Human Papillomavirus Infections
25
AT-A-GLANCE
■ Human papillomavirus (HPV) has a worldwide occurrence, affecting people of all ages and all races. It is most common in children and young adults.
■ There are more than 150 genotypes of HPV, with some regional specificity. Low-risk types cause warts; high-risk types are associated with intraepithelial neoplasia and malignancy.
■ The lesions are well-defined, raised papules or plaques with a rough or hard surface, usually without inflammation.
■ The lesions are most common on the hands or feet, but any skin site may be affected, including the lower genital or oral mucosa.
■ Treatments include destructive, antiviral, antiproliferative, and immunologic modalities.
INTRODUCTION
Human papillomavirus (HPV) infections are very common, occurring in a worldwide distribution, affecting all ages and lasting months or years. The majority of individuals will have at least one infection with the virus during the course of a lifetime, although the severity and duration of the disease will depend, to a large extent, on the immune response raised against the virus-infected cells. The clinical disease caused by the virus is also dependent on the viral genotype and the body site. Whereas skin and mucosal warts are benign and induced by one of several different types according to body site, premalignancies and invasive cancer of the anogenital area or oropharynx are associated with other, so-called high-risk, HPV types (Table 167-1).
VIROLOGY
The papillomaviruses form a large group of closely related viruses, defined by their host range. HPVs only infect humans and, in particular, epithelial keratinocytes. In experimental systems, the virus does not infect keratinocytes in monolayer tissue culture. Papillomaviruses are DNA viruses with each virus particle or virion consisting of a nonenveloped icosahedral capsid containing the double-stranded genetic material as a circular genome (Fig. 167-1). The virus is much smaller, both in particle size and length of genetic material, than other common viruses that
infect skin such as herpes simplex virus and molluscum contagiosum virus. The genes are all transcribed in one direction from one DNA strand, leading to the production of 5 to 6 early (E) proteins involved in DNA replication, cell cycle control and immune evasion; and 2 late (L) proteins, L1 and L2, that form the outer shell or capsid (Fig. 167-2). The virus is shed from the surface of the skin or mucosa within sloughed, dead keratinocytes. New infection occurs when the virus particle contacts the basal epidermal keratinocyte, presumed to be via small microabrasions in the skin or mucosa. Maceration of skin can increase the chance of infection because of impairment of barrier function. Cell entry depends on an initial adherence of the virion to the cell via heparin sulphate and α6-integrins,1,2 although the full process of receptor binding leading to internalization by endocytosis has not yet been clarified. Within a stem cell or transit amplifying cell of the basal layer, the virus is maintained in low copy number. It is carried to the surface in daughter cells, producing, as it goes, the early viral proteins. High-volume viral DNA amplification and L1 and L2 protein production occurs in the upper layers, with formation of completely new virus particles in the granular layer. The switch to capsid protein production depends on a change in splice site usage in the early genes.3 The E6 and E7 proteins are pivotal to the process of viral genome amplification, which also depends on the E1 and E2 proteins. The viral E1^E4 protein can interact with keratin filaments, weakening cytoplasmic structure and potentially facilitating virus particle release at the surface.4
There are more than 150 HPV types, defined according to the DNA sequence within the L1 gene.5 A virus is defined as a distinct type if there is greater than 10% dissimilarity from other known HPVs in the DNA of this region. The HPVs have been grouped, according to phylogeny, into five genera: alpha, beta, gamma, mu, and nu (see Table 167-1). HPVs that are not found in malignancies or premalignancies are termed low-risk types, and those found in invasive or preinvasive disease are called high-risk types. The high-risk anogenital HPVs fall into the large alpha genus. High-risk genital HPV types can integrate within the host cell genome, and the maintained expression of their E6 and E7 proteins has oncogenic effects on cell division and cell function. These E6 and E7 proteins affect cell cycle control and apoptosis via interaction with ubiquitin ligases, telomerase, and several other cellular pathways.6 In the process of integration, the E2, E4, L2, and to a lesser extent the L1 regions of the genome are frequently disrupted. In malignant lesions, late proteins and virus particles are rarely, if ever found, although episomal (nonintegrated) viral DNA may be maintained in preinvasive disease.
25
DISEASE CLINICAL
MOST COMMONLY ASSOCIATED HPV TYPESa PV GENUS
Cutaneous warts
Common warts, filiform warts, mosaic warts Palmar and plantar warts Butchers’ warts Plane warts
2, 27, 57 (7) 4, (60) (48) 1, (63)
Alpha Mu Gamma Nu
2, 7 3, 10 (28)
Alpha Alpha
Anogenital warts Vulval warts, vaginal warts, penile warts, perianal warts
6, 11 (and others) Alpha
Oral warts
6, 11 (and others) Alpha
EV and EV-like syndromes
Benign scaly or flaky lesions; Plane warts Skin SCC
9, 12, 15, 19, 22-25, 36-38, 80 3, 10 5, 8, 14, 17, 20, 21, 47, 93, 96
Beta
Alpha Beta
Skin SCC Periungual SCC 16 Alpha
Carcinoma cuniculatum or verrucous carcinoma
(11, 6) Alpha
AGIN VIN, VaIN, CIN, PIN, AIN 16, (18, 31, 33, 35, 45, 52, 58 and others)
Alpha
Anogenital SCC SCC of vulva, vagina, cervix, penis, anal area
16, 18, 31, 33, 35, 42 (and others) Alpha
Oropharyn-
SCC of mouth,
16 (18, 31, 33, 35
Alpha
Oropharyngeal SCC SCC of mouth, pharynx 16 (18, 31, 33, 35 and others) Alpha
geal SCC
pharynx
and others)
aHuman papillomavirus (HPV) types in parentheses are found less commonly. AGIN, anogenital intraepithelial neoplasia; AIN, anal and perianal intraepithelial neoplasia; CIN, cervical intraepithelial neoplasia; EV, epidermodysplasia verruciformis; PIN, penile intraepithelial neoplasia; PV, papilloma virus; SCC, squamous cell carcinoma; VaIN, vaginal intraepithelial neoplasia; VIN, vulval intraepithelial neoplasia.
EPIDEMIOLOGY
Infection with HPV occurs throughout the world and in all ages. Benign cutaneous warts are most common in childhood and into the 20s, with 30% to 70% of school-age children having skin warts,7,8 but anogenital warts, which are usually spread via sexual contact, are most common in early adult life. In children, anogenital warts should raise consideration of sexual abuse, although HPV types that cause common warts may often be found in warts of prepubertal children.9
Squamous cell malignancy, associated most strongly with the high-risk anogenital HPV types, usually only develops after an infection has persisted for several years.
3096
Spread of infection can be via direct contact, but the virus particles, released from epithelial surfaces as keratinocytes are shed, can remain present in the environment for an unknown duration and may later lead to infection in another individual.10 Even after infection, it can take months before a visible wart appears.11
After being established, infection can spread on the surface to adjacent skin. Protection against a new infection is via neutralizing antibodies. The anti-HPV vaccines, produced as the L1 capsid protein assembled into virus-like particles, lead to a humoral response against the virus particle. In natural infection, seroconversion also occurs, but in this situation, anti-HPV antibodies are not effective in
Genetic organization of papillomaviruses
E6
E8 E2
E7
E4 L2 L1
E1
E5
Regulatory region Early region Late region
the resolution of established infection. Clearance of the virus from infected tissue is dependent on a cell-mediated immune response, and as yet there is no available, effective therapeutic vaccine. Most warts in children will clear within 2 years,8 but in a minority of otherwise well individuals, warts can spread and persist longer.12
In individuals with long-term immune compromise, especially those with inherited immunodeficiency and transplant recipients receiving high-dose immune suppression, warts and malignancy caused by HPVs can be a major problem. Five years after renal transplant, it is estimated that approximately 90% of patients have warts13 caused by the HPV types that cause warts in healthy people.14 Many other HPV types, mainly from the beta papilloma viruses (PVs), can be detected by polymerase chain reaction (PCR) on the skin (normal or lesional) of transplant recipients.15-17 Using such sensitive methods, these virus types are also found on the skin and in the hair follicles of healthy individuals.18)
SKIN HUMAN PAPILLOMAVIRUS INFECTIONS
CUTANEOUS WARTS
CUTANEOUS WARTS
CLINICAL FEATURES
Viral warts are initially asymptomatic and often unnoticed but grow to form well-defined, thickened, hyperkeratotic lesions (Fig. 167-3). These are often unsightly and may cause pain if sited at pressure points or if they crack and bleed. Walking and use of the hands can be affected according to the site of the warts (Fig. 167-4). Common sites are the hands and feet, especially at areas of minor trauma, such as knuckles or around nails (Fig. 167-5). On the dorsal aspects of hands or feet or on the limbs, warts are exophytic or “cauliflower shaped” (Fig. 167-6), but on soles or palms, they are often relatively flat to the surface with a more
25
3097
25
endophytic growth pattern. The term mosaic warts is applied to a group of small adjacent but relatively flat warts on the sole (Fig. 167-7). Smaller and flatter warts, often on the backs of the hands or face, may be plane warts (also called verruca plana; see Fig. 167-8). On the face and limbs, warts can sometimes have a small base and longer, fingerlike projections, a morphological type called filiform warts (Fig. 167-9). Warts are most common in children and young adults19 but can occur at any age.
ETIOLOGY AND PATHOGENESIS
Common warts are caused most frequently by HPV- 2/27/57, HPV-4, and HPV-1 (soles and palms) and less frequently by HPV-7 (called butcher’s warts). Flat warts are usually caused by type 3 or 10 or very occasionally type 28. Butchers’ warts were originally described in meat workers, whose hands were in direct contact with wet meat. The finding of HPV-7 is not limited to these warts but has been reported rarely in hand warts, face warts, and HIV infection. HPV-1 warts are found only on the palms and soles and may be called myrmecia. They produce higher amounts of new particles compared to other cutaneous types. Some unusual HPV types, HPV-57 and -60, have been found in epidermoid plantar cysts of Japanese patients.20
DIAGNOSIS AND HISTOLOGY
Warts can usually be diagnosed clinically without the need for histologic confirmation. Paring the surface of a
3098
A
B
wart will reveal capillary loops close to the surface and often causes bleeding. These capillaries often thrombose and then appear as black dots (see Fig. 167-3). The histology is of acanthosis, hypergranulosis, and hyperkeratosis of the epidermis. The keratinocytes of the upper granular layer may show koilocytosis with clear cytoplasm and a dense twisted nucleus (Fig. 167-10). Detection of HPV DNA by PCR or in situ hybridization will confirm the diagnosis but is not in use for standard clinical care. The differential diagnoses are listed in Table 167-2.
CLINICAL COURSE, PROGNOSIS, AND MANAGEMENT
Untreated, warts in young people usually clear spontaneously within about 2 years, and only a few remain at 4 years.21 In adults, clearance can often be very slow, with warts persisting for years. Large and widespread warts (Fig. 167-11) are common in immunosuppressed individuals such as transplant recipients and in children or adults with genetic immunodeficiency (Table 167-3). In these cases, large areas of skin may be affected as well as mucous membranes, and the condition may be called generalized verrucosis.22
Treatment can speed clearance in warts but often fails in immunosuppressed individuals. There is no virus-specific anti-viral therapy for warts, so available treatments aim to (1) damage the infected epithelium and debulk the lesions, (2) have some effect on the virus life cycle, or (3) to stimulate an immune response (Table 167-4). It is possible that most treatments may have more than one effect. Recent reviews of treatments for warts give more detail of the
25
COMMON WARTS PLANE WARTS GENITAL WARTS
Seborrheic keratosis Seborrheic keratosis Seborrheic keratosis
Actinic keratosis Actinic keratosis Vulval or penile papillomatosis
Bowen disease Lichen planus Lichen planus
SCC, keratoacanthoma Adenoma sebaceum VIN, PIN, AIN
Acrokeratosis verruciformis Syringomas Verrucous carcinoma
Epidermal naevus Trichoepitheliomas Condyloma acuminatum (secondary syphilis)
Pyogenic granuloma Disseminated superficial actinic porokeratosis
Sebaceous gland hyperplasia
Fish tank granuloma
Verrucous tuberculosis
Callus
Soles and Palms Only
Palmoplantar keratoderma
Corn
Inclusion cyst
Palmar pits (Darier disease, Gorlin syndrome)
Carcinoma cuniculatum
Carcinoma cuniculatum
AIN, anal and perianal intraepithelial neoplasia; PIN, penile intraepithelial neoplasia; SCC, squamous cell carcinoma; VIN, vulval intraepithelial neoplasia.
spectrum and potential efficacy of the range of treatments used today.38–40
The most commonly used treatments for warts are destructive and include topical applications with salicylic acid and physical treatment with cryotherapy. For the greatest effect, treatment needs to be repeated and of long duration. It is worth informing patients that regular treatment for at least 3 months or longer is likely to be required. Even with assiduous treatment, the clearance rate for most common treatments is 60% to 70% compared with 30% clearing with placebo.41
Salicylic acid (12%–17% in a paint or up to 50% in plasters or an ointment) is applied to the wart, which can be rubbed down or pared gently beforehand. Occlusion with an adhesive dressing after application may improve clearance. Daily treatment is recommended, but as the salicylic acid gradually destroys and so removes the keratin layer, the wart or more likely surrounding tissue can become sore, and treatment may need to be reduced in frequency. For this reason, salicylic acid in these strengths is not recommended for facial or anogenital warts.
3099
25
Cryotherapy (see Chap. 206) with liquid nitrogen is best used as a double freeze, repeated every 3 weeks for at least 3 months. This is a painful treatment and often not tolerated to warts around nails, on the soles, or by children. Other treatments that damage or destroy the infected epithelium include caustics such as silver nitrate, phenol, mono- or trichloroacetic acid, and surgical approaches with laser or excisional surgery.
Plane warts require less keratolysis, and treatment with other topical applications such as the immune modulator imiquimod can be effective. Severe proliferative warts may be helped but sometimes only for the duration of the treatment by treatments that reduce or slow epidermal growth, such as podophyllotoxin or retinoids. In immune compromise, clearance of warts, either spontaneously or with treatment, is rare and treatment is usually aimed at measures to reduce wart bulk, maintain function, and avoid pain.
EPIDERMODYSPLASIA VERRUCIFORMIS AND EPIDERMODYSPLASIA VERRUCIFORMIS–LIKE SYNDROMES
EPIDERMODYSPLASIA
VERRUCIFORMIS AND
EPIDERMODYSPLASIA
VERRUCIFORMIS–LIKE
SYNDROMES
CLINICAL FEATURES
Epidermodysplasia verruciformis (EV) is a rare, heritable skin disorder with a mild underlying primary immunodeficiency. The signs of EV become apparent in late childhood or adolescence, but in the absence of a family history, diagnosis may be delayed until a decade or two later. Widespread flaky, scaly, or flat warty lesions are seen on the face, hands, and forearms and other sun-exposed sites (Fig. 167-12). There is often erythema, hyperpigmentation, or more rarely hypopigmentation of lesions, and there can be confusion with pityriasis versicolor and plane warts. In early adult life, actinic keratoses, Bowen disease, and invasive squamous cell carcinoma (SCC) can develop at affected sites (Fig. 167-13). Metastatic disease can follow.
ONSET SYNDROME FEATURES REFERENCES
Infancy SCID, both pre or post bone marrow transplant Warts 23
Infancy Wiskott Aldrich Warts 24
Early childhood Common variable immunodeficiency Warts 25
Early childhood Ataxia-telangiectasia Warts 26
Childhood Bittner syndrome Warts of palms and soles, Bowen disease 27
Childhood or adult GATA-2 deficiency (also called WILD syndrome) Warts, anogenital SCC 28-30
Childhood or adult DOCK-8 deficiency Warts; atopic disease, bacterial and viral infections 31
Childhood or adult Selective IgA deficiency Warts 32
Childhood or adult Intestinal lymphangiectasia, Waldman disease Lymphedema and rarely warts of hands and feet 33
Adult Idiopathic CD4 lymphocytopenia Cutaneous warts, anogenital warts, AGIN, EV-like 34,35
Adult IL-7 deficiency Warts; Cryptococcus meningitis 36
Adult WHIM syndrome Warts, anogenital SCC 37
Adult WHIM syndrome Warts, anogenital SCC 37
3100
AGIN, anogenital intraepithelial neoplasia; EV, epidermodysplasia verruciformis; IgA, immunoglobulin A; SCC, squamous cell carcinoma; SCID, severe combined immunodeficiency; WHIM, warts, hypogammaglobulinemia, immunodeficiency, and myelokathexis.
Treatments Damaging or Destroying the Epitheliuma
Topical Salicylic acid Cantharidin Phenol Monochloroacetic or trichloroacetic acid Silver nitrate 5-Fluorouracil Zinc oxide Retinoid Bleomycin (IL) Physical Cryotherapy Cautery Photodynamic therapy Laser (pulsed dye) Surgical removal
Reduction of Proliferation Retinoid (topical or oral) Podophyllotoxin Cidofovir
Virucidal Formalin Glutaraldehyde
Immune Modulation Imiquimod Diphencyprone or squaric acid topical immunotherapy Immunotherapy with Candida or mumps antigen (IL) Interferon (IL) Zinc sulphate (oral) Cimetidine (oral)
Immune Modulation Imiquimod Diphencyprone or squaric acid topical immunotherapy Immunotherapy with Candida or mumps antigen (IL) Interferon (IL) Zinc sulphate (oral) Cimetidine (oral)
Further details in References 37 to 39. IL, intralesional.
Patients with EV have a mild cell-mediated immune impairment.42 This is often not obvious on clinical grounds because widespread susceptibility to other infections is not a feature but can reduce susceptibility to contact allergy.
25
A clinical appearance very similar to EV, called acquired EV, may be seen after long-term immunocompromise from several causes43,44 (Table 167-5).
ETIOLOGY AND PATHOGENESIS
EV can be inherited, usually with an autosomal recessive pattern. The genes implicated most commonly are EVER-1 and -2, which produce the transmembrane, zinc-containing proteins TMC6 and TMC8.45
A large number of HPV types are associated with EV lesions and the clinically unaffected skin of patients.46 These include HPV-3 and -10, the cause of plane warts, as well as the beta PVs, some of which are found in SCCs and some of which are only found in benign lesions (see Table 167-1). Patients may also have warts harboring the usual HPV types found in common warts.
Transplantation (organ or bone marrow) HIV infection
Less Common Causes Common variable immunodeficiency Coronin-1-A deficiency Connective tissue disease (eg, SLE treated with long-term
Less Common Causes Common variable immunodeficiency Coronin-1-A deficiency Connective tissue disease (eg, SLE treated with long-term immunosuppression) Graft-versus-host disease IgM deficiency Leprosy Lymphoma Myasthenia gravis
immunosuppression) Graft-versus-host disease IgM deficiency Leprosy Lymphoma Myasthenia gravis
3101
IgM, immunoglobulin M; SLE, systemic lupus erythematosus.
25
DIAGNOSIS AND HISTOLOGY
Diagnosis may be made on a combination of clinical features and family history. Skin biopsy shows mild acanthosis and hyperkeratosis. In some lesions, there may also be pallor or clearing of the cytoplasm of the upper spinous layer keratinocytes, called ballooning, with small dense nuclei (so-called clear cells; see Fig. 167-14). With sensitive HPV detection, the beta PVs are found most commonly.
CLINICAL COURSE, PROGNOSIS, AND TREATMENT
Treatments usually make little lasting difference, but short-term, cosmetic improvement can be obtained by a number of approaches that remove the hyperkeratosis.42,43 Cryotherapy, topical salicylic acid, 5-fluorourcil, and imiquimod have all been used with varying results.47,48 Photodynamic therapy (PDT)49 or an oral retinoid, such as acitretin,50 can produce a useful improvement in lesions. To reduce the risk of skin cancers, sun protection is important. Regular surveillance for SCC and early treatment of suspicious lesions may avoid metastatic disease.
SQUAMOUS CELL CARCINOMA AND HUMAN PAPILLOMAVIRUS
SQUAMOUS CELL
CARCINOMA AND HUMAN
PAPILLOMAVIRUS
Common warts in immunocompetent individuals are not forerunners of skin cancer. However, there are a very few reports, usually in the setting of immunosuppression, of long-standing periungual warts progressing into Bowen disease (full-thickness dysplasia) or
3102
invasive SCC.51 In such cases, the high-risk anogenital HPV type, HPV-16, is usually present. Long-standing and slowly enlarging warty areas on the soles, fingers, or anogenital skin can be a feature of carcinoma cuniculatum or verrucous carcinoma (Buschke-Löwenstein tumour), in which the HPV types usually associated with anogenital warts, HPV-6 or -11, are occasionally detected.52,53
Skin SCCs on sun exposed skin are also found to contain a number of EV-related beta HPV types, with a higher yield in the cancers of immunosuppressed individuals. These HPVs are often found in normal skin of both immunocompetent and immunocompromised individuals,16,18 and the exact role they play in the steps of carcinogenesis is still under debate.54
MUCOSAL AND PERI-MUCOSAL HUMAN PAPILLOMAVIRUS INFECTIONS
ANOGENITAL WARTS
ANOGENITAL WARTS
CLINICAL FEATURES
Warts can affect the vulva, vagina, cervix, penis, scrotum, perianal skin, and anal canal. They may present singly but are usually found as multiple, well-defined papules or as flat or filiform lesions and may grow into larger protuberant lesions (Fig. 167-15). The moist fold beneath an abdominal apron of an obese patient is another site for these warts.55 On mucosal surfaces, they are often macerated and appear pale, but on drier skin, they can become more obviously hyperkeratotic and hard. They may be asymptomatic but can be itchy and uncomfortable and may be traumatized with movement or sexual activity.
DIAGNOSIS
HPV-6 or -11 are the most common causative agents, but other HPV types are found with PCR analysis. Anogenital warts produce less virus particles than cutaneous warts. For differential diagnosis, see Table 167-2.
CLINICAL COURSE, PROGNOSIS, AND TREATMENT
Anogenital warts are usually treated with a topical application as first-line therapy.56 Podophyllotoxin or imiquimod are both self-applied treatments with a 50% to 70% clearance rate.57 Recurrence rates after imiquimod treatment are slightly less than after podophyllotoxin.58
B
A
C
25
D
Other treatments in use include topical trichloroacetic acid,59 sinecatechins from green tea,60 and physical therapies with cryotherapy, PDT, laser, electrocautery, or surgery. Since the introduction of the quadrivalent anti-HPV vaccine in 2007, there has been a recorded decrease in presentation of genital warts or prevalence of HPV-6 and -11.61,62
ORAL WARTS
ORAL WARTS
Warts can develop on the lips, in the oral cavity, and in upper respiratory tract and are usually regarded as a sexually transmitted disease. Because of the moist site, they are usually macerated and can be flat or cauliflower shaped (Fig. 167-16). The low-risk genital HPV types are the usual cause. Laryngeal warts (laryngeal papillomatosis) can develop in childhood, probably caused by infection from the mother at birth, and can affect speech and breathing. Oral warts are common in HIV infection and may worsen, rather than improve, during antiretroviral therapy.63
ANOGENITAL INTRAEPITHELIAL NEOPLASIA AND CANCER
ANOGENITAL
INTRAEPITHELIAL
NEOPLASIA AND CANCER
CLINICAL FEATURES
Anogenital intraepithelial neoplasia (AGIN) includes dysplasia of the vulva (vulvar intraepithelial neoplasia; see Fig. 167-17), vagina (vaginal intraepithelial neoplasia), cervix (cervical intraepithelial neoplasia), penis (penile intraepithelial neoplasia), perianal skin, and anal canal (anal intraepithelial neoplasia). The term Bowenoid papulosis has been used to describe the disorder, especially when the lesions are pigmented and resemble seborrheic keratosis. AGIN may also present with velvety plaques, white macerated, warty lesions or less distinct erythematous areas.64
ETIOLOGY
The high risk HPV types, especially HPV-16, are associated with these disorders.
3103
25
Biopsy is essential for diagnosis with the histology showing full-thickness epidermal dysplasia, classified as undifferentiated intraepithelial neoplasia. Differentiated intraepithelial neoplasia occurs in association with chronic inflammatory genital disease, such as lichen sclerosus, and histologically is a subtler basal dysplasia, often with acanthosis and hyperkeratosis, and is not associated with HPV infection (see Chap. 64).
CLINICAL COURSE, PROGNOSIS, AND MANAGEMENT
Surgery is the treatment of choice for single lesions if the site is easily operable but may not be best for multifocal or multicentric disease. Laser or topical immunotherapy with imiquimod offers an alternative approach.65 Both the patient and physician need to be aware of the changes that could indicate malignant change, and these include a persistent area of discomfort, an ulcer, or a frank tumor. It is estimated that an individual with AGIN has an approximate 5% lifetime risk of developing cancer. Cancer can be the presenting feature.
3104
ORAL AND OROPHARYNGEAL SQUAMOUS CELL CARCINOMA
ORAL AND
OROPHARYNGEAL
SQUAMOUS CELL
CARCINOMA
Silent infection with high risk HPVs within the mouth or throat can present later in life with oropharyngeal SCC. The traditional association of this malignancy with smoking and alcohol is being replaced with a stronger association with HPV infection, especially in younger male patients. The incidence of this malignancy is rising but should be reduced following the introduction of the anti-HPV vaccine to male patients.66
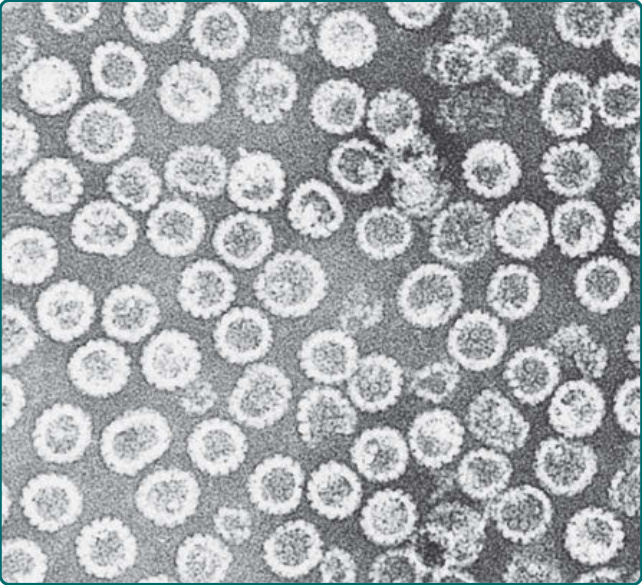
Figure 167-1 Papillomavirus virus–like particles. Transmission electron micrograph of human papillomavirus type 16 virus–like particles composed of the L1 and L2 proteins. These proteins were synthesized in cell culture and selfassembled into 55-nm particles that are morphologically similar to natural infectious virus except that they do not contain the viral DNA. The particles in the electron micrograph were purified from the cells. (Micrograph used with permission from Heather Greenstone. Courtesy of Prof. Elliot Androphy.)
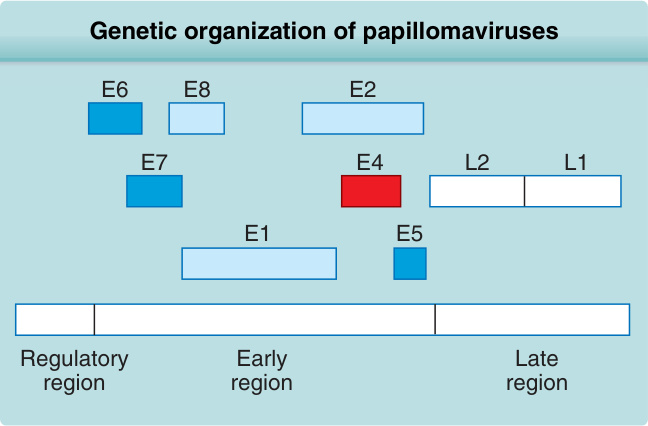
Figure 167-2 Genetic organization of papillomaviruses. The circular human papillomavirus genome of approximately 8000 nucleotide base pairs is represented here as a linear strand. (Used with permission from Prof. Elliot Androphy.)
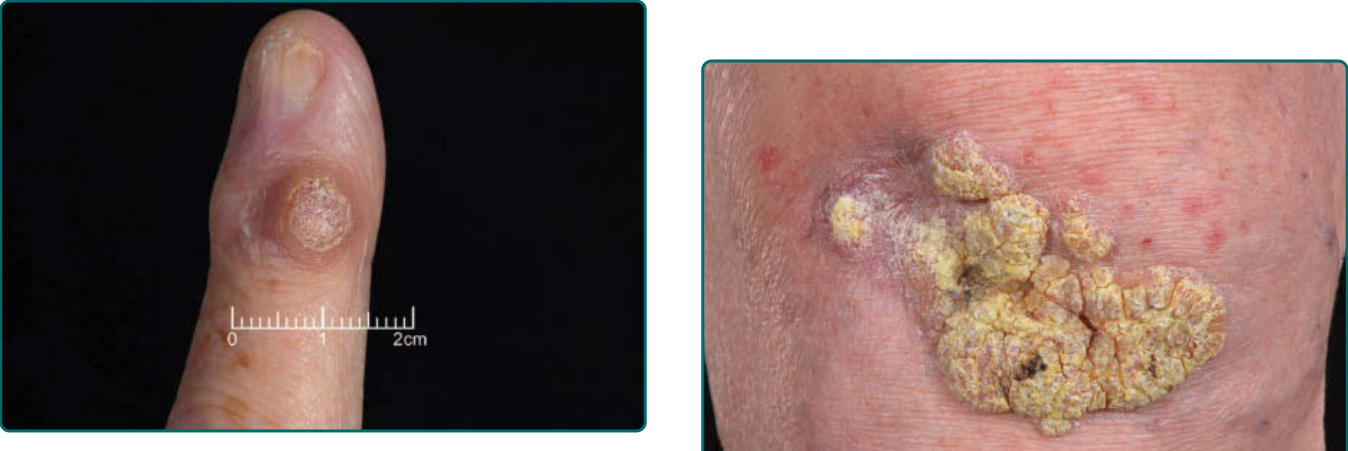
Figure 167-3 Well-defined wart on the finger. Small thrombosed capillaries are visible as black dots. (The nail had been damaged previously from trauma.)

Figure 167-4 Very hyperkeratotic warts over the Achilles tendon.

Figure 167-5 Multiple warts on the hand with periungual warts affecting nail growth.

Figure 167-6 Warts on the knee.

Figure 167-7 Mosaic warts on the sole.

Figure 167-8 Plane warts (verruca plana). A, Multiple pink flat warts on the face of an 11-year-old girl. B, Many flattopped papules occur in a linear configuration resulting from self-inoculation. (Used with permission from Prof. Elliot Androphy.)

Figure 167-9 Common warts. Filiform warts on the chin and lips of a child. (Used with permission from Prof. Elliot Androphy.)
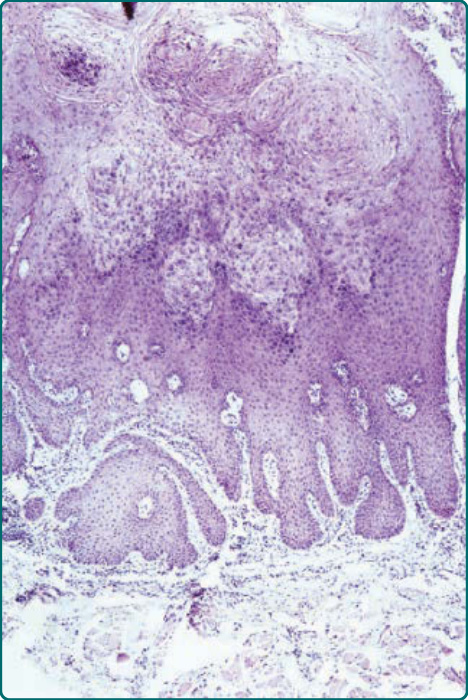
Figure 167-10 Verruca vulgaris. The process is one of extensive hyperplasia, and the hyperplastic cells contain both intranuclear and intracytoplasmic inclusion bodies. (Used with permission from Prof. Elliot Androphy.)

Figure 167-11 Leg with numerous warts. The large, scaly, and horny warts contain human papillomavirus (HPV)-
2. The smaller, flatter, less scaly papules are warts that contain HPV-3. With extensive warts such as these, an assessment of immune function is indicated. (Used with permission from Prof. Elliot Androphy.)

Figure 167-12 Epidermodysplasia verruciformis. Plane wart–like lesions on the dorsa of the hands and forearms associated with human papillomavirus-5 and -8. The lesions are numerous, flat, reddish, and partly confluent. (Used with permission from Prof. Elliot Androphy.)

Figure 167-13 Invasive cancer in an epidermodysplasia verruciformis patient infected with numerous human papillomavirus (HPV) types, including HPV-5, -8, -9, -14, and others. In the tumor cells, HPV-5 DNA was detected in a high copy number. This large squamous cell carcinoma did not metastasize and did not recur after surgery. There are numerous actinic keratoses on the forehead. (Used with permission from Prof. Elliot Androphy.)
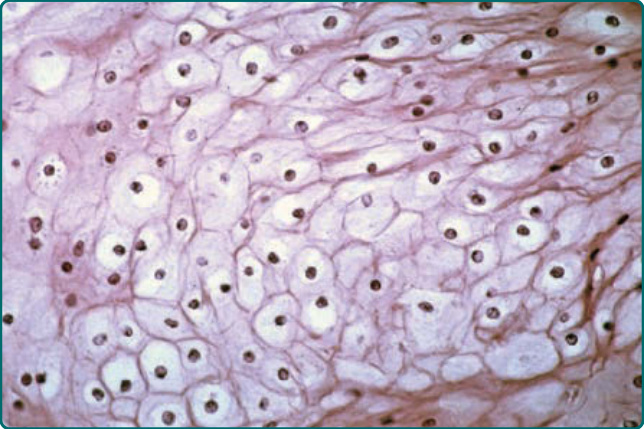
Figure 167-14 Characteristic cytopathic effect of epidermodysplasia verruciformis–specific human papillomavirus (HPV) in a patient found to be infected with HPV-5, -8, and -9. Very abundant clear large cells with small pyknotic nuclei replace almost the entire epidermis. (Used with permission from Prof. Elliot Androphy.)

Figure 167-15 Mucosal warts. A, Multiple condylomata acuminata on the shaft of the penis. B, Erythroplasia of the glans with exophytic squamous cell carcinoma extending onto prepuce. C, Multiple perianal condylomata in a child. Sexual abuse must be considered. D, Multiple confluent condylomata on the labia minora, majora, and fourchette. (Images A, C, Used with permission from Prof. Elliot Androphy. Image B, Used with permission from Reinhard Kirnbauer, MD.)

Figure 167-16 Multiple mucosal warts extending to the vermillion border, where they become highly keratinized. (Used with permission from Prof. Elliot Androphy.)

Figure 167-17 Vulval intraepithelial neoplasia, grade III. Small area of raised and minimally pigmented skin near the posterior fourchette.
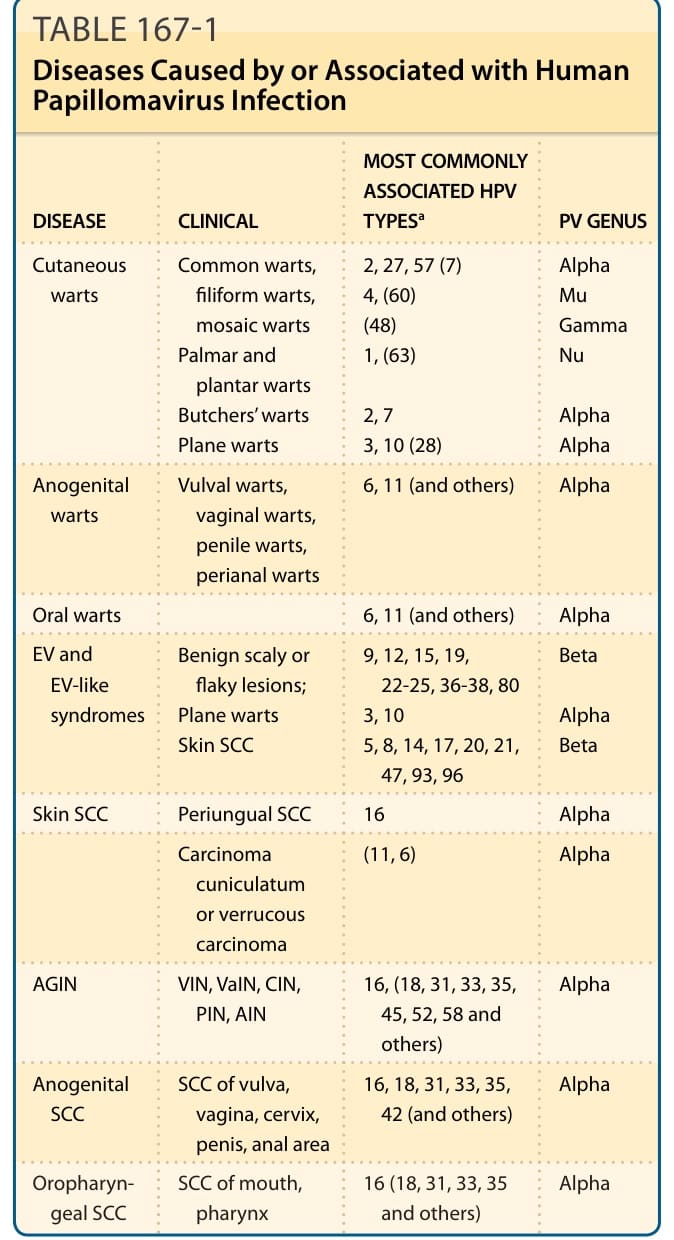
TABLE 167-1 Diseases Caused by or Associated with Human Papillomavirus Infection
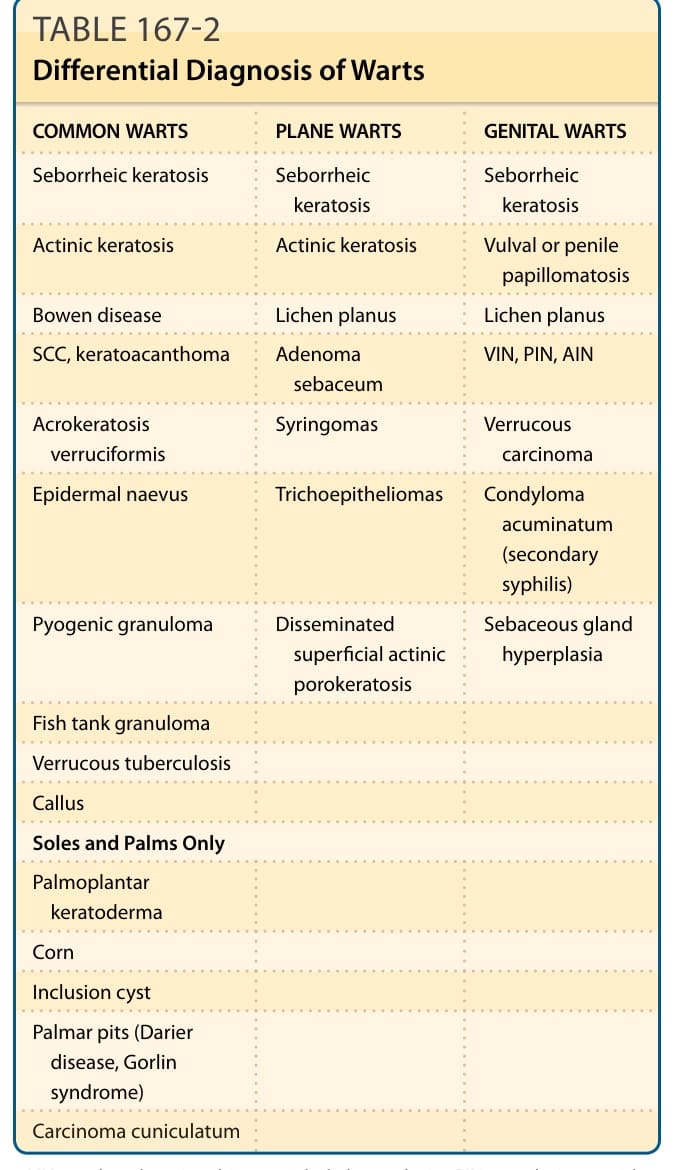
TABLE 167-2 Differential Diagnosis of Warts
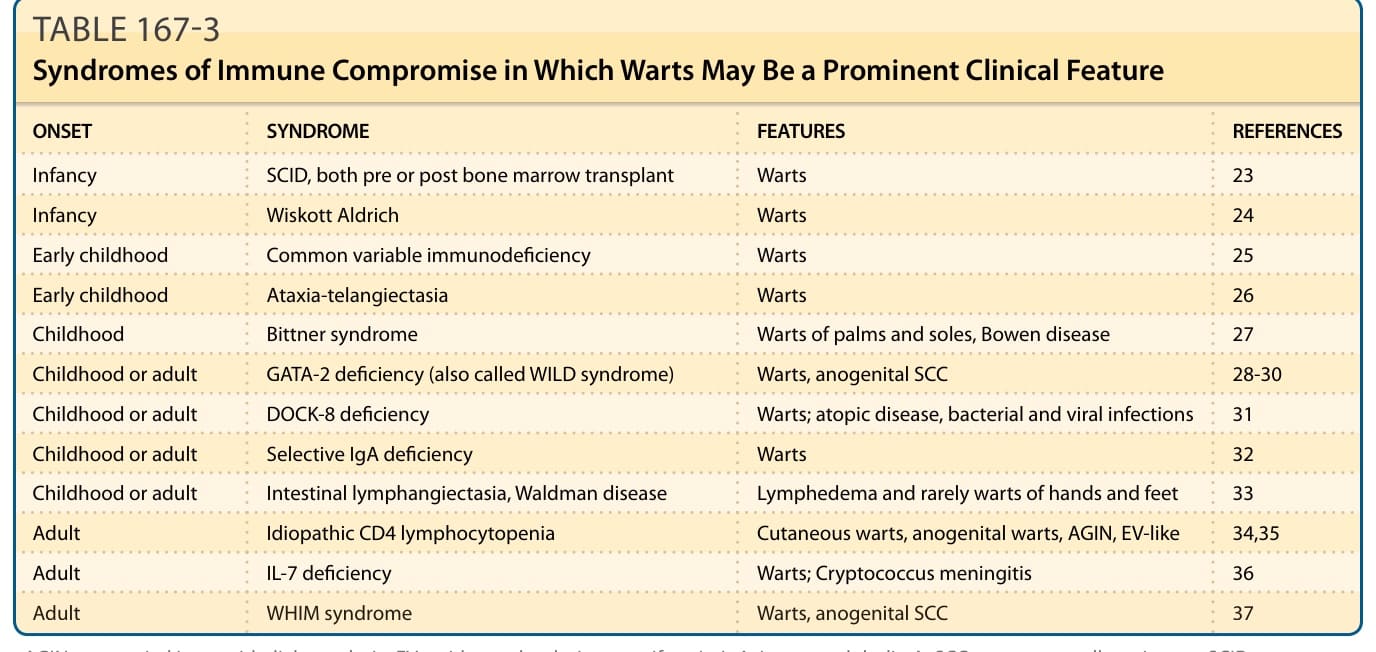
TABLE 167-3 Syndromes of Immune Compromise in Which Warts May Be a Prominent Clinical Feature
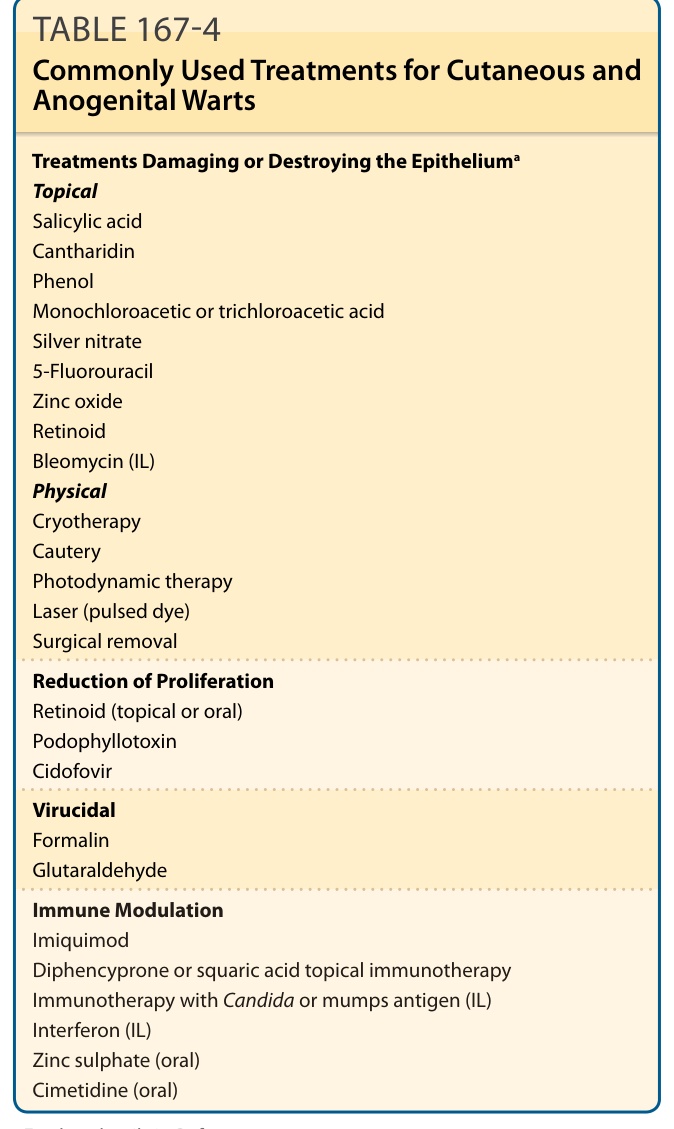
TABLE 167-4 Commonly Used Treatments for Cutaneous and Anogenital Warts
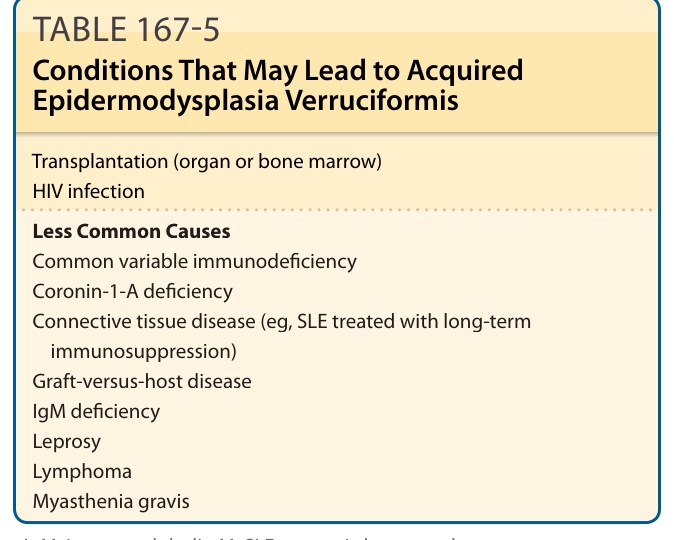
TABLE 167-5 Conditions That May Lead to Acquired Epidermodysplasia Verruciformis