion with 2 gloved fingers to induce the presence of a serous exudate on the surface, and collecting the exudate with a glass slide, cover slip, or bacteriologic loop. Only if the amount of exudate is insufficient to prevent the slide from drying out prior to microscopic examination should a drop of nonbacteriostatic normal saline be added before covering the slide with a cover slip. The slide is examined within 5 to 20 minutes by a trained microscopist, using a darkfield microscope, for the presence of organisms with the characteristic morphology and motility of T. pallidum.121 Sensitivity is approximately 74% to 79%, but declines as minutes elapse, as dead treponemes cannot exhibit the motility required for diagnosis.121 Of note, prior application of a topical antibiotic to a lesion can yield a false-negative darkfield specimen.
DIRECT FLUORESCENCE ANTIBODY TEST
The lesional exudate is smeared on a glass slide and stained with fluorescein-labeled anti–T. pallidum immunoglobulin. In contrast to darkfield microscopic examination, the smear can be held for later evaluation and oral or anal lesions can be examined because only T. pallidum is stained. The sensitivity of the test is 73% to 100%.121
3161
26
MOLECULAR TESTS
In research settings, PCR-based methods have been used to detect T. pallidum DNA from lesions.68
HISTOPATHOLOGIC EXAMINATION
HISTOPATHOLOGIC
EXAMINATION
Histopathologic examination is not essential for a diagnosis of syphilis, which can in many cases be made on the basis of clinical findings, serologic testing, and, for appropriate lesions, and if available, darkfield microscopy. In unusual or questionable cases, however, histopathologic examination can be useful.
PRIMARY SYPHILIS
At the edge of a chancre, the epidermis shows changes similar to those of secondary syphilis, discussed later.136 The papillary dermis shows edema and a perivascular and interstitial infiltrates characterized by lymphocytes (predominantly CD4+ T cells), histiocytes, and plasma cells, with neutrophils admixed. T. pallidum organisms can be visualized along the dermal–epidermal junction and in and around blood vessels, using Livaditis or Warthin-Starry stains or by immunofluorescent techniques.136
SECONDARY SYPHILIS
Although clinically different in appearance, lesions of primary and secondary syphilis share many histologic features, with changes more marked in papular lesions and less so in macular lesions.136 In the epidermis those changes include psoriasiform hyperplasia, exocytosis of lymphocytes, spongiform pustulation,
and parakeratosis; in the dermis those changes include marked papillary dermal edema and perivascular and/or periadnexal infiltrate composed of lymphocytes and/or histiocytes, sometimes granulomatous, and most intense in the papillary dermis. Plasma cells are present in three-fourths of cases, and T. pallidum organisms can be seen on appropriately stained sections in one-third of cases, usually in the epidermis and less commonly around superficial dermal blood vessels.136
TERTIARY SYPHILIS
Histopathologically, gummatous lesions are characterized by granulomas with central zones of acellular necrosis. Endarteritis obliterans and angiocentric plasma cell infiltrates of dermal blood vessels also can be present. Nodular lesions show small granulomas in the dermis, accompanied by islands of epithelioid cells, multinucleated giant cells, lymphocytes, and plasma cells.136
SEROLOGY
SEROLOGY
Serologic tests for syphilis include nontreponemal tests, which detect IgG and IgM antibodies to lipoidal material released from damaged host cells and possibly from T. pallidum, and treponemal tests, which detect antibodies to T. pallidum itself. Accurate serologic diagnosis of syphilis requires both types of test. Table 170-6 outlines the sensitivity and specificity of selected serologic tests for syphilis.121,126,137-139
NONTREPONEMAL SEROLOGIC TESTS
The 2 most widely used nontreponemal tests are the VDRL and rapid plasma reagin (RPR) tests. These
SENSITIVITY (%)
SPECIFICITY (%) PRIMARY SYPHILIS SECONDARY SYPHILIS LATENT SYPHILIS TERTIARY SYPHILIS
TEST
Nontreponemal Tests
RPR 86 (77-99) 100 98 (95-100) 73 98 (93-99)
VDRL 78 (74-87) 100 96 (88-100) 71 (37-94) 98 (96-99)
Treponemal Tests
TPPA 88 (86-100) 100 97 (97-100) 94 96 (95-100)
MHA-TP 76 (69-90) 100 97 (97-100) 94 99 (98-100)
FTA-ABS 84 (70-100) 100 100 96 97 (94-100)
TPHA 77 (53-86) 100 99 (99-100) 100 96-99
EIAa 85-97 97-100 100 (early latent) NA 99-100
75-100 (late latent)
y 75-100 (late latent)
aVarious EIAs from different manufacturers were tested. See Ref. 137 for details. EIA, enzyme immunoassay; FTA-ABS, fluorescent treponemal antibody absorption assay; MHA-TP, microhemagglutination assay for Treponema pallidum; RPR, rapid plasma reagin; TPHA, T. pallidum hemagglutination; TPPA, T. pallidum particle agglutination; VDRL, Venereal Disease Research Laboratory.
3162
26
Common patterns of serologic reactivity in syphilis patients
100
% of patients who test positive
80
60
IgM
40
20
FTA-ABS
TPHA
Untreated
VDRL/RPR
Treated
20 10 2 12 10 8 6 4 2
Time of infection
Weeks Time postinfection Years
Primary lesion
Secondary lesion
Clinical stages of syphilis
Primary
Secondary Latent (asymptomatic) Tertiary
tests are used both to diagnose syphilis, and to monitor response to treatment. The VDRL and RPR begin to become reactive 4 to 5 weeks after infection, with 100% sensitivity by approximately 12 weeks, and revert to nonreactive in 25% to 30% of cases during late latent syphilis (Fig. 170-38).140 Cases of seronegative secondary syphilis in HIV-infected persons have been reported.119 Results can be qualitative (reactive/ nonreactive) or quantitative. Quantitative results are reported as titer, which refers to serial dilutions of serum by a factor of 2 (1:2, 1:4, 1:8, and so on). The reported titer represents the most dilute sample that gives a reactive result. RPR and VDRL titers cannot be directly compared, and even for the same test, reported titers may differ slightly between laboratorians and laboratories. Because of the importance of using nontreponemal titers to assess response to treatment, a titer for each person diagnosed with syphilis must be obtained on the day-of-treatment. Without a day-of-treatment titer, it is very difficult to interpret subsequent titers to determine whether the person has responded to treatment appropriately. Treatment success is defined serologically as a fourfold (two-dilution) decline in nontreponemal test titer
(see section “Management”), although in many persons, following appropriate treatment nontreponemal titers will revert to nonreactive. In persons treated for primary syphilis, nontreponemal tests become nonreactive in 60% by 4 months, and in nearly all patients by 12 months.141 In persons treated for secondary syphilis, the tests usually become nonreactive 12 to 24 months after treatment. However, in some cases, more frequently if therapy is administered in the latent stage, nontreponemal tests may remain reactive in low titers for up to 5 years or longer. In some persons nontreponemal antibodies can persist at a low titer for long periods, and sometimes for life.142 Both patients who fail to achieve a fourfold decline in titer, as well as those who have adequate serologic decline but whose nontreponemal test titers do not become undetectable, have been referred to as serofast. However, current CDC guidelines recommend additional followup and testing only for the group of serofast patients who do not achieve a fourfold decline in titer (see section “Management”).35,133
False-negative results occur during very early infection or in latent and late syphilis. In a small percent of secondary syphilis cases, very high antibody titers inhibit test reactivity, producing a false-negative result,
3163
26
called the prozone phenomenon. To exclude the prozone phenomenon, the test must be repeated with diluted serum. Many laboratories do not routinely check for the prozone phenomenon, so clinicians must request a ruling out of the prozone phenomenon in the appropriate setting (eg, a patient with a suspicious rash and a negative nontreponemal test result). Importantly, nontreponemal titers may decline over time even in the absence of treatment, so persons with late latent syphilis who have never been treated may have nonreactive nontreponemal test results (see “The Reverse Sequence Algorithm” below).133
Biologic false-positive results constitute approximately 1% of reactive nontreponemal tests and usually have low titers (<1:8). Table 170-7 outlines the causes of biologic false-positive results. In the traditional algorithm for diagnosis of syphilis, the nontreponemal test is performed first, followed by a treponemal test for confirmation if the nontreponemal test is positive.
TREPONEMAL SEROLOGIC TESTS
Examples of treponemal serologic tests include the T. pallidum particle agglutination (TPPA) test, the microhemagglutination assay for T. pallidum (MHA-TP), the fluorescent treponemal antibody absorption assay (FTA-ABS), the T. pallidum hemagglutination test (TPHA), and various treponemal enzyme immunoassays (EIAs) and immunochemiluminescence assays. These tests, which use whole or fragments of T. pallidum as antigen, detect the presence of antibodies to T. pallidum. Compared with nontreponemal tests, they are more cumbersome to perform—except for treponemal EIAs—but have greater sensitivity in the primary and late stages and slightly higher specificity. They have historically been used, and in many settings are still used, to confirm syphilis, because a reactive treponemal test result essentially rules out the possibility of a biologic false-positive reaction on a nontreponemal test. Consequently, a reactive nontreponemal test result followed by a reactive treponemal test result confirms a diagnosis of syphilis. The test results must be interpreted in light of clinical findings and prior serologic test results to determine whether the case of syphilis is new or old, and if old, previously treated successfully or unsuccessfully. Persons who have had syphilis usually will have reactive treponemal test results for life, even after successful treatment, making a reactive treponemal test in a person with a history of syphilis generally not useful clinically. However, 15% to 25% of treponemal tests become nonreactive between 2 and 3 years after treatment of primary syphilis.143 The tests are highly specific and sensitive during the secondary and the late phases of the disease. Treponemal test titers do not correlate with, and are not used to monitor, disease activity. Sensitivity is low in the weeks after infection, but is nearly 100% by 12 weeks (see Fig. 170-38). Falsepositive results in treponemal tests are also rare, but are associated with infections, autoimmune or connective tissue disease, and narcotic addiction.126,143,144
3164
ACUTE CHRONIC
Physiologic Pregnancya Advanced age
Spirochete Leptospirosis Endemic syphilis
Infection
Lyme disease Rat-bite fever Relapsing fever
Pinta Yaws
Viral infection
Cytomegalovirus Infectious mononucleosis Hepatitis Herpes simplex Herpes zostervaricella infection Measles Mumps Mycoplasma pneumonia Toxoplasmosis Viral sepsis
Human T-cell leukemia/ lymphoma virus 1 HIV infection
Bacterial infection
Pneumonia
Lepromatous leprosy Lymphogranuloma venereum Tuberculosis
Protozoan infection
Malaria
Kala azar Trypanosomiasis
Autoimmune
Autoimmune hemolytic syndrome
Disease
Autoimmune thyroiditis Idiopathic thrombocytopenic purpura Mixed connective tissue disease Polyarteritis nodosa Primary biliary cirrhosis Rheumatoid arthritis Sjögren syndrome Systemic lupus erythematosus
Other Drug abuse Dysproteinemias Hepatic cirrhosis Malnutrition Malignancy Lymphoproliferative
Other
Drug abuse Dysproteinemias Hepatic cirrhosis Malnutrition Malignancy Lymphoproliferative disorders
disorders
aEvidence for pregnancy as a cause of biologic false-positive reactions is limited and concern persists for clinicians failing to diagnosis syphilis in pregnancy.
THE REVERSE SEQUENCE ALGORITHM
The automation of EIA tests, a form of treponemal test, has made EIAs less expensive for large-volume laboratories to perform.126,145 As a result, many large-volume
laboratories have begun to use EIAs rather than nontreponemal tests as the first step of the algorithm for laboratory diagnosis of syphilis.39 In this “reverse sequence” algorithm, a treponemal EIA is performed first. If and only if the EIA result is reactive, is a nontreponemal test is performed. Reactive results on both tests confirm a diagnosis of syphilis. In approximately 3% of cases, a reactive treponemal EIA result is followed by a nonreactive nontreponemal test result. In those cases, a tie-breaker test, consisting of an alternate treponemal test, can be performed, with data combined with clinical suspicion to determine diagnosis and treatment.145
The use of the reverse sequence algorithm does lead to the identification of a number of serodiscordant
26
patients in whom both the initial and “tie-breaker” treponemal tests are positive, but the nontreponemal test is negative. This can occur in the setting of the prozone phenomenon, early primary syphilis, adequately treated past syphilis, or untreated syphilis of long duration. Patients with a history of treatment will require no further management unless the sexual history suggests recent reexposure. Those without a history of treatment should be treated. Knowledge of sexual history, clinical findings and results of prior serologic tests for syphilis is therefore necessary to appropriately interpret the results of serologic testing.35,133 Figure 170-39 illustrates the interpretation of reverse sequence algorithm results.
Interpretation of the reverse sequence algorithm
Treponemal test positive (EIA/CIA+)
Nontreponemal test (eg, RPR)
Nontreponemal test positive (RPR+)
Syphilis
• Untreated infection
• Treated infection
Alternative treponemal test positive (TPPA+)
Syphilis
• Early primary syphilis
• Treated infection
• Untreated infection
Treponemal test (eg, EIA or CIA)
Treponemal test negative (EIA/CIA–)
Syphilis unlikely, although false negative in very early syphilis possible
Nontreponemal test negative (RPR–)
Alternative treponemal test (eg, TPPA)
Alternative treponemal test negative (TPPA–)
Syphilis unlikely
• If concern for incubating or very early primary syphilis, repeat in 2 to 4 weeks
3165
26
RAPID SEROLOGIC TESTS
Of note, several rapid, point-of-care serologic tests for syphilis are in use or under development internationally. One has been cleared for use outside of laboratory settings in the United States, and others are under development.146
CONGENITAL SYPHILIS
Transplacental transfer of maternal nontreponemal and treponemal IgG antibodies to the fetus complicates serologic diagnosis of congenital syphilis.35 Infants born to mothers with reactive nontreponemal and treponemal tests should be evaluated with a quantitative nontreponemal serologic test performed on infant serum, as umbilical cord blood might be contaminated with maternal blood, yielding a false-positive result. Treponemal tests are difficult to interpret in this setting and are not recommended by the CDC. All infants whose mothers have reactive serologic tests should be examined carefully for evidence of congenital syphilis. If possible, suspicious lesions or body fluids (eg, nasal discharge) should be tested using darkfield microscopy or PCR testing. Pathologic examination of the placenta using specific staining or a T. pallidum PCR test should be considered.35 Any neonate with proven, highly probable or possible congenital syphilis (based on assessment of physical examination, serologic tests, darkfield microscopy or PCR of lesions or body fluid, and adequacy of maternal treatment) should have CSF tested for VDRL reactivity, white blood cell count, and protein level, as well as other tests that would suggest other diseases in the differential diagnosis. Other tests, such as long-bone radiographs, chest radiographs, liver function tests, neuroimaging, ophthalmologic examination, and auditory brainstem response may be necessary as clinically indicated.35
CLINICAL COURSE AND PROGNOSIS
Despite decades of use, T. pallidum has remained sensitive to penicillin. Although treatment failures do occur, and may be more common in HIV-infected patients, penicillin treatment is generally very effective at eradicating the infection in all stages of syphilis. Although severe, and in a few rare cases, life-threatening complications of secondary syphilis can occur,147 the vast majority of patients with primary and secondary syphilis will have resolution of symptoms with no permanent sequelae (even without treatment). The goal of antibiotic therapy, then, is not only to address the immediate syndrome, but also to prevent transmission to sexual partners, and progression to tertiary syphilis. Unfortunately, in tertiary syphilis, irreversible damage to vital structures may occur through gummas or cardiovascular or CNS involvement. Neurosyphilis, which can occur at any stage, can be life-threatening. Of note, several patients in the recently reported
3166
cluster of 12 ocular syphilis cases developed permanent sequelae despite appropriate treatment; 2 of the 12 became legally blind.37
MANAGEMENT
Based on data from case series and clinical trials and long clinical experience,148 penicillin is the recommended treatment for all stages of syphilis, with the preparation, dose, and length of treatment dependent on the clinical manifestations, stage of disease, and age of the patient.35 Benzathine penicillin G, the recommended preparation of penicillin for most stages of syphilis, has a long half-life, which is critical therapeutically because of the slow dividing time of T. pallidum. The choice of penicillin formulation is important in assuring adequate treatment. In the United States, the only penicillin product that is appropriate for treatment of primary, secondary, or latent syphilis is Bicillin L-A, which contains only benzathine penicillin G. Another similarly packaged product, Bicillin C-R, contains procaine penicillin G in addition to benzathine penicillin G and is not an appropriate treatment. Substantial confusion and errors relating to those 2 products have been reported.149,150
Penicillin-allergic persons with syphilis who are not pregnant and do not have neurosyphilis may be treated with doxycycline. Pregnant women who are penicillin-allergic must be desensitized to and treated with penicillin, which is the only drug that is known to prevent maternal transmission and to treat infection in the fetus.35 Reports of treatment failures and emergence in T. pallidum of resistance to macrolides, including azithromycin, at one point a convenient alternative to penicillin because of its oral formulation, now precludes use of that class of drug in the United States and much of the world,151-153 although it may still be used with caution in some areas.137 As discussed previously, CDC-recommended treatment regimens do not differ on the basis of a person’s HIV infection status.35
Clinical and serologic followup is important to monitor response to treatment (see Table 170-5). Treatment success is generally defined as a fourfold decline in serologic nontreponemal titer (or reversion to nonreactive result) following appropriate treatment, in the absence of persistent signs or symptoms of syphilis, and within a specified time frame depending on stage of infection and HIV infection status of the infected person.35 An example of a fourfold decline in titer is a 1:64 titer declining to 1:16, or a 1:16 titer declining to 1:4. The CDC recommends followup at 6-month intervals until a fourfold decline is documented, except for HIV-infected persons with
primary or secondary syphilis, for whom followup at 3, 6, 9, 12, and 24 months is recommended, and congenital syphilis, for whom followup every 2 to 3 months is recommended.35 Approximately 15% to 20% of persons with primary and secondary syphilis who are treated appropriately will remain serofast and will not achieve the fourfold decline in titer. The CDC guidelines recommend additional clinical followup, and in some cases, retreatment or CSF evaluation to rule out CNS infection.35
A fourfold titer increase following appropriate treatment indicates reinfection or treatment failure—the latter in some cases associated with neurosyphilis—with treatment depending on which of those is believed to have caused the increase. Reinfection must be assessed by clinical history and physical examination. If treatment failure cannot be ruled out, the patient should be treated with 7.2 million units of benzathine penicillin G (divided into 3 weekly doses); CSF examination should be performed to determine whether neurosyphilis is present, and, if it is, the patient also should be treated for neurosyphilis.35
COMPLICATIONS OF TREATMENT
COMPLICATIONS OF
TREATMENT
The Jarisch-Herxheimer reaction is a self-limited clinical syndrome consisting of fever, headache, flare of mucocutaneous lesions, tender lymphadenopathy, pharyngitis, malaise, myalgia, and leukocytosis. It occurs within the first 24 hours after initiating therapy. The fever peaks 6 to 8 hours after the onset, usually around 39°C (102.2°F), but it can be as high as 42°C (107.6°F). Patients should be warned about the possibility of developing this reaction before receiving treatment. Acetaminophen can be used to attempt to diminish the reaction, although very little evidence of its effectiveness exists.35 The patient should be encouraged to rest, maintain fluid intake, and seek medical attention if symptoms are severe. The pathogenesis of the Jarisch-Herxheimer reaction is unknown, but is thought to result from cytokine release mediated by the release of lipoproteins from dying T. pallidum organisms.154 In pregnant patients, the Jarisch- Herxheimer reaction may lead to premature labor or fetal distress, events that should prompt the patient to seek evaluation. However, given the potentially devastating effects of congenital syphilis, prompt treatment of maternal syphilis is critical.35
Anaphylaxis from administration of penicillin injection is a life-threatening emergency that is managed by epinephrine and other medications, such as antihistamines, along with emergent transfer to a monitored setting.155
At the time of initial treatment, patients should be educated to distinguish an allergic reaction, which precludes further treatment with penicillin or related drugs, from a Jarisch-Herxheimer reaction, which does not.
26
DISEASE REPORTING AND MANAGEMENT OF PERSONS EXPOSED TO SYPHILIS
DISEASE REPORTING
AND MANAGEMENT
OF PERSONS EXPOSED
TO SYPHILIS
As reflected by the efforts to eliminate syphilis in the United States, prevention and control of syphilis are of substantial public health interest in the United States and worldwide.2,35 Syphilis is a nationally notifiable disease in the United States, meaning that both clinicians and laboratories are mandated by law to report cases or laboratory results diagnostic of or suspicious for syphilis to their local or state public health authorities. Clinicians should contact their local or state health department to familiarize themselves with local reporting requirements, including required forms and need for paper-based or electronic reports, for syphilis and other reportable diseases.35
Local or state public health authorities maintain databases of syphilis diagnoses, laboratory results, and treatments for persons diagnosed with syphilis. That information is available to clinicians taking care of persons with suspected syphilis and can be helpful in staging infections (eg, determining if criteria for early latent syphilis are met) and assuring appropriate treatment. Clinicians should routinely encourage persons diagnosed with syphilis to inform their sex partners of exposure to syphilis and followup with patients to assure that disclosure has occurred. Identifying which sex partners are at risk of infection depends both on the elapsed time since last exposure and stage of infection in the source patient. This risk period is 3 months plus duration of symptoms for primary syphilis, 6 months plus duration of symptoms for secondary syphilis, and 1 year for early latent syphilis and latent syphilis of unknown duration. Clinicians should also inform persons they diagnose with syphilis that the case will be reported to the public health authority and that, in many cases, health department workers (sometimes called Communicable Disease Investigators or Disease Intervention Specialists) will contact the person to ensure that treatment was adequate, provide education about syphilis, solicit contact information for sex partners, and inquire about sexual behaviors so that prevention and control resources can be targeted to affected populations. It is a principle of public health practice, including in syphilis contact-tracing investigations, to protect the confidentiality of the source partner.35
Management of at-risk sex partners of persons diagnosed with syphilis also depends on elapsed time since exposure. Sex partners exposed during the 90 days preceding the diagnosis of primary, secondary, or early latent syphilis should be examined and tested for syphilis. However, regardless of results of the physical examination and laboratory tests, those partners should be treated presumptively because of the high efficacy of prophylactic
3167
26
treatment and the likelihood (up to 63%) that they been infected but have yet to show clinical or laboratory evidence of disease. Persons exposed more than 90 days before the diagnosis of primary, secondary, or early latent syphilis should also be examined and tested and treated presumptively if serologic test results are not available immediately and the opportunity for followup is uncertain. Sex partners of persons with late latent syphilis should be evaluated and tested, and then managed on the basis of those findings.35
PREVENTION AND SCREENING
PREVENTION AND
SCREENING
Safer sex practices are critical for prevention of syphilis transmission. Screening also may be important in identifying asymptomatic patients who should be treated. The CDC recommends that all pregnant women be screened at the first prenatal visit, with retesting early in the third trimester and at delivery if at high risk for syphilis. Sexually active MSM should be screened at least annually, and every 3 to 6 months if at increased risk (eg, patient or sexual partner has multiple partners). Persons with HIV who are sexually active should be screened at first HIV evaluation and then at least annually thereafter, with more frequent screening depending on individual risk behaviors and the local epidemiology.35
ACKNOWLEDGMENTS
We appreciate the significant contributions of Dr. Kenneth Katz to this chapter. We also thank Dr. Gerald Lazarus for his help in reviewing and selecting the images for this chapter.

Figure 170-1 Early chancre presenting as a large oval ulcer with elevated borders on the shaft of the penis.

Figure 170-2 Early chancre on the penile shaft, demonstrating a clean base.

Figure 170-3 Chancre on the penile shaft, demonstrating a clean base and elevated borders
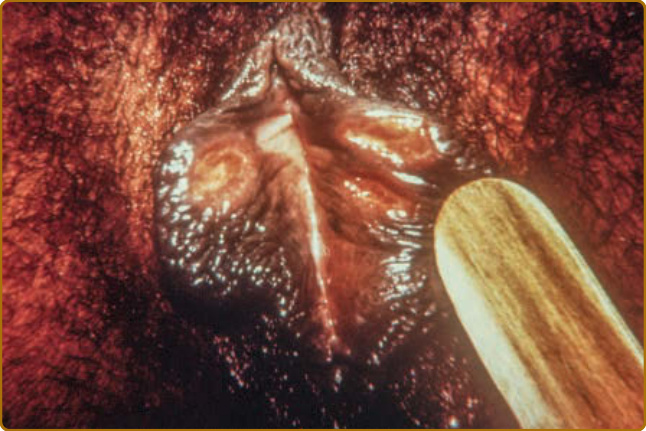
Figure 170-4 Chancres on the labia in a female.

Figure 170-5 Chancre on the tongue.

Figure 170-6 Chancre in the perianal area. Fecal material is also present in the area.

Figure 170-7 Rash of secondary syphilis with nonscaling, oval pink, ill-defined macules and patches on the trunk.

Figure 170-8 Papulosquamous syphilitic eruption with erythematous, well-demarcated, flattened plaques covered with scales (Biett collarette).

Figure 170-9 Secondary syphilis lesions: multiple, hyperpigmented scaly papules on the palms.

Figure 170-10 Secondary syphilis lesions: multiple, hyperpigmented papules with more pronounced scale on the palms.
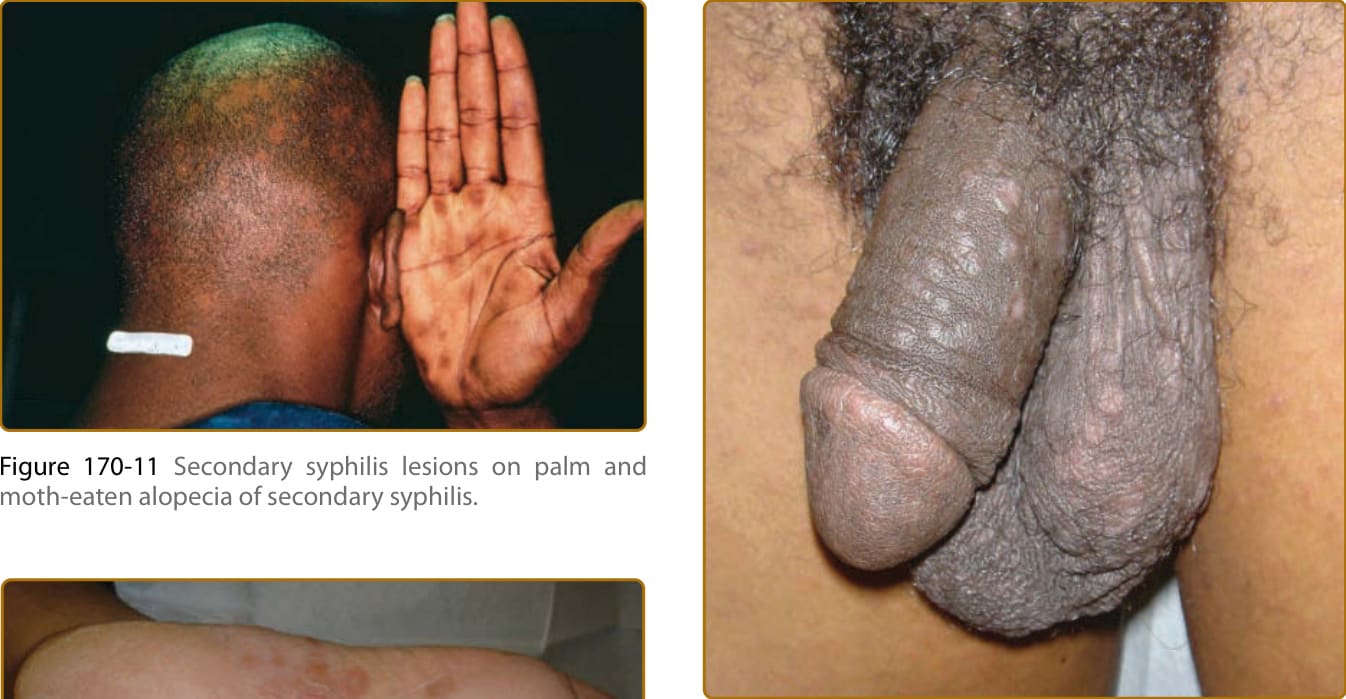
Figure 170-11 Secondary syphilis lesions on palm and moth-eaten alopecia of secondary syphilis.

Figure 170-12 Secondary syphilis lesions on sole of foot.
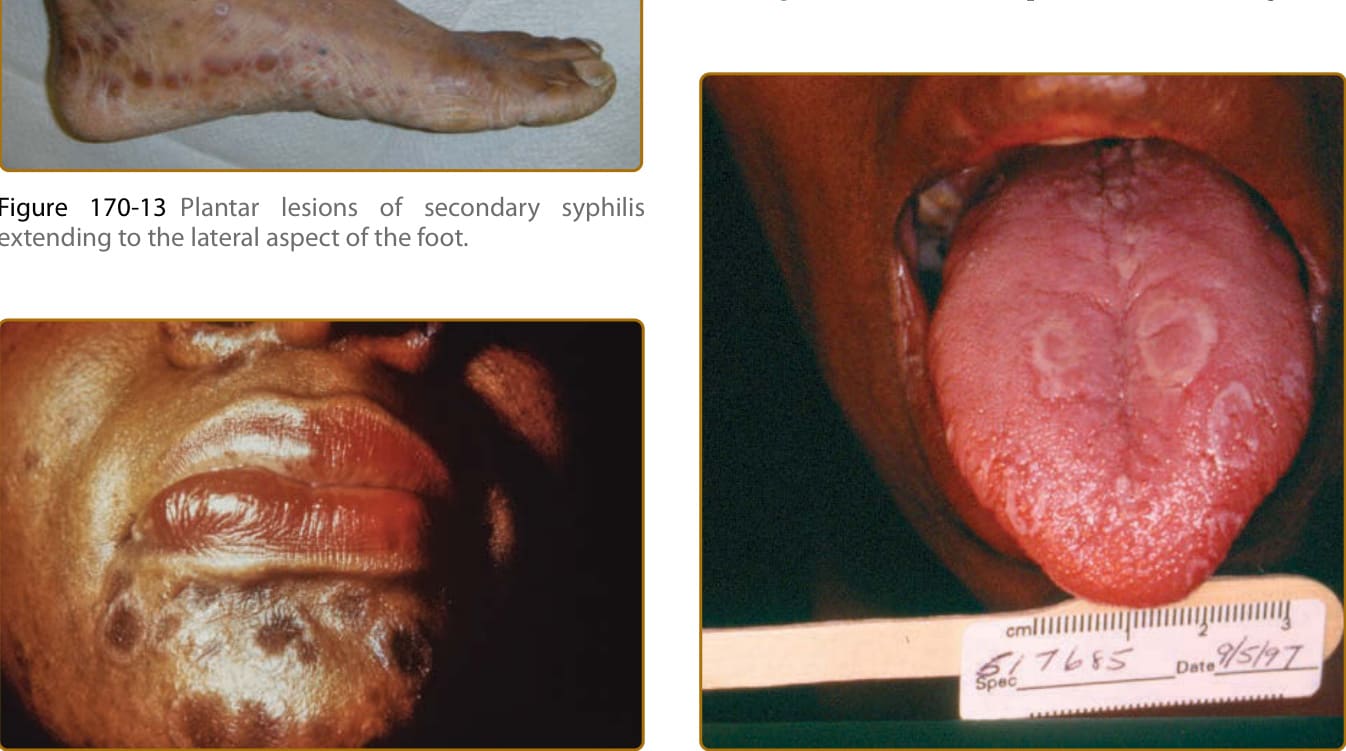
Figure 170-13 Plantar lesions of secondary syphilis extending to the lateral aspect of the foot.

Figure 170-14 Annular plaques of secondary syphilis on the face, colloquially referred to as “nickels and dimes.”

Figure 170-15 Papules of secondary syphilis on the penis.
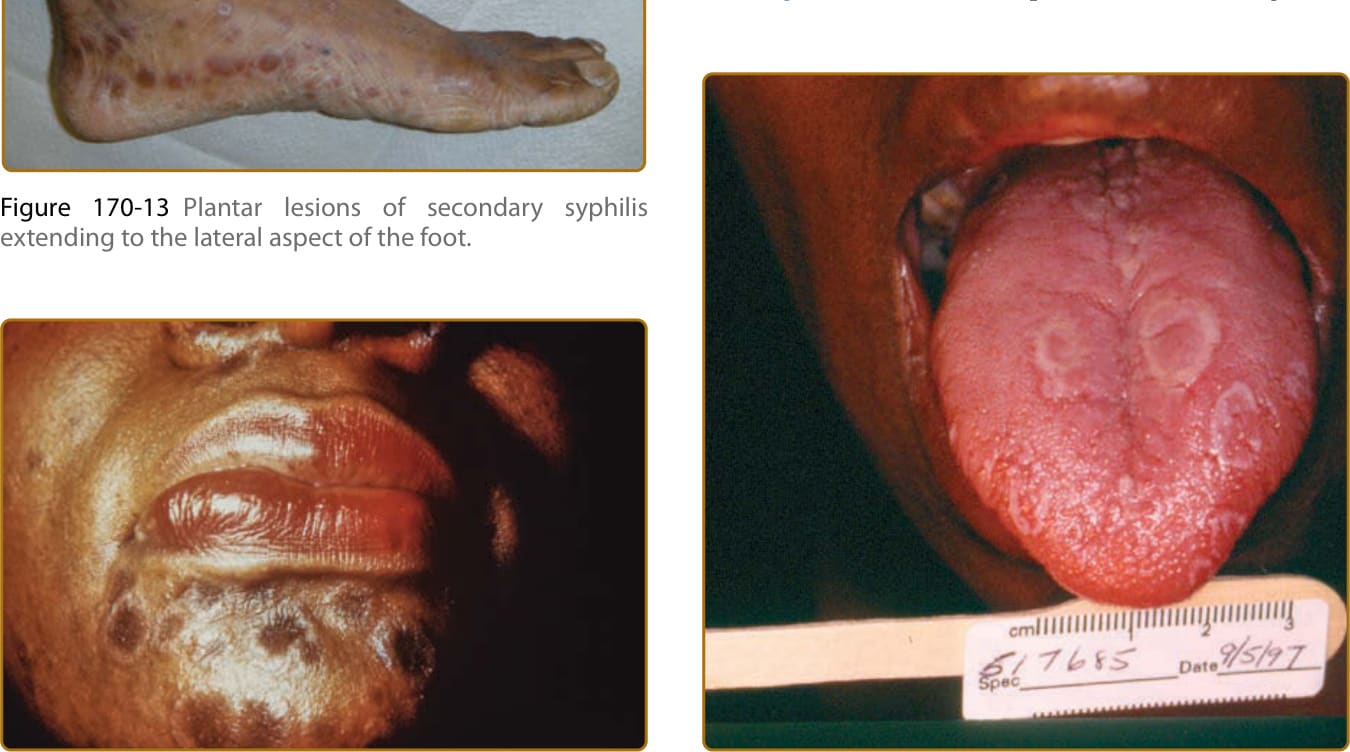
Figure 170-16 Mucous patches of the tongue in secondary syphilis. Note lack of typical lingual papillae in affected areas.

Figure 170-17 Mucous patches on hard palate.
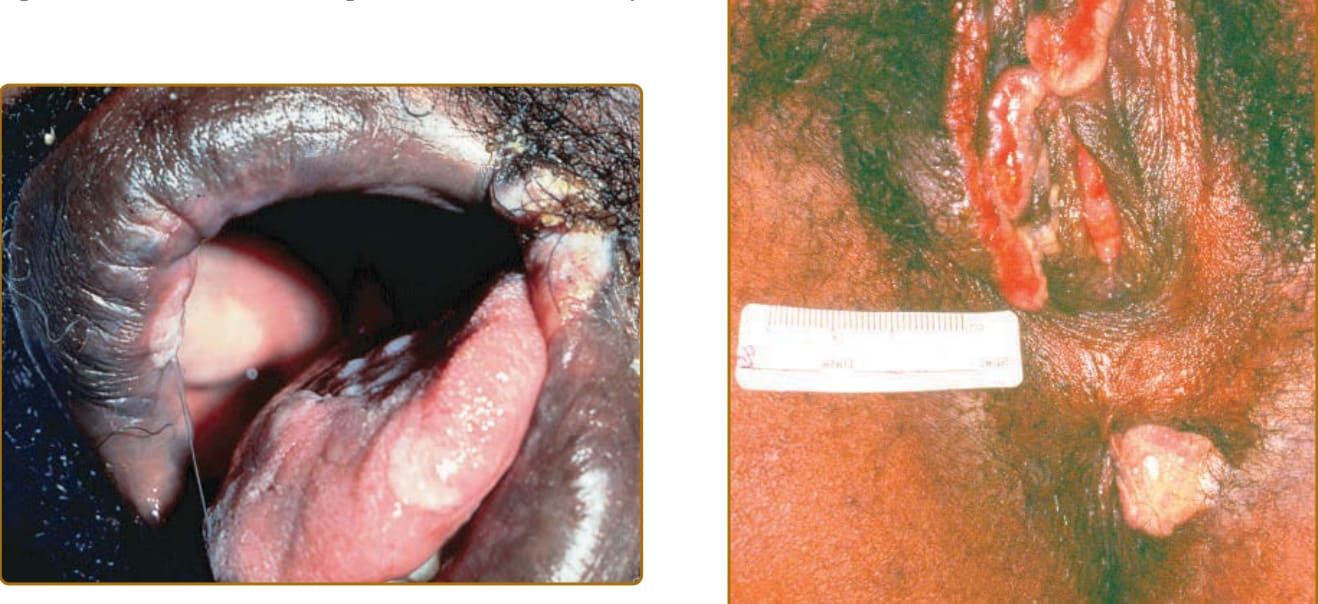
Figure 170-18 Split papule, a type of mucous patch of secondary syphilis that can be present at the angle of the mouth, with a characteristic slit traversing its center.
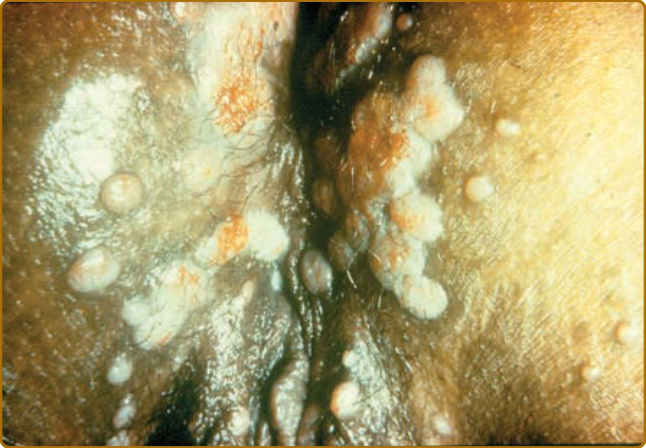
Figure 170-19 Condyloma lata, presenting as moist papules in the perineum.

Figure 170-20 Condyloma lata, presenting as moist, flattopped plaques on the buttocks.
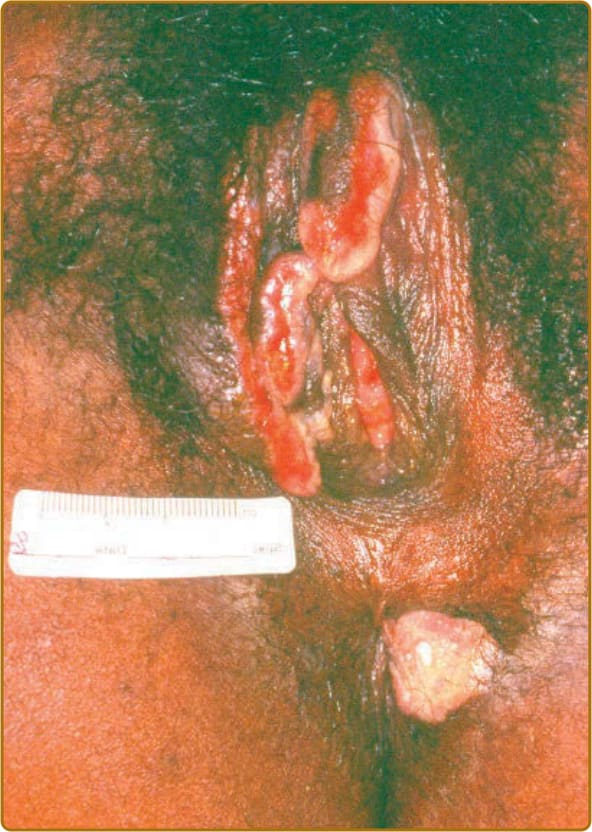
Figure 170-21 Condyloma lata in a female.

Figure 170-22 Moist papule in the umbilicus in secondary syphilis.

Figure 170-23 Sharply marginated, necrotic ulcers of secondary syphilis described as “rupioid,” covered by thick, dirty crusts (like oyster shells).

Figure 170-24 Multiple hyperpigmented papules of secondary syphilis on the arm.

Figure 170-25 Hyperkeratotic lesions of secondary syphilis on the soles.

Figure 170-26 Psoriaform lesions of secondary syphilis on the arm.

Figure 170-27 Disfiguring gummatous infiltration of the glabella and forehead with scattered ulcerations in a 60-year-old woman with late benign syphilis.
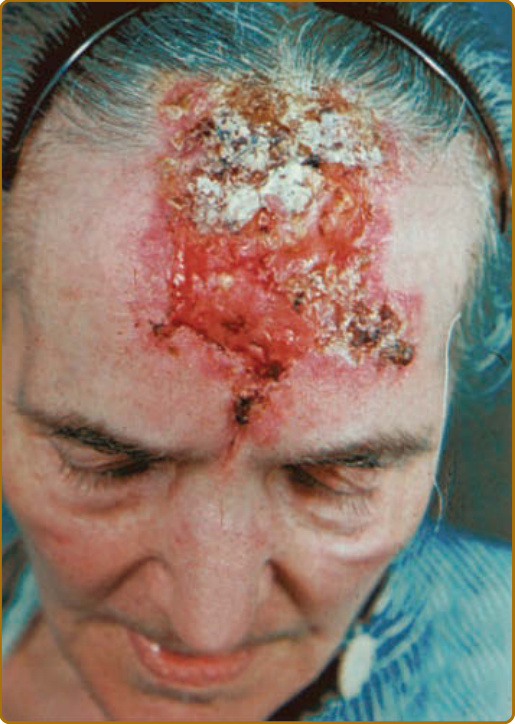
Figure 170-28 Aggressive gumma of the forehead causing destruction of the calvarium, mimicking advanced, destructive basal cell carcinoma.

Figure 170-29 Two deep, punched-out ulcers in the popliteal fossa covered with an adherent yellow slough at the base. This is the classical appearance of nodular gummas.

Figure 170-30 Destruction of the nasal cartilage and bone by a gumma leads to a saddle nose (A) and to the perforation of the nasal cartilage and skin and thus to considerable mutilation (B).

Figure 170-31 Premalignant, chronic, interstitial glossitis secondary to gummatous infiltration of the tongue.

Figure 170-32 Bullous eruptions on the soles of a newborn with early prenatal syphilis. Bullae have ruptured and now present as erosions (“syphilitic pemphigus”).

Figure 170-33 Hyperpigmented papules of syphilis in a neonate.

Figure 170-34 Early prenatal syphilis in a newborn. The skin is dry and wrinkled, with a yellowish-brownish hue. There is hemorrhagic rhinitis. This is what Diday described as “a little wrinkled potbellied (not seen here) old man with a cold in his head.” Note also the aged appearance of the fingers in this newborn.

Figure 170-35 Perioral rhagades are linear scars that result from ulcerations that appear during early congenital syphilis and persist to adulthood.

Figure 170-36 The presence of small, notched, pegshaped upper incisors (Hutchinson teeth) is also part of the late congenital syphilis triad.

Figure 170-37 Darkfield microscopy showing a treponeme.
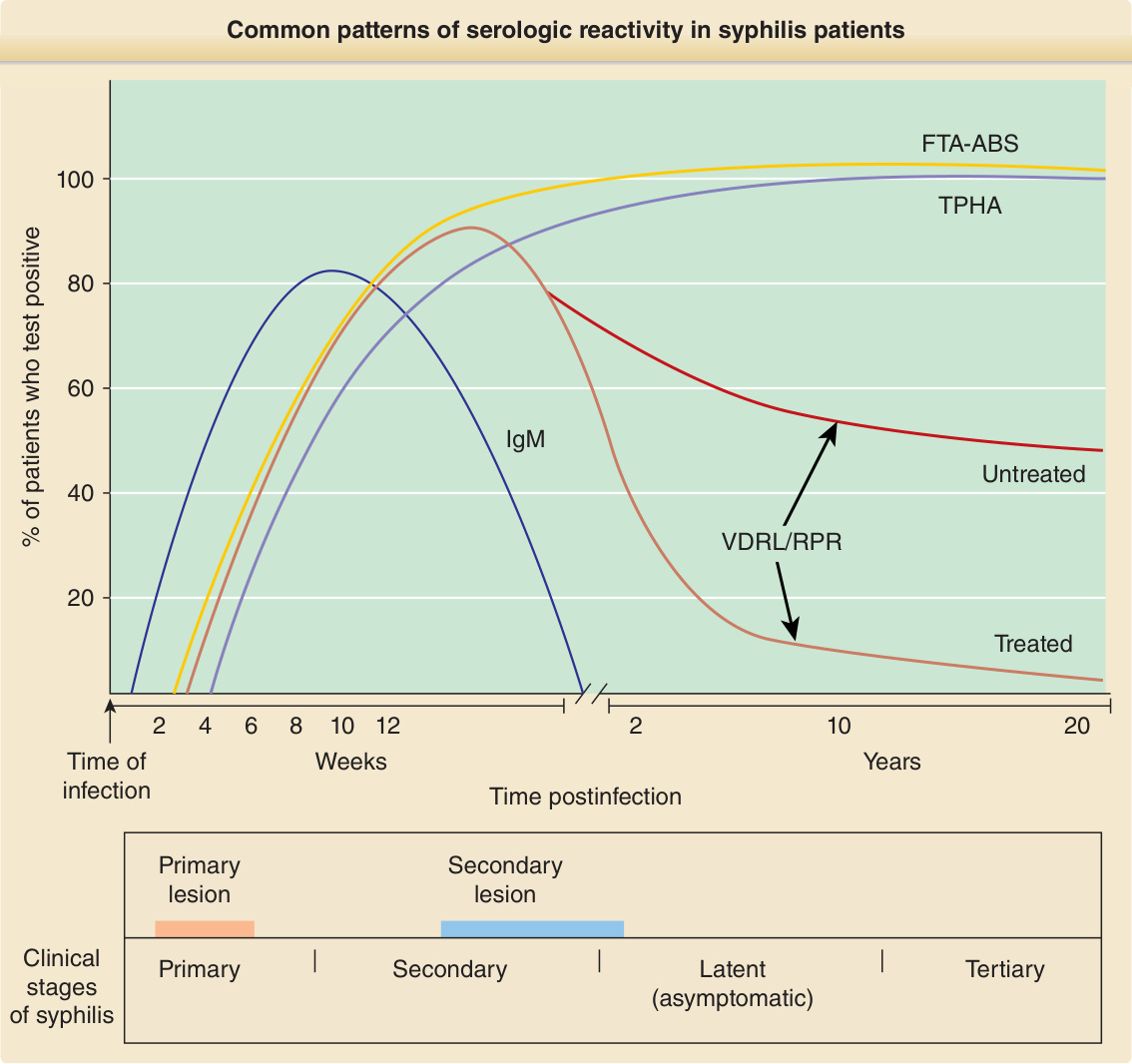
Figure 170-38 Common patterns of serologic reactivity in syphilis patients. FTA-ABS, Fluorescent treponemal antibody absorption assay; IgM, immunoglobulin M; RPR, rapid plasma reagin; TPHA, Treponema pallidum hemagglutination test; VDRL, Venereal Disease Research Laboratory. (From Peeling RW, Ye H. Diagnostic tools for preventing and managing maternal and congenital syphilis: an overview. Bull World Health Organ. 2004;82(6):439-446. By permission of World Health Organization.)
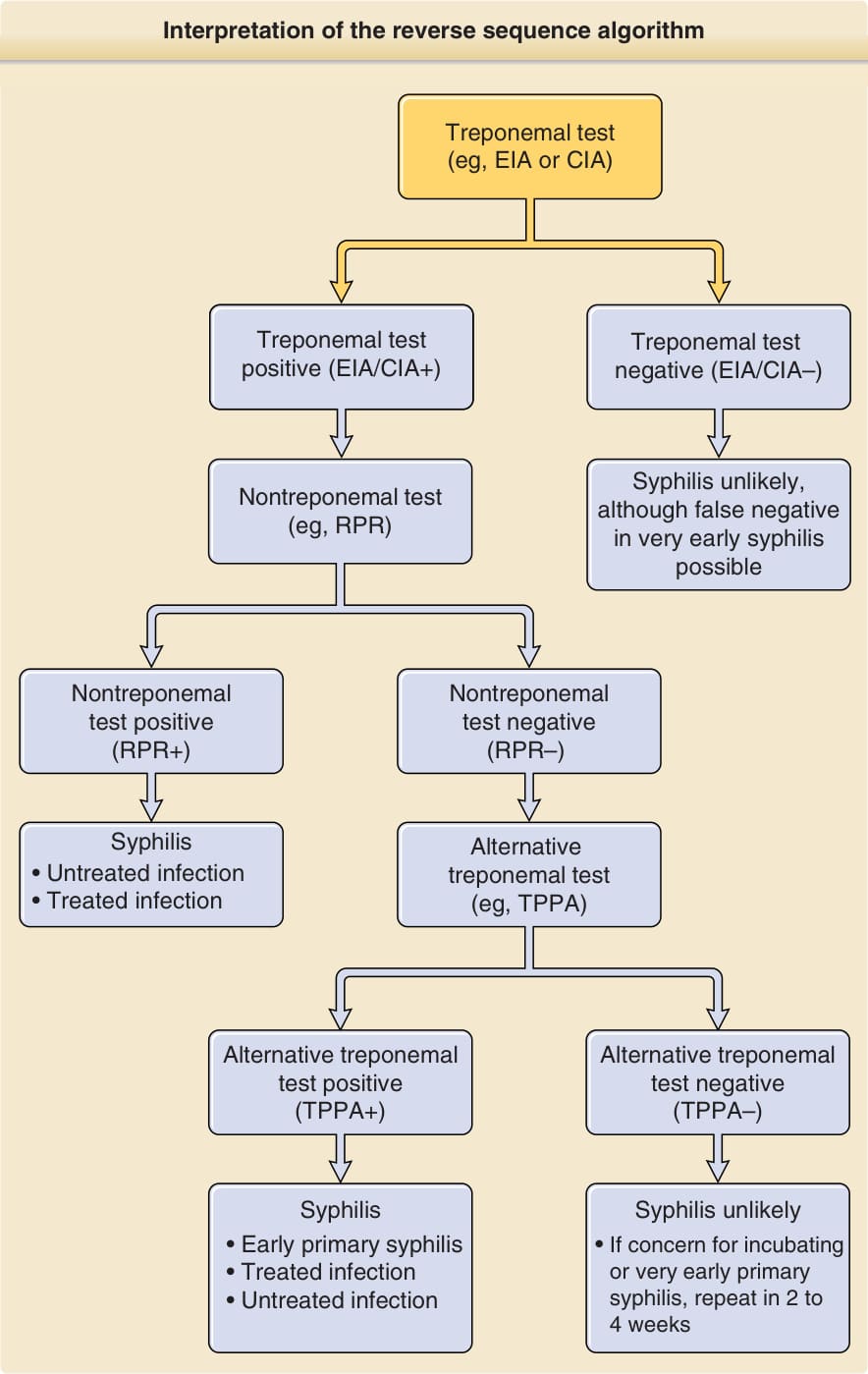
Figure 170-39 Interpretation of the reverse sequence algorithm.133,145 CIA, Chemiluminescent immunoassay; EIA, enzyme immunoassay; RPR, rapid plasma reagin; TPPA, Treponema pallidum particle agglutination.
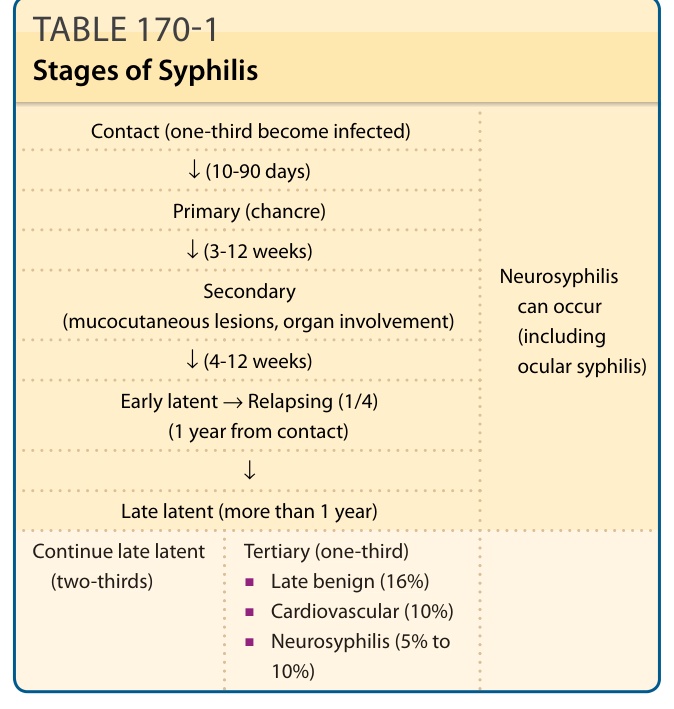
TABLE 170-1 Stages of Syphilis
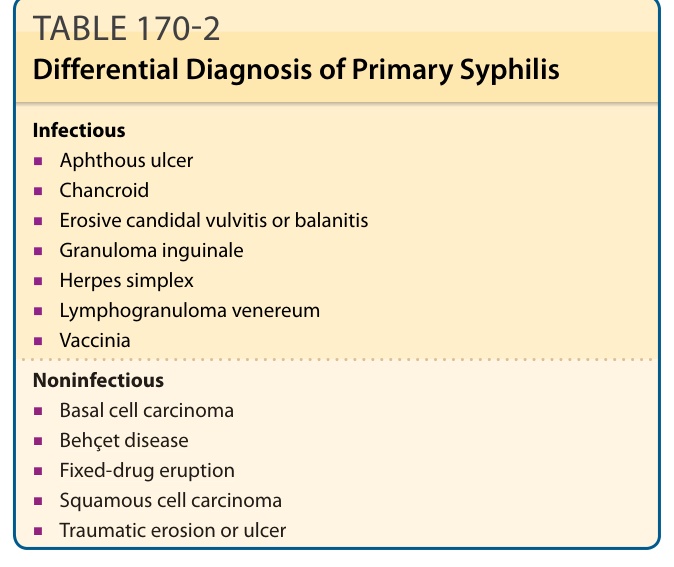
Table 170-2 outlines the differential diagnosis of chancres.
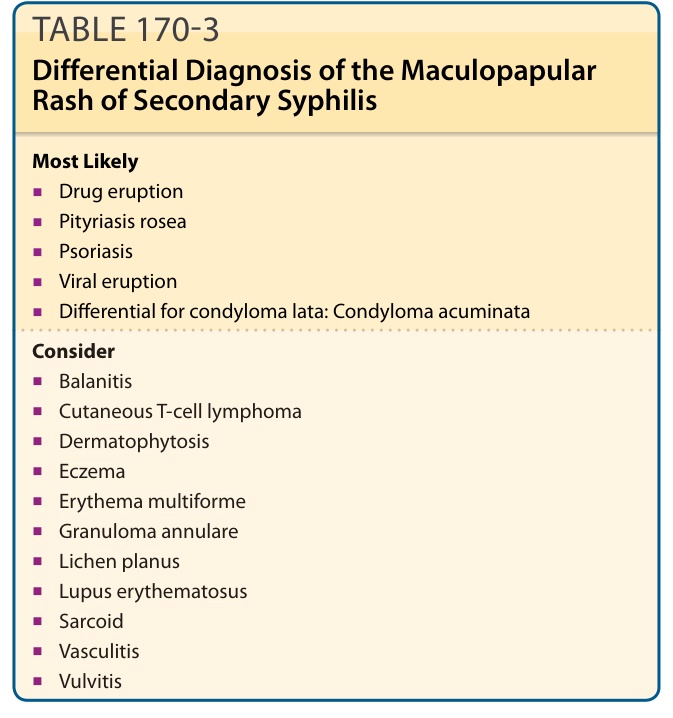
TABLE 170-3 Differential Diagnosis of the Maculopapular Rash of Secondary Syphilis
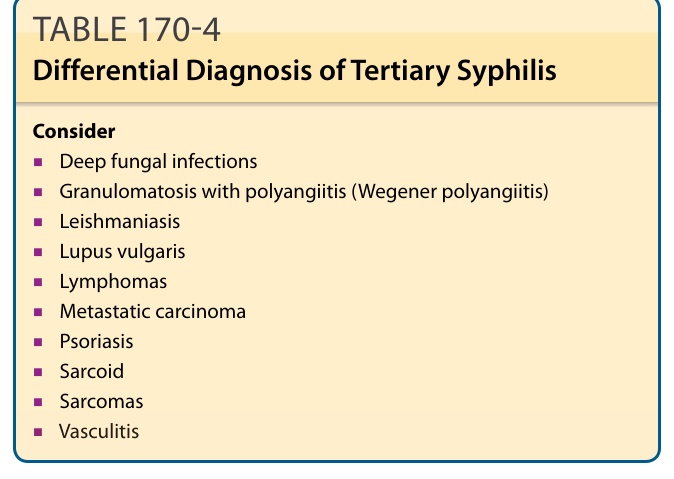
Table 170-4 outlines the differential diagnosis of dermatologic manifestations of tertiary syphilis.
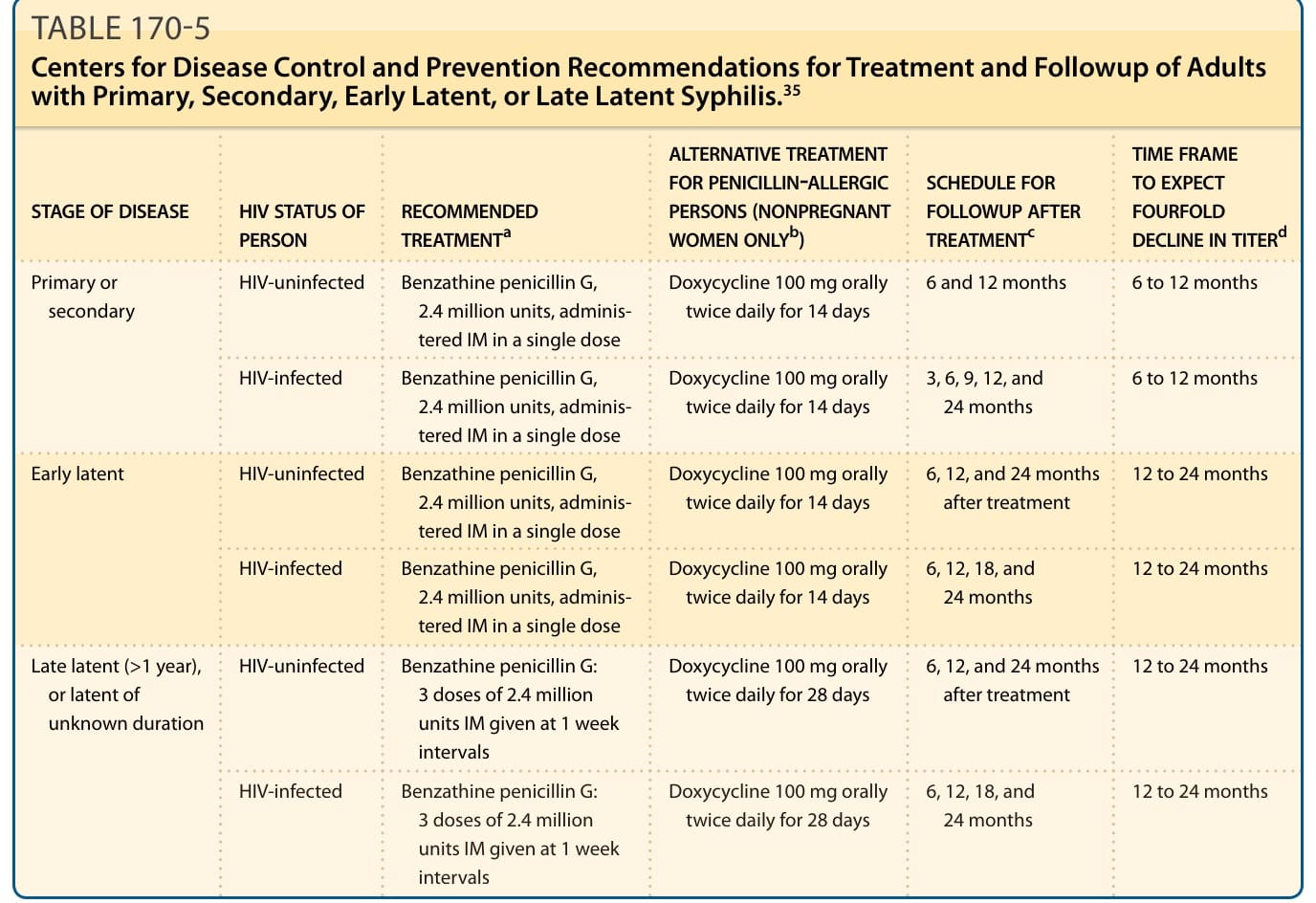
TABLE 170-5 Centers for Disease Control and Prevention Recommendations for Treatment and Followup of Adults with Primary, Secondary, Early Latent, or Late Latent Syphilis.35
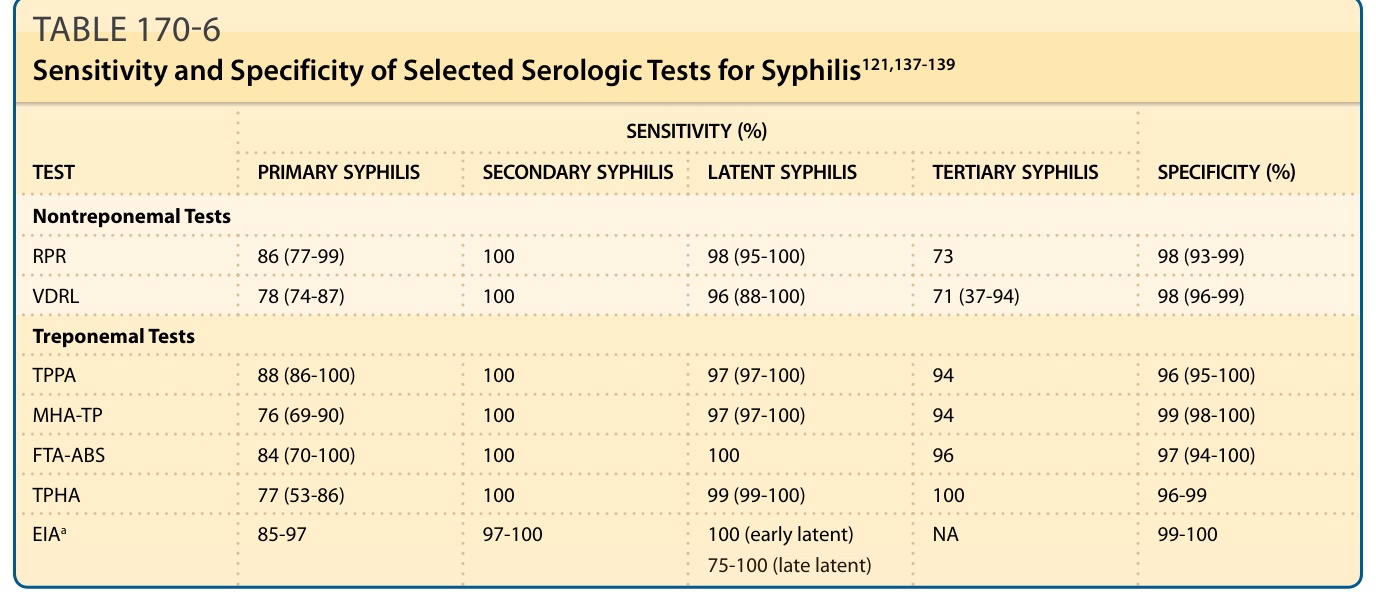
TABLE 170-6 Sensitivity and Specificity of Selected Serologic Tests for Syphilis121,137-139
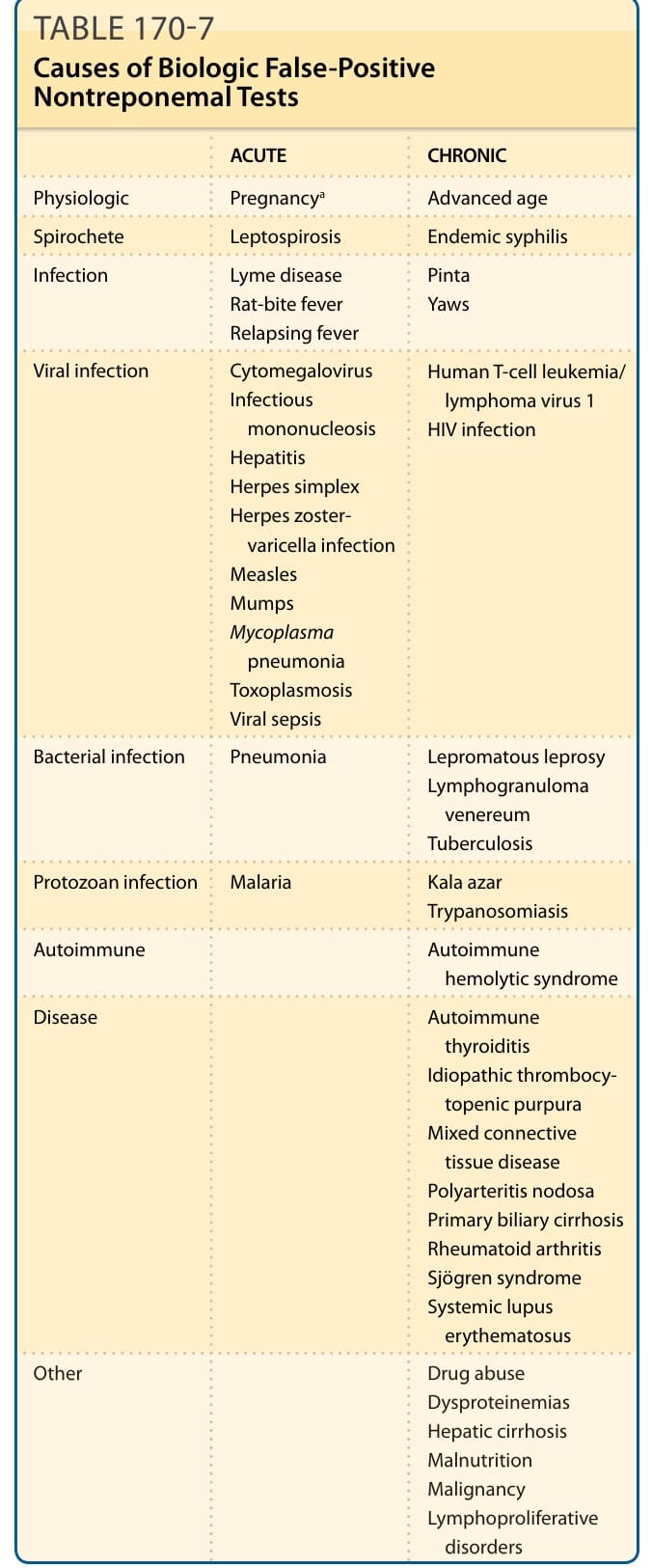
TABLE 170-7 Causes of Biologic False-Positive Nontreponemal Tests